August 13, 2019 VIA ELECTRONIC SUBMISSION Secretary Alex Azar Department of Health and Human Services Hubert H. Humphrey Building, Room 509F, 200 Independence Avenue SW, Washington, DC 20201 RE: HHS-OCR-2019-0007: Nondiscrimination in Health and Health Education Programs or Activities Dear Secretary Azar, On behalf of the American Academy of Pediatrics (AAP), a non-profit professional organization of 67,000 primary care pediatricians, pediatric medical subspecialists, and pediatric surgical specialists dedicated to the health, safety and well-being of infants, children, adolescents, and young adults, and the Society for Adolescent Health and Medicine (SAHM), a multidisciplinary organization that promotes optimal health, well- being, and equity for all adolescents and young adults by supporting adolescent health and medicine professionals through the advancement of clinical practice, care delivery, research, advocacy, and professional development, we write to express strong opposition to the proposed rule entitled “Nondiscrimination in Health and Health Education Programs or Activities” by the Department of Health and Human Services (HHS), the Centers for Medicare & Medicaid Services (CMS), and the Office for Civil Rights (OCR) (collectively, “the Department”). Many children face discrimination in health care systems and settings that can impede their ability to access the services they need for healthy development. Such limited access to comprehensive, developmentally appropriate care poses a barrier for children to thrive throughout their lives. For example, the impact of discrimination in childhood years has been linked to toxic stress, which compounded over time predisposes them to a higher likelihood of chronic disease in adulthood and other long-term negative health outcomes. 1 While the Department proposes to revise the regulation with the justification that it would “better comply with the mandates of Congress, address legal concerns, relieve billions of dollars in undue regulatory burdens, further substantive compliance, reduce confusion, and clarify the scope of Section 1557 in keeping with pre- existing civil rights statutes and regulations,” it is clear that end result of the proposed changes would be to reduce the number and type of entities required to comply with Section 1557’s non-discrimination protections. The 2016 rule removed barriers to health care for our nation’s children and adolescents. If finalized, these changes would have the opposite effect. 1 https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources/discrimination#5

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

August 13, 2019 VIA ELECTRONIC SUBMISSION Secretary Alex Azar Department of Health and Human Services Hubert H. Humphrey Building, Room 509F, 200 Independence Avenue SW, Washington, DC 20201 RE: HHS-OCR-2019-0007: Nondiscrimination in Health and Health Education Programs or Activities Dear Secretary Azar, On behalf of the American Academy of Pediatrics (AAP), a non-profit professional organization of 67,000 primary care pediatricians, pediatric medical subspecialists, and pediatric surgical specialists dedicated to the health, safety and well-being of infants, children, adolescents, and young adults, and the Society for Adolescent Health and Medicine (SAHM), a multidisciplinary organization that promotes optimal health, well-being, and equity for all adolescents and young adults by supporting adolescent health and medicine professionals through the advancement of clinical practice, care delivery, research, advocacy, and professional development, we write to express strong opposition to the proposed rule entitled “Nondiscrimination in Health and Health Education Programs or Activities” by the Department of Health and Human Services (HHS), the Centers for Medicare & Medicaid Services (CMS), and the Office for Civil Rights (OCR) (collectively, “the Department”). Many children face discrimination in health care systems and settings that can impede their ability to access the services they need for healthy development. Such limited access to comprehensive, developmentally appropriate care poses a barrier for children to thrive throughout their lives. For example, the impact of discrimination in childhood years has been linked to toxic stress, which compounded over time predisposes them to a higher likelihood of chronic disease in adulthood and other long-term negative health outcomes.1 While the Department proposes to revise the regulation with the justification that it would “better comply with the mandates of Congress, address legal concerns, relieve billions of dollars in undue regulatory burdens, further substantive compliance, reduce confusion, and clarify the scope of Section 1557 in keeping with pre-existing civil rights statutes and regulations,” it is clear that end result of the proposed changes would be to reduce the number and type of entities required to comply with Section 1557’s non-discrimination protections. The 2016 rule removed barriers to health care for our nation’s children and adolescents. If finalized, these changes would have the opposite effect.
1 https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-health/interventions-resources/discrimination#5
American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 2
The AAP and SAHM strongly oppose the proposed rule, which would severely threaten access to care for millions of children and adolescents, including those that identify as LGBTQ, those with limited English proficiency, and those who have sought or may seek comprehensive reproductive health services. Despite civil rights protections established in statute, the proposed rule could have grave consequences through the limited definitions of discrimination, the narrowing of covered entities, and the changes to enforcement. As such, we urge the Department to rescind the proposed rule in its entirety and leave the 2016 final rule in place. Our comments include numerous citations to supporting research, including direct links to the research for the benefit of HHS in reviewing our comments. We direct HHS to each of the studies cited and made available to the agency through active hyperlinks, and we request that the full text of each of the studies cited, along with the full text of our comments, be considered part of the administrative record in this matter for purposes of the Administrative Procedure Act. Our specific comments are below.
Discrimination on the Basis of Sex, Gender Identity, and Sexual Orientation
The AAP and SAHM strive to improve health care access and eliminate disparities for children and teenagers who identify as lesbian, gay, bisexual, transgender, or questioning (LGBTQ) of their sexual or gender identity.23 Despite some advances in public awareness and legal protections, youth who identify as LGBTQ continue to face disparities that stem from multiple sources, including inequitable laws and policies, societal discrimination, and a lack of access to quality health care, including mental health care. Such challenges are often more intense for youth who do not conform to social expectations and norms regarding gender.
Youth who identify as transgender and gender diverse (TGD) face unique health disparities.4 These youth often confront stigma and discrimination, which contribute to feelings of rejection and isolation that can adversely affect physical and emotional well-being. Youth who identify as TGD experience disproportionately high rates of homelessness, physical violence at home and in the community, substance abuse, and high-risk sexual behaviors.5,6 Among the 3 million HIV testing events that were reported in 2015, the highest percentages of new infections were among women who identified as transgender, and these women were also at particular risk for not knowing their HIV status.7
In addition to societal challenges, youth who identify as TGD face several barriers within the health care system, especially regarding access to care. One study from the National Center for Transgender Equality
2 Recommendations for Promoting the Health and Well-Being of Lesbian, Gay, Bisexual, and Transgender Adolescents: A Position Paper of the Society for Adolescent Health and Medicine.” Journal of Adolescent Health 52, no. 4 (2013): 506–10. doi:10.1016/j.jadohealth.2013.01.015 https://www.jahonline.org/article/S1054-139X%2813%2900057-8/fulltext 3 Rafferty J. Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and Adolescents. Pediatrics. 2018;142(4). https://pediatrics.aappublications.org/content/142/4/e20182162 4 Ibid. 5 Tishelman AC, Kaufman R, Edwards-Leeper L, Mandel FH, Shumer DE, Spack NP. Serving transgender youth: challenges, dilemmas and clinical examples. Prof Psychol Res Pr. 2015;46(1):37–45pmid:26807001 6 Adelson SL; American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2012;51(9):957–974pmid:22917211 7 Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N; HIV/AIDS Prevention Research Synthesis Team. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav. 2008;12(1):1–17pmid:17694429
American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 3
found that approximately 25% of individuals who identified as transgender were denied insurance coverage because of being transgender.8 In 2012, a large gender center in Boston, Massachusetts, reported that most young patients who identified as transgender and were deemed appropriate candidates for recommended gender care were unable to obtain it because of such denials, which were based on the premise that gender dysphoria was a mental disorder, not a physical one, and that treatment was not medically or surgically necessary.9
This evidence of discrimination against children and youth who identify as LGBTQ led the Academy to support the 2016 rule's prohibitions on discrimination on the basis of sex, which includes sex stereotyping and gender identity in the definition of sex discrimination. Prior to the finalization of the 2016 rule, the AAP also urged HHS to explicitly include protections based on sexual orientation as well as clarify protections for individuals with non-binary gender identities.10 Protections against discrimination based on sexual orientation and gender identity align with the AAP policy to provide youth with access to comprehensive gender-affirming and developmentally appropriate health care.
The Department proposes to remove gender identity and sex stereotyping from the definition of prohibited sex-based discrimination, which could allow health care providers to refuse to provide care to individuals who are transgender or who do not conform to traditional sex stereotypes. This would drastically exacerbate the stark inequities that already exist for youth who identify as TGD as it relates to access to care. This practice would only increase stigma, prolong gender dysphoria, and worsen already poor mental health outcomes. Furthermore, it may also lead patients to seek nonmedically supervised treatments that are potentially dangerous.
Moreover, the proposed rule would no longer prohibit covered entities from denying, limiting, or imposing additional cost-sharing for services that are ordinarily or exclusively available to one sex or gender when those services are sought by an individual of a different sex or gender. The proposal would also eliminate the provision that prohibits a health plan from categorically or automatically excluding or limiting coverage for health services related to gender transition. The rollback of these protections could have a devastating impact on access to medically necessary services for youth who identify as TGD and adversely affect self-esteem and contribute to the perception that they are undervalued by society and the health care system. Furthermore, insurance denials can reinforce a socioeconomic divide between those who can finance the high costs of uncovered care and those who cannot.
To illustrate the impact of such discrimination on children, a pediatrician from Arizona shared the experience of one of his transgender patients. After expressing a male gender identity at the age of 9, the boy was referred by his former physician to a psychiatrist who offered conversion therapy. The experience worsened the child’s mental health issues and depression until his mother pulled him out and started to affirm his identity. When the physician refused to use the patient’s preferred pronouns or call him by his new name, the family had to find a new provider. Later, when the patient needed medication to support his development through puberty, the family was repeatedly denied by his Medicaid provider. When the family took legal action, the patient prevailed in the case thanks to the strong protections outlined in Section 1557.
8 James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016 9 Edwards-Leeper L, Spack NP. Psychological evaluation and medical treatment of transgender youth in an interdisciplinary “Gender Management Service” (GeMS) in a major pediatric center. J Homosex. 2012;59(3):321–336pmid:22455323 10 https://downloads.aap.org/DOFA/1557%20comments%20final.pdf
American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 4
If finalized, this proposed rule would severely threaten TGD patients’ access to all forms of health care, including patients like this boy in Arizona. The rule would create confusion among patients and providers about their rights and obligations and would promote discrimination. The proposed rule would encourage hospitals to deny care to people who identify as TGD and enable insurance companies to deny individuals who identify as transgender coverage for health care services that they cover for those who identify as cisgender.
Furthermore, the proposed rule opens the door to discrimination on the basis of pregnancy termination or other pregnancy-related status, creating inappropriate barriers to realizing optimal sexual and reproductive health for adolescents and young adults. Ensuring that adolescents have access to comprehensive health care, including reproductive health care, has been a long-standing objective of our organizations. Timely access to medical care is especially important for pregnant teenagers because of the significant medical, personal, and social consequences of adolescent childbearing. The AAP and SAHM strongly advocate for the prevention of unintended adolescent pregnancy by supporting comprehensive health and sexuality education,1112 abstinence, and the use of effective contraception1314 by sexually active youth. We strongly support minors' access to all medical options regarding undesired pregnancy, including the right to obtain an abortion, and the right to access care unhindered by discrimination on the basis of their reproductive health decisions.
The 2016 rule is the product of a lengthy process of deliberation and public input. The rule was developed over the course of six years of study and following two comment periods, with more than 25,000 comments from stakeholders, including the Academy, which were overwhelmingly supportive of inclusion of protections against discrimination based on sex stereotyping and gender identity. HHS engaged stakeholders through listening sessions, participation in conferences, and other outreach prior to taking regulatory action.
The AAP and SAHM strive to improve health care access and eliminate disparities for children and teenagers including those who identify as LGBTQ and those who seek the full spectrum of reproductive health options. This proposed rule is in direct contradiction with that mission.
Explicit Religious Exemptions
The AAP and SAHM collectively represent nearly 70,000 members of all faiths and serve children and families of all faiths. The free exercise of religion is an important societal value, which must be balanced against other important societal values, such as protecting children from serious harm and ensuring child health and well-being. As outlined in previous comments regarding “Protecting Statutory Conscience Rights in Health Care,” the AAP urges HHS to ensure that health care providers follow evidence-based or evidence-informed practices that facilitate optimal access to services that support healthy children and families.15
We are concerned about the implications of the proposed rule, which would allow discrimination against children, adolescents, and young adults when a health care provider or other covered entity uses religious beliefs as justification to deny, delay, or discourage patients from receiving needed health care services. This
11 https://pediatrics.aappublications.org/content/138/2/e20161348 12 Improving Knowledge About, Access to, and Utilization of Long-Acting Reversible Contraception Among Adolescents and Young Adults.” Journal of Adolescent Health 60, no. 4 (2017): 472–74. doi:10.1016/j.jadohealth.2017.01.010. https://www.jahonline.org/article/S1054-139X(17)30053-8/fulltext 13 https://pediatrics.aappublications.org/content/134/4/e1244 14 Improving Knowledge About, Access to, and Utilization of Long-Acting Reversible Contraception Among Adolescents and Young Adults.” Journal of Adolescent Health 60, no. 4 (2017): 472–74. doi:10.1016/j.jadohealth.2017.01.010. https://www.jahonline.org/article/S1054-139X%2814%2900052-4/fulltext 15https://downloads.aap.org/DOFA/AAP%20Comments%20HHS%20Conscience%20Protections%20NPRM%20Final_March%202018.pdf

American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 5
could place patients at risk of serious or life-threatening outcomes in emergencies and other circumstances where the individual’s choice of health care provider is limited. For instance, the proposed rule may allow a health care provider to refuse care to an adolescent who seeks basic information on reproductive health, such as the routine use of contraception for pregnancy prevention, simply because the provider objects to such care. Situations such as these may be more likely to occur because the proposed rule raises more questions about nondiscrimination protections and exemptions than it answers.
By permitting sex discrimination based on a provider's religious beliefs, the proposed rule hinders the delivery of reproductive health care aligned with clinical guidelines and the recommendations of major professional medical organizations, including the AAP. As such, the AAP and SAHM strongly object to the blanket religious exemptions proposed by HHS. Allowing religious exemptions as the rule proposes will discriminate against women seeking necessary reproductive health care services. Any such exemption would be contrary to Congressional intent and the express purpose of Section 1557 and has the potential to cause great harm to our patients.
Rollback of Language Access Requirements
Immigrant children or children with immigrant parents, groups that face persistent discrimination in accessing health care, represent the fastest growing segment of the US population. One in every 4 children in the United States, approximately 18.6 million children, lives in an immigrant family.16 Children of immigrant families are nearly twice as likely to be uninsured compared to children of nonimmigrant families.
Even when immigrant children and families can access health care providers, they face further obstacles when language barriers prevent effective communication between pediatricians, children, and families on medical issues. Although many immigrant children speak English, their parents may not, creating a barrier that can prevent families from accessing needed health services and/or causing inadequate communication with health care providers. Without access to qualified medical interpreters in health care settings, language barriers can place English-speaking children in the difficult position of interpreting between health care providers and their family members.17
The Academy has previously recommended that all health facilities have access to trained interpreter services and that CMS require Medicaid to provide full payment for these services for patients with LEP.18 Similarly, we strongly supported the 2016 rule’s specific requirements to ensure meaningful access for individuals with limited English proficiency because they help to prevent discrimination and improve the quality of care for children and families. When in-person interpreter services are not possible, remote interpretation serves as a crucial tool for providers to improve communication with patients and families19 and we encourage the Department to maintain the current standards for remote video interpreting.
Patients and families with LEP need adequate language resources and access to language professionals—including posted signs in multiple languages, written materials, live interpreters (preferably in-person, but also remote video and telephonic interpreters), and dedicated translators of written instructions. Such services are not only crucial for equitable care but have been demonstrated to improve patient care outcomes and
16 Children of Immigrants Data Tool. https://datatool.urban.org/charts/datatool/pages.cfm#. 17 https://pediatrics.aappublications.org/content/131/6/e2028..info 18 https://downloads.aap.org/DOFA/1557%20RFI%20Comment%20Letter%20Final.pdf 19 Lion KC, Brown JC, Ebel BE et al. Effect of Telephone vs Video Interpretation on Parent Comprehension, Communication, and Utilization in the Pediatric Emergency Department: A Randomized Clinical Trial. JAMA Pediatr. 2015;169(12):1117-1125. doi:10.1001/jamapediatrics.2015.2630

American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 6
satisfaction.20 For example, a pediatrician from South Carolina shares the successful experience of a hospital with full-time, in-person interpreters, where parents and pregnant women often drive more than an hour to seek medical care for themselves and their children because they know they will have an in-person interpreter, which they know will improve their capacity to support their own health and well-being. In one instance, a child with severe visual impairment and limited English proficiency was able to connect to primary pediatric care only because the interpreter recognized that he did not have a medical home and called a case manager to facilitate connection to care.
When language services are lacking, patient care suffers. In one study, 80% of health care providers reported encountering patients with LEP,21 and under the proposed changes may be forced to resort to harmful alternatives to a licensed, qualified, medical interpreter: they may rely on inadequate second language skills, recruit untrained bilingual staff or strangers ad hoc, incorrectly assume patients understand English, or place children in the uncomfortable and unethical position of interpreting for their parents. Inadequate language resources can ultimately lead to negative, costly, and sometimes deadly consequences. For example, one New England Journal of Medicine article discusses cases of medication being placed in the ear instead of taken by mouth, resulting in paralysis and a $71 million lawsuit.22
A pediatrician from South Carolina shares a patient example from her local community hospital, where a pregnant mother presented in labor without the availability of an interpreter. The mother was subsequently not able to understand the questions or instructions provided due to a language barrier and lack of an interpreter. The infant was admitted to the neonatal intensive care unit, leading to increased medical expenses and serious stress for the family, an admission that may have been preventable and was attributed to communication barrier.
The Department has provided no explanation for how individuals will know of their rights and how elimination of notices will not deny individuals with LEP, LGBTQ persons, women, and persons with disabilities meaningful access. Similarly, without fully translated documents, taglines are necessary to ensure that individuals with LEP are aware of the protections available under the law, and to ensure compliance under Section 1557. Without notice and appropriate taglines, members of the public will have limited means of knowing that language services and auxiliary aids and services are available, how to request them, what to do if they face discrimination, that they have the right to file a complaint, and how to file such a complaint.
Overall, we strongly disagree with the Department’s assertions that the nondiscrimination notice, taglines and language access plan language in the 2016 Final Rule were not justified by need, or that they are overly burdensome. These proposed changes would limit access to care for the 25.5 million individuals with LEP in the U.S. and result in discrimination based on national origin for this already-vulnerable population. Further, our organizations oppose these changes because they can result in direct patient harm for patients with LEP, including improper use of medication, incorrect understanding of treatment options, or inadequate informed consent. Such errors could result in adverse, costly health consequences or death.
Discrimination on the Basis of Disability
Although the Department proposes to retain the protections outlined in the current regulation related to effective communication for individuals with disabilities, it requests public comment on whether some of
20 Karliner LS, Jacobs EA, Chen AH, Mutha S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42(2):727-754. doi:10.1111/j.1475-6773.2006.00629.x 21 Proctor K, Wilson-Frederick SM, Haffer SC. The Limited English Proficient Population: Describing Medicare, Medicaid, and Dual Beneficiaries. Health Equity. 2018;2(1):82-89. doi:10.1089/heq.2017.0036 22 Flores G. Language Barriers to Health Care in the United States. N Engl J Med. 2006;355(3):229-231. doi:10.1056/NEJMp058316
American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 7
these provisions should be relaxed, including: 1) exempting entities with fewer than 15 employees from providing auxiliary aids and services to ensure effective communication; 2) whether all covered entities should be subject to the architectural standards applicable to public buildings; and 3) whether the provision requiring covered entities to make reasonable modifications in policies, practices, and procedures to avoid disability-based discrimination should be revised to include an exemption for undue hardship.
Over the past 50 years, the number of children living with disabilities has tripled, largely as the result of health care advances that have allowed their survival. Despite these changing demographics, the health care system continues to use an outdated approach that emphasizes acute illness and well-child care and de-emphasizes long-term management of chronic conditions and disabilities. Children with disabilities and special health care needs disproportionately lack access to a comprehensive medical home, despite evidence that receiving care in a medical home can profoundly improve outcomes for these children: increased access to subspecialty care, fewer missed days of school, and decreased family financial burden.23 The AAP and SAHM urge the Department to maintain communication and physical access protections for individuals with disabilities to enable more children to benefit from the care coordination and other benefits of a medical home.
Our organizations strongly support the current provisions requiring effective communication for individuals with disabilities and accessibility standards, including the requirements for websites and electronic and information technology. Relaxing any of the provisions outlined above would disproportionately impact children and could harm their access to necessary services and care.
Narrowing the Scope of Application
While the AAP and SAHM are extremely concerned about the negative impact the proposed rule would have on the specific populations outlined above, we are also concerned about its broader impact on children and families as it relates to the proposed changes the Department outlines to the scope of application.
Section 1557, according to the statute and current regulations, applies to health care programs and activities receiving federal financial assistance or funding; programs administered by the federal government, including Medicare and the Indian Health Service (IHS); and entities created under Title I of the ACA. Covered entities include hospitals, clinics, and health care provider’s offices and issuers selling health insurance plans within and outside of the ACA Marketplaces.24 If an entity is principally engaged in providing or administering health services or health insurance coverage, the current regulations state that all of its activities are covered by Section 1557 if any part receives federal financial assistance.
The Department proposes to significantly limit the applicability of Section 1557 protections to exclude health insurance plans that do not receive federal financial assistance (ie, Qualified Health Plans sold through the marketplaces that receive premium tax credits, or Medicaid/Children’s Health Insurance Plan coverage that includes federal funding,) leaving children and families in other plans vulnerable to discrimination. In particular, the narrowing of scope would exclude short-term, limited duration (STLD) insurance plans, plans sold outside the marketplaces, and employer-sponsored plans – plans that consumers believe offer them the ACA’s protections against discrimination. As noted in prior comment letters opposing the expansion of STLD plans25 and Association Health Plans,26 families who purchase these plans could be subject to pre-existing condition exclusions, annual or lifetime limits, limited benefits with no guaranteed coverage of essential health benefits, rating restrictions based on health status, and no guaranteed renewability without medical
23 https://pdfs.semanticscholar.org/6dea/d6bdcc602e719951e1700aee223675d424d4.pdf 24 42 U.S.C. § 18116(a); 45 C.F.R. §§ 92.2(a), 92.4. 25 https://downloads.aap.org/DOFA/SKGSTLDI.pdf 26 https://downloads.aap.org/DOFA/SKGAHP.pdf

American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 8
underwriting. In addition, children may not have access to a full range of in-network pediatric providers to ensure they receive all necessary care, given the lack of network adequacy requirements for these plans. Our organizations oppose any expansion of short-term plans and is concerned that the language in the preamble will lead to the further proliferation of insurance products that do not comply with ACA consumer protections.
Additionally, the Department proposes narrowing the scope of the rule to cover only the specific programs and activities that receive federal funding, and not all operations, of health insurers that are not principally engaged in the business of providing health care. This change would dramatically limit the scope of nondiscrimination protections for health insurance products. Under current rules, Section 1557 applies to any insurer that receives federal financial assistance, including from premium tax credits or Medicaid/Children’s Health Insurance Program (CHIP) managed care payments. The current regulations apply to the insurer itself, meaning any product sold by that insurer must comply with Section 1557 and cannot discriminate based on race, color, national origin, age, disability, or sex. Thus, under the current rule, insurers must comply with Section 1557 across their various lines of business including in the individual marketplaces, in group markets, or in self-insured group plans, not just for the products for which they receive federal financial assistance.
In contrast, under the proposed rule, the Department would apply Section 1557 only to the specific operations for which insurers receive federal financial assistance. The other parts of an insurer’s business, such as their sale of non-ACA products, would no longer have to comply with Section 1557. As a result, Section 1557 would no longer apply to the insurer and its entire operations; but only to specific operations that are federally funded.
The result of these changes is an overall reduction of the number and type of entities required to comply with Section 1557’s non-discrimination protections. Thus, most patients who have healthcare coverage will be potentially subjected to discrimination at the plan and the provider level with no legal recourse. If finalized, the proposed rule would have severe implications for children and families’ access to care. We strongly oppose the proposed changes to scope of applicability of Section 1557 antidiscrimination protections.
Weakening of Enforcement Mechanisms
In addition to limiting the applicability of Section 1557, the proposed rule also weakens the enforcement mechanism that governs Section 1557, which will make it more difficult for children and families experiencing discrimination to seek legal recourse.
The proposed changes to section 92.301, newly designated section 92.5, would severely weaken the enforcement mechanisms that exist under the current regulation. In the case of a complaint against a recipient of federal financial assistance or a state-based marketplace, OCR currently enforces Section 1557 using the procedures applicable to Title VI of the Civil Rights Act. The rules also prohibit intimidation or retaliation and include an assurance that compensatory damages are available in 1557 actions.
All of these specific provisions would be eliminated under the proposed rule, which delegates full enforcement authority to the director of OCR to handle complaints, conduct compliance reviews, initiate investigations, and make referrals to the DOJ. Additionally, the Department would eliminate a current provision that allows individuals or entities to sue directly in federal court under Section 1557.
We strongly oppose the Department’s proposed weakening of the current enforcement mechanisms. A meaningful enforcement mechanism is necessary to ensure nondiscrimination in benefit design, including codification of the transgender-inclusive protections in the proposed rule and clarification that Section 1557 prohibits other forms of discrimination, such as restricting access to medications used to treat specific
American Academy of Pediatrics and Society for Adolescent Health and Medicine Page 9
conditions by placing them in high cost-sharing tiers, or by using discriminatory standards to determine medical necessity for specific populations or conditions.
In conclusion, our organizations appreciate the opportunity to comment on the proposed rule. We are concerned that the proposed changes would severely threaten access to care for millions of children, including those that identify as LGBTQ, those with limited English proficiency, and those who have sought or may seek comprehensive reproductive health services, ultimately leading to poorer health outcomes or unlawful coverage denials. We urge the Department to immediately rescind the proposed rule and confirm the retention of the current rule, finalized in 2016. If you have any further questions, please don’t hesitate to contact Stephanie Glier in the AAP Washington, D.C. office at 202-347-8600 or [email protected].
Sincerely,
Kyle E. Yasuda, MD, FAAP Maria Trent, MD, MPH, FSAHM President, American Academy of Pediatrics President, Society for Adolescent Health and Medicine KY/nw
Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and AdolescentsJason Rafferty, MD, MPH, EdM, FAAP, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH, COMMITTEE ON ADOLESCENCE, SECTION ON LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESS
As a traditionally underserved population that faces numerous health disparities, youth who identify as transgender and gender diverse (TGD) and their families are increasingly presenting to pediatric providers for education, care, and referrals. The need for more formal training, standardized treatment, and research on safety and medical outcomes often leaves providers feeling ill equipped to support and care for patients that identify as TGD and families. In this policy statement, we review relevant concepts and challenges and provide suggestions for pediatric providers that are focused on promoting the health and positive development of youth that identify as TGD while eliminating discrimination and stigma.
abstract
INTRODUCTION
In its dedication to the health of all children, the American Academy of Pediatrics (AAP) strives to improve health care access and eliminate disparities for children and teenagers who identify as lesbian, gay, bisexual, transgender, or questioning (LGBTQ) of their sexual or gender identity.1, 2 Despite some advances in public awareness and legal protections, youth who identify as LGBTQ continue to face disparities that stem from multiple sources, including inequitable laws and policies, societal discrimination, and a lack of access to quality health care, including mental health care. Such challenges are often more intense for youth who do not conform to social expectations and norms regarding gender. Pediatric providers are increasingly encountering such youth and their families, who seek medical advice and interventions, yet they may lack the formal training to care for youth that identify as transgender and gender diverse (TGD) and their families.3
This policy statement is focused specifically on children and youth that identify as TGD rather than the larger LGBTQ population, providing brief, relevant background on the basis of current available research
To cite: Rafferty J, AAP COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH, AAP COMMITTEE ON ADOLESCENCE, AAP SECTION ON LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESS. Ensuring Comprehensive Care and Support for Transgender and Gender Diverse Children and Adolescents. Pediatrics. 2018;142(4): e20182162
Department of Pediatrics, Hasbro Children’s Hospital, Providence, Rhode Island; Thundermist Health Centers, Providence, Rhode Island; and Department of Child Psychiatry, Emma Pendleton Bradley Hospital, East Providence, Rhode Island
Dr Rafferty conceptualized the statement, drafted the initial manuscript, reviewed and revised the manuscript, approved the final manuscript as submitted, and agrees to be accountable for all aspects of the work.
This document is copyrighted and is property of the American Academy of Pediatrics and its Board of Directors. All authors have filed conflict of interest statements with the American Academy of Pediatrics. Any conflicts have been resolved through a process approved by the Board of Directors. The American Academy of Pediatrics has neither solicited nor accepted any commercial involvement in the development of the content of this publication.
Policy statements from the American Academy of Pediatrics benefit from expertise and resources of liaisons and internal (AAP) and external reviewers. However, policy statements from the American Academy of Pediatrics may not reflect the views of the liaisons or the organizations or government agencies that they represent.
The guidance in this statement does not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be appropriate.
All policy statements from the American Academy of Pediatrics automatically expire 5 years after publication unless reaffirmed, revised, or retired at or before that time.
Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of all Children
POLICY STATEMENT
PEDIATRICS Volume 142, number 4, October 2018:e20182162 FROM THE AMERICAN ACADEMY OF PEDIATRICS at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

and expert opinion from clinical and research leaders, which will serve as the basis for recommendations. It is not a comprehensive review of clinical approaches and nuances to pediatric care for children and youth that identify as TGD. Professional understanding of youth that identify as TGD is a rapidly evolving clinical field in which research on appropriate clinical management is limited by insufficient funding.3, 4
DEFINITIONS
To clarify recommendations and discussions in this policy statement, some definitions are provided. However, brief descriptions of human behavior or identities may not capture nuance in this evolving field.
“Sex, ” or “natal gender, ” is a label, generally “male” or “female, ” that is typically assigned at birth on the basis of genetic and anatomic characteristics, such as genital anatomy, chromosomes, and sex hormone levels. Meanwhile, “gender identity” is one’s internal sense of who one is, which results from a multifaceted interaction of biological traits, developmental influences, and environmental conditions. It may be male, female, somewhere in between, a combination of both, or neither (ie, not conforming to a binary conceptualization of gender). Self-recognition of gender identity develops over time, much the same way as a child’s physical body does. For some people, gender identity can be fluid, shifting in different contexts. “Gender expression”
refers to the wide array of ways people display their gender through clothing, hair styles, mannerisms, or social roles. Exploring different ways of expressing gender is common for children and may challenge social expectations. The way others interpret this expression is referred to as “gender perception” (Table 1).5, 6
These labels may or may not be congruent. The term “cisgender” is used if someone identifies and expresses a gender that is consistent with the culturally defined norms of the sex that was assigned at birth. “Gender diverse” is an umbrella term to describe an ever-evolving array of labels that people may apply when their gender identity, expression, or even perception does not conform
FROM THE AMERICAN ACADEMY OF PEDIATRICS2
TABLE 1 Relevant Terms and Definitions Related to Gender Care
Term Definition
Sex An assignment that is made at birth, usually male or female, typically on the basis of external genital anatomy but sometimes on the basis of internal gonads, chromosomes, or hormone levels
Gender identity A person’s deep internal sense of being female, male, a combination of both, somewhere in between, or neither, resulting from a multifaceted interaction of biological traits, environmental factors, selfunderstanding, and cultural expectations
Gender expression The external way a person expresses their gender, such as with clothing, hair, mannerisms, activities, or social rolesGender perception The way others interpret a person’s gender expressionGender diverse A term that is used to describe people with gender behaviors, appearances, or identities that are incongruent with those culturally
assigned to their birth sex; genderdiverse individuals may refer to themselves with many different terms, such as transgender, nonbinary, genderqueer, 7 gender fluid, gender creative, gender independent, or noncisgender. “Gender diverse” is used to acknowledge and include the vast diversity of gender identities that exists. It replaces the former term, “gender nonconforming, ” which has a negative and exclusionary connotation.
Transgender A subset of genderdiverse youth whose gender identity does not match their assigned sex and generally remains persistent, consistent, and insistent over time; the term “transgender” also encompasses many other labels individuals may use to refer to themselves.
Cisgender A term that is used to describe a person who identifies and expresses a gender that is consistent with the culturally defined norms of the sex they were assigned at birth
Agender A term that is used to describe a person who does not identify as having a particular genderAffirmed gender When a person’s true gender identity, or concern about their gender identity, is communicated to and validated from others as
authenticMTF; affirmed female;
trans femaleTerms that are used to describe individuals who were assigned male sex at birth but who have a gender identity and/or expression
that is asserted to be more feminineFTM; affirmed male;
trans maleTerms that are used to describe individuals who were assigned female sex at birth but who have a gender identity and/or expression
that is asserted to be more masculineGender dysphoria A clinical symptom that is characterized by a sense of alienation to some or all of the physical characteristics or social roles of one’s
assigned gender; also, gender dysphoria is the psychiatric diagnosis in the DSM-5, which has focus on the distress that stems from the incongruence between one’s expressed or experienced (affirmed) gender and the gender assigned at birth.
Gender identity disorder
A psychiatric diagnosis defined previously in the DSM-IV (changed to “gender dysphoria” in the DSM-5); the primary criteria include a strong, persistent crosssex identification and significant distress and social impairment. This diagnosis is no longer appropriate for use and may lead to stigma, but the term may be found in older research.
Sexual orientation A person’s sexual identity in relation to the gender(s) to which they are attracted; sexual orientation and gender identity develop separately.
This list is not intended to be all inclusive. The pronouns “they” and ”their” are used intentionally to be inclusive rather than the binary pronouns “he” and “she” and “his” and “her.” Adapted from Bonifacio HJ, Rosenthal SM. Gender variance and dysphoria in children and adolescents. Pediatr Clin North Am. 2015;62(4):1001–1016. Adapted from Vance SR Jr, Ehrensaft D, Rosenthal SM. Psychological and medical care of gender nonconforming youth. Pediatrics. 2014;134(6):1184–1192. DSM5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; DSMIV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; FTM, female to male; MTF, male to female.
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

