Ef ficacy of Collagen Membrane Seeded With Autologous Gingival Fibroblasts in Gingival Recession Treatment: A Randomized, Controlled Pilot Study Serhat Ko ¨ seoglu,* Ismet Duran, †‡ Mehmet Saglam,* S. Buket Bozkurt, § Osman S. Kırtıloglu, i and Sema S. Hakkı ‡ Background: Gingival recession (GR) is one of the most common esthetic concerns associated with periodontal tis- sues. Recently, tissue engineering technology has been de- veloped and applied in periodontology for the treatment of GR. The aim of this study is to compare the clinical efficacy of collagen membrane with or without autologous gingival fi brobl asts u nd er a c or on al ly advanced fl ap for root coverage. Methods: In this spl it-mou th, controlled clinical stu dy, 22 sites are selected from 11 patients with Miller Class I re- ces sions aff ect ing canines or pre mol ars in the max ill ary arch. One tooth in each patient was randomized to receive either a collagen membrane (CM) (control group) or a col- lagen membrane seeded with autolo gous gin gival fibro- blasts (CM+GF) (te st group) und er a coronally advanc ed flap. Thickness of the gingiva, GR, and percentage of root coverage (PRC) were recorded by a calibrated examiner at baseline and 3, 6, and 12 months postoperatively. Further- more, GR and PRC were evaluated using photogrammetric analysis at baseline and 3, 6, and 12 months. Results: Bot h treatment s res ult ed in a sig nifican t gai n in root covera ge compar ed wit h baseli ne. A statis tically significant increase was detected in PRC in the test group compared with the control group. No significant difference was noted between the test and control sites regarding the thickness of the gingiva. Conclusions: The results indicated that CM+GF prepared by tissue engineering technology can be considered an alter- native method for the treatment of Miller Class I recession defects. J Periodontol 2013;84:1416-1424. KEY WORDS Fibroblasts; gingival recession; guided tissue regeneration; membranes; tissue engineering; transplantation, autologous. B uccal gingival recession is a common problem because of es- thetic concerns, root sensi tivity, and caries in patients. 1 Several surgical techniques have been proposed to ach- iev e pro per roo t covera ge in gingiv al recession (GR) def ects. Sur gical pro - cedures, including pedicle flaps (lateral and coronally positioned), 2,3 free gingi- val gr af ts, 4 allografts, 5 subepithelial connective tissu e graft s, 6,7 and guided tissue regeneration procedures (GTRPs), 8 have been used. In comparison wit h oth er soft tiss ue pr ocedures, th e bene fits of guided tissue regeneration include new atta chmen t forma tion, 9 lack of donor site morbidity, less chair time, unlimited availabi lit y, and uni for m thickness of the product. 10 Hist ologic observations fol lowing GTR P in GR def ect s sho wed insertion of conn ective tissue fibe rs with new cement um and li mi ted bone re- generation. 11-14 In another histol ogi c stu dy, GTRP showed less rec urr ence than coronally advanced flap (CAF) in terms of root coverage. 15 Amarante et al. 16 compared coronally positioned flap with and without a bio- degradable membrane in a split-mouth design with 20 pat ients and found no significant differences among the groups for any evaluated parameters. Compar- ing CAF with GTRP for 6 years’ follow- up, Leknes et al. 14 did not report any * Department of Periodontology, Faculty of Dentistry, Izmir Katip C xelebi University, Izmir, Turkey. † Department of Periodontology, Faculty of Dentistry, Abant Izzet Baysal University, Bolu, Turkey. ‡ Department of Periodontology, Faculty of Dentistry, Selcuk University, Konya, Turkey. § Research Center of Faculty of Dentistry, Selcuk University. i Department of Geomatics Eng ineering, Faculty of Engineerin g and Architecture, Selcuk University. doi: 10.1902/jop.2012.120529 Volume 84 • Number 10 1416

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 1/9
Efficacy of Collagen Membrane SeededWith Autologous Gingival Fibroblasts
in Gingival Recession Treatment:A Randomized, Controlled Pilot StudySerhat Koseoglu,* _Ismet Duran,†‡ Mehmet Saglam,* S. Buket Bozkurt,§ Osman S. Kırtıloglu,i
and Sema S. Hakkı‡
Background: Gingival recession (GR) is one of the mostcommon esthetic concerns associated with periodontal tis-sues. Recently, tissue engineering technology has been de-veloped and applied in periodontology for the treatment of
GR. The aim of this study is to compare the clinical efficacyof collagen membrane with or without autologous gingivalfibroblasts under a coronally advanced flap for rootcoverage.
Methods: In this split-mouth, controlled clinical study,22 sites are selected from 11 patients with Miller Class I re-cessions affecting canines or premolars in the maxillaryarch. One tooth in each patient was randomized to receiveeither a collagen membrane (CM) (control group) or a col-lagen membrane seeded with autologous gingival fibro-blasts (CM+GF) (test group) under a coronally advancedflap. Thickness of the gingiva, GR, and percentage of root
coverage (PRC) were recorded by a calibrated examiner atbaseline and 3, 6, and 12 months postoperatively. Further-more, GR and PRC were evaluated using photogrammetricanalysis at baseline and 3, 6, and 12 months.
Results: Both treatments resulted in a significant gainin root coverage compared with baseline. A statisticallysignificant increase was detected in PRC in the test groupcompared with the control group. No significant differencewas noted between the test and control sites regarding thethickness of the gingiva.
Conclusions: The results indicated that CM+GF preparedby tissue engineering technology can be considered an alter-native method for the treatment of Miller Class I recessiondefects. J Periodontol 2013;84:1416-1424.
KEY WORDS
Fibroblasts; gingival recession; guided tissue regeneration;membranes; tissue engineering; transplantation,autologous.
