1

Anatomy, Lecture 8, Heart Innervation & Posterior Mediastinum (Lecture Notes)
Nov 22, 2014
Anatomy, Lecture 8, Heart Innervation & Posterior Mediastinum (Lecture Notes)
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
2
Innervations of Heart (2) and Posterior Mediastinum
I will try to put everything what I’m gonna say - in the slides. so..instead of seeing 25 slides in the lecture, there will be more. Because everything what I’m going to say, it will be here for you. Nothing to be worried about.
In this lecture, we are going to talk about the innervations of the heart; which is a very simple topic today then we’ll move to the inferior and superior mediastinum. As I mentioned several times for you, the heart is involuntary muscles. It’s not subjected to our conscious control, so the muscle itself is able to generate pulses and induces its own contraction. because it has its own contracting system.
Is this conducting system a nervous tissue? No.
each cardiac cell we called it cardiomyocyte.so within these cells we have modified populations.. that are able to generate electrical pulses which will induce contraction.
Now .. the central nervous system, through the autonomic nervous system we just modify the contraction.it cant induce it, it cant generate it completely, it can only modify the increase or decrease. I guess you heard this word before – the sinoatrial node. Sinoatrial node as we said, population of specialized cardiac cells are located within the right atrium – they are the pacemaker. The pacemaker is the one who give the signal to start the pace.so to start the cardiac contraction, the part which gives this signal is the sinoatrial node. And this signal once it is given, it will spread to both right and left atrium. Why? Because the right and left atria are electrically connected. The signal will start from one cardiac cell to the next, until it is distributed in the atria.
Can it goes the same way to the ventricle?
No. because the ventricles and the atria are electrically isolated by fibrous skeleton, which are the valves and the attachments.
So we have a special pathway for the signal to travel, from the atria into the ventricles. And this pathway —is the AV-node. Again, specialized cardiomyocytes will receive the signal from the SA node, and then it will send them through another bundle called Bundle of His, it will go to the septum –the interventricular septum.
In the septum, this Bundle of His will give left and right branches. These branches will deliver the signals to a plexus within the ventricles we called it Purkinje fibres. Again, these are modified cardiac cells. Purkinje fibres will distribute the signal into the walls of the ventricles. Having this special pathway – will allow the atria to receive the signal first, contract, and pump blood to the ventricle and then the ventricles will contract and pump the blood out. This is just a slide that summarize what I talked just now [refer slides number 3- 6] . of course it has the locations of AV node, SA node- you need to know that. But don’t worry I have put them there for you, you can read them [the slides] right?
3
So, if the heart has its own conducting system, how does the autonomic nervous system affect the heart?
of course there’s no somatic innervations..because it’s involuntary. We just have autonomic - sympathetic and parasympathetic. As I said, it will increase or decrease. Mainly sympathetic and parasympathetic goes to the SA node and AV node. But also the sympathetic is richly distributed in the ventricle, we have little parts of it in the muscles but mostly in the ventricle.. what we have is sympathetic. This is why the contractility or the force of contraction is affected more by sympathetic and parasympathetic. ok?
Now this is just the summary of the effects of sympathetic and parasympathetic [refer slide number 7]. Sympathetic functions when we are in danger or when we’re in emergency,or you are escaping from dangerous things, your heart will beat faster,stronger and of course your heart will functions more - it needs blood supply..so the coronary arteries that supplies the heart will be dilated.
Are we cool? am I talking fast? Not easy..ya3ni gharib.
Ok. Parasympathetic, on the other hand, it will functions during energy storage or relaxing situations. You are relaxing after lunch, your heart does not need to pump faster so the heart rate will decrease. The force of contraction will be reduced. and of course we don’t need the heart to function that much..as there’s no need for blood supply, for pumping of blood. So there will be constriction of the coronary arteries.
Now. The blood does not cheat. It will not feed from the blood within its chamber.it will wait until the blood is ejected to the arterial system. After that it will spread its own blood to other part of the body. And the blood supply is from two coronary arteries; right and left.