to the norms and stereotypes others expect of their assigned sex. “Transgender” is usually reserved for a subset of such youth whose gender identity does not match their assigned sex and generally remains persistent, consistent, and insistent over time. These terms are not diagnoses; rather, they are personal and often dynamic ways of describing one’s own gender experience.
Gender identity is not synonymous with “sexual orientation, ” which refers to a person’s identity in relation to the gender(s) to which they are sexually and romantically attracted. Gender identity and sexual orientation are distinct but interrelated constructs.8 Therefore, being transgender does not imply a sexual orientation, and people who identify as transgender still identify as straight, gay, bisexual, etc, on the basis of their attractions. (For more information, The Gender Book, found at www. thegenderbook. com, is a resource with illustrations that are used to highlight these core terms and concepts.)
EPIDEMIOLOGY
In population-based surveys, questions related to gender identity are rarely asked, which makes it difficult to assess the size and characteristics of the population that is TGD. In the 2014 Behavioral Risk Factor Surveillance System of the Centers for Disease Control and Prevention, only 19 states elected to include optional questions on gender identity. Extrapolation from these data suggests that the US prevalence of adults who identify as transgender or “gender nonconforming” is 0.6% (1.4 million), ranging from 0.3% in North Dakota to 0.8% in Hawaii.9 On the basis of these data, it has been estimated that 0.7% of youth ages 13 to 17 years (∼150 000) identify as transgender.10 This number is much higher than previous estimates, which were
extrapolated from individual states or specialty clinics, and is likely an underestimate given the stigma regarding those who openly identify as transgender and the difficulty in defining “transgender” in a way that is inclusive of all gender-diverse identities.11
There have been no large-scale prevalence studies among children and adolescents, and there is no evidence that adult statistics reflect young children or adolescents. In the 2014 Behavioral Risk Factor Surveillance System, those 18 to 24 years of age were more likely than older age groups to identify as transgender (0.7%).9 Children report being aware of gender incongruence at young ages. Children who later identify as TGD report first having recognized their gender as “different” at an average age of 8.5 years; however, they did not disclose such feelings until an average of 10 years later.12
MENTAL HEALTH IMPLICATIONS
Adolescents and adults who identify as transgender have high rates of depression, anxiety, eating disorders, self-harm, and suicide.13 – 20 Evidence suggests that an identity of TGD has an increased prevalence among individuals with autism spectrum disorder, but this association is not yet well understood.21, 22 In 1 retrospective cohort study, 56% of youth who identified as transgender reported previous suicidal ideation, and 31% reported a previous suicide attempt, compared with 20% and 11% among matched youth who identified as cisgender, respectively.13 Some youth who identify as TGD also experience gender dysphoria, which is a specific diagnosis given to those who experience impairment in peer and/or family relationships, school performance, or other aspects of their life as a consequence of the
incongruence between their assigned sex and their gender identity.23
There is no evidence that risk for mental illness is inherently attributable to one’s identity of TGD. Rather, it is believed to be multifactorial, stemming from an internal conflict between one’s appearance and identity, limited availability of mental health services, low access to health care providers with expertise in caring for youth who identify as TGD, discrimination, stigma, and social rejection.24 This was affirmed by the American Psychological Association in 200825 (with practice guidelines released in 20158) and the American Psychiatric Association, which made the following statement in 2012:
Being transgender or gender variant implies no impairment in judgment, stability, reliability, or general social or vocational capabilities; however, these individuals often experience discrimination due to a lack of civil rights protections for their gender identity or expression.… [Such] discrimination and lack of equal civil rights is damaging to the mental health of transgender and gender variant individuals.26
Youth who identify as TGD often confront stigma and discrimination, which contribute to feelings of rejection and isolation that can adversely affect physical and emotional well-being. For example, many youth believe that they must hide their gender identity and expression to avoid bullying, harassment, or victimization. Youth who identify as TGD experience disproportionately high rates of homelessness, physical violence (at home and in the community), substance abuse, and high-risk sexual behaviors.5, 6, 12, 27 – 31 Among the 3 million HIV testing events that were reported in 2015, the highest percentages of new infections were among women who identified as transgender32 and were also at particular risk for not knowing their HIV status.30
PEDIATRICS Volume 142, number 4, October 2018 3 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
GENDER-AFFIRMATIVE CARE
In a gender-affirmative care model (GACM), pediatric providers offer developmentally appropriate care that is oriented toward understanding and appreciating the youth’s gender experience. A strong, nonjudgmental partnership with youth and their families can facilitate exploration of complicated emotions and gender-diverse expressions while allowing questions and concerns to be raised in a supportive environment.5 In a GACM, the following messages are conveyed:
• transgender identities and diverse gender expressions do not constitute a mental disorder;
• variations in gender identity and expression are normal aspects of human diversity, and binary definitions of gender do not always reflect emerging gender identities;
• gender identity evolves as an interplay of biology, development, socialization, and culture; and
• if a mental health issue exists, it most often stems from stigma and negative experiences rather than being intrinsic to the child.27, 33
The GACM is best facilitated through the integration of medical, mental health, and social services, including specific resources and supports for parents and families.24 Providers work together to destigmatize gender variance, promote the child’s self-worth, facilitate access to care, educate families, and advocate for safer community spaces where children are free to develop and explore their gender.5 A specialized gender-affirmative therapist, when available, may be an asset in helping children and their families build skills for dealing with gender-based stigma, address symptoms of anxiety or depression, and reinforce the child’s overall resiliency.34, 35 There is a limited but growing body
of evidence that suggests that using an integrated affirmative model results in young people having fewer mental health concerns whether they ultimately identify as transgender.24, 36, 37
In contrast, “conversion” or “reparative” treatment models are used to prevent children and adolescents from identifying as transgender or to dissuade them from exhibiting gender-diverse expressions. The Substance Abuse and Mental Health Services Administration has concluded that any therapeutic intervention with the goal of changing a youth’s gender expression or identity is inappropriate.33 Reparative approaches have been proven to be not only unsuccessful38 but also deleterious and are considered outside the mainstream of traditional medical practice.29, 39 – 42 The AAP described reparative approaches as “unfair and deceptive.” 43 At the time of this writing, * conversion therapy was banned by executive regulation in New York and by legislative statutes in 9 other states as well as the District of Columbia.44
Pediatric providers have an essential role in assessing gender concerns and providing evidence-based information to assist youth and families in medical decision-making. Not doing so can prolong or exacerbate gender dysphoria and contribute to abuse and stigmatization.35 If a pediatric provider does not feel prepared to address gender concerns when they occur, then referral to a pediatric or mental health provider with more expertise is appropriate. There is little research on communication and efficacy with transfers in care for youth who identify as TGD,
* For more information regarding statespecific laws, please contact the AAP Division of State Government Affairs at stgov@ aap.org.
particularly from pediatric to adult providers.
DEVELOPMENTAL CONSIDERATIONS
Acknowledging that the capacity for emerging abstract thinking in childhood is important to conceptualize and reflect on identity, gender-affirmation guidelines are being focused on individually tailored interventions on the basis of the physical and cognitive development of youth who identify as TGD.45 Accordingly, research substantiates that children who are prepubertal and assert an identity of TGD know their gender as clearly and as consistently as their developmentally equivalent peers who identify as cisgender and benefit from the same level of social acceptance.46 This developmental approach to gender affirmation is in contrast to the outdated approach in which a child’s gender-diverse assertions are held as “possibly true” until an arbitrary age (often after pubertal onset) when they can be considered valid, an approach that authors of the literature have termed “watchful waiting.” This outdated approach does not serve the child because critical support is withheld. Watchful waiting is based on binary notions of gender in which gender diversity and fluidity is pathologized; in watchful waiting, it is also assumed that notions of gender identity become fixed at a certain age. The approach is also influenced by a group of early studies with validity concerns, methodologic flaws, and limited follow-up on children who identified as TGD and, by adolescence, did not seek further treatment (“desisters”).45, 47 More robust and current research suggests that, rather than focusing on who a child will become, valuing them for who they are, even at a young age, fosters secure attachment and resilience, not only for the child but also for the whole family.5, 45, 48, 49
FROM THE AMERICAN ACADEMY OF PEDIATRICS4 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

MEDICAL MANAGEMENT
Pediatric primary care providers are in a unique position to routinely inquire about gender development in children and adolescents as part of recommended well-child visits50 and to be a reliable source of validation, support, and reassurance. They are often the first provider to be aware that a child may not identify as cisgender or that there may be distress related to a gender-diverse identity. The best way to approach gender with patients is to inquire directly and nonjudgmentally about their experience and feelings before applying any labels.27, 51
Many medical interventions can be offered to youth who identify as TGD and their families. The decision of whether and when to initiate gender-affirmative treatment is personal and involves careful consideration of risks, benefits, and other factors unique to each patient and family. Many protocols suggest that clinical assessment of youth who identify as TGD is ideally conducted on an ongoing basis in the setting of a collaborative, multidisciplinary approach, which, in addition to the patient and family, may include the pediatric provider, a mental health provider (preferably with expertise in caring for youth who identify as TGD ), social and legal supports, and a pediatric endocrinologist or adolescent-medicine gender specialist, if available.6, 28 There is no prescribed path, sequence, or end point. Providers can make every effort to be aware of the influence of their own biases. The medical options also vary depending on pubertal and developmental progression.
Clinical Setting
In the past year, 1 in 4 adults who identified as transgender avoided a necessary doctor’s visit because of fear of being mistreated.31 All clinical office staff have a role in affirming a patient’s gender identity. Making flyers available or displaying posters
related to LGBTQ health issues, including information for children who identify as TGD and families, reveals inclusivity and awareness. Generally, patients who identify as TGD feel most comfortable when they have access to a gender-neutral restroom. Diversity training that encompasses sensitivity when caring for youth who identify as TGD and their families can be helpful in educating clinical and administrative staff. A patient-asserted name and pronouns are used by staff and are ideally reflected in the electronic medical record without creating duplicate charts.52, 53 The US Centers for Medicare and Medicaid Services and the National Coordinator for Health Information Technology require all electronic health record systems certified under the Meaningful Use incentive program to have the capacity to confidentially collect information on gender identity.54, 55 Explaining and maintaining confidentiality procedures promotes openness and trust, particularly with youth who identify as LGBTQ.1 Maintaining a safe clinical space can provide at least 1 consistent, protective refuge for patients and families, allowing authentic gender expression and exploration that builds resiliency.
Pubertal Suppression
Gonadotrophin-releasing hormones have been used to delay puberty since the 1980s for central precocious puberty.56 These reversible treatments can also be used in adolescents who experience gender dysphoria to prevent development of secondary sex characteristics and provide time up until 16 years of age for the individual and the family to explore gender identity, access psychosocial supports, develop coping skills, and further define appropriate treatment goals. If pubertal suppression treatment is
suspended, then endogenous puberty will resume.20, 57, 58
Often, pubertal suppression creates an opportunity to reduce distress that may occur with the development of secondary sexual characteristics and allow for gender-affirming care, including mental health support for the adolescent and the family. It reduces the need for later surgery because physical changes that are otherwise irreversible (protrusion of the Adam’s apple, male pattern baldness, voice change, breast growth, etc) are prevented. The available data reveal that pubertal suppression in children who identify as TGD generally leads to improved psychological functioning in adolescence and young adulthood.20, 57 – 59
Pubertal suppression is not without risks. Delaying puberty beyond one’s peers can also be stressful and can lead to lower self-esteem and increased risk taking.60 Some experts believe that genital underdevelopment may limit some potential reconstructive options.61 Research on long-term risks, particularly in terms of bone metabolism62 and fertility, 63 is currently limited and provides varied results.57, 64, 65 Families often look to pediatric providers for help in considering whether pubertal suppression is indicated in the context of their child’s overall well-being as gender diverse.
Gender Affirmation
As youth who identify as TGD reflect on and evaluate their gender identity, various interventions may be considered to better align their gender expression with their underlying identity. This process of reflection, acceptance, and, for some, intervention is known as “gender affirmation.” It was formerly referred to as “transitioning, ” but many view the process as an affirmation and acceptance of who they have always been rather than a transition
PEDIATRICS Volume 142, number 4, October 2018 5 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
from 1 gender identity to another. Accordingly, some people who have gone through the process prefer to call themselves “affirmed females, males, etc” (or just “females, males, etc”), rather than using the prefix “trans-.” Gender affirmation is also used to acknowledge that some individuals who identify as TGD may feel affirmed in their gender without pursuing medical or surgical interventions.7, 66
Supportive involvement of parents and family is associated with better mental and physical health outcomes.67 Gender affirmation among adolescents with gender dysphoria often reduces the emphasis on gender in their lives, allowing them to attend to other developmental tasks, such as academic success, relationship building, and future-oriented planning.64 Most protocols for gender-affirming interventions incorporate World Professional Association of Transgender
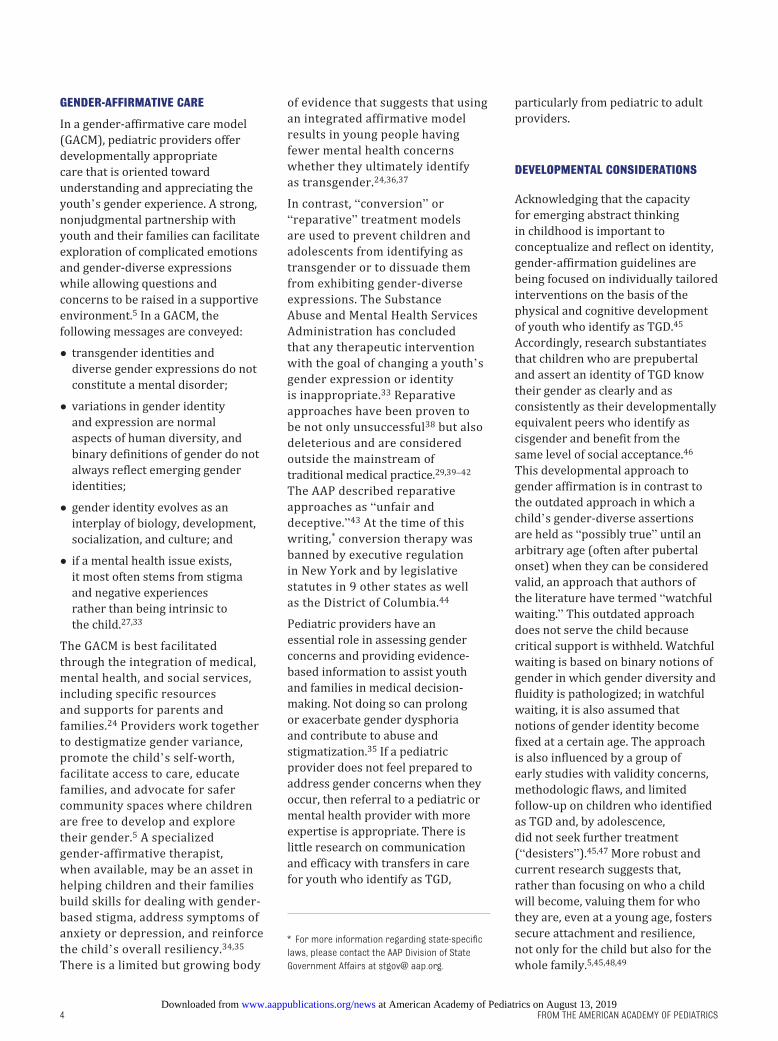
Health35 and Endocrine Society68 recommendations and include ≥1 of the following elements (Table 2):
1. Social Affirmation: This is a reversible intervention in which children and adolescents express partially or completely in their asserted gender identity by adapting hairstyle, clothing, pronouns, name, etc. Children who identify as transgender and socially affirm and are supported in their asserted gender show no increase in depression and only minimal (clinically insignificant) increases in anxiety compared with age-matched averages.48 Social affirmation can be complicated given the wide range of social interactions children have (eg, extended families, peers, school, community, etc). There is little guidance on the best approach (eg, all at once, gradual, creating new social networks, or affirming within existing networks, etc). Pediatric providers
can best support families by anticipating and discussing such complexity proactively, either in their own practice or through enlisting a qualified mental health provider.
2. Legal Affirmation: Elements of a social affirmation, such as a name and gender marker, become official on legal documents, such as birth certificates, passports, identification cards, school documents, etc. The processes for making these changes depend on state laws and may require specific documentation from pediatric providers.
3. Medical Affirmation: This is the process of using cross-sex hormones to allow adolescents who have initiated puberty to develop secondary sex characteristics of the opposite biological sex. Some changes are partially reversible if hormones are stopped, but others become
FROM THE AMERICAN ACADEMY OF PEDIATRICS6
TABLE 2 The Process of Gender Affirmation May Include ≥1 of the Following Components
Component Definition General Age Rangea Reversibilitya
Social affirmation Adopting genderaffirming hairstyles, clothing, name, gender pronouns, and restrooms and other facilities
Any Reversible
Puberty blockers Gonadotropinreleasing hormone analogues, such as leuprolide and histrelin
During puberty (Tanner stage 2–5)b Reversiblec
Crosssex hormone therapy Testosterone (for those who were assigned female at birth and are masculinizing); estrogen plus androgen inhibitor (for those who were assigned male at birth and are feminizing)
Early adolescence onward Partially reversible (skin texture, muscle mass, and fat deposition); irreversible once developed (testosterone: Adam’s apple protrusion, voice changes, and male pattern baldness; estrogen: breast development); unknown reversibility (effect on fertility)
Genderaffirming surgeries “Top” surgery (to create a maletypical chest shape or enhance breasts); “bottom” surgery (surgery on genitals or reproductive organs); facial feminization and other procedures
Typically adults (adolescents on casebycase basisd)
Not reversible
Legal affirmation Changing gender and name recorded on birth certificate, school records, and other documents
Any Reversible
a Note that the provided age range and reversibility is based on the little data that are currently available.b There is limited benefit to starting gonadotropinreleasing hormone after Tanner stage 5 for pubertal suppression. However, when crosssex hormones are initiated with a gradually increasing schedule, the initial levels are often not high enough to suppress endogenous sex hormone secretion. Therefore, gonadotropinreleasing hormone may be continued in accordance with the Endocrine Society Guidelines.68
c The effect of sustained puberty suppression on fertility is unknown. Pubertal suppression can be, and often is indicated to be, followed by crosssex hormone treatment. However, when crosssex hormones are initiated without endogenous hormones, then fertility may be decreased.68
d Eligibility criteria for genderaffirmative surgical interventions among adolescents are not clearly defined between established protocols and practice. When applicable, eligibility is usually determined on a casebycase basis with the adolescent and the family along with input from medical, mental health, and surgical providers.68 – 71
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
irreversible once they are fully developed (Table 2).
4. Surgical Affirmation: Surgical approaches may be used to feminize or masculinize features, such as hair distribution, chest, or genitalia, and may include removal of internal organs, such as ovaries or the uterus (affecting fertility). These changes are irreversible. Although current protocols typically reserve surgical interventions for adults, 35, 68 they are occasionally pursued during adolescence on a case-by-case basis, considering the necessity and benefit to the adolescent’s overall health and often including multidisciplinary input from medical, mental health, and surgical providers as well as from the adolescent and family.69 –71
For some youth who identify as TGD whose natal gender is female, menstruation, breakthrough bleeding, and dysmenorrhea can lead to significant distress before or during gender affirmation. The American College of Obstetrics and Gynecology suggests that, although limited data are available to outline management, menstruation can be managed without exogenous estrogens by using a progesterone-only pill, a medroxyprogesterone acetate shot, or a progesterone-containing intrauterine or implantable device.72 If estrogen can be tolerated, oral contraceptives that contain both progesterone and estrogen are more effective at suppressing menses.73 The Endocrine Society guidelines also suggest that gonadotrophin-releasing hormones can be used for menstrual suppression before the anticipated initiation of testosterone or in combination with testosterone for breakthrough bleeding (enables phenotypic masculinization at a lower dose than if testosterone is used alone).68 Masculinizing hormones in natal female patients may lead to a cessation of menses,
but unplanned pregnancies have been reported, which emphasizes the need for ongoing contraceptive counseling with youth who identify as TGD.72
HEALTH DISPARITIES
In addition to societal challenges, youth who identify as TGD face several barriers within the health care system, especially regarding access to care. In 2015, a focus group of youth who identified as transgender in Seattle, Washington, revealed 4 problematic areas related to health care:
1. safety issues, including the lack of safe clinical environments and fear of discrimination by providers;
2. poor access to physical health services, including testing for sexually transmitted infections;
3. inadequate resources to address mental health concerns; and
4. lack of continuity with providers.74
This study reveals the obstacles many youth who identify as TGD face in accessing essential services, including the limited supply of appropriately trained medical and psychological providers, fertility options, and insurance coverage denials for gender-related treatments.74
Insurance denials for services related to the care of patients who identify as TGD are a significant barrier. Although the Office for Civil Rights of the US Department of Health and Human Services explicitly stated in 2012 that the nondiscrimination provision in the Patient Protection and Affordable Care Act includes people who identify as gender diverse, 75, 76 insurance claims for gender affirmation, particularly among youth who identify as TGD, are frequently denied.54, 77 In 1 study, it was found that approximately 25% of individuals
who identified as transgender were denied insurance coverage because of being transgender.31 The burden of covering medical expenses that are not covered by insurance can be financially devastating, and even when expenses are covered, families describe high levels of stress in navigating and submitting claims appropriately.78 In 2012, a large gender center in Boston, Massachusetts, reported that most young patients who identified as transgender and were deemed appropriate candidates for recommended gender care were unable to obtain it because of such denials, which were based on the premise that gender dysphoria was a mental disorder, not a physical one, and that treatment was not medically or surgically necessary.24 This practice not only contributes to stigma, prolonged gender dysphoria, and poor mental health outcomes, 77 but it may also lead patients to seek nonmedically supervised treatments that are potentially dangerous.24 Furthermore, insurance denials can reinforce a socioeconomic divide between those who can finance the high costs of uncovered care and those who cannot.24, 77
The transgender youth group in Seattle likely reflected the larger TGD population when they described how obstacles adversely affect self-esteem and contribute to the perception that they are undervalued by society and the health care system.74, 77 Professional medical associations, including the AAP, are increasingly calling for equity in health care provisions regardless of gender identity or expression.1, 8, 23, 72 There is a critical need for investments in research on the prevalence, disparities, biological underpinnings, and standards of care relating to gender-diverse populations. Pediatric providers who work with state government and insurance officials can play an essential role in advocating for
PEDIATRICS Volume 142, number 4, October 2018 7 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

stronger nondiscrimination policies and improved coverage.
There is a lack of quality research on the experience of youth of color who identify as transgender. One theory suggests that the intersection of racism, transphobia, and sexism may result in the extreme marginalization that is experienced among many women of color who identify as transgender, 79 including rejection from their family and dropping out of school at younger ages (often in the setting of rigid religious beliefs regarding gender), 80 increased levels of violence and body objectification, 81 3 times the risk of poverty compared with the general population, 31 and the highest prevalence of HIV compared with other risk groups (estimated as high as 56.3% in 1 meta-analysis).30 One model suggests that pervasive stigma and oppression can be associated with psychological distress (anxiety, depression, and suicide) and adoption of risk behaviors by such youth to obtain a sense of validation toward their complex identities.79
FAMILY ACCEPTANCE
Research increasingly suggests that familial acceptance or rejection ultimately has little influence on the gender identity of youth; however, it may profoundly affect young people’s ability to openly discuss or disclose concerns about their identity. Suppressing such concerns can affect mental health.82 Families often find it hard to understand and accept their child’s gender-diverse traits because of personal beliefs, social pressure, and stigma.49, 83 Legitimate fears may exist for their child’s welfare, safety, and acceptance that pediatric providers need to appreciate and address. Families can be encouraged to communicate their concerns and questions. Unacknowledged concerns can contribute to shame and hesitation in regard to offering support and understanding, 84
which is essential for the child’s self-esteem, social involvement, and overall health as TGD.48, 85 – 87 Some caution has been expressed that unquestioning acceptance per se may not best serve questioning youth or their families. Instead, psychological evidence suggests that the most benefit comes when family members and youth are supported and encouraged to engage in reflective perspective taking and validate their own and the other’s thoughts and feelings despite divergent views.49, 82
In this regard, suicide attempt rates among 433 adolescents in Ontario who identified as “trans” were 4% among those with strongly supportive parents and as high as 60% among those whose parents were not supportive.85 Adolescents who identify as transgender and endorse at least 1 supportive person in their life report significantly less distress than those who only experience rejection. In communities with high levels of support, it was found that nonsupportive families tended to increase their support over time, leading to dramatic improvement in mental health outcomes among their children who identified as transgender.88
Pediatric providers can create a safe environment for parents and families to better understand and listen to the needs of their children while receiving reassurance and education.83 It is often appropriate to assist the child in understanding the parents’ concerns as well. Despite expectations by some youth with transgender identity for immediate acceptance after “coming out, ” family members often proceed through a process of becoming more comfortable and understanding of the youth’s gender identity, thoughts, and feelings. One model suggests that the process resembles grieving, wherein the family separates from their expectations for their child to embrace a new reality. This process may proceed through stages of shock,
denial, anger, feelings of betrayal, fear, self-discovery, and pride.89 The amount of time spent in any of these stages and the overall pace varies widely. Many family members also struggle as they are pushed to reflect on their own gender experience and assumptions throughout this process. In some situations, youth who identify as TGD may be at risk for internalizing the difficult emotions that family members may be experiencing. In these cases, individual and group therapy for the family members may be helpful.49, 78
Family dynamics can be complex, involving disagreement among legal guardians or between guardians and their children, which may affect the ability to obtain consent for any medical management or interventions. Even in states where minors may access care without parental consent for mental health services, contraception, and sexually transmitted infections, parental or guardian consent is required for hormonal and surgical care of patients who identify as TGD.72, 90 Some families may take issue with providers who address gender concerns or offer gender-affirming care. In rare cases, a family may deny access to care that raises concerns about the youth’s welfare and safety; in those cases, additional legal or ethical support may be useful to consider. In such rare situations, pediatric providers may want to familiarize themselves with relevant local consent laws and maintain their primary responsibility for the welfare of the child.
SAFE SCHOOLS AND COMMUNITIES
Youth who identify as TGD are becoming more visible because gender-diverse expression is increasingly admissible in the media, on social media, and in schools and communities. Regardless of whether a youth with a gender-diverse
FROM THE AMERICAN ACADEMY OF PEDIATRICS8 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

identity ultimately identifies as transgender, challenges exist in nearly every social context, from lack of understanding to outright rejection, isolation, discrimination, and victimization. In the US Transgender Survey of nearly 28 000 respondents, it was found that among those who were out as or perceived to be TGD between kindergarten and eighth grade, 54% were verbally harassed, 24% were physically assaulted, and 13% were sexually assaulted; 17% left school because of maltreatment.31 Education and advocacy from the medical community on the importance of safe schools for youth who identify as TGD can have a significant effect.
At the time of this writing, * only 18 states and the District of Columbia had laws that prohibited discrimination based on gender expression when it comes to employment, housing, public accommodations, and insurance benefits. Over 200 US cities have such legislation. In addition to basic protections, many youth who identify as TGD also have to navigate legal obstacles when it comes to legally changing their name and/or gender marker.54 In addition to advocating and working with policy makers to promote equal protections for youth who identify as TGD, pediatric providers can play an important role by developing a familiarity with local laws and organizations that provide social work and legal assistance to youth who identify as TGD and their families.
School environments play a significant role in the social and emotional development of children. Every child has a right to feel safe
* For more information regarding statespecific laws, please contact the AAP Division of State Government Affairs at stgov@ aap.org.
and respected at school, but for youth who identify as TGD, this can be challenging. Nearly every aspect of school life may present safety concerns and require negotiations regarding their gender expression, including name/pronoun use, use of bathrooms and locker rooms, sports teams, dances and activities, overnight activities, and even peer groups. Conflicts in any of these areas can quickly escalate beyond the school’s control to larger debates among the community and even on a national stage.
The formerly known Gay, Lesbian, and Straight Education Network (GLSEN), an advocacy organization for youth who identify as LGBTQ, conducts an annual national survey to measure LGBTQ well-being in US schools. In 2015, students who identified as LGBTQ reported high rates of being discouraged from participation in extracurricular activities. One in 5 students who identified as LGBTQ reported being hindered from forming or participating in a club to support lesbian, gay, bisexual, or transgender students (eg, a gay straight alliance, now often referred to as a genders and sexualities alliance) despite such clubs at schools being associated with decreased reports of negative remarks about sexual orientation or gender expression, increased feelings of safety and connectedness at school, and lower levels of victimization. In addition, >20% of students who identified as LGBTQ reported being blocked from writing about LGBTQ issues in school yearbooks or school newspapers or being prevented or discouraged by coaches and school staff from participating in sports because of their sexual orientation or gender expression.91
One strategy to prevent conflict is to proactively support policies and protections that promote inclusion and safety of all students. However, such policies are far from
consistent across districts. In 2015, GLSEN found that 43% of children who identified as LGBTQ reported feeling unsafe at school because of their gender expression, but only 6% reported that their school had official policies to support youth who identified as TGD, and only 11% reported that their school’s antibullying policies had specific protections for gender expression.91 Consequently, more than half of the students who identified as transgender in the study were prevented from using the bathroom, names, or pronouns that aligned with their asserted gender at school. A lack of explicit policies that protected youth who identified as TGD was associated with increased reported victimization, with more than half of students who identified as LGBTQ reporting verbal harassment because of their gender expression. Educators and school administrators play an essential role in advocating for and enforcing such policies. GLSEN found that when students recognized actions to reduce gender-based harassment, both students who identified as transgender and cisgender reported a greater connection to staff and feelings of safety.91 In another study, schools were open to education regarding gender diversity and were willing to implement policies when they were supported by external agencies, such as medical professionals.92
Academic content plays an important role in building a safe school environment as well. The 2015 GLSEN survey revealed that when positive representations of people who identified as LGBTQ were included in the curriculum, students who identified as LGBTQ reported less hostile school environments, less victimization and greater feelings of safety, fewer school absences because of feeling unsafe, greater feelings of connectedness to their school
PEDIATRICS Volume 142, number 4, October 2018 9 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

community, and an increased interest in high school graduation and postsecondary education.91 At the time of this writing, * 8 states had laws that explicitly forbade teachers from even discussing LGBTQ issues.54
MEDICAL EDUCATION
One of the most important ways to promote high-quality health care for youth who identify as TGD and their families is increasing the knowledge base and clinical experience of pediatric providers in providing culturally competent care to such populations, as recommended by the recently released guidelines by the Association of American Medical Colleges.93 This begins with the medical school curriculum in areas such as human development, sexual health, endocrinology, pediatrics, and psychiatry. In a 2009–2010 survey of US medical schools, it was found that the median number of hours dedicated to LGBTQ health was 5, with one-third of US medical schools reporting no LGBTQ curriculum during the clinical years.94
During residency training, there is potential for gender diversity to be emphasized in core rotations, especially in pediatrics, psychiatry, family medicine, and obstetrics and gynecology. Awareness could be promoted through the inclusion of topics relevant to caring for children who identify as TGD in the list of core competencies published by the American Board of Pediatrics, certifying examinations, and relevant study materials. Continuing education and maintenance of certification activities can include topics relevant to TGD populations as well.
* For more information regarding statespecific laws, please contact the AAP Division of State Government Affairs at stgov@ aap.org.
RECOMMENDATIONS
The AAP works toward all children and adolescents, regardless of gender identity or expression, receiving care to promote optimal physical, mental, and social well-being. Any discrimination based on gender identity or expression, real or perceived, is damaging to the socioemotional health of children, families, and society. In particular, the AAP recommends the following:
1. that youth who identify as TGD have access to comprehensive, gender-affirming, and developmentally appropriate health care that is provided in a safe and inclusive clinical space;
2. that family-based therapy and support be available to recognize and respond to the emotional and mental health needs of parents, caregivers, and siblings of youth who identify as TGD;
3. that electronic health records, billing systems, patient-centered notification systems, and clinical research be designed to respect the asserted gender identity of each patient while maintaining confidentiality and avoiding duplicate charts;
4. that insurance plans offer coverage for health care that is specific to the needs of youth who identify as TGD, including coverage for medical, psychological, and, when indicated, surgical gender-affirming interventions;
5. that provider education, including medical school, residency, and continuing education, integrate core competencies on the emotional and physical health needs and best practices for the care of youth who identify as TGD and their families;
6. that pediatricians have a role in advocating for, educating, and developing liaison relationships
with school districts and other community organizations to promote acceptance and inclusion of all children without fear of harassment, exclusion, or bullying because of gender expression;
7. that pediatricians have a role in advocating for policies and laws that protect youth who identify as TGD from discrimination and violence;
8. that the health care workforce protects diversity by offering equal employment opportunities and workplace protections, regardless of gender identity or expression; and
9. that the medical field and federal government prioritize research that is dedicated to improving the quality of evidence-based care for youth who identify as TGD.
LEAD AUTHOR
Jason Richard Rafferty, MD, MPH, EdM, FAAP
CONTRIBUTOR
Robert Garofalo, MD, FAAP
COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH, 2017–2018
Michael Yogman, MD, FAAP, Chairperson
Rebecca Baum, MD, FAAP
Thresia B. Gambon, MD, FAAP
Arthur Lavin, MD, FAAP
Gerri Mattson, MD, FAAP
Lawrence Sagin Wissow, MD, MPH, FAAP
LIAISONS
Sharon Berry, PhD, LP – Society of Pediatric Psychology
Ed Christophersen, PhD, FAAP – Society of Pediatric Psychology
Norah Johnson, PhD, RN, CPNPBC – National Association of Pediatric Nurse Practitioners
Amy Starin, PhD, LCSW – National Association of Social Workers
Abigail Schlesinger, MD – American Academy of Child and Adolescent Psychiatry
STAFF
Karen S. SmithJames Baumberger
FROM THE AMERICAN ACADEMY OF PEDIATRICS10 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

