Assessment of Myocardial Ischemia and Viability Using Cardiac Magnetic Resonance Nuno Bettencourt, MD, Amedeo Chiribiri, MD, Andreas Schuster, MD, and Eike Nagel, MD, PhD Corresponding author Eike Nagel, MD, PhD Division of Imaging Sciences, King’s College London British Heart Foundation Centre, National Institute for Health Research Biomedical Research Centre at Guy’s and Saint Thomas’ National Health Service Foundation Trust, The Rayne Institute, 4th Floor Lambeth Wing, Saint Thomas’ Hospital, London SE1 7EH, United Kingdom. E-mail: [email protected] Current Heart Failure Reports 2009, 6: 142–153 Current Medicine Group LLC ISSN 1546-9530 Copyright © 2009 by Current Medicine Group LLC In the past decade, cardiac magnetic resonance (CMR) has evolved dramatically. Its clinical appli- cations are now a major tool in the diagnosis and prognostic assessment of patients with ischemic heart disease. CMR can be used for detection and quantification of ischemia and for viability assess- ment using different techniques that are now well validated. Scar can be easily detected using contrast enhancement (late gadolinium enhancement). Isch- emia detection is usually achieved with stress CMR techniques, whereas prediction for the recovery of function (detection of dysfunctional but viable myo- cardial segments) can be deduced from scar and stress imaging. Although determination of which approach is better may depend on the population group, the major advantage of CMR is the ability to integrate different information about anatomy, wall motion, myocardial perfusion, and tissue characterization in a single comprehensive examination. Introduction Coronary artery disease (CAD) is one of the leading causes of death in industrialized countries. Because CAD is associated with high mortality and morbidity, most efforts must be aimed at detecting early stages of disease and preventing myocardial damage. However, when ischemic heart disease (IHD) is established, an accurate prediction of potential reversibility and benefit of myo- cardial revascularization is crucial. As first described by Rahimtoola [1], areas of dysfunctional myocardium at rest may represent scar or viable (hibernating or stunned) myocardium. Although scar may provide a substrate for ventricular tachyarrhythmia and does not benefit from revascularization, dysfunctional viable tissue is at higher risk of infarction and is capable of recovering function after revascularization. Differentiation of these conditions is therefore of major importance in the risk assessment and management of IHD. Cardiovascular magnetic resonance (CMR) is a com- prehensive examination that can provide left and right global and regional ventricular function, myocardial per- fusion, presence and extent of scar and, to some extent, the anatomy of the coronary arteries within a single study. Due to this integrating unique feature, allied to a high spa- tial resolution and absence of ionizing radiation, CMR is increasingly used in the assessment of CAD and viability. The diagnosis of CAD using CMR is based on two aspects: 1) assessment of ischemia, and 2) identifica- tion of myocardial scar compatible with an established myocardial infarction (MI). Ischemia assessment can be performed using two different CMR techniques: 1) first- pass myocardial perfusion imaging (perfusion CMR), or 2) detection of inducible wall motion abnormalities (WMA) under stress—most frequently pharmacologic stress with high-dose dobutamine (high-dose dobutamine stress magnetic resonance [DSMR]). Scar is visualized using the late gadolinium enhancement (LGE) technique. Detection of viability can also be achieved using two different magnetic resonance techniques: 1) low-dose DSMR, using the contractile reserve of viable myocar- dium to differentiate it from scar or nonnecrotic tissue without the ability to contract; and 2) the presence and transmurality of scar can be assessed with LGE and viable myocardium defined as dysfunctional but nonscared tissue. In 2006, the American College of Cardiology Founda- tion and specialized societies considered the appropriate indications for the use of CMR in the assessment of CAD and viability [2]. CMR is indicated for the diagnosis of ischemia in patients with chest pain and an intermediate

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Assessment of Myocardial Ischemia and Viability Using Cardiac Magnetic ResonanceNuno Bettencourt, MD, Amedeo Chiribiri, MD, Andreas Schuster, MD, and Eike Nagel, MD, PhD
Corresponding authorEike Nagel, MD, PhD
Division of Imaging Sciences, King’s College London
British Heart Foundation Centre, National Institute for
Health Research Biomedical Research Centre at Guy’s
and Saint Thomas’ National Health Service Foundation Trust,
The Rayne Institute, 4th Floor Lambeth Wing, Saint Thomas’
Hospital, London SE1 7EH, United Kingdom.
E-mail: [email protected]
Current Heart Failure Reports 2009, 6:142–153Current Medicine Group LLC ISSN 1546-9530
Copyright © 2009 by Current Medicine Group LLC
In the past decade, cardiac magnetic resonance (CMR) has evolved dramatically. Its clinical appli-cations are now a major tool in the diagnosis and prognostic assessment of patients with ischemic heart disease. CMR can be used for detection and quantifi cation of ischemia and for viability assess-ment using different techniques that are now well validated. Scar can be easily detected using contrast enhancement (late gadolinium enhancement). Isch-emia detection is usually achieved with stress CMR techniques, whereas prediction for the recovery of function (detection of dysfunctional but viable myo-cardial segments) can be deduced from scar and stress imaging. Although determination of which approach is better may depend on the population group, the major advantage of CMR is the ability to integrate different information about anatomy, wall motion, myocardial perfusion, and tissue characterization in a single comprehensive examination.
IntroductionCoronary artery disease (CAD) is one of the leading causes of death in industrialized countries. Because CAD is associated with high mortality and morbidity, most efforts must be aimed at detecting early stages of disease and preventing myocardial damage. However, when ischemic heart disease (IHD) is established, an accurate prediction of potential reversibility and benefi t of myo-
cardial revascularization is crucial. As fi rst described by Rahimtoola [1], areas of dysfunctional myocardium at rest may represent scar or viable (hibernating or stunned) myocardium. Although scar may provide a substrate for ventricular tachyarrhythmia and does not benefi t from revascularization, dysfunctional viable tissue is at higher risk of infarction and is capable of recovering function after revascularization. Differentiation of these conditions is therefore of major importance in the risk assessment and management of IHD.
Cardiovascular magnetic resonance (CMR) is a com-prehensive examination that can provide left and right global and regional ventricular function, myocardial per-fusion, presence and extent of scar and, to some extent, the anatomy of the coronary arteries within a single study. Due to this integrating unique feature, allied to a high spa-tial resolution and absence of ionizing radiation, CMR is increasingly used in the assessment of CAD and viability.
The diagnosis of CAD using CMR is based on two aspects: 1) assessment of ischemia, and 2) identifi ca-tion of myocardial scar compatible with an established myocardial infarction (MI). Ischemia assessment can be performed using two different CMR techniques: 1) fi rst-pass myocardial perfusion imaging (perfusion CMR), or 2) detection of inducible wall motion abnormalities (WMA) under stress—most frequently pharmacologic stress with high-dose dobutamine (high-dose dobutamine stress magnetic resonance [DSMR]). Scar is visualized using the late gadolinium enhancement (LGE) technique.
Detection of viability can also be achieved using two different magnetic resonance techniques: 1) low-dose DSMR, using the contractile reserve of viable myocar-dium to differentiate it from scar or nonnecrotic tissue without the ability to contract; and 2) the presence and transmurality of scar can be assessed with LGE and viable myocardium defi ned as dysfunctional but nonscared tissue.In 2006, the American College of Cardiology Founda-tion and specialized societies considered the appropriate indications for the use of CMR in the assessment of CAD and viability [2]. CMR is indicated for the diagnosis of ischemia in patients with chest pain and an intermediate

Assessment of MI and Viability Using CMR I Bettencourt et al. I 143
pretest probability of CAD, in whom the electrocardio-gram is not interpretable or who are unable to exercise. CMR is also indicated for post-test assessment of patients with coronary lesions of unclear functional signifi cance detected on coronary angiography. Furthermore, CMR is indicated in the evaluation of viability before revascu-larization and in the evaluation of the extent of necrosis following MI.
In the past decade, CMR developed into an attrac-tive tool for the assessment and follow-up of patients with IHD and is slowly becoming clinical routine in the evaluation of patients with known or suspected CAD. This article reviews CMR applications in the evaluation of myocardial ischemia and myocardial viability based on DSMR, perfusion CMR, and LGE.
Dobutamine Stress Magnetic ResonanceDobutamine is a sympathomimetic amine that acts through α- and β-adrenoceptor–inducing inotropic and chronotropic effects, as well as enhancing myocardial blood fl ow. It mimics the physiologic effects of exercise and refl ects a measure of metabolic demand ischemia. Dobutamine is usually well tolerated and has a favorable safety profi le. At higher doses, however, it may cause chest discomfort, arrhythmia, and myocardial ischemia. Major adverse events, including ventricular tachycardia, ventricular fi brillation, and MI, have been described in 0.3% of high-dose protocols. Contraindications include severe arterial hypertension, unstable angina, aortic ste-nosis, severe arrhythmias, obstructive cardiomyopathy, and acute myocarditis [3].
