2005;79:1724-1730 Ann Thorac Surg Ingemansson and Malin Malmsjö Angelica Wackenfors, Ronny Gustafsson, Johan Sjögren, Lars Algotsson, Richard Closure Therapy Blood Flow Responses in the Peristernal Thoracic Wall During Vacuum-Assisted http://ats.ctsnetjournals.org/cgi/content/full/79/5/1724 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 2, 2013 ats.ctsnetjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2005;79:1724-1730 Ann Thorac SurgIngemansson and Malin Malmsjö
Angelica Wackenfors, Ronny Gustafsson, Johan Sjögren, Lars Algotsson, Richard Closure Therapy
Blood Flow Responses in the Peristernal Thoracic Wall During Vacuum-Assisted
http://ats.ctsnetjournals.org/cgi/content/full/79/5/1724located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2005 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
BWALMDS
asesam
lnedcplc
itt
Mttmntoob
bsaiwtbp
A
As@
©P
GEN
ERA
LT
HO
RA
CIC
lood Flow Responses in the Peristernal Thoracicall During Vacuum-Assisted Closure Therapy
ngelica Wackenfors, MS, Ronny Gustafsson, MD, Johan Sjögren, MD,ars Algotsson, MD, PhD, Richard Ingemansson, MD, PhD, andalin Malmsjö, MD, PhD
epartments of Internal Medicine, Cardiothoracic Surgery, and Cardiothoracic Anesthesia, Lund University Hospital, Lund,
wedenbchwpp6mfl
aoenaflcc
Background. Vacuum-assisted closure (VAC) therapy isrecently introduced method for the treatment of post-
ternotomy mediastinitis. The aim of this study was toxamine the effects of negative pressure on peristernaloft tissue blood flow and metabolism because the mech-nisms by which vacuum-assisted closure therapy pro-otes wound healing are not known in detail.Methods. Microvascular blood flow was examined by
aser Doppler velocimetry in an uninfected porcine ster-otomy wound model. Microvascular blood flow wasxamined in the muscular and subcutaneous tissue, atifferent distances from the wound edge, after the appli-ation of �50 to �200 mm Hg. Wound fluid pH, partialressures of oxygen and carbon dioxide, bicarbonate, and
actate were analyzed after 0, 30, and 60 minutes ofontinuous negative pressure.
Results. Vacuum-assisted closure therapy induced anncrease in the microvascular blood flow a few centime-ers from the wound edge. In muscular tissue, the dis-
ance from the wound edge to the position at which thehtttwvm
flamptcpette(ows
earch, BMC A13, SE-221 84 Lund, Sweden; e-mail: angelica.wackenforsmed.lu.se.
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
lood flow was increased was shorter than that in sub-utaneous tissue. Close to the wound edge, relativeypoperfusion was observed. The hypoperfused zoneas larger at high negative pressures and was especiallyrominent in subcutaneous tissue. Wound fluid partialressure of oxygen and lactate levels were increased after0 minutes of vacuum-assisted closure therapy, whichay be the result of changes in the microvascular blood
ow.Conclusions. Vacuum-assisted closure therapy induceschange in microvascular blood flow that is dependent
n the pressure applied, the distance from the wounddge, and the tissue type. It may be beneficial to tailor theegative pressure used for vacuum-assisted closure ther-py according to the wound tissue composition. Wounduid partial pressure of oxygen and lactate levels in-reased during vacuum-assisted closure therapy. Thisombination is known to promote wound healing.
(Ann Thorac Surg 2005;79:1724–31)
© 2005 by The Society of Thoracic Surgeonsediastinitis is a devastating complication in openheart surgery. Vacuum-assisted closure (VAC)
herapy is a recently introduced technique that promoteshe healing of difficult wounds, including poststernotomy
ediastinitis [1]. The technique entails application of aegative pressure to a sealed, airtight wound. The suc-
ion force created by VAC therapy enables the drainagef excessive fluid and debris, which leads to the removalf wound edema, reduction in bacterial counts, enhancedlood flow, and granulation tissue formation [1–4].The physiologic, cellular, and molecular mechanisms
y which VAC therapy accelerates wound healing aretill not known in detail. Tissue perfusion and oxygen-tion are crucial to ensure healing [5]. The two mostmportant risk factors for developing a deep sternalound infection are diabetes and the use of internal
horacic arteries as bypass grafts [6, 7], both of which areelieved to decrease the peristernal soft tissue blooderfusion. Laser Doppler velocimetry measurements
ccepted for publication Oct 28, 2004.
ddress reprint requests to Ms Wackenfors, Experimental Vascular Re-
ave shown that VAC induces an increase in blood flowo a wound on the back of pigs [4]. Enhancing blood flowo the soft tissue of the peristernal wound may be one ofhe mechanisms by which VAC therapy facilitates sternalound healing. To evaluate this hypothesis, the micro-
ascular blood flow was studied by laser Doppler veloci-etry in a porcine sternotomy wound model.Previous observations show that microvascular blood
ow to a wound on the back of pigs increases four timesbove baseline value when a negative pressure of 125m Hg is applied, whereas it is inhibited at negative
ressures of 400 mm Hg and above [4]. Even though theissue type and distance from the wound edge were notonsidered in the above-mentioned study, a negativeressure of 125 mm Hg was selected for subsequentxperiments and is currently the pressure of choice forhe clinical treatment of poststernotomy mediastinitis. Inhe present study, the microvascular blood flow wasxamined in detail using different negative pressures�50 to �200 mm Hg) in an uninfected porcine sternot-my wound model. Subcutaneous and muscular tissuesere studied separately, and the blood flow was mea-
ured at different distances from the sternal wound edge.
