http://msj.sagepub.com/ Multiple Sclerosis Journal http://msj.sagepub.com/content/17/2/204 The online version of this article can be found at: DOI: 10.1177/1352458510383609 2011 17: 204 originally published online 4 October 2010 Mult Scler James T Reston, Stacey Uhl, Jonathan R Treadwell, Richard A Nash and Karen Schoelles Autologous hematopoietic cell transplantation for multiple sclerosis: a systematic review Published by: http://www.sagepublications.com can be found at: Multiple Sclerosis Journal Additional services and information for http://msj.sagepub.com/cgi/alerts Email Alerts: http://msj.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: by guest on May 22, 2011 msj.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
http://msj.sagepub.com/Multiple Sclerosis Journal
http://msj.sagepub.com/content/17/2/204The online version of this article can be found at:
DOI: 10.1177/1352458510383609
2011 17: 204 originally published online 4 October 2010Mult SclerJames T Reston, Stacey Uhl, Jonathan R Treadwell, Richard A Nash and Karen Schoelles
Autologous hematopoietic cell transplantation for multiple sclerosis: a systematic review
Published by:
http://www.sagepublications.com
can be found at:Multiple Sclerosis JournalAdditional services and information for
http://msj.sagepub.com/cgi/alertsEmail Alerts:
http://msj.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
by guest on May 22, 2011msj.sagepub.comDownloaded from
Research Paper
Multiple Sclerosis Journal
17(2) 204–213
! The Author(s) 2011
Reprints and permissions:
sagepub.co.uk/journalsPermissions.nav
DOI: 10.1177/1352458510383609
msj.sagepub.com
Autologous hematopoietic celltransplantation for multiple sclerosis:a systematic review
James T Reston1, Stacey Uhl1, Jonathan R Treadwell1,Richard A Nash2 and Karen Schoelles1
Abstract
Background and objectives: The purpose of this systematic review was to evaluate the safety and efficacy of autol-
ogous hematopoietic cell transplantation in patients with progressive multiple sclerosis (MS) refractory to conventional
medical treatment.
Methods: Eight case series met our a priori inclusion criteria for the primary outcome of progression-free survival.
Individual study quality was rated using an 11-item scale for case series. The strength of the overall body of evidence for
each outcome was rated using a system developed by the ECRI Institute. Data from different studies were statistically
combined using meta-analysis. An additional six studies were included for a summary of mortality and morbidity.
Results: For secondary progressive MS, immunoablative therapy with autologous bone marrow/peripheral blood stem
cell transplantation was associated with higher progression-free survival (up to 3 years following treatment) when using
intermediate-intensity conditioning regimens compared with high-intensity conditioning regimens. The evidence was
insufficient to determine whether the treatment was effective in patients with other types of MS. Treatment-related
mortality was about 2.7%.
Conclusions: Patients with secondary progressive MS refractory to conventional medical treatment have longer
progression-free survival following autologous stem cell transplantation with intermediate-intensity conditioning
regimens than with high-intensity conditioning regimens.
Keywords
meta-analysis, multiple sclerosis, progressive, stem cell transplantation
Date received: 13th April 2010; revised: 1st July 2010; 05 August 2010; accepted: 11th August 2010
Introduction
Multiple sclerosis (MS) is a chronic neurologicaldisease affecting an estimated 400,000 people inthe United States and more than 2 million peopleworldwide.1 Disease-modifying medications have beenshown to reduce the frequency and severity of relapsesor exacerbations in patients with relapsing–remittingMS (RRMS), reduce the accumulation of lesions, andslow down the accumulation of disability.2 However,there are currently no medications that can effectivelytreat secondary progressive MS (SPMS) or primaryprogressive (PPMS), and some individuals withRRMS do not respond to conventional medicaltherapy.
The most widely accepted hypothesis is that MS isan autoimmune disease triggered in susceptible individ-uals by an unknown environmental agent(s).1,3 Animalstudies have shown that immunosuppressive therapyfollowed by hematopoietic cell transplantation (HCT)can cure autoimmune diseases in mice and rats.4
1Evidence-Based Practice Center, Health Technology Assessment Group,
ECRI Institute, Plymouth Meeting, PA, USA.2Clinical Research Division, Fred Hutchinson Cancer Research Center,
Seattle, WA, USA.
Corresponding author:
Dr James Reston, ECRI Institute, 5200 Butler Pike, Plymouth Meeting, PA
19462-1298, USA
Email: [email protected]
by guest on May 22, 2011msj.sagepub.comDownloaded from

Some human studies also noted that cases of pre-exist-ing autoimmune disease coincidental with malignancieshave sometimes gone into prolonged remission whenthe malignancy was treated with immunoablation fol-lowed by HCT.5,6 These studies led to the hypothesisthat high-dose immunosuppressive therapy eliminatesthe components of the immune system that cause theautoimmune disease. Then, the patient’s full health maybe restored by reconstituting the immune system with atransplant of hematopoietic stem cells, either from acompatible donor (allogeneic) or from previouslystored bone marrow or blood cells from the patient(autologous), that either do not contain the autoim-mune generating components or that have beenpurged of them.5,6
Immunosuppressive regimens used for treatment ofMS can be divided into two categories: high intensityand intermediate intensity. The most commonly usedhigh-intensity regimen is a combination of total bodyirradiation (TBI) plus cyclophosphamide (CY); otherhigh-intensity regimens include busulfan plus CY orbusulfan alone. The most commonly used intermedi-ate-intensity regimen is the BEAM regimen, which isa combination of etoposide, melphalan, carmustine,and cytosine arabinoside. An alternative intermediate-intensity regimen is carmustine plus CY.4 Treatment ofMS with high-intensity regimens seemed to be morecommon in the earlier North American studies,whereas most European studies used the BEAMregimen.
Stem cells (usually collected from the patient’speripheral blood prior to conditioning) are reinfusedafter the conditioning regimen has been completed.Anti-thymocyte globulin (ATG) is often administeredas part of the conditioning stem-cell re-infusion todeplete any autoreactive T cells that survived the con-ditioning regimen or remained in the stem cells used forreinfusion.4
We conducted this systematic review to evaluate theevidence concerning the safety and efficacy of autolo-gous HCT in patients with progressive MS refractory toconventional medical treatment.
