Vol. 1, 607-614, June 1995 Clinical Cancer Research 607 Autologous Peripheral Blood Stem Cell Transplantation and Adoptive Immunotherapy with Activated Natural Killer Cells in the Immediate Posttransplant Period’ John Lister,2 Witold B. Rybka, Albert D. Donnenberg, Margarida deMagalhaes-Silverman, Steven M. Pincus, Elana J. Bloom, Elaine M. Elder, Edward D. Ball, and Theresa L. Whiteside Division of Hematology/Bone Marrow Transplantation, Department of Medicine [J. L., W. B. R., A. D. D., M. d-S., S. M. P., E. J. B., E. D. B.], and Departments of Pathology and Otolaryngology [E. M. E., T. L. W.], Pittsburgh Cancer Institute, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania 15213-2582 ABSTRACT Relapse after high-dose chemotherapy supported by pe- ripheral blood stem cell transplantation (HDC-PBSCT) is the main cause of therapeutic failure in patients with lymphoma and breast cancer. Adoptive immunotherapy with activated natural killer (A-NK) cells and interleukin 2 might eliminate surviving residual tumor without adding to toxicity. Eleven patients with relapsed lymphoma and one with metastatic breast cancer were entered on a pilot clinical trial of HDC-PBSCT followed on day 2 after transplant by infu- sion of cultured autologous A-NK cells. Simultaneously, re- combinant human interleukin 2 (rhIL-2) was initiated as a 4-day continuous i.v. infusion at 2 x 106 IU/m2/day, referred to as high-dose rhIL-2. Therapy with high-dose rhIL-2 was followed by a 90-day continuous i.v. infusion at 3 x i05 IU/m2/day, referred to as low-dose rhIL-2. All patients en- grafted and nine completed treatment. Posttransplant days to a neutrophil count of 500/pJ and to a platelet count of 50,000/p.l were similar to comparable patients treated with HDC-PBSCT alone. Generation of A-NK cells for therapy was feasible in all patients except the three patients with Hodgkin’s disease, whose cells did not proliferate in culture. Overall toxicity associated with early posttransplant trans- fer of A-NK cells and interleukin 2 did not differ from that observed with peripheral blood stem cell transplantation alone in comparable patients. There was early amplification of natural killer cell activity in the peripheral blood of four patients that appeared to result from the transfused A-NK cells. Adoptive transfer of A-NK cells and rhIL-2 during the pancytopenic phase after HDC-PBSCT was feasible and well tolerated, did not adversely affect engraftment, and resulted in amplified natural killer activity in the peripheral blood during the immediate posttransplantation period. INTRODUCTION The use of HDC3 and hemopoietic stem cell support has become widely employed in the treatment of relapsed lym- phoma and metastatic breast cancer (1-7). In chemotherapy- sensitive lymphoma and metastatic breast cancer, HDC can provide disease-free survival at S years in 40% and 15% of remitting patients, respectively. Nevertheless, the majority of completely remitting patients will relapse and die of their dis- ease. Dose escalation of chemotherapy and radiation therapy above conventional transplant doses has not improved disease- free survival. AlT with in vitro-activated autologous effector cells, either LAK cells or tumor-infiltrating lymphocytes, in combination with IL-2 has been shown to induce long-term responses in a small proportion of patients with metastatic melanoma or renal cell carcinoma (8, 9). These two types of cancer are generally chemoresistant but seem to be among the most responsive to biological therapy. Experience with the therapeutic use of cel- lular effectors and IL-2 in lymphoma or breast cancer has been limited, and only patients with advanced disease have been treated (10). Nevertheless, a few responses have been seen (1 1), indicating that AlT might be effective in these diseases. The treatment protocol described here is an attempt to evaluate the feasibility of AlT with A-NK cells and IL-2 in the setting of HDC-PBSCT in patients with lymphoma or breast cancer at the time of maximum chemotherapy effect. A-NK cells are a subset of CD3CD56m peripheral blood NK cells selected by adherence to plastic in the presence of 22 nM of IL-2 (12). A-NK cells can be expanded in culture with IL-2 for 2 to 3 weeks (12). This subset of NK cells has been shown recently to preferentially enter human tumor spheroids or established human tumor xenografts in nude mice and to kill NK-resistant tumor cells (13). In murine models of tumor me- tastasis, systemically delivered A-NK cells have been shown to preferentially localize to metastases (14). Our hypothesis has Received 11/i 1/94; accepted 3/9/95. 1 This study was supported in part by the Alcoa Foundation (Pittsburgh, PA), NIH/National Cancer Institute Grant 5U01-CA58271-02, and Pathology Education and Research Foundation. 2 To whom requests for reprints should be addressed, at Division of Hematology/Bone Marrow Transplantation, University of Pittsburgh Medical Center, 200 Lothrop Street, Pittsburgh, PA 15213-2582. 3 The abbreviations used are: HDC, high-dose chemotherapy; AlT, adoptive immunotherapy; LAK. lymphokine-activated killer cells; IL-2, interleukin 2; A-NK, activated natural killer; PBSCT, peripheral blood stem cell transplantation; NK, natural killer; G-CSF, granulocyte- colony-stimulating factor; PBSC, peripheral blood stem cell; rhIL-2, recombinant human IL-2; HD, high dose; LD, low dose; MNC, mono- nuclear cells; PE, phycoerythrin; ANC, absolute neutrophil count; CNS, central nervous system; UPN, unique patient number; PR, partial re- sponse(s); LU, lytic unit(s). Research. on August 1, 2020. © 1995 American Association for Cancer clincancerres.aacrjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vol. 1, 607-614, June 1995 Clinical Cancer Research 607
Autologous Peripheral Blood Stem Cell Transplantation and
Adoptive Immunotherapy with Activated Natural Killer
Cells in the Immediate Posttransplant Period’
John Lister,2 Witold B. Rybka,
Albert D. Donnenberg,
Margarida deMagalhaes-Silverman,
Steven M. Pincus, Elana J. Bloom,
Elaine M. Elder, Edward D. Ball, and
Theresa L. Whiteside
Division of Hematology/Bone Marrow Transplantation, Department
of Medicine [J. L., W. B. R., A. D. D., M. d-S., S. M. P., E. J. B.,
E. D. B.], and Departments of Pathology and Otolaryngology
[E. M. E., T. L. W.], Pittsburgh Cancer Institute, University of
Pittsburgh School of Medicine, Pittsburgh, Pennsylvania 15213-2582
ABSTRACT
Relapse after high-dose chemotherapy supported by pe-ripheral blood stem cell transplantation (HDC-PBSCT) is the
main cause of therapeutic failure in patients with lymphomaand breast cancer. Adoptive immunotherapy with activatednatural killer (A-NK) cells and interleukin 2 might eliminate
surviving residual tumor without adding to toxicity.Eleven patients with relapsed lymphoma and one with
metastatic breast cancer were entered on a pilot clinical trial
of HDC-PBSCT followed on day 2 after transplant by infu-sion of cultured autologous A-NK cells. Simultaneously, re-
combinant human interleukin 2 (rhIL-2) was initiated as a
4-day continuous i.v. infusion at 2 x 106 IU/m2/day, referredto as high-dose rhIL-2. Therapy with high-dose rhIL-2 wasfollowed by a 90-day continuous i.v. infusion at 3 x i05IU/m2/day, referred to as low-dose rhIL-2. All patients en-grafted and nine completed treatment. Posttransplant daysto a neutrophil count of 500/pJ and to a platelet count of50,000/p.l were similar to comparable patients treated withHDC-PBSCT alone. Generation of A-NK cells for therapywas feasible in all patients except the three patients with
Hodgkin’s disease, whose cells did not proliferate in culture.Overall toxicity associated with early posttransplant trans-fer of A-NK cells and interleukin 2 did not differ from thatobserved with peripheral blood stem cell transplantationalone in comparable patients. There was early amplificationof natural killer cell activity in the peripheral blood of fourpatients that appeared to result from the transfused A-NKcells. Adoptive transfer of A-NK cells and rhIL-2 during the
pancytopenic phase after HDC-PBSCT was feasible and well
tolerated, did not adversely affect engraftment, and resultedin amplified natural killer activity in the peripheral bloodduring the immediate posttransplantation period.