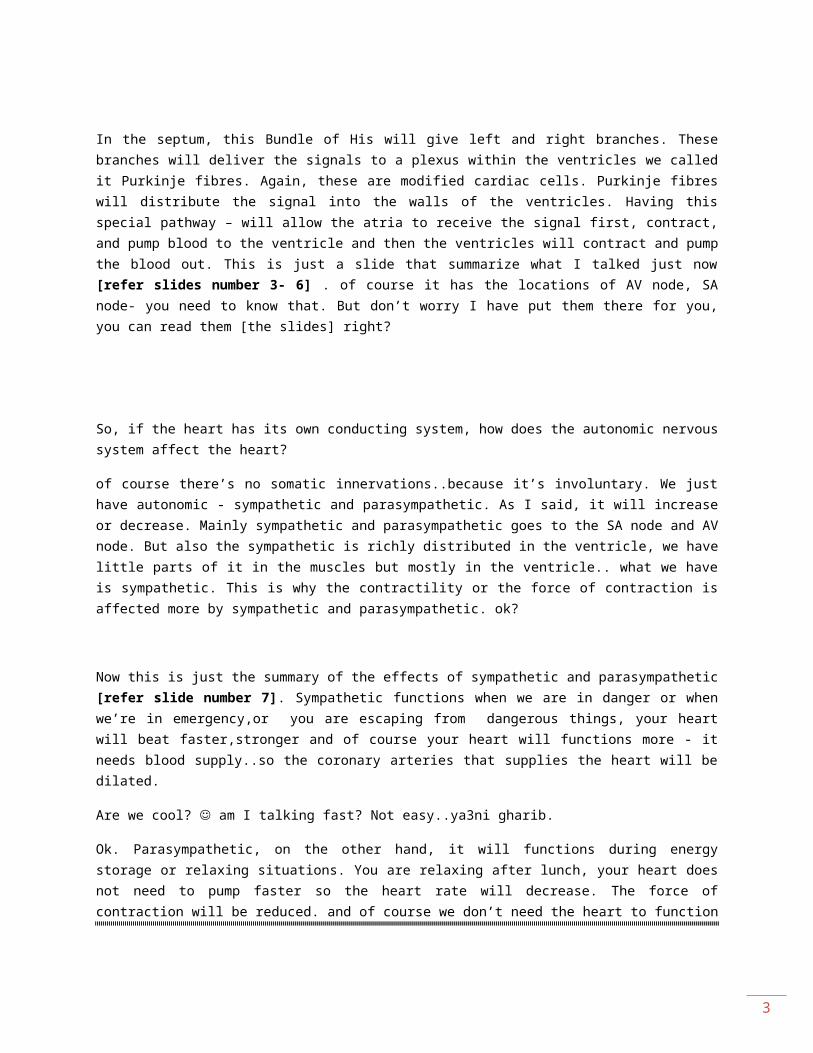
slide number 9+10 : coronary artery
Let’s start with the right coronary artery. As you can see [refer slide number 9] , it starts with a groove between right atrium and right ventricle. It will continue surrounds the heart, and it will goes posteriorly as the posterior interventricular artery. On the side of the heart, it will give a branch – called the right marginal artery. These are the major branches that you will be able to identify them or you are already identified them in the lab. Besides that we have other branches, the small ones - SA node and AV node, you see the blood supply comes from the right coronary artery.
4
This number here [ 85-90 %] in individuals, posterior interventricular is a branch of the right coronary artery. What happen to the other 10-15%? They are part of the left.this is what we called the right dominance or left dominance. So, most of us regarding our coronary circulations, we have right dominance. Those who have left dominance, their posterior interventricular comes from a branch of the left. Ok?
Also we have left coronary artery [refer slide number 10] , it’s larger but shorter [if compared to the right coronary artery]. Why is it larger? Maybe because the left ventricle ejects the blood, you know, to the rest of the body..not like the right ventricle which ejects to the lungs only. So more force needed [in left ventricle] , more blood supplies needed. That will be the reason. Also, it has major branches; like anterior interventricular artery, and the circumflex artery which continue posteriorly. sometimes it’s anastomoses with the right coronary. and on the margin here, we have a branch which is the left marginal artery.
Does it supplies the SA node?
Yes. In 20% of individuals, the SA node is supplied by the left coronary. And we called that branch – the artery of SA node.
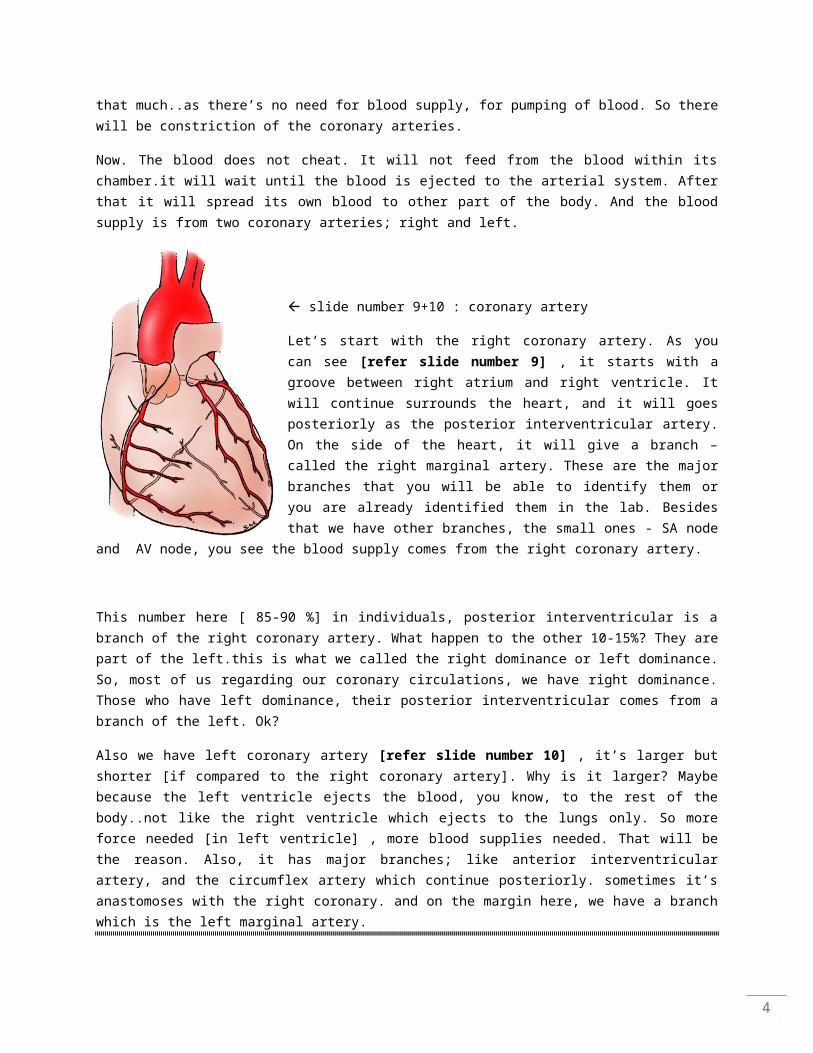
slide number 11 : anterior interventricular artery-
Now let’s talk about anterior interventricular artery [refer slide number 11]. Which is a branch of what? The right or the left?
