Prolactin and Autoimmunity Hyperprolactinemia Correlates with Serositis and Anemia in SLE Patients Hedi Orbach & Gisele Zandman-Goddard & Mona Boaz & Nancy Agmon-Levin & Howard Amital & Zoltan Szekanecz & Gabriella Szucs & Josef Rovensky & Emese Kiss & Andrea Doria & Anna Ghirardello & Jesus Gomez-Arbesu & Ljudmila Stojanovich & Francesca Ingegnoli & Pier Luigi Meroni & Blaz’ Rozman & Miri Blank & Yehuda Shoenfeld # Springer Science+Business Media, LLC 2011 Abstract Evidence points to an association of prolactin to autoimmune diseases. We examined the correlation be- tween hyperprolactinemia and disease manifestations and activity in a large patient cohort. Age- and sex-adjusted prolactin concentration was assessed in 256 serum samples from lupus patients utilizing the LIASON prolactin auto- mated immunoassay method (DiaSorin S.p.A, Saluggia, Italy). Disease activity was defined as present if European Consensus Lupus Activity Measurement (ECLAM)>2 or Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)>4. Lupus manifestations were grouped by organ involvement, laboratory data, and prescribed medications. Hyperprolactinemia was presented in 46/256 (18%) of the cohort. Hyperprolactinemic patients had significantly more serositis (40% vs. 32.4%, p =0.03) specifically, pleuritis (33% vs. 17%, p =0.02), pericarditis (30% vs. 12%, p =0.002), and peritonitis (15% vs. 0.8%, p =0.003). Hyper- prolactinemic subjects exhibited significantly more anemia H. Orbach Department of Medicine B, Wolfson Medical Center, Holon, Israel e-mail: [email protected] Y. Shoenfeld (*) Department of Medicine B, Sheba Medical Center, Tel-Hashomer, Israel e-mail: [email protected] G. Zandman-Goddard Department of Medicine C, Wolfson Medical Center, Holon, Israel e-mail: [email protected] M. Boaz Epidemiology Unit, Wolfson Medical Center, Holon, Israel e-mail: [email protected] N. Agmon-Levin : M. Blank : Y. Shoenfeld Zabludowicz Center for Autoimmune Diseases and Medicine B, Sheba Medical Center, Tel-Hashomer, Israel N. Agmon-Levin e-mail: [email protected] M. Blank e-mail: [email protected] H. Amital Department of Medicine D, Meir Medical Center, Tel-Aviv, Israel e-mail: [email protected] G. Zandman-Goddard : M. Boaz : N. Agmon-Levin : H. Amital : M. Blank : Y. Shoenfeld Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel Z. Szekanecz : G. Szucs University of Debrecen, Debrecen, Hungary Z. Szekanecz e-mail: [email protected] G. Szucs e-mail: [email protected] J. Rovensky National Institute of Rheumatic Diseases, Piest’any, Slovak Republic e-mail: [email protected] E. Kiss National Institute of Rheumatology and Physiology, Budapest, Hungary e-mail: [email protected] Clinic Rev Allerg Immunol DOI 10.1007/s12016-011-8256-0

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Prolactin and AutoimmunityHyperprolactinemia Correlates with Serositis and Anemia in SLE Patients
Hedi Orbach & Gisele Zandman-Goddard & Mona Boaz & Nancy Agmon-Levin &
Howard Amital & Zoltan Szekanecz & Gabriella Szucs & Josef Rovensky & Emese Kiss &
Andrea Doria & Anna Ghirardello & Jesus Gomez-Arbesu & Ljudmila Stojanovich &
Francesca Ingegnoli & Pier Luigi Meroni & Blaz’ Rozman & Miri Blank &
Yehuda Shoenfeld
# Springer Science+Business Media, LLC 2011
Abstract Evidence points to an association of prolactin toautoimmune diseases. We examined the correlation be-tween hyperprolactinemia and disease manifestations andactivity in a large patient cohort. Age- and sex-adjustedprolactin concentration was assessed in 256 serum samplesfrom lupus patients utilizing the LIASON prolactin auto-mated immunoassay method (DiaSorin S.p.A, Saluggia,Italy). Disease activity was defined as present if EuropeanConsensus Lupus Activity Measurement (ECLAM)>2 or
Systemic Lupus Erythematosus Disease Activity Index(SLEDAI)>4. Lupus manifestations were grouped by organinvolvement, laboratory data, and prescribed medications.Hyperprolactinemia was presented in 46/256 (18%) of thecohort. Hyperprolactinemic patients had significantly moreserositis (40% vs. 32.4%, p=0.03) specifically, pleuritis(33% vs. 17%, p=0.02), pericarditis (30% vs. 12%,p=0.002), and peritonitis (15% vs. 0.8%, p=0.003). Hyper-prolactinemic subjects exhibited significantly more anemia
H. OrbachDepartment of Medicine B, Wolfson Medical Center,Holon, Israele-mail: [email protected]
Y. Shoenfeld (*)Department of Medicine B, Sheba Medical Center,Tel-Hashomer, Israele-mail: [email protected]
G. Zandman-GoddardDepartment of Medicine C, Wolfson Medical Center,Holon, Israele-mail: [email protected]
M. BoazEpidemiology Unit, Wolfson Medical Center,Holon, Israele-mail: [email protected]
N. Agmon-Levin :M. Blank :Y. ShoenfeldZabludowicz Center for Autoimmune Diseases and Medicine B,Sheba Medical Center,Tel-Hashomer, Israel
N. Agmon-Levine-mail: [email protected]
M. Blanke-mail: [email protected]
H. AmitalDepartment of Medicine D, Meir Medical Center,Tel-Aviv, Israele-mail: [email protected]
G. Zandman-Goddard :M. Boaz :N. Agmon-Levin :H. Amital :M. Blank :Y. ShoenfeldSackler Faculty of Medicine, Tel-Aviv University,Tel-Aviv, Israel
Z. Szekanecz :G. SzucsUniversity of Debrecen,Debrecen, Hungary
Z. Szekanecze-mail: [email protected]
G. Szucse-mail: [email protected]
J. RovenskyNational Institute of Rheumatic Diseases,Piest’any, Slovak Republice-mail: [email protected]
E. KissNational Institute of Rheumatology and Physiology,Budapest, Hungarye-mail: [email protected]
Clinic Rev Allerg ImmunolDOI 10.1007/s12016-011-8256-0

(42% vs. 26%, p=0.02) and marginally more proteinuria(65.5% vs. 46%, p=0.06). Elevated levels of prolactinwere not significantly associated with other clinicalmanifestations, serology, or therapy. Disease activityscores were not associated with hyperprolactinemia.Hyperprolactinemia in lupus patients is associated withall types of serositis and anemia but not with other clinical,serological therapeutic measures or with disease activity.These results suggest that dopamine agonists may be anoptional therapy for lupus patients with hyperprolactinemia.
Keywords Prolactin . Systemic lupus erythematosus .
Disease activity . Serositis . AnemiaProteinuria . Rheumatoid arthritis . Multiple sclerosis .
Sjögren’s syndrome . Systemic sclerosis .
