Amy Killelea, NASTAD North Dakota 2014 HIV/STD/TB/Viral Hepatitis Symposium September 18, 2014 ACA and Public Health: Successes, Challenges, and Priorities Moving Forward

Amy Killelea, NASTAD North Dakota 2014 HIV/STD/TB/Viral Hepatitis Symposium September 18, 2014
Jan 01, 2016
ACA and Public Health: Successes, Challenges, and Priorities Moving Forward. Amy Killelea, NASTAD North Dakota 2014 HIV/STD/TB/Viral Hepatitis Symposium September 18, 2014. Presentation Overview. Part 1: ACA Opportunities: Where We Are and Where We’re Going - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Amy Killelea, NASTADNorth Dakota 2014 HIV/STD/TB/Viral Hepatitis Symposium
September 18, 2014
ACA and Public Health: Successes, Challenges, and Priorities
Moving Forward
Presentation Overview
Part 1: ACA Opportunities: Where We Are and Where We’re Going
Part 2: Implementation in Action:• Preparing for outreach and enrollment into new
ACA coverage options• Assessing and filling coverage gaps• Assessing and filling affordability gaps• Preparing providers for a changing health care
landscape
Questions/Discussion

About NASTAD
NASTAD is an international non-profit 501(c)(3) association of U.S. state health department AIDS directors who administer HIV/AIDS and viral hepatitis programs funded by U.S. state and federal governments
NASTAD was established in 1992 as the voice of the states
NASTAD is governed by a 20 member, elected Executive Committee (EC) charged with making policy and program decisions on behalf of the full membership
NASTAD has a Washington, DC headquarters and field offices/programs in Bahamas, Botswana, Ethiopia, Haiti, Mozambique, South Africa, Trinidad, Uganda and Zambia

Part 1ACA Opportunities: Where We Are and
Where We’re Going

ACA: Three Prongs
Public insurance reforms
Private insurance reforms
Health infrastructure
reforms
• Medicaid expansion
• Medicare Part D reforms
• Marketplaces• Prohibitions on
discriminatory insurance practices
• Investments in community health centers, health workforce, coordinated care, and prevention

ACA Insurance Expansions
ChildrenPregnant women
Working parents
Jobless parents
DisabledChildless adults
0%
50%
100%
150%
200%
250%
300%
350%
400%
Federal Poverty Level (FPL)
Current Medicaid/CHIP Eligibility
ChildrenPregnant women
Working parents
Jobless parents
DisabledChildless adults
0%
50%
100%
150%
200%
250%
300%
350%
400%
Medicaid Expansion 138% FPL
ChildrenPregnant women
Working parents
Jobless parents
DisabledChildless adults
0%
50%
100%
150%
200%
250%
300%
350%
400%
Medicaid Expansion 138% FPL
Subsidies for private insurance400% FPL
66% of Ryan White Clients had income below 100% FPL (in 2011)

Where States Stand on Medicaid Expansion
Source: Kaiser Family Foundation, August 28, 2014
Part 2: Implementation In Action

