Proc. Natl. Acad. Sci. USA Vol. 92, pp. 3541-3545, April 1995 Immunology Autoimmunity in Chagas disease cardiopathy: Biological relevance of a cardiac myosin-specific epitope crossreactive to an immunodominant Trypanosoma cruzi antigen EDIECIO CUNHA_NETO*, MARCIA DURANTI*, ARTHUR GRUBERt, BIANCA ZINGALESt, IARA DE MESSIASt, NOEDIR STOLF§, GIovANNI BELLOTTI§, MANOEL E. PATARROYOI, FuLvIo PILLEGGI§, AND JORGE KALIL*II *Laboratory of Transplantation Immunology, §Divisions of Surgical and Clinical Cardiology, Instituto do Coracao, Sao Paulo University Hospital, Faculty of Medicine, and tlnstituto de Quimica, Universidade de Sao Paulo, Sao Paulo, SP, 05403-000, Brazil; tImmunopathology Laboratory, Hospital de Clinicas, University of Parana, Curitiba, Brazil; and Instituto de Inmunologia, Hospital San Juan de Dios, Universidad Nacional de Colombia, Bogota, Colombia Communicated by Jean Dausset, Centre d'Etude du Polymorphisme Humain, Paris, France, October 21, 1994 ABSTRACT Heart tissue destruction in chronic Chagas disease cardiopathy (CCC) may be caused by autoimmune recognition of heart tissue by a mononuclear cell infiltrate decades after Trypanosoma cruzi infection. Indirect evidence suggests that there is antigenic crossreactivity between T. cruzi and heart tissue. As there is evidence for immune recognition of cardiac myosin in CCC, we searched for a putative myosin-crossreactive T. cruzi antigen. T. cruzi lysate immunoblots were probed with anti-cardiac myosin heavy chain IgG antibodies (AMA) affinity-purified from CCC or asymptomatic Chagas disease patient-seropositive sera. A 140/116-kDa doublet was predominantly recognized by AMA from CCC sera. Further, recombinant T. cruzi protein B13- whose native protein is also a 140- and 116-kDa double band-was identified by crossreactive AMA. Among 28 sera tested in a dot-blot assay, AMA from 100%6 of CCC sera but only 14% of the asymptomatic Chagas disease sera recognized B13 protein (P = 2.3 x 10-6). Sequence homology to B13 protein was found at positions 8-13 and 1442-1447 of human cardiac myosin heavy chain. Competitive ELISA assays that used the correspondent myosin synthetic peptides to inhibit serum antibody binding to B13 protein identified the heart- specific AAALDK (1442-1447) sequence of human cardiac myosin heavy chain and the homologous AAAGDK B13 se- quence as the respective crossreactive epitopes. The recogni- tion of a heart-specific T. cruzi crossreactive epitope, in strong association with the presence of chronic heart lesions, sug- gests the involvement of crossreactivity between cardiac my- osin and B13 in the pathogenesis of CCC. Chagas disease (American trypanosomiasis), caused by the protozoan Trypanosoma cruzi, is endemic in many countries of Latin America, where 16-18 million people may be infected. Chronic Chagas disease cardiopathy (CCC), a dilated cardiom- yopathy with a T-cell-rich inflammatory infiltrate that often leads to a fatal course, develops in 25-30% of infected individuals 5-30 yr after primary infection (1). The remaining 60-70% chronically T. cruzi-infected individuals either remain asymptomatic ("indeterminate" patients, ASY) or develop denervation of parietal smooth muscle in the digestive tract (5-10%). The pathogenesis of heart lesions in CCC has been the issue of much debate. Several lines of evidence-including the inability to consistently find parasites in damaged areas (2) and the passive transfer of heart lesions by CD4+ T cells from T. cruzi-infected mice (3)-indicated that the inflammatory heart lesion could be of an autoimmune nature (4). According to the antigenic mimicry hypothesis, lymphocytes in the heart should recognize and mount delayed-type hyper- The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. §1734 solely to indicate this fact. sensitivity responses toward a tissue-specific heart component bearing structural similarities to a given T. cruzi antigen. Several investigators found autoantibody and self-reactive T-cell formation in human and experimental T cruzi infection (5, 6). Crossreactive autoantibodies were mainly directed toward ubiquitous and evolutionarily conserved molecules (7, 8). A recent report (9) demonstrated an epitope shared between a recombinant flagellar T. cruzi molecule (Fl 160) and an undefined 48-kDa neuronal protein. However, Fl 160-nerve crossreactive antibodies did not correlate to CCC or chronic digestive forms of human Chagas disease. Most T. cruzi-host tissue crossreactive antigen systems described seemed to lack clinico-biological significance, as indicated by a lack of target organ specificity of self-antigen as well as lack of correlation between antibody detection and