BRONCHOPNEUMONIA

BRONCHOPNEUMONIA. Bronchopneumonia = acute inflammatory process in the area of respiratory bronchioli, alveolar structures and/or lung interstitium caused.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
BRONCHOPNEUMONIA

Bronchopneumonia• = acute inflammatory
process in the area of respiratory bronchioli, alveolar structures and/or lung interstitium
• caused by espec. infectious agent
• complications: pleuritis, parapneumonic empyema, lung abscess, lung gangrene and sepsis
• risk factors: age, CV and respiratory comorbidities, smoking, immunodeficiency
• = mortality over 70 yr. to 25%!
• Division according to agent: viral bacterial mycotic parasitic
• Division of clinical terms: CAP – community HAP – hospital acquired pneumonia
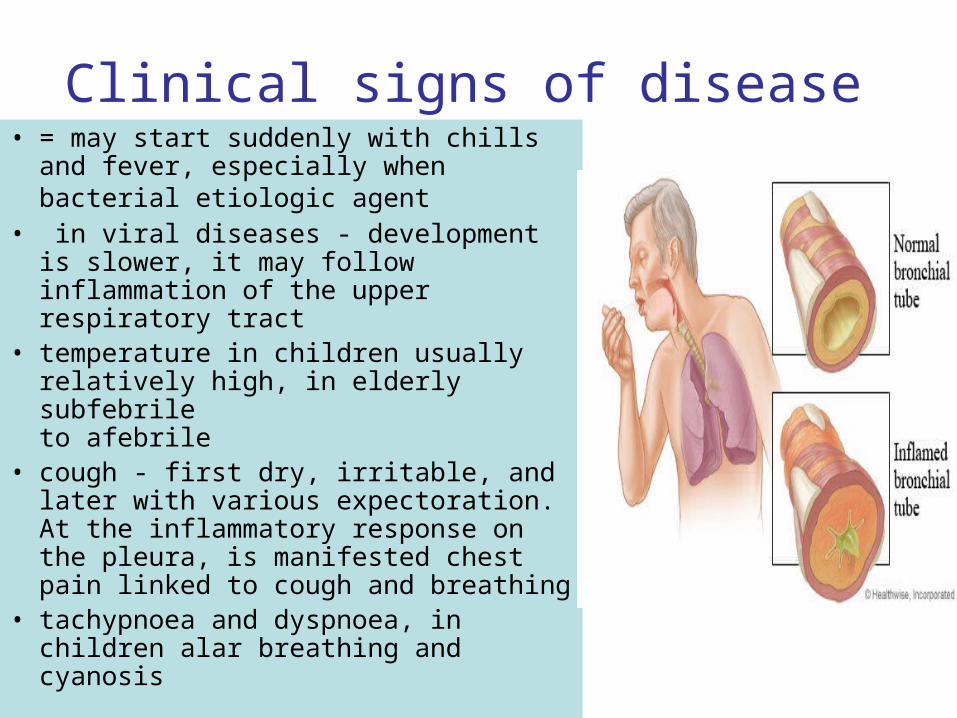
Clinical signs of disease• = may start suddenly with chills and
fever, especially when bacterial etiologic agent
• in viral diseases - development is slower, it may follow inflammation of the upper respiratory tract
• temperature in children usually relatively high, in elderly subfebrileto afebrile
• cough - first dry, irritable, and later with various expectoration. At the inflammatory response on the pleura, is manifested chest pain linked to cough and breathing
• tachypnoea and dyspnoea, in children alar breathing and cyanosis