0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.10.053
by on June 2, 2013 als.org

Tffwtdmd
M
AAfofaLpa“pSH
AKittmVtdnfapCnoca
LMoPLtaimLcialt
ilpt(wpews5awetwtoiiwmcfb
BTam“rtVcttwaahu
CTpVsstttctp
R
V
1725Ann Thorac Surg WACKENFORS ET AL2005;79:1724–31 VAC THERAPY OF STERNOTOMY WOUNDS
GEN
ERA
LT
HO
RA
CIC
he aim was to determine the optimal negative pressureor stimulating peristernal microvascular blood flow andor the treatment of deep sternal wounds. Wound fluidas trapped in the VAC tubing and analyzed with regard
o pH, partial pressures of oxygen (Po2) and carbonioxide (Pco2), bicarbonate, and lactate to evaluate theetabolic effects of altered microvascular blood flow
uring VAC therapy.
aterial and Methods
nimalsn uninfected porcine sternotomy wound model was use
or the present study. Nineteen domestic Landrace pigsf both sexes, with a mean body weight of 70 kg, wereasted overnight with free access to water. The study waspproved by the Ethics Committee for Animal Research,und University, Sweden, which conforms to the princi-les outlined in the Declaration of Helsinki. All thenimals received humane care in compliance with theGuide for the Care and Use of Laboratory Animals” asromulgated by the Council of the American Physiologicociety and published by the National Institutes ofealth (1985).
nesthesia and Surgical Procedureetamine was used for premedication. Anesthesia was
nduced by intravenous sodium thiopental and main-ained by continuous infusion of pentobarbital and fen-anyl. Pancuronium was given intravenously to achieve
uscle paralysis. The pigs were surgically prepared forAC therapy. A midline sternotomy was performed, and
he pericardium was opened. A polyurethane foamressing was placed between the sternal edges. Twooncollapsible drainage tubes were inserted into the
oam. The open wound was sealed with a transparentdhesive drape. The drainage tubes were connected to aurpose-built vacuum source (VAC pump unit; KCI,openhagen, Denmark), which delivered a continuousegative pressure of �50, �75, �100, �125, �150, �175,r �200 mm Hg. For details, see the study by Sjögren andolleagues [8], in which identical settings were used. Forschematic illustration, see Figure 1.
aser Doppler Velocimetryicrovascular blood flow was measured in 7 pigs by use
f laser Doppler velocimetry, using the multichanneleriFlux System 5000 (Perimed, Stockholm, Sweden).aser Doppler velocimetry is a technique that quantifies
he sum of motion of red blood cells in a specific volumend has been applied extensively to measure blood flown flaps during plastic surgery procedures [9, 10]. In this
ethod, a fiberoptic probe carries a beam of laser light.ight impinging on moving blood cells undergoes ahange in wavelength (Doppler shift), whereas lightmpinging on static objects is unchanged. The magnitudend frequency distribution of these changes in wave-ength are directly related to the number and velocity of
he blood cells. The information is collected by a return- tats.ctsnetjournDownloaded from
ng fiber, converted into an electronic signal and ana-yzed. In the current experiments, 0.5-mm filamentrobes (probe 418-1; Perimed) were inserted into subcu-
aneous and deep muscular tissue at 1-cm incrementsrange, 0.5 to 4.5 cm) from the wound edge. Recordingsere made with three parallel probes. The probes werelaced randomly at different distances from the wounddge. A skin probe was placed 10 cm from the wound andas not moved during the entire experiment. For a
chematic illustration, see Figure 1. Negative pressures of0, 75, 100, 125, 175, and 200 mm Hg were randomlypplied to the wound, and the microvascular blood flowas measured continuously. The laser Doppler velocim-
try experiments were performed on 7 pigs for eachissue and negative pressure. The results were comparedith the baseline blood flow immediately before the VAC
herapy was initiated. Each animal thereby served as itswn control. The experiments were concluded by admin-
stering 0.5 mg/kg adenosine triphosphate (Sigma Chem-cal Co, St. Louis, MO) intravenously, and the blood flowas measured in the skin and in the subcutaneous anduscular tissue to test the probes and equipment. Mi-
rovascular blood flow was expressed in terms of “per-usion units,” and the output was continuously registeredy the PeriSoft software.
lood and Wound Fluid Sampleswelve pigs underwent the surgical procedure describedbove. Six pigs were treated with VAC therapy of �75m Hg, and another 6 were used as controls termed
sham therapy.” Arterial blood was sampled from theight carotid artery, and venous blood was sampled fromhe right external jugular vein. Wound fluid from theAC-treated pigs was sampled from the drainage tube,
lose to the wound edge. Wound fluid from the sham-reated pigs was drawn from a tube that was inserted intohe substernal cavity in the upper part of the sternotomyound, not in contact with the heart. Wound fluid and
rterial and venous blood Po2, Pco2, bicarbonate, pH,nd lactate were analyzed (ABL 725; Radiometer Copen-agen, Brönshöj, Denmark) immediately before (0 min-tes) and after 30 and 60 minutes of VAC therapy.
alculations and Statisticshe laser Doppler experiments were performed on 7igs, and the blood and wound fluid was sampled from 6AC-treated and 6 sham-treated pigs. Calculations and
tatistical analysis were performed using GraphPad 4.0oftware (GraphPad Software Inc, San Diego, CA). Sta-istical significance was defined as p less than 0.05, usinghe Mann-Whitney test when comparing two groups andhe Kruskal-Wallis test with Dunnett’s post hoc test whenomparing three groups or more. All differences referredo in the text have been statistically verified. Values areresented as mean � standard error of the mean.
