Bone Healing and Anatomy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bone Healing and Anatomy
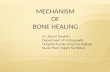
Long Bone Structure
Reference: http://www.sirinet.net/~jgjohnso/modlongbones.jpg
Osteon
Haversion
Canal
Important terms to know….
• Diaphysis-shaft of long bone
• Metaphysis-growth area of long bone
• Epiphysis-ends of long bone
• Periosteum-outer sheath, blood and nerve supply
• Endosteum-inner sheath of long bone
• Compact bone=cortical bone
• Cortical Wall = 1/16 in – ¼ in
• Spongy bone=cancellous bone =trabecular bone=woven bone
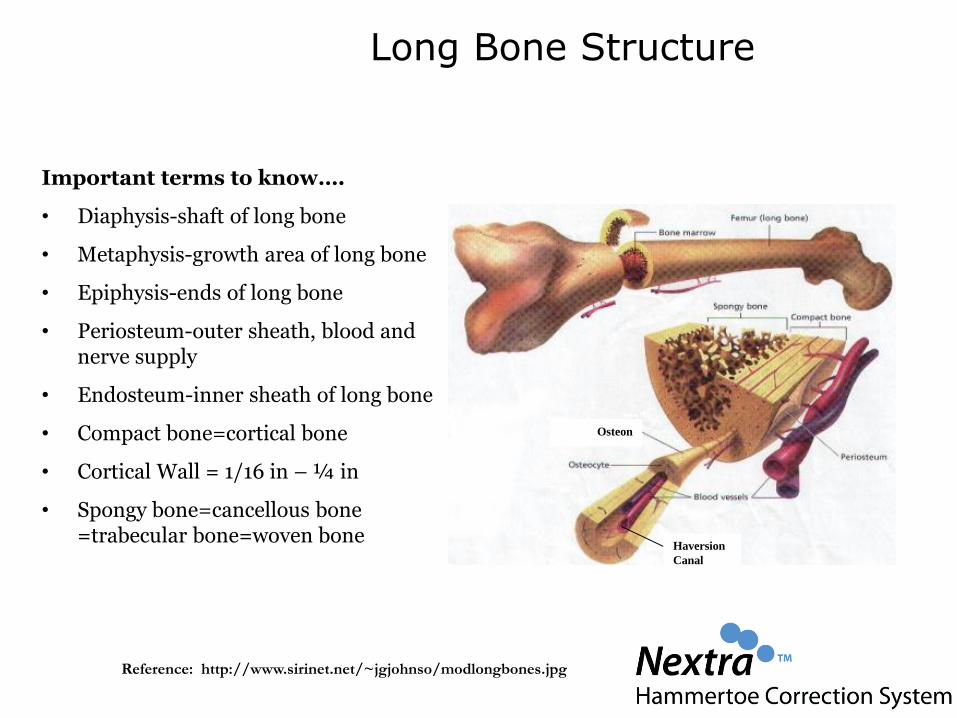
Periosteum
Cortical Wall
Long Bone Structure
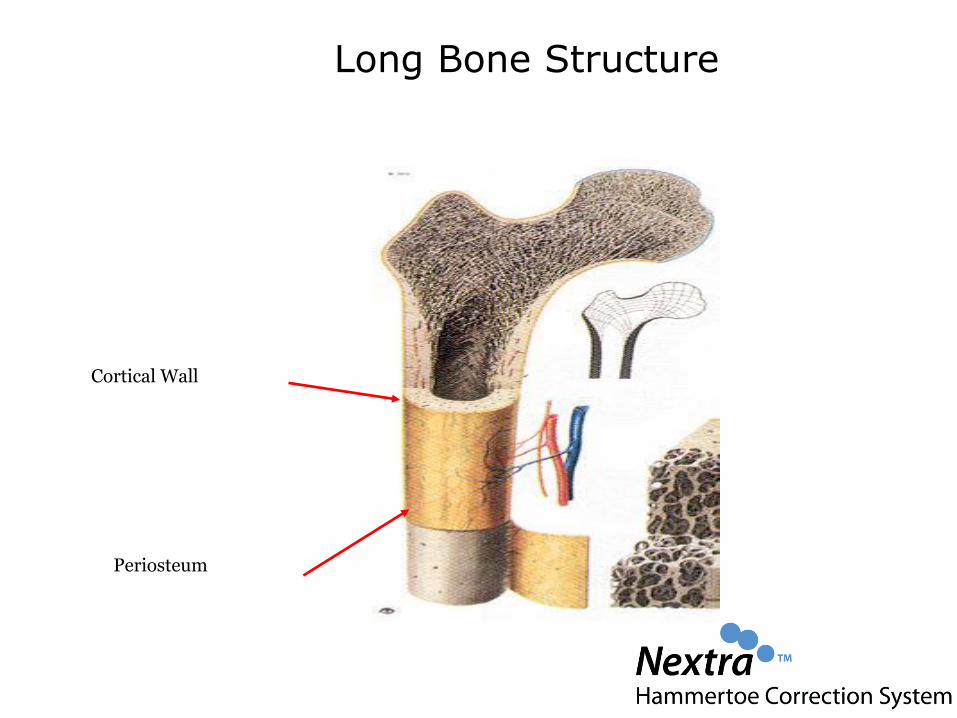