different clinical forms of chronic Chagas disease. The recognition of myosin by CD4+ T cells in a murine model of CCC (10) revealed a prime candidate target autoan- tigen in CCC. Myosin heavy chain (myosin HC) is the most abundant heart protein-50% of total protein by weight (11)-and is recognized in many situations of heart-specific autoimmunity, such as rheumatic heart disease (12) and murine post-Coxsackie B3 autoimmune cardiomyopathy (13). The presence of antibody against cardiac myosin HC is cor- related to the development of chronic inflammatory cardio- pathy in T cruzi-infected mice (14). Immunization with cardiac myosin HC induces an aggressive myocarditis (15, 16). These reports prompted us to look for anti-cardiac myosin HC immune reactivity in CCC patients and search for a possible myosin crossreactive T. cruzi antigen. MATERIALS AND METHODS Patients. CCC patients (severe heart failure, dilated car- diomyopathy with a positive serology for T. cruzi, and all other causes excluded) in waiting list for cardiac transplantation were subjected to transvenous endomyocardial biopsy. Sample collection procedures have been cleared by the Committee of Ethics. Peripheral blood was collected from 24 CCC patients, as well as from 14 asymptomatic Chagas disease patient (ASY) individuals (clinically asymptomatic individuals seropositive to T. cruzi, with a normal electrocardiograph and heart sonog- raphy) from Instituto do Cora-ao and from Parana University Hospital outpatient clinics, as well as from 10 normal volun- teers. Sera from Duchenne muscle dystrophy patients were provided by Mayana Zatz, University of Sao Paulo. His- Abbreviations: CCC, chronic Chagas disease cardiopathy; ASY, asymptomatic Chagas disease patient; myosin HC, myosin heavy chain; AMA, anti-cardiac myosin HC IgG antibodies; NR, nonrelated pep- tide; pB13, 19-mer that encompasses all possible linear epitopes within the 12-mer tandem repeats of B13 protein. IlTo whom reprint requests should be addressed. 3541 Downloaded by guest on June 11, 2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Proc. Natl. Acad. Sci. USAVol. 92, pp. 3541-3545, April 1995Immunology
Autoimmunity in Chagas disease cardiopathy: Biological relevanceof a cardiac myosin-specific epitope crossreactive to animmunodominant Trypanosoma cruzi antigenEDIECIO CUNHA_NETO*, MARCIA DURANTI*, ARTHUR GRUBERt, BIANCA ZINGALESt, IARA DE MESSIASt,NOEDIR STOLF§, GIovANNI BELLOTTI§, MANOEL E. PATARROYOI, FuLvIo PILLEGGI§, AND JORGE KALIL*II*Laboratory of Transplantation Immunology, §Divisions of Surgical and Clinical Cardiology, Instituto do Coracao, Sao Paulo University Hospital, Faculty ofMedicine, and tlnstituto de Quimica, Universidade de Sao Paulo, Sao Paulo, SP, 05403-000, Brazil; tImmunopathology Laboratory, Hospital de Clinicas,University of Parana, Curitiba, Brazil; and Instituto de Inmunologia, Hospital San Juan de Dios, Universidad Nacional de Colombia, Bogota, Colombia
Communicated by Jean Dausset, Centre d'Etude du Polymorphisme Humain, Paris, France, October 21, 1994
ABSTRACT Heart tissue destruction in chronic Chagasdisease cardiopathy (CCC) may be caused by autoimmunerecognition of heart tissue by a mononuclear cell infiltratedecades after Trypanosoma cruzi infection. Indirect evidencesuggests that there is antigenic crossreactivity between T.cruzi and heart tissue. As there is evidence for immunerecognition of cardiac myosin in CCC, we searched for aputative myosin-crossreactive T. cruzi antigen. T. cruzi lysateimmunoblots were probed with anti-cardiac myosin heavychain IgG antibodies (AMA) affinity-purified from CCC orasymptomatic Chagas disease patient-seropositive sera. A140/116-kDa doublet was predominantly recognized by AMAfrom CCC sera. Further, recombinant T. cruzi protein B13-whose native protein is also a 140- and 116-kDa doubleband-was identified by crossreactive AMA. Among 28 seratested in a dot-blot assay, AMA from 100%6 of CCC sera butonly 14% of the asymptomatic Chagas disease sera recognizedB13 protein (P = 2.3 x 10-6). Sequence homology to B13protein was found at positions 8-13 and 1442-1447 of humancardiac myosin heavy chain. Competitive ELISA assays thatused the correspondent myosin synthetic peptides to inhibitserum antibody binding to B13 protein identified the heart-specific AAALDK (1442-1447) sequence of human cardiacmyosin heavy chain and the homologous AAAGDK B13 se-quence as the respective crossreactive epitopes. The recogni-tion of a heart-specific T. cruzi crossreactive epitope, in strongassociation with the presence of chronic heart lesions, sug-gests the involvement of crossreactivity between cardiac my-osin and B13 in the pathogenesis of CCC.
