An Overview for Staff, Community Providers and Stakeholders Shelley Straughan & Dana Torrey Safety & Reunification Coordinators Department of Human Services 2012 Oregon Safety Model with Differential Response 1

An Overview for Staff, Community Providers and Stakeholders Shelley Straughan & Dana Torrey Safety & Reunification Coordinators Department of Human Services.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
An Overview for Staff, Community Providers and
Stakeholders
Shelley Straughan & Dana TorreySafety & Reunification
CoordinatorsDepartment of Human Services
2012Adapted from work by: ACTION for Child Protection, Inc.
Oregon Safety Model with Differential Response
1

Purpose and Goals of Presentation
To understand Differential Response (DR) as an accepted national practice leading to improved outcomes for families and child welfare systems
To learn how the Oregon Safety Model (OSM) and DR compliment each other and will work together to improve outcomes
To revisit the importance of Engagement in our work with families
2

Why Change Practice….again?All fields are consistently improving their practice
and skill…an ongoing professional obligation
Originally, abuse reports were handled by general child welfare programs…with a helping approach
Over time, the “legalistic” aspects of investigation, evidence, perpetrators, court involvement, etc. reinforced a more adversarial, unhelpful approach
Some areas, like central registry entries, have much greater impact on individuals than ever before yet…The process of reaching a finding/disposition
lacks precision and consistency
3

Why Change Practice?
Investigating and identifying a perpetrator does little to increase child safety
Families report being fearful or upset when CPS intervenes…Re-traumatization by the “system”Unlikely to divulge critical underlying needsCompliance rather than change
Circumstances and needs of families differ and so should the system’s response.
4

Majority of reports received today do not need adversarial approach or court-ordered interventions
Child protection intervention is governmental intrusion into private family life, and the level/type of intrusion should closely match the presenting concerns
Systems screen out or do not offer services in 50% or more of reports, yet many children and families are in need of some helpful intervention
Why Change Practice?
5

Differential Response
A National Perspective
6

Differential Response Defined
An approach that allows child protective services to respond differently to accepted reports of child abuse and neglect based on such factors as the type and severity of the alleged maltreatment, number and sources of previous reports, and willingness of the family to participate in services. (American Humane Association)
7
What is Differential Response?
A choice of approaches
At least 2 Tracks “Alternative” and
“Traditional”
No fault finding, “disposition” or entry of perpetrator into Central Registries
Typically applied to reports that do not allege serious harm
8

What is Differential Response?A choice of approaches Focus is more on assessing and
ensuring child safety. Less on investigative fact finding
Allows families to receive agency funded services without formal determination of abuse/neglect, and when children are “safe”
Families may refuse services if children are safe
9

DR Expectations: Parent(s)/Caregivers will report positive
experiences with the DHS worker and primary service provider
Parent(s)/Caregivers will report that services provided were what they needed
Children will report that they had opportunities to discuss issues in private environments
Children will report positive experiences with the DHS worker and the primary service provider
Parent(s)/Caregivers will report they were treated fairly and in culturally appropriate ways
10

DR Expectations:
11
Improved job satisfaction for DHS workers who provide DR assessments
All families will receive a competent safety assessment consistent with the OSM, regardless of the track assigned
All families served by DR will receive a focused assessment (PCA and Strength and Needs Assessment)
Services will match to child and family need and will be targeted, solution-focused, time-limited.
Simplified outcome tools and measures will be used to gauge effectiveness of interventions.

National Implementation StatusMissouri was first state in 1994
13 states now implemented statewide
11 are implementing in selected counties
Tribal groups in 6 states are implementing
4 more states and DC are planning or considering implementation
12

