Cancer Immunology Miniatures An Abscopal Response to Radiation and Ipilimumab in a Patient with Metastatic Non–Small Cell Lung Cancer Encouse B. Golden 1 , Sandra Demaria 1,2 , Peter B. Schiff 1 , Abraham Chachoua 3 , and Silvia C. Formenti 1 Abstract A posteriori evidence suggests that radiotherapy to a targeted tumor can elicit an immune-mediated abscopal (ab-scopus, away from the target) effect in nontargeted tumors, when combined with an anti-CTL antigen-4 (CTLA-4) monoclonal antibody. Concurrent radiotherapy and CTLA-4 blockade induced immune-mediated abscopal effects in poorly immunogenic preclinical tumor models and patients with metastatic melanoma. However, no such reports exist for patients with metastatic lung adenocarcinoma. We report the first abscopal response in a treatment-refractory lung cancer patient treated with radiotherapy and ipilimumab (a human anti- CTLA-4 monoclonal antibody). A posttreatment increase in tumor-infiltrating cytotoxic lymphocytes, tumor regression, and normalization of tumor markers was observed. One year after treatment with concurrent radiotherapy and ipilimumab, the patient is without evidence of disease. Cancer Immunol Res; 1(6); 365–72. Ó2013 AACR. Introduction The abscopal (ab-scopus, away from the target) effect is a term used to describe radiotherapy-induced tumor regression in lesions distant from a targeted site, and has been known for six decades as a rare unexplained phenomenon in patients receiving local radiotherapy (1). We hypothesized that the abscopal effect may result from a radiotherapy-induced immu- nogenic type of cancer cell death capable of generating an in situ vaccine (2–4). In support of this notion, interventions that promote the functionality of dendritic cells or improve T-cell activation are required to produce the abscopal effect (5–8). This strongly suggests that, while radiotherapy alone may be efficient at exposing cryptic tumor antigens, tumor cell–induced immunosuppression and immunotolerance hamper the development of therapeutically effective antitu- mor immune responses (3, 4). Immunotherapeutic strategies aimed at overcoming immu- notolerance and improving the activation of antitumor T cells represent a new promising therapeutic approach (9). Among them, the human anti-CTL antigen-4 (CTLA-4) antibody, ipi- limumab, has demonstrated activity in metastatic melanoma treatment, for which it has U.S. Food and Drug Administration (FDA) approval (10, 11). Yet, the role of ipilimumab in other malignancies and in combination with radiotherapy still remains investigational. In non–small cell lung cancer (NSCLC), ipilimumab has been tested in combination with chemotherapy [paclitaxel, 175 mg/m 2 body surface area (BSA), and carboplatin (area under the curve, 6), infused every 3 weeks] in a phase II trial, including 204 patients with stage IIIB/IV or recurrent disease (12). Induction ipilimumab was administered every 3 weeks for four doses at 10 mg/kg body weight, either concurrently with chemotherapy (concurrent regimen) or after two doses of chemotherapy (phased regimen). Patients without disease progression or adverse effects from ipilimumab continued with maintenance therapy once every 12 weeks. The study met its primary endpoint of improved immune-related pro- gression-free survival (referred to as irPFS, which takes into account tumor regression in the presence of new lesions) and the endpoint of PFS for the phased regimen, but not the concurrent regimen, when compared with chemotherapy alone (control regimen; refs. 12, 13). A difference was observed in the immune-related best overall response rates (irBORR) between the control regimen and the phased regimen, 18% versus 32%. In addition, a difference was observed in the median PFS between the control regimen and the phased regimen, 4.2 months versus 5.1 months. However, no difference was observed in the irBORR between the control regimen and the concurrent regimen, 18% versus 21%. Also, no difference was observed in the median PFS between the control regimen and the concurrent regimen, 4.2 months versus 4.1 months. Of note, on subset analysis, the nonsquamous histology group, including adenocarcinomas, treated with the phased regimen demonstrated a trend toward a worsened hazard ratio (HR) for overall survival, when com- pared with chemotherapy alone [HR, 1.17 (95% CI, 0.74–1.86)]. Because of these results, patients with squamous cell histology are currently being recruited for a phase III trial comparing the phased regimen with the control regimen for first-line treat- ment (14). Authors' Affiliations: Departments of 1 Radiation Oncology, 2 Pathology, and 3 Medicine, New York University School of Medicine, New York, New York Corresponding Author: Silvia C. Formenti, Department of Radiation Oncology, New York University School of Medicine, 160 East 34th Street, New York, NY 10016. Phone: 212-731-5039; Fax: 212-731-5513; E-mail: [email protected] doi: 10.1158/2326-6066.CIR-13-0115 Ó2013 American Association for Cancer Research. Cancer Immunology Research www.aacrjournals.org 365 on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cancer Immunology Miniatures
An Abscopal Response to Radiation and Ipilimumab in aPatient with Metastatic Non–Small Cell Lung Cancer
Encouse B. Golden1, Sandra Demaria1,2, Peter B. Schiff1, Abraham Chachoua3, and Silvia C. Formenti1
AbstractA posteriori evidence suggests that radiotherapy to a targeted tumor can elicit an immune-mediated abscopal
(ab-scopus, away from the target) effect in nontargeted tumors, when combined with an anti-CTL antigen-4(CTLA-4) monoclonal antibody. Concurrent radiotherapy and CTLA-4 blockade induced immune-mediatedabscopal effects in poorly immunogenic preclinical tumor models and patients with metastatic melanoma.However, no such reports exist for patients with metastatic lung adenocarcinoma. We report the first abscopalresponse in a treatment-refractory lung cancer patient treated with radiotherapy and ipilimumab (a human anti-CTLA-4 monoclonal antibody). A posttreatment increase in tumor-infiltrating cytotoxic lymphocytes, tumorregression, and normalization of tumor markers was observed. One year after treatment with concurrentradiotherapy and ipilimumab, the patient is without evidence of disease.Cancer Immunol Res; 1(6); 365–72.�2013AACR.