When administered at a low dose, dobutamine improves the contractility of hibernating myocardium (viable myocardium with impaired contraction at rest). At higher doses, the increasing myocardial oxygen demand results in ischemia in territories supplied by stenotic coro-nary arteries—inducing or worsening regional WMA.
Like dobutamine stress echocardiography (DSE), DSMR is based on the detection of wall motion changes in the cine images acquired during dobutamine infusion, taking advantage of this dual phase myocardial response to increasing doses. It can be used to detect viable hiber-nating myocardium (low-dose DSMR) or to unmask ischemia (high-dose DSMR). DSMR has a safety profi le similar to DSE [4], with the advantage of reaching a bet-ter image quality in a higher proportion of patients [5].
High-dose DSMRHigh-dose DSMR is used to diagnose myocardial isch-emia. Myocardial segments supplied by coronary arteries with signifi cant stenoses tend to develop or aggravate WMA as oxygen demand and workload increase under high-dose dobutamine stress. Ischemia is therefore defi ned as segments presenting new or worsening WMA.
During a high-dose DSMR protocol, a gradual increase of the dobutamine infusion rate—with step
increments of 10 μg/kg/min (starting at 10 μg/kg/min until a maximum of 40 μg/kg/min)—is used. Atropine may be added at peak dobutamine infusion if 85% of the maximum predicted heart rate is not achieved. Infusion is stopped when the target heart rate is reached [(220 – age) × 0.85], if new or worsening WMA develop, or in case of patient intolerance, intractable symptoms, or signifi cant changes in blood pressure [3].
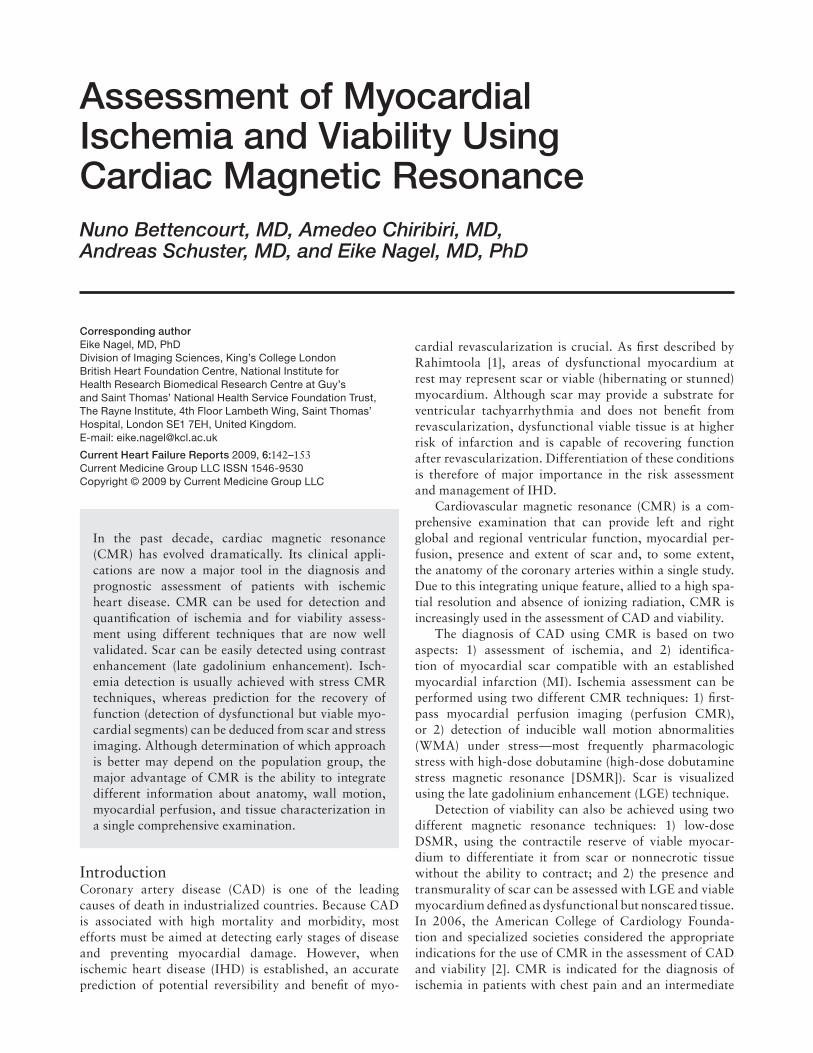
Accuracy in the diagnosis of CADSince DSMR was fi rst described, several studies have been published about its accuracy for detection of signifi cant CAD as assessed by catheter coronary angiography (Table 1).
A recent meta-analysis published by Nandalur et al. [6••] showed that high-dose DSMR had a sensitivity of 83% and a specifi city of 86% in a population of 735 patients with a CAD prevalence of 70.5%. On a coronary territory-level analysis, WMA analysis had a sensitivity of 79% and a specifi city of 93%.
DSMR has been shown to be superior to DSE, in detection of CAD. Nagel et al. [7] found that detection of WMA by DSMR provided a signifi cantly higher diagnostic accuracy compared with DSE. The superior performance of DSMR was mainly explained by the better image quality obtained at peak stress, particularly in patients with poor echocardiographic windows [5]. However, visual assess-ment might lead to different interpretation of the studies and requires adequate, time-consuming training. The addition of tagging to high-dose DSMR allows the use of quantitative methods and may improve analysis time and overall accuracy, potentially decreasing interobserver and intraobserver variability. It may also provide additional parameters, such as untwisting, that are currently under investigation and may prove to be useful for the study of ischemia and viability. Myocardial tagging during DSMR allows detection of more inducible WMA than the standard approach [8]. Recently, Korosoglou et al. [9] studied 65 patients with suspected or known CAD undergoing high-dose DSMR. Compared with visual assessment (sensitivity, 70%; specifi city, 95%), both conventional tagging and strain-encoded MRI had higher sensitivity for detection of CAD (81% and 89%, respectively), whereas specifi city was equally high (96% and 94%, respectively).
ReproducibilityLow interobserver variability and a high reproducibility for the detection of inducible WMA have been reported for high-dose DSMR. Syed et al. [10] studied 19 patients with class III/IV Canadian Cardiovascular Society angina undergoing two DSMR tests on separate occasions. WMA were found to be highly reproducible between the studies. Interobserver variability was also analyzed, yielding a κ value of 0.81.
In a multicenter study, 150 consecutive DSMR stud-ies were blindly analyzed by four different readers, and interobserver variability for the identifi cation of WMA was low, occurring in one of seven examinations [11].
144 I Imaging and Diagnostics
Tabl
e 1.
Dia
gnos
tic
accu
racy
of C
MR
(hi
gh-d
ose
DSM
R a
nd p
erfu
sion
CM
R)
for
dete
ctio
n of
CA
D*
usin
g C
A a
s st
anda
rd
Stud
yYe
arPa
tien
ts,
nIn
clus
ion
CA
D,
%Se
nsit
ivit
y,
%Sp
ecifi
city
, %
Com
men
ts
Hig
h-do
se
DSM
RPe
nnel
l et a
l. [5
7]19
9225
Exer
tiona
l che
st p
ain
and
abno
rmal
ETT
8891
100
–
van
Rugg
e et
al.
[58]
1993
45H
igh-
risk
patie
nts
refe
rred
for
CA
8281
100
Dos
es u
p to
20
μg/k
g/m
in
van
Rugg
e et
al.
[59]
1994
39–
8591
83Q
uant
itativ
e D
SMR
ana
lysi
s
Bae
r et
al.
[60]
1994
32K
now
n C
AD
100
84–
Com
paris
on v
s Tc
-SPE
CT
Nag
el e
t al.
[8]
1999
172
P re
ferr
ed fr
om C
A62
8686
–
Hun
dley
et a
l. [6
1]19
9941
Patie
nts
with
poo
r ac
oust
ic w
indo
w85
8383
Onl
y 4
1 pa
tient
s un
derw
ent C
A
(sel
ectio
n bi
as)
van
Dijk
man
et
al.
[62]
2002
42Su
spec
ted
CA
D p
lus
inco
nclu
sive
ETT
or
ST
abno
rmal
ities
on
rest
ing
ECG
9898
98O
nly
the
42 p
atie
nts
with
DSM
R
unde
rwen
t CA
(sel
ectio
n bi
as)
Paet
sch
et a
l. [6
3]20
0479
Susp
ecte
d or
kno
wn
CA
D67
8089
–
Wah
l et a
l. [6
4]20
0415
9Po
st-r
evas
cula
rizat
ion
7489
84Q
uant
itativ
e C
A a
naly
sis
Jahn
ke e
t al.