Autoimmune thyroid disease
Introduction
Prolactin (PRL) is a polypeptide hormone secreted by theanterior hypophysis. It is an integral member of theimmunoneuroendocrine network and has a role in thepathogenesis of autoimmune diseases mainly systemiclupus erythematosus (SLE).
Prolactin Structure Secretion and Function
Pituitary monomeric free PRL (little PRL, 23 kDa) is themain PRL isoform. Other isoforms include big PRL(56 kDa) and big big (macro) PRL (150–160 kDa). MacroPRL is mostly constituted by IgG monomeric PRL complex[1]. The different isoforms that are secreted from immunecells have variable biologic activity [2]. The PRL receptorbelongs to type 1 cytokine/hematopoietic receptor superfamily [3].
PRL secretion is inhibited by the hypothalamus viadopamine. Thyroid releasing hormone, hypothyroidism,and adrenal insufficiency stimulate PRL secretion byinhibiting dopamine secretion. The main cytokinesstimulating PRL secretion are interleukin (IL)-1, IL-2,and IL-6 while interferon-γ and endothelin 3 are inhibi-tory [4].
Besides breast feeding, chest wall stimulation and chestwall injury stimulate PRL secretion. Medications thatincrease PRL secretion by inhibition of dopamine secretioninclude neuroleptic drugs phenothiazines and haloperidol,antihypertensive medications calcium channel blockers andmethyldopa, tricyclic antidepressants, H2 antagonists, andopiates. Decreased elimination of PRL due to renal orhepatic failure increases PRL level. Estrogen has animportant role in PRL secretion in pregnancy and otherconditions. Prolactinoma is another cause of very highlevels of prolactin [5].
PRL is synthesized in several organs including neurons,mammary epithelium, prostate, endothelium, and skin [4].PRL is synthesized also in immune organs including thethymus, spleen, lymph nodes, and bone marrow as well asin mononuclear cells (mainly lymphocytes). The humanPRL gene is located on chromosome 6. Its expression is atmultiple extrapituitary sites, where it is under tissue-specificcontrol [6].
Estrogen has a role in the regulation of PRL geneexpression in humans [7]. PRL secreted from the hypoph-ysis acts as a hormone, while the PRL produced byextrahypophyseal organs functions as a cytokine as it issynthesized in multiple sites, has similar receptor structuresand signal transduction pathways [8, 9]. PRL receptors aredistributed throughout the immune system and are includedin the cytokine receptor family that includes receptors forIL-2β chain, IL-3, IL-4, IL-6, IL-7, growth hormone, anderythropoietin [10].
PRL’s main physiological role is to regulate the growthand differentiation of the mammary gland and ovary, toinitiate and sustain lactation and regulate maternal behavior.Other functions include role in osmoregulation, calciummetabolism, reduction of the threshold for glucose-stimulated insulin secretion, anti-angiogenesis, vasocon-striction, and anti-vasopermeability actions. Nevertheless,
A. Doria :A. GhirardelloDivision of Rheumatology, University of Padova,Padova, Italy
A. Doriae-mail: [email protected]
A. Ghirardelloe-mail: [email protected]
J. Gomez-ArbesuImmunology Department,Hospital Universitario Central de Asturias,Asturias, Spaine-mail: [email protected]
L. StojanovichBezhanijska Kosa University Medical Center,Belgrade, Serbiae-mail: [email protected]
F. Ingegnoli : P. L. MeroniUniversity of Milan,Milan, Italy
F. Ingegnolie-mail: [email protected]
P. L. Meronie-mail: [email protected]
B. RozmanUniversity Clinical Center Lubljiana,Lubljiana, Sloveniae-mail: [email protected]
Clinic Rev Allerg Immunol

in recent years, PRL’s role in immune regulation wasdefined [11].
The Role of Prolactin in Immune Modulation
Experimental studies in lupus murine models have shownthat hyperprolactinemia (HPRL) can interfere with B celltolerance induction by impairing the B cell receptor-mediated clonal deletion, deregulating receptor editing anddecreasing the threshold for activation of anergic B cells[12, 13].
Lupus murine model studies also demonstrated that PRLinduces a decrease in apoptosis of transitional B cellsthereby contributing into the breakdown of B cell toleranceto self and to the development of autoimmunity [14]. PRLinduces the production of IL-1 and interferon-γ andpromotes the expression of IL-2 receptor [15]. In addition,HPRL affects dendritic cell (DC) maturation, skewing DCfunction from antigen presentation to pro-inflammatoryphenotype with increased interferon α production [16].Moreover, PRL also enhances immunoglobulin production[17]. PRL regulates the maturation of CD4− CD8−thymocytes to CD4+ CD8+ T cells via IL-2 receptorexpression and leads to the enhancement of pro-B cellgeneration [12].
Hyperprolactinemia and Autoimmune Diseases
The mechanisms above may have a role in the increasedprevalence of autoimmune diseases in patients with HPRL.Moreover HPRL is observed in various autoimmunediseases [18]. HPRL has been demonstrated in multi-organ diseases as SLE, rheumatoid arthritis (RA), systemicsclerosis (SSc), Sjögren’s syndrome (SS), and reactivearthritis [18].
The organ-specific diseases correlated with HPRLinclude type 1 diabetes mellitus, Graves’ disease, Hashi-moto’s thyroiditis, Addison’s disease, lymphocytic hypo-physitis, celiac disease, multiple sclerosis, uveitis, andrejection of heart transplantation [18, 19].
Systemic Lupus Erythematosus
SLE is more common in women of reproductive age, andthis 9:1 ratio compared to men, with sex hormones estrogenand PRL implicated as explanatory mechanisms [12].
Mild to moderate HPRL is reported in 15–45% of SLEpatients [20–26], compared to a rate of 3% in the generalpopulation [27]. Studies on the correlation of PRL levelsand disease activity in SLE were inconsistent [18].
Few studies of dopaminergic agonist therapy for reduc-ing PRL levels were effective in experimental models oflupus and small clinical trials in SLE [28–33].
Inhibition of PRL secretion by bromocriptine decreasedserum anti-double-stranded DNA (ds-DNA) antibody titersand improved the survival of lupus-prone mice [29], andmice with estrogen-induced HPRL [30].
Bromocriptine therapy showed a beneficial effect in SLEpatients suffering from mild to moderate active disease andled to a significant improvement in disease activity scores[25, 31, 32]. Further, discontinuation of bromocriptinetherapy was followed by a flare of disease activity [32].In another study, the role of additional therapy withbromocriptine 2.5 mg/day added to 10 mg prednisone wasfound to be beneficial for pregnant SLE patients. In thisstudy, the added therapy given during weeks 25–35 ofgestation prevented lupus flare, premature rupture ofmembrane, and preterm birth [33].
Alternative therapy with low-dose quinagolide added tothe existing therapy of 25 SLE patients for 3 monthsdiminished significantly SLE patient’s PRL and IL-6 levelswith a significant reduction of SLEDAI score compared tobaseline [34].