INTRODUCTION
The use of HDC3 and hemopoietic stem cell support has
become widely employed in the treatment of relapsed lym-
phoma and metastatic breast cancer (1-7). In chemotherapy-
sensitive lymphoma and metastatic breast cancer, HDC can
provide disease-free survival at S years in 40% and 15% of
remitting patients, respectively. Nevertheless, the majority of
completely remitting patients will relapse and die of their dis-
ease. Dose escalation of chemotherapy and radiation therapy
above conventional transplant doses has not improved disease-
free survival.
AlT with in vitro-activated autologous effector cells, either
LAK cells or tumor-infiltrating lymphocytes, in combination
with IL-2 has been shown to induce long-term responses in a
small proportion of patients with metastatic melanoma or renal
cell carcinoma (8, 9). These two types of cancer are generally
chemoresistant but seem to be among the most responsive to
biological therapy. Experience with the therapeutic use of cel-
lular effectors and IL-2 in lymphoma or breast cancer has been
limited, and only patients with advanced disease have been
treated (10). Nevertheless, a few responses have been seen (1 1),
indicating that AlT might be effective in these diseases. The
treatment protocol described here is an attempt to evaluate the
feasibility of AlT with A-NK cells and IL-2 in the setting of
HDC-PBSCT in patients with lymphoma or breast cancer at the
time of maximum chemotherapy effect.
A-NK cells are a subset of CD3�CD56�m peripheral blood
NK cells selected by adherence to plastic in the presence of
22 nM of IL-2 (12). A-NK cells can be expanded in culture with
IL-2 for 2 to 3 weeks (12). This subset of NK cells has been
shown recently to preferentially enter human tumor spheroids or
established human tumor xenografts in nude mice and to kill
NK-resistant tumor cells (13). In murine models of tumor me-
tastasis, systemically delivered A-NK cells have been shown to
preferentially localize to metastases (14). Our hypothesis has
Received 11/i 1/94; accepted 3/9/95.
1 This study was supported in part by the Alcoa Foundation (Pittsburgh,
PA), NIH/National Cancer Institute Grant 5U01-CA58271-02, and
Pathology Education and Research Foundation.
2 To whom requests for reprints should be addressed, at Division ofHematology/Bone Marrow Transplantation, University of Pittsburgh
Medical Center, 200 Lothrop Street, Pittsburgh, PA 15213-2582.
3 The abbreviations used are: HDC, high-dose chemotherapy; AlT,
adoptive immunotherapy; LAK. lymphokine-activated killer cells; IL-2,
interleukin 2; A-NK, activated natural killer; PBSCT, peripheral blood
stem cell transplantation; NK, natural killer; G-CSF, granulocyte-
colony-stimulating factor; PBSC, peripheral blood stem cell; rhIL-2,
recombinant human IL-2; HD, high dose; LD, low dose; MNC, mono-
nuclear cells; PE, phycoerythrin; ANC, absolute neutrophil count; CNS,
central nervous system; UPN, unique patient number; PR, partial re-
sponse(s); LU, lytic unit(s).
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

608 Stem Cell Transplantation and Immunotherapy
Table I Patient characteristics
UPN
Age at Transplant
(yr) Diagnosis
Time between diagnosis and
transplant (months) Prior therapy”
380 46 BRC” 56 CMF (6), ROTh, ADRIA (3)
386 60 FML 32 CHOP (10)
385 49 DSCCL 12 ProMACE-CYTABOM (6), CNOP (2)
430 49 FML 50 ProMACE-CYTABOM (2), DICE (3)
448 42 DLCL 12 CHOP (6), ProMACE (1)459 26 HD-NS 43 MitoxBVD (8), ROTE, MOPP/ABV
463 29 HD-NS 46 MOPP-ABVD (12)
465 27 HD-NS 32 MOPP (6)
469 56 FSCCL-DML(T) 61 CHOP (6)
475 40 DML 17 ProMACE-CYTABOM (4), ROTh
485 61 FSCCL-DLCL(T) 131 COAMP (6), ROTL
61 DLCL 51 COP-BLAM (6), CVP (5)
“BRC, breast cancer;FML, follicular mixed lymphoma; DLCL, diffuse largecell lymphoma; HD-NS, nodular sclerosing Hodgkin’s disease;
FSCCL-DML(T), transformation (FSCCL to DML); ROTL, limited field radiotherapy; ROTE, extensive field radiotherapy; DML, diffuse mixed
lymphoma; DSCCL, diffuse small cleaved cell lymphoma; FSCCL-DLCL(T), transformation (FSCCL to DLCL).
h Numbers in parentheses, cycles of chemotherapy given.
been that A-NK cells mediate significant antitumor effects when
administered systemically and home to tumor metastases grow-
ing as solid tissue. Thus, systemic infusion of A-NK cells
supported with IL-2 might eliminate residual tumor surviving
HDC in patients with advanced cancer and decrease the relapse
rate following HDC-PBSCT. As a first step in testing this
hypothesis, this study demonstrates the feasibility of generating
A-NK cells in patients with advanced lymphoma and of corn-
bining HDC-PBSCT with AlT using A-NK cells and IL-2
during the cytopenic phase immediately after the transplant.
