NEW TECHNOLOGY Automatic Intraaortic Balloon Pump Timing Using an Intrabeat Dicrotic Notch Prediction Algorithm Jan J. Schreuder, MD, PhD, Alessandro Castiglioni, MD, Andrea Donelli, MS, Francesco Maisano, MD, Jos R. C. Jansen, PhD, Ramzi Hanania, MS, Pat Hanlon, RN, Jan Bovelander, CRNA, and Ottavio Alfieri, MD Department of Cardiac Surgery, San Raffaele University Hospital, Milan, Italy, Intensive Care, Leiden University Hospital, Leiden, the Netherlands, and Arrow International, Reading, Pennsylvania Purpose. The efficacy of intraaortic balloon counterpulsation (IABP) during arrhythmic episodes is questionable. A novel algorithm for intrabeat prediction of the dicrotic notch was used for real time IABP inflation timing control. Description. A windkessel model algorithm was used to calculate real-time aortic flow from aortic pressure. The dicrotic notch was predicted using a percentage of calculated peak flow. Automatic inflation timing was set at intrabeat predicted dicrotic notch and was combined with automatic IAB deflation. Evaluation. Prophylactic IABP was applied in 27 patients with low ejection fraction (< 35%) undergoing cardiac surgery. Analysis of IABP at a 1:4 ratio revealed that IAB inflation occurred at a mean of 0.6 5 ms from the dicrotic notch. In all patients accurate automatic timing at a 1:1 assist ratio was performed. Seventeen patients had episodes of severe arrhythmia, the novel IABP inflation algorithm accurately assisted 318 of 320 arrhythmic beats at a 1:1 ratio. Conclusions. The novel real-time intrabeat IABP inflation timing algorithm performed accurately in all patients during both regular rhythms and severe arrhythmia, allowing fully automatic intrabeat IABP timing. (Ann Thorac Surg 2005;79:1017–22) © 2005 by The Society of Thoracic Surgeons B eneficial effects of intraaortic balloon pump (IABP) counterpulsation have been well demonstrated in various pathologies resulting in improved left ventricular (LV) performance [1– 4]. However, the performance of current IABP devices during arrhythmia is suboptimal, resulting in inappropriate IABP timing with potentially negative hemodynamic effects [5, 6]. At the least, incor- rect timing reduces the efficacy of IABP [7]. In a previous study it was demonstrated that premature IAB inflation See page 872 markedly impaired LV ejection and relaxation by in- creasing LV afterload during the second part of the ejection phase, indicating that premature IAB inflation, which may occur during arrhythmia, can have detrimen- tal effects on cardiac performance in heart failure patients [8]. Late IAB deflation resulted in increased stroke vol- ume and increased stroke work due to afterload increase during early ejection followed by an afterload decrease in late ejection, demonstrating that incidental late IAB de- flation will not negatively affect cardiac performance [8]. Arrhythmia commonly occurs in heart failure patients and is even more pronounced during cardiac surgery and interventional cardiology procedures. Within the first 4 days after cardiac surgery 30% of patients may manifest episodes of atrial fibrillation [9]. Given the changing acuity of the cardiac population and the increasing severity of irregular arrhythmia, alternative timing methods must be developed to optimize IABP hemodynamic support. We developed an automatic IABP inflation timing using intrabeat dicrotic notch prediction (DNP) based on the windkessel model, where aortic flow is calculated from aortic pressure [10 –12]. This method accurately detected and predicted the dicrotic notch in animal aortic pressure signals and in man aortic pressure signals with marked arrhythmia [11, 12]. Automated DNP-IABP inflation com- bined with R-wave or predictive deflation should provide accurate automatic timing control during both regular and irregular cardiac rhythms. Patients and Methods Patients Twenty-seven consecutive patients, 49 to 74 years old, undergoing cardiac surgery and requiring prophylactic Accepted for publication July 29, 2004. Address reprint requests to Dr Schreuder, Department of Cardiac Sur- gery, San Raffaele University Hospital, Via Olgettina 60, 20132 Milan, Italy; e-mail: [email protected]. Dr Schreuder, Mr Hanania, Mr Bovelander, and Ms Hanlon disclose that they have a financial relationship with Arrow International; Dr Schreuder also has a financial relationship with CD Leycom. © 2005 by The Society of Thoracic Surgeons 0003-4975/05/$30.00 Published by Elsevier Inc doi:10.1016/j.athoracsur.2004.07.074 NEW TECHNOLOGY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AaJFJDt
Bv(crnrs
mcewt[udlflAa
A
AgI
©P
NEW TECHNOLOGY
utomatic Intraaortic Balloon Pump Timing Usingn Intrabeat Dicrotic Notch Prediction Algorithm
an J. Schreuder, MD, PhD, Alessandro Castiglioni, MD, Andrea Donelli, MS,rancesco Maisano, MD, Jos R. C. Jansen, PhD, Ramzi Hanania, MS, Pat Hanlon, RN,an Bovelander, CRNA, and Ottavio Alfieri, MDepartment of Cardiac Surgery, San Raffaele University Hospital, Milan, Italy, Intensive Care, Leiden University Hospital, Leiden,
he Netherlands, and Arrow International, Reading, Pennsylvania
ew
fpc
3otab
af
eneficial e
ery, San Raffaeletaly; e-mail: schre
2005 by The Sublished by El
NEW
TEC
HN
OLO
GY
Purpose. The efficacy of intraaortic balloon counterpulsation (IABP) during arrhythmicpisodes is questionable. A novel algorithm for intrabeat prediction of the dicrotic notchas used for real time IABP inflation timing control.
