Association between Cryptosporidium Infection and Human Leukocyte Antigen Class I and Class II Alleles Beth D. Kirkpatrick 1 , Rashidul Haque 4 , Priya Duggal 2 , Dinesh Mondal 4 , Cathy Larsson 1 , Kristine Peterson 3 , Jasmin Akter 4 , Lauren Lockhart 3 , Salwa Khan 1 , and William A. Petri Jr. 3 1 University of Vermont College of Medicine, Unit of Infectious Diseases, Burlington, Vermont 2 National Human Genome Research Institute, National Institutes of Health, Baltimore, Maryland 3 University of Virginia, Charlottesville, Virginia 4 Centre for Health and Population Research, International Centre for Diarrheal Disease Research, Dhaka, Bangladesh Abstract Background—Cryptosporidium species are a common cause of diarrhea, which can be severe and protracted in young children and immunocompromised individuals. Methods—A cohort of 226 Bangladeshi children aged 2–5 years was prospectively followed for >3 years to study the role of host genetics in susceptibility to infection, as well as the community impact of cryptosporidiosis on this population. Results—Ninety-six children (42.5%) received a diagnosis of Cryptosporidium infection. A total of 51 (22.6%) had asymptomatic infection. Fifty-eight (25.7%) had cryptosporidiosis, of whom 17 (29.3%) had recurrent disease. Children with cryptosporidiosis presented early, and most had abdominal pain and a short course of diarrhea. Infected children were more likely to carry the human leukocyte antigen (HLA) class II DQB1*0301 allele, particularly those with asymptomatic and symptomatic infection (P = .009); a strong association was found between carriage of the DQB1*0301/DRB1*1101 haplotype and development of both asymptomatic and symptomatic infection (P = .008). Infected children were also more likely to carry the B*15 HLA class I allele. Conclusions—This is the first study to describe a possible genetic component of the immune response to Cryptosporidium infection, which includes HLA class I and II alleles. Cryptosporidiosis in Bangladeshi children aged 2–5 years is common and often recurrent, but the duration is shorter and the abdominal pain greater than that described in children aged <2 years. Cryptosporidiosis is a common enteric infection that causes self-limiting diarrhea in healthy individuals but can cause severe, protracted, and life-threatening disease in immunocompromised adults and very young children [1–3]. The human immune response to cryptosporidiosis, particularly in children, is only partially understood [3]. Normal CD4 + T lymphocyte numbers and function and a T helper-1–biased cytokine pattern appear important for recovery from cryptosporidiosis, on the basis of data from susceptible animal models and individuals with advanced AIDS [1, 4, 5]. A modest pro-inflammatory cytokine response has also been reported in studies of childhood cryptosporidiosis [6, 7]. © 2008 by the Infectious Diseases Society of America. All rights reserved. Reprints or correspondence: Dr. Beth D. Kirkpatrick, Unit of Infectious Diseases, University of Vermont College of Medicine, 110 Stafford Hall, 95 Carrigan Ln., Burlington, VT 05405 ([email protected]). Potential conflicts of interest: none reported. NIH Public Access Author Manuscript J Infect Dis. Author manuscript; available in PMC 2012 July 24. Published in final edited form as: J Infect Dis. 2008 February 1; 197(3): 474–478. doi:10.1086/525284. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Association between Cryptosporidium Infection and HumanLeukocyte Antigen Class I and Class II Alleles
Beth D. Kirkpatrick1, Rashidul Haque4, Priya Duggal2, Dinesh Mondal4, Cathy Larsson1,Kristine Peterson3, Jasmin Akter4, Lauren Lockhart3, Salwa Khan1, and William A. Petri Jr.3
1University of Vermont College of Medicine, Unit of Infectious Diseases, Burlington, Vermont2National Human Genome Research Institute, National Institutes of Health, Baltimore, Maryland3University of Virginia, Charlottesville, Virginia 4Centre for Health and Population Research,International Centre for Diarrheal Disease Research, Dhaka, Bangladesh
AbstractBackground—Cryptosporidium species are a common cause of diarrhea, which can be severeand protracted in young children and immunocompromised individuals.
Methods—A cohort of 226 Bangladeshi children aged 2–5 years was prospectively followed for>3 years to study the role of host genetics in susceptibility to infection, as well as the communityimpact of cryptosporidiosis on this population.
Results—Ninety-six children (42.5%) received a diagnosis of Cryptosporidium infection. A totalof 51 (22.6%) had asymptomatic infection. Fifty-eight (25.7%) had cryptosporidiosis, of whom 17(29.3%) had recurrent disease. Children with cryptosporidiosis presented early, and most hadabdominal pain and a short course of diarrhea. Infected children were more likely to carry thehuman leukocyte antigen (HLA) class II DQB1*0301 allele, particularly those with asymptomaticand symptomatic infection (P = .009); a strong association was found between carriage of theDQB1*0301/DRB1*1101 haplotype and development of both asymptomatic and symptomaticinfection (P = .008). Infected children were also more likely to carry the B*15 HLA class I allele.
