CONTRACEPTION Associate Prof Dr Hanifullah Khan ultrasound scan of IUCD in situ

CONTRACEPTION OVERVIEW
Dec 02, 2014
A short overview of contraceptive methods and the philosophy behind their use.
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
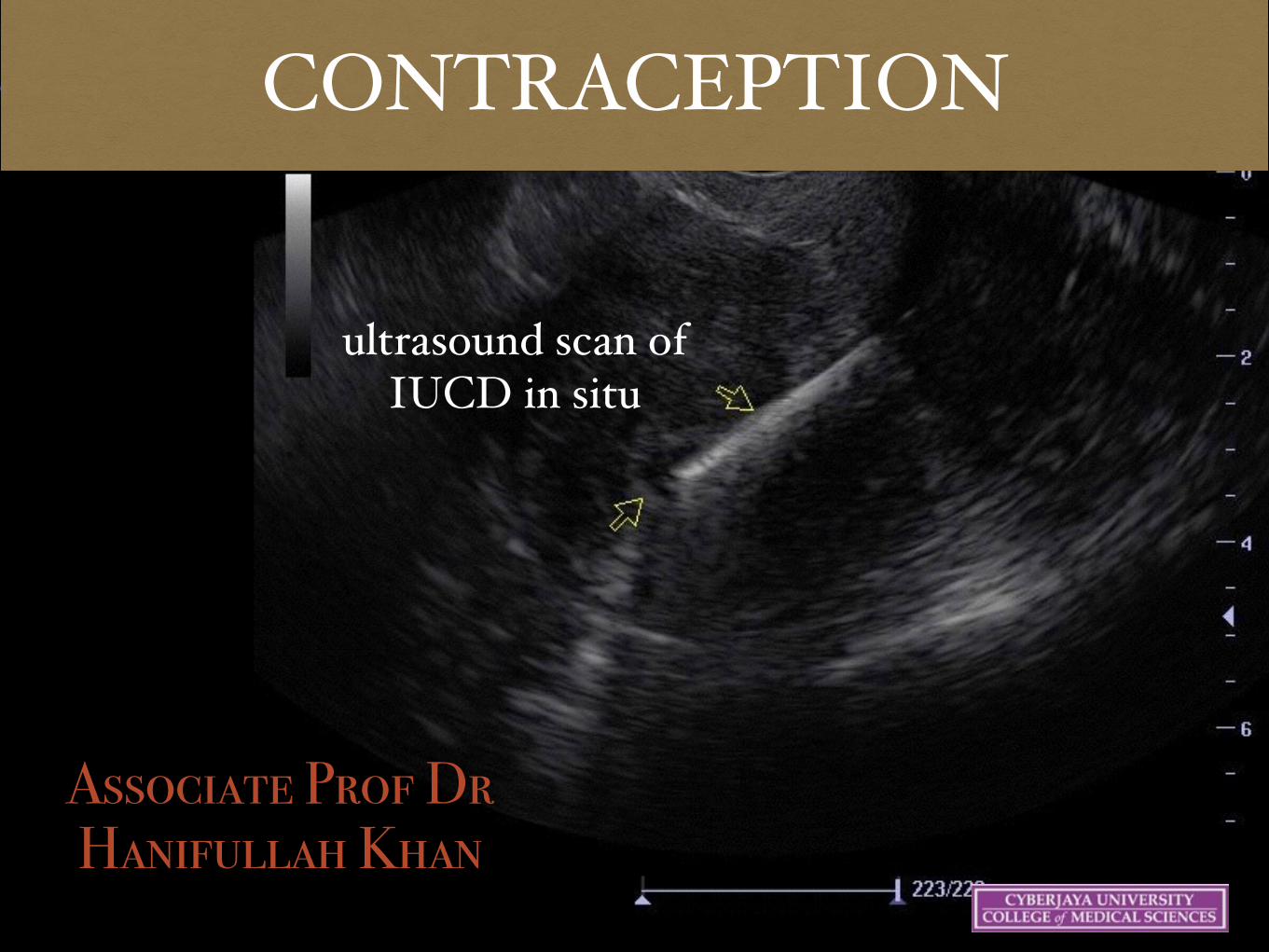
CONTRACEPTION
Associate Prof Dr Hanifullah Khan
ultrasound scan of IUCD in situ

Objectives
Understand the definition, classification & terminology
Understand the reason for contraception
Know the advantages & side-effects
Know the proper use of each method
To be able to advise on the use
19 May 07 3
Introduction
Definition – any method used to prevent pregnancy
• Allows to choose whether & when to
have a child