IntroductionThe abscopal (ab-scopus, away from the target) effect is a
term used to describe radiotherapy-induced tumor regressionin lesions distant from a targeted site, and has been known forsix decades as a rare unexplained phenomenon in patientsreceiving local radiotherapy (1). We hypothesized that theabscopal effectmay result from a radiotherapy-induced immu-nogenic type of cancer cell death capable of generating an insitu vaccine (2–4). In support of this notion, interventions thatpromote the functionality of dendritic cells or improveT-cell activation are required to produce the abscopal effect(5–8). This strongly suggests that, while radiotherapy alonemay be efficient at exposing cryptic tumor antigens, tumorcell–induced immunosuppression and immunotolerancehamper the development of therapeutically effective antitu-mor immune responses (3, 4).Immunotherapeutic strategies aimed at overcoming immu-
notolerance and improving the activation of antitumor T cellsrepresent a new promising therapeutic approach (9). Amongthem, the human anti-CTL antigen-4 (CTLA-4) antibody, ipi-limumab, has demonstrated activity in metastatic melanomatreatment, for which it has U.S. Food and Drug Administration(FDA) approval (10, 11). Yet, the role of ipilimumab in othermalignancies and in combination with radiotherapy stillremains investigational.
In non–small cell lung cancer (NSCLC), ipilimumab hasbeen tested in combination with chemotherapy [paclitaxel,175 mg/m2 body surface area (BSA), and carboplatin (areaunder the curve, 6), infused every 3 weeks] in a phase II trial,including 204 patients with stage IIIB/IV or recurrent disease(12). Induction ipilimumab was administered every 3 weeksfor four doses at 10 mg/kg body weight, either concurrentlywith chemotherapy (concurrent regimen) or after two dosesof chemotherapy (phased regimen). Patients without diseaseprogression or adverse effects from ipilimumab continuedwith maintenance therapy once every 12 weeks. The studymet its primary endpoint of improved immune-related pro-gression-free survival (referred to as irPFS, which takes intoaccount tumor regression in the presence of new lesions) andthe endpoint of PFS for the phased regimen, but not theconcurrent regimen, when compared with chemotherapyalone (control regimen; refs. 12, 13).
A difference was observed in the immune-related bestoverall response rates (irBORR) between the control regimenand the phased regimen, 18% versus 32%. In addition, adifferencewas observed in themedian PFSbetween the controlregimen and the phased regimen, 4.2 months versus 5.1months. However, no difference was observed in the irBORRbetween the control regimen and the concurrent regimen, 18%versus 21%. Also, no differencewas observed in themedian PFSbetween the control regimen and the concurrent regimen, 4.2months versus 4.1 months. Of note, on subset analysis, thenonsquamous histology group, including adenocarcinomas,treated with the phased regimen demonstrated a trend towarda worsened hazard ratio (HR) for overall survival, when com-pared with chemotherapy alone [HR, 1.17 (95% CI, 0.74–1.86)].Because of these results, patients with squamous cell histologyare currently being recruited for a phase III trial comparing thephased regimen with the control regimen for first-line treat-ment (14).
Authors' Affiliations: Departments of 1Radiation Oncology, 2Pathology,and 3Medicine, New York University School of Medicine, New York, NewYork
Corresponding Author: Silvia C. Formenti, Department of RadiationOncology, New York University School of Medicine, 160 East 34th Street,New York, NY 10016. Phone: 212-731-5039; Fax: 212-731-5513; E-mail:[email protected]
doi: 10.1158/2326-6066.CIR-13-0115
�2013 American Association for Cancer Research.
CancerImmunology
Research
www.aacrjournals.org 365
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

The improved efficacy of the phased approach, as opposedto the concurrent regimen, suggests that additional factors(other than CTLA-4 blockade) influence tumor-specific T-cellresponses in patients with advanced-stage NSCLC. Theobserved differences may have been the result of the qualityof tumor cell death (immunogenic vs. nonimmunogenic) or theimmune-modifying effects (inhibitory vs. stimulatory) of che-motherapy at the time of ipilimumab administration (4, 12)These are some of the issues that underscore the challengesthat remain in designing optimal combination therapies withipilimumab.