Rheumatoid Arthritis
The studies on PRL levels in RA found inconsistent results,varying from lower, equal to higher PRL serum levels [35].RA usually improves during pregnancy and may exacerbateafter delivery, a period when cortisol and estrogen declineand PRL increases [36]. The risk of RA is increased inwomen who breastfeed after the first pregnancy. Thepropensity to develop RA was suggested to be related toimmune stimulation by PRL [36, 37]. The dynamicresponse of hypothalamic–pituitary–adrenal axis and PRLpituitary secretion in women under 40 years old with RAshowed upregulation of PRL secretion while the level ofadrenocorticotropine hormone (ACTH) and cortisol did notincrease after corticotropine releasing hormone test [38].However, in newly diagnosed untreated RA patients thelevel of PRL, ACTH, and cortisol in response to stimula-tion test was the same as in the controls [39]. In tenpostmenapausal active RA women, a lower ACTH andcortisol level, respectively and higher PRL and PRL/cortisol ratio at 2:00 a.m. were demonstrated whencompared to controls [40].
The PRL response to induced hypoglycemia in active RAwas decreased and normalized after 6 months of therapy withdisease-modifying anti-rheumatic drugs (DMARDs) [41].However, another group could not find a significantdifference in PRL response to induced hypoglycemia inglucocorticoid-naive premenopausal patients with RA [42].
The pro-inflammatory cytokine macrophage inflamma-tory protein-1α is produced by cells involved in theinflammatory rheumatoid process and may stimulate pitu-itary production of PRL [43]. PRL is also produced in the
Clinic Rev Allerg Immunol

rheumatoid joint by fibroblast like synovial cells and by Tlymphocytes infiltrating the synovium and increases thesynthesis of matrix metalloproteinase-3, IL-6, and IL-8.PRL seems to stimulate collagenase activity and to act as agrowth factor for lymphocytes. Bromocriptine suppresses invitro the expression of messenger RNA for PRL and tumornecrosis factor α in the synovial cells and infiltratinglymphocytes [44]. These findings suggest that PRL mayhave a role in initiating or sustaining the inflammation inRA, but it is not clear if the stimulation is produced bypituitary PRL or by PRL of lymphocyte origin.
Three small cohorts of RA patients demonstrated normallevel of PRL in comparison with controls [39, 45, 46].Among 60 RA women, HPRL or macroprolactinemia werenot more prevalent compared with controls; however,serum PRL and free (monomeric) PRL were significantlyelevated in RA compared to controls [47]. Male RApatients showed high serum PRL levels. The serum PRLconcentration was found to be increased in relation to theduration and the activity of the disease [48]. Another cohortof 91 RA male patients demonstrated HPRL in 40% ofthem. Men with RA had high serum PRL levels incomparison to control group. PRL level correlated withlonger disease evolution and worse functional stage [49].Among 53 RA patients, we demonstrated HPRL in three(6%), this is twice the prevalence in a healthy population[50]. In a recent study, serum and synovial PRL levels weresignificantly higher in 29 RA patients compared withosteoarthritis patients. Serum PRL level correlated withtotal Larsen score meaning more severe radiographicdamage and synovial PRL levels correlated with diseaseactivity measured by DAS 28 score [35]. Bromocriptinetreatment for RA was tried in four small open-label trials.Bromocriptine 6.25 mg in addition to cyclosporine in sixRA patients did not improve clinical or laboratory measuresof disease activity [51]. In 30 active RA patients,bromocriptine therapy improved clinical activity as penicil-lamine, but failed to improve laboratory parameters ofinflammation [52]. Five refractory RA patients were treatedwith 5 mg bromocriptine once daily. Three of themimproved more than 25%, but only in two, the improvementlasted till the end of study therapy at 6 months. No correlationwas found between PRL levels and disease activity [53]. Nineseropositive postmenapausal RA patients that discontinuedDMARDs because of inefficacy or adverse effects weretreated for 3 months by bromocriptine 5–30 mg dailyaccording to tolerance. Clinical improvement was significantin morning stiffness and HAQ disability index. Four patientsfulfilled the American College of Rheumatology criteria forRA improvement. There was correlation between clinicalimprovement and reduction in immune activity includingperipheral blood mononuclear cells to antigen and produc-tion of IL-2 and nitric oxide [54].
Nine normoprolactinemic RA patients were treated byquinagolide in addition to prednisone and non-steroidalanti-inflammatory drugs for 6 months. There was noclinical or laboratory improvement with quinagolide [55].There is a single case report of cabergoline therapy forprolactinoma improving the RA manifestations [56].
Multiple Sclerosis
In studies in experimental allergic encephalomyelitis (EAE)the animal model of multiple sclerosis (MS) PRL levelswere elevated before the onset of neurological manifesta-tions. Bromocriptine therapy was protective when initiated1 week after the initial immunization and also suppressedlate disease [57]. Bromocriptine reduced the severity andduration of EAE in chronic relapsing model [58].
Studies that evaluated the serum levels of PRL in MSpatients have yielded conflicting results. Mild to moderateHPRL was found in 30% of MS patients and wasspeculated to be related to hypothalamic lesions [59].Twelve MS patients had elevated PRL levels in comparisonwith controls without HPRL. The PRL levels post-TRHstimulation were significantly higher in patients with MSwhen compared with control group [60]. PRL levels weremeasured in 49 MS patients and healthy controls. Excessiveconcentration of PRL in blood serum was observed in themenstruating women with MS and male MS patients incomparison to healthy menstruating women and men [61].
HPRL in Japanese female patients with an opticospinalvariant of MS (termed Asian type) was associated withhypothalamic lesions. All MS patients with HPRL showedrecurrent opticomyelitis and a higher Expanded DisabilityStatus Scale score. Severe inflammation in the optic nervesmay spread and damage the adjacent tuberoinfundibulardopaminergic neurons, which inhibit PRL secretion [62].Among 68 male MS patients, the rate of HPRL was 16.2%;however, the mean PRL level was not significantly differentfrom the mean PRL level in the control group. There wasno difference in PRL level between the relapsing–remittingand the progressive type of MS [63]. PRL levels in serumand cerebrospinal fluid (CSF) were found to be significant-ly higher in female relapsing–remitting MS patients but notin males. No associations were found with disease activity,disease duration, presence of active lesions, or the presenceof oligoclonal bands in CSF. This could be suggestive of asexually dimorphic response to central nervous systeminjury as a result of an increased proneness of females tosynthesize and release PRL, which is possibly linked to therelatively more favorable prognosis of MS in women [64].In our recent study, HPRL was documented in 10/150(6.7%) MS patients significantly more common comparedwith healthy controls. Among female MS patients, HPRLwas related to the secondary progressive type of disease
Clinic Rev Allerg Immunol

[65]. A case reported of a relapsing–remitting MS patientwho experienced the first MS clinical event during thedevelopment of a PRL secreting adenoma and the only twoMS relapses were during adenoma recurrence. PRL mayhave facilitated the inflammatory process and triggered MSclinical attacks [66]. Other studies did not find difference inPRL levels between MS patients and healthy controls andPRL level was not correlated with clinical disease activityor disease duration [67–70]. The role of bromocriptine intherapy for MS was suggested; however, an open-label pilotstudy did not show therapeutic effects on MS activity [71].A study of intravenous methylprednisolone therapy 500 mgmonthly caused a reduction of T2 lesion volume with aparallel decline in plasma PRL in nine relapsing–remittingMS patients [72].