[65]
2006
40–
7083
87Kt
-Bla
st (4
0% re
duct
ion
in a
cqui
sitio
n tim
e)
Koro
sogl
ou e
t al.
[9]
2009
65Su
spec
ted
or k
now
n C
AD
6289
94St
rain
-enc
oded
imag
ing
Nan
dula
r et
al.
[6••
]20
0773
5–
7183
86M
eta-
anal
ysis
*CA
D d
efi n
ed a
s pr
esen
ce o
f ste
nosi
s >
50%
in c
oron
ary
angi
ogra
phy,
unl
ess
othe
rwis
e st
ated
.† F
or d
etec
tion
of s
teno
ses
≥ 70
% (5
0% le
ft m
ain)
AC
S—ac
ute
coro
nary
syn
drom
e; C
A—
cath
eter
cor
onar
y an
giog
raph
y; C
AD
—co
rona
ry a
rter
y di
seas
e; C
MR
—ca
rdia
c m
agne
tic r
eson
ance
; DSM
R—
dobu
tam
ine
stre
ss m
agne
tic r
eson
ance
; EC
G—
elec
troc
ardi
ogra
m; E
TT—
exer
cise
trea
dmill
test
; Gd—
gado
liniu
m c
hela
te c
ontr
ast a
gent
; MI—
myo
card
ial i
nfar
ctio
n; M
PR—
myo
card
ial p
erfu
sion
res
erve
; per
fusi
on C
MR
—m
agne
tic
reso
nanc
e ca
rdia
c fi r
st-p
ass
perf
usio
n; S
PEC
T—si
ngle
pho
ton
emis
sion
com
pute
d to
mog
raph
y.
Assessment of MI and Viability Using CMR I Bettencourt et al. I 145
Tabl
e 1.
Dia
gnos
tic
accu
racy
of C
MR
(hi
gh-d
ose
DSM
R a
nd p
erfu
sion
CM
R)
for
dete
ctio
n of
CA
D*
usin
g C
A a
s st
anda
rd
Stud
yYe
arPa
tien
ts,
nIn
clus
ion
CA
D,
%Se
nsit
ivit
y,
%Sp
ecifi
city
, %
Com
men
ts
Low
-dos
e D
SMR
Ishi
da e
t al.
[29]
2003
104
Refe
rred
to C
A a
nd n
o pr
evio
us M
I74
9085
Subg
roup
of 6
9 pa
tient
s co
mpa
red
with
SP
ECT
Pilz
et a
l. [6
6]20
0617
1C
lass
II in
dica
tion
for
CA
6696
83–
Taka
se e
t al.
[67]
2004
102
Susp
ecte
d or
kno
wn
CA
D75
9385
Dip
yrid
amol
e
Doy
le e
t al.
[68]
2003
184
Wom
en a
nd s
ympt
oms
1457
78–
Nag
el e
t al.
[69]
2003
84Pa
tient
s re
ferr
ed fo
r C
A51
8890
Eval
uatio
n of
MPR
Plei
n et
al.
[27]
2004
68N
on-S
T se
gmen
t ele
vatio
n A
CS
82*
88*
93*
Perf
usio
n C
MR
vs
com
preh
ensi
ve C
MR
Plei
n et
al.
[70]
2005
82Su
spec
ted
or k
now
n C
AD
64*
88*
82*
Sens
itivi
ty-e
ncod
ing
(SEN
SE) t
urbo
gr
adie
nt e
cho
MR
I
Kle
m e
t al.
[26]
2006
92Su
spec
ted
CA
D40
*84
*58
*Pe
rfus
ion
CM
R v
s co
mpr
ehen
sive
CM
R
Wol
ff et
al.
[71]
2004
75Pa
tient
s re
ferr
ed fo
r C
A49
*93
*75
*M
ultic
ente
r st
udy.
Opt
imal
Gd
dose
(v
isua
l ass
essm
ent)
= 0
.05
mm
ol/k
g
Gia
ng e
t al.
[72]
2004
80Su
spec
ted
or k
now
n C
AD
6591
78M
ultic
ente
r st
udy.
Opt
imal
Gd
dose
(s
emi-
qual
itativ
e) =
0.1
–0.1
5 m
mol
/kg
Schw
itter
et
al.
[32•
•]20
0822
8Pa
tient
s re
ferr
ed fo
r C
A
and/
or S
PEC
T76
8567
Mul
ticen
ter
stud
y. O
ptim
al G
d do
se
(vis
ual a
sses
smen
t) =
0.1
–0.1
5 m
mol
/kg
Nan
dalu
r et
al.
[6••
]20
0711
83–
5791
81M
eta-
anal
ysis
*CA
D d
efi n
ed a
s pr
esen
ce o
f ste
nosi
s >
50%
in c
oron
ary
angi
ogra
phy,
unl
ess
othe
rwis
e st
ated
.† F
or d
etec
tion
of s
teno
ses
≥ 70
% (5
0% le
ft m
ain)
AC
S—ac
ute
coro
nary
syn
drom
e; C
A—
cath
eter
cor
onar
y an
giog
raph
y; C
AD
—co
rona
ry a
rter
y di
seas
e; C
MR
—ca
rdia
c m
agne
tic r
eson
ance
; DSM
R—
dobu
tam
ine
stre
ss m
agne
tic r
eson
ance
; EC
G—
elec
troc
ardi
ogra
m; E
TT—
exer
cise
trea
dmill
test
; Gd—
gado
liniu
m c
hela
te c
ontr
ast a
gent
; MI—
myo
card
ial i
nfar
ctio
n; M
PR—
myo
card
ial p
erfu
sion
res
erve
; per
fusi
on C
MR
—m
agne
tic
reso
nanc
e ca
rdia
c fi r
st-p
ass
perf
usio
n; S
PEC
T—si
ngle
pho
ton
emis
sion
com
pute
d to
mog
raph
y.
(Con
tinue
d)

146 I Imaging and Diagnostics
Prognosis assessmentIn recent years, several studies evaluated the prognostic value of high-dose DSMR. In a study of 279 patients with poor echocardiographic windows, Hundley et al. [12] found that evidence of MI in patients with left ventricular (LV) ejection fraction (LVEF) greater than 40% identifi ed subjects at risk for MI and cardiac death independently from any other risk factor, with a risk of events similar to patients with LVEF less than 40% without signs of isch-emia. Patients without inducible ischemia and with LVEF greater than 40% had an excellent cardiac prognosis in the 2 years following the CMR examination. High-dose DSMR has also been tested for preoperative risk assess-ment and proved to be an independent predictor of cardiac events during or after noncardiac surgery [13].
A recent study by Dall’Armellina et al. [14•] followed 200 patients with an LVEF level lower than 55% for an average of 5 years after DSMR. In the subgroup of patients with mild impairment of LV function (LVEF, 40%–55%), resting and stress-induced changes in LV wall motion score index during DSMR identifi ed patients with higher risk of adverse cardiac events, independent of conventional CAD risk factors. In the subgroup of patients with LVEF lower than 40%, an increase of this index did not forecast MI or cardiac death to a greater degree than LVEF at rest alone. In this subgroup, other CMR parameters, such as the pattern of LGE or perfusion, may help in prognostic stratifi cation.
Recently, Jahnke et al. [15••] evaluated 513 patients with known or suspected CAD using DSMR, as well as perfusion CMR. Patients were followed-up for an average period of 2.3 years. Myocardial ischemia detected by per-fusion CMR or DSMR identifi ed patients at high risk for subsequent cardiac death or nonfatal MI. Patients with nor-mal DSMR had low event rates (1.2%, 2.6%, and 3.3% at 1, 2, and 3 years, respectively). However, even lower event rates were observed with a negative perfusion CMR study (0.7%, 0.7%, and 2.3%, respectively). Perfusion defi cit is an earlier event in the ischemic cascade, which may explain this fi nding. Both results were superior to clinical data and rest wall motion assessment, including baseline LVEF, in terms of prognosis. In multivariate analysis, an abnormal stress test remained the only independent predictor of events. An abnormal perfusion CMR or DSMR meant a risk increase of 12- or 5-fold, respectively.
Low-dose DSMRLow-dose DSMR (5–10 μg/kg/min) is used for the assess-ment of myocardial viability in patients with established IHD and WMA at rest. The assessment of viable myocar-dium and differentiation from scarred tissue is essential for therapy optimization and decision on eventual revas-cularization procedures. Hibernating myocardium is deducted to be present in the myocardial segments with impaired contraction at rest that improves function dur-ing low-dose DSMR. DSMR can be used as an alternative to LGE—especially in patients in which contrast is con-traindicated—or as a complement to this technique.