Description. A windkessel model algorithm was used to calculate real-time aortic flowrom aortic pressure. The dicrotic notch was predicted using a percentage of calculatedeak flow. Automatic inflation timing was set at intrabeat predicted dicrotic notch and wasombined with automatic IAB deflation.
Evaluation. Prophylactic IABP was applied in 27 patients with low ejection fraction (<5%) undergoing cardiac surgery. Analysis of IABP at a 1:4 ratio revealed that IAB inflationccurred at a mean of 0.6 � 5 ms from the dicrotic notch. In all patients accurate automaticiming at a 1:1 assist ratio was performed. Seventeen patients had episodes of severerrhythmia, the novel IABP inflation algorithm accurately assisted 318 of 320 arrhythmiceats at a 1:1 ratio.
Conclusions. The novel real-time intrabeat IABP inflation timing algorithm performedccurately in all patients during both regular rhythms and severe arrhythmia, allowingully automatic intrabeat IABP timing.
(Ann Thorac Surg 2005;79:1017–22)
© 2005 by The Society of Thoracic Surgeonsffects of intraaortic balloon pump (IABP) interventional cardiology procedures. Within the first 4
deoidiwaasabai
P
PTu
counterpulsation have been well demonstrated inarious pathologies resulting in improved left ventricularLV) performance [1–4]. However, the performance ofurrent IABP devices during arrhythmia is suboptimal,esulting in inappropriate IABP timing with potentiallyegative hemodynamic effects [5, 6]. At the least, incor-ect timing reduces the efficacy of IABP [7]. In a previoustudy it was demonstrated that premature IAB inflation
See page 872
arkedly impaired LV ejection and relaxation by in-reasing LV afterload during the second part of thejection phase, indicating that premature IAB inflation,hich may occur during arrhythmia, can have detrimen-
al effects on cardiac performance in heart failure patients8]. Late IAB deflation resulted in increased stroke vol-me and increased stroke work due to afterload increaseuring early ejection followed by an afterload decrease in
ate ejection, demonstrating that incidental late IAB de-ation will not negatively affect cardiac performance [8].rrhythmia commonly occurs in heart failure patientsnd is even more pronounced during cardiac surgery and
ccepted for publication July 29, 2004.
ddress reprint requests to Dr Schreuder, Department of Cardiac Sur-
University Hospital, Via Olgettina 60, 20132 Milan,ociety of Thoracic Surgeonssevier Inc
ays after cardiac surgery 30% of patients may manifestpisodes of atrial fibrillation [9]. Given the changing acuityf the cardiac population and the increasing severity of
rregular arrhythmia, alternative timing methods must beeveloped to optimize IABP hemodynamic support.We developed an automatic IABP inflation timing using
ntrabeat dicrotic notch prediction (DNP) based on theindkessel model, where aortic flow is calculated from
ortic pressure [10–12]. This method accurately detectednd predicted the dicrotic notch in animal aortic pressureignals and in man aortic pressure signals with markedrrhythmia [11, 12]. Automated DNP-IABP inflation com-ined with R-wave or predictive deflation should provideccurate automatic timing control during both regular andrregular cardiac rhythms.
atients and Methods
atientswenty-seven consecutive patients, 49 to 74 years old,ndergoing cardiac surgery and requiring prophylactic
Dr Schreuder, Mr Hanania, Mr Bovelander, and MsHanlon disclose that they have a financial relationshipwith Arrow International; Dr Schreuder also has a
financial relationship with CD Leycom.0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.07.074
Iva(cfci
DTbmnfirtpatprw
IAItaotat
d
stoamasict
sIs7mC
DTddaswbtaa
R
O
Ftbt1
1018 NEW TECHNOLOGY SCHREUDER ET AL Ann Thorac SurgAUTOMATIC IABP TIMING DURING ARRHYTHMIA 2005;79:1017–22
NEW
TEC
HN
OLO
GY
ABP were studied. Surgical procedures included leftentricular aneurysmectomy (n � 11, 9 with coronaryrtery bypass grafting), coronary artery bypass graftingn � 10, 5 off-pump), and mitral valve repair (n � 6, 1 withoronary artery bypass grafting). Ejection fraction rangedrom 13% to 35%, mean of 26% � 6%. The hospital ethicsommittee approved the study and patients gave writtennformed consent.