19 May 07 4
Reproduction
Ovulation
Fertile period
Fertilisation
!

7 June 2006 8
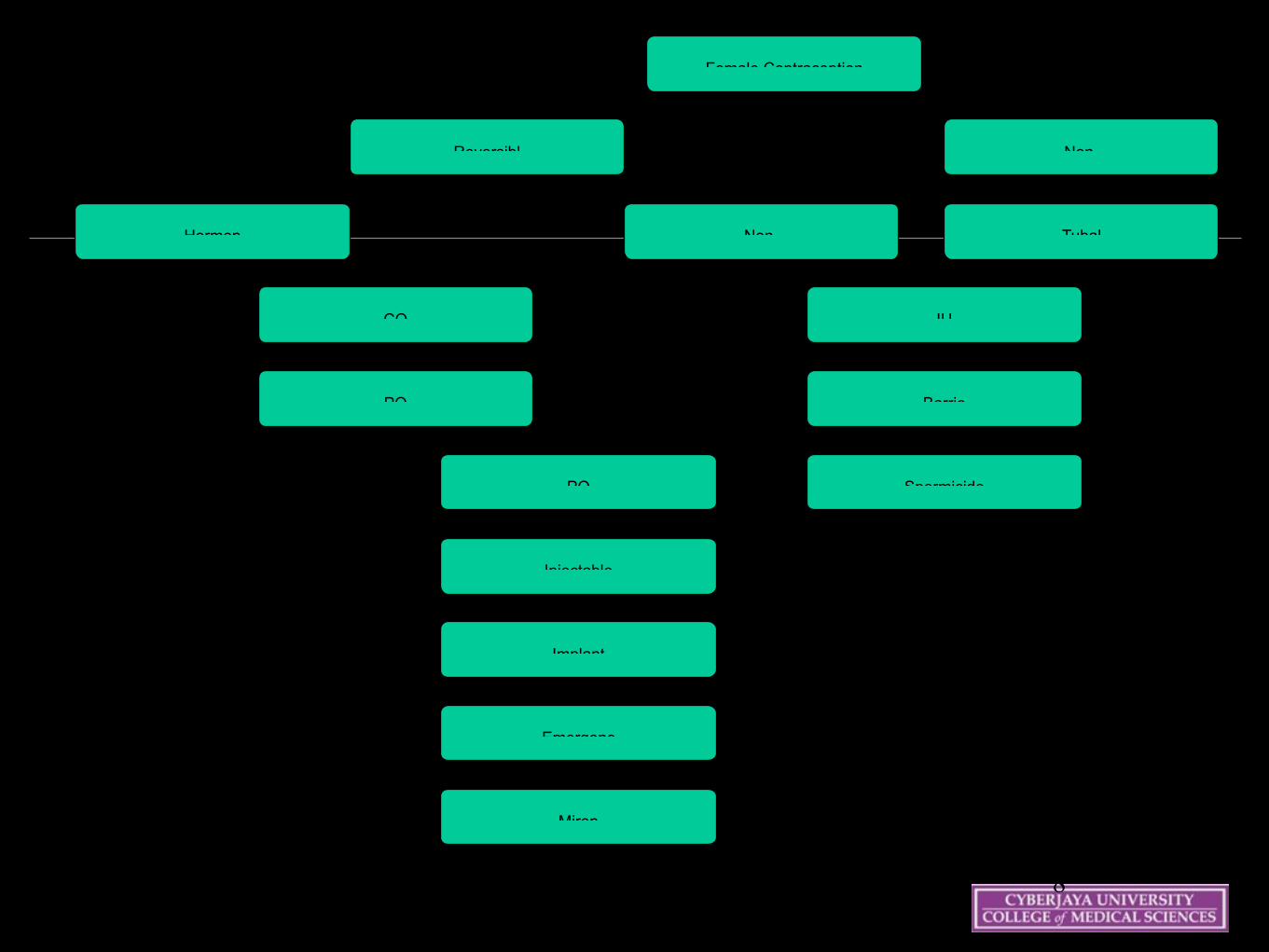
Female Contraception
Reversibl Non-
Hormon Non-
CO
PO
IU
Barrie
Spermicide
Tubal
PO
Injectable
Implant
Emergenc
Miren

COMBINED CONTRACEPTION
• BENEFICIAL EFFECTS ON FUTURE FERTILITY
– ↓ ASCENDING INFECTION & PID (PROGESTOGENIC EFFECT)

PROGESTOGEN ONLY CONTRACEPTION
● POP ● SUBDERMAL
IMPLANTS ● INJECTABLES ● COMBINED
INJECTABLES ● EMERGENCY
CONTRACEPTION



Emergency Contraception Levonorgestrel 0.15 mg +ethinyl estradio
Nordette (light orange tablets)
4 tablets/dose
2 doses
Levonorgestrel 0.75 mg
Plan B 1 tablet/dose
2 doses First dose within 72 hours of unprotected intercourse; second dose
• COPPER-CONTAINING
INTRAUTERINE DEVICE (IUD)
INSERTED WITHIN 120 HOURS OF
UNPROTECTED INTERCOURSE TO
PREVENT PREGNANCY
• A SHORT COURSE
– EITHER A HIGH-DOSE
COMBINATION OF ESTROGEN & PROGESTIN OR
– PROGESTIN-ONLY
– USED WITHIN 72 HOURS OF
UNPROTECTED INTERCOURSE TO PREVENT PREGNANCY
• TAKEN AFTER SI BUT BEFORE
IMPLANTATION • MORE
EFFECTIVE THE SOONER THEY ARE INITIATED
AFTER SI.