Interestingly, when given as a monotherapy in patients withNSCLC,CTLA-4 blockadedemonstrated nodifference in PFS ascomparedwith best supportive care (BSC). In a phase II trial, 87patients with NSCLC (locally advanced or metastatic) treatedwith four or more cycles of first-line platinum-based therapy[resulting in either stable disease or response per ResponseEvaluation Criteria in Solid Tumors (RECIST) criteria] were
randomized to tremelimumab (a CTLA-4–blocking immuno-globulin G2 monoclonal antibody) as maintenance therapy(n ¼ 43) or BSC (n ¼ 43; ref. 15). Tremelimumab did notimprove PFS; however, 2 (4.8%) partial responses (out of 9patients without disease progression) were seen in thetremelimumab arm, whereas no partial responses (out of6 patients without disease progression) were seen in theBSC arm. On the basis of these results as a single agent inNSCLC, future development of tremelimumab has not beenpursued (14).
We previously demonstrated in preclinical models of poorlyimmunogenic carcinomas not responsive to anti-CTLA-4monotherapy that local radiotherapy synergizes with anti-CTLA-4 antibody. Antitumor T-cell responses that inhibit thegrowth of locally irradiated tumors as well as their nonirradi-ated metastatic counterparts were demonstrated (abscopaleffect; refs. 5, 8, 16). Consistent with these findings, an abscopaleffect was recently reported in 2 patients with treatment-
Figure 1. Registration of PET/CTand CT/simulation to targetintrahepatic lesion. The PET/CTfrom August 2012 (left) wasimported into the Eclipse planningsoftware (Varian Medical Systems,Inc.) and registered to the CT/simulation (right) that was acquiredbefore treatment. Selected axial(top), coronal (middle), and sagittal(bottom) images are displayed. Themost hypermetabolic liver lesionwas selected as the gross tumorvolume (white arrows, left). Thetreatment plan was designed with6-MV photons by means of acoplanar five-field intensity-modulated technique toencompass the gross tumorvolume with a 1-cm margin (right).The treatment was prescribed tothe 100% isodose line to a totaldose of 30 Gy distributed over fivefractions. The isodose linesrepresent total doses of 30 Gy(yellow), 15 Gy (orange), and 9Gy (light blue; right).
Golden et al.
Cancer Immunol Res; 1(6) December 2013 Cancer Immunology Research366
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

refractory melanoma receiving radiotherapy with ipilimumab(17, 18). However, until now it was unknown whether radio-therapy can potentiate the response to CTLA-4 blockade intumor types that have previously shown little to no clinicalresponse. Herein, we report the first case of an abscopalresponse in a patient diagnosed with metastatic NSCLC trea-ted with radiotherapy and ipilimumab. Remarkably, thepatient showed regression, not only at the radiotherapy-tar-geted site but also in multiple abscopal sites of disease,including visceral and skeletal metastases.
Case PresentationIn March 2010, a 64-year-old Caucasian male with a 70
cigarette-pack-year history presented with a palpable leftsupraclavicular nodule. An excisional biopsy of the massshowed metastatic adenocarcinoma with an immunohisto-chemical profile consistent with a lung primary (CK7- andTTF-1–positive and CK20- and CDX2–negative). The pati-ent's initial positron emission tomography/computedtomography (PET/CT) scan showed two right upper lobenodules, a left lower lobe nodule, and right supraclavicularand bilateral hilar/mediastinal adenopathy. He was stagedas T1bN3M1a (stage IV) according to the AmericanJoint Commission on Cancer seventh edition cancer stagingmanual, with a predicted median survival of 7 months (19).The patient was initiated on pemetrexed, 500 mg/m2 BSAand carboplatin (area under the curve, 5) given every 3weeks for six cycles. After the sixth cycle, a surveillancePET/CT showed a decrease in size and metabolic activity ofboth the right supraclavicular adenopathy (from 2.8 cm �1.7 cm and a standard uptake value (SUV) of 10.2 to 2.0 cm� 1.2 cm and SUV of 3.8) and the left lower lobe nodule(from 6 mm and SUV of 2.3–3 mm and undetectable SUV).The two right upper lobe nodules and hilar/mediastinalnodal disease remained stable in size and metabolicactivity.The patient, thereafter, continued maintenance therapy
with pemetrexed, 500 mg/m2 BSA alone, given every 3 weeks.However, after three cycles, he developed severe lower extrem-ity cellulitis, at which point the pemetrexed was temporarilydiscontinued. After antibiotic treatment and resolution of thecellulitis, he received an additional three cycles of pemetrexedand subsequently underwent a repeat PET/CT. The PET/CTrevealed stable disease in the right upper lobe and left lowerlobe nodules and improvement in the size and metabolicactivity in the right supraclavicular and hilar/mediastinaladenopathy.From February 2011 to April 2011, systemic chemotherapy
was interrupted to start radiotherapy to the metabolicallyactive right lung nodules and the right supraclavicular, righthilar, and mediastinal adenopathy to a total dose of 59.4 Gydelivered over 33 fractions. Subsequent chest CTs in Mayand July 2011, in comparison with the CT before radiother-apy, showed a decrease in size of the irradiated pulmonarynodules and adenopathy. However, in September 2011, asurveillance PET/CT revealed increased metabolic activityand size of the right upper lobe nodule and the previously
seen left lower lobe nodule. Treatment with pemetrexed, 500mg/m2 BSA alone was resumed and given every 3 weeks foran additional 10 cycles.
