[Frontiers in Bioscience 4, e???-???, April 7, 1999] 1 AUTOLOGOUS PERIPHERAL BLOOD STEM CELL TRANSPLANTS IN COMMUNITY CANCER CENTERS C. D. Buckner, C. H. Weaver, L. S. Schwartzberg, R. Birch, B. Zhen and W. West Response Oncology, Inc., 600 Broadway, Suite 112, , Seattle, Washington TABLE OF CONTENTS 1. Abstract 2. Introduction 3. Mobilization and Harvesting of PBSC 4. Mobilization of PBSC with G-CSF Alone 5. Mobilization of PBSC with Chemotherapy and a Growth Factor 6. Mobilization of PBSC with cyclophosphamide, etoposide (CE) and G-CSF 7. Evaluation of 2 versus 4 g/m2 of Cyclophosphamide in the CE Regimen 8. Comparison of CE to CEP for Mobilization of PBSC 9. Evaluation of Cyclophosphamide, Paclitaxel and G-CSF for Mobilization of PBSC 10. Evaluation of Cyclophosphamide, Docetaxel and G-CSF for Mobilization of PBSC 11. Patients who have Low CD34+ Cell Yields with First Attempts 12. Conclusions Concerning Studies of PBSC Mobilization 13. Current Status of Purging of BM or PBSC 14. Purging of Grafts in Patients with Non-Hodgkin’s Lymphoma 15. Purging of Grafts in Patients with Multiple Myeloma 16. Purging of Grafts in Patients with Breast Cancer 17. Conclusions Concerning Purging of PBSC 18. Neutrophil and Platelet Recovery Following Infusion of PBSC 19. Effects of Infusion of PBSC with a Low CD34+ Cell Dose 21. Treatment Related Morbidity 22. Outcomes of Clinical Trials of Outpatient HDC with PBSC Support 23. Results of HDC in Patients with Breast Cancer 23.1. Patients with Metastatic Breast Cancer 24. Patients with Stage II-III Breast Cancer with ≥10+ Nodes 25. Patients with Stage II-III Breast Cancer with 5-9+Nodes 26. Conclusions Concerning Adjuvant Therapy for Patients with Breast Cancer 27. Results of HDC in Patients with Malignant Lymphoma 27.1. Patients with Hodgkin’s Disease 28. Patients with Low Grade NHL 29. Patients with Intermediate and High-Grade NHL 31. Results of HDC in Patients with Multiple Myeloma 32. Results of HDC in Patients with Ovarian Cancer 33. What is the Future of HDC with PBSC Support 33.1. Use of PBSC will Expand for Indicated Therapy and in the Evaluation of New Therapies 33.2. Immune Therapies will be Evaluated after HDC with PBSC Support 34. References 1. ABSTRACT AU: Please provide an abstract 2. INTRODUCTION The infusion of autologous hematopoietic stem cells allows the administration of higher than normal doses of marrow toxic chemotherapeutic agents. Further escalation of drug doses with stem cell support is ultimately limited by non-hematopoietic toxicities, primarily to the mucous membranes, lungs and liver. The source of stem cells for support following the administration of high-dose chemotherapy (HDC) was originally from bone marrow (BM) which essentially limited this technology to transplant referral centers. However, the emergence of peripheral blood stem cells (PBSC) over the past decade, as the preferred source of hematopoietic stem cells, has made HDC with stem cell support widely available. Peripheral

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

[Frontiers in Bioscience 4, e???-???, April 7, 1999]
1
AUTOLOGOUS PERIPHERAL BLOOD STEM CELL TRANSPLANTS IN COMMUNITY CANCER CENTERS
C. D. Buckner, C. H. Weaver, L. S. Schwartzberg, R. Birch, B. Zhen and W. West
Response Oncology, Inc., 600 Broadway, Suite 112, , Seattle, Washington
TABLE OF CONTENTS
1. Abstract2. Introduction3. Mobilization and Harvesting of PBSC4. Mobilization of PBSC with G-CSF Alone5. Mobilization of PBSC with Chemotherapy and a Growth Factor6. Mobilization of PBSC with cyclophosphamide, etoposide (CE) and G-CSF7. Evaluation of 2 versus 4 g/m2 of Cyclophosphamide in the CE Regimen8. Comparison of CE to CEP for Mobilization of PBSC9. Evaluation of Cyclophosphamide, Paclitaxel and G-CSF for Mobilization of PBSC10. Evaluation of Cyclophosphamide, Docetaxel and G-CSF for Mobilization of PBSC11. Patients who have Low CD34+ Cell Yields with First Attempts12. Conclusions Concerning Studies of PBSC Mobilization13. Current Status of Purging of BM or PBSC14. Purging of Grafts in Patients with Non-Hodgkin’s Lymphoma15. Purging of Grafts in Patients with Multiple Myeloma16. Purging of Grafts in Patients with Breast Cancer17. Conclusions Concerning Purging of PBSC18. Neutrophil and Platelet Recovery Following Infusion of PBSC19. Effects of Infusion of PBSC with a Low CD34+ Cell Dose21. Treatment Related Morbidity22. Outcomes of Clinical Trials of Outpatient HDC with PBSC Support23. Results of HDC in Patients with Breast Cancer
23.1. Patients with Metastatic Breast Cancer24. Patients with Stage II-III Breast Cancer with ≥10+ Nodes25. Patients with Stage II-III Breast Cancer with 5-9+Nodes26. Conclusions Concerning Adjuvant Therapy for Patients with Breast Cancer27. Results of HDC in Patients with Malignant Lymphoma
27.1. Patients with Hodgkin’s Disease28. Patients with Low Grade NHL29. Patients with Intermediate and High-Grade NHL31. Results of HDC in Patients with Multiple Myeloma32. Results of HDC in Patients with Ovarian Cancer33. What is the Future of HDC with PBSC Support
33.1. Use of PBSC will Expand for Indicated Therapy and in the Evaluation of New Therapies33.2. Immune Therapies will be Evaluated after HDC with PBSC Support
34. References
1. ABSTRACT
AU: Please provide an abstract
2. INTRODUCTION
The infusion of autologous hematopoietic stemcells allows the administration of higher than normal dosesof marrow toxic chemotherapeutic agents. Furtherescalation of drug doses with stem cell support is ultimatelylimited by non-hematopoietic toxicities, primarily to themucous membranes, lungs and liver. The source of stemcells for support following the administration of high-dosechemotherapy (HDC) was originally from bone marrow(BM) which essentially limited this technology totransplant referral centers. However, the emergence ofperipheral blood stem cells (PBSC) over the past decade, asthe preferred source of hematopoietic stem cells, has madeHDC with stem cell support widely available. Peripheral

Autologous peripheral blood stem cell transplantation
2
Table 1. Randomized trials demonstrating superiority of high dose chemotherapy with hematopoietic stem cell support compared to conventional chemotherapy
Event-Free SurvivalDisease Phase Years HDC CC Reference
Hodgkin’s Relapse 3 53% 10% 3NHL First Response 4.5 76% 49% 4NHL First Relapse 5 46% 12% 6NHL First Remission 5 59% 39% 5Myeloma Early Phase 5 28% 10% 9AML First Remission 5 48% 30% 9Breast Cancer Metastatic 2 42%* 4%* 7
*= overall survival; Ref. = reference; HDC = high dose chemotherapy; CC = conventional chemotherapy; NHL = non-Hodgkin'slymphoma; AML = acute myeloid leukemia
blood stem cells can be collected following theadministration of chemotherapy and a growth factor or agrowth factor alone in an outpatient or blood bank settingby apheresis(1) and cryopreservation technology isrelatively simple and widely available.(2)
Although there is controversy about the relativemerits of HDC with PBSC support compared to lower-dosechemotherapy treatments with or without the administrationof growth factors most published randomized trials haveshown superiority for HDC. Selected randomizedprospective clinical trials, summarized in table 1, havedemonstrated better event-free (EFS) or overall survival(OS) following HDC with stem cell support compared toconventional dose therapy for patients with: Hodgkin’sdisease who have relapsed with or without resistantdisease(3), aggressive non-Hodgkin’s lymphoma (NHL) asinitial therapy(4), aggressive NHL as consolidation in firstcomplete remission (CR)(5), NHL with responding diseasewho have relapsed after achieving a remission(6), newlydiagnosed metastatic breast cancer (7), newly diagnosedmultiple myeloma(8) acute myeloid leukemia (AML) infirst remission.(9) No randomized trial has shown HDCwith stem cell support to be inferior to conventional dosechemotherapy but some studies have shown equivalency ordifferences in favor of HDC that were not statisticallysignificant, possibly due to small numbers of patientsevaluated.(10,11)
Over the past two decades numerous phase IIstudies have evaluated HDC supported by autologoushematopoietic stem cells in a variety of chemosensitivemalignant diseases including malignant lymphoma, AML,chronic myeloid leukemia, multiple myeloma, breastcancer, ovarian cancer, neuroblastoma, Ewing’s sarcoma,germ cell tumors, brain tumors and lung cancer. Review ofresults of autologous transplants for all these diseases isbeyond the scope of this review but have been reviewedelsewhere.(12-14)
The purpose of this manuscript is to present theresults of clinical trials of HDC with PBSC supportperformed in community cancer centers under thesupervision of practicing oncologists. Diseases treated arebreast cancer, malignant lymphoma, multiple myeloma and
ovarian cancer where oncologists participating in thesestudies believe that HDC with PBSC support is “standardof care”. Data presented here were derived from protocolsdeveloped since 1989 by the Clinical Trials Division ofResponse Oncology Inc.(ROI) involving over 4,000patients treated with HDC and PBSC support.Approximately 1200 patients/year are evaluated and 650are treated with HDC and PBSC support in 50 centers by400 medical oncologists in the ROI network. The list ofparticipating centers is included at the end of thismanuscript. This is predominantly an outpatient programwith all drugs being administered, PBSC collected andinfused in an outpatient department with patients beingadmitted only for clearly defined complications requiringhospitalization.