Short Bone Structure
Reference: http://health.allrefer.com/health/short-bones-short-bones.html
Composition of Bone
• 65 -75% Inorganic material:
hydroxyapetites (calcium, other mineral salts)
• 25-35% Organic material:
collagen, proteoglycans, proteins, bone growth factors
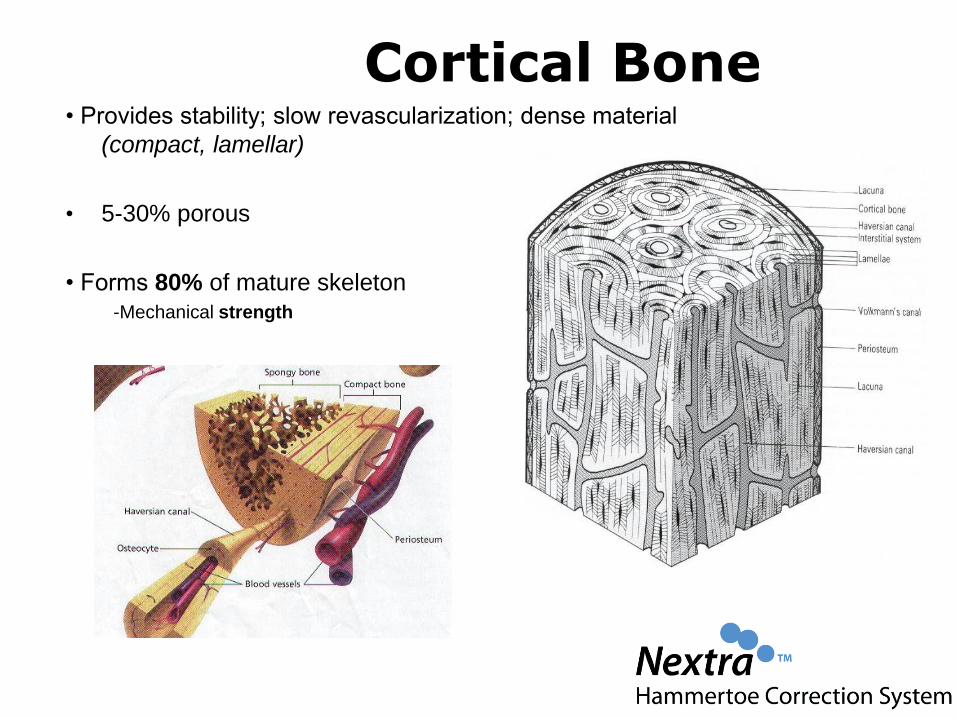
Cortical Bone• Provides stability; slow revascularization; dense material
(compact, lamellar)
• 5-30% porous
• Forms 80% of mature skeleton-Mechanical strength
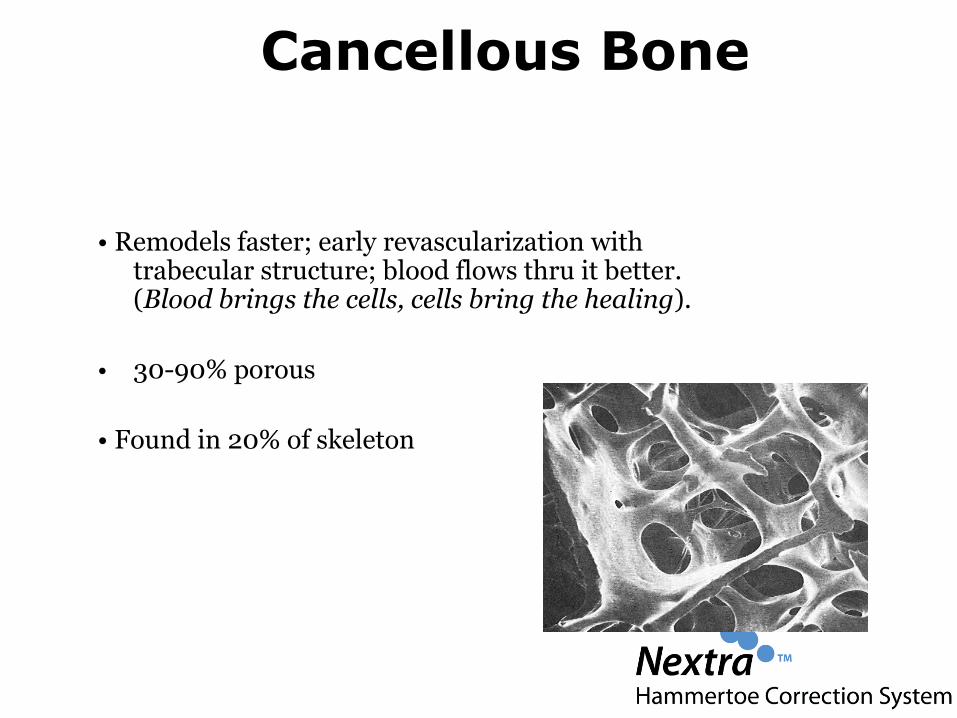
Cancellous Bone
• Remodels faster; early revascularization with trabecular structure; blood flows thru it better. (Blood brings the cells, cells bring the healing).