Buccal gingival recession is acommon problem because of es-thetic concerns, root sensitivity,
and caries in patients.1 Several surgicaltechniques have been proposed to ach-ieve proper root coverage in gingivalrecession (GR) defects. Surgical pro-cedures, including pedicle flaps (lateraland coronally positioned),2,3 free gingi-val grafts,4 allografts,5 subepithelial
connective tissue grafts,6,7
and guidedtissue regeneration procedures (GTRPs),8
have been used. In comparison with othersoft tissue procedures, the benefits of guided tissue regeneration include newattachment formation,9 lack of donorsite morbidity, less chair time, unlimitedavailability, and uniform thickness of the product.10 Histologic observationsfollowing GTRP in GR defects showedinsertion of connective tissue fibers withnew cementum and limited bone re-generation.11-14 In another histologicstudy, GTRP showed less recurrencethan coronally advanced flap (CAF) interms of root coverage.15
Amarante et al.16 compared coronallypositioned flap with and without a bio-degradable membrane in a split-mouthdesign with 20 patients and found nosignificant differences among the groupsfor any evaluated parameters. Compar-ing CAF with GTRP for 6 years’ follow-up, Leknes et al.14 did not report any
* Department of Periodontology, Faculty of Dentistry, _Izmir Katip Cxelebi University, _Izmir,Turkey.
† Department of Periodontology, Faculty of Dentistry, Abant _Izzet Baysal University, Bolu,Turkey.
‡ Department of Periodontology, Faculty of Dentistry, Selcuk University, Konya, Turkey.§ Research Center of Faculty of Dentistry, Selcuk University.i Department of Geomatics Engineering, Faculty of Engineering and Architecture, Selcuk
University. doi: 10.1902/jop.2012.120529
Volume 84 • Number 10
1416

8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 2/9
significant difference in terms of root coverage.Thus, short-term16 and long-term14 data reveal thatCAF is a simple and predictable treatment of GR andthat GTRP does not seem to give any additionaladvantage for root coverage.
Tissue engineering has been used recently in
periodontal surgery.17-19 The most common appli-cation involves a cell-expansion strategy in anex vivo environment followed by transplantationback into the defect area.17-20 Most studies havefocused on fibroblast explants because fibroblastsare a type of basic connective tissue that producescollagen and growth factors.17,20,21 Therefore, fi-broblasts can play an important role in soft tissuehealing and formation. The cells should be trans-ported to the defect site with the help of the mostbiologically suitable scaffold. Several scaffoldmaterials have been investigated for the trans-
portation of fibroblasts, including collagen,19
chito-san,21 hyaluronic acid,22 polyglactin mesh,23,24 andan acellular dermal matrix allograft.17 A previousexperiment by the authors (unpublished data) eval-uated three different scaffolds (collagen membrane,polyglycolic/lactic membrane, and an acellulardermal matrix allograft) from the aspect of thegrowth of gingival fibroblasts. The collagen mem-brane was found to be more effective than the otherscaffolds in that preclinical study. Mohammadiet al.25 evaluated the effectiveness of collagen gelseeding with gingival fibroblasts in patients with in-
adequately attached gingiva and reported that themean increase in the amount of keratinized tissue(KT) was higher at treated sites than in a controlgroup after 3 months. Collagen membrane seededwith autologous gingival fibroblasts (CM+GF) couldbe a suitable alternative treatment method in GR,and it would improve the results of root coverage inGTRP. However, to our knowledge, there is nodocumented human study of the use of CM+GF inthe treatment of GR.
This split-mouth study is designed to comparethe clinical efficacy of CM+GF placed under a CAF(test group) with CM under a CAF (control group) forroot coverage. The healing and gingival character-istics of the groups are also compared.
MATERIALS AND METHODS
Twenty-two sites of 11 patients (six males and fivefemales, aged 19 to 41 years; median: 31 years;mean – SD: 45 – 7.03 years) were selected frompatients referred to the Periodontology Department,Faculty of Dentistry, Selcuk University, Turkey, fromNovember 2008 to January 2010.
The inclusion criteria for the study were: 1) in goodsystemic and periodontal health; 2) not taking
medications that interfere with periodontal surgery;
3) not pregnant or lactating; 4) non-smoking; 5)having no known hypersensitivity to equine collagen;6) having no acute infectious lesions in the intendedsurgical areas; and 7) having bilateral Miller Class IGRs26 affecting cuspid or bicuspid teeth in themaxilla.
The study design was approved by the EthicalCommittee of Selcuk University, Faculty of Dentistry(project no. 2007/8-3). Written consent was obtainedfrom all participants after fully explaining the natureof the procedure and its potential risks.
The study procedure is divided into six stages: 1)clinical measurements; 2) photogrammetric areaanalysis; 3) gingival biopsy; 4) in vitro stage; 5)surgical procedure; and 6) post-surgical care andfollow-up.
Clinical Measurements Clinical measurements were taken at baseline and3, 6, and 12 months postoperatively. The measure-ments comprised an assessment of plaque index(PI),27 gingival index (GI),28 probing depth (PD),clinical attachment level (CAL), recession depth(RD), recession width (RW), KT, thickness of thegingiva (TG), and dentinal hypersensitivity (DH). Tostandardize the clinical measurements and thephotogrammetric analysis, acrylic stents were pre-pared on patients’ casts. PD (three points), CAL(three points), RD (three points), RW (cemento-enamel junction [CEJ]), and KT (mid) were mea-sured with a Williams periodontal probe. The TG was
measured by digital caliper with the help of anendodontic spreader¶ with a silicone stopper underlocal anesthesia. The endodontic spreader punctu-ated the mucosa vertically until resistance was feltfrom a point (mid) 3 mm below the gingival margin.The DH was evaluated with a visual analog score(VAS).29
Photogrammetric Analysis To perform a measurement directly on a photo-graph, its scale, the shooting angle, and the camera’sparameters (focal length, etc.) should be known. If there are fixed points on the photograph that can beused for standardization, affine transformation canuse those coordinates to calculate the scale of thephotograph. In this study, photographs of the positionof the occlusal stents in relation to the tooth are takenwith a digital camera at baseline and 3, 6, and 12months. At least five constant points in the occlusalstents helped calculate the area of recession withcomputer-assisted digitizing software.# Using thiscomputer program, the percentage of root coverage(PRC) was calculated with the following formula:
¶ Kerr, Karlsruhe, Germany.# Netcad 5.1, Ulusal CAD ve GIS Cxozumleri, Ankara, Turkey.