COMMITTEE ON ADOLESCENCE, 2017–2018
Cora Breuner, MD, MPH, FAAP, ChairpersonElizabeth M. Alderman, MD, FSAHM, FAAPLaura K. Grubb, MD, MPH, FAAPMakia E. Powers, MD, MPH, FAAPKrishna Upadhya, MD, FAAPStephenie B. Wallace, MD, FAAP
LIAISONS
Laurie Hornberger, MD, MPH, FAAP – Section on Adolescent HealthLiwei L. Hua, MD, PhD – American Academy of Child and Adolescent PsychiatryMargo A. Lane, MD, FRCPC, FAAP – Canadian Paediatric SocietyMeredith Loveless, MD, FACOG – American College of Obstetricians and GynecologistsSeema Menon, MD – North American Society of Pediatric and Adolescent GynecologyCDR Lauren B. Zapata, PhD, MSPH – Centers for Disease Control and Prevention
STAFF
Karen Smith
SECTION ON LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESS EXECUTIVE COMMITTEE, 2016–2017
Lynn Hunt, MD, FAAP, ChairpersonAnne Teresa Gearhart, MD, FAAPChristopher Harris, MD, FAAPKathryn Melland Lowe, MD, FAAPChadwick Taylor Rodgers, MD, FAAPIlana Michelle Sherer, MD, FAAP
FORMER EXECUTIVE COMMITTEE MEMBERS
Ellen Perrin, MD, MA, FAAP
LIAISON
Joseph H. Waters, MD – AAP Section on Pediatric Trainees
STAFF
Renee Jarrett, MPH
ACKNOWLEDGMENTS
We thank Isaac Albanese, MPA, and Jayeson Watts, LICSW, for their thoughtful reviews and contributions.
REFERENCES
1. Levine DA; Committee on Adolescence. Officebased care for lesbian, gay, bisexual, transgender, and questioning youth. Pediatrics. 2013;132(1). Available at: www. pediatrics. org/ cgi/ content/ full/ 132/ 1/ e297
2. American Academy of Pediatrics Committee on Adolescence. Homosexuality and adolescence. Pediatrics. 1983;72(2):249–250
3. Institute of Medicine; Committee on Lesbian Gay Bisexual, and Transgender Health Issues and Research Gaps and Opportunities. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: National Academies Press; 2011. Available at: https:// www. ncbi. nlm. nih. gov/ books/ NBK64806. Accessed May 19, 2017
4. Deutsch MB, Radix A, Reisner S. What’s in a guideline? Developing
collaborative and sound research designs that substantiate best practice recommendations for transgender health care. AMA J Ethics. 2016;18(11):1098–1106
5. Bonifacio HJ, Rosenthal SM. Gender variance and dysphoria in children and adolescents. Pediatr Clin North Am. 2015;62(4):1001–1016
6. Vance SR Jr, Ehrensaft D, Rosenthal SM. Psychological and medical care of gender nonconforming youth. Pediatrics. 2014;134(6):1184–1192
7. Richards C, Bouman WP, Seal L, Barker MJ, Nieder TO, T’Sjoen G. Nonbinary or genderqueer genders. Int Rev Psychiatry. 2016;28(1): 95–102
8. American Psychological Association. Guidelines for psychological practice with transgender and gender nonconforming people. Am Psychol. 2015;70(9):832–864
9. Flores AR, Herman JL, Gates GJ, Brown TNT. How Many Adults Identify as Transgender in the United States. Los Angeles, CA: The Williams Institute; 2016
10. Herman JL, Flores AR, Brown TNT, Wilson BDM, Conron KJ. Age of Individuals Who Identify as Transgender in the United States. Los Angeles, CA: The Williams Institute; 2017
11. Gates GJ. How Many People are Lesbian, Gay, Bisexual, and Transgender? Los Angeles, CA: The Williams Institute; 2011
12. Olson J, Schrager SM, Belzer M, Simons LK, Clark LF. Baseline physiologic and psychosocial characteristics of transgender youth seeking care for gender dysphoria. J Adolesc Health. 2015;57(4):374–380
13. Almeida J, Johnson RM, Corliss HL, Molnar BE, Azrael D. Emotional distress
DOI: https:// doi. org/ 10. 1542/ peds. 2018 2162
Address correspondence to Jason Rafferty, MD, MPH, EdM, FAAP. Email: [email protected]
PEDIATRICS (ISSN Numbers: Print, 00314005; Online, 10984275).
Copyright © 2018 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The author has indicated he has no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The author has indicated he has no potential conflicts of interest to disclose.
ABBREVIATIONS
AAP: American Academy of Pediatrics
GACM: gender-affirmative care model
GLSEN: Gay, Lesbian, and Straight Education Network
LGBTQ: lesbian, gay, bisexual, transgender, or questioning
TGD: transgender and gender diverse
PEDIATRICS Volume 142, number 4, October 2018 11 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

among LGBT youth: the influence of perceived discrimination based on sexual orientation. J Youth Adolesc. 2009;38(7):1001–1014
14. ClementsNolle K, Marx R, Katz M. Attempted suicide among transgender persons: the influence of genderbased discrimination and victimization. J Homosex. 2006;51(3):53–69
15. Colizzi M, Costa R, Todarello O. Transsexual patients’ psychiatric comorbidity and positive effect of crosssex hormonal treatment on mental health: results from a longitudinal study. Psychoneuroendocrinology. 2014;39:65–73
16. Haas AP, Eliason M, Mays VM, et al. Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: review and recommendations. J Homosex. 2011;58(1):10–51
17. Maguen S, Shipherd JC. Suicide risk among transgender individuals. Psychol Sex. 2010;1(1):34–43
18. Connolly MD, Zervos MJ, Barone CJ II, Johnson CC, Joseph CL. The mental health of transgender youth: advances in understanding. J Adolesc Health. 2016;59(5):489–495
19. Grossman AH, D’Augelli AR. Transgender youth and lifethreatening behaviors. Suicide Life Threat Behav. 2007;37(5):527–537
20. Spack NP, EdwardsLeeper L, Feldman HA, et al. Children and adolescents with gender identity disorder referred to a pediatric medical center. Pediatrics. 2012;129(3):418–425
21. van Schalkwyk GI, Klingensmith K, Volkmar FR. Gender identity and autism spectrum disorders. Yale J Biol Med. 2015;88(1):81–83
22. Jacobs LA, Rachlin K, EricksonSchroth L, Janssen A. Gender dysphoria and cooccurring autism spectrum disorders: review, case examples, and treatment considerations. LGBT Health. 2014;1(4):277–282
23. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; 2013
24. EdwardsLeeper L, Spack NP. Psychological evaluation and medical treatment of transgender youth in an
interdisciplinary “Gender Management Service” (GeMS) in a major pediatric center. J Homosex. 2012;59(3):321–336
25. Anton BS. Proceedings of the American Psychological Association for the legislative year 2008: minutes of the annual meeting of the Council of Representatives, February 22–24, 2008, Washington, DC, and August 13 and 17, 2008, Boston, MA, and minutes of the February, June, August, and December 2008 meetings of the Board of Directors. Am Psychol. 2009;64(5):372–453
26. Drescher J, Haller E; American Psychiatric Association Caucus of Lesbian, Gay and Bisexual Psychiatrists. Position Statement on Discrimination Against Transgender and Gender Variant Individuals. Washington, DC: American Psychiatric Association; 2012
27. Hidalgo MA, Ehrensaft D, Tishelman AC, et al. The gender affirmative model: what we know and what we aim to learn. Hum Dev. 2013;56(5):285–290
28. Tishelman AC, Kaufman R, EdwardsLeeper L, Mandel FH, Shumer DE, Spack NP. Serving transgender youth: challenges, dilemmas and clinical examples. Prof Psychol Res Pr. 2015;46(1):37–45
29. Adelson SL; American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2012;51(9):957–974
30. Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N; HIV/AIDS Prevention Research Synthesis Team. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav. 2008;12(1):1–17
31. James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016
32. Centers for Disease Control and Prevention. CDC-Funded HIV Testing:
United States, Puerto Rico, and the U.S. Virgin Islands. Atlanta, GA: Centers for Disease Control and Prevention; 2015. Available at: https:// www. cdc. gov/ hiv/ pdf/ library/ reports/ cdc hiv funded testing us puerto rico 2015. pdf. Accessed August 2, 2018
33. Substance Abuse and Mental Health Services Administration. Ending Conversion Therapy: Supporting and Affirming LGBTQ Youth. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2015
34. Korell SC, Lorah P. An overview of affirmative psychotherapy and counseling with transgender clients. In: Bieschke KJ, Perez RM, DeBord KA, eds. Handbook of Counseling and Psychotherapy With Lesbian, Gay, Bisexual, and Transgender Clients. 2nd ed. Washington, DC: American Psychological Association; 2007:271–288
35. World Professional Association for Transgender Health. Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People. 7th ed. Minneapolis, MN: World Professional Association for Transgender Health; 2011. Available at: https:// www. wpath. org/ publications/ soc. Accessed April 15, 2018
36. Menvielle E. A comprehensive program for children with gender variant behaviors and gender identity disorders. J Homosex. 2012;59(3):357–368
37. Hill DB, Menvielle E, Sica KM, Johnson A. An affirmative intervention for families with gender variant children: parental ratings of child mental health and gender. J Sex Marital Ther. 2010;36(1):6–23
38. Haldeman DC. The practice and ethics of sexual orientation conversion therapy. J Consult Clin Psychol. 1994;62(2):221–227
39. Byne W. Regulations restrict practice of conversion therapy. LGBT Health. 2016;3(2):97–99
40. CohenKettenis PT, Delemarrevan de Waal HA, Gooren LJ. The treatment of adolescent transsexuals: changing insights. J Sex Med. 2008;5(8):1892–1897
FROM THE AMERICAN ACADEMY OF PEDIATRICS12 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

41. Bryant K. Making gender identity disorder of childhood: historical lessons for contemporary debates. Sex Res Soc Policy. 2006;3(3):23–39
42. World Professional Association for Transgender Health. WPATH De-Psychopathologisation Statement. Minneapolis, MN: World Professional Association for Transgender Health; 2010. Available at: https:// www. wpath. org/ policies. Accessed April 16, 2017
43. American Academy of Pediatrics. AAP support letter conversion therapy ban [letter]. 2015. Available at: https:// www. aap. org/ en us/ advocacy and policy/ federal advocacy/ Documents/ AAPsupportletterc onversiontherapyb an. pdf. Accessed August 1, 2018
44. Movement Advancement Project. LGBT Policy Spotlight: Conversion Therapy Bans. Boulder, CO: Movement Advancement Project; 2017. Available at: http:// www. lgbtmap. org/ policy and issue analysis/ policy spotlight conversion therapy bans. Accessed August 6, 2017
45. Ehrensaft D, Giammattei SV, Storck K, Tishelman AC, KeoMeier C. Prepubertal social gender transitions: what we know; what we can learn—a view from a gender affirmative lens. Int J Transgend. 2018;19(2):251–268
46. Olson KR, Key AC, Eaton NR. Gender cognition in transgender children. Psychol Sci. 2015;26(4):467–474
47. Olson KR. Prepubescent transgender children: what we do and do not know. J Am Acad Child Adolesc Psychiatry. 2016;55(3):155–156.e3
48. Olson KR, Durwood L, DeMeules M, McLaughlin KA. Mental health of transgender children who are supported in their identities. Pediatrics. 2016;137(3):e20153223
49. Malpas J. Between pink and blue: a multidimensional family approach to gender nonconforming children and their families. Fam Process. 2011;50(4):453–470
50. Hagan JF Jr, Shaw JS, Duncan PM, eds. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. 4th ed. Elk Grove, IL: American Academy of Pediatrics; 2016
51. Minter SP. Supporting transgender children: new legal, social, and
medical approaches. J Homosex. 2012;59(3):422–433
52. AHIMA Work Group. Improved patient engagement for LGBT populations: addressing factors related to sexual orientation/gender identity for effective health information management. J AHIMA. 2017;88(3):34–39
53. Deutsch MB, Green J, Keatley J, Mayer G, Hastings J, Hall AM; World Professional Association for Transgender Health EMR Working Group. Electronic medical records and the transgender patient: recommendations from the World Professional Association for Transgender Health EMR Working Group. J Am Med Inform Assoc. 2013;20(4):700–703
54. Dowshen N, Meadows R, Byrnes M, Hawkins L, Eder J, Noonan K. Policy perspective: ensuring comprehensive care and support for gender nonconforming children and adolescents. Transgend Health. 2016;1(1):75–85
55. Cahill SR, Baker K, Deutsch MB, Keatley J, Makadon HJ. Inclusion of sexual orientation and gender identity in stage 3 meaningful use guidelines: a huge step forward for LGBT health. LGBT Health. 2016;3(2):100–102
56. Mansfield MJ, Beardsworth DE, Loughlin JS, et al. Longterm treatment of central precocious puberty with a longacting analogue of luteinizing hormonereleasing hormone. Effects on somatic growth and skeletal maturation. N Engl J Med. 1983;309(21):1286–1290
57. Olson J, Garofalo R. The peripubertal genderdysphoric child: puberty suppression and treatment paradigms. Pediatr Ann. 2014;43(6):e132–e137
58. de Vries AL, Steensma TD, Doreleijers TA, CohenKettenis PT. Puberty suppression in adolescents with gender identity disorder: a prospective followup study. J Sex Med. 2011;8(8):2276–2283
59. Wallien MS, CohenKettenis PT. Psychosexual outcome of genderdysphoric children. J Am Acad Child Adolesc Psychiatry. 2008;47(12):1413–1423
60. Waylen A, Wolke D. Sex ‘n’ drugs ‘n’ rock ‘n’ roll: the meaning and social consequences of pubertal timing. Eur J Endocrinol. 2004;151(suppl 3):U151–U159
61. de Vries AL, Klink D, CohenKettenis PT. What the primary care pediatrician needs to know about gender incongruence and gender dysphoria in children and adolescents. Pediatr Clin North Am. 2016;63(6):1121–1135
62. Vlot MC, Klink DT, den Heijer M, Blankenstein MA, Rotteveel J, Heijboer AC. Effect of pubertal suppression and crosssex hormone therapy on bone turnover markers and bone mineral apparent density (BMAD) in transgender adolescents. Bone. 2017;95:11–19
63. Finlayson C, Johnson EK, Chen D, et al. Proceedings of the working group session on fertility preservation for individuals with gender and sex diversity. Transgend Health. 2016;1(1):99–107
64. Kreukels BP, CohenKettenis PT. Puberty suppression in gender identity disorder: the Amsterdam experience. Nat Rev Endocrinol. 2011;7(8):466–472
65. Rosenthal SM. Approach to the patient: transgender youth: endocrine considerations. J Clin Endocrinol Metab. 2014;99(12):4379–4389
66. Fenway Health. Glossary of Gender and Transgender Terms. Boston, MA: Fenway Health; 2010. Available at: http:// fenwayhealth. org/ documents/ the fenway institute/ handouts/ Handout_ 7 C_ Glossary_ of_ Gender_ and_ Transgender_ Terms__ fi. pdf. Accessed August 16, 2017
67. de Vries AL, McGuire JK, Steensma TD, Wagenaar EC, Doreleijers TA, CohenKettenis PT. Young adult psychological outcome after puberty suppression and gender reassignment. Pediatrics. 2014;134(4):696–704
68. Hembree WC, CohenKettenis PT, Gooren L, et al. Endocrine treatment of genderdysphoric/genderincongruent persons: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2017;102(11):3869–3903
69. Milrod C, Karasic DH. Age is just a number: WPATHaffiliated surgeons’ experiences and attitudes toward
PEDIATRICS Volume 142, number 4, October 2018 13 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

vaginoplasty in transgender females under 18 years of age in the United States. J Sex Med. 2017;14(4):624–634
70. Milrod C. How young is too young: ethical concerns in genital surgery of the transgender MTF adolescent. J Sex Med. 2014;11(2):338–346
71. OlsonKennedy J, Warus J, Okonta V, Belzer M, Clark LF. Chest reconstruction and chest dysphoria in transmasculine minors and young adults: comparisons of nonsurgical and postsurgical cohorts. JAMA Pediatr. 2018;172(5):431–436
72. Committee on Adolescent Health Care. Committee opinion no. 685: care for transgender adolescents. Obstet Gynecol. 2017;129(1):e11–e16
73. Greydanus DE, Patel DR, Rimsza ME. Contraception in the adolescent: an update. Pediatrics. 2001;107(3):562–573
74. Gridley SJ, Crouch JM, Evans Y, et al. Youth and caregiver perspectives on barriers to genderaffirming health care for transgender youth. J Adolesc Health. 2016;59(3):254–261
75. Sanchez NF, Sanchez JP, Danoff A. Health care utilization, barriers to care, and hormone usage among maletofemale transgender persons in New York City. Am J Public Health. 2009;99(4):713–719
76. Transgender Law Center. Affordable Care Act Fact Sheet. Oakland, CA: Transgender Law Center; 2016. Available at: https:// transgenderlawcen ter. org/ resources/ health/ aca fact sheet. Accessed August 8, 2016
77. Nahata L, Quinn GP, Caltabellotta NM, Tishelman AC. Mental health concerns and insurance denials among transgender adolescents. LGBT Health. 2017;4(3):188–193
78. Grant JM, Mottet LA, Tanis J, Harrison J, Herman JL, Keisling M. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. Washington, DC: National Center for Transgender Equality and National Gay and Lesbian Task Force; 2011 Available at: http:// www. thetaskforce. org/ static_
html/ downloads/ reports/ reports/ ntds_ full. pdf. Accessed August 6, 2018
79. Sevelius JM. Gender affirmation: a framework for conceptualizing risk behavior among transgender women of color. Sex Roles. 2013;68(11–12):675–689
80. Koken JA, Bimbi DS, Parsons JT. Experiences of familial acceptancerejection among transwomen of color. J Fam Psychol. 2009;23(6):853–860
81. Lombardi EL, Wilchins RA, Priesing D, Malouf D. Gender violence: transgender experiences with violence and discrimination. J Homosex. 2001;42(1):89–101
82. Wren B. ‘I can accept my child is transsexual but if I ever see him in a dress I’ll hit him’: dilemmas in parenting a transgendered adolescent. Clin Child Psychol Psychiatry. 2002;7(3):377–397
83. Riley EA, Sitharthan G, Clemson L, Diamond M. The needs of gendervariant children and their parents: a parent survey. Int J Sex Health. 2011;23(3):181–195
84. Whitley CT. Transkin undoing and redoing gender: negotiating relational identity among friends and family of transgender persons. Sociol Perspect. 2013;56(4):597–621
85. Travers R, Bauer G, Pyne J, Bradley K, Gale L, Papadimitriou M; Trans PULSE; Children’s Aid Society of Toronto; Delisle Youth Services. Impacts of Strong Parental Support for Trans Youth: A Report Prepared for Children’s Aid Society of Toronto and Delisle Youth Services. Toronto, ON: Trans PULSE; 2012. Available at: http:// transpulseproject . ca/ wp content/ uploads/ 2012/ 10/ Impacts of Strong Parental Support for Trans Youth vFINAL. pdf
86. Ryan C, Russell ST, Huebner D, Diaz R, Sanchez J. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nurs. 2010;23(4):205–213
87. Grossman AH, D’augelli AR, Frank JA. Aspects of psychological resilience among transgender youth. J LGBT Youth. 2011;8(2):103–115
88. McConnell EA, Birkett M, Mustanski B. Families matter: social support and mental health trajectories among lesbian, gay, bisexual, and transgender youth. J Adolesc Health. 2016;59(6):674–680
89. Ellis KM, Eriksen K. Transsexual and transgenderist experiences and treatment options. Fam J Alex Va. 2002;10(3):289–299
90. Lamda Legal. Transgender Rights Toolkit: A Legal Guide for Trans People and Their Advocates. New York, NY: Lambda Legal; 2016 Available at: https:// www. lambdalegal. org/ publications/ trans toolkit. Accessed August 6, 2018
91. Kosciw JG, Greytak EA, Giga NM, Villenas C, Danischewski DJ. The 2015 National School Climate Survey: The Experiences of Lesbian, Gay, Bisexual, Transgender, and Queer Youth in Our Nation’s Schools. New York, NY: GLSEN; 2016. Available at: https:// www. glsen. org/ article/ 2015 national school climate survey. Accessed August 8, 2018
92. McGuire JK, Anderson CR, Toomey RB, Russell ST. School climate for transgender youth: a mixed method investigation of student experiences and school responses. J Youth Adolesc. 2010;39(10):1175–1188
93. Association of American Medical Colleges Advisory Committee on Sexual Orientation, Gender Identity, and Sex Development. In: Hollenback AD, Eckstrand KL, Dreger A, eds. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born With DSD: A Resource for Medical Educators. Washington, DC: Association of American Medical Colleges; 2014. Available at: https:// members. aamc. org/ eweb/ upload/ Executive LGBT FINAL.pdf. Accessed August 8, 2018
94. ObedinMaliver J, Goldsmith ES, Stewart L, et al. Lesbian, gay, bisexual, and transgenderrelated content in undergraduate medical education. JAMA. 2011;306(9):971–977
FROM THE AMERICAN ACADEMY OF PEDIATRICS14 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
Available at: https://members.aamc.org/eweb/upload/Executive LGBT FINAL.pdf. Accessed August 8, 2018
Available at: https://members.aamc.org/eweb/upload/Executive LGBT FINAL.pdf. Accessed August 8, 2018

DOI: 10.1542/peds.2018-2162 originally published online September 17, 2018; 2018;142;Pediatrics
LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESSFAMILY HEALTH, COMMITTEE ON ADOLESCENCE and SECTION ON
Jason Rafferty, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD ANDGender-Diverse Children and Adolescents
Ensuring Comprehensive Care and Support for Transgender and
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/142/4/e20182162including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/142/4/e20182162#BIBLThis article cites 72 articles, 8 of which you can access for free at:
Subspecialty Collections
ubhttp://www.aappublications.org/cgi/collection/psychosocial_issues_sPsychosocial Issuesal_issues_subhttp://www.aappublications.org/cgi/collection/development:behaviorDevelopmental/Behavioral Pediatricsfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2018-2162 originally published online September 17, 2018; 2018;142;Pediatrics
LESBIAN, GAY, BISEXUAL, AND TRANSGENDER HEALTH AND WELLNESSFAMILY HEALTH, COMMITTEE ON ADOLESCENCE and SECTION ON
Jason Rafferty, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD ANDGender-Diverse Children and Adolescents
Ensuring Comprehensive Care and Support for Transgender and
http://pediatrics.aappublications.org/content/142/4/e20182162located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2018 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
FROM THE AMERICAN ACADEMY OF PEDIATRICSPEDIATRICS Volume 138 , number 2 , August 2016 :e 20161348
Sexuality Education for Children and AdolescentsCora C. Breuner, MD, MPH, Gerri Mattson, MD, MSPH, COMMITTEE ON ADOLESCENCE, COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH
This document is copyrighted and is property of the American Academy of Pediatrics and its Board of Directors. All authors have fi led confl ict of interest statements with the American Academy of Pediatrics. Any confl icts have been resolved through a process approved by the Board of Directors. The American Academy of Pediatrics has neither solicited nor accepted any commercial involvement in the development of the content of this publication.
Clinical reports from the American Academy of Pediatrics benefi t from expertise and resources of liaisons and internal (AAP) and external reviewers. However, clinical reports from the American Academy of Pediatrics may not refl ect the views of the liaisons or the organizations or government agencies that they represent.
The guidance in this report does not indicate an exclusive course of treatment or serve as a standard of medical care. Variations, taking into account individual circumstances, may be appropriate.
All clinical reports from the American Academy of Pediatrics automatically expire 5 years after publication unless reaffi rmed, revised, or retired at or before that time.
DOI: 10.1542/peds.2016-1348
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2016 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have
no fi nancial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated
they have no potential confl icts of interest to disclose.
abstractThe purpose of this clinical report is to provide pediatricians updated
research on evidence-based sexual and reproductive health education
conducted since the original clinical report on the subject was published by
the American Academy of Pediatrics in 2001. Sexuality education is defi ned
as teaching about human sexuality, including intimate relationships, human
sexual anatomy, sexual reproduction, sexually transmitted infections, sexual
activity, sexual orientation, gender identity, abstinence, contraception, and
reproductive rights and responsibilities. Developmentally appropriate and
evidence-based education about human sexuality and sexual reproduction
over time provided by pediatricians, schools, other professionals, and
parents is important to help children and adolescents make informed,
positive, and safe choices about healthy relationships, responsible sexual
activity, and their reproductive health. Sexuality education has been shown
to help to prevent and reduce the risks of adolescent pregnancy, HIV, and
sexually transmitted infections for children and adolescents with and
without chronic health conditions and disabilities in the United States.
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
INTRODUCTION
The purpose of this clinical report is to provide pediatricians with
an update on the research regarding evidence-based sexual and
reproductive health education that has been conducted since the original
clinical report on the subject was published by the American Academy
of Pediatrics (AAP) in 2001. 1 Education about sexuality that is provided
by pediatricians can complement the education children obtain at school
or at home, 2, 3 but many pediatricians do not address it. In a review of
health maintenance visits, 1 of 3 adolescent patients did not receive
any information on sexuality from their pediatrician, and if they did, the
conversation lasted less than 40 seconds. 4To cite: Breuner CC, Mattson G, AAP COMMITTEE ON ADO-
LESCENCE, AAP COMMITTEE ON PSYCHOSOCIAL ASPECTS OF
CHILD AND FAMILY HEALTH. Sexuality Education for Children
and Adolescents. Pediatrics. 2016;138(2):e20161348
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

FROM THE AMERICAN ACADEMY OF PEDIATRICS
BACKGROUND
Children and adolescents with and
without chronic health conditions
and disabilities will benefit when
they are provided with accurate
and developmentally appropriate
information about the biological,
sociocultural, psychological,
relational, and spiritual dimensions
of sexuality. Information about
sexuality can be taught and shared
in schools, communities, homes,
and medical offices using evidence-
based interventions. Children
and adolescents should be shown
how to develop a safe and positive
view of sexuality through age-
appropriate education about their
sexual health. Sexuality education
can be disseminated through the
3 learning domains: cognitive
(information), affective (feelings,
values, and attitudes), and behavioral
(communication, decision-making,
and other skills). 5
Sexuality education is more than
the instruction of children and
adolescents on anatomy and the
physiology of biological sex and
reproduction. It covers healthy
sexual development, gender
identity, interpersonal relationships,
affection, sexual development,
intimacy, and body image for all
adolescents, including adolescents
with disabilities, chronic health
conditions, and other special needs. 6
Developing a healthy sexuality is a
key developmental milestone for
all children and adolescents that
depends on acquiring information
and forming attitudes, beliefs,
and values about consent, sexual
orientation, gender identity,
relationships, and intimacy. 7 Healthy
sexuality is influenced by ethnic,
racial, cultural, personal, religious,
and moral concerns. Healthy
sexuality includes the capacity to
promote and preserve significant
interpersonal relationships; value
one’s body and personal health;
interact with both sexes in respectful
and appropriate ways; and express
affection, love, and intimacy in ways
consistent with one’s own values,
sexual preferences, and abilities.
The various dimensions of healthy
sexuality comprise the anatomy,
physiology, and biochemistry
of the sexual response system;
identity, orientation, roles, and
personality; and thoughts, feelings,
and relationships. 6 Ideally, children
and adolescents receive accurate
information on sexual health from
multiple professional resources. 8, 9
All children and adolescents need
to receive accurate education about
sexuality to understand ultimately
how to practice healthy sexual
behavior. Unhealthy, exploitive, or
risky sexual activity may lead to
health and social problems, such as
unintended pregnancy and sexually
transmitted infections (STIs),
including gonorrhea, Chlamydia,
syphilis, hepatitis, herpes, human
papilloma virus (HPV); HIV infection;
and AIDS. 10 From a 2012 informative
report by the National Campaign
to Prevent Teen and Unplanned
Pregnancy that surveyed 1200 high
school seniors, many senior girls and
boys reported having mixed feelings
about the first time they had sex, with
more than three-quarters responding
that they would change the way their
first sexual experience occurred.
Interestingly, seniors in this study
wanted their younger peers to know
it was “fine to be a virgin” when they
graduated from high school. 11
It has been demonstrated that
sexuality education interventions
can prevent or reduce the risk of
adolescent pregnancy HIV, and
STIs for children and adolescents
with and without chronic health
conditions and disabilities in
the United States. 12 Adolescent
sexual activity and teen births and
pregnancies have been decreasing
since 1991, with the exception of
2005 to 2007, when there was a
5% increase in birth rates. The
decrease in adolescent birth rates
in the United States reflects an
increased use of contraception at first
intercourse and in the use of dual
methods of condoms and hormonal
contraception in already sexually
active teenagers. 13 Nevertheless,
the United States continues to
lead industrialized countries with
the highest rates of adolescent
pregnancy. 14 Importantly, 88% of
births to adolescents 15 to 17 years
of age in the United States continued
to be unintended (unwanted or
mistimed). 15
Sexual health information
messages are received by children
and adolescents multiple times
throughout the day from the media,
religious organizations, schools, and
family peers, parents/caregivers, and
partners, although the quality of the
information varies. 16, 17 In an article
published in 2013 on how sexually
experienced adolescents in the
United States receive sexual health
information, parents and teachers
were the source of information
for 55% of girls and 43% of boys
about birth control and for 59%
of girls and 66% of boys about
STIs/HIV. 18 Only 10% of sexually
experienced adolescents reported
health care providers as a source of
birth control/STI/HIV information.
More than 80% of adolescents 15
to 19 years of age received formal
instruction about STIs, HIV, or how to
say "no" to sex between 2011-2013,
yet only 55% of males and 60% of
females received instruction about
birth control. 19 Strong support of
multilevel expanded and integrative
sex education is warranted now more
than ever.20
Delivery of Sexuality Education
Pediatricians/Health Care Providers
Pediatricians are in an excellent
position to provide and support
longitudinal sexuality education to
all children, adolescents, and young
adults with and without chronic
health conditions and disabilities as
part of preventive health care. Over
e2 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 2 , August 2016
the past decade, increasing numbers
of adolescents contend with sexuality
in the context of their own chronic
physical or mental health condition
and/or developmental disability. 21, 22
When sexuality is discussed routinely
and openly during well-child visits
for all children and adolescents
in the pediatrician’s office,
conversations are easier to initiate,
more comfortable to continue, and
more effective and informative for
all participants. Pediatricians and
other primary care clinicians can
explore the expectations of parents
for their child’s sexual development
while providing general, factual
information about sexuality and can
monitor adolescent use of guidance
and resources offered over time.
Pediatricians can introduce issues of
physical, cognitive, and psychosexual
development to parents and their
children in early childhood and
continue discussions at ongoing
health maintenance visits throughout
school age, adolescence, and young
adulthood. Sharing this information
can help overcome barriers to
discussing the sexual development
of all children and adolescents and
to improve screening rates for STIs,
pregnancy, and partner violence. It is
also important to provide access to
current accurate sexuality education
and to provide access to confidential
relevant information, services,
and support over the course of a
lifetime. 18, 21 These conversations can
begin with questions the family might
have about the child and his or her
body as well as about self-stimulation
and “safe touch.” With insights
into the typical stages of child and
adolescent sexual development,
parents can better understand their
own child’s behaviors. For example,
by recognizing that masturbation
is typical toddler behavior, parents
can better understand and discuss
self-stimulatory behaviors of their
teenager. The problem is often the
inability to distinguish between
behaviors that are publicly and
privately appropriate as children
grow older. 23
Often, the pediatrician can take the
lead from the parent or caregiver
and then ask a few gentle leading
questions about how much
information the family would
like to receive with the child and
parent together in the room. The
dynamics of the sexuality education
conversation can then change as the
child becomes a young adolescent
by asking the parent or caregiver
to leave the room after the initial
introductions and history taking has
occurred with the parent in the room.
Parents and adolescents benefit from
being prepared for these changes in
adolescent interactions when there
will be time alone for the adolescent
to engage with the pediatrician to
discuss sexuality, as well as personal
and mental health, drug and tobacco
use, and other psychosocial issues.
The importance of confidentiality
and its role in adolescent health
care autonomy should be discussed
with both adolescents and their
parents. Unlike school-based
instruction, a conversation about
sexuality with pediatricians
can provide an opportunity for
personalized information, for
confidential screening of risks, and
for addressing risks and enhancing
existing strengths through health
promotion and counseling. Children
and adolescents may ask questions,
discuss potentially embarrassing
experiences, or reveal highly
personal information to their
pediatricians. Families and children
may obtain education together or in
a separate but coordinated manner.
Prevention and counseling can
be targeted to the needs of youth
who are and those who are not yet
sexually active and to groups at high
risk of early or unsafe sexual activity,
which includes children with and
without chronic health conditions
and disabilities.
Use of a psychosocial behavior
screening tool or the Bright Futures
Previsit Questionnaire (available
at https:// brightfutures. aap. org/
Bright%20 Futures%20 Documents/
CoreTools11- 14YearOCVisit.
pdf) is a good way to address
all of these topics, in addition to
physical activity, nutrition, school,
and relationships. The AAP policy
statement on providing care for
lesbian, gay, bisexual, transgender,
and questioning youth, as well as
other resources, offer suggestions
on how to incorporate important
conversations about sexual and
gender identity in the health
supervision visit. 24 – 26
In the office setting, children and
adolescents have been shown to
prefer a pediatrician who is open
and nonjudgmental and comfortable
with discussions to address
knowledge, questions, worries,
or misunderstandings among
children, adolescents with and
without chronic health conditions
and disabilities, and their parents/
caregivers related to a wide range
of topics. These topics include,
but are not limited to, anatomy,
masturbation, menstruation,
erections, nocturnal emissions
(“wet dreams”), sexual fantasies,
sexual orientation, and orgasms.
Information regarding availability
and access to confidential sexual
and reproductive health services
and emergency contraception
is important to discuss with
adolescents and with parents. During
these discussions, pediatricians also
can address homosexual or bisexual
experiences or orientation, including
topics related to gender identity. It
is also important to acknowledge
the influence of media imagery
on sexuality as it is portrayed in
music and music videos, movies,
pornography, and television,
print, and Internet content and to
address the effects of social media
and sexting. According to the US
Preventive Services Task Force,
intensive behavioral counseling
is important for all sexually active
e3 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