• 30-90% porous
• Found in 20% of skeleton
Mechanisms of Bone Formation
Osteogenesis- capable of forming new bone from live cells (osteoblasts, pre-osteoblast cells)
-Source: Autograft, bone marrow
Osteoinduction- the formation of new bone by recipient mesenchymal cells that differentiate into bone
-Source: active BMP’s, DBM, demineralization process
Osteoconduction- inert scaffolding permits cell migration & ingrowth of new host bone. Creeping substitution
-Source: Allografts, ceramics, collagen
Remodeling/Wolff’s Law
• “Wolff's law" states that bone models and remodels in response to the mechanical stresses it experiences so as to produce a minimal-weight structure that is 'adapted' to its applied stresses.
• If loading on a particular bone increases, the bone will remodel itself over time to become stronger to resist that sort of loading .
• Bone Heals Under Compression• Astronauts: weak bones• Weightlifts: more bone density
AO Basic Principles
• Anatomical reduction and compression
• Stable fixation
• Preservation of blood supply
• Early mobilization
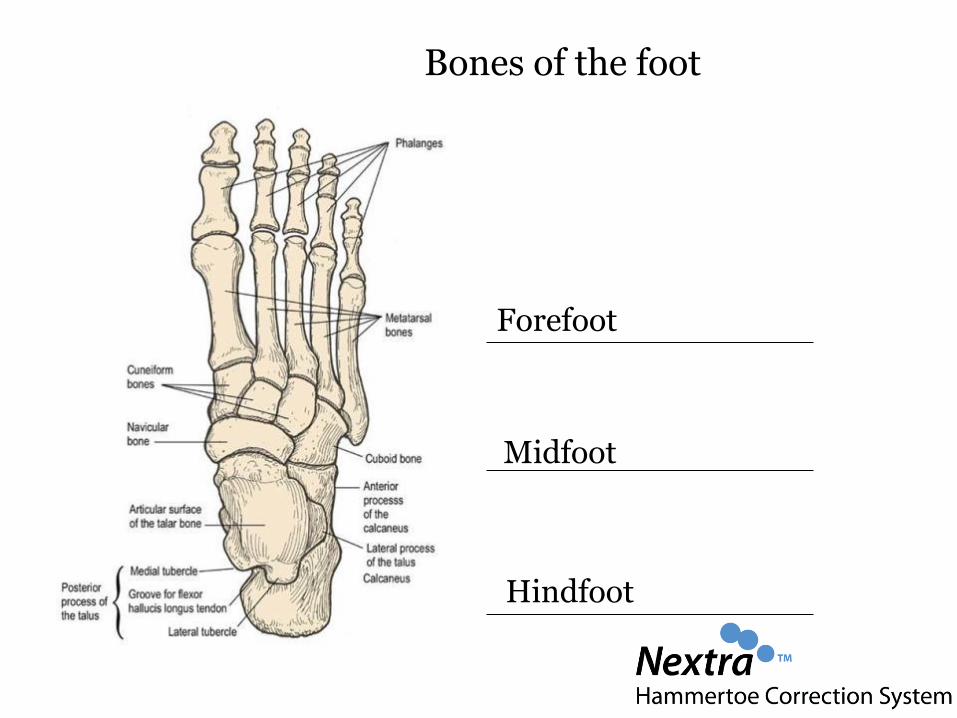
Bones of the foot
Forefoot
Midfoot
Hindfoot
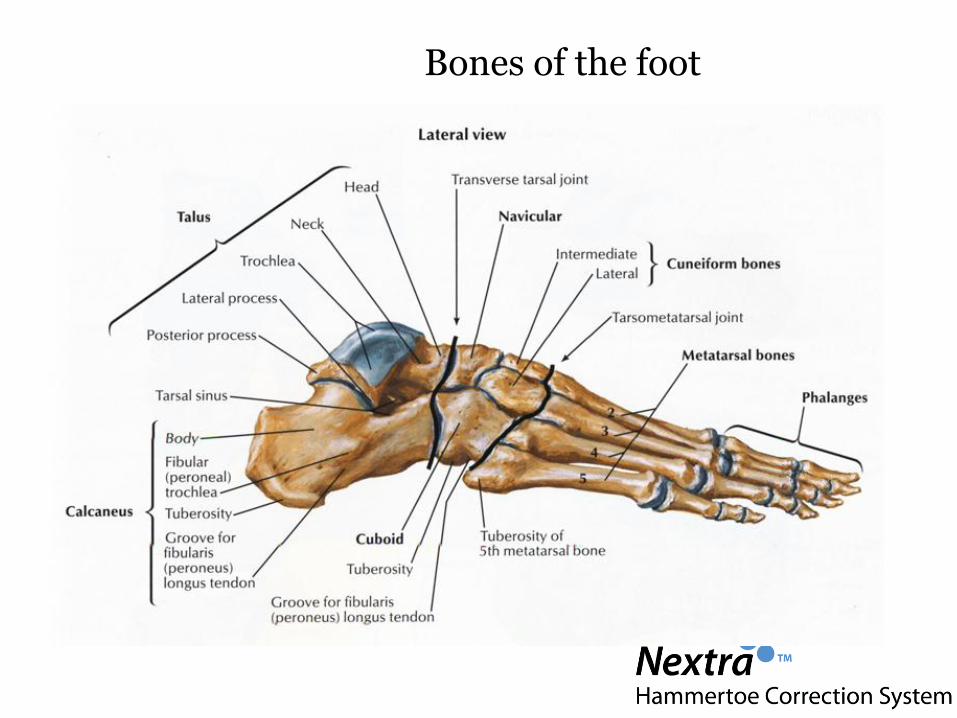
Bones of the foot
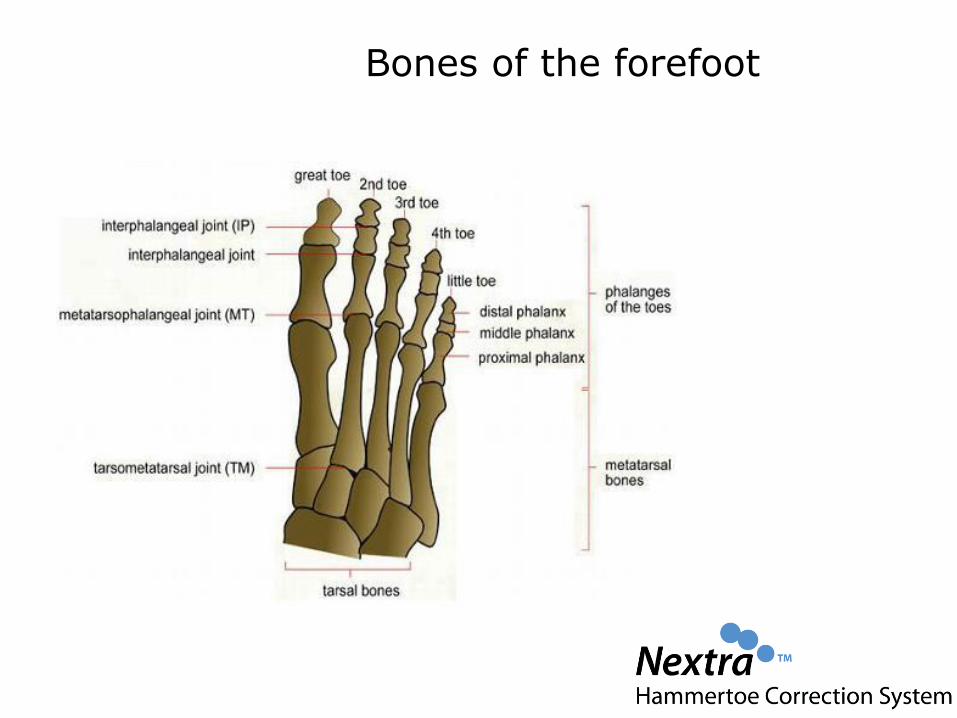
Bones of the forefoot
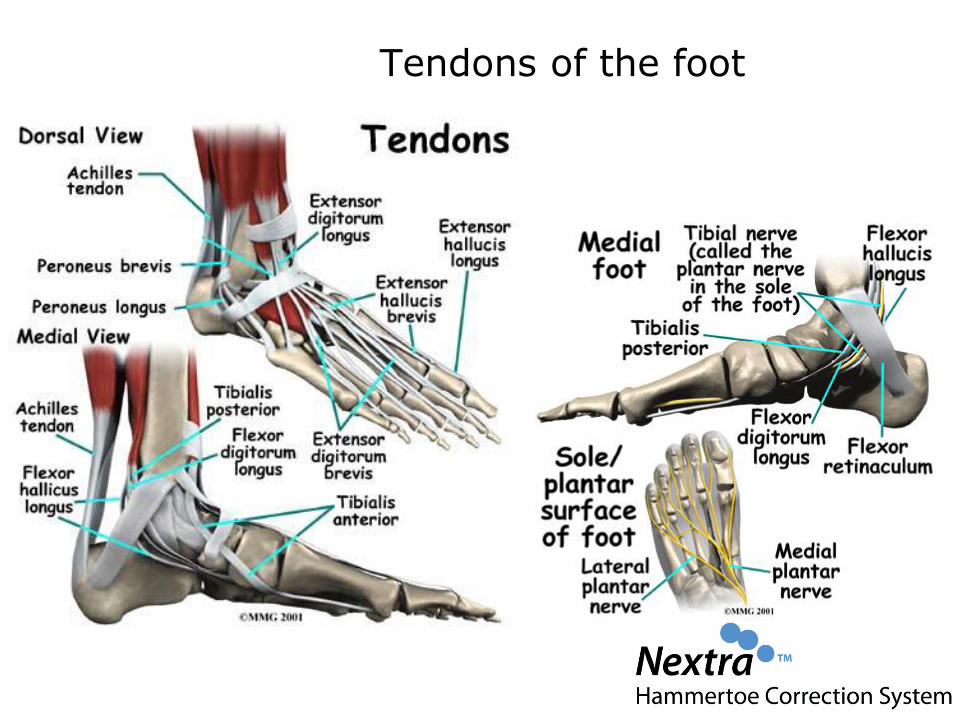
Tendons of the foot
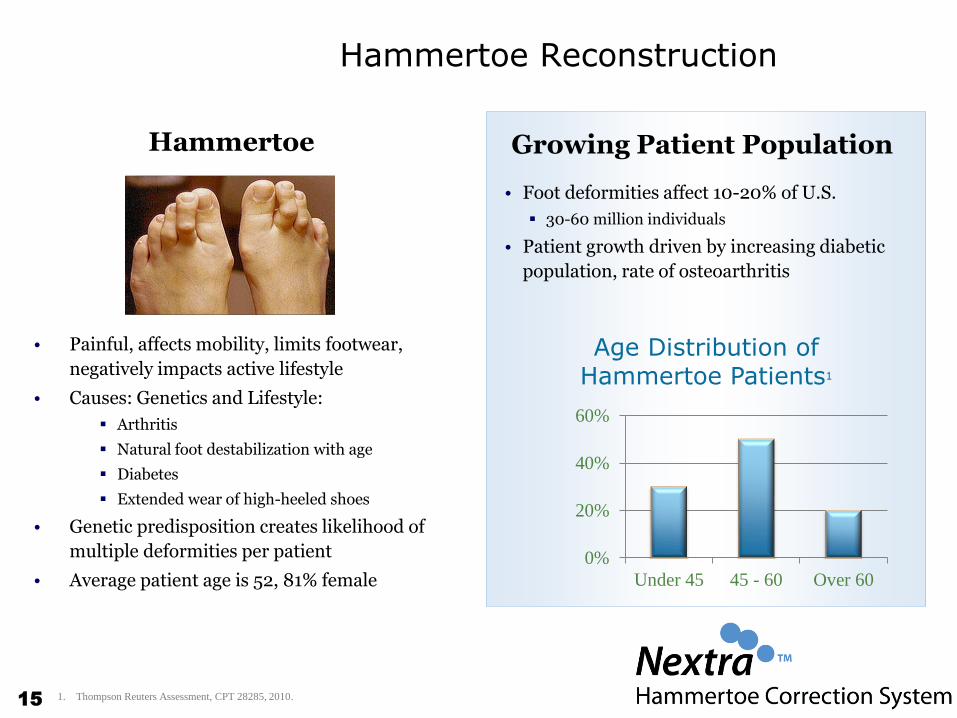
Hammertoe Reconstruction
• Painful, affects mobility, limits footwear,
negatively impacts active lifestyle
• Causes: Genetics and Lifestyle:
Arthritis
Natural foot destabilization with age
Diabetes