Systemic Sclerosis
SSc is at least five times more common in women inchildbearing age than in men [73]. That may suggest apathogenic role of sex hormones in SSc. PRL serum levelswere high in a wide range of 3–81% of patients sufferingfrom SSc in different cohorts [6, 50, 74–76]. A possibleexplanation of HPRL in SSc may be the sustained releaseof PRL over 24 h and a change in the diurnal rythm withpeaks of secretion between 6 and 11 a.m., instead of 2–6 a.m.[74]. Basal and after stimulation with thyroid releasinghormone PRL levels were found to be higher than incontrols in women suffering from SSc in childbearing ageand not in postmenapausal SSc patients in comparison withhealthy controls. The HPRL may be a factor in the decreasedfertility in SSc. Scores on the SSc organ severity scale werenot associated with PRL levels, but PRL level wassignificantly correlated with skin sclerosis, peripheral vascu-lar, and lung involvement [77]. Basal HPRL and dramaticincrease in PRL levels after metochlorpropamide test in SScpatients and not in controls suggest increased dopaminergictone in SSc. In the same study, CT scan revealed micro-adenoma in 80% of SSc patients most of them asymptomatic[78]. HPRL in SSc and not in controls was demonstrated,with correlation of PRL level in the diffuse SSc patientswith disease manifestations as the rate of skin tethering,diastolic dysfunction of the left ventricle, and diseaseduration. In all patients, HPRL in early disease wasassociated significantly with more aggressive skin involve-ment [75]. SSc patients with severe disease manifestationsin comparison with more mild SSc patients have signifi-cantly more HPRL and lower serum dehydroepiandroster-one sulfate level. These abnormalities were associated withhigher soluble IL-2 receptor (sIL-2R) and vascular celladhesion molecule [79]. Peripheral blood mononuclear cells(PBMC) supernatants of SSc patients contain significantlyincreased amounts of PRL as compared to healthy donors’
PBMC. These results show that lymphocytes in SScpatients are active producers of extrapituitary PRL. PRL-stimulated lymphocytes produced an increased amount ofsIL-2R (CD25). The same cells besides producing PRL arealso sensitive to PRL stimulation [76]. The cause of HPRLin SSc may be increased dopaminergic tone or secretion ofPRL from lymphocytes.
Sjögren’s Syndrome
HPRL has been reported in 3.6–45.5% of SS patients [50].Among hyperprolactinemic women, one study found that75% of them had at least one antibody detected in serum andnone in the control group. Anti-SSAwas present in 27% andanti-SSB in 12% of hyperprolactinemic women [80].
Young SS patients with active disease had highprevalence of HPRL associated with internal organ disease,but not with disease duration, serum immune globulins,autoantibodies, or focus score in minor salivary glandbiopsy [81]. HPRL was found in 45.5% of SS patients andnot in control group, without any correlation betweenHPRL and systemic manifestations or presence of autoanti-bodies [82]. Another group did not find correlation betweenPRL levels and systemic disease manifestations nor withhormonal status or autoantibodies [27].
The presence of PRL and PRL receptor was detected byimmunohistochemistry in ductal epithelial cells of minorsalivary glands in SS and not in the lymphocytes infiltratingaround the ducts. Big PRL of 60 kDa and a 16-kDa PRL-like protein were demonstrated. A positive correlation wasfound between the presence of PRL-like proteins in acinarepithelial cells of SS patients and clinical extraglandularmanifestations. The presence of anti-Ro and anti-La anti-bodies also positively correlated with a higher percentageof PRL in acinar epithelial cells demonstrating localsynthesis of PRL-like proteins in the acinar ducts insalivary glands [83]. A central deficiency in all threeneuroendocrine axes: adrenal, gonadal, and thyroid wasfound in SS with elevated PRL levels, probably affectsimmune function in SS patients [84]
Autoimmune Thyroid Disease
Hashimoto’s thyroiditis patients exhibit significantly higherPRL and lower cortisol levels than healthy controls [85].Nineteen percent of patients with Hashimoto’s thyroiditishad HPRL; however, the prevalence of HPRL in theprimary hypothyroid group was much higher (42.4%) thanin euthyroid patients that were not different from thecontrol group [86]. HPRL induced by anti-psychoticmedications in schizophrenic patients, who did not haveclinical thyroid disease, is related with significantlyincreased thyroid antibodies [87].
Clinic Rev Allerg Immunol
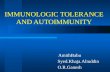
In our previous study, HPRL was detected in 24% ofpolymyositis patients, 21% of lupus patients, 6.7% ofmultiple sclerosis patients, 6% of rheumatoid arthritispatients, and 3% of systemic sclerosis patients [18]. InSLE, PRL levels did not correlate with lupus diseaseactivity measured by ECLAM score; however, HPRL wassignificantly associated with anemia and proteinuria.
In the current study, we expanded our cohort to assessthe possible association of HPRL with lupus subsets andclinical activity of the disease.
Methods and Patients
Serum samples from 256 SLE patients were evaluated forelevated PRL levels. Patients serum samples were providedby two European clinics: University of Debrecen, Hungary(n=156) and University of Padova, Italy (n=100). Eachclinic provided a database including, in addition todemographic characteristics, SLE clinical manifestations,serology, and disease activity scores. Manifestations werefurther grouped according to organ system involvementconsistent with clinical disease and included cutaneous,joints, hematological, renal, and neuropsychiatric findings.Serology included antinuclear antibodies, antibodies to ds-DNA, ENA (Ro/La/ribonucleoprotein particles (RNP)/Sm),cardiolipin, β-2-glycoprotein I, lupus anticoagulant, andC3/C4 levels.
In the Italian patients, disease activity was determinedusing the ECLAM score (n=100) while in the Hungariangroup, SLEDAI score (n=156) was used. Both scores arewidely utilized for assessment of disease activity in SLE[88]. In order to unify the description of disease activity forthe entire cohort, we chose disease activity cutoffs such thatSLEDAI greater than 4 and ECLAM greater than 2indicating active disease. We evaluated the association ofHPRL with medications utilized (corticosteroids, low-dosecorticosteroids less than 10 mg of prednisone, anti-malarialdrugs, or other medications).
PRL level was detected by the LIASON PRL method.This is a chemiluminescent fully automated immunoassay.Monoclonal antibodies are utilized for the coating of solidphase (magnetic particles) and for the tracer. The tests wereperformed on the LIASON analyzer (DiaSorin S.p.A,Saluggia, Italy). PRL levels were gender- and age-adjusted. The normal range of PRL in women ≤45 yearsold is ≤498 mIU/L and in men and women above 45 yearsold the normal PRL level is ≤392 mIU/L.
Statistical Analysis Clinical manifestations were comparedby HPRL (which acquire a value of 0 or 1) using the chi-square test. Continuous variables were compared by an HPRLusing the t test for independent samples or the Mann–
Whitney U as appropriate. To preserve the overall alpha of agiven organ group, the grouped manifestations were testedby disease activity and if this was found to differsignificantly, subsequent by-manifestation testing was per-formed. All tests were two-sided and significant at p<0.05.
Results
Our cohort was comprised of 256 lupus patients, medianage 36.5 [13–77] years, 88% females, and the mean diseaseduration was 10.5±7.7 years. HPRL was observed in46/256 (18%) of lupus patients.