In June 2012, a repeat PET/CT revealed disease progressionwith new hypermetabolic liver lesions, new periaortic adeno-pathy, and a new bony lesion in the sacrum. In addition, theright upper lobe and left lower lobe nodules and hilar/medi-astinal adenopathy showed an increase in metabolic activity.
Figure 2. Ipilimumab and local radiotherapy result in an abscopalresponse. PET imaging and select fused PET/CT axial images fromAugust 2012 (left) and January 2013 (right) are displayed. The axialimages in the second row reveal the hypermetabolic liver lesion that wastargeted and responded to radiotherapy (white arrows, second row). Anabscopal responsewas seen in a left lower lobe lung lesion (white arrows,third row) and a left sacral lesion (white arrows, bottom row). A mixedresponse was seen in the hilar/mediastinal lymph nodes (striped arrows,third row).
An Abscopal Response to Radiation and Ipilimumab
www.aacrjournals.org Cancer Immunol Res; 1(6) December 2013 367
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

The patient was then treated with gemcitabine, 750 mg/m2
BSA, and vinorelbine, 30mg/m2 BSA, given every 2 weeks. Afterthe fourth cycle, in August 2012, a PET/CT showed further
disease progression in the liver and growth of new lytic lesionsin the bony pelvis, thoracolumbar spine, and right humerus(Figs. 1 and 2).
GemcitabineVinorelbine
Jun-12
12
8
4
0
150
100
50
0
3
2
1
0
1.5
1
0.5
0
Aug-12
Progression(PET/CT)
103 /
mL
CE
A [
ng
/mL
]
103 /
mL10
3 /mL
Progression(PET/CT)
WBC
A
B
ALC
AEC
Response(CT)
Response(PET/CT)
Oct-12 Dec-12
RT 30 GyIpilimumab
RT 30 GyIpilimumab
8/10
/12
11/1
0/12
2/10
/13
5/10
/13
Figure 3. Treatment timeline and the absolute peripheral blood cell counts. A detailed clinical timeline is displayed (A, top). A PET/CT on June 8, 2012, showeddisease progression, prompting a change in the patient's chemotherapy regimen. On June 15, 2012, the patient was started on a chemotherapy regimencontaininggemcitabine and vinorelbine. The greenmarker indicates the treatment timeline for gemcitabine and vinorelbine (A, top). A repeat PET/CTonAugust 6,2012, showed continued disease progression. From August 22, 2012, to August 31, 2012, the patient was treated with concurrent radiotherapy (RT) andipilimumab. Afterward, he received three additional cycles of ipilimumab alone. The bluemarker indicates the treatment timeline for radiotherapy and ipilimumab[A (top) and B], and data plotted to the right of the vertical dashed line in each graph represents postinitiation of radiotherapy and ipilimumab treatment[A (bottom threegraphs) andB]. Thefinal doseof ipilimumabwasgivenonOctober 26, 2012. ImagingonNovember8, 2012 (CTof thechest, abdomen, andpelvis)and January 17, 2013 (PET/CT), showed significant treatment responses. During the course of treatment, the patient had serial blood draws. The results of theperipheral absolute blood cell counts [white blood cells (WBC), absolute leukocyte count (ALC), and absolute eosinophil count (AEC)] are displayed as number ofcells (�103) per mL of whole blood (A, bottom three graphs), in accordance with the aforementioned treatment timeline (A, top). A dramatic drop incarcinoembryonicantigen levels (anonspecific tumormarker) wasobservedafter treatmentwith radiotherapyand ipilimumab (B). Themarkerpeakedat 119.6 ng/mL (normal levels 0–5 ng/mL) onSeptember 7, 2012, showing a dramatic drop to 5.8 ng/mL onOctober 26, 2012, and thereafter wasmaintained at normal levels.
Golden et al.
Cancer Immunol Res; 1(6) December 2013 Cancer Immunology Research368
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115
Ipilimumab (received as a compassionate exemption)with local radiotherapy to one of the hepatic metastaseswas initiated, with the intent to generate an abscopalresponse. The experimental nature of this approach wasextensively discussed with the patient, who was informed ofthe only two available reports in melanoma and the lack ofavailable evidence for patients with NSCLC.The patient was simulated in the supine position and his
CT/simulation was registered to the August 2012 PET/CT fortreatment planning purposes (Fig. 1). The most metaboli-cally active liver mass, located in the caudate lobe, wasselected as the radiotherapy target and contoured as thegross tumor volume (GTV). An additional 0.5-cm margin wasadded to create a clinical target volume (CTV), and another0.5 cm margin was added to the CTV to create a planningtarget volume (Fig. 1). Radiotherapy to a total dose of 30 Gydistributed over five fractions was delivered over a period of10 days with 6-MV photons and a coplanar five-field inten-sity-modulated technique (Fig. 1). The day after the firstradiotherapy fraction, the patient was infused with ipilimu-mab, 3 mg/kg body weight. Thereafter, the patient complet-ed three more cycles of ipilimumab, 3 mg/kg body weight,infused at 3-week intervals. The patient tolerated radiother-apy and ipilimumab without any treatment-related adverse
events. Maintenance infusions of ipilimumab were not givenafterward.