3. MOBILIZATION AND HARVESTING OF PBSC
Initially, PBSC were harvested afterchemotherapy alone, usually high doses ofcyclophosphamide (Cy) and infused after HDC.(15,16)Following the availability of recombinant growth factors,granulocyte-colony stimulating factor (G-CSF) orgranulocyte macrophage-colony stimulating factor (GM-CSF) were added to high doses of Cy with or without otherdrugs such as etoposide and cisplatin.(15) With the use ofchemotherapy and G-CSF or GM-CSF adequate quantitiesof PBSC, as measured by the number of CD34+ cells, canbe collected in 1-3 aphereses in the majority ofpatients.(17-19) The administration of G-CSF or GM-CSFalone, without chemotherapy, for mobilization of PBSC isassociated with lower, but generally adequate, CD34+ cellyields, has lower morbidity, no hospitalization andapheresis can be scheduled for weekday performancemaking this the method of choice for blood banks.(1,20,21)
Several studies, summarized in table 2, havebeen carried out to define yields of PBSC followingdifferent regimens. In all these studies CD34+ cell numberwas used as a measure of hematopoietic PBSC content ofthe apheresis product.(22) In these studies the minimumCD34+ cell dose necessary for proceeding to HDC wasassumed to be ≥2.5 x 106/kg and the optimal dose was ≥5.0x 106 CD34+ cells/kg.(23,24,20,25,1,22) For comparisonsbetween regimens, effectiveness of a mobilization regimen

Autologous peripheral blood stem cell transplantation
2
Table 2. Evaluation of regimens for mobilization of PBSCNumber ofPatients
Regimen Diagnosis CD34+ Cells/kg/ Apheresis(range)
Reference
31 G-CSF 10 µg/kg Breast Cancer 0.70 (0.1-4.4) 2132 G-CSF 30 µg/kg Breast Cancer 1.20 (0.1-6.8) 21497 CE/G-CSF Varied 5.84 (0.002-56.31) 17162 C (2 g/m2) E/G-CSF Breast Cancer (II-III) 9.90 (0.4-100.3) 26156 C (4 g/m2) E/G-CSF Breast Cancer (II-III) 11.10 (0.01-158.1) 2641 CE/G-CSF Lymphoma 8.16 (0.02-42.16) 1940 CEP/G-CSF Lymphoma 4.62 (0.01-21.02) 1944 CE/G-CSF Multiple Myeloma 18.72 (0.64-65.91) 52141 C paclitaxel/G-CSF Breast Cancer (IV) 3.66 (0.06-25.8) 1866 C docetaxel/G-CSF Breast Cancer (IV) 7.12 (0.01-47.07) 27
G-CSF = granulocyte-colony stimulating factor; C = cyclophosphamide, E = etoposide, P = cisplatin, II, III, IV = clinical stageof breast cancer
was evaluated by determining the number of CD34+ cellsharvested/kg/apheresis.(20)
4. MOBILIZATION OF PBSC WITH G-CSF ALONE
Peripheral blood stem cells can be mobilized with growthfactors alone without chemotherapy.(20) The optimalgrowth factor or combination of growth factors formobilization of PBSC has yet to be defined. However, themost commonly used growth factor for mobilization ofPBSC is G-CSF administered in doses of 5-10 µg/kg withinitiation of collections on day 5.(20) In order to optimizeusage different doses and schedules of G-CSF are stillbeing evaluated.(21)
The effects of escalating doses of G-CSF onyields of CD34+ stem cells were evaluated in 90 patientswith metastatic breast cancer and the results aresummarized in table 2.(21) Fifty-five patients wererandomized to receive G-CSF 10, 20, 30 or 40 µg/kg/daywith more CD34+ cells/kg/apheresis being harvested afterthe 3 highest dose levels. Thirty-five additional patientswere randomized to receive 10 or 30 µg/kg of G-CSF. Themedian number of CD34+ cells collected after 10 µg/kg(n=31) was 0.7 x 106/kg/apheresis (range 0.1-4.4)compared to 1.2 (range 0.1-6.8) after 30 µg/kg (n=32)(p=0.04). Among patients randomized to 10 versus 30µg/kg, more achieved ≥5.0 x 106 CD34+ cells/kg and lessaphereses were required to achieve ≥2.5 x 106 CD34+cells/kg after the higher dose (p=0.04). In multivariateanalyses patients receiving 10 µg/kg (n=31) had loweryields of CD34+ cells (p=0.026) and had a 3.3 fold increasein the probability of not achieving ≥5.0 x 106 CD34+cells/kg as compared to patients receiving 20-40 µg/kg(n=59). Patients who had received radiation had a 2.9 foldprobability of not achieving ≥2.5 x 106 CD34+ cells/kg.These data suggested that, in patients with good marrowreserves, doses of G-CSF above 10 µg/kg/day mobilizedmore CD34+ cells with fewer aphereses and may be usefulwhen high numbers of CD34+ cells are desired. However,as a generality, increasing the dose of G-CSF did notimprove CD34+ yields in heavily pretreated patients. Asshown in table 2 the highest dose of G-CSF mobilizedfewer CD34+cells/kg/apheresis than any of thechemotherapy regimens evaluated.
5. MOBILIZATION OF PBSC WITHCHEMOTHERAPY AND A GROWTH FACTOR
A variety of chemotherapy and growth factorregimens for mobilization of PBSC have been evaluatedand results of studies carried out in an outpatient setting byphysicians affiliated with the Clinical Trials Division ofROI are reviewed below and in table 2.
6. MOBILIZATION OF PBSC WITHCYCLOPHOSPHAMIDE, ETOPOSIDE (CE) AND G-CSF
Four hundred ninety seven patients with a varietyof malignant diseases received Cy (4 g/m2), etoposide (600mg/m2) and G-CSF (6 µg/kg/day) for mobilization andcollection of a target CD34+ cell harvest ≥2.5 x106/kg.(17) Results of this study are summarized in table2. A median of 14.71 x 106 CD34+ cells/kg (range, 0.08-137.55) was harvested with a median of 2 (range, 1-11)aphereses. Ninety-one percent of patients yielded ≥2.5 x106 CD34+ cells/kg. Patients with stage II-III breastcancer, with pre-treatment platelet counts ≥150 x 109/L andpatients who had received ≤1 prior chemotherapy regimenhad improved CD34+ cell yields. However, the majority ofpatients with adverse risk factors yielded ≥2.5 x 106CD34+ cells/kg. These observations confirm previousreports that the intensity of prior therapy adversely affectsthe quantity of CD34+ cells harvested. Pre- and post-treatment variables did not predict with any certainty thesmall fraction of patients who failed to yield ≥2.5 x 106CD34+ cells/kg with multiple aphereses.
7. EVALUATION OF 2 VERSUS 4 G/M2 OFCYCLOPHOSPHAMIDE IN THE CE REGIMEN
The purpose of this study was to develop a lesstoxic outpatient chemotherapy regimen for mobilizingPBSC in patients with non-metastatic breast cancer and theresults of this study are summarized in table 2(26). Threehundred and eighteen patients with newly diagnosed stageII-III breast cancer who had received conventional-doseadjuvant chemotherapy were randomized to receiveintermediate-dose Cy (2 g/m2), etoposide (600 mg/m2) andG-CSF 6 µg/kg/day (ID-Cy, N=162) or high-dose Cy (4
Autologous peripheral blood stem cell transplantation
2
g/m2) and the same doses of etoposide and G-CSF (HD-Cy, N=156) followed by the collection of PBSC. Patientswho received the highest dose of Cy also received mesnafor prevention of hemorrhagic cystitis. Three hundredseventeen of 318 patients had apheresis performed. Themedian numbers of CD34+ cells collected in a median of 2aphereses following ID-Cy and HD-Cy were 19.9 and 22.2x 106/kg, respectively (p=0.04). The fractions of patientsachieving CD34+ cell harvests ≥2.5 or ≥5.0 x 106/kg werenot different between the two regimens. More patientsreceiving HD-Cy had grade 3-4 nausea (p=0.001), vomiting(p=0.03) and mucositis (p=0.04). The fractions of patientshaving a neutrophil nadir <0.5 x 109/L following ID-Cyand HD-Cy were .83 and .95, respectively (p=<0.001). Thefractions of patients having a platelet nadir <25 x 109/Lfollowing ID-Cy and HD-Cy were .13 and .51, respectively(p=<0.001). More patients in the HD-Cy group receivedplatelet (p<0.001) and red blood cell (p<0.001) transfusionsand were admitted to the hospital more frequently (p=0.03)than patients receiving ID-Cy. It was concluded that aregimen of Cy 2 g/m2 with etoposide and G-CSF withoutmesna was effective for mobilization of PBSC with lowmorbidity and resource utilization in patients with limitedprior chemotherapy exposure.
8. COMPARISON OF CE TO CEP FORMOBILIZATION OF PBSC
The purpose of this study was to evaluate theeffects of dose intensity on CD34+ cell yieds. Eighty-onepatients with malignant lymphoma were randomized toreceive Cy (4 g/m2), etoposide (600 mg/m2) and G-CSF (6µg/kg/day) (CE, N=41) or the same drugs with cisplatin(105 mg/m2) (CEP, N=40) followed by collection ofPBSC.(19) Results of this study are summarized in table 2.Seventy-eight of 81 patients (96%) had apheresisperformed and 70 (86%) received HDC with PBSCsupport. The median number of CD34+ cells collectedfollowing CE was 19.77 compared to 9.39 x 106/kgfollowing CEP (p=0.09). More patients receiving CEP hadgrade 3-4 gastrointestinal (p=0.03) and neurologictoxicities (p=0.05), had significant delays in recovery ofneutrophils (p=0.0001) and platelets (p=0.009) andreceived more red blood cell (p=0.03) and platelet (p=0.08)transfusions than patients receiving CE. There were nosignificant differences in treatment-related deaths, relapseor EFS between patients receiving CE or CEP when all 81patients or the 70 patients receiving HDC were evaluated.It was concluded that the addition of cisplatin to CE did notimprove CD34+ cell yields, was associated with highermorbidity and resource utilization and was not associatedwith improvement in outcomes.
9. EVALUATION OF CYCLOPHOSPHAMIDE,PACLITAXEL AND G-CSF FOR MOBILIZATIONOF PBSC
Paclitaxel is an effective agent for the treatmentof patients with breast and ovarian cancer. The purpose ofthis study was to determine if paclitaxel could be utilizedfor mobilization of PBSC. One hundred forty-one patientswith metastatic breast (n=115) or advanced ovarian cancer
(n=26) received paclitaxel 170 mg/m2 and Cy, 2 g/m2(n=42) or paclitaxel 200 mg/m2 and Cy, 3 g/m2 (n=99) andG-CSF (6 µg/kg/day) followed by collection of PBSC byapheresis.(18) Results of this study are summarized intable 2. The 2 dose levels of paclitaxel and Cy tested werewell tolerated. The median yield of CD34+ cells from allpatients was 6.53 x 106/kg (range, 0.11-51.76) collectedwith a median of 2 aphereses (range, 1-8). A target CD34+cell yield ≥2.5 x 106/kg was achieved in 85% of patients.The mean daily collection of CD34+ cells was 5.46 x106/kg for patients receiving 200 mg/m2 of paclitaxel and3 g/m2 of Cy as compared to 2.77 for patients receiving thelower doses (p=0.0005). Increasing the dose of paclitaxeland Cy did not significantly increase the fraction of patientsachieving a target CD34+ cell harvest ≥2.5 x 106/kg (87%vs. 81%, p=0.367) but did increase the fraction achieving≥5.0 x 106 CD34+ cells/kg (73% vs. 45%, p=0.002). Themean daily collection of CD34+ cells for patients who hadreceived only 1 prior chemotherapy regimen was 6.59 x106/kg as compared to 3.47 for patients who had receivedmore than 1 prior chemotherapy regimen (p<0.0001). Priorradiation therapy (p=0.003) and patient performance status(p=0.047) were adverse risk factors for achieving a targetCD34+ cell yield ≥2.5 x 106/kg.
It was concluded from this study that paclitaxelcould be incorporated into a strategy of treatment ofpatients with breast cancer which involved induction,mobilization of PBSC and HDC.