MATERIALS AND METHODS
Patients. All patients gave informed consent for partici-
pation in the AlT protocol, which was approved by the Pitts-
burgh Cancer Institute and the Institutional Review Board of the
University of Pittsburgh. The patient characteristics are listed in
Table 1 . Six women and six men were entered on the study. The
mean age of the patients was 44 (range, 26-61) years. Eight
patients had lymphoma, three had Hodgkin’s disease, and one
had metastatic breast cancer. Compassionate approval was ob-
tamed for treatment of the breast cancer patient. These patients
received transplants between November 1992 and February
1994. All patients had failed at least one chemotherapy regimen.
Five of the 12 patients entered on this protocol were judged to
have chemotherapy-responsive disease, demonstrated as a par-
tial or complete response to ifosfamide chemotherapy on eval-
uation 4-8 weeks after its administration.
The patients participating in this study were compared to
42 patients who had received transplants consecutively, between
March 1992 and February 1993, with autologous PBSCT for
recurrent lymphoma or Hodgkin’s disease on another protocol
open at our institution. This protocol targeted the same patient
population, and all patients would have been eligible for trans-
plant on the AlT protocol. Reasons for not participating in the
AlT protocol were patient refusal, or a period of time, January
1993 to April 1993, when the AlT protocol was not open for
accrual, because it was under review by the Food and Drug
Administration. All of the 42 patients who received PBSCT
alone received G-CSF after transplant to accelerate leukocyte
recovery and to potentially reduce the length of hospital stay.
Patients on the AlT protocol did not receive G-CSF posttrans-
plant, so as not to mask any adverse effect of AlT on engraft-
ment or to add a confounding variable to the attribution of
toxicity posttransplant. The comparison targeted toxicity and
engraftment, looking for clinically relevant differences.
Treatment Protocol. The treatment schema for the lym-
phoma patients is shown in Fig. 1. Patients were admitted to
hospital and had a Hickman pheresis catheter placed in the
subclavian position under local anesthesia. Chemotherapy con-
sisting of ifosfamide and Mesna at 3 g/m2/day by continuous i.v.
infusion for 4 and S days, respectively, for the lymphorna
patients and cyclophosphamide and mesna at 5 g/m2 by contin-
uous i.v. infusion for 1 and 2 days, respectively, for the patient
with breast cancer was given. Following chemotherapy, G-CSF
(Neupogen; Arngen, Thousand Oaks, CA) at S p.gfkg/day s.c.
was administered. Daily blood counts were performed. On the
first week day, after ifosfamide-induced leukocyte nadir, with
WBC >1000/pA, leukapheresis for collection of PBSC was
started. A total of 7-9 X 108 MNC/kg were collected.
On the first Monday after PBSC collection, rhIL-2 (Chiron
Corp., Emeryville, CA) at 3 X i0� IU/m2/day by continuous i.v.
infusion was started, using a Pharmacia-Deltec CADD-1 pump
(Pharmacia Deltec, St. Paul, MN) and was continued for 6 days.
The following Monday, daily 4-h leukapheresis began and con-
tinued for 4 days (second leukapheresis series). The time from
the first day of leukapheresis for PBSCs (first leukapheresis)
and the beginning of leukapheresis for A-NK cells (second
leukapheresis) varied between 2 and 4 weeks. The WBC was
normal at the time of the second leukapheresis procedure. The
collections were processed by the Cellular Adoptive Immuno-
therapy Laboratory of the Pittsburgh Cancer Institute and were
cultured for the generation of A-NK cells as described below.
The patients were then admitted to the Bone Marrow
Transplant Unit to begin HDC. Supportive care included single
rooms with positive pressure high efficiency particular air fil-
tered air, low microbial content diets, prophylactic antibiotics
and acyclovir, blood product support, and i.v. antibiotics and
amphotericin as clinically indicated. The patients with lym-
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Begin LD - CII - LL-2 day +6at 3 X 105 lU/rn2 IV CII daily
continue to day +96
Clinical Cancer Research 609
( High dose Ifosfamide I Mesas
I 3 gm/m2/d CII X 4 days
� MesnaCil
r� G-CSF
I to begin after chemotherapy and to continue� until end offirst leukapheresis J
Fig. I Flow diagram of the treatment plan for patients with lymphomaundergoing HDC-PBSCT followed by AlT with A-NK cells and IL-2.
cli, continuous iv. infusion; LD-Cll-IL-2, low-dose continuous iv.
infusion of IL-2.
phoma received busulfan (16 mg/kg) and cyclophosphamide
(120 mg/kg) as conditioning (15). The patient with breast cancer
received cyclophosphamide (1500 mg/m2/day), thiotepa (125
mg/m2/day), carboplatinum (200 mg/m2/day), and mesna (1500
mg/m2/day), all for 4 days (day-6 to day-3) by continuous i.v.
infusion (16).
Patients received the PBSCT product on day 0 and the
A-NK cells on day +2, both as a rapid i.v. infusion. On day +2,
coincident with the A-NK cell infusion, a continuous i.v. infu-
sion of rhIL-2 at 2 X 106 IU/m2/day (HD-rhIL-2) was started
and continued for 4 days. Thereafter, the dose of rhIL-2 was
reduced to 3 X i0� IU/m2/day (LD-rhIL-2), and IL-2 was
continued as outpatient therapy for 90 days.
Clinical evaluations of response were performed at 1 and 3
months posttransplantation and then every 3 months for 2 years.
Toxicity grading was performed daily during hospitalization and
then weekly during outpatient treatment.
PBSC Product. PBSCs were obtained daily by 4-h leu-
kapheresis (Cobe Spectra; Cobe BC!’, Inc., Lakewood, CO)
until the total collected MNC count was 7-9 X 108/kg. All
patients received 7 X 108 MNCIkg, with the excess portion
reserved for treatment of graft failure. A median number of
seven collections (range, 5-1 1) was performed per patient. Total
cell counts were determined on an automated cell counter
(Coulter ZM; Coulter, Hialeah, FL). The pheresis product (50%
v/v) was mixed with 10% DMSO (v/v, Cryoserv; Research
Industries Corporation, Salt Lake City, UT), and 20% autolo-
gous plasma (v/v) in 20% Medium 199 (Life Technologies, Inc.,
Grand Island, NY). The cell concentration was adjusted to not
exceed 2 X 10� cells/ml, and 60-ml aliquots were transferred to
bags (Cel Freeze Cryogenic Storage Containers; Chartermed,
Lakewood, NJ) for controlled rate freezing. The bags were
stored in liquid nitrogen and thawed in a 37#{176}Cwater bath at the
bedside immediately prior to infusion.
