Aryadi Kurniawan A.Dohar A . L. Tobing D ep. of S urgery D iv. O rthopaedics & Traumatology, F K UI/R S C M Kuliah MS – Des 08 Kuliah MS – Des 08

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Aryadi KurniawanA.Dohar A. L. Tobing
Dep. of S urgeryDiv. Orthopaedics & Traumatology, FKUI/RS CM
Kuliah MS – Des 08Kuliah MS – Des 08
2
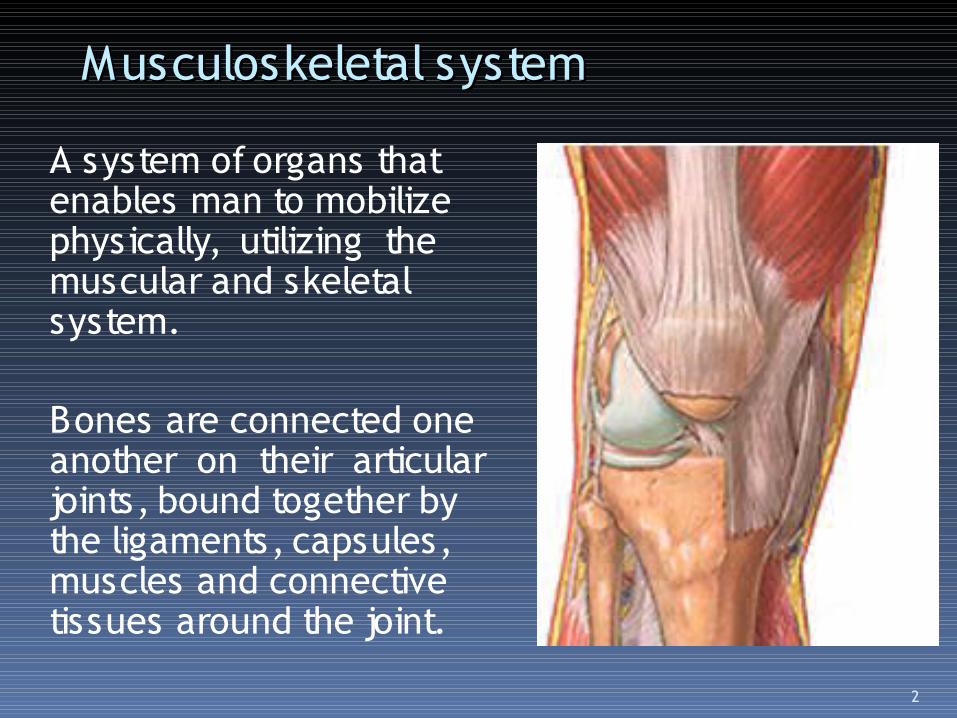
Musculoskeletal systemMusculoskeletal system
A system of organs that enables man to mobilize physically, utilizing the muscular and skeletal system.
Bones are connected one another on their articular joints, bound together by the ligaments, capsules, muscles and connective tissues around the joint.

3

4

5

6
Basic Knowledge
Anatomy Physiology Histology Biochemistri
Kinesiology Biomechanic Kinemathics Engineering

7
Comprehensive understanding on normal musculoskeletal system will ensure a better knowledge on musculoskeletal pathologies

8
Musculoskeletal pathologies in general
Trauma Infection Congenital anomalies Neoplasma / tumor Degenerative (osteoporosis, osteoarthritis) Metabolic

9
Musculoskeletal injury Bone:
Epiphyseal plate Cortical bone Cancellous bone
Joint: Articular cartilage Joint Capsule Ligaments
Muscles Tendon Peripheral nerve

10
Forces responsible for the injury
Mechanism of injury : Direct Indirect
Orientation : Axial / compresion S hearing Twisting / rotation

11
Forces responsible for the injury
Capacity of the forces : High energy Low energy
12
FRACTUREFRACTURE S tructural discontinuity of bone, articular
cartilage or epiphyseal growth plate
Depending on the skin and soft tissue coverage around the fracture site
1. Closed : intact2. Open / COMPOUND : The soft tissue coverage
is breech and there is an open communication with the outer environment

13
FRACTURE ETI OLOGI ESNon Pathological
1. S IN G LE TR AU M AS IN G LE TR AU M A2. Repetitive stress
Pathological1. Malignancy2. Infection3. Osteoporosis (insufficient fracture)