Chagas disease (American trypanosomiasis), caused by theprotozoan Trypanosoma cruzi, is endemic in many countries ofLatin America, where 16-18 million people may be infected.Chronic Chagas disease cardiopathy (CCC), a dilated cardiom-yopathy with a T-cell-rich inflammatory infiltrate that oftenleads to a fatal course, develops in 25-30% of infectedindividuals 5-30 yr after primary infection (1). The remaining60-70% chronically T. cruzi-infected individuals either remainasymptomatic ("indeterminate" patients, ASY) or developdenervation of parietal smooth muscle in the digestive tract(5-10%).The pathogenesis of heart lesions in CCC has been the issue
of much debate. Several lines of evidence-including theinability to consistently find parasites in damaged areas (2) andthe passive transfer of heart lesions by CD4+ T cells from T.cruzi-infected mice (3)-indicated that the inflammatory heartlesion could be of an autoimmune nature (4).According to the antigenic mimicry hypothesis, lymphocytes
in the heart should recognize and mount delayed-type hyper-
The publication costs of this article were defrayed in part by page chargepayment. This article must therefore be hereby marked "advertisement" inaccordance with 18 U.S.C. §1734 solely to indicate this fact.
sensitivity responses toward a tissue-specific heart componentbearing structural similarities to a given T. cruzi antigen.Several investigators found autoantibody and self-reactiveT-cell formation in human and experimental T cruzi infection(5, 6). Crossreactive autoantibodies were mainly directedtoward ubiquitous and evolutionarily conserved molecules (7,8). A recent report (9) demonstrated an epitope sharedbetween a recombinant flagellar T. cruzi molecule (Fl 160) andan undefined 48-kDa neuronal protein. However, Fl 160-nervecrossreactive antibodies did not correlate to CCC or chronicdigestive forms of human Chagas disease. Most T. cruzi-hosttissue crossreactive antigen systems described seemed to lackclinico-biological significance, as indicated by a lack of targetorgan specificity of self-antigen as well as lack of correlationbetween antibody detection and different clinical forms ofchronic Chagas disease.The recognition of myosin by CD4+ T cells in a murine
model of CCC (10) revealed a prime candidate target autoan-tigen in CCC. Myosin heavy chain (myosin HC) is the mostabundant heart protein-50% of total protein by weight(11)-and is recognized in many situations of heart-specificautoimmunity, such as rheumatic heart disease (12) andmurine post-Coxsackie B3 autoimmune cardiomyopathy (13).The presence of antibody against cardiac myosin HC is cor-related to the development of chronic inflammatory cardio-pathy in T cruzi-infected mice (14). Immunization with cardiacmyosin HC induces an aggressive myocarditis (15, 16). Thesereports prompted us to look for anti-cardiac myosin HCimmune reactivity in CCC patients and search for a possiblemyosin crossreactive T. cruzi antigen.
MATERIALS AND METHODSPatients. CCC patients (severe heart failure, dilated car-
diomyopathy with a positive serology for T. cruzi, and all othercauses excluded) in waiting list for cardiac transplantationwere subjected to transvenous endomyocardial biopsy. Samplecollection procedures have been cleared by the Committee ofEthics. Peripheral blood was collected from 24 CCC patients,as well as from 14 asymptomatic Chagas disease patient (ASY)individuals (clinically asymptomatic individuals seropositive toT. cruzi, with a normal electrocardiograph and heart sonog-raphy) from Instituto do Cora-ao and from Parana UniversityHospital outpatient clinics, as well as from 10 normal volun-teers. Sera from Duchenne muscle dystrophy patients wereprovided by Mayana Zatz, University of Sao Paulo. His-
Abbreviations: CCC, chronic Chagas disease cardiopathy; ASY,asymptomatic Chagas disease patient; myosin HC, myosin heavy chain;AMA, anti-cardiac myosin HC IgG antibodies; NR, nonrelated pep-tide; pB13, 19-mer that encompasses all possible linear epitopes withinthe 12-mer tandem repeats of B13 protein.IlTo whom reprint requests should be addressed.
3541
Dow
nloa
ded
by g
uest
on
June
11,
202
1
-
3542 Immunology: Cunha-Neto et al
topathological scoring for myocarditis of biopsy samples wasdone as described (17).
Antigens. Purified human cardiac myosin (for ELISA), aswell as myosin-rich 0.3 M KCl soluble fraction of hearthomogenate (for immunoblots and immunosorbent prepara-tion), was obtained from normal human heart ventriculartissue of an organ donor as described (18). After SDS/7.5%PAGE (19), the myosin-rich heart lysate was electroblotted tonitrocellulose sheets (20). Cardiac myosin HC-containing ni-trocellulose strips (major 210-kDa protein band) were used asimmunosorbents. Tissue culture-derived T. cruzi Y straintrypomastigotes obtained from infected LLC-MK2 cell linemonolayers (21) were fractionated by SDS/7.5% PAGE in thepresence of 2-mercaptoethanol, being subsequently trans-ferred to nitrocellulose sheets (20).Recombinant T. cruzi Antigen. The recombinant T. cruzi
clone B13 was originally isolated from a Agtll expressionlibrary, as described (22). The insert of B13 was subcloned invector pMSgtll, in phase with the lacZ gene. The expressedfusion protein B13 and ,B-galactosidase were affinity-purifiedon p-aminophenyl-f3-D-galactopyranoside-agarose columns.B13 recombinant protein contains 16 tandemly repeated 12-amino acid motifs. A rabbit antiserum to B13 protein wasobtained as described (22).