A-NK Cell Product. Following low-dose IL-2 priming
(see Fig. 1), leukapheresis was performed daily for 4 consecu-
tive days to collect cells for the generation of A-NK cells. MNC
were separated by Ficoll-Hypaque density gradient centrifuga-
tion and depleted of monocytes by treatment with 5 m�i phe-
nylalanine methyl ester (Terumo Medical Corp., Elkton, MD)
for 40 mm at room temperature (17). Monocyte depletion was
previously found to be necessary for optimal culture of A-NK
cells (12). The monocyte-depleted MNC were washed and re-
suspended at a concentration of 5 X 10” cells/ml in the complete
culture medium (RPMI 1640 from GIBCO, Grand Island, NY)
containing 6000 IU/ml rhIL-2 (Chiron Corp.), 10% pooled,
heated-inactivated human AB serum (v/v; Nabi, Miami, FL),
and 50 p.g/ml gentamicin (GIBCO). A-NK cells were captured
on the surface of plastic culture flasks during 4-5-h incubation
in the presence of 6000 lU/mi of IL-2 in an atmosphere of 5%
CO2 in air at 37#{176}C,as previously described (12). Nonadherent
MNC were removed by vigorous washing of the flasks with
warm culture medium containing 2% human AB serum (v/v).
Fresh complete culture medium containing 6000 lU/mI rhIL-2
was added back to the plastic culture flasks, and the number of
cells adherent to plastic determined using an inverted micro-
scope. A-NK cell cultures were supplemented with irradiated
allogeneic concanavalin A-preactivated MNC on day 1, as de-
scribed earlier (12), and cultured for 14-18 days. A-NK cell
cultures were monitored three times a week for growth and
viability of cells by hemacytometer counts performed with
trypan blue dye on aliquots of the culture. Cultures were main-
tamed at a cell density of 1-2 X 10” cells/mi by supplementa-
tion with complete culture medium containing rhIL-2 every 4
days. On the day of patient infusion (day +2), aliquots of the
A-NK cell product were sampled for flow cytometry, and as-
sessments of cytotoxic activity against K562 and Daudi cell
lines as well as bacterial and fungal culture were made. The
A-NK cell product was characterized by purity of the cells
(% CD3CD56�), fold expansion in culture based on the initial
and final cell counts (12), and cytotoxic activity against the
selected tumor cell targets (Table 2).
Flow Cytometry. MNC were isolated from the patients’
peripheral blood by centrifugation over Ficoll, washed, and
incubated with FITC- and PE-conjugated mAbs in preparation
for two-color flow cytometry. In some cases, peridinin chloro-
phyll protein-conjugated mAbs were also used for three-color
flow. Isotype controls used were IgG1-FITC, IgG2A-PE, and
IgG1-peridinin chlorophyll protein. Gates were set to include
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

610 Stem Cell Transplantation and Immunotherapy
Table 2 Proportions of NK cells a nd NK activity in the pheresis products used to start the A-NK cell cul
generated for therapy
tures and character istics of A-NK cells
Pheresis product A-NK cells
Fold proliferation’
Total no. ofcells infused”
CD3CD56�(%)“
Cytotoxicityvs. Daudi”UPN
CD3CD56�(%)(i
Cytotoxicityi.s. K562’�
380
386
385
430
448
459
463
465
469
475
485
501
2511
2
9
8
11
8
18
1 1
11
14
10
348
319
36
97
177
116
120
147
48
313
341
153
75
148
30
12
76
1
1
1
19
9
1
3
2.4 X i01#{176}
4.0 X iO’#{176}
1.6 x 10”
8.3 x 10�2.0 x iO’#{176}
1.2 X 10�
6.8 X 108
1.2 x i0�
4.6 X 10�
1.2 X iO’#{176}
oe1.0 X 10”
98
91
64
7080
95
69
97
87
88
95
95
3,363
6,174
3,631
23,435
5,388
14,411
2,621
5,389
14,437
8,712
5,398
13,733
a Determined by two-color flow cytometry.
I, Cytotoxicity expressed as LU24,/107 cells determined in 4-h 51Cr release assays.
( Total number of cells on day 14 of culture divided by number of initial plastic-adherent cells.
(I Number of therapeutic culture cells infused.
(� I . 1 X iO� cells were generated from this culture; however, these were not infused because the patient was taken off protocol on day -5 due
to the appearance of symptomatic CNS lymphoma.
CD45 � cells and to exclude debris. The mAb-labeled cells were
analyzed with a FACScan flow cytometer using Consort-32
software (Becton Dickinson, San Jose, CA). The mAbs used for
staining were specific for CD3, CD45, CD56 (Becton Dickin-
son), and CD16 (Medarex, West Lebanon, NH). When cell
numbers permitted, i04 gated events were analyzed (approxi-
mately 90% of samples).
Total numbers of CD34� and lineage negative
(CD34 ‘ ‘“‘ ) cells were determined in the daily PBSC product
by flow cytometry. An aliquot of the PBSC daily product was
stained with two anti-CD34, FITC-conjugated mAbs (8G12;
Becton Dickinson and Qbend-10; GenTrak, Plymouth Meeting,
PA) and four lineage specific PE-conjugated mAbs with spec-
ificity for CD3, CD11b, CD14, and CD19 (Becton Dickinson).
U937 cells were used to gate out autofluorescence, and debris
was excluded by reference to 6-p.m beads. The percentage of
each CD34� population in 20,000 events was used to quantify
the total count of each population in the PBSC product.
Cytotoxicity Assay. The 51Cr release assay used in our
laboratories has been described in detail previously (18).
Briefly, resting NK or A-NK cells were incubated with 51Cr-
labeled K562 or Daudi target cells for 4 h at E:T ratios ranging
from 6 to 50: 1 for resting NK cells and from 0.3 to 6:1 for A-NK
cells. Cytotoxicity was expressed as LU2�J107 effector cells,
where one LU20 is the number of cellular effectors required for
20% lysis of 1 X � target cells (18).
Statistics. The Wilcoxon rank sum test (two-tailed) was
used to compare engraftment parameters between the control
patients and the patients participating in the AlT protocol.
Patients from both groups who received <6 X 10” CD34�”
cells/kg and who had reached the target engraftment parameters
before 40 days after transplant were compared. Patients in both
groups who had received >6 X 106 CD34�” cells/kg all
engrafted rapidly and were excluded from the analysis.