The left. It wil be in the interventricular groove. And it will be left anterior descending [LAD]. It will pass and rotates around the apex of the heart. Before doing so, sometimes it takes off a branch we called it the diagonal artery.
5
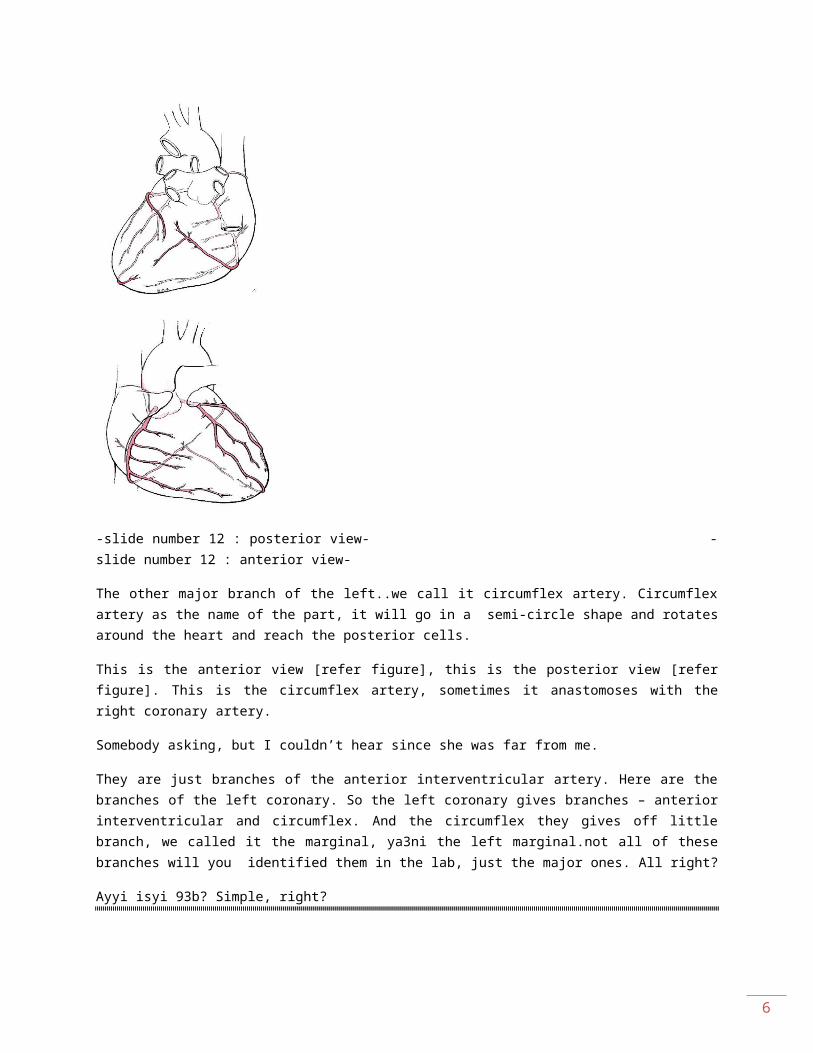
-slide number 12 : posterior view- -slide number 12 : anterior view-
The other major branch of the left..we call it circumflex artery. Circumflex artery as the name of the part, it will go in a semi-circle shape and rotates around the heart and reach the posterior cells.
This is the anterior view [refer figure], this is the posterior view [refer figure]. This is the circumflex artery, sometimes it anastomoses with the right coronary artery.
Somebody asking, but I couldn’t hear since she was far from me.
They are just branches of the anterior interventricular artery. Here are the branches of the left coronary. So the left coronary gives branches – anterior interventricular and circumflex. And the circumflex they gives off little branch, we called it the marginal, ya3ni the left marginal.not all of these branches will you identified them in the lab, just the major ones. All right?
Ayyi isyi 93b? Simple, right?
Ok. we just talked about the arterial supply,now we talk about the venous drainage [refer slide number 13] . this is the part after delivering oxygen and nutrients, the blood will be collected and returned to the left atrium. mainly, the veins of the heart together will coalesce, merge together to form something we called as the coronary sinus. It’s located at the junction between posterior surface and anterior surface of the heart. We have three names - the great cardiac vein, which is usually will be closed to the anterior interventricular. we have the middle cardiac vein which is usually will be closed to the posterior interventricular. And we have small one, we call it..the small cardiac vein.
We have anymore veins?
Yes. We call it the anterior cardiac veins – they don’t coalesce with the coronary sinus but they empty immediately into the right atrium.
Ok?
