
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript



Contents Abbreviations
Chapter-1: Background & Context ................................................................................ 1
1.1. Context ................................................................................................................... 1
1.1.1. Health and Institutional Context ............................................................................. 1
1.1.2. Capacity Development & Training Strategy .......................................................... 2
1.1.3. Rationale for Capacity Development & Training Strategy ....................................... 3
1.2. Objectives and Scope of Work for the Assignment ................................................. 3
1.3. Methodology of Development of Capacity Building & Training Strategy ................ 4
1.3.1. Steps for Development of CB&T Strategy ................................................................ 4
1.4. Gap Analysis and Capacity Needs Assessment ........................................................ 5
1.4.1. Overview of the Capacity Assessment ..................................................................... 6
1.4.2. Coverage and Stakeholder Analysis of the Capacity Needs Assessment ................. 6
1.4.3. Capacity Axis and Capacity Areas Covered .............................................................. 8
1.5. Gap Analyses of Competency of Health Staff .......................................................... 9
1.5.1 Competencies in Gaps ............................................................................................. 9
1.5.2 Desired Competencies and Gaps in Competencies of every Stakeholder ............... 10
1.6 Review of Existing Trainings .................................................................................... 22
1.6.1 Stakeholder-wise Trainings ...................................................................................... 22 1.6.2 General Trainings ..................................................................................................... 25 Chapter-2 : Capacity Building & Training Strategy .......................................................... 27
2.1. Guiding Principles for the Capacity Building & Training Strategy ............................ 27
2.2. Strategic Framework for Systems Strengthening .................................................... 28
2.3. Target Trainees ........................................................................................................ 30
2.4. Capacity Building and Training Objectives ............................................................... 32
2.5. Capacity Building and Training Activities ................................................................ 41
2.5.1. Capacity Priority Areas ............................................................................................ 41
2.6. Modes of Training Delivery ...................................................................................... 51
2.7. Target Group-wise Trainings .................................................................................... 54
2.7.1. Developing competencies for Core Competencies .................................................. 55
2.7.2. Developing competencies for Specialized Competencies ....................................... 59

Chapter-3: Capacity Building & Training Plan ................................................................. 60
3.1. Individual Capacity Development Plan .................................................................... 60
3.2. Capacity Development: Organisational/Support System Strengthening ................. 63
3.3. Enabling Environment Development Plan ............................................................... 64
3.4. Human Resource Management & Institutional Roles and Responsibilities ............. 66
3.5. Quality Assurance and Training Management ........................................................ 68
3.5.1 Pre-Training Activities ............................................................................................. 68
3.5.2 During Training Activities ......................................................................................... 69
3.5.3 Post-Training Activities ............................................................................................ 69
3.5.4 Quality Assurance Committee (QAC) ....................................................................... 70
3.5.5 Budgetary Considerations ....................................................................................... 70
Chapter-4: Monitoring & Evaluation Framework .......................................................... 71
4.1. Introduction & Rationale for M&E ........................................................................... 71
4.2. Objectives of M&E Framework ................................................................................ 72
4.3. Target Users of M&E Framework ........................................................................... 72
4.4. Guidelines for M&E framework ............................................................................... 73
4.5. Key Evaluation Questions & Logframe .................................................................... 74
4.6. Methodology and Work Plan ................................................................................... 77
4.7. M&E Operationalization Plan .................................................................................. 79
4.8 Human Resources for CB&T M&E ............................................................................ 80
4.9 Activity Timeline ...................................................................................................... 82
Annexure: Annexure-I: District-Wise Distribution of Health Facilities .............................................. 84
Annexure-II: Year-wise Budget Details ............................................................................. 87
Annexure–III: RCH-II Training ............................................................................................ 96
Annexure-IV: Suggested Training Venues .......................................................................... 112
Annexure-V: State Institute of Health & Family Welfare Indra Nagar, Lucknow .............. 113
Annexure VI: Stakeholder-Wise & Training Wise Budget .................................................. 117

Contents: List of Tables Chapter-1: Background & Context ................................................................................ 1
Table 1.1: Comparative health indicators of India and Uttarakhand ................................ 1
Table: 1.2: Stakeholder Analysis ........................................................................................ 7
Table 1.3: Capacity areas Identified for Assessment ........................................................ 9
Table 1.4: Capacity areas for Medical Officers Cadres ...................................................... 10
Table 1.5: Capacity areas for the PARAMEDICALS – Pharmacists ..................................... 12
Table 1.6: Capacity areas for Medical Technicians ........................................................... 13
Table 1.7: Capacity areas for Nurses ................................................................................. 15
Table 1.8: Capacity areas for Outreach Workers - Frontline Health Workers (FLWs) ....... 16
Table 1.9: Capacity areas for OUTREACH WORKERS- ASHAs ............................................ 18
Table 1.10: Capacity areas for GDAs ................................................................................... 20
Table 1.11: Trainings provided to Medical Officers in the last 2 financial years ................. 22
Table 1.12: Trainings provided to Nurses in the last 2 financial years ................................ 23
Table 1.13: Trainings provided to Nurses in the last 2 financial years ................................ 24
Table 1.14: Training duration for different stakeholder categories .................................... 26 Chapter-2: Capacity Building & Training Strategy .......................................................... 27
Table 2.1: CB&T objectives for the Stakeholders .............................................................. 33
Table 2.2: Priority Core Competencies for Staff ................................................................ 42
Table 2.3: Capacity development plan: Priority Activities ................................................ 49
Table 2.4: Suggested Training Types for Different Capacity Aspects ................................ 54
Table 2.5a: Project Management-Strategic and Coordinated Planning, Monitoring, Reporting, HR management ............................................................................. 55
Table 2.5b: Communication, and Liasoning Skills ............................................................... 55
Table 2.5c: Leadership, Motivation and Teamwork Skills ................................................... 56
Table 2.5d: Medico-Legal Practices .................................................................................... 57
Table 2.5e: Biomedical Waste Management & Infection Control ...................................... 57
Table 2.5f: Quality Assurance ............................................................................................ 58
Table 2.5g: Disaster Preparedness & Response .................................................................. 58

Table 2.5h: Finance and Budgeting ..................................................................................... 59 Chapter-3: Capacity Building & Training Plan ................................................................. 60
Table 3.1: Proposed Training duration for different stakeholder categories .................... 60
Table 3.2: Core competency Trainings .............................................................................. 61
Table 3.3: Capacity development Initiatives at the Organisational Level ......................... 63
Table 3.4: Capacity development Initiatives to Strengthen Enabling Environment .......... 65
Table 3.5: Human Resource Management in Capacity Development & Training of Health Staff of Uttarakhand Health Department ......................................................... 66
Table 3.6 : Tentative Budget for Trainings ....................................................................... 70 Chapter-4: Monitoring & Evaluation Framework .......................................................... 71
Table 4.1: Logframe for CB&T interventions ..................................................................... 74
Table 4.2: Modalities of Reporting and Data Collection Monitoring ................................ 77
Table 4.3: Framework for Developing Operationalization Plan of CB&T M&IE Framework in the state. .......................................................................................................... 80
Table 4.4: Details of Human Resource and their responsibilities ..................................... 80

Abbreviations
ANM - Auxiliary Nurse Midwife
ASHA - Accredited Social Health Activist
AWW - Anganwadi Worker CHC Community Health Centre
CNAA - Community Need Assessment Approach
DMO - District Medical Officer
DPM - District Programme Manager
DTO - District Tuberculosis Officer
EmOC - Emergency Obstetric Care
FP - Family Planning
FRU - First Referral Unit
IDSP - Integrated Disease Surveillance Programme
IEC - Information, Education and Communication
IMNCI - Integrated Management of Neonatal and Childhood Illnesses
IMR - Infant Mortality Rate
IUCD - Intra Uterine Contraceptive Device
LBW - Low Birth Weight
LHV - Lady Health Visitor
LT - Laboratory Technician
MH - Maternal Health
MMR - Maternal Mortality Ratio
MO - Medical Officer
MOHFW - Ministry of Health and Family Welfare
MWCD - Ministry of Women and Child Development
NDCP - National Disease Control Programme
NGO - Non-Governmental Organisation

NICD - National Institute of Communicable Diseases
NIHFW - National Institute of Health and Family Welfare
NLEP - National Leprosy Elimination Programme
NPCB - National Programme for Control of Blindness
NRHM - National Rural Health Mission
NVBDCP - National Vector Borne Disease Control Programme
PHC - Primary Health Centre
PIP - Programme Implementation Plan
PMU - Programme Management Unit
PRI - Panchayati Raj Institution
QAC - Quality Assurance Committee
RCH - Reproductive Child Health
RKS - Rogi Kalyan Samiti
RNTCP - Revised National Tuberculosis Control Programme
RTI/STIs - Reproductive Tract Infections/Sexually Transmitted Infections
SBA - Skilled Birth Attendant
SC - Sub-Centre
SIHFW - State Institute of Health and Family Welfare
SHP - State Health Programme
SPM - State Programme Manager
SRS - Sample Registration System
STLS - State Tuberculosis Laboratory Supervisor
STS - Senior Treatment Supervisor
TOT - Training of Trainers
VHND - Village Health and Nutrition Day

Capacity Building & Training Strategy 1
Background & Context
“Most performance problems can be attributed to unclear expectations, skills deficit, resource or equipment shortages or a lack of motivation.”
- Hughes et al., 2002 -
1.1. Context
1.1.1. Health and Institutional Context
The shortage of trained professionals owing to the challenging terrain of the state, the out-of-reach healthcare facilities and transportation facilities have been persistent challenges in the systematic health care delivery and access in Uttarakhand. Limited service availability had consequently negatively influenced health seeking behavior due to availability, access, cost and quality constraints.
At the same time, the state is witnessing a trend of burgeoning burden of Non-Communicable Diseases (NCDs) as evidenced in the Table 1.1 below, while the status of maternal, neonatal and child care shows only marginal improvement in the state. This is evidence of a dire need for enhancing health care access and improving its delivery.
Table 1.1 : Comparative health indicators of India and Uttarakhand Indicator Status of Health Indicators
(India) Status of Health Indicators
(Uttarakhand)
Infant Mortality Rate 41/1000 (Total,NFHS-4) 57/1000 (Total,NFHS-3)
40/1000 (Total,NFHS-4) 42/1000 (Total,NFHS-3)
Complete Immunization 61.3% (NFHS 4) 58.2% (NFHS 4)
Maternal Mortality Ratio
122/1,00,000 live birth (SRS-2015-17)
167/1,00,000 live birth (SRS-2011-13)
89/1,00,000 live birth (SRS-2015-17)
165/1,00,000 live birth (AHS-2012-13)
Institutional Births 75.1 (Rural, NFHS 4)
63.7 (Rural, NFHS 4)
Men with Slightly above normal Blood Pressure (Systolic 140-159 mm of Hg and/or Diastolic 90-99 mm of Hg) (%)
10.3 (Total, NFHS 4) 9.7 ( Rural, NFHS 4)
7.2 (Total, NFHS 4) 6.7 ( Rural, NFHS 4)
Men with high blood sugar level(>140
mg/dl) (%)
7.9 (Total, NFHS 4) 7.4 (Rural, NFHS 4)
8.8 (Total, NFHS 4) 8.2 (Rural, NFHS 4)
Source: National Family & Health Survey-4; Annual Health Survey, 2012-13; Sample Registration System (SRS), 2015-17
It is against this context that the World Bank is supporting the Uttarakhand Health Systems Development Project (UKHSDP) to improve access to quality health services, particularly in the hilly districts of the state, and to expand health financial risk protection for the residents of Uttarakhand. The project is characterized by two components as described below:
1
Capacity Building & Training Strategy 2
As described above, Component II of the UKHSDP strives to strengthen the capacity of the state machinery to provide effective stewardship to improve the quality of services in the entire health system. To assist in these efforts, it was deemed necessary to plan for system strengthening through a comprehensive capacity development and training of the Department of Health & Family Welfare, GoUK which will strengthen the state institutions and health actors, thus ultimately improve health care access, delivery, utilization of health services and thereby health outcomes.
1.1.2. Capacity Development & Training Strategy
Research shows that Uttarakhand is one of the many states in the country where less than 50% of the required staff is available to serve rural populations, while at times care is provided by non-qualified staff (WHO, 2006). This situation seriously compromises the health status of the communities, as poor performance of service providers leads to inaccessibility of care and sub-optimum quality of care, which contribute to reduced health outcomes as people may not use services or may not receive optimal care. This sub-optimal performance may be attributed to inadequate staff, unmotivated or apathetic staff, staff not providing care according to standards and not being responsive to the needs of the community and patients. Here, performance is understood as a combination of staff being available, competent, productive and responsive1.
Capacity development is one solution to address these performance gaps. Capacity Development Interventions can only be designed based on an analysis of the determinants that influence health workers’ performance. Implementation of these interventions (trainings and institutional/system
strengthening interventions) is expected to yield improved working conditions, improved
motivation, improved staff retention, etc. These, in turn, result in the effects of the intervention in terms of improvements on availability, competence and/or responsiveness of health workers and
ultimately affecting performance of the health system and the health actors. Improved performance in turn contributes to improved health status. Globally, policy makers and planners alike realize that
1 WHO (2006) Improving health worker performance: in search of promising practices, Evidence and Information for Policy, Department of Human Resources for Health Geneva,
Component I Component II
Strengthening institutional structures for stewardship
and service delivery and augmenting the state’s
human resource capacity,
Innovations in Engaging the
Private Sector
Data
Textbox
Reference??

3 Capacity Building & Training Strategy
3
attaining Sustainable Development Goals is not possible unless the Human Resource Crisis is addressed, regardless of increase in health financing.
It has also been emphasized that now that success in staff retention and improvement in performance can be ensured by developing capacity development interventions or approaches that are evidence and need-based, to inform policy-makers as to which interventions may be suitable under which circumstances and for which groups of staff (Buchan, 2002).
1.1.3. Rationale for Capacity Development & Training Strategy
Therefore, to aid state-wide system strengthening and implementation of the UKHSDP, a need emerged to identify gaps between the desired and current performance of the Department of Health & Family Welfare staff. A major pre-requisite for providing quality health care services is ensuring the optimum performance of the health personnel by upgrading their knowledge and skills. However, planners must caution themselves from implementing “one-size-fits all trainings” or “policy straightjackets” that do not address the performance or learning/skill gaps of the stakeholders. Therefore, performance gaps were captured through a rigorous capacity gap analysis and training needs assessment of the different cadres of health staff in the State and documented in the Gap Analysis Report. This data allows evidence-based strategic planning to develop a comprehensive capacity building strategy and plan that will provide the framework for the design and roll-out suitable capacity building and training programs that can strengthen the capacities of different cadres of health staff vis-à-vis their performance gaps. This document is the outcome of the capacity analysis and planning, and outlines the comprehensive capacity development and training strategy that will guide the development of state and district level training implementation plans. This document would also be useful for state and central officials and policy makers to understand the training for effective integrated Health, Family Welfare service delivery at below district level. 1.2. Objectives and Scope of Work for the Assignment
The section below describes the overall objective and the scope of work that characterized the entire assignment, including the CB&T strategy given below:
• Conduct a TNA to identify the capacity building needs of the various cadres of the health staff in
the state like MOs, Nurses, ANMs, GDAs etc.
• Conduct needs assessment for PG level specialization training required by medical officers and
identify such institutes across India to fulfil gaps of specialists in Dept. of Health
• Review the existing training programs and materials and identify gaps
• Prepare a training strategy and a plan to meet the training needs of various categories of
healthcare providers
OBJECTIVES OF THE ASSIGNMENT
Data
Highlight
Data
Textbox

4 Capacity Building & Training Strategy
4
Developing a training and capacity building strategy to
address critical knowledge and capacity gaps for all levels
of staff, that will address
§ Training objectives and needs for each cadre of staff
§ Measures to address identified challenges/ capacity
gaps
§ Profile of trainees at all levels
§ Trainer requirements/ capacity
§ Training approach/ methodology/ duration and
content for each level of trainee
§ Linkages between individual training plans and
performance management system and
§ Indicative training content and broad plan including a
plan for the preparation of training and learning
materials for each type of training and resource
persons to be involved
Development of a detailed annual training
plan with the following components:
§ Training load,
§ Training schedule
§ Costs for various categories of
identified staff.
SCOPE OF WORK 1.3. Methodology of Development of Capacity Building & Training Strategy
The previous section laid out the overall objectives of the current assignment, i.e. to develop a Capacity Development and Training Strategy. This section outlines the methodology that was followed by the AMS to design and develop a comprehensive CB&T strategy that not only strives to meet the diverse training needs of the diverse stakeholders engaged in the implementation of UKHSDP, but is also cost effective and practical with regards to its implementation. 1.3.1. Steps for Development of CB&T Strategy
The Implementation Process has four (4) steps as shown below. The AMS team has been charged with carrying out Step 1 and Step 2 with the support of the Training and Capacity Building Cell in the SPIU. Steps 3 and 4 will be carried out by the Training
Service Provider.

5 Capacity Building & Training Strategy
5
1.4. Gap Analysis and Capacity Needs Assessment
The previous section describes the methodology and the work plan that was adopted while designing and developing the Capacity Building and Training Strategy for UKHSDP. The following section will describe Step 1 described in the methodology – Capacity Needs Assessment or Training Needs
Assessment. This section will briefly describe the methodology of the TNA exercise; the stakeholders covered and finally detail the stakeholder-wise capacity gaps as well as the results of the Competency analysis undertaken for the different stakeholder categories.
Step 1: Capacity
Assessment
Step 2: Design of Training Programme
Step 3: Preparation of
Action Plan
Step 4:
Implementation & Monitoring
§ Identify and define the target beneficiaries § Identify desired capacities in a competency framework based on
strategy, policies, mandates, etc. through desk review & stakeholder consultations
§ Assess the current capacity of each target group through interviews § Identify capacity gaps and training needs
§ Define objectives for the CB&T § Draft a framework to design training programmes § Identify facilitators to conduct the training § Design a detailed schedule and contents of the training
§ Arrange the venue and needed equipment. § Implement the training § Monitoring the training participants and facilitator(s). § Participants undergo pre and post training assessments § Analyse the process of the training and the results of feedback sheet
§ Form a steering committee at the state level & Nodal officers at District.
§ Present the state action plan & budget in front of DG and senior staff in the participants’ directorate.
§ Capacity Building of District Level Staff on Action Plan § Preparation & Approval of District Level Action Plan and budget.

6 Capacity Building & Training Strategy
6
1.4.1. Overview of the Capacity Assessment
The overall capacity assessment exercise assessed four ` `Capacity Axis’ for ‘health provider capacity’ and covered a broad spectrum of issues under each axis (Figure 1.1). These were framed by a detailed questionnaire which collected data on each of the axes, and included a Self-Reported
Competency Analysis & Training Needs Assessment. The questionnaire was the main instrument for data collection; field work included few FGDs with various Health staff, some
key stakeholder consultations followed by document analyses that included a desk review of various guidelines and documents related to the State Health Department and UKHSDP will be undertaken to establish an organizational context of the project. These processes provided ample opportunities for the various service providers to discuss the capacity issues that were most seriously inhibiting their ability to perform their tasks effectively. The Training Needs Assessment can be divided into five stages-
• Identifying Problem Needs: Determine organisational context; perform gap analyses and set objectives supported by desk review of secondary literature & project documents.
• Design of Needs Analysis: Determine the target groups; draw up competency framework to establish desired performance criteria using project documents.
• Data Collection: Review documents of existing trainings planned; conduct interviews/surveys to conduct a self-assessed competency analysis; self-reported training needs.
• Analysis of Data: Quantitative and qualitative analyses of data; draw findings, conclusions and recommendations on training content
• Provide Feedback: Share the findings of the TNA with the UKHSDP Project team and discuss framework for the Training Strategy and Plan.
1.4.2. Coverage and Stakeholder Analysis of the Capacity Needs Assessment
Table 1.2. Given below describes all the different stakeholders engaged in different roles in the healthcare service delivery in the state. Along with the stakeholder category, the types of stakeholder, their job role and responsibility and numbers covered in each category out of the total available staff, during the need analysis is outlined below. At least 10% of each stakeholder category has been covered to ensure statistical validity of the findings.
Clinical Management & Administrative
Soft Skills Other Functional Areas
Capacity Axis for Capacity Analysis
Identifying Problem Needs-
Determine design of Needs Analysis
Data Collection
Analyse Data
Provide Feedback
Figure 1. Capacity Axes

7 Capacity Building & Training Strategy
7
Table: 1.2. Stakeholder Analysis
SN Level Stakeholder Category
Stakeholder Job Role Coverage
1. Medical Medical Officers
• Medical officers
• Specialists
Overall management of the Healthcare facility- proper medical care and treatment of patients.
123 (14%)
2. Para-medical
Pharmacists
• Chief
Pharmacists
• Senior Pharmacists
Responsible for keeping dispensary / pharmacy in a neat and tidy manner;
Supply, maintenance and dispensation of drugs
85 (10%)
Technicians
• Lab
Technician
• Dark room
assistant
• X-Ray
Technician
• ECG
Technician
• Senior Lab
Technician
• Dental
Hygienist
• ICTC Consultation
Health care delivery, especially for services that depend on diagnostic testing for decision making;
Collect and prepare blood, urine and tissue samples; taking MRIs and X-Rays
Maintain patient records and develop exposed radiographs; maintain laboratory inventory levels; keep equipment in good working order and if necessary, place orders for new supplies
30 (10%)
Para-medical Nurses
• Matron
• Staff Nurse
• Assistant
Matron
• Responsible for
managing the care and attending to the needs of the patient; direct patient care like bed making, bed bathing etc.
• Provide comfort to the patients and
82 (10%)

8 Capacity Building & Training Strategy
8
Table: 1.2. Stakeholder Analysis
SN Level Stakeholder Category
Stakeholder Job Role Coverage
ensure safety of the patients
Outreach Workers
Frontline Health Workers
• ANMs
• Health supervisor
• Lady Health Visitor
• Patient Care- taking and recording vital signs, blood pressure and temperatures
• Conduct independent
deliveries; New born resuscitation; New born and maternal care
504 (12%)
• ASHAs
• Keep record of pregnancies, births, deaths and immunizations in the community
• Creating awareness in the community on health, diet and nutrition, basic sanitation and hygienic practices, health services and the need for timely utilization of health and family welfare services at doorsteps
177
Administrators GDAs • Ward Boy
• Class IV Staff
• Patient Care; managing the front office; handling emergency services; maintaining hygiene etc.
181 (14%)
-
This analysis maps generic and functional competencies of the different stakeholders to gauge the existing gaps in their capacities, which will then inform training interventions outlined in the strategy ahead.
1.4.3. Capacity Axis and Capacity Areas Covered
The main areas of capacity assessment are given below in Table 1.3. Since this Capacity Development Plan is underpinned by the same framework, it ensures that the Plan is also aligned with the actual needs of the health staff.