RESULTS
Generation of A-NK Cells. A-NK cells obtained from
the peripheral blood of normal volunteers were previously found
to proliferate extensively (up to 5000-fold expansion during 14
days of culture) in our hands (12). However, it was uncertain
whether it would be feasible to generate these effector cells in
patients with lymphoma or metastatic breast cancer. We found
that in all patients, it was possible to generate highly purified
A-NK cells from leukapheresis products collected after 6-day
priming with LD-rhIL-2 (Table 2). In three patients with
Hodgkin’s disease, A-NK cells failed to expand in culture under
conditions used routinely in our laboratory (Table 2). The levels
of proliferation in 14-day cultures of A-NK cells obtained from
patients with NHL varied from 1- to 148-fold. Neither the
percentage of CD3CD56� cells nor levels of NK activity were
lower in the pheresis products of patients with HD, as compared
to the patients with lymphoma (Table 2). All three patients with
Hodgkin’s disease had a nodular sclerosing histology. Extent of
prior treatment, time interval between diagnosis and transplant,
and disease extent did not predict for the ability to generate
A-NK cells in this group of patients. Overall, in 6 of 12 patients,
it was possible to obtain > 1 X 10’#{176}A-NK cells for AlT. In 8
of 12 patients, cultured A-NK cells were >85% CD3CD56�
cells, and the A-NK cell culture with the lowest purity contained
64% CD3CD56� cells.
Engraftment. All patients engrafted and became trans-
fusion independent following HDC-PBSCF and AlT. The me-
dian day to reach an ANC of 500/pA was 14 (range, 1 1-19) days.
The median day to reach a platelet count of 50,000/pA was 13.5
(range, 9-200) days. The median time for granulocyte recovery
was significantly (P < 0.001) shortened in 42 patients treated
with G-CSF after HDC-PBSCT relative to 1 1 patients who
received AlT with A-NK cells posttransplant. This difference is
consistent with G-CSF administration, suggesting no adverse
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

BA
Liz.<
0
0
I I I
PBSC+A-NK #{149}
PBSC + G.CSF 0
S
15 5
S SS 0
0
0 �
10 5 00
0 0
0
5
I I I
0 40
Clinical Cancer Research 611
20
10 20 30
Day to Platelet Count > 50,000/pi
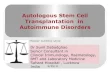
Fig. 2 Scatterplot of day posttransplant to an ANC > 500/�i.l and a
platelet count > 50,000/pJ in patients undergoing PBSCT with AlT or
G-CSF posttransplant. All patients received <6 X 10” CD34�1��
cells/kg.
effect on neutrophil engraftment from AlT. Seven patients had
rapid, sustained platelet engraftment and achieved a platelet
count of 50,000/pA 1-3 days before their ANC reached 500/pA.
Five of these patients received less than 6 X 10” of CD341�_
cells/kg, and in comparison to control patients, whose grafts
contained similar numbers of stem cells, their platelet engraft-
ment was significantly more rapid (Fig. 2; P < 0.001). Our
experience has been that regardless of the type of transplant or
the source of stem cells, any patient receiving >1 X i0�
CD34�� cells/kg rapidly engrafted, achieving an ANC >
500/pA and a platelet count > 50,000/pA on or before day + 13.
The same was true for PBSCT, when >6 X 10” CD34�”�
cells/kg were transplanted. Therefore, we compared patients
who received <6 X 10” CD34�’”’ cells/kg and reached a
platelet count of 50,000/pA before 40 days in both the AlT and
G-CSF transplant groups. Those patients who received AlT had
significantly accelerated platelet production after transplantation
(Fig. 2).
In aggregate, these data indicate that AlT with A-NK cells
plus IL-2 did not adversely affect hematopoietic recovery, in a
clinically relevant fashion, when administered immediately after
PBSCT and may have accelerated platelet engraftment in a
subset of patients.
Toxicity. Therapy was discontinued in three patients
(UPN 485, 465, and 448 on days + 1, +5, and +25, respective-
ly). Reasons for discontinuation were: CNS lymphoma (UPN
448 and 485) and severe anxiety (UPN 465). Both patients with
CNS lymphoma were free of symptoms on entry into the study,
but developed signs of CNS involvement before A-NK cells and
HD-rhIL-2 were administered. One patient (UPN 448) received
intrathecal chemotherapy and radiation to the pons for CNS
lymphoma before HDC began. She continued on treatment until
day +25, when she requested to be withdrawn from the proto-
col, because of persistent quadraparesis. Four patients have
died; UPN 385 on day + 109 from interstitial pneumonitis, UPN
448 on day +72 and UPN 485 on day + 162 from CNS lym-
phoma, and UPN 469 on day + 171 from recurrent lymphoma.
Toxicity from the rhIL-2 and A-NK cells was limited to mild
hypotension and edema occurring from days +3 to +7. Two
patients received low-dose dopamine for hypotension and had
reduced urine output during this time. No patient experienced
renal failure, veno-occlusive disease, hemorrhagic cystitis, or
diffuse alveolar hemorrhage.
Immunological Modulation. The percentage of
CD3CD56� or CD3CD56�CD16� (NK) cells and NK ac-
tivity against K562 targets in the patients’ peripheral blood were
measured at various times during the treatment. Table 3 shows
the results of NK phenotyping and NK activity in four patients
for whom serial data were available before and in the early
posttransplant period. Of the four patients, three (UPN 380, 386,
and 475) had normal NK activity before therapy. During the
period between day +3 and +8, when the absolute leukocyte
count was <200/pA, variable but detectable cytotoxicity was
observed in the blood, which might be attributable to A-NK cell
infusion. Fig. 3 shows serial results in UPN 386, demonstrating
the initial peak of NK activity followed by the gradual rise
attributed to LD-rhIL-2 over 90 days posttransplant. In general,
the number of circulating NK cells after transplant did not
correlate with NK activity. As illustrated in Fig. 3, despite a
rapid fall in cytotoxicity from the peak on day +3, the number
of NK cells continued to increase in the peripheral blood.
Similar increases in the absolute number of circulating NK cells
were seen in other patients. Spontaneous cytolytic activity of
fresh peripheral blood mononuclear cells against Daudi targets
was detected in the peripheral blood of two patients (UPN 385
and 386) in the immediate posttransplant period, and this could
be interpreted as additional evidence in support of the presence
of circulating transferred A-NK cells.
Ifosfamide. Ifosfamide chemotherapy was used to test for
chemosensitivity of each lymphoma and for mobilization of
PBSCS. Five of 10 patients responded to ifosfamide (2 complete
responses, 3 PR, overall response rate of 50%). No patient exhib-
ited progressive disease on ifosfamide. One patient (UPN 485)
developed a Fanconi-like renal wasting syndrome that recovered
spontaneously. Outside of predictable pancytopenia, there were no
other side effects directly attributable to ifosfamide.