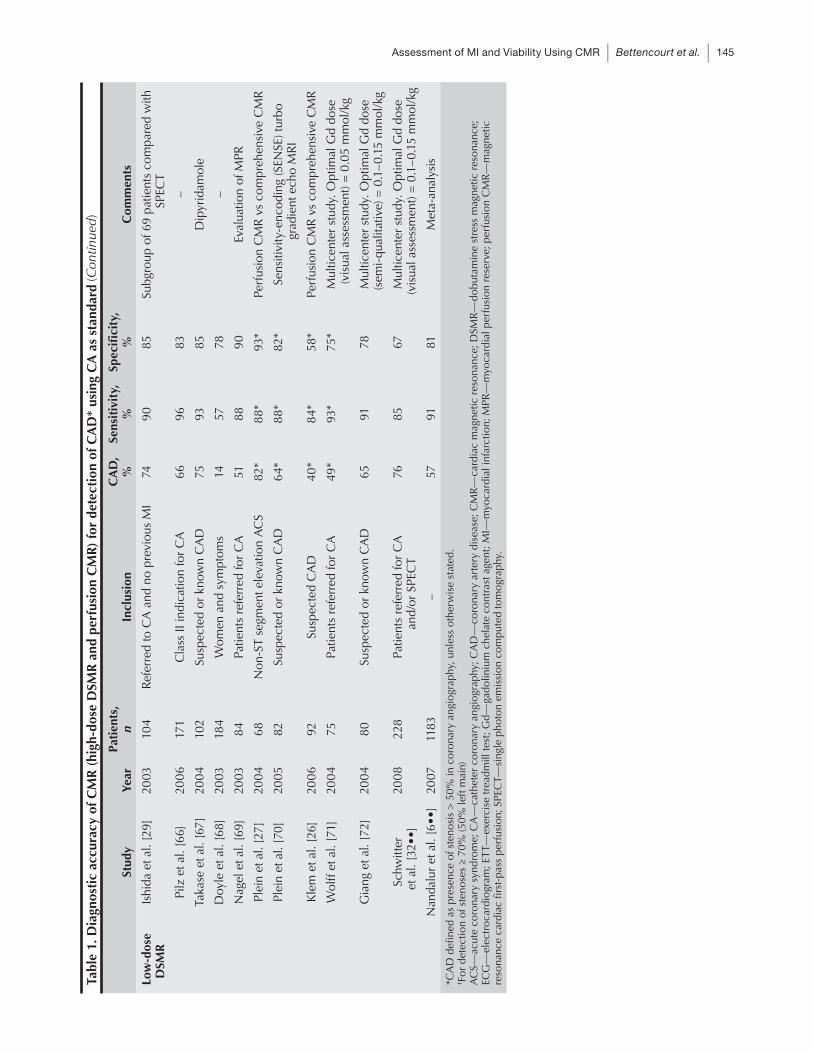
Several studies evaluated the value of low-dose DSMR for the prediction of WMA recovery after revascular-ization (Table 2). Evaluation of viability with low-dose DSMR has also been compared with the assessment of scar as evaluated by the LGE technique. Rerkpat-tanapipat et al. [16] showed that response to dobutamine was inversely related to the extent and transmurality of LGE. Wellnhofer et al. [17] found that contractile reserve with low-dose DSMR was superior to LGE in predicting improvement in wall motion after revascularization. This was especially relevant in segments with intermediate scar transmurality (1%–75%). In contrast, Gutberlet et al. [18] found that LGE was a better predictor of recov-ery; both CMR techniques were superior to thallium-201 (TI-201)–gated single photon emission computed tomog-raphy (SPECT). Bove et al. [19] studied 15 patients with multivessel CAD and LV systolic dysfunction and found that in segments with an intermediate LGE transmural-ity (1%–50%), recruitment under low-dose dobutamine identifi es those with greater functional recovery. These fi ndings may justify an integrated CMR approach using low-dose DSMR and LGE for viability detection.
Bree et al. [20] studied low-dose DSMR myocardial tagging with three-dimensional analysis in 16 normal volunteers and 14 patients with ischemic cardiomyopa-thy. Regional circumferential strain in viable segments increased signifi cantly in response to dobutamine but did not change in nonviable segments, suggesting that systolic strain during low-dose DSMR could be useful for identifi -cation of viability.
Cardiac Magnetic Resonance Myocardial PerfusionPerfusion CMR aims to detect myocardial ischemia through identifi cation of perfusion imbalances during pharmacologic stress that are not present at rest. Myo-cardial perfusion is imaged during a fi rst-pass transit of contrast media through the heart muscle.
Perfusion CMR was fi rst introduced in 1990 and is currently being extensively studied as a modality that may improve detection of myocardial perfusion defects com-pared with started SPECT imaging. Whereas angiography demonstrates the luminal narrowing of the coronary arteries without information on their hemodynamic signifi cance, perfusion CMR detects the downstream microvascular blood fl ow within the myocardium. Other noninvasive tests currently used to detect reduced myo-cardial blood fl ow, including SPECT, echocardiography, or positron emission tomography (PET), are limited by relatively poor image resolution and exposure to ioniz-ing radiation. CMR offers better image detail, does not expose patients to harmful radiation, and has been favor-ably compared with these techniques.
Adenosine is the usual pharmacologic stressor used in perfusion CMR. It binds to membrane-bound receptors inducing vascular smooth muscle relaxation. Dipyridam-
Assessment of MI and Viability Using CMR I Bettencourt et al. I 147
ole, another commonly used stressor, acts by inhibiting the reuptake of endogenous adenosine. Both drugs result in coronary vasodilation, increasing the downstream coronary blood fl ow of normal coronary arteries by a fac-tor of 3 to 5. However, they do not increase blood fl ow downstream to stenotic arteries as the arteriolar beds are already maximally dilated. In this way, the inhomogeneous distribution of signal during stress allows identifi cation of hypoperfused myocardium distal to a signifi cant stenosis.
Dobutamine may also be used for perfusion assessment and, despite the associated increase of heart rate with potential negative effects in image quality, has the advan-tage of enabling the combined assessment of WMA [21]. In clinical practice, however, adenosine (140 μg/kg/min) is usually the preferred pharmacologic agent for perfusion CMR mainly because of its excellent safety profi le and patient tolerance. The most common side effects include fl ushing, shortness of breath, and chest discomfort. More
Table 2. CMR (low-dose DSMR and LGE) for prediction of myocardial functional recovery (per segment analysis)
Study YearPatients,
nMean LVEF
Recovery, %
Sensitivity, %
Specifi city, %
Follow-up CMR after revascularization,
mo
Low-dose DSMR
Baer et al. [73]
1995 35 42 52 81 95 No follow-up. FDG-PET as
gold standard
Dendale et al. [74]
1998 26 45 50 85 68 3–4
Gunning et al. [75]
1998 23 24 57 50 81 3–6
Sayad et al. [76]
1998 10 NA 69 89 93 1–2
Baer et al. [77]
1998 43 41 46 89 94 4–6
Geskin et al. [78]
1998 20 NA 46 87 43 2
Sandstede et al. [79]
1999 25 NA 51 61 90 3–6
Baer et al. [80]
2000 52 41 50 86 92 5
Trent et al. [81]
2000 25 53 40 71 70 3–6
Lauerma et al. [82]
2000 10 44 66 79 93 6
Wellnhofer et al. [17]
2004 29 32 NA 75 93 3
Gutberlet et al. [18]
2005 20 29 86 88 90 6
LGE Kim et al. [37]
2000 41 43 53 97 44 2–3
Lauerma et al. [82]
2000 10 44 66 62 98 6
Selvanayagan et al. [83]
2004 52 62 59 95 26 6
Wellnhofer et al. [17]
2004 29 32 NA 90 52 3
Gutberlet et al. [18]
2005 20 29 86 99 94 6
Beek et al. [47]
2009 37 38 28 70 65 6
CMR—cardiac magnetic resonance; DSMR—dobutamine stress magnetic resonance; FDG-PET—fl udeoxyglucose–positron emission tomography; LGE—late gadolinium enhancement; LVEF—left ventricular ejection fraction; perfusion CMR—magnetic resonance cardiac fi rst-pass perfusion.

148 I Imaging and Diagnostics
serious side effects of bronchospasm and atrioventricular block are rare and rapidly reversed after stopping adenosine infusion. Contraindications to adenosine administration include unstable angina, severe hypotension (systolic blood pressure < 90 mm Hg), uncontrolled asthma or severe chronic obstructive pulmonary disease, and second- or third-degree atrioventricular block [3].
The evaluation of myocardial perfusion during the fi rst passage of gadolinium-based contrast is usually made with three to six slices continuously imaged in every heart beat. This approach allows coverage of 16 segments of the heart, maintaining a high temporal resolution. Ischemic myocardium with reduced perfusion has a slightly slower uptake of gadolinium and, therefore, appears darker com-pared with normal myocardium.