Conclusions—This is the first study to describe a possible genetic component of the immuneresponse to Cryptosporidium infection, which includes HLA class I and II alleles.Cryptosporidiosis in Bangladeshi children aged 2–5 years is common and often recurrent, but theduration is shorter and the abdominal pain greater than that described in children aged <2 years.
Cryptosporidiosis is a common enteric infection that causes self-limiting diarrhea in healthyindividuals but can cause severe, protracted, and life-threatening disease inimmunocompromised adults and very young children [1–3]. The human immune response tocryptosporidiosis, particularly in children, is only partially understood [3]. Normal CD4+ Tlymphocyte numbers and function and a T helper-1–biased cytokine pattern appearimportant for recovery from cryptosporidiosis, on the basis of data from susceptible animalmodels and individuals with advanced AIDS [1, 4, 5]. A modest pro-inflammatory cytokineresponse has also been reported in studies of childhood cryptosporidiosis [6, 7].
© 2008 by the Infectious Diseases Society of America. All rights reserved.
Reprints or correspondence: Dr. Beth D. Kirkpatrick, Unit of Infectious Diseases, University of Vermont College of Medicine, 110Stafford Hall, 95 Carrigan Ln., Burlington, VT 05405 ([email protected]).
Potential conflicts of interest: none reported.
NIH Public AccessAuthor ManuscriptJ Infect Dis. Author manuscript; available in PMC 2012 July 24.
Published in final edited form as:J Infect Dis. 2008 February 1; 197(3): 474–478. doi:10.1086/525284.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
The role of host genetics, including the human leukocyte antigen (HLA) genes responsiblefor the major histocompatibility complex (MHC) presentation of antigen to CD4+ T cells, inthe susceptibility or resistance to symptomatic (i.e., diarrheal) or asymptomaticCryptosporidium infection has not been comprehensively evaluated. We prospectivelystudied a large cohort of preschool-aged and grade school–aged children for >3 years.Genetic information on allelic differences was used to describe the role of HLA class I andII polymorphisms in their susceptibility to Cryptosporidium infection. Detailed clinical andepidemiologic data also contributed to understanding the community impact ofcryptosporidiosis in this population.
METHODSStudy protocol
The study was approved by the institutional review boards of the University of Vermont(Burlington, VT), the University of Virginia (Charlottesville, VA), the University ofMaryland (Baltimore, MD), the National Institutes of Health (Bethesda, MD), and theCenter for Health and Population Research, International Centre for Diarrheal DiseaseResearch (Dhaka, Bangladesh). Human experimentation guidelines of the participatinginstitutions and the US Department of Health and Human Services were followed inconducting the research.
Preschool-aged children (aged 2–5 years old) from an urban slum of Dhaka (Mirpur) wereenrolled from 1999 through 2002, as previously described [8, 9]. Parents and children werevisited and interviewed every other day by health care workers for symptoms of diarrhea.Informed consent was obtained from the parents or guardians prior to enrollment. Treatmentprotocols for diarrheal diseases have been described elsewhere but did not include treatmentfor Cryptosporidium infection during the period of the study [9].
Clinical definitionsDiarrhea was defined as ≥3 loose or watery stools in a 24-h period. Cryptosporidiosis (i.e.,symptomatic Cryptosporidium infection) was defined as the presence of diarrhea and thedetection of Cryptosporidium oocysts in stool by the Cryptosporidium antigen-detection kit(Techlab). Asymptomatic Cryptosporidium infection was defined as the absence of diarrheaand the detection of Cryptosporidium oocysts in stool by an antigen detection test. Controlchildren were all other children without a diagnosis of symptomatic or asymptomaticCryptosporidium infection during the study period. Stool specimens positive forCryptosporidium organisms were considered indicative of a distinct episode ofCryptosporidium infection if they were collected ≥60 days after negative results of stoolsurveillance assays were obtained. Infections were defined as recurrent if they were <60days apart with a negative stool examination between episodes. The severity of diarrhea wasdefined by a numerical scoring system known as the Ruuska score, which accounts forduration of diarrhea, maximum number of diarrheal stools/day, vomiting, fever, dehydration,and the level of clinical care required (ranging from no need for clinical care through theneed for hospitalization) [10].
Stool sampling and microbiological analysisStool specimens were collected ≤24 h after a report of a new diarrhea episode and everymonth for surveillance in all children. Microbiologic analysis of stool specimens has beendescribed elsewhere but included performance of standard bacteriologic cultures, testing forpathogenic Escherichia coli; testing for parasitic ova; commercial assays for adenovirus,rotavirus, and astrovirus; and antigen testing for Entamoeba histolytica [9]. Evaluation for
Kirkpatrick et al. Page 2
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
asymptomatic Cryptosporidium infection involved analysis of frozen and bankedsurveillance stools by the Cryptosporidium antigen-detection kit (Techlab).
Genetic analysesGenomic DNA was extracted from 200 μL of peripheral blood, using the Qiagen DNAextraction kit. HLA class I and II typing was performed using polymerase chain reaction(PCR) and sequence-specific oligonucleotides provided by Dynal, as previously described[11]. For genetic comparisons, all siblings were removed from analysis.