Busulfan/Cyclophosphamide. There was no mortality
attributable to the conditioning regimen, and toxicity was tran-
sient. The 3-month response evaluations showed that response
had improved in five patients, was unchanged in three, and had
worsened in two. Three of the five patients experienced im-
provement from a PR to complete response and two from stable
disease to PR. This conditioning regimen was well tolerated and
active in this group of patients.
DISCUSSION
This clinical trial demonstrates the feasibility of adding
AlT with autologous A-NK cells and IL-2 in the pancytopenic
period immediately after PBSCT. This is a rational combination
of therapies, because they differ in their mechanism of action,
mechanism of disease resistance, and toxicity. In our hands, AlT
was used in an effort to exert a further antitumor effect at the
time of minimal disease after HDC-PBSCT.
The choice of A-NK cells for AlT was based on our
preliminary data indicating that this subset of IL-2-activated
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Table 3 NK activity and percentage of MNC with NK cell phenotype in the blood of patients treated with HDC-PBSCT and AlT
UPN (diagnosis)”Before therapy”
LU’
Days +3 to �8d Day +90�
LUC
% NKcellse LU�
% NKcellse
380 (BRC)
385 (DSCCL)
386 (FML)
475 (DML)
319
33
325
415
772
2641673
287
32
2
41
n/a
833
440883
1290
25
3
48
32
a Only the patients cited exhibited increased NK activity in the blood on days +3 to +8, the other patients had values between 0 and 33 LU (see
Table 1 for diagnosis codes).6 This measurement (LU) was obtained before any protocol therapy had started and at least 4 weeks past any prior therapy.
C NK activity was measured in the PBMC of patients using 4-h 51Cr release assays with K562 as targets and is expressed as LU2(,/107 effector
cells (LU). The normal range in our laboratory is 50-300 LU, with a median of 132 LU.d The absolute leukocyte count was <200/jil at the time of this measurement. No lytic activity is detectable in the absence of A-NK cell infusion.
e % NK cells was determined by flow cytometry in two (CD356�) or three-color (CD356� 16k) analysis. The normal range for our laboratoryis 6-21%, with a median of 12%.
1The absolute leukocyte count was normal at the time of this measurement.
400
0
350 B�C’
0�
C’
0
zC.)
C’
.�
0-I
0�
00
0.0
-20 0 20 40 60 80 100
Day relative to transplant
Fig. 3 Changes in NK activity (LU7�1/107 cells) and in the absolute number of NK cells/pA in the peripheral blood of UPN 386 between days -20and + 100 of therapy relative to transplantation (day 0).
612 Stem Cell Transplantation and Immunotherapy
1800
. 1600
� 1400
U
� 1200
� 1000
I: 800
.� 600
� 400
200
0
CDrCD56(�mCD16_ or dim NK cells has potent antitumor
activity in vitro and in vivo (12, 19) and is particularly effective
in targeting metastases (14, 20). A-NK cells have been shown to
be able to produce a variety of cytokines (20, 21), localize to
metastases (20), and rapidly eliminate established metastases in
animal tumor models (13, 14, 19). Activities of A-NK cells are
strictly dependent on the presence of IL-2 (10, 22). At 2 X 106
IU/m2/day (HD-rhIL-2), the serum concentration of IL-2 was
estimated to be sufficient to bind high affinity IL-2 receptor
(22). Thus, we reasoned that the infused A-NK cells, a propor-
tion of which expresses the high affinity IL-2 receptor (12),
were likely to be stimulated in vivo, at least during the initial 4
days after adoptive transfer.
We hypothesized that the timing of A-NK cell transfusion
might be critical for cure. Animal models of combined chemo-
therapy and AlT have shown that the smaller the time interval
between the two therapies, the greater the cure rate (23, 24). On
300
250
200
150
100
50
0
the basis of earlier observations, we planned to give the A-NK
cells and IL-2 as close to the chemotherapy as possible.
Our main concerns were the possible adverse effect of AlT
on engraftment and the added toxicity of AlT in the pancyto-
penic phase after HDC-PBSCT. Our preclinical studies showed
no suppression of colony formation in vitro by human A-NK
cells and that at the higher A-NK to progenitor ratios, there may
actually be enhancement of growth (25). Murphy et a!. (26, 27)
and Siefer et a!. (28) have shown accelerated platelet production
after marrow transplantation, in a murine model, that is depen-
dent upon infusion of murine NK cells. We believe that we may
have observed an analogous phenomenon in humans.
The administration of IL-2 at doses sufficiently high to
support the antitumor activity of A-NK cells was an essential
component of the therapy. To reduce IL-2-related toxicity, two
design principles were used in this trial. First, the doses of
rhIL-2 used were one to two orders of magnitude less than those
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 613
used previously for therapy. Second, during the pancytopenic
phase, induction of cytokine secretion from monocytes and
thromboxane A2 from neutrophils would be absent. These sec-
ondarily generated molecules are thought to mediate the toxic
effects of IL-2 (29), and their absence would be expected to
reduce IL-2-induced toxicity. Indeed, toxicity attributable to
IL-2 was tolerable in this trial. The subsequent 90-day infusion
with LD-rhIL-2 was used in the hope of sustaining or expanding
in vivo antitumor effector cells. It has been shown previously to
expand the number of circulating CD56� NK cells without
affecting the number of T lymphocytes in patients with cancer
and prime for LAK activity generated in vitro with higher
concentrations of IL-2 (30-32).
The NK and LAK activity observed in the blood of these
patients can be explained by the persistence in the circulation of
functional transfused A-NK cells. NK activity in the blood is
normally absent after transplant and returns no earlier than the
third week. In Fig. 3, the initial peak of activity observed at day
+3 coincides with the transfusion of the A-NK cells and their
support with HD-rhIL-2. The subsequent fall in activity can be
ascribed to the death of the A-NK cells, which may at least
partially be due to the withdrawal of HD-rhIL-2. The presence
of cells with NK phenotype but lack of activity suggests the
presence of a nonfunctional precursor that acquires NK activity
with maturation. The cells responsible for this activity are prob-
ably not of transfused A-NK cell origin.