9 Capacity Building & Training Strategy
9
Table 1.3. Capacity areas Identified for Assessment
Capacity Axis Capacity Areas
Clinical Care
This competency attempts to understand the perception of the health staff regarding their ability to carry out their clinical duties effectively and efficiently, and also tries to understand the barriers or challenges they face, if any.
This competency attempts to understand the perception of the health staff regarding their ability to carry out their administrative and management duties effectively and efficiently, and also tries to understand the barriers or challenges they face, if any
Soft Skills
This competency attempts to understand the perception of the health staff regarding their personal attributes they use to influence and enhance the way they communicate and relate to patients, colleagues and peers. These relate to attitudes and intuitions.
Other functional competencies
Apart from clinical, administrative and soft-skills, it is also instructive to understand the status of knowledge, awareness and other skills that are critical in undertaking other peripheral functions of the health staff such as disaster management, biomedical waste management and infection control.
1.5. Gap Analyses of Competency of Health Staff
Training & capacity building is the means to ensure that the official stakeholders have the right knowledge and professional skills that can enable them to deliver on their roles & responsibilities with full competency and efficiency. It becomes a necessity when there is a gap between the desired
performance, and the current performance, owing to a lack of the concerned
skill or knowledge (see graphical representation ahead). In other words, gaps in competencies denote current competencies of the stakeholders and its failure to keep at par with the competencies/ skills (mentioned above) desired or expected from the health staff.
1.5.1 Competencies in Gaps
A Gap Analysis exercise was carried as part of this assessment by first benchmarking the desired competencies of each stakeholder based on their job roles. These competencies were then compared with the current competencies of the different stakeholder categories to reveal the gaps in the
clinical, administration and management and soft skills of the stakeholders under scrutiny. This will
in turn translate into the capacity building and training needs for each of the stakeholder category.
Administrative & Management

10 Capacity Building & Training Strategy
10
1.5.2 Desired Competencies and Gaps in Competencies of every Stakeholder
To understand the capacity needs of the Stakeholders, it is important to separately look at the desired competencies of every stakeholder
described above. The desired competencies of every stakeholder are given below:
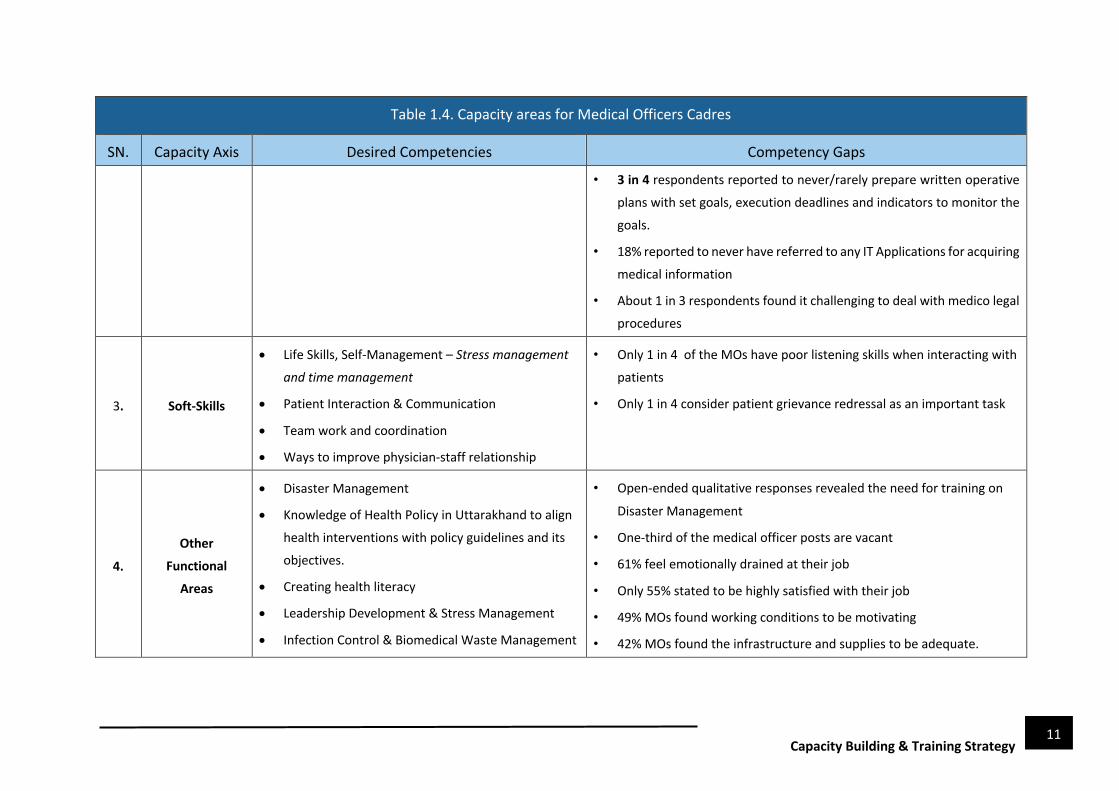
Table 1.4. Capacity areas for Medical Officers Cadres
SN. Capacity Axis Desired Competencies Competency Gaps
1. Clinical Care
• Analyzing records, reports and exam data to help
them diagnose patients’ condition
• Effective Clinical Treatment and evaluation
• Follow-up on any patients referred to a higher
facility.
• Conduct basic examinations, & Emergency
Preparedness
• Only 5% reported to provide instructions to the patients on the do’s and
don'ts to be observed at home; 20% were found to be irregular.
• 58% find it challenging to maintain records of medical history, physical
examination, diagnosis and treatment details of each patient.
• 54% Doctors expressed gap in their ability to provide
Emergency/Critical Care Service like – Basic/ Advanced Life Support; Life Saving intubation techniques; Cardiac Life Support; trauma life support, General Emergency Care; Functioning of ICCUs, etc.
• 69% report that patients experience long waiting times to see a doctor
or to receive treatment. One-third of the medical officer positions are
vacant.
2. Administrative
& Management
• General Management (Problem Solving, Time-
management, conflict resolution, M&E, financial
management )
• Record Keeping and Documentation
• Medico-legal Procedures
• Regulation of clinical establishment
• 3 in 10 or more considered tasks like – HR Mgmt., Supervision & Coordination of peripheral services, Scheme implementation, etc. to be
challenging. This becomes more critical when they reach middle or
higher level.
• 1 in 10 considered themselves efficient in prioritising tasks
11 Capacity Building & Training Strategy
11
Table 1.4. Capacity areas for Medical Officers Cadres
SN. Capacity Axis Desired Competencies Competency Gaps
• 3 in 4 respondents reported to never/rarely prepare written operative
plans with set goals, execution deadlines and indicators to monitor the
goals.
• 18% reported to never have referred to any IT Applications for acquiring
medical information
• About 1 in 3 respondents found it challenging to deal with medico legal
procedures
3. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Patient Interaction & Communication
• Team work and coordination
• Ways to improve physician-staff relationship
• Only 1 in 4 of the MOs have poor listening skills when interacting with
patients
• Only 1 in 4 consider patient grievance redressal as an important task
4.
Other
Functional
Areas
• Disaster Management
• Knowledge of Health Policy in Uttarakhand to align
health interventions with policy guidelines and its
objectives.
• Creating health literacy
• Leadership Development & Stress Management
• Infection Control & Biomedical Waste Management
• Open-ended qualitative responses revealed the need for training on
Disaster Management
• One-third of the medical officer posts are vacant
• 61% feel emotionally drained at their job
• Only 55% stated to be highly satisfied with their job
• 49% MOs found working conditions to be motivating
• 42% MOs found the infrastructure and supplies to be adequate.

12 Capacity Building & Training Strategy
12
Table 1.5 : Capacity areas for the PARAMEDICALS – Pharmacists
SN. Capacity Axis Capacity Areas/ Desired Competencies Gaps in Competencies
1. Clinical Care
• Health Assessment & Diagnosis
• Knowledge of Dispensation of medications by
compounding, packaging, & labelling pharmaceuticals.
• Assisting doctors in emergency cases
• 26% do not report cases of Adverse Drug Reactions
(ADRs) by their patients
• 22% cannot identify problems/errors in prescription
order
2. Administrative &
Management
• Drug Logistics and Supply Chain Management - Stock
Verification and Inventory Management and
distribution
• Record Keeping and Documentation
• General Management (Problem Solving, Time-
management, conflict resolution, M&E, financial
management at facility level )
• More than half of the respondents (around 53%) were
found to be lacking in confidence in using IT tools.
• 19% were found to be unskilled in maintaining
inventory, update patient information, billing etc.
• Around 28% reported to rarely/never store expired
medicines separately/condemned drugs; 7% stated to
be irregular in carrying out this activity and 2% were
found to be unsure at carrying out the activity.
• 40% of the respondents reported to face challenges in
Staff/HR management
• 45% face challenges related to material management
and procurement
• 10% face challenges related to record
keeping/documentation

13 Capacity Building & Training Strategy
13
Table 1.5 : Capacity areas for the PARAMEDICALS – Pharmacists
SN. Capacity Axis Capacity Areas/ Desired Competencies Gaps in Competencies
3. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Interpersonal Interaction & Patient counselling
• While only about 16% of the pharmacists report feeling
stressed and emotionally drained at their jobs, it is
useful to organise trainings time-management & stress
management as pharmacists often have many
responsibilities.
4. Other Competencies
• Disaster Management
• Leadership Development & Stress Management/Conflict
Resolution
• Infection Control & Biomedical Waste Management
• Open-ended responses highlight that pharmacists, who
are often in-charge of the lower-level facilities – are
inadequately prepared to respond to disasters such as
landslides or cloud-bursts that may affect the facilities.
• Open-ended responses also reveal that pharmacists need
a detailed training on infection control and biomedical
waste management.
Table 1.6 Capacity areas for Medical Technicians
SN. Capacity Axis Capacity Areas/ Desired Competencies Gaps in Competencies
1. Clinical Care
• Rationally Conducting Lab tests/Diagnostic tests
• Knowledge of safety protocols and controlling sources
of error during clinical practice
• Knowledge of molecular diagnosis
• 40% claim difficulties in their ability to interpret
prescriptions and rationally carry out diagnostic tests.
• Around 1/4th of the medical technicians (about 23%)
do not regularly carry out safety procedures in the
laboratory

14 Capacity Building & Training Strategy
14
Table 1.6 Capacity areas for Medical Technicians
SN. Capacity Axis Capacity Areas/ Desired Competencies Gaps in Competencies
• 16.7% face challenges related to shortage of staffs
• 10% face challenges regarding lack of knowledge in
molecular diagnosis.
2. Administrative &
Management
• General Management
• Record Keeping and documentation
• Medical Equipment Management
• Only 56% of the respondents are aware that patients
must not ideally receive iron or any other metallic
preparations for 5 days
• 40% face challenges regarding Staff/HR Management
• 45% also stated to face challenges related to Material
management/procurement
3. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Patient Interaction
• Team work and coordination
-
4. Other Functional
Competencies
• Knowledge of National Health Programmes
• Knowledge of Life Cycle Parameters (Molecular Diagnosis)
• Only 60% of the respondents possess awareness about
RMNCH- stimulations harmful for a newborn having
difficulty breathing
• 13% of the respondents are aware to a little extent
about the life cycle parameters/indicators (e.g. ideal HB
levels for pregnant women etc.); 50% possess
awareness to some extent

15 Capacity Building & Training Strategy
15
Table 1.7 Capacity areas for Nurses
SN. Capacity Axis Capacity Areas/ Desired Competencies Gaps in Competencies
1. Clinical Care
• Health Assessment and Diagnosis
• Management of Treatment
• Attention to detail
• Professional, Legal and Ethical Nursing Practice
• Emergency care/Role in assisting clinicians in handling
emergency cases
• Newborn care, especially critical newborn care and
incubation technology
• Only about 1/4th of the respondents reported to confidently
undertake clinical functions like urinary catherization and enema.
• Open-ended responses on desired trainings on clinical care
revealed a strong need for training on dealing with high-risk
deliveries and complications in birth.
2. Administrative &
Management
• Management of Care
• Leadership and Nursing Management
• Only 2 in 5 respondents prepare written operative plans in a
routine manner
• 1 in 3 respondents find HR Management as challenging
• 3 out of 5 respondents reflected absolute confidence in ability to
maintain patients’ files.
3. Soft-Skills
• Life Skills, Self-Management – Stress management and
time management
• Leadership
• Patient Interaction
• Team work and coordination
• Only 63% of the respondents displayed proper communication
skills with different health staff and departments
• 1 in 3 do not give enough importance to two-way communication
with patients and their families i.e. they do not encourage too
many questions from patients regarding diagnosis or treatment
nor do they believe in educating the patients about the potential

16 Capacity Building & Training Strategy
16
risks/ side effects of any treatment/procedures during pregnancy,
post pregnancy etc.
4. Other Functional
Competencies
• Knowledge and Awareness about National Health
Programmes
• Bio Medical waste management and infection control
• 65% possess awareness about NCDs and 48% are aware about 5
National Programmes
• 89% of the Nurses reported motivating working conditions.
• Yet, a little less than half of the nurses feel that their work affects
their duties towards their families.
• Also, 54% Nurses claimed they are stressed or emotionally
drained.
• Open-ended responses reveal that nurses require more training
on infection control and biomedical waste management.
Table 1.8 : Capacity areas for Outreach Workers - Frontline Health Workers (FLWs)
SN. Capacity Axis Desired Competencies Gaps in Competencies
1. Clinical Care
• New Born Care /New born Resuscitation
• Screening of NCDs
• Hands on training on administration of
vaccination
• Maternal Death Review & Child Death Review
• About half of respondents reported to face difficulties in conducting basic examinations such as BP, blood Sugar, Hb levels etc.
• 11% lack absolute confidence in their ability to screen for NCD or
confidently diagnose or identify illnesses in children.
• 4 out of 10 ANMs absolutely confident in –
• Diagnosing delivery related complications
• Conducting Newborn resuscitation
• Diagnosing Serious Illnesses in Newborns

17 Capacity Building & Training Strategy
17
Table 1.8 : Capacity areas for Outreach Workers - Frontline Health Workers (FLWs)
SN. Capacity Axis Desired Competencies Gaps in Competencies
• 4 in 10 respondents expressed need for training in immunization
covering new vaccines and related diseases, and techniques of
administering them
2. Administrative &
Management
• General Management
• Record Keeping & Documentation
• Online reporting of vaccination
• 2 out of 5 reported difficulties in organising VHNDs every month
• 1 in 3 found material management to be challenging
• 30% reported to rarely/never discuss diagnosis, problems or challenges
in mobilising resisting groups with their supervisors (MOs);
Open ended responses revealed need for training in –
• Cold-chain management and supplies logistic
• Immunization related programs like Mission Indradhanush & Online reporting systems
3. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Patient Interaction
• Team work and coordination
• Over half of respondents reflect less than optimal communication
skills (Scored less than 4 on a 6 point scale)
• 30% do not believe in educating the community about the potential
risks/side effects of any treatment/ procedure such as pregnancy, post
pregnancy etc.
• More than 1/4th believe the FLWs to be sole participants/speakers
during any counselling session.
• (54%) reported to face difficulties in undertaking field activities.
4. Other Functional
Competencies • Knowledge & Awareness on National Health
Programmes
• 71% possess awareness about Leprosy eradication and 65% are aware
about 5 National Programmes

18 Capacity Building & Training Strategy
18
Table 1.8 : Capacity areas for Outreach Workers - Frontline Health Workers (FLWs)
SN. Capacity Axis Desired Competencies Gaps in Competencies
• Less than 2 out of 5 respondents reported to manage work/life balance,
especially with regard to duties towards their families
• 85% FLWs expressed their satisfaction with the jobs
• 93% FLWs reported working conditions as motivating.
• 54% FLWs claimed infrastructure & supplies to be adequate
Table 1.9 : Capacity areas for OUTREACH WORKERS- ASHAs
SN. Capacity Axis Desired Competencies Gaps in Competencies
1. Clinical Care
• Analyzing records, reports and exam data to help them
diagnose patients’ conditions
• Patient Care
• Maternal Care
• Basic knowledge of symptoms, treatment and prevention,
especially in malaria prone areas.
• 1/4th of the respondents reported to find Maternal Care
challenging.
• More than 1/4th of the respondents reported to find
activities related to social mobilisation challenging.
2. Administrative &
Management
• Record Keeping/Documentation
• General Management
• 1/4th of the respondents reported to be ‘less confident’
in preparing village health plans.
• More than 1/4th of the respondents reported to find
activities related to social mobilisation challenging.
• More than 1/4th stated to be less confident in their
ability to keep records and maintain patients’ files.

19 Capacity Building & Training Strategy
19
Table 1.9 : Capacity areas for OUTREACH WORKERS- ASHAs
SN. Capacity Axis Desired Competencies Gaps in Competencies
3. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Patient Interaction
• Team work and coordination
• Over 1/4th respondents believe in being aggressive and
force the community members to see things their way
• 36% agree in not educating the community about the
potential risks/side effects of any treatment/procedure
such as during pregnancy, post pregnancy,
administration of drugs etc.
• Over 1/4th agree that its appropriate to scold/ force the
community members to speak up in case a patient or a
community member is afraid to speak up
• 72% face difficulties in undertaking field activities
4. Other Functional
Competencies • Knowledge and Awareness on National Programmes
• 88% believe in the long term financial security provided
by their job
• 21% reported to be ‘fairly satisfied’ with their job
• 23% reported to be ‘fairly motivation’ to perform their
tasks as an ASHA worker.

20 Capacity Building & Training Strategy
20
Table 1.10 : Capacity areas for GDAs
SN. Capacity Axis Desired Competencies Gaps in Competencies
1. Management Skills
• Routine work related issues, such as, administering
injections, dressing, BP measurement, glucose
administration, hospital bedding, applying splints,
sterilization of equipment, use of safety appliances, first-aid,
oxygenating, applying Vigo, shifting patients to wards, etc.
• Assisting doctors while attending emergency cases
• Open-ended responses by the GDA reveal that regular
trainings on aspects of their routine work would be very
helpful as currently GDA do not receive any trainings.
• Multi-skilling of GDA is instructive to support senior
officers in emergency cases.
2. Soft-Skills
• Life Skills, Self-Management – Stress management and time management
• Patient Interaction
• Team work and coordination
• 22% stated to be unconfident in their ability to address patient grievances
• 16% were found to be unconfident in their ability to successfully identify the issues/discomfort of the patients
• Over1/4th respondents reported to get irritated and speak rudely with the patients

21 Capacity Building & Training Strategy
21
Table 1.10 : Capacity areas for Office Management
SN Capacity Axis Desired Competencies Gaps in Competencies
Knowledge & Awareness
• Responsibilities
• Skills needed in office Management
• Routine chores to be overseen
• Office procedure
• Handling of incoming & outgoing correspondence
• Handling of files (Preparing office notes, Guidelines for
drafting communication, etc)
• Recording of files & retention schedule
• Common terms associated with Official Correspondence
• Lack of knowledge about handling of files &
movement of files from lower level to higher level
and back
• Lack of knowledge about noting and drafting
Note:- The provisions for office staff may also be incorporated in subsequent sections as and where required.

22 Capacity Building & Training Strategy
22
1.6 Review of Existing Trainings
Apart from the competency analysis, the training needs of the health staff was also determined after
analysing the trainings provided by the Department of Health in the last three years. An analysis of
the financial activities, funds allocated and spent on different trainings for different components of
the health care programmes running in state. In the following section, the first part describes the
trainings that have been planned and implemented for different health staff categories in the staff,
directing its gaze on the trainings that haven’t been planned for or implemented as per proposal. The
second part focuses its attention on general trainings that are not stakeholder specific.
1.6.1 Stakeholder-wise Trainings
Stakeholder-wise review of the trainings planned and implemented is given below:
(a) Medical Officers
Trainings for medical officers have focused on the National Health Programmes in the last two
financial years – 2018-19 and 2019-20. Trainings have been provided on National Programme for
Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS); National
Vector Borne Disease Control Programme (NVBDCP); Revised National Tuberculosis Control
Program (RNTCP); and other communicable diseases such as etc. Additionally, some non-clinical
trainings have been organised such as `Kayakalp’ under Swachya Barat Abhiyan and `Lakshya’ that
is a Labour Room Quality Improvement Initiative to aid efforts to reduce preventable maternal and
newborn mortality, morbidity and stillbirths associated with the care around delivery in Labour room
and Maternity OT and ensure respectful maternity care. The figure below outlines the different
trainings that have been provided to the staff.
Table 1.11 : Trainings provided to Medical Officers in the last 2 financial years (Source: Training Calendar of Dept. of Health & Family Welfare)
Sl. No Name of Training 2018-19 2019-20
1 NPCDCS Yes
2 Lakshya Yes Yes
3 Kayakalp Swachya Barat Abhiyan Yes
4 Immunization Yes Yes
5 Certificate course in Gestational Diabetes Melitus Yes
6 Training on Malaria Yes 7 Training on Chikungunia/Dengue Yes 8 Training on AES/JE Yes
9 Training on NLEP Yes 10 Training on RNTCP Yes 11 Training on NMHP Yes 12 Training NTCP Yes 13 Training on National Programme for Prevention and Control of Fluorosis (NPPCF). Yes 14 NVHCP Yes
It is self-evident in that most of the trainings were focused around knowledge enhancement and
addressing knowledge gaps around National Health Programmes. None of the trainings sought to develop

23 Capacity Building & Training Strategy
23
the skills of the medical officers. A glance at the budget for capacity development and training for the
Department of Health Staff (Refer to Annexure II), demonstrates that budget has allocated and approved
funding for skill upgradation of medical officers though training such as EmoOC or Emergency Obstetric
Care, Life Saving Anaesthesia Skills, BeMOC, or basic emergency obstetric care. Integrated Disease
Surveillance Programme (IDSP, but these trainings have not been implemented. Besides these trainings,
no fund allocation has been done for F-IMNCI training for Medical Officers, NSSK training for Medical
Officers, Family Participatory Care and New Born Stabilisation; Laproscopic sterilization, NSV, Minilap
training for doctors etc. A detailed list of these trainings is given below. It is also evident that there is no
provision for administrative and management training for these medical officers.
(b) Nurses
Like medical officers, trainings for Nurses have also been based on the National Health Programmes
in the last two financial years – 2018-19 and 2019-20. There has been a considerable focus on
Maternal, Newborn and Child Health Care as exhibited in trainings on Immunization, infant and Young
Child feeding, counselling and insertion of contraceptives and post-mortem related procedures such
as Maternal Death Review and Child Death Review since these make-up for a large part of their job
role.
Besides RMNCH, trainings have been provided on National Programme for Prevention and Control of
Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS); Revised National Tuberculosis
Control Program (RNTCP); National Mental Health Program etc. Additionally, some non-clinical
trainings have been organised such as `Kayakalp’ under Swachya Barat Abhiyan and `Lakshya’ that
is a Labour Room Quality Improvement Initiative to aid efforts to reduce preventable maternal and
newborn mortality, morbidity and stillbirths associated with the care around delivery in Labour room
and Maternity OT and ensure respectful maternity care. The figure below outlines the different
trainings that have been provided to the staff.
Table 1.12 : Trainings provided to Nurses in the last 2 financial years (Source: Training Calendar of Dept. of Health & Family Welfare)
S. No Name of Training 2018-19 2019-20
1 Syphilis
2 NPCDCS Yes Yes
3 MDR/CDR Yes Yes
4 Immunization Yes
5 IYCF Yes
6 Injectable Contraceptive Yes
7 Training on NMHP Yes
8 Training NTCP Yes
9 Training of NCD Yes
10 Training on NPPCF Yes
However, a look at the funding allocation for the capacity development of nurses in the last two years
also highlight the focus on Reproductive, Maternal, Neonatal and Child Health. The plan allocated and

24 Capacity Building & Training Strategy
24
approves funding for the on-site/exposure visit for nurses of delivery points to strengthen their skills in
assisting in complicated births, classroom training on Skill Birth Attendant, midwifery, trainings on family
planning especially sterilisations and IUCD insertions; however many of these trainings were not carried
out in the last 2 years. Additionally, the plan does not allocate for funding for training in RTI/ST (budgeted
for in 2017-18), F-IMNCI, NSSK, IDSP, and Facility-based Newborn Care among others. There is absolutely
no provision for administration and management trainings for nurses in the last two years, although
these tasks play a key role in the everyday job of the nurses irrespective of the facility.
(c) Pharmacists
The training calendar provided by the Department reveals severe gaps in the trainings planned and
carried out for Pharmacists. A careful review reveals that two of the three trainings were organised
for the pharmacists in the last two years which focused on enhancing the knowledge and skills of
pharmacists on the National Health Schemes; Trainings on Malaria/National Vector borne Disease
Control Program and the National Viral Hepatitis Control Program. The final training was a non-clinical
training to address gaps in biomedical waste management and infection control in the respective
facility. However, there has been no budget allocated for Training for Pharmacists under integrated
Disease Surveillance programme (IDSP) in the last two years either.
(d) Medical Technicians
Mostly targeting the lab technicians, the training calendar only mentions training on National Viral
Hepatitis Control Program, to raise the knowledge and awareness of lab technicians about diagnostics
of this program. No other knowledge enhancement or skill training has been organised or even
planned for any category of Medical Technicians. Quality Assurance Trainings are essential for this
cadre and have been budgeted for, although the proportion of funds directed have reduced in the last
three years.
(e) Frontline Health workers & ASHA
As non-facility based health staff, the frontline workers and ASHAs are the foundation of the public
health care system. Although these outreach workers do not have many clinical duties, ANMs and
LHVs are required to conduct some basic examinations and also assist or conduct normal deliveries.
However, most of the trainings provided to the frontline workers are aimed at enhancing their
knowledge and awareness levels on new health programmes or schemes that are introduced. Much
like the other health staff, trainings for frontline workers have also focused on the National Health
Programmes.
Table 1.13 : Trainings provided to Nurses in the last 2 financial years (Source: Training Calendar of Dept. of Health & Family Welfare)
S. No Name of Training 2016-17 2018-19 2019-20
1 Training at Skill Lab Yes Yes
2 Multi-Skilling of ANM Yes

25 Capacity Building & Training Strategy
25
(f) General Duty Attendant
Currently there are no trainings organised or
budgeted for the General Duty Attendant. This
category of staff also do not have any orientation or
refresher trainings.
(g) Accounts Officer
No Public Finance Management Training(s) have
been budgeted and approved since 2017-18 for
Accounts Officer. IDSP training is also instructive for
Accounts officers.
(h) National Health Mission /State /District Program Managers
As programme management staff, it is critical that their management skills are strengthened. These
skills include logistics management, monitoring and evaluation, Human resource management etc.
Programme management training has not be budgeted since 2017-18. Short trainings on data entry
operations and analysis for district and block level programme manager are essential.
1.6.2 General Trainings
Besides the stakeholder-wise trainings, there are some trainings that are vital for the general skill
upgradation of the across the different staff cadres:
(a) Orientation Trainings
Currently, Orientation or Pre-service Trainings are held for medical officers and other senior level
staff. But these trainings are not always regular and not standardised/institutionalised. Staff cadres
such as the Programme Managers, Finance Departments, and even the General Duty Attendants do
not have dedicated orientation trainings. It is thus instructive to institutionalise orientation trainings
or pre-service trainings for all staff cadres. The duration of the trainings may vary depending on the
stakeholder. For instance, for staff medical and paramedical staff, a two week orientation training may
be recommended. On the other hand, outreach workers will benefit from a 20 day training as they
have more frequent refresher trainings compared to the other cadres of staff. Week-long trainings
are recommended for the administrative and Finance Staff at the State, District and Block levels. The
table below summarises the training duration for different stakeholder categories:

26 Capacity Building & Training Strategy
26
Table 1.14 : Proposed Training duration for different stakeholder categories
SN Stakeholder Duration of Induction Training
1. Medical 14 Days
2. Administrative (including Procurement &
Finance) at State, District & Block Level
5 Days
3. Paramedical 7 Days
4. Outreach workers 5 Days
5. General Duty Attendants 3 Days
These trainings must have components of requisite skill enhancement, management and knowledge
about the drugs/equipment and services offered at all levels of health care. This must be completed
in a fixed time frame. The foundation course syllabus mentioned in the Annexure V can be referred
to while designing these trainings.
(b) Refresher Trainings
Besides Orientation Trainings, refresher trainings should also be institutionalised, which is absent at
the moment. While refresher trainings for frontline workers are undertaken at the district level with
the introduction of a new scheme but these are rarely organised for
the purpose of skill upgradation, oriented mostly at enhancing
knowledge. 85% Doctors affirmed conduct of Refresher trainings,
but added that these are infrequent & insufficient given the pace
of change.
In the last two years, very few refresher trainings have been
organised. There is an urgent need for skill training across all cadres
of staff.
(c) Training of Trainers (TOTs)
Besides trainings for the medical and paramedical staff, trainers need to be well equipped to carry out
these trainings. Consequently, apart from accreditation, trainings should be regularly organised for
trainers as TOTs. While the Capacity Building and Training budget mentions TOTs, they have not been
allocated funds in the last two years.
Thedistrictmustensurethatallpersonnelareexposedtothetrainingprogrammesatregularspecifiedintervals.