FROM THE AMERICAN ACADEMY OF PEDIATRICS
adolescents and for adults who are
at increased risk of STIs. 27 Although
there may not be time to address all
of these topics in a brief office visit,
the longitudinal relationship and
annual well visit present several
opportunities for discussion. In
addition, more information and
resources can be shared with
adolescents, many of which are easily
accessible and listed at the end of this
report.
Most adolescents have the
opportunity to explore intimacy and
sexuality in a safe context, but some
others experience coercion, abuse,
and violence. In fact, unwanted first
sexual encounters were reported
in the National Survey of Family
Growth among 11% of female
and male subjects 18 to 24 years
of age who had first intercourse
before age 20 years. 28 Teenagers
who report first sex at 14 years of
age and younger are more likely
to report that it was nonvoluntary,
compared with those who were 17
to 19 years of age at sexual debut. 29
Unwanted encounters may include
dating violence, stranger assaults,
and intrafamilial sexual abuse/incest.
Screening for sexual violence and
nonconsensual sexual encounters
is important when evaluating all
sexually active adolescents, especially
for adolescents with chronic health
conditions and disabilities, because
they may be more likely to be victims
of sexual abuse. 5, 30
In the Schools
Formal sexuality education in
schools that includes instruction
about healthy sexual decision-
making and STI/HIV prevention
can improve the health and well-
being of adolescents and young
adults. 31 If comprehensive sexuality
education programs are offered in
the schools, positive outcomes can
occur, including delay in the initiation
and reduction in the frequency of
sexual intercourse, a reduction in the
number of sexual partners, and an
increase in condom use. 12, 32 Some
studies also have shown less truancy
and an improvement in academic
performance in those who have taken
sexuality education courses. 33
A student’s experience in school
with sexuality education can
vary a great deal. The Sexuality
Information and Education Council
of the United States and the Future
of Sex Education (FoSE) promote
evidence-informed comprehensive
school-based sexuality education
appropriate to students’ age,
developmental abilities, and cultural
background as an important part
of the school curriculum at every
grade. 34 A comprehensive sexuality
program provides medically accurate
information, recognizes the diversity
of values and beliefs represented in
the community, and complements
and augments the sexuality education
children receive from their families,
religious and community groups,
and health care professionals.
Adolescents and most parents agree
that school-based programs need
to be an important source of formal
education for adolescent sexual
health. 35 – 37
The protective influence of sexuality
education is not limited to the
questions about if or when to have
sex, but extends to issues of partner
selection, contraceptive use, and
reproductive health outcomes. 38
Creating access to medically
accurate comprehensive sexuality
education by using an evidence-
based curriculum and reducing
sociodemographic disparities in
its receipt remain a primary goal
for improving the well-being of
teenagers and young adults. Ideally,
this education happens conjointly in
the home and in the school. 39
Factors that shape the content and
delivery of sexuality education
include state and school district
policies, state education standards,
funding from state and federal
sources, and individual teacher
comfort, knowledge, and skills. Fewer
than half of states require public
schools to teach sexuality education,
and even fewer states require
that, if offered, sexuality education
must be medically, factually, or
technically accurate. State definitions
of “medically accurate” vary, from
requiring that the department
of health review curriculum
for accuracy to mandating that
curriculum be based on published
medical information. 40
Two-thirds of states and the District
of Columbia allow parents to remove
their children from participation or
opt out from sexuality education.
Fewer than half of states and
the District of Columbia require
parents to be notified that sexuality
education will be provided. Other
states have specific content
requirements, including “stressing
abstinence” or precluding discussion
of homosexuality or abortion. 41
The status of sexuality education in
private schools is less well known.
There is little to no information
available from parochial or private
scholastic institutions on the
provisions of sexuality education.
Although policies exist requiring
sexuality education, it may not
be occurring in an unbiased and
systematic manner. From the 2012
School Health Policies and Practices
Survey, only 71% of US high school
districts have adopted a policy
specifying that human sexuality is
taught. In a separate study comparing
high schools, middle schools, and
elementary schools, sexuality
education taught in middle schools
across states was more likely to
be focused on “how to say no to
sex” rather than other topics, with
approximately 1 in 5 teenagers
reporting that they first received
instruction on “how to say no to sex”
while in the first through fifth grade.
Adolescent boys were slightly more
likely than girls to be instructed on
how to say no to sex or were using
birth control while in middle school
(52% of male teenagers, compared
e4 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 2 , August 2016
with 46% of female teenagers).
Male teenagers were less likely than
female teenagers to report first
receiving instruction on methods of
birth control while in high school
(38% of male teenagers, compared
with 47% of female teenagers). 42
Teacher training in the United
States is quite variable from district
to district and school to school
especially in sexuality education.
The FoSE Initiative has released
the National Teacher Preparation
Standards for Sexuality Education
to provide guidance to institutions
of higher education to better
prepare future teachers. 9 The
FoSE teacher standards include
professional disposition, diversity
and equity, content knowledge, legal
and professional ethics, planning,
implementation, and assessment.
According to these standards,
teachers may benefit from receiving
specialized training on human
sexuality, which includes accurate
and current knowledge about
biological, social, and emotional
stages of child and adolescent sexual
development (including sexual
orientation) and legal aspects of
sexuality (ie, age of consent).
Professionals responsible for
sexuality education may benefit from
receiving training in several learning
and behavior theories and how to
provide age- and developmentally
appropriate instruction as part of
sexuality education lesson planning.
Ideally, teachers would be familiar
with relevant and current state
and/or district laws, policies, and
standards to help them choose
and adapt an evidence-based and
scientifically accurate curriculum
that is appropriate and permissible
within a school district. Ongoing
professional development and
participation in continuing education
classes or intensive seminars is
advised. Teachers can benefit from
access to updated and current
sexuality information, curricula,
policies, laws, standards, and other
materials. The FoSE standards advise
that teachers are aware of and take
into account their own biases about
sexuality, understand guidelines
for discussion of sensitive subjects
in the classroom and addressing
confidentiality, and know how to
address disclosure by students of
sexual abuse, incest, dating violence,
pregnancy, and other associated
sexual health issues. The goal is for
teachers to feel comfortable and
committed to discussing human
sexuality and to know how to
conduct themselves appropriately
with students as professionals both
inside and outside of the classroom
and school. It is important for
teachers to have an appreciation for
how students’ diverse backgrounds
and experience may affect students’
personal beliefs, values, and
knowledge about sexuality. In the
United States, 35.5% of districts
have adopted a policy stating that
there is a requirement that those
who teach health education must
earn continuing education credits
on strategies or on health-related
topics. It is important for teachers
to develop skills in creating a safe,
respectful, and inclusive classroom. 41
In the Home
Fundamentally, parents and
caregivers can have an important
role as their children’s primary
sexuality educators. However, a
number of factors, including lack of
knowledge, skills, or comfort, may
impede a parent’s or caregiver’s
successful fulfillment of that role.
Health care providers, schools,
faith-based institutions, the
media, and professional sexuality
educators are resources that guide
and advise parents by providing
training, resources, understanding,
and encouragement. One program,
"Talking Parents, Healthy Teens, "
aims to influence parents’ skills,
such as communication, monitoring,
and involvement. These include
intentions to talk about sex, to
monitor and stay involved, and
to understand environmental
barriers and facilitators that
influence talking about sexuality (eg,
community norms that discourage or
encourage such communication). 43
By increasing parents’ skills and
facilitating opportunities for
communication through take-home
activities, the program also aims
to affect the parent-adolescent
relationship, further influencing
adolescent behavior change (eg, the
likelihood that adolescents will delay
intercourse or use condoms). 44
In one study, adolescents were
asked whether they received formal
instruction on 4 topics of sexuality
education at home, school, church,
a community center, or some other
place before they were 18 years old. 42
They were specifically asked whether
they spoke to their parents before
the age of 18 about topics concerning
sex, birth control, STIs, and HIV/AIDS
prevention. Two-thirds of male and
80% of female adolescents reported
having talked with a parent about at
least 1 of 6 sexuality education topics
(“how to say no to sex, ” methods of
birth control, STIs, where to get birth
control, how to prevent HIV/AIDS,
and how to use a condom). Younger
(15–17 years old) female teenagers
were more likely (80%) than younger
male teenagers (68%) to have talked
to their parents about these topics. 42
The medical literature supports that
family and parental characteristics
can dictate patterns of sexual
experience among teenagers, as
shown in the National Survey of
Family Growth data from 2006 to
2010. 28 For example, in both male
and female teenagers, a significantly
smaller percentage were sexually
experienced if they lived with both
parents when they were 14 years
of age, if their mothers had their
first birth at 20 years or older, if
the teenager’s mother was a college
graduate, or if the teenager lived
with both of his or her parents. 28
Further, the approaches parents take
when talking with their adolescent
e5 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

FROM THE AMERICAN ACADEMY OF PEDIATRICS
about sex may have a tremendous
influence on the teenager. 45 Parents
who dominate the conversation have
teenagers who do not have as much
knowledge. Conversely, parents who
are engaged and comfortable talking
about sexual health have teenagers
who are more knowledgeable and
may even be more proactive in
seeking reproductive health medical
services. 45
A review of 12 studies on parental
communication about sex revealed
that parents who received training on
this topic had better communication
with their adolescents about
sexuality compared with those who
did not. 46 Parental conversations
with their adolescents about
sexuality education is correlated with
a delay in sexual debut and increased
use of contraception and condoms. 47
Jaccard and Levitz 45 identified
multiple effective components in
parent-adolescent sexual health
communication, including (1)
the extent of communication as
measured by frequency and depth
of discussions, (2) informational
style, (3) the content of data that
is discussed, (4) when and how
the communication occurs, and (5)
the overall environment where the
conversation takes place.
Discussions of sexuality do not occur
equally among mothers and fathers.
One review found that overall, the
number of discussions parents
have with teenagers about sex has
decreased from 1995 to 2002. 48
From a separate review covering
1980 through July 2010, mothers
were the primary discussant in
all interventions. 49 In reviewing
the role of fathers in sexual health
discussions, Kirkman et al 50 found
that fathers recognized, by self-
report, that they need to share
the role of communication about
this topic with their teenagers but
that they leave the conversation to
the mothers more often than not.
Although mothers can also effectively
teach their sons about sexuality, 51
the relationship boys have with their
fathers or other male role models
plays a crucial role in their sexual
health, including reducing sexual
risk taking and delaying initiation
of sexual intercourse, especially in
those boys with a connection to their
fathers, whether they live in the same
home or not.52, 53
It is clear that parents would
benefit from support to improve
communication with their
adolescents about sex.
ABSTINENCE EDUCATION
We know that abstinence is 100%
effective at preventing pregnancy
and STIs; however, research has
conclusively demonstrated that
programs promoting abstinence-
only until heterosexual marriage
occurs are ineffective. 54 – 57 A recent
systematic review examined the
evidence supporting both abstinence-
only programs and comprehensive
sexuality education programs
designed to promote abstinence from
sexual intercourse. In that review,
most comprehensive sexuality
education programs showed
efficacy in delaying initiation of
intercourse in addition to promoting
other protective behaviors, such as
condom use. There was no evidence
that abstinence-only programs
effectively delayed initiation of
sexual intercourse.57 In another
review of sexuality education,
Cavazos-Rehg et al 35 found that the
literature examining the efficacy
of current school-based sexuality
education programs had insufficient
evidence to support the intervention
of abstinence on the basis of
inconsistent results across studies.
The federal government has
historically provided $178 million for
abstinence-only education through
Title V, Section 510 of the Social
Security Act in 1996, Community-
Based Abstinence Education projects
through the Patient Protection
and Affordable Care Act, and the
Adolescent Family Life Act program.
The Community-Based Abstinence
Education program received the
most federal funds and made
direct grants to community-based
organizations, including faith-based
organizations. Federal guidance
required all programs to adhere to an
8-point definition of abstinence-only
education and prohibited programs
from disseminating information
on contraceptive services, sexual
orientation and gender identity, and
other aspects of human sexuality.
Programs promoted exclusive
abstinence outside of heterosexual
marriage and required that
contraceptive use, contraceptive
methods, and specifically condoms
must not be discussed except to
demonstrate failure rates. 58
The Obama administration’s
proposed budget for fiscal year
2014 created funding for programs
that have been proven effective in
reducing teen pregnancy, delaying
sexual activity, or increasing
contraceptive use. 32, 59 – 61 There are
still Title V–funded programs for
abstinence-only programs in the
schools and in other places in the
community. However, most public
funding now supports evidence-
informed interventions that have
been proven to delay onset of sexual
activity, reduce numbers of partners,
increase condom and contraceptive
use, and decrease incidence of teen
pregnancy and STIs, including
HIV.32, 59 – 61 Private and parochial
schools also have their own standards/
polices and limited funding stream
for sexuality education. 57
In a 2005 study by Brückner and
Bearman, 62 a review of Add Health
data suggested that many teenagers
who take a “virginity pledge” and
intend to be abstinent before
marriage fail to do so and that
when these teenagers do initiate
intercourse, they fail to protect
themselves by using contraception.
In a review of the virginity pledge
movement, these researchers found
e6 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 138 , number 2 , August 2016
that 88% of teenagers who took the
pledge had initiated intercourse
before marriage, compared with 99%
of those who did not take the pledge.
They also found that teenagers who
took the pledge were less likely to use
contraception after they did initiate
sexual intercourse and not to seek
STI screening. At 6-year follow-up,
the prevalence of STIs (Chlamydia,
gonorrhea, trichomoniasis, and HPV
infection) was comparable among
those who took the abstinence pledge
and those who did not. 62
The American College of
Obstetricians and Gynecologists, the
Society for Adolescent Health and
Medicine, the AAP, the American
Medical Association, the American
Public Health Association, National
Education Association, and the
National School Boards Association
oppose abstinence-only education
and endorse comprehensive sexuality
education that includes both
abstinence promotion and accurate
information about contraception,
human sexuality, and STIs. 62 – 67
CLINICAL GUIDANCE FOR PEDIATRICIANS
1. The pediatrician should
encourage early parental
discussion with children at home
about sexuality, contraception,
and Internet and social
media use that is consistent
with the child’s and family’s
attitudes, values, beliefs, and
circumstances.
2. Diverse family circumstances,
such as families with same-
sex parents or children who
identify as lesbian, gay, bisexual,
transgender, or questioning,
create unique guidance needs
regarding sexuality education.
3. Modeling ways to initiate talks
about sexuality with children at
pertinent opportunities, such
as the birth of a sibling can
encourage parents to answer
children's questions fully and
accurately.
4. Parents and adolescents are
encouraged to receive information
from multiple sources, including
health care providers and
sexuality educators, about
circumstances that are associated
with earlier sexual activity.
Adolescents are encouraged to feel
empowered through discussing
strategies that allow for practicing
social skills, assertiveness, control,
and rejection of unwanted sexual
advances and cessation of sexual
activity when the partner does not
consent.
5. Discussions regarding healthy
relationships and intimate
partner violence can be effectively
included in health care visits.
6. Pediatricians are encouraged to
acknowledge that sexual activity
may be pleasurable but also
must be engaged in responsibly.
7. Specific components of sexuality
education offered in schools,
religious institutions, parent
organizations, and other
community agencies vary
based on many factors. The
pediatrician can serve as a
resource to each.
8. School-based comprehensive
sexuality education that
emphasizes prevention of
unintended pregnancy and STIs
should be encouraged.
9. The discussion of methods
of contraception and STI and
HPV cancer prevention with
male and female adolescents
is encouraged before the onset
of sexual intercourse (see the
AAP statement “Contraception
and Adolescents”). It is also
important to discuss consistent
use of safer sex precautions with
sexually active teens. Bright
Futures recommendations can
be used.
10. Abstinence is the most effective
strategy for preventing HIV
infection and other STIs, as well
as for prevention of pregnancy.
11. Preparation for college entry
is an excellent opportunity for
pediatricians to address issues
such as the effects of alcohol,
marijuana, and other drug
consumption on decisions about
safe, consensual sexual practices.
12. Children and adolescents with
special issues and disabilities
may benefit from additional
counseling, referrals, and sharing
of online resources listed at the
end of this report.
ONLINE SEXUALITY EDUCATION RESOURCES
School and Community
• United Nations Population
Fund: http:// www. unfpa. org/
public/ home/ adolescents/ pid/
6483. Advocates for and supports promotion of comprehensive sexuality education, provides programming guidance for both school and community settings, and advocates for wider educational opportunities for all young people and partners with civil society organizations.
• The National Alliance to Advance
Adolescent Health: http:// www.
thenationalallian ce. org/ . Uses resources, advocacy, collaboration, and research to improve and increase access to integrated physical, behavioral, and sexual health care for adolescents.
• The Future of Sexuality
Education (FoSe): http:// www.
futureofsexed. org/ documents/
josh- fose- standards- web. pdf.
Developed the National Sexuality Education Standards for teachers to standardize and improve the quality of sexuality education provided in
schools.
e7 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
FROM THE AMERICAN ACADEMY OF PEDIATRICS
• Sexuality Information and
Education Council of the
United States: http:// www.
sexedlibrary. org/ index. cfm. A resource for educators, counselors, administrators, and health professionals about human sexuality research, lesson plans, and professional development. The SexEd Library is a comprehensive online collection of lesson plans relate to sexuality education.
• Sexual Education: Get Real: http://
www. getrealeducation. org. Get Real: Comprehensive Sex Education is a unique curriculum designed for implementation in both middle and high schools. Information provided is medically accurate and age-appropriate and can reinforce family communication and improve communication skills for healthy relationships.
• Centers for Disease Control and
Prevention Health Education
Curriculum Analysis Tool: http://
www. cdc. gov/ healthyyouth/
hecat/ pdf/ HECAT_ Module_
SH. pdf. The Health Education Curriculum Analysis Tool can help school districts, schools, and others conduct a clear, complete, and consistent analysis of health education curricula based on the National Health Education Standards and the Centers for Disease Control and Prevention’s Characteristics of an Effective Health Education Curriculum. The Health Education Curriculum Analysis Tool can help schools select or develop appropriate and effective health education curricula and can be customized to meet local community needs and conform to the curriculum requirements of the state or school district.
Health Care Providers
• Bright Futures: http://
brightfutures. aap. org/ pdfs/
Guidelines_ PDF/ 9- Promoting-
Healthy- Sexual- Development. pdf.
Preventive health information and
recommendations about promoting healthy sexual development and sexuality to help health care providers during health supervision visits from early childhood through adolescence.
• The Community Preventive
Services Task Force: http://
www. thecommunityguide
. org/ hiv/ RRriskreduction.
html. Recommendations about interventions to promote behaviors that prevent or reduce the risk of pregnancy, HIV, and other STIs in adolescents.
• American Congress of Obstetricians
and Gynecologists: http:// www.
acog. org/ About- ACOG/ ACOG-
Departments/ Adolescent- Health-
Care. Information and resources about adolescent sexuality and sex education.
Youth
• Scarleteen: http:// www. scarleteen.
com/ . Scarleteen is an independent, grassroots sexuality education and support organization and Web site. Founded in 1998, Scarleteen.com is visited by approximately three-quarters of a million diverse people each month worldwide, most between the ages of 15 and 25. It is the highest-ranked Web site for sex education and sexuality advice online and has held that rank through most of its tenure.
• Sex, etc: http:// sexetc. org/ .
Sexetc.org has comprehensive sex
education information, including
the following:
⚬ Stories written by teen
staff writers and national
contributors.
⚬ Opportunities to get involved
and make a difference on sexual
health issues.
⚬ The Sex, etc. blog, which
addresses timely and relevant
news.
⚬ Forums where teens can
participate in moderated
discussions with other teens.
⚬ “Sex in the States, ” which is a
state-by-state guide to teens’
rights to sex education, birth
control, and more.
⚬ Videos about sexual health.
⚬ A sex terms glossary of almost
400 terms.
• Love is Respect: http:// www.
loveisrespect. org/ . Loveisrespect is a project of the National Domestic Violence Hotline and Break the Cycle. By combining our resources and capacity, we are reaching more people, building more healthy relationships, and saving more lives.
Youth With Disabilities
• Parent Advocacy Coalition
for Educational Rights: www.
pacer. org. Parent training and information center for families of children and youth with all disabilities from birth through 21 years old. Parents can find publications, workshops, and other resources about a number of topics, including sexuality and disabilities.
• Your Child Development and
Behavioral Resources: www.
med. umich. edu/ 1libr/ yourchild/
disabsex. htm. A program at the University of Michigan that houses a resource list of materials and Web sites about sexuality education for youth with disabilities for families as well as for teachers, and providers.
• Center for Parent Information
and Resources: http:// www.
parentcenterhub. org/ repository/
sexed/ . Contains information about sexuality education for students with disabilities for use with parents and teachers. The site also contains information about specific disabilities and sexuality, such as autism spectrum disorders, cerebral palsy, and spina bifida.
e8 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
PEDIATRICS Volume 138 , number 2 , August 2016
Advocacy
• United Nations Population
Fund: http:// www. unfpa. org/
public/ home/ adolescents/ pid/
6483. Advocates for and supports promotion of comprehensive sexuality education, provides programming guidance for both school and community settings, and advocates for wider educational opportunities for all young people and partners with civil society organizations.
• National Alliance to Advance
Adolescent Health: http:// www.
thenationalallian ce. org/ . Uses resources, advocacy, collaboration, and research to improve and increase access to integrated physical, behavioral, and sexual health care for adolescents.
• Futures Without Violence: http://
www. futureswithoutvio lence.
org/ . Uses advocacy, collaboration, and training with policy makers; health care, legal, and educational professionals; and others to improve responses to violence and abuse against women and children.
• Advocates for Youth: http://
www. advocatesforyouth . org/ sex-
education- home. Leads efforts that help young people make informed and responsible decisions about their reproductive and sexual health and focuses its work on young people ages 14 to 25 in the United States and around the globe. There are a number of resources for multiple audiences on the Sex Education home page.
• The National Campaign to Prevent
Teen and Unplanned Pregnancy:
http:// thenationalcampai gn. org/
featured- topics/ sex- education-
and- effective- programs. A series of resources that relate to sex education and a database of those sex education programs and interventions that work as well as online curricula that can be used with various audiences, including teens, college students, and others.
LEAD AUTHORS
Cora C. Breuner, MD, MPH
Gerri Mattson, MD, MSPH
COMMITTEE ON ADOLESCENCE, 2015–2016
Cora C. Breuner, MD, MPH, FAAP, Chairperson
William P. Adelman, MD, FAAP
Elizabeth M. Alderman, MD, FSAHM, FAAP
Robert Garofalo, MD, FAAP
Arik V. Marcell, MD, MPH, FAAP
Makia E. Powers, MD MPH, FAAP
Krishna Kumari Upadhya, MD, FAAP
LIAISONS
Laurie L. Hornberger, MD, MPH, FAAP – Section on
Adolescent Health
Margo Lane, MD, FRCPC, FAAP – Canadian
Pediatric Society
Benjamin Shain, MD, PhD – American Academy of
Child and Adolescent Psychiatry
Julie Strickland, MD – American College of
Obstetricians and Gynecologists
Lauren B. Zapata, PhD, MSPH – Centers for
Disease Control and Prevention
STAFF
Karen S. Smith
James D. Baumberger, MPP
COMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY HEALTH, 2015–2016
Michael W. Yogman, MD, FAAP, Chairperson
Nerissa S. Bauer, MD, MPH, FAAP
Thresia B. Gambon, MD, FAAP
Arthur Lavin, MD, FAAP
Keith M. Lemmon, MD, FAAP
Gerri Mattson, MD, FAAP
Jason R. Rafferty, MD, MPH, EdM
Lawrence S. Wissow, MD, MPH, FAAP
CONSULTANT
George J. Cohen, MD
LIAISONS
Sharon Berry, PhD, LP – Society of Pediatric
Psychology
Terry Carmichael, MSW – National Association of
Social Workers
Edward R. Christophersen, PhD, FAAP – Society of
Pediatric Psychology
Norah L. Johnson, PhD, RN, CPNP-BC – National
Association of Pediatric Nurse Practitioners
Leonard R. Sulik, MD – American Academy of
Child and Adolescent Psychiatry
STAFF
Stephanie Domain, MS, CHES
Tamar M. Haro
ABBREVIATIONS
AAP: American Academy of
Pediatrics
FoSE: Future of Sex Education
Initiative
HPV: human papillomavirus
STI: sexually transmitted
infection
REFERENCES
1. American Academy of Pediatrics,
Committee on Psychosocial Aspects of
Child and Family Health and Committee
on Adolescence. Sexuality education
for children and adolescents.
Pediatrics. 2001;108(2):498–502
2. Gruber EL, Wang PH, Christensen JS,
Grube JW, Fisher DA. Private television
viewing, parental supervision, and
sexual and substance use risk
behaviors in adolescents [abstract]. J
Adolesc Health. 2005;36(2):107
3. Strasburger VC; Council on
Communications and Media. American
Academy of Pediatrics. Policy
statement—sexuality, contraception,
and the media. Pediatrics.
2010;126(3):576–582
4. Boekeloo BO. Will you ask? Will they
tell you? Are you ready to hear and
respond? Barriers to physician-
adolescent discussion about sexuality.
JAMA Pediatr. 2014;168(2):111–113
5. Duncan P, Hagan JF Jr, Shaw JS.
Promoting healthy sexual development
and sexuality. In: American Academy of
Pediatrics. Bright Futures: Guidelines
for Health Supervision of Infants,
Children, and Adolescents. Elk Grove
Village, IL: American Academy of
Pediatrics; 2008:169–176. Available at:
https:// brightfutures. aap. org/ Bright%20
Futures%20 Documents/ 9- Sexuality. pdf.
Accessed September 28, 2015
6. Martino SC, Elliott MN, Corona R, Kanouse
DE, Schuster MA. Beyond the “big talk”:
the roles of breadth and repetition in
parent-adolescent communication about
sexual topics. Pediatrics. 2008;121(3).
Available at: www. pediatrics. org/ cgi/
content/ full/ 121/ 3/ e612
7. Swartzendruber A, Zenilman JM. A
national strategy to improve sexual
health. JAMA. 2010;304(9):1005–1006
e9 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

FROM THE AMERICAN ACADEMY OF PEDIATRICS
8. Sexuality Information and Education
Council of the United States. Position
Statement on Human Sexuality.
Available at: www. siecus. org/ index.
cfm? fuseaction= page. viewPage&
pageId= 494& parentID= 472. Accessed
July 16, 2015
9. Future of Sex Education (FoSE).
National Sexuality Education Standards
Tools. Available at: http:// www.
futureofsexed. org/ documents/ josh-
fose- standards- web. pdf. Accessed July
16, 2015
10. Jackson CA, Henderson M, Frank JW,
Haw SJ. An overview of prevention of
multiple risk behaviour in adolescence
and young adulthood. J Public Health
(Oxf). 2012;34(suppl 1):i31–i40
11. Kramer A. Girl Talk: What High School
Senior Girls Have to Say About Sex,
Love, and Relationships. Washington,
DC: The National Campaign to Prevent
Teen and Unplanned Pregnancy; 2012
12. Chin HB, Sipe TA, Elder R, et al;
Community Preventive Services
Task Force. The effectiveness of
group-based comprehensive risk-
reduction and abstinence education
interventions to prevent or reduce the
risk of adolescent pregnancy, human
immunodefi ciency virus, and sexually
transmitted infections: two systematic
reviews for the Guide to Community
Preventive Services. Am J Prev Med.
2012;42(3):272–294
13. Hamilton BE, Ventura SJ; Centers
for Disease Control and Prevention,
National Center for Health Statistics.
Birth rates for U.S. teenagers reach
historic lows for all age and ethnic
groups. NCHS Data Brief. 2012;(89):1–8
14. United Nations. Statistics Division. Live
births by age of mother and sex of child,
general and age-specifi c fertility rates:
latest available year, 2002–2011. In:
Demographic Yearbook. New York, NY:
United Nations, Statistics Division; 2012.
Available at: http:// unstats. un. org/ unsd/
demographic/ products/ dyb/ dyb2011/
Table10. pdf. Accessed July 16, 2015
15. Finer LB, Zolna MR. Unintended
pregnancy in the United States:
incidence and disparities, 2006.
Contraception. 2011;84(5):478–485
16. Centers for Disease Control and
Prevention. Health Education
Curriculum Analysis Tool (HECAT).
Available at: www. cdc. gov/ HealthyYouth/
HECAT/ . Accessed July 16, 2015
17. Wilson SF, Strohsnitter W, Baecher-Lind
L. Practices and perceptions among
pediatricians regarding adolescent
contraception with emphasis on
intrauterine contraception. J Pediatr
Adolesc Gynecol. 2013;26(5):281–284
18. Donaldson AA, Lindberg LD, Ellen JM,
Marcell AV. Receipt of sexual health
information from parents, teachers,
and healthcare providers by sexually
experienced U.S. adolescents. J
Adolesc Health. 2013;53(2):235–240
19. Lindberg LD, Maddow-Zimet I, Boonstra
H. Changes in adolescents' receipt of
sex education, 2006-2013. J Adolesc
Health. 2016;58(6):621–627
20. Hall KS, McDermott Sales J, Komro KA,
Santelli J. The state of sex education
in the United States. J Adolesc Health.
2016;58(6):595–597
21. Cheng MM, Udry JR. Sexual behaviors
of physically disabled adolescents in
the United States. J Adolesc Health.
2002;31(1):48–58
22. Florida Developmental Disabilities
Council Inc. Developmental disabilities:
an instructional manual for parents
of and individuals with developmental
disabilities. Available at: www. fddc. org/
sites/ default/ fi les/ fi le/ publications/
Sexuality%20 Guide- Parents- English. pdf.
Accessed July 16, 2015
23. Murphy NA, Elias ER; American
Academy of Pediatrics, Council on
Children With Disabilities. Sexuality
of children and adolescents with
developmental disabilities. Pediatrics.
2006;118(1):398–403
24. Committee On Adolescence. Offi ce-
based care for lesbian, gay, bisexual,
transgender, and questioning youth.
Pediatrics. 2013;132(1):198–203
25. Institute of Medicine, Committee on
Lesbian, Gay, Bisexual, and Transgender
Health Issues and Research Gaps and
Opportunities. The Health of Lesbian,
Gay, Bisexual, and Transgender
People: Building a Foundation for
Better Understanding. Washington, DC:
National Academies Press; 2011
26. Spigarelli MG. Adolescent sexual
orientation. Adolesc Med State Art Rev.
2007;18(3):508–518, vii
27. US Preventive Services Task Force.
Sexually transmitted infections: behavioral
counseling. Released September 2014.
Available at: www. uspreventiveservi
cestaskforce. org/ uspstf/ uspsstds. htm.
Accessed July 16, 2015
28. Martinez G, Copen CE, Abma JC;
Centers for Disease Control and
Prevention, National Center for Health
Statistics. Teenagers in the United
States: sexual activity, contraceptive
use, and childbearing, 2006-2010
national survey of family growth. Vital
Health Stat 23. 2011;23(31):1–35
29. Eaton DK, Kann L, Kinchen S, et
al; Centers for Disease Control
and Prevention (CDC). Youth risk
behavior surveillance - United
States, 2011. MMWR Surveill Summ.
2012;61(4):1–162
30. Caldas SJ, Bensy ML. The sexual
maltreatment of students with
disabilities in American school
settings. J Child Sex Abuse.
2014;23(4):345–366
31. Lindberg LD, Santelli JS, Singh S.
Changes in formal sex education: 1995-
2002. Perspect Sex Reprod Health.
2006;38(4):182–189
32. Kohler PK, Manhart LE, Lafferty WE.
Abstinence-only and comprehensive
sex education and the initiation of
sexual activity and teen pregnancy. J
Adolesc Health. 2008;42(4):344–351
33. Advocates for Youth. Science and
Success. 3rd ed. Programs that
Work to Prevent Teen Pregnancy, HIV
and STIs in the US. Washington, DC:
Advocates for Youth; 2012
34. Sexuality Information and Education
Council of the United States. Sexuality
Education Q & A. Available at: www.
siecus. org/ index. cfm? fuseaction=
page. viewpage& pageid= 521&
grandparentID= 477& parentID= 514.
Accessed July 16, 2015
35. Cavazos-Rehg PA, Krauss MJ,
Spitznagel EL, et al. Associations
between sexuality education in schools
and adolescent birthrates: a state-
level longitudinal model. Arch Pediatr
Adolesc Med. 2012;166(2):134–140
36. Frappier JY, Kaufman M, Baltzer F, et
al. Sex and sexual health: a survey of
Canadian youth and mothers. Paediatr
Child Health. 2008;13(1):25–30
e10 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 2 , August 2016
37. Merzel CR, VanDevanter NL,
Middlestadt S, Bleakley A, Ledsky R,
Messeri PA. Attitudinal and contextual
factors associated with discussion
of sexual issues during adolescent
health visits. J Adolesc Health.
2004;35(2):108–115
38. Mueller TE, Gavin LE, Kulkarni A. The
association between sex education
and youth’s engagement in sexual
intercourse, age at fi rst intercourse,
and birth control use at fi rst sex. J
Adolesc Health. 2008;42(1):89–96
39. Grossman JM, Tracy AJ, Charmaraman
L, Ceder I, Erkut S. Protective effects
of middle school comprehensive sex
education with family involvement. J
Sch Health. 2014;84(11):739–747
40. Guttmacher Institute. State policies in
brief: sex and HIV education. Available at:
www. guttmacher. org/ statecenter/ spibs/
spib_ SE. pdf. Accessed July 16, 2015
41. Kann L, Telljohan S, Hunt H, Hunt P, Haller
R. Health education. In: Centers for
Disease Control and Prevention. Results
from the School Health Policies and
Practices Study. Atlanta, GA: Centers for
Disease Control and Prevention; 2013.
Available at: www. cdc. gov/ healthyyouth/
shpps/ 2012/ pdf/ shpps- results_ 2012.
pdf#page= 27. Accessed July 16, 2015
42. Martinez G, Abma J, Copen C. Educating
teenagers about sex in the United
States. NCHS Data Brief. 2010;(44):1–8
43. Eastman KL, Corona R, Schuster MA.
Talking parents, healthy teens: a
worksite-based program for parents
to promote adolescent sexual health.
Prev Chronic Dis. 2006;3(4):A126
44. Strasburger VC, Brown SS. Sex
education in the 21st century. JAMA.
2014;312(2):125–126
45. Jaccard J, Levitz N. Counseling
adolescents about contraception:
towards the development of
an evidence-based protocol for
contraceptive counselors. J Adolesc
Health. 2013;52(suppl 4):S6–S13
46. Wight D, Fullerton D. A review of
interventions with parents to promote
the sexual health of their children. J
Adolesc Health. 2013;52(1):4–27
47. Klein JD, Sabaratnam P, Pazos B,
Auerbach MM, Havens CG, Brach MJ.
Evaluation of the parents as primary
sexuality educators program. J Adolesc
Health. 2005;37(suppl 3):S94–S99
48. Robert AC, Sonenstein FL. Adolescents’
reports of communication with their
parents about sexually transmitted
diseases and birth control: 1988,
1995, and 2002. J Adolesc Health.
2010;46(6):532–537
49. Akers AY, Holland CL, Bost J.
Interventions to improve parental
communication about sex: a
systematic review. Pediatrics.
2011;127(3):494–510
50. Kirkman M, Rosenthal DA, Feldman SS.
Talking to a tiger: fathers reveal their
diffi culties in communicating about
sexuality with adolescents. New Dir
Child Adolesc Dev. 2002;(97):57–74
51. Jemmott LS, Outlaw FH, Jemmott
JB, Brown EJ, Howard M, Hopkins B.
Strengthening the bond: the Mother
and Son Health Promotion Project.
In: Pequegnat W, Szapocznik J, eds.
Inside Families: The Role of Families
in Preventing and Adapting to HIV/
AIDS. Bethesda, MD: Sage Publications;
2000:133–151
52. King V, Sobolewski JM. Nonresident
fathers’ contributions to adolescent
well-being. J Marriage Fam.
2006;68(3):537–557
53. Carlson MJ. Family structure,
father involvement, and adolescent
behavioral outcomes. J Marriage Fam.
2006;68(1):137–154
54. Ball H. Theory-based abstinence-only
intervention may delay sexual initiation
among black urban youth. Perspect
Sex Reprod Health. 2010;42(2):135–136
55. Jemmott JB III, Jemmott LS, Fong GT.
Effi cacy of a theory-based abstinence-
only intervention over 24 months: a
randomized controlled trial with young
adolescents. Arch Pediatr Adolesc
Med. 2010;164(2):152–159
56. Kirby D. The impact of abstinence
and comprehensive sex and STD/HIV
education programs on adolescent
sexual behavior. Sexuality Research
and Social Policy. 2008;5(3):18–27
57. Trenholm C, Devaney B, Fortson K, Quay
L, Wheeler J, Clark M; Mathematica
Policy Research Inc. Impacts of
Four Title V, Section 510 Abstinence
Education Programs. Final Report.
Submitted to US Department of Health
and Human Services, Offi ce of the
Assistant Secretary for Planning and
Evaluation. Princeton, NJ: Mathematica
Policy Research Inc; 2007. Available at:
www. mathematica- mpr. com/ ~/ media/
publications/ PDFs/ impactabstinence.
pdf. Accessed July 16, 2015
58. Catalog of Federal Domestic
Assistance. Community-based
abstinence education. Available
at: https:// www. cfda. gov/ index? s=
program& mode= form& tab= core& id=
7a526272ffcfea290 497a3548fb92654.
Accessed July 16, 2015
59. Ott MA, Santelli JS. Abstinence and
abstinence-only education. Curr Opin
Obstet Gynecol. 2007;19(5):446–452
60. Santelli J, Ott MA, Lyon M, Rogers
J, Summers D. Abstinence-only
education policies and programs:
a position paper of the Society for
Adolescent Medicine. J Adolesc Health.
2006;38(1):83–87
61. Advocates for Youth. Comprehensive
sex education: research and results.
Available at: www. advocatesforyouth .
org/ storage/ advfy/ documents/ fscse.
pdf. Accessed July 16, 2015
62. Brückner H, Bearman P. After the
promise: the STD consequences of
adolescent virginity pledges. J Adolesc
Health. 2005;36(4):271–278
63. Kirby DB, Laris BA, Rolleri LA. Sex and
HIV education programs: their impact
on sexual behaviors of young people
throughout the world. J Adolesc
Health. 2007;40(3):206–217
64. Kirby D. Emerging Answers: Research
Findings on Programs to Reduce Teen
Pregnancy. Washington, DC: National
Campaign to Prevent Teen Pregnancy;
2001
65. Manlove J, Romano-Papillo A,
Ikramullah E. Not Yet: Programs
to Delay First Sex Among Teens.
Washington, DC: National Campaign to
Prevent Teen Pregnancy; 2004
66. Bearman PS, Brueckner H. Promising
the future: virginity pledges and fi rst
intercourse. American Journal of
Sociology. 2001;106(4):859–912
67. Kraft JM, Kulkarni A, Hsia J, Jamieson
DJ, Warner L. Sex education and
adolescent sexual behavior: do
community characteristics matter?
Contraception. 2012;86(3):276–280
e11 at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2016-1348 originally published online July 18, 2016; 2016;138;Pediatrics
HEALTHCOMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY
Cora C. Breuner, Gerri Mattson, COMMITTEE ON ADOLESCENCE andSexuality Education for Children and Adolescents
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/138/2/e20161348including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/138/2/e20161348#BIBLThis article cites 48 articles, 6 of which you can access for free at:
Subspecialty Collections
icine_subhttp://www.aappublications.org/cgi/collection/adolescent_health:medAdolescent Health/Medicinesocial_aspects_of_child_and_family_healthhttp://www.aappublications.org/cgi/collection/committee_on_psychoCommittee on Psychosocial Aspects of Child and Family Healthencehttp://www.aappublications.org/cgi/collection/committee_on_adolescCommittee on Adolescencehttp://www.aappublications.org/cgi/collection/current_policyCurrent Policyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2016-1348 originally published online July 18, 2016; 2016;138;Pediatrics
HEALTHCOMMITTEE ON PSYCHOSOCIAL ASPECTS OF CHILD AND FAMILY
Cora C. Breuner, Gerri Mattson, COMMITTEE ON ADOLESCENCE andSexuality Education for Children and Adolescents
http://pediatrics.aappublications.org/content/138/2/e20161348located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2016 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