The ability to consistently generate A-NK cells from the
peripheral blood of patients with advanced lymphoma or solid
tumors has also been of concern (33). To facilitate A-NK cell
generation, a 6-day-long infusion of LD-rhIL-2 before the series
of phereses for A-NK cell generation was included in the
protocol. The intent was to increase the yield of A-NK cells in
culture by priming their progenitors in vivo. Using this approach
and the improved culture conditions, i.e., short adherence time
and irradiated feeder cells, as described earlier (12), we have
been able to generate cell cultures which were highly enriched
in CD3CD56� cells in all patients with lymphoma. However,
A-NK cells obtained from the peripheral blood of the 3 patients
with Hodgkin’s disease showed poor in vitro growth. No spe-
cific cause for this poor A-NK cell generation in culture could
be discerned, and it did not appear to be related to the extent of
prior treatment these patients received or to the extent of their
disease. Both the number of NK cells in the peripheral circula-
tion and NK activity were normal at baseline in these three
patients. Hodgkin’s disease is known to be associated with a
profound cellular immune deficit (34), and it is intriguing to
speculate that the observed inability to generate A-NK cells
might be related to a low number or poor function of A-NK cell
precursors in the peripheral blood of these patients.
Using a combination of HDC-PBSCT and AlT with A-NK
cells and IL-2 had no clinically relevant adverse effects on
engraftment and toxicity, which were both comparable to those
seen with HDC-PBSCT alone. In a subset of patients treated
with AlT, platelet engraftment may have been accelerated. In
addition, early amplification of NK cell function in the cytope-
nic phase after transplantation, that could have its origin in the
transfused A-NK cells, was observed in some patients. Future
studies will attempt to optimize AlT with A-NK cells and to
dissect the contribution of each transfused cell population to the
immunological changes observed.
ACKNOWLEDGMENTS
We thank Dr. Ronald B. Herberman and Dr. A. Louie for critical
review of the treatment protocol.
REFERENCES
1. Antman, K. Dose-intensive therapy in breast cancer. In: J. Armitageand K. Antman (eds.), High-Dose Cancer Therapy-Pharmacology,
Hematopoietins, Stem Cells, p. 701 . Baltimore: Williams & Wilkins,
1992.
2. Appelbaum, F., Thomas, E., and Buckner, C. Treatment of non-
Hodgkin’s lymphoma with chemoradiotherapy and allogeneic marrow
transplantation. Hematol. Oncol., 1: 149-157, 1983.
3. Fefer, A., Cheever, M. A., and Greenberg, P. D. Identical-twin
(syngeneic) marrow transplantation for hematologic cancers. J. Natl.
Cancer Inst., 76: 1269-1273, 1986.
4. Appelbaum F. R., Sullivan, K. M., Buckner, C. D., Clift R. A., Deeg,
H. J., Fefer, A., Hill, R., Mortimer, J., Neiman, P. E., Sanders, J. E.,
Singer, J., Stewart, P., Storb, R., and Thomas E. D. Treatment of
malignant lymphoma in 100 patients with chemotherapy, total body
irradiation, and marrow transplantation. J. Clin. Oncol., 5: 1340-1347,
1987.
5. Armitage, J. 0., Jagannath, S., Spitzer, G., Bierman, P., Kessinger,
A., Kumar, P., Cabanillas, F., Zander, A., Vellekoop, L., and Dicke,K. A. High-dose therapy and autologous marrow transplantation assalvage treatment for patients with diffuse large cell lymphoma. Eur. J.
Cancer Clin. Oncol., 22: 871, 1986.
6. Weisdorf, D. J., Haake, R., Miller, W. J., McGlave, P. B., LeBien,
T. W., Vallera, D. A., Lasky, L. C., Kim, T. H., Peterson, B. A.,Ramsay, N. K., Kersey, J. H., and Hurd, D. D. Autologous bone marrow
transplantation for progressive non-Hodgkin’s lymphoma: Clinical im-
pact of immunophenotyping and in vitro purging. Bone Marrow
Transpl., 8: 135-142, 1991.
7. Takvorian, T., Canellos, G. P., Ritz, J., Freedman, A. S., Anderson,
K. C., Mauch, P., Tarbell, N., Coral, F., Daley, H., Yeap, B., Schloss-
man, S. F., and Nadler, L. M. Prolonged disease-free survival after
autologous bone marrow transplantation in patients with non-Hodgkin’s
lymphoma with a poor prognosis. N. EngI. J. Med., 316: 1499-1505,
1987.
8. Rosenberg, S. A., Lotze, M. T., Muul, L. M., Chang, A. E., Avis,
F. P., Leitman, S., Lineban, W. M., Robertson, C. N., Lee, R. E., Rubin,J. T., Seipp, C. A., Simpson, C. G., and White, D. E. A progress reporton the treatment of 157 patients with advanced cancer using lympho-
kine-activated killer cells and interleukin 2 or high-dose interleukin 2
alone. N. Engl. J. Med., 316: 889-897, 1987.
9. Rosenberg, S. A., Yannelli, J. R., Yang, J. C., Topalian, S. L.,
Schwartzentruber, D. J., Weber, J. S., Parkinson, D. R., Seipp, C. A.,
Einhorn, J. H., and White, D. E. Treatment of patients with metastatic
melanoma with autologous tumor-infiltrating lymphocytes and interleu-
kin 2. J. Natl. Cancer Inst., 86: 1159-1166, 1994.
10. Rosenberg, S. A., Lotze, M. T., Yang, J. C., Topalian, S. L., Chang,
A. E., Schwartzentruber, D. J., Aebersold, P., Leitman, S., Linehan,W. M., Seipp, C. A., White, D. E., and Steinberg, S. M. Prospective
randomized trial of high-dose interleukin-2 alone or in conjunction with
lymphokine-activated killer cells for the treatment of patients with
advanced cancer. J. Natl. Cancer Inst., 85: 622-632, 1993.
11. Bernstein, Z. P., Vaickus, L., Friedman, N., Goldrosen, M. H.,Watanabe, H., Rahman, R., Arbuck, S. G., Sweeney, J., Vesper, D.,
Henderson, E. D., Zeffren, J., Dennin, R. A., Levitt, D., and Foon,
K. A. Interleukin 2 lymphokine-activated killer cell therapy of non-
Hodgkin’s lymphoma and Hodgkin’s disease. J. Immunother., 10:
141-146, 1991.
12. Vujanovic, N. L., Rabinowich, H., Lee, Y. J., Jost, L., Herberman,
R. B., and Whiteside, T. L. Distinct phenotypic and functional character-
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

614 Stem Cell Transplantation and Immunotherapy
istics of human natural killer cells obtained by rapid interleukin 2-induced
adherence to plastic. Cell. Immunol., 151: 133-157, 1993.
13. Vujanovic, N. L., Yasumura, S., Hirabayashi, H., Lin, W. C.,
Watkins, S., Herberman, R. B., and Whiteside, T. L. Antitumor activi-
ties of human 1L2-activated natural killer (A-NK) cells in solid tumor
tissues. J. Immunol., 154: 281-289, 1995.