27 Capacity Building & Training Strategy
27
Capacity Building & Training Strategy
“Much of the global debate about human resources for health is focused on macro issues, such as the existing or needed absolute numbers of workers with different skills…Insufficient attention is paid to retaining and
managing the health workers available within any health system.”
WHO, 2006
The previous section discusses in details the technical approach and methodology adopted in the
design and development of the capacity building and training strategy, the results of the competency
gap analysis and training needs for different health staff and also a desk review of the existing trainings
that have been planned and implemented in the Department of Health & Family Welfare, Government
of Uttarakhand. Informed by the gap analysis, the following section systematically described the
strategic framework that govern the capacity building and Training Strategy and Plan for the
mentioned Department. The problem analysis and training-needs assessment carried out ensures that
there is no mismatch between training contents and skills required in the field, the choice of target
group or training methods.
2.1. Guiding Principles for the Capacity Building & Training Strategy
The following section outlines the strategic considerations and principles that underpin the process of
developing the Capacity Building and Training Strategy. These principles framing the development of
this strategy will be useful while updating it, if required in the future, and aid the development of a
new strategy.
Stakeholder-driven: The training needs assessment drew its mandate and legitimacy
from the expressed collective will of all of the stakeholders across the different cadres
of health staff across the state–right from the Medical officers to General Duty
Attendant. Special discussions were held with the Project Director, NHM officials and
some CMOs to gain their perspectives on the priority training areas for the different staff members
across the project. This maximizes ownership and empowerment, which contributes to increased staff
satisfaction and motivation.
Demand Driven; Each of the major stakeholder groups/divisions was provided with
adequate opportunities to identify their concerns, outline their perspectives, and clear
doubts, not only regarding the questions asked during the survey but also regarding the
intent and purpose of the survey. This ensured that the solutions/suggestions evolved
through fully participatory consultative processes, although all factors influencing performance can
be addressed at the same time, and because the priorities of health worker needs differ.
2

28 Capacity Building & Training Strategy
28
Flexible: As a matter of precaution, the research staff endeavoured to make the
consultative process flexible so that the capacity development interventions could be
adjusted and adapted with ease, to suit the stakeholder category or staff. To ensure this,
individual interviews were undertaken with stakeholders of not just different stakeholder
cadres, but off different age groups and experience levels.
Building Consensus and Holistic Interventions: The participatory processes were strive
to establish a common understanding on different issues affecting performance and build
consensus. Interventions should consist of a combination of actions, addressing working
and living conditions, pay, motivation and accountability.
Decentralised and Horizontally-Integrated Trainings: The Training strategy will ensure
that training programmes are integrated horizontally to ensure that there are no
duplications in organisation of trainings and it will address issues of planning and
operationalisation of health facilities, synchrony of supplies, gender, quality issues and
fund flow mechanism of all training. Furthermore, the development of the detailed
training plan and its implementation will take place at the district level, based on the state level
capacity development and training framework. This ensures local autonomy over financial, material
and human resources, to enable implementation of locally developed strategies, matching the needs
of workers.
2.2. Strategic Framework for Systems Strengthening
Along with the guiding philosophy, the Capacity Building and Training Strategy will be framed by the
strategic framework described below. This framework also lends an insight into the understanding of
individual capacities that characterize the individual performance of the project staff as well as the
systems, processes and the enabling environment that enables and hinders individual performance.
Enabling Environment
Support Systems & Processes
Individual Capacity
(Knowledge, attitude &
Skills)
Will lead to Improved health services &
sector Goals (SDGs)
Figure 2. Strategic Framework for Systems Strengthening (Source: Adapted from WHO,2006)

29 Capacity Building & Training Strategy
29
As illustrated in the diagram above, it has been argued that staff performance is not merely a function
of knowledge and skills but is framed by a host of other factors. To effect high performance, it is
important not just to address gaps in the individual capacity but also strengthen systems and
processes along with the enabling environment. The framework argues that sub-optimal performance
consists of a complex set of factors, which are interrelated. Adapting WHO, 20062 conceptual
framework, the different components of this framework:
(a) Individual Capacity
Individual capacity is determined by the Availability, Competencies, Productivity and
Responsiveness. Inadequate knowledge, skills and inappropriate attitudes can all form obstacles to
good health care. Advances in insights into treatment and diagnosis, as well as changes in roles and
responsibilities, require continuous professional development among health workers. Lack of
competences occurs because of limited access to training and inadequate training methods and
subject matter. Along with knowledge and skill gaps that are a critical part of the competency gaps
assessed, health service provider attitude is another factor that can disrupt health provider/patient
relationships, and thereby treatments. This also includes the level of motivation and job satisfaction
of the health service providers. Demotivation and dissatisfaction with work lead to poor attitudes on
the part of providers towards their work and their patients, not using standard protocols for treatment
or behaving rudely towards patients and stigmatizing patients.
(b) Support Systems and Processes (Micro-Level)
Capacity building at the individual and organizational level coincide in order to achieve the
developmental goals in a given time frame. Besides the intellectual resources of the effective
workforce (determined by developing the proper skills, attitudes and knowledge of the workforce),
the efficiency of the organization (the primary health centers and community health centers) is
determined by the effective its cost effectiveness, physical resources, together with processes for
management of the facility through quality management, performance improvement. Quality
assurance and performance improvement require skilled, motivated and well-performing staff
(Martinez, 2001) and therefore these interventions consist largely of human resource management
practice. Some of these practices include granting greater autonomy to staff regarding their work,
delegating more responsibility, and finally enhanced skills and knowledge building and created
opportunities to apply these skills and knowledge within the organization. Here, it is also important to
remember that human resource management practices are aimed at obtaining high commitment can
be achieved only in an organizational culture that enhances trust and mutual respect among
colleagues and staff members.
Additionally, health workers are more responsive to patient needs with financial and non-financial
incentives. Research shows that financial incentives do not necessarily enhance professional
2 WHO (2006) Improving health worker performance: in search of promising practices, Evidence and Information for Policy, Department of Human Resources for Health Geneva.

30 Capacity Building & Training Strategy
30
motivation in solitary. Other complementary methods are required, such as supportive supervision,
an appropriate regulatory framework and careful monitoring and evaluation. Performance-
assessment systems must be in place and implementation must be transparent for all involved. All
these reforms can only be successful when this happens in an enabling environment, with committed
management and strong leadership.
(c) Enabling Environment (Macro-Level)
Enabling environment refers to the legal and policy framework at the macro-level that lay out the
framework for micro-level governance systems through health sector reforms. The major impact of
health sector reform on the workforce is in terms of changes in working conditions, payment, labour
relations, the demand for certain skills, and terms of employment. Positive experiences in staff
performance have been gained during the implementation of health sector reforms by creating
autonomy over resources at facility level, together with an accountability system, quality assurance
mechanisms and financial incentives for good performance.
2.3. Target Trainees
Informed by the strategic guidelines and the conceptual framework for the CB&T strategy outlines in
the previous section, this section will map the main stakeholders who will benefit from capacity
development intervention to raise their general and functional competencies. The project design and
implementation plan for the UKHSDP helped identify the different stakeholder categories and how
they relate to each other, we have divided them under the main stakeholder categories –
(a) Medical Officer Cadre- The chief stakeholders covering the Medical Officer Cadre include- MOs,
CMO, dental specialists etc.
E MOs- Medical Officers are typically in charge at hospitals. They serve as
advisors on health issues and disease control, provide medical support,
discover inconsistencies and investigate problem. Aside from treatment
to the patients they also provide training to junior/senior residents, and
paramedical staff in the specialty concerned as per the instructions of
the MS.
E CMOs- Chief Medical Officers or CMOs Chief Medical Officers are
responsible for managing hospital budgets, recruiting and training
healthcare physicians, ensuring that all staff adheres to safety standards
and delivering the highest quality of medical care. Chief Medical
Officers will assume responsibility for the faults of their subordinates
E Dental Surgeons- They are the oral health care providers who perform many types
of surgical procedures in and about the entire face, mouth, and jaw area.
Figure 3. Medical Officer

31 Capacity Building & Training Strategy
31
(b) Paramedical Cadre- Paramedics are trained to assist medical professionals and to give
emergency medical treatment. Their functions include-assessing
patients, providing emergency treatment and making diagnoses;
monitoring and administering medication, pain relief and intravenous
infusions and dressing wounds/injuries. The target trainees covering this
category include-
E Pharmacists- They practice pharmacy, focusing on safe and effective
medication use. They are entrusted with the responsibility to ensure
staff and medicines are managed in line with relevant legislation and regulations, and that national
and professional guidance on medicines governance is followed within their facility.
E Medical Technicians- They prepare and analyse the results of
blood and bodily fluid. Mainly working in hospitals and
independent laboratories, their other duties include
collecting, testing and recoding samples. Medical Technicians
comprise Lab Technicians responsible for conducting
experiments, gathering data, and carrying out the basic
investigations like preparing and conducting chemical and
biological analyses; and X-Ray Technicians who use medical
imaging equipment to produce images of tissues, organs,
bones, and vessels and, with advanced training, assisting in the administration of radiation therapy
treatments.
E Nurses- Their roles revolve either directly around patient
care and various responsibilities attached to it. Amongst
nurses, Sisters are the experienced senior nurses
responsible for undertaking management of staff &
delivery of patient care. Staff nurses, on the other hand
are entrusted with the tasks of evaluating patients and
plan, implement and document nursing care like
recording a patient’s medical histories and teaching them
about the ways to handle illness at home.
© Outreach Workers- Their primary role coincides with community sensitization- creating awareness
amongst the community members and sensitising them about the various social issues through an
effective interaction. The Outreach Workers can be sub categorized into-
Figure 6 Nurse
Figure 5. Lab Technician
Figure 4. Pharmacist

32 Capacity Building & Training Strategy
32
E Frontline Health Workers (FLWs)– Including the
ANMs, Health Supervisors and LHVs, frontline
health workers are the backbone of the healthcare
delivery system. They form an important link
between the Primary Health Centers and the
community, ensuring no one is left without access
to basic primary health services. Their major duties
include maternal and new born care; organising events like VHND or UHND etc. in collaboration
with other community workers like ASHAs and AWWs.
E ASHAs- An ASHA’s role is three-fold: to be a facilitator of health
services and link people to health care facilities, to be a provider of
community level health care, and an activist, who builds people
understanding of health rights and enables them to access their
entitlements.
General Duty Attendants’ main
functions are- planning and
organising the units, assistance in housekeeping and sanitation;
transportation of patients and specimens to Emergency Rooms;
participation in ward management, post-mortem etc. The GDAs
comprise of hospital staff like ward boys, sweepers and drivers.
2.4. Capacity Building and Training Objectives
The capacity gap analysis and the needs assessment discuss the diverse barriers and challenges to
effective and efficient performance by the different health staff. In line with the strategic framework
outlined in section 2.2, after mapping the target trainees that will benefit from the capacity building
and training exercises, the section 1.5 has clearly identified the target/desired capacities and the
performance challenges; i.e. the knowledge, attitude and skill gaps that comprise individual
competencies. Based on these competency gaps, the capacity building and training objective(s) will
indicate the roadmap for achieving the desired knowledge, attitude and skills change, to what extent
and over what period of time. They have been defined based on the results of the capacity needs
assessment exercise as well as interaction with the senior staff members of the Uttarakhand Health
Systems Development Project, National Health Mission and other relevant staff members.
The matrix given below lays out the capacity building and training objectives for all the Stakeholders.
These objectives have been defined based on the expected/desired change in capacities of the
concerned stakeholders to address the barriers/gaps faced by them. The objectives are defined for
each category of stakeholders below:
Figure 8. ASHA
Figure 7. Frontline Health Workers
Figure 9: GDA
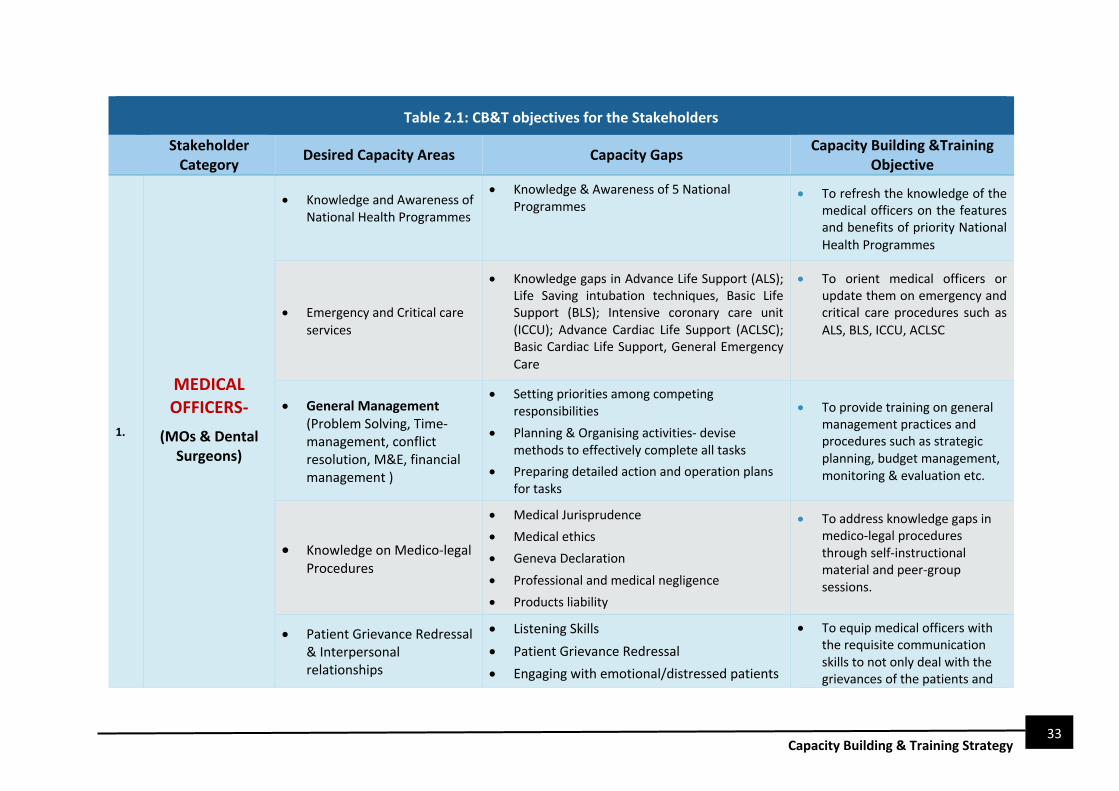
33 Capacity Building & Training Strategy
33
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective
1.
MEDICAL OFFICERS-
(MOs & Dental Surgeons)
• Knowledge and Awareness of National Health Programmes
• Knowledge & Awareness of 5 National Programmes
• To refresh the knowledge of the medical officers on the features and benefits of priority National Health Programmes
• Emergency and Critical care services
• Knowledge gaps in Advance Life Support (ALS); Life Saving intubation techniques, Basic Life Support (BLS); Intensive coronary care unit (ICCU); Advance Cardiac Life Support (ACLSC); Basic Cardiac Life Support, General Emergency Care
• To orient medical officers or update them on emergency and critical care procedures such as ALS, BLS, ICCU, ACLSC
• General Management (Problem Solving, Time-management, conflict resolution, M&E, financial management )
• Setting priorities among competing responsibilities
• Planning & Organising activities- devise methods to effectively complete all tasks
• Preparing detailed action and operation plans for tasks
• To provide training on general management practices and procedures such as strategic planning, budget management, monitoring & evaluation etc.
• Knowledge on Medico-legal Procedures
• Medical Jurisprudence
• Medical ethics
• Geneva Declaration
• Professional and medical negligence
• Products liability
• To address knowledge gaps in medico-legal procedures through self-instructional material and peer-group sessions.
• Patient Grievance Redressal & Interpersonal relationships
• Listening Skills
• Patient Grievance Redressal
• Engaging with emotional/distressed patients
• To equip medical officers with the requisite communication skills to not only deal with the grievances of the patients and

34 Capacity Building & Training Strategy
34
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective • Inspiring Trust and honour
• Influence and respect amongst peers
their family but also internal staff members.
• Other functional competencies
• Disaster Management
• Knowledge on health policy for tracking health outcomes in the state
• To establish and equip medical officers on the procedures and protocols for disaster preparedness and response
2.
PARAMEDICAL PHARMACISTS
(Chief Pharmacists, Hospital
Pharmacists & CHC Pharmacists)
• Drug Dispensation & Basic clinical diagnosis and assessment
• Correct identification of errors or problems in prescription.
• To orient pharmacists in the correct method to handle and dispense drugs and supplies
• Diagnosis and basic health assessment
• Ability to check and record basis vital signs
• Reporting ADRs to medical officers
• To orient pharmacists on basic diagnostic assessments such as checking BP, blood sugar etc.
PHARMACIST
(Chief Pharmacists, Hospital
Pharmacists & CHC Pharmacists))
• Drug supply chain logistics
• Proper drug storage- avoid contamination; disfiguring of labels and infections by pests or vermin
• Ensuring a secured storage environment- adequate temperature; clean conditions & cold storage facilities.
• Ensure proper dispensation of drugs that include knowledge about the expired products and the expiry dates of all the products
• Drug supply/procurement from e-aushadhi
• To train and update the pharmacists on systematic storage and management of drug supply logistics, including procurement, storage, maintenance etc.

35 Capacity Building & Training Strategy
35
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective
• General Management (Problem solving, conflict resolution
• Inventory management and update
• Record keeping and documentation of stock
• To train pharmacists on general management including strategic planning, problem solving, HR Management etc.
• Bio Medical Waste management and Infection Control
• How to dispose chemical and bio-chemical wastes in different types of facilities
• To train pharmacists on methods and protocols for approved and safe disposal methods for waste.
3
Medical Technicians
(Lab Technicians & X Ray
Technicians)
• Knowledge and awareness on molecular diagnosis & equipment management
• Awareness about National Health Programmes
• Awareness on life cycle parameters/indicators (e.g. ideal HB levels for pregnant women etc.)
• To orient medical technicians on molecular biology and hematology
• Knowledge and practice of safe and correct practices related to job
• Knowledge of correct interpretation of prescriptions and rationally carrying out diagnostic tests
• To train medical technicians on how to interpret instructions by medical officers on which tests to conduct and how to conduct them rationally.
• Record Keeping/Documentation
• Transcribing and organising patients’ medical histories, symptoms and diagnosis
• Categorizing treatments and procedures for insurance billing
• To train medical technicians on how to keep records of the observation and analysis of diagnostic tests carried out.
• Bio Medical Waste management and Infection Control
• How to conduct dispose of chemical waste and other medical and biomedical wastes.
• To orient medical technicians on how to dispose off and treat chemical wastes from the lab.

36 Capacity Building & Training Strategy
36
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective
Nurses
(Sisters and Staff Nurses)
• Clinical Function
• undertake clinical functions like urinary catherization and enema. Regular refresher trainings is instructive for these respondents.
• training on dealing with high-risk deliveries and complications in birth
• To orient and refresh the knowledge and awareness of Nurses on the features and benefits of National Health programmes.
Record Keeping/Documentation
• Maintaining Patients' records- a clear account of a particular episode of care but also a comprehensive and concise record of what has occurred
• Healthcare record of the patients
• To train medical technicians on how to keep records of the observation and analysis of diagnostic tests carried out.
General Management
• Goal setting and meeting goals
• Managing appointments
• Strategic thinking
• Implementing strategy
• Reviewing, reporting, and research
• Analysis, Assessment & evaluation
• To train nurses on strategic planning and management to ensure they perform their duties efficiently.
Time Management & stress management
• Focus on the most important activities first-
focus on the tasks with the highest priority.
• frame.
• To train nurses on time management between clinical and non-clinical duties.
Leadership and Coordination
• Inspiring Trust and honour
• Influence and respect amongst peers
• Effective Interaction with co-workers
• To conduct workshop and encourage nurses to develop their capacities as leaders
Patient Interaction • Taking questions from the patients
• Active Listening • To train nurses on how to
communicate efficiently with

37 Capacity Building & Training Strategy
37
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective • Educating Patients- explain disease processes,
medications, and self-care to the patients
• Inspire Trust- Listen to your patients and take
all their complaints or concerns seriously
• Show Compassion- Treat patients with respect
and dignity; Put yourself in the shoes of your
patient; convey empathy.
other staff members as well as with patients and their families.
Bio Medical Waste management and Infection Control
• How to conduct dispose chemical waste and other medical and biomedical wastes.
• To orient nurses on how to dispose and treat chemical wastes from the lab.
OUTREACH WORKERS-
Frontline Health Workers (FLWs)
• Diagnosis and basic health assessment
• Ability to check and record basis vital signs such as checking BP, pulse, blood sugar etc.
• To orient frontline health workers on basic diagnostic assessments such as checking BP, blood sugar etc.
• Clinical services like Delivery & Newborn Care
• Diagnosing delivery related complications
• Conducting Newborn resuscitation
• Diagnosing Serious Illnesses in Newborns
• To orient frontline health workers to perform delivery and newborn care, especially addressing complications in these procedures
• Latest advancements in Immunization & Cold Chain Mgmt.
• Cold-chain management and supplies logistic
• Immunization related programs like Mission Indradhanush & Online reporting systems
• To orient frontline health workers on cold-chain management and manage supply and logistics of drugs

38 Capacity Building & Training Strategy
38
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective
• General Management, especially concerning VHNDs
• Micro planning of events, coordinating supply
and logistics
• Systematic reporting- systematic recording of all attendees of the given event, and that prescribed formats for the event reporting all filled and submitted.
• To train nurses on strategic planning and management to ensure they perform their duties efficiently.
• Patient/Community Interaction
• Treat patients with respect and dignity.
• Counselling skills-Explain disease processes,
medications, and self-care techniques to
patients and their families; breakdown medical
jargon into simple terms.
• Active Listening
• To conduct workshop and encourage nurses to develop their capacities for effective communication
• Self-Management
• Planning & Organising activities- devise
methods to effectively complete all tasks
• Minimising 'time-wasters'- interruptions,
distractions and other delays that reduce
productive time.
• To train FLWs on time management between clinical and non-clinical duties.
• Bio Medical Waste
management and Infection Control
• How to conduct dispose chemical waste and other medical and biomedical wastes.
• To orient FLWs on how to dispose and treat chemical wastes from the lab.
General Duty Attendant
• Routine non-clinical care of patients
• Looking after all the non-clinical needs of
patients
• First aid & glucose administration
• To orient GDA on how to carry out non-clinical duties such as making the bed, making sure GDA is comfortable

39 Capacity Building & Training Strategy
39
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective • Patient/Community
Interaction
• Treat patients with respect and dignity.
• Active Listening
• Counselling skills
• To conduct workshop and
encourage GDA for effective
communication & counselling
• Bio Medical Waste management and Infection Control
• How to conduct dispose chemical waste and other medical and biomedical wastes.
• To orient GDA on how to dispose and treat chemical wastes from the lab.
Clerical & Administrative Staff
(Program Managers at State, District & Block level)
• Office Management & Documentation skills
• Rules for handling correspondence; Handling and indexing of office files, Preparing Office Note and order by decision taking Officer, etc.
• To orient the administrative and clerical staff on the Govt. of Uttarakhand’s rules for handling correspondence; Handling and indexing of office files
• General Management (time management, decision making, problem solving, etc.)
• Micro planning of events, coordinating supply
and logistics
• How to take better decisions and problem
solve
• Systematic reporting- systematic recording of
all attendees of the given event, and that
prescribed formats for the event reporting all
filled and submitted.
• Quality Assurance,
• Supportive Supervision,
• Management of logistics of supplies and
maintenance of adequate stock of lab material,
medicines,
• To orient the administrative and clerical staff on how to improve general management

