Antibiotics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Antibiotics
Antimicrobial drugs
Antimicrobial drugs
Antibiotics Synthetics
Antibiotic: Chemical produced by a microorganism that kills or inhibits the growth of another microorganism
Synthetic antimicrobial agent: Chemical that kills or inhibits the growth of microorganisms

Definition of AntibioticA substance of biological, semisynthetic (orsynthetic) origin of low molecular weight producedby a fungus or bacterium as secondary metabolitesthat inhibits or stop growth of other microorganismsin vitro and in vivo selectively, when it used in lowconcentration
Literal translation: anti – against, biotic – livingthings
Antibiotics cause greater harm to microorganismsthan to human host
Discovery of antibiotics
Alexander Fleming discovered penicillin while working with Staphylococcus. Noticed there were no Staph colonies growing near a mold contaminant. Identified mold as Penicillium and was producing a bactericidal substance that was effective against a wide range of microbes. But Fleming was unable to purify compound.Ernst Chain and Howard Florey successfully purified penicillinIn 1941 tested on human subject with life threaten Staphylococcus
aureus infection
Selman Waksman isolated streptomycin from soil bacterium Streptomyces
griseus
History and Development ofAntimicrobial Drugs
Antimicrobial action:
1. bacteriocidal - Kill bacteria2. bacteriostatic - Reversibly inhibit growth
Spectrum of activity:
1. Narrow spectrum: Gram positive only OR Gram negative only
2. Broad spectrum: Gram positive AND Gram negative(Disadvantage of broad spectrum is disruption of normal
flora)
Features of Antimicrobial Drugs

1. Diagnosis?
- Accurate history, physical exam, imaging, labs
-Microbiological tests
- Differential diagnosis
2. Host?
- Age
-Immunity
- Renal and liver function
- Allergies
- Pregnancy, breastfeeding
- Genetics
Principles of antibacterial therapy
3. Treatment strategy?
Which antibacterial drug?
- Empiric therapy ( treatment of an infection beforespecific culture information has been reported orobtained) in severe infections
- Definitive therapy
- Prophylaxis (treatment with antibiotics to prevent aninfection, as in intra-abdominal surgery)
Which route? Duration? Minimum duration 5 days (andthe patient has been afebrile for at least 3 days)
4. Observation (temperature, functons of kidneys and liver and other)
Principles of antibacterial therapy

Effects of combinations of antimicrobial drugs
Combination some times used to treat infections
When action of one drug enhances another, effect is synergistic
When action of one drug interferes with another, effect is antagonistic
When effect of combination is neither synergistic or antagonistic, effect said to be additive
Adverse effects
⚫ Allergic reactions⚫ Irritant effect on the ways of administration (i.v. - phlebitis,
i.m. - infiltration, orally - diarrhea)• Toxic effects• Disbacteriosis (Overuse of antibiotics can damage our normal/good bacteria. Many antibiotics prescribed by the doctor kill the good bacteria as well as the bad. With the good bacteria gone there is more room for bad microbes to invade!)• Formation of the drug resistance

Antimicrobial drug resistance
The acquired ability of a microorganism to resist
the effects of a chemotherapeutic agent to
which it is normally sensitive
Means that the bacteria survive and continue to multiply after administration of the antibiotic

Agriculture
Inpatient
Outpatient
Antibiotic Use Leads to Antibiotic Resistance
Factors promoting drug resistance Exposure to sub-optimal levels of antimicrobial
Exposure to microbes carrying resistance genes
Inappropriate drug use-
Lack of quality control in manufacture or outdated antimicrobial
Inadequate surveillance or defective susceptibility assays
Poverty or war
Use of antibiotics in foods-Antibiotics are used in animal feeds and sprayed on plants to prevent infection and promote growth

13
Antimicrobial Drug Resistance
• Resistance can be minimized by using antibiotics
correctly and only when needed
• Resistance to a certain antibiotic can be lost if
antibiotic is not used for several years
De-escalation of therapy
Once micro results are available, therapy can be targeted at the causative organism based on its antibiotic susceptibilities
May mean switching to a more narrow-spectrum antibiotic, which reduces negative effects on the body’s natural flora
15

Acquisition of resistance- Can be due to spontaneous mutation(vertical evolution)- Or acquisition of new genes:* horizontal transfer* Plasmid mediated
Antimicrobial Drug Resistance

Mechanisms Of Antibiotic Resistance
• Bacteria are capable of becoming resistant through several mechanisms
• One or many mechanisms may exist in an organism
• Multidrug-resistant bacteria often have multiple mechanisms
• Genes encoding resistance may exist on plasmid or chromosome
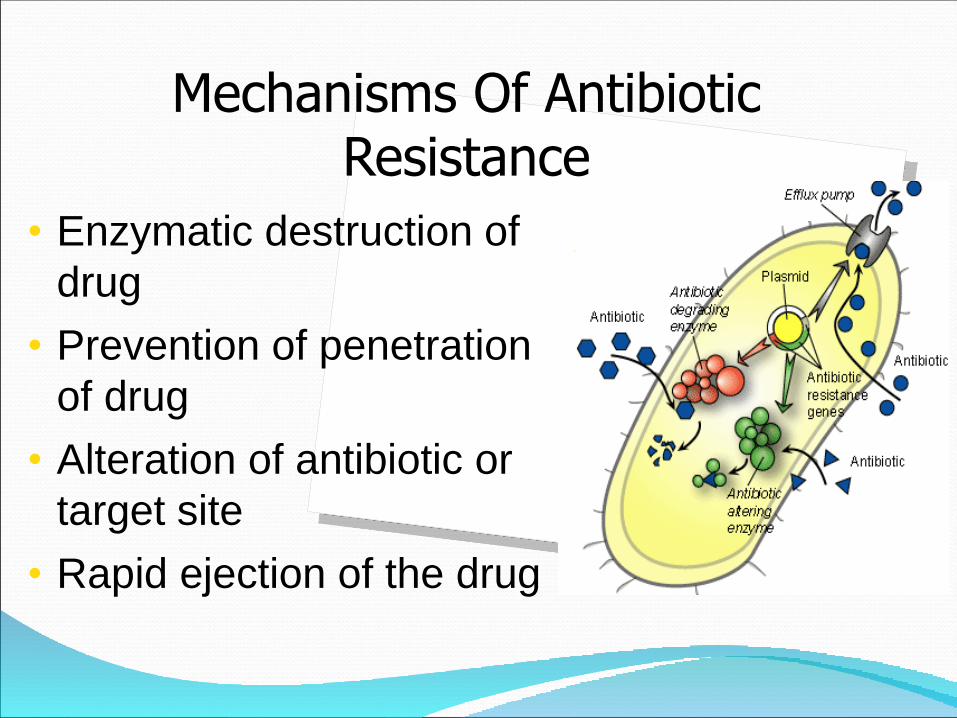
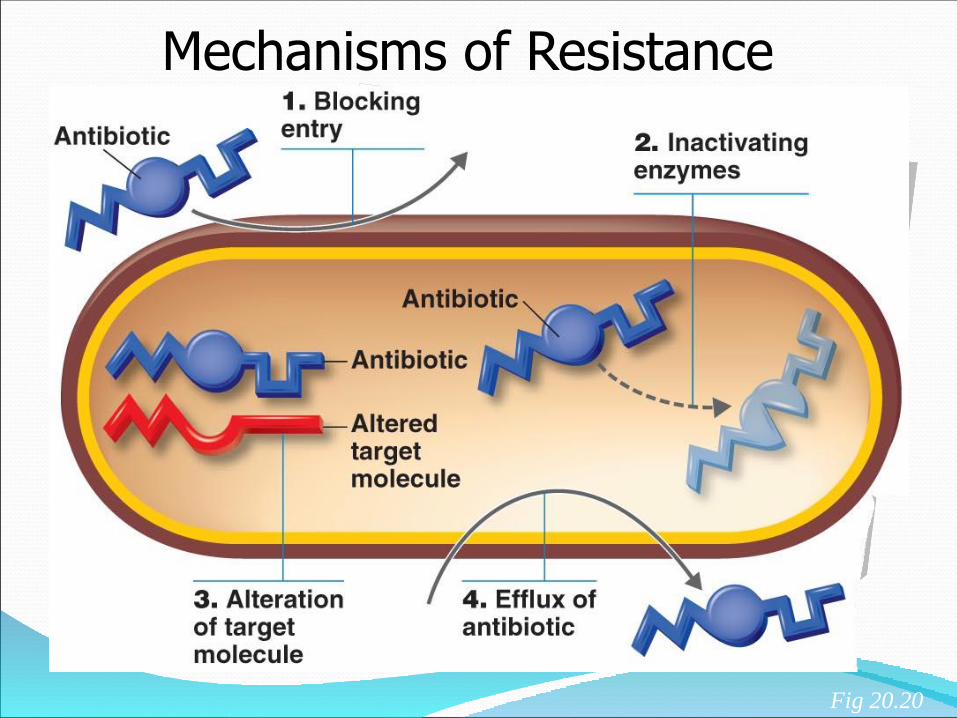
• Enzymatic destruction of
drug
• Prevention of penetration
of drug
• Alteration of antibiotic or
target site
• Rapid ejection of the drug
Mechanisms Of Antibiotic Resistance

