Race and Outcomes of Autologous Hematopoietic Cell Transplantation for Multiple Myeloma PN Hari, MD, MS 1 , NS Majhail, MD, MS 2,3 , M-J Zhang, PhD 1 , A Hassebroek, MPH 2 , F Siddiqui, MD 4 , K Ballen, MD 5 , A Bashey, MD, PhD 6 , J Bird, MD 7 , CO Freytes, MD 8 , J Gibson, MD, PhD 9 , G Hale, MD 10 , L Holmberg, MD, PhD 11 , R Kamble, MD 12 , RA Kyle, MD 13 , HM Lazarus, MD 14 , CF LeMaistre, MD 15 , F Loberiza, MD, MS 16 , A Maiolino, MD, PhD 17 , PL McCarthy, MD 18 , G Milone, MD 19 , N Omondi 20 , DE Reece, MD 21 , M Seftel, MD 22 , M Trigg, MD 23 , D Vesole, MD, PhD 24 , B Weiss, MD 25 , P Wiernik, MD 26 , SJ Lee, MD, MPH 11 , JD Rizzo, MD, MS 1 , and P Mehta, MD 27 1 Center for International Blood and Marrow Transplant Research, Medical College of Wisconsin, Milwaukee WI 2 Center for International Blood and Marrow Transplant Research, National Marrow Donor Program, Minneapolis MN 3 University of Minnesota, Minneapolis MN 4 Medical College of Wisconsin 5 Massachusetts General Hospital, Boston MA 6 Blood and Marrow Transplant Group of Georgia, Atlanta GA 7 Bristol Haematology And Oncology Centre, Bristol UK 8 South Texas Veterans Health Care System and University of Texas Health Center at San Antonio, San Antonio TX 9 Royal Prince Alfred Hospital, Camperdown, Australia 10 A Children’s Hospital, Saint Petersburg FL 11 Fred Hutchinson Cancer Research Center, Seattle WA 12 Baylor College of Medicine, Houston TX 13 Mayo Clinic, Rochester MN 14 University Hospitals Case Medical Center, Cleveland OH 15 Texas Transplant Institute, San Antonio TX 16 University of Nebraska Medical Center, Omaha NE 17 Hospital Univarstario Clementino Frago Filho, Rio de Janeiro Brazil 18 Roswell Park Cancer Institute, Buffalo NY Address for correspondence: Parameswaran Hari, MD, MS, CIBMTR, Medical College of Wisconsin, PO Box 26509, 8701 Watertown Plank Road, Milwaukee, WI 53226, Telephone: 414-805-4604, Fax: 414-805-4606, [email protected]. Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting typesetting and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. NIH Public Access Author Manuscript Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1. Published in final edited form as: Biol Blood Marrow Transplant. 2010 March ; 16(3): 395–402. doi:10.1016/j.bbmt.2009.11.007. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Race and Outcomes of Autologous Hematopoietic CellTransplantation for Multiple Myeloma
PN Hari, MD, MS1, NS Majhail, MD, MS2,3, M-J Zhang, PhD1, A Hassebroek, MPH2, F Siddiqui,MD4, K Ballen, MD5, A Bashey, MD, PhD6, J Bird, MD7, CO Freytes, MD8, J Gibson, MD,PhD9, G Hale, MD10, L Holmberg, MD, PhD11, R Kamble, MD12, RA Kyle, MD13, HM Lazarus,MD14, CF LeMaistre, MD15, F Loberiza, MD, MS16, A Maiolino, MD, PhD17, PL McCarthy,MD18, G Milone, MD19, N Omondi20, DE Reece, MD21, M Seftel, MD22, M Trigg, MD23, DVesole, MD, PhD24, B Weiss, MD25, P Wiernik, MD26, SJ Lee, MD, MPH11, JD Rizzo, MD,MS1, and P Mehta, MD271 Center for International Blood and Marrow Transplant Research, Medical College of Wisconsin,Milwaukee WI2 Center for International Blood and Marrow Transplant Research, National Marrow Donor Program,Minneapolis MN3 University of Minnesota, Minneapolis MN4 Medical College of Wisconsin5 Massachusetts General Hospital, Boston MA6 Blood and Marrow Transplant Group of Georgia, Atlanta GA7 Bristol Haematology And Oncology Centre, Bristol UK8 South Texas Veterans Health Care System and University of Texas Health Center at San Antonio,San Antonio TX9 Royal Prince Alfred Hospital, Camperdown, Australia10 A Children’s Hospital, Saint Petersburg FL11 Fred Hutchinson Cancer Research Center, Seattle WA12 Baylor College of Medicine, Houston TX13 Mayo Clinic, Rochester MN14 University Hospitals Case Medical Center, Cleveland OH15 Texas Transplant Institute, San Antonio TX16 University of Nebraska Medical Center, Omaha NE17 Hospital Univarstario Clementino Frago Filho, Rio de Janeiro Brazil18 Roswell Park Cancer Institute, Buffalo NY
Address for correspondence: Parameswaran Hari, MD, MS, CIBMTR, Medical College of Wisconsin, PO Box 26509, 8701 WatertownPlank Road, Milwaukee, WI 53226, Telephone: 414-805-4604, Fax: 414-805-4606, [email protected]'s Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customerswe are providing this early version of the manuscript. The manuscript will undergo copyediting typesetting and review of the resultingproof before it is published in its final citable form. Please note that during the production process errors may be discovered which couldaffect the content, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptBiol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
Published in final edited form as:Biol Blood Marrow Transplant. 2010 March ; 16(3): 395–402. doi:10.1016/j.bbmt.2009.11.007.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

19 Angelica Ocampo-Hospital and Research Center, Fundaleu Buenos Aires Argentina20 National Marrow Donor Program, Minneapolis MN21 University of Toronto, Toronto Ontario Canada22 CancerCare Manitoba, Manitoba Canada23 Merck & Co. Inc., Wilmington DE24 Loyola University Health System, Maywood IL25 Walter Reed Army Medical Center, Washington DC26 New York Medical College, Bronx NY27 University of Arkansas, Little Rock AR
AbstractBlacks are twice as likely to develop and die from multiple myeloma (MM) and are less likely toreceive an autologous hematopoietic-cell transplant (AHCT) for MM compared to whites. Theinfluence of race on outcomes of AHCT for MM is not well described. We compared the probabilityof overall survival, progression-free survival, disease progression and non-relapse mortality amongblack (N=303) and white (N=1892) recipients of AHCT for MM, who were reported to the Centerfor International Blood and Marrow Transplant Research (CIBMTR) from 1995 to 2005. The blackcohort was more likely to be female, had better Karnofsky performance scores but lower hemoglobinand albumin levels at diagnosis. Black recipients were younger and more likely to be transplantedlater in their disease course. Disease stage and treatment characteristics prior to AHCT were similarbetween the two groups. Black and white recipients had similar probabilities of 5-year overallsurvival (52% vs. 47%, P=0.19) and progression-free survival (19% vs. 21%, P=0.64) as well ascumulative incidences of disease progression (72% vs. 72%, P=0.97) and non-relapse mortality (9%vs. 8%, P=0.52). In multivariate analyses, race was not associated with any of these endpoints. Blackrecipients of AHCT for MM have similar outcomes compared to whites, suggesting that the reasonsunderlying lower rates of AHCT in blacks need to be studied further to ensure equal access to effectivetherapy.