Material and methods
Study selection
We applied the following a priori inclusion criteria.Studies must have been full articles published inEnglish language journals that enrolled at least fivepatients for autologous HCT. Patients must have hadprogressive MS (defined as disability progression �1point on the Expanded Disability Status Scale [EDSS]sustained for at least 6 months the previous year)
refractory to alternative treatments (e.g. interferonbeta-1a). To evaluate progression-free survival, werequired at least 2 years median followup.
Immunoablative therapy followed by autologousHCT is considered a treatment of last resort in patientswith progressive MS whose condition has continued toworsen despite conventional non-invasive medical ther-apy (e.g. immunosuppressant drugs). Such patients areless likely to stabilize or improve than patients whohave not undergone conventional medical therapy.However, some patients with progressive MS mayhave temporary stabilization of their symptoms dueto regression to the mean. Studies only enroll patientswith disease progression in the previous year, andpatients might be more likely to show less progressionin the year following treatment simply because theywere enrolled at peak symptomatology. Studies with acomparison arm of patients receiving conventional orno therapy would address this problem, but no con-trolled studies of immunoablative therapy for MShave yet been published.
Study identification
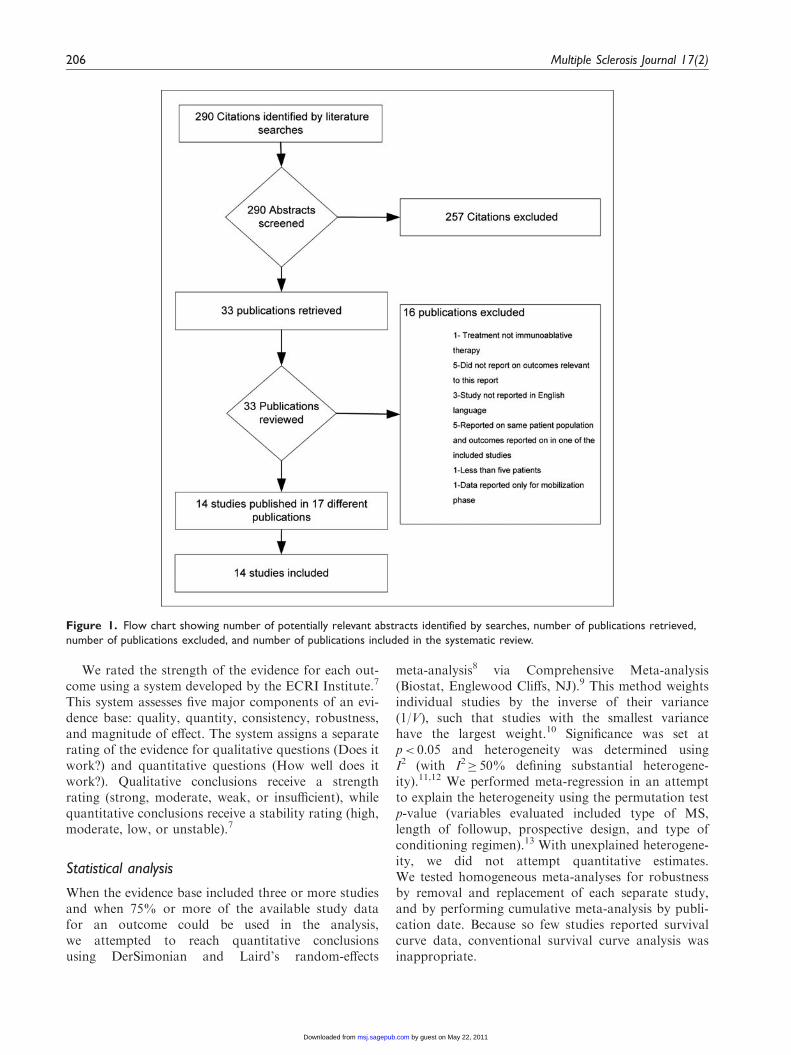
We searched PubMED and EMBASE (throughFebruary 2009) for identification of relevant studies,and 15 other databases were searched for additionalinformation. (A complete list of the databases wesearched can be obtained from the correspondingauthor.) Figure 1 illustrates the screening, retrieval,and inclusion process for the case series. Of 290 identi-fied studies, 33 were retrieved and 14 met our inclusioncriteria.
Key outcomes
Key outcomes of interest included rates of progression-free survival (the primary outcome) and major compli-cations. Progression-free survival is defined as theprobability of being alive without confirmed disabilityprogression (increase in EDSS �1 if initial EDSS �5.0or �0.5 if initial score �5.5 for at least 6 months) aftertransplantation.
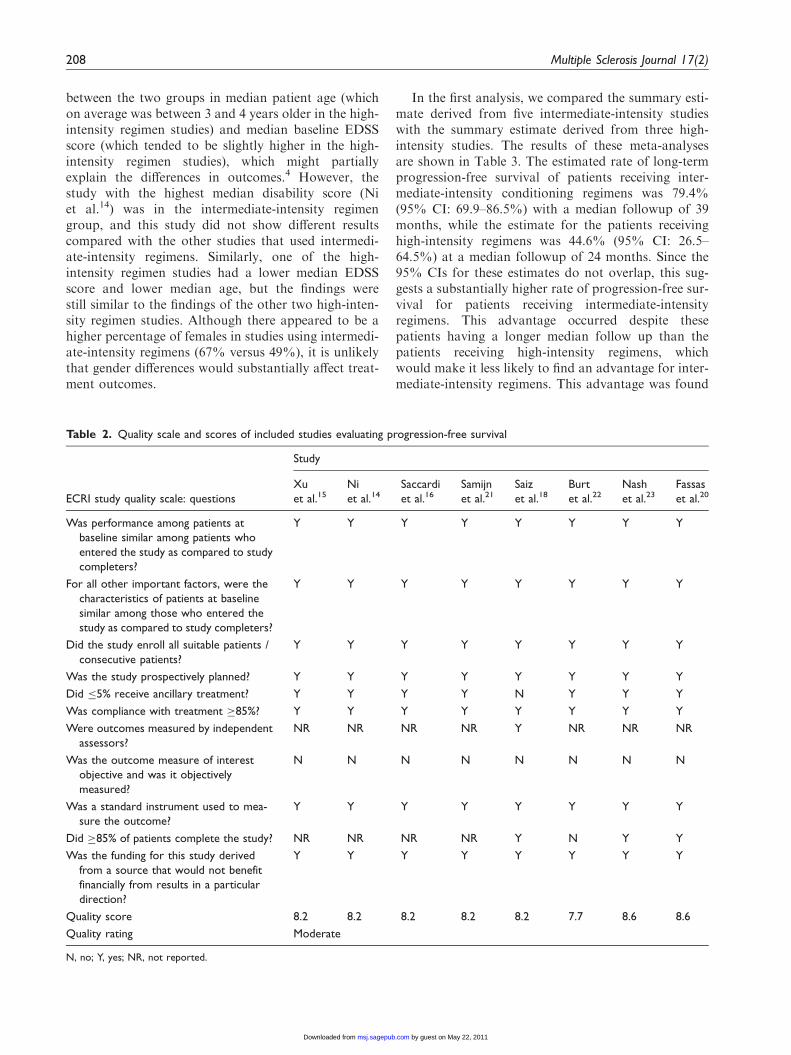
Evaluation of study quality and strength of evidence
Individual study quality was rated separately for eachoutcome using an 11-item scale developed by the ECRIInstitute specifically for case series. The items werechosen by a consensus of methodologists using a nom-inal group technique (unpublished work). Scores wereconverted to a 0–10 scale, with a score �7.0 indicatingmoderate quality, and scores <7.0 indicating low qual-ity (the lack of a within-study control group precludedthe possibility of a high-quality score).