40 Capacity Building & Training Strategy
40
Table 2.1: CB&T objectives for the Stakeholders
Stakeholder Category Desired Capacity Areas Capacity Gaps Capacity Building &Training
Objective
• IT Skills • Use of Tally, MIS, and basic MS Office. • To orient the administrative and
clerical staff on how to use MS
Office software and other IT
tools
Finance Department & Accounts Officers
• Financial Rules & regulation
• Financial Rules & regulation Govt. of Uttarakhand
• To orient the Accounts Officer on how to use MS Office software and other IT tools
41 Capacity Building & Training Strategy
41
2.5. Capacity Building and Training Activities
The previous section laid out the capacity building and training objectives for the diverse project staff.
The proposed activities seek to address key capacity gaps of the health staff engaged in Uttarakhand,
identified in the capacity assessment study. These activities also complement and build on various
activities already organised and carried out by the state. However, these trainings are mostly
restricted to introduction of a new health scheme or a new procedure or technology, sometimes.
2.5.1. Capacity Priority Areas
Framed by the conceptual framework described in section 2.2, the capacity priority areas will not only
address the target group specific capacity gaps described in Section 1.4 of the report. At the heart of
the Capacity Development Plan Activities is the development of a range of competencies that include
a combination of few ̀ Hard’ (Clinical & Management) as well as and ̀ Soft’ (interpersonal skills) which
are appropriate to the needs and constraints of the target groups. The following section presents
competencies which are considered, as a whole, a priority for upgrading:
(a) Individual Capacity While the project staff have been recruited after due procedure,
advances in insights into treatment and diagnosis, as well as changes in
roles and responsibilities, require continuous professional development
among health workers. Individual performance is influenced by
retention, motivation and job satisfaction, obtaining knowledge, skills and attitudes, accountability and working conditions, all interrelated. All of these factors have demonstrably adversely affected performance,
and interventions to address these gaps will be explored in great detail below.
The method most frequently used to upgrade skills and knowledge is off-site training courses and seminars. To ensure that there is no mismatch between the training content and the skills that need
upgradation, the capacity building interventions are informed by the knowledge and skill gaps
identified by the Gap & Training needs analysis. Now, Knowledge and Skill training will be divided into
two categories: (i) Core Skills, which need to be possessed by all personnel of each category; (ii) Specialised Skills to be imparted as per the institutions where the trainees are posted.
Core Skills: Regarding the core skills, the basic nature of the skill gaps may be the same across
different staff categories or even for the same stakeholder category, for staff members it is primary,
secondary or tertiary care institution, there will be substantial variation in skills required for
management of complications

42 Capacity Building & Training Strategy
42
Table 2.2 : Priority Core Competencies for Staff
1. Competency 1: Project Management - Strategic and Coordinated Planning, Monitoring, Reporting, HR management
• Establishing a clear vision for the goal/objective
• Designing and developing activities to achieve said vision
• Budget discipline and monitoring
• Ability to carry out tendering and procurement, and effective contractor
supervision
• Establishing baseline development data, indicators, benchmarks
• Translating development data, indicators and benchmarks into realistic development plans which take
account of budget capacities
• Establishing result-oriented management systems for performance, monitoring and review, reporting
and assessment outcomes and outputs
• Ensuring the planning is both top-down (clarity of direction) and bottom-up (taking
account of feedback from the clients on priorities)
• Disciplinary proceedings
• Maintenance of Service books and personal files
2. Competency 2: Communication & Liasoning
• Providing regular reports to key stakeholder agencies
• Operational coordination with key stakeholder agencies
• Identifying various interest groups within civil society & Strategies on
how to work with different interest groups
• Managing differing points of view and conflicting interests
• Maintaining channels of communication with patients & staff
• Using the role of feedback from patient & family to improve development planning, management, and
services
• How to put across one's points sensitively & empathetically to patient & family
• How not use complex terminology to refrain from confusing patients & family
• Speak at an appropriate speed, volume, tone and pitch to communicate the idea effectively to the
audience
• Rapport building techniques including precision in communication, patience, team spirit, conflict
resolution and promoting positive communication patterns
• Role of communication in improving health literacy
3. Competency 3: Self-Management
• Motivating staff for greater productivity
• Approaches to instilling discipline
• Decision Making & setting priorities
• Time Management

43 Capacity Building & Training Strategy
43
• Conflict Resolution
• Stress Management and Problem-Solving Techniques
• Self-Assessment Exercises
• Use of IT Tools for documentation and reporting
• HR management - Maintenance of Service books and personal files & staff appraisal
• Legal safeguards to Public Servants / Medical Professionals
4. Competency 4: Leadership &. Motivation
• Leadership Concept & types of Leaders
• Ensuring observance of Office Decorum by staff
• Ways to improve Doctor-Staff Relationships
• Influencing skills and techniques
• Team Building
• Managing change effectively
• Introducing and sustaining organizational change effectively and Action planning
• Stress Management
• Motivational techniques and practices
5. Competency 5: Budgeting & Accounts
• Functioning and basic rules of Treasury
• Audit and functioning of AG Office
• Accounting network system
• Condemnation procedure and disposal of dead items
6. Competency 6: Medico-legal Practices
• Reporting of accidents and police cases
• Medico Legal examination
• Post mortem examination guidelines (Rules for CMOs, Directions for preserving and packing Viscera, etc.)
• Instructions for the guidance of MOs regarding Medico Legal Work and Expert Professional Opinion
• Medical negligence Syn. Mal Practice
• Contractual relation between Doctor and Patient
• Preparation of medico legal reports in different situation and police formalities
• Issuing Death Certificate
7. Competency 7: Biomedical Waste Management & Infection Control
• Waste Management
• Segregation of Biomedical Waste
• Collection and transportation of Biomedical waste
• Sharp Management
• Storage of Biomedical Waste

44 Capacity Building & Training Strategy
44
• Disposal of Biomedical waste
• Management Hazardous waste
• Solid general waste management
• Liquid waste management
• Equipment and supplies for Bio Medical Waste Management
• Statuary Compliances
• Hand Hygiene
• Personal Protective Equipment & Practices
• Decontamination & Cleaning of Instruments
• Disinfection & Sterilization of Instruments
• Spill Management
• Infection Control Program
• Hospital / Facility Acquired Infection Surveillance
8. Competency 8: Disaster Management
• Types of Disasters
• Phases of Disaster Management
• Key Components of effective emergency management plan
• State Emergency Management Authority & Executive Committee
• Obligation of Health Department as per clause 30 of the Disaster Management Act
• Development of Disaster Management Plan by Health Department under section 40 of the Act
• Preparing Disaster Response Plan
• Preparedness Checklist for public health department
Specialised Skills: Unlike the Core Skills, specialised skills are not only stakeholder specific but also
specific to the specific job role and position and the institutions where the trainees are posted. Most
of the specialised skills concerning our target trainees are clinical skills.
(b) Organisational Capacity/Support Systems & Processes
Training is successful in improving performance only when it is embedded in a broader strategy that
includes job satisfaction and motivation issues, working conditions and accountability to patients,
colleagues or managers. Good performance and responsive staff is enabled via a supportive working
environment and thus reduces turnover, absenteeism and enhances productivity.
§ Physical Infrastructure & Working Conditions: This not only encompasses having sufficient
equipment and supplies in the respective facility that can hamper performance of skilled
personnel; but also includes systems issues, such as decision-making and information-exchange
processes, and capacity issues such as workload, support services and infrastructure. Suggested
guidelines for facility-level level capacity development & system strengthening are:
• The facility must ensure adequate supplies and infrastructure.

45 Capacity Building & Training Strategy
45
• Currently, acute workforce shortage results in high workload on existing staff. Well-defined
and targeted HR policies can help reduce turnover.
§ Human Resource Management: Besides financial incentives, the lack of supportive supervision
and heavy workload due to inadequate human resources plays a critical role in low motivation
and poor performance. Moreover, the lack of professional development opportunities in the
absence of regular skill upgradation exacerbates low job satisfaction. Professional development is
important for staff, but various learning approaches can be applied to learning such as though on-
the-job training and at the workplace through supportive supervision, clinical meetings or peer
support and through distance-learning schemes.
Additionally, staff members need to be able to work in teams, and a relationship of trust between
staff and management is imperative. Given the limited management capacity at lower levels of
the health system such interventions must be preceded by efforts to build management capacity.
Suggested guidelines for facility-level level capacity development & system strengthening are:
• Weekly staff meetings at the facility, headed by the head of the facility, will ensure better
communication & support between colleagues. The minutes of these weekly meetings should
be recorded and documented by the staff.
• Fostering improved communication between supervisors and subordinated to ensure free
communication channel.
• Organising daily morning meetings during which medical officers plan for the day ahead.
• Grievance redressal box for those wishing to submit grievances anonymously should be
provided for and addressed at weekly meetings.
• Positive affirmation and supportive supervision go a long way towards helping the staff feel
valued.
• Gender-sensitive strategies at the workplace may further raise the motivation levels of staff.
For example, rules may be in place that allow the female staff to return while the daylight is
still out.
§ Quality Assurance (QA) & Performance Management Strategies: Unethical behaviour through
forms of mismanagement and corruption or the non-adherence to protocols, can occur because
of a lack of accountability mechanisms and also heavy workloads. Holding staff accountable for
their performance towards their clients, colleagues or managers through structural supervision
and support, might offer opportunities to improve performance. Here, structural support means supervision, performance appraisals, rewards and punishment to ensure quality and
productivity of their staff. This allows a continuous supervision and motivation of staff, ensure
appropriate tools and resources, and identify performance gaps and address them. Supervisors
must be appropriately trained to implement these procedures. Some of these procedures

46 Capacity Building & Training Strategy
46
• Quarterly performance appraisals should be conducted by the head of the facility.
• Peer reviews will be co-terminus with the quarterly performance appraisals to receive input
from colleagues as well as supervisors.
• Third Party Quality Audits should be conducted every-six months.
• inputs from the Performance appraisals and peer reviews should feed into development of
district action plans for Capacity building.
(c) Enabling Environment
Sustainability of capacity development interventions can only be ensured when there is an enabling
environment that supports the transfer of knowledge within the organization, upgradation of skills
and knowledge and also creates and maintains a positive atmosphere for the cultivation, sharing and
enhancement of this knowledge. Health sector reforms through a robust policy framework at the state
have shown to support this endeavour.
This framework seeks at strengthening the health workforce in by addressing working conditions, payment, labour relations, the demand for certain skills, and terms of employment at a macro-level. But the success of such approaches requires the commitment of senior management, availability of financial resources and delegation of decision-making to lower levels/decentralisation of public health governance. Research indicates that such changes have a significant impact on productivity of
services, which indirectly shows an increased productivity of staff.
Some of the following strategies must be adopted to strengthen the enabling environment are given
below.
1. Mainstreaming Capacity Development & Training: It may be useful to increase Government
Commitment for mainstreaming Capacity development in State Policy to ensure sustainability of
any such interventions undertaken. The state will develop the strategic framework that will be
converted into detailed district level training plans.
2. Dedicated State Capacity Building and Training Cell: Currently, the state does not have a
dedicated Capacity Building and Training Cell to closely implement and monitor these
interventions. Having a dedicated cadre of professionals to plan and implement trainings across
the State will benefit programme implementation and overall effectiveness of health care service
delivery in the state. Accordingly, district level training officers should be trained in the CB&T
policy and plans.
3. Develop Digital Platform for Capacity Building & Training : To keep the momentum of the digital
transformation in India going, it is recommended that the State Monitoring Cell team up with the
Capacity building & Training Cell/Staff to create a digital platform to develop Training MIS that
may be integrated with HMIS of the state. This MIS be useful in carrying out the following:

47 Capacity Building & Training Strategy
47
(a) HR Management System: Information on the health staff currently in position such as their
age, experience, skills, certifications, availability etc. is useful to keep track of available resource
people. This information from the district level should feed into the State MIS.
(b) Performance Management System: To track progress on individual staff members, i.e. Inputs
from performance appraisals and Peer reviews should feed into development of district action
plans for Capacity building.
(c) Monitoring & Evaluation System: A continuous monitoring and evaluation system should be
designed and operationalised by the State M&E department in concert with the newly formed
Training Cell. A tentative strategy with input-output monitoring and outcome-impact evaluation
indicators and methodology has been outlined ahead in Chapter 4.
(d) Training Curricula & Material/Modules: Will contain training curricula along with pre-existing
ones developed by NHM, DHFW, and other training institutions. It should also have annotated
digital library with downloadable learning material and e-modules available for reference of
Health Staff.
(e) Develop and Institutionalise Training Institutions: There is a need for upgrading training
institutes by providing requisite equipment & ICT Infrastructure. It is also instructive to
restocking physical libraries with updated reference books and journals. Developing Skill labs
for various clinical trainings for different cadre of staff and Model facilities for organizing
exposure visits to gain hands on learning will complement individual capacity building efforts.
The State has already done a lot of work on upgrading the Divisional Health & Family Welfare
Training Center, Motibagh, Haldwani (NTL) as the ‘State institute of Health & Family Welfare’.
The State has also developed a framework to commission and operationalize the Institute. In
order to strengthen the training competent, The State could expedite the process. Once
operationalized, many of the functions as outlined above could be transferred to the SIHFW.
District-Level Training Implementation: While public health governance and implementation of
health programmes is already decentralised in the context of Uttarakhand, it is recommended that
District Health Programme Management Units develop and incorporate district capacity building and
training plans in the District Action Plans to address local training needs and other operational
problems. This also ensures optimum utilisation of available resources and programmes without any
duplication. The district training plan will adhere to the following guidelines to ensure smooth and
sustainable implementation of trainings:
(a) Annual District Training plans will be prepared with the time-frame for the trainings based on
the State Strategy
(b) Trainings can be organised in synergy with the availability of continuous supply of drugs and
equipment so that the trainees can practice the skills.

48 Capacity Building & Training Strategy
48
(c) Synchronous Trainings in area: Training of all functionaries in an area/institution in a
synchronous manner or integrated manner such that the respective facilities that already suffer
from workforce shortages is not deprived of essential personnel.
(d) District Training Plan will include the plan for monitoring the quality of training and also the
utilisation of trained personnel, based on the budget provided by the state.
(e) While a norms for training load and batch size will be outlined in the State Strategy, they should
be suggestive only. The total training load should be calculated on the basis of the health
functionaries currently in position and existing functional health facilities. Batch size to be
decided according to the skills which are to be provided to the health functionaries and the
training venues available.
• Convergence with non-health departments that work on health and family/nutrition components - Convergence with PRI, WCD, AYUSH & Department of Drinking Water & Sanitation
at the district level will help in delivery of specialised skill trainings effectively such as regarding
Safe Sanitation, Infection Control, RMNCH+ etc. Additionally, as part of an overall system
strengthening and capacity development effort, strong support of PRI, WCD etc. will facilitate any
local level health interventions that are carried out by the health Department in collaboration.

49 Capacity Building & Training Strategy
The framework of activities essentially creates the space the health staff of the Uttarakhand Health Department to learn a range of skills to effectively meet
the challenges identified by the capacity assessment exercise. The capacity development activities in Table 2.3 are broken down into high and low priority
areas, and into short (6 months), medium (1 year) and long term (1-2 years) targets. They approach capacity building at three analytical levels—individual, organizational, and enabling environment—with particular reference to the gaps identified in the capacity assessment process.
Table 2.3 : Capacity development plan: Priority Activities
Short-Term (6Months) Medium (1 Year) Long-term (1-2 years)
Individual
§ Ensure Induction/Pre-service training incorporating
Foundation course is provided to all
§ Increased frequency of Capacity development and
trainings by training in batches. More demonstration
and field-based training
§ To organise peer learning sessions facilitated by
self-instructional materials to address knowledge and awareness gaps related to the National Health
Programme components and their roles and responsibilities
§ Preparation of District Training Plans informed by the Annual Training Strategy & Plan
§ Develop and Institutionalise existing
Training Institutions at Haldwani and Dehradun. Upgrade Training Institute
at Chandernagar to establish it as SIFHW.
Organisation
§ Weekly staff meetings at the facility, headed by the
head of the facility, will ensure better communication &
support between colleagues. The minutes of these
weekly meetings should be recorded and documented
by the staff. Also, organisin/g daily morning meetings
during which medical officers plan for the day ahead.
§ Quarterly performance appraisals should be conducted by the head of the facility.
§ Peer reviews will be co-terminus with the quarterly performance appraisals to receive input from colleagues as well as supervisors.
§ Third Party Quality Audits should be
conducted every-six months.
§ Currently, acute workforce shortage results in high workload on existing staff. Well-defined and targeted HR policies can help reduce turnover.

50 Capacity Building & Training Strategy
Table 2.3 : Capacity development plan: Priority Activities
Short-Term (6Months) Medium (1 Year) Long-term (1-2 years) § Grievance redressal box for those wishing to submit
grievances anonymously should be provided for and
addressed at weekly meetings.
§ Gender-sensitive strategies at the workplace may
further raise the motivation levels of staff. For example,
rules may be in place that allow the female staff to
return while the daylight is still out
§ inputs from the Performance appraisals and peer reviews should feed into development of district action plans for Capacity building.
Enabling Environment
§ Standardize and integrate trainings to prevent course
duplications and gaps. This may be done by developing
a State Manual for Capacity Development & Training
guided by the Strategy by AMS
§ Prepare Annual Training plan informed by the Training
Strategy
§ Create a detailed M&E plan with the M&E cell and CB&T
cell to monitor the efficiency of the training and
capacity building exercise
§ Digital platform to should also have annotated digital
library with downloadable learning material and e-
modules available for reference of Health Staff.
§ Establish Training of Health – MIS that is linked H-
MIS to keep track of trainings and trained
manpower
§ Establish a performance management system as
part of the HR management system and the data should feed into TH-MIS
§ To provide essential equipment at the facility level
§ Along with Pre-Post Training Assessments, regular monitoring of Training Quality needs to be done through audits, evaluations, along the lines of TNA

51 Capacity Building & Training Strategy
2.6. Modes of Training Delivery
The previous section outlined the capacity development activities addressed through the capacity
development plan. This section describes the different modes of delivery that will ensure effective
reach and consumption of the trainings. Mode of delivery of training programmes determines the
structure, nature, and contents of training modules and learning materials that need to be developed.
A sustainable cost effective training programme for a large number of staff will require delivery modes different from those conventionally used, bound by time and space, and face-to-face training workshops which are also costly.
Thus, both conventional components such as lectures and handbooks, and modern components such
as peer-to-peer learning groups and on-the job mentoring is recommended as effective training
modalities. Looking beyond formal learning modalities (ex. Classroom lectures) that involve high costs
and time (including long-distance travel) are not always practical. Some of these modes of delivery
are described below:
(a) Master Trainers Training or Training of Trainers
The strategy encourages the ‘train-the-trainers’ programme to develop the ability of senior project
staff to ensure that the Trainers have adequate training and pedagogy skills to impart to the trainees.
If trainings are supported by external institutions or medical colleges or nursing colleges, the faculty
of state level institutions and Medical Colleges need to update their skills on a continuous basis to be
able to provide quality training. It is also important that any private health facility or trust-run hospital
that may be supporting this capacity building must be accredited. A database of guest faculty to
support the in-house faculty must be available with the State.
The train-the-trainers’ programme is therefore intended to initiate the process of developing capacity
to work within the community and the project framework. The component of on-the- job mentoring
can also be achieved through the use of a ‘train-the-trainers’ network.
(b) On-the-Job Mentoring
On-the-job mentoring is an effective that way to provide an
environment in which these skills can be more effectively
acquired by the staff members by improving team-work and
team collaboration, thereby the enabling environment to
provide effective capacity development. It is particularly
instructive after a training course by a district training officer to
follow up on the impact of the trainings provided and provide
handholding support in case of any difficulties.

52 Capacity Building & Training Strategy
(c) Peer-to-Peer Networks/Group Mentoring
The creation of peer-to-peer networks to
enable staff to come together and learn
from one another is not only cost-effective
but facilitates discussion, engagement and
better learning. Such a modality could play
a key role in ensuring that relevant skills are
transferred among those who hold similar functional roles.
Where possible, organizations should enable staff members who
have undertaken training to work with their colleagues who have
not, in order facilitate transfer of information between these
peer networks.
(d) Development of Trainers Manual
Development of materials should include a trainer’s manual, which includes facilitation techniques for
mentoring and coaching learners, presentations and small group activities. Trainers should act more
in the role of mentors to alleviate learning difficulties of learners, and as motivators to encourage
learners’ self-esteem and incite active participation in the training programmes.
(e) Classroom Lectures/Seminars/Workshops
One of the most common training method, off-site classroom method or lecture method involves a
classroom to give training by trainer in the form of lectures. It is effective
for the purpose of teaching to make aware of procedures and to give
instructions on a particular topic. But not only is this method costly given
the number of staff, it is not very engaging and generates little interest in
the trainees. Using audio-visual in the form of films, Video, and
Presentations etc. have been successful in encouraging students to
understand and assimilate easily and help them to remember forever.
Additionally, it is also recommended that role-playing activities and other
games may be used by the trainer to create a more engaging environment conducive to learning.
A critical addition may be the use of demonstrations using models and practice exercises to encourage
applied learning. Currently states use mannequins for Anaesthesia and EmOC training. Similarly, Zoë
model is being used for Family Planning Trainings especially IUCD. Female pelvic models are being
given to all district hospitals and many ANM Training Schools. Exposure visits or monitoring of
actual/live procedures in the field will boost the confidence of the trainees.
Mentoring as a mechanism, of supportive supervision for bringing attitudinal change in health care providers, needs to be restored. Team leaders need to be provided with skills for mentoring and supportive supervision on the job.

53 Capacity Building & Training Strategy
(f) Self–instructional Materials
Instructional materials will facilitate self-directed learning as well as peer group interactions. These
texts should be prepared in the language that is easy to read and understand, and is able to maintain
sustained interest. Materials should take into consideration the following:
• Having clear set of leaning objectives/outcomes at the beginning of each unit of the course
• Keeping sentences short, simple consistent and structured
• Visually appealing with illustrations
• Local Context
• Relevant Examples
• User friendly
To facilitate learning, problem-solving exercises, case studies, assignments, group works contained in
the learning material should be prepared and be relevant to the work place. The instructional
materials should be tailored to the needs of the different target groups. For example, for the outreach workers, instructional materials should be brief, crisp with well-illustrated graphics used to describe
a point. On the other hand the self-instructional material for the state and district staff members will
be more detailed in the form of a handbook.
(g) Webinars/E-learning modules
E-learning is the act of engaging in an educational course in an online
setting. E-learning courses can exist in a variety of forms, using a range of
technologies, including audio and video recordings, presentations,
quizzes, surveys, games, discussion groups, and more. The curriculum
and modules can be prepared by the regional training institutes and
medical colleges. E-learning can help learners complete education and
training objectives with greater ease and flexibility than they can with traditional classroom-based
learning. This mode can be particularly helpful in the Garhwal area, where the terrain is difficult and
vast to facilitate communication with regional medical colleges and other training institutes.
Besides its cost effectiveness, e-learning modules and webinars can be available as and when needed
without any disturbance to the work schedule of the health staff in the state. Along with post training
follow-up and support, webinars ensure quality assurance by participants’ support, faculty support
and evaluation and assessment. However, this mode may not be recommended for the delivery of
core skills’ training, and may be useful only for more specialised or niche trainings. NIFHW has a online
PG diploma course for programme management - PG Diploma in Management (PGDM-Executive), recognised by AICTE, that can be completed online.