ACA and Public Health ProgramsYear One: Redux
Pu
blic
Healt
h P
rogra
ms Client transition and enrollment
Coverage gaps
Affordability gaps
Coordination & integration of public health providers and services with
broader health systems
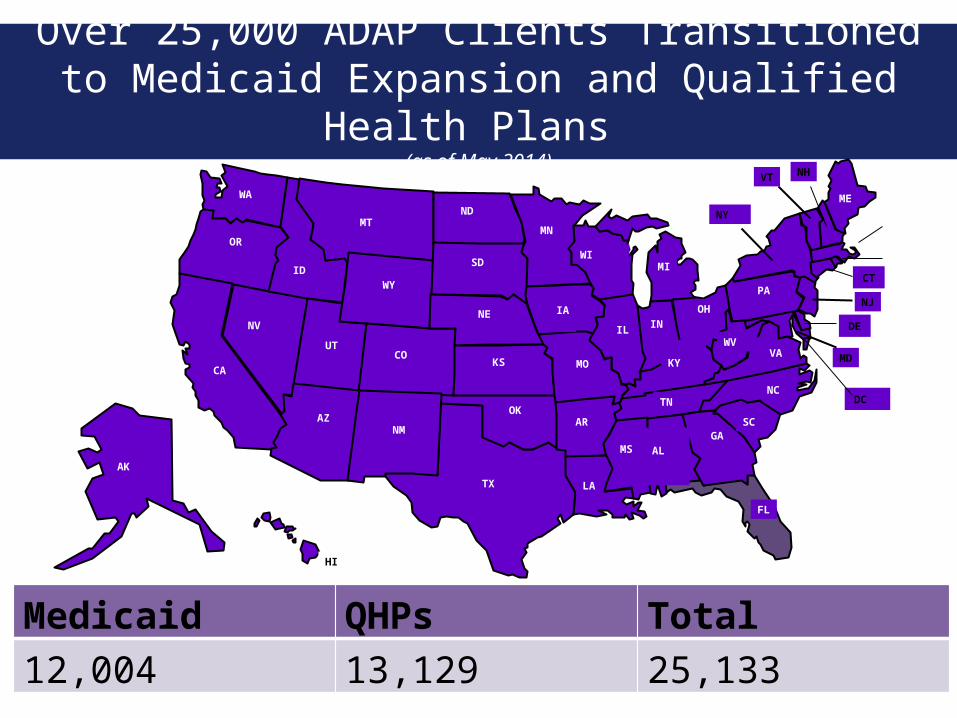
Over 25,000 ADAP Clients Transitioned to Medicaid Expansion and Qualified Health Plans
(as of May 2014)
AL
ARGA
ID
IL IN
KY MO
MT
NV
NH
OH
SC
SD
TX
VA
WY
OK
ME
MD
NJ
NY
OR
AK
CO
LA
UT
CAKS
MS
FL
HI
NMAZ
ND
MN
IA
WIMI
NE
WA
PA
NCTN
WV
VT
DE
CT
DC
Medicaid QHPs Total12,004 13,129 25,133

ACA Outreach and Enrollment Programs and Resources
Consumer outreach
and enrollment
Patient Navigator Program
Insurance Assisters
Certified Application Counselors Community
Health Centers
Enroll America
HIV/AIDS Care Programs and Providers
HIV
Pre
venti
on P
rogr
ams
?

Coordinating Enrollment to Ensure No Disruptions in Care
Open Enrollment for Marketplace Coverage
Open enrollment (October 1st through March 31st in first year) and limited special enrollmentBased on MAGIDates matter! Coverage effective date depends on when you apply and payment of premium
ADAP Application and Recertification
Continuous enrollment6 month recertificationBased on MAGI?
Medicaid
Continuous enrollment Based on MAGI (for new expansion group)
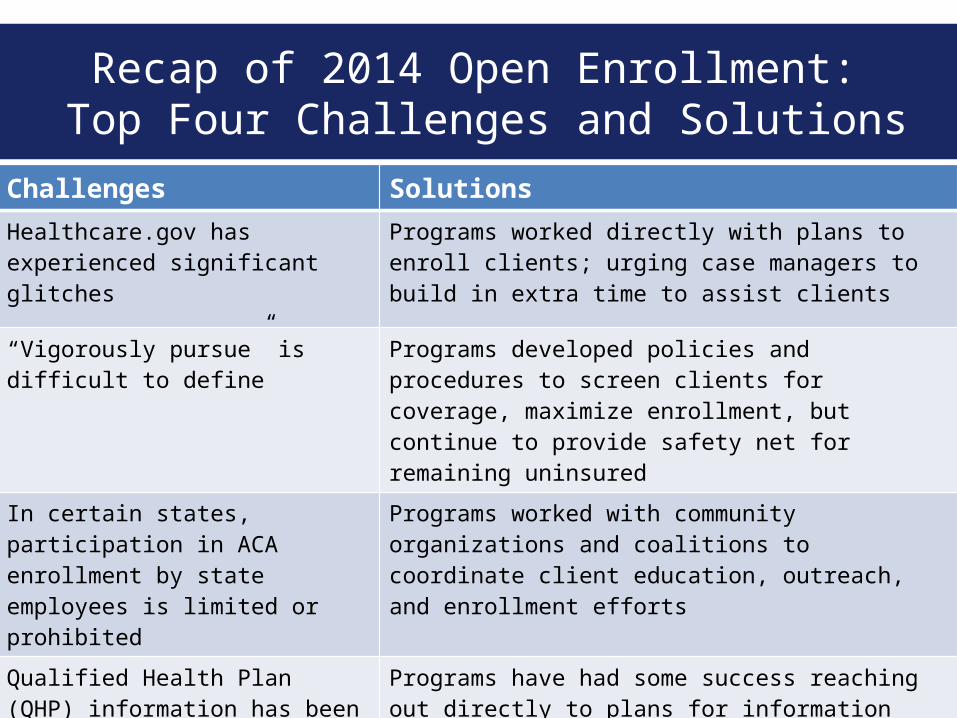
Challenges Solutions
Healthcare.gov has experienced significant glitches
Programs worked directly with plans to enroll clients; urging case managers to build in extra time to assist clients
“Vigorously pursue” is difficult to define
Programs developed policies and procedures to screen clients for coverage, maximize enrollment, but continue to provide safety net for remaining uninsured
In certain states, participation in ACA enrollment by state employees is limited or prohibited
Programs worked with community organizations and coalitions to coordinate client education, outreach, and enrollment efforts
Qualified Health Plan (QHP) information has been incomplete or unavailable
Programs have had some success reaching out directly to plans for information
Recap of 2014 Open Enrollment: Top Four Challenges and Solutions