J Periodontol • October 2013 Koseoglu, Duran, Saglam, Bozkurt, Kırtıloglu, Hakkı
1417

8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 3/9
[presurgery area (mm2) - post-surgery area(mm2) / presurgery area (mm2)] · 100
Gingival Biopsy After local anesthesia, a window (3 · 3 mm borderand 1 mm thickness) containing epithelium was
removed from the palatal mucosa, and a smallportion (2 · 2 · 1 mm) of connective tissue biopsywas obtained with a surgical blade. The window wasthen replaced. Slight pressure with sterile gauze wasapplied to the donor site to control bleeding. Healingwas uneventful, and there was no need for suturing inmost cases. The sample was immediately placed inDulbecco modified Eagle medium (DMEM)** con-taining 10% fetal bovine serum (FBS)†† and antibi-otics (100 IU/mL penicillin and 100 mg/mLstreptomycin)‡‡ in a sterile tube.§§
In Vitro Stage
The samples were rinsed in phosphate-bufferedsaline (PBS)ii and transferred into a Petri dish.¶¶ If an epithelial layer was present, it was peeled off gently from the connective tissue. The connectivetissue sample was cut into small pieces and rinsedwith biopsy medium. Small pieces of connectivetissue were incubated with medium containing 10%FBS and antibiotics (penicillin and streptomycin)without moving for 24 hours. After cells were 70%to 80% confluent on the surface of the Petri dishes,they were passaged. When they reached passage 3,they were checked for mycoplasma contamination
before surgical intervention. Gingival fibroblasts atpassage 3 were seeded onto collagen membranes,the area of which had been previously calculated.The calculation of the area was performed on atemplate prepared during control surgery, and thetemplates were photographed on the paper at milli-meter scales. Photogrammetric analysis was per-formed to ensure an appropriate cell density onthe membranes. The cells were seeded onto thecollagen membranes at a density of 150,000 cells/cm2 using tissue culture inserts.## They were thenincubated for 48 hours and transferred to 35-mmculture dishes.*** Before the cells were transferred tothe surgical unit for surgical intervention, the cells onthe membranes were rinsed with PBS five times toeliminate remnants of FBS. All procedures wereperformed in a Class II laminar cabinet and an air-filtered area. As cell amplification by culture mighthave a xenogenic risk due to the FBS, the rawmaterials for the serum were imported only fromInternational Office of Epizootics countries where nobovine spongiform encephalopathy cases have everbeen reported.
Before the clinical phase of the therapy, the mosteffective scaffold was selected according to the re-
sults of preclinical study. The adhesion, proliferation,
and type I collagen mRNA expression of the gingi-val fibroblasts on different membranes, includingcollagen,††† an acellular dermal matrix‡‡‡ and poly-lactic acid, polyglycolic acid, and lactide/glycolidecopolymer§§§ biodegradable membranes, were an-alyzed. The data revealed that seeding favors the
adherence and proliferation of primary gingivalfibroblasts on collagen-based membrane (un-published data).
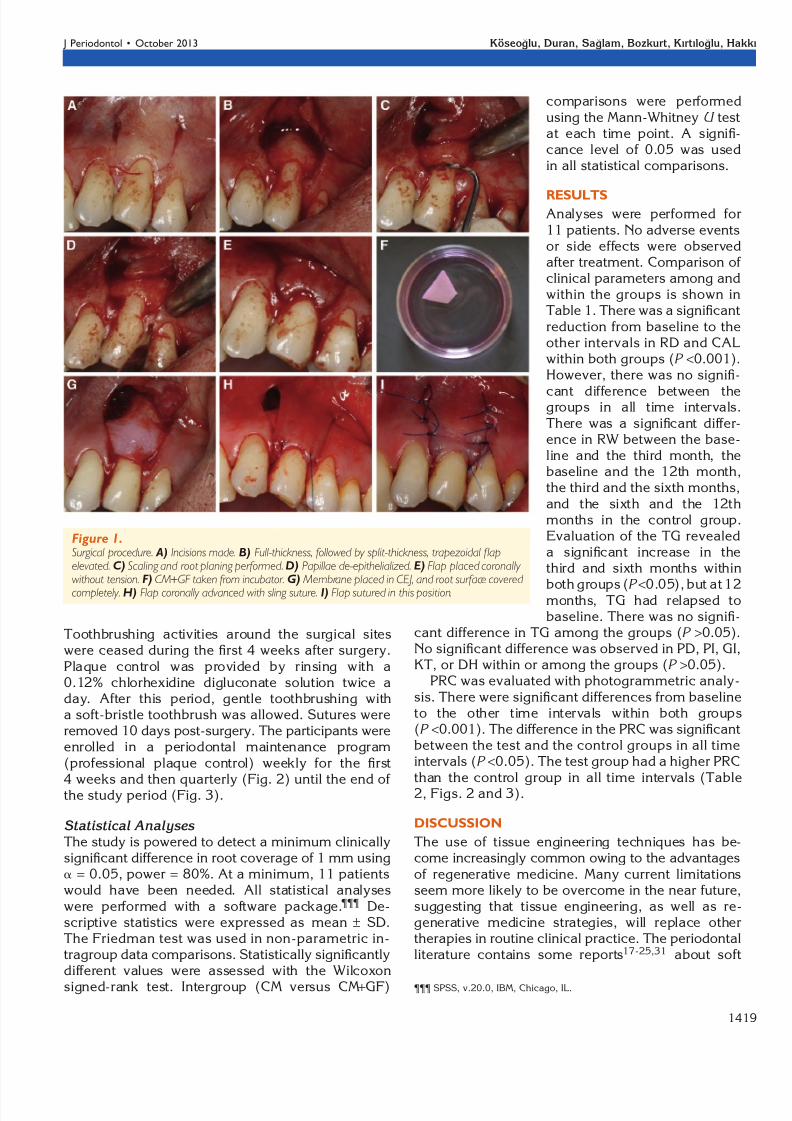
Surgical Procedure In each study group, the surgical procedures wereperformed by the same surgeon (SK). The test andcontrol sites were determined randomly by a cointoss. The participants were masked during the studyperiod. Extraoral antisepsis was provided with al-cohol and intraoral antisepsis with a 0.12% chlo-rhexidine rinse.iii The sites were treated using thetechnique described by Shieh et al.30 After rootplaning, an intrasulcular incision was extended tohorizontal incisions mesially and distally. The local-ization of the horizontal incisions was determinedaccording to the recession depth. These incisionswere perpendicular to the bone surface. Two verticalreleasing incisions were extended apically into thealveolar mucosa to displace the flap coronally. Re-verse incisions were made in the apical end of thevertical incision to loosen the flap (Fig. 1A). Fol-lowing elevation of a full-thickness flap, a split-thickness flap was elevated (Fig. 1B). At least 3 mmof bone surrounding the denuded root was exposed.