It is now possible to achieve an in-plane resolution of 1 to 3 mm × 1 to 3 mm, allowing differentiation between endocardial and epicardial perfusion. This may be use-ful for the detection of smaller subendocardial perfusion defects that might be missed by other diagnostic modali-ties. Stress perfusion imaging may be followed by rest perfusion imaging and analysis can be performed by visual assessment or by quantitative and semiquantita-tive methods. Findings should then be integrated with the information obtained from resting cine imaging and LGE to improve diagnostic accuracy.
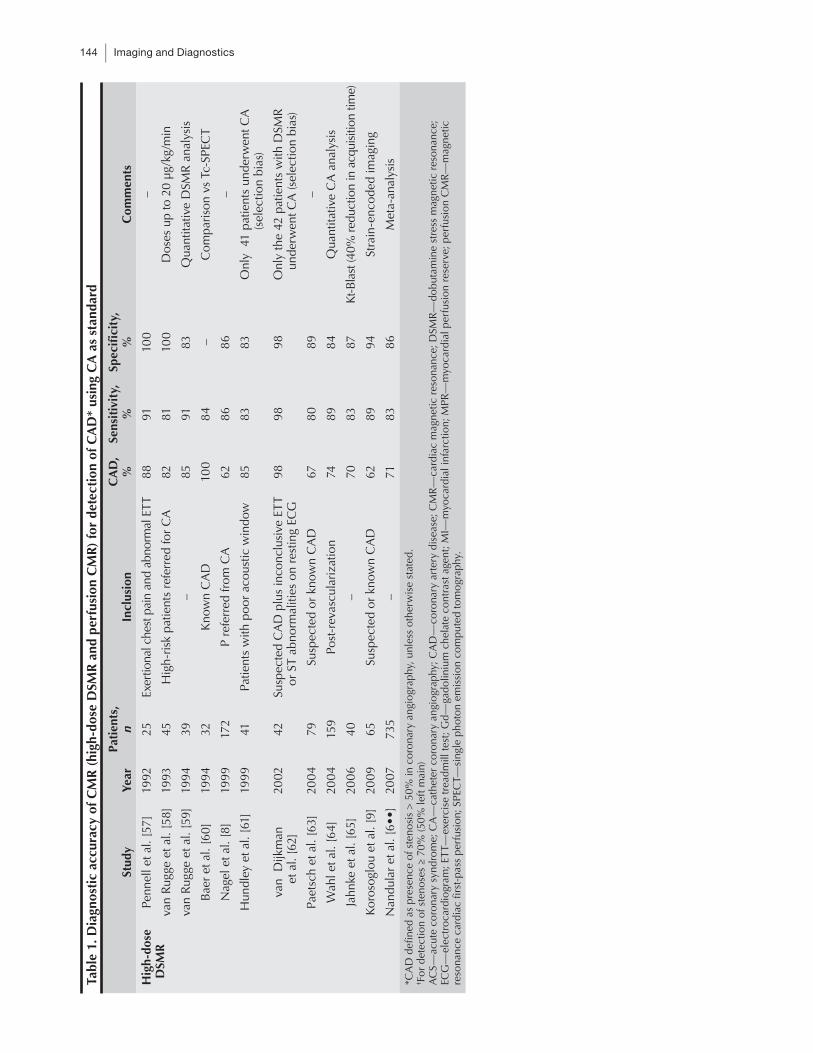
Accuracy in the diagnosis of CADPerfusion CMR showed good diagnostic performances in several clinical studies (Table 1). As described for DSMR, the majority of studies published evaluated perfusion CMR diagnostic accuracy, having as a gold standard the detection of stenoses ≥ 50% in the radiograph coronary angiogram.
In a meta-analysis by Nandalur et al. [6••] involving 1183 patients with a CAD prevalence of 57.4%, perfusion CMR had a sensitivity of 91% and a specifi city of 81% in a per-patient analysis. On a coronary territory-level analysis, perfusion CMR showed a sensitivity of 84% and a specifi c-ity of 85% for the identifi cation of ischemic segments.
Perfusion CMR has also been validated against frac-tional fl ow reserve for the discrimination of relevant from nonrelevant coronary lesions [22–25].
Finally, Klem et al. [26] reported that an integrat-ing algorithm using LGE as complementary information improved perfusion CMR diagnostic performance in patients with suspected CAD. The interpretation algo-rithm yielded a better accuracy for the detection of important stenoses (≥ 70% in major coronary artery or ≥ 50% in left main) than perfusion CMR alone. This con-trasts with the results of Plein et al. [27], in which the comprehensive approach did not improve accuracy of perfusion CMR alone in patients presenting with non–ST-elevation acute coronary syndromes. The comprehensive approach seems to be advantageous for CMR diagnostic accuracy in populations with suspected CAD but not as good when a history of CAD is known. In a very recent paper, Klein et al. [28] studied the diagnostic performance
of the combination protocol (perfusion CMR + LGE), in patients after coronary artery bypass graft (CABG). In the 78 patients studied, the combination of perfusion CMR and LGE had a good overall diagnostic accuracy for the detection and localization of signifi cant stenoses but reduced sensitivity compared with published data in patients without CABG.
Comparison with other noninvasive techniquesA subgroup of 69 patients in Ishida et al. [29] had either TI-201 or technetium SPECT in addition to coronary angiography and perfusion CMR. Perfusion CMR had a sensitivity of 94% compared with only 82% for SPECT. MRI was superior in diagnosing ischemia in patients without a prior infarction. In an animal model, perfusion CMR identifi ed regional reduction in myocardial blood fl ow during global coronary vasodilatation better than SPECT and was capable of detecting nontransmural per-fusion defects in intermediate coronary stenosis that were missed by SPECT [30].
Perfusion CMR assessment of coronary fl ow reserve has also been evaluated against PET and an excellent correlation between the two methods was found [31]. Recently, the Magnetic Resonance Imaging for Myocar-dial Perfusion Assessment in Coronary Artery Disease Trial (MR-IMPACT) enrolled 234 patients in 18 centers and compared the results of perfusion CMR with coro-nary artery angiography and SPECT [32••]. The results of this study confi rmed the high diagnostic accuracy of perfusion CMR and showed that, at least, it is not inferior to SPECT for CAD detection.
Prognosis assessmentIngkanisorn et al. [33] published the fi rst evidence of the usefulness of perfusion CMR in the prognostication of patients with chest pain in patients presenting to the emer-gency department with chest pain and normal cardiac enzymes. Perfusion CMR predicted with high accuracy which patients had signifi cant CAD (evidence of coronary artery stenosis greater than 50%, abnormal stress test, MI, death) during the 1-year follow-up. No patients with a normal perfusion CMR suffered an adverse event dur-ing follow-up.
In Jahnke et al. [15••], patients with a positive perfu-sion DSMR had a 12-fold increased risk of a subsequent cardiac event over an average follow-up of 2.3 years. Con-versely, patients with normal stress perfusion had a 2-year event rate of 0.7% (2.3% at 3 y).
In a 2009 study, Doesch et al. [34•] used perfusion CMR to examine 81 patients with stable angina and intermediate coronary stenosis (as accessed by coronary angiography). Perfusion CMR was able to correctly iden-tify patients with a higher rate of major adverse cardiac events after a mean follow-up of 18 months. The authors concluded that perfusion CMR may identify patients at risk who would benefi t from intensifi ed medical treatment and close follow-up.

Assessment of MI and Viability Using CMR I Bettencourt et al. I 149
Late Gadolinium EnhancementA major breakthrough for the use of CMR was the devel-opment of the LGE technique, which allows identifi cation of myocardial scar over the entire heart in less than 10 minutes. In these images, normal myocardium appears uniformly dark whereas necrotic or fi brotic myocardial tissue appears bright. LGE takes advantage of gadolinium properties, which shortens tissue T1 relaxation time and tends to accumulate in fi brous areas. Under normal conditions, gadolinium-based contrast agents remain confi ned to the extracellular space and diffuse passively from the intravascular compartment to the third space. With MI, the distribution volume for gadolinium con-trast is signifi cantly expanded—thought to be due to the loss of myocardial cell membranes integrity and intercel-lular edema—and reaches 60% to 70% in myocardial scar tissue. Relative increases in gadolinium concentra-tion in both acute infarctions and chronic scars produce T1 shortening—and these areas appear enhanced. To increase contrast between scar and myocardium, images are acquired 10 to 30 minutes after paramagnetic con-trast injection (to allow gadolinium redistribution) and the sequence contrast parameters are chosen in order to ‘‘null’’ normal myocardium.