esults
acuum-assisted closure therapy induced an increase in
he peristernal soft tissue and muscle tissue blood flowby on June 2, 2013 als.org
(w(tibc1(tip
caolp�
t�fsnm
icatisti8i�tmevitlc
crW
Fc(etiebduwmtpflfe
Faif
1726 WACKENFORS ET AL Ann Thorac SurgVAC THERAPY OF STERNOTOMY WOUNDS 2005;79:1724–31
GEN
ERA
LT
HO
RA
CIC
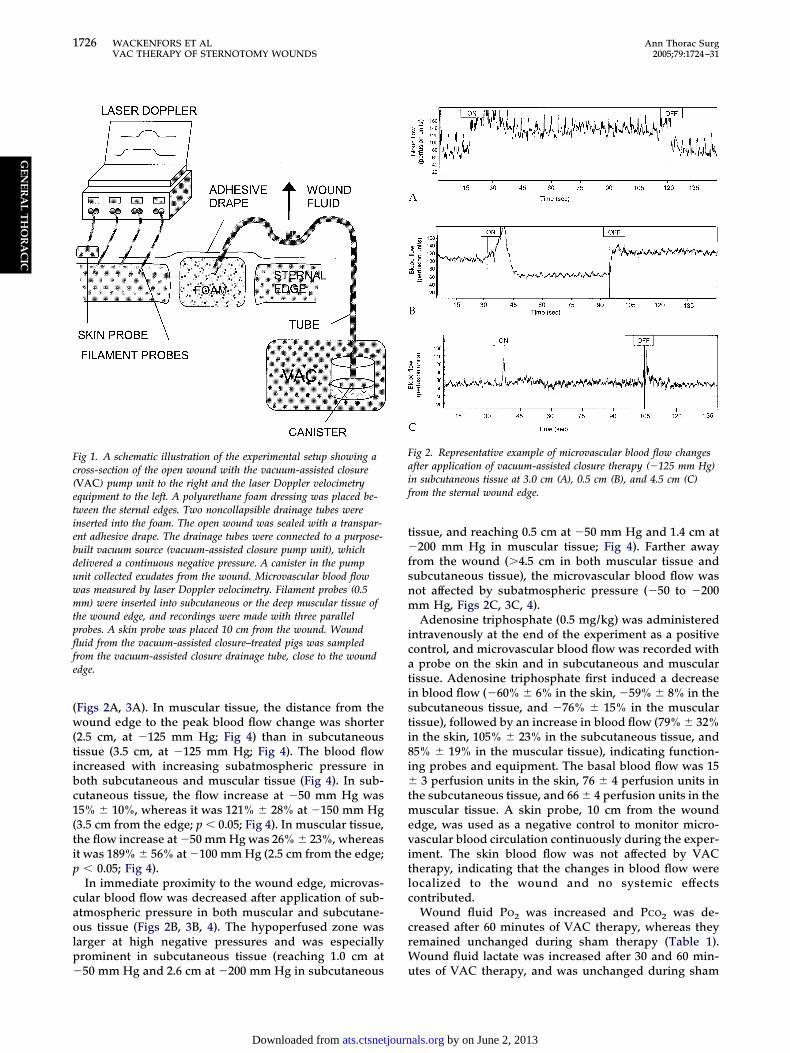
Figs 2A, 3A). In muscular tissue, the distance from theound edge to the peak blood flow change was shorter
2.5 cm, at �125 mm Hg; Fig 4) than in subcutaneousissue (3.5 cm, at �125 mm Hg; Fig 4). The blood flowncreased with increasing subatmospheric pressure inoth subcutaneous and muscular tissue (Fig 4). In sub-utaneous tissue, the flow increase at �50 mm Hg was5% � 10%, whereas it was 121% � 28% at �150 mm Hg3.5 cm from the edge; p � 0.05; Fig 4). In muscular tissue,he flow increase at �50 mm Hg was 26% � 23%, whereast was 189% � 56% at �100 mm Hg (2.5 cm from the edge;
� 0.05; Fig 4).In immediate proximity to the wound edge, microvas-
ular blood flow was decreased after application of sub-tmospheric pressure in both muscular and subcutane-us tissue (Figs 2B, 3B, 4). The hypoperfused zone was
arger at high negative pressures and was especiallyrominent in subcutaneous tissue (reaching 1.0 cm at
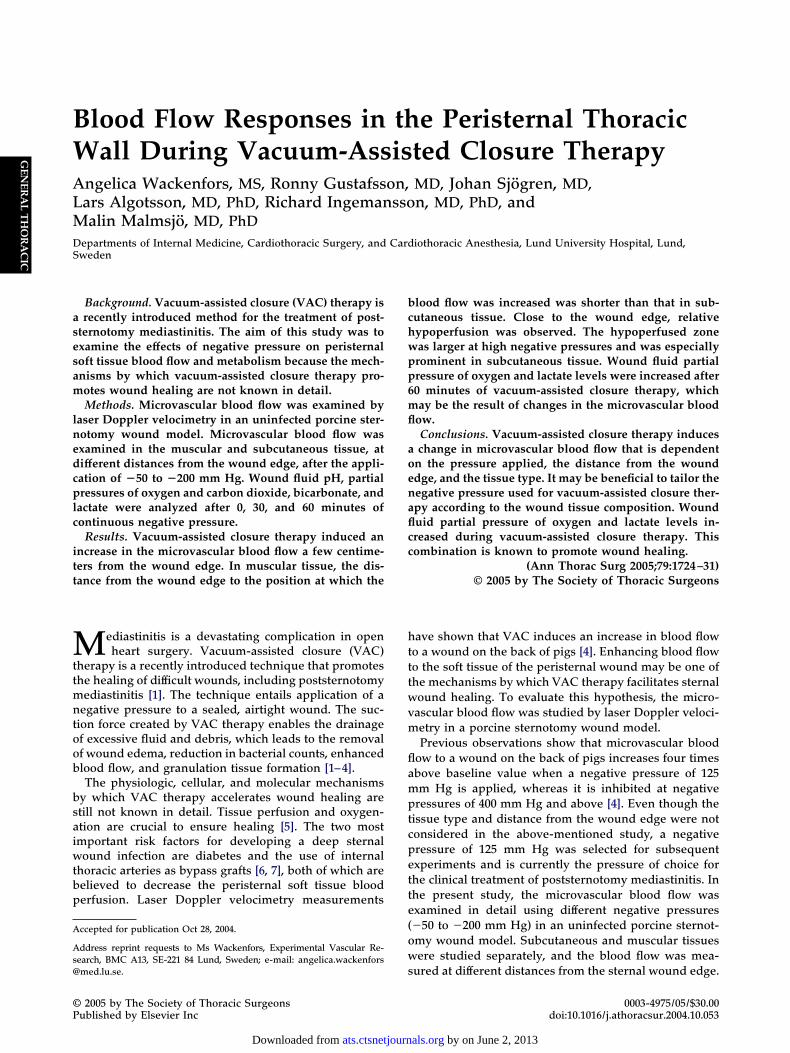
ig 1. A schematic illustration of the experimental setup showing aross-section of the open wound with the vacuum-assisted closureVAC) pump unit to the right and the laser Doppler velocimetryquipment to the left. A polyurethane foam dressing was placed be-ween the sternal edges. Two noncollapsible drainage tubes werenserted into the foam. The open wound was sealed with a transpar-nt adhesive drape. The drainage tubes were connected to a purpose-uilt vacuum source (vacuum-assisted closure pump unit), whichelivered a continuous negative pressure. A canister in the pumpnit collected exudates from the wound. Microvascular blood flowas measured by laser Doppler velocimetry. Filament probes (0.5m) were inserted into subcutaneous or the deep muscular tissue of
he wound edge, and recordings were made with three parallelrobes. A skin probe was placed 10 cm from the wound. Wounduid from the vacuum-assisted closure–treated pigs was sampled
rom the vacuum-assisted closure drainage tube, close to the wounddge.
50 mm Hg and 2.6 cm at �200 mm Hg in subcutaneous u
ats.ctsnetjournDownloaded from
issue, and reaching 0.5 cm at �50 mm Hg and 1.4 cm at200 mm Hg in muscular tissue; Fig 4). Farther away
rom the wound (�4.5 cm in both muscular tissue andubcutaneous tissue), the microvascular blood flow wasot affected by subatmospheric pressure (�50 to �200m Hg, Figs 2C, 3C, 4).Adenosine triphosphate (0.5 mg/kg) was administered
ntravenously at the end of the experiment as a positiveontrol, and microvascular blood flow was recorded withprobe on the skin and in subcutaneous and muscular