Reston et al. 205
by guest on May 22, 2011msj.sagepub.comDownloaded from
We rated the strength of the evidence for each out-come using a system developed by the ECRI Institute.7
This system assesses five major components of an evi-dence base: quality, quantity, consistency, robustness,and magnitude of effect. The system assigns a separaterating of the evidence for qualitative questions (Does itwork?) and quantitative questions (How well does itwork?). Qualitative conclusions receive a strengthrating (strong, moderate, weak, or insufficient), whilequantitative conclusions receive a stability rating (high,moderate, low, or unstable).7
Statistical analysis
When the evidence base included three or more studiesand when 75% or more of the available study datafor an outcome could be used in the analysis,we attempted to reach quantitative conclusionsusing DerSimonian and Laird’s random-effects
meta-analysis8 via Comprehensive Meta-analysis(Biostat, Englewood Cliffs, NJ).9 This method weightsindividual studies by the inverse of their variance(1/V), such that studies with the smallest variancehave the largest weight.10 Significance was set atp< 0.05 and heterogeneity was determined usingI2 (with I2� 50% defining substantial heterogene-ity).11,12 We performed meta-regression in an attemptto explain the heterogeneity using the permutation testp-value (variables evaluated included type of MS,length of followup, prospective design, and type ofconditioning regimen).13 With unexplained heterogene-ity, we did not attempt quantitative estimates.We tested homogeneous meta-analyses for robustnessby removal and replacement of each separate study,and by performing cumulative meta-analysis by publi-cation date. Because so few studies reported survivalcurve data, conventional survival curve analysis wasinappropriate.
Figure 1. Flow chart showing number of potentially relevant abstracts identified by searches, number of publications retrieved,
number of publications excluded, and number of publications included in the systematic review.
206 Multiple Sclerosis Journal 17(2)
by guest on May 22, 2011msj.sagepub.comDownloaded from
Results
Progression-free survival
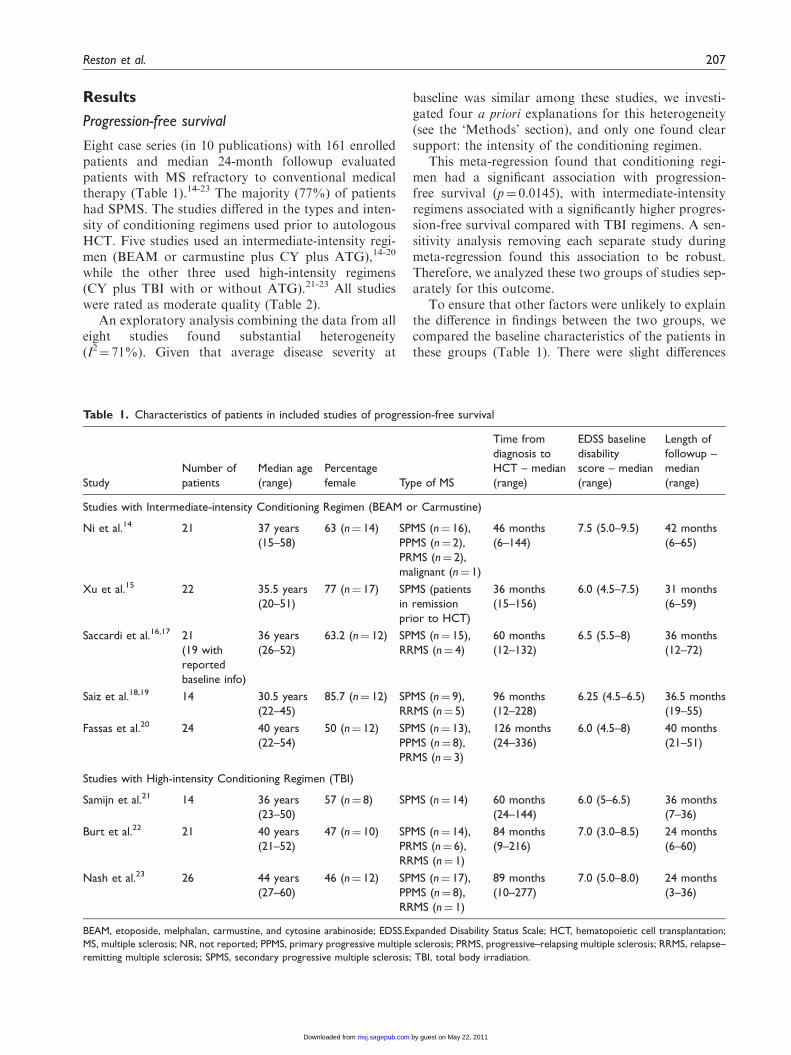
Eight case series (in 10 publications) with 161 enrolledpatients and median 24-month followup evaluatedpatients with MS refractory to conventional medicaltherapy (Table 1).14-23 The majority (77%) of patientshad SPMS. The studies differed in the types and inten-sity of conditioning regimens used prior to autologousHCT. Five studies used an intermediate-intensity regi-men (BEAM or carmustine plus CY plus ATG),14-20
while the other three used high-intensity regimens(CY plus TBI with or without ATG).21-23 All studieswere rated as moderate quality (Table 2).