Scaling and root planing were performed (Fig. 1C).The papillae adjacent to the involved tooth werede-epithelialized (Figs. 1D and 1E). A resorbablecollagen membrane was trimmed and fixed overthe root and the surrounding bone (Fig. 1F). Thecoronal margin of the membrane was placed atthe CEJ (Fig. 1G). The flap was then coronally ad-vanced to totally cover the membrane with a slingsuture, and it was sutured in that position (Figs. 1Hand 1I). As a comparison, CM+GF was used insteadof the collagen membrane in the test group. Theside of the membrane with the cells was placed
carefully at the gingival side.
Post-Surgical Care and Follow-Up Postoperative instructions were given to each patient,and analgesics and mouthwash were prescribed.
** Biological Industries, Belt Haemek, Israel.†† Biological Industries.‡‡ Biological Industries.§§ Corning, Corning, NY.ii Biological Industries.¶¶ Corning.## Millipore, Billerica, MA.*** Corning.††† Collagene AT, Centro di Odontoiatria Operative, Padova, Italy.‡‡‡ SureDerm, Hans Biomed, Seoul, South Korea.§§§ Biomesh, Samyang, Seoul, South Korea.iii Klorhex, Drogsan, Ankara, Turkey.
Efficacy of Collagen Membrane with Autologous Fibroblasts Volume 84 • Number 10
1418
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 4/9
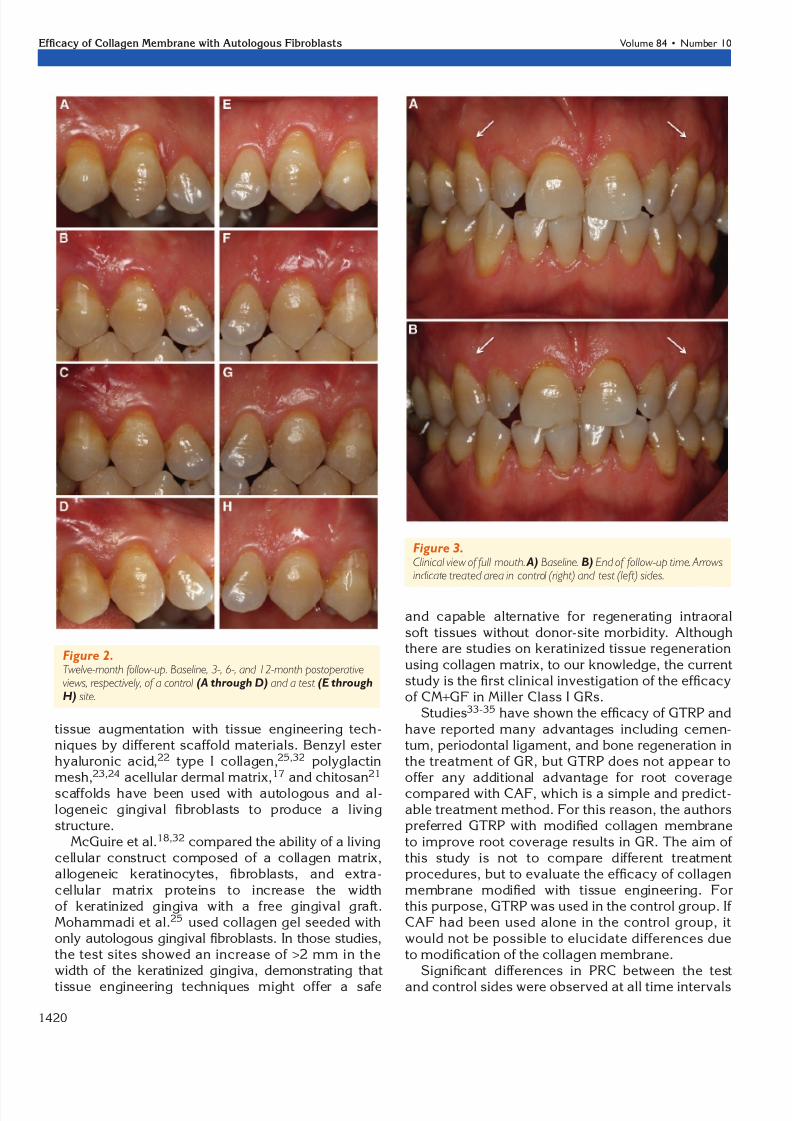
Toothbrushing activities around the surgical siteswere ceased during the first 4 weeks after surgery.Plaque control was provided by rinsing with a0.12% chlorhexidine digluconate solution twice aday. After this period, gentle toothbrushing witha soft-bristle toothbrush was allowed. Sutures wereremoved 10 days post-surgery. The participants wereenrolled in a periodontal maintenance program(professional plaque control) weekly for the first4 weeks and then quarterly (Fig. 2) until the end of the study period (Fig. 3).
Statistical Analyses The study is powered to detect a minimum clinicallysignificant difference in root coverage of 1 mm usinga = 0.05, power = 80%. At a minimum, 11 patientswould have been needed. All statistical analyseswere performed with a software package.¶¶¶ De-scriptive statistics were expressed as mean – SD.The Friedman test was used in non-parametric in-tragroup data comparisons. Statistically significantlydifferent values were assessed with the Wilcoxon
signed-rank test. Intergroup (CM versus CM+GF)
comparisons were performedusing the Mann-Whitney U testat each time point. A signifi-cance level of 0.05 was usedin all statistical comparisons.
RESULTS
Analyses were performed for11 patients. No adverse eventsor side effects were observedafter treatment. Comparison of clinical parameters among andwithin the groups is shown inTable 1. There was a significantreduction from baseline to theother intervals in RD and CALwithin both groups (P <0.001).However, there was no signifi-
cant difference between thegroups in all time intervals.There was a significant differ-ence in RW between the base-line and the third month, thebaseline and the 12th month,the third and the sixth months,and the sixth and the 12thmonths in the control group.Evaluation of the TG revealeda significant increase in thethird and sixth months within
both groups (P <
0.05), but at 12months, TG had relapsed tobaseline. There was no signifi-
cant difference in TG among the groups (P >0.05).No significant difference was observed in PD, PI, GI,KT, or DH within or among the groups (P >0.05).