ResultsAfter treatment with radiotherapy in combination with
ipilimumab, a posttreatment chest CT (November 2012) andPET/CT (January 2013) showed a dramatic treatment responseof the patient's known disease. Not only was an objectiveresponse detected in the radiotherapy field, but strikingresponses were also observed at distant sites (Fig. 2). Metabolicactivity seen previously at the irradiated site in the liverresolved. In addition, there was resolution of multiple nonir-radiated foci within the liver and skeleton. There was signif-icant decrease in themetabolic activity and size of the left lowerlobe nodule and the previously irradiated right upper lobenodule. However, a mixed metabolic response was seen in theright hilar adenopathy (increased SUV uptake from 4 to 5.4).
After treatment with ipilimumab and radiotherapy, therewas an increase in absolute lymphocyte counts (ALC) andabsolute eosinophil counts (AEC), two biomarkers associatedwith improved survival rates in ipilimumab-treated melanomapatients (Fig. 3A; refs. 20–22). An ALC � 1,000/mL of wholeblood (vs. ALC < 1,000/mL of whole blood) before the third
2010A B
H&E
CD8
CD8
Cel
ls/H
PF
Cel
ls/H
PF
Rat
io C
D8/
Fox
P3
Fox-P3
TIA-1
2013 200
150
100
50
0
200
150
100
50
0
2.5
2.0
1.5
1.0
0.5
0.0
2010 2013
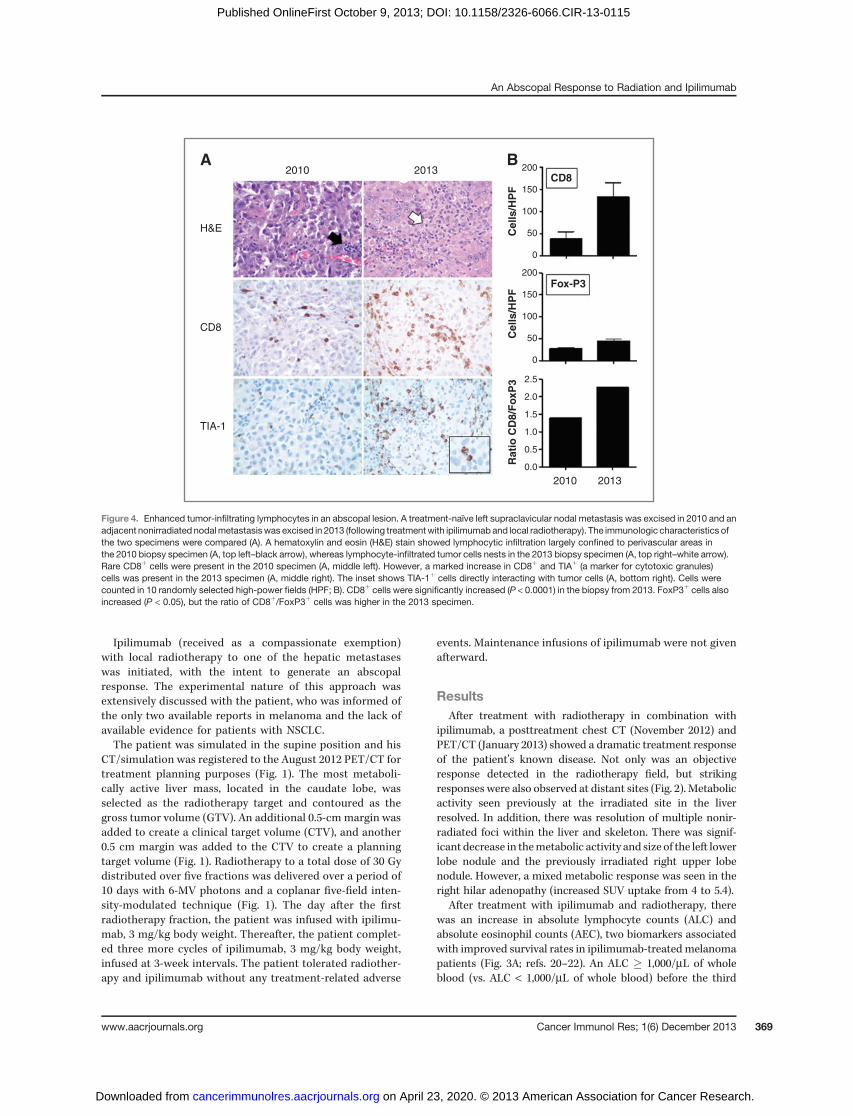
Figure 4. Enhanced tumor-infiltrating lymphocytes in an abscopal lesion. A treatment-naïve left supraclavicular nodal metastasis was excised in 2010 and anadjacent nonirradiated nodalmetastasiswas excised in 2013 (following treatmentwith ipilimumab and local radiotherapy). The immunologic characteristics ofthe two specimens were compared (A). A hematoxylin and eosin (H&E) stain showed lymphocytic infiltration largely confined to perivascular areas inthe 2010 biopsy specimen (A, top left–black arrow), whereas lymphocyte-infiltrated tumor cells nests in the 2013 biopsy specimen (A, top right–white arrow).Rare CD8þ cells were present in the 2010 specimen (A, middle left). However, a marked increase in CD8þ and TIAþ (a marker for cytotoxic granules)cells was present in the 2013 specimen (A, middle right). The inset shows TIA-1þ cells directly interacting with tumor cells (A, bottom right). Cells werecounted in 10 randomly selected high-power fields (HPF; B). CD8þ cells were significantly increased (P < 0.0001) in the biopsy from 2013. FoxP3þ cells alsoincreased (P < 0.05), but the ratio of CD8þ/FoxP3þ cells was higher in the 2013 specimen.