DR Evaluation/Outcomes to Date
What have we learned?
13
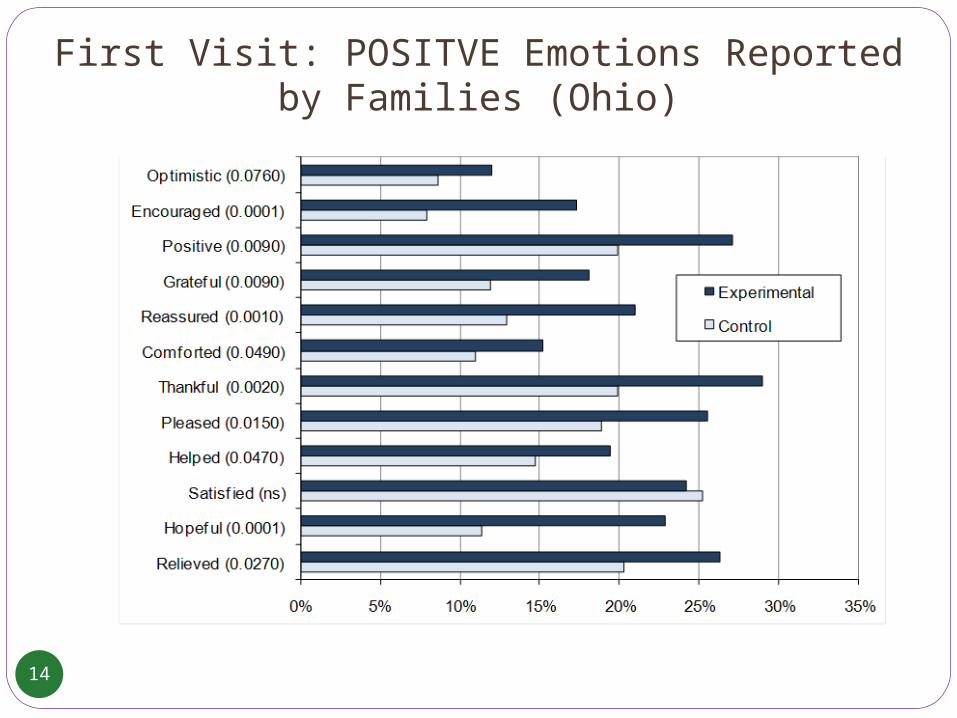
First Visit: POSITVE Emotions Reported by Families (Ohio)
14
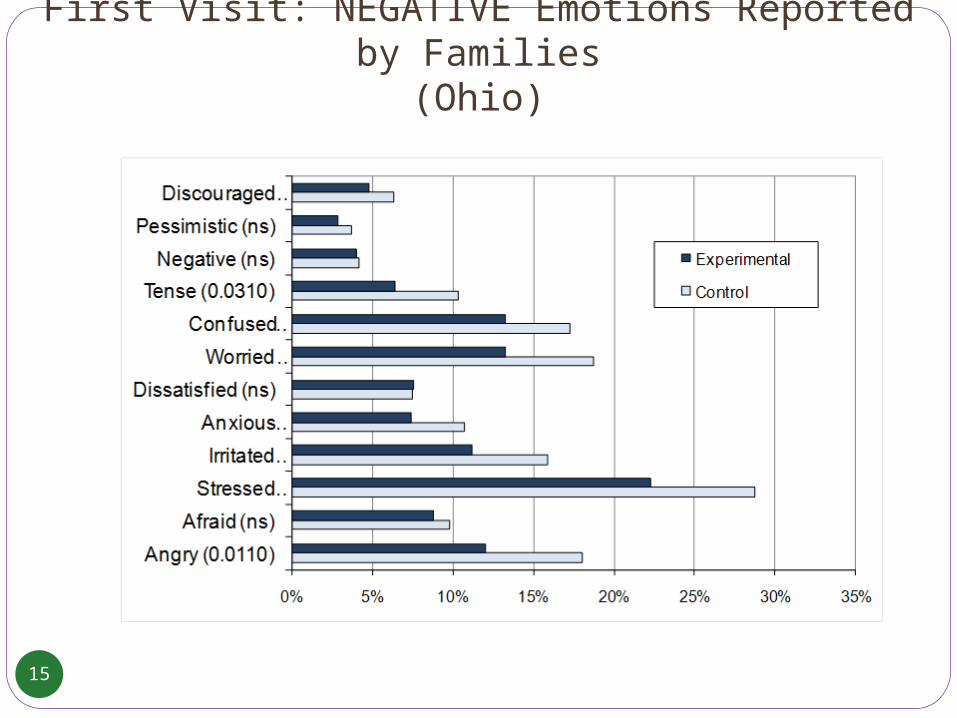
First Visit: NEGATIVE Emotions Reported by Families(Ohio)
15

Characteristics of families served through DR (Ohio):
Neglect was most common reportAbout half had previous accepted
reports of abuse/neglect 1 in 10 had a child placed in the pastA substantial portion were “chronic
CPS” familiesPoverty was prevalentMost received concrete help with utility
payments, unreliable transportation, lack of household goods/appliances, etc.

