Blutkonserven versus Erythropoietin in der Onkologie K. Strasser-Weippl Zentrum für Hämatologie und Onkologie Wilhelminenspital © KSW 5-08

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Blutkonserven versus Erythropoietinin der Onkologie
K. Strasser-WeipplZentrum für Hämatologie und Onkologie
Wilhelminenspital
© KSW 5-08

Anämie bei onkologischen Patienten
• Definition:• Männer: Hb <13.5g/dL • Frauen: Hb <11.5g/dL
• Prävalenz:• ~20–60% aller Krebspatienten
• Inzidenz/Ausprägung abhängig von:• Alter• Anwesenheit/Abwesenheit von Comorbiditäten• Histologie/Stadium der Erkrankung• Therapie
© KSW 5-08

< 6.5< 6.5< 6.5< 6.5< 6.5< 6.54
6.5-7.96.5-7.96.5-7.96.5-7.96.5-7.96.5-7.93
8-10.08-10.08-9.98-10.08-10.08-9.42
10-WNL10-WNL10-WNL10-WNL10-WNL9.5-10.51
WNLWNLWNLWNLWNL> 110
GOGCALGBSWOGECOGNCIWHOGrad
WNL: „within normal limits“ d.h. bei Frauen Hb = 12.0-16.0 g/dl; bei Männern Hb = 14.0-18.0g/dl
Einteilung der Anämie nach Hb (g/dl)
© KSW 5-08

Prävalenz der Anämie bei onkologischen Patienten
© KSW 5-08

Ätiologie / Pathophysiologie der Anämie
• Myelosuppression durch Chemo- und/oder Radiotherapie
• Verringerte EPO Produktion: renale Toxizität, Chemotherapie, tumorbedingte Anämie
• Verringerte EPO Sensitivität: inflammatorische Zytokine(z.B. TNF-, IL-1, IL-6), Knochenmarksinfiltration
© KSW 5-08

Formen der Anämie bei Tumorpatienten
• Tumor-induzierte Anämie= anemia of chronic disease
• Chemotherapie-induzierte Anämie
• Radiotherapie-induzierte Anämie
© KSW 5-08

Verkürzte Überlebenszeit
Pathomechanismen der tumorinduzierten Anämie
Tumorzellen
ErythrozytenAktiviertes Immunsystem
MakrophagenTNF
Anämie
IFN-α,β IFN-γ IFN-γIL-1 IL-1 IL-1TNF TNF TNF
α1-Antitrypsin
Suppression Störung Suppressionder EPO- der erythrozytärer
Produktion Eisenutilisation Vorstufen
Nowrousian MR. Med Oncol 1998;15(Suppl. 1):S19–28
Erythrophagozytose
Dyserythropoese
TNF = Tumour Necrose Factor; IFN =Interferon; IL-1 = Interleukin-1;
© KSW 5-08

Inzidenz der Anämie
Groopmann JE et al. J Natl Cancer Inst 1999; 91: 1616-1634* Tandem 1998; BioMedical Insights Inc. 1999
NCI und WHO: Grad 3: Hb = 6.5 –7.9 g/dl; Grad 4: < 6.5 g/dl
4% - 13%Prostatakarzinom*
5% - 40%Ovarialkarzinom
20% - 40%NSCLC
10% - 80%Lymphome
5% - 10%Kolorektale Karzinome
2% - 20%Mammakarzinom
Anämie Grad 3-4 bei Standardchemotherapie
Tumorart
© KSW 5-08

Chemotherapie-induzierte Anämie
© KSW 5-08

Radiotherapie-induzierte Anämie
• RT supprimiert die Erythropoese (abhängig vom Bestrahlungsfeld)
• Langzeitschäden des hämatopoetischenZellpools
© KSW 5-08

Radiotherapie-induzierte Anämie
0 20 40 60 80 100Häufigkeit (%)
Prostata
Mamma
Bronchial
Kolorektal
Uterus/Cervix
nach RTx
vor RTx
Harrison et al. Proc. ASCO 2000 © KSW 5-08