Compared to normoprolactinemic lupus patients, thosewith HPRL had significantly more serositis (40% vs. 32.4%,p=0.03) specifically, pleuritis (33% vs. 17%, p=0.02),pericarditis (30% vs. 12%, p=0.002), and peritonitis(15% vs. 0.8%, p=0.003) (Fig. 1).
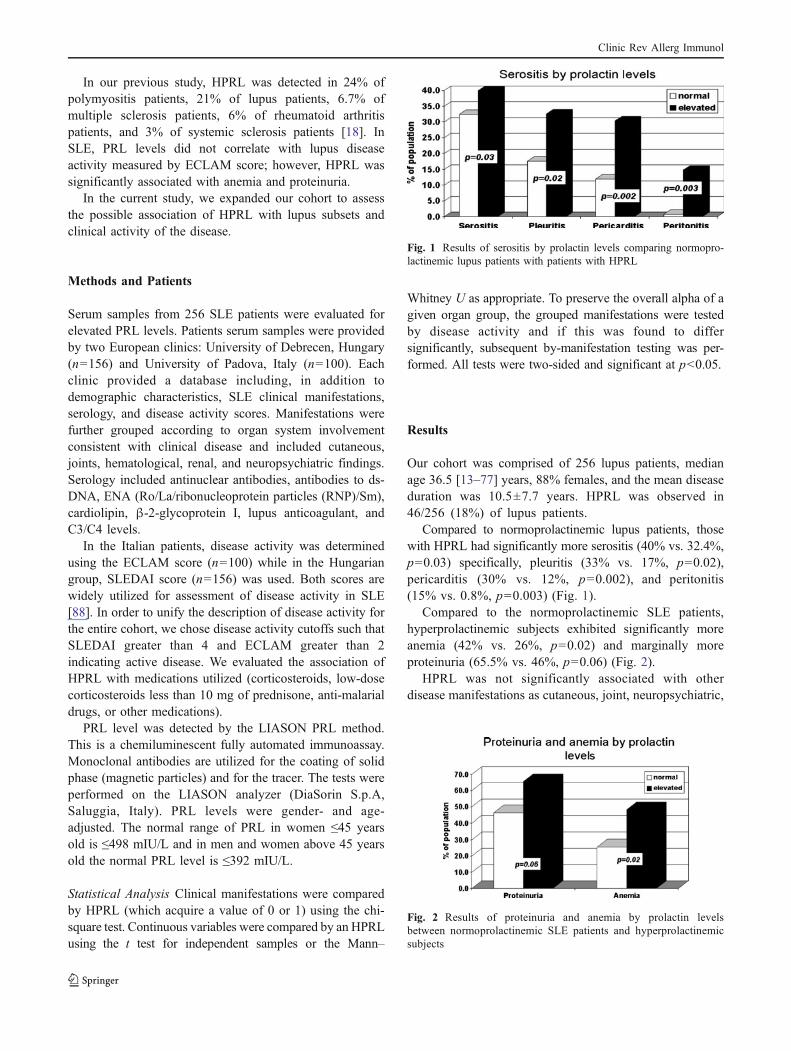
Compared to the normoprolactinemic SLE patients,hyperprolactinemic subjects exhibited significantly moreanemia (42% vs. 26%, p=0.02) and marginally moreproteinuria (65.5% vs. 46%, p=0.06) (Fig. 2).
HPRL was not significantly associated with otherdisease manifestations as cutaneous, joint, neuropsychiatric,
Fig. 1 Results of serositis by prolactin levels comparing normopro-lactinemic lupus patients with patients with HPRL
Fig. 2 Results of proteinuria and anemia by prolactin levelsbetween normoprolactinemic SLE patients and hyperprolactinemicsubjects
Clinic Rev Allerg Immunol

other hematological or renal manifestations, serology, orany pharmacologic interventions. Disease activity measuredeither by ECLAM or by SLEDAI score was not associatedwith the level of PRL.
Discussion
HPRL is associated with lupus disease activity in somehuman studies [20, 26, 89–92]. While studies in murinemodels demonstrate a clear correlation between HPRL andlupus activity [30, 93, 94], the human data are notconsistent. An association between HPRL and more activedisease coupled with diminished response to prednisonetherapy has been reported [95], but others, including us,found no correlation between HPRL and lupus activity[18, 22, 96–98]. The association between HPRL andspecific manifestations of SLE was seldom reported.
In the current study, we found an association betweenhigh levels of PRL and several manifestations of lupusdisease, namely serositis (pleuritis, pericarditis, andperitonitis) and anemia as well as a marginal correlationwith proteinuria. This stands in agreement with severalother studies. For instance, the level of little PRL(23 kDa) correlated with neurological, renal, and hemato-logical involvement, as well as the presence of serositis,anti-ds-DNA antibodies and low levels of complement. Incontrast, macroprolactinemia, anti-PRL antibodies or lowlevels of little PRL were negatively related to lupusactivity [25, 99, 100].
Others have shown that HPRL is linked to lupusnephritis, central nervous system, cutaneous, and artic-ular manifestations [101, 102] as well as with severalautoantibodies, such as anti-ds-DNA, anti-SSA, anti-SSB,anti-Sm, and anti-RNP [103]. Among 30 SLE patients,HPRL was demonstrated in ten patients and PRL levelscorrelated to disease activity, malar rash, nephritis, andanti-ds-DNA antibody levels [26]. HPRL and decreasedserum dehydroepiandrosterone in SLE patients was asso-ciated with anti-ds-DNA antibody elevation and a decreasein almost all lymphocyte subsets [104]. Intriguingly, it hasbeen suggested that HPRL in SLE patients increases thedisease activity by inducing autoantibodies to phospho-lipids which are associated by adverse pregnancyoutcomes, thus bromocriptine may prevent this effect[28]. HPRL was more prevalent in patients with primaryand seconday antiphospholipid syndrome than in healthypopulation and HPRL correlated with adverse pregnancyoutcomes [105].
The variability of the association between diseaseactivity and organ manifestations and HPRL reported inthe literature may be explained by selection bias—specif-ically, differences in study populations, therapies, abnormal
circadian PRL rhythm, and presence of different PRLisoforms and anti-PRL antibodies [101].
Although in our cohort of 256 patients we found nocorrelation between HPRL and disease activity scoresmeasured in SLEDAI or ECLAM scores, we found asignificantly more serositis (pleuritis, pericarditis, andperitonitis) and anemia and marginally more proteinuria inthe hyperprolactinemic SLE patients than in patients withnormal PRL levels. However, PRL levels were notmeasured before and after therapy, and different PRLisoforms were also not examined.
In conclusion, the present study suggests a role forHPRL in SLE and manifestations including serositis andanemia. These findings indicate the need for randomizeddouble-blind placebo controlled trials to study the effect ofdopamine agonists as disease-modifying drugs in normo-prolactinemic and hypeprolactinemic autoimmune diseasesincluding SLE [106].