10. EVALUATION OF CYCLOPHOSPHAMIDE,DOCETAXEL AND G-CSF FOR MOBILIZATIONOF PBSC
Docataxel is an active agent for the treatment ofpatients with breast cancer. The purpose of this study wasto develop a regimen of docetaxel, Cy and G-CSF formobilization of PBSC in patients with metastatic breastcancer (N=66). A phase I trial of Cy 2, 3 or 4 g/m2 withdocetaxel 100 mg/m2, in consecutive cohorts of 4 patientseach, did not reveal any dose-limiting toxicities andsubsequent patients were randomized to receive 3 or 4g/m2 of Cy.(27) Patients receiving Cy 4 g/m2 alsoreceived mesna for protection against hemorrhagic cystitis.Results of this study are summarized in table 2. Themedian yield of CD34+ cells from all patients was 11.06 x106/kg (range, 0.03-84.77) from a median of 2 aphereses(range, 1-7); 6.52 x 106 CD34+ cells/kg/apheresis (range,0.01-52.07). Target CD34+ cell harvests ≥2.5 and ≥5.0 x106/kg were achieved in 89% and 79%, respectively.There were no statistically significant differences in CD34+cell yields or target CD34+ cell harvests following 3 or 4g/m2 of Cy. Patients with only one prior chemotherapyregimen yielded a median of 12.82 x 106 CD34+cells/kg/apheresis compared to 5.85 for those receiving ≥2regimens (p=0.03). It was concluded that the combinationof docetaxel, 100 mg/m2 and Cy 3 g/m2 without mesnacould be administered with acceptable toxicity withcollection of adequate quantities of PBSC from themajority of patients with metastatic breast cancer.

Autologous peripheral blood stem cell transplantation
3
11. PATIENTS WHO HAVE LOW CD34+ CELLYIELDS WITH FIRST ATTEMPTS
A small but significant fraction of patients havelow CD34+ cell yields with initial mobilization attemptsand management of such patients is problematic. Twohundred fifty of 2,157 patients (12%) with breast cancer,lymphoma and multiple myeloma failed to harvest ≥2.5 x106 CD34+ cells/kg in a median of 4 aphereses (range, 1-11).(28) Repeat mobilization attempts were made withchemotherapy and G-CSF (N=61) or G-CSF alone (N=58)in patients who failed initial mobilization withchemotherapy and G-CSF (N=92) or G-CSF alone (N=27).A median of 0.27 x 106 CD34+ cells/kg/apheresis wascollected following second mobilization compared to 0.16with initial harvests (p=0.0001). Forty-eight percentachieved a target CD34+ cell harvest ≥2.5 x 106/kg whencollections from first and second mobilizations werecombined. Fifteen of 17 patients (88%) with ≥1.5 x 106CD34+ cells/kg harvested following first mobilization had≥2.5 x 106 CD34+ cells/kg collected when first and secondharvests were combined compared to 42 of 102 (41%)achieving <1.5 x 106 CD34+ cells/kg with first PBSCharvests (p=0.0001). Second mobilizations withchemotherapy and G-CSF or G-CSF alone resulted insimilar CD34+ cell yields. Toxicities of secondmobilizations were comparable to first mobilizations. Itwas concluded that second mobilization attempts inpatients who fail to achieve ≥2.5 x 106 CD34+ cells/kg oninitial mobilization were successful in 48% of patients. G-CSF alone was as effective as chemotherapy plus G-CSF inmobilizing CD34+ cells and was associated with lessmorbidity. The data also suggested that doses of G-CSF≥10 µg/kg/day were more effective than 10 µg/kg/day.
12. CONCLUSIONS CONCERNING STUDIES OFPBSC MOBILIZATION
It is evident that PBSC can be harvested after theadministration of a growth factor or a combination ofgrowth factors without chemotherapy(20,29,30,21) orfollowing the administration of a variety ofchemotherapeutic agents and a growthfactor.(31,32,24,33,1,22,17,18) More CD34+ cells can becollected following chemotherapy and a growth factor thanfollowing a growth factor alone. However, the potentialadvantages to administering a growth factor alone includeless toxicity and ease of scheduling of apheresis. It is notclear that any chemotherapy regimen is more optimal thananother and at the present time it would seem prudent toutilize chemotherapeutic agents for mobilization of PBSCthat are appropriate for the disease being treated.
Approximately 5% of patients will fail to achieveadequate doses of CD34+ cells despite second and thirdmobilization regimens. These patients cannot be identifiedwith any certainty prior to initial mobilization. Suchpatients would be ideal candidates for future ex-vivo cellexpansion studies or for evaluation of new growth factors.However, at the present time ex-vivo cell expansion is notfeasible in patients who do not mobilize adequate quantities
of CD34+ cells. Whether or not newer growth factors willbe effective in this patient population will be of interest.
13. CURRENT STATUS OF PURGING OF BM ORPBSC
The success of HDC with PBSC support islimited mainly by disease recurrence, which ranges from30-90%. Relapses following HDC are predominantly dueto the failure to eradicate residual disease in the patient butare possibly contributed to by infusion of malignant cellscontained in the graft.(34) The current status of purging ofautologous grafts has recently been reviewed.(35,36)
14. PURGING OF GRAFTS IN PATIENTS WITHNON-HODGKIN’S LYMPHOMA
There have been no randomized trials comparingunpurged to purged grafts in patients with NHL. However,recently the European Bone Marrow Transplant Grouppublished an analysis of 448 patients with NHL receivingpurged or unpurged BM following several HD treatmentregimens.(37) Purging was performed utilizing a variety ofnegative techniques, i.e., monoclonal antibodies withcomplement, immunomagnetic beads or cytotoxic drugs toremove putative tumor cells from the graft. These analysesdemonstrated no decrease in relapses or improvement inOS or EFS for patients receiving purged BM. It can beconcluded from these analyses that the infusion of occulttumor cells either had no impact on outcomes of patientswith NHL or that the purging techniques used wereineffective.
Gribben, et al reported that patients with low-grade NHL who had BM purged with monoclonalantibodies and complement to BCL-2 negativity prior toautologous BM transplantation had a 20% probability ofrelapse as compared to >85% for patients who did not haveBM purged to BCL-2 negativity.(38) All patients hadPCR-detectable lymphoma cells in the BM before purgingwas performed. These observations could be interpreted asdirect evidence that the infusion of BCL-2 positive BMcaused relapses. However, it is just as likely that patientswho are purged to BCL-2 negativity have less endogenoustumor which may be more sensitive to chemo-radiotherapycompared to patients whose BM were not purged to BCL-2negativity.
In summary, current data would suggest that thebenefit of purging of BM or PBSC in patients with low-grade or any other histologic types of NHL has not yet beendocumented.
15. PURGING OF GRAFTS IN PATIENTS WITHMULTIPLE MYELOMA
Most studies of autologous transplantation forpatients with multiple myeloma have utilized unpurged BMor PBSC,(39,40) including the only randomized trialdemonstrating superiority of autologous transplantation

Autologous peripheral blood stem cell transplantation
4
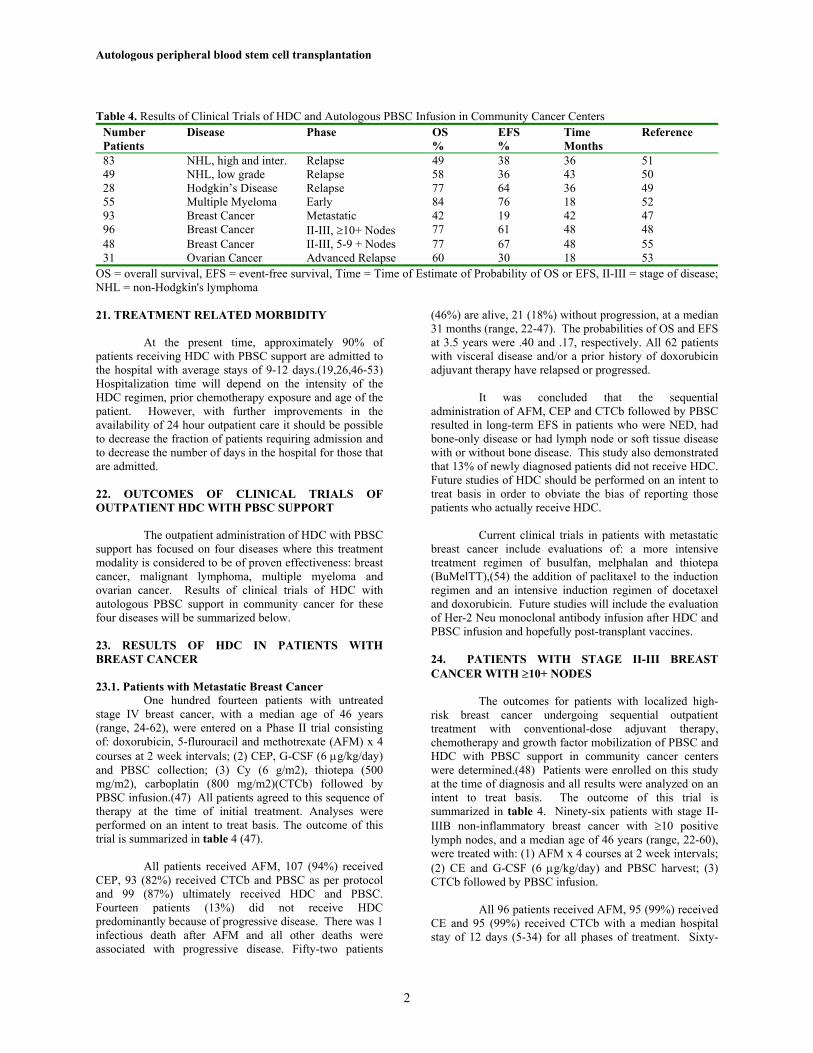
Figure 1. Stage II-III Breast Carcinoma after High-DoseChemotherapy: Probability of Relapse (P=0.826). Theprobabilities of relapse for patients with stage II-III breastcancer infused with ICC positive or negative PBSC. Tickmarks represent the date of last contact for patientssurviving without relapse.