issue. Adenosine triphosphate first induced a decreasen blood flow (�60% � 6% in the skin, �59% � 8% in theubcutaneous tissue, and �76% � 15% in the muscularissue), followed by an increase in blood flow (79% � 32%n the skin, 105% � 23% in the subcutaneous tissue, and5% � 19% in the muscular tissue), indicating function-ng probes and equipment. The basal blood flow was 15
3 perfusion units in the skin, 76 � 4 perfusion units inhe subcutaneous tissue, and 66 � 4 perfusion units in the
uscular tissue. A skin probe, 10 cm from the wounddge, was used as a negative control to monitor micro-ascular blood circulation continuously during the exper-ment. The skin blood flow was not affected by VACherapy, indicating that the changes in blood flow wereocalized to the wound and no systemic effectsontributed.
Wound fluid Po2 was increased and Pco2 was de-reased after 60 minutes of VAC therapy, whereas theyemained unchanged during sham therapy (Table 1).
ound fluid lactate was increased after 30 and 60 min-
ig 2. Representative example of microvascular blood flow changesfter application of vacuum-assisted closure therapy (�125 mm Hg)n subcutaneous tissue at 3.0 cm (A), 0.5 cm (B), and 4.5 cm (C)rom the sternal wound edge.
tes of VAC therapy, and was unchanged during sham
by on June 2, 2013 als.org

tncbtt
C
DtlehflbdtmnaiptniTdn
ibbdistcbmpiOfbscbflew[bwidmwt
Fait
Ftdtom
1727Ann Thorac Surg WACKENFORS ET AL2005;79:1724–31 VAC THERAPY OF STERNOTOMY WOUNDS
GEN
ERA
LT
HO
RA
CIC
herapy (Table 1). Wound fluid pH and bicarbonate wereot altered by VAC or sham therapy (Table 1). Nohanges were observed in systemic arterial or venouslood pH, bicarbonate, Po2, Pco2, or lactate during VAC
herapy (Table 1), indicating that the alteration seen inhe wound fluid was the result of local effects.
omment
espite the extensive clinical use of VAC therapy for thereatment of deep sternal wound infections, the physio-ogic, cellular, and molecular mechanisms are to a largextent unknown. A subatmospheric pressure of 125 mm Hgas been shown to be optimal because it increases bloodow to a wound on the pig back, although only the peaklood flow was measured and the tissue type and theistance from the wound edge were not considered at that
ime [4]. A negative pressure of 125 mm Hg is now com-only used for the treatment of poststernotomy mediasti-
itis [11] and is preferred because it stabilizes the sternumnd allows early mobilization. When VAC therapy is usedn a sternotomy wound, patients sometimes experienceain, and the pressure may have to be reduced. The soft
issue effects of VAC treatment in a sternotomy wound haveot been described earlier and may be an important issue
n the choice of wound-healing strategy for mediastinitis.o delineate the blood flow changes in the wound edgeuring VAC therapy in detail, an uninfected porcine ster-otomy wound model was used.
ig 3. Representative example of microvascular blood flow changesfter application of vacuum-assisted closure therapy (�125 mm Hg)n muscular tissue at 2.0 cm (A), 0.5 cm (B), and 4.5 cm (C) fromhe sternal wound edge.