Now. We have medical conditions that is related or affected by the circulation of the heart. The first condition we call it the angina pectoris [refer slide number 14] . sometimes, we have diet nutrition fats, low exercise, atherosclerosis will happen. narrowing of the vessels, in general. The most serious one is the vessels of the heart, coronary arteries. If there is a narrowing in their lumen, because of atherosclerosis –there will be shortage of blood supply to the heart. What will happen? If I climb stairs, I run and I do any exercises, I will start to feel chest pain, and shortness of breath – we called it dyspnea.
Usually this pain is revealed if you relaxed, you sit down .. but the problem is there. If this condition is left untreated, this narrow in the coronary artery’s lumen will increase, and you’ll end up with total blockage of coronary artery. And it will happen. The blood of the cardiac muscle that supply by that artery, will die.
Death of cardiac muscle – we call it infarction. And it takes us to myocardiac infarction [refer slide number 15] , or sometimes we call it heart attack, based on failure or complete blockage of coronary artery leading to this unperformed cardiac muscle. It can be
6
fatal if not treated. And the treatment to this disease we call it coronary bypass surgery. Basically we need to open that closed artery.
Somebody was asking, what is dyspnea?
Doctor answered; shortness of breathing.
[refer slide number 16] We have chambers of the heart, we have vessels that emanating from those chambers, and there are valves regarding the artery and the openings of the chambers. We have four valves- two semilunar and two atrioventricular. The atrioventricular is between the atrium and the ventricle. We have right and left. The right - we called tricuspid - because it has 3 cusps, ya3ni each gate we call it cusp.. bawwabah ta3atil valves..nusammiha cusp. And the left - we called it the bicuspid or the mitral valve.
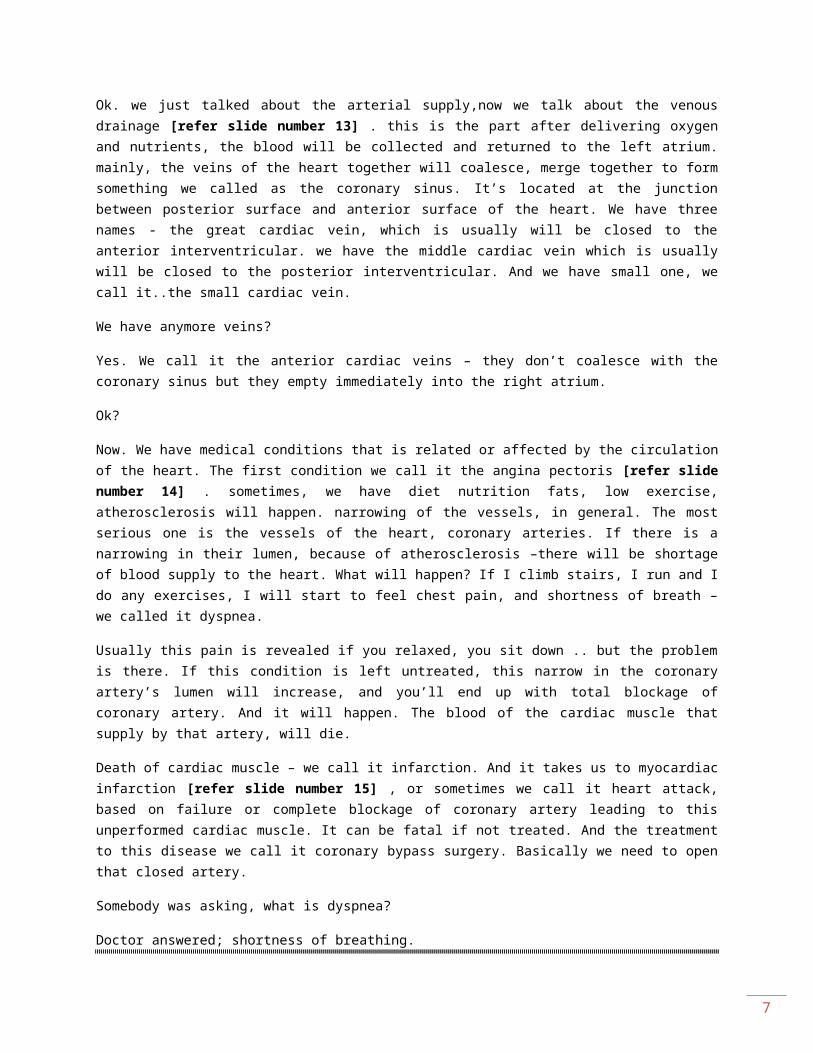
[refer slide number 17] We have two semilunar, one is where the aorta emanating from the left ventricle. It’s guarded by the aortic valve. And the pulmonary trunk, which is emanating from right ventricle, is also guarded by a valve. So semilunar valve - semilunar is actually a shape - we have 3 cusps, 2 anterior and 1 posterior. this is the pulmonary. And each cusp is made by folding of endocardium. We said that endocardium is a layer of epithelium; a layer which is supportive connective tissue. We have three layer – two layers of epithelium, with a layer connective tissues in between. This is how the cusp is made.
slide number 17 : valves
And if you can see [refer figure] , between the wall of the artery and the cusp, there will be a space. We call this space – sinus. So behind each cusp there’s a space we call it sinus.
The same thing applied to the aortic valve, with the exception – we have 2 posterior and 1 anterior cusps.