Statistical analysisEpidemiologic and genetic data were analyzed by SPSS software (version 7.5) or Statasoftware (version 8.0). The Student t test was used for comparison between means;nonparametric tests were used if the data were not normally distributed. χ2 analysis and theFisher exact test were used for categorical variables. P < .05 was considered statisticallysignificant for all tests.
For analysis of HLA data, allele frequencies were counted. Because of the large number ofHLA alleles, it was decided a priori that only cases or controls with an allele frequency of>10% would be involved in genetic association analysis. The magnitude of the associationbetween HLA markers and occurrence of Cryptosporidium infection was measured bycalculating the odds ratio (OR), using logistic regression. For multiple-case categories (noinfection, Cryptosporidium infection without diarrhea, and Cryptosporidium infection withdiarrhea), the OR was determined using polychotomous logistic regression. Theconservative Bonferroni correction was used to correct for multiple comparisons. Thismethod assumes that the statistical tests performed on the data set are independent.However, because of known interdependence among HLA alleles, we could not considertests involving the 20 HLA alleles as being separate. We adjusted for this by using thefollowing HLA class categories: A, B, C, DQB1, and DRB1 (n = 5 in the Bonferroni-adjusted analyses; the P value was multiplied by 5).
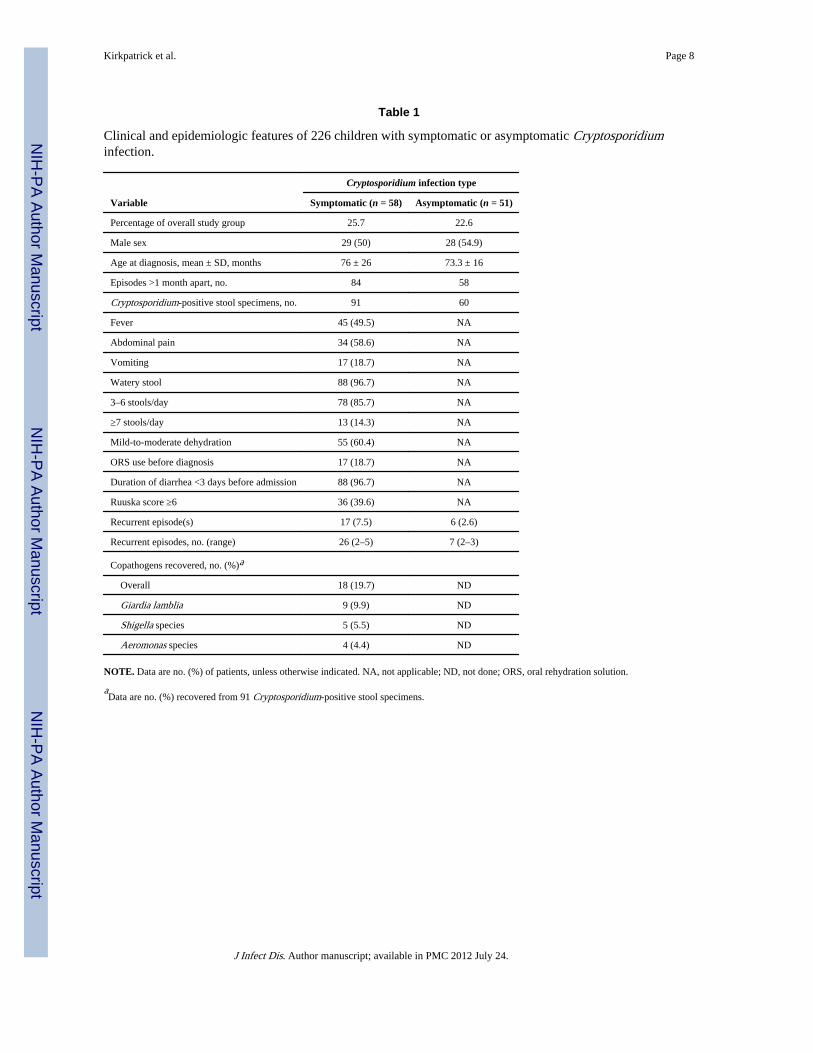
RESULTSThere were 289 children (147 boys and 142 girls) from Dhaka (Mirpur) who were enrolledduring 1999–2002. A total of 226 children were observed for >3 years, with a mean follow-up duration of 2316 days (6.3 years); 8980 stool specimens collected from these patientsduring the first 3 years of study participation were evaluated for the presence ofCryptosporidium organisms by an antigen-detection assay. One hundred fifty-two stoolspecimens involving 142 distinct episodes of Cryptosporidium infection in 96 children(42.5%) tested positive for Cryptosporidium organisms. Fifty-eight (25.7%) children hadCryptosporidium diarrhea, 51 (22.6%) had asymptomatic infection, and 13 (5.8% [13.5% of96 who tested positive for Cryptosporidium organisms]) had both. Clinical andepidemiologic characteristics of children with asymptomatic Cryptosporidium infection andthose with cryptosporidiosis are presented in table 1.