Synthetic Peptides. Peptides were synthesized with the"teabag" method (23), HPLC-purified, and sequenced. Table1 lists the peptides used, including a 19-mer that encompassesall possible linear epitopes (24) within the 12-mer tandemrepeats of B13 protein (pB13) (22). In addition, 9-mer B13peptides (S1-6) were designed in "sliding window" fashion(25) for epitope mapping. Peptides pl-20 and p1439-1453 arederived from the sequence of human cardiac myosin HC, (3isoform, and contain B13-homologous sequences (bold-facedtype). The nonrelated peptide (NR) represents residues 22-41of the human T-cell receptor variable-region a-subunit 13chain.
Affinity Purification of Anti-Cardiac Myosin HC Antibod-ies (AMA). Immunoselection of specific antibodies was doneas described (26). After adequate blocking, myosin HC im-munosorbents (50 ,ug of myosin per strip) were incubatedovernight at 4°C with 1.5 ml of a 1:10 dilution of each serumsample. Bound antibodies were eluted with 0.02 M glycine, pH2.8, neutralized with 1 M Tris, pH 8.6, and reconstituted toTris-buffered saline/1% nonfat milk. Each AMA preparationwas tested for specific anti-myosin HC IgG antibody activity byincubation with human heart lysate immunoblots.Immunoblots. Immunoblots were done as described (20).
Briefly, electroblotted nitrocellulose strips were incubatedovernight at 4°C with either AMA obtained from individualsera or 1:40 dilutions of unfractionated sera, followed by goat
Table 1. Synthetic peptides
PeptidesB13-derivedpB13SiS2S3S4S5S6
Human cardiac myosinHC-derivedpl-20p1439-1453
Human T-cell receptorVa chainNR
GDKPSLFGQAAAGDKPSLFGDKPSLFGQ
KPSLFGQAASLFGQAAAGFGQAAAGDK
QAAAGDKPSAAGDKPSLF
MGDSEMAVFGAAAPYLRKSENAAAAALDRKQRNFD
NKSAKQFSLHIMDSQPDGS
Va, variable region a.
anti-human IgG-alkaline phosphatase conjugate (Sigma), anddeveloped with nitro blue tetrazolium/5-bromo-4-chloro-3-indolyl phosphate chromogens. T. cruzi strips were alterna-tively incubated with a rabbit antiserum to B13 recombinantprotein, when a goat anti-rabbit IgG-alkaline phosphataseconjugate (Sigma) was used. Recombinant B13 protein andnonrecombinant ,B-galactosidase were dot-blotted on nitrocel-lulose membranes with a BRL 96-well manifold (50 ng perdot). AMA of all tested sera were incubated overnight at 4°Cand processed as described for immunoblots.ELISA Assays. Anti-myosin antibody assays were done
essentially as described (13). In our system, 1:200 dilutions ofindividual sera were incubated overnight, at 4°C, in triplicates,over purified human cardiac myosin as the solid-phase antigen,followed by goat anti-human IgG-peroxidase conjugate (Sig-ma) and developed with O-phenylenediamine chromogen. Forepitope mapping of B13 protein, we adapted competitiveELISA protocols (13, 14). Briefly, appropriate dilutions of sera(yielding OD values in the 0.35-0.6 range) were preincubatedwith 1, 10, or 100,uM of each synthetic peptide for 1 hr at 37GC.Each serum/peptide mixture was then incubated overnight intriplicate wells of a B13 protein-sensitized polyvinyl chloridemicrotiter plate (50 ng per well). The reaction was developedas described above. The percentage inhibition of serum bind-ing to solid-phase B13 protein by each peptide at 100 ,uMconcentration was normalized to allow inter-test comparisonsaccording to the equation:
% inhibition = [1 - (OD of peptide
- OD of pB13/OD ofNR - OD of pB13)] x 100.
Statistical Methods. Fisher's exact test was used to evaluatefrequency differences between different patient groups. Stu-dent's t test was used to compare means ofOD values in ELISAtests between different groups of serum. The MACAW program(27) was used for protein-sequence alignment.
RESULTSPrevalence of Anti-Cardiac Myosin IgG Antibodies in Pa-
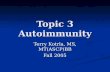
tients' and Normal Sera. All 45 sera from CCC, ASY, andnormal groups were reactive when tested in a purified humancardiac ELISA. The distribution of reactivities was compara-ble, and mean ODs (horizontal bars) in each group were notsignificantly different by Student's t test (Fig. 1). In addition,all sera recognized the major 210-kDa band-comigratingwith myosin HC-in human heart lysate immunoblots (datanot shown).