Extended wear of high-heeled shoes
• Genetic predisposition creates likelihood of
multiple deformities per patient
• Average patient age is 52, 81% female
• Foot deformities affect 10-20% of U.S.
30-60 million individuals
• Patient growth driven by increasing diabetic
population, rate of osteoarthritis
0%
20%
40%
60%
Under 45 45 - 60 Over 60
Age Distribution of Hammertoe Patients1
Growing Patient Population
1. Thompson Reuters Assessment, CPT 28285, 2010.
Hammertoe
15
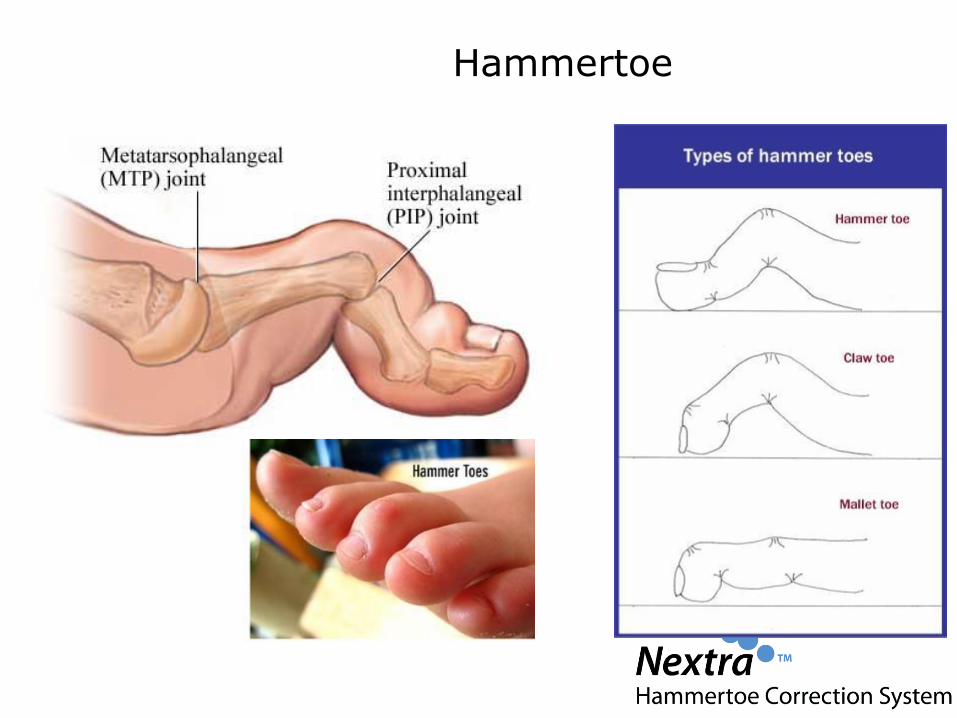
Hammertoe
Typical Symptoms
• Pain or irritation of the affected toe when wearing shoes.• Corns and calluses (a buildup of skin) on the toe, between two
toes, or on the ball of the foot. Corns are caused by constant friction against the shoe. They may be soft or hard, depending upon their location.
