ARTHRITIS By Hasan & Hamza MA Physical Activity and Health Institute of Sport Sciences

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ARTHRITIS
ByHasan & Hamza
MA Physical Activity and Health
Institute of Sport Sciences

SEARCH ENGINE & RESULTS Under the Keyword of “Arthritis ”244,309 Articles on PubMed.“Osteoarthritis AND Physical Activity”2242 on PubMed“Meta-Analysis of 5 Year older” 13 Results <After Review> 9 were related to effectiveness of
some modalities intervention.4 were found relevant.

EXERCISE FOR LOWER LIMB OSTEOARTHIRITS Title of the Article:“Exercise for lower limb
osteoarthritis: systematic review incorporating trial sequential analysis and network meta-analysis”
Authors:Olalekan , Danielle and all. Published: 20 September 2013.
INTODUCTION: Osteoarthritis is the most common form of arthritis and one of
the leading cause of pain and disability worldwide.
*Prevalence of Hip OA is 25.3% & Knee OA is 45.7%
Economic Burden: Direct & Indirect Uk† (1990 to 2000) 36M working days were Lost OA Which cost €3.8bn ($5.1bn)Productivity loss to UK economy is being estimated about 1% of
total GNP(gross national product)/ Year.
USA total(direct and indirect) economical losses in 2003 is €95.8bn ($128 Bn)
* Murphy et al. One in four people may develop symptomatic hip osteoarthritis in his or her lifetime.2010
† National Collaborating Centre for Chronic Conditions 2008
METHODOLOGY: Network Meta-analysis of RCTs Information sources and search strategyOne Inf.Specialist develop strategies. And Six
Reviewer in pairs study the articles form data bases.
Exercise interventions were defined as any type of therapeutic exercise (land or water based), regardless of content, duration,
frequency, or intensity. Data Bases: Medline, Embase, CINAHL, AMED,
HMIC, CENTRAL, DARE and NHS EED. From Inception to March 2012 No language restriction and bibliography is also
studied.
STUDY SELECTION Study population: Adult of
clinical/Radiographical diagnosis of OA of hip or Knee.
Interventions: Therapeutic Exercise Comparator:other form of Ex or Control Group. Outcome measure: the core set of outcome
measures for clinical trials in osteoarthritis. include assessment of at least one of self reported pain and function
Study Design: RCT, Trials were excluded if they concerned pre-operative exercise therapy (immediately before or after surgery

QUALITY ASSESSMENT They used the Cochrane Collaboration’s
tool for assessing risk of bias for quality assessment of the included trials. The trials were graded (unclear, high, or low risk of bias) based on sequence generation, allocation concealment, blinding of outcome assessor, incomplete outcome data, and selective outcome reporting.

RESULTS: Number of Studies: 3796 full text articles 177
(Critical Reading)115(did not match inclusion criteria) 60 RCT selected (8218 patients).
Time Frame: The trials were published between 1989 and 2012. The maximum length of follow-up ranged from 4 weeks to 79 weeks (median 15 weeks).
Risk of bias of included trials: The potential risk of bias likely to be introduced by
incomplete data was high in 10 trials (18%). The risk of selective reporting bias was low in most trials (n=53,88%).

Fig 1 Study selection of trials examining exercise in treatment of lower limb osteoarthritis

CONCLUSION: Implications for practice: > It also shows that some therapeutic
intervention are more beneficial to others.
>Exercise programs that combine strengthening exercise with exercise aimed at increasing flexibility and aerobic capacity seem to be the “best” exercise option that clinicians can offer to patients as a
“core” treatment.
CONCLUSION:
Implications for research:Further research is required inHow? adhere people to exercise and PAWhich? patients with lower limb
osteoarthritis benefit most from exercise.
What? mode of delivery is beneficial for Intervention.