icrotic Notch Predictionhe dicrotic notch detection algorithm has previouslyeen described [10–12]. Briefly, a simplified windkesselodel of the arterial tree was used to calculate real-time
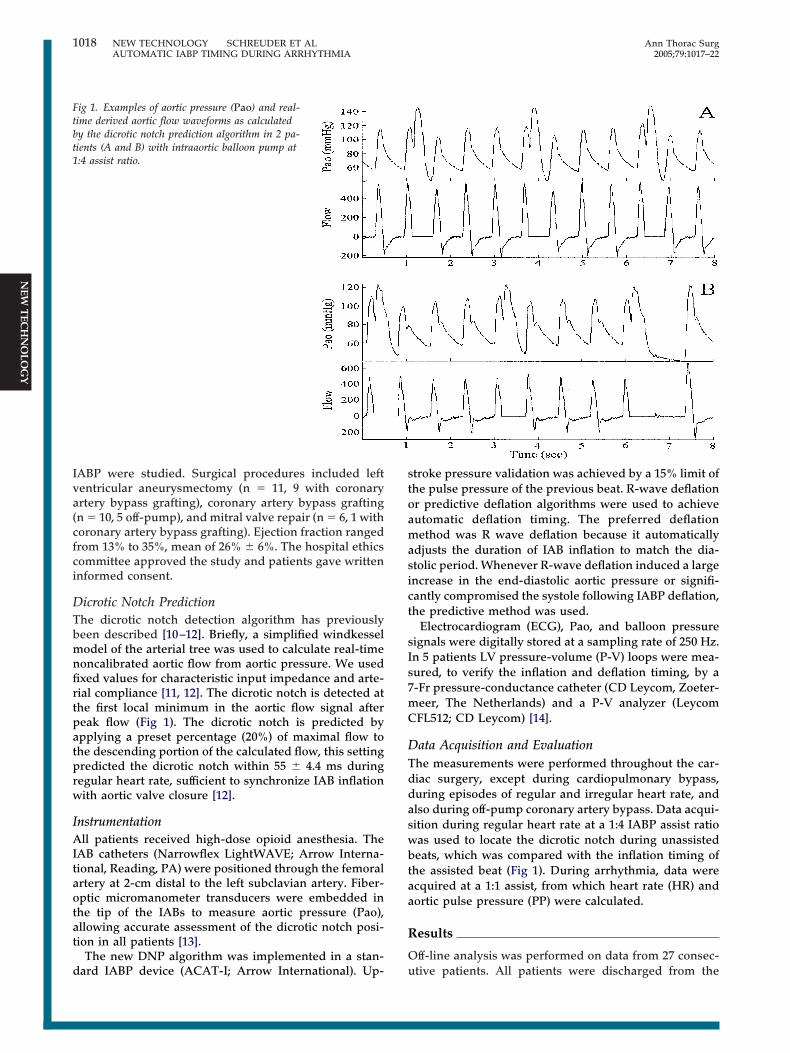
oncalibrated aortic flow from aortic pressure. We usedxed values for characteristic input impedance and arte-ial compliance [11, 12]. The dicrotic notch is detected athe first local minimum in the aortic flow signal aftereak flow (Fig 1). The dicrotic notch is predicted bypplying a preset percentage (20%) of maximal flow tohe descending portion of the calculated flow, this settingredicted the dicrotic notch within 55 � 4.4 ms duringegular heart rate, sufficient to synchronize IAB inflationith aortic valve closure [12].
nstrumentationll patients received high-dose opioid anesthesia. The
AB catheters (Narrowflex LightWAVE; Arrow Interna-ional, Reading, PA) were positioned through the femoralrtery at 2-cm distal to the left subclavian artery. Fiber-ptic micromanometer transducers were embedded inhe tip of the IABs to measure aortic pressure (Pao),llowing accurate assessment of the dicrotic notch posi-ion in all patients [13].
The new DNP algorithm was implemented in a stan-
ig 1. Examples of aortic pressure (Pao) and real-ime derived aortic flow waveforms as calculatedy the dicrotic notch prediction algorithm in 2 pa-ients (A and B) with intraaortic balloon pump at:4 assist ratio.
ard IABP device (ACAT-I; Arrow International). Up- u
troke pressure validation was achieved by a 15% limit ofhe pulse pressure of the previous beat. R-wave deflationr predictive deflation algorithms were used to achieveutomatic deflation timing. The preferred deflationethod was R wave deflation because it automatically
djusts the duration of IAB inflation to match the dia-tolic period. Whenever R-wave deflation induced a largencrease in the end-diastolic aortic pressure or signifi-antly compromised the systole following IABP deflation,he predictive method was used.
Electrocardiogram (ECG), Pao, and balloon pressureignals were digitally stored at a sampling rate of 250 Hz.n 5 patients LV pressure-volume (P-V) loops were mea-ured, to verify the inflation and deflation timing, by a-Fr pressure-conductance catheter (CD Leycom, Zoeter-eer, The Netherlands) and a P-V analyzer (LeycomFL512; CD Leycom) [14].
ata Acquisition and Evaluationhe measurements were performed throughout the car-iac surgery, except during cardiopulmonary bypass,uring episodes of regular and irregular heart rate, andlso during off-pump coronary artery bypass. Data acqui-ition during regular heart rate at a 1:4 IABP assist ratioas used to locate the dicrotic notch during unassistedeats, which was compared with the inflation timing of
he assisted beat (Fig 1). During arrhythmia, data werecquired at a 1:1 assist, from which heart rate (HR) andortic pulse pressure (PP) were calculated.