An exploratory analysis combining the data from alleight studies found substantial heterogeneity(I2¼ 71%). Given that average disease severity at
baseline was similar among these studies, we investi-gated four a priori explanations for this heterogeneity(see the ‘Methods’ section), and only one found clearsupport: the intensity of the conditioning regimen.
This meta-regression found that conditioning regi-men had a significant association with progression-free survival (p¼ 0.0145), with intermediate-intensityregimens associated with a significantly higher progres-sion-free survival compared with TBI regimens. A sen-sitivity analysis removing each separate study duringmeta-regression found this association to be robust.Therefore, we analyzed these two groups of studies sep-arately for this outcome.
To ensure that other factors were unlikely to explainthe difference in findings between the two groups, wecompared the baseline characteristics of the patients inthese groups (Table 1). There were slight differences
Table 1. Characteristics of patients in included studies of progression-free survival
Study
Number of
patients
Median age
(range)
Percentage
female Type of MS
Time from
diagnosis to
HCT – median
(range)
EDSS baseline
disability
score – median
(range)
Length of
followup –
median
(range)
Studies with Intermediate-intensity Conditioning Regimen (BEAM or Carmustine)
Ni et al.14 21 37 years
(15–58)
63 (n¼ 14) SPMS (n¼ 16),
PPMS (n¼ 2),
PRMS (n¼ 2),
malignant (n¼ 1)
46 months
(6–144)
7.5 (5.0–9.5) 42 months
(6–65)
Xu et al.15 22 35.5 years
(20–51)
77 (n¼ 17) SPMS (patients
in remission
prior to HCT)
36 months
(15–156)
6.0 (4.5–7.5) 31 months
(6–59)
Saccardi et al.16,17 21
(19 with
reported
baseline info)
36 years
(26–52)
63.2 (n¼ 12) SPMS (n¼ 15),
RRMS (n¼ 4)
60 months
(12–132)
6.5 (5.5–8) 36 months
(12–72)
Saiz et al.18,19 14 30.5 years
(22–45)
85.7 (n¼ 12) SPMS (n¼ 9),
RRMS (n¼ 5)
96 months
(12–228)
6.25 (4.5–6.5) 36.5 months
(19–55)
Fassas et al.20 24 40 years
(22–54)
50 (n¼ 12) SPMS (n¼ 13),
PPMS (n¼ 8),
PRMS (n¼ 3)
126 months
(24–336)
6.0 (4.5–8) 40 months
(21–51)
Studies with High-intensity Conditioning Regimen (TBI)
Samijn et al.21 14 36 years
(23–50)
57 (n¼ 8) SPMS (n¼ 14) 60 months
(24–144)
6.0 (5–6.5) 36 months
(7–36)
Burt et al.22 21 40 years
(21–52)
47 (n¼ 10) SPMS (n¼ 14),
PRMS (n¼ 6),
RRMS (n¼ 1)
84 months
(9–216)
7.0 (3.0–8.5) 24 months
(6–60)
Nash et al.23 26 44 years
(27–60)
46 (n¼ 12) SPMS (n¼ 17),
PPMS (n¼ 8),
RRMS (n¼ 1)
89 months
(10–277)
7.0 (5.0–8.0) 24 months
(3–36)
BEAM, etoposide, melphalan, carmustine, and cytosine arabinoside; EDSS.Expanded Disability Status Scale; HCT, hematopoietic cell transplantation;
MS, multiple sclerosis; NR, not reported; PPMS, primary progressive multiple sclerosis; PRMS, progressive–relapsing multiple sclerosis; RRMS, relapse–
remitting multiple sclerosis; SPMS, secondary progressive multiple sclerosis; TBI, total body irradiation.
Reston et al. 207
by guest on May 22, 2011msj.sagepub.comDownloaded from
between the two groups in median patient age (whichon average was between 3 and 4 years older in the high-intensity regimen studies) and median baseline EDSSscore (which tended to be slightly higher in the high-intensity regimen studies), which might partiallyexplain the differences in outcomes.4 However, thestudy with the highest median disability score (Niet al.14) was in the intermediate-intensity regimengroup, and this study did not show different resultscompared with the other studies that used intermedi-ate-intensity regimens. Similarly, one of the high-intensity regimen studies had a lower median EDSSscore and lower median age, but the findings werestill similar to the findings of the other two high-inten-sity regimen studies. Although there appeared to be ahigher percentage of females in studies using intermedi-ate-intensity regimens (67% versus 49%), it is unlikelythat gender differences would substantially affect treat-ment outcomes.
In the first analysis, we compared the summary esti-mate derived from five intermediate-intensity studieswith the summary estimate derived from three high-intensity studies. The results of these meta-analysesare shown in Table 3. The estimated rate of long-termprogression-free survival of patients receiving inter-mediate-intensity conditioning regimens was 79.4%(95% CI: 69.9–86.5%) with a median followup of 39months, while the estimate for the patients receivinghigh-intensity regimens was 44.6% (95% CI: 26.5–64.5%) at a median followup of 24 months. Since the95% CIs for these estimates do not overlap, this sug-gests a substantially higher rate of progression-free sur-vival for patients receiving intermediate-intensityregimens. This advantage occurred despite thesepatients having a longer median follow up than thepatients receiving high-intensity regimens, whichwould make it less likely to find an advantage for inter-mediate-intensity regimens. This advantage was found
Table 2. Quality scale and scores of included studies evaluating progression-free survival
ECRI study quality scale: questions
Study
Xu
et al.15Ni
et al.14Saccardi
et al.16Samijn
et al.21Saiz
et al.18Burt
et al.22Nash
et al.23Fassas
et al.20
Was performance among patients at
baseline similar among patients who
entered the study as compared to study
completers?
Y Y Y Y Y Y Y Y
For all other important factors, were the
characteristics of patients at baseline
similar among those who entered the
study as compared to study completers?
Y Y Y Y Y Y Y Y
Did the study enroll all suitable patients /
consecutive patients?
Y Y Y Y Y Y Y Y
Was the study prospectively planned? Y Y Y Y Y Y Y Y
Did �5% receive ancillary treatment? Y Y Y Y N Y Y Y
Was compliance with treatment �85%? Y Y Y Y Y Y Y Y
Were outcomes measured by independent
assessors?