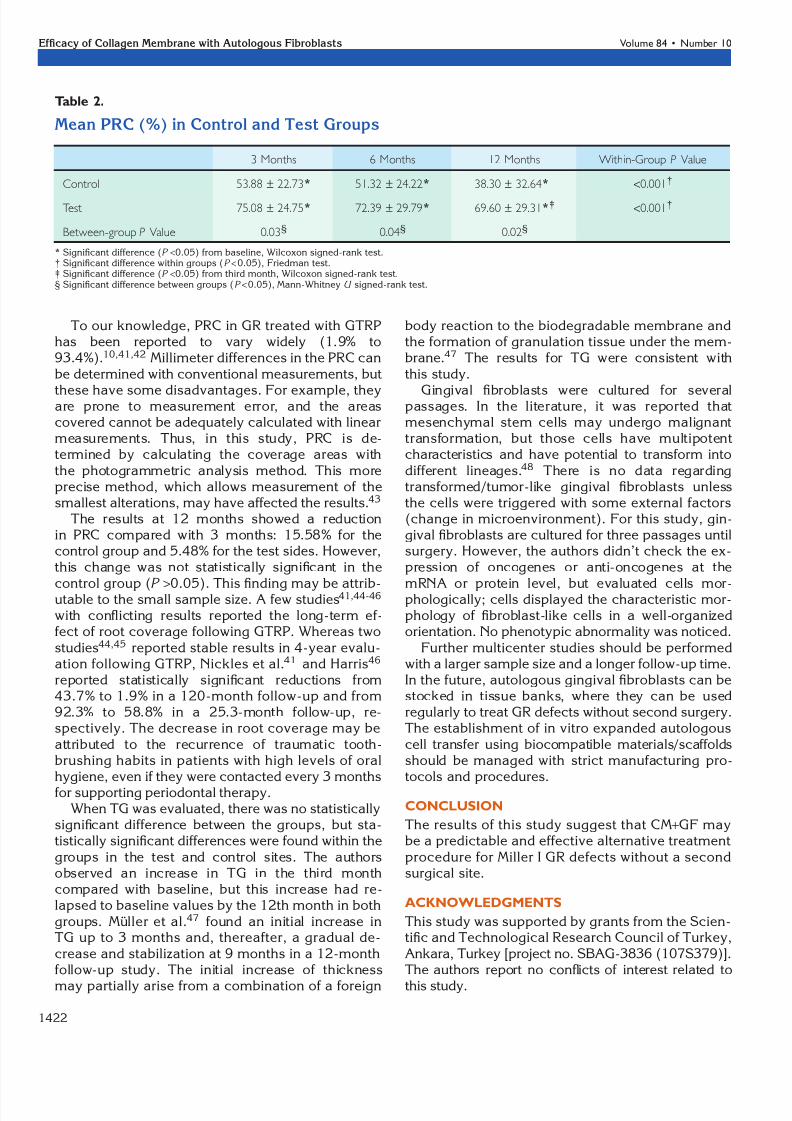
PRC was evaluated with photogrammetric analy-sis. There were significant differences from baselineto the other time intervals within both groups(P <0.001). The difference in the PRC was significantbetween the test and the control groups in all timeintervals (P <0.05). The test group had a higher PRCthan the control group in all time intervals (Table2, Figs. 2 and 3).
DISCUSSION
The use of tissue engineering techniques has be-come increasingly common owing to the advantagesof regenerative medicine. Many current limitationsseem more likely to be overcome in the near future,suggesting that tissue engineering, as well as re-generative medicine strategies, will replace othertherapies in routine clinical practice. The periodontalliterature contains some reports17-25,31 about soft
Figure 1.Surgical procedure. A) Incisions made. B) Full-thickness, followed by split-thickness, trapezoidal flapelevated. C) Scaling and root planing performed. D) Papillae de-epithelialized. E) Flap placed coronally without tension. F) CM+GF taken from incubator. G) Membrane placed in CEJ, and root surface covered
completely. H) Flap coronally advanced with sling suture. I) Flap sutured in this position.
¶¶¶ SPSS, v.20.0, IBM, Chicago, IL.
J Periodontol • October 2013 Koseoglu, Duran, Saglam, Bozkurt, Kırtıloglu, Hakkı
1419
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 5/9
tissue augmentation with tissue engineering tech-niques by different scaffold materials. Benzyl esterhyaluronic acid,22 type I collagen,25,32 polyglactinmesh,23,24 acellular dermal matrix,17 and chitosan21
scaffolds have been used with autologous and al-logeneic gingival fibroblasts to produce a livingstructure.
McGuire et al.18,32 compared the ability of a livingcellular construct composed of a collagen matrix,allogeneic keratinocytes, fibroblasts, and extra-cellular matrix proteins to increase the widthof keratinized gingiva with a free gingival graft.Mohammadi et al.25 used collagen gel seeded withonly autologous gingival fibroblasts. In those studies,the test sites showed an increase of >2 mm in thewidth of the keratinized gingiva, demonstrating that
tissue engineering techniques might offer a safe
and capable alternative for regenerating intraoralsoft tissues without donor-site morbidity. Althoughthere are studies on keratinized tissue regenerationusing collagen matrix, to our knowledge, the currentstudy is the first clinical investigation of the efficacyof CM+GF in Miller Class I GRs.
Studies33-35 have shown the efficacy of GTRP andhave reported many advantages including cemen-tum, periodontal ligament, and bone regeneration inthe treatment of GR, but GTRP does not appear tooffer any additional advantage for root coveragecompared with CAF, which is a simple and predict-able treatment method. For this reason, the authorspreferred GTRP with modified collagen membraneto improve root coverage results in GR. The aim of this study is not to compare different treatmentprocedures, but to evaluate the efficacy of collagenmembrane modified with tissue engineering. Forthis purpose, GTRP was used in the control group. If CAF had been used alone in the control group, itwould not be possible to elucidate differences dueto modification of the collagen membrane.
Significant differences in PRC between the test
and control sides were observed at all time intervals
Figure 2.Twelve-month follow-up. Baseline, 3-, 6-, and 12-month postoperativeviews, respectively, of a control (A through D) and a test (E throughH) site.
Figure 3.Clinical view of full mouth. A) Baseline. B) End of follow-up time. Arrowsindicate treated area in control (right) and test (left) sides.