KeywordsAutologous hematopoietic cell transplantation; multiple myeloma; race; survival; progression-freesurvival
BackgroundMultiple myeloma (MM) remains an incurable disease, although prognosis has improved inthe past decade.1,2 It is the most common hematologic malignancy among blacks and is theonly hematologic malignancy that is more frequent in this racial group compared with whites.In the United States, myeloma and its precursor disease monoclonal gammopathy ofundetermined significance (MGUS) are twice as common in blacks (annual incidence of14.4/100,000 in men and 9.8/100,000 in women compared with 6.6/100,000 in white men and4.1/100,000 in white women).1,3–7 Proposed factors to explain the increased incidence amongblacks include socioeconomic factors, greater exposure to hazardous materials, geneticpredisposition, greater degree of background antigenic stimulation, and a greater prevalenceof obesity.8–10 Mortality rates from MM in the United States are twice as high for blackscompared to whites (8.3/100,000 for men and 6.0/100,000 for women compared to 4.3/100,000and 2.8/100,000 for white men and women, respectively).11
Hari et al. Page 2
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Socioeconomic factors that may impact access to cancer therapy and therapeutic choicesinclude place of residence, distance from care centers, unemployment, availability and qualityof health insurance, poor nutrition, exposure to infectious agents, lower educational level andannual income.12,13 Prior comparisons have drawn conflicting conclusions on treatmentoutcomes among blacks compared with white patients with MM. Savage et al found that blackpatients had shorter survival times following similar therapy for MM. Presentation at laterstages of disease, socioeconomic factors or differential access to care were thought to explainthis disparity.13,14 Other investigators have suggested that these disparities in outcomes areprimarily due to biological characteristics.15,16
Randomized clinical trials support the use of AHCT as a standard therapy for MM.17,18 Wehave previously shown that blacks are less likely to receive AHCT for MM compared withtheir age and sex matched white counterparts.19 In the current study, we compared outcomesbetween black and white patients receiving AHCT for MM to determine if disparate posttransplant outcomes validate lower AHCT use in blacks.
Patients and MethodsThe Center for International Blood and Marrow Transplant Research (CIBMTR) consists of avoluntary working group of more than 450 transplant centers worldwide. Centers contributedetailed data on consecutive allogeneic and autologous transplants to a statistical center ateither the Medical College of Wisconsin in Milwaukee or the National Marrow Donor ProgramCoordinating Center in Minneapolis. Subjects are followed longitudinally, with yearly follow-up. Computerized checks for errors, physicians’ review of submitted data and on-site audits ofparticipating centers ensure data quality. Observational studies conducted by the CIBMTR aredone with a waiver of informed consent and in compliance with HIPAA regulations asdetermined by the Institutional Review Board and the Privacy Officer of the Medical Collegeof Wisconsin.
PatientsThe study included 2195 (303 black and 1892 white) adult (age ≥ 18 years) recipients of AHCTfor MM who were transplanted between January 1995 and June 2005 (Table 1). Only recipientsof peripheral blood AHCT were included in this study; patients who had received plannedtandem AHCT (N=582) were excluded. Centers obtained information about patient race andthen reported it to the CIBMTR.
Statistical MethodsPatient-, disease- and treatment-related factors were compared between the black and whitecohorts, using Chi-square test for categorical and Kruskal-Wallis test for continuous variables.Outcomes analyzed included non-relapse mortality (NRM), relapse/progression, progression-free survival (PFS) and overall survival (OS). NRM was defined as death occurring in theabsence of relapse or progression of MM following AHCT. Responses, relapse/progressionwere defined according to standard criteria20. Chemotherapy sensitivity was defined asachievement of a partial or complete response to pretransplant therapy. PFS was defined assurvival without disease progression or relapse. Patients alive and with no evidence of diseaseprogression or relapse were censored at the time of last follow-up. The survival interval variablewas defined as time from the date of transplant to the date of death or last contact andsummarized by a survival curve. Probabilities of OS and PFS were calculated using the Kaplan-Meier estimator.21,22 NRM and relapse/progression were calculated using cumulativeincidence estimates. The log-rank test was used for univariate comparisons.
Hari et al. Page 3
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
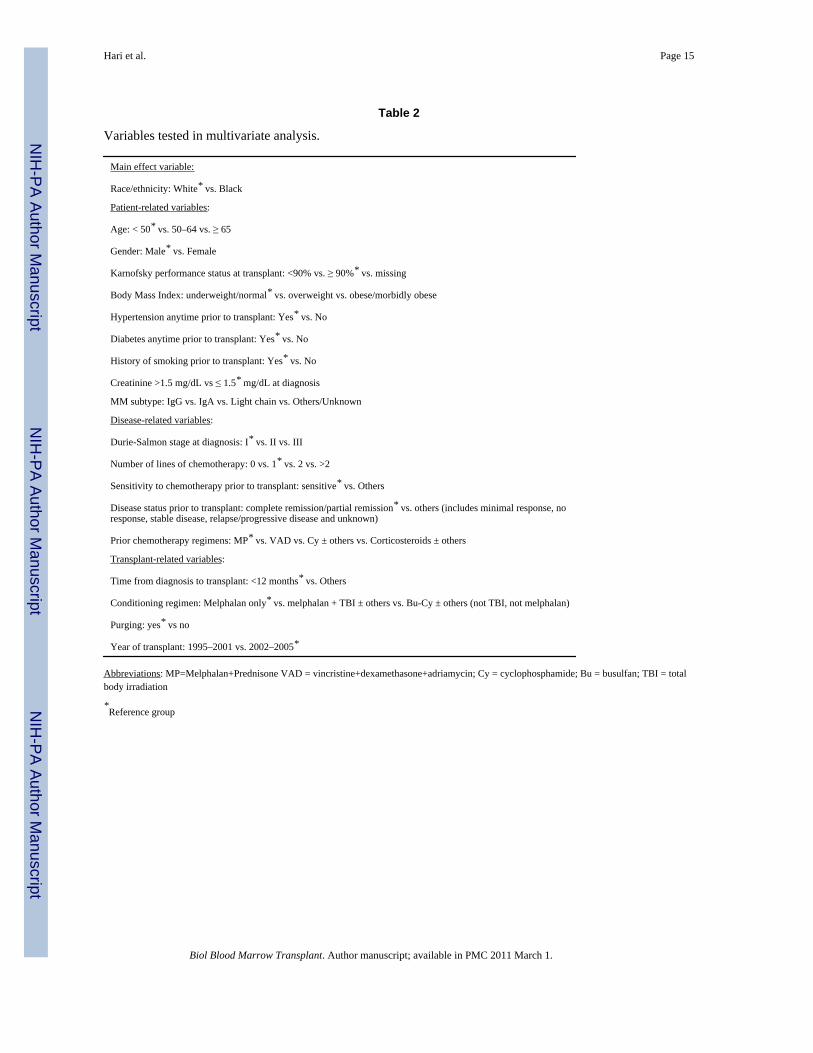
Multivariate Cox proportional hazards regression was used to examine the outcomes betweenblack and white patient cohorts and to identify risk factors associated with outcomes.23 Astepwise forward selection multivariate model was built to identify covariates that influencedoutcomes. Any covariate with a P-value < 0.05 was considered significant. The proportionalityassumption for Cox regression was tested by adding a time-dependent covariate for each riskfactor and each outcome. Tests indicated that all variables met the proportional hazardsassumption. Results were expressed as relative risks (RR). Any risk factors found to besignificant were adjusted in the final Cox model. The main effect tested (i.e. black vs. white)was included in all models. The variables considered in multivariate analyses are summarizedin table 2. Analyses were performed using SAS software, version 9.1 (SAS Institute, Cary,NC).