Therapy of Bronchopneumonia
• immediately begin initial empirical anti-infective therapy, with the spectrum of effect covering the most prevailing pathogens, also taking into account individual risk factors
• knowledge of the epidemiological situation + resistance of respiratory pathogens to antibiotics in the region
• antimicrobial therapy should be directed = necessity to determine etiology and sensitivity of microorganisms to antibiotics /after identification of the pathogen, initial therapy adequately adjusted /
+ bronchodilators
mucolytics
expectorances
antitussics
+ rest in bedfluid intakecalories intake vitamin intake
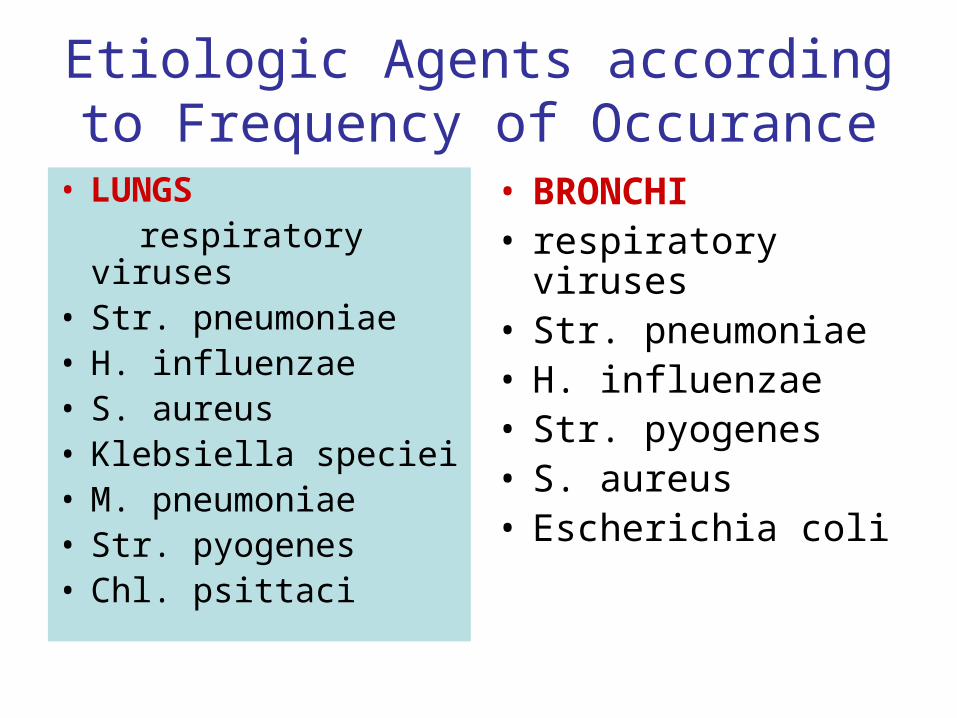
Etiologic Agents according to Frequency of Occurance
• LUNGS respiratory viruses • Str. pneumoniae • H. influenzae • S. aureus • Klebsiella speciei • M. pneumoniae • Str. pyogenes • Chl. psittaci
• BRONCHI• respiratory viruses • Str. pneumoniae • H. influenzae • Str. pyogenes • S. aureus • Escherichia coli
Antimicrobial Drugs
• with targeted mechanism affect the structure or function of microorganism cells, and thus they either kill - bactericidal effect, or inhibit their growth and multiplication - bacteriostatic effect/immunodeficiency and cachect. patients! /
• selective action on the cells of microorganisms:effect on the synthesis of cell wall - bactericideffect on protein and NA synthesis + inhibition of metabolic procedures – bacteriostatic

Division of Antimicrob. Substances
• chemical – according to similar structure, substance with the same mechanism of action have usually the same AE
• baktericid: ß-laktamic ATB, aminoglycosides, bacitracin, isoniazid, metronidazole, quinolones, vancomycin, teicoplanin, rifampin
• bacteriostatic: macrolides, tetracyclines, chloramphenicol, sulfonamides, trimetoprim, linkomycin, klindamycin, ethambutol, nitrofurantoin

Ideal Antibiotic• Wide spectrum• Rapid action• Bactericid• High selectivity, without AE, not causing
allergy• Not to occur resistance• High biologiavailability, good penetration
to tissues, long biolog. half-life• Low price
Choice of Antimicrobial Substance
• Ideal antibiotic drug• absorption• distribution • elimination • ADR • price
• Which available ATB is close to ideal?
• ß-lactams • Macrolides • Quinolones • Tetracyclines • Cotrimoxazol
Principles of Antimicrob. Therapy for Respiratory Diseases
• racional indication • take into account the nature and severity of
infection• take into consideration the clinical condition of the
patient• Individual choice of drug • prevent the increase in resistance due to :
– incorrect prescription – incorrect dosage – not keeping the optimal length of therapy
Choice of the Right Antibiotic
• Targeted administration on the basis of identification of causative agent of infection
• Consider pharmacokinetic properties • Choosing the most appropriate route of
administration and site of administration. At severe infections we begin with parenteral therapy. At limited function of elimination organs we reduce the dose or prolong dosing interval
• Reducing the risk of administration by revealing of predisposing factors such as drug allergy
• Determination of the risk groups of patients