An Abscopal Response to Radiation and Ipilimumab
www.aacrjournals.org Cancer Immunol Res; 1(6) December 2013 369
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

infusion of ipilimumab, 10mg/kg body weight, in patients withchemotherapy-refractory melanoma predicted for higher 6-month (75% vs. 0%) and 12-month (47% vs. 0%) survival rates(20–22). Also, an AEC increase >100/mL of whole bloodbetween the first two ipilimumab infusions was associatedwith a longer median survival (11.3 months vs. 6.8 months;ref. 22).We observed that the ALC increased after radiotherapyand ipilimumab treatment (1,100/mL of whole blood at base-line, 2,700/mL of whole blood at peak levels, and 2,200/mL ofwhole blood before the third infusion of ipilimumab) andthat the AEC increased between the first two infusions ofipilimumab (200/mL of whole blood before the first infusionand 470/mL of whole blood before the second infusion ofipilimumab; Fig. 3A). In addition, the posttreatment carci-noembryonic antigen levels (a nonspecific tumor marker)showed a dramatic drop to normal levels after a peak of119.6 ng/mL (Fig. 3B).
Although the tumor markers remained at normal levels, aPET/CTonApril 2013 showed an isolated increase inmetabolicactivity of a newnonirradiated left supraclavicular lymphnode.The lymph node was excised and was found to have persistentdisease. However, to our surprise, this specimen exhibiteddistinct immunologic differences in comparison with thepreviously excised left supraclavicular lymph node from2010. Upon staining with hematoxylin and eosin, lymphocyticinfiltration was largely confined to perivascular areas in the2010 biopsy, whereas the biopsy from 2013 showed lymphocyteinfiltration into the tumor cell nests (Fig. 4A). On furtherimmunohistochemical analysis with CD8 (a marker for CTLs)and TIA-1 (a marker for cytotoxic granules) stains, the spec-imen from 2013 showed a marked increase in CD8þ and TIAþ
cells (Fig. 4A and B). In addition, FoxP3þ (a marker forregulatory T cells) was also increased in the 2013 specimen,although the ratio of CD8þ/FoxP3þ cells was much higher inthe 2013 specimen (Fig. 4B).
An increased ratio of effector to regulatory T cells fol-lowing anti-CTLA-4 treatment is a hallmark of successfultumor rejection (23). The persistence of tumor cells in thislesion suggests the possibility for the development of adap-tive resistance mediated by tumor cell upregulation ofligands inhibitory to T cells (14). Importantly, the detectedPET/CT signal in the excised lesion, although nonspecific,could be caused by both heightened antitumoral inflamma-tion and the proliferation of tumor cells, suggesting a needfor caution in the interpretation of such signals in patientsfollowing immunotherapy (13).
After excision of the newly hypermetabolic left supraclavi-cular lymph node, the patient underwent further systemictreatment with ipilimumab alone. From June 2013 to August2013, the patient received an additional four cycles of ipilimu-mab, 3 mg/kg given every 3 weeks. In September 2013, 1 yearafter treatment with concurrent radiotherapy and ipilimumab,the patient's newPET/CT showednoevidence of disease (Fig. 5).
DiscussionHistorically, abscopal responses are of rare occurrence.
Few cases have been reported in several tumor types,
including melanoma, renal cell carcinoma, and lymphoma(17, 18, 24–26). The remarkable abscopal response seen inthis patient after treatment with local radiotherapy andipilimumab is consistent with data in preclinical modelsthat this combination can induce therapeutically effectiveantitumor immune responses to poorly immunogenic car-cinomas (5, 8, 16). In the 4T1 mouse model, tumor-specificCD8þ T cells were responsible for tumor regression. Thesynergy between radiotherapy and anti-CTLA-4 antibodywas at least in part due to improved recruitment of theseeffector T cells to the tumor and their enhanced interactionwith tumor cells via NKG2D receptor engagement (16, 27).In addition, tumor-specific CD8þ T cells were expanded inmice treated with radiotherapy and anti-CTLA-4 antibody,consistent with the ability of radiotherapy to generate anin situ tumor vaccine (28).