Vacuum-assisted closure therapy induced an increase t
ats.ctsnetjournDownloaded from
n the peristernal soft tissue blood flow. The change inlood flow is probably related to local effects because thelood flow was not affected by the negative pressure at aistance of 4.5 cm from the wound edge. The blood flow
ncreased with elevated subatmospheric pressure in bothubcutaneous and muscular tissue. When the area underhe flow-distance curve was analyzed, covering 0.5 to 4.5m from the wound edge, a maximal net increase inlood flow was observed at �75 and �100 mm Hg, inuscular tissue. There is a discrepancy between the
resent results and previous data that show a peakncrease in wound edge blood flow at �125 mm Hg [4].
ne explanation of this discrepancy may be that theormer study was performed on a wound on the pigs’ack, whereas the present study is performed on aternotomy wound. The differences in wound tissueomposition may alter the effects of negative pressure onlood flow. Furthermore, in the present study, the bloodow was analyzed in detail 0.5 to 4.5 cm from the wounddge at 1-cm increments, whereas no specific distancesere analyzed in the study by Morykwas and associates
4]. Vacuum-assisted closure therapy has been shown toe advantageous in infected or nonhealing chronicounds, but not in acutely injured wounds [12]. An
nfected wound is often edematous and perfusion isecreased, leading to decreased nutrition of the woundargins. Vacuum-assisted closure therapy decreasesound edema [2] and improves blood flow, as shown in
he present study. The effects of VAC therapy may
ig 4. Microvascular blood flow in subcutaneous (Œ) and muscularissue (�), at increasing distance from the sternal wound edge in 6omestic pigs after application of subatmospheric pressures of �50o �200 mm Hg. Changes in blood flow were calculated as percentf baseline flow and are presented as mean � standard error of theean.
herefore be even more pronounced in an infected
by on June 2, 2013 als.org

wf
flndbtamVcttsws
wdfsmiwbbpnzaht
TL
V
W
A
V
a
h
H Po2 �
1728 WACKENFORS ET AL Ann Thorac SurgVAC THERAPY OF STERNOTOMY WOUNDS 2005;79:1724–31
GEN
ERA
LT
HO
RA
CIC
ound than in this experimental setup using a nonin-ected acute sternotomy wound.
Interestingly, a difference in the profiles of the bloodow responses could be observed between the subcuta-eous and the muscular tissue. In muscular tissue, theistance from the wound edge to the point at which thelood flow increased was shorter than in subcutaneous
issue. Pressure may be transduced differently in a softnd in a dense tissue, and a less dense tissue collapsesore easily when affected by pressure. Thus, the effect ofAC therapy may vary according to the wound tissue
omposition. Currently, the pressure in the tubing guideshe VAC therapy. We suggest that the pressure transduc-ion in the tissue is of greater importance. To obtainimilar therapeutic effects of VAC therapy in differentounds, it may be beneficial to tailor the negative pres-
able 1. Wound Fluid and Arterial and Venous Blood Partialactate Immediately Before (0 minutes) and After 30 and 60 M
ariable Therapy
ound fluidPo2 (kPa) VAC 13
Sham 4Pco2 (kPa) VAC 2
Sham 3Lactate (mmol/L) VAC 2
Sham 2HCO3
� (mmol/L) VAC 26Sham 22
pH VAC 7Sham 7
rterial bloodPo2 (kPa) VAC 31
Sham 26Pco2 (kPa) VAC 4
Sham 5Lactate (mmol/L) VAC 1
Sham 1HCO3
� (mmol/L) VAC 29Sham 30
pH VAC 7Sham 7
enous bloodPo2 (kPa) VAC 3
Sham 4Pco2 (kPa) VAC 6
Sham 6Lactate (mmol/L) VAC
ShamHCO3
� (mmol/L) VAC 30Sham 30
pH VAC 7Sham 7
Values are presented as mean � standard error of the mean. b Statistoc test (p � 0.05). Values obtained at 30 and 60 minutes were compared
CO3� � bicarbonate; Pco2 � partial pressure of carbon dioxide;
ure according to wound tissue composition. s
ats.ctsnetjournDownloaded from
This study shows that the changes in the peristernalound blood flow caused by VAC therapy vary with theistance from the wound edge. A few centimeters away
rom the wound edge, the blood flow increases whenubatmospheric pressure is applied. Conversely, in im-ediate proximity to the wound, the negative pressure
nduces relative hypoperfusion. Pressure against theound wall may be beneficial during surgical proceduresecause it has been shown to tamponade superficialleeding [13]. On the other hand, long-standing hypo-erfusion may cause ischemia. To balance these effects, aegative pressure that does not cause a large ischemicone, but still eliminates interstitial fluid accumulationnd bleeding, may be preferable. In muscular tissue, theypoperfused zone is smaller than in the subcutaneous
issue, which may be attributable to the easier collapse of
sures of Oxygen and Carbon Dioxide, Bicarbonate, pH, andtes of Vacuum-Assisted Closure Therapya
in 30 min 60 min
1.70 21.58 � 1.48 24.20 � 2.11b
0.83 4.56 � 0.06 4.71 � 0.280.50 0.64 � 0.28b 1.62 � 0.61b
0.91 5.23 � 0.26 3.24 � 0.700.30 4.57 � 0.40b 4.88 � 0.34b
0.18 2.87 � 0.38 3.00 � 0.344.60 17.99 � 2.46 20.26 � 2.255.30 29.56 � 0.73 22.08 � 7.120.09 8.01 � 0.20 7.87 � 0.130.06 7.53 � 0.02 7.52 � 0.05
1.67 30.82 � 0.60 27.65 � 1.711.79 29.72 � 1.35 23.50 � 1.350.19 4.89 � 0.10 4.83 � 0.170.44 4.74 � 0.45 4.93 � 0.380.29 1.72 � 0.19 1.47 � 0.190.26 1.30 � 0.27 1.15 � 0.051.31 29.45 � 1.15 28.87 � 1.030.22 29.90 � 0.00 29.70 � 0.940.02 7.52 � 0.02 7.51 � 0.030.03 7.54 � 0.04 7.51 � 0.02
0.34 4.45 � 0.38 4.72 � 0.440.56 4.65 � 0.68 4.80 � 0.300.29 5.98 � 0.34 6.20 � 0.260.55 5.45 � 0.15 5.79 � 0.59
. . . . . . .