New Coverage Opportunities
Plans must cover 10 Essential Health Benefits (EHB) Scope of coverage will vary – but clients and providers
should look for THREE things:– Does the provider network include HIV providers?– Does the formulary include client’s treatment
regimen?– How much does the plan cost?
Preventive and wellness
services
Laboratory services
Ambulatory services
Prescription drugs
Maternity and newborn care
Emergency services
Rehabilitative and habilitative
services
Mental health and substance use
disorder services
Pediatric services
Hospitalization
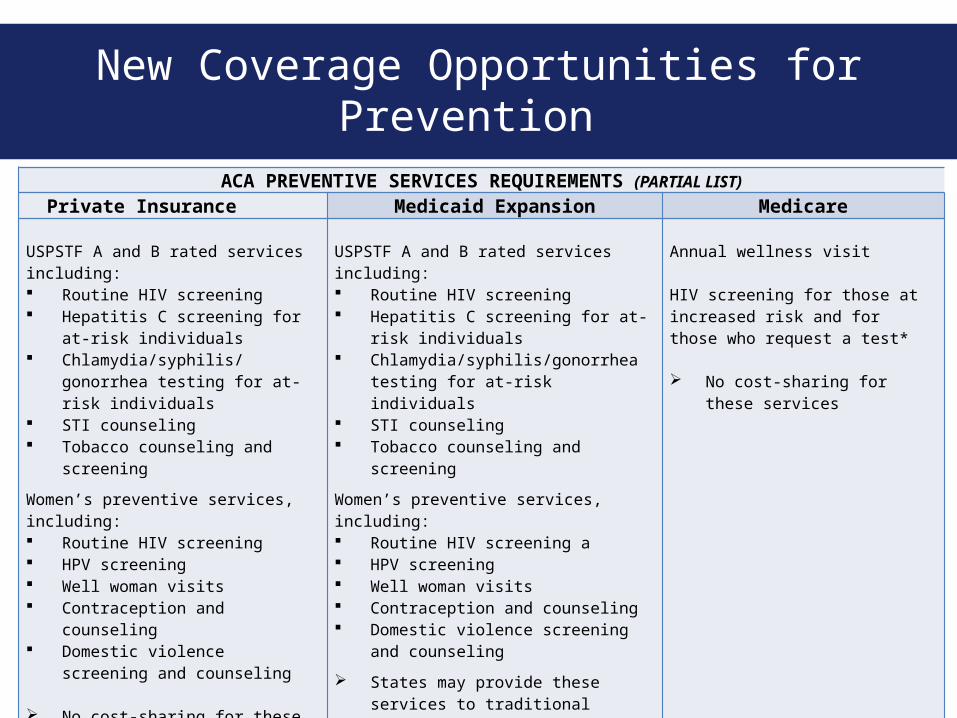
New Coverage Opportunities for Prevention
ACA PREVENTIVE SERVICES REQUIREMENTS (PARTIAL LIST)
Private Insurance Medicaid Expansion Medicare USPSTF A and B rated services including: Routine HIV screening Hepatitis C screening for at-risk
individuals Chlamydia/syphilis/gonorrhea
testing for at-risk individuals STI counseling Tobacco counseling and
screening
Women’s preventive services, including: Routine HIV screening HPV screening Well woman visits Contraception and counseling Domestic violence screening
and counseling No cost-sharing for these
services
USPSTF A and B rated services including: Routine HIV screening Hepatitis C screening for at-risk
individuals Chlamydia/syphilis/gonorrhea
testing for at-risk individuals STI counseling Tobacco counseling and screening
Women’s preventive services, including: Routine HIV screening a HPV screening Well woman visits Contraception and counseling Domestic violence screening and
counseling
States may provide these services to traditional Medicaid beneficiaries and will get increased federal funding if they do so
Annual wellness visit HIV screening for those at increased risk and for those who request a test* No cost-sharing for these
services
* CMS is in process of issuing new coverage determinations adopting USPSTF revised recommendations for Medicare.