• Inflammation, redness, or a burning sensation• Contracture of the toe• In more severe cases of hammertoe, open sores may form.
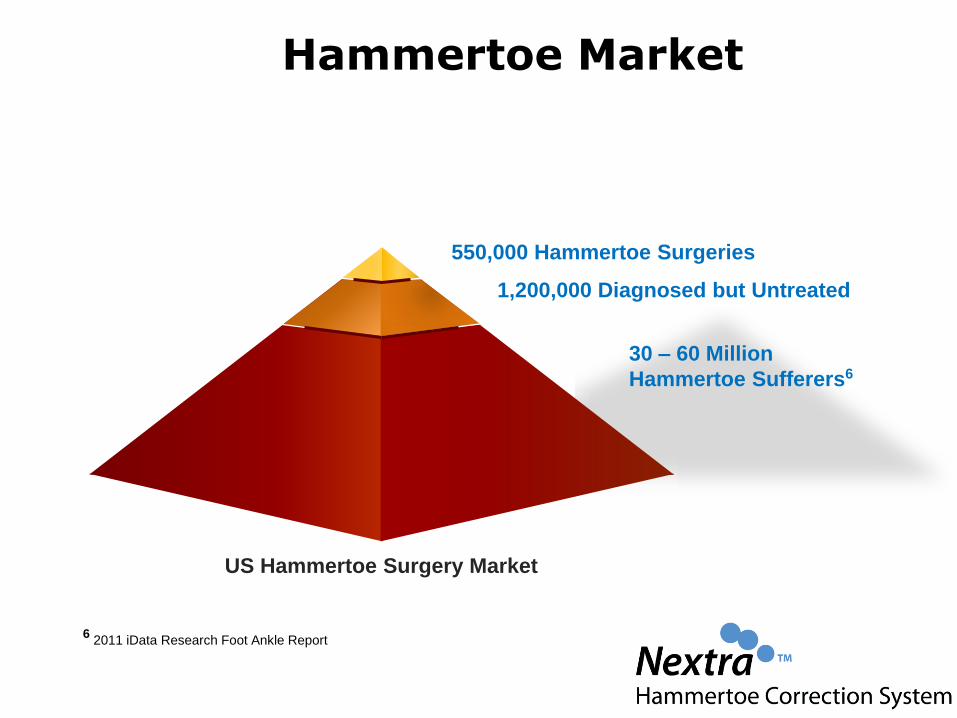
Hammertoe Market
550,000 Hammertoe Surgeries
1,200,000 Diagnosed but Untreated
6 2011 iData Research Foot Ankle Report
30 – 60 Million
Hammertoe Sufferers6
US Hammertoe Surgery Market
Surgery- Legacy Standard of Care
• Varies based on severity (MPJ sometimes addressed)• Arthodesis or Arthroplasty- or a combination of both
• Major steps:• Preparation – Sometimes• Incision- dorsolinear over joint PIP• Capsulotomy• Tendon Release or transfer (extensor sometimes flexor)• Retrograde Wire into middle and distal phalanx• Wire back into proximal phalanx and sometimes
metatarsal

Surgical Treatment- Planning

Surgical Treatment - Incision