esults
ff-line analysis was performed on data from 27 consec-
tive patients. All patients were discharged from the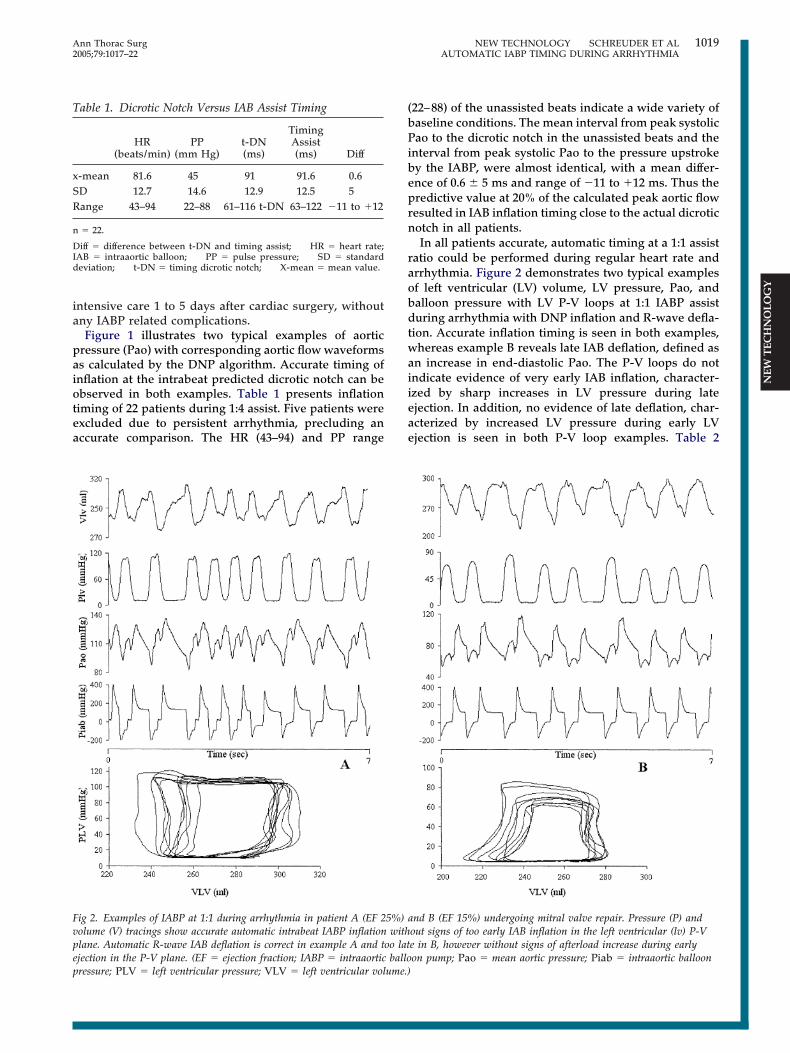
ia
paiotea
(bPibeprn
raobdtwaiieae
Fvpep
T
xSR
n
DId
1019Ann Thorac Surg NEW TECHNOLOGY SCHREUDER ET AL2005;79:1017–22 AUTOMATIC IABP TIMING DURING ARRHYTHMIA
NEW
TEC
HN
OLO
GY
ntensive care 1 to 5 days after cardiac surgery, withoutny IABP related complications.Figure 1 illustrates two typical examples of aortic
ressure (Pao) with corresponding aortic flow waveformss calculated by the DNP algorithm. Accurate timing ofnflation at the intrabeat predicted dicrotic notch can bebserved in both examples. Table 1 presents inflationiming of 22 patients during 1:4 assist. Five patients werexcluded due to persistent arrhythmia, precluding anccurate comparison. The HR (43–94) and PP range
ig 2. Examples of IABP at 1:1 during arrhythmia in patient A (EF 2olume (V) tracings show accurate automatic intrabeat IABP inflationlane. Automatic R-wave IAB deflation is correct in example A and tjection in the P-V plane. (EF � ejection fraction; IABP � intraaortic
able 1. Dicrotic Notch Versus IAB Assist Timing
HR(beats/min)
PP(mm Hg)
t-DN(ms)
TimingAssist(ms) Diff
-mean 81.6 45 91 91.6 0.6D 12.7 14.6 12.9 12.5 5ange 43–94 22–88 61–116 t-DN 63–122 �11 to �12
� 22.
iff � difference between t-DN and timing assist; HR � heart rate;AB � intraaortic balloon; PP � pulse pressure; SD � standardeviation; t-DN � timing dicrotic notch; X-mean � mean value.
ressure; PLV � left ventricular pressure; VLV � left ventricular volume.)