Mechanisms of ResistanceAntibiotic Degrading Enzymes
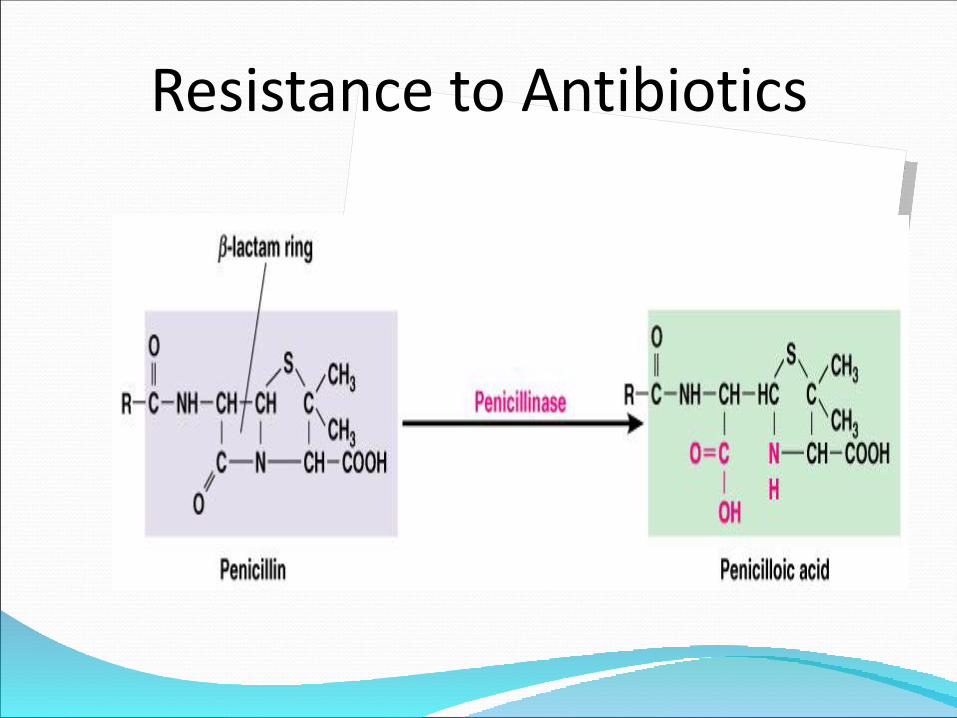
β-lactamases
Simple, extended spectrum β-lactamases (ESBL), cephalosporinases, carbapenemases
Confer resistance to some, many, or all beta-lactam antibiotics
Chloramphenicol acetyltransferase-inactivates the drug by 3-o-acetylation
Erythromycin esterase - seen in E.coli-hydrolyze lactone ring thus deactivating it - limits utility of oral erythromycin
Resistance to Antibiotics
Mechanisms of Resistance
Decreased uptake of the drug (Altered influx)
Mutation in a transporter (alterations in porin proteins) necessary to import antibiotic can lead to resistance (Carbapenems).
Increased elimination of the drug (Altered efflux)
Acquire transporter gene that will pump the antibiotic out (efflux pumps) - Tetracycline resistance
Mechanisms of Resistance
Alteration of target molecule (Mutation in the target site)
Minor structural changes in antibiotic target can prevent binding
- Changes in ribosomal RNA prevent macrolids from binding to ribosomal subunits - Alteration of ribosomal target sites-hence
failure to inhibit protein synthesis and cell growth.
- Penicillin binding proteins (penicillins) - MRSA
- RNA polymerase (rifampin)
- 30S ribosome (streptomycin)
Mechanisms of Resistance
Fig 20.20
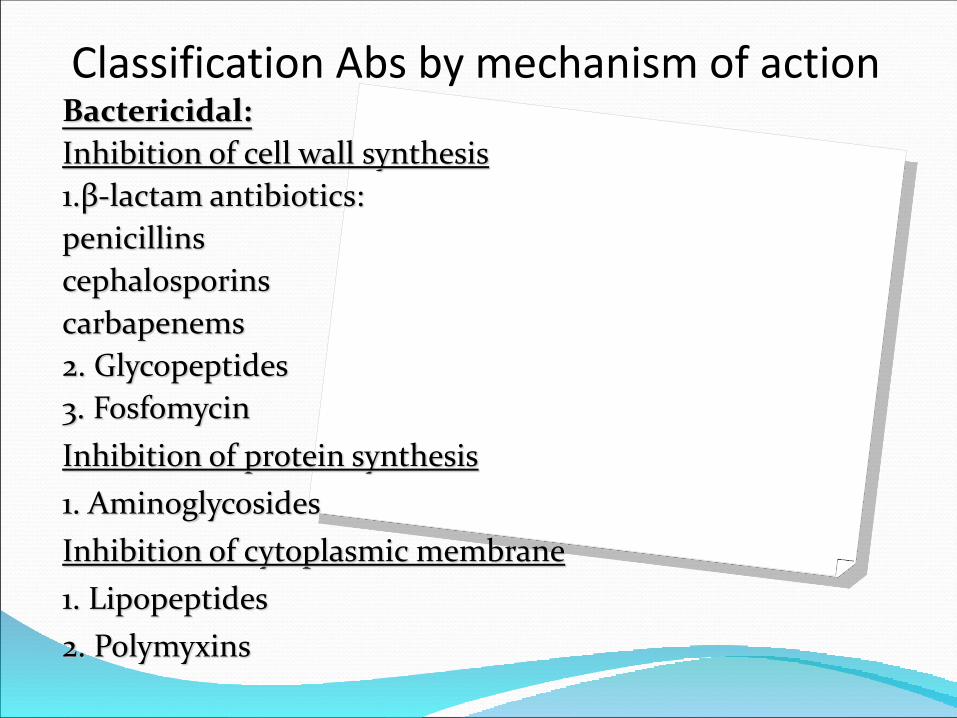
Classification Abs by mechanism of actionBactericidal:
Inhibition of cell wall synthesis
1.β-lactam antibiotics:
penicillins
cephalosporins
carbapenems
2. Glycopeptides
3. Fosfomycin
Inhibition of protein synthesis
1. Aminoglycosides
Inhibition of cytoplasmic membrane
1. Lipopeptides
2. Polymyxins