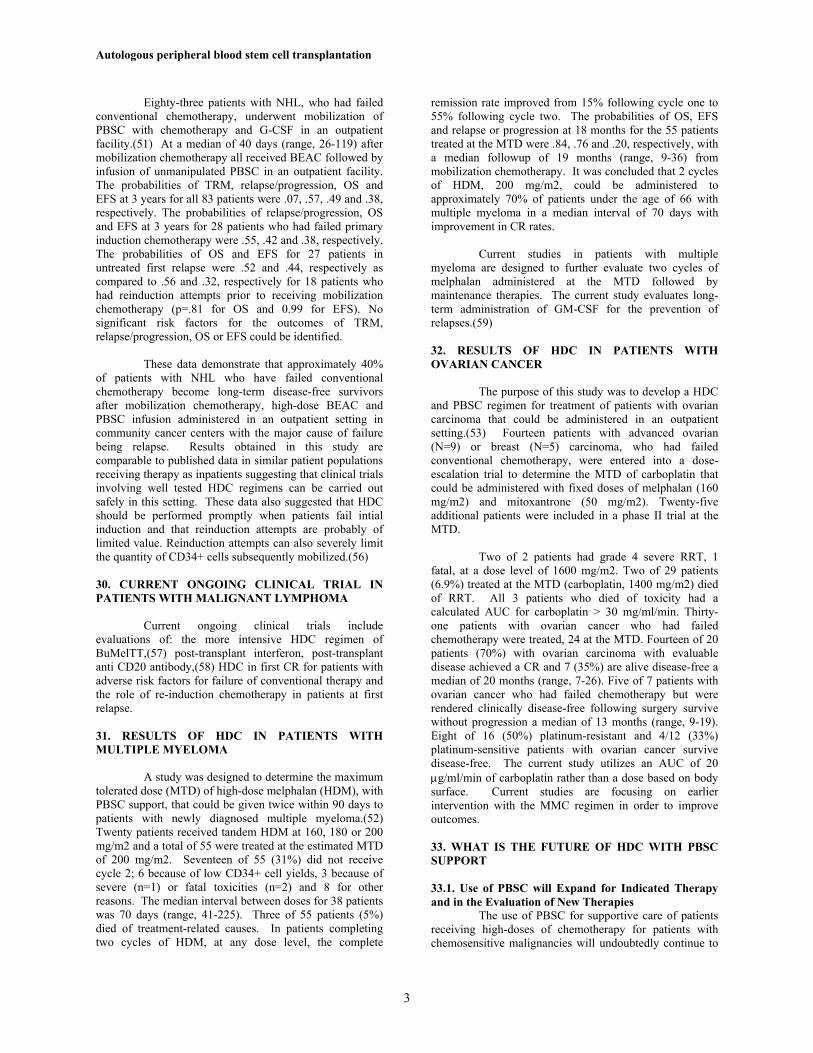
Figure 2. Patients with Metastatic or Adjuvant BreastCancer Treated with CTCb and Infused >5.0 x 106 CD34+Cells. Neutrophil and platelet recovery following infusionof ≥5.0 x 106 CD34+ cells/kg in patients with breast cancerreceiving high-dose cyclophosphamide, thiotepa andcarboplatin.
compared to conventional therapy.(8) There have beenattempts to purge BM with anti-B cell monoclonalantibodies and complement(41) or more recently withCD34+ selection using the Ceprate device.(42) A currentrandomized trial of purging of PBSC in patients withmultiple myeloma with the Ceprate columns has beencompleted but not reported in detail. Unless a survivalbenefit is demonstrated in this study this relativelyexpensive technology should not be used routinely inpatients with multiple myeloma receiving HDC with PBSCsupport.(36)
16. PURGING OF GRAFTS IN PATIENTS WITHBREAST CANCER
The role of infused tumor cells in causing relapseafter HDC for breast cancer is unresolved. In order toaddress this issue an evaluation of occult tumorcontamination of PBSC, using a sensitive
immunocytochemistry (ICC) test in conjunction with BISLaboratories, was carried out.(43) The purpose of thisstudy was to evaluate the frequency of detecting occulttumor cells in PBSC harvests and to determine the impactof infusing such cells on relapses after HDC. Peripheralblood stem cell harvests from 223 patients with breastcancer were examined by ICC and infused after HDCwithout consideration of test results. Fifty-three of 581harvests (9%); 8% from stage II-III and 10% from stage IVpatients, were positive by ICC (p=0.68). Forty-one of 223patients (18%), 17/122 (14%) with stage II-III and 24/101(24%) with stage IV disease, had positive harvests(p=0.06). Eleven % of patients who had 1-2 harvests testedwere positive as compared to 32% of patients who had ≥3PBSC harvests tested (p<0.001). These data suggest thatthe number of patients with positive ICC tests can beincreased by increasing the number of cells tested orincreasing the number of apheresis products tested.Implicit in this observation is the likelihood that all patientswill have positive tests if enough PBSC products areanalyzed.
The probabilities of relapse at 24 months for 97patients with stage II-III disease infused with ICC negativeand the 17 with ICC positive PBSC were .19 and .13,respectively (p=0.48). Probabilities of relapse for the 2groups of patients, updated to April 1, 1998, are shown infigure 1. The probabilities of relapse at 18 months forpatients achieving a CR or a CR in non-bone sites andimprovement in bone lesions were .55 for the ICC negativegroup (n=30) and .45 for the ICC positive group (n=11)(p=0.60). It was concluded that occult tumor cells weredetected by ICC in PBSC harvests from a relatively smallfraction of women with breast cancer, but were notassociated with a significant increase in the probability ofearly relapse or progression when infused after HDC.
Positive selection of BM or PBSC, using theCeprate device, has been utilized to purge autologous graftsin patients with breast cancer with a 1-2 log reduction oftumor cells.(44) A randomized trial of unselected versusCD34+ cell selected BM was performed in patients withmetastatic breast cancer receiving HDC showing a 31%EFS for both groups.(44) Thus, there was no effect onsurvival of CD34+cell selection in patients with metastaticbreast cancer.
17. CONCLUSIONS CONCERNING PURGING OFPBSC
Despite intense efforts in the laboratory todevelop techniques to remove tumor cells from BM orPBSC grafts there have been few randomized clinical trialsperformed and the only one reported in a definitive formshowed no effect on EFS.(44) There are several possiblereasons for this but the major one is the large number ofpatients that are required to document the efficacy ofpurging, predominantly due to the high relapse rate fromendogenous tumor in most clinical situations. As long astreatment failures occur because of failure to eradicatedisease in the patient, purging studies will be difficult toperform. However, until data is available documenting a

Autologous peripheral blood stem cell transplantation
5
Table 3. Treatment-Related Mortality in the First One hundred Days Following HDC and PBSC Support in Community CancerCenters
Number Regimen Disease Phase TRM Reference1,000 Varied Varied Varied 3.4% 46208 BEAC Malignant Lymphoma Relapsed 3.6-10% 49,50,19,5155 Mel. x 2 Multiple Myeloma Newly diagnosed 5% 5293 CTCb Breast Cancer Metastatic, Early 0% 4795 CTCb Breast Cancer Stage II-III 0% 48315 CTCb Breast Cancer Stage II-III 0.3% 2629 MMC Ovarian Cancer Relapsed 6.9% 53
BEAC = carmustine, etoposide, cytarabine and cyclophosphamide; Mel = melphalan, BuMelTT = busulfan, melphalan andthiotepa, CTCb = cyclophosphamide, thiotepa and carboplatin, MMC = melphalan, mitoxantrone and carboplatin; TRM =treatment-related mortality
survival benefit of purging the most rational approach is tonot purge the graft.
18. NEUTROPHIL AND PLATELET RECOVERYFOLLOWING INFUSION OF PBSC
Autologous BM infusion after HDC resulted in 3-4 weeks of pancytopenia with a small but significantfraction of patients, depending on the quality of themarrow, having prolonged pancytopenia requiringextensive transfusion support and antibiotic therapy.(45)With the use of PBSC larger quantities of stem cells can becollected resulting in more rapid recovery of neutrophilsand platelets with virtually all patients recovering bloodcounts within 2 weeks. The single most powerful mediatorof both platelet and neutrophil recovery is the CD34+ cellcontent of the PBSC product.(22) An evaluation of over600 patients has shown that the optimal cell dose for rapidand complete engraftment of all patients is ≥5 x 106CD34+ cells/kg.(22) Patients will spend <7 days withneutrophils <0.5 and platelets <20 x 109/L followinginfusion of ≥5.0 x 106 CD34+ cells/kg. figure 2 shows themean neutrophil and platelet counts following high-doseCTCb and PBSC infusion of ≥5.0 x 106 CD34+ cells/kg inpatients with breast cancer. This short period ofpancytopenia has significantly lowered the cost ofadminstering HDC by allowing much of the treatment totake place in an outpatient setting. Neutropenia is nolonger a reason to admit patients to the hospital if patientsare carefully monitored in an outpatient setting and receiveprophylactic antibiotics and platelet transfusions.
19. EFFECTS OF INFUSION OF PBSC WITH A LOWCD34+ CELL DOSE
There are clinical situations where infusion ofPBSC with relatively low CD34+ cell numbers is areasonable therapeutic choice. In order to evaluateoutcomes in this situation, engraftment kinetics after HDCwere determined in patients receiving autologous PBSCinfusions with a low CD34+ cell content.(28) Forty-eightpatients were infused with <2.5x 106 CD34+ cells/kg; 36because of poor harvests and 12 because they electivelyreceived only a fraction of their harvested cells. A medianof 2.l2 x 106 CD34+ cells/kg (range, 1.17-2.48) wereinfused following 1 of 7 different HDC regimens. All
patients achieved absolute neutrophil counts ≥0.5 x 109/Lat a median of day 11 (range, 9-16). Forty-seven patientsachieved platelet counts ≥20 x 109/L at a median of day 14(range, 8-250). Nine of 47 (19%) had platelet recoveryafter day 21, 4/47 (9%) after day 100 and one died on day240 without platelet recovery. Twenty-six patients (54%)died of progressive disease in 51-762 days; 22 (46%) arealive at a median of 450 days (range, 94-1844), 17 (35%)of whom are surviving disease-free at a median of 494 days(range, 55-1263). No patient died as a direct consequenceof low blood cell counts. These data demonstrate thatPBSC products containing 1.17-2.48 x 106 CD34+ cells/kgresulted in relatively prompt neutrophil recovery in allpatients but approximately 10% had delayed plateletrecovery.
The results of infusing PBSC with a low CD34+cell content are remarkably similar to results of autologousBM transplantation(45) and suggest that HDC supported bya relatively low CD34+ cell dose is a reasonable option forsome patients if warranted by the clinical situation.
Treatment Related Mortality and Morbidity ofHigh-Dose Chemotherapy and PBSC SupportAdministered in an Outpatient Setting in CommunityCancer Centers.