22–88) of the unassisted beats indicate a wide variety ofaseline conditions. The mean interval from peak systolicao to the dicrotic notch in the unassisted beats and the
nterval from peak systolic Pao to the pressure upstrokey the IABP, were almost identical, with a mean differ-nce of 0.6 � 5 ms and range of �11 to �12 ms. Thus theredictive value at 20% of the calculated peak aortic flowesulted in IAB inflation timing close to the actual dicroticotch in all patients.In all patients accurate, automatic timing at a 1:1 assist
atio could be performed during regular heart rate andrrhythmia. Figure 2 demonstrates two typical examplesf left ventricular (LV) volume, LV pressure, Pao, andalloon pressure with LV P-V loops at 1:1 IABP assisturing arrhythmia with DNP inflation and R-wave defla-
ion. Accurate inflation timing is seen in both examples,hereas example B reveals late IAB deflation, defined as
n increase in end-diastolic Pao. The P-V loops do notndicate evidence of very early IAB inflation, character-zed by sharp increases in LV pressure during latejection. In addition, no evidence of late deflation, char-cterized by increased LV pressure during early LVjection is seen in both P-V loop examples. Table 2
nd B (EF 15%) undergoing mitral valve repair. Pressure (P) andout signs of too early IAB inflation in the left ventricular (lv) P-Ve in B, however without signs of afterload increase during earlyon pump; Pao � mean aortic pressure; Piab � intraaortic balloon
5%) awith
oo latballo
prticpd2abelsbpati
oebfinOaccaw
C
Ti
Iadattwppt
ipKtwfieeidcdtn
rmadKsdo
T
1111112222
n
A surec
1020 NEW TECHNOLOGY SCHREUDER ET AL Ann Thorac SurgAUTOMATIC IABP TIMING DURING ARRHYTHMIA 2005;79:1017–22
NEW
TEC
HN
OLO
GY
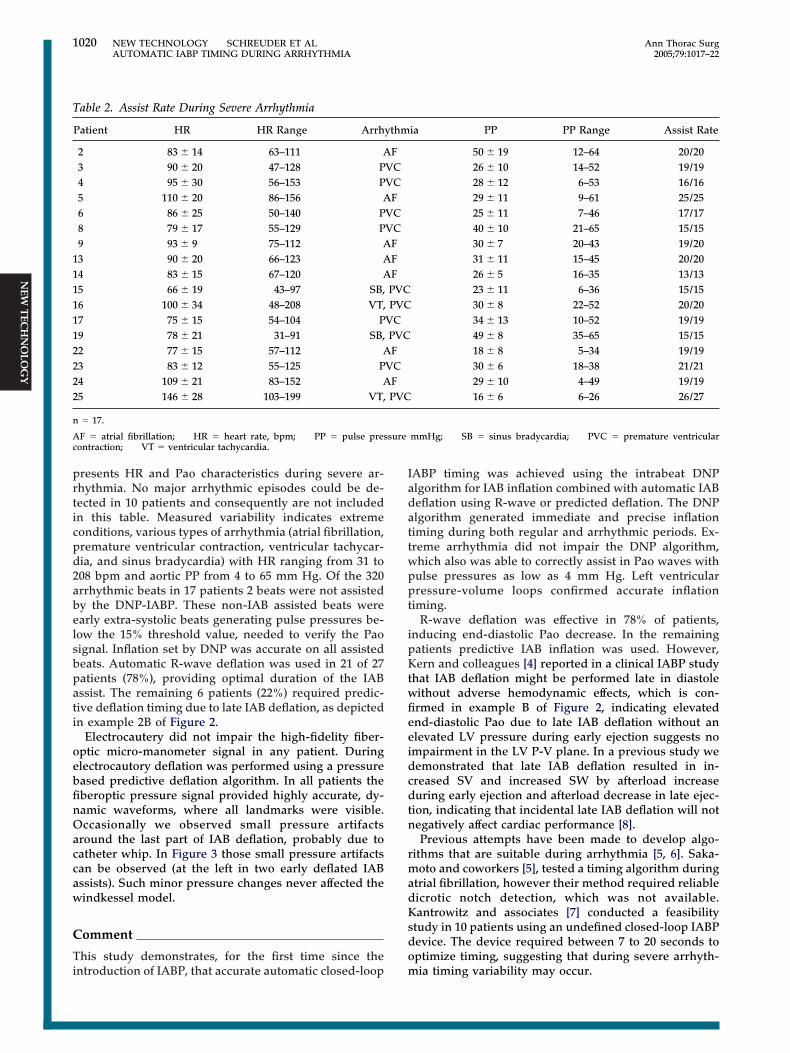
resents HR and Pao characteristics during severe ar-hythmia. No major arrhythmic episodes could be de-ected in 10 patients and consequently are not includedn this table. Measured variability indicates extremeonditions, various types of arrhythmia (atrial fibrillation,remature ventricular contraction, ventricular tachycar-ia, and sinus bradycardia) with HR ranging from 31 to08 bpm and aortic PP from 4 to 65 mm Hg. Of the 320rrhythmic beats in 17 patients 2 beats were not assistedy the DNP-IABP. These non-IAB assisted beats werearly extra-systolic beats generating pulse pressures be-ow the 15% threshold value, needed to verify the Paoignal. Inflation set by DNP was accurate on all assistedeats. Automatic R-wave deflation was used in 21 of 27atients (78%), providing optimal duration of the IABssist. The remaining 6 patients (22%) required predic-ive deflation timing due to late IAB deflation, as depictedn example 2B of Figure 2.