CONCLUSION: What this study adds As of the year 2002, there was enough
evidence to show significant benefit of exercise interventions versus no exercise in lower limb osteoarthritis, indicating that further trials of exercise versus no exercise are unlikely to overturn this positive result.
Evidence from the network meta-analysis, largely based on studies in knee osteoarthritis, indicates that a programmed combining flexibility, strengthening, and aerobic exercise is most likely to improve outcomes of pain and function
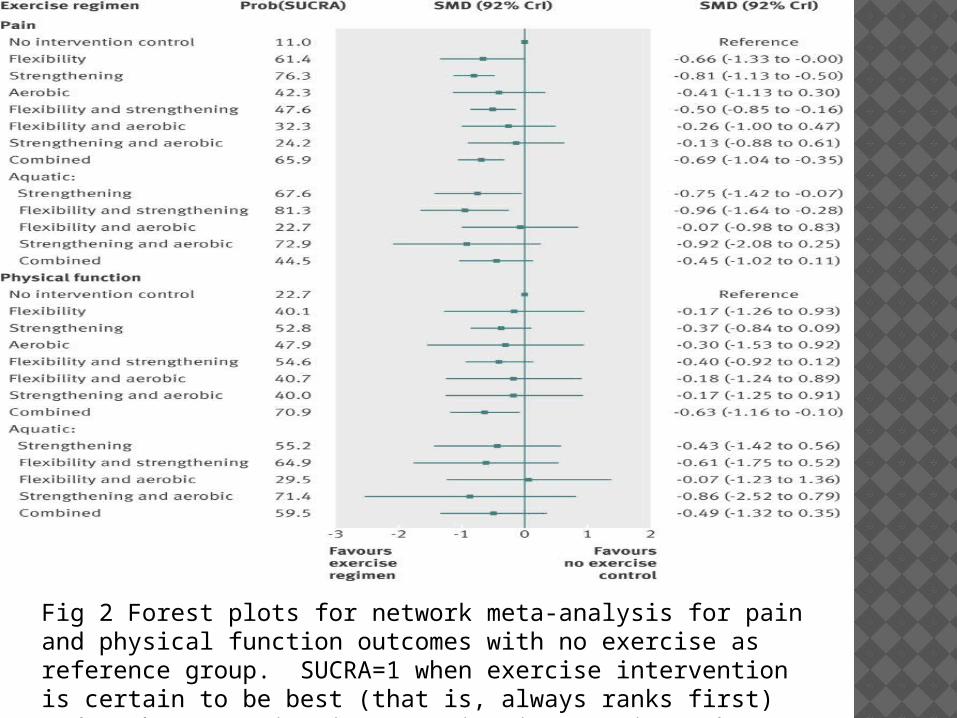
Fig 2 Forest plots for network meta-analysis for pain and physical function outcomes with no exercise as reference group. SUCRA=1 when exercise intervention is certain to be best (that is, always ranks first) and 0 when exercise intervention is certain to be worst
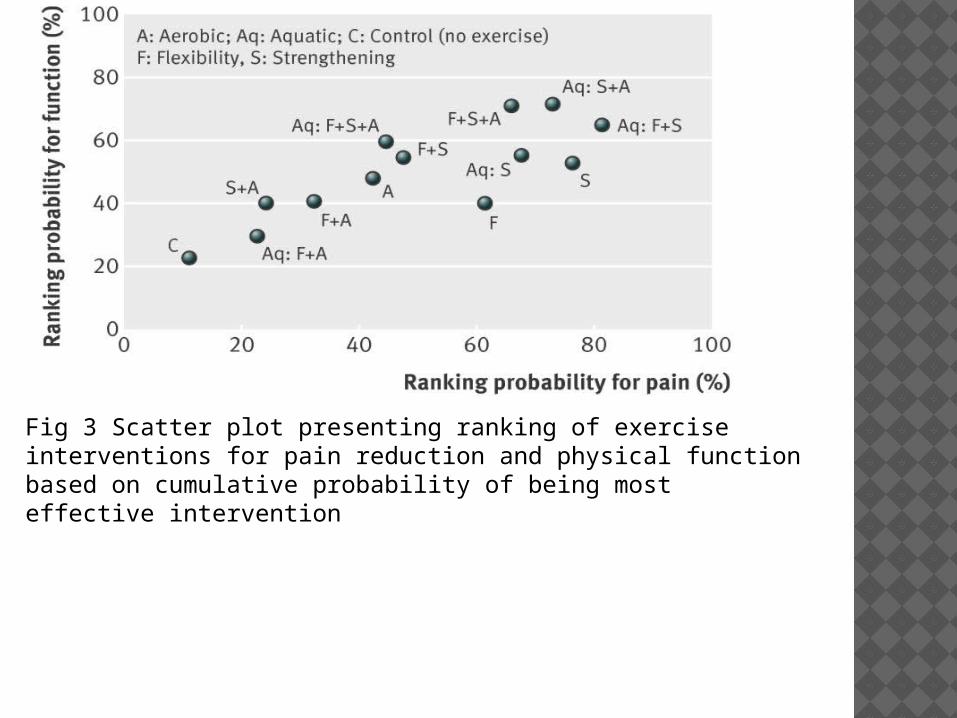
Fig 3 Scatter plot presenting ranking of exercise interventions for pain reduction and physical function based on cumulative probability of being most effective intervention
SUMMARY All studies shows The greatest
improvements were found in pain, quality of life, and functional status.

REFERENCES:
1-http: //www.ncbi.nlm.nih.gov/pmc/articles/PMC3779121/pdf/bmj.f5555.pdf
2-www.scopus.com 3- http://www.ncbi.nlm.nih.gov
Related Documents