20. TREATMENT RELATED MORTALITY
Several published HDC regimens withhematopoietic stem cell support have become widely used.Treatment related mortality (TRM) following commonlyused HDC regimens administered in community cancercenters was determined and the results are summarized intable 3 (46). This retrospective study evaluated 1,000consecutive patients with AML, NHL, Hodgkin’s disease,multiple myeloma, sarcoma, ovarian cancer, or breastcancer who received 1 of 5 published HDC regimensfollowed by PBSC infusion over a 5 year period. Fifty-nine patients (5.9%) died within 100 days of PBSCinfusion. Twenty-five patients (2.5%) died predominantlyof causes related to disease progression. Thirty-fourpatients (3.4%) died of TRM, 15 (1.5%) from infection and19 (1.9%) from regimen related toxicities. In a logisticmodel, increasing age (p=0.001) and lower numbers ofCD34+ cells infused (p=0.003) were associated with an
Autologous peripheral blood stem cell transplantation
2
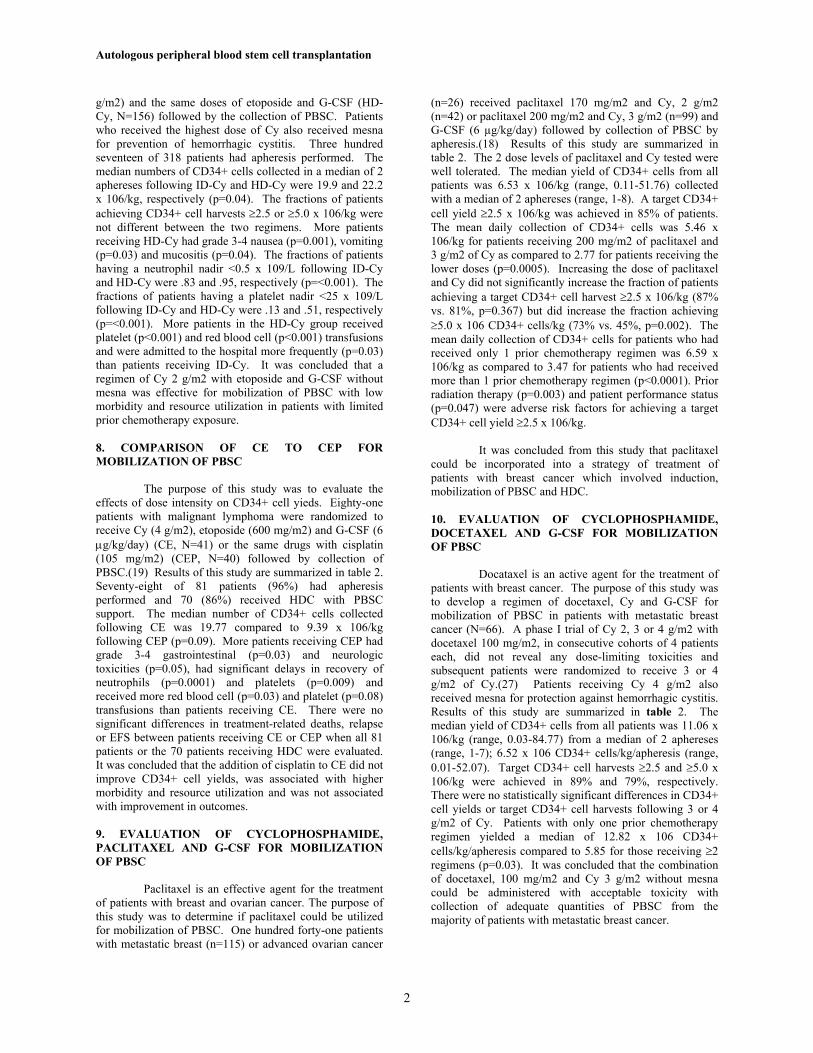
Table 4. Results of Clinical Trials of HDC and Autologous PBSC Infusion in Community Cancer CentersNumberPatients
Disease Phase OS%
EFS%
TimeMonths
Reference
83 NHL, high and inter. Relapse 49 38 36 5149 NHL, low grade Relapse 58 36 43 5028 Hodgkin’s Disease Relapse 77 64 36 4955 Multiple Myeloma Early 84 76 18 5293 Breast Cancer Metastatic 42 19 42 4796 Breast Cancer II-III, ≥10+ Nodes 77 61 48 4848 Breast Cancer II-III, 5-9 + Nodes 77 67 48 5531 Ovarian Cancer Advanced Relapse 60 30 18 53
OS = overall survival, EFS = event-free survival, Time = Time of Estimate of Probability of OS or EFS, II-III = stage of disease;NHL = non-Hodgkin's lymphoma
21. TREATMENT RELATED MORBIDITY
At the present time, approximately 90% ofpatients receiving HDC with PBSC support are admitted tothe hospital with average stays of 9-12 days.(19,26,46-53)Hospitalization time will depend on the intensity of theHDC regimen, prior chemotherapy exposure and age of thepatient. However, with further improvements in theavailability of 24 hour outpatient care it should be possibleto decrease the fraction of patients requiring admission andto decrease the number of days in the hospital for those thatare admitted.
22. OUTCOMES OF CLINICAL TRIALS OFOUTPATIENT HDC WITH PBSC SUPPORT
The outpatient administration of HDC with PBSCsupport has focused on four diseases where this treatmentmodality is considered to be of proven effectiveness: breastcancer, malignant lymphoma, multiple myeloma andovarian cancer. Results of clinical trials of HDC withautologous PBSC support in community cancer for thesefour diseases will be summarized below.
23. RESULTS OF HDC IN PATIENTS WITHBREAST CANCER
23.1. Patients with Metastatic Breast CancerOne hundred fourteen patients with untreated
stage IV breast cancer, with a median age of 46 years(range, 24-62), were entered on a Phase II trial consistingof: doxorubicin, 5-flurouracil and methotrexate (AFM) x 4courses at 2 week intervals; (2) CEP, G-CSF (6 µg/kg/day)and PBSC collection; (3) Cy (6 g/m2), thiotepa (500mg/m2), carboplatin (800 mg/m2)(CTCb) followed byPBSC infusion.(47) All patients agreed to this sequence oftherapy at the time of initial treatment. Analyses wereperformed on an intent to treat basis. The outcome of thistrial is summarized in table 4 (47).
All patients received AFM, 107 (94%) receivedCEP, 93 (82%) received CTCb and PBSC as per protocoland 99 (87%) ultimately received HDC and PBSC.Fourteen patients (13%) did not receive HDCpredominantly because of progressive disease. There was 1infectious death after AFM and all other deaths wereassociated with progressive disease. Fifty-two patients
(46%) are alive, 21 (18%) without progression, at a median31 months (range, 22-47). The probabilities of OS and EFSat 3.5 years were .40 and .17, respectively. All 62 patientswith visceral disease and/or a prior history of doxorubicinadjuvant therapy have relapsed or progressed.
It was concluded that the sequentialadministration of AFM, CEP and CTCb followed by PBSCresulted in long-term EFS in patients who were NED, hadbone-only disease or had lymph node or soft tissue diseasewith or without bone disease. This study also demonstratedthat 13% of newly diagnosed patients did not receive HDC.Future studies of HDC should be performed on an intent totreat basis in order to obviate the bias of reporting thosepatients who actually receive HDC.
Current clinical trials in patients with metastaticbreast cancer include evaluations of: a more intensivetreatment regimen of busulfan, melphalan and thiotepa(BuMelTT),(54) the addition of paclitaxel to the inductionregimen and an intensive induction regimen of docetaxeland doxorubicin. Future studies will include the evaluationof Her-2 Neu monoclonal antibody infusion after HDC andPBSC infusion and hopefully post-transplant vaccines.
24. PATIENTS WITH STAGE II-III BREASTCANCER WITH ≥10+ NODES
The outcomes for patients with localized high-risk breast cancer undergoing sequential outpatienttreatment with conventional-dose adjuvant therapy,chemotherapy and growth factor mobilization of PBSC andHDC with PBSC support in community cancer centerswere determined.(48) Patients were enrolled on this studyat the time of diagnosis and all results were analyzed on anintent to treat basis. The outcome of this trial issummarized in table 4. Ninety-six patients with stage II-IIIB non-inflammatory breast cancer with ≥10 positivelymph nodes, and a median age of 46 years (range, 22-60),were treated with: (1) AFM x 4 courses at 2 week intervals;(2) CE and G-CSF (6 µg/kg/day) and PBSC harvest; (3)CTCb followed by PBSC infusion.
All 96 patients received AFM, 95 (99%) receivedCE and 95 (99%) received CTCb with a median hospitalstay of 12 days (5-34) for all phases of treatment. Sixty-

Autologous peripheral blood stem cell transplantation
2
nine patients (72%) are alive, 55 (57%) without relapse at amedian followup of 53 months (range, 37-77). One patient(1%) died of AML and all other deaths were associatedwith recurrent breast cancer. The probabilities of EFS at 4years for patients with or without locally advanced diseasewere .37 and .69, respectively (p=0.004) and .71 and .48,respectively, for patients who were ER/PR+ or ER/PR-,respectively (p=0.016). In multivariate analyses, locallyadvanced disease (RR=2.3, p=0.021) and ER/PR- hormonereceptor status (RR=2.2, p=0.014) were the only adverserisk factors for EFS identified. Patients with 0, 1 or 2 ofthese adverse risk factors had 4 year EFS of .80, .56 and.33, respectively.
25. PATIENTS WITH STAGE II-III BREASTCANCER WITH 5-9+NODES
Forty-three patients with stage II-III disease with5-9+ axillary lymph nodes, with a median age of 44 years(range, 27-60), were enrolled on a study which included (1)standard dose AFM adjuvant therapy (2) CE and G-CSFmobilization of PBSC; (3) high-dose CTCb followed byPBSC infusion.(55) The outcome of this trial issummarized in table 4. All 43 patients received AFM, 42(98%) received CE and 41 (95%) received CTCb. Thirty-two patients (74%) are alive, 28 (65%) without relapse at amedian of 55 months (range, 41-87). Two died (5%) oftreatment-related causes, (subclavian catheter complicationafter CE and late radiation pneumonitis) with 9 other deaths(21%) being associated with recurrent breast cancer. Theprobabilities of OS and EFS at 4 years were .77 and .67,respectively, compared to .82 and .69, respectively, for 72similar patients with ≥10+ axillary nodes receiving thesame sequence of therapy. Thus, patients with 5-9+axillary lymph nodes have a similar risk of failurefollowing HDC and PBSC support as patients with ≥10+axillary lymph nodes.
26. CONCLUSIONS CONCERNING ADJUVANTTHERAPY FOR PATIENTS WITH BREASTCANCER
It was concluded that the sequentialadministration of AFM, CE or CEP and CTCb followed byPBSC in an outpatient community setting was welltolerated in patients with high-risk stage II-III breastcancer. More intensive and/or more novel treatmentstrategies will be required to decrease relapses in patientswho have ER/PR- tumors and/or have locally advanceddisease.
Current studies are evaluating the effects ofpaclitaxel following AFM induction. A randomized trialcomparing BuMelTT to CTCb is also being initiated inpatients with locally advanced breast cancer. Patients withlocally advanced and/or inflammatory breast cancer arealso receiving intensive neoadjuvant chemotherapy prior tosurgery followed by HDC. The post-transplantadministration of a Her-2 Neu antibody will be performedin patients with Her-2 Neu positive tumors.
27. RESULTS OF HDC IN PATIENTS WITHMALIGNANT LYMPHOMA
27.1. Patients with Hodgkin’s DiseaseThirty-eight patients with relapsed or refractory
Hodgkin’s disease (HD) received CE or CEP and G-CSFfor mobilization of PBSC with the intent to treat with HDCwith carmustine, etoposide, cytarabine and Cy(BEAC).(49) Analyses were performed on an intent-to-treat basis. A median of 6.4 x 106 CD34+ cells/kg (range,0.66-2.3) was collected with a median of 3 (range, 2-9)aphereses. Twenty-eight of 38 (74%) patients harvested≥2.5 x 106 CD34+ cells/kg. Analyses of variablespotentially effecting mobilization revealed that the amountof prior chemotherapy statistically influenced the yield ofCD34+ cells (p = 0.005). Twenty-eight patients (74%)received BEAC followed by PBSC infusion. The 3-yearprobabilities of OS and EFS for all 38 patients were 65%and 53%, respectively. The 3-year probabilities of OS andEFS for the 28 patients receiving BEAC were 77% and64% respectively vs. 33% and 30% for the 10 patients notreceiving BEAC. The strategy of administering CE or CEPfollowed by BEAC was well tolerated with a 100-day TRMof 3.6%. Although development of better strategies tomobilize PBSC may benefit additional patients, currentlythe best strategy is to collect PBSC early before patientshave received extensive chemotherapy. Collection ofPBSC immediately following initial relapse or inductionfailure using CE or CEP allows sufficient CD34+ cells tohe collected in greater than 90% of patients.