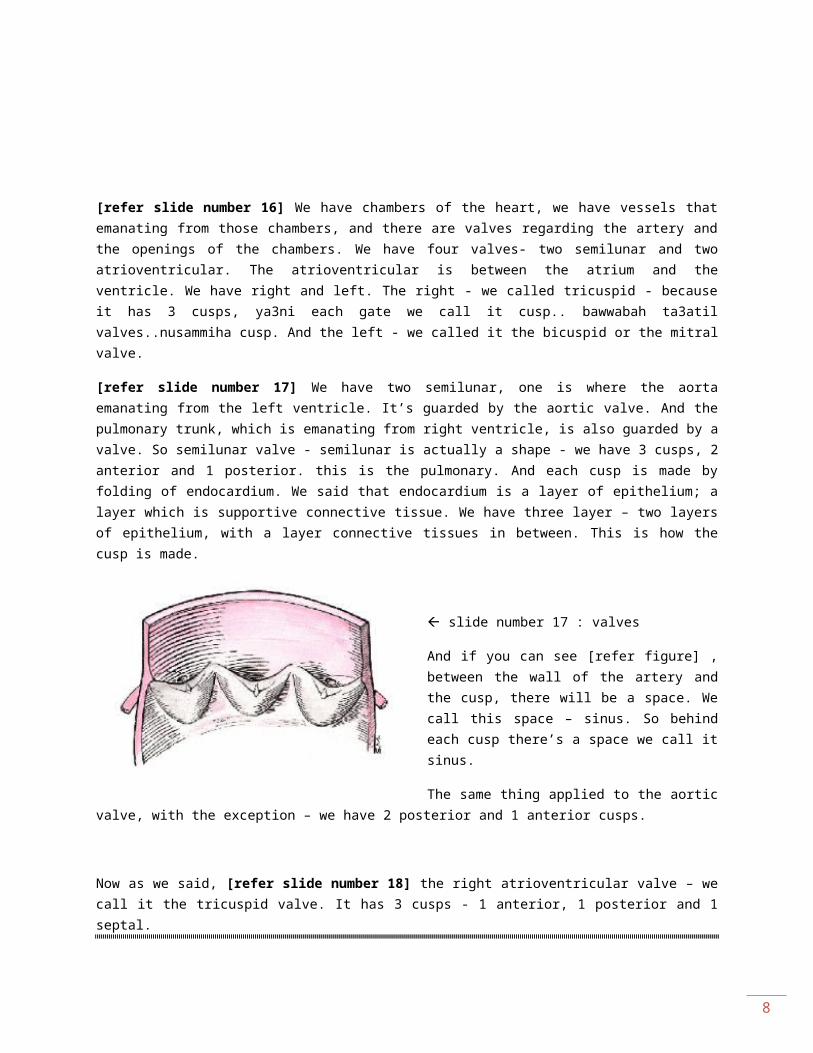
Now as we said, [refer slide number 18] the right atrioventricular valve – we call it the tricuspid valve. It has 3 cusps - 1 anterior, 1 posterior and 1 septal.
What does septal means?
It [the cusp] is located next to the ventricular septum. And this is something special about the atrioventricular valve, it has the main difference between semilunar and aortic & pulmonary valves. the cusps are attached to the muscles of the ventricle by fibrous branch,
7
we call them – tendon. And the reason we have this attachment .. so that when these cusps close, we don’t want them to open to the other direction..so it’s a one way gate. Alright?
slide number 18 : tricuspid valve
And here, is said that fibers from one papillary muscle they will attach to different cusps. So that the attachment will interdigitate, and those cusps are bonded as one unit.
[refer slide number 19] Mitral valve, as we said – it’s also called as the bicuspid, also is attached to the papillary muscles through chordae tendinae. Now the location of this valve, is so relevant to medical field, because you can tell a lot about the heart by listening to the sounds. The sounds we are listening to, are the sounds of the closure of the valves. So, when we use the stethoscope, [there is a] put it on the heart to listen, we will actually listen to the valves. And the sounds of blood rushing through them.