Classification by mechanism of actionBacteriostatic:
Inhibition of protein synthesis
1. Macrolides
2. Tetracyclines
3. Chloramphenicol
4. Lincosamides
5. Oxazolidinones
6. Glycylcyclines
Injury the synthesis of RNA in a bacterial cell
1. Ansamycins

Bactericidal antibiotics
Inhibition the synthesis of cell walls

-lactam antibiotics
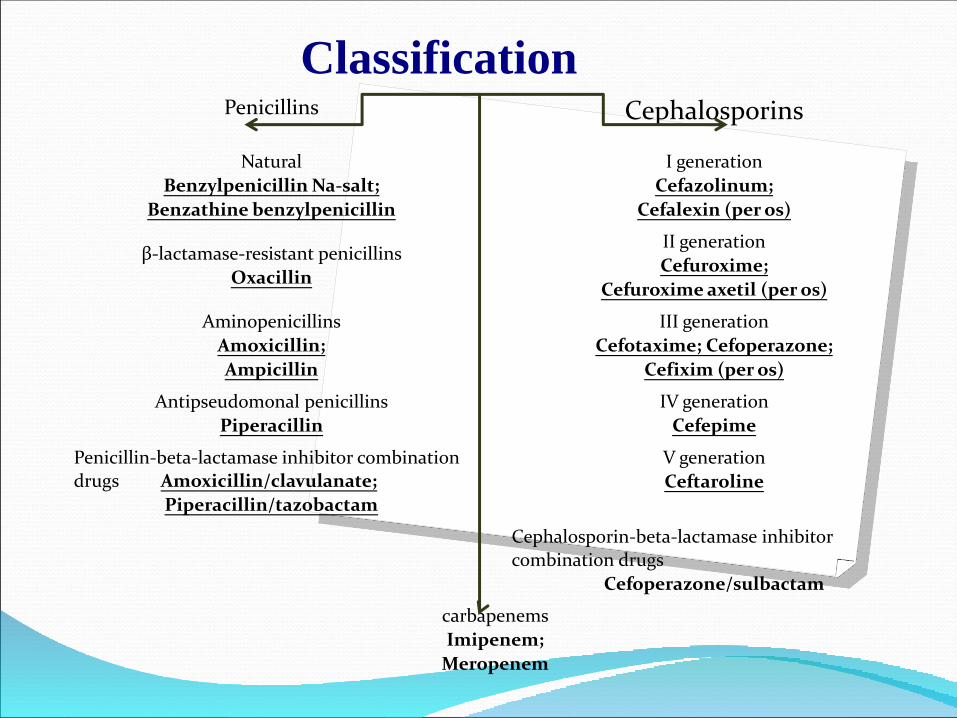
ClassificationPenicillins Cephalosporins
Natural
Benzylpenicillin Na-salt;
Benzathine benzylpenicillin
I generation
Cefazolinum;
Cefalexin (per os)
β-lactamase-resistant penicillins
Oxacillin
II generation
Cefuroxime;
Cefuroxime axetil (per os)
Aminopenicillins
Amoxicillin;
Ampicillin
III generation
Cefotaxime; Cefoperazone;
Cefixim (per os)
Antipseudomonal penicillins
Piperacillin
IV generation
Cefepime
Penicillin-beta-lactamase inhibitor combination drugs Amoxicillin/clavulanate;
Piperacillin/tazobactam
V generation
Ceftaroline
Cephalosporin-beta-lactamase inhibitor combination drugs
Cefoperazone/sulbactam
carbapenems
Imipenem;
Meropenem

The structure of the cell walls of bacteria
A-Gram" +»
B-Gram «-»

The composition of the cell wall includes a special peptidoglycan-murein. Peptidoglycan fibers are very long and are fastened together by a set of cross-sections. Monomers are molecules formed by aminosaccharides and Penta peptide L-Ala-D-Glu-L-Lys-D-Ala-d-Ala.

β-lactam AB penetrate peptidoglycan and bind with "penicillin binding proteins" → the formation of an inhibitory complex, which:
1. inhibits the transpeptidase reaction → as result the formation of cross-linking between molecules of peptidoglycans is disturbed,
2. activates autolytic enzymes in the cell wall → a partial destruction of peptidoglycans,
Inhibition and lysis of the cell wall.
Bactericidal action.
Low toxicity.
Excretion by the kidneys.
Wide range of dosages.
Cross allergy between penicillins, cephalosporins and carbapenems
1. PenicillinsGeneral property