28. PATIENTS WITH LOW GRADE NHL
Forty-nine patients with low-grade NHL receivedHDC with busulfan and Cy (BuCy) or BEAC followed byunpurged autologous PBSC infusion.(50) All patients hadfailed initial chemotherapy or progressed after an initialcomplete remission. Peripheral blood stem cells weremobilized with Cy alone (n=1), CE (n=19), or CEP (n=29)followed by G-CSF. Twenty-two patients received Bu, 16mg/kg, and Cy, 120 mg/kg. Twenty-seven patientsreceived BEAC. Four patients (8%) died of non-relapsecauses, two (9%) in the BuCy group and two (7%) in theBEAC group. Twenty-seven patients (55%) relapsed orprogressed at a median of 9.4 months (range, 2-38) fromPBSC infusion. Ten patients who relapsed are alive amedian of 31 months (range, 6-47) after relapse. Theprobabilities of relapse at 3.6 years for patients receivingBuCy or BEAC were .57 and .70, respectively (p=0.92).Twenty-seven patients (55%) are alive at a median of 3.6years (range, 1-5). The probabilities of OS at 3.6 years forpatients receiving BuCy or BEAC were .58 and .55,respectively (p=0.72). The probabilities of EFS at 3.6years for patients receiving BuCy or BEAC were .36 and.28, respectively (p=0.82). It was concluded that BuCy isan active regimen for the treatment of patients with low-grade NHL.
29. PATIENTS WITH INTERMEDIATE AND HIGH-GRADE NHL
Autologous peripheral blood stem cell transplantation
3
Eighty-three patients with NHL, who had failedconventional chemotherapy, underwent mobilization ofPBSC with chemotherapy and G-CSF in an outpatientfacility.(51) At a median of 40 days (range, 26-119) aftermobilization chemotherapy all received BEAC followed byinfusion of unmanipulated PBSC in an outpatient facility.The probabilities of TRM, relapse/progression, OS andEFS at 3 years for all 83 patients were .07, .57, .49 and .38,respectively. The probabilities of relapse/progression, OSand EFS at 3 years for 28 patients who had failed primaryinduction chemotherapy were .55, .42 and .38, respectively.The probabilities of OS and EFS for 27 patients inuntreated first relapse were .52 and .44, respectively ascompared to .56 and .32, respectively for 18 patients whohad reinduction attempts prior to receiving mobilizationchemotherapy (p=.81 for OS and 0.99 for EFS). Nosignificant risk factors for the outcomes of TRM,relapse/progression, OS or EFS could be identified.
These data demonstrate that approximately 40%of patients with NHL who have failed conventionalchemotherapy become long-term disease-free survivorsafter mobilization chemotherapy, high-dose BEAC andPBSC infusion administered in an outpatient setting incommunity cancer centers with the major cause of failurebeing relapse. Results obtained in this study arecomparable to published data in similar patient populationsreceiving therapy as inpatients suggesting that clinical trialsinvolving well tested HDC regimens can be carried outsafely in this setting. These data also suggested that HDCshould be performed promptly when patients fail intialinduction and that reinduction attempts are probably oflimited value. Reinduction attempts can also severely limitthe quantity of CD34+ cells subsequently mobilized.(56)
30. CURRENT ONGOING CLINICAL TRIAL INPATIENTS WITH MALIGNANT LYMPHOMA
Current ongoing clinical trials includeevaluations of: the more intensive HDC regimen ofBuMelTT,(57) post-transplant interferon, post-transplantanti CD20 antibody,(58) HDC in first CR for patients withadverse risk factors for failure of conventional therapy andthe role of re-induction chemotherapy in patients at firstrelapse.
31. RESULTS OF HDC IN PATIENTS WITHMULTIPLE MYELOMA
A study was designed to determine the maximumtolerated dose (MTD) of high-dose melphalan (HDM), withPBSC support, that could be given twice within 90 days topatients with newly diagnosed multiple myeloma.(52)Twenty patients received tandem HDM at 160, 180 or 200mg/m2 and a total of 55 were treated at the estimated MTDof 200 mg/m2. Seventeen of 55 (31%) did not receivecycle 2; 6 because of low CD34+ cell yields, 3 because ofsevere (n=1) or fatal toxicities (n=2) and 8 for otherreasons. The median interval between doses for 38 patientswas 70 days (range, 41-225). Three of 55 patients (5%)died of treatment-related causes. In patients completingtwo cycles of HDM, at any dose level, the complete
remission rate improved from 15% following cycle one to55% following cycle two. The probabilities of OS, EFSand relapse or progression at 18 months for the 55 patientstreated at the MTD were .84, .76 and .20, respectively, witha median followup of 19 months (range, 9-36) frommobilization chemotherapy. It was concluded that 2 cyclesof HDM, 200 mg/m2, could be administered toapproximately 70% of patients under the age of 66 withmultiple myeloma in a median interval of 70 days withimprovement in CR rates.
Current studies in patients with multiplemyeloma are designed to further evaluate two cycles ofmelphalan administered at the MTD followed bymaintenance therapies. The current study evaluates long-term administration of GM-CSF for the prevention ofrelapses.(59)
32. RESULTS OF HDC IN PATIENTS WITHOVARIAN CANCER
The purpose of this study was to develop a HDCand PBSC regimen for treatment of patients with ovariancarcinoma that could be administered in an outpatientsetting.(53) Fourteen patients with advanced ovarian(N=9) or breast (N=5) carcinoma, who had failedconventional chemotherapy, were entered into a dose-escalation trial to determine the MTD of carboplatin thatcould be administered with fixed doses of melphalan (160mg/m2) and mitoxantrone (50 mg/m2). Twenty-fiveadditional patients were included in a phase II trial at theMTD.
Two of 2 patients had grade 4 severe RRT, 1fatal, at a dose level of 1600 mg/m2. Two of 29 patients(6.9%) treated at the MTD (carboplatin, 1400 mg/m2) diedof RRT. All 3 patients who died of toxicity had acalculated AUC for carboplatin > 30 mg/ml/min. Thirty-one patients with ovarian cancer who had failedchemotherapy were treated, 24 at the MTD. Fourteen of 20patients (70%) with ovarian carcinoma with evaluabledisease achieved a CR and 7 (35%) are alive disease-free amedian of 20 months (range, 7-26). Five of 7 patients withovarian cancer who had failed chemotherapy but wererendered clinically disease-free following surgery survivewithout progression a median of 13 months (range, 9-19).Eight of 16 (50%) platinum-resistant and 4/12 (33%)platinum-sensitive patients with ovarian cancer survivedisease-free. The current study utilizes an AUC of 20µg/ml/min of carboplatin rather than a dose based on bodysurface. Current studies are focusing on earlierintervention with the MMC regimen in order to improveoutcomes.
33. WHAT IS THE FUTURE OF HDC WITH PBSCSUPPORT
33.1. Use of PBSC will Expand for Indicated Therapyand in the Evaluation of New Therapies
The use of PBSC for supportive care of patientsreceiving high-doses of chemotherapy for patients withchemosensitive malignancies will undoubtedly continue to

Autologous peripheral blood stem cell transplantation
4
expand. If PBSC are collected early in the malignantdisease course there is no reason not to incorporate theiruse into the management strategies. High-dosechemotherapy with PBSC support is best suited for diseaseswhere intensive consolidation is an integral component ofdisease management. In this setting it makes sense toassure hematopoietic and immunologic recovery by theinfusion of PBSC that have not been extensively exposed tochemotherapy or radiotherapy. However, at the presenttime HDC with PBSC support should only be carried out inthe context of clinical trials generating meaningful outcomedata.
33.2. Immune Therapies will be Evaluated after HDCwith PBSC Support
High-dose chemotherapy support can providesignificant cytoreduction of patients already in remissionbut who still have a high probability of relapse. Thiscreates an ideal setting of minimal residual disease for theevaluation of biological modifiers (IL-2, IL-12)(60,61)monoclonal antibodies (Rituximab, HER2-Neu)(58) andvaccines. In addition, the infusion of PBSC that have notbeen extensively exposed to chemotherapy and radiationmay result in a more immunocompetent patient than onewho has been extensively treated without cellular support.
Studies of immune therapies will requireenrollment of large numbers of patients in clinical trials todocument benefit. For example, one could envisionevaluating an immune therapy where the cure rate is 50%with HDC and PBSC support. In order to detect a 20 %decrease in relapses one would have to enroll over 200patients in each arm and even more if one wanted to detecta 10% difference. These kinds of studies will requireaccess to large numbers of patients which can best beachieved by including patients being treated in communitycancer centers.