Anämie und PrognoseReferenz n Erkran-
kung Prognostischer Indikator
(PI) p-Wert
Sokal JE, et al. 1987 678 CML Niedriger Hämatokrit 0.0004
Binet JL, et al. 1981 295 CLL Hb <10g/dL* <0.001
Durie BGM, Salmon SE. 1975 71 MM Hb <8.5g/dL <0.02
Hasenclever D, Diehl V. 1988 1618 HD Hb <10.5/dL <0.001
Moullet I, et al. 1998 341 NHL Hb <12g/dL** <0.0001
* und Thrombozyten 100,000/mm3
** bei Patienten >50 Jahre. Hb-Wert <11g/dL bei Frauen <50 Jahre
© KSW 5-08

Anämie und Prognose
1.0
0.8
0.6
0.4
0.2
0
% R
ezid
izvf
reih
eit
0 1 2 3 4 5Jahre
Nicht anämisch
anämisch
Frommhold H. et al., Strahlenther Onkol 1998;174 (Suppl. 4)
Patienten behandelt mit Strahlentherapie und stratifiziertnach dem Grad der Anämie (n=889)
P<0.0001
© KSW 5-08

Anämie und Prognose
© KSW 5-08

Anämiebehandlung beim Tumorpatienten
• prinzipiell kausal und individuell
• Erythrozyten-Substitution• in D.: 3 Mio EK/Jahr; davon > 50% bei
Tumoroperationen (Heiss M; 2000)
• in USA: 1 Mio EK/J v.a. in der palliativen Tumortherapie (Abels R. 1993)
• Erythropoetin-Gabe
© KSW 5-08

Blutkonserven in der Onkologie
• entscheidend: klinische Symptomatik(bei onkologischen Patienten v.a. Fatigue)
• Bei Notwendigkeit eines schnellen Hb-Anstiegs
• Notwendigkeit einer Transfusion nach Hb:– Hb < 6 praktisch immer
– Hb < 8 oft
– Hb < 10 selten (nur bei schweren Begleiterkrankungen)
• bei reduzierter EPO-Empfindlichkeit
© KSW 5-08

• Medizinische Transfusionsrisken:– Immunologisch
• Unmittelbare Transfusionsreaktionen• GvHD• Allo-Immunisierung• Immunsuppression• Acute lung injury
– Volumenüberladung– Eisenüberladung– Infektionsrisiko
• Organisatorische Transfusionsrisken:– Fehltransfusion– Hohes Alter des Erythrozytenkonzentrats
• Weitere Probleme:– Verfügbarkeit– Kosten
Transfusionsrisiken
© KSW 5-08

Nichthämolytische Reaktionen:(z.B. durch Eiweißunverträglichkeiten Zytokinausschüttung)
– Fieber, Schüttelfrost, Übelkeit, Kopfschmerzen, RR-Abfall bis zumanaphylaktischen Schock
– Acute lung injury
Hämolytische Reaktionen(Fehltransfusion oder andere Antikörperreaktionen)
– Akut mit Fieber, Schüttelfrost, RR-Abfall, Kreislaufschock;– Verzögert (Protrahiert)
Bakteriell bedingte Reaktionen(v.a. endotoxinbildende Keime)
– Mit Schüttelfrost, Fieber, Hyperventilation bis Schocksymptomatik
Immunologische Transfusionsrisiken
© KSW 5-08

Allogene Bluttransfusion – mehr Infektionen
Jensen et al.; Lancet 1996
05
10152025303540
Infektionsrate (%)
postop. Wundinfektion nicht Op.-bedingteInfektion
Immunsuppression durch allogenes Blut
Buffy coat depl. Konserven Leukozytendepletierte Konserven
© KSW 5-08

Allogene Bluttransfusion –schlechteres Überleben?
Amato et al, Cochrane Database 2006
• Cochrane Review 2006:
• 36 Studien aus 237 Referenzen
• Moderate Assoziation zwischen Rezidivrisiko beikolorektalem Karzinom und perioperativenTransfusionen
• OR 1.42 (95% CI 1.20-1-67)
• vorsichtige Indikationsstellung für perioperativeTransfusionen bei kurativ operierten Karzinompatienten
© KSW 5-08