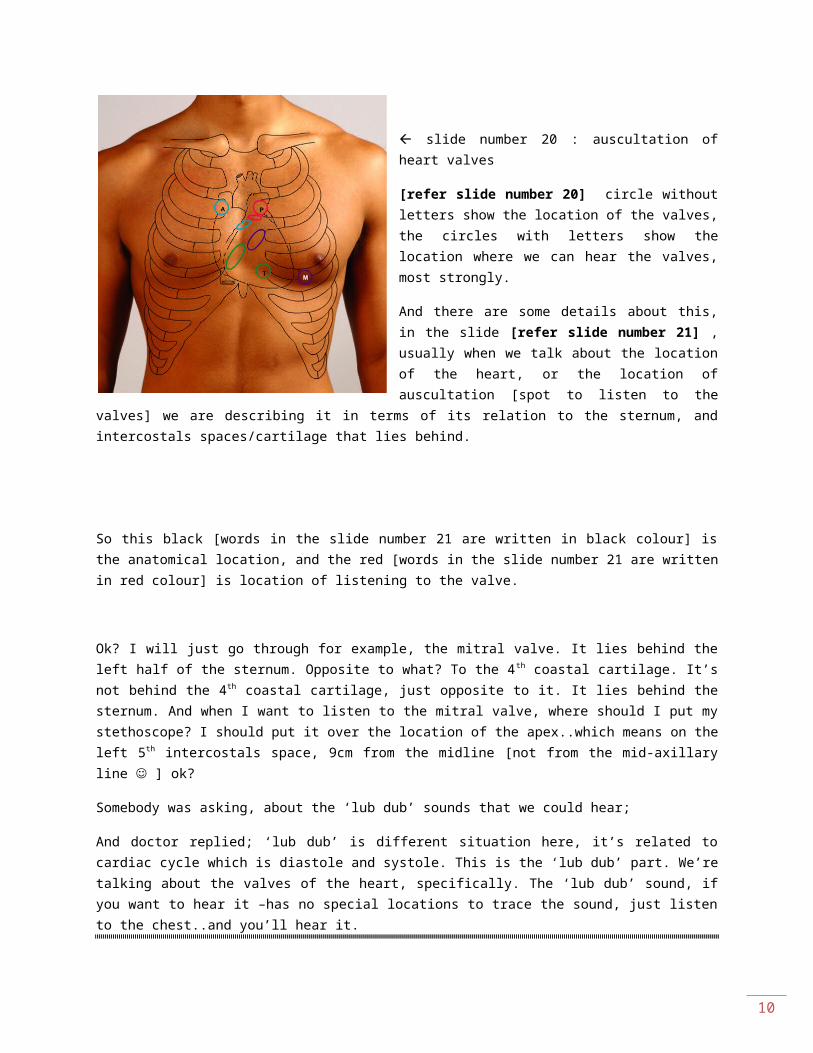
slide number 20 : auscultation of heart valves
[refer slide number 20] circle without letters show the location of the valves, the circles with letters show the location where we can hear the valves, most strongly.
And there are some details about this, in the slide [refer slide number 21] , usually when we talk about the location of the heart, or the location of auscultation [spot to listen to the
8
valves] we are describing it in terms of its relation to the sternum, and intercostals spaces/cartilage that lies behind.
So this black [words in the slide number 21 are written in black colour] is the anatomical location, and the red [words in the slide number 21 are written in red colour] is location of listening to the valve.
Ok? I will just go through for example, the mitral valve. It lies behind the left half of the sternum. Opposite to what? To the 4th coastal cartilage. It’s not behind the 4th coastal cartilage, just opposite to it. It lies behind the sternum. And when I want to listen to the mitral valve, where should I put my stethoscope? I should put it over the location of the apex..which means on the left 5th intercostals space, 9cm from the midline [not from the mid-axillary line ] ok?
Somebody was asking, about the ‘lub dub’ sounds that we could hear;
And doctor replied; ‘lub dub’ is different situation here, it’s related to cardiac cycle which is diastole and systole. This is the ‘lub dub’ part. We’re talking about the valves of the heart, specifically. The ‘lub dub’ sound, if you want to hear it –has no special locations to trace the sound, just listen to the chest..and you’ll hear it.
Somebody somewhere was asking, but her voice was so far from me;
But the doctor answered; both ventricles will contract at the same time. So blood will be pumped to the aorta and to the pulmonary trunk at the same time. This is what cause the ‘dub’ sound, I think. The ‘lub’ is the sound of blood rushing into the ventricles [from the atrium].
So the ‘lub dub’ sound corresponds with the cardiac cycle – diastole and systole phases.
Here we’re talking about different matters, either the valve does not closed tightly..so the valve is incompetent. Or either the valve does not open completely,so we have valvular stenosis. How they diagnose where the problem is located? By listening to each valve and detecting which sound is abnormal. What I said is just to explain, you don’t have to memorize this.
ok. We finished the innervations of the heart.
Now let’s talk about the posterior mediastinum..we talk about the middle part; which basically the heart and the pericardium. So now the posterior mediastinum means, it lies posterior to the heart and to the pericardium. The boundaries ? so basically this is the
9
posterior mediastinum [refer slide number 23] , and these are the boundaries [refer slide number 24] .
Anteriorly, we talk about the pericardium and the diaphragm. Posteriorly, we talk about the thoracic vertebrae – from T5 to T12. The superior boundary is an imaginary plane, from sternal angle to the intervertebral disk between T4 and T5. And inferiorly by the diaphragm.
So if you want to see the contents of this posterior mediastinum, you should remove the heart and everything, and this is how the cadaver will looks like [refer slide number 24] .