Coordination Across Payers:Translating Coverage into Care and Treatment
SERVICE QHP MEDICAID RW/ ADAP/CDC
HIV Testing Continue to cover in certain settings
RX Cost-sharing assistance
MEDICAL CASE MANAGEMENT
ORAL HEALTH
LABS Cost-sharing assistance
MENTAL HEALTH SERVICES
Cost-sharing assistance
SUBSTANCE ABUSE TREATMENT
Cost-sharing assistance
HIV PRIMARY CARE Cost-sharing assistance
MEDICAL TRANSPORTATION Limited Coverage
INPATIENT HOSPITAL SERVICES
Adapted from West Virginia Ryan White Part B Program

Example: Case Management Coverage
Private Insurance Benchmark Plan
Ryan White Program Medicaid
Case managementPeriodic phone calls to discuss appointments and assist in finding services.
Medical case management Coordination and follow-up of medical treatments, ongoing assessment of the client’s and other key family members’ needs and personal support systems, development of a service plan, coordination of services, provision of treatment adherence counseling to ensure readiness for, and adherence to HIV/AIDS treatments.
Non-medical case management Includes provision of advice and assistance in obtaining medical, social, community, legal, financial, and other needed services (does not include coordination and follow-up of medical treatments).
Targeted case managementOptional benefit that allows states to provide a range of care coordination and support services to eligible beneficiaries. Eligibility criteria typically require high level of need.
Medicaid Health Home ProgramNew option that allows states to provide a range of care coordination services (including care management, patient and family support, referral to community and social support services, and use of health information technology to link services) to high-need Medicaid beneficiaries with chronic conditions (including HIV).

Significant Coverage Gap: Prescription Drug Formulary
EHB Standard = same number of drugs per U.S. Pharmacopeia (USP) category/class as state’s benchmark plan
USP Category
USPClass
Anti-viral NRTIs
NNRTIs
Protease inhibitors
Anti-Cytomegalovirus (CMV) agents
Anti-hepatitis agents
Other
Missing from USP classification system = combination therapies