Neutrophil and platelet recovery followinginfusion of ≥5.0 x 106 CD34+ cells/kg in patients withbreast cancer receiving high-dose cyclophosphamide,thiotepa and carboplatin. ROI Treatment Sites
34. REFERENCES1. Demirer, T., Buckner, C.D. & Bensinger, W.I.:Optimization of peripheral blood stem cell mobilizationStem Cells, 14, 106-16 (1996)2. Buckner, C.D., Appelbaum, F.R. & Thomas, E.D.: Bonemarrow and fetal liver. In Organ Preservation ForTransplantation, Chapter 16. (Ed, Karow, J., A.M. andPegg, D. E.) Marcel Dekker, Inc., New York, 355-75(1981)3. Linch, D.C., Hancock, B., Winfield, D., McMillan, A.,Hudson, G.V., Goldstone, A.H., Chopra, R., Moir, D. &Milligan, D.: Dose intensification with autologous bone-marrow transplantation in relapsed and resistant Hodgkin'sdisease: results of a BNLI randomised trial Lancet, 341,1051-4 (1993)4. Gianni, A.M., Bregni, M., Siena, S., Brambilla, C.,DiNicola, M., Lombardi, F., Gandola, L., Tarella, C., Pileri,
A., Ravagnani, F., Valagussa, P. & Bonadonna, G.: High-dose chemotherapy and autologous bone marrowtransplantation compared with MACOP-B in aggressive B-cell lymphoma N Engl J Med, 336, 1290-7 (1997)5. Haioun, C., Lapage, E., Gisselbrecht, C., Bastion, Y.,Coiffier, B., Brice, P., Bosly, A., Dupriez, B., Nouvel, C.,Tilly, H., Lederlin, P., Biron, P., Briere, J., Gaulard, P. &Reyes, F., for the Groupe d'Etude des Lymphomes deAdulte: Benefit of autologous bone marrow transplantationover sequential chemotherapy in poor-risk aggressive non-Hodgkin's lymphoma: Updated results of the prospectivestudy LNH87-2 J Clin Oncol, 15, 1131-7 (1997)6. Philip, T., Guglielmi, C., Hagenbeek, A., Somers, R.,Lelie, H.V.D., Bron, D., Sonneveld, P., Gisselbrecht, C.,Cahn, J., Harousseau, J., Coiffier, B., Biron, P., Mandelli,G. & Chauvin, G.: Autologous bone marrowtransplantation as compared with salvage chemotherapy inrelapses of chemotherapy-sensitive non-Hodgkin'slymphoma N Engl J Med, 333, 1540-5 (1995)7. Bezwoda, W.R., Seymour, L. & Dansey, R.D.: High-dose chemotherapy with hematopoietic rescue as primarytreatment for metastatic breast cancer: a randomized trial JClin Oncol, 13, 2483-9 (1995)8. Attal, M., Harousseau, J.-L., Stoppa, A.M., Sotto, J.-J.,Fuzibet, J.-G., Rossi, J.-F., Casassus, P., Maisonneuve, H.,Facon, T., Ifrah, N., Payen, C. & Bataille, R.: Aprospective, randomized trial of autologous bone marrowtransplantation and chemotherapy in multiple myeloma NEngl J Med, 335, 91-7 (1996)9. Zittoun, R.A., Mandelli, F., Willemze, R., De Witte, T.,Labar, B., Resegotti, L., Leoni, F., Damasio, E., Visani, G.,Papa, G., Caronia, F., Hayat, M., Stryckmans, P., Rotoli,B., Leoni, P., Peetermans, M.E., Dardenne, M., Vegna,M.L., Petti, M.C., Solbu, G. & Suciu, S.: Autologous orallogeneic bone marrow transplantation compared withintensive chemotherapy in acute myelogenous leukemia NEngl J Med, 332, 217-23 (1995)10. Harousseau, J., Cahn, J., Pignon, B., Witz, F., Milpied,N., Delain, M., Lioure, B., Larny, T., Desabiens, B.,Guilhot, F., Caillot, D., Abgrall, J., Francois, S., Briere, J.,Guyorat, D., Casassus, P., Audhuy, B., Tellier, Z.,Hurteloup, P. & Herve, P., for the Groupe Ouest EstLeucemies Aigues Myeloblastiques (GOELAM):Comparison of autologous bone marrow transplantationand intensive chemotherapy as postremission therapy inadult acute myeloid leukemia Blood, 90, 2978-86 (1997)11. Verdonck, L.F., van Putten, W.L., Hagenbeek, A.,Schouten, H.C., Sonneveld, P., van Imhoff, G.W., Kluin-Nelemans, H.C., Raemaekers, J.M., van Oers, R.H. &Haak, H.L., et al.: Comparison of CHOP chemotherapywith autologous bone marrow transplantation for slowlyresponding patients with aggressive non-Hodgkin'slymphoma N Engl J Med, 332, 1045-51 (1995)12. Clinical Bone Marrow Transplant: a reference textbook,(Ed, Atkinson, K.) (1994) Cambridge University Press,Cambridge.13. Bone Marrow Transplantation, (Ed, Forman, S. J.,Blume, K. G. and Thomas, E. D.) (1994) BlackwellScientific Publications, Boston.14. High-dose cancer therapy (pharmacology,hematopoietins, stem cells), (Ed, Armitage, J. O. and
Autologous peripheral blood stem cell transplantation
5
Antman, K. H.) (1992) Williams & Wilkins, Baltimore,MD.15. Schwartzberg, L., Birch, R., Hazelton, B., Tauer, K.,Lee, P., Altemose, R., George, C., Blanco, R., Wittlin, F.,Cohen, J., Muscato, J. & West, W.: Peripheral blood stemcell mobilization by chemotherapy with and withoutrecombinant human granulocyte colony-stimulating factor JHematother, 1, 317-27 (1992)16. Schwartzberg, L., Birch, R., Blanco, R., Wittlin, F.,Muscato, J., Tauer, K., Hazelton, B. & West, W.: Rapidand sustained hematopoietic reconstitution by peripheralblood stem cell infusion alone following high-dosechemotherapy Bone Marrow Transplant, 11, 369-74 (1993)17. Weaver, C.H., Schwartzberg, L.S., Birch, R., Greco,F.A., Rhinehart, S., Hainsworth, J., Beeker, T., Price, H.,Geier, L., Foster, J., West, J., Hazelton, B. & Buckner,C.D.: Collection of peripheral blood progenitor cellsfollowing the administration of cyclophosphamide,etoposide and granulocyte-colony stimulating factor: ananalysis of 497 patients Transfusion, 37, 896-903 (1997)18. Weaver, C.H., Schwartzberg, L.S., Birch, R., Greco, A.,Hainsworth, J., Drapkin, R., Campos, L., Grapski, R.,Schwerkoske, J., Lautersztain, J., Hazelton, B., Schnell, F.,Babcock, W. & Buckner, C.D.: Collection of peripheralblood stem cells following the administration of paclitaxel,cyclophosphamide and filgrastim in patients with breastand ovarian cancer Biol Blood Marrow Transplant, 3, 83-90 (1997)19. Weaver, C., Zhen, B., Schwartzberg, L., Walker, C.,Upton, S. & Buckner, C.: A randomized trial ofmobilization of peripheral blood stem cells withcyclophosphamide, etoposide and G-CSF with or withoutcisplatin in patients with malignant lymphoma receivinghigh-dose chemotherapy Am J Clin Oncol, 21, 141-50(1998)20. Bensinger, W.I., Longin, K., Appelbaum, F., Rowley,S., Weaver, C., Lilleby, K., Gooley, T., Lynch, M., Higano,T., Klarnet, J., Chauncey, T., Storb, R. & Buckner, C.D.:Peripheral blood stem cells (PBSCs) collected afterrecombinant granulocyte colony stimulating factor (rhG-CSF): an analysis of factors correlating with the tempo ofengraftment after transplantation Br J Haematol, 87, 825-31(1994)21. Weaver, C.H., Birch, R., Greco, F.A., Schwartzberg,L.S., McAneny, B., Moore, M., Oviatt, D., Redmond, J.,George, C., Alberico, T. & Buckner, C.D.: Mobilizationand harvesting of peripheral blood stem cells: Arandomized dose escalation trial of filgrastim Br JHaematol, 100, 338-47 (1998)22. Weaver, C.H., Hazelton, B., Birch, R., Palmer, P.,Allen, C., Schwartzberg, L. & West, W.: An analysis ofengraftment kinetics as a function of the CD34 content ofperipheral blood progenitor cell collections in 692 patientsafter the administration of myeloablative chemotherapyBlood, 86, 3961-9 (1995)23. Bensinger, W.I., Singer, J., Appelbaum, F., Lilleby, K.,Longin, K., Rowley, S., Clark, E., Clift, R., Hansen, J.,Shieds, T., Storb, R., Weaver, C.H., Weiden, P. & Buckner,C.D.: Autologous transplantation with peripheral bloodmononuclear cells collected after administration ofrecombinant granulocyte stimulating factor Blood, 81,3158-63 (1993)
24. Bensinger, W., Appelbaum, F., Rowley, S., Storb, R.,Sanders, J., Lilleby, K., Gooley, T., Demirer, T.,Schiffman, K., Weaver, C., Clift, R., Chauncey, T.,Klarnet, J., Montgomery, P., Petersdorf, S., Weiden, P.,Witherspoon, R. & Buckner, C.D.: Factors that influencecollection and engraftment of autologous peripheral-bloodstem cells J Clin Oncol, 13, 2547-55 (1995)25. Bensinger, W.I., Demirer, T., Rowley, S. & Buckner,C.D.: Factors predictive of rapid engraftment afterperipheral blood stem cell infusions Bone MarrowTransplant, 15, S83-S5 (1995)
26. Schwartzberg, L., Weaver, C., Birch, R., Manner, C.,Tauer, K., Beeker, T., Morgan-Ihrig, C., MacAneny, B.,Leff, R., Smith, R., Hainsworth, J., Greco, T.,Schwerkoske, J., Murphy, M. & Buckner, C.: Arandomized trial of two doses of cyclophosphamide withetoposide and G-CSF for mobilization of peripheral bloodstem cells in 318 patients with stage II-III breast cancer JHematother, (in press)(1997)27. Weaver, C., Schwartzberg, L., Zhen, B., Franco, C.,Moore, M., Smith, J., R, White, L., Van Amburg, A.,Hazelton, B. & Buckner, C.: Mobilization of peripheralblood stem cells with docetaxel and cyclophosphamide(CY) in patients with metastatic breast cancer: Arandomized trial of 3 versus 4 g/m2 of CY Bone MarrowTransplant, (in press)(1998)28. Weaver, C.H., Potz, J., Redmond, J., Tauer, K.,Schwartzberg, L.S., Kaywin, P., Drapkin, R., Grant, B.,Unger, P., Allen, C., Longin, K., Zhen, B., Hazelton, B. &Buckner, C.D.: Engraftment and outcomes of patientsreceiving myeloablative therapy followed by autologousperipheral blood stem cells with a low CD34+ contentBone Marrow Transplant, 19, 1103-10 (1997)29. Ho, A.D., Young, D., Marayuma, M., Corringham,R.E., Mason, J.R., Thompson, P., Grenier, K., Law, P.,Terstappen, L.W. & Lane, T.: Pluripotent and lineage-committed CD34+ subsets in leukapheresis productsmobilized by G-CSF, GM-CSF vs. a combination of bothExp Hematol, 24, 1460-8 (1996)30. Moskowitz, C., Stiff, P., Gordon, M., McNiece, I., Ho,A., Costa, J., Broun, E., Bayer, R., Wyres, M., Hill, J.,Jelaca-Maxwell, K., Nichols, C., Brown, S., Nimer, S. &Gabrilove, J.: Recombinant methionyl human stem cellfactor and filgrastim for peripheral blood progenitor cellmobilization and transplantation in non-hodgkin'slymphoma patients - results of a phase I/II trial Blood, 89,3136-47 (1997)31. Brugger, W., Bross, K., Frisch, J., Dern, P., Weber, B.,Mertelsmann, R. & Kanz, L.: Mobilization of peripheralblood progenitor cells by sequential administration ofinterleukin-3 and granulocyte-macrophage colony-stimulating factor following polychemotherapy withetoposide, ifosfamide and cisplatin Blood, 79, 1193-200(1992)32. Haas, R., Möhle, R., Frühauf, S., Goldschmidt, H.,Witt, B., Flentje, M., Wannenmacher, M. & Hunstein, W.:Patient characteristics associated with successfulmobilizing and autografting of peripheral blood progenitorcells in malignant lymphoma Blood, 83, 3787-94 (1994)33. Tricot, G., Jagannath, S., Vesole, D., Nelson, J., Tindle,S., Miller, L., Cheson, B., Crowley, J. & Barlogie, B.:

Autologous peripheral blood stem cell transplantation