Problematic of ATB Resistance• = the ability of the bacterial population to survive
inhibitory concentration of the given antimicrobial drug, becomes a significant problem nowadays
1. Primary resistance = natural resistance of microbial species, which are outside the range of ATB action /missing are „mechanisms“ (receptors) for the effect of antimicrobial drugs/ absolut resistance + relevant resistance /mikroorganism not sensitive to antibiotic concentrations reachable in human organism, but sensitive to high concentration of antibiotic reached in vitro
2. Secondary resistance occurs during antibiotic therapy, when initially sensitive bacterial population during antibiotic treatment become resistant to them.
Resistance to ATB
mechanism of resistance:- productions of enzymes, which change structure ofantimicrob. substance the way that it loosesantimicrobial effect- mutation changes on the level of intracelular recep./betalact. ATB – structure change of binding place forPNC/ - preventing penetration of ATB through cell wall /making impossible binding of ATB to the site of action on intracel.rec./ - change of metabolic pathway

Possibilities of Slowing Down Resistance Appearance
• the right choice of antimicrobial drug
• optimal and enough long administration
• right dose
• in special cases stable combinations /treatment of TBC/
Development of Actual Resistance
• Penicillin resistant pneumococs (PRP)
• Meticillin resistant staphylococs (MRSA)
• CA-MRSA (Community-Associated Methicillin-Resistant Staphylococcus Aureus)
• Streptococcus pyogenes/macrolides
• Quinolone resistant E. coli
Agents Causing Pneumonia of Adults
lobal: S. pneumoniae, H. influenzae, K. pneumoniae
bronchopneumonia: S. pneumoniae, S. aureus, L. pneumophilla
atypical: influensa virus, RSV, adenoviruses, HZV, Mycoplasma pneumoniae, Chlamydia pneumoniae
Pharmacotherapy of Bronchopneumonia Caused by Streptococcus pneumoniae
• Aminopenicillins at high doses
• Aminopenicillins protected with inhibitors of betalactamases /ampicillin-sulbactam, amoxicillin-clavulanic acid/
• Cephalosporins III. generation
• Fluoroquinolones /levofloxacin, moxifloxacin/ = advantage is higher concentration in the site of action /alveol. fluid, macrophages/ than in plasma!
Betalactamic Antibiotics- in structure betalactamic circle- bactericid- inhibit synthesis of cell wall of mikroorganisms in the last
phase of its consolidation with peptidoglycan- hydrophil- low direct toxicity- low occurance of AE- spectrum of effect depends on substance- here belong PNC cephalosporins monobactams carbapenems

Penicillins• absorption of peroral PNC after p.o.
administration better from empty stomach• G-penicillin, meticillin, carboxypenicillin,
ureidopenicillin – unstable in acid environment of stomach - administration parenteral
• don´t cross intracelullarly, metabolised a little, excreted through kidneys through glom. filtr. and also tubul. secretion, high concentrations reached in urine
• minimal AE, also in high doses not toxic, allergy 5-8%
• resistance: enzyme type – betalactamases + mutations – not letting to recognise of recept.
site

PNC with Narrow SpectrumBenzylpenicillin – natural PNC, acidolabile, only parent.mainly g+, streptococci, pneumococci, meningococcimedium serious inf. caused mailnly by betahaemol. streptococciserious infections – high plasmat. concentrations of Na or K salts of crystalic PNC i.v. /renal diseases!/ depot preparations – i.m.- Procain PNC – 2 times per day 1g
Penicillin V – biosynthet., acidostable, g+ microorg., identicaleffect spectrum, lower plasm. concentration – mild streptoc.infections and their healing Penamecillin – prolonged effect, á 8h.
Oxacillin, cloxacillin, dicloxacillin, meticillinantistaphylococcal, resistant against betalactamases produced by staphylococci, very narrow spectrum, peroral also perenteral administration, á 4 till 6 h.