Assessing Qualified Health Plan (QHP) Metal Tiers
QHP Metal Tiers
What It Means
Bronze Plan pays 60% of costs (on average)/enrollee pays 40%
Silver Plan pays 70% of costs (on average)/enrollee pays 30%
Gold Plan pays 80% of costs (on average)/enrollee pays 20%
Platinum Plan pays 90% of costs (on average)/enrollee pays 10%
Lower premiums, but less generous
Higher premiums, but more generous
Clients must enroll in a silver level plan to get cost-sharing reductions
Premium tax credits to help offset cost of Qualified Health Plan premiums available for people with income up to 400% FPL
Cost-sharing reductions to reduce out-of-pocket costs available for people with income up to 250% FPL
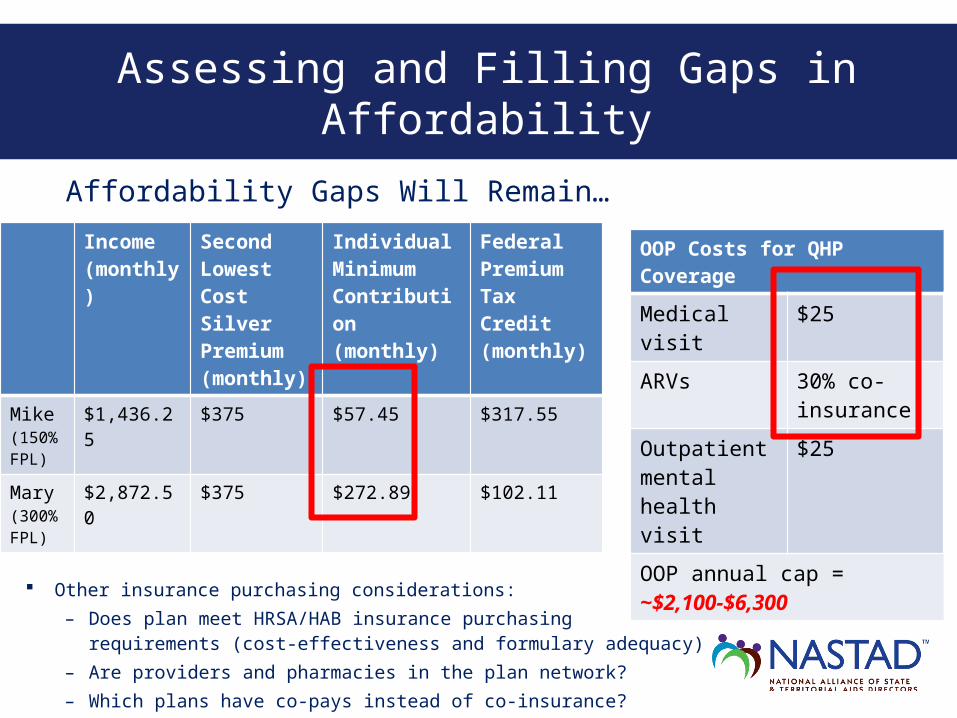
Assessing and Filling Gaps in Affordability
Affordability Gaps Will Remain…
OOP Costs for QHP Coverage
Medical visit $25
ARVs 30% co-insurance
Outpatient mental health visit
$25
OOP annual cap = ~$2,100-$6,300
Income (monthly)
Second Lowest Cost Silver Premium (monthly)
Individual Minimum Contribution (monthly)
Federal Premium Tax Credit (monthly)
Mike(150% FPL)
$1,436.25 $375 $57.45 $317.55
Mary(300% FPL)
$2,872.50 $375 $272.89 $102.11
Other insurance purchasing considerations:– Does plan meet HRSA/HAB insurance purchasing
requirements (cost-effectiveness and formulary adequacy)
– Are providers and pharmacies in the plan network?– Which plans have co-pays instead of co-insurance?

ADAP purchasing QHPs (premiums, Rx co-pays, or deductibles)
ADAP piloting QHP purchase
ADAP not currently purchasing QHPs (most are planning)
AL
ARGA
ID
IL IN
KY MO
MT
NV
NH
OH
SC
SD
TX
VA
WY
OK
ME
MD
NJ
NY
OR
AK
CO
LA
UT
CAKS
MS
FL
HI
NMAZ
ND
MN
IA
WIMI
NE
WA
PA
NCTN
WV
VT
MA
RI
DE
CT
DC
ADAP/Part B Programs Currently Purchasing Qualified Health Plans (QHPs) for Clients (June 2014)

Even after full ACA implementation, there will be populations left out of reform:– Low-income individuals in states that do not
expand Medicaid– Undocumented populations– Hard-to-reach “eligible but not enrolled”
populations
Assessing the Gaps: Planning for Public Health Safety Net
HRSA/HAB ACA Policies
HRSA encourages state ADAP/Part B Programs to use their Ryan White funding to help clients access insurance, as long as:– Formulary includes at least one drug in each class of core ARVs
from the HHS Clinical Guidelines– It is cost-effective in aggregate as compared to purchasing
medications Other Ryan White Program grantees may also use their funds to
help clients with the cost of insurance The Ryan White Program is the payer of last resort and grantees
must “vigorously pursue” client eligibility for public and private insurance– Grantees may not dis-enroll clients from services for failure to
enroll in public or private insurance coverage Ryan White Program funds may be used to cover services not
covered or inadequately covered by public and private insurance