POLICY STATEMENT
Contraception for Adolescents
abstractContraception is a pillar in reducing adolescent pregnancy rates. TheAmerican Academy of Pediatrics recommends that pediatricians de-velop a working knowledge of contraception to help adolescents reducerisks of and negative health consequences related to unintended preg-nancy. Over the past 10 years, a number of new contraceptive methodshave become available to adolescents, newer guidance has been issuedon existing contraceptive methods, and the evidence base for contracep-tion for special populations (adolescents who have disabilities, areobese, are recipients of solid organ transplants, or are HIV infected)has expanded. The Academy has addressed contraception since 1980,and this policy statement updates the 2007 statement on contraceptionand adolescents. It provides the pediatrician with a description and ra-tionale for best practices in counseling and prescribing contraceptionfor adolescents. It is supported by an accompanying technical report.Pediatrics 2014;134:e1244–e1256
INTRODUCTION
Pediatricians play an important role in adolescent pregnancy pre-vention and contraception. Nearly half of US high school studentsreport ever having had sexual intercourse.1 Each year, approximately750 000 adolescents become pregnant, with more than 80% of thesepregnancies unplanned, indicating an unmet need for effective con-traception in this population.2,3 Although condoms are the most fre-quently used form of contraception (52% of females reported condomuse at last sex), use of more effective hormonal methods, includingcombined oral contraceptives (COCs) and other hormonal methods,was lower, at 31% and 12%, respectively, in 2011.1 Use of highly ef-fective long-acting reversible contraceptives, such as implants or in-trauterine devices (IUDs), was much lower.1
Adolescents consider pediatricians and other health care providersa highly trusted source of sexual health information.4,5 Pediatricians’long-term relationships with adolescents and families allow them toask about sensitive topics, such as sexuality and relationships, and topromote healthy sexual decision-making, including abstinence andcontraceptive use for teenagers who are sexually active. Additionally,medical indications for hormonal contraception, such as dysmenor-rhea, heavy menstrual bleeding or other abnormal uterine bleeding,acne, and polycystic ovary syndrome, are often uncovered duringadolescent visits. A working knowledge of contraception will assist thepediatrician in both sexual health promotion and treatment of common
COMMITTEE ON ADOLESCENCE
KEY WORDScontraception, adolescent, birth control, intrauterine device,contraceptive implant, oral contraceptive pills, contraceptiveinjection
ABBREVIATIONSAAP—American Academy of PediatricsACOG—American College of Obstetricians and GynecologistsBMD—bone mineral densityCDC—Centers for Disease Control and PreventionCOC—combined oral contraceptiveDMPA—depot medroxyprogesterone acetateEC—emergency contraceptionFDA—Food and Drug AdministrationHIPAA—Health Insurance Portability and Accountability ActIUD—intrauterine deviceLARC—long-acting reversible contraceptionPID—pelvic inflammatory diseaseSTI—sexually transmitted infection
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The guidance in this statement does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account individual circumstances, may beappropriate.
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-2299
doi:10.1542/peds.2014-2299
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
e1244 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the ChildHealth Care System and/or Improve the Health of all Children

adolescent gynecologic problems. Contra-ception has been inconsistently coveredas part of insurance plans. However, theInstitute of Medicine has recommendedcontraception as an essential componentof adolescent preventive care,6 and thePatient Protection and Affordable CareAct of 2010 (Pub L No. 111–148) requirescoverage of preventive services forwomen, which includes contraception,without a copay.7,8
SETTING THE STAGE
Confidentiality and Consent
In the setting of contraception and sexualhealth care, the American Academy ofPediatrics (AAP) believes that policiessupporting adolescent consent and pro-tecting adolescent confidentiality are inthe best interests of adolescents. Ac-cordingly, best practice guidelines rec-ommend confidentiality around sexualityand sexually transmitted infections (STIs)and minor consent for contraception.9–11
The majority of states have specific lawsregarding minor consent to contracep-tion (see State Minor Consent Laws:A Summary12 and the Guttmacher Insti-tute’s State Center13 at http://www.guttmacher.org/statecenter/ for reg-ularly updated state-by-state summaries).For states without specific laws, bestpractice guidelines, federal statutes, andfederal case law may support minorconfidentiality and consent.12 For exam-ple, family planning clinics funded byTitle X of the federal Public Health Ser-vices Act (42 USC xx300–300a-6 [1970])are required to provide confidentialservices to adolescents.12
The Health Insurance Portability andAccountability Act (HIPAA [Pub L No.104–191, 1996]) specifically addressesminor confidentiality. Although HIPAAallows parents access to a minor’srecords as personal representatives,that access is denied when the minor isprovided with confidentiality under stateor other laws or when the parent agreesthat the minor may have confidential
care.14 Therefore, the AAP recommendsthat pediatricians have an office policythat explicitly describes confidentialservices and that pediatricians discuss(and document) confidentiality with allparents and adolescents. As an addi-tional protection for minors’ confiden-tiality, HIPAA states that if there is noapplicable state law about the rightsof parents to access the protectedhealth information of their children,pediatricians (or other licensed healthprofessionals) may exercise their pro-fessional judgment to provide or denyparental access to the records.14 Thiscan be accomplished with careful docu-mentation of their professional judgment.
Insurance, billing, and electronic healthrecord systems create additionalchallenges, including maintaining theconfidentiality of visits, visit content,associated laboratory test results, andpayment for the contraceptive methoditself.15 For additional discussion ofelectronic health records, see the AAPpolicy statement on health informationtechnology.16
Careful attention to minor consent andconfidentiality is important, because lim-itations on confidentiality and consent arelinked to lower use of contraceptives andhigher adolescent pregnancy rates.17–21
Parents need not be adversaries; infact, many parents are supportive ofminor consent and confidentiality forsexual health services.22,23 As per-mitted by law, adolescent contraceptionshould be provided as a confidentialservice, with adolescents encouragedto involve parents or trusted adultsas they are able.
Sexual History Taking andCounseling
Bright Futures recommends that pedia-tricians take a developmentally targetedsexual history, assess STI and pregnancyrisk, and provide appropriate screening,counseling, and, if needed, contra-ceptives.24 Key to history taking is an
honest, caring, nonjudgmental attitudeand a comfortable, matter-of-fact ap-proach to asking questions. This canbe accomplished by assessing the 5 Psof sexual history taking, as describedby the Centers for Disease Control andPrevention (CDC): partners, preventionof pregnancy, protection from STIs, sex-ual practices, and past history of STIsand pregnancy.25 Counseling should drawon motivational interviewing approaches,with the focus of the interview on futuregoals, belief in the adolescents’ capacityto change, and engagement of theadolescent in the process of adoptinghealth-promoting behaviors.26 For anexample of motivational interviewingfor sexual health counseling, see Ottet al (2007),27 and for a more detaileddiscussion of counseling approaches,see the accompanying technical re-port.28
Counseling About Abstinence andContraception
Counseling about abstinence andpostponement of sexual intercourseis an important aspect of adolescentsexual health care. Abstinence is 100%effective in preventing pregnancy andSTIs and is an important part of con-traceptive counseling. Adolescents shouldbe encouraged to delay sexual onset untilthey are ready. However, existing datasuggest that, over time, perfect ad-herence to abstinence is low (ie, manyadolescents planning on abstinence donot remain abstinent).29,30 Therefore,pediatricians should not rely on absti-nence counseling alone but shouldadditionally provide access to com-prehensive sexual health informationto all adolescents. For sexually activeadolescents, including gay and lesbianadolescents,31 and those consideringinitiation of sexual activity, counselingadditionally includes initiating contra-ception, supporting adherence to thecontraceptive method, managing ad-verse effects, and providing periodicscreening for STIs.24
PEDIATRICS Volume 134, Number 4, October 2014 e1245
FROM THE AMERICAN ACADEMY OF PEDIATRICS
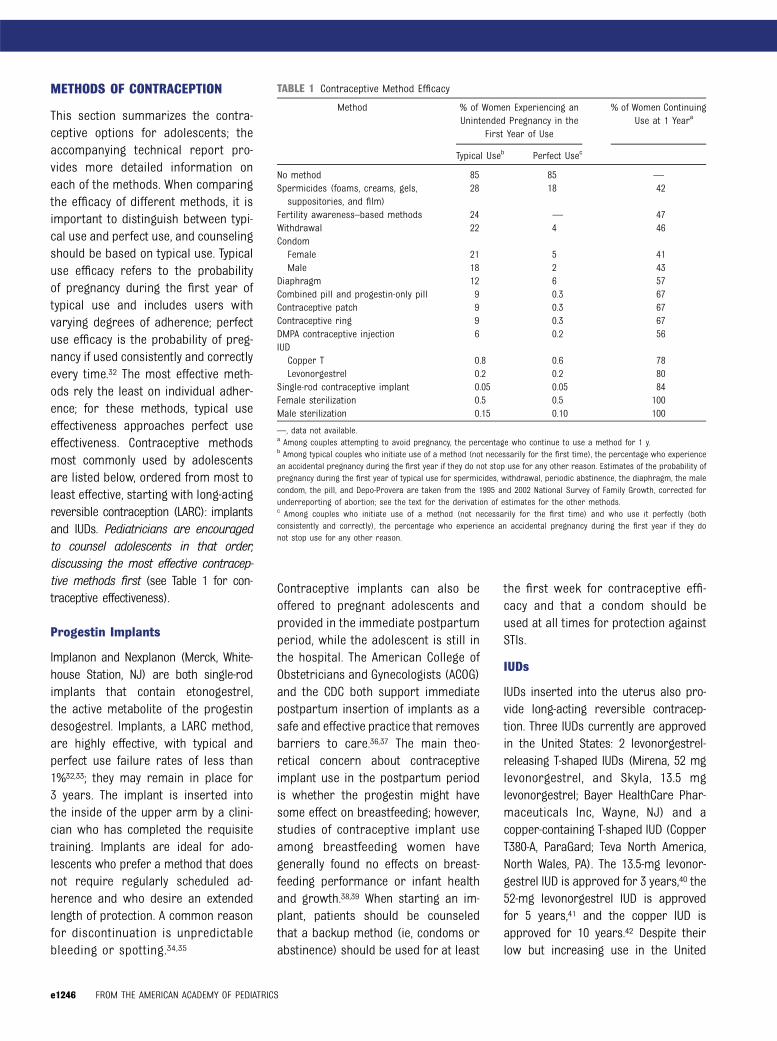
METHODS OF CONTRACEPTION
This section summarizes the contra-ceptive options for adolescents; theaccompanying technical report pro-vides more detailed information oneach of the methods. When comparingthe efficacy of different methods, it isimportant to distinguish between typi-cal use and perfect use, and counselingshould be based on typical use. Typicaluse efficacy refers to the probabilityof pregnancy during the first year oftypical use and includes users withvarying degrees of adherence; perfectuse efficacy is the probability of preg-nancy if used consistently and correctlyevery time.32 The most effective meth-ods rely the least on individual adher-ence; for these methods, typical useeffectiveness approaches perfect useeffectiveness. Contraceptive methodsmost commonly used by adolescentsare listed below, ordered from most toleast effective, starting with long-actingreversible contraception (LARC): implantsand IUDs. Pediatricians are encouragedto counsel adolescents in that order,discussing the most effective contracep-tive methods first (see Table 1 for con-traceptive effectiveness).
Progestin Implants
Implanon and Nexplanon (Merck, White-house Station, NJ) are both single-rodimplants that contain etonogestrel,the active metabolite of the progestindesogestrel. Implants, a LARC method,are highly effective, with typical andperfect use failure rates of less than1%32,33; they may remain in place for3 years. The implant is inserted intothe inside of the upper arm by a clini-cian who has completed the requisitetraining. Implants are ideal for ado-lescents who prefer a method that doesnot require regularly scheduled ad-herence and who desire an extendedlength of protection. A common reasonfor discontinuation is unpredictablebleeding or spotting.34,35
Contraceptive implants can also beoffered to pregnant adolescents andprovided in the immediate postpartumperiod, while the adolescent is still inthe hospital. The American College ofObstetricians and Gynecologists (ACOG)and the CDC both support immediatepostpartum insertion of implants as asafe and effective practice that removesbarriers to care.36,37 The main theo-retical concern about contraceptiveimplant use in the postpartum periodis whether the progestin might havesome effect on breastfeeding; however,studies of contraceptive implant useamong breastfeeding women havegenerally found no effects on breast-feeding performance or infant healthand growth.38,39 When starting an im-plant, patients should be counseledthat a backup method (ie, condoms orabstinence) should be used for at least
the first week for contraceptive effi-cacy and that a condom should beused at all times for protection againstSTIs.
IUDs
IUDs inserted into the uterus also pro-vide long-acting reversible contracep-tion. Three IUDs currently are approvedin the United States: 2 levonorgestrel-releasing T-shaped IUDs (Mirena, 52 mglevonorgestrel, and Skyla, 13.5 mglevonorgestrel; Bayer HealthCare Phar-maceuticals Inc, Wayne, NJ) and acopper-containing T-shaped IUD (CopperT380-A, ParaGard; Teva North America,North Wales, PA). The 13.5-mg levonor-gestrel IUD is approved for 3 years,40 the52-mg levonorgestrel IUD is approvedfor 5 years,41 and the copper IUD isapproved for 10 years.42 Despite theirlow but increasing use in the United
TABLE 1 Contraceptive Method Efficacy
Method % of Women Experiencing anUnintended Pregnancy in the
First Year of Use
% of Women ContinuingUse at 1 Yeara
Typical Useb Perfect Usec
No method 85 85 —
Spermicides (foams, creams, gels,suppositories, and film)
28 18 42
Fertility awareness–based methods 24 — 47Withdrawal 22 4 46CondomFemale 21 5 41Male 18 2 43
Diaphragm 12 6 57Combined pill and progestin-only pill 9 0.3 67Contraceptive patch 9 0.3 67Contraceptive ring 9 0.3 67DMPA contraceptive injection 6 0.2 56IUDCopper T 0.8 0.6 78Levonorgestrel 0.2 0.2 80
Single-rod contraceptive implant 0.05 0.05 84Female sterilization 0.5 0.5 100Male sterilization 0.15 0.10 100
—, data not available.a Among couples attempting to avoid pregnancy, the percentage who continue to use a method for 1 y.b Among typical couples who initiate use of a method (not necessarily for the first time), the percentage who experiencean accidental pregnancy during the first year if they do not stop use for any other reason. Estimates of the probability ofpregnancy during the first year of typical use for spermicides, withdrawal, periodic abstinence, the diaphragm, the malecondom, the pill, and Depo-Provera are taken from the 1995 and 2002 National Survey of Family Growth, corrected forunderreporting of abortion; see the text for the derivation of estimates for the other methods.c Among couples who initiate use of a method (not necessarily for the first time) and who use it perfectly (bothconsistently and correctly), the percentage who experience an accidental pregnancy during the first year if they donot stop use for any other reason.
e1246 FROM THE AMERICAN ACADEMY OF PEDIATRICS

States, IUDs are used extensively world-wide because they are safe and effectivemethods of contraception with typicaland perfect use failure rates of less than1%.43 The copper IUD can be used asemergency contraception (EC) within 5days of unprotected intercourse.43,44
Despite past concerns, IUDs are nowknown to be safe for nulliparous ado-lescents. IUDs themselves do not causetubal infertility in nulliparous women,45
and studies support a rapid return tofertility after IUD removal.46,47 The riskof pelvic infection with IUDs occursonly during insertion. Beyond the first21 days, IUDs do not increase rates ofSTIs or pelvic inflammatory disease(PID).48,49 Unless the adolescent is atvery high risk for STIs (eg, had sexwith a partner with known gonorrhea),screening for gonorrhea and chlamydiacan be performed on the day of in-sertion.50 Treatment, if needed, canbe subsequently provided without IUDremoval, because studies have dem-onstrated that, provided the patientimproves with treatment, both STIsand PID can be treated with the IUDin place.51,52 Contraindications to IUDplacement are limited to current pu-rulent cervicitis, gonorrhea, or chla-mydia, current PID and other currentpelvic infections (see “US Medical Eli-gibility Criteria for Contraceptive Use”for more extensive discussion).37 PastPID is not a contraindication to IUD use.HIV infection and immunosuppressionare also not contraindications to IUDuse.
IUDs can also be offered to pregnantadolescents and provided in the im-mediate postpartum period, while theadolescent is still in the hospital. Twosystematic reviews concluded that im-mediate postpartum insertion of IUDsis safe and effective,53,54 and both ACOGand the CDC support this practice.36,37,55
Studies have shown that many womenwho desire an IUD at the time of deliverydo not return for later insertion and
that immediate insertion of IUDs pro-vides similar contraceptive coverageas delayed insertion, even with higherexpulsion rates with immediate in-sertion.56,57
The emerging adolescent-specific dataon IUDs are promising. However, thereare some disadvantages. The limiteddata in adolescents suggest that ex-pulsion, which occurs in fewer than5% of women using IUDs, may occurmore frequently in younger women.58
Another concern is that more than half ofyoung nulliparous women report mod-erate to severe pain with insertion.59,60
Nonetheless, studies demonstrate IUDcontinuation rates in adolescents thatexceed those with other hormonalmethods and effective use of the levo-norgestrel IUD for menstrual suppres-sion in adolescent patients with complexmedical conditions.61–67
Progestin-Only InjectableContraception
Depot medroxyprogesterone acetate(DMPA, also known by the brand nameDepo-Provera; Pfizer, New York, NY) isa long-acting progestin that is given asa single injection every 13 weeks (upto 15 weeks) using a dose of either150 mg delivered intramuscularly or104 mg delivered subcutaneously. Manyhealth care providers schedule visitsevery 11 to 12 weeks for adolescentsto allow for missed or delayed visits.Both regimens have similar effective-ness and side effects68 and are highlyeffective in preventing pregnancy. Inthe first year of use, the probability ofbecoming pregnant with typical use isapproximately 6%.32 DMPA can be ini-tiated on the same day as the visit(“mid-cycle” or “quick” start) as longas the health care provider is reason-ably certain the adolescent is notpregnant. For additional details, seethe accompanying technical report andthe CDC’s 2013 “US Selected PracticeRecommendations for Contraceptive
Use.”52 When starting DMPA, patientsshould be counseled that a backupmethod (eg, condoms or abstinence)should be used for at least the firstweek for contraceptive efficacy andthat a condom should be used at alltimes for protection against STIs.
DMPA is convenient for many adoles-cents because of its ease of use. Otheradvantages include improvement indysmenorrhea and protection againstiron deficiency anemia and endome-trial cancer.69 DMPA is safe for mostpatients with chronic illness,37 is thoughtto raise the seizure threshold in ado-lescents with epilepsy,70 and may de-crease sickle cell crises.71,72
The major disadvantages of DMPA in-clude the need for an injection every13 weeks and the menstrual cycleirregularities that are present fornearly all patients initially. These men-strual irregularities typically improveover time73,74 and may be less likely toresult in discontinuation if patients arecounseled about these effects beforethe first injection.75,76 Other possible ad-verse effects include headache, mastalgia,hair loss, change in libido, and weightgain. Studies in both adolescents77 andadults78 suggest that weight gain statusat 6 months is a strong predictor of fu-ture excessive weight gain with ongoingDMPA use, but that weight gain does notoccur in all patients.79,80
DMPA causes reductions in bone min-eral density (BMD),81–83 and in 2004 theUS Food and Drug Administration (FDA)issued a black-box warning about therisk of decreased BMD among DMPAusers.84 Subsequent publications doc-ument a substantial recovery of BMDafter the patient discontinues DMPA,85–87
and ACOG, recognizing the risk of un-wanted pregnancy if women’s contra-ceptive options are limited, does notadvise limiting DMPA use to 2 years (incontrast to earlier concerns88) or rou-tinely monitoring bone density after thattime frame.89 Nonetheless, it remains
PEDIATRICS Volume 134, Number 4, October 2014 e1247
FROM THE AMERICAN ACADEMY OF PEDIATRICS

important to consider other risk factorsfor osteoporosis and to tailor counselingand recommendations to each patient.All patients should be counseled aboutmeasures that promote skeletal health,such as daily intake of 1300 mg of cal-cium and 600 IU of vitamin D and regularweight-bearing exercise.90
Combined Oral Contraceptive Pills
COCs are the most popular methodof hormonal contraception for ado-lescents. COCs all contain a progestinand an estrogen. In almost every pill, theestrogen component is ethinyl estradiolin amounts varying from 10 to 50 μg.Many adolescent medicine experts be-gin with a COC containing 30 to 35 μgof ethinyl estradiol and a progestinsuch as levonorgestrel or norgestimate.However, any “low-dose” pill (ie, con-taining ethinyl estradiol 35 μg or less )can be used. Although inspection of theexternal genitalia and a vaginal swab orurine screen for STIs are recommendedpractices in the care of sexually activepatients,91 no gynecologic examinationis needed to determine eligibility forCOC use. Like other combined methodsincluding the contraceptive vaginal ringand transdermal patch, COCs can bestarted on the same day as the visit(“quick start”) in healthy, nonpregnantadolescents. Patients should be coun-seled that a backup method (ie, con-doms or abstinence) should be used forat least the first 7 days for contracep-tive efficacy and that a condom shouldbe used at all times for protectionagainst STIs. The CDC recommends pre-scribing up to 1 year of COCs at a time.52
Additionally, a routine follow-up visit 1 to3 months after initiating COCs is usefulfor addressing adverse effects or ad-herence issues.
COCs have few contraindications inhealthy female adolescents. They shouldnot be prescribed for patients withsevere and uncontrolled hypertension(systolic pressure ≥160 mm Hg or
diastolic pressure ≥100 mmHg), ongo-ing hepatic dysfunction, complicatedvalvular heart disease, migraines withaura or focal neurologic symptoms,thromboembolism or thrombophilia,complications of diabetes (ie, nephropathy,retinopathy, neuropathy, or other vas-cular disease), and complicated solidorgan transplantation.37 The most se-rious adverse event associated with COCuse is the increased risk of blood clots,which increases from 1 per 10 000 to3 to 4 per 10 000 woman-years duringCOC use.92,93 In comparison, the in-cidence of venous thromboembolismassociated with pregnancy and post-partum is 10 to 20 per 10 000 woman-years, of which 1% to 2% are fatal.94,95
Although smoking should be discouraged,it is not a contraindication to COC usein teenagers and adults younger than35 years old.37
Patients should be informed that com-mon transient adverse effects of COCsinclude irregular bleeding, headache,and nausea. Recommendations formanaging adverse effects have beenpublished elsewhere96 or can be foundonline (http://www.managingcontraception.com/qa/index.php or http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6205a1.htm?s_cid=rr6205a1_w).52
Drug interactions should also beavoided. With medications that de-crease COC effectiveness (eg, anti-convulsants and antiretroviral drugs),patients may benefit from choosingan alternative method or dosing97 (seethe accompanying technical report foradditional details). Most broad-spectrumantibiotics (rifampin is an exception) donot affect the contraceptive effectivenessof COCs.37
Typical use failure rates are 9% inadults and may be higher in adoles-cents.32,98 Counseling should includestrategies to promote daily adher-ence, such as cell phone alarms andsupport from a family member orpartner. Patients should be instructed
on what to do if pills are missed. Amissed pill should be taken as soon asit is remembered. If more than 1 pill ina row is missed, only the most recentlymissed pill should be taken as soonas possible, and the remaining pillsshould be taken at the usual time.Patients should be reminded that 7consecutive hormone pills are neededto prevent ovulation. Additional instruc-tions can be accessed online (http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6205a1.htm?s_cid=rr6205a1_w#Fig2).52
EC is indicated if 2 or more pills aremissed in the first week of the cycle.99,100
EC should also be considered if 1 ormore pills were missed earlier in thesame cycle as a missed pill or late inthe previous cycle (see online instruc-tions provided earlier for details).
Many patients may benefit from de-creasing or eliminating the hormone-free (placebo) interval. Extended orcontinuous cycles may be useful fortreating medical conditions such asanemia, acne, severe dysmenorrhea,endometriosis, dysfunctional or heavymenstrual bleeding, Von Willebrand dis-ease, and other bleeding diatheses andfor adolescents who prefer amenor-rhea.101 These regimens may also beuseful for conditions that can be exac-erbated cyclically, such as migraine(without aura), epilepsy, irritable bowelsyndrome, inflammatory bowel disease,and some psychiatric and behavioralsymptoms102; the most common adverseeffect of extended or continuous cyclesis unscheduled bleeding. Patients maybe reassured to know that observationaldata indicate that COC use does not in-crease the risk of infertility or breastcancer103 and that use of COCs for morethan 4 years provides significant pro-tection against endometrial and ovariancancers.104
Contraceptive Vaginal Ring
The vaginal ring (NuvaRing; Merck, White-house Station, NJ) releases a combination
e1248 FROM THE AMERICAN ACADEMY OF PEDIATRICS
of estrogen and progestin and thus hasthe same eligibility criteria for use asCOCs. As with COCs, a same-day start(“quick start”) can also be used withthe vaginal ring. The ring is inserted inthe vagina and stays in place for 3weeks, with removal for 1 week to in-duce withdrawal bleeding, followedby insertion of a new ring. Patientsshould be instructed to insert a newring after 7 days even if bleeding hasnot ceased.
The ring has comparable efficacy, risks,and benefits as other combined hor-monal methods but provides the sim-plest regimen.32,105,106 Adverse effectsare also similar, with the additionalvaginal symptoms of discharge, dis-comfort, and problems related to thedevice (eg, expulsion).107 The ring is anexcellent method for extended usebecause, although labeled for 28 daysof use, the rings contain sufficientmedication to be used for up to 35days108 and thus can be replacedonce every calendar month. Sexuallyactive patients may be reassured toknow that most men were not both-ered by its presence, if it was notedat all.109,110
Transdermal Contraceptive Patch
The combination hormone (estrogen andprogestin) transdermal contraceptivepatch (Ortho Evra; Ortho-McNeil Phar-maceutical, Raritan, NJ) is placed onthe abdomen, upper torso, upper outerarm, or buttocks using 1 patch for eachof 3 weeks in a row, followed by 1 weekoff the patch, during which a with-drawal bleed usually occurs. Typicaluse failure rates are similar to thoseof COCs at 9%.32 The FDA has identi-fied increased estrogen exposure (1.6times higher than with a low-doseCOC111) and a potential increased riskof venous thromboembolism with thepatch112,113 (see accompanying tech-nical report for more completediscussion).
The patch has comparable efficacy,benefits, eligibility criteria for use, anddrug interactions as COCs; side effectsare similar to those of other combinedmethods, with the addition of dislodgedpatches and skin effects, such ashyperpigmentation,114,115 contact der-matitis, and other irritation.116 The riskof pregnancy with correct (“perfect”)use of the patch is slightly higher forwomen who weigh more than 198pounds than for women who weighless (0.9% vs 0.3% in first 12 months ofuse).117,118
Progestin-Only Pills
Progestin-only pills (also known as“mini-pills”) work primarily by thick-ening cervical mucus, not by inhibitingovulation. Because very stringent ad-herence is necessary, their failurerate can be significantly higher thanthose of other combined hormonaland progestin-only methods (IUDs andcontraceptive implants and injections).However, they provide an additionaloption for patients who have safetyconcerns about estrogen use (seeaccompanying technical report foradditional details).37
Male Condoms
The male condom is the most commoncontraceptive method used by ado-lescents, with up to 52% of female and75% of male adolescents reportingcondom use at last intercourse.1 Ad-vantages include male involvement inthe responsibility for contraception,easy accessibility by minors without aprescription, and low cost. Latex con-doms also reduce STI transmission,with consistent evidence for thereduction of gonorrhea, chlamydia,trichomoniasis,119–123 and hepatitis Band HIV transmission124 and emergingevidence for the reduction of herpessimplex virus,125,126 human papilloma-virus,127,128 and syphilis transmission.129
However, condom use requires com-
mitment at every sex act, tends to dropoff over time, and is influenced by in-dividual, relationship, and broader socialfactors.130–133 Although the perfect usefailure rate of condoms is 2%, the typicaluse failure rate is 18% for all users andcan be higher among adolescents.32 Thehigh typical use failure rate, coupledwith the condom’s high STI protection,has led to the recommendation for dualcontraception: condoms plus a highlyeffective hormonal or other long-actingmethod. Instructions for condom usecan be found in the accompanyingtechnical report, and additional detailsare provided in the AAP policy state-ment on condoms.133
Emergency Contraception
In the United States, EC is available asoral levonorgestrel; an oral progesteronereceptor modulator, ulipristal acetate;high-dose combined estrogen–progestinoral contraceptive pills (the Yuzpe regi-men); and placement of a copper IUD.Levonorgestrel EC is preferred to theYuzpe regimen because of the superioradverse effect profile and effectiveness,which is up to 85%.44,134 Ulipristal acetatemay have greater effectiveness than orallevonorgestrel at the end of the 5-daywindow of use, and its remaining effec-tiveness and adverse effect profile aresimilar to those of levonorgestrel.135,136 Inaddition, on the basis of recent dataabout lower efficacy of levonorgestrel EC,ulipristal may be more effective in peoplewho weigh more than 165 pounds.137,138
Placement of a copper-bearing IUD isless commonly used for EC in ado-lescents but is the most effective ECmethod, with a failure rate of lessthan 1%.139
The recommended dosage of levonor-gestrel is a single 1.5-mg dose.134,140 Itis available either as 2 pills (0.75 mgeach) or as 1 pill (Plan B One-Step;Teva Pharmaceuticals, Petah Tikva,Israel). Levonorgestrel-based EC delaysor inhibits ovulation and does not
PEDIATRICS Volume 134, Number 4, October 2014 e1249
FROM THE AMERICAN ACADEMY OF PEDIATRICS

appear to be effective once ovulationhas occurred. If used inadvertentlyduring early pregnancy, it is not ter-atogenic, only ineffective.141 Thus, apregnancy test is not mandatory beforelevonorgestrel EC is prescribed.44
Plan B One-Step is approved by theFDA as a nonprescription product forall women of childbearing potential.142
Generic versions are approved as anonprescription product for women17 years of age and older; however,proof of age is not required to pur-chase them. Providing EC in advanceincreases the likelihood of use whenit is needed without increasing sexualor contraceptive risk-taking behav-ior.143,144 Therefore, EC should be pre-scribed or recommended in advancefor use for up to 5 days after an eventof unprotected intercourse.44 Addi-tional details on EC mechanisms anduse can be found in the AAP policystatement on emergency contracep-tion44 and the accompanying technicalreport.
Withdrawal
Withdrawal, or coitus interruptus, isa method in which the male partnerattempts to pull out his penis beforeejaculation. Because 57% of femaleadolescents report using withdrawal,1
pediatricians should ask about it.However, because of its limited ef-fectiveness (22% failure rate amongall users)32 and lack of STI pro-tection, pediatricians should encour-age adolescents to adopt more effectivemethods.
Other Methods
The female condom, periodic abstinence(fertility awareness or “the rhythmmethod”), vaginal spermicides, thecervical cap, and the diaphragm aremethods less commonly used byadolescents. Additional descriptionsare available in the accompanyingtechnical report.
SPECIAL POPULATIONS
Adolescents With Disabilities andMedically Complex Illness
An estimated 16% to 25% of adoles-cents are identified as having specialhealth care needs, including physicaldisability, developmental disability, andmedically complex illness.145 The im-proved survival of adolescents withmedically complex illnesses, such asdisabilities, chronic disease, HIV, andsolid organ transplants, has promptedgreater attention to quality-of-life is-sues. These issues, including adoles-cent interest in romantic and sexualrelationships, are typically addressedby a pediatrician. Sexuality and sexualhealth care needs in this populationare often overlooked, yet data demon-strate that, compared with healthyadolescents, adolescents with chronicillness have similar levels of sexualbehaviors and sexual health outcomes(eg, STIs).146,147 In addition to pregnancyprevention, these adolescents may needmenstrual suppression for heavy men-strual bleeding, bleeding disorders, orchemotherapy. Other patients may beusing teratogenic medications and needcontraception for that reason. Issuesthat arise include safety concerns withestrogen use, medication interactions,and complications from the underlyingdisease. The CDC has recently addressedthe contraceptive needs of young womenwith medical conditions by publishingthe “US Medical Eligibility Criteria forContraceptive Use.”37 Available online,this document summarizes the literatureon safety and efficacy of different con-traceptive methods by medical condition.Additional details on specific populations(eg, those with disabilities) are sum-marized in the accompanying technicalreport.
Adolescents With Obesity
The sexual health needs and sexualbehaviors of adolescents with obesityare substantially similar to those of
their normal-weight peers.148,149 Inaddressing contraception, it is impor-tant to note that obesity and relatedendocrine effects can influence theefficacy and adverse effects profiles ofcontraceptives. For example, a smallnumber of excess pregnancies werefound among transdermal contracep-tive patch users weighing more than90 kg (198 lb).117,118 The World HealthOrganization and CDC report that dataare limited and inconsistent aboutwhether COC effectiveness varies bybody weight or BMI.37,150–152 A commonconcern of both adolescents and pro-viders is additional weight gain amongadolescents with obesity after theystart contraception. Data suggest thatwomen with obesity are no more likelyto gain weight with COCs, the vaginalring, IUDs, or implants than normal-weight peers. In contrast, adolescentswith obesity who used DMPA weremore likely than nonusers with obesity,COC users with obesity, and normal-weight DMPA users to gain weight.80
Increasing numbers of adolescents arehaving bariatric surgery proceduresperformed, and these patients needhighly effective contraception. Post-surgery data reveal an improvement infertility coupled with the potential fordecreased contraceptive effectivenessthrough malabsorption, vomiting, anddiarrhea.86 Professional consensusstatements recommend delaying preg-nancy for at least 12 months after theprocedure.153 All contraceptive meth-ods are safe for women with a historyof bariatric surgery, with the exceptionof oral contraceptives for women whohave undergone malabsorptive proce-dures.37 There is increasing experienceand success with the levonorgestrelIUD placed at the time of surgery.154
ADHERENCE AND FOLLOW-UP
Frequent follow-up is important tomaximize adherence for all methodsof contraception and to promote and
e1250 FROM THE AMERICAN ACADEMY OF PEDIATRICS