54 Capacity Building & Training Strategy
The Table in the following page outlines the suggested mode of training delivery for the different core skill areas for the different health staff:
Table 2.4 : Suggested Training Types for Different Capacity Aspects
SN Aspect of capacity Required Activities Training Type
1. Knowledge and Awareness
• Knowledge of the National
Programmes
• Peer-Group Sessions
• Self-instructional materials
(Booklet or e-learning
modules)
2. Clinical Skills
Effectively carry out clinical
functions like-
• Patient Care (follow up &
required instructions)
• Accurately Interpreting
diagnostic results
• Knowledge of drugs
• Peer-Group Sessions
• Self-instructional materials
(Booklet or e-learning
modules)
• Off-site
training/demonstration/expos
ure visit
3. Management Skills
• General Management
(Project management, HR,
budget, procurement etc.)
• Performance & Quality
Management
• Record
keeping/documentation
• Self-instructional materials
(Booklet or e-learning
modules)
• Workshop/Classroom session
• Off-site
training/demonstration/expos
ure visit
4 Soft Skills
• Motivation Levels
• Patient/Community
Interaction
• Communications &
Coordination.
• Self-instructional materials
(Booklet or e-learning
modules)
• Workshop/Classroom session
5.
Other Functional competencies
• Biomedical Waste
Management
• Infection Control
• Self-instructional materials
(Booklet or e-learning
modules)
• Demonstration/Field-visit
2.7. Target Group-wise Trainings
In terms of skill and knowledge requirements, the different target stakeholder categories will require
slightly different set of competencies. Since the training they undergo may vary, a clustering of
competencies and broad training objective for each group is necessary. The Tables given below

55 Capacity Building & Training Strategy
presents an outline of the priority competencies for each learning group. Furthermore, attempt has
been made to develop the training modules required for enhancing the functional knowledge of the
concerned staff; improving their skills to become more effective in their role; and help them change
attitude.
2.7.1. Developing competencies for Core Competencies
The following tables present the breakdown of competencies for building core skills that is important
for most target groups, irrespective of their functions. However, the level of these competencies will
vary from one stakeholder to another depending on their job role and qualification. It includes training
components and the resulting competencies, from the list of priority competencies identified in the
previous section.
Table 2.5b:: Communication, and Liasoning Skills
Target Groups MO, Nurse, Technicians, Pharmacists, FLWS, ASHAs
Objective: Instil key communication and liasoning techniques
• Interpersonal communication
• How to put across one's points briefly.
• Does not use complex terminology to refrain from confusing the other
stakeholders
Table 2.5a: Project Management-Strategic and Coordinated Planning, Monitoring, Reporting, HR management
Target Groups State Administration, MOs, DPMs, Nurses, Pharmacists, FLWs
Objective: Instil key programme and project planning techniques
Training Components • Introduction to project cycle management
• Project identification & formulation
• Approaches to project planning
• Participatory techniques
• Stakeholder analysis and interventions
• Working with the Logical Framework Approach
• Project documentation and reporting, Effective report writing
• Analysis of numerical data
• Contingency plans
• Work plans (1-3 months), Operational plans (6-12 months)
Competencies Developed
Competency 1: Strategic and coordinated planning, monitoring, reporting
Mode of Delivery Workshop, Self-instructional material/Brochure
Training Duration (No. of Days)
5
Frequency of Training
Annual

56 Capacity Building & Training Strategy
Table 2.5b:: Communication, and Liasoning Skills
• Uses appropriate grammar and language when communicating with others.
• Break down explanations of complex processes, rules into everyday situations to
engage listeners.
• Speak at an appropriate speed, volume, tone and pitch to communicate the idea
effectively to the audience.
• Connecting with stakeholders to nurture relationships over time to build trust
and to develop a basis for future interactions.
Competencies
Developed Competency 2: Effective communication and liasoning
Mode of Delivery Workshop Training and Self-Instructional material
Training Duration (No.
of Days) 5
Frequency of Training Workshop (Nos.1)
Table 2.5c: Leadership, Motivation and Teamwork Skills
Target Groups MOs, Nurses, Pharmacists, ANMs
Objective: Provide skills and techniques to develop team, increase motivation, manage organizational change, and understand and communicate with people
Training Components:
• Management and leadership (and their difference)
• Leadership styles: from vision to implementation
• Developing, communicating and implementing the vision-building capability
• Matching staff capability to facility needs
• Influencing skills and techniques
• Matching influencing to target audience
• Building trust
• Building and sustaining high performing teams
• Managing change effectively
• Introducing and sustaining organizational change effectively
• Action Planning
Competencies
Developed Competency 5: Self-Management
Mode of Delivery Workshop Training, Self-instructional Material
Training Duration (No.
of Days) 4 Days
Frequency of Training Workshop (Nos.1)

57 Capacity Building & Training Strategy
Table 2.5d: Medico-Legal Practices
Target Groups MOs, Nurses, Pharmacists, ANMs
Objective: Instil basic programme and project planning techniques
Training Components
• Reporting of accidents and police cases
• Medico Legal examination
• Post mortem examination guidelines (Rules for CMOs, Directions for preserving and packing Viscera, etc.)
• Instructions for the guidance of MOs regarding Medico Legal Work and Expert
Professional Opinion
• Medical negligence Syn. Mal Practice
• Contractual relation between Doctor and Patient
• Preparation of medico legal reports in different situation and police formalities
• Issuing Death Certificate
Competencies
Developed Competency 6: Medico-legal Practice
Mode of Delivery Self-instruction/webinar
Training Duration
(No. of Days) 3
Table 2.5e : Biomedical Waste Management & Infection Control
Target Groups MOs, Nurses, Pharmacists, Medical Technicians, FLWs, GDA
Objective: Instil techniques and protocols for biomedical waste management
Training Components
• Improving Hospital/Facility Upkeep
• Improving Sanitation and Hygiene
• Improving waste Management
• Infection Control
• Hospital Support Services
• Hygiene Promotion
Competencies
Developed Competency 7: Biomedical Waste Management & Infection Control
Mode of Delivery Workshop, self-instructional manual (NHM-`Kayakalp’ Implementation Manual)
Training Duration
(No. of Days) 4

58 Capacity Building & Training Strategy
Table 2.5f: Quality Assurance
Target Groups MOs, Nurses, Pharmacists, Medical Technicians, FLWs, GDA
Objective: Instil knowledge of QA protocols and procedures
Training Components
• Understanding Quality Assurance
• Framework of Quality of Care (QoC)
• The Organisational Structures
• The Process of Implementation
• The Process of Implementation
Competencies
Developed Competency 9: Quality Assurance
Mode of Delivery Self-instructional manual (NHM; Operational Guidelines for QA in public health facilities)
& workshop
Training Duration
(No. of Days)
4
Table 2.g: Disaster Preparedness & Response
Target Groups MOs, Nurses, Pharmacists, Medical Technicians, FLWs, GDA
Objective: Instil basic programme and project planning techniques
Training Components
• Types of Disasters
• Phases of Disaster Management
• Key Components of effective emergency management plan
• State Emergency Management Authority & Executive Committee
• Obligation of Health Department as per clause 30 of the Disaster Management
Act
• Development of Disaster Management Plan by Health Department under
section 40 of the Act
• Preparing Disaster Response Plan
• Preparedness Checklist for public health department
Competencies
Developed Competency 8: Disaster Preparedness, Management & Response
Mode of Delivery Workshop
Training Duration
(No. of Days) 2
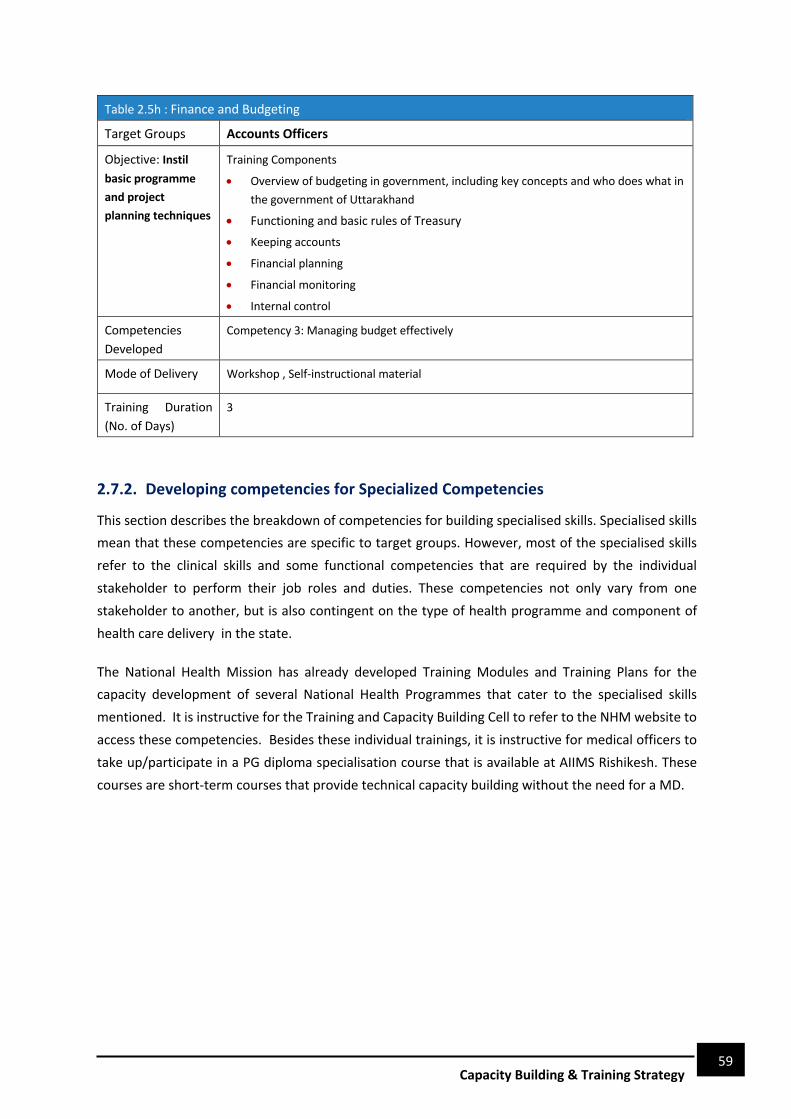
59 Capacity Building & Training Strategy
Table 2.5h : Finance and Budgeting
Target Groups Accounts Officers
Objective: Instil basic programme and project planning techniques
Training Components
• Overview of budgeting in government, including key concepts and who does what in
the government of Uttarakhand
• Functioning and basic rules of Treasury
• Keeping accounts
• Financial planning
• Financial monitoring
• Internal control
Competencies
Developed Competency 3: Managing budget effectively
Mode of Delivery Workshop , Self-instructional material
Training Duration
(No. of Days)
3
2.7.2. Developing competencies for Specialized Competencies
This section describes the breakdown of competencies for building specialised skills. Specialised skills
mean that these competencies are specific to target groups. However, most of the specialised skills
refer to the clinical skills and some functional competencies that are required by the individual
stakeholder to perform their job roles and duties. These competencies not only vary from one
stakeholder to another, but is also contingent on the type of health programme and component of
health care delivery in the state.
The National Health Mission has already developed Training Modules and Training Plans for the
capacity development of several National Health Programmes that cater to the specialised skills
mentioned. It is instructive for the Training and Capacity Building Cell to refer to the NHM website to
access these competencies. Besides these individual trainings, it is instructive for medical officers to
take up/participate in a PG diploma specialisation course that is available at AIIMS Rishikesh. These
courses are short-term courses that provide technical capacity building without the need for a MD.

60 Capacity Building & Training Strategy
Capacity Building & Training Plan
The previous sections described a framework for the different capacity building and training activities
that will serve to address the capacity gaps of the different target groups. This section will lay out a
structural framework for implementation or roll out of the Training suggested in the previous sections.
The implementation framework will be broken down according to the following categories of capacity
development (i) Individual; (ii) System Strengthening & Processes; (iii) Enabling Environment. 3.1. Individual Capacity Development Plan
We have already argued that individual competencies and attitudes form an integral part of the overall
capacity of the health staff of the Department of Health in Uttarakhand.
It is instructive to plan for and provide refresher trainings on some aspects
of the project (especially for the grassroot level staff) and also support the
enhancement of certain identified skills that are instrumental to the
smooth planning and implementation of the project. Here we have laid
out a plan for the organization of the activities suggest for capacity
building and training of the staff in two broad categories: (i) Induction Training for new recruits; (Ii) In-service Training for all health cadres that includes orientation trainings as well as refresher trainings -
• Induction Training: At the time of entry into service, Induction Training must be made mandatory
for newly joined staff across all categories of health care workers. This must have components of
requisite skill enhancement, management and knowledge about the drugs/equipment and
services as well as management, planning and financial planning offered at all levels of health
care. This must be completed in a fixed time frame. The Induction training course curriculum must
be developed at the state level based on the framework provided by the foundation courses
prepared & developed in Uttar Pradesh. It may be instructive to revise and update this curriculum
to align with current health needs, learning gaps and responsibilities.
A draft curriculum for medical officers is attached in the annexure 5. The proposed duration of
induction/orientation training for different stakeholder categories are given below.
Table 3.1 : Proposed Training duration for different stakeholder categories
SN Stakeholder Duration of Induction Training
1. Medical 14 Days
2. Administrative (including Procurement &
Finance) at State, District & Block Level
5 Days
3. Paramedical 7 Days
3

61 Capacity Building & Training Strategy
Table 3.1 : Proposed Training duration for different stakeholder categories
SN Stakeholder Duration of Induction Training
4. Outreach workers 5 Days
5. General Duty Attendants 3 Days
• In-service Training: In-service Training is the major component of training. As refresher training
or Continuous Professional Education, it must be provided to all categories of health care workers
to upgrade their knowledge and skills in technical and management fields at least once every two
years or earlier based on the capacity development need. Based on the capacity development
activities outlined in Section 2.5, a draft training and capacity building plan is described below.
It is instructive to remember that the CB&T plan is designed as a State Level framework. It is
supposed to serve as a rubric for respective district level training cells to prepare district level
training plan as trainings will take place at the district level. A tentative list of Training venues is
also given in the Annexure IV.
Table 3.2: Core competency Trainings
SN Types of Training
Category Durati
on (Days)
Batch Size
Venue Mode of Training
Responsibility
1
1
.
.
1.
Strategic and Coordinated Management, Monitoring, Reporting, HR management
Orientation
Training State PMU, MOs, DPMs,
Nurses, Pharmacists,
FLWs
5 30 Region
al Level
Classroo
m
District Training
Coordinator
/DPMU
Refresher
Training 2 30
District
/ Block Level
Self/
Manual/
E-module
2
Communication, and Liasoning Skills
Orientation
Training MO, Nurse, Technician, Pharmacist,
FLWS, ASHAs
5 30
District
/ Block Level
Classroo
m
District Training
Coordinator/DPM
U
Refresher
Training 2 30
strict/
Block Level
Self/
Manual/E-
module
4. 3
.v
3.
Leadership, Motivation and Teamwork Skills
Orientation
Training
MO, Nurse, Technician, Pharmacist,
4 30
District
/
Block
Level
Classroo
m
District Training
Coordina

62 Capacity Building & Training Strategy
Refresher
Training
FLWS, ASHAs
2 30
District
/
Block Level
Self/
Manual/
E-module
tor
/DPMU
5. 2
.
25.
4.
Medico-Legal & Ethics
Orientation
Training MOs, Nurses,
Pharmacists, Medical
Technicians
3 30
District
/
Block Level
Classroo
m
District Training Coordina
tor /DPMU
Refresher
Training 1 30
District
/
Block Level
Self/
Manual/E-
module
6.
5.
Biomedical Waste Management & Infection Control
Orientation
Training MOs,
Nurses, Pharmacist,
Medical Technicians, FLWs, GDA
4 30
District
/
Block Level
Classroo
m
District Training
Coordinator
/DPMU Refresher
Training 2 30
District
/
Block Level
Self/
Manual/E-
module
7. 7
6.
Quality Assurance
Orientation
Training MOs,
Nurses, Pharmacist,
Medical Technicians, FLWs, GDA
4 30
District
/
Block Level
Classroo
m
District
Training Coordina
tor
/DPMU
Refresher
Training 2 30
District
/
Block Level
Self/
Manual/
E-module
7.
Disaster Preparedness & Response
Orientation
Training MOs,
Nurses, Pharmacists
, Medical Technicians, FLWs, GDA
3 30
District
/
Block Level
Classroo
m
District
Training Coordina
tor
/DPMU
8.
Refresher
Training
1 30
District
/
Block Level
Self/
Manual/E-
module

63 Capacity Building & Training Strategy
9.
Finance and Budgeting
Orientation
Training
MOs,
Nurses,
3 30
District
/
Block
Level
Classroo
m
District
Training Coordina
tor
/DPMU
Refresher
Training
1 30
District
/
Block
Level
Self/
Manual/ E-
module
With regard to the specialized competency skills, it is advisable for the State and District level capacity
development staff or cells to refer to the existing training strategy by NHM to prepare State and
District level Training Plans. Refer to the Annexure III for the Strategy for RCH-II and National Health
Programmes Training Strategy.
3.2. Capacity Development: System Strengthening & Processes
Along with individual competencies, the organisational environment plays
a critical role in serving as enablers or barriers in allowing the individual
staff members to perform their roles and responsibilities in a systematic
and smooth manner, and therefore achieve organisational and
institutional change. The lack of good working conditions at the facility
level, very restrictive HR rules and regulations, or the pace of the project
with little visible outputs can impede performance by creating discontent
and lower the motivation of the staff. The table 3.2 given below outlines some initiatives that should
be taken to improve the facility-level capacity of the Department of Health & Family Welfare, Govt. of
Uttarakhand –
Table 3.3 : Capacity development Initiatives at the Organisational Level
SN Capacity development initiative Stakeholder Responsible
1. Regularly conducting weekly staff meetings at the facility, headed by
the head of the facility, will ensure better communication & support
between colleagues. The minutes of these weekly meetings should
be recorded and documented by the staff.
Head of Facility or MO I/C
2. Fortnightly district-level meetings with the MO-I/C
Head of Facility or MO I/C &
CMO
3. Grievance redressal box for those wishing to submit grievances
anonymously should be provided for and addressed at weekly
meetings
Respective Cells of the SPIU

64 Capacity Building & Training Strategy
Table 3.3 : Capacity development Initiatives at the Organisational Level
SN Capacity development initiative Stakeholder Responsible
4. Gender-sensitive strategies at the workplace may further raise the
motivation levels of staff
Head of Facility or MO I/C &
CMO & DPM
5. The facility must ensure adequate supplies and infrastructure.
Head of Facility or MO I/C &
CMO & DPM
6. Well-defined and targeted HR policies can help reduce turnover and
address acute workforce shortage. This includes keeping track of
workforce details (skills, experiences, certifications), attendance,
trainings attended. This data will be shared in the MIS at the District
level.
Head of Facility or MO I/C &
CMO & DPM
7. Quarterly performance appraisals should be conducted by the head
of the facility. Inputs from the Performance appraisals should feed
into development of district action plans for Capacity building.
Head of Facility or MO I/C,
DPM & CMO
8. Peer reviews will be co-terminus with the quarterly performance
appraisals to receive input from colleagues as well as supervisors.
Inputs from peer reviews should feed into development of district
action plans for Capacity building.
Head of Facility or MO I/C,
DPM & CMO
9. Third Party Quality Audits should be conducted every six-months. Head of Facility or MO I/C,
DPM & CMO
10. Pre and Post Training Tests & Feedback
Head of Facility or MO I/C,
DPM & District Training
Nodal Officer
11. Non-monetary and monetary incentives for those performing well
after performance appraisal or trainings.
Head of Facility or MO I/C,
DPM & District Training
Nodal Officer
12. Action against those not attending trainings after due process
Head of Facility or MO I/C,
DPM & District Training
Nodal Officer
13. Regular Liasoning with PRI members, WCD/ICDS Dept. to collaborate
and ensure smooth implementation of services.
Head of Facility or MO I/C,
DPM & CMO
3.3. Enabling Environment Development Plan
An important aspect of the capacity development is the sustainability of the
trainings provided and/or any organisational changes made. Sustainability can
only be ensured when there is an enabling environment that supports the
transfer of knowledge within the organization, upgradation of skills and

65 Capacity Building & Training Strategy
knowledge and also creates and maintains a positive atmosphere for the cultivation, sharing and
enhancement of this knowledge.
Table 3.4: Capacity development Initiatives to Strengthen Enabling Environment
SN Capacity development initiative Conducted by
State-Level
1. • Commitment for mainstreaming Capacity development in
State Policy. Development of strategic framework that will be
converted into detailed district level training plans.
Project Director, UKHSDP,
Director, HSS & State
Training Coordinator/Cell
2. • Dedicated cadre of professionals to plan and implement
training – State CB&T cell
Director, HSS & State
Training Coordinator/Cell
3.
• Digital Platform for Capacity Building & Training. This should
include HR and Performance System that contains a database
of workforce with personal details including age, qualifications
experience etc along with the skills, certifications, trainings
attended. Should be linked to HMIS.
Director, HSS & State
Training Coordinator/Cell
4 • The digital platform should contain training curricula along
with pre-existing ones developed by NHM, DHFW, and other
training institutions. It should also have annotated digital
library with downloadable learning material and e-modules
available for reference of Health Staff.
Director, HSS & State
Training Coordinator/Cell
5. • Develop and upgrading training institutes by providing
requisite equipment & ICT Infrastructure. It is also instructive
to restock physical libraries with updated reference books and
journals. Special focus is required to operationalise the SIFHW
Director, HSS & State
Training Coordinator/Cell
District-Level
6 • Annual District Training plans will be prepared with the time-
frame for the trainings based on the State Strategy
District Training
Coordinator
7 • District Training Plan will include the plan for monitoring the
quality of training and also the utilisation of trained personnel,
based on the budget provided by the state.
District Training
Coordinator
8. • The total training load should be calculated on the basis of the
health functionaries currently in position and existing
functional health facilities. Batch size to be decided according
to the skills which are to be provided to the health
functionaries and the training venues available.
District Training
Coordinator

66 Capacity Building & Training Strategy
3.4. Human Resource Management & Institutional Roles and Responsibilities
With all the capacity development and training activities laid out in the
previous sections, this section will define the institutional set-up of the
capacity development plan and the various stakeholders that will be engaged
in its implementations along with their respective roles and responsibilities.
The set-up is given below:
Table 3.5 : Human Resource Management in Capacity Development & Training of Health Staff of Uttarakhand Health Department
S. No. Institution(s)/Stakeholder Roles and Responsibilities
STATE/REGIONAL
1. State Nodal Officer
(Project Director, HSS and NHM Director)
• Facilitate in preparing database of training centres and health care
service delivery institutions in all sectors, the training courses offered
and trainee load.
• Planning and implementation of State Training Plan.
• Liaison with State Programme Officer/District Programme Officer,
Director of Training Institution, Medical Colleges and Nursing
Colleges.
• To release funds for Training under UKHSDP component or NRHM.
• Ensure completion of training within a fixed time frame.
• Ensure that each training is synchronized with provision of necessary
supplies and development of referral linkages.
• Ensure that report on training is an integral part of routine reporting
of RCH (as per prescribed format).
• Ensure that training is an agenda item in all meetings with District and
State Officials to discuss programme issues.
• Ensure the linkages of training with operationalisation of health
facilities.
• Build a system for monitoring and evaluation of in-service training
using available training infrastructure in the district.
• Develop a district wise database of trained manpower to prevent
duplication and gaps in training of personnel and perhaps facilitate
their posting in appropriate health facility.
2. State Level Training
Institutions3
• Identification of training centres and hospitals for various types of
training based on case load/faculty position.
• Assist the state in listing training centres and health care service
delivery institutions in all sectors (district-wise), the services provided
in these and the case load.
3 Yet to be formed. Meanwhile the regional/divisional training institute such as in Haldwani can perform this function.