Andere med. Transfusionsrisiken
• Volumenüberladung – kardiale Dekompensation• Eisenüberladung• Infektionsrisiko
– HIV ca. 1: 5 Mio, HCV ca. 1: 5 Mio., HBV ca. 1: 230.000.3 (PCR-Test, in Ö gesetzlich).
– Die Virus-C-Hepatitis ist in mehr als 90% der Fälle eineTransfusionshepatitis!
– Getestet wird in Ö: HIV, HCV, HBV, Ringelröteln, Lues, der LeberwertGPT und Neopterin (= unspezifischer Infektionsmarker)2
• Weitere Infektionsrisiken (nicht getestet)– Sämtliche Tropenerkrankungen (Malaria, Leishmaniosen, Chagas-
Krankheit, Dengue-Fieber etc) – Zunahme durch verstärkteReisetätigkeiten
– Prionenerkrankungen oder Retroviren
© KSW 5-08

Transfusionsassoziiertes Infektionsrisiko
© KSW 5-08

Häufigkeit von Transfusionsrisiken
© KSW 5-08

Anämiebehandlung beim Tumorpatienten
• prinzipiell kausal und individuell
• Erythrozyten-Substitution• in D.: 3 Mio EK/Jahr; davon > 50% bei
Tumoroperationen (Heiss M; 2000)
• in USA: 1 Mio EK/J v.a. in der palliativen Tumortherapie (Abels R. 1993)
• Erythropoetin-Gabe
© KSW 5-08

Die physiologische Aufgabe von Erythropoetin
Abnahme der O2-Versorgung der Niere
Peritubuläre interstitielle Zellen detektieren niedrigen O2-Gehalt im Blut
Pro-Erythroblasten im Knochenmark reifen schneller zu Retikulozyten
Mehr Retikulozytenim peripheren Blut
Größere Anzahl von Erythrozyten (RBC)im Blutkreislauf
Steigende O2 -Abgabe ins Gewebe
Rückkehr zur Homöostasis sobald sich dieO2-Versorgung der Niere normalisiert hat
EPO
Peritubuläre interstitielle Zellensezernieren Erythropoetin (EPO)in das Blut
© KSW 5-08

Erythropoetin - Charakteristika
• Glykoprotein: 165 AS, 4 KH-Seitenketten
• induziert Proliferation, Differenzierung und Ausreifung erythroider Vorläuferzellen
• hemmt die Apoptose erythroider Stammzellen
• normaler Plasmaspiegel: 10-25 U/l (3-7 pmol/l)
• Bei 02-Mangel: nach ca 1,5 h Anstieg der EPO-Konz.
© KSW 5-08

Die Geschichte von rHuEPO
• In den späten 1980ern von Amgen entwickelt• Dzt verfügbar:
– Epoetin alfa (Erypo®)– Epoetin beta (NeoRecormon ®)– Darbepoetin (Aranesp ®)
• Längere HWZ durch längerenKohlehydratanteil
• Gruppe: ESA (erythropoietin-stimulating agent)
rHuEPO
© KSW 5-08

ESAs führen zu Hb-Anstieg
Zyklus 1 Zyklus 2 Zyklus 3 Zyklus 4 Zyklus 5
Chemotherapie-Zyklus
AsynchronSynchron
Mitt
lere
r Hb-
Ans
tieg
(g/d
l)
Glaspy J, Henry D, Patel R, et al. European Journal of Cancer 2005 © KSW 5-08

Hb-Anstieg bei versch. Tumortypen gleich
© KSW 5-08

Effektivität von ESAs wöchentlich
Meta-Analyse von 4296 Patienten, wöchentliches Epoetin –alfa:Signifikante Reduktion der Transfusionshäufigkeit
Gascon et al: Ann Oncol 2006 © KSW 5-08