LGE has been shown to be a robust technique with a soft learning curve [35•]. It also represents a major contribution of CMR for the understanding of ischemic cardiomyopathy that is universally used for the diag-nosis of established MI and differential diagnosis with other causes of myocardial infl ammation and fi brosis. Furthermore, it has proven to be an accurate method for the assessment of myocardial viability. For that purpose, it can be used alone—precluding the need for cardiac stress—or in combination with low-dose DSMR.
Assessment of myocardial viabilityAnimal studies have demonstrated that LGE is a specifi c marker of myocardial necrosis and correlates closely with histology and biomarkers [36]. Multiple studies have also shown the inverse relationship between the transmural extent of MI and recovery of function after revasculariza-tion in chronic IHD (Table 2).
In a landmark paper, Kim et al. [37] demonstrated an inverse correlation between the transmural extent of LGE before revascularization and the likelihood of improvement in regional contractility 2 to 3 months after revascularization in 50 patients with chronic IHD. Improved contractility was found in 78% of segments with no enhancement but in only 10% of the segments with LGE accounting for more than 50% of wall thick-ness. Similarly, in patients with reperfused acute MI, Choi et al. [38] showed that the transmural extent of infarction as seen on LGE following revascularization predicted improvement in contractility.
LGE was shown to have signifi cantly better accuracy than resting TI-201 SPECT in the prediction of regional myocardial viability [18,39]. Due to the higher spatial res-
olution, LGE detects infarctions that are not visualized by PET or SPECT. Wagner et al. [40] demonstrated a better detection of subendocardial infarcts with LGE compared with SPECT in the experimental animal and in patients with CAD. Klein et al. [41] showed that more than half of subendocardial infarcts detected by LGE were classi-fi ed as normal by PET. The same observation was made by Lund et al. [42], who studied patients with thallium SPECT and LGE 6 days after reperfused MI. The mean infarct size was not signifi cantly different as evaluated by SPECT and LGE but 20% of inferior infarcts detected by LGE were missed by scintigraphy.
Roes et al. [43] recently investigated the performance of LGE and nuclear imaging (SPECT and fl udeoxyglucose [FDG]-PET) for the assessment of viability in a popula-tion of 60 patients with severe ischemic LV dysfunction. A good agreement was found in segments without scar tis-sue and in segments with transmural scar but an evident disagreement was observed in segments with subendocar-dial scar tissue detected on LGE. These fi ndings illustrate that the nonenhanced epicardial rim may contain either normal or jeopardized myocardium.
Combined approaches of different imaging methods to improve prediction of functional recovery have also been tested. Recently, Hoffmann et al. [44] studied 59 patients with ischemic LV dysfunction using LGE and pixel-track-ing–derived myocardial deformation echocardiography to predict recovery of function at 9 months after revascular-ization. The combination of both parameters improved the predictive accuracy to identify reversibility compared with LGE alone. The advantage of image integration was particularly strong in segments with intermediate degrees of LGE. The transmural extent of LGE is also a good and independent predictor of LV function improvement in patients with heart failure undergoing β-blockers [45].
Research on LGE for the prediction of dysfunctional myocardial recovery continues. Recently, Vosseler et al. [46] demonstrated in an animal model the feasibility to determine the area at risk and myocardial viability early after myocardial ischemia-reperfusion using LGE. Fur-thermore, automatic quantifi cation approaches based on thresholds have been tested, as a way to increase repro-ducibility and to facilitate multicenter comparisons but they are not fully validated. Beek et al. [47] found that simple thresholding techniques strongly infl uence global and segmental extent of LGE, but have relatively little infl uence on the accuracy to predict segmental functional improvement after revascularization.
Prognosis assessmentDetermination of scar size by LGE was shown to be the strongest independent predictor of LVEF and LV vol-umes in patients with acute MI and signs or symptoms of heart failure [48]. In patients with IHD referred for an electrophysiology study, the infarct mass and surface area as shown by LGE were better predictors of inducible sus-tained ventricular tachycardia than LVEF alone [49].

150 I Imaging and Diagnostics
Data also suggest that infarct characteristics by LGE may prove to be a unique and valuable noninvasive pre-dictor of post-MI mortality. In a study of patients with established CAD and abnormal LGE consistent with an infarction, Yan et al. [50] showed that extensive peri-infarct regions of intermediate signal intensity conferred increased mortality risk. The extent of the peri-infarct zone characterized by LGE provided incremental prog-nostic value beyond LV systolic volume index or LVEF. Furthermore, the causal relationship between subendo-cardial infarction detected by LGE and reverse regional remodeling has recently been demonstrated [51]. Even in patients without previous history of MI, detection of small areas of scar with LGE has been shown to predict a higher risk. LGE provides incremental prognostic value of major adverse cardiac events and cardiac mortality beyond common clinical, angiographic, and functional predictors even in patients with normal LV function and no regional WMA [52].
LGE technique also allows identifi cation of regions of microvascular obstruction in the setting of acute MI (visualized as hypoenhanced zones within an area of infarction). Detection of these areas has been shown to predict impaired LV remodeling, as well as adverse clini-cal prognosis [53,54].
ReproducibilityThe interstudy reproducibility of scar size measurements with LGE has been favorably compared with TI-201 SPECT [55,56]. Therefore, if infarct size is chosen as an end point for a trial, the study cohort for a CMR-based trial needs to reach only 42% of the cohort size of a SPECT-based study. LGE has the potential to serve as a surrogate end point to uncover advantages of new reper-fusion strategies in acute MI in future trials.
ConclusionsCMR is a unique noninvasive technique that allows accu-rate assessment of ischemia and viability. Different CMR methods, which can be selected to suit patient character-istics and diagnostic needs, can be used to achieve these goals in patients with known or suspected CAD. Further-more, different from other techniques, a comprehensive and integrative approach, including information about anatomy, function, perfusion, and tissue characterization is possible, which renders CMR an unparalleled tool for the management of IHD.
During the past decade, CMR evolved from a research tool performed in a few selected centers to one that enjoys routine clinical use. Several studies confi rmed the impor-tant role of CMR in risk stratifi cation and in prognostic evaluation of patients with known or suspected CAD. The few available data comparing CMR techniques with pre-viously established diagnostic and prognostic tools also seem to confer CMR-consistent advantages that may be translated into better management of patients.
DisclosureDr. Eike Nagel received minor consultancy fees from Gen-eral Electric and Philips Healthcare and minor speaker honoraria from General Electric, Philips Healthcare, and Bayer Schering Pharma.
No further potential confl icts of interest were reported.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Rahimroola SH: The hibernating myocardium. Am Heart J 1989, 117:211–221.
2. Hendel RC, Patel MR, Kramer CM, et al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriate-ness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Com-mittee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006, 48:1475–1497.
3. Nagel E, Lorenz C, Baer F, et al.: Stress cardiovascular magnetic resonance: consensus panel report. J Cardiovasc Magn Reson 2001, 3:267–281.
4. Wahl A, Paetsch I, Gollesch A, et al.: Safety and feasibility of high-dose dobutamine-atropine stress cardiovascular magnetic resonance for diagnosis of myocardial ischaemia: experience in 1000 consecutive cases. European Heart J 2004, 25:1230–1236.
5. Nagel E, Lehmkuhl HB, Klein C, et al.: Infl uence of image quality on the diagnostic accuracy of dobutamine stress magnetic resonance imaging in comparison with dobutamine stress echocardiography for the noninvasive detection of myocardial ischemia [in German]. Zeitschrift für Kardiologie 1999, 88:622–630.
6.•• Nandalur KR, Dwamena BA, Choudhri AF, et al.: Diag-nostic performance of stress cardiac magnetic resonance imaging in the detection of coronary artery disease: a meta-analysis. J Am Coll Cardiol 2007, 50:1343–1353.
This meta-analysis compared the results of cardiac stress CMR (DSMR and perfusion CMR) with coronary angiography.7. Nagel E, Lehmkuhl HB, Bocksch W, et al.: Noninvasive
diagnosis of ischemia-induced wall motion abnormalities with the use of high-dose dobutamine stress MRI: compari-son with dobutamine stress echocardiography. Circulation 1999, 99:763–770.
8. Kuijpers D, Ho KY, van Dijkman PR, et al.: Dobutamine cardiovascular magnetic resonance for the detection of myocardial ischemia with the use of myocardial tagging. Circulation 2003, 107:1592–1597.
9. Korosoglou G, Futterer S, Humpert PM, et al.: Strain-encoded cardiac MR during high-dose dobutamine stress testing: comparison to cine imaging and to myocardial tagging. J Magn Reson Imaging 2009, 29:1053–1061.
10. Syed MA, Paterson DI, Ingkanisorn WP, et al.: Reproducibility and inter-observer variability of dobutamine stress CMR in patients with severe coronary disease: implications for clinical research. J Cardiovasc Magn Reson 2005, 7:763–768.
