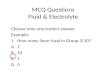
1.A 21 year old female came with a chief complaint of forwardly placed lower jaw. On clinical examination, there was mid- maxillary deficiency. Molar relation was class I bilaterally and upper arch had anterior crowding. There was a negative overjet and edge-to-edge bite. Cephalometric analysis revealed ANB to be -4° with decreased maxillary and increased mandibular length. Upper incisors were proclined and lower incisors were slightly protruded. 1 The case should be diagnosed as a. Skeletal Class I b. Skeletal Class II c. Skeletal Class III d. Skeletal End-on

Ahead 29 Nth Dec Online live lecture Mcq
Nov 27, 2015
50 MCQs Based Lecture at Ahead cademy on Dentistry Exam
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1.A 21 year old female came with a chief complaint of forwardly placed lower jaw. On clinical examination, there was mid-maxillary deficiency. Molar relation was class I bilaterally and upper arch had anterior crowding. There was a negative overjet and edge-to-edge bite. Cephalometric analysis revealed ANB to be -4° with decreased maxillary and increased mandibular length. Upper incisors were proclined and lower incisors were slightly protruded.1 The case should be diagnosed asa. Skeletal Class Ib. Skeletal Class IIc. Skeletal Class IIId. Skeletal End-on

Ans: c. Skeletal Class III (Ref: Page no 507 Proffit, White and Sarver) Class III problems, by definition, are those caused by some combination of
maxillary deficiency and mandibular excess. SNA angle will be decreased and SNB angle will be increased. Maxillary deficiency and mandibular excess may be seen alone or in
combination
What is pseudo class III ?.............. 2. Most common cause of an enlarged
mandible isa. Environmental factorsb. Cleft palatec. Heredityd. Impaired maxillary growth

Ans: c. Heredity (Ref: Page no 508 Proffit, White and Sarver)
A strong familial tendency exists towards the excessive growth that leads to mandibular prognathism.
The Hapsburg jaw, the prognathic mandible of European royal family is the best known example.
3. What should be the treatment plan ?a. Orthodontic treatmentb. Reverse twin blockc. Orthognathic surgeryd. Surgico-orthodontic treatment

Ans: d. Surgico-orthodontic treatment (Ref: Page no 691 Proffit 4/e)
Class III problems are less amenable to camouflage than class II because retraction of lower incisors makes the chin appear more prominent.
Reverse twin block is a myofuntional appliance given in growing children.
Orthognathic surgery alone would not be able to address the crowding and molar relation.
Orthodontic treatment combined with surgery is an appropriate treatment plan