Thirty-two episodes of recurrent symptomatic and asymptomatic cryptosporidiosis werediagnosed, not including the initial episode. Twenty-six episodes of recurrentCryptosporidium diarrhea were detected in 17 children (7.5% [29.3% of 58 with priorCryptosporidium diarrhea]); 12 had 1 recurrent episode, 2 had 2 recurrent episodes, 2 had 3recurrent episodes, and 1 had 4 recurrent episodes. Six children had recurrent asymptomaticinfection, for a total of 13 episodes. Children with symptomatic infection did not differ fromchildren with asymptomatic infection with respect to age at enrollment (47.9 vs. 50.2months) or age at the time of Cryptosporidium diagnosis (76 vs. 73.3 months).
Kirkpatrick et al. Page 3
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Among the children with symptomatic infection, 57 (75%) presented within the first day ofillness, which is a possible indication of the severity of diarrhea; almost all (56 [96.6%])presented by the third day of diarrhea. More than half (34 [58.6%]) had abdominal pain, and18.6% had vomiting at presentation. Using the Ruuska score of disease severity, 40% ofchildren with cryptosporidiosis had a score ≥6, indicating that most children had a diseaseseverity similar to that of other watery, nonrotavirus causes of diarrhea.
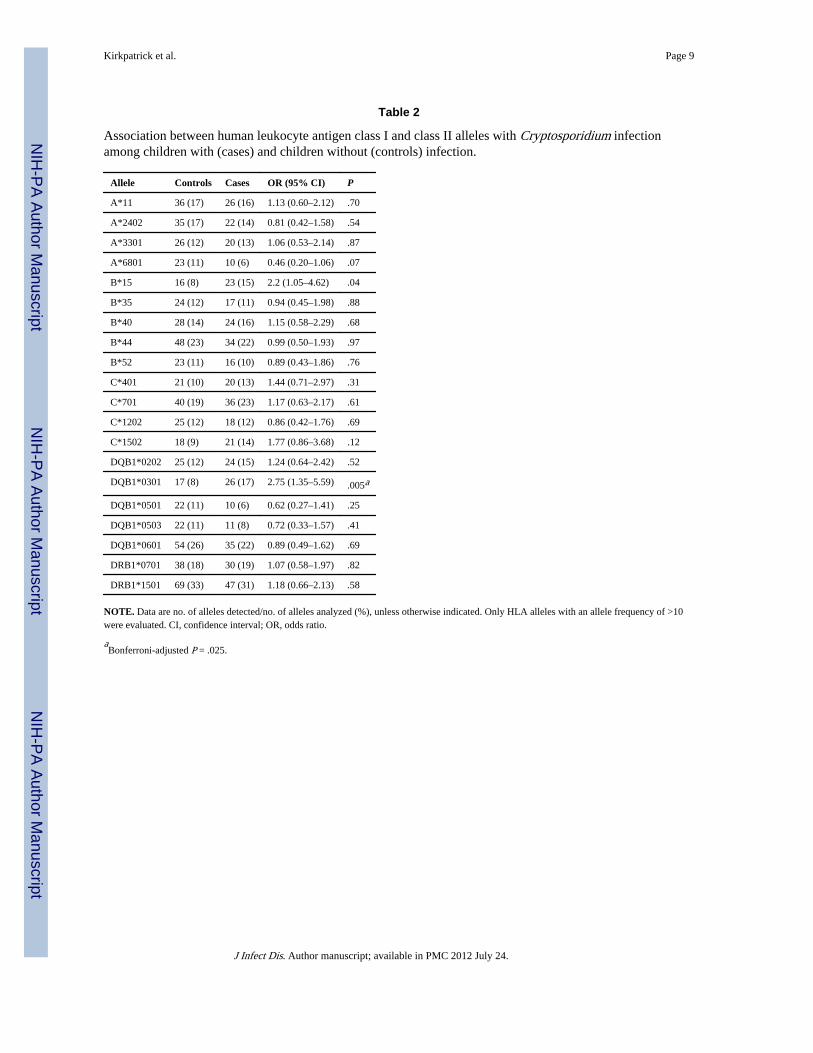
For the genetic analysis, 78 unrelated children with Cryptosporidium infection (i.e., cases)were compared to 104 children without infection (i.e., controls). For the HLA class I alleles,2 of these 182 individuals did not have sufficient DNA for complete analysis and were notincluded. There were 20 class I or II alleles with an allele frequency >10% in either thecases or the controls (table 2). For the HLA class I region, 1 allele (HLA B*15) showedstatistically significant associations with Cryptosporidium infection (OR, 2.16; P = .04). ForHLA class II, children with Cryptosporidium infection were nearly 3 times as likely thancontrols to carry the DQB1*0301 allele (OR, 2.75; P = .005 [Pcorrected = .025]).