25 %
46 %
0 %5 %
10 %15 %20 %25 %30 %35 %40 %45 %50 %
Plazebo (n = 50) Aranesp® (n = 188)
trans
fusi
onsp
flich
tige
Pat
ient
en (%
)
Effektivität von ESAs 3-wöchentlich
Kotasek D, et al. Eur J Cancer. 2003:39:2026-2034. © KSW 5-08

Definition Response auf ESA-Therapie
© KSW 5-08

Verträglichkeit von ESAs – Vergleich mit Placebo
bei ≥ 15% der Patienten38%
32%
22%
21%
21%
19%
18%
15%
9%
33%
39%
20%
18%
20%
18%
14%
8%
18%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Übelkeit
Fatigue
Erbrechen
Verstopfung
Diarrhoe
Dyspnoe
Bauchschmerzen
Periphere Ödeme
Knochenschmerzen
Aranesp® (n = 198)
Plazebo (n = 51)
Kotasek D, et al. Eur J Cancer. 2003:39:2026-2034. © KSW 5-08

Zulassungsdaten von ESAs: Signifikante Reduktion der Transfusionshäufigkeit
ESA zugelassene Indikationen in der Onkologie:Patienten:
• Mit nicht-myeloischen Malignomen• Unter Chemotherapie für mindestens 2 Monate• Um die Transfusionshäufigkeit zu reduzieren
© KSW 5-08

ESA Zulassungs-Eckpunkte
© KSW 5-08

ESA-Verschreibungen USA 2002-07
FDA Briefing Document for ODAC 2008 © KSW 5-08
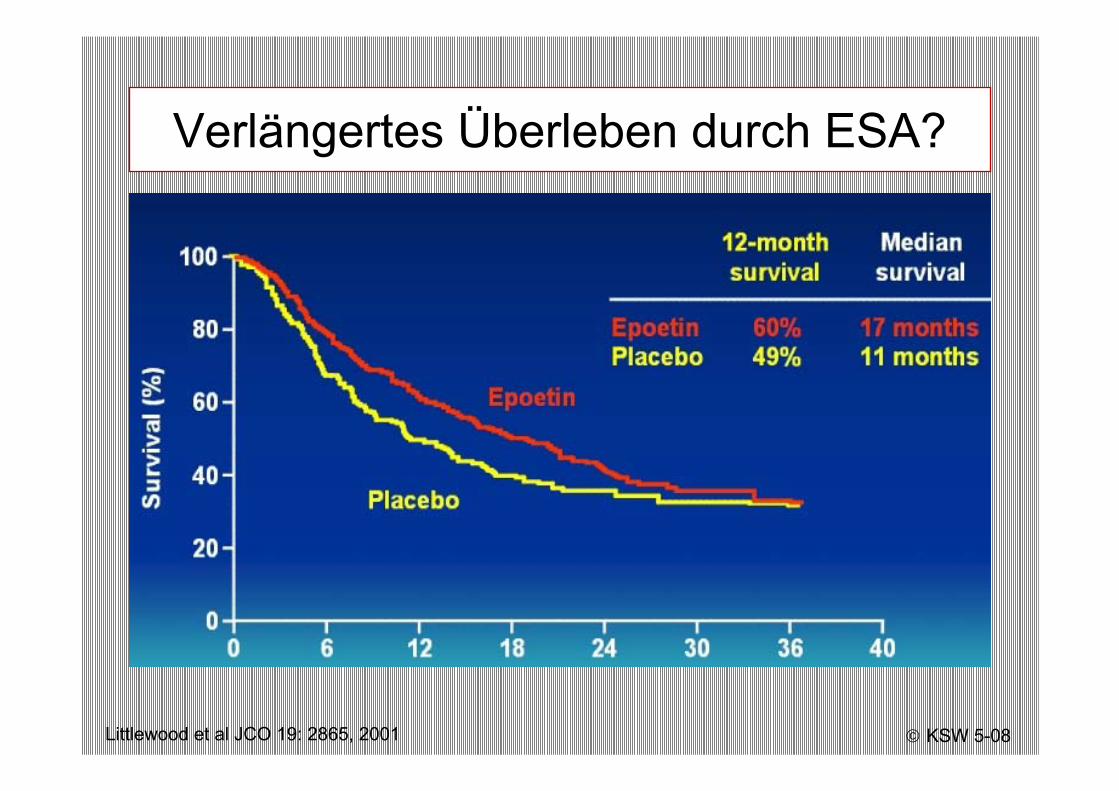
Verlängertes Überleben durch ESA?
Littlewood et al JCO 19: 2865, 2001 © KSW 5-08