reinforce healthy decision-making. Ad-olescents count on trusted health pro-fessionals, such as pediatricians, forsupport and problem solving aroundcontinuation and adherence. Regularlyscheduled contraceptive follow-up vis-its should address use, adherence,adverse effects, and complications.Pediatricians can use motivational inter-viewing approaches to increase effectiveand consistent contraceptive use, in-cluding engaging parental support forcontraceptive adherence, when possi-ble. Follow-up visits should additionallyinclude reassessment of relationships,sexual behaviors, contraceptive needs,STI surveillance and prevention, andother sexual health prevention mea-sures, such as human papillomavirusimmunization.
RECOMMENDATIONS
1. Pediatricians should counsel aboutand ensure access to a broadrange of contraceptive servicesfor their adolescent patients. Thisincludes educating patients aboutall contraceptive methods that aresafe and appropriate for them anddescribing the most effective meth-ods first.
2. Pediatricians should be able toeducate adolescent patients aboutLARC methods, including the pro-gestin implant and IUDs. Given theefficacy, safety, and ease of use,LARC methods should be consid-ered first-line contraceptive choicesfor adolescents. Some pediatriciansmay choose to acquire the skills toprovide these methods to adoles-cents. Those who do not shouldidentify health care providers intheir communities to whom patientscan be referred.
3. Despite increased attention to ad-verse effects, DMPA and the con-traceptive patch are highly effectivemethods of contraception that aremuch safer than pregnancy. Pedia-
tricians should continue to makethem available to their patients.
4. Pediatricians should allow the ad-olescent to consent to contraceptivecare and to control the disclosureof this information within the limitsof state and federal laws. There area number of supports for protectingminor consent and confidentiality,including state law, federal statutes,and federal case law. Pediatricianswill need to be familiar with nationalbest practice recommendations forconfidential care and with the rele-vant minor consent laws in theirstates.
5. Pediatricians should be awarethat it is appropriate to prescribecontraceptives or refer for IUDplacement without first conductinga pelvic examination. Screeningsfor STIs, especially chlamydia, canbe performed without a pelvic ex-amination and should not bedelayed.
6. Pediatricians should encouragethe consistent and correct use ofcondoms with every act of sexualintercourse.
7. Pediatricians should have a work-ing knowledge of the differentcombined hormonal methods andregimens, because these provideexcellent cycle control both forcontraception and medical man-agement of common conditions,such as acne, dysmenorrhea, andheavy menstrual bleeding.
8. Pediatricians should rememberthat adolescents with chronic ill-ness and disabilities have similarsexual health and contraceptiveneeds to healthy adolescents whilerecognizing that medical illness maycomplicate contraceptive choices.
9. Pediatricians should regularly updatetheir adolescent patients’ sexual his-tories and provide a confidential andnonjudgmental setting in which to
address needs for contraception,STI screening, and sexual risk re-duction counseling for patientswho choose not to be abstinent.
10. Pediatricians should allow suffi-cient time with their adolescentpatients to address contraceptiveneeds using a developmentallyappropriate, patient-centered ap-proach, such as motivational inter-viewing. If necessary, arrangementsshould be made for a separate visitfor contraceptive follow-up to in-crease adherence and monitor foradverse effects and complications.
11. Pediatricians can complement theskills and resources of the pedi-atric office by being aware ofstate or federally subsidized in-surance programs and clinicsthat provide confidential and freeor low-cost reproductive healthcare services and supplies, in-cluding contraception.
LEAD AUTHORSMary A. Ott, MD, MA, FAAPGina S. Sucato, MD, MPH, FAAP
COMMITTEE ON ADOLESCENCE,2013–2014Paula K. Braverman, MD, ChairpersonWilliam P. Adelman, MD, FAAPElizabeth M. Alderman, MD, FAAP, FSHAMCora C. Breuner, MD, MPH, FAAPDavid A. Levine, MD, FAAPArik V. Marcell, MD, FAAPRebecca F. O’Brien, MD, FAAP
PAST COMMITTEE MEMBERPamela J. Murray, MD, MPH, FAAP
LIAISONSLoretta E. Gavin, PhD, MPH – Centers for DiseaseControl and PreventionMargo Lane, MD, FRCPC – Canadian PediatricSocietyRachel J. Miller, MD – American College ofObstetricians and GynecologistsBenjamin Shain, MD, PhD – American Academyof Child and Adolescent Psychiatry
STAFFKaren S. SmithJames D. Baumberger, MPP
PEDIATRICS Volume 134, Number 4, October 2014 e1251
FROM THE AMERICAN ACADEMY OF PEDIATRICS

REFERENCES
1. Martinez G, Copen CE, Abma JC. Teenagersin the United States: sexual activity, con-traceptive use, and childbearing, 2006–2010 national survey of family growth.Vital Health Stat 23. 2011; (31):1–35
2. Kost K, Henshaw S, Carlin L. US TeenagePregnancies, Births and Abortions: Na-tional and State Trends and Trendsby Race and Ethnicity. New York, NY:Guttmacher Institute; 2010
3. Finer LB, Zolna MR. Unintended pregnancyin the United States: incidence and dis-parities, 2006. Contraception. 2011;84(5):478–485
4. Ott MA, Rosenberger JG, McBride KR,Woodcox SG. How do adolescents viewhealth? Implications for state health pol-icy. J Adolesc Health. 2011;48(4):398–403
5. Jones RK, Biddlecom AE. The more thingschange…: the relative importance of theinternet as a source of contraceptive in-formation for teens. Sex Res Soc Policy.2011;8(1):27–37
6. Institute of Medicine, Committee on Pre-ventive Services for Women. Clinical Pre-ventive Services for Women: Closing theGaps. Washington, DC: National Acade-mies Press; 2011
7. Health Resources and Services Adminis-tration. Women’s Preventive Services: Re-quired Health Plan Coverage Guidelines.Rockville, MD: Health Resources andServices Administration; 2012
8. The Patient Protection and AffordableCare Act. Pub L No. 111-148 (2010). Avail-able at: www.dol.gov/ebsa/healthreform/.Accessed January 13, 2014
9. Ford C, English A, Sigman G. ConfidentialHealth Care for Adolescents: position pa-per for the society for adolescent medi-cine. J Adolesc Health. 2004;35(2):160–167.Available at: www.adolescenthealth.org/SAHM_Main/media/Advocacy/Positions/Aug-04-Confidential_Health_Care_for_Adolescents.pdf. Accessed June 22, 2014
10. American College of Obstetricians andGynecologists. Guidelines for AdolescentHealth Care. Washington, DC: AmericanCollege of Obstetricians and Gynecolo-gists; 2011
11. American Academy of Pediatrics, Com-mittee on Adolescence. Policy statement:achieving quality health services foradolescents. Pediatrics. 2008;121(6):1263–1270. Available at: http://pediatrics.aap-publications.org/content/121/6/1263.full.pdf+html. Accessed June 22, 2014
12. Center for Adolescent Health and the Law.State Minor Consent Laws: A Summary.
3rd ed. Chapel Hill, NC: Center for Ado-lescent Health and the Law; 2010
13. Guttmacher Institute. An overview of minors’consent law. State policies in briefas of June 1, 2014. Available at: www.guttmacher.org/statecenter/spibs/spib_MACS.pdf. Accessed June 20, 2014
14. English A, Ford CA. The HIPAA privacy ruleand adolescents: legal questions and clinicalchallenges. Perspect Sex Reprod Health.2004;36(2):80–86
15. Spooner SA; Council on Clinical In-formation Technology, American Academyof Pediatrics. Special requirements ofelectronic health record systems in pedi-atrics. Pediatrics. 2007;119(3):631–637 http://pediatrics.aappublications.org/content/119/3/631.full.pdf+html. Accessed June 22, 2014
16. Council on Clinical Information Technology.Health information technology and the med-ical home. Pediatrics. 2011;127(5):978–982.Available at: http://pediatrics.aappublications.org/content/127/5/978.full?sid=f3089a2a-b98c-4046-99c3-4e5386ef6e20. Accessed June22, 2014
17. Reddy DM, Fleming R, Swain C. Effect ofmandatory parental notification on ado-lescent girls’ use of sexual health careservices. JAMA. 2002;288(6):710–714
18. Zabin LS, Stark HA, Emerson MR. Reasonsfor delay in contraceptive clinic utilization.Adolescent clinic and nonclinic populationscompared. J Adolesc Health. 1991;12(3):225–232
19. Guldi M. Fertility effects of abortion andbirth control pill access for minors. De-mography. 2008;45(4):817–827
20. Zavodny M. Fertility and parental consentfor minors to receive contraceptives. AmJ Public Health. 2004;94(8):1347–1351
21. Lehrer JA, Pantell R, Tebb K, Shafer MA.Forgone health care among U.S. adoles-cents: associations between risk char-acteristics and confidentiality concern.J Adolesc Health. 2007;40(3):218–226
22. Dempsey AF, Singer DD, Clark SJ, DavisMM. Adolescent preventive health care:what do parents want? J Pediatr. 2009;155(5):689.e1–694.e1
23. Jones RK, Purcell A, Singh S, Finer LB.Adolescents’ reports of parental knowl-edge of adolescents’ use of sexual healthservices and their reactions to mandatedparental notification for prescription con-traception. JAMA. 2005;293(3):340–348
24. Hagan JF, Shaw JS, Duncan PM, eds.Bright Futures: Guidelines for Health Su-pervision of Infants, Children, and Ado-lescents. Elk Grove Village, IL: American
Academy of Pediatrics; 2008. Available at:http://brightfutures.aap.org/pdfs/Guide-lines_PDF/18-Adolescence.pdf. AccessedJune 22, 2014
25. Centers for Disease Control and Pre-vention. A Guide to Taking a Sexual History.Atlanta, GA: Centers for Disease Controland Prevention; 2005. Available at: www.cdc.gov/std/treatment/SexualHistory.pdf.Accessed June 22, 2014
26. Blum RW. Healthy youth development asa model for youth health promotion. A re-view. J Adolesc Health. 1998;22(5):368–375
27. Ott MA, Labbett RL, Gold MA. Counselingadolescents about abstinence in the officesetting. J Pediatr Adolesc Gynecol. 2007;20(1):39–44
28. American Academy of Pediatrics, Com-mittee on Adolescence. Technical report:contraception for adolescents. Pediatrics.2014; (in press)
29. Brückner H, Bearman P. After the prom-ise: the STD consequences of adolescentvirginity pledges. J Adolesc Health. 2005;36(4):271–278
30. Pinkerton SD. A relative risk-based, disease-specific definition of sexual abstinencefailure rates. Health Educ Behav. 2001;28(1):10–20
31. Committee on Adolescence. Office-basedcare for lesbian, gay, bisexual, trans-gender, and questioning youth. Pediatrics.2013;132(1):198–203. Available at: http://pediatrics.aappublications.org/content/132/1/198.full.pdf. Accessed June 22,2014
32. Hatcher RA, Trussell J, Nelson AL, Cates WJr, Kowal D, Policar MS. ContraceptiveTechnology. 20th rev ed. Valley Stream,NY: Ardent Media; 2011
33. Graesslin O, Korver T. The contraceptiveefficacy of Implanon: a review of clinicaltrials and marketing experience. Eur JContracept Reprod Health Care. 2008;13(suppl 1):4–12
34. Lakha F, Glasier AF. Continuation rates ofImplanon in the UK: data from an obser-vational study in a clinical setting. Con-traception. 2006;74(4):287–289
35. Harvey C, Seib C, Lucke J. Continuationrates and reasons for removal amongImplanon users accessing two familyplanning clinics in Queensland, Australia.Contraception. 2009;80(6):527–532
36. Committee on Adolescent Health Care Long-Acting Reversible Contraception WorkingGroup, The American College of Obstetri-cians and Gynecologists. Committee opinionno. 539: adolescents and long-acting reversible
e1252 FROM THE AMERICAN ACADEMY OF PEDIATRICS

contraception: implants and intrauterinedevices. Obstet Gynecol. 2012;120(4):983–988
37. Centers for Disease Control and Prevention.US medical eligibility criteria for contra-ceptive use, 2010. MMWR Recomm Rep.2010;59(RR-4):1–6. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5904a1.htm?s_cid=rr5904a1_e. Accessed June 22,2014
38. Gurtcheff SE, Turok DK, Stoddard G, MurphyPA, Gibson M, Jones KP. Lactogenesis afterearly postpartum use of the contraceptiveimplant: a randomized controlled trial.Obstet Gynecol. 2011;117(5):1114–1121
39. Kapp N, Curtis K, Nanda K. Progestogen-only contraceptive use among breast-feeding women: a systematic review.Contraception. 2010;82(1):17–37
40. Bayer HealthCare Pharmaceuticals. Skylapackage insert. Wayne, NJ: Bayer Health-Care Pharmaceuticals; 2013. Available at:http://labeling.bayerhealthcare.com/html/products/pi/Skyla_PI.pdf. Accessed Janu-ary 13, 2014
41. Bayer HealthCare Pharmaceuticals. Mirenapackage insert. Wayne, NJ: Bayer Health-Care Pharmaceuticals; 2013. Available at:http://labeling.bayerhealthcare.com/html/products/pi/Mirena_PI.pdf. Accessed January13, 2014
42. Teva Women’s Health Inc/Teva Pharma-ceuticals. Paragard package insert. Sell-ersville, PA: Teva Woman’s Health Inc/TevaPharmaceuticals; 2011. Available at: http://paragard.com/Pdf/ParaGard-PI.pdf. AccessedJune 22, 2014
43. Trussell J. Update on and correction tothe cost-effectiveness of contraceptives inthe United States. Contraception. 2012;85(6):611
44. Committee on Adolescence. Emergency con-traception. Pediatrics. 2012;130(6):1174–1182
45. Hubacher D, Lara-Ricalde R, Taylor DJ,Guerra-Infante F, Guzmán-Rodríguez R. Useof copper intrauterine devices and therisk of tubal infertility among nulligravidwomen. N Engl J Med. 2001;345(8):561–567
46. Hov GG, Skjeldestad FE, Hilstad T. Use ofIUD and subsequent fertility: follow-upafter participation in a randomized clini-cal trial. Contraception. 2007;75(2):88–92
47. Penney G, Brechin S, de Souza A, et al;Faculty of Family Planning and ReproductiveHealth Care Clinical Effectiveness Unit.FFPRHC guidance (January 2004). The cop-per intrauterine device as long-term con-traception. J Fam Plann Reprod Health Care.2004;30(1):29–41, quiz 42
48. Mohllajee AP, Curtis KM, Peterson HB.Does insertion and use of an intrauterine
device increase the risk of pelvic in-flammatory disease among women withsexually transmitted infection? A system-atic review. Contraception. 2006;73(2):145–153
49. Farley TM, Rosenberg MJ, Rowe PJ, ChenJH, Meirik O. Intrauterine devices andpelvic inflammatory disease: an internationalperspective. Lancet. 1992;339(8796):785–788
50. American College of Obstetricians andGynecologists. ACOG practice bulletin no.121: Long-acting reversible contraception:implants and intrauterine devices. ObstetGynecol. 2011;118(1):184–196
51. Grimes DA. Intrauterine device andupper-genital-tract infection. Lancet. 2000;356(9234):1013–1019
52. Centers for Disease Control and Pre-vention. US selected practice recom-mendations for contraceptive use, 2013:adapted from the World Health Organiza-tion Selected Practice Recommendationsfor Contraceptive Use, 2nd Edition. MMWRRecomm Rep. 2013;62(RR-5):1–60
53. Grimes DA, Lopez LM, Schulz KF, Van VlietHA, Stanwood NL. Immediate post-partuminsertion of intrauterine devices. CochraneDatabase Syst Rev. 2010; (5):CD003036
54. Kapp N, Curtis KM. Intrauterine deviceinsertion during the postpartum period:a systematic review. Contraception. 2009;80(4):327–336
55. American College of Obstetricians andGynecologists. Increasing use of contra-ceptive implants and intrauterine devicesto reduce unintended pregnancy. ACOGcommittee opinion no. 450. Obstet Gynecol.2009;114(6):1434–1438
56. Chen BA, Reeves MF, Hayes JL, HohmannHL, Perriera LK, Creinin MD. Postplacentalor delayed insertion of the levonorgestrelintrauterine device after vaginal delivery:a randomized controlled trial. Obstet Gynecol.2010;116(5):1079–1087
57. Ogburn JA, Espey E, Stonehocker J. Barriersto intrauterine device insertion in post-partum women. Contraception. 2005;72(6):426–429
58. Deans EI, Grimes DA. Intrauterine devicesfor adolescents: a systematic review.Contraception. 2009;79(6):418–423
59. Thonneau P, Almont T, de La RochebrochardE, Maria B. Risk factors for IUD failure:results of a large multicentre case–controlstudy. Hum Reprod. 2006;21(10):2612–2616
60. Suhonen S, Haukkamaa M, Jakobsson T,Rauramo I. Clinical performance of alevonorgestrel-releasing intrauterinesystem and oral contraceptives in youngnulliparous women: a comparative study.Contraception. 2004;69(5):407–412
61. Bayer LL, Jensen JT, Li H, Nichols MD,Bednarek PH. Adolescent experience withintrauterine device insertion and use:a retrospective cohort study. Contracep-tion. 2012;86(5):443–451
62. Alton TM, Brock GN, Yang D, Wilking DA,Hertweck SP, Loveless MB. Retrospectivereview of intrauterine device in adoles-cent and young women. J Pediatr AdolescGynecol. 2012;25(3):195–200
63. Godfrey EM, Memmel LM, Neustadt A, et al.Intrauterine contraception for adoles-cents aged 14–18 years: a multicenterrandomized pilot study of levonorgestrel-releasing intrauterine system comparedto the Copper T 380A. Contraception. 2010;81(2):123–127
64. Paterson H, Ashton J, Harrison-WoolrychM. A nationwide cohort study of the use ofthe levonorgestrel intrauterine device inNew Zealand adolescents. Contraception.2009;79(6):433–438
65. Pillai M, O’Brien K, Hill E. The levonorges-trel intrauterine system (Mirena) for thetreatment of menstrual problems in ado-lescents with medical disorders, or physi-cal or learning disabilities. BJOG. 2010;117(2):216–221
66. Toma A, Jamieson MA. Revisiting the in-trauterine contraceptive device in ado-lescents. J Pediatr Adolesc Gynecol. 2006;19(4):291–296
67. Lara-Torre E, Spotswood L, Correia N,Weiss PM. Intrauterine contraception inadolescents and young women: a de-scriptive study of use, side effects, andcompliance. J Pediatr Adolesc Gynecol.2011;24(1):39–41
68. Kaunitz AM, Darney PD, Ross D, Wolter KD,Speroff L. Subcutaneous DMPA vs. in-tramuscular DMPA: a 2-year randomizedstudy of contraceptive efficacy and bonemineral density. Contraception. 2009;80(1):7–17
69. Kaunitz AM. Depot medroxyprogesteroneacetate contraception and the risk ofbreast and gynecologic cancer. J ReprodMed. 1996;41(5 suppl):419–427
70. Herzog AG. Progesterone therapy inwomen with epilepsy: a 3-year follow-up.Neurology. 1999;52(9):1917–1918
71. de Abood M, de Castillo Z, Guerrero F,Espino M, Austin KL. Effect of Depo-Provera or Microgynon on the painfulcrises of sickle cell anemia patients.Contraception. 1997;56(5):313–316
72. Manchikanti A, Grimes DA, Lopez LM,Schulz KF. Steroid hormones for contra-ception in women with sickle cell disease.Cochrane Database Syst Rev. 2007; (2):CD006261
PEDIATRICS Volume 134, Number 4, October 2014 e1253
FROM THE AMERICAN ACADEMY OF PEDIATRICS

73. Hubacher D, Lopez L, Steiner MJ, DorflingerL. Menstrual pattern changes from levo-norgestrel subdermal implants andDMPA: systematic review and evidence-based comparisons. Contraception. 2009;80(2):113–118
74. Arias RD, Jain JK, Brucker C, Ross D, RayA. Changes in bleeding patterns with de-pot medroxyprogesterone acetate sub-cutaneous injection 104 mg. Contraception.2006;74(3):234–238
75. Hubacher D, Goco N, Gonzalez B, Taylor D.Factors affecting continuation rates ofDMPA. Contraception. 1999;60(6):345–351
76. Canto De Cetina TE, Canto P, Ordoñez LunaM. Effect of counseling to improve com-pliance in Mexican women receiving depot-medroxyprogesterone acetate. Contraception.2001;63(3):143–146
77. Bonny AE, Secic M, Cromer B. Early weightgain related to later weight gain in ado-lescents on depot medroxyprogesteroneacetate. Obstet Gynecol. 2011;117(4):793–797
78. Le YC, Rahman M, Berenson AB. Earlyweight gain predicting later weight gainamong depot medroxyprogesterone ace-tate users. Obstet Gynecol. 2009;114(2 pt1):279–284
79. Risser WL, Gefter LR, Barratt MS, RisserJM. Weight change in adolescents whoused hormonal contraception. J AdolescHealth. 1999;24(6):433–436
80. Bonny AE, Ziegler J, Harvey R, DebanneSM, Secic M, Cromer BA. Weight gain inobese and nonobese adolescent girls ini-tiating depot medroxyprogesterone, oralcontraceptive pills, or no hormonal con-traceptive method. Arch Pediatr AdolescMed. 2006;160(1):40–45
81. Cromer BA, Blair JM, Mahan JD, Zibners L,Naumovski Z. A prospective comparison ofbone density in adolescent girls receivingdepot medroxyprogesterone acetate (Depo-Provera), levonorgestrel (Norplant), or oralcontraceptives. J Pediatr. 1996;129(5):671–676
82. Lara-Torre E, Edwards CP, Perlman S,Hertweck SP. Bone mineral densityin adolescent females using depotmedroxyprogesterone acetate. J PediatrAdolesc Gynecol. 2004;17(1):17–21
83. Cromer BA, Stager M, Bonny A, et al. Depotmedroxyprogesterone acetate, oral con-traceptives and bone mineral density ina cohort of adolescent girls. J AdolescHealth. 2004;35(6):434–441
84. Pfizer. DepoProvera 150 mg and DepoSubQ Provera 104 package inserts. Cam-bridge, MA: Pfizer; 2005
85. Scholes D, LaCroix AZ, Ichikawa LE, BarlowWE, Ott SM. Change in bone mineral den-
sity among adolescent women using anddiscontinuing depot medroxyprogesteroneacetate contraception. Arch Pediatr Ado-lesc Med. 2005;159(2):139–144
86. Harel Z, Johnson CC, Gold MA, et al. Re-covery of bone mineral density in ado-lescents following the use of depotmedroxyprogesterone acetate contracep-tive injections. Contraception. 2010;81(4):281–291
87. Berenson AB, Rahman M, Breitkopf CR, BiLX. Effects of depot medroxyprogesteroneacetate and 20-microgram oral contra-ceptives on bone mineral density. ObstetGynecol. 2008;112(4):788–799
88. US Pharmaceuticals/Pfizer Inc. Letter tohealth care professionals. November 18,2004. Available at: www.fda.gov/downloads/Safety/MedWatch/SafetyInformation/Safe-tyAlertsforHumanMedicalProducts/UCM1-66395.pdf. Accessed January 13, 2014
89. American College of Obstetricians andGynecologists Committee on GynecologicPractice. ACOG committee opinion no. 415:depot medroxyprogesterone acetate andbone effects. Obstet Gynecol. 2008;112(3):727–730
90. Institute of Medicine. Dietary referenceintakes for calcium and vitamin D. Wash-ington, DC: National Academies Press; 2010.Available at: www.iom.edu/Reports/2010/Dietary-Reference-Intakes-for-calcium-and-vitamin-D.aspx
91. Braverman PK, Breech L; Committee onAdolescence. American Academy of Pedi-atrics. Clinical report: gynecologic exam-ination for adolescents in the pediatricoffice setting. Pediatrics. 2010;126(3):583–590.Available at: http://pediatrics.aappublications.org/content/126/3/583.full.pdf+html. AccessedJune 22, 2014
92. Trenor CC III, Chung RJ, Michelson AD,et al. Hormonal contraception and throm-botic risk: a multidisciplinary approach.Pediatrics. 2011;127(2):347–357
93. Vandenbroucke JP, Rosing J, BloemenkampKW, et al. Oral contraceptives and the riskof venous thrombosis. N Engl J Med. 2001;344(20):1527–1535
94. Walker ID. Venous and arterial thrombosisduring pregnancy: epidemiology. Semin VascMed. 2003;3(1):25–32
95. Heit JA, Kobbervig CE, James AH, PettersonTM, Bailey KR, Melton LJ III. Trends in theincidence of venous thromboembolismduring pregnancy or postpartum: a 30-yearpopulation-based study. Ann Intern Med.2005;143(10):697–706
96. Dickey R. Managing Contraceptive PillPatients. Fort Collins, CO: EMIS Inc MedicalPublishers; 2010
97. Gaffield ME, Culwell KR, Lee CR. The use ofhormonal contraception among womentaking anticonvulsant therapy. Contra-ception. 2011;83(1):16–29
98. Mosher WD, Jones J. Use of contraceptionin the United States: 1982–2008. VitalHealth Stat 23. 2010; (29):1–44
99. Faculty of Sexual and ReproductiveHealthcare, Royal College of Obstetriciansand Gynaecologists. Faculty of Sexual andReproductive Healthcare Clinical Guid-ance: Combined Hormonal Contraception.London, UK: Faculty of Sexual and Re-productive Healthcare, Royal College ofObstetricians and Gynaecologists; October2011. Updated August 2012. Available at:www.fsrh.org/pdfs/CEUGuidanceCombined-HormonalContraception.pdf. Accessed January13, 2014
100. Mansour D. Revision of the “missed pill”rules. J Fam Plann Reprod Health Care.2011;37(3):128–131
101. Sucato GS, Gold MA. Extended cycling oforal contraceptive pills for adolescents.J Pediatr Adolesc Gynecol. 2002;15(5):325–327
102. Sucato GS, Gerschultz KL. Extended cyclehormonal contraception in adolescents.Curr Opin Obstet Gynecol. 2005;17(5):461–465
103. ACOG Committee on Practice Bulletins–Gynecology. ACOG practice bulletin no. 73:Use of hormonal contraception in womenwith coexisting medical conditions. ObstetGynecol. 2006;107(6):1453–1472
104. Vessey M, Painter R. Oral contraceptiveuse and cancer. Findings in a large cohortstudy, 1968–2004. Br J Cancer. 2006;95(3):385–389
105. Roumen FJ, Apter D, Mulders TM, DiebenTO. Efficacy, tolerability and acceptabilityof a novel contraceptive vaginal ring re-leasing etonogestrel and ethinyl oestr-adiol. Hum Reprod. 2001;16(3):469–475
106. Dieben TO, Roumen FJ, Apter D. Efficacy,cycle control, and user acceptability ofa novel combined contraceptive vaginalring. Obstet Gynecol. 2002;100(3):585–593
107. Edwardson J, Jamshidi R. The contracep-tive vaginal ring. Semin Reprod Med. 2010;28(2):133–139
108. Timmer CJ, Mulders TM. Pharmacokinet-ics of etonogestrel and ethinylestradiolreleased from a combined contraceptivevaginal ring. Clin Pharmacokinet. 2000;39(3):233–242
109. Guida M, Di Spiezio Sardo A, Bramante S,et al. Effects of two types of hormonalcontraception—oral versus intravaginal—onthe sexual life of women and their partners.Hum Reprod. 2005;20(4):1100–1106
e1254 FROM THE AMERICAN ACADEMY OF PEDIATRICS

110. Veres S, Miller L, Burington B. A compar-ison between the vaginal ring and oralcontraceptives. Obstet Gynecol. 2004;104(3):555–563
111. van den Heuvel MW, van Bragt AJ, AlnabawyAK, Kaptein MC. Comparison of ethinylestradiolpharmacokinetics in three hormonal contra-ceptive formulations: the vaginal ring, thetransdermal patch and an oral contraceptive.Contraception. 2005;72(3):168–174
112. Cole JA, Norman H, Doherty M, Walker AM.Venous thromboembolism, myocardial in-farction, and stroke among transdermalcontraceptive system users. Obstet Gynecol.2007;109(2 pt 1):339–346
113. Dore DD, Norman H, Loughlin J, Seeger JD.Extended case–control study results onthromboembolic outcomes among trans-dermal contraceptive users. Contracep-tion. 2010;81(5):408–413
114. Harel Z, Riggs S, Vaz R, Flanagan P, Dunn K,Harel D. Adolescents’ experience with thecombined estrogen and progestin trans-dermal contraceptive method Ortho Evra.J Pediatr Adolesc Gynecol. 2005;18(2):85–90
115. Rubinstein ML, Halpern-Felsher BL, IrwinCE Jr. An evaluation of the use of thetransdermal contraceptive patch in ado-lescents. J Adolesc Health. 2004;34(5):395–401
116. Stricker T, Sennhauser FH. Allergic contactdermatitis due to transdermal contra-ception patch. J Pediatr. 2006;148(6):845
117. Audet MC, Moreau M, Koltun WD, et al;ORTHO EVRA/EVRA 004 Study Group. Eval-uation of contraceptive efficacy and cyclecontrol of a transdermal contraceptivepatch vs an oral contraceptive: a random-ized controlled trial. JAMA. 2001;285(18):2347–2354
118. Zieman M, Guillebaud J, Weisberg E,Shangold GA, Fisher AC, Creasy GW. Con-traceptive efficacy and cycle control withthe Ortho Evra/Evra transdermal system:the analysis of pooled data. Fertil Steril.2002;77(2 Suppl 2):S13–S18
119. Holmes KK, Levine R, Weaver M. Effective-ness of condoms in preventing sexuallytransmitted infections. Bull World HealthOrgan. 2004;82(6):454–461
120. Gallo MF, Steiner MJ, Warner L, et al. Self-reported condom use is associated withreduced risk of chlamydia, gonorrhea,and trichomoniasis. Sex Transm Dis. 2007;34(10):829–833
121. Warner L, Macaluso M, Newman D, et al.Condom effectiveness for prevention of Ctrachomatis infection. Sex Transm Infect.2006;82(3):265
122. Paz-Bailey G, Koumans EH, Sternberg M,et al. The effect of correct and consistent
condom use on chlamydial and gonococ-cal infection among urban adolescents.Arch Pediatr Adolesc Med. 2005;159(6):536–542
123. Niccolai LM, Rowhani-Rahbar A, Jenkins H,Green S, Dunne DW. Condom effectivenessfor prevention of Chlamydia trachomatisinfection. Sex Transm Infect. 2005;81(4):323–325
124. Weller S, Davis K. Condom effectiveness inreducing heterosexual HIV transmission.Cochrane Database Syst Rev. 2002; (1):CD003255
125. Martin ET, Krantz E, Gottlieb SL, et al. Apooled analysis of the effect of condomsin preventing HSV-2 acquisition. Arch In-tern Med. 2009;169(13):1233–1240
126. Stanaway JD, Wald A, Martin ET, GottliebSL, Magaret AS. Case-crossover analysis ofcondom use and herpes simplex virustype 2 acquisition. Sex Transm Dis. 2012;39(5):388–393
127. Winer RL, Hughes JP, Feng Q, et al.Condom use and the risk of genital hu-man papillomavirus infection in youngwomen. N Engl J Med. 2006;354(25):2645–2654
128. Shew ML, Fortenberry JD, Tu W, et al. As-sociation of condom use, sexual behav-iors, and sexually transmitted infectionswith the duration of genital human pap-illomavirus infection among adolescentwomen. Arch Pediatr Adolesc Med. 2006;160(2):151–156
129. Koss CA, Dunne EF, Warner L. A systematicreview of epidemiologic studies assessingcondom use and risk of syphilis. SexTransm Dis. 2009;36(7):401–405
130. Matson PA, Adler NE, Millstein SG,Tschann JM, Ellen JM. Developmentalchanges in condom use among urbanadolescent females: influence of part-ner context. J Adolesc Health. 2011;48(4):386–390
131. Bearinger LH, Sieving RE, Duke NN,McMorris BJ, Stoddard S, Pettingell SL.Adolescent condom use consistencyover time: global versus partner-specific measures. Nurs Res. 2011;60(3suppl):S68–S78
132. Kenyon DB, Sieving RE, Jerstad SJ, PettingellSL, Skay CL. Individual, interpersonal, andrelationship factors predicting hormonaland condom use consistency among ado-lescent girls. J Pediatr Health Care. 2010;24(4):241–249
133. American Academy of Pediatrics, Com-mittee on Adolescence. Policy statement:condom use by adolescents. Pediatrics.2013;132(5):973–981
134. Cheng L, Gülmezoglu AM, Piaggio G,Ezcurra E, Van Look PF. Interventions foremergency contraception. Cochrane Da-tabase Syst Rev. 2008; (2):CD001324
135. Fine P, Mathé H, Ginde S, Cullins V, MorfesisJ, Gainer E. Ulipristal acetate taken 48–120hours after intercourse for emergencycontraception. Obstet Gynecol. 2010;115(2 Pt1):257–263
136. Glasier AF, Cameron ST, Fine PM, et al.Ulipristal acetate versus levonorgestrelfor emergency contraception: a randomisednon-inferiority trial and meta-analysis. Lan-cet. 2010;375(9714):555–562
137. Rockoff JD. FDA reviewing efficacy ofPlan B contraception in women over 165pounds. The Wall Street Journal. Novem-ber 25, 2013. Available at: http://online.wsj.com/news/articles/SB1000142405270-2304011304579220533719517944. AccessedJanuary 13, 2014
138. Glasier A, Cameron ST, Blithe D, et al. Canwe identify women at risk of pregnancydespite using emergency contraception?Data from randomized trials of ulipristalacetate and levonorgestrel. Contracep-tion. 2011;84(4):363–367
139. Cleland K, Zhu H, Goldstuck N, Cheng L,Trussell J. The efficacy of intrauterinedevices for emergency contraception:a systematic review of 35 years of ex-perience. Hum Reprod. 2012;27(7):1994–2000
140. von Hertzen H, Piaggio G, Ding J, et al;WHO Research Group on Post-ovulatoryMethods of Fertility Regulation. Low dosemifepristone and two regimens of levo-norgestrel for emergency contraception:a WHO multicentre randomised trial. Lan-cet. 2002;360(9348):1803–1810
141. Gallo MF, Grimes DA, Schulz KF, HelmerhorstFM. Combination estrogen–progestin contra-ceptives and body weight: systematic reviewof randomized controlled trials. Obstet Gynecol.2004;103(2):359–373
142. US Food and Drug Administration. FDAapproves Plan B One-Step emergencycontraceptive for use without a pre-scription for all women of child-bearingpotential. June 20, 2013. Available at:www.fda.gov/NewsEvents/Newsroom/Press-Announcements/ucm358082.htm. AccessedJanuary 13, 2014
143. Ellertson C, Ambardekar S, Hedley A,Coyaji K, Trussell J, Blanchard K. Emer-gency contraception: randomized com-parison of advance provision andinformation only. Obstet Gynecol. 2001;98(4):570–575
144. Meyer JL, Gold MA, Haggerty CL. Advanceprovision of emergency contraception
PEDIATRICS Volume 134, Number 4, October 2014 e1255
FROM THE AMERICAN ACADEMY OF PEDIATRICS