ResultsPatient Characteristics
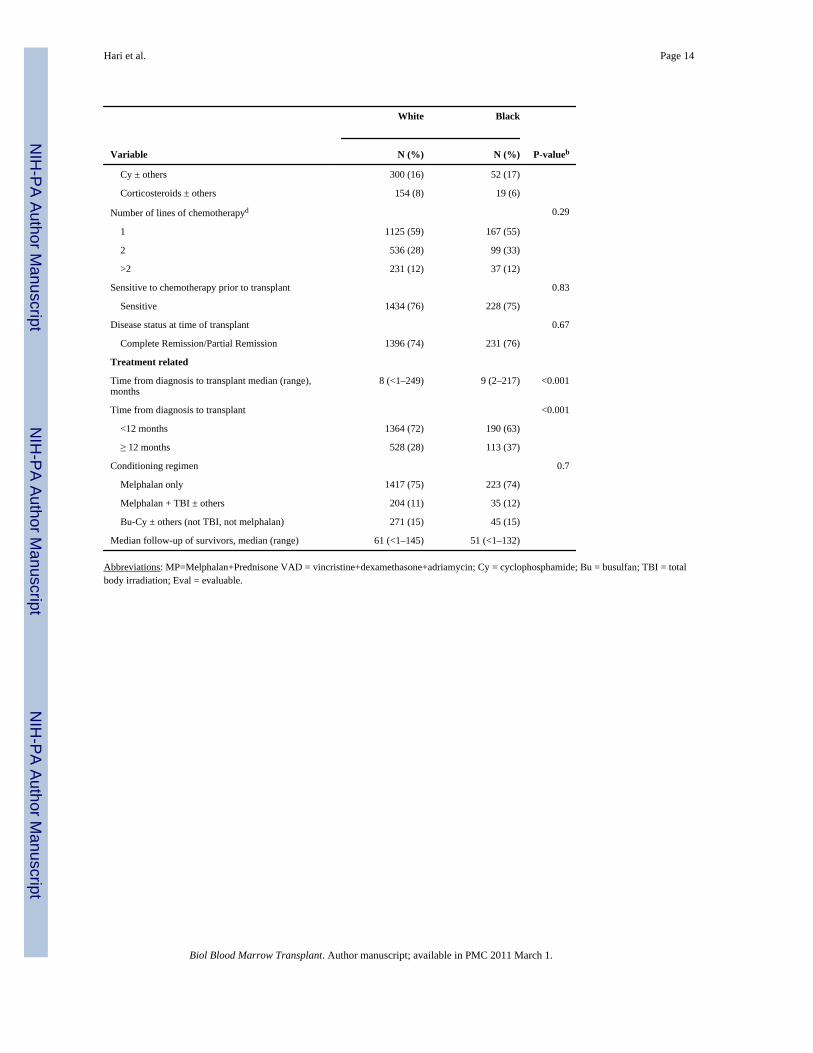
Table 1 shows the characteristics of all patients evaluated. Median ages at AHCT were 55 yearsfor black compared to 57 years for white patients (p<0.001). The black cohort had a higherproportion of females and patients with Karnofsky performance status scores (KPS) > 90 (69% vs. 61%, p=0.005). Blacks were more likely to have co-morbidities such as hypertension(47% vs. 25%, p<0.001), diabetes mellitus (17% vs. 9%, p<0.001), and obesity (38%vs. 31%,p=0.01). No statistically significant differences in disease stage or MM subtype were identified.Blacks were also more likely to have a lower hemoglobin (Hb <10 g/dL in 45% vs. 29%,p<0.001) at diagnosis. No significant differences in the levels of serum creatinine, beta-2microglobulin, calcium or marrow plasmacytosis were identified. The cohorts did not differwith respect to the type and number of prior therapies or sensitivity to therapies applied beforetransplantation. Blacks were transplanted later in the disease course, with 37% receiving AHCTa year or more from diagnosis vs. 28% in whites (p<0.001). There were no significantdifferences in conditioning regimens used or the receipt of a salvage second AHCT.