1.8
1.60
1.4]-1.2-
a 1-00.8-
0.6-
0.4
0.2iIn
00
0
i
0
IS
0
I1
Ba
Normal ASY CCC(n=10) (n=11) (n=24)
FIG. 1. ELISA with purified human cardiac myosin as the solid-phase antigen incubated with 1:200 dilution of sera from normal, ASY,and CCC individuals. A 1:200 dilution was found to yield OD valuesin the most informative range. Horizontal lines represent mean values.
u YIV
Proc. Natl. Acad Sci USA 92 (1995)
Dow
nloa
ded
by g
uest
on
June
11,
202
1
-
Proc. Natl. Acad. Sci. USA 92 (1995) 3543
A B
a b
kDa
210
140116
97
68
FIG. 2. (A) Immunoblot with T. cruzi trypomastigote lysate incu-bated with AMA purified from a CCC serum (strip a) and a rabbitantiserum to B13 recombinant protein (strip b); molecular massmarkers (kDa) are shown at left. Arrowheads indicate 140/116-kDabands. (B) Dot-blots with 50 ng of B13 recombinant protein incubatedwith AMA immunoselected from 14 CCC sera (strip a) and 14 ASYsera (strip b). The positions where protein and antibody samples wereapplied are indicated with dashes.
Identification of a Cardiac Myosin HC Crossreactive T.cruzi Antigen. Trypomastigote lysate immunoblots wereprobed with AMA individually purified from 23 CCC and 11ASY sera. A doublet of bands of 140 and 116 kDa (Fig. 2A,strip a) was recognized by AMA from 14 of 23 (61%) CCCpatients, in contrast to 1 of 11 (9%) ASYs. The difference incrossreactive recognition among AMA from CCC and ASYsera is statistically significant (P = 5.1 X 10-3 , Fisher's exacttest). AMA from normal individuals did not recognize thedoublet of T. cruzi bands. Furthermore, AMA from chagasicpatients or normal subjects do not bind to LLC-MK2 cell lineantigens in immunoblots (data not shown).
Fig. 2A, strip b, shows the same 140/116-kDa doubletrecognized by a rabbit antiserum to the recombinant T. cruziprotein B13 (22). We then investigated whether AMA fromchagasic patients recognized B13 immobilized in dot blots. Fig.2B indicates that AMA from 14 of 14 CCC sera (100%) and2 of 14 ASY sera (14%) give a positive reaction. The differencein binding to B13 between AMA from CCC and ASY sera ishighly significant (P = 2.3 x 10-6, Fisher's exact test). Cross-reactivity in CCC AMA was not secondary to higher levels ofantimyosin or anti-B13 antibody levels, as they were compa-rable in both CCC and ASY unfractionated sera groups, asassessed by ELISA tests (data not shown). AMA from alimited number of ASY individuals with myocarditis at en-domyocardial biopsy also recognized B13 in dot-blots (data notshown). ,B-Galactosidase, the fusion protein support, was notrecognized by AMA from any of the sera.Mapping of the Immunodominant and Cardiac Myosin
HC-Crossreactive B13 Epitopes. To identify regions of pri-mary sequence homology between B13 and cardiac myosinthat could harbor a crossreactive epitope, the sequence of theB13 repetitive motif was aligned (27) to the f3 isoform ofhuman cardiac myosin HC, the prevalent isoform in humanventricle (28). Two hexapeptide regions of 80% homologywere disclosed, at positions 8-13 (VFGAAA vs. B13FGQAAA) and 1442-1447 (AAALDK vs. B13 AAAGDK),respectively, of cardiac myosin HC. Synthetic peptides span-ning the B13-homologous sequences in cardiac myosin HC(pl-20 and p1439-1453) were incubated with CCC and ASYsera in competitive ELISA experiments with B13 as thesolid-phase antigen. Fig. 3A shows that p1439-1453, but not
the pl-20 peptide, competes for binding of the anti-B13antibodies in serum of a CCC patient in a dose-dependentfashion. On the other hand, neither myosin peptide competesfor binding of the antibodies in a ASY serum (Fig. 3B).Apart from the myosin-crossreactive epitope, the B13 pro-
tein repeat motif is known to contain an immunodominant T.cruzi epitope, recognized by unfractionated sera from 97% ofT. cruzi-infected individuals irrespective of disease manifesta-tion (22, 29). To map this immunodominant epitope, synthetic9-mer peptides derived from B13 were also tested. Fig. 5indicates that only the 9-mer S4 peptide, apart from the 19-merpB13 peptide, completely inhibits the binding of both CCCserum (Fig. 4A) and ASY serum (Fig. 4B) to B13 recombinantprotein. The p1439-1453 myosin peptide, along with pB13 andS4 B13-derived peptides, consistently inhibits the binding ofCCC anti-B13 antibodies in six CCC sera in B13 ELISA (Fig.5). Three other ASY sera were tested, corroborating that onlyB13-derived peptides pB13 and S4 inhibit ASY serum antibodybinding to B13 (data not shown). At low dilutions (1:40-1:160),sera from 10 normal controls and 10 cardiopathic Duchennemuscular dystrophy patients displayed OD readings in therange of 0.2-0.3. Such OD readings in B13 ELISA could notbe inhibited by preincubation with peptides p1439-1453 andpB13, thus demonstrating that Duchenne muscle dystrophypatient sera and normal sera are devoid of specific anti-B13antibodies (data not shown).