67 Capacity Building & Training Strategy
Table 3.5 : Human Resource Management in Capacity Development & Training of Health Staff of Uttarakhand Health Department
S. No. Institution(s)/Stakeholder Roles and Responsibilities • Assist the state government and provide guidance to the districts in
preparation of district training plans in accordance with the state and
national guidelines and strategy such that health facilities with skilled
manpower could be made operational at the earliest.
• Support the state in developing training materials from nodal agency,
adapt/translate and reproduce as per requirement of the state. • Identify training opportunities and institutions within and outside the
state for emerging and critical issues, within and outside the state, at
any point of time.
• Conduct additional research
2. Joint Director, HSS
• Overseeing the development and implementation of all District Action
Plans including trainings.
• Designing systems and procedures for independent feedback
mechanisms for assessing access to and quality of services and
updating of database of trainings.
• Liaison with SIHFW/CTIs, State Programme Officers and District
Programme Officers.
• Monitoring appropriate utilisation of trained personnel.
• Ensuring up-to-date data of persons trained and being trained
DISTRICT
6. District Training
Officer
• Prepare a training calendar for the trainings to be conducted in the
district.
• Ensure the proper implementation of district training programme.
• Develop database of personnel and update the same from time to
time.
• Plan implementation and monitoring of trainings at regular intervals
• Ensure that best options be given to the poor people by providing
skills appropriate to the job functions of health personnel and
available facilities in the various institutions.
• Ensure maximum utilisation of resources within the district for
training like ANM schools, district training centres, district hospitals,
sub-district hospitals/FRUs/PHCs/hospitals in other sectors.
• Procure adequate funds, modules and materials from the State/
Central Government.
• Ensure training of trainers of district in consultation with the State
Government/State Training Institution.
• Ensure completion of training within a time frame

68 Capacity Building & Training Strategy
Table 3.5 : Human Resource Management in Capacity Development & Training of Health Staff of Uttarakhand Health Department
S. No. Institution(s)/Stakeholder Roles and Responsibilities • The district level trainer will use and interpret standardized training
material and ensure appropriate skill upgradation.
7. District Programme
Manager (DPM)
• Assist DMO in preparing work plans.
• Create and maintain district resource database for the health sector.
• Procurement of supplies, logistics and inventory management to
dovetail with training.
• Develop strategies/plan to improve the quality of services.
• Liasion links with SIHFW, State Programme Officers and District
Programme Officers.
8. District Training
Officer/Coordinator
• Assist DPM in preparing training work plans.
• Create and maintain district resource database for trainings and link
with HMiS
• Create and maintain district resource database for workforce to
record status of trainings
• With DPM, maintain district resource database of performance
appraisal and internal competency evaluations
• Record pre-post training assessment data
• Procurement of supplies, logistics and inventory management to
dovetail with training.
• Develop strategies/plan to improve the quality of trainings services.
• Liasion links with SIHFW, State Programme Officers and District
Programme Officers.
3.5. Quality Assurance and Training Management
The key processes and measures that should be followed during the implementation of the training
are described below:
3.5.1 Pre-Training Activities
Training needs assessment carried out should inform the preparation of a training plan. While the
existing training needs assessment focused on non-clinical aspects of health care service delivery, it
has considered the capacities required to address or strengthen the IMR/MMR/TFR/ Disease
prevalence of the state and its linkage with plan for making its facilities operational. It will be more
appropriate to have district specific training needs which will help in prioritizing the training activities
needed in the particular district. This should include the following:

69 Capacity Building & Training Strategy
• Identification of Training institutes: Essential infrastructure required for training to be made
available in the training institutes and attached hospitals. Identified centres for training shall have
adequate infrastructure, availability of trained trainers and case load for training.
• Identification of Faculty for training: Besides the trainers at the respective training institutes, it is
instructive to identify resources who will serve as trainers for the trainings. This may include
retired medical professionals, faculty at training institutes from within and outside the state.
• Trainees and Training Load: Identification of categories of trainees and types of training.
• Adequate external capacity: Supplies, equipment and drugs required for trainings should be
made available continuously with interruptions.
• Adequate Training material: Training manuals for trainers and training. Kits for trainees should
be prepared and ready. The training material for RCH–II has already been provided.
3.5.2 During Training Activities
• Cascading model of Trainings: Health personnel at each level will be trained by personnel of one
level above them/team leader/supervisor.
• District-level Trainings: The training of primary health care functionaries eg. frontline health
workers, ASHA, lab technicians, pharmacist etc. should be at the district level.
• Residential Trainings: Residential facilities including basic amenities in the hospitals and transport
facilities for field visit need to be provided.
• Practical Skills- The trainers conducting trainings should be practicing the skills as per protocols
which are to be taught to trainees. Necessary supplies need to be continuously provided in
training institutions.
• Regular monitoring/assessment of skills: Assessment of skills should be done by the immediate
supervisor (PHC MO) and also by the functionaries of FRUs/District hospitals (appropriateness and
timeliness of referral. This needs to be collated at district level for identification of lacunae and
appropriate correction).
• Proficiency certification of Training: Proficiency certification of trainees by the trainers based on
norms (whether the trainee has acquired the skills) should be mandatory. The proficiency
certificate should be validated after assessing performance at the place of posting over a period
of 6-12 months after the training.
• Monitoring: Regular monitoring needs to be done for assessing extent of adherence to norms as
per course reports.
3.5.3 Post-Training Activities
• Database of trained personnel should be maintained at state/district level.

70 Capacity Building & Training Strategy
• Follow-up of trained professional to assess extent of service utilization of skills is essential. This
may be done by Master Trainers at the district level or block programme managers at the block
level to assess the extent of the effectiveness of the trainings.
• Mentoring as a mechanism, of supportive supervision and handholding for bringing attitudinal
change in health care providers, needs to be restored. Team leaders need to be provided with
skills for mentoring and supportive supervision on the job. These will include proficiency in
technical skills and ability to observe and identify mistakes and correct them after six-months of
the training.
• After each training cycle the outcome of the training should be evaluated at the field level in terms
of improvement of service delivery.
3.5.4 Quality Assurance Committee (QAC)
Quality assurance means maintaining high quality of health care by constantly measuring the
effectiveness of the organization that provide it. As per the Operational Guidelines (2013) for Quality
Assurance in Public Health Facilities issued by MoHFW, Quality Assurance Committees in the State at
State, District & District Hospital Level need to be set up to ensure that standards for various Health
Care Services / facilities as laid down by the GOI are being followed.
3.5.5 Budgetary Considerations
A tentative budget has been drawn up at a stakeholder level for different trainings. It is instructive to
understand that this is not an annual budget but a stakeholder and training-wise budget that may be
spread across the different years. A detailed budget with training wise cost break-up can be found in
Annexure VI.
Table 3.6 : Tentative Budget for Trainings SN Stakeholder Budget 1 Medical Officers 32,78,70,194
2 Pharmacist 41,95,36,783
3 Nurses 7,07,26,206
4 Technicians 1,86,23,280
5 FLW 6,54,99,280
6 GDA 2,74,20,867
TOTAL 92,96,76,610

71 Capacity Building & Training Strategy
Monitoring & Evaluation Framework
4.1. Introduction & Rationale for M&E
The success of the implementation of UKHSDP relies on various factors, particularly the capacity of
the staff charged with the responsibility of designing, planning, and managing the implementation of
the project. To support the process of state-wide system strengthening and implementation of
UKHSDP, a need emerged to identify critical and functional gaps in the service providers involved in
this project. Capacity Building and Training interventions will be designed to address the capacity gaps
as laid out in the Capacity Building and Training Strategy & Plan.
Regular monitoring and evaluation of the campaign can strengthen the effectiveness of the Capacity Building interventions. Period tracking of the training plan is critical to build a compelling evidence
base which can be used to support the CB&T campaign – not only to ensure effective utilisation of
resources, but in a larger context to improve the staff’s ability to strengthen the implementation and
management of the UKHSDP, viz-a-viz improving overall health outcomes by improving the individual
competency through developing knowledge, skills and attitude. This is not an easy task because of
multiple reasons such as the sheer number of health staff that would constitute as the trainees and
the difficulty in measuring performance in the governance and management.
Here, a monitoring and evaluation framework will support in building institutional capacity and
strengthen the existing training and capacity building efforts for this project. The technical support in
this regard, is aimed at enabling the institution and key stakeholders carry out the activities with
informed evidence based planning yielding better results. The activities proposed under this partnership seeks to make a long-lasting and sustainable impact at three levels described ahead.
Level 1: Enabling Environment/Policies & Guidelines: The support activities proposed under this
partnership will seek to develop data and evidence for advocating quality improvements in the
existing policies and guidelines that influence the implementation of varied training interventions
being carried out. The project attempts to ensure sustainability of results by – ensuring that the
concerned departments have comprehensive programme and district specific data that can help them
make informed policy decisions that will guide future plans and interventions of the Project.
• Developing benchmark indicators that will help set goals and assess progress of training
interventions/activities in the future.
• Demonstrating certain best practices in management and learning.
4

72 Capacity Building & Training Strategy
Level 2: Organisation/ Systems And Procedures: The support offered during the project period will
have sustainable impact on the systems & procedures by –
• Building the capacities of concerned officials and key functionaries for planning, implementing
and monitoring project interventions in a better way.
• Facilitating hierarchical and interdepartmental convergence, and ensuring that the concerned
stakeholders also develop the ability to continue such efforts in future as well.
LEVEL 3: INDIVIDUAL CAPACITY : While working to develop the individual capacities of the staff, the
project will have brought certain changes. The project will seek to ensure that –
• The staff members are better informed not only about technical knowledge but also about their
roles and responsibilities, obligations and are empowered to demand better services.
• The individual develops the ability to undertake cohesive and collective action for bringing about
quality changes in the management of the healthcare service provision in the state.
• Some of staff members may develop into becoming harbingers of change influencing adoption
of desired health seeking behaviour among masses.
Establishing and instituting a Monitoring and Evaluation Framework will support the efforts to ensure that the communication intervention is able to leave behind lessons and capabilities that will continue to bring about positive changes in future as well.
4.2. Objectives of M&E Framework
Overall, this primary objective of the monitoring and evaluation framework described in this
document is to help the state program team spearheading the implementation of health care delivery
by strengthening routine M&E of the training and system strengthening activities. A framework for
this exercise described in this document will more specifically help:
E Develop comprehensive M&E plans in parallel with CB&T intervention planning.
E Utilize a strategic and practical mix of M&E methods to design, implement, and assess the
outcomes of CB&T activities.
E Systematically apply results of M&E to adapt and improve the performance of CB&T
interventions.
4.3. Target Users of M&E Framework
The M&E framework is at the overall level for the state and not micro-level monitoring and evaluation
of a single training programme/event. Therefore, formats will need to be developed for reporting units
at regional/district/block/trainer levels as appropriate when the detailed M&E system is
operationalized.

73 Capacity Building & Training Strategy
This guiding document is envisaged to be utilised by the state for the monitoring of the CB&T and
evaluate the impacts that can be attributed to CB&T initiatives of the project. The users of this
document will include:
• State Capacity Building and Training Cell/Staff
• District level Training officers
• Technical partners/Service Providers who are providing support in the design and implementation
of the UKHSDP activities
4.4. Guidelines for M&E framework
The guiding principles that will frame and inform the process of monitoring and evaluation of the
Capacity Building and Training Activities of UKHSDP are described below: -
• Performance-Oriented’ Approach instead of `Output-Oriented’
Traditional Monitoring and Evaluation exercises were focused on input-output. However, the
approach was not observed to be adequate to generate result-oriented information and does not
guarantee or capture results/outcomes nor does it any provide any information on the value for
money spent on training activities. The following document outlines a performance-oriented
planning framework that will be result-oriented and robust outcome-based M&E.
• Systems Approach to assess effectiveness of CB&T interventions; Looking beyond `individual’
The outcomes and impacts are influenced not only by the outputs (and inputs) but are subject to
many external influences and factors. However, it is important to make it clear to what extent the
planned CB&T interventions’ outputs have contributed to the outcomes/impact, i.e., trainings and
institutional changes have lent to strengthening health systems, improving health facility access
and utilization and ultimately the health outcomes in the state.
• Comprehensive & Uniform Reporting of CB&T across the state
A comprehensive strategy that monitors all the CB&T across the state and not just a single training
programme and intervention is required currently. Moreover, regular data in terms of coverage,
expenditures, utilization certificates and future needs of funds should be reported to the state. It
is important to compile information received from across the state according to standard
definitions of performance indicators across states/UTs, M&E systems currently are utilized
largely for the purpose of reporting rather than as a system for providing feedback on and
strengthening implementation.
• M&E should be embedded in the CB&T programme cycle
M&E should not be a retrospective exercise and should be embedded in the Capacity Building and
Training cycle that is designed to address the capacity needs of the project staff.

74 Capacity Building & Training Strategy
4.5. Key Evaluation Questions & Logframe
The figure 4.1 below comprises the “Theory of Change’, i.e. the major steps of a capacity
building/training cycle with major externalities. This framework informs the design of the monitoring
and evaluation activities to track the progress of the CB&T activities and the Key Evaluation Questions
are the high-level questions that the M&E activities will attempt to address.
Figure 4.1 : Analytical Model of the CB&T
Table 4.1 : Logframe for CB&T interventions
S.N Stage Key Evaluation
Question Indicators
Means of Verification
1.
Planning for CB&T
(INPUT)
Are the CB&T interventions suited to address the capacity gaps?
• CB&T Strategy & Policy
Development
• CB&T Monitoring
Framework
• CB&T Training Needs
Assessment & Baseline
Evaluation
Desk Review of
MIS & Project
Reports
EXTERNALITIES
CB&T Planning
Individual Learning
CB&T Implementa
tion
Organisational Performance &
Health Outcomes
INPUT OUPUT OUTCOME IMPACT
Training Reaction
Social Environment
Individual Learning Capacity
Organisational Environment

75 Capacity Building & Training Strategy
Table 4.1 : Logframe for CB&T interventions
S.N Stage Key Evaluation
Question Indicators
Means of Verification
• Module & Material
design and
Development
• CB&T planning including
resources (facilities,
service providers,
infrastructure, funds)
• CB&T budgeting
• ToT development
• Resources development
(faculties selection,
ToTs)
• Micro Planning and
scheduling
2.
CB&T
Implementation
(PROCESS/OUTPUT)
To what extent is the
relationship between
the inputs-outputs
timely, cost-effective
and to expected
standards?
(INPUT-OUTPUT MONITORING)
• No. of self-instruction
materials prepared
• No. of modules
prepared for training
• No. of Training batches
• Payments and
Accounting
• No. of CB activities
organized and
operationalized
• No. of Trainers
• Participant attendance
in trainings/CB events
(%)
• % of participants
covered under various
CB activities
• Desk Review
of MIS &
Project
Reports
3.
Training Reaction
(OUTPUT)
To what extent is the
program producing
worthwhile results
(outputs, outcomes),
and/or meeting each of
its objectives?
End of training/Post-Test
evaluation on
- Trainer
- Content
- Presentation
Pre-Post Test
evaluation &
Trainer
Observations

76 Capacity Building & Training Strategy
Table 4.1 : Logframe for CB&T interventions
S.N Stage Key Evaluation
Question Indicators
Means of Verification
(INPUT-OUTPUT EVALUATION
- Training
Arrangements
4.
Individual
Performance
(OUTCOME)
To what extent is the
program achieving the
intended outcomes, in
the short, medium and
long-term?
(OUTCOME-IMPACT EVALUATION).
• Increase in knowledge,
attitude and skills/
behavior regarding
responsibilities and
functions of the
individual staff and
therefore functioning of
the
• Sample
Survey and
Training
Needs
Assessment
for baseline
• Training
Needs
Assessment
Report
5.
Organisational
Performance
(IMPACT)
• Changes in efficiency,
effectiveness,
timeliness, in
functioning and
achievement of
outcomes,
6.
Externalities/
Institutional
Capacity
(ENABLING ENVIRONMENT)
• Learning Capacity (Ability to
absorb the inputs provided
through the CB&T)
• Facilitation/Support of
state government
functionaries and other
local level government
functionaries
• Extent of peer learning and
support
• Infrastructure:
Building/space, computers,
furniture, connectivity,
availability of varied
information and databases
• Political Will of the state
level unit
• Timely and adequate fund
flows
•

77 Capacity Building & Training Strategy
4.6. Methodology and Work Plan
To accurately capture, analyze and report data on the indicators mentioned in table above. Reporting
on these indicators may be done on paper, although using web-enabled software with the help of IT
or IT-enabled technology. This data may be captured using the following methods and techniques:
Table 4.2: Modalities of Reporting and Data Collection Monitoring
SN Indicator/Parameter Purpose/Objective Frequency Source of
Verification/Assessment
1
Training Strategy &
Plan
To assess the relevance of
Training Strategy & Plan
Annual • Capacity Building and
Training Strategy
Document
• Proof of
operationalization of
CB&T– annual report of
the program, contracts,
monitoring reports, etc.
2.
Training
Institutional
Arrangement
To assess the adequacy of the
Training Institutional
Arrangement
Annual • Proof of
operationalization of
CB&T– annual report of
the program, contracts,
monitoring reports, etc.
3. Training Needs
Assessment
To assess the adequacy of the
Training Institutional
Arrangement
Annual • Training Needs
Assessment Report
4 Module Design
Development
To assess the relevance,
effectiveness and adequacy of
the Training Institutional
Arrangement
Quarterly • Capacity Building and
Training Strategy
Document
• Training Modules
developed by the
Centre/State
• Experiential learning
aids designed in the
modules provided by
the state
5
Micro-Planning To assess the adequacy of the
Training Institutional
Arrangement
Quarterly • Proof of
operationalization of
CB&T– annual report of
the program, contracts,
monitoring reports, etc.

78 Capacity Building & Training Strategy
Table 4.2: Modalities of Reporting and Data Collection Monitoring
SN Indicator/Parameter Purpose/Objective Frequency Source of
Verification/Assessment
6
Budgeting & Cash
Flow
To assess the adequacy of the
Training Institutional
Arrangement
Quarterly • Proof of
operationalization of
CB&T– annual report of
the program, contracts,
monitoring reports, etc.
7
Training Experience To assess the adequacy of the
Training Institutional
Arrangement
Quarterly • Feedback forms of
Trainees
• Training Reports
8
Training
Infrastructure
To assess the adequacy of the
Training Institutional
Arrangement
Quarterly • List of Training Venues
• Feedback forms by
Participants
• Photos of Training
Venues
9
HR management of
Capacity Building &
Training
To assess the adequacy of the
Training Institutional
Arrangement
Quarterly • Training Strategy
10 Knowledge
Assessment
To assess the knowledge and
awareness of the health staff
Annual • Sample Survey and
Training Needs
Assessment for
baseline
• Training Needs
Assessment Report
11 Attitude
Assessment
To assess the attitude of the
health staff
Annual
12
Skill
Assessment
To assess the skills of the staff Annual
Outcome/impact evaluation is an exercise that does not have to be conducted frequently since
outcomes and impact is witnessed over longer time periods. Therefore, it is recommended that a
Mixed-Methods study to be carried out annually to track the progress in the achievement of the
outcomes of the CB&T interventions across all the staff in the Department of Health.
Outcome Evaluation: This study evaluates the outcomes of capacity strengthening and competency
development of the staff across knowledge, attitude and skills as outlined in the Table above. A
mixture of qualitative and quantitative techniques will be employed to collect the data. The sample
size and strategy used in the Training Needs Assessment which also serves as the Baseline Evaluation,
may be referred to for subsequent rounds of evaluation.
Impact Evaluation: It would also study its impact on the overall performance of the state of
Uttarakhand in delivering adequate health service. This would be measured by tracking the progress

79 Capacity Building & Training Strategy
of the project in achieving performance outputs as earmarked in the Project Log frame for UKHSDP by
referring to Monitoring Informatics System of the Project.
4.7. M&E Operationalization Plan
With the methodology and brief work plan for the different evaluations described in the previous
sections, this section will illustrate the work plan for finalisation and implementation of the
Monitoring and Evaluation Framework. Monitoring and Evaluation is part of a continuous process of
learning and improvement that enables assessment of the performance of your communications
against the aim and objectives. The broad framework that should be followed for preparing and
implementing an M&E plan is given below.
A framework is provided for developing the operationalization plan of the M&E framework based on
the overall methodology illustrated above.
Set Monitoring aims & Objectives
Identify Activities to be monitored
Develop Indicators
Identify data requirements
Collect Data
Analyze & Evaluate Data
Identify Improvements
Take Action
A
B
C
D
H
E
G
F
Feedback on aims & objectives
CONTINUOUS IMPROVEMENT LOOP

80 Capacity Building & Training Strategy
Table 4.3 : Framework for Developing Operationalization Plan of CB&T M&IE Framework in the state.
TASK RESPONSIBILITY TIMELINE
Finalizing the M&IE framework with State specific modifications M&E Cell & State
CB&T Officer
M1
Formalizing the M&IE Data flow structure and nominating the
functionary responsible for data compilation and reporting at each
level
M&E Cell & State
CB&T Officer
M1
Identifying any additional requirements for operationalizing the
framework, if any
M&E Cell & State
CB&T Officer
M1
Developing reporting formats for Block/district/regional levels M&E Cell M2
Developing data compilation structure in Excel or compatible
software and installing the same at all reporting units M&E Cell
M2
Conducting Training of all Concerned M&E Persons (A training
schedule may be prepared and shared)
M&E Cell & State
CB&T Officer
M3
During the State level ToT Workshops on the M&E Framework, formats will be provided for
developing:
§ Data Flow structure: Reporting Units through which data for M&E systems will flow in the state
§ Training Plan for training of concerned M&E functionaries of the state
§ These formats will be developed as per their need and structure.
4.8 Human Resources for CB&T M&E
The human resources and budget required for carrying out monitoring and impact evaluation will be
drawn from the overall budget of PRI CB&T. We suggest the following Human resources for this
exercise.
Table 4.4 : Details of Human Resource and their responsibilities
SN Institution Designation of
Stakeholder Roles & Responsibilities
State
1. Capacity Building &
Training Cell
Training
Coordinator
• Overall supervision of the monitoring and evaluation of
the CB&T intervention.
• Supporting the preparation of templates for process
monitoring.

81 Capacity Building & Training Strategy
Table 4.4 : Details of Human Resource and their responsibilities
SN Institution Designation of Stakeholder Roles & Responsibilities
State
2. MIS and
Monitoring &
Evaluation
Coordinator
• Supporting the supervision of the monitoring and
evaluation of the CB&T intervention, including contract
management of Third-Party Agency.
• Prepare templates and formats for monthly progress
reports and Quarterly Progress Reports for CB&T
activities at state, district and cluster levels.
• Support the development of MIS for program monitoring
along with hired agency.
• Develop and finalise program indicators for tracking
progress of CB&T intervention
supervise and monitor
3. Third Party
Evaluation Coordinator
• Primary responsibility of undertaking M&E activities at
the Central, district and cluster level.
• Support preparation of templates for process monitoring.
• Undertaking quarterly qualitative I/O analysis, outcome
and impact evaluation.
District/Cluster
4. District Training
Officer
Field Level
Coordinator & Data
Monitoring
• Supervise data monitoring of MIS at the cluster level
• Support data collection at the field level
• Provide support to the Third-Party Agency during data
collection
• Support Training of Cluster Level staff in completion of
monitoring formats
5. District Programme
Manager
Field Level
Coordinator & Data
Monitoring
• Ensure data monitoring of formats at the cluster level
• Assist in computerization of data generated during data
validation exercise.
6. Training Officer
CB&T
Field Level
Coordinator & Data
Monitoring
• Ensure data monitoring of formats at the cluster level
• Support data collection at the field level
• Support Training of Cluster Level staff in completion of
monitoring formats

82 Capacity Building & Training Strategy
4.9 Activity Timeline A tentative activity schedule for the Monitoring and Evaluation Activities for the Capacity Building and Training Activities are given below.
Monitoring & Evaluation
2019 2020 2021
Quarter 1 Quarter 2 Quarter 3 Quarter 4 Quarter 5 Quarter 5 Quarter 6 Quarter 7 Quarter 8
May June July Aug Sep Oct Nov. Dec. Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov. Dec. Jan Feb Mar Apr May Jun Jul
Output
Monitoring
Weekly MIS
reporting
Training
Reports
Outcome
Evaluation
Training
Reports
which
includes pre-
post training
formats
Outcome-
impact
Evaluation
Field
validation
* * * * *

83 Capacity Building & Training Strategy
ANNEXURE

84 Capacity Building & Training Strategy
Annexure - I
DISTRICT-WISE DISTRIBUTION OF HEALTH FACILITIES
(Source: Department of Medical Health & Family Welfare, Govt. of Uttarakhand, Health Resources -Medical & Paramedical4)
HEALTH FACILITIES IN UTTARAKHAND
Division District SCs PHCs CHCs SDHs DHs
Garhwal
Total Sample Total Sample Total Sample Total Sample Total Sample
Bageshwar 84 9 12 2 2 1 1 1
Pithoragarh 155 16 18 2 4 1 2 1
Almora 206 21 28 3 4 1 2 1 2 1
Champawat 68 7 6 1 2 1 1 1 1 1
Nainital 143 15 19 2 8 1 4 1 2 1
U.S. Nagar 153 16 27 3 6 1 1 1 1 1
Kumaon
Uttarkashi 82 9 10 1 4 1 2 1
Chamoli 110 11 13 2 5 1 1 1
Rudraprayag 68 7 13 2 2 1 1 1
Tehri 204 21 28 3 5 1 1 1 1 1
Pauri 239 24 32 4 5 1 3 1 2 1
Dehradun 175 18 23 3 7 1 4 1 2 1
Haridwar 160 16 28 3 6 1 1 1 2 1
1847 190 257 31 60 13 17 8 20 13
GRAND
TOTAL
TOTAL 2201
SAMPLE 255
4 http://health.uk.gov.in/pages/display/113-human-resource-medical-and-paramedical

85 Capacity Building & Training Strategy
HEALTH CADRE-WISE DISTRIBUTION OF AVAILABLE
HEALTH STAFF & SAMPLE SELECTED
(Source: Department of Medical Health & Family Welfare, Govt. of Uttarakhand, Health Resources -Medical & Paramedical5)
HEALTH STAFF OF DIFFERENT CADRES
SN Staff Position Total Nos in Position* Sample
1 Medical Officer /Lady Medical Officer 825 97
2 Deputy CMO/ Administrative 121 14
3 Super Specialist -
4 Dental Surgeon 39 5
5 Matron/Assistant Matron/Sister-in-charge 21 3
6 Assistant Matron 15 2
7 Sister 143 17
8 Staff Nurse 626 74
9 District Pharmacy Officer 10 1
10 Chief Pharmacist/treatment supervisor 170 20
11 Pharmacist 715 84
12 X-Ray Technician 70 8
13 Dark Room Assistant 32 4
14 BCG Team Leader 4 1
15 BCG Technician 17 2
16 Occupational Therapist /Physiotherapist 6 3
17 Health educator/NHM/Vertical program
counsellor 8 1
18 Dental Hygienist 17 2
19 Senior Lab Technician /SLS -
20 Lab Technician 132 16
21 ECG Technician -
5 http://health.uk.gov.in/pages/display/113-human-resource-medical-and-paramedical