NR NR NR NR Y NR NR NR
Was the outcome measure of interest
objective and was it objectively
measured?
N N N N N N N N
Was a standard instrument used to mea-
sure the outcome?
Y Y Y Y Y Y Y Y
Did �85% of patients complete the study? NR NR NR NR Y N Y Y
Was the funding for this study derived
from a source that would not benefit
financially from results in a particular
direction?
Y Y Y Y Y Y Y Y
Quality score 8.2 8.2 8.2 8.2 8.2 7.7 8.6 8.6
Quality rating Moderate
N, no; Y, yes; NR, not reported.
208 Multiple Sclerosis Journal 17(2)
by guest on May 22, 2011msj.sagepub.comDownloaded from

to be robust by sensitivity analyses, so the strength ofevidence for this comparison is moderate.
Although the majority of patients in the immunoa-blative therapy studies had SPMS, we performed amore specific analysis by excluding data from patientswith other types of MS (data not shown). We did thisfor the four intermediate-intensity studies that reportedresults separately by type of MS. At a median followupof 38 months, the summary progression-free survivalrate was almost identical to that observed in the origi-nal analysis using all patients (81.9%; 95% CI: 69.4–90.0%). A similar analysis using only SPMS patientsfrom the three studies that used TBI as part of theconditioning regimen also yielded findings similar tothe all-patient analysis; progression-free survival wasonly 37.4% (21.3–57%) at a median followup of24 months. As before, the 95% CIs for the twogroups of studies do not overlap, suggesting that inter-mediate-intensity regimens lead to better progression-free survival than high-intensity regimens in patientswith SPMS. This finding was robust, which means thestrength of evidence for the difference between regimensis moderate. There were too few patients with othertypes of MS to allow conclusions from separate sub-group analyses of PPMS, RRMS, and PRMS.
Morbidities and mortality
Twelve prospective case series (n¼ 250) stud-ies,14-23,25,27-29 one retrospective case series (n¼ 9),24
and one retrospective database study (n¼ 169 evaluablepatients)26,30 that met our inclusion criteria reported onadverse events (no minimum followup period wasrequired). However, the variability in methods forreporting adverse events, failure to report the absenceof unobserved but potential adverse events in somestudies, inconsistent reporting or definitions of events,and absence of control groups precluded our pooling ofadverse event data for meta-analysis. Thus, to addressthis question we catalogued all of the reported adverseevents. Fever was the most frequently reported eventoccurring during the mobilization and conditioningphase of autologous HCT. Fever, engraftment syn-drome, enteritis, and transient neurological worseningwere the most frequently reported complications occur-ring within 6 months of autologous HCT.
A total of seven treatment-related deaths wererecorded in the 13 case series with post-treatmentfollow up, with the leading cause being pneumonia(three cases; Table 4). Six non-treatment-relateddeaths also occurred; five of these were associatedwith disease progression. Two of the three studiesthat reported mortality related to disease progressionused high-intensity conditioning regimens. In the retro-spective database study, a total of 15 deaths occurred:9 treatment-related (5.3%) and 6 non-treatment-relateddeaths (3.5%). The leading cause of treatment-relateddeath was infection (four cases), and the only reportedcause of non-treatment-related death was disease pro-gression (six cases).
Table 3. Progression-free survival in studies with different conditioning regimens compared with placebo reference controls
Study
Number of patients
for which data was reported
Progression-free survival
at median followup Median followup
Studies with Intermediate-intensity Conditioning Regimen (BEAM or Carmustine)
Ni et al.14,a 21 75% (n¼ 16/21) 42 months (Range: 6–65)
Xu et al.15 22 77% (n¼ 17/22) 39 months (Range: 6–59)
Saccardi et al.16,17 21 95% (n¼ 20/21) 36 months (Range: 12–72)
Saiz et al.18,19 14 85.7% (n¼ 12/14) 36 months (Range: 19–55)
Fassas et al.20 24 75%* (n¼ 18/24) 40 months (Range: 21–51)
Summary 102 79.4% (95% CI: 69.9–86.5%) 39 months (Range: 6–72 months)
Studies with High-intensity Conditioning Regimen (TBI)
Samijn et al.21 14 36% (n¼ 5/14) 36 months (Range: 7–36)
Burt et al.22 21 33.3%* (n¼ 7/21) 24 months (Range: 6–60)
Nash et al.23 26 62.5%* (n¼ 15/24) 24 months (Range: 6–36)
Summary 61 44.6% (95% CI: 26.5–64.3%) 24 months (Range: 6–60 months)
aNi et al.14 used the BEAM regimen on 20/21 patients; the remaining patient received CYþTBI. We considered this an intermediate-intensity regimen
study because all but one patient received BEAM.
*Calculated by ECRI Institute based on our definition of progression (increase in Expanded Disability Status Scale [EDSS] score of �1 if baseline EDSS
score is �5, increase in EDSS score of �0.5 if baseline EDSS score >5). Death from any cause was included in these calculations.
BEAM, etoposide, melphalan, carmustine, and cytosine arabinosode; CY, cyclophosphamide; TBI, total body irradiation.