PNC with Broader Spectrum- also G- microorg./E. coli, salmonellas, shigellas, H. influensae/
Aminopenicillins - ampicillin, amoxicillin /=better penetration, higher plasm. conc./ acidostable, aren´t resistant againstnie betalactam.uncomplic. infections of urinary,airway and gallbladder pathways mainly in combination with inhibitors of betalactamases, peror. also parent. admin.
Carboxypenicillins /carbenicillin, tikarcillin/ semisynthet. PNC, also Pseudomonas aeruginosa, Proteus - at syst.infections alone or in combination with aminoglykosides acidolabile – parenter. adm., tikarcillin in comb. with inh. of betalactamases
Ureidopenicillins /azlocillin, mezlocillin, piperacillin/acidolabile, good penetration to tissues, more intensive on Proteus,Pseudomonas aeruginosa, piperacillin also to some anaerobes,the highest effectivity, reserved to serious infections
Cephalosporines
• similar mechanism of action as PNC• wide use, in pediatria and geriatria• good efficacy and low toxicity • good penetration to tissues• excretion through kidneys by glom. filtr., tub.
secretion• according to pharmacodynamic – spectrum of
efficacy, ability to penetrate to cells, stability against betalactamases - 4th generation
Cephalosporins of 1st and 2nd Generation
1st generation
cefalotin, cefazolin, cephalexin,cefradil
narrow spectrum, against G+/also staphylococci/,
G-sticks, airway, urinary and skin infections
2nd generation
cefoxitin, cefaclor, cefamandol
expanded spectrum to G-bact., resistant against
betalactamases, act against H. influenzae +
some anaerobes, less against staphylococci
Cephalosporins of 3rd and 4th Generation
3rd generation cefotaxime, ceftazidime, ceftriaxon,empir. treatment of severe life threatening infectionstargeted treatment of microorg. resist. to PNC andceph. of lower gen. - parent. adm. - oft aplicationinfections of airways – p.o. – 1 times per day4th generation cefepime, cefpiromintensified effect against staphyloc.,streptococci and pseudomonads severe nosocomial infections

Rezistance of Pneumococci to Antibiotics
• increase of rezistance to pneumococci to natural penicillins, also to cephalosporins, macrolides, doxycycline = drug-resistant Streptococcus pneumoniae
• risk factors of occurance: age over 65 years ATB therapy in last 3 months
immunodeficiency comorbidities

Fluoroquinolones• chemotherapeutic with high ATB activity• baktericid effect – select. inh. of bacterial gyrase activity
and so inhibiton of the replication of bacterial DNA• resistance – mutation of DNA gyrase • fluor – increased efficacy, better kinetic properties – use at
systemic infections, also serious, serious nosocomial pneumonias, uroinfections, gynecol. infections, GIT infections, infections of airways
• good absorption after peror. administration, some also parenter. administration /ciprofloxacin/, possible parenteral. starting therapy, than peroral administration
• good penetration to soft tissues, bones and lungs
Levofloxacin • high bioavailability • good penetration to bronchial mucosa and lung
parenchyma• at middle serious and serious inf. of airways, complic.
uroinfections, inf. of skin and soft tissues • interactions at absorption are occuring at
simultaneous administration of iron salts, or antacides containing magnesium and alluminium
• „respiratory quinolone“ – effect on G+ causative agents of respiratory infections
• AE: nausea, diarrhoea, increases hepatic enzymes

Moxifloxacin
• fast perfect absorption after peroral administration, quickly distributed to extravasc. space
• at metabolism doesn´t undergo oxidation, that´s why not showing signs of interaction with other substances, which are metab. through cytochrome P-450
• excretion by faeces, less by urine• „respiratory quinolone“ – effect on G+
causative agents of respiratory infections

Bronchopneumonia Caused by Pseudomonas aeruginosa
• risk factors of occurance: structural changes of airways and lungs, systemic therapy
with glucocorticoids, wide-spectrum ATB therapy in the last month, malnutrition
• antipseudomonad betalactamic ATB: cefepime, piperacillin-tazobactam / both also effective on
pneumococci/, at allergy to betalactams monobactam aztreonam
always combined therapy with aminoglykosides /gentamicin/ and antipseudomonad fluoroquinolone /ciprofloxacin/