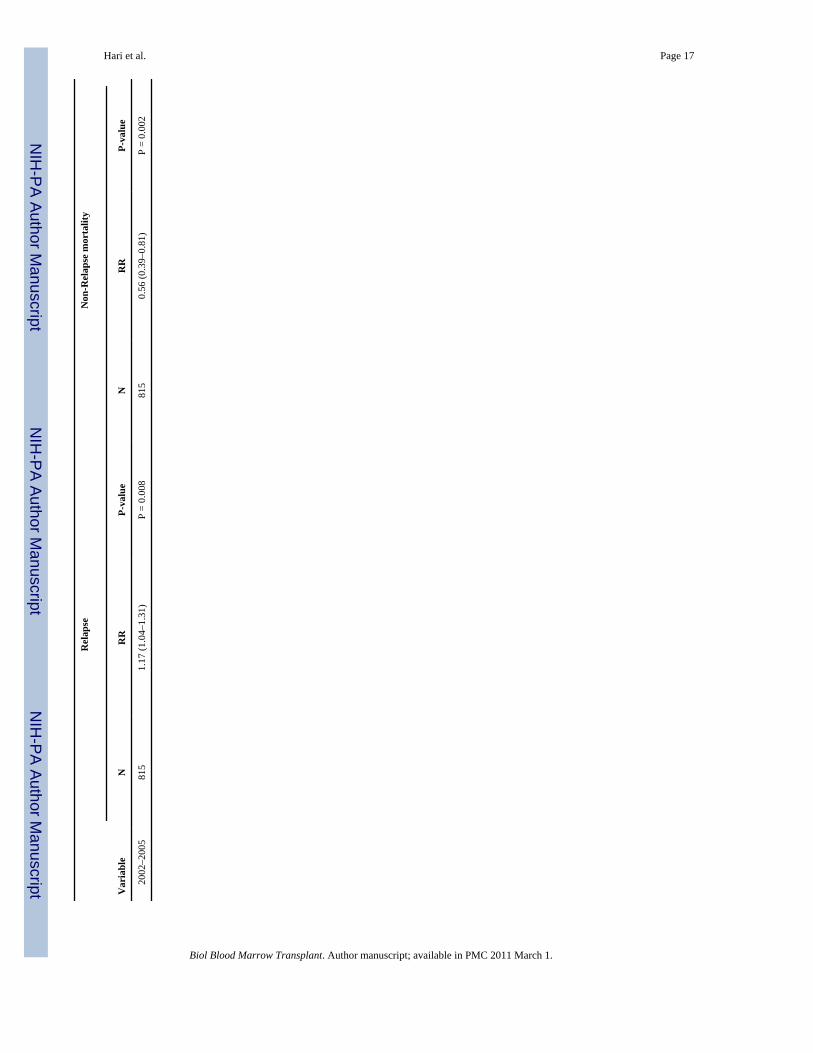
Non-relapse Mortality and Relapse/ProgressionFigure 1 shows the cumulative incidence of NRM. The cumulative incidence of NRM wassimilar in both groups. At 1 year was 5% (95% CI 4–6%) in whites vs. 3% (95% CI 2–6%) inblacks. At 5 years it was 8% (95% CI 7–9%) vs. 9% (95% CI 6–14%) in whites and blacksrespectively. In multivariate analysis (Table 3), race was not associated with NRM. Factorsassociated with an increased risk of NRM were age ≥ 65 years, KPS <90 and AHCT prior to2002.
Figure 2 shows cumulative incidence of relapse/progression. The cumulative incidence ofrelapse/progression was similar in both groups. At 1 year it was 27% (95% CI 25–29%) inwhites vs. 28% (95% CI 23–34%) in blacks. At 5 years it was 72% (95% CI 69–74%) vs. 72%(95% CI 65–78%) in whites and blacks respectively. In multivariate analysis (Table 3), racewas not associated with disease relapse or progression. Factors associated with an increasedrisk of relapse included KPS score < 90, Durie-Salmon stage III at diagnosis, receipt of 3 ormore lines of chemotherapy before AHCT, lack of chemosensitive disease prior to AHCT,AHCT ≥ 12 months from diagnosis and later year of AHCT.
Progression-free Survival and Overall SurvivalFigure 3 shows the probability of PFS. The 1 and 5 year probabilities of PFS were similar inboth groups. At 1 year it was 68% (95% CI 66–70%) in whites vs. 68% (95% CI 63–74%) inblacks. At 5 years it was 21% (95% CI 18–23%) vs. 19% (95% CI 14–25%) in whites andblacks respectively. In multivariate analysis (Table 4), race was not associated with PFS.
Hari et al. Page 4
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4 shows the probability of overall survival after AHCT. The 1 and 5 year survival rateswere also similar between the two cohorts. At 1 year it was 87% (95% CI 85–88%) in whitesvs. 90% (95% CI 87–93%) in blacks. At 5 years it was 47% (95% CI 44–49%) vs. 52% (95%CI 45–59%) in whites and blacks respectively. In multivariate analysis (Table 4), race was nota significant predictor of survival.
PFS and overall survival were worse in patients with older age at AHCT (>50 years), KPSscore <90, higher Durie-Salmon stage, those who received two or more lines of therapy priorto AHCT, AHCT ≥ 12 months from diagnosis and chemotherapy resistant disease (Table 4).Overall survival was also lower in patients who underwent AHCT prior to 2002.
The major cause of mortality in both cohorts was relapse or progression of MM that accountedfor 72% of all deaths.
DiscussionOur analysis establishes that black and whites have very similar outcomes after AHCT forMM. These results concur with observations in other studies of non-transplant therapy that thedisparity in outcomes for MM disappears when blacks receive identical therapy.28
Several investigators have shown that blacks have outcomes similar to whites when given thesame non-transplant treatment for MM. Rohatgi et al showed that blacks were less likely toreceive chemotherapy but they responded with similar outcomes when given similar non-transplant therapy for MM.24 In the pre-transplant era, Modiano et al. retrospectively evaluatedthe impact of race in the results of the SWOG 8829 study of conventional chemotherapy forMM.25 From 99 study sites in the US, 116 black and 467 white patients were shown to havesimilar median survival (32 and 30 months, respectively). There were no differences by stageor MM subtype. A smaller study from the Department of Defense equal access health caresystem, reported on the outcomes of 36 black and 55 white newly diagnosed patients receivingAHCT for MM and observed comparable outcomes between the two groups.26 In their study,there were no differences in the stage, hemoglobin, calcium or creatinine levels, althoughblacks did have higher CRP levels and a trend for less skeletal involvement. The authorsrecommended a larger retrospective study such as the current one. Other single center analysescomparing black and white recipients of AHCT for MM have drawn conflicting conclusions.Khaled et al. analyzed 101 black patients and concluded that they were likely to relapse earlierafter AHCT.27 Survival was not compared in this study. Saraf et al. in their comparative studythat included 38 black and 32 white AHCT recipients, found that black patients had moreprolonged responses and greater event free survival.28
Unfortunately, there is ample evidence that blacks are less likely to receive chemotherapy forMM as well as AHCT. Rohatgi et al. reviewed patterns of chemotherapy use for patients withMM outside the clinical trial setting.24 From a population based retrospective cohort of 49,021patients of age 65 years or older with stage II or III MM, they found that only 52% receivedchemotherapy. Blacks were less likely to receive chemotherapy compared to whites (47.6%vs. 52.8%) despite evidence that use of chemotherapy decreased all cause mortality, myelomaspecific mortality and increased survival. 24 The reasons for the disparate access are unclear,since controlling for socioeconomic status did not eliminate the disparity in the receipt ofchemotherapy.
These disparities in the receipt of therapy occur in the transplant setting as well. Joshua et al,in a previous study from the CIBMTR demonstrate that whites are more likely to receive AHCTfor newly diagnosed MM compared to an age and sex adjusted black population.19 Using datafrom the SEER and CIBMTR registries, the study showed that age and sex adjusted odds ofreceiving AHCT for MM is 1.72 times greater in whites compared to blacks. Although our
Hari et al. Page 5
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

study cannot address the reasons for this under utilization of AHCT in blacks, interestingconclusions can be drawn regarding AHCT for MM in black patients.