Other important findings (Missouri and Ohio)Child safety was NOT reducedFamilies reported more involvement in decision-
making and said services “really helped”More worker contacts with families and providersHigher family satisfaction with their caseworkerHigher job satisfaction for caseworkersLess subsequent reports of abuse/neglectLess out of home placementsCost slightly more upfront, but potential for
reduced long-term costs

Families were more likely to participate in services post-assessment.
The family friendly, non adversarial, participatory and voluntary aspects of DR led to reduced levels of future reports…
…Regardless of whether services were or were not offered to the families.

The Essential Nature of Engagement
19

Engagement is the means we use to offer hope,
the promise that things will be better,and the only way to establish rapport
leading to positive and powerful relationships.
20

Factors Accounting For Success in Change
Client – 40%
Relationship – 30%
Hope/Expectancy – 15%
Models/Techniques – 15%
Hubble, M., Duncan, B., & Miller, S. (1999). The Heart and Soul of Change. Washington, D.C.: APA Press21

Exercise: Self-Determination
22

Valuing Self-Determination in CPS: Proximity Scale (Not Scientific but Sufficient for Training Purposes)
23 – 30Strongly believe that client choice is not a realistic
concept to apply in CPS and must be guarded against. 15 – 22
Believe that client choice can only be applied selectively in CPS and must be regulated.
7 – 14Believe that client choice is an admirable objective, but
may vary in how practical a concept it is for CPS intervention.
0 – 6Strongly believe that client choice is fundamental to
successful CPS intervention.
23

Shared SW Philosophy: OSM and DRSummarized and adapted from: DuBois, B. & Miley, K.K. (1992). Social Work: An Empowering Profession, Boston: Allyn and Bacon, pp. 135-141.
24

Oregon Safety ModelIntegrating Differential Response
25

The Oregon Safety Model
Implementation of The Oregon Safety Model (OSM) was begun in 2006-07
Consistent efforts will continue to improve the application of OSM safety concepts and family-centered practices
Oregon DHS will continue all OSM practices while integrating Differential Response
26

Oregon’s Child Welfare System Goals:
The principles of the OSM, DR, SB 964 are working in concert toward:Keeping children safe and at home.Increasing and enhancing effective
preventive and family reunification services Decreasing the number of African-American
and Native American children placed in foster care and reducing the length of stay when they are placed
Strengthening partnerships between child welfare agencies, community-based organizations, and families
27

Why Differential Response?
DR is driven by the desire to….Be more flexible in the response to child
abuse/neglect.Address family needs more quickly; most cases not
driven by court intervention, so evidence collection is not necessary.
Build family support systems; DR is often accompanied by greater efforts to identify, build, and coordinate formal and informal family supports.
Be more intentional about connecting families to resources when children are “safe” (as defined by Oregon Safety Model practice)
28

Development of DR in OregonDR in Oregon is a work in progress.
Internal DHS research Legislative Presentation DR Manager Hired Focus Groups: DHS staff, Providers, Tribes, Families,
Advocates, Legal and Judicial, etc. Core and Design Teams In-Home Safety and Reunification Team hired 12 Orientations around the state in May 2012
Planning and development will continue, we are now in the design phrase and will be moving into both the developmental phrases and implementation phrase
No date for implementation at this time period
29

DR is not being considered as a method to reduce workload and will not increase the number of cases opened by DHS Child Welfare.