Atypical Bronchopneumonia
• disease development and a mild physical symptoms does not correspond to significant signs on X-ray of lungs, but some of them have severe acute development with the possible occurance of serious complications / ARDS /
• 30 – 40% of bronchopneumonias• causative agents = intracelular parasits /Mycoplasma pneumonie,
Chlamydia pneumoniae, Legionella pneumophila, Coxiella burnetii/ + respiratory viruses
• occurance mainly in societies of young people• ATB therapy which penetrates intracelullarly and interferes with
proteosynthesis of atypical microorganisms

Occurance of Bronchopneumonias Caused by Mycoplasmas according to Age
Pharmacotherapy of Atypical Pneumonias
• Macrolides
/erythromycin, klarithromycin, azithromycin/
• Tetracyclines
/doxycycline/
• Fluoroquinolones
/antipneumococcal/

Macrolides
• bakteriostatic effect – inhibit proteosynthesis of microorganisms
• spectrum mainly G+ bacterias, H. influenzae, some anaerobic bacterias
• penetration to cells and influence on intracel. pathogens /M. pneumoniae, chlamydias/
• good penetration to tissues • metabolis. in liver by cytochr. P-450 interactions:
increases plasmat. conc. of theophylline, digoxin, anticoagulants. Interaction with antihistaminics causings severe ventricular arrhytmia

Macrolides
slower and lower development of resistance • stability in acidic surrounding • longer biologic half-life • high concentration in tissues and serum• 2nd generation /erythromycin+spiramicin/
roxithromycin, azithromycin, clarithromycin = better pharmacokinetics and tollerability/
• little toxic, good tolleration• AE: GIT + liver functions
Clarithromycin
• semisyntetic • verry good tollerance • biotransformation to antimicrobically more
effective 14-OH-clarithromycin • typical, atypical, intracelular and ß-laktamase
producing pathogens • 8 times more effective as erythromycin to Chl.
pneumoniae and M. pneumoniae • very good at infections caused by Legionella
pneumophilla and Moraxella catarrhalis

Tetracyclines• bakteriostatic, strong occurance of resistance• infections caused by mykoplasmas, chlamydias,
rickettsias• resorption at fasting good, not with milk, antacids,
Fe 3+, which prevent their resorption• good penetration to tissues except to CNS• at renal diseases needed dose reduction• 2nd generation: tetracyclin doxycyclin – better pharmacokin. properties
/higher bioavailability, longer half-life = administratio 1-2 times per day/
• AE: oft but not severe, GIT, disorders of bones and teeth by calcium chelation = contraindic. at children
Tigecycline• Broad spectrum antibiotic from new group
of glycylcyclines, derived from TTC,
since the year 2005
spectrum:• G+ and G- including multiresistant
– methicillin/oxacillin-resistant strains of Staph.aureus– penicillin-resistant streptococci– vancomycin-resistant enterococci – bacterias producing broad spectrum betalactamases – anaerobes (group Bacteroides)– mycoplasmas, chlamydia– rapidly growing mycobacteria
Tigecycline
• treatment of complicated skin and intra-abdominal infections, which are often caused simultaneously by more bacteria (not rarely by multiresistant strains)
• it can be used in the treatment of documented infections, as well as initial empiric therapy, before definitive identification of the pathogen
• i.v. application
Linezolid• yet the only representative of new group of
oxazolidinones• broad spectrum of effectiveness including
community-acquired
and nosocomial G+ pathogens• oxacillin-resistant staphylococci
(S. aureus, S. epidermidis) • vankomycin-resistant enterococci
(E. faecalis, E. faecium)• penicillin and erythromycin-resistant pneumococci• interaction potential of linezolid is low, enzyme complex
cytochrome P-450 is not participating in metabolism of linezolid
Linezolid
• oral form achieves the same pharmacologic parameters as parenteral
(serum and tissue concentrations)• reaches high concentrations in bones, cerebrospinal
liquor and mainly in lung parenchyma• therapy of nosocomial pneumonias
and severe infections of skin and soft tissues• bioavailability is very good, what allows administration
also initially in p.o. form or as follow-on treatment - p.o. after initial i.v. therapy
Daptomycin
• representative of lipopeptide antibiotics• effective only against G+ microorganisms except
enterococci• treatment of skin and soft tissue infections • potentially also for treatment of catether
infections
Super-Resistant Bacterias• superbugs or extensively drug-resistant microorganisms • gramnegative bacterias (Pseudomonas aeruginosa,
Klebsiella, Enterobacter a Enterobacteriaceae)• carry genes producing metallo-beta-lactamases
/broad-spectrum beta-lactamases containing Zn, which break down also ATB, which were so far to gramnegative bacterias the most effective – carbapenems/
• are resistant to all cephalosporis and penicillins, quinolones, aminoglycosides - are resistant also to so called reserve ATB