Natural penicillinsPenicillin G (benzylpenicillin)
Pharmacokinetics: Acid resistance → parenteral route: i.v, i.m., epidural T1 / 2 3-4 hours → take 6-8 times a day;It is excreted unchanged by the kidneysSpectrum of activity narrow (mostly Gr "+»):Streptococcus and pneumococcus (skin and soft tissue infections, sore throat, outpatient pneumonia);Corinebacteria diphtheria (diphtheria)Spore-forming anaerobes: clostridia, anthrax Bacillus (tetanus, gas gangrene, anthrax);Meningococc (meningitis);
Pale Treponema (syphilis)
NO effect ON GONOCOCCI AND STAPHYLOCOCCI (produce β-lactamase)
Long duration of action (action 7-14 days).
Taken only i.m.
Indications: treatment of streptococcal infections (erysipelatous inflammation, prevention of attack of rheumatism) and syphilis.
Natural penicillinsBenzathine benzylpenicillin
(bicillin-1 )
Oxacillin,
The spectrum: as natural penicillins + staphylococci, producing β-lactamases (resistant to penicillin, aminopenicillins, anti-Pseudomonas penicillins).
Route of administration: i.m., i.v., per os
Indications: infections of the skin, soft tissues, bones and joints, pneumonia, endocarditis, meningitis, sepsis.
β-lactamase-resistant penicillins (antistaphylococcal)
Methicillin is a isoxazolylpenicillins. It is not used now.
In the case of MRSA-infection penicillins, cephalosporins and carbapenems not used.
Methicillin-resistant Staphylococcus (MRSA)
➢ Ampicillin➢ AmoxicillinDegraded by β-lactamases.Acid-resistant.A Broad spectrum of action: G + cocci: pneumococci,
enterococci, Neisseria, Treponema, Gr " - " intestinal group (Escherichia coli, Shigella,
Salmonella); hemophilic bacteria, Spore-forming bacteria: clostridia, anthrax Bacillus; H. pylori (amoxicillin), Listeria, Bordetella
Aminopenicillins
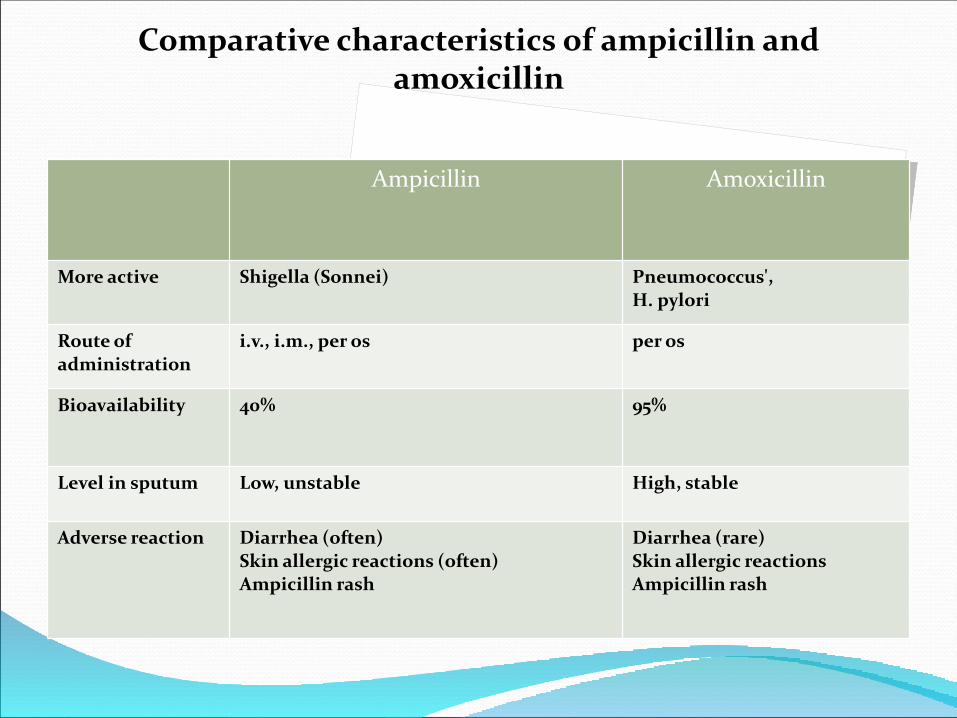
Ampicillin Amoxicillin
More active Shigella (Sonnei) Pneumococcus', H. pylori
Route of administration
i.v., i.m., per os per os
Bioavailability 40% 95%
Level in sputum Low, unstable High, stable
Adverse reaction Diarrhea (often)Skin allergic reactions (often)Ampicillin rash
Diarrhea (rare)Skin allergic reactionsAmpicillin rash
Comparative characteristics of ampicillin and amoxicillin
Compounds, inactivating β-lactamases:
clavulanic acid (clavulanate), sulbactam
and tazobactam.
Combination penicillins:
Amoxicillin/clavulanate;
Ampicillin / sulbactam;
Ticarcillin / clavulanate;
Piperacillin / tazobactam
Penicillin-beta-lactamase inhibitor combination drugs
Taken orally and i.v. every 8 hsIt is excreted by kidney and GIT.Spectrum of action: Gr ( + ) cocci: staph (including penicillin-resistant S. aureus and S. epidermidis), Streptococcus, Enterococcus;
Gr ( - ) bacillus: N. influenzae, M. catarrhalis, N.
gonorrhoeae, E. coli, Proteus spp., Klebsiella spp. etc., (including β-lactamase-producing );Anaerobic bacteria: spore - and asporogenous.Indications: sinusitis, otitis, bronchitis, pneumonia;acute cholecystitis, cholangitis, intraabdominal infections;acute pyelonephritis, cystitis, gynecological infections;infections of the skin, soft tissues, bones and joints, sepsis
Amoxicillin/clavulanate
This group consists of two subgroups: carboxypenicillins (ticarcillin)ureidopenicillins (piperacillin).
Piperacillin is mainly used .
Active against P. aeruginosa, as well as some ampicillin-resistant gram-negative bacteria (Enterobacter, Proteus, Morganella).
Used: Pseudomonas aeruginosa infection in combination with aminoglycosides II-III generation or ciprofloxacin.Route of administration: i.v. every 6-8 hs
Anti-Pseudomonas penicillins
Allergic reaction,
Diarrhea (ampicillin, amoxicillin),
Maculopapular rashes (not allergy, but usually if a patient has mononucleosis and takes ampicillin or amoxicillin),
Neurotoxicity (high doses of penicillin)
Side effects
Bactericidal action.
Broad spectrum.
Cross allergy with penicillin.
No effect on enterococci, Listeria, MRSA.
They are destroyed by β-lactamases.
Synergism with aminoglycosides.
2. CephalosporinsGeneral property

➢Cefazolinum
➢Cefalexin (per os)
Spectrum of action: narrow, mainly Streptococcus and Staphylococcus
Indications:
For Cefazolin: perioperative prevention;
For Cefalexin: Streptococcus. tonsillopharyngitis
For both: skin and soft tissue infections
I generation cephalosporins

➢Cefuroxime➢Cefuroxime axetil (per os)
Spectrum: broad, same I generation + H.influenzae, M. catarrhalis, E. coli, some strains of Klebsiella andProteus.
Indications: Acute otitis media (except Cefaclor), acute sinusitis,
bronchitis, pneumonia;Pyelonephritis;Infections of the skin, soft tissues, bones and joints.Perioperative antibiotic prophylaxis.
II generation cephalosporins
Spectrum: broad, same generation II + enterobacteria + meningo and gonococci + Pseudomonas aeruginosa (ceftazidime, cefoperazone)
BUT! Antistaphylococcal activity is less than that of first generation
Indications: severe infectionsUpper and lower respiratory tract, including nosocomial infections, biliary and urinary tract, bone, joint, skin and soft tissue, intra-abdominal and pelvic infections (in combination antianaerobic agent with drugs), shigellosis, salmonellosis, Bacterial meningitis.Sepsis.Gonorrhea
III generation cephalosporins
Parenteral Oral
Cefotaxime
Cefoperazone
Cefixime

Cefoperazone/sulbactam
Pharmacokinetics, adverse reactions are similar tocefoperazone, but more active against G «-» bacteria wichsynthesize β-lactamase - Enterobacteriaceae, Acinetobacter +effect on B. fragilis and other anaerobes nonspore
in abdomen and pelvis infections can be used asmonotherapy.
Cephalosporin-beta-lactamase inhibitor combination drugs