Efficacy of Collagen Membrane with Autologous Fibroblasts Volume 84 • Number 10
1420

8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 6/9
(P <0.05). The relative values expressed as a per-centage at the 12th month were 69.6% and 38.3%,respectively (Table 2). Autologous gingival fibro-blasts may account for this difference between thetest and control groups. Gingival fibroblasts, whichhave an important role in oral soft tissue re-generation, appear in the wound area at early stages
and proliferate rapidly as the tissue heals. They ac-
celerate the healing process by upregulation of matrix deposition (collagens, proteoglycans, hy-aluronic acid, elastin, and laminin).36,37 In addition,fibroblasts synthesize various growth factors suchas platelet-derived growth factor, epidermal growthfactor, transforming growth factor a and b, fibroblastgrowth factor, and insulin-like growth factor, as well
as cytokines that stimulate wound healing.38-40
Table 1.
Mean – SD Clinical Parameters of Control and Test Groups
Parameter Baseline 3 Months 6 Months 12 Months Within-Group P Value
PD (mm)
Control 1.24 – 0.15 1.45 – 0.47 1.36 – 0.40 1.24 – 0.33 0.27Test 1.21 – 0.22 1.33 – 0.39 1.30 – 0.31 1.23 – 0.25 0.7
Between-group P Value 0.56 0.56 0.08 0.1
PI
Control 1.00 – 0.00 1.09 – 0.30 1.00 – 0.00 1.10 – 0.31 0.57
Test 1.09 – 0.30 1.00 – 0.00 1.18 – 0.40 1.09 – 0.30 0.49
Between-group P Value 0.74 0.74 0.47 1
GI
Control 1.00 – 0.00 1.00 – 0.00 1.09 – 0.30 1.09 – 0.30 0.39
Test 1.00 – 0.00 1.00 – 0.00 1.09 – 0.30 1.09 – 0.30 0.39
Between-group P Value 1 1 1 1
RD (mm)Control 1.72 – 0.71 0.72 – 0.60* 0.73 – 0.55* 0.78 – 0.71* <0.001†
Test 1.62 – 0.52 0.33 – 0.47* 0.33 – 0.49* 0.42 – 0.63* <0.001†
Between-group P Value 0.94 0.1 0.05 0.11
RW (mm)
Control 3.86 – 0.63 2.72 – 1.55* 3.68 – 1.00‡ 3.09 – 0.83*§ 0.002†
Test 3.63 – 0.80 2.13 – 1.81* 2.13 – 1.81* 1.90 – 1.62* 0.003†
Between-group P Value 0.94 0.1 0.56 0.11
CAL (mm)
Control 2.96 – 0.73 2.17 – 0.84* 2.10 – 0.66* 2 – 0.80* 0.006†
Test 2.83 – 0.57 1.66 – 0.69* 1.63 – 0.70* 1.66 – 0.62* <0.001†
Between-group P Value 0.94 0.17 0.08 0.33
KT (mm)
Control 2.95 – 1.01 2.90 – 1.28 2.63 – 0.89 2.59 – 0.97 0.57
Test 3.27 – 1.34 3.09 – 1.15 3.22 – 1.12 2.86 – 1.05 0.75
Between-group P Value 0.69 0.79 0.3 0.47
TG (mm)
Control 1.00 – 0.31 1.38 – 0.35* 1.26 – 0.33* 1.09 – 0.31‡§ 0.003†
Test 1.07 – 0.29 1.34 – 0.45* 1.30 – 0.25* 1.15 – 0.27‡§ 0.003†
Between-group P Value 0.47 0.84 0.79 0.56
DH
Control 2.36 – 3.04 2.45 – 2.11 2 – 1.84 2.63 – 2.50 0.38
Test 2.54 – 2.11 2.72 – 2.05 2.27 – 2.10 1.90 – 1.92 0.06
Between-group P Value 0.47 0.69 0.84 0.47
* Significant difference (P <0.05) from baseline, Wilcoxon signed-rank test.† Significant difference within groups (P <0.05), Friedman test.‡ Significant difference (P <0.05) from third month, Wilcoxon signed-rank test.§ Significant difference (P <0.05) from sixth month, Wilcoxon signed-rank test.
J Periodontol • October 2013 Koseoglu, Duran, Saglam, Bozkurt, Kırtıloglu, Hakkı
1421
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 7/9
To our knowledge, PRC in GR treated with GTRPhas been reported to vary widely (1.9% to93.4%).10,41,42 Millimeter differences in the PRC canbe determined with conventional measurements, but
these have some disadvantages. For example, theyare prone to measurement error, and the areascovered cannot be adequately calculated with linearmeasurements. Thus, in this study, PRC is de-termined by calculating the coverage areas withthe photogrammetric analysis method. This moreprecise method, which allows measurement of thesmallest alterations, may have affected the results.43
The results at 12 months showed a reductionin PRC compared with 3 months: 15.58% for thecontrol group and 5.48% for the test sides. However,this change was not statistically significant in the
control group (P >
0.05). This finding may be attrib-utable to the small sample size. A few studies41,44-46
with conflicting results reported the long-term ef-fect of root coverage following GTRP. Whereas twostudies44,45 reported stable results in 4-year evalu-ation following GTRP, Nickles et al.41 and Harris46
reported statistically significant reductions from43.7% to 1.9% in a 120-month follow-up and from92.3% to 58.8% in a 25.3-month follow-up, re-spectively. The decrease in root coverage may beattributed to the recurrence of traumatic tooth-brushing habits in patients with high levels of oralhygiene, even if they were contacted every 3 monthsfor supporting periodontal therapy.
When TG was evaluated, there was no statisticallysignificant difference between the groups, but sta-tistically significant differences were found within thegroups in the test and control sites. The authorsobserved an increase in TG in the third monthcompared with baseline, but this increase had re-lapsed to baseline values by the 12th month in bothgroups. Muller et al.47 found an initial increase inTG up to 3 months and, thereafter, a gradual de-crease and stabilization at 9 months in a 12-monthfollow-up study. The initial increase of thickness
may partially arise from a combination of a foreign
body reaction to the biodegradable membrane andthe formation of granulation tissue under the mem-brane.47 The results for TG were consistent withthis study.