References
1. De Schepper J, Schiettecatte J, Velkeniers B et al (2003)Clinical and biological characterization of macroprolactinemia withand without prolactin-IgG complexes. Eur J Endocrinol149:201–207
2. Freeman ME, Kanyicska B, Lerant A, Nagy G (2000) Prolactin:structure, function, and regulation of secretion. Physiol Rev80:1523–1631
3. Bole-Feysot C, Goffin V, Edery M, Binart N, Kelly PA (1998)Prolactin (PRL) and its receptor: actions, signal transductionpathways and phenotypes observed in PRL receptor knockoutmice. Endocr Rev 19:225–258
4. Chikanza IC (1999) Prolactin and neuroimmunomodulation: invitro and in vivo observations. Ann NY Acad Sci 876:119–130
5. Serri O, Chik CL, Ur E, Ezzat S (2003) Diagnosis and managementof hyperprolactinemia. Can Med Assoc J 169:575–581
6. Jara LJ, Medina G, Saavedra MA, Vera-Lastra O, Navarro C(2011) Prolactin and autoimmunity. Clin Rev Allergy Immunol40:50–59
7. Adamson AD, Friedrichsen S, Semprini S et al (2008) Humanprolactin gene promoter regulation by estrogen: convergencewith tumor necrosis factor-alpha signaling. Endocrinology149:687–694
8. Vera-Lastra O, Jara LJ, Espinoza RL (2002) Prolactin andautoimmunity. Autoimmun Rev 1:360–364
9. Walker SE, Jacobson JD (2000) Roles of prolactin andgonadotropin-releasing hormone in rheumatic diseases. RheumDis Clin North Am 26:713–736
10. Thoreau E, Petridou B, Kelly PA, Djiane J, Mornon JP (1991)Structural symmetry of the extracellular domain of the cytokine/growth hormone/prolactin receptor family and interferon recep-tors revealed by hydrophobic cluster analysis. FEBS Lett282:26–31
11. Ben-Jonathan N, Mershon JL, Allen DL, Steinmetz RW (1996)Extrapituitary prolactin: distribution, regulation, functions, andclinical aspects. Endocr Rev 17:639–669
12. Peeva E, Zouali M (2005) Spotlight on the role of hormonalfactors in the emergence of autoreactive B-lymphocytes. Immu-nol Lett 101:123–143
Clinic Rev Allerg Immunol

13. Saha S, Gonzalez J, Rosenfeld G, Keiser H, Peeva E (2009)Prolactin alters the mechanisms of B cell tolerance induction.Arthritis Rheum 60:1743–1752
14. Athreya BH, Pletcher J, Zulian F, Weiner DB, Williams WV(1993) Subset-specific effects of sex hormones and pituitarygonadotropins on human lymphocyte proliferation in vitro. ClinImmunol Immunopathol 66:201–211
15. Sousa GM, Olivera RC, Perelra MM, Paraná R, Sousa-AttaML, Atta AM (2010) Autoimmunity in hepatitis C viruscarriers: involvement of ferritin and prolactin. AutoimmunRev (in press)
16. Jara LJ, Benitez G, Medina G (2008) Prolactin, dendritic cells,and systemic lupus erythematosus. Autoimmun Rev 7:251–255
17. Lahat N, Miller A, Shtiller R, Toubi E (1993) Differential effectsof prolactin upon activation and differentiation of human Blymphocytes. J Neuroimmunol 47:35–40
18. Orbach H, Shoenfeld Y (2007) Hyperprolactinemia and autoim-mune diseases. Autoimmun Rev 6:537–542
19. Cejkova P, Fojtikova M, Cerna M (2009) Immunomudulatoryrole of prolactin in diabetes mellitus. Autoimmun Rev 9:23–27
20. Jara LJ, Gomez-Sanchez C, Silveira LH, Martinez-Osuna P,Vasey FB, Espinoza LR (1992) Hyperprolactinemia in systemiclupus erythematosus: association with disease activity. Am JMed Sci 303:222–226
21. Allen SH, Sharp GC, Wang G et al (1996) Prolactin levels andantinuclear antibody profiles in women tested for connectivetissue disease. Lupus 5:30–37
22. Buskila D, Lorber M, Neumann L, Flusser D, Shoenfeld Y(1996) No correlation between prolactin levels and clinicalactivity in patients with systemic lupus erythematosus. JRheumatol 23:629–632
23. Alvarez-Nemegyei J, Cobarrubias-Cobos A, Escalante-Triay F etal (1998) Bromocriptine in systemic lupus erythematosus: adouble-blind, randomized, placebo-controlled study. Lupus7:414–419
24. Szyper-Kravitz M, Zandman-Goddard G, Lahita RG, ShoenfeldY (2005) The neuroendocrine-immune interactions in systemiclupus erythematosus: a basis for understanding disease patho-genesis and complexity. Rheum Dis Clin North Am 31:161–175
25. Leanos-Miranda A, Cardenas-Mondragon G (2006) Serum freeprolactin concentrations in patients with systemic lupus eryth-ematosus are associated with lupus activity. Rheumatology45:97–101
26. Rezaieyazdi Z, Hesamifard A (2006) Correlation between serumprolactin levels and lupus activity. Rheumatol Int 26:1036–1039
27. El Miedany YM, Ahmed I, Moustafa H, El Baddini M (2004)Hyperprolactinemia in Sjogren’s syndrome: a patient subset or adisease manifestation? Joint Bone Spine 71:203–208
28. Peeva E (2011) Reproductive immunology: a focus on the role offemale sex hormones and other gender-related factors. Clin RevAllergy Immunol 40:1–7
29. Blank M, Krause I, Buskila D et al (1995) Bromocriptineimmunomodulation of experimental SLE and primary antiphos-pholipid syndrome via induction of nonspecific T suppressorcells. Cell Immunol 162:114–122
30. Peeva E, Grimaldi C, Spatz L, Diamond B (2000) Bromocriptinerestores tolerance in estrogen-treated mice. J Clin Invest106:1373–1379
31. Walker SE (2001) Bromocriptine treatment of systemic lupuserythematosus. Lupus 10:762–768
32. McMurray RW, Weidensaul D, Allen SH, Walker SE (1995)Efficacy of bromocriptine in an open label therapeutic trial forsystemic lupus erythematosus. J Rheumatol 22:2084–2091
33. Jara LJ, Cruz-Cruz P, Saavedra MA et al (2007) Bromocriptineduring pregnancy in systemic lupus erythematosus. A pilotclinical trial. Ann NY Acad Sci 1110:297–304
34. Hrycek A, Pochopien-Kenig G, Cieszka J (2007) Selected acutephase proteins and interleukin-6 in systemic lupus erythematosuspatients treated with low doses of quinagolide. Autoimmunity40:217–222
35. Fojtíková M, Tomasová Studýnková J, Filková M et al (2010)Elevated prolactin levels in patients with rheumatoid arthritis:association with disease activity and structural damage. Clin ExpRheumatol 28:849–854
36. Olsen NJ, Kovacs WJ (2002) Hormones, pregnancy, andrheumatoid arthritis. J Gend-Specif Med 5:28–37