DISCUSSIONIn this study, we identify the myosin crossreactive T. cruziantigen B13, and we have mapped the crossreactive epitope toa cardiac myosin-specific 6-amino acid region. The almost
0.40.35
0.3
g 0.2n +
0.1
0.05
0
0.6 _
0.5
n A
0 n 'AL
0.2
0.1
A
p10NR
bpl-20
1 J,M 10,lM
F- .;E-
\pl439-1453
lOOulLM
B
NR
------- -~ pl-20
p1439 -1453
pB1310,lM 100 ,uM
FIG. 3. Competitive ELISA for B13 protein. Different concentra-tions of synthetic peptides derived from human cardiac myosin HC ,3isoform (pl-20 and p1439-1453), B13 protein (pB13), and humanT-cell receptor variable-region a chain (NR) were preincubated withserum from CCC patient WA (A) or ASY CA (B). Each mixture wasadded to wells of a microtiter plate sensitized with B13 protein. pB13and NR stand as positive and negative competition controls, respec-tively. Resulting OD values are displayed for each peptide concentra-tion.
_
0.25 -1- -- " 17'N-,
34
IU.15
jk_
l l~i
u.-4
.. II
Immunology: Cunha-Neto et at
.f:
fl
31.
)0-
U.J,
Dow
nloa
ded
by g
uest
on
June
11,
202
1
-
3544 Immunology: Cunha-Neto et at
n A-
0.41"0.35-0.3-
0 0.25-0 0.2-
0.15-
0.1As AC
A
oS1-- S2
--cS3-4.-54
-S6-x- pB13--- NR
K`>
NR
_ x pB13Ul-
1 pLM 10 AM
1 ,M 10 ,uM
100 JIM
pB13
100 ,uM
FIG. 4. Competitive ELISA for B13 protein. Different concentra-tions of synthetic peptides (S1-S6 and pB13, compare with Table 1)covering B13 linear epitopes, as well as peptides derived from T-cellreceptor variable-region a chain (NR), were preincubated with serumfrom CCC patient WA (A) or from ASY CA (B). Assays were doneas described in the Fig. 3 legend.
exclusive presence of cardiac myosin HC-B13 140/116-kDacrossreactive antibodies in CCC sera (Fig. 2) suggests thatcardiac myosin HC-B13 crossreactive recognition may bebiologically relevant to the pathogenesis of CCC.The universal reactivity of sera from CCC, ASY, and normal
controls against human cardiac myosin both in immunoblotsand in ELISA (Fig. 1) indicates the existence of naturalantimyosin antibodies. Although "natural" anti-cardiac myo-sin antibodies have already been reported in mice (30) andhumans (31), our data establish their finding at high preva-lence. Our results show a qualitative difference between"cardiopathy-related" anti-myosin antibodies in CCC sera and"natural" anti-myosin antibodies in ASY sera (Fig. 2), match-ing the findings in experimental murine infection (14). Thepresence of crossreactive antibodies in sera from ASYs withsubclinical Chagas myocarditis may indicate that such anti-bodies are associated to Chagas myocarditis per se rather thanto extensive heart damage. It is tempting to speculate whetherthe two ASYs whose sera displayed crossreactive antibodies in
human cardiachuman cardiac ahuman adult skeleletalrabbit smooth musclehuman nonmuscle
w
m.2a._2._
Sl S2 S3 S4 S5 S6 pl-20p1439-1453
FIG. 5. Epitope mapping of the B13 repeat motif. Competitiveinhibition of the binding of anti-B13 antibodies in B13 ELISA bysynthetic peptides at 100 ,uM concentration. The percentage ofinhibition of serum antibody-binding solid-phase B13 protein wascalculated according to the equation in Materials and Methods. Inhi-bition values for each peptide were averaged from six CCC sera afternormalization.
Fig. 2B, strip b, could also present subclinical Chagas myo-carditis.The presence of two distinct epitopes in the B13 repeat
motifs was suspected in face of the findings of restrictedrecognition of B13 by AMA from CCC sera (Fig. 2B) andunrestricted recognition of an "immunodominant" epitope byunfractionated serum in B13 ELISA serodiagnosis tests (22,29). Epitope mapping with competitive inhibition of B13ELISA (Figs. 3-5) suggested the existence of two distinctspecificities of B13-binding antibodies: (i) antibodies inhibitedby B13 peptides pB13 or S4, found in unfractionated sera fromall T. cruzi-infected individuals tested and possibly responsiblefor the binding of B13 protein in serodiagnosis tests, recog-nizing the immunodominant epitope contained in B13 peptideS4; and (ii) antibodies inhibited by the cardiac myosin peptidep1439-1453, found mainly in CCC sera and representing theantibodies that recognize B13 protein and the 140/116-kDadoublet in AMA preparations, indicating the sequencesAAALDK in myosin and AAAGDK in B13 as the respectivecrossreactive epitopes. B13 peptide S5 (QAAAGDKPS) wasunable to inhibit antibody binding to B13 in CCC sera (Figs.3-5), which may indicate that residues neighboring the cross-reactive hexapeptide also play a role in antibody reactivity.The characterization of the p1439-1453 myosin peptide
containing the AAALDK hexapeptide homologous to B13AAAGDK as the crossreactive epitope established a structuralbasis for myosin-B13 crossreactivity. The AAALDK 1442-1447 myosin sequence is strictly conserved only among cardiacmyosin HC isoforms (Fig. 6). Thus, the B13-crossreactivemyosin epitope recognized by serum antibodies of CCC pa-tients is cardiac myosin HC-specific. The fact that the cross-reactive epitope in B13, AAAGDK, is embedded into theimmunodominant epitope FGQAAAGDK (S4 peptide) ispuzzling, as ASY sera recognize the latter and ignore theformer. This finding suggests that production of cardiac myosin
1428IEDLMVDVERSNAAAAALDDEKQRNFDKILAE1458
V . . .. I .. . .T . . .C .. .. . .. T . .. .. .. .