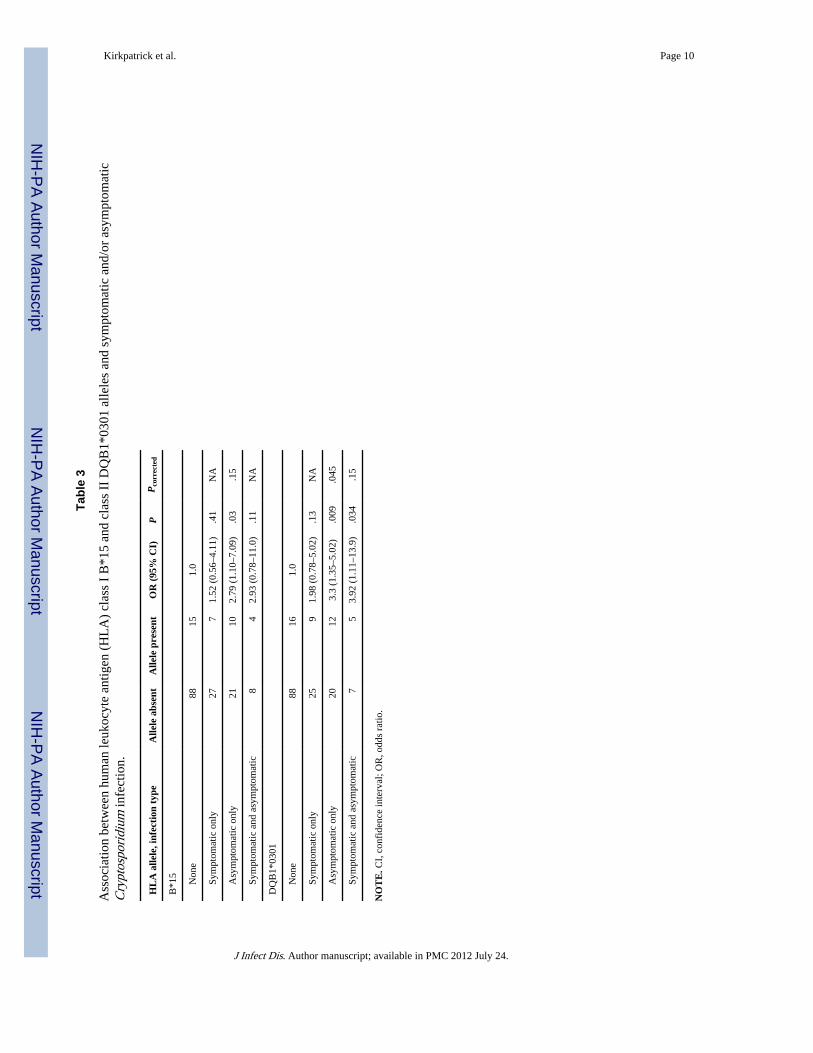
To determine whether these alleles were associated with symptomatic infection, westratified our analysis into children with no infection, children with asymptomatic infection,children with symptomatic infection, and children with both asymptomatic and symptomaticinfection (table 3). For both the HLA class I B*15 allele and the DQB1*0301 allele, theassociation persisted for children with at least 1 episode of asymptomatic Cryptosporidiuminfection. However, children with only symptomatic infection were not more likely to carrythe B*15 and/or DQB1*0301 alleles.
In addition, children who had both asymptomatic and symptomatic infection appeared toshare a haplotype with DRB1*1101 (DQB1*0301/DRB1*1101; OR, 7; P = .008 [Pcorrected= .04]). Associations with other HLA class II alleles were not found, including DQB1*0601and DRBq*1501, which have been previously described in this cohort to be associated withE. histolytica infection [11].
DISCUSSIONThe evaluation of a large, prospectively followed cohort of children offered a uniqueopportunity to evaluate the role of host genetics in susceptibility to both symptomatic andasymptomatic Cryptosporidium infection. We hypothesized that the HLA class I or II allelescould be an important component of the human immune response to Cryptosporidiuminfection. The most important findings of our work is that children with Cryptosporidiuminfection are more likely to carry the HLA class II DQB1*0301 allele (OR, 2.75) and theclass I B*15 allele (OR, 2.16). These associations were strongest in children withasymptomatic infection (DQB1*0301: OR, 3.3; B*15: OR, 2.78) and in children with bothsymptomatic and asymptomatic infection (DQB1*0301: OR, 3.92; B*15: OR, 3.2).However, children with only symptomatic infection associated with diarrhea were notassociated with these alleles. This suggests a role for these alleles in the susceptibility toasymptomatic infection. Our cohort also demonstrated an association betweenCryptosporidium infection (both symptomatic and asymptomatic) and both alleles of theHLA II *0301/DRB1*1101 haplotype (OR, 7; P = .008 [Pcorrected = .04]). However, thenumber of children with this haplotype is small in our cohort (n = 20), and further work willbe needed to determine its clinical significance in Cryptosporidium infection.