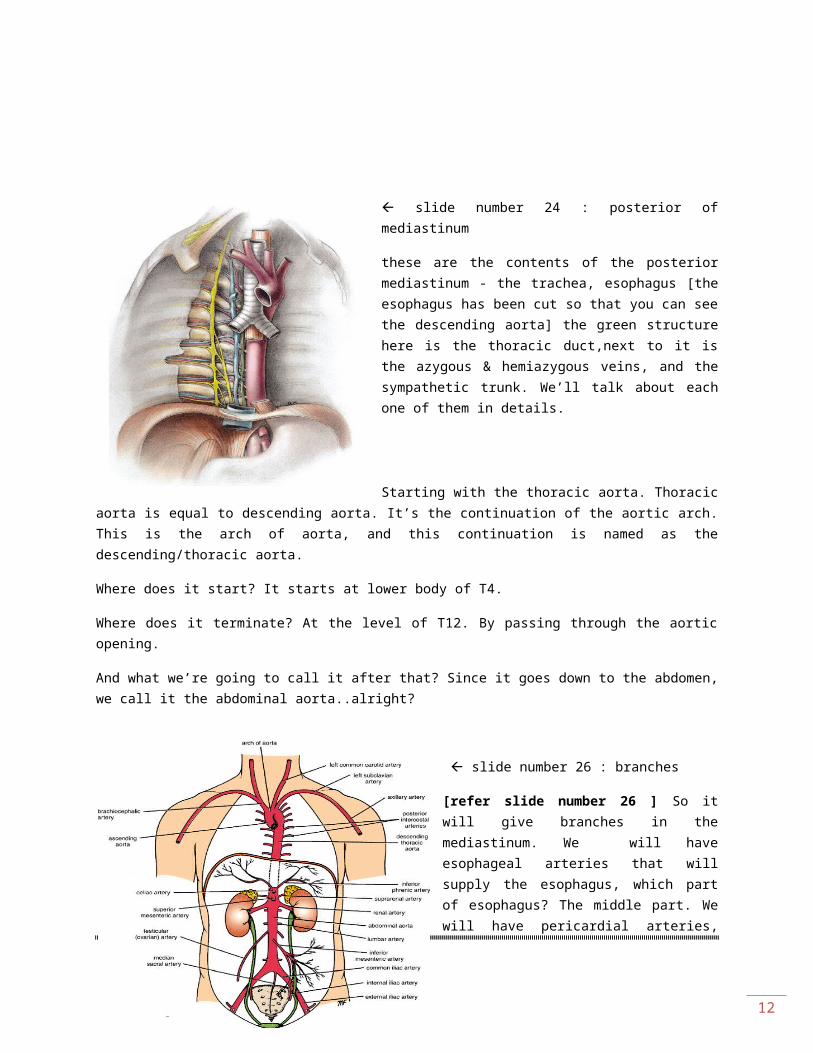
slide number 24 : posterior of mediastinum
these are the contents of the posterior mediastinum - the trachea, esophagus [the esophagus has been cut so that you can see the descending aorta] the green structure here is the thoracic duct,next to it is the azygous & hemiazygous veins, and the sympathetic trunk. We’ll talk about each one of them in details.
Starting with the thoracic aorta. Thoracic aorta is equal to descending aorta. It’s the continuation of the aortic arch. This is the arch of aorta, and this continuation is named as the descending/thoracic aorta.
Where does it start? It starts at lower body of T4.
Where does it terminate? At the level of T12. By passing through the aortic opening.
And what we’re going to call it after that? Since it goes down to the abdomen, we call it the abdominal aorta..alright?
10
slide number 26 : branches
[refer slide number 26 ] So it will give branches in the mediastinum. We will have esophageal arteries that will supply the esophagus, which part of esophagus? The middle part. We will have pericardial arteries, which supply the pericardium. It will also give the posterior intercostals arteries from the 3rd until diaphragm. Where does the 1st
and 2nd get supply from? We said this before, from the costocervical trunk. Ok. You don’t need to know…at least for this lecture.
And the 12th intercostals artery – we call it the subcostal artery. It will run along the inferior border of both rib and it will supplies structures in the abdomen.
We talked about the descending aorta. Now we talk about the venous structure [refer slide number 27] , we call it the azygous system. Mainly it is made of the azygous vein, and two accessories veins – we call it inferior hemiazygous and the other we call it superior hemiazygous.
Azygous means single. So in the exam, if I ask you if we have the right and left azygous vein, it’s a trick. You should say no. We have only one azygous vein, ok?
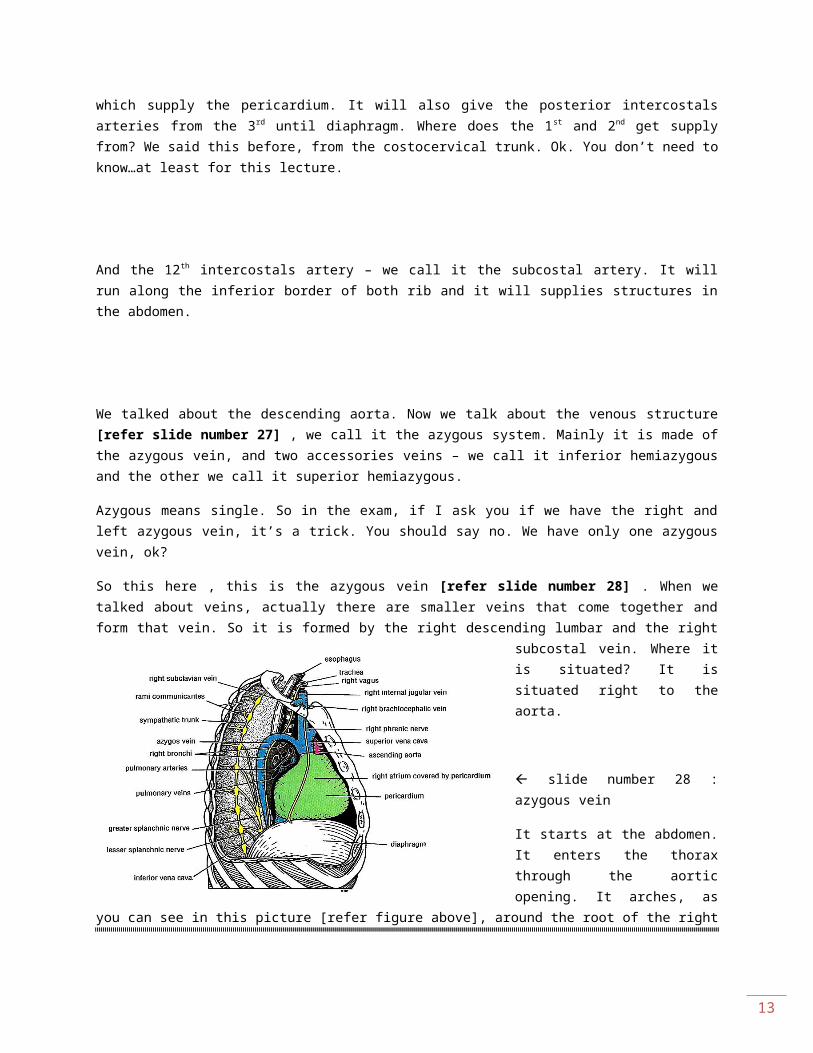
So this here , this is the azygous vein [refer slide number 28] . When we talked about veins, actually there are smaller veins that come together and form that vein. So it is formed by the right descending lumbar and the right subcostal vein. Where it is situated? It is situated right to the aorta.