11. Paetsch I, Jahnke C, Ferrari VA, et al.: Determination of interobserver variability for identifying inducible left ventricular wall motion abnormalities during dobutamine stress magnetic resonance imaging. European Heart J 2006, 27:1459–1464.
Assessment of MI and Viability Using CMR I Bettencourt et al. I 151
12. Hundley WG, Morgan TM, Neagle CM, et al.: Magnetic resonance imaging determination of cardiac prognosis. Circulation 2002, 106:2328–2333.
13. Rerkpattanapipat P, Morgan TM, Neagle CM, et al.: Assessment of preoperative cardiac risk with magnetic resonance imaging. Am J Cardiol 2002, 90:416–419.
14.• Dall’Armellina E, Morgan TM, Mandapaka S, et al.: Prediction of cardiac events in patients with reduced left ventricular ejection fraction with dobutamine cardiovas-cular magnetic resonance assessment of Wall Motion Score Index. J Am Coll Cardiol 2008, 52:279–286.
This recent study demonstrates DSMR’s usefulness in prognostic stratifi cation of patients with reduced left ventricular function.15.•• Jahnke C, Nagel E, Gebker R, et al.: Prognostic value of
cardiac magnetic resonance stress tests: adenosine stress perfusion and dobutamine stress wall motion imaging. Circulation 2007, 115:1769–1776.
This study demonstrates the prognostic value of CMR in patients with known and suspected CAD. The authors used a combined protocol, which allowed a direct comparison between DSMR and perfusion CMR.16. Rerkpattanapipat P, Little WC, Clark HP, et al.: Effect of
the transmural extent of myocardial scar on left ventricular systolic wall thickening during intravenous dobutamine administration. Am J Cardiol 2005, 95:495–498.
17. Wellnhofer E, Olariu A, Klein C, et al.: Magnetic resonance low-dose dobutamine test is superior to SCAR quantifi ca-tion for the prediction of functional recovery. Circulation 2004, 109:2172–2174.
18. Gutberlet M, Fröhlich M, Mehl S, et al.: Myocardial viability assessment in patients with highly impaired left ventricular function: comparison of delayed enhancement, dobutamine stress MRI, end-diastolic wall thickness, and TI201-SPECT with functional recovery after revasculariza-tion. Euro Radiol 2005, 15:872–880.
19. Bove CM, DiMaria JM, Voros S, et al.: Dobutamine response and myocardial infarct transmurality: functional improvement after coronary artery bypass grafting—initial experience. Radiology 2006, 240:835–841.
20. Bree D, Wollmuth JR, Cupps BP, et al.: Low-dose dobu-tamine tissue-tagged magnetic resonance imaging with 3-dimensional strain analysis allows assessment of myo-cardial viability in patients with ischemic cardiomyopathy. Circulation 2006, 114:I33–36.
21. Al-Saadi N, Gross M, Paetsch I, et al.: Dobutamine induced myocardial perfusion reserve index with cardiovascular MR in patients with coronary artery disease. J Cardiovasc Magn Reson 2002, 4:471–480.
22. Rieber J, Huber A, Erhard I, et al.: Cardiac magnetic resonance perfusion imaging for the functional assessment of coronary artery disease: a comparison with coronary angiography and fractional fl ow reserve. Eur Heart J 2006, 27:1465–1471.
23. Kühl HP, Katoh M, Buhr C, et al.: Comparison of magnetic resonance perfusion imaging versus invasive fractional fl ow reserve for assessment of the hemodynamic signifi cance of epicardial coronary artery stenosis. Am J Cardiol 2007, 99:1090–1095.
24. Costa M, Shoemaker S, Futamatsu H, et al.: Quantitative magnetic resonance perfusion imaging detects anatomic and physiologic coronary artery disease as measured by coronary angiography and fractional fl ow reserve. J Am Coll Cardiol 2007, 50:514–522.
25. Futamatsu H, Klassen C, Pilla M, et al.: Diagnostic accuracy of quantitative cardiac MRI evaluation compared to stress single-photon-emission computed tomography. Int J Cardiovasc Imaging 2008, 24:293–299.
26. Klem I, Heitner JF, Shah DJ, et al.: Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhancement infarction imaging. J Am Coll Cardiol 2006, 47:1630–1638.
27. Plein S, Greenwood JP, Ridgway JP, et al.: Assessment of non-ST-segment elevation acute coronary syndromes with cardiac magnetic resonance imaging. J Am Coll Cardiol 2004, 44:2173–2181.
28. Klein C, Nagel E, Gebker R, et al.: Magnetic resonance adenosine perfusion imaging in patients after coronary artery bypass graft surgery. J Am Coll Cardiol 2009, 2:437.
29. Ishida N, Sakuma H, Motoyasu M, et al.: Noninfarcted myocardium: correlation between dynamic fi rst-pass contrast-enhanced myocardial MR imaging and quantita-tive coronary angiography. Radiology 2003, 229:209–216.
30. Lee DC, Simonetti OP, Harris KR, et al.: Magnetic reso-nance versus radionuclide pharmacological stress perfusion imaging for fl ow-limiting stenoses of varying severity. Circulation 2004, 110:58–65.
31. Schwitter J, Nanz D, Kneifel S, et al.: Assessment of myocardial perfusion in coronary artery disease by magnetic resonance: a comparison with positron emission tomography and coronary angiography. Circulation 2001, 103:2230–2235.
32.•• Schwitter J, Wacker CM, van Rossum AC, et al.: MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomog-raphy for the detection of coronary artery disease in a multicentre, multivendor, randomized trial. Eur Heart J 2008, 29:480–489.
This recent multicenter, multivendor, randomized trial compared perfusion CMR with SPECT. 33. Ingkanisorn WP, Kwong RY, Bohme NS, et al.: Prognosis
of negative adenosine stress magnetic resonance in patients presenting to an emergency department with chest pain. J Am Coll Cardiol 2006, 47:1427–1432.
34.• Doesch C, Seeger A, Doering J, et al.: Risk stratifi cation by adenosine stress cardiac magnetic resonance in patients with coronary artery stenoses of intermediate angiographic severity. J Am Coll Cardiol 2009, 2:424.
This recent study evaluated the role of perfusion CMR for risk stratifi cation in patients with coronary artery stenoses of interme-diate angiographic severity.35.• Kim RJ, Albert TS, Wible JH, et al.: Performance of
delayed-enhancement magnetic resonance imaging with gadoversetamide contrast for the detection and assessment of myocardial infarction: an international, multicenter, double-blinded, randomized trial. Circulation 2008, 117:629–637.
This multicenter trial evaluated LGE for detecting and localizing both acute and chronic MI.36. Kim RJ, Fieno DS, Parrish TB, et al.: Relationship of MRI
delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation 1999, 100:1992–2002.
37. Kim RJ, Wu E, Rafael A, et al.: The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med 2000, 343:1445–1453.
38. Choi KM, Kim RJ, Gubernikoff G, et al.: Transmural extent of acute myocardial infarction predicts long-term improvement in contractile function. Circulation 2001, 104:1101–1107.
39. Kitagawa K, Sakuma H, Hirano T, et al.: Acute myocardial infarction: myocardial viability assessment in patients early thereafter comparison of contrast-enhanced MR imag-ing with resting (201)Tl SPECT. Single photon emission computed tomography. Radiology 2003, 226:138–144.
40. Wagner A, Mahrholdt H, Holly TA, et al.: Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imag-ing study. Lancet 2003, 361:374–379.
41. Klein C, Nekolla SG, Bengel FM, et al.: Assessment of myocardial viability with contrast-enhanced magnetic resonance imaging: comparison with positron emission tomography. Circulation 2002, 105:162–167.
152 I Imaging and Diagnostics
42. Lund GK, Stork A, Saeed M, et al.: Acute myocardial infarction: evaluation with fi rst-pass enhancement and delayed enhancement MR imaging compared with 201Tl SPECT imaging. Radiology 2004, 232:49–57.
43. Roes SD, Kaandorp TA, Marsan NA, et al.: Agreement and disagreement between contrast-enhanced magnetic resonance imaging and nuclear imaging for assessment of myocardial viability. Eur J Nucl Med Mol Imaging 2009, 36:594–601.
44. Hoffmann R, Stempl K, Kühl H, et al.: Integrated analysis of cardiac tissue structure and function for improved identifi cation of reversible myocardial dysfunction. Coron Artery Dis 2009, 20:21–26.
45. Bello D, Shah DJ, Farah GM, et al.: Gadolinium cardiovas-cular magnetic resonance predicts reversible myocardial dysfunction and remodeling in patients with heart failure undergoing beta-blocker therapy. Circulation 2003, 108:1945–1953.
46. Vosseler M, Abegunewardene N, Hoffmann N, et al.: Area at risk and viability after myocardial ischemia and reperfu-sion can be determined by contrast-enhanced cardiac magnetic resonance imaging. Eur Surg Res 2009, 43:13–23.