Recently, an abscopal response was reported in a patientwith NY-ESO-1 (cancer-testis antigen)–positive melanomatreated with local radiotherapy in combination with ipili-mumab (17). The patient received ipilimumab at a dose of 10mg/kg body weight every 3 weeks, for a total of four doses, aspart of her induction therapy. Her follow-up CT scan showedoverall stable disease. Nevertheless, while on maintenanceipilimumab (given every 12 weeks), the patient showedradiographic evidence of disease progression. Specifically,there was growth of a paraspinal mass, causing her right-sided back pain. However, when local radiotherapy (28.5 Gyin three fractions over a period of 7 days) was administeredto the paraspinal metastasis, concurrently with maintenanceipilimumab, an abscopal response was detected 4 monthslater. Concurrent treatment led to the regression of distantdisease in the spleen and mediastinal lymph nodes.
Figure 5. PET image 1 year after treatment with concurrent radiotherapyand ipilimumab. A PET/CT was completed in September 2013. The PETimage is displayed and reveals no evidence of disease.
Golden et al.
Cancer Immunol Res; 1(6) December 2013 Cancer Immunology Research370
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

Interestingly, the therapeutic response temporarily correlat-ed with an increase in antibody titers targeting epitopes inthe central portion of NY-ESO-1 and other tumor-associatedantigens, an increase in CD4þ T-cell and myeloid lineageactivation, and a decline in the quantity of myeloid-derivedsuppressor cells.Herein, we report the first abscopal response seen 2.5
months after the start of treatment with ipilimumab andfractionated radiotherapy in a patient with chemotherapy-refractory metastatic adenocarcinoma of the lung. We trea-ted this patient with a radiotherapy dose and fractionationschedule similar to that used to convert tumor cells intoan in situ vaccine and generate an abscopal response inour preclinical model (5). Although CTLA-4 blockade as amonotherapy or given as a concurrent regimen with chemo-therapy did not lead to a benefit in PFS, the possibility thatipilimumab alone might be responsible for this patient'sresponse cannot be ruled out (12, 15). Nevertheless, this casereport supports the belief that a combination of localradiotherapy and immunotherapy might prove to be auseful strategy to improve the outcomes of some patientswith metastatic disease that are historically known to havedismal prognoses (3). In conclusion, this approach in NSCLC
and other types of cancer represents a new paradigm worthyof establishing clinical trials for patients with advanceddisease.
Disclosure of Potential Conflicts of InterestS.C. Formenti is a consultant/advisory board member for Bristol-Myers
Squibb. No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: E.B. Golden, A. Chachoua, S.C. FormentiDevelopment of methodology: E.B. Golden, P.B. Schiff, A. Chachoua, S.C.FormentiAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): E.B. Golden, S.C. FormentiAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): E.B. Golden, P.B. Schiff, S.C. FormentiWriting, review, and/or revision of themanuscript: E.B. Golden, S. Demaria,P.B. Schiff, A. Chachoua, S.C. FormentiAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): E.B. Golden, S.C. FormentiStudy supervision: S.C. Formenti
The costs of publication of this article were defrayed in part by the paymentof page charges. This article must therefore be hereby marked advertisementin accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received August 5, 2013; revised September 12, 2013; accepted September 23,2013; published OnlineFirst October 8, 2013.
References1. MoleRH.Wholebody irradiation; radiobiologyormedicine?Br JRadiol
1953;26:234–41.2. Formenti SC, Demaria S. Systemic effects of local radiotherapy.
Lancet Oncol 2009;10:718–26.3. Formenti SC, Demaria S. Combining radiotherapy and cancer immu-
notherapy: a paradigm shift. J Natl Cancer Inst 2013;105:256–65.4. Ma Y, Kepp O, Ghiringhelli F, Apetoh L, Aymeric L, Locher C, et al.
Chemotherapy and radiotherapy: cryptic anticancer vaccines. SeminImmunol 2010;22:113–24.
5. Dewan MZ, Galloway AE, Kawashima N, Dewyngaert JK, Babb JS,Formenti SC, et al. Fractionated but not single-dose radiotherapyinduces an immune-mediated abscopal effect when combined withanti-CTLA-4 antibody. Clin Cancer Res 2009;15:5379–88.
6. Demaria S, Ng B, Devitt ML, Babb JS, Kawashima N, Liebes L, et al.Ionizing radiation inhibition of distant untreated tumors (abscopaleffect) is immune mediated. Int J Radiat Oncol Biol Phys 2004;58:862–70.
7. Chakravarty PK, Alfieri A, Thomas EK, Beri V, Tanaka KE, Vikram B,et al. Flt3-ligand administration after radiation therapy prolongs sur-vival in a murine model of metastatic lung cancer. Cancer Res 1999;59:6028–32.
8. Demaria S, Kawashima N, Yang AM, Devitt ML, Babb JS, Allison JP,et al. Immune-mediated inhibition of metastases after treatment withlocal radiation and CTLA-4 blockade in a mouse model of breastcancer. Clin Cancer Res 2005;11:728–34.
9. Pardoll DM. The blockade of immune checkpoints in cancer immu-notherapy. Nat Rev Cancer 2012;12:252–64.
10. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, HaanenJB, et al. Improved survival with ipilimumab in patients with metastaticmelanoma. N Engl J Med 2010;363:711–23.
11. Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, et al.Ipilimumab plus dacarbazine for previously untreated metastatic mel-anoma. N Engl J Med 2011;364:2517–26.