Electrocautery did not impair the high-fidelity fiber-ptic micro-manometer signal in any patient. Duringlectrocautory deflation was performed using a pressureased predictive deflation algorithm. In all patients theberoptic pressure signal provided highly accurate, dy-amic waveforms, where all landmarks were visible.ccasionally we observed small pressure artifacts
round the last part of IAB deflation, probably due toatheter whip. In Figure 3 those small pressure artifactsan be observed (at the left in two early deflated IABssists). Such minor pressure changes never affected theindkessel model.
omment
his study demonstrates, for the first time since the
able 2. Assist Rate During Severe Arrhythmia
Patient HR HR Range Arrh
2 83 � 14 63–111 A3 90 � 20 47–128 P4 95 � 30 56–153 P5 110 � 20 86–156 A6 86 � 25 50–140 P8 79 � 17 55–129 P9 93 � 9 75–112 A3 90 � 20 66–123 A4 83 � 15 67–120 A5 66 � 19 43–97 SB,6 100 � 34 48–208 VT,7 75 � 15 54–104 P9 78 � 21 31–91 SB,2 77 � 15 57–112 A3 83 � 12 55–125 P4 109 � 21 83–152 A5 146 � 28 103–199 VT,
� 17.
F � atrial fibrillation; HR � heart rate, bpm; PP � pulse presontraction; VT � ventricular tachycardia.
ntroduction of IABP, that accurate automatic closed-loop m
ABP timing was achieved using the intrabeat DNPlgorithm for IAB inflation combined with automatic IABeflation using R-wave or predicted deflation. The DNPlgorithm generated immediate and precise inflationiming during both regular and arrhythmic periods. Ex-reme arrhythmia did not impair the DNP algorithm,hich also was able to correctly assist in Pao waves withulse pressures as low as 4 mm Hg. Left ventricularressure-volume loops confirmed accurate inflation
iming.R-wave deflation was effective in 78% of patients,
nducing end-diastolic Pao decrease. In the remainingatients predictive IAB inflation was used. However,ern and colleagues [4] reported in a clinical IABP study
hat IAB deflation might be performed late in diastoleithout adverse hemodynamic effects, which is con-rmed in example B of Figure 2, indicating elevatednd-diastolic Pao due to late IAB deflation without anlevated LV pressure during early ejection suggests nompairment in the LV P-V plane. In a previous study weemonstrated that late IAB deflation resulted in in-reased SV and increased SW by afterload increaseuring early ejection and afterload decrease in late ejec-
ion, indicating that incidental late IAB deflation will notegatively affect cardiac performance [8].Previous attempts have been made to develop algo-
ithms that are suitable during arrhythmia [5, 6]. Saka-oto and coworkers [5], tested a timing algorithm during
trial fibrillation, however their method required reliableicrotic notch detection, which was not available.antrowitz and associates [7] conducted a feasibility
tudy in 10 patients using an undefined closed-loop IABPevice. The device required between 7 to 20 seconds toptimize timing, suggesting that during severe arrhyth-
ia PP PP Range Assist Rate
50 � 19 12–64 20/2026 � 10 14–52 19/1928 � 12 6–53 16/1629 � 11 9–61 25/2525 � 11 7–46 17/1740 � 10 21–65 15/1530 � 7 20–43 19/2031 � 11 15–45 20/2026 � 5 16–35 13/1323 � 11 6–36 15/1530 � 8 22–52 20/2034 � 13 10–52 19/1949 � 8 35–65 15/1518 � 8 5–34 19/1930 � 6 18–38 21/2129 � 10 4–49 19/1916 � 6 6–26 26/27
mmHg; SB � sinus bradycardia; PVC � premature ventricular
ythm
FVCVC
FVCVC
FFFPVCPVC
VCPVCF
VCFPVC
ia timing variability may occur.
p4t
caiamceaetitbcawdct
rcflsDance
C
Ttfrm
D
T
1021Ann Thorac Surg NEW TECHNOLOGY SCHREUDER ET AL2005;79:1017–22 AUTOMATIC IABP TIMING DURING ARRHYTHMIA
NEW
TEC
HN
OLO
GY
The applied fiberoptic pressure signal provided aorticressure waveforms at high-time resolution during 20 to8 hours of IABP, necessary for accurate flow calcula-ions, and was not influenced by electrocautory [13].