➢Cefepime
Spectrum: same III generation (including strains synthesizing β-lactamases class AMRs-nosocomial Enterobacter and Citrobacter strains) + Pseudomonas aeruginosa.
Indications:Severe nosocomial infections caused by multiresistant
bacteria (pneumonia, urinary tract infections, intraabdominal and pelvic infections, skin infections, soft tissue infections, bone and joint infections), sepsis, neutropenic fever.
IV generation cephalosporins
➢Ceftaroline is an active metabolite of ceftaroline fosamil.
Spectrum: same III-IV generation, including Str.pneumoniae resistant to penicillins, cephalosporins, macrolides and fluoroquinolones, + H. Influenzae, producing β-lactamases + MRSA.
Indications: complicated skin and soft tissue infections, community-acquired pneumonia caused by MRSA, Str. pneumoniae, H. influenzae, H. parainfluenzae, K. pneumoniae, and E. coli.
V generation cephalosporins
Allergy (cross with penicillins);
Irritation at the injection site: phlebitis and infiltration;
Diarrhea (in cephalosporins excreted in bile);
Leukopenia (rarely);
Nephrotoxicity (in the presence of kidney diseases)
Hypoprothrombinemia (cefoperazone);
Disulfiram-like effect (cefoperazone).
Side effects
➢ Imipenem/cilastatin (inhibitor of renal dehydropeptidase I)➢ Meropenem
Spectrum: broad, same cephalosporins III-IV, including resistant strains producing β-lactamases, + P. aeruginosa + nonsporous anaerobes.
Indications: severe infections caused by multiresistant or mixed flora: nosocomial pneumonia, complicated bone and soft tissue infections, intraabdominal and pelvic infections, pyelonephritis, sepsis, neutropenic fever, Pseudomonas infection + meningitis caused by Gr " - " bacteria (Meropenem)
3. CarbapenemsGeneral property

Allergic reactions (rarely cross Allergy with penicillins);
Dyspepsia;
Imipenem - convulsions (due to competitive antagonism with GABA)
Side effects
Glycopeptides

➢ VancomycinMechanism of action: block the synthesis of the cell wall of
bacteria by irreversible binding to the end portion of the amino acid bridge involved in the formation of cross-links between polysaccharide chains D-Ala-d-Ala.
Spectrum: narrow, Gr " + " aerobic and anaerobic: Staphylococcus (including MRSE, MRSA), Streptococcus, pneumococcus, Enterococcus, Peptostreptococcus, Listeria, corynebacteria, Clostridium (including C. difficult).
Glycopeptides are inactive against almost all Gr "-", since their large molecule is not able to penetrate the outer membrane of bacteria.
Indications: in case of allergy or resistance to β-lactam antibiotics (severe Staphylococcus (MRSA), streptococcal infections + pseudomembranous colitis (C. Difficile).Pharmacokinetics:Penetrate well into tissue (peritoneal cavity, pericardium, valves, endocardium, pleura, joints)Not absorbed in GITExcreted by the kidneys unchangedVancomycin: t1∕2 of 6-8 hs,
Syndrome "red neck" or "red man" (flushing of the upper body, spasm of the thoracic muscles, breathing difficulty);
Makulo-like or urticaria rash, allergic reactions;
Reversible nephrotoxicity;
Ototoxicity;
Transient neutropenia or thrombocytopenia
Side effects of Vancomycin

Fosfomycin
Well absorbed, well penetrates into various organsand tissues.
Mechanism of action: blocks cell wall synthesis m/oby inhibiting enolpyruvylshikimate (involved in thesynthesis of precursors peptidoglycan).
Spectrum: broad, but more often is used to treat Gr"-" -infections: E. coli, Salmonella, Klebsiella, Proteus,including bacteria resistant to other AB.
Indications: orally: acute and recurrent cystitis,urethritis, bacteriuria in pregnant women, preventionUGT-infection in transurethral studies andinterventions; i.v. or i.m. - in severe infections of variouslocalization
nausea, vomiting, diarrhea.
allergic reactions: rash, urticaria, itching
when parenteral application: transient increase in liver transaminases, anaphylactic shock, pancytopenia, headache, dizziness, phlebitis/infiltration at the injection site.
Side effects of fosfomycin
Bactericidal antibiotics
II. Inhibition of cytoplasmic membrane
➢ DaptomycinRA: i.v. 1 time a day, not metabolized, excreted by the kidneysMechanism: cyclic lipopeptide → there are hydrophilic core
and hydrophobic tail → irreversibly binds to the cellmembrane Gr " + " bacteria → channel is formed → outputK+ → rapid depolarization → inhibition of synthesis ofprotein, DNA and RNA → cell death
Spectrum: narrow, Cr " + " including Clostridium, strepto -and poly-resistant: staphylo - and enterococci (MRSA andvancomycinresistant, E. faecium).
Indications: complicated skin and soft tissue infections,bacteremia and infectious endocarditis caused by MRSA
Side effects: allergic reactions, transient increase in AST andALT, reversible myopathy (rarely)
Lipopeptides
Bacillus polymyxa produces 3 polypeptides: polymyxins M, B,E.Toxicity, are used locally.Not absorbed. Do not pass the BBB. Metabolized in the liver,excreted by kidneys.Spectrum: narrow, Gr" -": P. aeruginosa, Acinetobacter andenterobacteriaMechanism: polymyxins (are cationic compounds) areembedded in the CPM and "dissolve" it (cationic detergent)→ lysis of bacteria.Indications: p. aeruginosa and enterobacteriainfections(reserve);Side effect: NephrotoxicityNeurotoxicity and neuromuscular blockade
Polymyxins

➢Colistimethate - derived methansulfonate acid colistin(polymyxin E).
RA: Powder for solution for inhalationIndications: P. Aeruginosa respiratory infections,
mucoviscidosis.Side effect:Allergic reactions (angioedema);Paresthesia, dizziness;Bronchospasm, ↑ sputum, pharyngitis, dyspnea;Acute renal failure
Sodium colistimethate