among adolescent and young adultwomen: a systematic review of literature.J Pediatr Adolesc Gynecol. 2011;24(1):2–9
145. Bethell CD, Read D, Blumberg SJ, NewacheckPW. What is the prevalence of children withspecial health care needs? Toward an un-derstanding of variations in findings andmethods across three national surveys.Matern Child Health J. 2008;12(1):1–14
146. McRee AL, Haydon AA, Halpern CT. Re-productive health of young adults withphysical disabilities in the U.S. Prev Med.2010;51(6):502–504
147. Surís JC, Resnick MD, Cassuto N, Blum RW.Sexual behavior of adolescents with chronicdisease and disability. J Adolesc Health.1996;19(2):124–131
148. Akers AY, Lynch CP, Gold MA, et al. Exploringthe relationship among weight, race, andsexual behaviors among girls. Pediatrics.2009;124(5). Available at: www.pediatrics.org/cgi/content/full/124/5/e913
149. Mond J, van den Berg P, Boutelle K, HannanP, Neumark-Sztainer D. Obesity, body dissat-isfaction, and emotional well-being in earlyand late adolescence: findings from theproject EAT study. J Adolesc Health. 2011;48(4):373–378
150. Xu H, Wade JA, Peipert JF, Zhao Q, MaddenT, Secura GM. Contraceptive failure ratesof etonogestrel subdermal implants in over-weight and obese women. Obstet Gynecol.2012;120(1):21–26
151. Hormonal contraceptives for contraceptionin overweight or obese women. ObstetGynecol. 2010;116(5):1206–1207
152. Brunner Huber LR, Toth JL. Obesity and oralcontraceptive failure: findings from the2002 National Survey of Family Growth. AmJ Epidemiol. 2007;166(11):1306–1311
153. American College of Obstetricians andGynecologists. ACOG practice bulletin no.105: bariatric surgery and pregnancy. ObstetGynecol. 2009;113(6):1306–1311
154. Hillman JB, Miller RJ, Inge TH. Menstrualconcerns and intrauterine contraceptionamong adolescent bariatric surgerypatients. J Womens Health (Larchmt).2011;20(4):533–538
e1256 FROM THE AMERICAN ACADEMY OF PEDIATRICS
POLICY STATEMENT
Providing Care for Immigrant, Migrant, and BorderChildren
abstractThis policy statement, which recognizes the large changes in immi-grant status since publication of the 2005 statement “Providing Carefor Immigrant, Homeless, and Migrant Children,” focuses on strate-gies to support the health of immigrant children, infants, adolescents,and young adults. Homeless children will be addressed in a forthcom-ing separate statement (“Providing Care for Children and AdolescentsFacing Homelessness and Housing Insecurity”). While recognizing thediversity across and within immigrant, migrant, and border popula-tions, this statement provides a basic framework for serving andadvocating for all immigrant children, with a particular focus onlow-income and vulnerable populations. Recommendations includeactions needed within and outside the health care system, includingexpansion of access to high-quality medical homes with culturally andlinguistically effective care as well as education and literacy pro-grams. The statement recognizes the unique and special role thatpediatricians can play in the lives of immigrant children and families.Recommendations for policies that support immigrant child healthare included. Pediatrics 2013;131:e2028–e2034
INTRODUCTION
Many children in immigrant communities face multiple barriers toaccessing comprehensive, affordable, and culturally and linguisticallyeffective health care services. Some of these barriers include poverty,fear and stigma, high mobility, limited English proficiency, little in-formation or misunderstandings about how the US health care systemworks, and lack of insurance and/or access to care. Many children ofimmigrant families belong to racial and ethnic minority groups thatface health status disparities resulting from complex determinantsthat are exacerbated by children’s living circumstances. Inadequateavailability of basic necessities, such as housing, and lack of in-formation regarding previous medical care are among the persistentchallenges faced by these vulnerable families. For some, the fear ofviolence or harassment because of their immigrant status com-pounds their already fragile living conditions. For many within thispopulation, care can be episodic, fragmented, and oriented to care ofacute conditions.1 Although many children in these circumstancesface similar challenges, there are some differences of experiencesamong migrant and border immigrant subgroups (see Fig 1).
COUNCIL ON COMMUNITY PEDIATRICS
KEY WORDSimmigrant, migrant, border, underserved communities
ABBREVIATIONSCHIP—Children’s Health Insurance Program
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The recommendations in this statement do not indicate anexclusive course of treatment or serve as a standard of medicalcare. Variations, taking into account individual circumstances,may be appropriate.
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1099
doi:10.1542/peds.2013-1099
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
e2028 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the ChildHealth Care System and/or Improve the Health of all Children
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
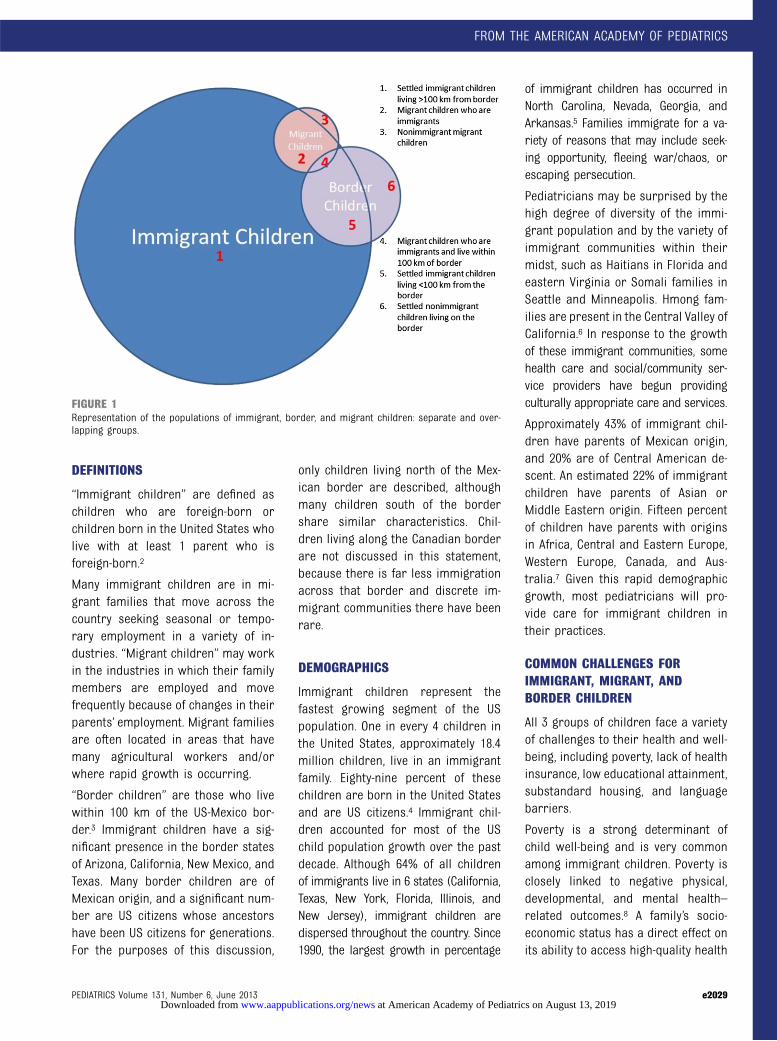
DEFINITIONS
“Immigrant children” are defined aschildren who are foreign-born orchildren born in the United States wholive with at least 1 parent who isforeign-born.2
Many immigrant children are in mi-grant families that move across thecountry seeking seasonal or tempo-rary employment in a variety of in-dustries. “Migrant children” may workin the industries in which their familymembers are employed and movefrequently because of changes in theirparents’ employment. Migrant familiesare often located in areas that havemany agricultural workers and/orwhere rapid growth is occurring.
“Border children” are those who livewithin 100 km of the US-Mexico bor-der.3 Immigrant children have a sig-nificant presence in the border statesof Arizona, California, New Mexico, andTexas. Many border children are ofMexican origin, and a significant num-ber are US citizens whose ancestorshave been US citizens for generations.For the purposes of this discussion,
only children living north of the Mex-ican border are described, althoughmany children south of the bordershare similar characteristics. Chil-dren living along the Canadian borderare not discussed in this statement,because there is far less immigrationacross that border and discrete im-migrant communities there have beenrare.
DEMOGRAPHICS
Immigrant children represent thefastest growing segment of the USpopulation. One in every 4 children inthe United States, approximately 18.4million children, live in an immigrantfamily. Eighty-nine percent of thesechildren are born in the United Statesand are US citizens.4 Immigrant chil-dren accounted for most of the USchild population growth over the pastdecade. Although 64% of all childrenof immigrants live in 6 states (California,Texas, New York, Florida, Illinois, andNew Jersey), immigrant children aredispersed throughout the country. Since1990, the largest growth in percentage
of immigrant children has occurred inNorth Carolina, Nevada, Georgia, andArkansas.5 Families immigrate for a va-riety of reasons that may include seek-ing opportunity, fleeing war/chaos, orescaping persecution.
Pediatricians may be surprised by thehigh degree of diversity of the immi-grant population and by the variety ofimmigrant communities within theirmidst, such as Haitians in Florida andeastern Virginia or Somali families inSeattle and Minneapolis. Hmong fam-ilies are present in the Central Valley ofCalifornia.6 In response to the growthof these immigrant communities, somehealth care and social/community ser-vice providers have begun providingculturally appropriate care and services.
Approximately 43% of immigrant chil-dren have parents of Mexican origin,and 20% are of Central American de-scent. An estimated 22% of immigrantchildren have parents of Asian orMiddle Eastern origin. Fifteen percentof children have parents with originsin Africa, Central and Eastern Europe,Western Europe, Canada, and Aus-tralia.7 Given this rapid demographicgrowth, most pediatricians will pro-vide care for immigrant children intheir practices.
COMMON CHALLENGES FORIMMIGRANT, MIGRANT, ANDBORDER CHILDREN
All 3 groups of children face a varietyof challenges to their health and well-being, including poverty, lack of healthinsurance, low educational attainment,substandard housing, and languagebarriers.
Poverty is a strong determinant ofchild well-being and is very commonamong immigrant children. Poverty isclosely linked to negative physical,developmental, and mental health–related outcomes.8 A family’s socio-economic status has a direct effect onits ability to access high-quality health
FIGURE 1Representation of the populations of immigrant, border, and migrant children: separate and over-lapping groups.
PEDIATRICS Volume 131, Number 6, June 2013 e2029
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

care services and to achieve goodhealth, social, and emotional out-comes. In 2010, 30% of children inimmigrant families lived below thefederal poverty level, compared with19% of children with US-born pa-rents.4 This is despite the fact thatimmigrant children are more likely tolive in 2-parent families and haveparents who work and work morehours compared with parents of US-born children.9 Immigrant childrentend to live in larger families, with19% having 4 or more siblings, com-pared with 14% of US-born families.10
Housing is often substandard and/orovercrowded for these families.
Lack of health care coverage is morecommon among children in each ofthese groups than for nonimmigrantchildren. Children of immigrants arenearly twice as likely to be uninsured(15%) as are children of nonimmigrantfamilies (8%).4 Many of the immigrantchildren who are uninsured are eligi-ble for Medicaid or the Children’sHealth Insurance Program (CHIP) butare not enrolled. Many immigrant pa-rents fear that accessing services fortheir eligible children will lead themto be considered a “public charge” (aperson dependent on the governmentfor the expenses of living11) and worryabout how that may negatively affecttheir immigration status and pros-pects. They may also fear that agenciesoffering assistance will share infor-mation with immigration enforcementagencies. Other families may not beaware of their children’s eligibility forcoverage. These same reasons mayaffect parents’ ability and willingnessto access other programs and benefitsthat their children may be eligible for,such as the Special Supplemental Nu-trition Program for Women, Infants,and Children; Supplemental NutritionAssistance Program; the Temporary As-sistance for Needy Families program;and Supplemental Security Income.
Current federal law allows states toapply waiting periods for up to 5years for legal permanent residentsto become eligible for Medicaid cover-age. Medicaid also excludes undocu-mented children from all but emergencyhealth care. Although states may chooseto cover children sooner, waiting peri-ods can exacerbate the lack of healthinsurance coverage for immigrant chil-dren. The Affordable Care Act of 2010(Pub L No. 111-148) also restricts theaccess to health insurance exchangesof children and adults who are un-documented immigrants.12
Language and communication barriersmay impede medical care for manychildren in each of these 3 groups.Although many immigrant childrenspeak English, their parents may not,creating a barrier that can preventfamilies from accessing health servicesand/or causing inadequate communi-cation with health care providers.Without access to qualified medicalinterpreters in health care settings,language barriers can place English-speaking children in the difficult po-sition of interpreting between healthcare providers and their family mem-bers. Use of children and other familymembers as untrained interpretersshould be avoided. These challengescan result in major barriers to ac-cessing health care and decreasedsatisfaction with services received.Providing care to families with limitedEnglish proficiency without appropri-ate medical interpretation services canultimately lead to a higher incidence ofmedical errors when delivering care.13
Educational levels and health literacyare often lower among parents ofimmigrant, border, and migrant fami-lies than among native-born US fami-lies. Thirty-one percent of immigrantchildren have a mother without a highschool education; the proportion offathers without a high school educa-tion is similar.4 It is important to note
that the level of maternal education isan important determinant of childhealth. Lower education levels areassociated with lower health literacy.Low health literacy creates a barrierfor patients in understanding medicalinformation and is associated withpoor health outcomes.
Health Status and HealthDisparities
Although immigrant children may bevulnerable to many risk factors forpoorer health outcomes, some groupsof immigrant children enjoy a healthierinfancy than expected. For example,Latino families have a relatively lowincidence of low birth weight, pretermbirth, and infant mortality comparedwith children of US-born parents.4
This phenomenon has been called the“healthy immigrant phenomenon.”9
Immigrant mothers are more likely tobreastfeed their infants than mothersborn in the United States.14 Immigrantchildren also seem to benefit fromsome additional protective factors,such as growing up in 2-parent orextended families,9 as well as closeidentification with the cultural andspiritual practices of their family andcommunity. In addition, as they growup, immigrant children may also dis-play relatively better adjustment andbehavior in school compared withnonimmigrant peers. This phenome-non has been shown to fade with in-creased length of stay in the UnitedStates and is, therefore, an infrequentprotective factor for health outcomes.
On the other hand, the health of im-migrant children as a group is, in somerespects, worse than US-born children.For example, they are less likely to beperceived by their parents to be inexcellent/good health and are lesslikely to have a usual source of medicalcare and to obtain specialty care whenneeded.15 They also have less accessto dental care, despite the fact that
e2030 FROM THE AMERICAN ACADEMY OF PEDIATRICS at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

they have a higher prevalence of den-tal caries.16 The Affordable Care Actexcluded undocumented immigrantsfrom health care coverage madeavailable through the Act, leaving thatgroup of adults and children as thelargest group who still will not havehealth insurance after the changes of2014.12
Immigrant children who are foreign-born may not have been screened atbirth for congenital syphilis, hemo-globinopathies, hearing deficits, andinborn errors of metabolism. In com-parison with US-born children, theyalso have lower immunization rates,especially for vaccines that are notroutinely administered in their coun-tries of origin. Some children may lackimmunization records. Foreign-bornimmigrant children have a higher in-cidence or prevalence of some infec-tious diseases, such as tuberculosis,hepatitis A, amebiasis, and parasito-sis.17 Immigrant children with asthmaare less likely to be prescribed the re-commended preventive medications.18
Immigrant families may be uniquelyvulnerable to mental health problemsand experience high levels of stress,depression, grief, and traumatic eventscompared with nonimmigrant fami-lies.19 Additionally, many experiencethe stress of family separation, inwhich some of the siblings or, in somecases, 1 or both of the parents do notreside in this country with them.
Development, Early Education, andSchool Success
Many immigrant, migrant, and borderchildren also experience educationaldisparities compared with US-bornchildren. As noted, immigrant childrenmay enjoy a healthy start as infants butmay experience developmental stag-nation as toddlers compared with non-immigrant children.20
In general, children who grow up inbilingual homes should attain major
language developmental milestones atthe normally expected times. At thesame time, children raised in homeswith impoverished language have agreater chance of being delayed inlanguage acquisition, whether theirfamilies are monolingual or bilingual.When language delays are suspectedin children growing up in limitedEnglish proficiency households, theypresent complex evaluation and inter-vention issues. When in doubt abouta suspected language delay in a bi-lingual child, timely referral to aknowledgeable, bilingual speech andlanguage pathologist is ideal.
Many immigrant children have lessaccess to quality early educationprograms and are less likely to beenrolled in preschool programs, suchas Head Start.4 Once enrolled inschool, cultural and linguistic barriersbetween parents and schools can leadto decreased family interaction andinvolvement. As they advance in theirschooling, children in immigrantfamilies are less likely to graduatefrom high school than are their non-immigrant peers.4
Fear and Discrimination
Immigrant children and families mayface discrimination and be fearful ofattitudes and behaviors of the peoplethey interact with outside their com-munities, including health care pro-viders, which can reduce access tohealth care and lead to negative childhealth outcomes. Families may faceanti-immigrant sentiment. Fear anddiscrimination can exacerbate a feel-ing of isolation and contribute tomental health problems, such as childand family depression, leaving thesepopulations vulnerable.
Family Separation
Immigrant children may have 1 ormore undocumented family members.An undocumented immigrant lacks the
proper records and identification tolive in the United States.21 Immigrationenforcement and related policies canlead to the sudden removal of an un-documented parent or other keyfamily member without notice orpreparation. Children whose parentsare taken into custody and/or depor-ted have been shown to experiencemental and emotional health prob-lems, including sleeping and eatingdisturbances, anxiety, depression, poorschool performance, and other typesof distress. Forced separations be-cause of immigration enforcement canalso result in the loss of family incomeand have been shown to result infamily housing and food instability.22
This can negatively affect a child’ssafety, health, and development.
FACTORS SPECIFIC TO MIGRANTCHILDREN
A large number of migrant childrenare also immigrants. For that reason,virtually all of the points made earlierabout immigrant children may alsoapply to those who are migrants. Be-cause of their migration patterns,migrant children are even more likelyto lack medical coverage and a medi-cal home than other immigrant chil-dren. They are also more likely to besocially, culturally, and linguisticallyisolated because of their mobile life-style.
Many migrant children face a panoplyof health problems related to theirliving and working conditions, includ-ing workplace injuries, substandardhousing, and unreliable transporta-tion.23 These factors can contribute tohigher rates of respiratory tract andear infections, bacterial and viral gas-troenteritis, tuberculosis, nutritionaldeficiencies, intestinal parasites, skininfections, dental problems, lead andpesticide exposure, and undiagnosedcongenital anomalies.24 Additionally,at times, migrant adolescents travel
PEDIATRICS Volume 131, Number 6, June 2013 e2031
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

on their own from 1 job site to an-other, putting them at increased riskof many health-related problems.
FACTORS SPECIFIC TO BORDERCHILDREN
Immigrant children living at the US-Mexico border share almost all ofthe characteristics of other immigrantchildren but may experience additionalchallenges. Children who have crossedthe border to enter the United Statesmay have experienced trauma in theform of threat of death, abuse, andexploitation that leave serious psy-chological scars. Once in the UnitedStates, these children may experiencean enhanced fear of a family member’sdeportation, imprisonment, or abusebecause of documentation status.Children and families who have re-cently crossed the border can alsoexperience difficulty adapting to thenew cultural environment of theUnited States and experience stressfrom the absence of an extendedfamily (including a parent or head ofhousehold) that is located in anothercountry. Border children may be evenmore stigmatized or mistreated by thenonimmigrant populations livingnearby, as their families are falselypresumed to take advantage of scarceresources and not pay taxes.
Many border communities are poorand lacking in resources, includingmedical care. In general, border com-munities lack sufficient numbers ofprimary care pediatricians, and thosepresent may lack appropriate culturaland linguistic capacity to serve mi-nority border children. In addition,primary care providers bear an es-pecially high proportion of Medicaid,CHIP, and self-pay patients, with fewprivately insured patients to whomcosts may be shifted. As a conse-quence of these deficiencies and be-cause of high costs of medical care inthe United States, families living close
to the border may use medical careand pharmaceutical resources southof the border.
RECOMMENDATIONS
Immigrant children represent a con-siderable part of the economic andsocial future of the nation. It is in thenational interest that we work to en-sure that all children within the UnitedStates, including immigrant, border,and migrant children, grow up physi-cally and developmentally healthy. Thefuture prosperity and well-being of theUnited States depends on the healthand vitality of all of its children,without exception. The following rec-ommendations address how pedia-tricians can help support immigrantchild health in practice.
1. Pediatricians and the AmericanAcademy of Pediatrics should ad-vocate for health insurance cover-age for every child and everyindividual living in the UnitedStates, as lack of coverage forany family member affects thehealth of the entire family.25 Thisadvocacy should focus on expand-ing access to quality health carewithin a medical home. Barriersto enrollment must be addressed,including the removal of any wait-ing periods for documented immi-grant children to enroll intocoverage. Efforts must also ad-dress barriers to enrollment forchildren who are potentially eligi-ble for Medicaid and CHIP but notenrolled. Simplified enrollmentfor both programs and federalor state funding for those whoare not currently eligible for Med-icaid or CHIP is also essential.
2. The provision of comprehensive,coordinated, culturally and lin-guistically effective care, and con-tinuous health services providedin a quality medical home shouldbe integral to all efforts on behalf
of immigrant children.26 This isespecially critical for children withchronic health care needs andemotional or behavioral healthproblems. Private and public in-surance payers should pay forqualified medical interpretationservices.
3. Pediatricians caring for immigrantchildren should evaluate immu-nization adequacy and shouldconduct careful developmentalsurveillance and screening at reg-ular intervals as recommended bythe American Academy of Pediat-rics.27 Appropriate referral forearly intervention services or psy-choeducational evaluation shouldbe initiated as soon as a concernis identified.
4. Pediatricians should recognizethe barriers to health that arefaced by immigrant children andtake these barriers into accountwhile providing care. They shouldinquire about beliefs and practi-ces related to health, illness, anddisability, as well as traditionalhealing practices and medicationuse while obtaining a patient’smedical history. Knowledge, atti-tude, and skill development in cul-turally and linguistically effectivepractices and cross-cultural com-munication should be part of ev-ery pediatrician’s professionalagenda.
5. Pediatricians should be knowledge-able about the unique emotional,behavioral, mental, and physicalhealth advantages and problemsthat may be faced by immigrantchildren, including those relatedto family separation. Appropriatescreening to identify family, envi-ronmental, and social circumstan-ces, as well as biological factors,should be incorporated into rou-tine pediatric assessments, suchas in Bright Futures history forms.
e2032 FROM THE AMERICAN ACADEMY OF PEDIATRICS at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

6. Pediatricians should have accessto information regarding federal,state, and community programsthat can serve as resources toat-risk children and families. Cul-turally relevant programs thataddress social and economic chal-lenges, such as food and housingsecurity, English literacy, and legalservices, are particularly impor-tant. Medical-legal partnershipsshould be supported to help immi-grant families with these issues.
7. Pediatricians should play a keyrole in helping immigrant parentsassess and review the educa-tional progress of the child andencouraging parents to becomeinvolved in and interact withteachers and the school commu-nity. If a child exhibits difficulty oracademic underachievement, pe-diatricians are in a unique posi-tion to advocate for the child andencourage and help parents toobtain appropriate evaluationand intervention from the schoolsystem.
8. Pediatricians should routinelyuse available screening and diag-nostic protocols for evaluatingforeign-born children for infec-tious diseases and other medicalconditions when providing carefor newly arrived immigrant chil-dren.28 Additional screenings, in-cluding lead, vision, and hearingscreenings, should be consideredwhether required for school entryor not.
9. Pediatricians should advocate foran array of culturally effective earlyintervention services, including theestablishment of evidence-basedearly literacy promotion programs,such as Reach Out and Read, inimmigrant, border, and migrantcommunities. Because reading issuch an important skill, these pro-grams are important tools for im-proving the school readiness of allchildren, just as fostering healthliteracy in parents is important tothe well-being of their children.
10. Pediatricians should use their posi-tions of respect in communities topromote the value of diversity andinclusion and to advocate for chil-dren and families of all backgrounds.
Given the challenging circumstancesmany immigrant children face becauseof their family’s immigration status, thefollowing recommendations addresshow immigration policies can supportchild health and well-being.
11. The health, well-being, and safety ofchildren should be prioritized in allimmigration proceedings. Wheneverpossible, the separation of a childfrom his or her family and homeenvironment should be prevented,and family reunions should be ex-pedited.
12. In no circumstances should a childhave to represent himself or her-self in an immigration proceeding.
13. Health care facilities should be safesettings for immigrant children
and families to access healthcare. Medical records and healthcare facilities should not be usedin any immigration enforcementaction.
LEAD AUTHORSLance A. Chilton, MDGilbert A. Handal, MDGonzalo J. Paz-Soldan, MD
COUNCIL ON COMMUNITY PEDIATRICSEXECUTIVE COMMITTEE, 2011–2012Deise C. Granado-Villar, MD, MPH, ChairpersonBenjamin A. Gitterman, MD, Vice ChairpersonJeffrey M. Brown, MD, MPHLance A. Chilton, MDWilliam H. Cotton, MDThresia B. Gambon, MDPeter A. Gorski, MD, MPAColleen A. Kraft, MDAlice A. Kuo, MD, PhDGonzalo J. Paz-Soldan, MDBarbara Zind, MD
CONTRIBUTORRicky Choi, MD, MPH – Chairperson, SpecialInterest Group on Immigrant Health
LIAISONSBenjamin Hoffman, MD – Chairperson, IndianHealth Special Interest GroupMelissa A. Briggs, MD – Section on MedicalStudents, Residents, and Fellowship TraineesFrances J. Dunston, MD, MPH – Commission toEnd Health Care DisparitiesCharles R. Feild, MD, MPH – Chairperson, Pre-vention and Public Health Special InterestGroupM. Edward Ivancic, MD – Chairperson, RuralHealth Special Interest GroupDavid M. Keller, MD – Chairperson, CommunityPediatrics Education and Training SpecialInterest Group
STAFFCamille Watson, MS
REFERENCES
1. Okie S. Immigrants and health care—atthe intersection of two broken systems.N Engl J Med. 2007;357(6):525–529
2. Child Trends. Immigrant children. Availableat: www.childtrendsdatabank.org/?q=node/333. Accessed July 19, 2012
3. United States-Mexico Border Health Com-mission. What is defined as the border
region? Available at: www.borderhealth.org/show_faq.php?id=16. Accessed July 19,2012
4. Foundation for Child Development. Chil-dren in immigrant families: essentialto America’s future. Available at: http://fcd-us.org/node/1232. Accessed July 19,2012
5. Fortuny K, Ajay C. Children of Immigrants:Growing National and State Diversity. Brief5. Washington, DC: The Urban Institute;2011
6. Fadiman A. The Spirit Catches You and YouFall Down: A Hmong Child, Her AmericanDoctors, and the Collision of Two Cultures.New York, NY: Noonday Press; 1998
PEDIATRICS Volume 131, Number 6, June 2013 e2033
FROM THE AMERICAN ACADEMY OF PEDIATRICS
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

7. Fortuny K, Hernandez DJ, Ajay C. YoungChildren of Immigrants: The Leading Edgeof America’s Future. Brief 3. Washington,DC: The Urban Institute; 2010
8. Conroy K, Sandel M, Zuckerman B. Povertygrown up: how childhood socioeconomicstatus impacts adult health. J Dev BehavPediatr. 2010;31(2):154–160
9. Mendoza FS. Health disparities and chil-dren in immigrant families: a researchagenda. Pediatrics. 2009;124(suppl 3):S187–S195
10. Lansford JE, Deater-Deckard K, BornsteinMH, eds. Immigrant Families in Contempo-rary Society. New York, NY: Guilford Press;2007
11. US Citizenship and Immigration Services.Public Charge Fact Sheet, April 2011. Availableat: www.uscis.gov/portal/site/uscis/menuitem.5af9bb95919f35e66f614176543f6d1a/?vgnextoid=775d23cbea6bf210VgnVCM100000082ca60aRCRD&vgnextchannel=8a2f6d26d17df110VgnVCM1000004718190aRCRD.Accessed July 19, 2012
12. National Immigration Law Center. How areimmigrants included in health care re-form? Washington, DC: National Immigra-tion Law Center; April 2010. Available at:www.nilc.org/contact_us.html. AccessedJuly 19, 2012
13. Flores G, Laws MB, Mayo SJ, et al. Errors inmedical interpretation and their potentialclinical consequences in pediatric encoun-ters. Pediatrics. 2003;111(1):6–14
14. Singh GK, Kogan MD, Dee DL. Nativity/immigrant status, race/ethnicity, and so-cioeconomic determinants of breastfeedinginitiation and duration in the United States,2003. Pediatrics. 2007;119(1 suppl 1):S38–S46
15. Capps R, Fix M, Ost J, Reardon-Anderson J,Passel JS. The Health and Well-Being ofYoung Children of Immigrants. Washington,DC: The Urban Institute; 2004
16. Liu J, Probst JC, Martin AB, Wang JY, Sali-nas CF. Disparities in dental insurancecoverage and dental care among US chil-dren: the National Survey of Children’sHealth. Pediatrics. 2007;119(suppl 1):S12–S21
17. Strine TW, Barker LE, Mokdad AH, Luman ET,Sutter RW, Chu SY. Vaccination coverage offoreign-born children 19 to 35 months ofage: findings from the National Immuniza-tion Survey, 1999-2000. Pediatrics. 2002;110(2 pt 1):e15
18. Tienda M, Haskin R. Immigrant children:introducing the issue. Immigrant Children.2011;21(1):3–18
19. Kupersmidt JB, Martin SL. Mental healthproblems of children of migrant and sea-sonal farm workers: a pilot study. J AmAcad Child Adolesc Psychiatry. 1997;36(2):1–9
20. Fuller B, Bridges M, Bein E, et al. The healthand cognitive growth of Latino toddlers: atrisk or immigrant paradox? Matern ChildHealth J. 2009;13(6):755–768
21. Legal Information Institute. Immigrationlaw: an overview. Available at: www.law.cornell.edu/wex/Immigration. Accessed July19, 2012
22. Chaudry A, Capps R, Pedroza JM, CastenadaRM, Santos R, Scott MM. Facing Our Future:Children in the Aftermath of ImmigrationEnforcement. Washington, DC: The UrbanInstitute; 2010
23. McLaurin J, ed; American Academy of Pe-diatrics. Guidelines for the Care of MigrantFarmworker’s Children. Elk Grove Village, IL:American Academy of Pediatrics; 2000
24. Migrant Clinician’s Network. Children’shealth. Available at: www.migrantclinician.org/issues/childrens-health.html. AccessedJuly 19, 2012
25. Ku L, Broaddus M. Coverage for ParentsHelps Children, Too. Washington, DC: Centeron Budget and Policy Priorities; 2006
26. American Academy of Pediatrics Committeeon Pediatric Workforce. Culturally effectivepediatric care: education and trainingissues. Pediatrics. 1999;103(1):167–170
27. Hagan JF, Jr, Shaw JS, Duncan P, eds. BrightFutures: Guidelines for Health Supervisionof Infants, Children, and Adolescents. 3rded. Elk Grove Village, IL: American Academyof Pediatrics; 2008
28. Pickering LK, Baker CJ, Kimberlin DW, LongSS, eds; American Academy of Pediatrics.Red Book: 2012 Report of the Committee onInfectious Diseases. 29th ed. Elk Grove Village,IL: American Academy of Pediatrics; 2012
e2034 FROM THE AMERICAN ACADEMY OF PEDIATRICS at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-1099 originally published online May 6, 2013; 2013;131;e2028Pediatrics
COUNCIL ON COMMUNITY PEDIATRICSProviding Care for Immigrant, Migrant, and Border Children
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/131/6/e2028including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/131/6/e2028#BIBLThis article cites 11 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/immigration_subImmigrationalth_subhttp://www.aappublications.org/cgi/collection/international_child_heInternational Child Healthy_pediatricshttp://www.aappublications.org/cgi/collection/council_on_communitCouncil on Community Pediatricshttp://www.aappublications.org/cgi/collection/current_policyCurrent Policyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2013-1099 originally published online May 6, 2013; 2013;131;e2028Pediatrics
COUNCIL ON COMMUNITY PEDIATRICSProviding Care for Immigrant, Migrant, and Border Children
http://pediatrics.aappublications.org/content/131/6/e2028located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2013 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at American Academy of Pediatrics on August 13, 2019www.aappublications.org/newsDownloaded from