37. Brennan P, Ollier B, Worthington J, Hajeer A, Silman A (1996)Are both genetic and reproductive associations with rheumatoidarthritis linked to prolactin? Lancet 348:106–109
38. Jorgensen C, Bressot N, Bologna C, Sany J (1995) Dysregula-tion of the hypothalamo-pituitary axis in rheumatoid arthritis. JRheumatol 22:1829–1833
39. Templ E, Koeller M, Riedl M, Wagner O, Graninger W, Luger A(1996) Anterior pituitary function in patients with newlydiagnosed rheumatoid arthritis. Br J Rheumatol 35:350–356
40. Zoli A, Lizzio MM, Ferlisi EM et al (2002) ACTH, cortisol andprolactin in active rheumatoid arthritis. Clin Rheumatol21:289–293
41. Eijsbouts AM, van den Hoogen FH, Laan RF, Sweep CG,Hermus AR, van de Putte LB (2005) Decreased prolactinresponse to hypoglycaemia in patients with rheumatoidarthritis: correlation with disease activity. Ann Rheum Dis64:433–437
42. Rovensky J, Imrich R, Malis F et al (2004) Prolactin andgrowth hormone responses to hypoglycemia in patients withrheumatoid arthritis and ankylosing spondylitis. J Rheumatol31:2418–2421
43. Kullich WC, Klein G (1998) High levels of macrophageinflammatory protein-1alpha correlate with prolactin in femalepatients with active rheumatoid arthritis. Clin Rheumatol17:263–264
44. Nagafuchi H, Suzuki N, Kaneko A, Asai T, Sakane T (1999)Prolactin locally produced by synovium infiltrating T lympho-cytes induces excessive synovial cell functions in patients withrheumatoid arthritis. J Rheumatol 26:1890–1900
45. Cutolo M, Balleari E, Giusti M, Monachesi M, Accardo S (1986)Sex hormone status in women suffering from rheumatoidarthritis. J Rheumatol 13:1019–1023
46. Gutierrez MA, Garcia ME, Rodriguez JA, Mardonez G, JacobelliS, Rivero S (1999) Hypothalamic-pituitary-adrenal axis functionin patients with active rheumatoid arthritis: a controlled studyusing insulin hypoglycemia stress test and prolactin stimulation.J Rheumatol 26:277–281
47. Ram S, Blumberg D, Newton P, Anderson NR, Gama R (2004)Raised serum prolactin in rheumatoid arthritis: genuine orlaboratory artefact? Rheumatol (Oxford) 43:1272–1274
48. Seriolo B, Ferretti V, Sulli A, Fasciolo D, Cutolo M (2002)Serum prolactin concentrations in male patients with rheumatoidarthritis. Ann NY Acad Sci 966:258–262
49. Mateo L, Nolla JM, Bonnin MR, Navarro MA, Roig-Escofet D(1998) High serum prolactin levels in men with rheumatoidarthritis. Rheumatol 25:2077–2082
50. Orbach H, Zandman-Goddard G, Amital H et al (2007) Novelbiomarkers in autoimmune diseases: prolactin, ferritin, vitaminD, and TPA levels in autoimmune diseases. Ann NY Acad Sci1109:385–400
51. Dougados M, Duchesne L, Amor B (1988) Bromocriptine andcyclosporin A combination therapy in rheumatoid arthritis.Arthritis Rheum 31:1333–1334
52. Marguerie C, David J, So A, Walport M (1990) A pilot studycomparing bromocriptine with D-penicillamine in the treatmentof rheumatoid arthritis. Br J Rheumatol 29(suppl 2):3
Clinic Rev Allerg Immunol
53. Mader R (1997) Bromocriptine for refractory rheumatoidarthritis. Harefuah 133:527–529
54. Figueroa F, Carrion F, Martinez M, Rivero S, Mamani I (1997)Bromocriptine induces immunological changes related to diseaseparameters in rheumatoid arthritis. Br J Rheumatol 36:1022–1027
55. Eijsbouts A, van den Joogen F, Laan R, Hermus A, Sweep F,van de Putte L (1999) Treatment of rheumatoid arthritis withthe dopamine agonist quinagolide. J Rheumatol 26:2284–2285
56. Erb N, Pace A, Delamere J, Kitas G (2001) Control ofunremitting rheumatoid arthritis by the prolactin antagonistcabergoline. Rheumatology 40:237–239
57. Riskind PN, Massacesi L, Doolittle TH, Hauser SL (1991) Therole of prolactin in autoimmune demyelination: suppression ofexperimental allergic encephalomyelitis by bromocriptine. AnnNeurol 29:542–527
58. Dijkstra CD, van der Voort ER, De Groot CJ et al (1994)Therapeutic effect of the D2-dopamine agonist bromocriptine onacute and relapsing experimental allergic encephalomyelitis.Psychoneuroendocrinology 19:135–142
59. Kira J, Harada M, Yamaguchi Y, Shida N, Goto I (1991)Hyperprolactinemia in multiple sclerosis. J Neurol Sci102:61–66
60. Azar ST, Yamout B (1999) Prolactin secretion is increased inpatients with multiple sclerosis. Endocrin Res 25:207–214
61. Zych-Twardowska E, Wajgt A (1999) Serum prolactin and sexhormone concentrations in patients withmultiple sclerosis. MedSci Monit 5:216–220
62. Yamasaki K, Horiuchi I, Minohara M et al (2000) Hyper-prolactinemia in optico-spinal multiple sclerosis. Intern Med39:296–299
63. Safarinejad MR (2008) Evaluation of endocrine profile, hypo-thalamic–pituitary–testis axis and semen quality in multiplesclerosis. J Neuroendocrinol 20:1368–1375
64. Markianos M, Koutsis G, Evangelopoulos ME, Mandellos D,Sfagos C (2010) Serum and cerebrospinal fluid prolactin levelsin male and female patients with clinically-isolated syndrome orrelapsing-remitting multiple sclerosis. J Neuroendocrinol22:503–508
65. Da Costa R, Szyper-Kravitz M, Szekanecz Z et al. (2011)Ferritin and prolactin levels in multiple sclerosis. Isr Med AssocJ (in press)
66. Nociti V, Frisullo G, Tartaglione T et al (2010) Multiple sclerosisattacks triggered by hyperprolactinemia. J Neurooncol 98:407–409
67. RederAT LMT (1993) Serum prolactin levels in active multiplesclerosis and during cyclosporin treatment. J Neurol Sci117:192–196
68. Wei T, Lightman SL (1997) The neuroendocrine axis in patientswith multiple sclerosis. Brain 120:1067–1076
69. Heesen C, Gold SM, Bruhn M, Mönch A, Schulz KH (2002)Prolactin stimulation in multiple sclerosis—an indicator ofdisease subtypes and activity? Endocr Res 28:9–18
70. Harirchian MH, Sahralan MA, Shirani A (2006) Serum prolactinlevel in patients with multiple sclerosis: a case control study.Med Sci Monit 12:177–180
71. Bissay V, De Klippelm N, Herroelenm L et al (1994)Bromocriptine therapy in multiple sclerosis: an open label pilotstudy. Clin Neuropharmacol 17:473–476
72. Then Bergh F, Kuemple T, Schumann E et al (2006) Monthly i.v.methylprednisolone in relapsing remitting MS-reduction ofenhancing lesions, T2 lesion volume and plasma prolactinconcentrations. BMC Neurol 23:19