ANTITUSSIVES• cough = reflex. protective mechanism, with witch
airways are getting rid of any foreign materiala, and also secretory products
• complete cough supression is unwanted and unreal• but long-lasting cough cand weaken patient and
strained breathing muscles are painful, that´s when are indicated antitussives
• antitussives we use only when we know ethiology of cough and when we treat causally given disease!
Division: 1. antitussives with central effect and with the structure of opioids2. antitussives with central effect and peripheral effect
with different structure

CODEINE
= decreases sensitivity of center for cough • properties similar to morphine, less effective• p.o. administered good absorption from GIT, metabolis. in liver to morphine and norcodeine, excreted by kidneys
unchanged or as glucuronide, transfer to breast milk = supress of child´s breathing
• interactions: + IMAO, thymoleptics, physostigmine, neostigmine
- naloxone, nalorphine, pentazocine= increases analgetic effect of analgetics-antipyretics= potentiation of suppressive effect of other CNS drugs= with opioid analgetics – deepening depression of CNS and
breathing center
CODEINE
• indication: symptomat. supressing of irritating non-productive cough of known etiology in combination with causal therapy of given disease
• contraindications: difficult expectoration, mainly at advanced stage of bronchopulmonal disease, hypersensitivity to drug, prohibition of alcohol /strongly increases depressive effect on CNS/!
• dose: 15 – 30 mg 3 times per day

FOLCODINE
= derivate of codeine with bigger efficacy, doesn´t decrease bronchial secretion, isn´t usually cause of dependence, supresses cough reflex inhib. by inhibition of centrum for cough in medulla
- therapy of dry irritating cough - increases depressive effect of substances
supressing CNS and also alcoholdosage: 10 – 20mg 3 times per day

ANTITUSSIVES OF CODEINE TYPE
Etylmorphine = derivate of morphine similar to codeine, stronger analgetic and antitussic effect
at dry irritating cough at acute inflammation of airway system, TBC, spontaneous pneumothorax and before diagnostic procedurelong-lasting aplication in pregnancy = abstinent signs at newborn, passes to milk!
Dextromethorphan = antitussive drug without analgetic. effect, doesn´t supress breathing center, minimal risk of dependence, minimal AE
not at patients with bronchial asthma!
ANTITUSSIVES OF NONCOD. TYPE
central effect: pentoxyverine /one-third effect of codeine, lower effects, at antitus. doses proven no depressive influence on breathing center/, butamirate /effective antitussic used in pediatria, minimum AE/, clobutinol /contraindicated in pregnancy and at breast feeding/
peripheral effect: benzonatate, dropropizine /strong antitussive with properties similar to butamirate, mild antihistaminic effect, minimal effect on on breathing center /
EXPECTORANTS= getting rid of viscous mucus from airways1. Mucolytics and secretolytics – lower viscosity of
mucus, resp. increase production of mucus CAREFUL AT SIMULTANEOUS ADMINISTRATION
OF ANTITUSSÍVE AGENTS!BROMHEXINE – increasing proportion of liquid bronchial mucus
and reduces its viscosity by reduction of transversal bonds of acid mucopolysaccharides, promotes secretion of mucus, improves cilliar function, pharmaco-therapeutically active is metabolite ambroxol
AMBROXOL – mukolytic and secretolytic effects, activation of cilliar epithelium
N-ACETYLCYSTEINE - cleaves disulfidic bridges connecting mucopolysacharid fibers in sputum, at difficult expectoration, at chronic bronchitis and mucoviscidosis, also prophylactically
2. Secretomotorics – are increasing activity of cilliar epithelium /β-sympathomimetics, eteric oils/
Related Documents