The human immune response to Cryptosporidium infection is incompletely understood, andthe severity of clinical disease varies widely by age and immune status [12]. Nevertheless,the role of cellular immunity, particularly the CD4+ T cell, in protection from and resolutionof disease has been demonstrated by the presence of cryptosporidiosis in individuals with
Kirkpatrick et al. Page 4
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
advanced AIDS and findings of CD4+ adoptive-transfer experiments in susceptible animalmodels [4, 5, 13]. The HLA-encoded MHC II molecules are equally essential to presentCryptosporidium antigens to naive CD4+ T cells. As anticipated, the severity ofCryptosporidium disease is enhanced in MHC class II–deficient mice, which are incapableof presenting antigen and activating CD4+ T cells [13].
Increased allelic frequencies of HLA II DQB1*0301 have been associated with otherintracellular pathogens, particularly the hepatitis viruses. In hepatitis C virus (HCV)infection involving both ethnically homogenous and mixed populations, DQB1*0301 isassociated with susceptibility to infection and with clearance of circulating virus [14, 15]. Incontrast, DQB1*0301 is associated with persistent infection with hepatitis B virus in apopulation of injection drug users [16]. Of interest, clearance of HCV infection is alsoassociated with DRB1*11 in linkage disequilibrium with DQB1*0301; the protective rolesof these alleles in HCV has been confirmed by a recent meta-analysis [14, 15].
The additional finding of an association between Cryptosporidium infection and the HLAclass I B*15 allele suggests that the human immune response involves the interaction ofadditional lymphocyte populations in addition to the role of CD4+ T cells. Further work onhuman populations is needed to understand the significance of the HLA class IB association,including the additional role of CD8+ T cells, natural killer (NK) cells, and other atypicallymphocyte populations (e.g., NK T cells and γδ T cells). In addition, genetic analysis ofother components of the immune response (e.g., single nucleotide polymorphisms of thecytokine genes thought to be involved in susceptibility to or control of Cryptosporidiuminfection) is needed. Further advances in high-throughput analyses of these genes, as well asgene chip assays to assess actual gene expression, will be essential to more completelyunderstand the role of these genes in Cryptosporidium infection. Larger samples sizes willalso be needed to increase the power of our observations.
By virtue of the size and follow-up duration of this cohort, our work also adds to data on thecommunity impact of Cryptosporidium infection. In particular, it highlights the differencesin disease expression between preschool-aged and grade school–aged children and the moresevere and often persistent disease found in infants and toddlers [17, 18]. Although thechildren were all beyond the age of highest incidence of infection (≤2 years of age) atenrollment, infection was still extremely common. During the first 3 years of the study, 43%of the children had an episode of Cryptosporidium infection. More than 25% of children hadcryptosporidiosis (i.e., Cryptosporidium diarrhea), and ~23% had asymptomatic disease,which was diagnosed by detection of antigen in surveillance stool specimens. Recurrentepisodes of cryptosporidiosis were found in 29.3% of children (7.5% of the totalpopulation). Unlike studies involving younger children, the incidence of infection wassimilar across age groups in this cohort [19, 20]. Abdominal pain in more than half ofchildren with cryptosporidiosis and a short duration (i.e., 3 days) of watery diarrheacharacterizes cryptosporidiosis in this population. Persistent and chronic diarrhea, a highseverity of disease (evaluated by the Ruuska score), and severe dehydration were rarelyseen.
Although we were fortunate to work with an exceptionally well-followed cohort (childrenhave been observed every other day for >6 years at the time of writing), our work hasseveral important limitations. First, children with Cryptosporidium were compared tocontrol children, all of whom had known infection or exposure to another protozoan, E.histolytica, and some of whom had coinfections with other enteric pathogens. Comparison toa control group of children with no enteric infections or coinfections, although difficult inthis population, would help confirm our data. Second, our diagnostic work on asymptomaticinfections was limited to antigen testing of frozen surveillance stool aliquots, which may
Kirkpatrick et al. Page 5
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
have underestimated the prevalence of asymptomatic infection in our cohort. Future workwill benefit from recently developed PCR-based diagnostic techniques and more-frequentsurveillance. Finally, our study evaluated only children >2 years of age and cannot addressthe impact of Cryptosporidium infection in younger members of this population. Thispotential confounding factor can only be eliminated by further work involving closeobservation of a birth cohort of children to detect their first Cryptosporidium infection.These data are necessary to clarify whether infection at a very young age has a protectiveeffect against future infections and to confirm the association between HLA alleles andinfection. Nevertheless, this work is the first human data to identify HLA genetic differencesin Cryptosporidium infection that may explain clinical disease variability, as well as a newavenue for identifying the immunodominant antigens of Cryptosporidium organisms.
AcknowledgmentsFinancial support: National Institutes of Health (awards U54 AI57168 to B.D.K. and AI0143596 to R.H. andW.A.P.); University of Vermont New Research Initiative (to B.D.K.); Intramural Research Program of the NationalHuman Genome Research Institute, National Institutes of Health (to P.D.).