LD. .V. .LDNQRQLVSN.E ... KK. .L...
LD. .L. .LDHQRQS.CN.E .. .KK. .QL ...
FIG. 6. Alignment of the 1428-1458 region of human cardiac myosin HC containing the B13-crossreactive epitope with other tissue-specificmyosin HC isoforms. Genenbank peptide locus codes are as follows: human cardiac ,B myosin HC, HUMBMYH7CD_1; human cardiac a myosinHC, HUMCAMHC 1; human adult skeletal myosin HC, HSMYH1R 1; rabbit uterus smooth muscle myosin HC, S68021 1; and human nonmusclemyosin HC, HUMMYONM_1.
0
V.-4J
39E-m- ----- \o~-- Z:Z_ ]
.,. 4i.!-
., I .-1
I
Proc. Natl. Acad Sci. USA 92 (1995)
Dow
nloa
ded
by g
uest
on
June
11,
202
1
-
Proc. Natl. Acad Sci. USA 92 (1995) 3545
HC-B13 crossreactive antibodies in CCC may be secondaryto selective recognition of the crossreactive sequencesAAAGDK/AAALDK, under immune response gene control.Thus, it can be hypothesized that crossreactive recognition-and the attending heart damage of CCC-would only occur inT. cruzi-infected individuals endowed, for instance, with per-missive HLA alleles. Family clustering (32) and HLA associ-ation (33, 34) studies support a possible role for immunoge-netic components in the differential susceptibility of the20-30% of T. cruzi-infected individuals who develop CCC. Theabsence of crossreactive antibodies in cardiopathic Duchennemuscular dystrophy patients' sera (data not shown) suggeststhat such antibodies may not be formed as a consequence ofheart damage alone. However, it cannot be formally discardedthat heart damage in a T. cruzi-infected individual might raisesuch crossreactive antibodies.
In spite of the 100% association with CCC patients, directparticipation of the myosin-B13 crossreactive antibody in CCCpathogenesis is not likely. The bulk of evidence supports theparticipation of T cells rather than antibody in heart damage(2, 3, 5, 10, 35). The association of cardiac myosin HC-B13crossreactive antibodies with CCC may be only signaling thepresence of "helper" T cells of similar specificity, these onespotentially involved in heart tissue damage. The identificationof a defined heart-specific epitope (AAALDK) of a majorheart protein (cardiac myosin HC) that is antigenically mim-icked by a secondary epitope (AAAGDK) of an immunodom-inant T. cruzi antigen (B13) is in itself a corollary of the theoryof autoimmune pathogenesis of CCC. The demonstration thatcrossreactive antibody recognition is mainly restricted to CCCpatients defines human cardiac myosin HC and T. cruzi proteinB13 as an antigen pair of potential relevance to the pathogen-esis of heart lesions in human CCC. Specific treatment withanti-T cruzi drugs may not abort the progression of CCCamong T. cruzi-infected individuals (36). Thus, alternativeantigen-specific immunosuppression approaches blocking thedeleterious autoimmune response without interfering withantiparasite immunity may help control heart damage inChagas disease. Further, our findings may allow the search foreffective subunit vaccines devoid of components of T. cruzithat bear the pathogenic heart-crossreactive determinants.
We thank Drs. A. C. Pereira-Barreto and B. Ianni for allowingaccess to patients. We are indebted to Dr. A. C. Goldberg for criticallyreviewing the manuscript. This work has been supported by grantsfrom the Brazilian National Research Council (CNPq) and the SpecialProgram for Research and Training in Tropical Diseases/WorldHealth Organization.
1. Rassi, A., Tranchesi, J. & Tranchesi, B. (1982) in DoenqasInfecciosas e Parasitdrias, ed. Veronesi, R. (Guanabara Koogan,Rio de Janeiro, Brazil), 7th Ed., pp. 675-712.
2. Torres, C. M. (1930) An. 5a Reun. Soc. Argent. Pat. Reg. Norte 2,902-916.
3. Ribeiro-dos-Santos, R., Rossi, M.-A., Laus, J. L., Santana Silva,J., Savino, W. & Menguel, J. (1992) J. Exp. Med. 175, 29-39.