Verkürztes Überleben durch ESA?
Henke et al, Lancet 2003
SCCHN während Radiatio; Trigger: Hb 12-13
© KSW 5-08

Verkürztes Überleben durch ESA?
Leyland-Jones JCO 2005
Mamma-CA während Chemotherapie
© KSW 5-08

Epoietin Beta Meta-Analyse
Aapro, Br J Cancer 2006
9 Studien; OS nicht primärer Endpunkt; Log-rank test P=0.87
© KSW 5-08

Unabhängige Meta-Analysen
Bohius JNCI 2006
Epoietin alfa und beta; Daten bis 2006
© KSW 5-08

Cochrane-Subgruppen
Bohius JNCI 2006 © KSW 5-08

Rezente Studien mit Survival-Endpunkt
© KSW 5-08

Neg. Studien: ESA + Chemotherapie
FDA Briefing Document for ODAC 2008 © KSW 5-08

Neg. Studien: ESA + Radiatio
FDA Briefing Document for ODAC 2008 © KSW 5-08

Neg. Studien: ESA ohne Radiatio/Chemo
FDA Briefing Document for ODAC 2008 © KSW 5-08

Benett JAMA 2008
Meta-Analyse 2008
Mortalität in onkologischen Phase-III Studien mit ESA vs Placebo/Kontrolle:„ANEMIA OF CANCER“
HR 1.29, 95% CI 1.00-1.67, P=.05
© KSW 5-08

Benett JAMA 2008
Meta-Analyse 2008
„TREATMENT-RELATED ANEMIA“
HR 1.09, 95% CI 0.99-1.19, n.s.
•GESAMT: n=13 61151 Phase-III StudienHR (Mortalität) 1.10 (95% CI 11.01-1.20, P=.03)
OR (TVT) 1.57 (95% CI 1.31-1.87)
© KSW 5-08

• Use the lowest dose of ESAs that will gradually increase thehemoglobin concentration to the lowest level sufficient to avoidblood transfusions.
• ESAs increased the risk for death and for serious cardiovascularevents when administered to target a hemoglobin greater than 12g/dL.
• A higher incidence of deep venous thrombosis was documented in patients receiving epoetin alfa pre-operatively for reduction of allogeneic blood transfusions. These patients did not receiveprophylactic anticoagulation.
• FDA reminds physicians that ESAs are approved for the reduction in red blood cell transfusions.
• These products have not been shown to improve or relieve the symptoms of anemia nor to improve quality of life in patients with cancer.
FDA Safety Update 2007
© KSW 5-08

• Anämie als kausalen Faktor für Symptome identifizieren
• Falls möglich Behandlung der Ursache
• Beginn ESA-Therapie bei Hb < 10 mit Zielwert 10-12 bei Patienten unter laufender Chemotherapie für noch mind. 2 Monate
• Ende ESA-Therapie bei Nichtansprechen nach 4-6 Wochen oder Ende Chemotherapie oder Hb > 12
• Gabe von Transfusionen bei stark symptomatischen Patienten mit mittelgradiger oder schwerer Anämie und Notwendigkeit eines raschen Hb-Anstiegs oder ESA-Non-Responder
ESA vs Konserven -Zusammenfassung
© KSW 5-08

Vielen Dank!
K. Strasser-WeipplZentrum für Hämatologie und Onkologie
Wilhelminenspital
Related Documents