12. Lynch TJ, Bondarenko I, Luft A, Serwatowski P, Barlesi F, Chacko R,et al. Ipilimumab in combinationwith paclitaxel and carboplatin as first-line treatment in stage IIIB/IV non-small-cell lung cancer: results from arandomized, double-blind, multicenter phase II study. J Clin Oncol2012;30:2046–54.
13. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbe C, et al.Guidelines for the evaluation of immune therapy activity in solidtumors: immune-related response criteria. Clin Cancer Res 2009;15:7412–20.
14. Brahmer JR,Pardoll DM. Immune checkpoint inhibitors:making immu-notherapy a reality for the treatment of lung cancer. Cancer ImmunolRes 2013;1:85–91.
15. Zatloukal P, Heo DS, Park K, Kang J, Butts C, Bradford D, et al.Randomized phase II clinical trial comparing tremelimumab (CP-675,206) with best supportive care (BSC) following first-line plati-num-based therapy in patients (pts) with advanced non–small celllung cancer (NSCLC). J Clin Oncol 27:15s, 2009 (suppl; abstr 8071).
16. Ruocco MG, Pilones KA, Kawashima N, Cammer M, Huang J, BabbJS, et al. Suppressing T cell motility induced by anti-CTLA-4 mono-therapy improves antitumor effects. J Clin Invest 2012;122:3718–30.
17. Postow MA, Callahan MK, Barker CA, Yamada Y, Yuan J, Kitano S,et al. Immunologic correlates of the abscopal effect in a patient withmelanoma. N Engl J Med 2012;366:925–31.
18. Stamell EF, Wolchok JD, Gnjatic S, Lee NY, Brownell I. The abscopaleffect associated with a systemic anti-melanoma immune response.Int J Radiat Oncol Biol Phys 2013;85:293–5.
19. Edge SBAmerican Joint Committee on Cancer. AJCC cancer stagingmanual. 7th ed. New York, London: Springer; 2010.
20. Ku GY, Yuan J, Page DB, Schroeder SE, Panageas KS, Carvajal RD,et al. Single-institution experience with ipilimumab in advanced mel-anoma patients in the compassionate use setting: lymphocyte countafter 2 doses correlates with survival. Cancer 2010;116:1767–75.
21. Callahan MK, Wolchok JD, Allison JP. Anti-CTLA-4 antibody therapy:immune monitoring during clinical development of a novel immuno-therapy. Semin Oncol 2010;37:473–84.
22. Delyon J, Mateus C, Lefeuvre D, Lanoy E, Zitvogel L, Chaput N, et al.Experience in daily practice with ipilimumab for the treatment ofpatients with metastatic melanoma: an early increase in lymphocyteand eosinophil counts is associatedwith improved survival. AnnOncol2013;24:1697–703.
23. Quezada SA, Peggs KS, Curran MA, Allison JP. CTLA4 blockade andGM-CSF combination immunotherapy alters the intratumor balance ofeffector and regulatory T cells. J Clin Invest 2006;116:1935–45.
An Abscopal Response to Radiation and Ipilimumab
www.aacrjournals.org Cancer Immunol Res; 1(6) December 2013 371
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

24. Robin HI, AuBuchon J, Varanasi VR, Weinstein AB. The abscopaleffect: demonstration in lymphomatous involvement of kidneys. MedPediatr Oncol 1981;9:473–6.
25. Wersall PJ, Blomgren H, Pisa P, Lax I, Kalkner KM, Svedman C.Regression of non-irradiated metastases after extracranial stereotac-tic radiotherapy in metastatic renal cell carcinoma. Acta Oncol 2006;45:493–7.
26. Sullivan RJ, Lawrence DP, Wargo JA, Oh KS, Gonzalez RG, Piris A.Case records of the Massachusetts General Hospital. Case 21-2013.
A 68-year-old man with metastatic melanoma. N Engl J Med 2013;369:173–83.
27. Matsumura S, Wang B, Kawashima N, Braunstein S, Badura M,Cameron TO, et al. Radiation-induced CXCL16 release by breastcancer cells attracts effector T cells. J Immunol 2008;181:3099–107.
28. Pilones KA, Kawashima N, Yang AM, Babb JS, Formenti SC, DemariaS. Invariant natural killer T cells regulate breast cancer response toradiation and CTLA-4 blockade. Clin Cancer Res 2009;15:597–606.
Golden et al.
Cancer Immunol Res; 1(6) December 2013 Cancer Immunology Research372
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115

2013;1:365-372. Published OnlineFirst October 9, 2013.Cancer Immunol Res Encouse B. Golden, Sandra Demaria, Peter B. Schiff, et al.
Small Cell Lung Cancer−with Metastatic Non An Abscopal Response to Radiation and Ipilimumab in a Patient
Updated version
10.1158/2326-6066.CIR-13-0115doi:
Access the most recent version of this article at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/1/6/365.full#ref-list-1
This article cites 26 articles, 9 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/1/6/365.full#related-urls
This article has been cited by 44 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/1/6/365To request permission to re-use all or part of this article, use this link
on April 23, 2020. © 2013 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst October 9, 2013; DOI: 10.1158/2326-6066.CIR-13-0115
Related Documents