Bacteriostatic antibiotics

Bind to the 50S:macrolideslincosamideschloramphenicoloxazolidinones
Bind to the 30S:aminoglycosidestetracyclinesglycylcyclines
Antibacterial agents that inhibit protein synthesis
I. Macrolides
Antimicrobials that Bind to the 50S Ribosomal Subunit
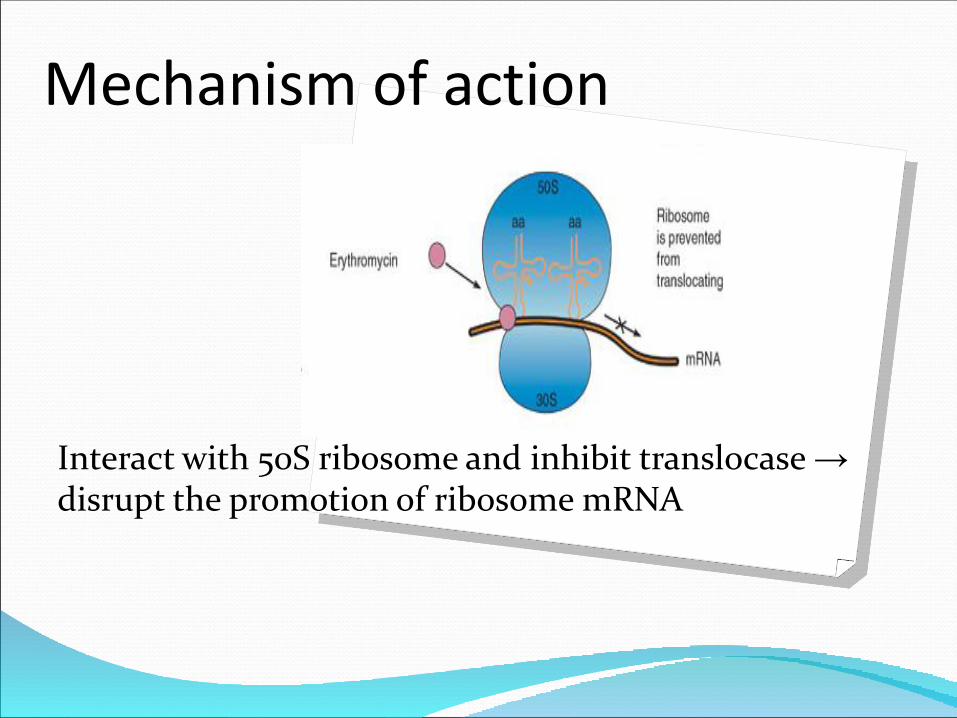
Mechanism of action
Interact with 50S ribosome and inhibit translocase →disrupt the promotion of ribosome mRNA
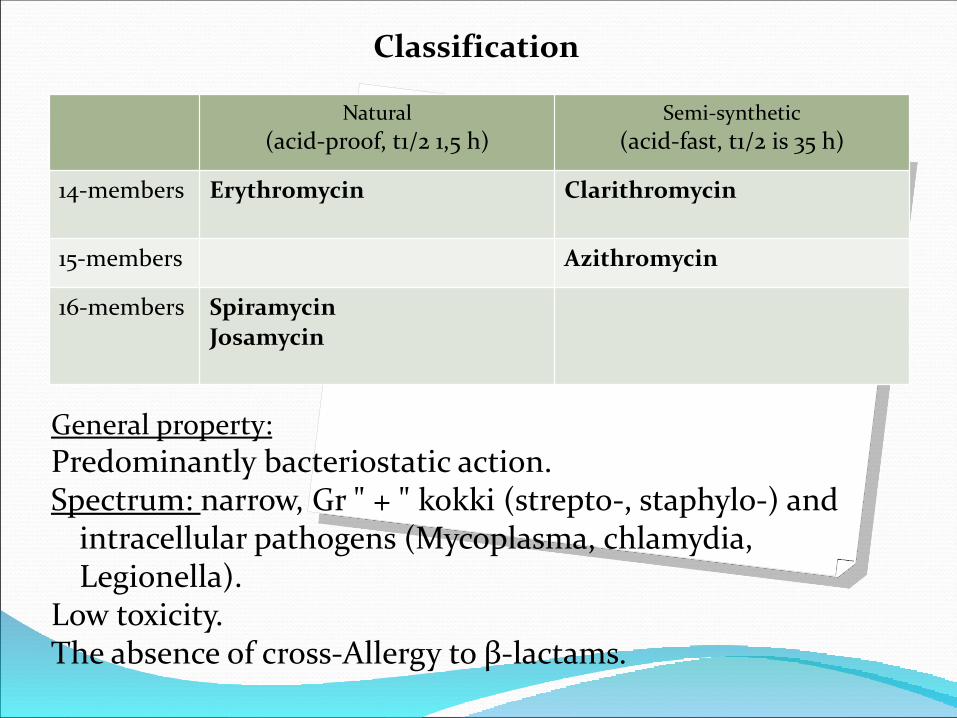
General property:
Predominantly bacteriostatic action.Spectrum: narrow, Gr " + " kokki (strepto-, staphylo-) and
intracellular pathogens (Mycoplasma, chlamydia, Legionella).
Low toxicity.The absence of cross-Allergy to β-lactams.
Classification
Natural
(acid-proof, t1/2 1,5 h)Semi-synthetic
(acid-fast, t1/2 is 35 h)
14-members Erythromycin Clarithromycin
15-members Azithromycin
16-members Spiramycin
Josamycin

Spectrum: narrow (mostly Gr "+") or broad, depends on the dose
and drug.
Gr " + " cocci: staphylo -, including penicillin resist. S. aureus, Streptococcus and pneumococcus;
Gr "+" bacillus: corynebacteria diphtheria, Listeria;
Gr "-" cocci: Moraxella of catarhalis;
G-bacillus: Bordetella, pertussis, Haemophilus influenzae, Bacillus, Campylobacter, Helicobacter;
Pathogens of intracellular infections: chlamydia, Mycoplasma, spirochetes, Legionella
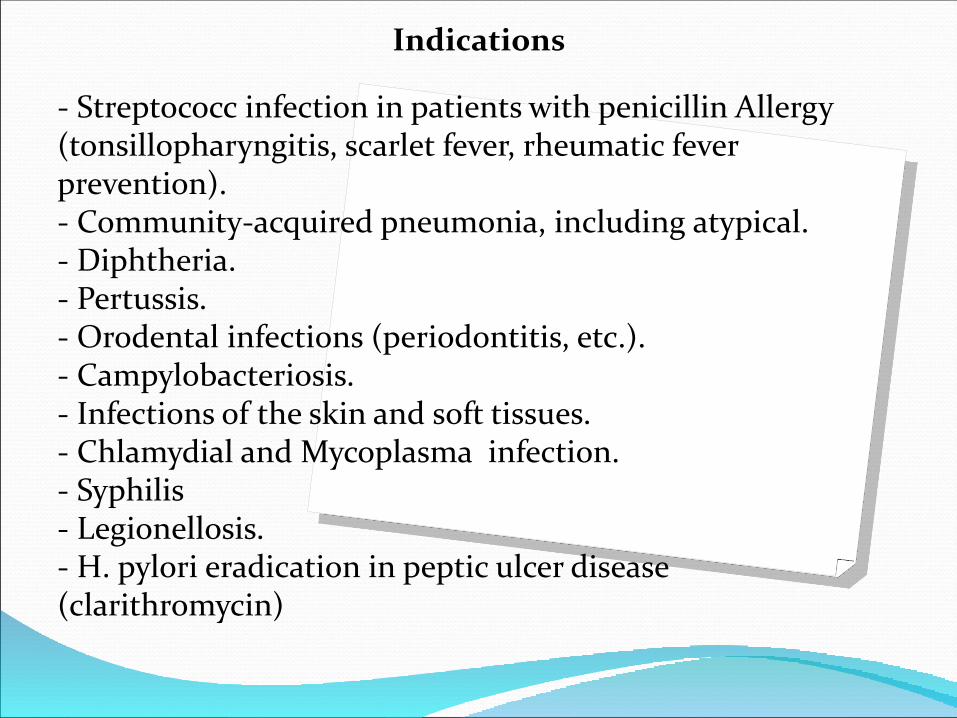
- Streptococc infection in patients with penicillin Allergy (tonsillopharyngitis, scarlet fever, rheumatic fever prevention).- Community-acquired pneumonia, including atypical.- Diphtheria.- Pertussis.- Orodental infections (periodontitis, etc.).- Campylobacteriosis.- Infections of the skin and soft tissues.- Chlamydial and Mycoplasma infection.- Syphilis- Legionellosis.- H. pylori eradication in peptic ulcer disease (clarithromycin)
Indications

↑ intestinal motility due to stimulation of motiline
receptors - motiono-like syndrome (erythromycin,
spiramycin, josamycin);
Pyloric stenosis in newborns (erythromycin,
clarithromycin, azithromycin)
↑ levels of hepatic transaminases, cholestatic hepatitis,
jaundice (erythromycin, clarithromycin);
↑ QT interval on ECG, reversible ototoxicity (i.v. high
doses);
Allergic reaction.
Side effects
II. Lincosamides