. . . . . . .1.12 31.58 � 0.89 31.64 � 1.130.63 23.77 � 5.20 29.20 � 2.390.02 7.41 � 0.05 7.44 � 0.030.03 7.46 � 0.03 7.43 � 0.03
alyses were performed using the Kruskal-Wallis test with Dunnett’s postthose before therapy was started (0 minutes).
partial pressure of oxygen; VAC � vacuum-assisted closure.
Presinu
0 m
.22 �
.73 �
.68 �
.42 �
.01 �
.27 �
.70 �
.08 �
.77 �
.47 �
.73 �
.01 �
.79 �
.17 �
.68 �
.30 �
.28 �
.70 �
.52 �
.49 �
.95 �
.95 �
.07 �
.18 �
. .
. ..80 �
.52 �
.44 �
.22 �
ical anwith
oft tissue during pressure. The size of the hypoperfused
by on June 2, 2013 als.org

za
cPwtpzflttrssAoseslanV
ahpHiasaptaeibptLblpTtttttswifletiba
bPettbTwSpbsbnpc
cetIrlptatcmtzitflmdoewmh
TtciHf
R
1729Ann Thorac Surg WACKENFORS ET AL2005;79:1724–31 VAC THERAPY OF STERNOTOMY WOUNDS
GEN
ERA
LT
HO
RA
CIC
one depends on the subatmospheric pressure applied,nd increases with increasing pressure.To evaluate the nutritive effects of the blood flow
hanges in the uninfected sternotomy wound edge, pH,o2, Pco2, bicarbonate, and lactate were analyzed in theound fluid at �75 mm Hg. This pressure was chosen on
he basis of the blood flow studies, in which �75 mm Hgroduced a high net increase in blood flow and a smallone of relative hypoperfusion. When analyzing wounduid factors, it was found that Po2 increased during VAC
herapy at �75 mm Hg. This increase in oxygen supply tohe peristernal wound edges may well have been theesult of the change in microvascular blood flow demon-trated by the laser Doppler experiments. Blood perfu-ion and oxygenation are crucial to ensure healing [5].lready in 1969, Hunt and coworkers [14] suggested thatxygen was required for the oxidation of metabolicubstrates by inflammatory cells present in the woundnvironment. Oxygen is an essential cofactor in collagenynthesis, and participates in the regulation of cell pro-iferation [14]. Oxygen is also important in the defensegainst infections [15]. This may be one of the mecha-isms by which the wound repair process is facilitated byAC therapy.Wound fluid lactate was increased during VAC ther-
py. One explanation of this increase may be the relativeypoperfusion that is created by the subatmosphericressure in the immediate proximity of the wound edge.owever, it has been shown that hypoxia only marginally
ncreases wound lactate [16], and ischemia produces ancidotic local wound effluent [17], which was not ob-erved in our study. More important sources of lactatere neutrophils, macrophages and fibroblasts, and otherroliferating cells that are present in the granulation
issue of wounds [18–20]. These cells produce largemounts of lactate through aerobic glycolysis [21]. Inter-stingly, our results showed that both Po2 and lactatencreased in the wound fluid during VAC therapy. It haseen shown that elevated lactate levels often are accom-anied by increased oxygen tension, and this combina-
ion appears to promote healing of wounds [16, 22, 23].actate stimulates wound granulation tissue formationy inducing collagen transcription and vascular endothe-
ial growth factor production, whereas increased Po2
romotes collagen deposition and angiogenesis [24–26].he increases in wound fluid Po2 and lactate observed in
he present experiments may initiate the granulationissue formation that has been demonstrated during VACherapy [4]. Because of the high pressure gradient acrosshe tissue in the close proximity of the VAC wound edge,his zone may be perfused by diffusion. This theory isupported by the high Po2 levels without acidosis in theound fluid and the fact that no development of necrosis
s observed clinically during VAC therapy. The wounduid variables were analyzed at �75 mm Hg, and theffects at �125 mm Hg therefore cannot be deduced fromhe present study. It may be assumed that �125 mm Hgnduces similar changes in Po2 and lactate concentrationsecause the blood flow to the wound edge increases also
t �125 mm Hg, although to a lesser extent.ats.ctsnetjournDownloaded from
A common practice in thoracic surgery is unilateral orilateral harvesting of the internal mammary arteries.ostoperative mediastinitis is more common when bilat-ral harvesting has been performed, especially in pa-ients with diabetes and obesity [6, 12, 27]. The reason forhe high risk of infection in these groups of patients maye that the soft tissue is poorly perfused postoperatively.he blood flow and the subsequent nutrition of theound edge may then not be sufficient for healing.timulating blood flow to the sternotomy wound edge inatients with diabetes or when bilateral harvesting haseen conducted may be crucial to ensure healing. Furthertudies aimed at optimizing sternotomy wound edgelood flow may lead to the development of safe tech-iques for wound closure in patients at high risk ofostoperative mediastinitis, eg, performing delayed sub-utaneous closure after a brief period of VAC therapy.