The Oregon Safety Model Guides DR Decisions
31
A Comprehensive Safety Assessment is completed by a CPS worker in both tracks
If children are determined to be “unsafe” the case will be opened by Child Welfare
If children are determined to be “safe” Child Welfare will not open a case
If children are “safe”, but moderate to high needs are identified, families may receive services from community providers (no Child Welfare case open)
Protective Capacity Assessment guides case planning by Child Welfare and influences voluntary services to DR families.

Oregon’s 2 Tracks : Traditional and Alternative?
(Handout)
32

33
Traditional Track Alternative Track
Safety Assessment Safety Assessment
Joint Assessment with provider strongly encouraged
Joint Assessment with provider strongly encouraged
Disposition/finding required No disposition/finding required
Central Registry entry as indicated No entry in Central Registry
Services offered if child is “unsafe” as defined in OSM practice
Services Offered if Mod to High Needs & children are “safe” as defined in OSM practice
Participation is not voluntary Participation is Voluntary/Family may decline services
May involve court action No court involvement

34
Traditional Track Alternative Track
There will be an in-home or out-of-home safety plan
No Safety Plan is needed
Children remain in the home with in- home safety plan if:• parent is willing/able to engage• home is safe and calm enough to allow safety service providers access• sufficient safety service providers available to assist in managing the child(ren)’s safety
Children remain in the home
Out-of-home safety plan required if above not met; court involvement
No out-of-home placements; no court-involvement
Protective Capacity Assessment (PCA) directs Case Planning
Protective Capacity Assessment (PCA) forms core of Strength and Needs Assessment, voluntary service provision
DHS opens and carries the case if child(ren) determined “unsafe”
DHS does not open a case when children are determined “safe”

35
Traditional Track Alternative Track
Services provided based on case plan, continue until case closure
Services provided based on Strengths and Needs Assessment, time limited, solution focused
Ongoing Safety Management Ongoing attention to child safety
Case closed when threats are eliminated or protective capacities are sufficiently enhanced to manage the safety threats, children are “safe”
Case closed when client opts out, goals reached, no services needed, or service time frame complete

36
CALL/REFERRAL TO DHS
INITIAL CONTACT:DHS AND PROVIDER
SAFETY ASSESSMENT COMPLETED BY DHS
INITIAL CONTACTDHS AND PROVIDER
SAFETY ASSESSMENT COMPLETED BY DHS
SAFETY THREATS EXISTOR TRADITIONAL INTERVENTION IS NEEDED. DETERMINE DISPOSITION,
CENTRAL REGISTRYENTRY PER POLICY: FOLLOWS OSM FOR SAFETY PLANNING AND INTERVENTION
DHS OPENS AND CARRIES CASE
FAMILY DECLINES SERVICES
NO SAFETY THREATS
DHS DOES NOT OPEN CASE** PROVIDER DOES STRENGTHS/
NEEDS ASSESSMENT WITH FAMILY SERVICES OFFERED
PROVIDER CONTINUES SERVICES WITH FOCUS ON
CHILD SAFETY
90 DAY SUMMARY AND OUTCOME REPORT BY PROVIDER TO DHS
DIFFERENTIAL RESPONSEPROCESS AND
DECISION FLOWACTION FOR CHILD PROTECTION INC
MEETS CRITERIA ASREPORT OF CHILD ABUSE OR
NEGLECT
NO SAFETY THREATS PROVIDER CONDUCTS
STRENGTHS/ NEEDS ASSESSMENTMOD TO HIGH
NEED=SERVICES OFFERED.
REPORT NOT ACCEPTED/REFER TO OTHER
RESOURCES
FAMILY ACCEPTS SERVICES
Alternative Track Traditional Track
IF NEW REPORT OF CA/N
No services needed or family declines
service
PROVIDER CLOSES CASE
FAMILY SEEMS TO HAVE MOD
TO HIGH NEED AND WANTS SERVICES
PROVIDER REQUESTS EXTENSION IF NEEDED. CONTINUES SERVICES WITH FOCUS ON CHILD SAFETY
DHS DOES NOT OPEN CASE
DHS DOES NOT OPEN CASE
DHS DOES NOT OPEN CASE
** If no provider at initial contact, worker arranges warm handoff with provider/family

Questions & Answers
Related Documents