86 Capacity Building & Training Strategy
HEALTH STAFF OF DIFFERENT CADRES
SN Staff Position Total Nos in Position* Sample
22 OT Technician 3 1
23 Health Supervisor (Male)/TB health visitor 417 49
24 Health Supervisor (Female)/TB health
visitor 343 40
25 Female Health worker (ANMs) 1925 227
26 ANM (As per NRHM) 1631 192
27 District Malaria Officer (DMO) District
NVDC Officer/IDSP district epidemiologist 13 2
28 ASHA ~12,000 177
29 Ward Boys 170 20
30 Class 4 Staff 1170 138
TOTAL 8,643 1,024

87 Capacity Building & Training Strategy
Anneuxre-2 YEAR-WISE BUDGET DETAILS
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
Maternal Health Trainings
1 Maternal Death Review 9.43 9.43 9.43 9.43 2.67 2.67
2 Onsite monitoring delivery points /Nursing institutions/ Nursing school 2.6 2.6 2.6 2.6 1.43 1.43
3 TOT for skill Lab 0 0 0 0
4 Training at skill Lab 3.43 3.43 3.43 3.43
5 TOT for SBA 0 0 0 0 9.97 9.97
6 Training of staff Nurses/ ANMs/ LHV in SBA 6.13 6.13 3.83 3.83 9.97 9.97
7 TOT for EMOC 0 0 0 0 7.16 7.16 8 Training of Medical Officer in EMOC 7.58 7.57 0 0 7.16 7.16 9 TOT for Anaesthesia skills training 0 0 0 0 0.32 0.32
10 Training of medical officer in life saving anaesthesia skills 9.62 9.62 0 0 13.94 13.94
11 Training of Medical Officers in ATLS/BLS Trg. 0 0 0 0 4.63 4.63
12 TOT for safe abortion services 0 0 0 0 0 0
13 Training of medical officers in safe abortion 1.44 1.44 0.79 0.79 3.16 3.16
14 TOT for RTI/STI training 0 0 0 0 4.22 4.22
15 Training of laboratory technicians in RTI/STI 0 0 0.98 0.67 0.98 0.98
16 Training on ANM/Staff nurses in RTI/STI 0 0 0.98 0.67
17 Training on Medical Officer in RTI/STI 0 0 1.09 1.08 2.18 2.18 18 TOT for BMOC training 0 0 0 0 0.29 0.29 19 BMOC training for Mos/LMOs 1.4 1.44 1.4 1.4 6.66 6.66 20 DAKSHATA training 9.94 9.94 4.26 4.26 20.62 20.62 21 TOT for DAKSHATA 0 0 0 0 0 0 22 Onsite Monitoring for DAKSHATA 0 0 0 0 0 0 23 Lakshaya training /workshops 13.48 13.48 18.49 18.4
24 Training for Mos/SNs 0 0 0 0
25 Onsite Monitoring at delivery points 0 0 0 0 1.43 1.43
26 Training of Nurse Practitioners in midwifery 19.5 19.5 - -
27 Other maternal health training 0.72 0.72 46.52 30.77 Child Health Trainings
1 IMNCI 0 0 0 0 0 0 2 Orientation on IDCF/ARI (Pneumonia) 6.83 6.82 0 0 13 0

88 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
3 6 weeks training at State Nodal Center
9.72 9.72
4 Orientation on activities on vitamin A supplementation and Anemia Mukta
Bharat Programme 0 0
5 Child Death review training 7.88 7.88 7.88 7.88 0 0
6 Provision for State & District level (Training and workshop) 0 0 0 0
7 TOT on IMNCI (pre service- in service) 0 0 0 0 0 0 8 IMNCI training for AMN/LHVs 0 0 0 0
9 TOT on F-IMNCI 0 0 0 0 0 0 10 F-IMNCI training for Medical Officer 0 0 0 0 0 0 11 F-IMNCI training for Staff Nurse 0 0 0 0 0 0
12 Training on Facility based
management of service acute malnutrition(including refresher)
0 0 1.13 1.12 0 0
13 TOT for NSSK 0 0 0 0 0 0 14 NSSK training for Medical Officers 0 0 0 0 0 0 15 NSSK training for SNs 0 0 0 0 0 0 16 NSSK training for ANMs 0 0 0 0 0 0
17 4 days training for facility based newborn care 0 0 0 0 1.92 1.92
18 2 weeks observer ship for facility based newborn care 0 0 0 0 13.19 13.19
19 4 Days training for IYCF for Mos, SNs, ANMs, all DPs, and SCs 19.5 19.5 0 0 24.5 24.5
20 Orientation on National Deworming Day 44.8 44.8 44.8 44.8 13 13
21 TOT (MO, SN) For family participatory Care (KMC) 0 0 0 0
22 Training for family participatory care (KMC) 4.62 4.62 4.62 4.62
23 New Born Stabilization training
package for Medical Officer and Staff Nurses
0 0 0 0
24 Other Child Health Training 4.62 4.62 0 0 52.61 52.61
25 NRC (Nutritional Rehabilitation Center Training) 0 0 0 0 1.13 1.13
Family Planning Training

89 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
1
Orientation/ review of ANM/AWW as applicable for New Scheme, FP-LMIS, New contraceptives, post-partum and
post abortion, family planning scheme for home delivery of
contraceptive (HDC), Ensuring spacing at birth (ESB{wherever applicable},
pregnancy testing kits(ptk)
4.75 4.75 4.75 4.75 4.18 4.18
2 Dissemination of FP manuals and guidelines (workshop only) 0 0 0 0 0
3 TOT on laparoscopic sterilization 0.42 0.42 0 0 0.3 0.3
4 Laparoscopic sterilization training for doctors (team of doctors, SN and OT
assistant) 0.71 0.71 0.71 0.71 0.71 0.71
5 Refresher training on laparoscopic sterilization 0 0 0 0 0 0
6 TOT on minilap 0 0 0 0 0 0 7 Minilap training for medical officer 0.92 0.92 0.92 0.92 2.77 2.77
8 Refresher training on Minilap Sterilization 0 0 0 0.52 0.52 0.52
TOT on NSV 0 0 0 0 0 0 9 NSV training of Mos 0 0 0 0 0.41 0.41
10 Refresher Training on NSV sterilization 0 0 0 0 0.26 0.26
11 TOT (IUCD insertion training) 0 0 0 0 0 0
12 Training on Medical officer (IUCD insertion training) 1.04 1.04 1.04 1.04 2.07 2.07
13 Training of AYUSH doctors (IUCD insertion training) 0 0 0 0 0 0
14 Training of Nurse (Staff
Nurse/LHV/ANM) (IUCD insertion training)
0.86 0.86 0.86 0.86 0.86 0.86
15 TOT (PPIUCD insertion training) 0 0 0 0 0 0
16 Training of Medical officers (PPIUCD insertion training) 0.5 0.5 0.5 0.5 1.01 1.01
17 Training of AYUSH doctors (PPIUCD insertion training) 0 0 0 0 0 0
18 Training of Nurse (Staff
Nurse/LHV/ANM) (PPIUCD insertion training)
0.44 0.44 0.44 0.44 0.87 0.87
19 Training for post abortion family planning 0 0 0 0 6.55 6.55
20 Training of RMNCH+A/FP Counsellors 1 1 0 0 1.5 1.5

90 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
21 TOT (Injectable Contraceptive Trainings) 0 0 0 0 0 0
22 Training of Medical Officers (injectable Contraceptive Trainings) 0 0 5.56 5.56 5.56 5.56
23 Training of AYUSH Doctors (Injectable Contraceptive Trainings) 0 0 0 0 0 0
24 Training of Nurse (Staff
Nurse/LHV/ANM) (Injectable Contraceptive Trainings)
6.8 5.23 6.8 6.8 6.8 6.8
25 Training of Logistic Personnel on injectable Contraceptive 0 0 0 0 6.8 6.8
26 Oral Pills Trainings 0 0 0 0 0 0
27 Contraceptive update seminar/ meeting 0 0 0 0 1 1
28 FP-LMIS Trainings 2 2 1 1
29 Other Family Planning Trainings 0 0 0 0 Adolescent Health Trainings
1 Dissemination workshop under RKSK 3.5 3.5 1.95 1.95 1.85 1.85
2 TOT for Adolescent friendly Health service Trainings 0 0 0 0 0 0
3 AFHS training of Medical Officers 4.5 4.5 0 0
4 AFHS training of ANM/LHV/MPW 3.44 3.4 0 0
5 Training of AH counsellors 0 0 0 0 1.85 1.85
6 Training of Peer educators (District level) 0 0 0 0 0 0
7 Training of Peer educators (Block level) 0 0 0 0 0 0
8 Training of Peer educators (Sub Block level) 0 0 0 0 0 0
9 WIFS training (District) 0 0 0 0 0 0 10 WIFS training (block) 0 0 0 0 0 0 11 MHS Training (District) 0 0 0 0 0 0 12 MHS Training (block) 0 0 0 0 0 0
Programme Management Training (e.g. M&E, Logistics Management,
HRD, etc.)
1 Training of SPMU Staff 0 0 0 0 12 12 2 Other Training 0 0 0 0 2.6 0
Intensification of School Health Activities
1 Training of Master trainers at district and block level 15 15 0 0 2 0

91 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
2 Training of two nodal teachers per school 0 0 0 0 2 0
3 Any other 0 0 0 0 0 0 Account Training 0 0 0 0 0 0
1 Public Finance Management (PFMS) Training for Accounts personnel 0 0 0 0 2.66 0
RBSK Trainings
1 RBSK Trainings- trainings of mobile
health team-technical and managerial (5 days)
0 0 0 0 24.94 24.94
2 RBSK DEIC Staff Training (15 Days) 0 0 0 0 0 0
3 One Day orientation for MO/ other staff Delivery points (RBSK trainings) 0 0 0 0 0 0
4 Training/ Refresher training - ANM (one day) (RBSK trainings) 0 0 0 0
5 Other RBSK training 0 0 0 0 0 0
Training for Blood Services & Disorder
1 Blood bank/blood storage Unit (BSU) training 6.9 6.9 0 0
2 Training for Haemoglobino-pathies 0 0 5.13 5.12 2.38 0 3 Any other 2.08 2.08 0 0 0 0 Training under NPPCD
1 Training at District Hospital @20rs. Lakh/dist. 0 0 0 0
2 Training of PHC medical officer,
Nurse, Paramedical workers& other health Staff under NPPC
10 10 3.5 3.5
3 Any other 0 0 0 0 Training under NPPCF
1 Training of medical and paramedical personal at district level under NPPCF 7.06 7.06 0 0
2 Any other 15.23 15.23 0 0
Training under Routine Immunization
1 Training under Immunization 30 30 30 30
2 Any other 15.23 15.23 15.23 15.23 Training under IDSP
1 Medical Officer (1 day) 4.34 4.34 4.34 4.34
2 Medical collage doctor (1day) 0 0 0 0
3 Hospital Pharmacists/Nurses Training (1 day) 0 0 0 0
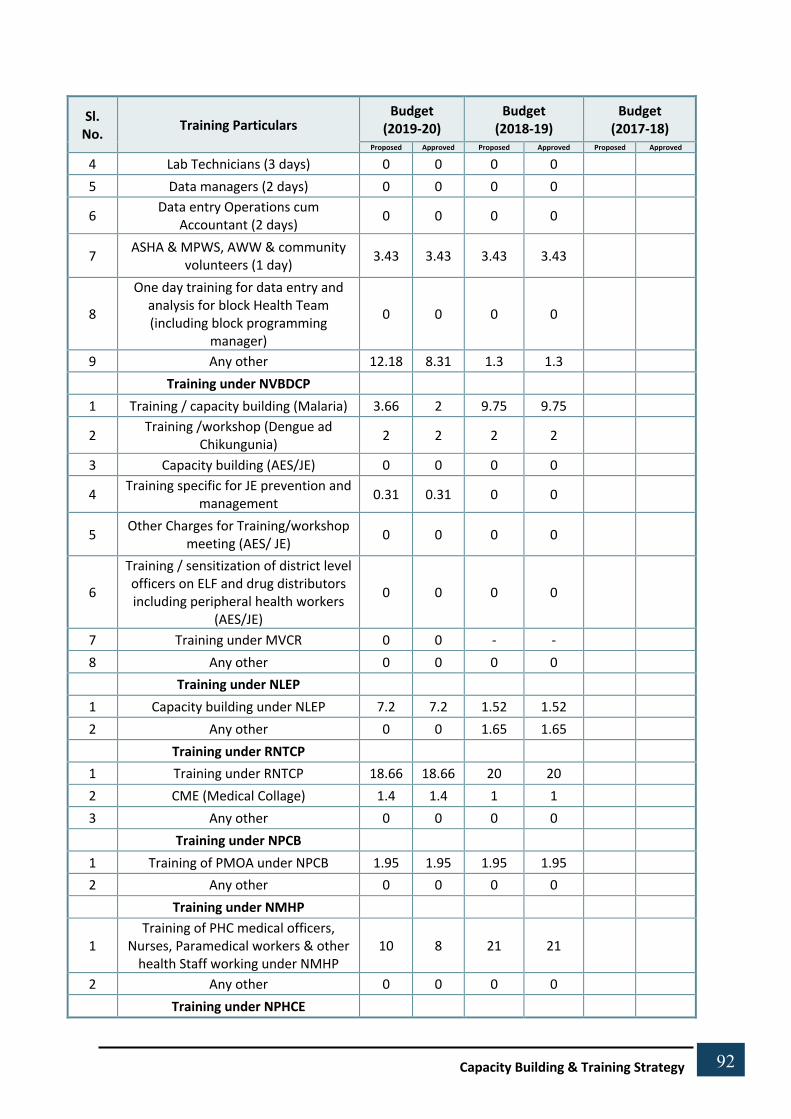
92 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
4 Lab Technicians (3 days) 0 0 0 0
5 Data managers (2 days) 0 0 0 0
6 Data entry Operations cum Accountant (2 days) 0 0 0 0
7 ASHA & MPWS, AWW & community volunteers (1 day) 3.43 3.43 3.43 3.43
8
One day training for data entry and analysis for block Health Team (including block programming
manager)
0 0 0 0
9 Any other 12.18 8.31 1.3 1.3 Training under NVBDCP
1 Training / capacity building (Malaria) 3.66 2 9.75 9.75
2 Training /workshop (Dengue ad Chikungunia) 2 2 2 2
3 Capacity building (AES/JE) 0 0 0 0
4 Training specific for JE prevention and management 0.31 0.31 0 0
5 Other Charges for Training/workshop meeting (AES/ JE) 0 0 0 0
6
Training / sensitization of district level officers on ELF and drug distributors including peripheral health workers
(AES/JE)
0 0 0 0
7 Training under MVCR 0 0 - -
8 Any other 0 0 0 0 Training under NLEP
1 Capacity building under NLEP 7.2 7.2 1.52 1.52
2 Any other 0 0 1.65 1.65 Training under RNTCP
1 Training under RNTCP 18.66 18.66 20 20
2 CME (Medical Collage) 1.4 1.4 1 1
3 Any other 0 0 0 0 Training under NPCB
1 Training of PMOA under NPCB 1.95 1.95 1.95 1.95
2 Any other 0 0 0 0 Training under NMHP
1 Training of PHC medical officers,
Nurses, Paramedical workers & other health Staff working under NMHP
10 8 21 21
2 Any other 0 0 0 0 Training under NPHCE

93 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
1 Training of Doctors and Staff from CHC and PHC under NPHCE 5.25 5.25 4 4
2 Training per CHC under NPHCE 0 0 0 0
3 Training per PHC under NPHCE (IEC to be budgeted) 0 0 0 0
4 Any other 0 0 0 0 Training under NTCP
1 Training for district Tobacco Control Center 5.07 5.07 8.12 8.12
2 Orientation of stakeholder organization 3.25 3.25 7 7
3 Training of Health Professionals 1.17 1.17 0.72 0.72
4 Orientation of Law enforcers 0.65 0.65 0.4 0.4
5 Other training /orientation -sessions incorporated in other trainings 0 0 0 0
Training for State Tobacco Control Centre
1 State Level Advocacy Workshop 1 1 1 1
2 Training of Trainers, Refresher Trainings 0.5 0.5 0.5 0.5
3 Training on Tobacco cessation for health care providers 0.25 0.25 0.5 0.5
4 Law enforces training / sensitization programme 0 0 0 0
5 Any other 0 0 0 0 Training under NPCDCS
1 State NCD cell 0.3 0.3 0.5 0.5
2 District NCD cell 2.6 2.6 6.5 6.5
3 Training for Universal Screening for NCDs
151.98 142.6 91.02 15.83
4 Any other 0 0 0 0 PMU Training
1 Training on Finance 2 2 2 2
2 Training in on HR 4 4 8 8
3 Any other 31.52 31.52 0 0 Training of DPMSU
1 Training on Finance 0 0 0 0
2 Training on HR 0 0 0 0
3 Any other 0 0 0 0 Training of BPMSU
1 Training on Finance 0 0 0 0

94 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
2 Training on HR/ 0 0 0 0
3 Any other 0 0 0 0 PNDT Training
1 PC/PNDT training 1.6 1.6 1.6 1.6 0 0 2 Any other 0 0 0.24 0.24 0.24 0.24 ASHA Facilitators/ ARC Trainings
1 Training of District Trainers 0 0 0 0
2 Capacity Building of ASHA Resource Center 0 0 0 0
3 HR at State Level (PM & HR only) 0 0 0 0
4 HR at District Level (PM & HR only) 0 0 0 0
5 HR at Block Level 0 0 0 0
6 Any other 0 0 0 0 Training on Outreach Services
1 Trainings / orientation (MMU) 0 0 0 0
2 Trainings / orientation (MMV) 0 0 0 0
3 Trainings / orientation (Ambulance) 0 0 0 0
4 Any other 0 0 0 0 Training under AYUSH
1 Training under AYUSH 0 0 0 0
2 Any other 0 0 0 0 Quality Assurance Trainings
1 Quality Assurance Training 6.7 6.7 12.02 12.02
2 Miscellaneous Activities 3.69 3.69 3.69 3.69
3 Kayakalp Training 8.78 8.78 15.1 15.1
4 Any Other 0 0 0 0 HMIS/MCTS Training
1 Training cum review meeting for HMIS & MCTS state level 1 1 1 1
2 Training cum review meeting for HMIS & MCTS district level 1.9 1.9 1 1
3 Training cum review meeting for HMIS & MCTS at Block Level 51.65 51.65 50.81 50.81
4 Any other 0 0 0 0
Trainings for Health & Wellness centre (H & WC)
1 Bridge Course/ Training on the Standard Treatment protocols 0 0 0 0
2 Multi-skilling of ANMs ASHA, MPW 25.4 25.4 0 0

95 Capacity Building & Training Strategy
Sl. No.
Training Particulars Budget
(2019-20) Budget
(2018-19) Budget
(2017-18) Proposed Approved Proposed Approved Proposed Approved
3 BSc Community Health/Bridge Course for MLPs for CPHC 413.6 413.6 341.22 341.22
4 Any other 28.28 28.27 0 0 Any other Trainings
1 PGDHM Courses 0 0 0 0
2 Training (Implementation of Clinical Establishment Act) 7 7 7 0
3 Promotional Training of ANMs to lady health visitor, etc. 0 0 0 0
4 Training of ANMs, Staff Nurses, AWW, AWs 0 0 9.72 5.51 3.82 3.82
IMEP Training
1 TOT on IMEP 0 0 0 0 0 0
2 IMEP training for State and district programme managers 0 0 0 0 0 0
3 IMEP training for medical officers 0 0 0 0 0 0 4 Other 0 0 0 0 0 0

96
Capacity Building & Training Strategy
Annexure - III RCH-II TRAINING
(Source: National Training Strategy for In-service under National Rural Health Mission)
Sl. No.
Type of Trg. Category of Participants Duration Batch Size Venue Trainers Responsibility
1. SBA SN/ANM/LHV 3 – 6 Weeks 2 – 4 Identified District Hospitals
TOT trained Obstetrician/MO/ SN& Paed. M.O.
MH Division/ NIHFW
2. EmOC MOs 16 Weeks Up to 8 Identified Medical Colleges
Faculty Med. College (Gyn)/Dist Gynaecologist.
MH Division/ FOGSI
3. Life Saving Skills in Obs. Anesthesia
MOs 18 Weeks Up to 8 Identified Medical Colleges
Faculty Med. Coll. (Anes)/Distt. Anaes
MH Division
4. Blood Storage MOs, Lab. Tech. 3 Days 2 – 3 Instt. where Blood Banks are available
I/c of trg. instt. State/SIHFW
5. RTI/STI MO/SN/ANM/ LHV 2 Days 5 Identified Medical Colleges/RHFWTC
Oriented team of trainers at State Level
MH Division
6. MTP including MVA
MOs 15 Days 5 Identified Trg. Institutes Gynaecologist from Medical Colleges
MH Division
7. IMNCI MO/ANM/LHV/ AWW, etc.
8 days 24 National/State/District Trg. Centers
Faculty of Paediatrics and P&SM deptt.
CH Division/State
8. Immunisation Health Workers 2 days 20-25 District Trg. Centers Trained Trainers Imm. Division 9. Mini Lap MOs for CHCs/ FRU & DH 12 Working
Days 1 - 2 Identified Trg. Institutes Gynaecologist FP Division
10. Lap. Ster. Gynaecol./Surgeon with OT Nurse & Assistant
12 Working Days
1 team at a time
Identified Trg. Institutes Gynaecologist FP Division

97
Capacity Building & Training Strategy
Sl. No.
Type of Trg. Category of Participants Duration Batch Size Venue Trainers Responsibility
11. IUCD ANM/LHV 5 days 5 – 10 Identified Trg. Institutes FP Division
12. NSV MOs 5 days 4 Master/State Level Trainers
FP Division
13. Adolescent Health MOs/ANM 5 Days 25 – 30 IEC Division
14. PDC CMO/Civil Sur./ Hosp. Suptd.
10 Weeks 20 - 25 Identified 13 Trg. Institutes
Faculty of NIHFW NIHFW & Trg. Div
15. PMU 5 Days 20 – 25 NIHFW/SIHFW Faculty of NIHFW NIHFW & DC Div.

