Bridging the Gap: Knowledge and Information Services Collaboration Katherine Cheema, Quality Observatory, NHS South East Coast Emma Aldrich, Maidstone & Tunbridge Wells NHS Trust

Bridging the Gap: Knowledge and Information Services Collaboration Katherine Cheema, Quality Observatory, NHS South East Coast Emma Aldrich, Maidstone.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bridging the Gap: Knowledge and Information
Services Collaboration
Katherine Cheema, Quality Observatory, NHS South East Coast
Emma Aldrich, Maidstone & Tunbridge Wells NHS Trust

Who are we?Katherine Cheema:• Specialist Information Analyst at NHS South
East Coast Quality Observatory with interests in healthcare associated infections, maternity and neonates and long term conditions.
Emma Aldrich:• Knowledge Manager, working within the Library
and Knowledge Team at Maidstone & Tunbridge Wells NHS Trust with interests in rolling out knowledge management tools across the trust

Problem…….• Evidence
– The need for it……– ….and the apparent lack of it
• Quantitative, numerical, driven by the performance agenda
• Information for judgement!• Issues with commissioner resources and skills

Case study• MRSA trajectories
– Traditionally acute trust focussed– But almost 50% cases acquired in the
community– How can these cases be factored into PCO
focussed envelopes?– On the basis of the information generally
available such an exercise would be very difficult

….Solution• Bring together the surveillance data and the
research evidence: • Define an end point for community MRSA
which is – realistic in terms of ability for organisations
to achieve– representative of the research to date and
the surveillance information available• So rather than ‘best guesses’ and an
assumption of a blanket reduction in CA-MRSA across all organisations……

Pre-48 hour cases(Source: HPA DCS)
PRE 48-HOUR CASES (COMMUNITY ACQUIRED)
Post-48 hour avoidable cases
(Source: Local retrospective review)
Post-48 hour unavoidable/complex
cases
(Source:Local retrospective review)
POST 48-HOUR CASES (TRUST ACQUIRED)
ALL CASES
FUTURE TRAJECTORIES
STATIC
DEFINED %
REDUCTION
Reduction
to an
estimated
prevalence
informed
by
evidence
base
We have something more structured utilising all the quantitative and qualitative knowledge we have available at each stage of the model……..

Sounds simple….?
Ask a Librarian…..• 15 years experience of searching healthcare
databases• Advanced searching skills, filters, subheading
searches• Specificity, sensitivity• Teaming clinical/ mathematical skills with
evidence seeking skills
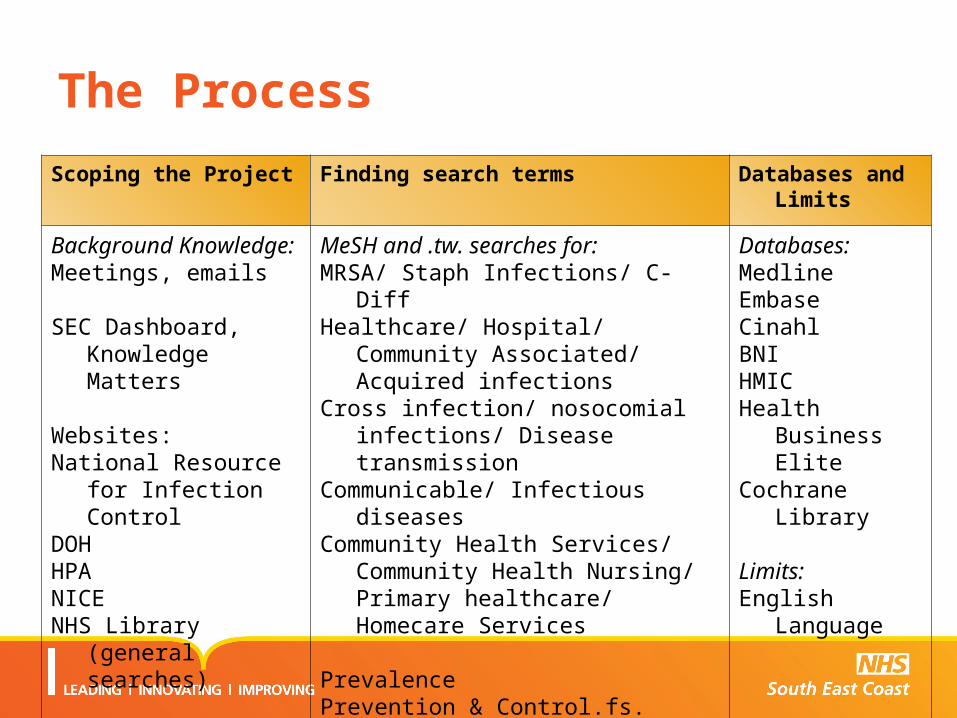
The Process
Scoping the Project Finding search terms Databases and Limits
Background Knowledge:Meetings, emails
SEC Dashboard, Knowledge Matters
Websites:National Resource for
Infection ControlDOHHPANICENHS Library (general
searches)
MeSH and .tw. searches for:MRSA/ Staph Infections/ C-DiffHealthcare/ Hospital/ Community
Associated/ Acquired infectionsCross infection/ nosocomial infections/
Disease transmissionCommunicable/ Infectious diseasesCommunity Health Services/
Community Health Nursing/ Primary healthcare/ Homecare Services
PrevalencePrevention & Control.fs. Transmission.fs.
Databases:MedlineEmbaseCinahlBNIHMICHealth Business
EliteCochrane Library
Limits:English Language

The Process
• Results reviewed collaboratively
- Articles selected
- Searches refined and re-run
• Joint critical appraisal
• Literature review

Results
• Ability to develop a statistical model of community acquired MRSA to predict incidence using existing surveillance data sources and the associated evidence base
• Interest from local health economies on utilising findings for own improvement programmes and strategies
• Development of recommendations with regards definitions used in monitoring of community acquired MRSA cases at a strategic level

0
2
4
6
8
10
12
14
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64 67 70 73 76 79 82 85 88 91 94 97 100103106109112115118121124127130133136139142145148151
Trust (anon)
All
MR
SA
bac
tera
emia
rat
e p
er 1
00,0
00 h
ead
of
po
pu
lati
on
Rate Median Best quartile
Brighton And Hove City
Selected trust MRSA objective details & calculation method
Baseline rate:
Best quartile status:
Median status:
MRSA objective (cases):
Reduction from baseline required (cases):
Reduction where 20% rate reduction applied (cases):
6.235
11
5
3
Methodology applied: Reduce rate per 100,000 bed days to median or by 20%,
whichever is the greater challenge
Baseline cases: 16
Select acute trust:Select acute trust (a-z):
MRSA PCO Objective 2010-2011: modelling options and explorer
ABOVE
ABOVE
Proposed MRSA stretch limit (cases):
9
Baseline data is all cases attributed to PCT responsible population from October 2008 to September 2009. Rates are measured per 100,000 head of resident population.

What can we learn? Personal reflections…
• Greater understanding of what each function does – broadening knowledge of where NHS staff can go for information
• Process different for LKS professional – greater involvement than usual in results/ follow up: seeing it through to the end
• Discovery of how much more ‘information’ there is out there, and that there are people with the expertise to search, review and collate it

What can we learn? Implications for the wider NHS…
• This project – A meeting and discussion between two regional leads which evolved into a unique collaboration.
• The collaborative approach must continue to underpin the commissioning and service improvement processes and the promotion of quality.
• Active marketing of library resources and staff expertise, including outside of the acute sector
• A formal communication mechanism to be put in place to ensure that these collaborative projects can be undertaken easily in the future.

Any questions….?
Related Documents