14. Yasumura, S., Lin, W., Hirabayashi, H., Vujanovic, N. L., Herber-
man, R. B., and Whiteside, T. L. Immunotherapy of liver metastases of
human gastric carcinoma with IL2-activated natural killer cells. Cancer
Res., 54: 3808-3816, 1994.
15. Tutschka, P., Copelan, E., and Klein, J. Bone marrow transplanta-
tion for leukemia following a new busulfan and cyclophosphamide
regimen. Blood, 70: 1382-1388, 1987.
16. Antman, K., Ayash, L., Elias, A., Wheeler, C., Hunt, M., Eder, J. P.,
Teicher, B. A., Critchlow, J., Bibbo, J., Schnipper, L. E., and Frei, E. A
phase II study of high-dose cyclophosphamide, thiotepa and carboplatin
with autologous marrow support in women with measureable advanced
breast cancer responding to standard-dose therapy. J. Clin. Oncol., 10:
102-110, 1992.
17. Rabinowich, H., Sedlmayr, P., Herberman, R. B., and Whiteside,
T. L. Increased proliferation, lytic activity and purity of natural killercells co-cultured with mitogen-activated feeder cells. Cell. Immunol.,
135: 454-470, 1991.
18. Whiteside, T. L., Bryant, J., Day, R., and Herberman, R. B. Natural
killer cytotoxicity in the diagnosis of immune dysfunction: criteria for areproducible assay. J. Clin. Lab. Anal., 2: 102-114, 1990.
19. Sacchi, M., Vitolo, D., Sedlmayr, P., Rabinowich, H., Johnson,J. T., Herberman, R. B., and Whiteside, T. L. Induction of tumorregression in an experimental model of human head and neck cancer byhuman A-LAK cells and IL2. Int. J. Cancer, 47: 784-791, 1991.
20. Basse, P., Herberman, R. B., Nannmark, U., Johansson, B. R.,
Hokland, M., Wasserman, K., and Goldfarb, R. H. Accumulation ofadoptively transferred adherent, lymphokine-activated killer cells in
murine metastases. J. Exp. Med., 174: 479-488, 1991.
21. Vitolo, D., Vujanovic, N., Rabinowich, H., Schlesinger, M.,
Herberman, R. B., and Whiteside, T. L. Rapid interleukin-2 induced
adherence of human natural killer (NK) cells: II. Expression of
mRNA for cytokines and IL2 receptors in adherent NK cells. J.Immunol., 151: 1926-1937, 1993.
22. Smith, K. Lowest dose interleukin 2 immunotherapy. Blood, 81:
1414-1423, 1993.
23. Basse, P. H., Goldfarb, R. H., Herberman, R. B., and Hokland,
M. E. Accumulation of adoptively transferred A-NK cells in murine
metastases: kinetics and role of interleukin-2. In Vivo, 8: 17-24,
1994.
24. Norton, L., and Surbone, A. Cytokinetics. In: J. Holland, E. Frei,R. Bast, D. Kufe, D. Morton, and R. Weischselbaum (eds.), Cancer
Medicine, pp. 598-617. Philadelphia: Lea and Febiger, 1993.
25. Pincus, S., Lister, J., Silla, L., Belts, L., Elder, E., Rybka, W.,
Donnenberg, A., and Whiteside, T. Effects of interleukin 2 (1L2)-
activated adherent natural killer (A-NK) cells on hematopoiesis. Clin.
Res., 41: 365a, 1993.
26. Murphy, W. J., and Longo, D. L. Hematopoietic growth-promot-
ing effects of natural killer cells in mice in response to in vivo
administration of human interleukin 2. J. Natl. Cancer Inst., 84:
1195-1200, 1992.
27. Murphy, W. J., Keller, J. R., Harrison, C. L., Young, H. A., and
Longo, D. L. Interleukin 2-activated natural killer cells can support
hematopoiesis in vitro and promote marrow engraftment in vivo. Blood,80: 670-677, 1992.
28. Siefer, A. K., Longo, D. L., Harrison, C. L., Reynolds, C. W., and
Murphy, W. J. Activated natural killer cells and interleukin 2 promote
granulocytic and megakaryocytic reconstitution after syngeneic bone
marrow transplantation in mice. Blood, 82: 2577-2584, 1993.
29. Lotze, M. Interleukin 2: basic principles, In: V. De Vita, S. Hell-man, and S. Rosenberg (eds.), Biologic Therapy of Cancer, pp. 123-
141. Philadelphia: J. B. Lippincott Co., 1991.
30. Caligiuri, M. A., Murray, C., Soiffer, R. J., Klumpp, T. R., Seiden,M., Cochran, K., Cameron, C., Ish, C., Buchanan, L., Perillo, D., Smith,
K., and Ritz, J. Extended continuous infusion low-dose recombinantinterleukin 2 in advanced cancer: Prolonged immunomodulation without
significant toxicity. J. Clin. Oncol., 9: 21 10-21 19, 1991.
31. Caligiuri, M. A., Murray, C., Robertson, M. J., Wang, E., Cochran,
K., Cameron, C., Schow, P., Ross, M. E., Klumpp, T. R., Soiffer, R. J.,Smith, K. A., and Ritz, J. Selective modulation of human natural killer
cells in vivo after prolonged infusion of low dose recombinant interleu-
kin 2. J. Clin. Invest., 91: 123-132, 1993.
32. Soiffer, R. J., Murray, C., Cochran, K., Cameron, C., Wang, E.,
Schow, P. W., Daley, J. F., and Ritz, J. Clinical and immunologic effects
of prolonged infusion of low-dose recombinant interleukin 2 after au-
tologous and T-cell depleted allogeneic bone marrow transplantation.
Blood, 79: 517-526, 1992.
33. Sedlmayr, P., Rabinowich, H., Elder, E. M., Ernstoff, M. S., Kirk-wood, J. M., Herberman, R. B., and Whiteside, T. L. Depressed ability
of patients with melanoma or renal cell carcinoma to generate adherent
lymphokine activated killer (A-LAK) cells. J. Immunother., 10: 336-
346, 1992.
34. Bierman, P. J., Vose, J. M., and Armitage, J. 0. Autologous trans-
plantation for Hodgkin’s disease: coming of age? Blood, 83: 1161-
1164, 1994.
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

1995;1:607-614. Clin Cancer Res J Lister, W B Rybka, A D Donnenberg, et al. immediate posttransplant period.
theadoptive immunotherapy with activated natural killer cells in Autologous peripheral blood stem cell transplantation and
Updated version
http://clincancerres.aacrjournals.org/content/1/6/607
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/1/6/607To request permission to re-use all or part of this article, use this link
Research. on August 1, 2020. © 1995 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Related Documents