It has been proposed that reduced access to treatment for myeloma may be related to actual orperceived worse outcomes in black patients. Our study clearly shows that outcomes are notdifferent between blacks and whites receiving AHCT for MM suggesting this treatmentmodality should be offered to all patients when medically appropriate. These results are inaccordance with a meta-analysis of patients treated for 14 different cancers, where survival inthe majority of cancers was similar between races when comparable treatment was given.29
The pre-transplant characteristics of black recipients of AHCT are interesting. The black cohortwas younger and had better performance status than the white cohort, despite higher rates ofanemia and other co- morbidities at diagnosis. These differences likely indicate a selection biasoperating against older black patients with lower KPS scores with regard to referral forconsideration of AHCT. Black patients were also likely to have had a longer time betweendiagnosis and transplantation compared to whites, while receiving a similar number ofchemotherapy regimens and having similar responses. This suggests delayed referral forconsideration of AHCT. A referral bias favoring only the healthiest black patients for transplantmay be in effect, while patients with less favorable clinical features may only be offered non-transplant or even non-treatment options.
The major strength of our study is the broad representation of transplant centers making it verylikely that these results are applicable to the transplant community as a whole. In this analysiswe are unable to draw any conclusions about factors associated with non-receipt of transplantin blacks since a non-transplant population is not represented. The characteristics of thepopulation of black MM patients not receiving AHCT need to be analyzed to identify the causesof a under utilization of AHCT. It is possible that many blacks who are not receiving stem-celltransplantation for myeloma are forgoing the transplant by choice. However it is also possiblethat referral bias, unequal access to tertiary care, compliance gap, reluctance to enter clinicaltrials and socioeconomic disparities account for some of the differences in utilization of AHCTfor patients with MM. With the demonstration of equal outcomes for black with MM, furtherstudy and definitive action to ensure better awareness and delivery of transplant options forthe black population is warranted.
AcknowledgmentsThe CIBMTR is supported by Public Health Service Grant/Cooperative Agreement U24-CA76518 from the NationalCancer Institute (NCI), the National Heart, Lung and Blood Institute (NHLBI) and the National Institute of Allergyand Infectious Diseases (NIAID); a Grant/Cooperative Agreement 5U01HL069294 from NHLBI and NCI; a contractHHSH234200637015C with Health Resources and Services Administration (HRSA/DHHS); two GrantsN00014-06-1-0704 and N00014-08-1-0058 from the Office of Naval Research; and grants from AABB; Aetna;American Society for Blood and Marrow Transplantation; Amgen, Inc.; Anonymous donation to the Medical Collegeof Wisconsin; Association of Medical Microbiology and Infectious Disease Canada; Astellas Pharma US, Inc.; BaxterInternational, Inc.; Bayer HealthCare Pharmaceuticals; BloodCenter of Wisconsin; Blue Cross and Blue ShieldAssociation; Bone Marrow Foundation; Canadian Blood and Marrow Transplant Group; Celgene Corporation;CellGenix, GmbH; Centers for Disease Control and Prevention; ClinImmune Labs; CTI Clinical Trial and ConsultingServices; Cubist Pharmaceuticals; Cylex Inc.; CytoTherm; DOR BioPharma, Inc.; Dynal Biotech, an InvitrogenCompany; Enzon Pharmaceuticals, Inc.; European Group for Blood and Marrow Transplantation; Gambro BCT, Inc.;Gamida Cell, Ltd.; Genzyme Corporation; Histogenetics, Inc.; HKS Medical Information Systems; Hospira, Inc.;Infectious Diseases Society of America; Kiadis Pharma; Kirin Brewery Co., Ltd.; Merck & Company; The MedicalCollege of Wisconsin; MGI Pharma, Inc.; Michigan Community Blood Centers; Millennium Pharmaceuticals, Inc.;Miller Pharmacal Group; Milliman USA, Inc.; Miltenyi Biotec, Inc.; National Marrow Donor Program; NaturePublishing Group; New York Blood Center; Novartis Oncology; Oncology Nursing Society; Osiris Therapeutics, Inc.;Otsuka Pharmaceutical Development & Commercialization, Inc.; Pall Life Sciences; PDL BioPharma, Inc; Pfizer Inc;Pharmion Corporation; Saladax Biomedical, Inc.; Schering Plough Corporation; Society for Healthcare Epidemiologyof America; StemCyte, Inc.; StemSoft Software, Inc.; Sysmex; Teva Pharmaceutical Industries; The MarrowFoundation; THERAKOS, Inc.; Vidacare Corporation; Vion Pharmaceuticals, Inc.; ViraCor Laboratories;ViroPharma, Inc.; and Wellpoint, Inc. The views expressed in this article do not reflect the official policy or position