Lincomycin
Clindamycin
Mechanism: binds to 50S bacterial ribosome and inhibits the peptide portion of peptidyltransferase →inhibition of protein synthesis in bacterial cell.
Bacteriostatic Narrow spectrum of activity: gram-positive cocci and
non-sporadic anaerobes + some protozoa (Toxoplasma gondii, Pneumocystis).
High concentrations in bones and joints. Poor penetration through the BBB. The absence of cross-Allergy to β-lactams. Relatively frequent development of antibiotic-
associated (C. difficult-associated) diarrhea.
General property of lincosamides
Indications:⚫ Streptococcal tonsillopharyngitis.⚫ Aspiration pneumonia, lung abscess, empyema.⚫ Infections of the skin and soft tissues, bones and joints.⚫ Intra-abdominal infections: peritonitis, abscess.⚫ Infection of the pelvic organs are: endometritis, adnexitis,
oophoritis, postoperative anaerobic vaginal infections.⚫ Chloroquinine-resistant tropical malaria (clindamycin).⚫ Toxoplasmosis (clindamycin).⚫ Bacterial vaginosis (local).
Acne (locally).
Indications
Antibiotic-associated diarrhea, pseudomembranous colitis (C. difficult-associated).
Increased activity of liver enzymes.
Neuromuscular blockade (in high doses).
Allergic reaction.
Side effects
III. Chloramphenicol
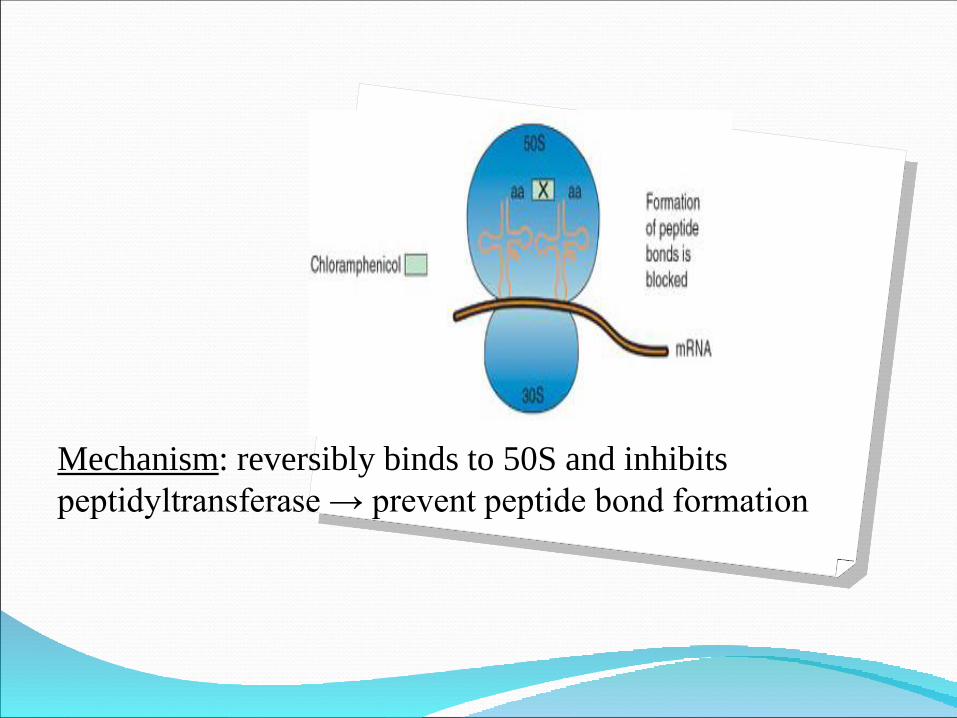
Mechanism: reversibly binds to 50S and inhibits
peptidyltransferase → prevent peptide bond formation
Spectrum: broad : Salmonella, anaerobes (bacteroids), meningococcus and Rickettsia.
Indications:Bacterial meningitis, brain abscessGeneralized forms of salmonellosis, typhoid feverRickettsiosis (ku-fever, typhoid fever, etc.) Brucellosis!Gas gangreneBacterial infections of eyes (locally)

Reversible anemia, leukopenia, thrombocytopenia (dose-dependent);
Aplastic anemia (idiosyncrasy of chloramphenicol 1:10 000 – 40 000, does not depend on dose and number of doses, mortality 50-100%)
Neurotoxicity (psychosis, perif. neuropathies);
Dermatitis;
"Grey collapse" of the newborn ("Grey baby syndrome"): vomiting, abdominal distension, respiratory distress, cardiotoxicity, cyanosis collapse, hypothermia, acidosis. The reason: insufficient conjugation in the liver + functional imperfection of the renal tubules (the first 2-4 weeks of life).
Side effects

IV. Oxazolidinones
Linezolid

Mechanism: interacts with the 50S and prevents formation of the initiation complex (mRNA, tRNA, and 50S).
Spectrum: narrow, C "+": cocci resistant to other antibiotics including MRSA, penicillinresistant pneumococci, enterococci vancomycinresistant; anaerobic bacteria: Clostridium (except C. difficile), nekot. strains of B. fragilis, Peptostreptococcus.
Indications: Nosocomial infection of any localization caused by
MRSA, community-acquired pneumonia, complicated infection: intraabdominal , skin and soft tissues.
Reversible anemia and thrombocytopenia;
Increased activity of transaminases and AF, increased levels of bilirubin in the blood;
Dyspepsia;
Headache
Side effects

Antimicrobials that Bind to the 30S Ribosomal Subunit
I. Tetracyclines

Tetracycline
Doxycycline
Mechanism: bind to 30S and inhibit binding of aminoacyl-tRNA to the aminoacyl center (inhibit initiation)
Spectrum: broad: Gr " + " bacillus: Listeria, anthrax wand, P. acne;Gr " + " bacillus: H. pylori (tetracycline), H. influenzae, cholera Vibrio, causative agents of plague, tularemia and brucellosis;Intracellular pathogens: chlamydia, Mycoplasma, Legionella, Rickettsia;Spirochete: Treponema pallidum
Indications: ⚫ genital chlamydia and Mycoplasma infections, ⚫ syphilis and gonorrhoea - in case of β-lactam
intolerance)⚫ Atypical pneumonia⚫ Peptic ulcer disease (H. pylori eradication, only
tetracycline)⚫ Acne⚫ plague, cholera, anthrax ⚫ Rickettsiosises⚫ Zoonoses (leptospirosis, brucellosis, tularemia)

HepatotoxicityPhotosensitization (rash, dermatitis, nail damage due to sunlight)Antianabolic action (↓ synthesis ↑ protein catabolic)In children: violation of bone development (deceleration of their longitudinal growth) and teeth (change in color of teeth, enamel defects)*
** form chelate compounds with calcium orthophosphate
Side effects
children up to 8 years
pregnancy and breast-feeding
severe pathology of the liver
renal failure (except doxycycline)
Contraindications
II. Aminoglycosides