4.What extractions should be performed for an optimum occlusion?
a. Lower central incisor and upper first premolarb. Upper first premolarc. Lower second premolard. Upper first and lower second premolar.
Ans: d. Upper first and lower second premolar (Ref: Page no 308, 693 Proffit 4/e)
Surgical preparation requires extraction of upper first premolars for retraction of upper incisors, correcting the crowding and increasing the reverse overjet, referred to as 'decompensation'.
Lower second premolar extraction provides space for protraction of lower molars so that molars come into class III relation so that after surgery, the molar relation is class I.
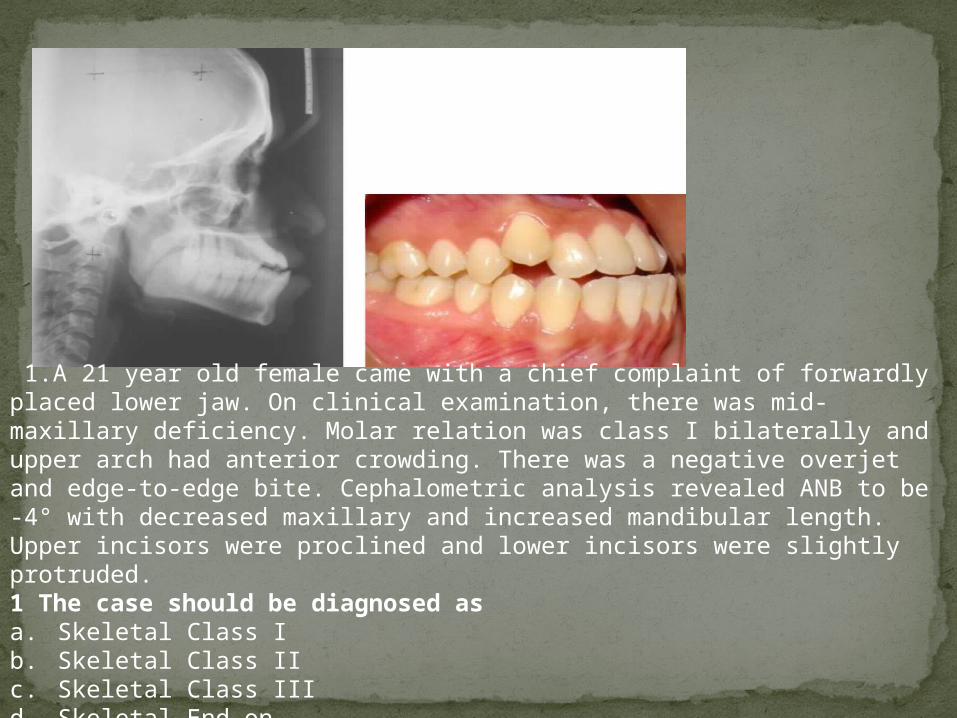
A 12 year old female came reported with bilateral cleft lip and palate. History taking revealed that lip repair was done at age of 10 months and palate repair was done at 2 years. posterior crossbite. 12 and 22 were missing. Bony defects were seen bilaterally in lateral incisor region.
5.The teratogens affecting cleft lip and palate area. Ethyl alcoholb. 6-Mercaptopurinec. X-radiationd. Vitamin D excess

Ans: b. 6-Mercaptopurine (Ref: Page no 131 Proffit 4/e)Following are the teratogens affecting development of cleft lip
and palate :AspirinCigarette smoke (hypoxia)Dilantin6-MercaptopurineValium
6.Infant orthopaedics necessary in such cases was pioneered by
a. Burstonb. Harvoldc. Millardd. Rosenbeck
Ans: a. Burston (Ref: Page no 321 Proffit 4/e)Infant orthopaedics - orthodontic intervention to reposition the
lateral segments and to bring the protruding premaxillary segment back into the arch to obtain good surgical repair of the lip.
Accomplished by light elastic strap across anterior segment and orthodontic appliance pinned to the segments to apply contraction force.
Pioneered by Burston in Liverpool in late 1950s.
7.The ideal time for lip repair isa. 10 daysb. 10 weeksc. 10 monthsd. None of the above

b.10 weeks (Ref: Page no 321 Proffit 4/e)Millard advocated lip repair at the age of 10 weeks
(Rule of 10s).If presurgical movement of maxillary segments is
indicated, it is beginned at 3-6 weeks, so that lip closure can be done at age of 10 weeks.
A passive plate is used for few months after lip closure
.8.The ideal age for alveolar bone grafting isa. 5-7 yearsb. 6-8 yearsc. 7-10 yearsd. 7-9 years
Ans: c. 7-10 years (Ref: Page no 324 Proffit 4/e)The permanent lateral incisors and canines should ideally
be made to erupt through the graft.The best time to place the graft is between 7-10 years.Necessary alignment or expansion of posterior segments
should be completed before alveolar grafting.
9.A removable orthodontic appliance, producing a light force on the labial of a proclined maxillary central incisor will cause
A. lingual movement of the crown and lingual movement of the root apex.
B. intrusion of the central incisor and lingual movement of the crown.
C. lingual movement of the crown and labial movement of the root apex.
D. intrusion of the central incisor.