Reston et al. 209
by guest on May 22, 2011msj.sagepub.comDownloaded from
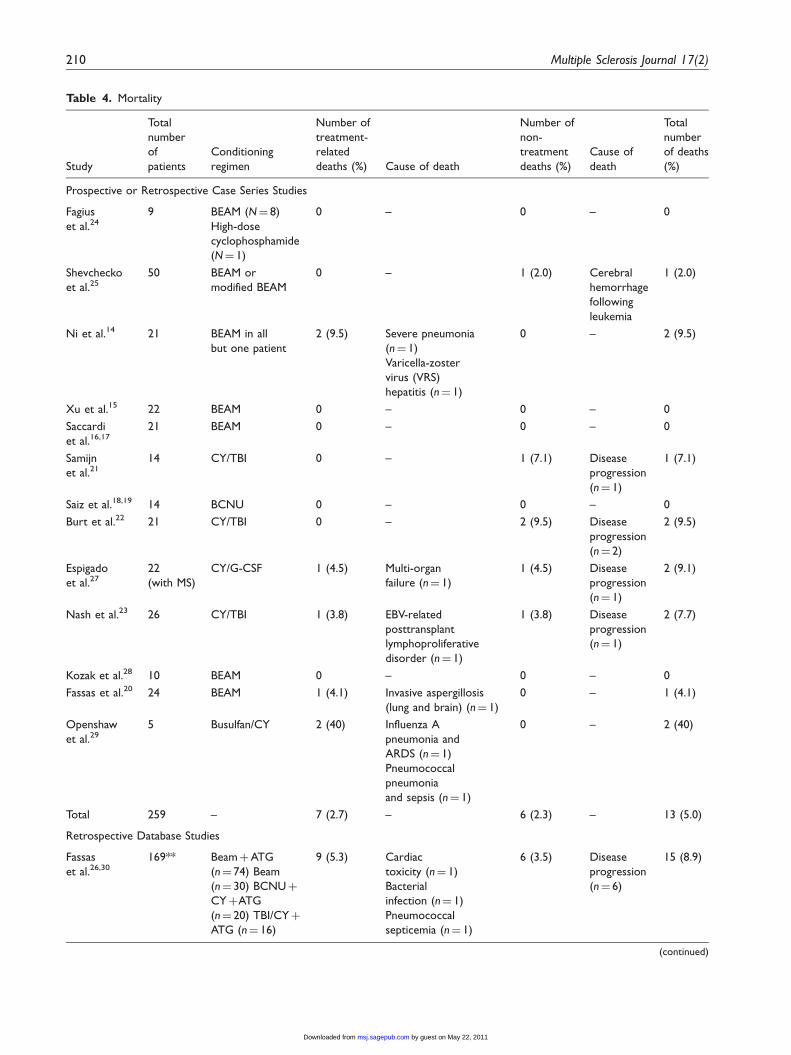
Table 4. Mortality
Study
Total
number
of
patients
Conditioning
regimen
Number of
treatment-
related
deaths (%) Cause of death
Number of
non-
treatment
deaths (%)
Cause of
death
Total
number
of deaths
(%)
Prospective or Retrospective Case Series Studies
Fagius
et al.249 BEAM (N¼ 8)
High-dose
cyclophosphamide
(N¼ 1)
0 – 0 – 0
Shevchecko
et al.2550 BEAM or
modified BEAM
0 – 1 (2.0) Cerebral
hemorrhage
following
leukemia
1 (2.0)
Ni et al.14 21 BEAM in all
but one patient
2 (9.5) Severe pneumonia
(n¼ 1)
Varicella-zoster
virus (VRS)
hepatitis (n¼ 1)
0 – 2 (9.5)
Xu et al.15 22 BEAM 0 – 0 – 0
Saccardi
et al.16,1721 BEAM 0 – 0 – 0
Samijn
et al.2114 CY/TBI 0 – 1 (7.1) Disease
progression
(n¼ 1)
1 (7.1)
Saiz et al.18,19 14 BCNU 0 – 0 – 0
Burt et al.22 21 CY/TBI 0 – 2 (9.5) Disease
progression
(n¼ 2)
2 (9.5)
Espigado
et al.2722
(with MS)
CY/G-CSF 1 (4.5) Multi-organ
failure (n¼ 1)
1 (4.5) Disease
progression
(n¼ 1)
2 (9.1)
Nash et al.23 26 CY/TBI 1 (3.8) EBV-related
posttransplant
lymphoproliferative
disorder (n¼ 1)
1 (3.8) Disease
progression
(n¼ 1)
2 (7.7)
Kozak et al.28 10 BEAM 0 – 0 – 0
Fassas et al.20 24 BEAM 1 (4.1) Invasive aspergillosis
(lung and brain) (n¼ 1)
0 – 1 (4.1)
Openshaw
et al.295 Busulfan/CY 2 (40) Influenza A
pneumonia and
ARDS (n¼ 1)
Pneumococcal
pneumonia
and sepsis (n¼ 1)
0 – 2 (40)
Total 259 – 7 (2.7) – 6 (2.3) – 13 (5.0)
Retrospective Database Studies
Fassas
et al.26,30169** BeamþATG
(n¼ 74) Beam
(n¼ 30) BCNUþ
CYþATG
(n¼ 20) TBI/CYþ
ATG (n¼ 16)
9 (5.3) Cardiac
toxicity (n¼ 1)
Bacterial
infection (n¼ 1)
Pneumococcal
septicemia (n¼ 1)
6 (3.5) Disease
progression
(n¼ 6)
15 (8.9)
(continued)
210 Multiple Sclerosis Journal 17(2)
by guest on May 22, 2011msj.sagepub.comDownloaded from

Discussion
Immunoablative therapy has an associated risk of treat-ment-related mortality (about 2.7% in our analysis),mostly due to increased vulnerability to infections.A recent review of the European Bone MarrowTransplant (EBMT) database reported that the treat-ment-related mortality rate has decreased to 1.3% forpatients treated during 2001–2007. The reviewers sug-gest that the decreased mortality is most likely due tothe avoidance of high-intensity conditioning regimensand better patient selection.4 It is unclear whether thisrisk of treatment-related mortality is offset by longer-term decreases in mortality related to disease progres-sion, a question that may require controlled studies fora definitive answer. However, patients at risk of pro-gression to severe disability who have not responded toconventional medical therapy may be willing to accepta low risk of treatment-related mortality to improve orstabilize their symptoms.
The finding that high-intensity regimens using TBIare associated with lower progression-free survival ratescompared with intermediate-intensity conditioningregimens suggests that regimens using BEAM orcarmustine are more appropriate for patients with pro-gressive MS. This difference occurred despite the longerfollowup in intermediate-intensity studies (mean 37.4months versus mean 24.8 months in high-intensitystudies), which decreased the chances of survival with-out progression in the intermediate-intensity studiescompared with the high-intensity studies. Althoughthis finding has not been confirmed in an analysis ofpatients in the EBMT registry,26 a much lower percent-age of patients in the registry (9%) had received TBIcompared with the patients in the case series used in ouranalysis (34.8%). Therefore, the EBMT analysis
probably lacked the statistical power to detect a differ-ence in outcome for TBI versus other conditioning reg-imens. Regardless, the authors of a recent review4
discussed the EBMT database and stated that high-intensity regimens ‘do not result in a better neurologicaloutcome than do intermediate-intensity regimens’.