14
Pattern of Complete Fracture
S IMPLE Transverse Oblique S piral Impacted
COMPLEX Comminutive S egmental

15

16

17
Incomplete Fracture
Involve only one cortex Intact Periosteum Children/ Paediatric Greenstick #, torus #

18
19

20
St r es s Fr ac t ur e / Fat i gue Fr ac t ur e Mostly on tibia/fibula Occurs frequently on athlete, dancer, new
army recruits

21
Pathological fracture
Normal S tress for normal bone Deteriorated bone microstructural
Osteoporosis Malignancy Paget disease

22
Sites associated with low BMD
HIP SPINE WRIST
23

24
Paget DISEASE

25
Open Fracture
Gustillo & Anderson clasification :
Grade I Grade II Grade III : III A III B III C

26
Grade I
Open wound < 1 cm Clean Low energy trauma

27
Grade II
Wound > 1 cm No extensive soft tissue stripping Moderate energy trauma

28
Grade III
High energy trauma High velocity trauma Gun shot Grosly contaminated ( farm injury,
barnyard injury ) Associated Neurovascular injury Open fracture > 8 jam

29
Grade III
III A : Adequate soft tissue coverage III B :
Bone exposed Extensive periosteal stripping Grosly comminutive
III C : With vascular injury which otherwise repaired will jeopardize the limb vitality

30
31
FRACTURE DISPLACEMENT
o/ Trauma force o/ Muscle pull o/ Gravity

32
FRACTURE DISPKACEMENT
Aposition Angulation Rotation S hortening/ Distraction

33
FRACTURE HEALING
Hematoma Inflamation and cell proliferation Callus formation Consolidation Remodelling

34

35
36
PHYSICAL EXAMINATION PR IM ARY S U RV E YPR IM ARY S U RV E Y Look :
S welling and edema Deformity open wound S kin colour
Feel : Tenderness Neurovascular distal

37
PHYSICAL EXAMINATION
Move : Functio Laesa Mobilize the uninvolved joint to
asses the motoric scale

38
X- ray
Fracture configuration Further management Follow up Medical record

39
X ray
2 views : AP/Lat/Oblik
2 joints Confirm no intra articular injury
2 extremities especially in children
2 times

40
I MAGI NG
Bone scanning CT scan (computerized tomography) MR I (Magnetic Resonance Imaging) MS CT (Multi S liced CT)

41
BONE SCAN

42
3D CT SCAN

43

44
CT SCAN

45
PRINCIPLE OF MANAGEMENT
Recognize Reduce Retain Rehabilitation

46
REDUCTION
Reduce = reposition reduction closed manipulation open surgery reduksi a vue
( direct vision)

47
CLOSED REDUCTION
General anaesthesia Muscle relaxant 3 Manouvre manipulation
Apply taction on the distal fragment along its longitudinal axis (disengagement)
Reduce to anatomical position Realign on 2 dimension

48
OPEN REDUCTION
Debridemen open fracture Closed frakture
Failed closed reduction Intra articular fracture Avulsion fraktur

49
OPEN FRACTURE

50
RETAINMENT / IMOBILIZATION
S plint S kin traction Circular cast Internal fixation Exeternal fixation

51
GIPS
= Plaster = POP = Plaster of Paris S plint Circular cast

52
OPEN FRACTURE
Contamination higher risk of infection Principles of management eradicate
infection S tart with primary survey Therapeutic IV antibiotic (not prophylactic) Tetanus Prophylactic : Toxoid, ATS

53
OPEN FRACTURE
Emergency Debridement
Decontamination from dirt, foreign body (The best solution for pollution is dilution)
Excision of non vital tissue Open reduction
General anaesthesia

54
EPIPHYSEAL PLATE INJURY
Paediatric If managed unproperly may lead to growth
disturbance or even cessation

55

56
FRACTURE COMPLICATION
Early : Viseral injury Vaskuler injury Compartment syndrome
( Volkmann’s ischemia) Nerve injury Infection
57
COMPARTMENT SYNDROME
An increased pressure in closed osseofasial compartment that compromise the intrinsic vascularization and jeopardize the vitality of the involved limb
The plaster is too tight Vascular injury Haemophillia

58
COMPARTMENT SYNDROME
High risk elbow fracture, forearm, tibia proksimal
5 P S IGN: Pain Paraesthesia Pallor Paralis is Pulselessness
Tx : fasiotomi