11
Ans C (Ref : page no. 374 proffit
4/e)uncontrolled tipping
Movement of the root apex and crown in opposite direction Crot – Between Cres and apex Mc/F ratio 0:1 to 5:1 Mc/MF= 0
10.When a controlled tipping force is applied to the crown of a single-rooted tooth, the centre of rotation is located
A. at the apex. B. at the cervical line.C. within the apical half of the root.D. within the cervical one third of the root.
Ans A [Ref: Proffit’s 3rd Ed Pg 340, 341]

13
TOOTH MOVEMENT POSITION OF CROT
Translation Infinity
Uncontrolled Tipping Slightly apical to Cres
Controlled Tipping Root Apex
Root Movement Incisal Edge
Pure Rotation At Cres

11.The sound which is most affected in a patient of Class-Ill malocclusion ?
A. Linguoalveolar consonants B Sibiliant Sounds C. Linguoalveolar Frecatives D. Labiodental Fricatives

[Ans. (D) Ref. Proffit 4th Ed Pg 175 & Boucher’s 11th Ed Pg 351]
12.Maxillary incisor protrusion can be treated by
1. premolar extraction with orthodontic retraction of the incisors.
2. premolar extraction with surgical repositioning of the anterior dentoalveolar segment.
3. extraction of the incisors, alveoloplasty and prosthodontic replacement.
4. Reduction genioplasty.A. (1)(2) (3) B. (l)and(3) C. (2) and
(4)D. (4) only E. All of the above

Ans A (Ref : page no. 204 and 701 proffit 4/e)Orthodontic treatment of maxillary incisor
protrusion:Excessive protrusion of incisors( bimaxillary
protrusion,(not excessive overjet) usually is an indication for premolar extraction and retraction of the protruding incisors.
Surgical treatment of maxillary incisor protrusion:
Segments of the dentoalveolar process can be repositioned surgically in all three planes of space. Genioplasty is the surgical repositioning of the chin. It can not be used for maxillary incisor protrusion

13.The mandible grows primarily at theA. symphysis and condyles.B. posterior border of the ramus and the
alveolar crest.C. condyles and lateral border of the body.D. condyles and posterior border of the
ramus.E. symphysis and posterior border of the
ramus.
Ans D (Ref : page no. 46 proffit 4/e) If data from vital staining experiments are examined,
it becomes apparent that the principal sites of growth of the mandible are the posterior surface of the ramus and the condylar and coronoid processes.There is little change along the anterior part of the mandible.
As a growth site, the chin is almost inactive. It is transIated downward and forward, as the actual growth occurs at the mandibular condyle and along the posterior surface of the ramus. The body of the mandible grows longer by periosteal apposition o f bone on its posterior s urface,while the ramus grows longer by endochondralr eplacemenat the condyle accompanied by surface remodeling.
14. Which of the following are mechanisms of growth of the naso-maxillary complex?A. Sutural. B. Cartilaginous.C. Appositional. D. All of the above

Ans D (Ref : page no. 51 proffit 4/e & Graber pg 43 3/ed
Proponents of the cartilage theory hypothesize that the cartilaginous nasal septum serves as a pacemaker for other aspects of maxillary growth. growth.

15.The principal growth sites of the maxilla in a downward and forward direction include the
a.frontomaxillary suture.
b.zygomaticomaxillary suture.
c.pterygopalatine suture.
d.median palatine suture. A. (1)(2)(3) B. (l)and(3) C. (2) and (4) D. (4) only. E. All of the above.

16. Following orthodontic rotation of teeth, which of the periodontal ligament fibres are most commonly associated with relapse?
A. Oblique. B.Diagonal. C.Horizontal. D.Supracresta
17. Which type of malocclusion should be corrected as early as possible?
A. Class II Division 1 associated with an anterior open bite.B. Class II Division 2 associated with an increased anterior
overbite.C. Class III associated with an anterior open bite.D. Cross-bite associated with a functional shift of the
mandible from initial contact to maximum intercuspation.E. Anterior open bite associated with a lip or digit sucking
habit.