slide number 28 : azygous vein
It starts at the abdomen. It enters the thorax through the aortic opening. It arches, as you can see in this picture
11
[refer figure above], around the root of the right lung, to join the superior venacava. Usually structures in the abdomen or in the lower part of the body may drain into the inferior venacava.
Here we have the example where, the blood can be drawn from those structures into the inferior venacava and be taken to the superior venacava. It’s an alternative pathway in our body.
The inferior hemiazygous vein, [refer slide number 29] , which is this part, it extends from T12 to T8, it takes blood from the lower intercostals veins. At which side? The left side..because the right side is the azygous vein!
slide number 30 : superior hemiazygous vein
We have also a superior hemiazygous vein, this part here [refer figure above] . Together they [the superior and inferior hemiazygous] make an H-shape in our body. And we mentioned this point – that it’s an alternative pathway to drain the blood from lower parts of the body.
We talked about thoracic aorta & the azygous vein. Now let’s talk about another contents of posterior mediastinum.
On the posterior mediastinum, we have thoracic duct. We mentioned that in the introduction. [refer slide number 32] . Thoracic duct starts in the abdomen, as dilated sac - we call it cisterna chyli. It will sends to the thorax, through the aortic opening. It drains lymphs from all parts of the body except the right upper quadrant, you know that already.
We also have right lympathic duct, which drains the right upper quadrant [refer slide number 33].
And where this structure empties?
It empties at the junction of right internal jugular and right subclavian vein. This is the internal jugular, it comes from the neck. This is subclavian vein, it comes from the upper limbs, just at the junction between them – right lymphatic duct empties. The thoracic duct empties in the internal jugular.
Are these ducts separated?
12
No. they communicate with each other. And this is significant special when we have cancer. When we have cancer in hepatocytes,it will travel throughout the body. They can jump from the right to the left side. By following the lymphatic system..which is very hazardous to the patient.
Now, the rest thing we should talk about the posterior mediastinum, is the sympathetic trunk [refer slide number 34] . For this lecture, we just want to know that, it is the most lateral structure in the posterior mediastinum. The location of the trunk, correspond to the location of the heads of the ribs. And it leaves behind the medial arcuate ligament.
Where does it go?
To the abdomen, extends from the thorax. Medial arcuate ligament is the attachment of the diaphragm, so the sympathetic trunk will not go through the diaphragm, it will goes behind the diaphragm. Ok?
Now we talk about the esophagus, which is part of our GIT system – gastrointestinal tract system [refer slide number 35] . The esophagus starts at the level of the cervical vertebrae number 6, and it will terminates by joining the stomach, after passing through the esophageal opening [at T10].
What we need to talk here is the thoracic part [refer slide number 36] . when we say relations of any structure of the body, we need to know - what lies anterior, what lies posterior, what lies to the left and right. That’s what we meant by relations. So, anterior to the esophagus we have trachea, and the left recurrent laryngeal nerve. I’m going to tell you in a bit, where this is come from. It comes from the base, posterior to the esophagus – we have the bodies of the thoracic vertebrae and the thoracic aorta, and the thoracic duct and azygous vein. They are posterior and slightly to the right.
[refer slide number 37] So when we talk about the right, we have the right of the surface. We have mediastinal pleura, we have azygous vein. On the left side of the esophagus, by looking at the picture you can simply know the relations.
slide number 37 : thoracic part relations
We have aortic arch, left subclavian artery and the upper part of the thoracic duct.
Vagus nerves, when we go to the thorax in the lower part, they will join the esophagus. They will travel closely with the esophagus. And we have both – right and left vagus nerves. They will rotate the esophagus, and the right vagus will become posterior. While the left will become anterior.
13
****************************
Before jumping to the superior mediastinum, [I should tell this at the beginning] for your practical exam, it’s gonna be straight forward. Pictures you see in the lab, pictures you see in the atlas [textbook]. The checklists have been given to the class representatives. So all of you should have the access to the checklists.
What’s included in the exam? Thoracic wall, thoracic cavity and heart. This 1st practical exam is online..you’ll have multiple choice questions regarding that pictures. The exam will be at November 2nd, 2010. The exam will be on the lecture’s time.
Allah yu3tiku l-3aafiyah.
Done by ;
Nabilah Yaakob
Related Documents