Preparing Providers for Health Reform
Local preparation for health reform
Relationship w/safety net
providers
Preparation for insured clients (e.g., billing)
Preparation to provide vital enabling services
not covered by ACA insurance expansion
Strategic planning to
negotiate new health care landscape

Leveraging New Resources/Payers: It’s Complicated!
Service covered?
Provider in network and credentialed with payer?
Does reimbursement
cover cost of service?
What is impact on
client/patient?
Translate public health service into language of payers/insurance (e.g., CPT codes)
Assess provider requirements (licensed provider; provider supervision; provider recommendation; setting)
Compare reimbursement rate (within capitation or FFS) with cost of providing service
Are privacy and confidentiality concerns addressed?
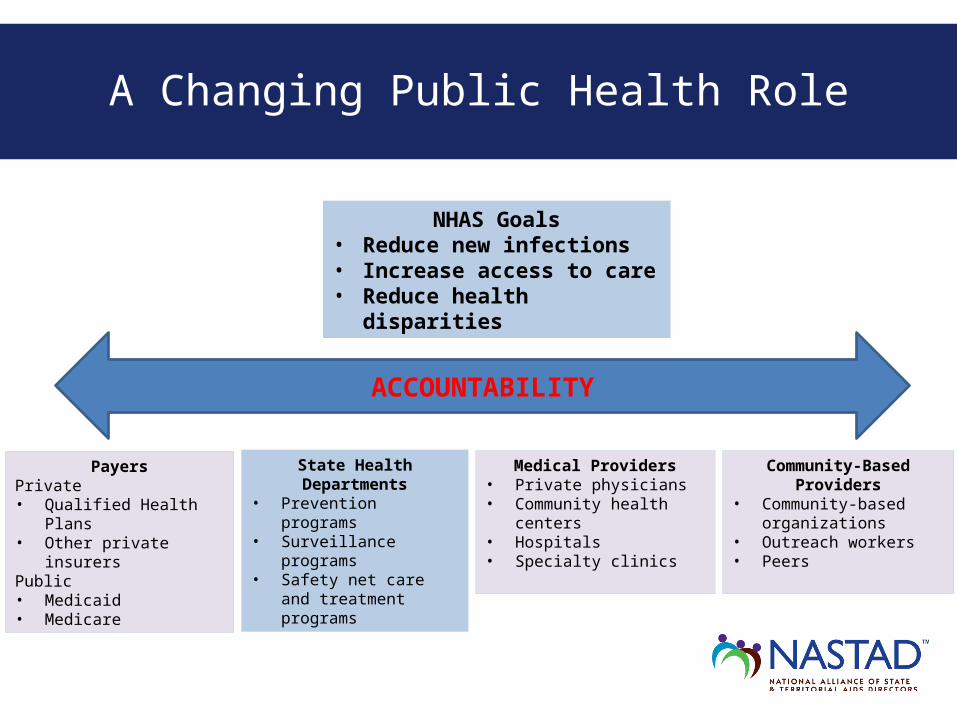
A Changing Public Health Role
NHAS Goals• Reduce new infections• Increase access to care• Reduce health
disparities
ACCOUNTABILITY
PayersPrivate• Qualified Health Plans• Other private insurersPublic• Medicaid• Medicare
Medical Providers• Private physicians• Community health
centers• Hospitals • Specialty clinics
Community-Based Providers
• Community-based organizations
• Outreach workers• Peers
State Health Departments
• Prevention programs• Surveillance
programs• Safety net care and
treatment programs

Questions

Resources
National Alliance of State & Territorial AIDS Directors (NASTAD), www.NASTAD.org – Amy Killelea, [email protected]
HIV Health Reform, http://www.hivhealthreform.org/ Treatment Access Expansion Project, www.taepusa.org HIV Medicine Association, www.hivma.org Health Care Reform Resources
– State Refo(ru)m, www.statereforum.org– Kaiser Family Foundation, www.kff.org – Healthcare.gov, www.healthcare.gov
Related Documents