References1. Petersen C. Cryptosporidiosis in patients infected with the human immunodeficiency virus. Clin
Infect Dis. 1992; 15:903–9. [PubMed: 1457661]
2. Guerrant RL. Cryptosporidiosis: an emerging, highly infectious threat. Emerg Infect Dis. 1997;3:51–7. [PubMed: 9126444]
3. McDonald V, Smith R, Robinson H, Bancroft G. Host immune responses against Cryptosporidium.Contrib Microbiol. 2000; 6:75–91. [PubMed: 10943508]
4. Flanigan T, Whalen C, Turner J, et al. Cryptosporidium infection and CD4 counts. Ann Intern Med.1992; 116:840–2. [PubMed: 1348918]
5. Perryman LE, Mason PH, Chrisp CE. Effect of spleen cell populations on resolution ofCryptosporidium parvum infection in SCID mice. Infect Immun. 1994; 62:1474–7. [PubMed:7907581]
6. Alcantara CS, Yang CH, Steiner TS, et al. Interleukin-8, tumor necrosis factor-alpha, and lactoferrinin immunocompetent hosts with experimental and Brazilian children with acquiredcryptosporidiosis. Am J Trop Med Hyg. 2003; 68:325–8. [PubMed: 12685639]
7. Kirkpatrick BD, Daniels MM, Jean SS, et al. Cryptosporidiosis stimulates an inflammatoryintestinal response in malnourished Haitian children. J Infect Dis. 2002; 186:94–101. [PubMed:12089667]
8. Haque R, Ali IM, Sack RB, Farr BM, Ramakrishnan G, Petri WA Jr. Amebiasis and mucosal IgAantibody against the Entamoeba histolytica adherence lectin in Bangladeshi children. J Infect Dis.2001; 183:1787–93. [PubMed: 11372032]
9. Haque R, Mondal D, Kirkpatrick BD, et al. Epidemiologic and clinical characteristics of acutediarrhea with emphasis on Entamoeba histolytica infections in preschool children in an urban slumof Dhaka, Bangladesh. Am J Trop Med Hyg. 2003; 69:398–405. [PubMed: 14640500]
10. Ruuska T, Vesikari T. Rotavirus disease in Finnish children: use of numerical scores for clinicalseverity of diarrhoeal episodes. Scand J Infect Dis. 1990; 22:259–67. [PubMed: 2371542]
11. Duggal P, Haque R, Roy S, et al. Influence of human leukocyte antigen class II alleles onsusceptibility to Entamoeba histolytica infection in Bangladeshi children. J Infect Dis. 2004;189:520–6. [PubMed: 14745711]
12. Theodos CM. Innate and cell-mediated immune responses to Cryptosporidium parvum. AdvParasitol. 1998; 40:87–119. [PubMed: 9554071]
13. Aguirre SA, Mason PH, Perryman LE. Susceptibility of major histocompatibility complex (MHC)class I- and MHC class II-deficient mice to Cryptosporidium parvum infection. Infect Immun.1994; 62:697–9. [PubMed: 7905464]
Kirkpatrick et al. Page 6
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

14. Minton EJ, Smillie D, Neal KR, Irving WL, Underwood JC, James V. Association between MHCclass II alleles and clearance of circulating hepatitis C virus. Members of the Trent Hepatitis CVirus Study Group. J Infect Dis. 1998; 178:39–44. [PubMed: 9652421]
15. Hong X, Yu RB, Sun NX, Wang B, Xu YC, Wu GL. Human leukocyte antigen class IIDQB1*0301, DRB1*1101 alleles and spontaneous clearance of hepatitis C virus infection: a meta-analysis. World J Gastroenterol. 2005; 11:7302–7. [PubMed: 16437632]
16. Thio CL, Carrington M, Marti D, et al. Class II HLA alleles and hepatitis B virus persistence inAfrican Americans. J Infect Dis. 1999; 179:1004–6. [PubMed: 10068598]
17. Sallon S, Deckelbaum RJ, Schmid II, Harlap S, Baras M, Spira DT. Cryptosporidium,malnutrition, and chronic diarrhea in children. Am J Dis Child. 1988; 142:312–5. [PubMed:3344720]
18. Agnew DG, Lima AA, Newman RD, et al. Cryptosporidiosis in northeastern Brazilian children:association with increased diarrhea morbidity. J Infect Dis. 1998; 177:754–60. [PubMed:9498458]
19. Mølbak K, Højlyng N, Gottschau A, et al. Cryptosporidiosis in infancy and childhood mortality inGuinea Bissau, west Africa. BMJ. 1993; 307:417–20. [PubMed: 8374453]
20. Newman RD, Sears CL, Moore SR, et al. Longitudinal study of Cryptosporidium infection inchildren in northeastern Brazil. J Infect Dis. 1999; 180:167–75. [PubMed: 10353875]
Kirkpatrick et al. Page 7
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kirkpatrick et al. Page 8
Table 1
Clinical and epidemiologic features of 226 children with symptomatic or asymptomatic Cryptosporidiuminfection.