Surgical Treatment- Open

Surgical Treatment- Capsule, Tendon Release

Surgical Treatment- K-wire

Surgical Treatment- Kwire

Surgical Treatment - Bending

Surgical Treatment- the reality
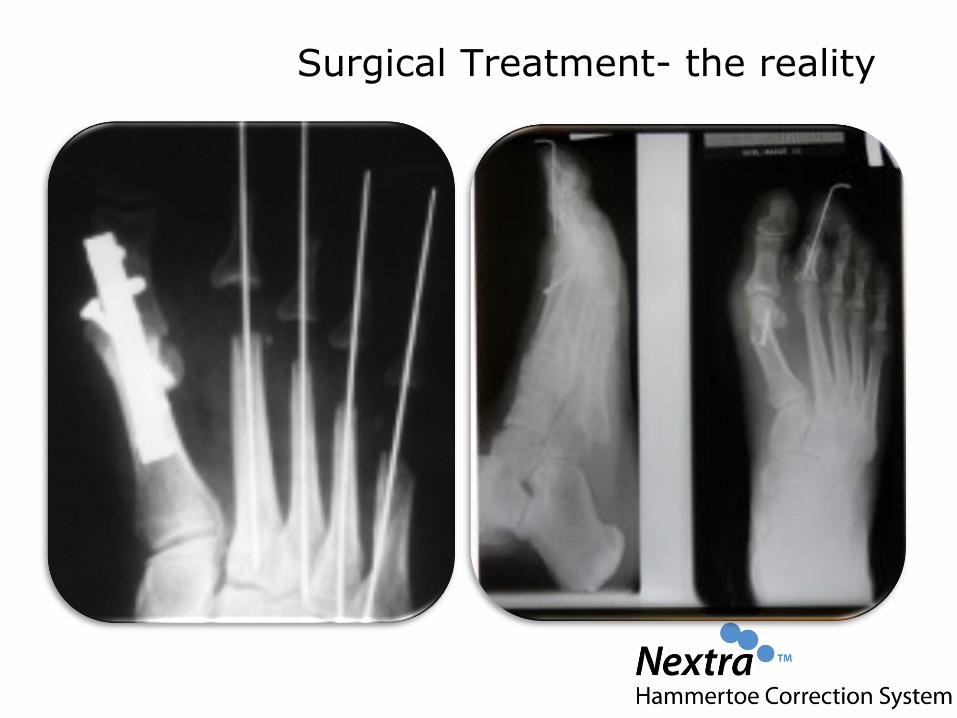
Surgical Treatment- the reality
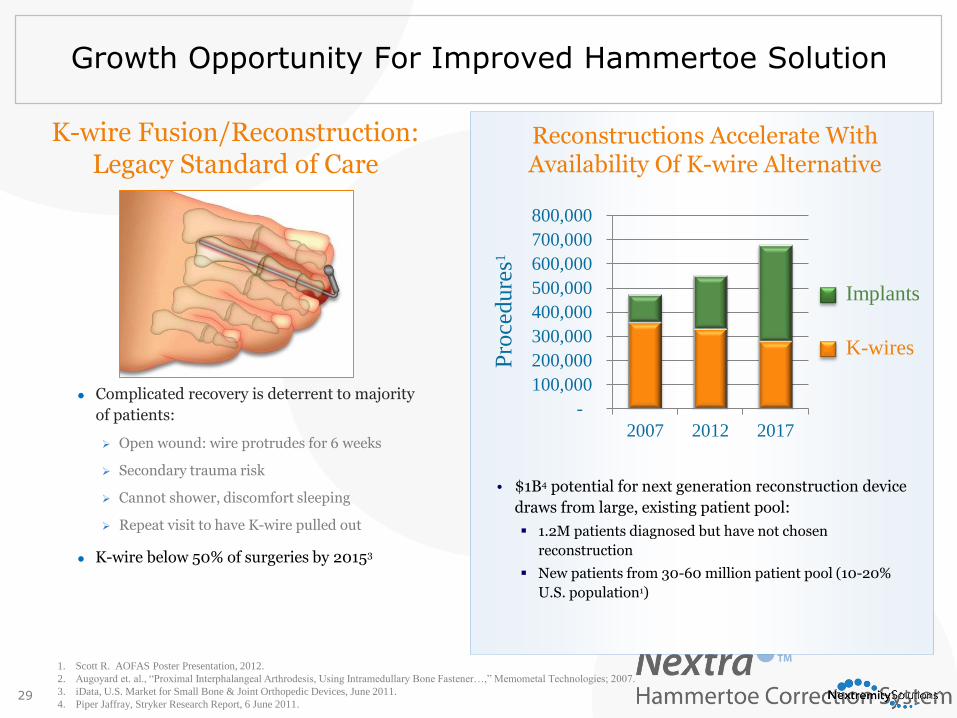
Growth Opportunity For Improved Hammertoe Solution
• $1B4 potential for next generation reconstruction device
draws from large, existing patient pool:
1.2M patients diagnosed but have not chosen
reconstruction
New patients from 30-60 million patient pool (10-20%
U.S. population1)
1. Scott R. AOFAS Poster Presentation, 2012.
2. Augoyard et. al., “Proximal Interphalangeal Arthrodesis, Using Intramedullary Bone Fastener…,” Memometal Technologies; 2007.
3. iData, U.S. Market for Small Bone & Joint Orthopedic Devices, June 2011.