98
Capacity Building & Training Strategy
TRAINING UNDER NATIONAL DISEASE CONTROL PROGRAMMES (Source: National Training Strategy for In-service under National Rural Health Mission)
Sl. No.
Types of Training Category Duration Batch Size Venue Responsibility
1. National Leprosy Elimination Programme (NLEP)
Orientation Training
MO/HA (M)/HA (F), MPW
3 days
30
District/Block Level
State/District Leprosy Officer
Refresher Training MO/HA (M)/HA (F), MPW
1 day 30 District/Block
Level State/District
Leprosy Officer
2. Revised National Tuberculosis Control Programme (RNTCP)
Initial Training STD/DTO 14 days 20 Identified Director
MO – TC 12 days 20 Central Instt. Central Instt.
MO STS/TO/SA/ 5 days 20 Identified Director
IEC 6 days 12 Central Instt. STDC
STLS Lab. Tech. 15 days 6 STDC
MPHS MPHW/ 10 days 8 STDC I/c DTC
TBHV Pharmacist 3 days 25 STDC
Trg. of Staff Drug 2 days 25 Dist. Trg. Centre
Mgt. Accountant 2 days 25 (DTC)
Community 1 day 25 DTC
Volunteer Private 1 day 25 DTC

99
Capacity Building & Training Strategy
Sl. No.
Types of Training Category Duration Batch Size Venue Responsibility
Practitioner 2 days 25 DTC
Pvt. LTs 20 DTC
8 DTC
Update Training EQA Trg. Update Training TB – HIV
Master Trainers & Microbiologist IRL & LTs
STDC (Dir.)/STD DTO/ MO – TC STLS LTs
Master Trainers
DTO/MO – TC MO STLS/STS
2 days
14 days
2 days 2 days 2 days 1 day
10
6
15 25 6
25
10
10 30 10
Identified Central Instt.
Identified Central Instt.
STDC STDC STDC DTC
Identified
Central Instt. STDC DTC
STDC
Director Central Instt Director STDC
Director Central Instt. Director STDC
I/c DTC
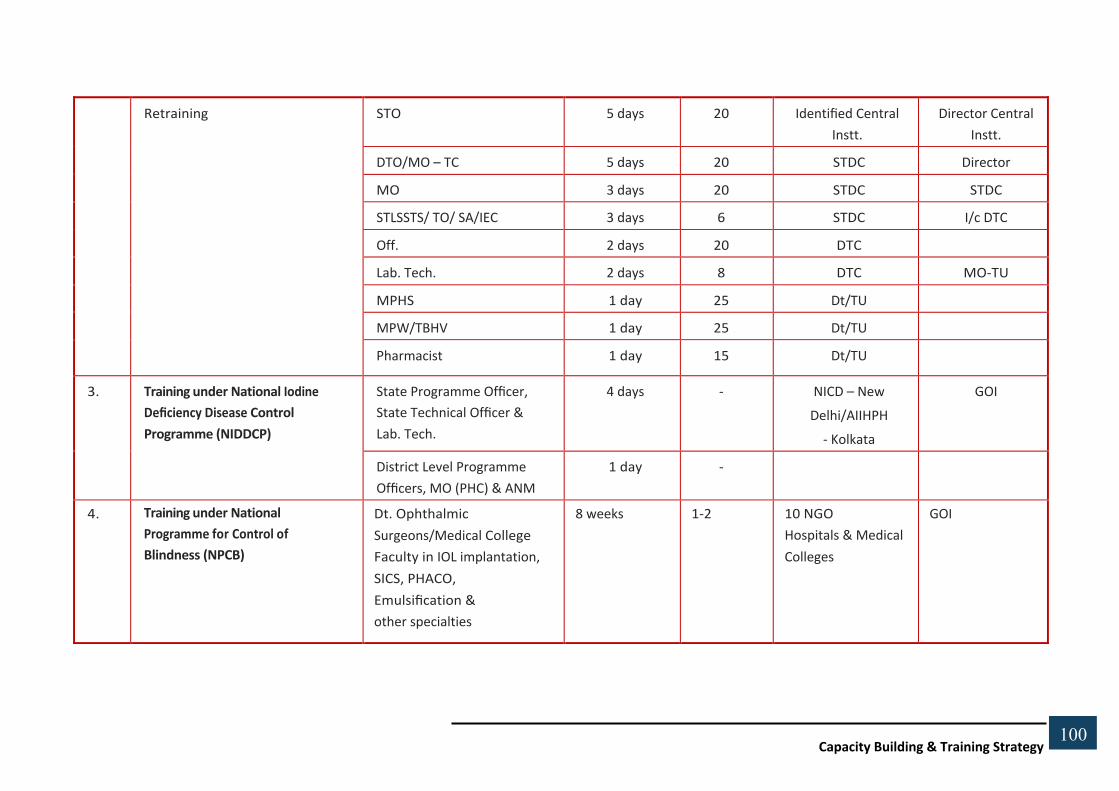
100
Capacity Building & Training Strategy
Retraining STO 5 days 20 Identified Central Instt.
Director Central Instt.
DTO/MO – TC 5 days 20 STDC Director
MO 3 days 20 STDC STDC
STLSSTS/ TO/ SA/IEC 3 days 6 STDC I/c DTC
Off. 2 days 20 DTC
Lab. Tech. 2 days 8 DTC MO-TU
MPHS 1 day 25 Dt/TU
MPW/TBHV 1 day 25 Dt/TU
Pharmacist 1 day 15 Dt/TU
3. Training under National Iodine Deficiency Disease Control Programme (NIDDCP)
State Programme Officer, State Technical Officer & Lab. Tech.
4 days - NICD – New Delhi/AIIHPH
- Kolkata
GOI
District Level Programme Officers, MO (PHC) & ANM
1 day -
4. Training under National Programme for Control of Blindness (NPCB)
Dt. Ophthalmic Surgeons/Medical College Faculty in IOL implantation, SICS, PHACO, Emulsification & other specialties
8 weeks 1-2 10 NGO Hospitals & Medical Colleges
GOI
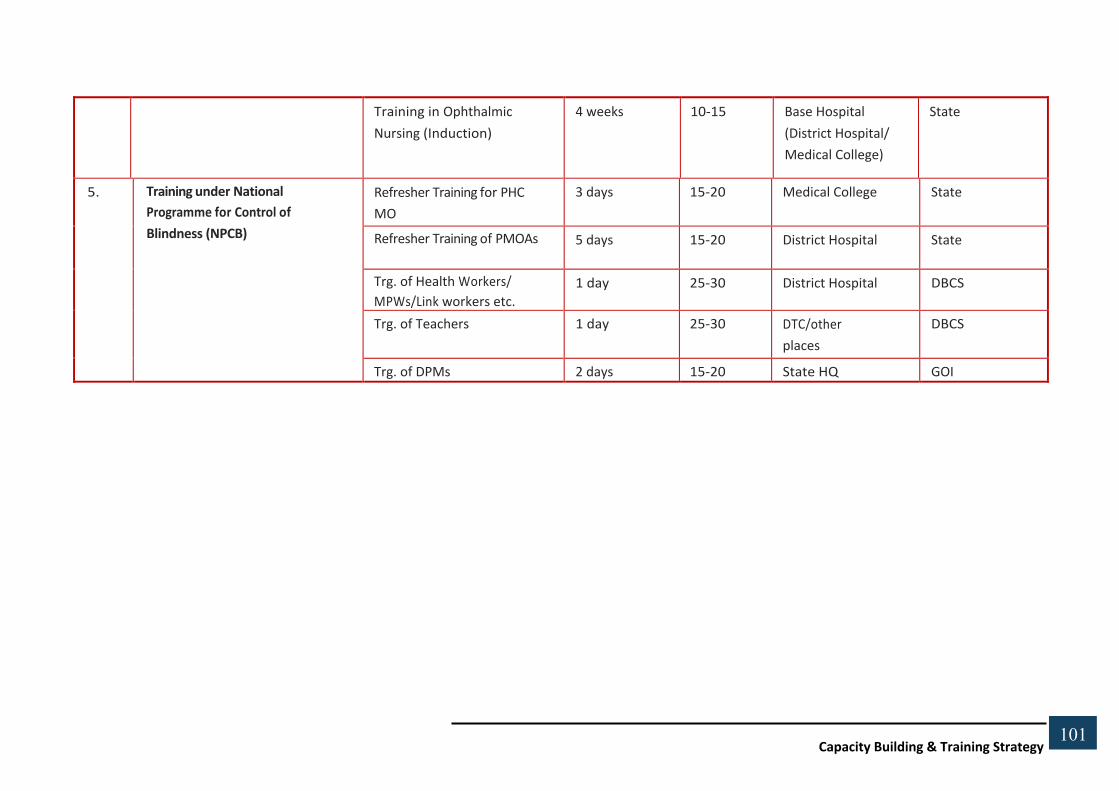
101
Capacity Building & Training Strategy
Training in Ophthalmic Nursing (Induction)
4 weeks 10-15 Base Hospital (District Hospital/ Medical College)
State
5. Training under National Programme for Control of Blindness (NPCB)
Refresher Training for PHC MO
3 days 15-20 Medical College State
Refresher Training of PMOAs 5 days 15-20 District Hospital State
Trg. of Health Workers/ MPWs/Link workers etc.
1 day 25-30 District Hospital DBCS
Trg. of Teachers 1 day 25-30 DTC/other places
DBCS
Trg. of DPMs 2 days 15-20 State HQ GOI

Capacity Building & Training Strategy
102 102
102
NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAMME (NVBDCP) (Source: National Training Strategy for In-service under National Rural Health Mission)
National Level Training Courses
Sl. No.
Name of Training Courses/ Workshop
Category Duration Batch Size
Name of the Institution/ Venue
Responsibility
1 Tertiary level training for medical college faculty
Medical College Faculty 2 days 25 Medical Colleges Concerned Regional Director
2 Rapid Response Team on management of VBD
Members of State/ Distt Rapid Response Teams
2 days 25 AIIMS/NICD Concerned Institute
3 Trg. on Laboratory Diagnosis of JE & Dengue/ HF
Microbiologists/Lab. Technicians.
2 days 25 Apex Referral Labs./ NICD/NIMHANS
Concerned Institute
4 Trg. on Prevention & Control of VBDs
State/District Level Officers. 20 working days
25 NICD NICD
5 Trg. for Entomologists & Biologists
Entomologists/Biologists 20 working days
25 NIMR/IVCZ Hosur Concerned Institute
6 Trg. for Laboratory Technicians for Military/ Para Military Forces.
Lab. Technicians 5 days 25 To be conducted in coordination with respective organisations.
Concerned Institute
7 Trg. for Medical Officers/Military/Para Military forces
Medical Officers 2 days 25 To be conducted in coordination with respective organisations.
Concerned Institute
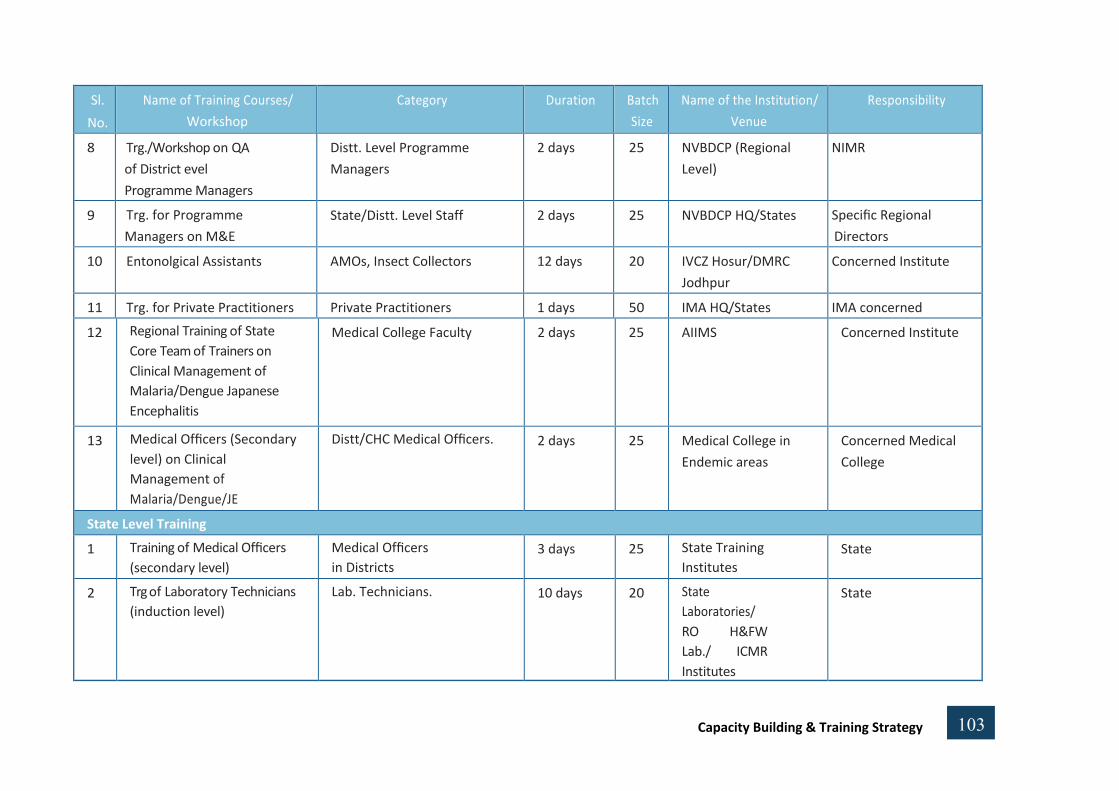
Capacity Building & Training Strategy
103 103
103
Sl. No.
Name of Training Courses/ Workshop
Category Duration Batch Size
Name of the Institution/ Venue
Responsibility
8 Trg./Workshop on QA of District evel Programme Managers
Distt. Level Programme Managers
2 days 25 NVBDCP (Regional Level)
NIMR
9 Trg. for Programme Managers on M&E
State/Distt. Level Staff 2 days 25 NVBDCP HQ/States Specific Regional Directors
10 Entonolgical Assistants AMOs, Insect Collectors 12 days 20 IVCZ Hosur/DMRC Jodhpur
Concerned Institute
11 Trg. for Private Practitioners Private Practitioners 1 days 50 IMA HQ/States IMA concerned
12 Regional Training of State Core Team of Trainers on Clinical Management of Malaria/Dengue Japanese Encephalitis
Medical College Faculty 2 days 25 AIIMS Concerned Institute
13 Medical Officers (Secondary level) on Clinical Management of Malaria/Dengue/JE
Distt/CHC Medical Officers. 2 days 25 Medical College in Endemic areas
Concerned Medical College
State Level Training
1 Training of Medical Officers (secondary level)
Medical Officers in Districts
3 days 25 State Training Institutes
State
2 Trg of Laboratory Technicians (induction level)
Lab. Technicians. 10 days 20 State Laboratories/ RO H&FW Lab./ ICMR Institutes
State

Capacity Building & Training Strategy
104 104
104
Sl. No.
Name of Training Courses/ Workshop
Category Duration Batch Size
Name of the Institution/ Venue
Responsibility
3 Trg of Lab. Technicians (re-orientation level)
Lab. Technicians. 5 days 20 State Laboratories/ RO H&FW Lab./ ICMR Institutes
State
4 Trg of Health Supervisors, Health Workers
Health Supervisors/ Health Workers
2 days 25 Block level PHC MO of block PHC
5 Trg of Community Health Workers
Community Health Workers 1 day 50 PHC MO of PHC
6 Trg of ASHAs (Proposed) ASHA 3 days 25 Block level PHC MO of block PHC

105
105 Capacity Building & Training Strategy
Model District Training Plan
Sl.
No.
Type of Facility
No. of Facilities
No. of Staff required as per the NRHM framework for
Implementation
Desired Training
Load
1. Sub – Centre 400 @ 2 ANM per SC 800
2. Primary Health Centre
60 – 70 @ 1 MO 60
(PHC) @ 3 SN 180 – 200
@ 1 PHN Practitioner 60 – 70
@ 1 Lab. Technician 60 – 70
@ 1 Pharmacist 60 – 70
3. Community Health
15 – 20 @ 7 Specialist MOs (Paed., Obs. 45 – 60
150 – 200
15 – 20
15 – 20
15 – 20
15 – 20
Centre (CHC)/First
& Gynae., Surgeon, Anaes. & 3
Referral Unit (FRU)
MOs)
@ 10 SN
@ 1 Lab. Technician
@ 1 Pharmacist
@ 1 BEE
@ 1 Radiographer
4. District Hospital (DH)
1

106
106 Capacity Building & Training Strategy
Anneuxre-IV
SUGGESTED TRAINING VENUES (Based on stakeholder consultation & desk review)
CLINICAL TRAININGS
Medical College, Haldwani, Dehradun, Sri Nagar
District Skill Lab Haridwar, Pauri, TehrI
Nursing College Dehradun, Chamoli, Nainital
AIIMS Rishikesh
FOR INDUCTION, MANAGEMENT & SOFT SKILL TRAININGS
ANM Training College U.S Nagar, Pithoragarh, Dehradun, Pauri & Chamoli
Administrative Training Institute Nainital
Indian Institute of Management Rudrapur
Divisional Health & Family Welfare Training Centre (DHFWTC)
Dehradun & Haldwani
Medical College Sri Nagar For the use of Medical colleges, it may be instructive to sign MOUs with medical colleges in the area.

107
107 Capacity Building & Training Strategy
Annexure-V
STATE INSTITUTE OF HEALTH & FAMILY WELFARE INDRA NAGAR, LUCKNOW
FOUNDATION COURSE FOR NEWLY APPOINTED MEDICAL OFFICERS
Duration- Six Weeks
OBJECTIVE
1. To provide motivation towards Administrative, Professional. Human and Medical values.
2. To make the participants familiarize with different programmes related to Medical, Health & Family Welfare and there implementation.
3. To make the participants aware about different concept of management and to provide skills.
COURSE CONCEPTS & TIME SCHEDULE
Sl. No. Topic
Part-I Medical, Health & Family Welfare Department.
1. Administrative structure and functioning : State Division- District-CHC-PHC-Grassroots Level
2. Job responsibility of PHC Staff & Ideal PHC :Criteria
3. NRHM/RCH-II- approach, different components, different new formats under CAN
4. NRHM Financial Management at PHC
5. Rogi Kalyan Samiti & Operation of Bank Account
6. Functioning of ASHA
7. Sanitation & Safe Drinking Water
8. Community participation & Role of NGOs (CBDs)
9. National Leprosy Eradication Programme
10. Blindness Control & IDD Programme
11. T.B. Programme
12. AIDS Control Programme
13. Vector Born Disease Control Programme

108
108 Capacity Building & Training Strategy
Sl. No. Topic
14. Immunization- Vaccine Storage and Cold Chain Maintenance
15. Home Based New Born Care
16. Child Care-Diahorria, Pneumonia, Malnutrition
17. Maternal Health, Institutional Delivery, PNC, ANC
18. FP Programme- Method, Counseling (Cafeteria Approach, Gather Approach) MTP Services, FP Camps
19. Fare Festival & Meals, Huz Duties
20. 21.
Monitoring and Evaluation of Programmes Population Issues & Factors affecting population growth, National Health policy, National Population Policy & State Population Policy
22. Demographic Indicators (BR, DR, DPR, IMR, MMR, NRR & Growth rate
23. Communicable Disease-Prevention & Control
24. RTI/STI Management
25. IMEP/Hospital Waste Management
Part- II Management
1. Meaning, principals and Technique of Management
2. H.R.D.- Motivation and work performance, Leadership and Team Work
3. Supportive Supervision
4. Communication: Strategy in Health & F.W. Programme
5. Decision making & Problem solving Techniques
6. Hospital Management: Emergency services, Hospital performance appraisal, Ambulance & Transportation, Medical audit, Store management, Display chart of services, Getting feedback, Hospital statistics etc.
7. Public dealing, Grievance handling and dealing with Public representatives.
8. Disaster Management & Out Break Investigation
9. Stress Management
Part-III Personnel Management and Service Procedure
1. Government servant conduct rule & M.G.O.
2. Cadre Restructuring & Division of Labor
3. Service rule and disciplinary proceedings
4. Annual Charter Role (ACR) entry

109
109 Capacity Building & Training Strategy
Sl. No. Topic
5. Reservation , Promotion, Annual increment
6. Confirmation, Voluntary retirement etc.
Part-IV Financial Procedure
1. Basic Concept of Financial Management. Functioning and Basic Rule of Treasury
2. Duties and responsibilities of DDO
3. TA/DA Rules and preparation of TA bills
4. Pay fixation, Leave rules, Loans and Advances, Pension and Other welfare schemes
5. Audit and functioning of A.G. Office
6. Store Purchase rules
7. Condemnation procedure & disposal of dead items
8. Income Tax Rules & Investment Counseling
Part-V Office Procedure
1. Noting drafting & correspondence Receipt & dispatch Filing system and Record Keeping
2. Maintenance of office records: Service book, GPF Pass Book personal file and register of registers etc.
3. Meeting, inspections, Tours and their Report Celebrations of National day & Special Day e.g. - Doctors Day, Population Day, Safe Motherhood Day etc.
Part-VI Constitution & Legal Procedures
1 Legal safeguards to public servants
2. Structure and jurisdiction of different Courts, Writ petition, Counter Affidavit, Stay order, Appeal and Contempt of Court
3. Consumer Protection Act, Food Adulteration Act, Drug & Cosmetic Act, PPNDP Act, Death- Birth Registration Act, IMA Act, RTI Act, MTP Act etc.
Part-VII Medico Legal
1. Meaning and procedure
2. Preparation of Medico Legal Report under situation like:- Accident, Injuries, Electric burn, Burn MTP, Death, Rape, Legation death, Poisoning
3. Informing Police, Keeping body in Mortuary and its disposal
4. Post-mortem

110
110 Capacity Building & Training Strategy
Sl. No. Topic
5. Dying declaration & Issuing Death Certificate
6. Treatment and referral of Convicts and under trials
Part-VIII Medical Ethics
1. Medical values and Standards, Human and Social Commitment of a Medical Practitioner
2. Doctor- Patient relation, Issuing of Certificate, Referral System and Patient’s Counseling
Part-IX Development and Planning
1 Different Development Scheme related to Medical Health & FW.
2. Intersectoral Co-ordination and Cooperation
3. Planning Process, Decentralized Planning, District Plan
4. Panchayati Raj, ICDS, Medical Health & FW
Part-X Computer and MIES
1. Use of Computer in Hospital Management
2. PMIS & HMIS
Part-XI General Arrangement
1. Registration
2. Introduction-SIHFW, Course & Curriculum
3. Self Introduction (Ice breaking)
4. Pre test
5. Visit to District Hospital Male & Female (Pre Lunch)
6. Visit to Health Directorate (Post Lunch)
7. Visit to Family Welfare Directorate (Post Lunch)
8. Post Test & Course Evaluation
9. Viva
10. Panel Discussion & Valedictory

111 Capacity Building & Training Strategy
Annexure VI
STAKEHOLDER-WISE & TRAINING WISE BUDGET
TRAINING FOR MEDICAL OFFICERS
Training Course Title Total Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-
Residential
Place of
Training Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 139 5 14 30 65 Residential Regional 1,22,12,834
2 Strategic and Coordinated Management,
Monitoring, Reporting, HR management 1394 46 5 30 232 Residential Regional 5,08,11,300
3 Communication, and Liasoning Skills 1394 46 5 30 232 Residential Regional 5,08,11,300
4 Leadership, Motivation and Teamwork Skills 1394 46 4 30 186 Residential Regional 4,07,18,740
5 Medico-Legal & Ethics 1394 46 3 30 139 Residential Regional 3,06,26,180
6 Biomedical Waste Management & Infection Control 1394 46 4 30 186 Residential Regional 4,07,18,740
7 Quality Assurance 1394 46 4 30 186 Residential Regional 4,07,18,740
8 Disaster Preparedness & Response 1394 46 3 30 139 Residential Regional 3,06,26,180
9 Finance and Budgeting 1394 46 3 30 139 Residential Regional 3,06,26,180
TOTAL 32,78,70,194

112 Capacity Building & Training Strategy
SL.
No.
TRAINING FOR NURSES
Training Course Title Total Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-
Residential
Place of
Training
Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 112 4 7 30 26 Residential District 15,78,321
2 Strategic and Coordinated Management,
Monitoring, Reporting, HR management 1117 37 5 30 186 Residential District 1,13,37,550
3 Communication, and Liasoning Skills 1117 37 5 30 186 Residential District 1,13,37,550
4 Leadership, Motivation and Teamwork Skills 1117 37 4 30 149 Residential District 91,14,720
5 Medico-Legal & Ethics 1117 37 3 30 112 Residential District 68,91,890
6 Biomedical Waste Management & Infection Control 1117 37 4 30 149 Residential District 91,14,720
7 Quality Assurance 1117 37 4 30 149 Residential District 91,14,720
8 Disaster Preparedness & Response 1117 37 3 30 112 Residential District 68,91,890
9 Finance and Budgeting 1117 37 3 30 112 Residential District 68,91,890
TOTAL 7,07,26,206

113 Capacity Building & Training Strategy
SL.
No.
TRAINING FOR PHARMACIST
Training Course Title Total
Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-Residential
Place of
Training Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 140 5 5 30 23 Residential District
2 Strategic and Coordinated Management,
Monitoring, Reporting, HR management 1399 47 5 30 233 Residential District 81165317
3 Communication, and Liasoning Skills 1399 47 5 30 233 Residential District 81165317
4 Leadership, Motivation and Teamwork Skills 1399 47 4 30 187 Residential District 53768233
5 Medico-Legal & Ethics 1399 47 3 30 140 Residential District 31967150
6 Biomedical Waste Management & Infection
Control 1399 47 4 30 187 Residential District 53768233
7 Quality Assurance 1399 47 4 30 187 Residential District 53768233
8 Disaster Preparedness & Response 1399 47 3 30 140 Residential District 31967150
9 Finance and Budgeting 1399 47 3 30 140 Residential District 31967150
TOTAL 41,95,36,783

114 Capacity Building & Training Strategy
Sl.
No.
TRAINING FOR MEDICAL TECHNICIANS
Training Course Title Total
Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-
Residential
Place of
Training
Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 38 1 7 30 9 Residential District 5,86,931
2 Strategic and Coordinated Management, Monitoring,
Reporting, HR management 381 13 5 30 64 Residential District 42,19,575
3 Communication, and Liasoning Skills 381 13 5 30 64 Residential District 42,19,575
4 Leadership, Motivation and Teamwork Skills 381 13 4 30 51 Residential District 33,94,710
5 Biomedical Waste Management & Infection Control 381 13 4 30 51 Residential District 33,94,710
6 Quality Assurance 381 13 4 30 51 Residential District 33,94,710
TOTAL 1,86,23,280

115 Capacity Building & Training Strategy
Sl.
No.
TRAINING FOR FRONTLINE HEALTH WORKERS
Training Course Title Total
Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-
Residential
Place of
Training
Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 205 7 5 30 34 Residential District 14,81,645
2 Strategic and Coordinated Management, Monitoring, 2046 68 5 30 341 Residential District 1,48,16,450
3 Communication, and Liasoning Skills 2046 68 5 30 341 Residential District 1,48,16,450
4 Leadership, Motivation and Teamwork Skills 2046 68 4 30 273 Residential District 1,19,55,460
5 Biomedical Waste Management & Infection Control 2046 68 4 30 273 Residential District 1,19,55,460
6 Quality Assurance 2046 68 4 30 273 Residential District 1,19,55,460
Total 6,54,99,280

116 Capacity Building & Training Strategy
Sl. No.
TRAINING FOR GDA
Training Course Title Total Staff Batches Days
No. of
Trainees
per
batch
Total
Training
Days
Residential/
Non-
Residential
Place of
Training
Total
A B C D E F G H I (J+K+L+M+N+O)
1 Induction Training @10% of total strength 134 4 3 30 13 Residential Block 491780
2 Communication, and Liasoning Skills 1340 45 5 30 223 Residential Block 8017666.667
3 Leadership, Motivation and Teamwork Skills 1340 45 4 30 179 Residential Block 6467733.333
4 Biomedical Waste Management & Infection Control 1340 45 4 30 179 Residential Block 6467733.333
5 Quality Assurance 1340 45 4 30 179 Residential Block 6467733.333
TOTAL 2,74,20,867
Related Documents