6
Peripheral blood stem cell transplants for multiplemyeloma: identification of favorable variables for rapidengraftment in 225 patients Blood, 85, 588-96 (1995)34. Brenner, M.K., Rill, R.D., Moen, R.C., Kranee, R.A.,Mirro, J., Anderson, M.F. & Ihle, W.F.: Gene-marking totrace origin of relapse after autologous bone marrowtransplantation Lancet, 341, 85-6 (1993)35. Bensinger, W.: Should we purge? [Editorial] BoneMarrow Transplant, 21, 113-5 (1998)36. Buckner, C., Birch, R. & Weaver, C.: The rationale fornot routinely purging autologous blood stem cell graftsHematology, (in press)(1997)37. Williams, C.D., Goldstone, A.H., Pearce, R.M., Philip,T., Hartmann, O., Colombat, P., Santini, G., Foulard, L. &Gorin, N.C.: Purging of bone marrow in autologous bonemarrow transplantation for non-hodgkin's lymphoma: acase-matched comparison with unpurged cases by theEuropean Blood and Marrow Transplant LymphomaRegistry J Clin Oncol, 14, 2454-64 (1996)38. Gribben, J.G., Neuberg, D., Freedman, A.S., Gimmi,C.D., Pesek, K.W., Barber, M., Saporito, L., Woo, S.D.,Coral, F., Spector, N., Rabinowe, S.N., Grossbard, M.L.,Ritz, J. & Nadler, L.M.: Detection by polymerase chainreaction of residual cells with the bcl-2 translocation isassociated with increased risk of relapse after autologousbone marrow transplantation for B-cell lymphoma Blood,81, 3449-57 (1993)39. Barlogie, B., Jagannath, S., Vesole, D. & Tricot, G.:Autologous and allogeneic transplants for multiplemyeloma Sem Hematol, 32, 31-44 (1995)40. Bensinger, W.I., Rowley, S.D., Demirer, T., Lilleby,K., Schiffman, K., Clift, R.A., Appelbaum, F.R., Fefer, A.,Barnett, T., Storb, R., Chauncey, T., Maziarz, R.T.,Klarnet, J., McSweeney, P., Holmberg, L., Maloney, D.G.,Weaver, C. & Buckner, C.D.: High-dose therapy followedby autologous hematopoietic stem cell infusion for patientswith multiple myeloma J Clin Oncol, 14, 1447-56 (1996)41. Anderson, K.C., Andersen, J., Soiffer, R., Freedman,A.S., Rabinowe, S.N., Robertson, M.J., Spector, N., Blake,K., Murray, C., Freeman, A., Coral, F., Marcus, K.C.,Mauch, P., Nadler, L.M. & Ritz, J.: Monoclonal antibody-purged bone marrow transplantation therapy for multiplemyeloma Blood, Vol. 82, 2568-76 (1993)42. Schiller, G., Vescio, R., Freytes, C., Spitzer, G., Sahebi,F., Lee, M., Wu, C.H., Cao, J., Lee, J.C., Hong, C.H.,Lichtenstein, A., Lill, M., Hall, J., Berenson, R. &Berenson, J.: Transplantation of CD34+ peripheral bloodprogenitor cells after high-dose chemotherapy for patientswith advanced multiple myeloma Blood, 86, 390-7 (1995)43. Weaver, C.H., Moss, T., Schwartzberg, L.S., Zhen, B.,West, J., Rhinehart, S., Campos, L., Beeker, T.,Lautersztain, L. & Buckner, C.D.: High-dose chemotherapyin patients with breast cancer: impact of infusing peripheralblood stem cells containing occult tumor cells BoneMarrow Transplant, (in press)(1998)44. Shpall, E., LeMaistre, C., Holland, K., Ball, E., Jones,R., Saral, R., Jacobs, C., Heimfeld, S., Berenson, R. &Champlin, R.: A prospective randomized trial of buffy coatversus CD34-selected autologous bone marrow support inhigh-risk breast cancer patients receiving high-dosechemotherapy Blood, 90, 4313-20 (1997)
45. Hill, R.S., Mazza, P., Amos, D., Buckner, C.D.,Appelbaum, F.R., Still, B.J., Berenson, R., Bensinger, W.,Clift, R.A., Stewart, P., Doney, K., Sanders, J., Singer, J.,Sullivan, K.M., Witherspoon, R.P., Storb, R., Livingston,R., Chard, R. & Thomas, E.D.: Engraftment in 86 patientswith lymphoid malignancy after autologous marrowtransplantation Bone Marrow Transplant, 4, 69-74 (1989)46. Weaver, C.H., Schwartzberg, L.S., Hainsworth, J.,Greco, F.A., Li, W., Buckner, C.D. & West, W.: Treatmentrelated mortality in 1,000 consecutive patients receivinghigh-dose chemotherapy and peripheral blood progenitorcell transplantation in community cancer centers BoneMarrow Transplant, 19, 671-8 (1997)47. Weaver, C.H., West, W.H., Schwartzberg, L.S., Birch,R., McAneny, B., Alberico, T., Hainsworth, J., Greco, F.A.,Leff, R. & Buckner, C.D.: Induction, mobilization ofperipheral blood stem cells (PBSC), high-dosechemotherapy and PBSC infusion in patients with untreatedstage IV breast cancer: outcomes by intent to treat analysesBone Marrow Transplant, 19, 661-70 (1997)48. Schwartzberg, L.S., Birch, R., West, W.H., Tauer, K.,Wittlin, F., Leff, R., Campos, l., Rymer, W., George, C.,Carter, P., Mangum, M., Greco, F.A., Hainsworth, J.,Raefsky, E., Blanco, R., Buckner, C.D. & Weaver, C.H.:Sequential treatment including high-dose chemotherapywith peripheral blood stem cell support in patients withhigh-risk stage II-III breast cancer: outpatientadministration in community cancer centers Am J ClinOncol, (in press)(1998)49. Weaver, C.H., Schwartzberg, L.S., Li, W., Hazelton, B.& West, W.: High-dose chemotherapy and autologousperipheral blood progenitor cell transplant for the treatmentof Hodgkin's disease Bone Marrow Transplant, 17, 715-21(1996)50. Weaver, C., Schwartzberg, L., Rhinehart, S., West, J.,Zhen, B., West, W. & Buckner, C.: High-dosechemotherapy with BUCY or BEAC and unpurgedperipheral blood stem cell infusion in patients with low-grade non-hodgkin’s lymphoma Bone Marrow Transplant,21, 383-9 (1998)51. Weaver, C.H., Schwartzberg, L.S., Zhen, B., Mangum,M., Leff, R., Tauer, K., Rosenberg, A., Pendergrass, K.,Kaywin, P., Hainsworth, J., Greco, F.A., West, W.H. &Buckner, C.D.: High-dose chemotherapy and peripheralblood stem cell infusion in patients with Non-Hodgkin'slymphoma: Results of outpatient treatment in communitycancer centers Bone Marrow Transplant, 20, 753-60 (1997)52. Weaver, C.H., Zhen, B., Schwartzberg, L.S., Leff, R.,Magee, M., Geier, L., Deaton, K., Lewkow, L. & Buckner,C.D.: Phase I-II evaluation of rapid sequence tandem high-dose melphalan with peripheral blood stem cell support inpatients with multiple myeloma Bone Marrow Transplant,(in press)(1998)53. Weaver, C.H., Greco, F.A., Hainsworth, J., Zhen, B.,Baldwin, P., Wittlin, F., Lewis, M., Schwartzberg, L.S. &Buckner, C.D.: A phase I-II study of high-dose melphalan,mitoxantrone and carboplatin with peripheral blood stemcell support in patients with advanced ovarian or breastcarcinoma Bone Marrow Transplant, 20, 847-53 (1997)54. Bensinger, W.I., Schiffman, K.S., Holmberg, L.,Appelbaum, F.R., Maziarz, R., Montgomery, P., Ellis, E.,Rivkin, S., Weiden, P., Lilleby, K., Rowley, S., Petersdorf,

Autologous peripheral blood stem cell transplantation
7
S., Klarnet, J.P., Nichols, W., Hertler, A., McCroskey, R.,Weaver, C.H. & Buckner, C.D.: High-dose busulfan,melphalan, thiotepa and peripheral blood stem cell infusionfor the treatment of metastatic breast cancer Bone MarrowTransplant, 19, 1183-9 (1997)55. Schwartzberg, L.S., Birch, R., Tauer, K.W., Leff, R.,Greco, F.A., Hainsworth, J., Raefsky, E., McAneny, B.,Weaver, Z., West, J., Buckner, C.D. & Weaver, C.H.:Adjuvant dose-intense chemotherapy with peripheral bloodstem cell support in stage II-III breast cancer with 5-9involved axillary lymph nodes Am J Clin Oncol, (inpress)(1998)56. Weaver, C.H., Zhen, B. & Buckner, C.D.: Treatment ofpatients with malignant lymphoma with mini-BEAMreduces the yield of CD34+ peripheral blood stem cells(letter) Bone Marrow Transplant, (in press)(1998)57. Schiffman, K., Buckner, C., Maloney, D., Appelbaum,F., Press, O., Gooley, T., Holmberg, L., Lilleby, K., Clift,R., Zuckerman, N., Maziarz, R., Klarnet, J., Weaver, C.,Chauncey, T. & Bensinger, W.: High-dose busulphan,melphalan and thiotepa followed by autologous peripheralblood stem cell transplantation in patients with aggressivelymphoma or relapsed Hodgkin's disease Biol BloodMarrow Transplant, 3, 261-6 (1997)58. Maloney, D., Grillo-Lopez, A., White, C., Bodkin, D.,Schilder, R., Neidhart, J., Janakiraman, N., Foon, K., Liles,T., Dallaire, B., Wey, K., Royston, I., Davis, T. & Levy, R.:IDEC-C2B8 (Rituximab) anti-CD20 monoclonal antibodytherapy in patients with relapsed low-grade non-Hodgkin'slymphoma Blood, 90, 2188-95 (1997)59. Richard, C., Baro, J. & Bello-Fernandez, C., et al:Recombinant human granulocyte-macrophage colony-stimulating factor (rhGM-CSF) administration afterautologous bone marrow transplantation for acutemyeloblastic leukemia enhances activated killer cellfunction and may diminish leukemic relapse Bone MarrowTransplant, 15, 721-6 (1995)60. Fefer, A., Benyunes, M.C., Massumoto, C., Higuchi,C., York, A., Buckner, C.D. & Thompson, J.A.:Interleukin-2 therapy after autologous bone marrowtransplantation for hematologic malignancies Semin Oncol,20, 41-5 (1993)61. Caligiuri, M.: Low-dose recombinant interleukin-2therapy: Rationale and potential clinical applications SeminOncol, 20, 3-10 (1993)
Key Words: AU: Please provide key words
Send correspondence to: C. Dean Buckner, M.D., ResponseOncology, Inc., 600 Broadway, Suite 112,, Seattle,Washington 98122, Tel: 206-726-8921, Fax:206-726-9068, E-mail: [email protected]
Received 5/4/98 Accepted 7/21/98
AU:
1. The manuscript has been reformatted. Please checkthe table of contents and make changes to the numbersthat are used in the table of contents and in the text.Change if necessary.
2. Due to formatting, some special characters may belost. Please read the galley carefully and substitute suchcharacters preferably with their English correlates.2. Please format the references as follows:
Journal citation:Novick, R., G. Adler, S. Projan, S. Carleton, S. Highlander,A. Gruss, S. Khan, & S. Iordanescu: Control of pT181replication I. The pT181 copy control function acts byinhibiting the synthesis of a replication protein. EMBO J10, 2399-2405 (1984)
Book citation:Novick, R., S. Projan, S. Kumar, C. Carleton, S. Gruss, S.Highlander, & J. Kornblum: Replication control for pT181,an indirectly regulated plasmid. In: Plasmids in bacteria.Eds: Helinski DR, Clewell DB, Jackson DA , & HollaenderA, Plenum Press: New York & London 299-320 (1985)
Please note that the name of the journals is italicized.
Related Documents




![Hematological malignancies - БГМУHematological malignancies Leukemia is a malignant proliferation of white blood cells (lymphoid cells [lymphocytes] or myeloid cells [granulocytes](https://static.cupdf.com/doc/110x72/5f0624c37e708231d416825d/hematological-malignancies-oe-hematological-malignancies-leukemia-is-a-malignant.jpg)