4. Piper Jaffray, Stryker Research Report, 6 June 2011.
K-wire Fusion/Reconstruction:Legacy Standard of Care
Complicated recovery is deterrent to majority
of patients:
Open wound: wire protrudes for 6 weeks
Secondary trauma risk
Cannot shower, discomfort sleeping
Repeat visit to have K-wire pulled out
K-wire below 50% of surgeries by 20153
Reconstructions Accelerate With Availability Of K-wire Alternative
-
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
2007 2012 2017
Implants
K-wires
Pro
cedure
s1
29
Patient Brochures
“Happy Toes” Promotions & Website Help Surgeons Grow Practice
3030
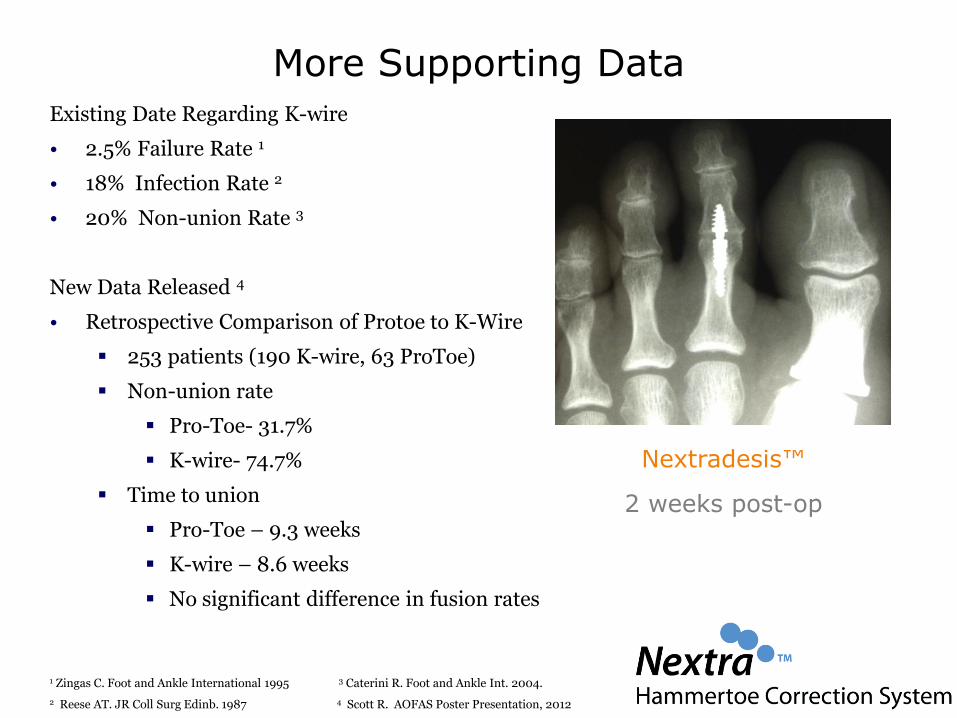
More Supporting DataExisting Date Regarding K-wire
• 2.5% Failure Rate 1
• 18% Infection Rate 2
• 20% Non-union Rate 3
New Data Released 4
• Retrospective Comparison of Protoe to K-Wire
253 patients (190 K-wire, 63 ProToe)
Non-union rate
Pro-Toe- 31.7%
K-wire- 74.7%
Time to union
Pro-Toe – 9.3 weeks
K-wire – 8.6 weeks
No significant difference in fusion rates
1 Zingas C. Foot and Ankle International 1995 3 Caterini R. Foot and Ankle Int. 2004.
2 Reese AT. JR Coll Surg Edinb. 1987 4 Scott R. AOFAS Poster Presentation, 2012
Nextradesis™
2 weeks post-op
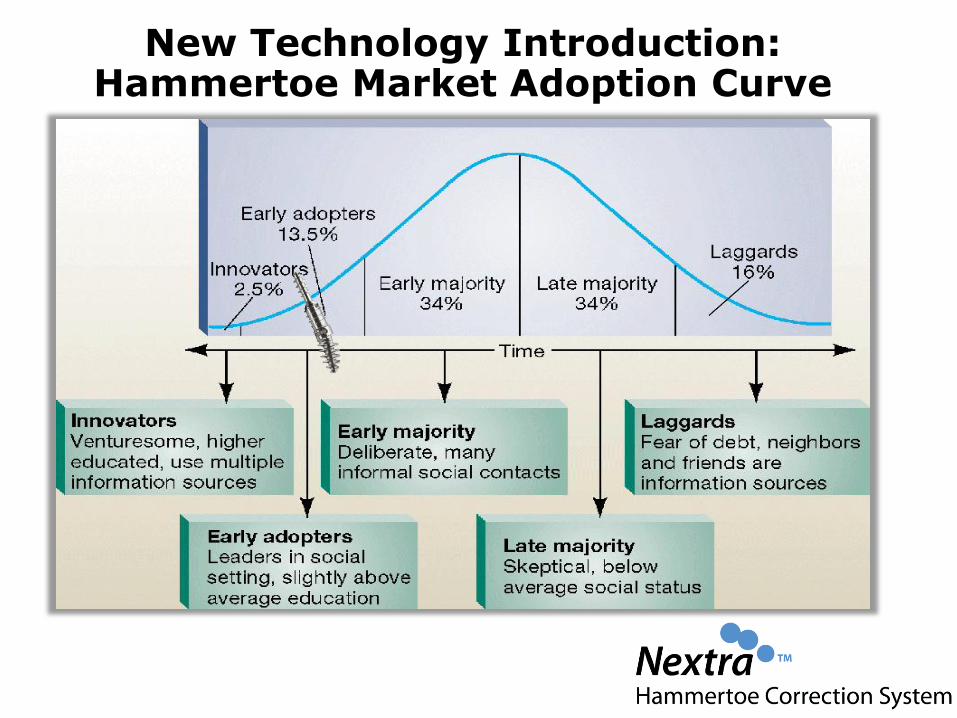
New Technology Introduction: Hammertoe Market Adoption Curve

Thank You
Related Documents