73. Steen VD (1999) Pregnancy in women with systemic sclerosis.Obstet Gynecol 94:15–20
74. Hilty C, Brühlmann P, Sprott H et al (2000) Altered diurnalrhythm of prolactin in systemic sclerosis. J Rheumatol 27:2160–2165
75. Shahin AA, Abdoh S, Abdelrazik M (2002) Prolactin andthyroid hormones in patients with systemic sclerosis: corre-lations with disease manifestations and activity. Z Rheumatol61:703–709
76. Czuwara-Ladykowska J, Sicinska J, Olszewska M, Uhrynowska-Tyszkiewicz I, Rudnicka L (2006) Prolactin synthesis bylymphocytes from patients with systemic sclerosis. BiomedPharmacother 60:152–155
77. La Montagna G, Baruffo A, Pasquali D, Bellastella A, Tirri G,Sinisi AA (2001) Assessment of pituitary gonadotropin releaseto gonadotropin releasing hormone/thyroid-stimulating hormonestimulation in women with systemic sclerosis. Rheumatol(Oxford) 40:310–314
78. Vera-Lastra O, Jara LJ, Medina G et al (2006) Functionalhyperprolactinemia and hypophyseal microadenoma in systemicsclerosis. J Rheumatol 33:1108–1112
79. Straub RH, Zeuner M, Lock G, Schölmerich J, Lang B (1997)High prolactin and low dehydroepiandrosterone sulphate ser-umlevels in patients with severe systemic sclerosis. Br JRheumatol 36:426–432
80. Buskila D, Berezin M, Gur H et al (1995) Autoantibody profilein the sera of women with hyperprolactinemia. J Autoimmun8:415–424
81. Haga HJ, Rygh T (1999) The prevalence of hyperprolactinemiain patients with primary Sjögren’s syndrome. J Rheumatol26:1291–1295
82. Gutiérrez MA, Anaya JM, Scopelitis E, Citera G, Silveira L,Espinoza LR (1994) Hyperprolactinaemia in primary Sjögren’ssyndrome. Ann Rheum Dis 53:425
83. Steinfeld S, Rommes S, François C et al (2000) Big prolactin60 kDa is overexpressed in salivary glandular epithelial cellsfrom patients with Sjögren’s syndrome. Lab Invest 80:239–247
84. Johnson EO, Moutsopoulos HM (2000) Neuroendocrine mani-festationsin Sjögren’s syndrome. Relation to the neurobiology ofstress. Ann NY Acad Sci 917:797–808
85. Legakis I, Petroyianni V, Saramantis A, Tolis G (2001) Elevatedprolactin to cortisol ratio and polyclonal autoimmune activationin Hashimoto’s thyroiditis. Horm Metab Res 33:585–589
86. Notsu K, Ito Y, Furuya H, Ohguni S, Kato Y (1997) Incidence ofhyperprolactinemia in patients with Hashimoto’s thyroiditis.Endocr J 44:89–94
87. Poyraz BC, Aksoy C, Balcıoğlu I (2008) Increased incidenceof autoimmune thyroiditis in patients with antipsychotic-induced hyperprolactinemia. Europ Neuropsychopharmacol18:667–672
88. Ward MM, Marx AS, Barry NN (2000) Comparison of thevalidity and sensitivity to change of 5 activity indices in systemiclupus erythematosus. J Rheumatol 27:664–670
89. Jacobi AM, Rohde W, Ventz M, Riemekasten G, Burmester GR,Hiepe F (2001) Enhanced serum prolactin (PRL) in patients withsystemic lupus erythematosus: PRL levels are related to thedisease activity. Lupus 10:554–561
90. Leaños-Miranda A, Pascoe-Lira D, Chávez-Rueda KA, Blanco-Favela F (2001) Antiprolactin autoantibodies in systemic lupuserythematosus: frequency and correlation with prolactinemia anddisease activity. J Rheumatol 28:1546–1553
91. Paciliom M, Migliaresim S, Melim R, Ambrosonem L, BigliardomB, Di Carlo R (2001) Elevated bioactive prolactin levels in systemiclupus erythematosus-association with disease activity. J Rheumatol28:2216–2221
92. Shabanova SS, Ananieva LP, Alekberova ZS, Guzov II (2008)Ovarian function and disease activity in patients with systemiclupus erythematosus. Clin Exp Rheumatol 26:436–441
Clinic Rev Allerg Immunol

93. McMurray R, Keisler D, Kanuckel K, Izui S, Walker SE (1991)Prolactin influences autoimmune disease activity in the femaleB/W mouse. J Immunol 147:3780–3787
94. McMurray R, Keisler D, Izui S, Walker SE (1994) Hyper-prolactinemia in male NZB/NZW (B/W) F1 mice: acceleratedautoimmune disease with normal circulating testosterone. ClinImmunol Immunopathol 71:338–343
95. Rovenský J, Juránková E, Rauová L et al (1997) Relationshipbetween endocrine, immune, and clinical variables in patientswith systemic lupus erythematosus. J Rheumatol 24:2330–2334
96. Ferreira C, Paes M, Gouveia A, Ferreira E, Padua F, Fiuza T(1998) Plasma homovanillic acid and prolactin in systemic lupuserythematosus. Lupus 7:392–397
97. Jimena P, Aguirre MA, Lopez-Curbelo A, de Andres M, Garcia-Courtay C, Cuadrado MJ (1998) Prolactin levels in patient withsystemic lupus erythematosus: a case controlled study. Lupus7:383–386
98. Blanco-Favela F, Quintal-Alvarez G, Leanos-Miranda A (1999)Association between prolactin and disease activity in systemiclupus erythematosus. Influence of statistical power. J Rheumatol26:55–59
99. Leanos-Miranda A, Chavez-Rueda KA, Blanco-Favela F (2001)Biologic activity and plasma clearance of prolactin-IgG complex
in patients with systemic lupus erythematosus. Arthritis Rheum44:866–875
100. Leanos A, Pascoe D, Fraga A, Blanco-Favela F (1998) Anti-prolactin autoantibodies in systemic lupus erythematosuspatients with associated hyperprolactinemia. Lupus 7:398–403
101. Jara LJ, Vera-Lastra O, Miranda JM, Alcala M, Alvarez-Nemegyei J (2001) Prolactin in human systemic lupus eryth-ematosus. Lupus 10:748–756
102. Jara LJ, Irigoyen L, de Ortiz MJ, Zazueta B, Bravo G, EspinozaLR (1998) Prolactin and interleukin-6 in neuropsychiatric lupuserythematosus. Clin Rheumatol 17:110–114
103. Zoli A, Ferlisi EM, Pompa A et al (1999) Basal and after-stimulitest for prolactinemia in systemic lupus erythematosus. Ann NYAcad Sci 876:155–158
104. Rastin M, Hatef MR, Tabasi N, Sheikh AM, Abbasi J,Mahmoudi M (2007) Sex hormones and peripheral white bloodcell subsets in systemic lupus erythematosus patients. Iran JImmunol 4:110–115
105. Praprotnik S, Agmon-Levin N, Porat-Katz BS et al (2010)Prolactin’s role in the pathogenesis of the antiphospholipidsyndrome. Lupus 19:1515–1519
106. Alarcón-Segovia D (2001) The future of treatment for systemiclupus erythematosus. Isr Med Assoc J 3:127–130
Clinic Rev Allerg Immunol
Related Documents