47. Beek AM, Bondarenko O, Afsharzada F, et al.: Quantifi cation of late gadolinium enhanced CMR in viability assessment in chronic ischemic heart disease: a comparison to functional outcome. J Cardiovasc Magnetic Reson 2009, 11:6.
48. Orn S, Manhenke C, Anand IS, et al.: Effect of left ventricular scar size, location, and transmurality on left ventricular remodeling with healed myocardial infarction. Am J Cardiol 2007, 99:1109–1114.
49. Bello D, Fieno DS, Kim RJ, et al.: Infarct morphology identifi es patients with substrate for sustained ventricular tachycardia. J Am Coll Cardiol 2005, 45:1104–1108.
50. Yan AT, Shayne AJ, Brown KA, et al.: Characterization of the peri-infarct zone by contrast-enhanced cardiac magnetic resonance imaging is a powerful predictor of post-myocar-dial infarction mortality. Circulation 2006, 114:32–39.
51. Chan J, Khafagi F, Young A, et al.: Impact of coronary revas-cularization and transmural extent of scar on regional left ventricular remodelling. Eur Heart J 2008, 29:1608–1617.
52. Kwong RY, Chan AK, Brown KA, et al.: Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients pre-senting with signs or symptoms of coronary artery disease. Circulation 2006, 113:2733–2743.
53. Hombach V, Grebe O, Merkle N, et al.: Sequelae of acute myocardial infarction regarding cardiac structure and func-tion and their prognostic signifi cance as assessed by magnetic resonance imaging. Eur Heart J 2005, 26:549–557.
54. Baks T, van Geuns RJ, Biagini E, et al.: Effects of primary angioplasty for acute myocardial infarction on early and late infarct size and left ventricular wall characteristics. J Am Coll Cardiol 2006, 47:40–44.
55. Mahrholdt H, Wagner A, Holly TA, et al.: Reproducibility of chronic infarct size measurement by contrast-enhanced mag-netic resonance imaging. Circulation 2002, 106:2322–2327.
56. Thiele H, Kappl MJ, Conradi S, et al.: Reproducibility of chronic and acute infarct size measurement by delayed enhancement-magnetic resonance imaging. J Am Coll Cardiol 2006, 47:1641–1645.
57. Pennell DJ, Underwood SR, Manzara CC, et al.: Magnetic resonance imaging during dobutamine stress in coronary artery disease. Am J Cardiol 1992, 70:34–40.
58. van Rugge FP, Holman ER, van der Wall EE, et al.: Quan-titation of global and regional left ventricular function by cine magnetic resonance imaging during dobutamine stress in normal human subjects. Eur Heart J 1993, 14:456–463.
59. van Rugge FP, van der Wall EE, Spanjersberg SJ, et al.: Magnetic resonance imaging during dobutamine stress for detection and localization of coronary artery disease. Quantitative wall motion analysis using a modifi cation of the centerline method. Circulation 1994, 90:127–138.
60. Baer FM, Voth E, Theissen P, et al.: Coronary artery disease: fi ndings with GRE MR imaging and Tc-99m-methoxyisobutyl-isonitrile SPECT during simultaneous dobutamine stress. Radiology 1994, 193:203–209.
61. Hundley WG, Hamilton CA, Thomas MS, et al.: Utility of fast cine magnetic resonance imaging and display for the detection of myocardial ischemia in patients not well suited for second harmonic stress echocardiography. Circulation 1999, 100:1697–1702.
62. van Dijkman PR, Kuijpers DA, Blom BM, et al.: Dobuta-mine stress magnetic resonance imaging: a valuable method in the noninvasive diagnosis of ischemic heart disease. J Electrocardiol 2002, 35(Suppl):57–59.
63. Paetsch I, Jahnke C, Wahl A, et al.: Comparison of dobuta-mine stress magnetic resonance, adenosine stress magnetic resonance, and adenosine stress magnetic resonance perfu-sion. Circulation 2004, 110:835–842.
64. Wahl A, Paetsch I, Roethemeyer S, et al.: High-dose dobu-tamine-atropine stress cardiovascular MR imaging after coronary revascularization in patients with wall motion abnormalities at rest. Radiology 2004, 233:210–216.
65. Jahnke C, Paetsch I, Gebker R, et al.: Accelerated 4D dobu-tamine stress MR imaging with k-t BLAST: feasibility and diagnostic performance. Radiology 2006, 241:718–728.
66. Pilz G, Bernhardt P, Klos M, et al.: Clinical implication of adenosine-stress cardiac magnetic resonance imaging as potential gatekeeper prior to invasive examination in patients with AHA/ACC class II indication for coronary angiography. Clin Res Cardiol 2006, 95:531–538.
67. Takase B, Nagata M, Kihara T, et al.: Whole-heart dipyri-damole stress fi rst-pass myocardial perfusion MRI for the detection of coronary artery disease. Japan Heart J 2004, 45:475–486.
68. Doyle M, Fuisz A, Kortright E, et al.: The impact of myocardial fl ow reserve on the detection of coronary artery disease by perfusion imaging methods: an NHLBI WISE study. J Cardiovasc Magn Reson 2003, 5:475–485.
69. Nagel E, Klein C, Paetsch I, et al.: Magnetic resonance perfusion measurements for the noninvasive detection of coronary artery disease. Circulation 2003, 108:432–437.
70. Plein S, Radjenovic A, Ridgway JP, et al.: Coronary artery disease: myocardial perfusion MR imaging with sensitiv-ity encoding versus conventional angiography. Radiology 2005, 235:423–430.
71. Wolff SD, Schwitter J, Coulden R, et al.: Myocardial fi rst-pass perfusion magnetic resonance imaging: a multicenter dose-ranging study. Circulation 2004, 110:732–737.
72. Giang TH, Nanz D, Coulden R, et al.: Detection of coronary artery disease by magnetic resonance myocardial perfusion imaging with various contrast medium doses: fi rst European multi-centre experience. Eur Heart J 2004, 25:1657–1665.
73. Baer FM, Voth E, Schneider CA, et al.: Comparison of low-dose dobutamine-gradient-echo magnetic reso-nance imaging and positron emission tomography with [18F]fl uorodeoxyglucose in patients with chronic coronary artery disease. A functional and morphological approach to the detection of residual myocardial viability. Circulation 1995, 91:1006–1015.
74. Dendale P, Franken PR, Holman E, et al.: Validation of low-dose dobutamine magnetic resonance imaging for assessment of myocardial viability after infarction by serial imaging. Am J Cardiol 1998, 82:375–377.
75. Gunning MG, Anagnostopoulos C, Knight CJ, et al.: Comparison of 201Tl, 99mTc-tetrofosmin, and dobutamine magnetic resonance imaging for identifying hibernating myocardium. Circulation 1998, 98:1869–1874.
76. Sayad DE, Willett DL, Hundley WG, et al.: Dobutamine magnetic resonance imaging with myocardial tagging quantitatively predicts improvement in regional function after revascularization. Am J Cardiol 1998, 82:1149–1151.
Assessment of MI and Viability Using CMR I Bettencourt et al. I 153
77. Baer FM, Theissen P, Schneider CA, et al.: Dobutamine magnetic resonance imaging predicts contractile recovery of chronically dysfunctional myocardium after successful revascularization. J Am Coll Cardiol 1998, 31:1040–1048.
78. Geskin G, Kramer CM, Rogers WJ, et al.: Quantitative assessment of myocardial viability after infarction by dobutamine magnetic resonance tagging. Circulation 1998, 98:217–223.
79. Sandstede JJ, Bertsch G, Beer M, et al.: Detection of myocardial viability by low-dose dobutamine Cine MR imaging. Magn Reson Imaging 1999, 17:1437–1443.
80. Baer FM, Theissen P, Crnac J, et al.: Head to head comparison of dobutamine-transoesophageal echocardiog-raphy and dobutamine-magnetic resonance imaging for the prediction of left ventricular functional recovery in patients with chronic coronary artery disease. Eur Heart J 2000, 21:981–991.
81. Trent RJ, Waiter GD, Hillis GS, et al.: Dobutamine magnetic resonance imaging as a predictor of myocardial functional recovery after revascularisation. Heart 2000, 83:40–46.
82. Lauerma K, Niemi P, Hänninen H, et al.: Multimodality MR imaging assessment of myocardial viability: combina-tion of fi rst-pass and late contrast enhancement to wall motion dynamics and comparison with FDG PET-initial experience. Radiology 2000, 217:729–736.
83. Selvanayagam JB, Kardos A, Francis JM, et al.: Value of delayed-enhancement cardiovascular magnetic resonance imaging in predicting myocardial viability after surgical revascularization. Circulation 2004, 110:1535–1541.
Related Documents