A possible explanation for why high-intensity regi-mens using TBI may lead to lower progression-freesurvival than intermediate-intensity regimens is thatthe neurotoxicity of the high-intensity TBI plus CYregimen could lead to increased axonal damage anddegeneration in patients with progressive MS, therebycontributing to disease progression.21,22 We note thatthe study that used the lowest total radiation dose hadthe highest progression-free survival rate of the threestudies that used high-intensity regimens;23 conversely,the study with the highest total radiation dose had thelowest progression-free survival rate.22
Since the three studies that represented high-inten-sity conditioning regimens in our primary analysis allused TBI, we cannot rule out the possibility that thefindings might have differed if alternative high-intensityregimens (e.g. busulfan) had been used in these studies.However, a multivariate analysis of the EBMT registryfound that full-dose busulfan regimens were signifi-cantly associated with higher rates of transplant-relatedmortality (p¼ 0.001) in patients with progressive MS.26
This suggests that the negative effects of high-intensityconditioning regimens are not confined solely to regi-mens using TBI.
Authors of another recent systematic review per-formed a qualitative assessment of the evidence andconcluded that high-dose immunosuppressive therapyfollowed by autologous HCT for MS should be doneearly while the disease is inflammatory and with anintermediate-intensity conditioning regimen, such as
Table 4. Continued
Study
Total
number
of
patients
Conditioning
regimen
Number of
treatment-
related
deaths (%) Cause of death
Number of
non-
treatment
deaths (%)
Cause of
death
Total
number
of deaths
(%)
BusulfanþATG
(n¼ 10) Others
(n¼ 19) Unknown
(n¼ 9) N’s based
on total study
population,
not on evaluable
patients.
Influenza (n¼ 1)
Cerebral asperigillosis
(n¼ 1) Infection,
neurologic deterioration
(n¼ 3) Acquired factor
VIII inhibitor (n¼ 1)
**Evaluable number of patients.
ATG, antilymphocyte globulins; BCNU, carmustine; BEAM, etoposide, melphalan, carmustine, and cytosine arabinosode; CY, cyclophosphamide; EBV,
Epstein–Barr virus; G-CSF, granulocyte colony stimulating factor; TBI, total body irradiation.
Reston et al. 211
by guest on May 22, 2011msj.sagepub.comDownloaded from

BEAM, which has been associated with a lower risk oftreatment-related toxicity.31
The major limitation of this analysis is the lack ofcontrolled studies (randomized or non-randomized); todate, the only published evidence concerning immunoa-blative therapy for MS consists of case series andretrospective database studies. However, the patientsin these studies had not responded to conventionalmedical therapy, which decreases the likelihood thatpatients would remain progression-free 2–3 years afterimmunoablative therapy. Furthermore, a substantialproportion (45%) of patients who received intermedi-ate-intensity regimens not only stabilized but showedimprovement (as measured by decreased EDSS score)at last followup compared with baseline (data notshown). In contrast, only 9.2% of patients who receivedhigh-intensity regimens showed improvement at lastfollowup (data not shown).
Nevertheless, the lack of randomized trials directlycomparing the two conditioning regimens increases thechance that the included study groups receiving high-intensity regimens might differ from study groupsreceiving intermediate-intensity regimens with respectto unknown prognostic factors. Another limitation isthe lack of controlled studies comparing patients whoreceived immunoablative therapy plus autologous HCTto similar patients who did not undergo this treatment.This type of study would be necessary to assess therelative benefit of autologous HCT compared to alter-native treatment or no treatment.
Finally, the EDSS has a number of shortcomings asa measurement of disability. It has been criticized asbeing unresponsive to changes in disease activity dueto its bimodal distribution, with patients tending toscore at the low or higher ranges of the scale withrelatively few in the mid-ranges.32 The median EDSSscore in some of the included studies was in the less-responsive mid-range of the scale. Other limitations ofthe EDSS include poor reproducibility between differ-ent evaluators and inability to measure disability of theupper limbs or cognitive decline.32
Because relatively few patients with PPMS, PRMS,and RRMS have thus far received immunoablativetherapy with stem cell transplants, it is not yet possibleto determine whether patients with these subtypes ofMS have better outcomes with intermediate-intensityconditioning regimens compared to high-intensity con-ditioning regimens. Future studies should evaluatemore patients with these other types of MS.
Acknowledgements
We wish to thank the following individuals: Dr James Bowen(Clinical Associate Professor of Neurology, University of
Washington) for a helpful review of the manuscript; Jen deRichmond at ECRI Institute for performing the literature
search; and Lydia Dharia at the ECRI Institute for assistancein preparing this manuscript.
Funding
This study was funded in part by Department of DefenseTRICARE Management Activity under general contract
H94002-05-D-0003 and by ECRI Institute.
Conflict of interest statement
None declared.
References
1. Peterson JW and Trapp BD. Neuropathobiology of mul-
tiple sclerosis. Neurol Clin 2005; 23: 107–129, vi-vii.2. National MS Society. The disease-modifying drugs.
Newly diagnosed, 2008. Available at: http://www.natio-
nalmssociety.org/download.aspx?id¼45.3. Oksenberg JR and Hauser SL. Genetics of multiple scle-
rosis. Neurol Clin 2005; 23: 61–75, vi.
4. Mancardi G and Saccardi R. Autologous haematopoieticstem-cell transplantation in multiple sclerosis. LancetNeurol 2008; 7: 626–636.
5. Atkins H and FreedmanM. Immunoablative therapy as a
treatment aggressive multiple sclerosis. Neurol Clin 2005;23: 273–300, ix.
6. Griffith LM, Pavletic SZ, Tyndall A, Bredeson CN,
Bowen JD, Childs RW, et al. Feasibility of allogeneichematopoietic stem cell transplantation for autoimmunedisease: position statement from a National Institute of
Allergy and Infectious Diseases and National CancerInstitute—sponsored international workshop. Bethesda,MD, March 12 and 13, 2005. Biol Blood Marrow
Transplant 2005; 11: 862–870.7. Treadwell JT, Tregear SJ, Reston JT and Turkelson CM.
A system for rating the stability and strength of medicalevidence. BMC Med Res Methodol 2006; 6: 52. Available
at: http://www.biomedcentral.com/1471–2288/6/52.8. DerSimonian R and Laird N. Meta-analysis in clinical
trials. Control Clin Trials 1986; 7: 177–188.