Gingival fibroblasts were cultured for severalpassages. In the literature, it was reported thatmesenchymal stem cells may undergo malignanttransformation, but those cells have multipotentcharacteristics and have potential to transform intodifferent lineages.48 There is no data regardingtransformed/tumor-like gingival fibroblasts unlessthe cells were triggered with some external factors(change in microenvironment). For this study, gin-gival fibroblasts are cultured for three passages untilsurgery. However, the authors didn’t check the ex-pression of oncogenes or anti-oncogenes at the
mRNA or protein level, but evaluated cells mor-phologically; cells displayed the characteristic mor-phology of fibroblast-like cells in a well-organizedorientation. No phenotypic abnormality was noticed.
Further multicenter studies should be performedwith a larger sample size and a longer follow-up time.In the future, autologous gingival fibroblasts can bestocked in tissue banks, where they can be usedregularly to treat GR defects without second surgery.The establishment of in vitro expanded autologouscell transfer using biocompatible materials/scaffoldsshould be managed with strict manufacturing pro-tocols and procedures.
CONCLUSION
The results of this study suggest that CM+GF maybe a predictable and effective alternative treatmentprocedure for Miller I GR defects without a secondsurgical site.
ACKNOWLEDGMENTS
This study was supported by grants from the Scien-tific and Technological Research Council of Turkey,Ankara, Turkey [project no. SBAG-3836 (107S379)].The authors report no conflicts of interest related to
this study.
Table 2.
Mean PRC (%) in Control and Test Groups
3 Months 6 Months 12 Months Within-Group P Value
Control 53.88 – 22.73* 51.32 – 24.22* 38.30 – 32.64* <0.001†
Test 75.08 – 24.75* 72.39 – 29.79* 69.60 – 29.31*‡ <0.001†
Between-group P Value 0.03§ 0.04§ 0.02§
* Significant difference (P <0.05) from baseline, Wilcoxon signed-rank test.† Significant difference within groups (P <0.05), Friedman test.‡ Significant difference (P <0.05) from third month, Wilcoxon signed-rank test.§ Significant difference between groups (P <0.05), Mann-Whitney U signed-rank test.
Efficacy of Collagen Membrane with Autologous Fibroblasts Volume 84 • Number 10
1422
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 8/9
REFERENCES
1. Lindhe J, Maynard JG, Miller PD, et al. Consensusreport. Mucogingival therapy. Ann Periodontol 1996;1:702-706.
2. Grupe HE, Warren RF. Repair of gingival defects bya sliding flap operation. J Periodontol 1956;27:92-95.
3. Harvey PM. Management of advanced periodontitis. I.
Preliminary report of a method of surgical reconstruc-tion. N Z Dent J 1965;61:180-187.
4. Sullivan HC, Atkins JH. Free autogenous gingivalgrafts. 3. Utilization of grafts in the treatment of gingivalrecession. Periodontics 1968;6:152-160.
5. Harris RJ. A comparative study of root coverageobtained with an acellular dermal matrix versus a con-nective tissue graft: Results of 107 recession defects in50 consecutively treated patients. Int J Periodontics
Restorative Dent 2000;20:51-59.6. Langer B, Langer L. Subepithelial connective tissue
graft technique for root coverage. J Periodontol 1985;56:715-720.
7. Nelson SW. The subpedicle connective tissue graft. A
bilaminar reconstructive procedure for the coverage of denuded root surfaces. J Periodontol 1987;58:95-102.8. Borghetti A, Glise JM, Monnet-Corti V, Dejou J.
Comparative clinical study of a bioabsorbable mem-brane and subepithelial connective tissue graft in thetreatment of human gingival recession. J Periodontol 1999;70:123-130.
9. Karring T, Nyman S, Gottlow J, Laurell L. Developmentof the biological concept of guided tissue regeneration— Animal and human studies. Periodontol 2000 1993;1:26-35.
10. Wang HL, Modarressi M, Fu JH. Utilizing collagenmembranes for guided tissue regeneration-based rootcoverage. Periodontol 2000 2012;59:140-157.
11. Cortellini P, Clauser C, Prato GP. Histologic assessment
of new attachment following the treatment of a humanbuccal recession by means of a guided tissue regener-ation procedure. J Periodontol 1993;64:387-391.
12. Parma-Benfenati S, Tinti C. Histologic evaluation of new attachment utilizing a titanium-reinforced barriermembrane in a mucogingival recession defect. A casereport. J Periodontol 1998;69:834-839.
13. Vincenzi G, De Chiesa A, Trisi P. Guided tissue re-generation using a resorbable membrane in gingivalrecession-type defects: A histologic case report inhumans. Int J Periodontics Restorative Dent 1998;18:24-33.
14. Leknes KN, Amarante ES, Price DE, Bøe OE, SkavlandRJ, Lie T. Coronally positioned flap procedures with
or without a biodegradable membrane in the treatmentof human gingival recession. A 6-year follow-up study.J Clin Periodontol 2005;32:518-529.
15. Lee EJ, Meraw SJ, Oh TJ, Giannobile WV, Wang HL.Comparative histologic analysis of coronally advancedflap with and without collagen membrane for rootcoverage. J Periodontol 2002;73:779-788.
16. Amarante ES, Leknes KN, Skavland J, Lie T. Coronallypositioned flap procedures with or without a bioabsorb-able membrane in the treatment of human gingivalrecession. J Periodontol 2000;71:989-998.
17. Jhaveri HM, Chavan MS, Tomar GB, Deshmukh VL,Wani MR, Miller PD Jr. Acellular dermal matrixseeded with autologous gingival fibroblasts for thetreatment of gingival recession: A proof-of-concept
study. J Periodontol 2010;81:616-625.
18. McGuire MK, Scheyer ET, Nevins ML, et al. Livingcellular construct for increasing the width of keratinizedgingiva: Results from a randomized, within-patient,controlled trial. J Periodontol 2011;82:1414-1423.
19. Morelli T, Neiva R, Nevins ML, et al. Angiogenicbiomarkers and healing of living cellular constructs.J Dent Res 2011;90:456-462.
20. Rodrigues AZ, Oliveira PT, Novaes AB Jr., Maia LP,Souza SL, Palioto DB. Evaluation of in vitro humangingival fibroblast seeding on acellular dermal matrix.Braz Dent J 2010;21:179-189.
21. Lotfi G, Shokrgozar MA, Mofid R, et al. A clinical andhistologic evaluation of gingival fibroblasts seeding ona chitosan-based scaffold and its effect on the widthof keratinized gingiva in dogs. J Periodontol 2011;82:1367-1375.