In conclusion, VAC therapy elicits an increase in mi-rovascular blood flow a few centimeters from the wounddge. The peak increase in blood flow occurred closer tohe wound edge in muscular than in subcutaneous tissue.n the immediate proximity of the wound edge, a zone ofelative hypoperfusion was observed. This zone wasarger at high negative pressures and was especiallyrominent in subcutaneous tissue. It may be concluded
hat the vacuum pressure is transduced differently in softnd dense tissue. Therefore, it may be beneficial to tailorhe VAC negative pressure according to the wound tissueomposition. A negative pressure of 75 or 100 mm Hgay be profitable because it effectively stimulates peris-
ernal soft tissue blood flow without producing a largeone of relative hypoperfusion. Wound fluid Po2 wasncreased and Pco2 decreased after 60 minutes of VACherapy, which may be a result of the changes in bloodow. Furthermore, lactate levels were increased, whichay be related to inflammation and rapid cell growth
uring granulation tissue formation. The combinationf increased Po2 and lactate levels in the woundnvironment has previously been reported to promoteound healing [16, 22, 23], and may in part explain theechanisms by which VAC therapy accelerates wound
ealing.
his study was supported by the Swedish Hypertension Society,he Swedish Medical Association, the Royal Physiographic So-iety (Lund), the Swedish Medical Research Council, the Med-cal Society in Lund, the Crafoord Foundation, the Swedish
eart-Lung Foundation, and the Swedish Government Grantor Clinical Research.
eferences
1. Domkowski PW, Smith ML, Gonyon DL Jr, et al. Evaluationof vacuum-assisted closure in the treatment of poststerno-tomy mediastinitis. J Thorac Cardiovasc Surg 2003;126:386–90.
2. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a newmethod for wound control and treatment: clinical experi-ence. Ann Plast Surg 1997;38:563–77.
3. Clare MP, Fitzgibbons TC, McMullen ST, et al. Experiencewith the vacuum assisted closure negative pressure tech-
by on June 2, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
I
Vswppefiwiecpiatigesvu
e
1730 WACKENFORS ET AL Ann Thorac SurgVAC THERAPY OF STERNOTOMY WOUNDS 2005;79:1724–31
©P
GEN
ERA
LT
HO
RA
CIC
nique in the treatment of non-healing diabetic anddysvascular wounds. Foot Ankle Int 2002;23:896–901.
4. Morykwas MJ, Argenta LC, Shelton-Brown EI, McGuirt W.Vacuum-assisted closure: a new method for wound controland treatment: animal studies and basic foundation. AnnPlast Surg 1997;38:553–62.
5. Jonsson K, Jensen JA, Goodson WHI, et al. Tissue oxygen-ation, anemia, and perfusion in relation to wound healing insurgical patients. Ann Surg 1991;214:605–13.
6. Gummert JF, Barten MJ, Hans C, et al. Mediastinitis andcardiac surgery—an updated risk factor analysis in 10,373consecutive adult patients. Thorac Cardiovasc Surg 2002;50:87–91.
7. Milano CA, Kesler K, Archibald N, Sexton DJ, Jones RH.Mediastinitis after coronary artery bypass graft surgery: riskfactors and long-term survival. Circulation 1995;92:2245–51.
8. Sjögren J, Gustafsson R, Wackenfors A, et al. Effects ofvacuum-assisted closure on central hemodynamics in asternotomy wound model. ICVTS. 2004;3:666–71.
9. Zografos GC, Martis K, Morris DL. Laser Doppler flowmetryin evaluation of cutaneous wound blood flow using varioussuturing techniques. Ann Surg 1992;215:266–8.
0. Larrabee WF Jr, Holloway GA Jr, Sutton D. Wound tensionand blood flow in skin flaps. Ann Otol Rhinol Laryngol1984;93(2 Pt 1):112–5.
1. Gustafsson RI, Sjögren J, Ingemansson R. Deep sternalwound infection: a sternal-sparing technique with vacuum-assisted closure therapy. Ann Thorac Surg 2003;76:2048–53.
2. Miller Q, Bird E, Bird K, Meschter C, Moulton MJ. Effect ofsubatmospheric pressure on the acute healing wound. CurrSurg 2004;61:205–8.
3. Sjögren J, Gustafsson R, Koul B, Ingemansson R. Selectivemediastinal tamponade to control coagulopathic bleeding.Ann Thorac Surg 2003;75:1311–3.