4. Andrade, Z. (1958) Rev. Goiana Med. 4, 103-119.5. Teixeira, A., Teixeira, M. L. & Santos-Buch, C. (1975) Am. J.
Pathol. 80, 163-180.6. Cossio, P. M., Diez, C., Szarfman, A., Kreutzer, E., Candiolo, B.
& Arana, R. M. (1974) Circulation 49, 13-21.7. Levin, M. J., Mesri, E., Benarous, R., Levitus, G., Schijman, A.,
Torres, H. & Segura, E. (1989) Am. J. Trop. Med. Hyg. 41,530-538.
8. Kerner, N., Liegeard, P., Levin, M. J. & Joskowicz, M. H. (1991)Exp. Parasitol. 73, 451-459.
9. Van Voorhis, W., Schelekewy, L. & Trong, H. (1991) Proc. Natl.Acad. Sci. USA 88, 5993-5997.
10. Rizzo, L. V., Cunha-Neto, E. & Teixeira, A. (1989) Infect.Immun. 57, 2640-2644.
11. Harrington, W. F. & Rodgers, M. E. (1984)Annu. Rev. Biochem.53, 35-73.
12. Dale, J. B. & Beachey, E. H. (1986) J. Exp. Med. 164, 1785-1790.13. Neu, N., Beisel, K., Traytsman, M., Rose, N. & Craig, S. (1987)
J. Immunol. 138, 2488-2492.14. Tibbetts, R. S., McCormick, T. S., Rowland, E. C., Miller, S. D.
& Engman, D. M. (1994) J. Immunol. 152, 1493-1499.15. Neu, N., Rose, N., Beisel, K., Herskowitz, A., Gurri-Glass, G. &
Craig, S. (1987) J. Immunol. 139, 3630-3636.16. Smith, S. & Allen, P. (1991) J. Immunol. 147, 2141-2147.17. Higuchi, M. L., Floriano de Morais, C., Pereira Barreto, A. C.,
Lopes, E. A., Stolf, N., Bellotti, G. & Pileggi, F. (1987) Clin.Cardiol. 10, 665-669.
18. Margossian, S. & Lowey, S. (1982) Methods Enzymol. 85, 55-71.19. Laemmli, U. K. (1970) Nature .(London) 227, 680-685.20. Towbin, H., Staehelin, L. & Gordon, J. (1979) Proc. Natl. Acad.
Sci. USA 76, 4350-4354.21. Zingales, B., Andrews, N. W., Kuwajima, V. Y. & Colli, W.
(1982) Mol. Biochem. Parasitol. 6, 111-124.22. Gruber, A. & Zingales, B. (1993) Exp. Parasitol. 76, 1-12.23. Houghten, R. A. (1985)Proc. Natl. Acad. Sci. USA 82, 5131-5135.24. Kabat, E. A. (1970) Ann. N.Y Acad. Sci. 169, 43-54.25. Geysen, H. M., Rodda, S. J., Mason, T., Tribbick, G. & Schoofs,
P. (1987) J. Immunol. Methods 102, 259-274.26. Tovey, E. & Baldo, B. (1989) in Protein Blotting, eds. Baldo, B.,
Tovey, E. & St. Leonards, N. (Karger, Basel), pp. 43-64.27. Schuler, G. D., Altschul, S. F. & Lipman, D. J. (1991) Proteins
Struct. Funct. Genet. 9, 180-190.28. Gorza, L., Mercadier, J.-J., Schwartz, K., Thornell, L. E., Sartore,
S. & Schiaffino, S. (1984) Circ. Res. 54, 694-702.29. Tropical Disease Research/World Health Organization (1990)
Mem. Inst. Oswaldo Cruz 85, 487-543.30. Berneman, A., Ternynck, T. & Avrameas, S. (1992) Eur. J.
Immunol. 22, 625-633.31. Cunningham, M. W., McCormack, J. M., Talaber, L. R., Harley,
J. B., Ayoub, E. M., Muneer, R. S., Chun, L. T. & Reddy, L. V.(1988) J. Immunol. 14, 2760-2766.
32. Zicker, F., Smith, P. G., Almeida Netto, J. C., Oliveira, R. M. &Zicker, E. M. S. (1990) Am. J. Trop. Med. Hyg. 43, 498-505.
33. Layrisse, Z., Acquatella, H., Piccone, C., Catalioti, C. & Gomez,J. R. (1988) Hum. Immunol. 23, 116 (abstr.).
34. Ascurra, M., Pistilli, N., Otha, N. & Rosner, J. (1990) Mem. Inst.Oswaldo Cruz. 85, Suppl. 1, 78 (abstr.).
35. Khoury, E. L., Diez, C., Cossio, P. M. & Arana, R. M. (1983)Clin. Immunol. Immunopathol. 27, 283-288.
36. Teixeira, A., Cunha-Neto, E., Rizzo, L. & Silva, R. (1990) J.Infect. Dis. 162, 1420.
Immunology: Cunha-Neto et at
Dow
nloa
ded
by g
uest
on
June
11,
202
1
Related Documents