I generation II generation III generation
Streptomycin Gentamycin Amikacin
Kanamycin Tobramycin
Classification
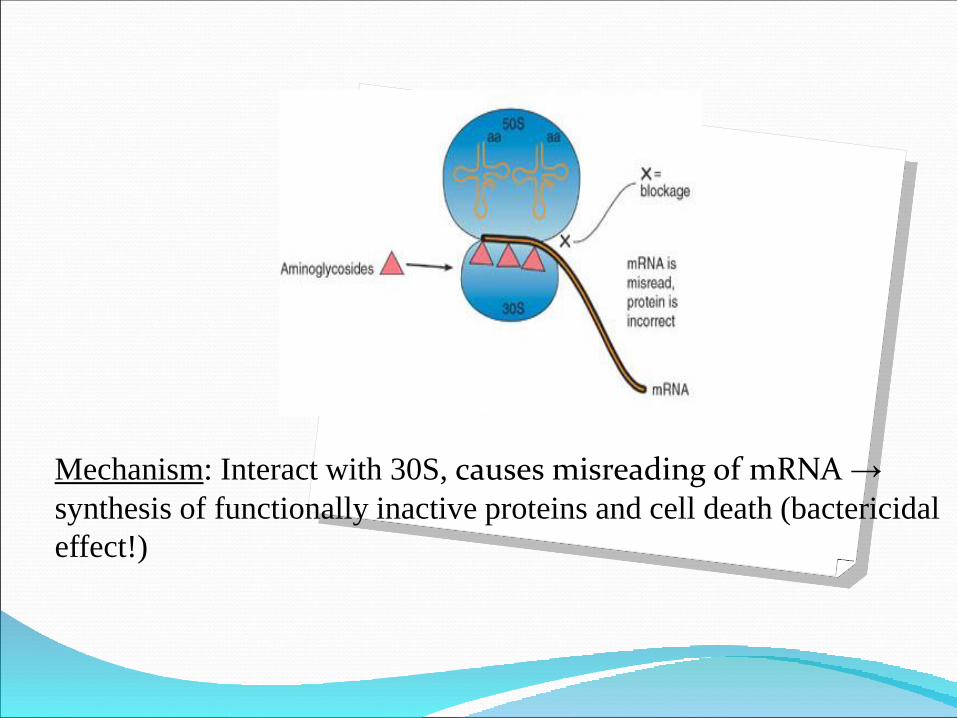
Mechanism: Interact with 30S, causes misreading of mRNA →
synthesis of functionally inactive proteins and cell death (bactericidal
effect!)
Spectrum: broad, the main clinical importance: aerobic Gr " - ": enterobacteria and Pseudomonas aeruginosa (gentamicin, amikacin), as well as infectious endocarditis ++ M. tuberculosis (streptomycin, kanamycin and amikacin)++ Gr + cocci: Staphylococcus aureus, Streptococcus (in combination with aminopenicillins or cephalosporins)++ causative agents of plague, tularemia, brucellosisPneumococci resistant! Not active against anaerobes and intracellular microorganisms!

Enterobacteriaceae infections of different localization - II-III generations.
Pseudomonas aeruginosa infection- II-III generations. Enterococcal infections-gentamicin or streptomycin in
combination with penicillin or ampicillin. Tuberculosis - streptomycin, kanamycin, amikacin -
always in combination with other anti-TB drugs. Zoonotic infections: plague, brucellosis
(streptomycin); tularemia (streptomycin, gentamicin).
Indications
⚫ Ototoxicity (vestibular disorders, Meniere's syndrome, hearing loss up to complete deafness)
⚫ Nephrotoxicity (proteinuria, creatinine and blood urea)
⚫ Neuromuscular blockade (paresthesia, muscle weakness, respiratory arrest with rapid i.v. of high doses)
Side effects
III. Glycylcyclines
Tigecycline
Bacteriostatic, but for some m/o acts bactericidal.
Mechanism: binds to the special spiral region of the a-section 30S and blocks the penetration of aminoacyl-tRNA to the a-site of the ribosome and the addition of amino acids to the peptide chain.

Spectrum: broad: all anaerobes, G + cocci (includingMRSA, enterococci vancomycinresistant,penicillinresistant Str. pneumoniae), Gr " - "(Haemophillus spp., Moraxella catarrhalis, Neisseriahonorrhoeae, Citrobacter, multi-resistant strains ofAcinetobacter, Enterobacter spp., E. coli and Klebsiellaproducing β-lactamases of the extended spectrum andcarbapenemases), "atypical" bacteria (Leginella,Mycoplasma, Chlamydophila pneumoniae).
Not active against P. aeruginosa!
Indications:complicated skin and soft tissue infections, intraabdominal infections;community-acquired pneumonia.
Side effect:Nausea and vomiting, abdominal painHyperbilirubinemia , high level of AST, ALT, APh, urea in the blood, pancreatitisHypoproteinemiaPossible photosensitization and tooth damageAllergic cross-reaction with tetracyclines
Do not use in pregnancy, lactation and children below the age of 18 years
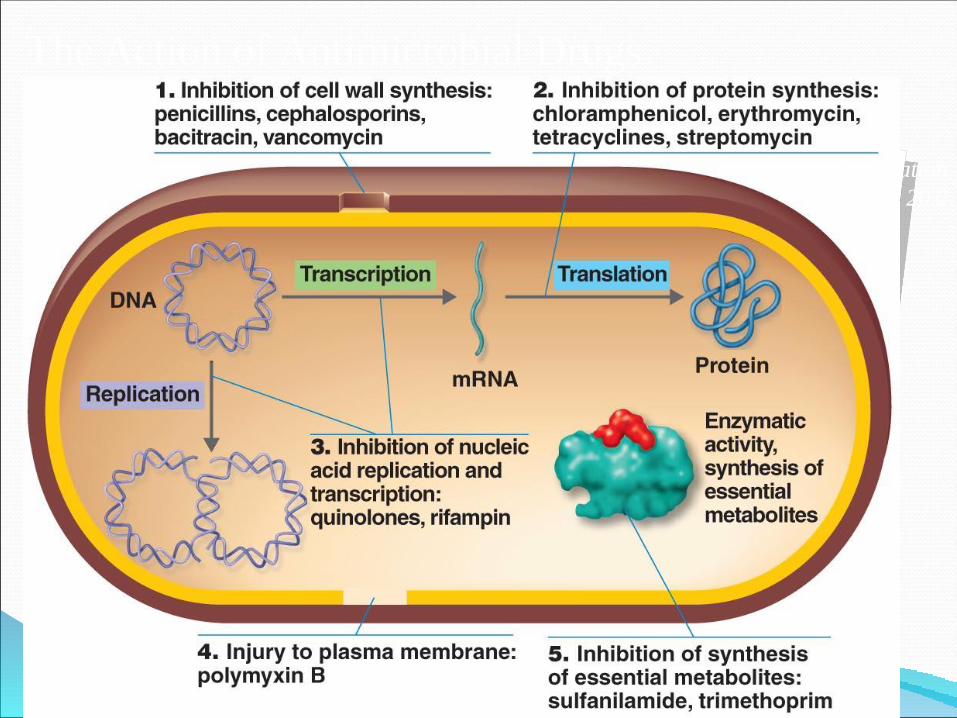
The Action of Antimicrobial Drugs
Foundation
Fig 20.2
Related Documents