4. Hunt TK, Zederfeldt B, Goldstick TK. Oxygen and healing.Am J Surg 1969;118:521–5.
5. Mader JT, Brown GL, Guckian JC, Wells CH, Reinarz JA. Amechanism for the amelioration by hyperbaric oxygen ofexperimental staphylococcal osteomyelitis in rabbits. J Infect
Dis 1980;142:915–22.xperiments, have the obvious limitation of differing
feactcIuliciweddEVtotrp
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
6. Hunt TK, Conolly WB, Aronson SB, Goldstein P. Anaerobicmetabolism and wound healing: an hypothesis for the initi-ation and cessation of collagen synthesis in wounds. Am JSurg 1978;135:328–32.
7. Mazzoni MC, Cragoe EJ Jr, Arfors KE. Systemic bloodacidosis in low-flow ischemia induces capillary luminalnarrowing. Int J Microcirc Clin Exp 1994;14:144–50.
8. Gosain A, Rabkin J, Reymond JP, et al. Tissue oxygen tensionand other indicators of blood loss or organ perfusion duringgraded hemorrhage. Surgery 1991;109:523–32.
9. Jonsson K, Jensen JA, Goodson WHI, West JM, Hunt TK.Assessment of perfusion in postoperative patients usingtissue oxygen measurements. Br J Surg 1987;74:263–7.
0. Chang N, Goodson WH 3rd, Gottrup F, Hunt TK. Directmeasurement of wound and tissue oxygen tension in post-operative patients. Ann Surg 1983;197:470–8.
1. Caldwell MD, Shearer J, Morris A, et al. Evidence for aerobicglycolysis in lambda-carrageenan-wounded skeletal muscle.J Surg Res 1984;37:63–8.
2. Hussain MZ, Ghani QP, Hunt TK. Inhibition of prolylhydroxylase by poly(ADP-ribose) and phosphoribosyl-AMP.Possible role of ADP-ribosylation in intracellular prolylhydroxylase regulation. J Biol Chem 1989;264:7850–5.
3. Hunt TK. Basic principles of wound healing. J Trauma1990;30(12 Suppl):S122–8.
4. Constant JS, Feng JJ, Zabel DD, et al. Lactate elicits vascularendothelial growth factor from macrophages: a possiblealternative to hypoxia. Wound Repair Regen 2000;8:353–60.
5. Knighton DR, Hunt TK, Scheuenstuhl H, et al. Oxygentension regulates the expression of angiogenesis factor bymacrophages. Science 1983;221:1283–5.
6. Jensen JA, Hunt TK, Scheuenstuhl H, Banda MJ. Effect oflactate, pyruvate, and pH on secretion of angiogenesis andmitogenesis factors by macrophages. Lab Invest 1986;54:574–8.
7. Zacharias A, Habib RH. Factors predisposing to mediansternotomy complications: deep vs superficial infection.
Chest 1996;110:1173–8.NVITED COMMENTARY
acuum-assisted wound infection management repre-ents a relatively novel strategy [1] that is gaining world-ide acceptance and is yielding encouraging results forostoperative mediastinitis, as the authors of this articlereviously reported [2]. The mechanisms underlying theffectiveness of this method have been partially identi-ed (ie, the application of negative pressure to healingound tissue is expected to prevent local ischemia by
ncreasing microvascular blood flow to eventually accel-rate the process of wound closure [3]). Wackenfors andolleagues have tried to verify this hypothesis of patho-hysiologic mechanism in an animal model. The study
dentifies a correlation between microvascular flow andpplied pressure, distance from the wound edge andissue density. The finding that both O2 and lactatencrease in the wound during VAC therapy is also ofreat interest because it supports the hypothesis ofnhanced migration and proliferation in granulation tis-ue cells. Nevertheless, the present study does not pro-ide direct demonstration (ie, evidence of the biomolec-lar mechanisms involved in this theory).Animal models, although widely validated in previous
rom the human setting. In the clinical situation, postop-rative mediastinitis is a multifarious entity, representingmore or less challenging complication because of the
oexistence of several patient-related factors related tohe perioperative course [4]. Both systemic and localonditions may affect the mechanisms of wound healing.n this perspective, a major limitation of this study is these of noninfected animals that lack the systemic and
ocal conditions associated with active sternal woundnfection. How would changes in local oxygenation, mi-rocirculation, and metabolism occurring with bacterialnfection interact with the mechanism of vacuum? Howould these factors have influenced the results of such
xperiments? One wonders whether the pressure-ependence of the VAC effect would maintain the sameynamics in infected wounds as shown by the authors.ven tissue density itself, which influences the effect ofAC on the wound by modulating negative pressure
ransduction to the wound tissue is greatly altered in casef infection. Further studies are needed to generate datahat are more applicable to clinical practice; animals witheproduced clinical sternal wounds and greater negative
ressures, similar to those used in clinical wound treat-0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.12.006
by on June 2, 2013 als.org

2005;79:1724-1730 Ann Thorac SurgIngemansson and Malin Malmsjö
Angelica Wackenfors, Ronny Gustafsson, Johan Sjögren, Lars Algotsson, Richard Closure Therapy
Blood Flow Responses in the Peristernal Thoracic Wall During Vacuum-Assisted
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/79/5/1724including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/79/5/1724#BIBL
This article cites 26 articles, 7 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/79/5/1724#otherarticleThis article has been cited by 16 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/chest_wall Chest wall
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 2, 2013 ats.ctsnetjournals.orgDownloaded from
Related Documents






![Technical Note on Vacuum Assisted Closure-Basket …...sisted Closure (VAC)-Basket for Easy Fixation of Scrotal Skin Grafts” by Huettinger et al. [1]. The authors describe their](https://static.cupdf.com/doc/110x72/5e6e1f667785227fac2863d1/technical-note-on-vacuum-assisted-closure-basket-sisted-closure-vac-basket.jpg)