9. Borenstein M, Hedges L, Higgins J and Rothstein H.Comprehensive Meta-analysis, Version 2. EnglewoodCliffs, NJ: Biostat, 2005. Available at: http://www.meta-
analysis.com/pages/about_us.html.10. Borenstein M, Hedges L, Higgins J and Rothstein H.
Introduction to Meta-analysis. Hoboken, NJ: JohnWiley & Sons, Inc, 2009.
11. Higgins JP, Thompson SG, Deeks JJ and Altman DG.Measuring inconsistency in meta-analyses. BMJ 2003;327: 557–560.
12. Higgins JP and Thompson SG. Quantifying heterogene-ity in a meta-analysis. Stat Med 2002; 21: 1539–1558.
13. Higgins JP and Thompson SG. Controlling the risk of
spurious findings from meta-regression. Stat Med 2004;23: 1663–1682.
14. Ni XS, Ouyang J, Zhu WH, Wang C and Chen B.
Autologous hematopoietic stem cell transplantation forprogressive multiple sclerosis: report of efficacy andsafety at three yr of follow up in 21 patients. ClinTransplant 2006; 20: 485–489.
212 Multiple Sclerosis Journal 17(2)
by guest on May 22, 2011msj.sagepub.comDownloaded from
15. Xu J, Ji BX, Su L, Dong HQ, Sun XJ and Liu CY.Clinical outcomes after autologous haematopoietic stemcell transplantation in patients with progressive multiple
sclerosis. Chin Med J (Engl) 2006; 119: 1851–1855.16. Saccardi R, Mancardi GL, Solari A, Bosi A, Bruzzi P, Di
Bartolomeo P, et al. Autologous HSCT for severe pro-gressive multiple sclerosis in a multicenter trial: impact on
disease activity and quality of life. Blood 2005; 105:2601–2607.
17. Capello E, Saccardi R, Murialdo A, Gualandi F, Pagliai
F, Bacigalupo A, et al. Italian GITMO-Neuro Intergroupon ASCT for Multiple Sclerosis. Intense immunosuppres-sion followed by autologous stem cell transplantation in
severe multiple sclerosis. Neurol Sci 2005; 26(Suppl 4):S200–S203.
18. Saiz A, Blanco Y, Carreras E, Berenguer J, Rovira M,
Pujol T, et al. Clinical and MRI outcome after autolo-gous hematopoietic stem cell transplantation in MS.Neurology 2004; 62: 282–284.
19. Carreras E, Saiz A, Marin P, Martinez C, Rovira M,
Villamor N, et al. CD34þ selected autologous peripheralblood stem cell transplantation for multiple sclerosis:report of toxicity and treatment results at one year of
follow-up in 15 patients. Haematologica 2003; 88:306–314.
20. Fassas A, Anagnostopoulos A, Kazis A, Kapinas K,
Sakellari I, Kimiskidis V, et al. Autologous stem celltransplantation in progressive multiple sclerosis—aninterim analysis of efficacy. J Clin Immunol 2000; 20:24–30.
21. Samijn JP, te Boekhorst PA, Mondria T, van Doom PA,Flach HZ, van der Meche FG, et al. Intense T cell deple-tion followed by autologous bone marrow transplanta-
tion for severe multiple sclerosis. J Neurol NeurosurgPsychiatry 2006; 77: 46–50.
22. Burt RK, Cohen BA, Russell E, Spero K, Joshi A,
Oyama Y, et al. Hematopoietic stem cell transplantationfor progressive multiple sclerosis: failure of a total bodyirradiation-based conditioning regimen to prevent disease
progression in patients with high disability scores. Blood2003; 102: 2373–2378.
23. Nash RA, Bowen JD, McSweeney PA, Pavletic SZ,Maravilla KR, Park MS, et al. High-dose immunosup-
pressive therapy and autologous peripheral blood stem
cell transplantation for severe multiple sclerosis. Blood2003; 102: 2364–2372.
24. Fagius J, Lundgren J and Oberg G. Early highly aggres-
sive MS successfully treated by hematopoietic stem celltransplantation. Mult Scler 2009; 15: 229–237.
25. Shevchenko YL, Novik AA, Kuznetsov AN, AfanasievBV, Lisukov IA, Kozlov VA, et al. High-dose immuno-
suppressive therapy with autologous hematopoietic stemcell transplantation as a treatment option in multiple scle-rosis. Exp Hematol 2008; 36: 922–928.
26. Saccardi R, Kozak T, Bocelli-Tyndall C, Fassas A, KazisA, Havrdova E, et al. Autologous stem cell transplanta-tion for progressive multiple sclerosis: update of the
European Group for Blood and MarrowTransplantation autoimmune diseases working partydatabase. Mult Scler 2006; 12: 814–823.
27. Espigado I, Marin-Niebla A, Rovira M, Julia A,Rodriguez JM, Altes A, et al. Phase I/II trials of autolo-gous peripheral blood stem cell transplantation in auto-immune diseases resistant to conventional therapy:
preliminary results from the Spanish experience.Transplant Proc 2003; 35: 742–743.
28. Kozak T, Havrdova E, Pit’ha J, Gregora E, Pytlik R,
Maaloufova J, et al. Immunoablative therapy with autol-ogous stem cell transplantation in the treatment of poorrisk multiple sclerosis. Transplant Proc 2001; 33:
2179–2181.29. Openshaw H, Lund BT, Kashyap A, Atkinson R,
Sniecinski I, Weiner LP, et al. Peripheral blood stemcell transplantation in multiple sclerosis with busulfan
and cyclophosphamide conditioning: report of toxicityand immunological monitoring. Biol Blood MarrowTransplant 2000; 6: 563–575.
30. Fassas A, Passweg JR, Anagnostopoulos A, Kazis A,Kozak T, Havrdova E, et al. Hematopoietic stem celltransplantation for multiple sclerosis. A retrospective
multicenter study. J Neurol 2002; 249: 1088–1097.31. Burt RK, Loh Y, Pearce W, Beohar N, Barr WG, Craig
R, et al. Clinical applications of blood-derived and
marrow-derived stem cells for nonmalignant diseases.JAMA 2008; 299: 925–936.
32. Joy JE, Johnston Jr RB (Eds) Multiple Sclerosis: CurrentStatus and Strategies for the Future. National Academy
Press, 2001.
Reston et al. 213
by guest on May 22, 2011msj.sagepub.comDownloaded from
Related Documents