Hari et al. Page 6
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
of the National Institute of Health, the Department of the Navy, the Department of Defense, or any other agency ofthe U.S. Government.
References1. Kyle RA, Rajkumar SV. Epidemiology of the plasma-cell disorders. Best Pract Res Clin Haematol
Dec;2007 20(4):637–664. [PubMed: 18070711]2. Kumar SK, Rajkumar SV, Dispenzieri A, et al. Improved survival in multiple myeloma and the impact
of novel therapies. Blood Mar 1;2008 111(5):2516–2520. [PubMed: 17975015]3. Brown LM, Gridley G, Check D, Landgren O. Risk of multiple myeloma and monoclonal gammopathy
of undetermined significance among white and black male United States veterans with priorautoimmune, infectious, inflammatory, and allergic disorders. Blood Apr 1;2008 111(7):3388–3394.[PubMed: 18239085]
4. Landgren O, Gridley G, Turesson I, et al. Risk of monoclonal gammopathy of undeterminedsignificance (MGUS) and subsequent multiple myeloma among black and white veterans in the UnitedStates. Blood Feb 1;2006 107(3):904–906. [PubMed: 16210333]
5. Ries, L.; Melbert, D.; Krapcho, M., et al. SEER Cancer Statistics Review. National Cancer Institute;Bethesda, MD: 1975–2005 [accessed January 2009]. http://seer.cancer.gov/csr/1975_2005/, based onNovember 2007 SEER data submission, posted to the SEER web site, 2008. last
6. Singh J, Dudley AW Jr, Kulig KA. Increased incidence of monoclonal gammopathy of undeterminedsignificance in blacks and its age-related differences with whites on the basis of a study of 397 menand one woman in a hospital setting. J Lab Clin Med Dec;1990 116(6):785–789. [PubMed: 2246554]
7. Landgren O, Katzmann JA, Hsing AW, et al. Prevalence of monoclonal gammopathy of undeterminedsignificance among men in Ghana. Mayo Clin Proc Dec;2007 82(12):1468–1473. [PubMed:18053453]
8. Samanic C, Gridley G, Chow WH, Lubin J, Hoover RN, Fraumeni JF Jr. Obesity and cancer risk amongwhite and black United States veterans. Cancer Causes Control Feb;2004 15(1):35–43. [PubMed:14970733]
9. Benjamin M, Reddy S, Brawley OW. Myeloma and race: a review of the literature. Cancer MetastasisRev Mar;2003 22(1):87–93. [PubMed: 12716040]
10. Friedman GD, Herrinton LJ. Obesity and multiple myeloma. Cancer Causes Control Sep;1994 5(5):479–483. [PubMed: 7999970]
11. [accessed January 2009]. http://seer.cancer.gov/statfacts/html/mulmy.html. last12. Abou-Jawde RM, Baz R, Walker E, et al. The role of race, socioeconomic status, and distance traveled
on the outcome of black patients with multiple myeloma. Haematologica Oct;2006 91(10):1410–1413. [PubMed: 16963396]
13. Savage D, Lindenbaum J, Van Ryzin J, Struening E, Garrett TJ. Race, poverty, and survival in multiplemyeloma. Cancer Dec 15;1984 54(12):3085–3094. [PubMed: 6498786]
14. Cella DF, Orav EJ, Kornblith AB, et al. Socioeconomic status and cancer survival. J Clin Oncol Aug;1991 9(8):1500–1509. [PubMed: 2072149]
15. Lyn D, Cherney BW, Lalande M, et al. A duplicated region is responsible for the poly(ADP-ribose)polymerase polymorphism, on chromosome 13, associated with a predisposition to cancer. Am JHum Genet Jan;1993 52(1):124–134. [PubMed: 8434580]
16. Cao J, Hong CH, Rosen L, et al. Deletion of genetic material from a poly(ADP-ribose) polymerase-like gene on chromosome 13 occurs frequently in patients with monoclonal gammopathies. CancerEpidemiol Biomarkers Prev Oct-Nov;1995 4(7):759–763. [PubMed: 8672993]
17. Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of autologous bone marrowtransplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myelome. N EnglJ Med Jul 11;1996 335(2):91–97. [PubMed: 8649495]
18. Child JA, Morgan GJ, Davies FE, et al. High-dose chemotherapy with hematopoietic stem-cell rescuefor multiple myeloma. N Engl J Med May 8;2003 348(19):1875–1883. [PubMed: 12736280]
19. Joshua TV, Rizzo JD, Zhang MJ, Horowitz MM. Access to hematopoietic stem cell transplantation:Effect of race and gender. Biol Blood Marrow Transplant 2007;13(Suppl 2):22.
Hari et al. Page 7
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

20. Blade J, Samson D, Reece D, et al. Criteria for evaluating disease response and progression in patientswith multiple myeloma treated by high-dose therapy and haemopoietic stem cell transplantation.Myeloma Subcommittee of the EBMT. European Group for Blood and Marrow Transplant. Br JHaematol Sep;1998 102(5):1115–1123. [PubMed: 9753033]
21. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc1958;53:457–481.
22. Klein, JP.; Moeschberger, ML. Survival analysis: techniques for censored and truncated data. 2. NewYork: Springer Verlag; 2003.
23. Cox DR. Regression models and life tables. J R Stat Soc B 1972;34:187–220.24. Rohatgi N, Du XL, Coker AL, Moye LA, Wang M, Fang S. Chemotherapy and survival for patients
with multiple myeloma: findings from a large nationwide and population-based cohort. Am J ClinOncol Oct;2007 30(5):540–548. [PubMed: 17921717]
25. Modiano MR, Villar-Werstler P, Crowley J, Salmon SE. Evaluation of race as a prognostic factor inmultiple myeloma. An ancillary of Southwest Oncology Group Study 8229. J Clin Oncol Mar;199614(3):974–977. [PubMed: 8622048]
26. Verma PS, Howard RS, Weiss BM. The impact of race on outcomes of autologous transplantation inpatients with multiple myeloma. Am J Hematol May;2008 83(5):355–358. [PubMed: 18186525]
27. Khaled Y, Abidi MH, Janakiraman N, et al. Outcomes after auto-SCT in blacks with multiplemyeloma. Bone Marrow Transplant Jun;2009 43(11):845–851. [PubMed: 19139731]
28. Saraf S, Chen YH, Dobogai LC, et al. Prolonged responses after autologous stem cell transplantationin black patients with multiple myeloma. Bone Marrow Transplant Jun;2006 37(12):1099–1102.[PubMed: 16699527]
29. Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, Begg CB. Survival of blacks and whitesafter a cancer diagnosis. Jama Apr 24;2002 287(16):2106–2113. [PubMed: 11966385]
Hari et al. Page 8
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
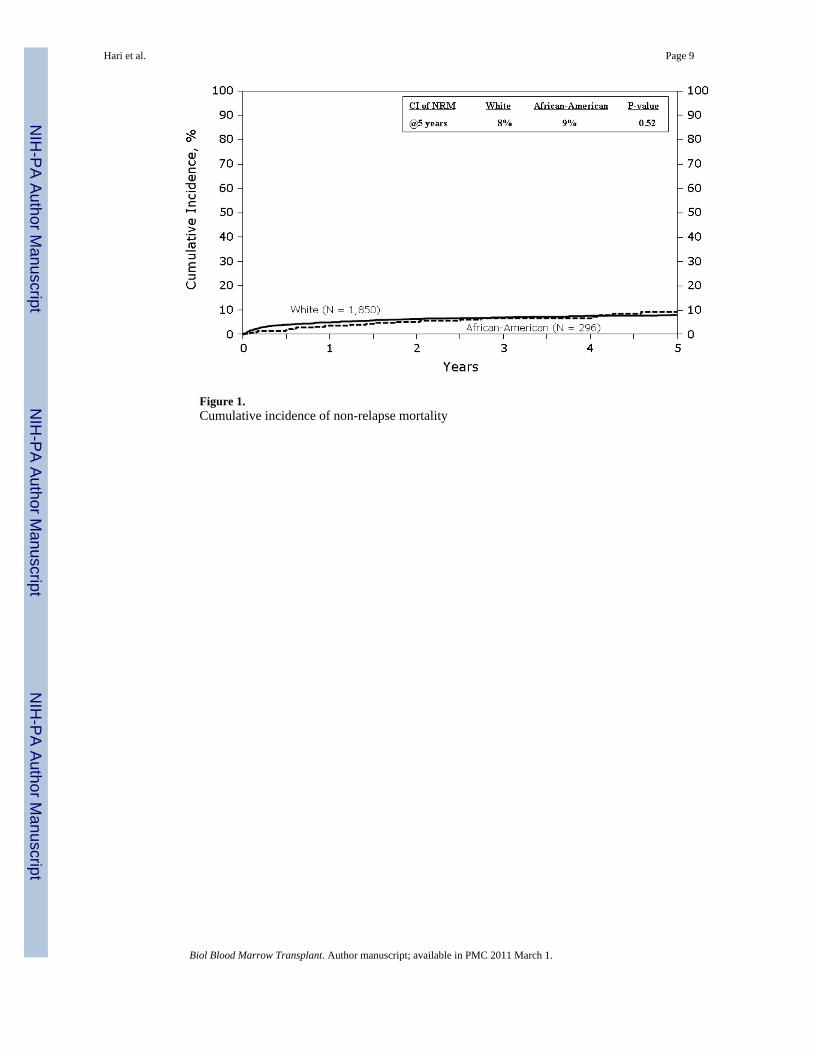
Figure 1.Cumulative incidence of non-relapse mortality
Hari et al. Page 9
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
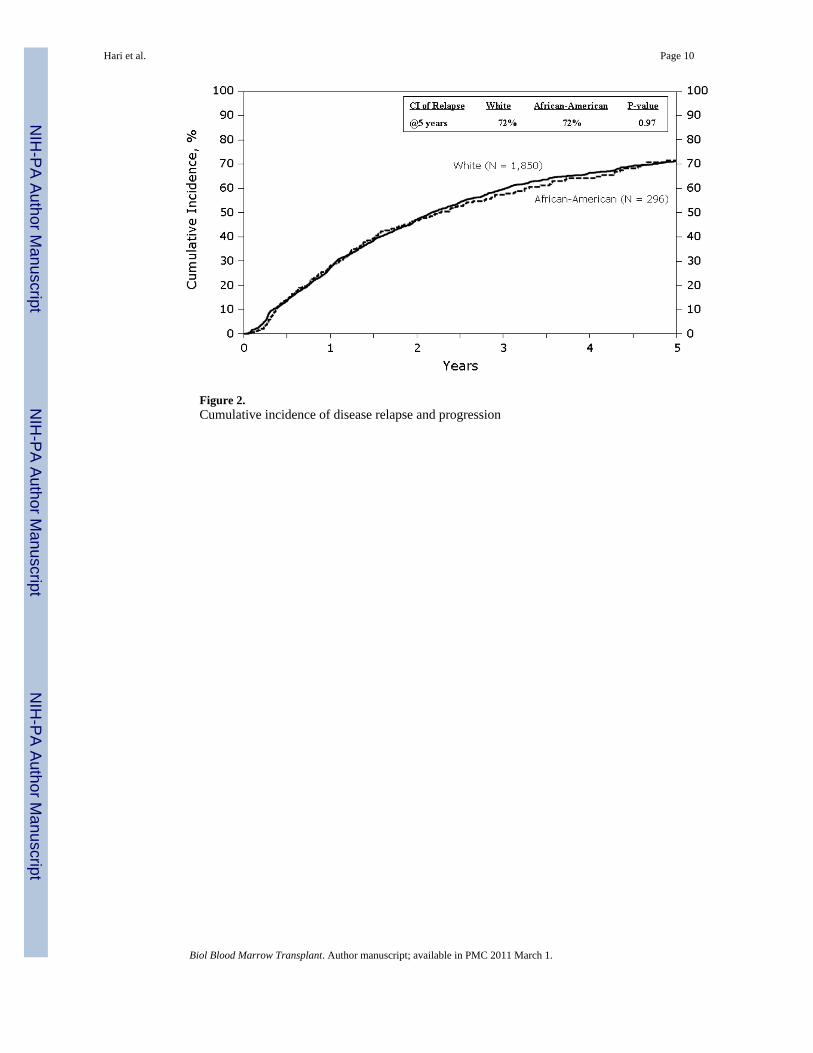
Figure 2.Cumulative incidence of disease relapse and progression
Hari et al. Page 10
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Probability of progression-free survival
Hari et al. Page 11
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 4.Probability of overall survival
Hari et al. Page 12
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 13
Table 1
Patient Characteristics
White Black
Variable N (%) N (%) P-valueb
Number of patientsa 1892 303
Age median (range), years 57 (27–80) 55 (27–74) <0.001
Age group at transplant, years 0.002
<50 396 (21) 88 (29)
50–64 1111 (59) 172 (57)
≥ 65 385 (20) 43 (14)
Male sex 1136 (60) 164 (54) 0.05
Karnofsky score pre-transplant 0.005
≥ 90 1153 (61) 210 (69)
Hypertension <0.001
Yes 471 (25) 143 (47)
Diabetes <0.001
Yes 169 (9) 50 (17)
Body Mass Index 0.01
Underweight/Normal (<25) 557 (29) 67 (22)
Overweight (25–29.9) 741 (39) 120 (40)
Obese/Morbidly Obese (≥ 30) 594 (31) 116 (38)
Disease related
Durie-Salmon stage at diagnosis 0.25
I 203 (11) 25 (8)
II 562 (30) 101 (33)
III 1127 (60) 177 (58)
Immunochemical subtype of myeloma 0.34
IgG 1003 (53) 173 (57)
IgA 359 (19) 45 (15)
Light chain 329 (17) 54 (18)
Others/Unknown 125 (11) 16 (10)
Albumin level at diagnosis 0.05
> 3.5 g/dL 732 (39) 101 (33)
Hemoglobin at diagnosis <10 g/dL <0.001
< 10 g/dL 552 (29) 135 (45)
Creatinine at diagnosis 0.09
>1.5 mg/dL 361 (19) 74 (24)
B-2 microglobulin level at diagnosis 0.83
≥ 5.5 mg/L 195 (10) 31 (10)
Prior chemotherapy regimens 0.78
MP ± others 334 (18) 50 (17)
VAD ± others (not MP) 1104 (58) 182 (60)
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 14
White Black
Variable N (%) N (%) P-valueb
Cy ± others 300 (16) 52 (17)
Corticosteroids ± others 154 (8) 19 (6)
Number of lines of chemotherapyd 0.29
1 1125 (59) 167 (55)
2 536 (28) 99 (33)
>2 231 (12) 37 (12)
Sensitive to chemotherapy prior to transplant 0.83
Sensitive 1434 (76) 228 (75)
Disease status at time of transplant 0.67
Complete Remission/Partial Remission 1396 (74) 231 (76)
Treatment related
Time from diagnosis to transplant median (range),months
8 (<1–249) 9 (2–217) <0.001
Time from diagnosis to transplant <0.001
<12 months 1364 (72) 190 (63)
≥ 12 months 528 (28) 113 (37)
Conditioning regimen 0.7
Melphalan only 1417 (75) 223 (74)
Melphalan + TBI ± others 204 (11) 35 (12)
Bu-Cy ± others (not TBI, not melphalan) 271 (15) 45 (15)
Median follow-up of survivors, median (range) 61 (<1–145) 51 (<1–132)
Abbreviations: MP=Melphalan+Prednisone VAD = vincristine+dexamethasone+adriamycin; Cy = cyclophosphamide; Bu = busulfan; TBI = totalbody irradiation; Eval = evaluable.
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 15
Table 2
Variables tested in multivariate analysis.