CLINICAL REPORT
Parent-Provider-Community Partnerships: OptimizingOutcomes for Children With Disabilities
abstractChildren with disabilities and their families have multifaceted medical,developmental, educational, and habilitative needs that are best ad-dressed through strong partnerships among parents, providers, andcommunities. However, traditional health care systems are designedto address acute rather than chronic conditions. Children with disabil-ities require high-quality medical homes that provide care coordina-tion and transitional care, and their families require social and finan-cial supports. Integrated community systems of care that promoteparticipation of all children are needed. The purpose of this clinicalreport is to explore the challenges of developing effective community-based systems of care and to offer suggestions to pediatricians andpolicy-makers regarding the development of partnerships among chil-dren with disabilities, their families, and health care and other provid-ers to maximize health and well-being of these children and their fam-ilies. Pediatrics 2011;128:795–802
INTRODUCTIONChildren with special health care needs are a group of 10 million USchildren with a wide variety of conditions, medical needs, and caregiv-ing requirements.1 However, children with disabilities, a subset of chil-dren with special health care needs, tend to have more complexconditions and functional impairments, often with technology depen-dencies and recurrent hospitalizations. In fact, 6.3% of US childrenbetween 5 and 15 years of age have 1 or more disabilities, and approx-imately 1%, or nearly one-half million children, are unable to care forthemselves.2 Over the past 50 years, the number of children living withdisabilities has tripled, largely as the result of health care advancesthat have allowed the survival of children with conditions that werehistorically incompatible with life.3 Children and adolescents have hadthe highest growth rate of disability of any age group during the pastdecade.3 Despite these changing demographics, the current system ofhealth care continues to use an outdated system that emphasizesacute illness and well-child care at the expense of long-term manage-ment of chronic conditions and disabilities.
Historically, hospital-based or institutional care was the only option formost children with complex medical conditions, technology depen-dence, and significant behavioral and emotional needs. More recently,social policy has promoted community-based programs that providecare for childrenwith disabilities in their homes and communities.4 For
Nancy A. Murphy, MD, Paul S. Carbone, MD, and theCOUNCIL ON CHILDREN WITH DISABILITIES
KEY WORDSdisabilities, children with special health care needs, community,medical home
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The guidance in this report does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account individual circumstances, may beappropriate.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1467
doi:10.1542/peds.2011-1467
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Guidance for the Clinician inRendering Pediatric Care
PEDIATRICS Volume 128, Number 4, October 2011 795by guest on April 9, 2017Downloaded from

example, Healthy People 2010 set agoal of reducing to zero the number ofchildren and youth living in congregatecare settings. These well-intentionedefforts to care for all children with dis-abilities in their homes and communi-ties rather than congregate care cen-ters have benefitted many childrenand families. However, community-based care has also brought new andunanticipated challenges for somechildren with disabilities, their fami-lies, communities, and health care sys-tems. The purpose of this clinical re-port is to explore the challenges ofdeveloping effective community-basedsystems of care and to offer sugges-tions to pediatricians and policy-makers regarding the development ofpartnerships among children with dis-abilities, their families, and healthcare and other providers to maximizethe health and well-being of these chil-dren and their families.
ADDRESSING THE NEEDS OFCHILDREN WITH DISABILITIES
Children With Disabilities RequireMedical Homes
It is a national health care objective toensure that all children with specialhealth care needs have access to com-prehensive health care consistent withthe standard of a medical home.5,6 Acore component of community-basedsystems of care, the medical home ide-ally comprises providers who areknowledgeable in the area of chroniccondition management and activelyscreen all children for developmentaldisability.4 Children with disabilitiescared for in medical homes that pro-vide care coordination benefit from in-creased access to subspecialty care,fewer missed days of school, and de-creased family financial burden.7
Moreover, having a medical home is apredictor for less inpatient and emer-gency department utilization8 andfewer unmet medical and support-
service needs.9 The longitudinal rela-tionship between medical home pro-viders, children with disabilities, andtheir families provides a comfortableand trusted framework for shareddecision-making and, in some in-stances, end-of-life discussions. De-spite these benefits, only half of all chil-dren with special health care needscurrently receive care consistent withan ideal medical home, a proportionthat is significantly lower than that oftheir typically developing peers.7 Livingin poverty or certain geographic loca-tions and having amore severe disabil-ity or certain conditions, such as au-tism, further limit a child’s access to amedical home.9–11
Beyond access, care coordinationwithin themedical homematters. Carecoordination facilitates strong part-nerships between families and physi-cians and supports shared medicaldecision-making. Providers beyond themedical home are frequently involvedin the care of children with disabilitiesin emergency departments, subspe-cialty clinics, and hospitals. Even if theydo not participate directly in care de-livery, medical homes can collaboratewith providers and families to fostertrust, provide information, and assistin treatment planning.12 Without suchcollaborations, children with disabili-ties are at increased risk of experienc-ing adverse events related to delayedor incomplete information transfer be-tween providers.13 However, nearlyhalf of all children with special healthcare needs do not receive adequatecare coordination, at least in part be-cause of inadequate payment to pro-viders.14,15 Eliminating barriers to ef-fective care coordination within themedical home is essential if pediatricsystems of care are to effectively ad-dress the needs of children withchronic conditions and disabilities.
Pediatricians have a vital role inlinking medical homes with other
community-based services for chil-dren with disabilities and theirfamilies. With universal approachesto developmental surveillance andscreening, providers can make timelyreferrals for at-risk children to educa-tional services, such as early interven-tion and special education programs.Familiarity with the Individuals WithDisabilities Education Act and Section504 of the Rehabilitation Act can helppediatricians effectively advocate forchildren with disabilities and theirfamilies in the development and imple-mentation of individualized educa-tional plans that are family centeredand goal directed.16,17 Likewise, themedical home should be a clearing-house of information for potentialsources of support for families and as-sist in providing medical informationto agencies to facilitate the eligibilityprocess.18 For example, the Supple-mental Security Income (SSI) programcan provide financial assistance andestablish eligibility for other vital ser-vices that may not otherwise beaccessed.19
Although financing the critical aspectsof the medical home has been a bar-rier for implementation, recent na-tional policy changes have improvedthe outlook on providing these ser-vices for children with disabilities. TheChildren’s Health Insurance ProgramReauthorization Act of 2009 containsseveral provisions that support stateinitiatives to strengthen medicalhomes for children with disabilities.For example, Idaho and Utah are usingelectronic health records and otherhealth information technology andplacing medical home coordinators inprimary and subspecialty practices toimprove care coordination.20 In addi-tion, section 2702 of the AffordableCare Act (Health Home for EnrolleesWith Chronic Conditions) providesstates the option to receive an en-hanced federal match if they amend
796 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 9, 2017Downloaded from

state plans to fund medical home ser-vices for children with disabilities.21
Youth With Disabilities RequireTransitional Care
Every year, more than one-half millionyouth with disabilities transition toadulthood.22 This process may includeparticipation in postsecondary educa-tion, vocational training, employment,independent or supported living ar-rangements, and adult health care sys-tems. However, for children with com-plex chronic conditions and lifelongfunctional limitations, the transitionprocess can be complex and fraughtwith barriers, particularly for thosewho are uninsured, poor, or lackingmedical homes or who have more se-vere disabilities.23 Not all youth withdisabilities transition fully into inde-pendent or supported living arrange-ments; for example, more than half ofyoung adults with autism continue tolive with their parents.24 Uninterruptedcomprehensive health care; coordi-nated transfers of medical informa-tion; and accessible, affordable, andcontinuous health insurance coverageare core elements of successful healthcare transitions.25 Lack of adult pro-vider expertise and experience in thecare of youth with child-onset disabili-ties creates additional access barri-ers, even for those young adults withinsurance coverage. Changes in insur-ance rules and training for themedicalworkforce would improve transitionprocesses.26 Several pilot programsthat provide clinical services duringthe late adolescent/young adult yearsor deliberate transition-specific carecoordination offer promising ap-proaches to health care transitions foryouth with disabilities.26
Pediatricians can assist in the transi-tion of youth with disabilities into adulthealth care systems by preparing fam-ilies well in advance, assisting in theidentification of adult providers, and
communicating relevant patient infor-mationwith adult providers via writtenmedical summaries and current careplans. Provisions in the IndividualsWith Disabilities Education Act man-date the development of an individual-ized transition plan (ITP) to prepareyouth with disabilities to enter theadult community. Pediatricians can as-sist youth with disabilities by encour-aging pursuit of identified vocationalgoals and advocating for implementa-tion of an appropriate individualizedtransition plan.27
ADDRESSING THE NEEDS OFFAMILIES OF CHILDREN WITHDISABILITIES
Parents of Children WithDisabilities Need Opportunities toPromote Their Own Health andWell-being
Parents of children with disabilitiesoften experience unrecognized and,therefore, unaddressed negative con-sequences of long-term caregiving.They are in poorer physical and emo-tional health than are parents of typi-cally developing children.28,29 Whencompared with others, parents of chil-dren with cerebral palsy reportgreater chronic distress and higherrates of back problems, migraineheadaches, stomach/intestinal ulcers,and chronic pain.30 Parents of childrenwith technology dependencies reportlimited time for sleep and for partici-pation in social and community activi-ties.31 Behavioral problems in childrenwith autism spectrum disorders arestrongly associated with parentalstress.32,33
When parents of children with disabil-ities experience poor health, they maybe less able to care for their children,which sets up a vicious cycle of nega-tive outcomes for all family mem-bers.30,34 In fact, the physical health ofparents is directly associated with thephysical health of their children with
cerebral palsy, and theirmental healthis significantly associated with the psy-chosocial function and total quality oflife of their children.35 Strategies thatpromote the health and well-being ofparents might benefit the entire familythrough these complex, reciprocal in-teractions. For example, resilient fam-ilies of children with autism find a pos-itive meaning in the disability, mobilizeresources, and gain spiritual strength,which culminates in greater familycohesion and appreciation of life.36
Linking parents of children with dis-abilities to appropriate family organi-zations and peer support has beenshown to positively affect both parentsand children.37–40
Siblings of Children WithDisabilities Need Support
Living with a child with a disabilitychanges the childhood experiencefor siblings. Many siblings reportthat family routines are focused andplanned around the sibling with adisability. Older siblings report thatthey have provided nursing and re-spite care, which limits their owntime for social activities outside thehome. Nearly half of all siblings re-port that their attendance and per-formance at school is negatively af-fected by the home care regimen of asibling dependent on technology.31
The caregiving responsibilities andfrustration about perceived competi-tion for parental attention rendersiblings of children with disabilitiesat heightened risk of negative psy-chological effects such as anxietyand depression.40 Despite these chal-lenges, nearly 40% of parents of chil-dren with developmental disabilitiesreport positive outcomes for sib-lings.41 Family-based interventionsthat enrich sibling experiences whileminimizing negative consequencesare needed.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 4, October 2011 797by guest on April 9, 2017Downloaded from

Parents of Children WithDisabilities Need Financial Support
Forty percent of families with childrenwith special health care needs experi-ence financial burden related to theirchild’s condition.42 Although most fam-ilies of children with special healthcare needs have medical insurance,underinsurance resulting in financialstress preferentially affects families ofchildren with disabilities.43 Reports offinancial hardship are more frequentin families with children with more se-vere disabilities, those with lower in-comes,44 and those with certain condi-tions such as autism spectrumdisorders.45,46 Hopeful investment inunproven interventions can further de-plete family finances.
At the same time that families ofchildren with disabilities experiencegreater financial demands, nearly 30%of them also contend with loss of in-come secondary to the need to reduceor eliminate employment.47 Althoughsome innovative employers offer bene-fits that might support employees ofchildren with disabilities,48 having achild with a disability is still associatedwith reduced parental employment.Single parents of children with tech-nology dependencies are 15 timesmore likely to quit employment sec-ondary to care responsibilities athome than those in 2-parent families.49
Lower financial stress is associatedwith receipt of coordinated care in amedical home, having adequate insur-ance, and access to organized and ac-cessible community-based service sys-tems.42 Beyondreducingfinancial stress,employment builds resilience in parentsby offering challenges and rewards thatare distinct from the complex responsi-bilities of caregiving.49
The recently enacted Affordable CareAct contains several provisions withinprivate insurance reform that benefitfamilies of children with disabilities:(1) elimination of lifetime and annual
caps on benefits; (2) guaranteed cov-erage through elimination of preexist-ing condition denials; and (3) expan-sion of dependent coverage up to theage of 26 years. Once exchanges areestablished by 2014, benefits forhealth plans must include chronic dis-ease management, behavioral healthtreatment, habilitation and rehabilita-tion services and devices, and oral andvision care. The scope of each of thesebenefits is yet to be defined.21
Families of children with disabilitiesrely on a variety of public and privateprograms such as private insurance,Title V programs, special educationservices, Supplemental Security In-come (SSI), and Medicaid. SSI can bean important source of financial sup-port for low-income families of chil-dren with disabilities.19 Since 1993, theFamily Medical Leave Act (FMLA) hasafforded parents of children with dis-abilities the option of taking up to 12weeks of excused absence from theirwork per year to better balance workand family obligations.50 The mix ofsupport variesdependingongeographiclocation, parental income, and eligibilityfactors, and pediatricians can guide par-ents as they navigate these complex sys-tems of funding.3 Family coordinators inmedical homes can identify communityresources and offer supports for bothfamilies and providers of children withdisabilities.51
Families Require Options for High-Quality Care Outside the Home
With proper support, most childrenwith disabilities thrive at home.52 Al-though home is the ideal place formost children, it may not be the bestplace for every child. In 1997, approxi-mately 1 per 1000 (nearly 25 000) chil-dren and youth were cared for in con-gregate care settings, including grouphomes and residential centers.53
Healthy People 2010 established an ob-jective to reduce this number to zero.
Five years later, the percentage of chil-dren and youth cared for in congre-gate care settings was nearly un-changed,53 which may relate to theunpredictable and often unavoidablecircumstances that necessitate thatchildren with disabilities receive inter-vals of care outside of their homes. Thelong-term demands of addressing thephysical, emotional, and behavioralneeds of some children with disabili-ties may periodically exceed thatwhich their parents and families canmanage, particularly when financialand social supports are limited.28 Insuch instances, the stress of caregiv-ing can lead to disrupted parentingand poor child outcomes.54 For exam-ple, children with disabilities are 3 to 4times more likely to be neglected orabused than are typically developingchildren.55 Community-based congre-gate care options can offer safe har-bor for children with disabilities whenfamilies find themselves in need of re-spite or when facing crisis situations.By maintaining strong partnerships,pediatricians can recognize families incrisis and assist them with finding ap-propriate resources.
ADDRESSING NATIONAL GOALS
Communities Must Promote theParticipation of All People,Including Children With Disabilities
The World Health Organization’s Inter-national Classification of Functioncharacterizes people with disabilitiesaccording to their ability to participatein meaningful community activitiesrather than diagnostic groupings. Itemphasizes what children do ratherthan how they do it and note that thepresence of a disability does not sug-gest an absence of health.56 The partic-ipation of each child is influenced bycontextual elements such as interac-tions between the child, family, andcommunity. Although all children, in-cluding those with disabilities, can
798 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 9, 2017Downloaded from

benefit from participation in sports,recreation, and physical activities, per-sonal and societal barriers need to ad-dressed.57 In general, children withdisabilities are less involved in leisureactivities than their peers and engagein activities that are more passive,home based, and less varied.58 Parentsand children with physical disabilitiesdescribe architectural barriers, re-strictive policies, limited personal as-sistance, cultural biases, and inade-quate social support asmajor barriersto community participation.59 Age, gen-der, activity limitations, family prefer-ences, and coping, motivation, and en-vironmental resources are otherdeterminants of participation.58
Coordinated Systems of Care forChildren With Disabilities NeedUniversal Implementation
A well-functioning system of family-centered, coordinated health care forchildren with disabilities would com-prise a full range of health care, edu-cation, and social services.50 The over-arching goal would be to address eachchild’s mental, physical, emotional,and social needs to optimize functionand participation according to the In-ternational Classification of Functionmodel of disability. Regardless of thepoint of entry, children and their fami-lies would be linked to other necessaryservices, because the systemwould beaccessible, flexible, and responsive.Family partnerships would lie at thehub of this system, consistent with thefact that families know their childrenbest and make decisions on behalf oftheir children.50 This community-basedsystem of service would be universallyaccessible, equitable, and organized topromote the cost-effective provision ofevidence-based care.60
A comprehensive community-basedsystem has been conceptualized butnot implemented. Despite the evidencethat a sense of partnership between
families and providers is associatedwith fewer unmet needs and betteroutcomes overall, of US families of chil-dren with special health care needs, 1million (14%) report a lack of suchpartnerships.61 Poverty, minority sta-tus, lack of insurance, and greater se-verity of functional limitations are as-sociated with greater risk of lacking asense of partnership.61 The barriers toimplementation include lack of inte-gration, coordination, and communi-cation between various service provid-ers and agencies; lack of adequatefunding to develop system infrastruc-ture; lack of funding sources to meetchildren’s needs; and balancing pri-vacy concerns with service providers’need for information.50 Although oursociety expects that parents will un-conditionally and indefinitely care fortheir children with disabilities, ourhealth care system offers, at best, afragmented and 1-size-fits-all re-sponse to their individualized and of-ten changing needs.62 The AffordableCare Act addresses several of theseshortcomings with provisions thatstrengthen community-based optionsfor long-term services and supportsfor children with disabilities: (1) theCommunity First Choice Option; (2)new options for home- and community-based services in Medicaid; and (3) ex-tension of “money follows the person”demonstration grants.63
Analogous to Russian nesting dolls,children with disabilities do not live inisolation but are embraced by theirparents, who function within familyunits, which are, in turn, nested incommunities and, ultimately, in localand national health care systems.64
This social ecological framework of hu-man development illustrates the criti-cal importance of community-basedsystems response to the multifac-eted and dynamic interdependenciesamong children with disabilities andtheir parents, families, communities,
and health care systems.65 Becausethe characteristics of each child andfamily, their shared history, and thesocial, economic, and cultural contextswithin which they find themselvescombine to create an infinite variety ofcircumstances,66 care must be individ-ualized and based on the tenets ofmutual trust, respect, and family-centered decision-making.
SUGGESTIONS FOR PEDIATRICIANS
1. Provide a medical home for childrenwith disabilities that emphasizes thefamily as a valued partner indecision-making, coordinates carewith subspecialists, and links fami-lies with community-based services.
2. Ensure coordinated, deliberate, andcommunity-based transitions for allyouth with disabilities by advocatingfor access to appropriate educa-tional and related community-basedtransition services and coordinatingwith adult medical providers.
3. Recognize the unique needs of par-ents and siblings of children withdisabilities, and offer strategies forthem to promote their own physicaland emotional health and well-being, including links to family sup-port groups and mental healthservices.
4. Understand and promote access tofinancial supports for families ofchildren with disabilities, includingMedicaid, Supplemental Security In-come, and Family Medical Leave Actprograms.
5. Recognize caregiver stress and en-sure that all parents are aware ofself-care strategies and options forhigh-quality care for their childrenwith disabilities, both inside andoutside the home.
6. Encourage participation of childrenwith disabilities and their familiesin educational, recreational, andsocial activities by actively linking
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 4, October 2011 799by guest on April 9, 2017Downloaded from

them to community-based agenciesand organizations.
7. Adopt a family-centered approachto the care of children with disabil-ities by involving families in all as-pects of medical decision-making.
SUGGESTIONS FOR POLICY-MAKERS
1. Ensure enforcement of health in-surance reforms that benefit chil-dren with disabilities under the Af-fordable Care Act, including theelimination of lifetime and annualcaps on benefits, guaranteed cov-erage through elimination ofpreexisting-condition denials, andthe expansion of dependent cover-age up to the age of 26 years.
2. Adopt models that support essen-tial functions of medical homes forchildren with disabilities, includingcare coordination and telephonemanagement.67
3. Advocate for the continuous provi-sion of vital public health servicesthat support families of childrenwith disabilities, including state Ti-tle V programs and Family-to-FamilyHealth Information Centers.
4. Maintain and extend public cover-age options (Medicaid and Chil-dren’s Health Insurance Program)for children with disabilitiesthrough Affordable Care Act initia-tives, such as simplifying eligibilityrequirements and amending stateMedicaid plans to fund medicalhome activities.
LEAD AUTHORSNancy A. Murphy, MDPaul S. Carbone, MD
COUNCIL ON CHILDREN WITHDISABILITIES EXECUTIVE COMMITTEE,2010–2011Nancy A. Murphy, MD, ChairpersonRichard C. Adams, MDRobert T. Burke, MD, MPH
Sandra L. Friedman, MDMiriam A. Kalichman, MDSusan E. Levy, MDGregory S. Liptak, MD, MPHDouglas McNeal, MDKenneth W. Norwood Jr, MDRenee M. Turchi, MD, MPHSusan E. Wiley, MD
PAST EXECUTIVE COMMITTEEMEMBERSLarry W. Desch, MDEllen Roy Elias, MDPaul H. Lipkin, MD, Immediate PastChairpersonPaul J. Sagerman, MD
LIAISONSGeorgina Peacock, MD, MPH – Centers forDisease Control and PreventionNora Wells, MSEd – Family VoicesBonnie Strickland, PhD – Maternal and ChildHealth BureauCarolyn Bridgemohan, MD – Section onDevelopmental and Behavioral PediatricsMax Wiznitzer, MD – Section on Neurology
STAFFStephanie Mucha Skipper, MPH
REFERENCES
1. Kogan MD, Strickland BB, Newacheck PW.Building systems of care: findings from theNational Survey of Children Special HealthCare Needs. Pediatrics. 2009;124(suppl 4):S333–S336
2. Erickson WA, Lee CG. 2007 Disability StatusReports: United States. Ithaca, NY: CornellUniversity Rehabilitation Research andTraining Center on Disability Demographicsand Statistics; 2008
3. Perrin JM. Health services research forchildren with disabilities. Milbank Q. 2002;80(2):303–324
4. McPherson M, Weissman G, Strickland BB,van Dyck PC, Blumberg SJ, Newacheck PW.Implementing community-based systems ofservices for children and youths with spe-cial health care needs: how well are we do-ing? Pediatrics . 2004;113(5 suppl) :1538–1544
5. American Academy of Pediatrics, MedicalHome Initiatives for Children With SpecialNeeds Project Advisory Committee. Themedical home. Pediatrics. 2002;110(1 pt 1):184–186
6. National Center for Medical Home Imple-mentation. Home page. Available at: www.medicalhomeinfo.org. Accessed March 1,2011
7. Turchi RM, Berhane Z, Bethell C, PomponioA, Antonelli R, Minkovitz CS. Care coordina-tion for CSHCN: associations with family-provider relations and family/child out-comes. Pediatrics. 2009;124(suppl 4):S428–S434
8. Cooley WC, McAllister JW, Sherrieb K,Kuhlthau K. Improved outcomes associatedwith medical home implementation in pedi-atric primary care. Pediatrics. 2009;124(1):358–364
9. Strickland BB, Singh GK, Kogan MD, MannMY, van Dyck PC, Newacheck PW. Access tothe medical home: new findings from the2005–2006 National Survey of Children WithSpecial Health Care Needs. Pediatrics. 2009;123(6). Available at: www.pediatrics.org/cgi/content/full/123/6/e996
10. Singh GK, Strickland BB, Ghandour RM, vanDyck PC. Geographic disparities in access tothe medical home among US CSHCN. Pediat-rics. 2009;124(suppl 4):S352–S360
11. Brachlow AE, Ness KK, McPheeters ML, Gur-ney JG. Comparison of indicators for a pri-mary care medical home between childrenwith autism or asthma and other specialhealth care needs: National Survey of Chil-dren’s Health. Arch Pediatr Adolesc Med.2007;161(4):399–405
12. Percelay JM. Physicians’ roles in coordinat-
ing care of hospitalized children. Pediatrics.2003;111(3):707–709
13. Kripalani S, LeFevre F, Phillips CO, WilliamsMV, Basaviah P, Baker DW. Deficits in com-munication and information transfer be-tween hospital-based and primary carephysicians: implications for patient safetyand continuity of care. JAMA. 2007;297(8):831–841
14. Antonelli RC, Antonelli DM. Providing a med-ical home: the cost of care coordination ser-vices in a community-based, general pediat-ric practice. Pediatrics. 2004;113(5 suppl):1522–1528
15. Antonelli RC, Stille CJ, Antonelli DM. Care co-ordination for children and youth with spe-cial health care needs: a descriptive, multi-site study of activities, personnel costs, andoutcomes. Pediatrics. 2008;122(1). Avail-able at: www.pediatrics.org/cgi/content/full/122/1/e209
16. American Academy of Pediatrics, Council onChildren With Disabilities. Role of the medi-cal home in family-centered early interven-tion services. Pediatrics. 2007;120(5):1153–1158
17. American Academy of Pediatrics, Council onChildren With Disabilities. Provision of edu-cationally related services for children andadolescents with chronic diseases and dis-
800 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 9, 2017Downloaded from

abling conditions. Pediatrics. 2007;119(6):1218–1223
18. The Medical Home Portal. Home page. Avail-able at: www.medicalhomeportal.org. Ac-cessed July 21, 2010
19. American Academy of Pediatrics, Councilon Children With Disabilities. Policystatement—Supplemental Security Income(SSI) for children and youth with disabili-ties. Pediatrics. 2009;124(6):1702–1708
20. InsureKidsNow.gov. CHIPRA quality demon-stration grants: summary. Available at:www.insurekidsnow.gov/professionals/CHIPRA/grants_summary.html. AccessedMarch 1, 2011
21. National Academy for State Health Policy.The Affordable Care Act and Children WithSpecial Health Care Needs. Available at:http://www.nashp.org/publication/aca-children-special-health-care-needs. Ac-cessed March 1, 2011
22. Cameto R, Levine P, Wagner M. TransitionPlanning for Students With Disabilities: ASpecial Topic Report of Findings From theNational Longitudinal Transition Study-2(NLTS2). Washington, DC: National Centerfor Special Education Research; 2004
23. Lotstein DS, Ghandour R, Cash A, McGuire E,Strickland B, Newacheck P. Planning forhealth care transitions: results from the2005–2006 National Survey of Children WithSpecial Health Care Needs. Pediatrics. 2009;123(1). Available at: www.pediatrics.org/cgi/content/full/123/1/e145
24. Farley MA, McMahon WM, Fombonne E, et al.Twenty-year outcome for individuals withautism and average or near-average cogni-tive abilities. Autism Res. 2009;2(2):109–118
25. American Academy of Pediatrics; AmericanAcademy of Family Physicians; AmericanCollege of Physicians-American Society ofInternal Medicine. A consensus statementon health care transitions for young adultswith special health care needs. Pediatrics.2002;110(6 pt 2):1304–1306
26. Gleason BL, Palmer J, Bhagat SKM, Reiss J.Enhancing Health Care Transition for Youthand Young Adults Living With Chronic Medi-cal Conditions and Disabilities: Suggestionsfor Reform. Rockville, MD: Coalition forYoung Adults Living With Chronic MedicalConditions and Disabilities; 2009. Availableat: http://physicianparent.org/siteimages/PPCpaper_web.pdf. Accessed July 21, 2010
27. American Academy of Pediatrics, AmericanAcademy of Family Physicians, and Ameri-can College of Physicians, Transitions Clini-cal Report Authoring Group. Supporting thehealth care transition from adolescence toadulthood in the medical home. Pediatrics.2011;128(1):182–200
28. Murphy NA, Christian B, Caplin DA, Young PC.The health of caregivers for children withdisabilities: caregiver perspectives. ChildCare Health Dev. 2007;33(2):180–187
29. Lach LM, Kohen DE, Garner RE, et al. Thehealth and psychosocial functioning ofcaregivers of children with neurodevelop-mental disorders. Disabil Rehabil. 2009;31(9):741–752
30. BrehautJC,KohenDE,RainaP,etal. Thehealthofprimary caregivers of children with cerebralpalsy: how does it compare with that of otherCanadian caregivers? Pediatrics. 2004;114(2).Available at: www.pediatrics.org/cgi/content/full/114/2/e182
31. Heaton J, Noyes J, Sloper P, Shah R. Fami-lies’ experiences of caring for technology-dependent children: a temporal perspec-tive. Health Soc Care Community. 2005;13(5):441–450
32. Bromley J, Hare DJ, Davison K, Emerson E.Mothers supporting children with autisticspectrum disorders: social support, mentalhealth status and satisfaction with ser-vices. Autism. 2004;8(4):409–423
33. Lecavalier L, Leone S, Wiltz J. The impact ofbehaviour problems on caregiver stress inyoung people with autism spectrum disor-ders. J Intellect Disabil Res. 2006;50(pt 3):172–183
34. Benson PR, Karlof KL. Anger, stress prolifer-ation, and depressed mood among parentsof children with ASD: a longitudinal replica-tion. J Autism Dev Disord. 2009;39(2):350–362
35. Murphy NA, Caplin DA, Christian B, LutherBL, Holobkov R, Young PC. The function ofparents and their children with cerebralpalsy. Phys Med Rehabil. 2011;3(2):98–104
36. Bayat M. Evidence of resilience in families ofchildren with autism. J Intellect Disabil Res.2007;51(pt 9):702–714
37. Ireys HT, Chernoff R, DeVet KA, Kim Y. Mater-nal outcomes of a randomized controlledtrial of a community-based support pro-gram for families of children with chronicillnesses. Arch Pediatr Adolesc Med. 2001;155(7):771–777
38. Chernoff RG, Ireys HT, DeVet KA, Kim YJ. Arandomized , contro l led tr ia l o f acommunity-based support program forfamilies of children with chronic illness: pe-diatric outcomes. Arch Pediatr AdolescMed. 2002;156(6):533–539
39. Farmer JE, ClarkMJ, Sherman A, MarienWE,Selva TJ. Comprehensive primary care forchildren with special health care needs inrural areas. Pediatrics . 2005;116(3):649–656
40. Sharpe D, Rossiter L. Siblings of children
with a chronic illness: a meta-analysis. J Pe-diatr Psychol. 2002;27(8):699–710
41. Dauz Williams P, Piamjariyakul U, Graff JC,et al. Developmental disabilities: effects onwell siblings. Issues Compr Pediatr Nurs.2010;33(1):39–55
42. Kuhlthau K, Hill KS, Yucel R, Perrin JM. Finan-cial burden for families of children withspecial health care needs. Matern ChildHealth J. 2005;9(2):207–218
43. Kogan MD, Newacheck PW, Blumberg SJ, etal. State variation in underinsuranceamong children with special health careneeds in the United States. Pediatrics. 2010;125(4):673–680
44. Newacheck PW, Inkelas M, Kim SE. Healthservices use and health care expendituresfor children with disabilities. Pediatrics.2004;114(1):79–85
45. Kogan MD, Strickland BB, Blumberg SJ,Singh GK, Perrin JM, van Dyck PC. A nationalprofile of the health care experiences andfamily impact of autism spectrum disorderamong children in the United States,2005–2006. Pediatrics. 2008;122(6). Avail-able at: www.pediatrics.org/cgi/content/full/122/6/e1149
46. Montes G, Halterman JS. Child care prob-lems and employment among families withpreschool-aged children with autism in theUnited States. Pediatrics. 2008;122(1). Avail-able at: www.pediatrics.org/cgi/content/full/122/1/e202
47. Looman WS, O’Conner-Von SK, Ferski GJ,Hildenbrand DA. Financial and employmentproblems in families of children with spe-cial health care needs: implications for re-search and practice. J Pediatr Health Care.2009;23(2):117–125
48. Perrin JM, Fluet CF, Honberg L, et al. Benefitsfor employees with children with specialneeds: findings from the collaborative em-ployee benefit study. Health Aff (Millwood).2007;26(4):1096–1103
49. Thyen U, Kuhlthau K, Perrin JM. Employ-ment, child care, andmental health ofmoth-ers caring for children assisted by technol-ogy. Pediatrics. 1999;103(6 pt 1):1235–1242
50. Perrin JM, Romm D, Bloom SR, et al. Afamily-centered, community-based systemof services for children and youth with spe-cial health care needs. Arch Pediatr AdolescMed. 2007;161(10):933–936
51. Tinajero A, Garneau D. Evaluation of RhodeIsland’s Pediatric Practice EnhancementProject (PPEP). Med Health R I. 2009;92(7):253–255
52. Homer CJ, Klatka K, Romm D, et al. A reviewof the evidence for the medical home forchildren with special health care needs. Pe-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 4, October 2011 801by guest on April 9, 2017Downloaded from

diatrics . 2008;122(4) . Avai lable at :www.pediatrics.org/cgi/content/full/122/4/e922
53. Prouty R, Lakin KC, Coucouvanis K, AndersonL. Progress toward a national objective ofHealthy People 2010: “reduce to zero thenumber of children 17 years and youngerliving in congregate care.” Ment Retard.2005;43(6):456–460
54. Schor EL; American Academy of Pediatrics,Task Force on the Family. Family pediatrics:report of the Task Force on the Family. Pe-diatrics. 2003;111(6 pt 2):1541–1571
55. Sullivan PM, Knutson JF. Maltreatment anddisabilities: a population-based epidemio-logical study. Child Abuse Negl. 2000;24(10):1257–1273
56. Murphy NA. Is cerebral palsy a health prob-lem? J Pediatr. 2008;153(2):158–160
57. Murphy NA, Carbone PS; American Academyof Pediatrics, Council on Children With Dis-abilities. Promoting the participation ofchildren with disabilities in sports, recre-
ation, and physical activities. Pediatrics.2008;121(5):1057–1061
58. Shikako-Thomas K, Majnemer A, Law M,Lach L. Determinants of participation in lei-sure activities in children and youth withcerebral palsy: systematic review. Phys Oc-cup Ther Pediatr. 2008;28(2):155–169
59. Law M, Petrenchik T, King G, Hurley P. Per-ceived environmental barriers to recre-ational, community, and school participa-tion for children and youth with physicaldisabilities. Arch Phys Med Rehabil. 2007;88(12):1636–1642
60. Roberts RN, Behl DD, Akers AL. Building asystem of care for children with specialhealthcare needs. Infants Young Child.2004;17(3):213–222
61. Denboba D, McPherson MG, Kenney MK,Strickland B, Newacheck PW. Achieving fam-ily and provider partnerships for childrenwith special health care needs. Pediatrics.2006;118(4):1607–1615
62. Stein RE. Challenges in long-term health
care for children. Ambul Pediatr. 2001;1(5):280–288
63. National Academy for State Health Policy.Implementing the Affordable Care Act: newoptions for Medicaid home and communitybased services. Available at: www.nashp.org/node/2131. Accessed March 1, 2011
64. Murphy N, Christian B. Disability in childrenand young adults: the unintended conse-quences. Arch Pediatr Adolesc Med. 2007;161(10):930–932
65. Bronfenbrenner U. Ecology of the family as acontext for human development. Dev Psy-chol. 1986;22(6):723–742
66. Raina P, O’Donnell M, Schwellnus H, et al.Caregiving process and caregiver burden:conceptual models to guide research andpractice. BMC Pediatr. 2004;4:1
67. Strickland BB, Jones JR, Ghandour RM,Kogan MD, Newacheck PW. The medicalhome: health care access and impact forchildren and youth in the United States. Pe-diatrics. 2011;127(4):604–611
802 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 9, 2017Downloaded from

DOI: 10.1542/peds.2011-1467; originally published online September 26, 2011;Pediatrics
DISABILITIESNancy A. Murphy, Paul S. Carbone and COUNCIL ON CHILDREN WITH
With DisabilitiesParent-Provider-Community Partnerships: Optimizing Outcomes for Children
ServicesUpdated Information &
/content/early/2011/09/21/peds.2011-1467including high resolution figures, can be found at:
Citations /content/early/2011/09/21/peds.2011-1467#related-urls
This article has been cited by 12 HighWire-hosted articles:
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 9, 2017Downloaded from
DOI: 10.1542/peds.2011-1467; originally published online September 26, 2011;Pediatrics
DISABILITIESNancy A. Murphy, Paul S. Carbone and COUNCIL ON CHILDREN WITH
With DisabilitiesParent-Provider-Community Partnerships: Optimizing Outcomes for Children
/content/early/2011/09/21/peds.2011-1467
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 9, 2017Downloaded from
Related Documents