Intraaortic balloon pump has shown to stabilize medi-ally refractory ventricular arrhythmia [15]. Methods, suchs the DNP algorithm, which are capable of providingntrabeat beat adjustment in timing, may provide optimalssist under a wide range of patient conditions and mayarkedly increase the therapeutic effectiveness of IABP in
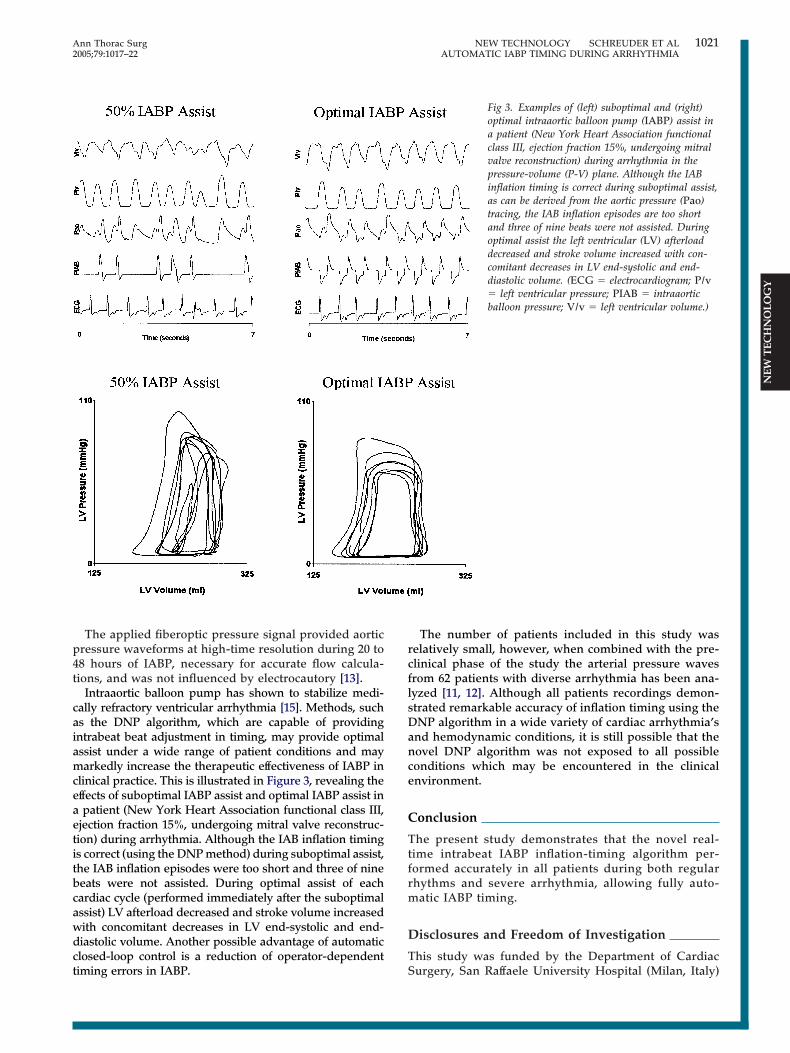
linical practice. This is illustrated in Figure 3, revealing theffects of suboptimal IABP assist and optimal IABP assist inpatient (New York Heart Association functional class III,
jection fraction 15%, undergoing mitral valve reconstruc-ion) during arrhythmia. Although the IAB inflation timings correct (using the DNP method) during suboptimal assist,he IAB inflation episodes were too short and three of nineeats were not assisted. During optimal assist of eachardiac cycle (performed immediately after the suboptimalssist) LV afterload decreased and stroke volume increasedith concomitant decreases in LV end-systolic and end-iastolic volume. Another possible advantage of automaticlosed-loop control is a reduction of operator-dependent
iming errors in IABP. SThe number of patients included in this study waselatively small, however, when combined with the pre-linical phase of the study the arterial pressure wavesrom 62 patients with diverse arrhythmia has been ana-yzed [11, 12]. Although all patients recordings demon-trated remarkable accuracy of inflation timing using theNP algorithm in a wide variety of cardiac arrhythmia’s
nd hemodynamic conditions, it is still possible that theovel DNP algorithm was not exposed to all possibleonditions which may be encountered in the clinicalnvironment.
onclusion
he present study demonstrates that the novel real-ime intrabeat IABP inflation-timing algorithm per-ormed accurately in all patients during both regularhythms and severe arrhythmia, allowing fully auto-atic IABP timing.
isclosures and Freedom of Investigation
his study was funded by the Department of Cardiac
Fig 3. Examples of (left) suboptimal and (right)optimal intraaortic balloon pump (IABP) assist ina patient (New York Heart Association functionalclass III, ejection fraction 15%, undergoing mitralvalve reconstruction) during arrhythmia in thepressure-volume (P-V) plane. Although the IABinflation timing is correct during suboptimal assist,as can be derived from the aortic pressure (Pao)tracing, the IAB inflation episodes are too shortand three of nine beats were not assisted. Duringoptimal assist the left ventricular (LV) afterloaddecreased and stroke volume increased with con-comitant decreases in LV end-systolic and end-diastolic volume. (ECG � electrocardiogram; P/v� left ventricular pressure; PIAB � intraaorticballoon pressure; V/v � left ventricular volume.)
urgery, San Raffaele University Hospital (Milan, Italy)

auCcccw
R
1
1
1
1
1
1
D
TSn
I
Tdcfd2gwPta
htmppwtrrTaifii
1022 NEW TECHNOLOGY SCHREUDER ET AL Ann Thorac SurgAUTOMATIC IABP TIMING DURING ARRHYTHMIA 2005;79:1017–22
©P
NEW
TEC
HN
OLO
GY
nd Arrow International (Reading, PA). Doctor Schre-der serves as a consultant for Arrow International andD Leycom. The tested technology was borrowed to
onduct the study. The authors state that they had fullontrol of the design of the study, methods used, out-ome parameters, analysis of data, and production of theritten report.
eferences
1. Kantrowitz A, Kantrowitz A. Experimental augmentation ofcoronary flow by retardation of arterial pressure pulse.Surgery 1953;34:678.
2. Willerson J, Curry G, Watson J, et al. Intraaortic ballooncounterpulsation in patients in cardiogenic shock, medicallyrefractory left ventricular failure and/or recurrent ventricu-lar tachycardia. Am J Med 1975;58:183–91.
3. Nichols AB, Pohost GM, Gold HK, et al. Left ventricularfunction during intra-aortic balloon pumping assessed bymultigated cardiac blood pool imaging. Circulation 1978;58(Suppl 1):176–83.