Main effect variable:
Race/ethnicity: White* vs. Black
Patient-related variables:
Age: < 50* vs. 50–64 vs. ≥ 65
Gender: Male* vs. Female
Karnofsky performance status at transplant: <90% vs. ≥ 90%* vs. missing
Body Mass Index: underweight/normal* vs. overweight vs. obese/morbidly obese
Hypertension anytime prior to transplant: Yes* vs. No
Diabetes anytime prior to transplant: Yes* vs. No
History of smoking prior to transplant: Yes* vs. No
Creatinine >1.5 mg/dL vs ≤ 1.5* mg/dL at diagnosis
MM subtype: IgG vs. IgA vs. Light chain vs. Others/Unknown
Disease-related variables:
Durie-Salmon stage at diagnosis: I* vs. II vs. III
Number of lines of chemotherapy: 0 vs. 1* vs. 2 vs. >2
Sensitivity to chemotherapy prior to transplant: sensitive* vs. Others
Disease status prior to transplant: complete remission/partial remission* vs. others (includes minimal response, noresponse, stable disease, relapse/progressive disease and unknown)
Prior chemotherapy regimens: MP* vs. VAD vs. Cy ± others vs. Corticosteroids ± others
Transplant-related variables:
Time from diagnosis to transplant: <12 months* vs. Others
Conditioning regimen: Melphalan only* vs. melphalan + TBI ± others vs. Bu-Cy ± others (not TBI, not melphalan)
Purging: yes* vs no
Year of transplant: 1995–2001 vs. 2002–2005*
Abbreviations: MP=Melphalan+Prednisone VAD = vincristine+dexamethasone+adriamycin; Cy = cyclophosphamide; Bu = busulfan; TBI = totalbody irradiation
*Reference group
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 16
Tabl
e 3
Mul
tivar
iate
ana
lysi
s for
rela
pse
and
non-
rela
pse
mor
talit
y
Rel
apse
Non
-Rel
apse
mor
talit
y
Var
iabl
eN
RR
P-va
lue
NR
RP-
valu
e
Rac
e
W
hite
1850
1.00
a18
501.
00a
B
lack
296
0.92
(0.7
8–1.
08)
P =
0.28
296
1.16
(0.7
5–1.
80)
P =
0.51
Patie
nt A
ge
<
5047
51.
00a
P <
0.00
1
50
–64
1253
1.55
(1.0
1–2.
39)
P =
0.05
≥
6541
83.
50 (2
.17–
5.65
)P
< 0.
001
Kar
nofs
ky S
core
prio
r to
cond
ition
ing
<9
081
51.
00a
815
1.00
a
≥
9013
310.
88 (0
.79–
0.98
)P
= 0.
0213
310.
72 (0
.53–
0.98
)P
= 0.
03
Dur
ie-S
alm
on st
age
at d
iagn
osis
I
222
1.00
aP
< 0.
001
222
1.00
aP
= 0.
004
II
652
1.23
(1.0
0–1.
51)
P =
0.05
652
0.61
(0.3
5–1.
06)
P =
0.08
II
I12
721.
54 (1
.27–
1.87
)P
< 0.
001
1272
1.16
(0.7
1–1.
88)
P =
0.56
Num
ber o
f lin
es o
f che
mot
hera
pyc
1
1256
1.00
aP
= 0.
001
2
628
1.12
(0.9
9–1.
27)
P =
0.07
>
226
21.
39 (1
.16–
1.66
)P
< 0.
001
Sens
itivi
ty to
che
mot
hera
py p
rior t
o tra
nspl
ant
O
ther
522
1.00
a
Se
nsiti
ve16
240.
76 (0
.67–
0.85
)P
< 0.
001
Tim
e fr
om d
iagn
osis
to tr
ansp
lant
<
12 m
onth
s15
191.
00a
≥
12 m
onth
s62
71.
19 (1
.04–
1.35
)P
= 0.
009
Yea
r of t
rans
plan
t
19
95–2
001
1331
1.00
a13
311.
00a
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 17
Rel
apse
Non
-Rel
apse
mor
talit
y
Var
iabl
eN
RR
P-va
lue
NR
RP-
valu
e
20
02–2
005
815
1.17
(1.0
4–1.
31)
P =
0.00
881
50.
56 (0
.39–
0.81
)P
= 0.
002
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Hari et al. Page 18
Tabl
e 4
Mul
tivar
iate
ana
lysi
s for
ove
rall
surv
ival
and
pro
gres
sion
-fre
e su
rviv
al
Ove
rall
Surv
ival
Prog
ress
ion-
free
surv
ival
Var
iabl
eN
RR
P-va
lue
NR
RP-
valu
e
Rac
e
W
hite
1892
1.00
a18
501.
00a
B
lack
303
0.94
(0.7
8–1.
13)
P =
0.50
296
0.94
(0.8
1–1.
09)
P =
0.39
Patie
nt A
ge
<
5048
41.
00a
Pb < 0
.000
147
51.
00a
P =
0.03
50
–64
1283
1.26
(1.0
9–1.
46)
P =
0.00
212
531.
12 (0
.99–
1.27
)P
= 0.
08
≥
6542
81.
52 (1
.26–
1.83
)P
< 0.
0001
418
1.24
(1.0
6–1.
46)
P =
0.00
7
Kar
nofs
ky S
core
prio
r to
cond
ition
ing
<9
083
21.
00a
815
1.00
a
≥
9013
630.
74 (0
.66–
0.83
)P
< 0.
0001
1331
0.87
(0.7
9–0.
97)
P =
0.00
9
Dur
ie-S
alm
on st
age
at d
iagn
osis
I
228
1.00
aPb <
0.0
001
222
1.00
aP
< 0.
0001
II
663
1.13
(0.8
9–1.
44)
P =
0.32
652
1.12
(0.9
3–1.
36)
P =
0.23
II
I13
041.
67 (1
.34–
2.09
)P
< 0.
0001
1272
1.49
(1.2
5–1.
79)
P <
0.00
01
Num
ber o
f lin
es o
f che
mot
hera
pyc
1
1292
1.00
aPb <
0.0
001
1256
1.00
aP
= 0.
0002
2
635
1.10
(0.9
6–1.
27)
P =
0.17
628
1.13
(1.0
0–1.
27)
P =
0.04
>
226
81.
66 (1
.37–
2.01
)P
< 0.
0001
262
1.41
(1.1
9–1.
67)
P <
0.00
01
Sens
itivi
ty to
che
mot
hera
py p
rior t
o tra
nspl
ant
O
ther
533
1.00
a52
21.
00a
Se
nsiti
ve16
620.
82 (0
.72–
0.94
)P
= 0.
003
1624
0.76
(0.6
8–0.
85)
P <
0.00
01
Tim
e fr
om d
iagn
osis
to tr
ansp
lant
<
12 m
onth
s15
541.
00a
1519
1.00
a
≥
12 m
onth
s64
11.
16 (1
.01–
1.34
)P
= 0.
0462
71.
16 (1
.03–
1.31
)P
= 0.
01
Biol Blood Marrow Transplant. Author manuscript; available in PMC 2011 March 1.
Related Documents