Variable
Cryptosporidium infection type
Symptomatic (n = 58) Asymptomatic (n = 51)
Percentage of overall study group 25.7 22.6
Male sex 29 (50) 28 (54.9)
Age at diagnosis, mean ± SD, months 76 ± 26 73.3 ± 16
Episodes >1 month apart, no. 84 58
Cryptosporidium-positive stool specimens, no. 91 60
Fever 45 (49.5) NA
Abdominal pain 34 (58.6) NA
Vomiting 17 (18.7) NA
Watery stool 88 (96.7) NA
3–6 stools/day 78 (85.7) NA
≥7 stools/day 13 (14.3) NA
Mild-to-moderate dehydration 55 (60.4) NA
ORS use before diagnosis 17 (18.7) NA
Duration of diarrhea <3 days before admission 88 (96.7) NA
Ruuska score ≥6 36 (39.6) NA
Recurrent episode(s) 17 (7.5) 6 (2.6)
Recurrent episodes, no. (range) 26 (2–5) 7 (2–3)
Copathogens recovered, no. (%)a
Overall 18 (19.7) ND
Giardia lamblia 9 (9.9) ND
Shigella species 5 (5.5) ND
Aeromonas species 4 (4.4) ND
NOTE. Data are no. (%) of patients, unless otherwise indicated. NA, not applicable; ND, not done; ORS, oral rehydration solution.
aData are no. (%) recovered from 91 Cryptosporidium-positive stool specimens.
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kirkpatrick et al. Page 9
Table 2
Association between human leukocyte antigen class I and class II alleles with Cryptosporidium infectionamong children with (cases) and children without (controls) infection.
Allele Controls Cases OR (95% CI) P
A*11 36 (17) 26 (16) 1.13 (0.60–2.12) .70
A*2402 35 (17) 22 (14) 0.81 (0.42–1.58) .54
A*3301 26 (12) 20 (13) 1.06 (0.53–2.14) .87
A*6801 23 (11) 10 (6) 0.46 (0.20–1.06) .07
B*15 16 (8) 23 (15) 2.2 (1.05–4.62) .04
B*35 24 (12) 17 (11) 0.94 (0.45–1.98) .88
B*40 28 (14) 24 (16) 1.15 (0.58–2.29) .68
B*44 48 (23) 34 (22) 0.99 (0.50–1.93) .97
B*52 23 (11) 16 (10) 0.89 (0.43–1.86) .76
C*401 21 (10) 20 (13) 1.44 (0.71–2.97) .31
C*701 40 (19) 36 (23) 1.17 (0.63–2.17) .61
C*1202 25 (12) 18 (12) 0.86 (0.42–1.76) .69
C*1502 18 (9) 21 (14) 1.77 (0.86–3.68) .12
DQB1*0202 25 (12) 24 (15) 1.24 (0.64–2.42) .52
DQB1*0301 17 (8) 26 (17) 2.75 (1.35–5.59) .005a
DQB1*0501 22 (11) 10 (6) 0.62 (0.27–1.41) .25
DQB1*0503 22 (11) 11 (8) 0.72 (0.33–1.57) .41
DQB1*0601 54 (26) 35 (22) 0.89 (0.49–1.62) .69
DRB1*0701 38 (18) 30 (19) 1.07 (0.58–1.97) .82
DRB1*1501 69 (33) 47 (31) 1.18 (0.66–2.13) .58
NOTE. Data are no. of alleles detected/no. of alleles analyzed (%), unless otherwise indicated. Only HLA alleles with an allele frequency of >10were evaluated. CI, confidence interval; OR, odds ratio.
aBonferroni-adjusted P = .025.
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Kirkpatrick et al. Page 10
Tabl
e 3
Ass
ocia
tion
betw
een
hum
an le
ukoc
yte
antig
en (
HL
A)
clas
s I
B*1
5 an
d cl
ass
II D
QB
1*03
01 a
llele
s an
d sy
mpt
omat
ic a
nd/o
r as
ympt
omat
icC
rypt
ospo
ridi
um in
fect
ion.
HL
A a
llele
, inf
ecti
on t
ype
Alle
le a
bsen
tA
llele
pre
sent
OR
(95
% C
I)P
Pco
rrec
ted
B*1
5
N
one
8815
1.0
Sy
mpt
omat
ic o
nly
277
1.52
(0.
56–4
.11)
.41
NA
A
sym
ptom
atic
onl
y21
102.
79 (
1.10
–7.0
9).0
3.1
5
Sy
mpt
omat
ic a
nd a
sym
ptom
atic
84
2.93
(0.
78–1
1.0)
.11
NA
DQ
B1*
0301
N
one
8816
1.0
Sy
mpt
omat
ic o
nly
259
1.98
(0.
78–5
.02)
.13
NA
A
sym
ptom
atic
onl
y20
123.
3 (1
.35–
5.02
).0
09.0
45
Sy
mpt
omat
ic a
nd a
sym
ptom
atic
75
3.92
(1.
11–1
3.9)
.034
.15
NO
TE
. CI,
con
fide
nce
inte
rval
; OR
, odd
s ra
tio.
J Infect Dis. Author manuscript; available in PMC 2012 July 24.
Related Documents