Wednesday 15 October 2003 25
NATURAL METHODS
Avoid sex at the fertile times
Unsuitable for:
Women who can't check their temperature and cervix every day
Couples who are even slightly disorganised
Women with very irregular periods
!
!

Wednesday 15 October 2003 28
Methods
Coitus Interruptus
Rhythm Method
Calendar
BBT
Cervical Mucous (Ovulation)
Symptothermal
Ovulation Predictor Kits
Abstinence
Lactational Amenorrhoea Method

Wednesday 15 October 2003 38
Shortest cycle (S) minus 18 = Last infertile day of the pre-ovulatory phase
Longest cycle (L) minus 11 = Last fertile day
For example:- Length of cycles during last six months = 28, 29, 28, 27, 30, 28
(S = 27) S - 18 = Last infertile day 27 - 18 = 9
(L = 30) L - 11 = Last fertile day 30 - 11 = 19

Wednesday 15 October 2003 39
Basal Body Temperature Method
Keeping track of body temperature
Body temperature rises two days prior to ovulation.

Wednesday 15 October 2003 42
Ovulation (Billing) Method
Requires feeling and observing the cervical mucus to determine the time of ovulation.
Note the production of clear, watery mucus in the days immediately before ovulation
To avoid pregnancy, intercourse is avoided for several days following change in the color and consistency of cervical mucus.

Wednesday 15 October 2003 45
Sensation at Vulva Finger Test Appearance
Moist orSticky
Early Mucus Scanty Thick WhiteSticky Holds its shape
Wetter
Transitional Mucus Increasing Amounts Thinner Cloudy Slightly Stretchy
Slippery
Highly Fertile Mucus ProfuseThin TransparentStretchy (like raw egg white)

Wednesday 15 October 2003 46
Mucus changes throughout the cycle
Complete cycle showing typical pattern of menstruation, pre-ovulatory dry days, mucus days with increasingly fertile characteristics approaching peak day, the abrupt change back to less fertile characteristics, the count of four after peak day and post-ovulatory dry days

Wednesday 15 October 2003 48
Interpretation of the Sympto-Thermal Chart
This sympto-thermal chart shows the correlation between all indicators of fertility

Wednesday 15 October 2003 49
Fertility Chart

Wednesday 15 October 2003 50
Ovulation Predictor Kits
used to test urine to identify hormones that indicate ovulation is about to occur
electronic fertility computer tells a woman which days she is fertile
Persona: fertile days are indicated with a red light and infertile days with a green light
failure rate as low as 6% among women who abstain on fertile days as indicated by the device

Wednesday 15 October 2003 57
LAM
Conditions to be fulfilled
Fully BF
No periods
Recommended up to 6 months - the longer LAM is used, the more likely it is that ovulation will precede the first menses

INTRAUTERINE DEVICES

Copper IUDs: Mechanisms of Action
Interfere with reproductive process before ova reach
uterine cavity
Thicken cervical mucus
Interfere with ability of sperm to pass through
uterine cavity
Change endometrial lining
IUDs: Who Should Not Use (WHO Class 4)
IUDs should not be used if woman:
Is pregnant (known or suspected)
Has unexplained vaginal bleeding until the cause is determined and any serious problems are treated
Has current, recent PID
Has acute purulent (pus-like) discharge
Has distorted uterine cavity
Has malignant trophoblast disease
Has genital tract cancer
Has an active genital tract infection (e.g., vaginitis, cervicitis)19 May 07 67Source: WHO 1996.

19 May 07 68
IUDs: Common Side Effects
Copper-releasing:
Heavier menstrual bleeding
Irregular or heavy vaginal bleeding
Intermenstrual cramps
Increased menstrual cramping or pain
Vaginal discharge
Progestin-releasing:
Amenorrhea or very light menstrual bleeding/spotting

19 May 07 69
IUDs: Possible Other Problems
Missing strings
Slight increased risk of pelvic infection (up to 20 days after insertion)
Perforation of the uterus (rare)
Spontaneous expulsion
Ectopic pregnancy
Spontaneous abortion
Partner complains about feeling strings

19 May 07 79
Failure rates
Implants, IUDs and LNG-IUS - <1% #
Contraceptive pills - 5% #
Male condoms - 14% #
Diaphragm with spermicide - 20% #
Cap with spermicide - 20-40% #
'Natural' methods - 35% #
Withdrawal - 19%


KEY POINTS
Contraception provides an effective means to plan a family
Many methods are available -
suitability has to be decided based on a proper history & examination
Pregnancy should be ruled out first
You should know the advantages & side effects
Contraception also provides non-contraceptive benefits

Further reading
Cleland et al. Family Planning as a cost saving preventive health service. NEJM April 20, 2011.
Trussell J. Update on the cost effectiveness of contraceptives in the United States. Contraception 2010;82:391.
!

Related Documents