59
FRACTURE COMPLICATION
Late : Delayed union Non-union Malunion Joint stifness Muscle Hypotrofi/atrofi M iositis osifikans Avascular Necrosis Algodystrophy (S udeck’s atrophy) Osteoarthritis

60
Del ayed Uni on
At the time of estimated union such fracture healing is not attained yet
Cause : S evere soft tissue injury Infection Inadequate stabilization
TX : bone graft

61
Non- union
Fracture site is filled with fibrosis Pseudoarthrosis No sign of fracture healing process at all X ray : obvious fracture line

62
Malunion
Fracture united in malposition leading to impairment of fucntion

63
Avascular Necrosis Dislokation Bone ischemic avascular
necrosis Occurs frequently : feoral head, proximal
scafoid, lunate, talus

64
Fr ac t ur e di s eas e
Prolonged immobilization Muscle hypotrofi/atrofi Disuse osteoporosis Joint stifness

65
Sprain ligament
Ligamentous injury without any structural discontinuity
i.e. sprain ankle Clinical sign : tenderness, swelling,
blueish

66

67
Sprain ankle

68
Strain ligament
Ligamentous injury with partial structural discontinuity which doesn’t affect the joint stability

69
LIGAMENTOUS RUPTURE
Partial or total structural discontinuity May be associated with aulsion fracture Knee, ankle, Haematoma, severe tenderness and
swelling

70
DISLOCATION Total loss of joint contact S evere pain, deformity, limited range of
motion

71
Dislokasi posteriorkaput femur

72
Dislokasi
Dislok CMC 1 Dislok TMJ

73
SUBLUXATION
Partial joint contact is maintained

74
St r ai n mus c l e

75
Strain Muscle

76
Tendon
Tendonitis : inflamation on the tendon sheath
example : tendonitis achilles (heel cord ) tendonitis supraspinnatus dll
77
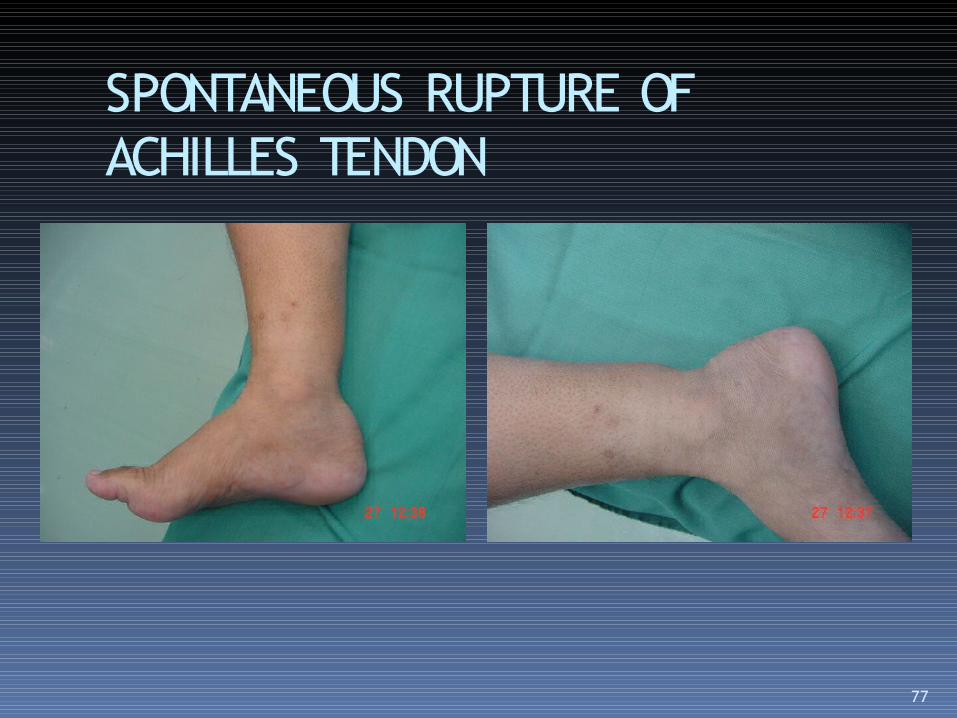
SPONTANEOUS RUPTURE OF ACHILLES TENDON

78
Rupture of long head of biceps

79
THANK YOU
Related Documents