22. Prato GP, Rotundo R, Magnani C, Soranzo C, Muzzi L,Cairo F. An autologous cell hyaluronic acid grafttechnique for gingival augmentation: A case series.J Periodontol 2003;74:262-267.
23. McGuire MK, Nunn ME. Evaluation of the safety andefficacy of periodontal applications of a living tissue-
engineered human fibroblast-derived dermal sub-stitute. I. Comparison to the gingival autograft: Arandomized controlled pilot study. J Periodontol 2005;76:867-880.
24. Wilson TG Jr., McGuire MK, Nunn ME. Evaluation of the safety and efficacy of periodontal applications of a living tissue-engineered human fibroblast-deriveddermal substitute. II. Comparison to the subepithelialconnective tissue graft: A randomized controlled feasi-bility study. J Periodontol 2005;76:881-889.
25. Mohammadi M, Shokrgozar MA, Mofid R. Culture of human gingival fibroblasts on a biodegradable scaffoldand evaluation of its effect on attached gingiva: Arandomized, controlled pilot study. J Periodontol 2007;
78:1897-1903.26. Miller PD Jr. A classification of marginal tissue re-cession. Int J Periodontics Restorative Dent 1985;5:8-13.
27. Silness J, Loe H. Periodontal disease in pregnancy. II.Correlation between oral hygiene and periodontalcondition. Acta Odontol Scand 1964;22:121-135.
28. Loe H, Silness J. Periodontal disease in pregnancy. I.Prevalence and severity. Acta Odontol Scand 1963;21:533-551.
29. Huskisson EC. Measurement of pain. Lancet 1974;2:1127-1131.
30. Shieh AT, Wang HL, O’Neal R, Glickman GN, MacNeilRL. Development and clinical evaluation of a rootcoverage procedure using a collagen barrier mem-
brane. J Periodontol 1997;68:770-778.31. Yamada K, Yamaura J, Katoh M, Hata K, Okuda K,
Yoshie H. Fabrication of cultured oral gingiva by tissueengineering techniques without materials of animalorigin. J Periodontol 2006;77:672-677.
32. McGuire MK, Scheyer ET, Nunn ME, Lavin PT. A pilotstudy to evaluate a tissue-engineered bilayered celltherapy as an alternative to tissue from the palate.J Periodontol 2008;79:1847-1856.
33. Cetiner D, Parlar A, Balosx K, Alpar R. Comparativeclinical study of connective tissue graft and two typesof bioabsorbable barriers in the treatment of localizedgingival recessions. J Periodontol 2003;74:1196-1205.
34. Wang HL, Bunyaratavej P, Labadie M, Shyr Y, MacNeilRL. Comparison of 2 clinical techniques for treatment
J Periodontol • October 2013 Koseoglu, Duran, Saglam, Bozkurt, Kırtıloglu, Hakkı
1423
8/12/2019 Articulo CIOE Maria Hp
http://slidepdf.com/reader/full/articulo-cioe-maria-hp 9/9
of gingival recession. J Periodontol 2001;72:1301-1311.
35. Paolantonio M. Treatment of gingival recessions bycombined periodontal regenerative technique, guidedtissue regeneration, and subpedicle connective tissuegraft. A comparative clinical study. J Periodontol 2002;73:53-62.
36. McCulloch CA, Bordin S. Role of fibroblast subpopula-tions in periodontal physiology and pathology. J Peri- odontal Res 1991;26:144-154.
37. Sappino AP, Schurch W, Gabbiani G. Differentiationrepertoire of fibroblastic cells: Expression of cytoskel-etal proteins as marker of phenotypic modulations.Lab Invest 1990;63:144-161.
38. Hill SJ, Ebersole JL. The effect of lipopolysaccharideon growth factor-induced mitogenesis in human gingi-val fibroblasts. J Periodontol 1996;67:1274-1280.
39. Bartold PM. Connective tissues of the periodontium —Preface. Periodontol 2000 2000;24:7-8.
40. Bartold PM, Narayanan AS. Molecular and cell biologyof healthy and diseased periodontal tissues. Periodon- tol 2000 2006;40:29-49.
41. Nickles K, Ratka-Kruger P, Neukranz E, Raetzke P,Eickholz P. Ten-year results after connective tissuegrafts and guided tissue regeneration for root cover-age. J Periodontol 2010;81:827-836.
42. Harris RJ. A comparison of 2 root coverage tech-niques: Guided tissue regeneration with a bioabsorb-able matrix style membrane versus a connectivetissue graft combined with a coronally positionedpedicle graft without vertical incisions. Results of
a series of consecutive cases. J Periodontol 1998;69:1426-1434.
43. Rosetti EP, Marcantonio RA, Rossa C Jr., Chaves ES,Goissis G, Marcantonio E Jr. Treatment of gingivalrecession: Comparative study between subepithelialconnective tissue graft and guided tissue regeneration.J Periodontol 2000;71:1441-1447.
44. Prato GP, Clauser C, Tonetti MS, Cortellini P. Guidedtissue regeneration in gingival recessions. Periodontol 2000 1996;11:49-57.
45. Scabbia A, Trombelli L. Long-term stability of themucogingival complex following guided tissue regen-eration in gingival recession defects. J Clin Periodontol 1998;25:1041-1046.
46. Harris RJ. GTR for root coverage: A long-term follow-up. Int J Periodontics Restorative Dent 2002;22:55-61.
47. Muller HP, Stahl M, Eger T. Dynamics of mucosaldimensions after root coverage with a bioresorbablemembrane. J Clin Periodontol 2000;27:1-8.
48. Liu J, Zhang Y, Bai L, Cui X, Zhu J. Rat bone marrowmesenchymal stem cells undergo malignant transfor-mation via indirect co-cultured with tumour cells. Cell
Biochem Funct 2012;30:650-656.
Correspondence: Dr. Serhat Koseoglu, Department of Periodontology, Faculty of Dentistry, _Izmir Katip CxelebiUniversity, _Izmir 35640, Turkey. E-mail: [email protected].
Submitted August 30, 2012; accepted for publicationOctober 30, 2012.
Efficacy of Collagen Membrane with Autologous Fibroblasts Volume 84 • Number 10
1424
Related Documents