4. Kern MJ, Aguirre FV, Caracciolo EA, et al. Hemodynamiceffects of new intra-aortic balloon counterpulsation timingmethods in patients: a multicenter evaluation. Am Heart J1999;137:1129–36.
5. Sakamoto T, Arai H, Maruyama T, Suzuki A. New algorithmof intra-aortic balloon pumping in patients with atrial fibril-lation. ASAIO J 1995;41:79–83.
6. Kantrowitz A, Freed PS, Cardona RR, et al. Initial clinicaltrial of a closed loop, fully automatic intra-aortic balloonpump. ASAIO J 1992;38:M617–21.
7. Kantrowitz A, Cardona RR, Freed PS. Percutaneous intra-
aortic balloon counterpulsation. Crit Care Clin 1992;8:819–37. os a malignant arrhythmia that generates pulse pressures
bmlripcmda
umbbsbc
W
DU1RBe
2005 by The Society of Thoracic Surgeonsublished by Elsevier Inc
8. Schreuder JJ, Maisano F, Donelli A, et al. Beat-to-beat effectsof intraaortic balloon pump timing on left ventricular per-formance in patients with low ejection fraction. Ann ThoracSurg 2005;79:872–80.
9. Greengurg M, Katz N, Juliano S, et al. Atrial pacing for theprevention of atrial fibrillation after cardiovascular surgery.J Am Coll Cardiol 2000;35:1416–22.
0. Wesseling KH, Jansen JRC, Settels JJ, Schreuder JJ. Compu-tation of aortic flow from pressure in humans using anonlinear, three-element model. J Applied Physiol 1993;74:2566–73.
1. Hoeksel SAAP, Jansen JRC, Blom JA, Schreuder JJ. Detectionof dicrotic notch in arterial pressure signals. J Clin Monit1997;13:309–16.
2. Donelli A, Jansen JRC, Hoeksel B, et al. Performance of areal-time dicrotic notch prediction algorithm in arrhythmichuman aortic pressure signals. J Clin Monit 2002;17:181–5.
3. Reesink KD, Van der Nagel T, Bovelander J, Jansen JRC, vander Veen FH, Schreuder JJ. Feasibility of a fiber-optic systemfor invasive blood pressure measurements. Cathet Cardio-vasc Intervent 2002;57:272–6.
4. Schreuder JJ, Steendijk P, van der Veen FH, et al. Acute andshort-term effects of partial left ventriculectomy in dilatedcardiomyopathy: Assessment by pressure-volume loops.J Am Coll Cardiol 2000;36:2104–14.
5. Fotopoulos GD, Mason MJ, Walker S, et al. Stabilization ofmedically refractory ventricular arrhythmia by intra-aorticballoon counter pulsation. Heart 1999;82:96–100.
isclaimer
he Society of Thoracic Surgeons, the Southern Thoracicurgical Association, and The Annals of Thoracic Surgeryeither endorse nor discourage use of the new technol-
gy described in this article.NVITED COMMENTARY
his article describes a novel algorithm to predict theicrotic notch for timing intraaortic balloon pump (IABP)ounterpulsation. The algorithm uses pressure readingsrom a high fidelity fiberoptic micromanometer embed-ed in the tip of the IABP. This system was evaluated in7 patients with low ejection fractions who were under-oing cardiac operations. Balloon inflation and deflationere accurate in the vast majority of arrhythmic beats.ressure-volume data were shown that suggests this
echnology will provide better support than convention-lly timed IABP counterpulsation.Since the initial use of IABP counterpulsation, attempts
ave been made to improve the timing of balloon infla-ion and deflation, particularly in patients with arrhyth-
ias. The present attempt at such a system appears torovide good results, at least in a limited number ofatients, but obstacles remain. One potential problemith using pressure data from transducers embedded in
he tip of the IABP is artifact. The system is essentially aefined pulse pressure-based sensing algorithm that de-ives flow from high fidelity pressure measurements.hus the system is vulnerable to timing errors due tortifacts in the pressure data. This was not encounteredn the study, but it can occur even with readings from aberoptic micromanometer. Another potential problem
elow the threshold for detection. These are arguably theost dangerous arrhythmias to a patient. What are the
imits for pulse pressure and first derivative of pressureelative to time (dP/dt) below which the system becomesnaccurate? A third issue is the rate limit of the system. It isresumably the same as the limit for IABPs that useonventional electrocardiogram or pressure triggers. Ulti-ately, the problem with effective IABP counterpulsation
uring a tachyarrhythmia becomes shuttling helium backnd forth in the IABP and not tracking the dicrotic notch.
The final question relates to cost and indications forse. Catheters with embedded micromanometers costore than conventional IABP catheters, but an outcome
enefit for this novel IABP timing system has not yeteen demonstrated. Determining the benefit in terms ofurvival, morbidity, and duration of hospitalization wille crucial for defining the role of this technology inlinical practice.
illiam L. Holman, MD
epartment of Surgeryniversity of Alabama at Birmingham
530 3rd Ave Soom 719irmingham, AL 35294-0007
-mail: [email protected]0003-4975/05/$30.00doi:10.1016/j.athoracsur.2004.08.072
Related Documents