18. Long term stability of the orthodontic correction of a deep anterior overbite is better
A. in growing children compared to adults.B. when the correction is accomplished by
protrusion and intrusion of the lower anterior teeth.
C. when a low interincisal angle is established as a result of orthodontic correction
. D. in non-extraction versus extraction cases.
E. in patients with a high mandibular plane angle.

Ans E (Ref : page 209 Proffit 4/e)Long term stability of the orthodontic correction of a deep
anterior overbite is better in patients with a high mandibular plane angle
19. The angles, SNA, SNB and ANB are often used to describe relationships of the maxilla and mandible. The reliability of interpretations based on these angles is
A. good because research has proven their accuracy.B. good because these landmarks can be identified
accurately on the cephalometric radiograph.C. questionable because of variations in vertical
relationships in the lower face.D. questionable because of variations in head posture.
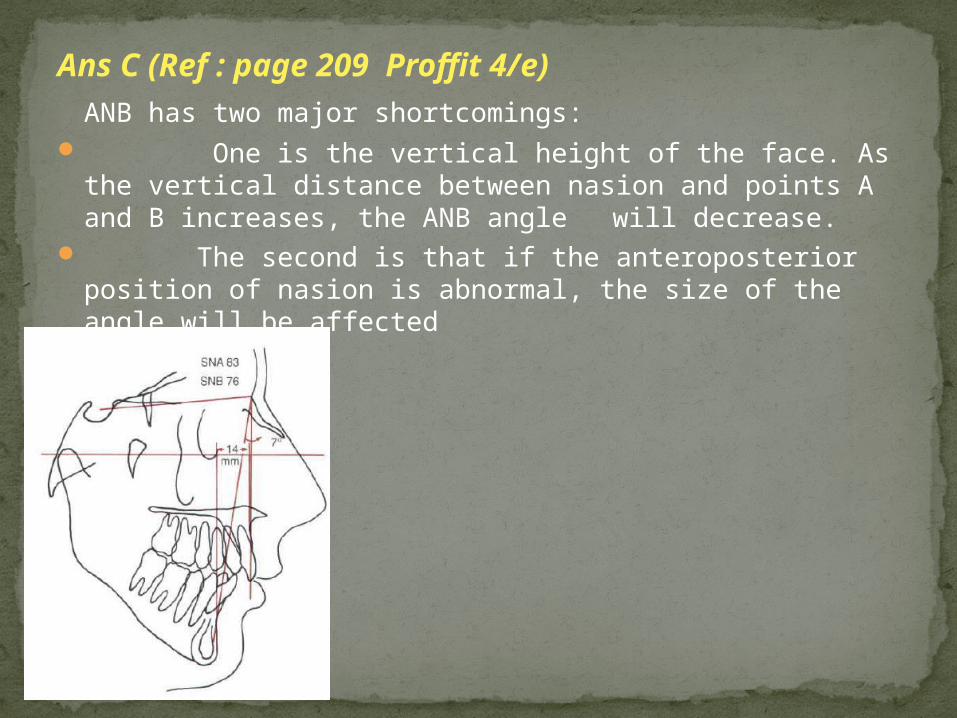
Ans C (Ref : page 209 Proffit 4/e)ANB has two major shortcomings:
One is the vertical height of the face. As the vertical distance between nasion and points A and B increases, the ANB angle will decrease.
The second is that if the anteroposterior position of nasion is abnormal, the size of the angle will be affected
20. A 12-year old male with a history of thumbsucking has an Angle Class II molar relationship with a SNA =83° and a SNB = 79°. The etiology of this patient's malocclusion is
A. dental. B. skeletal. C. neuromuscular.
D. dental and neuromuscular.E. skeletal and neuromuscular.
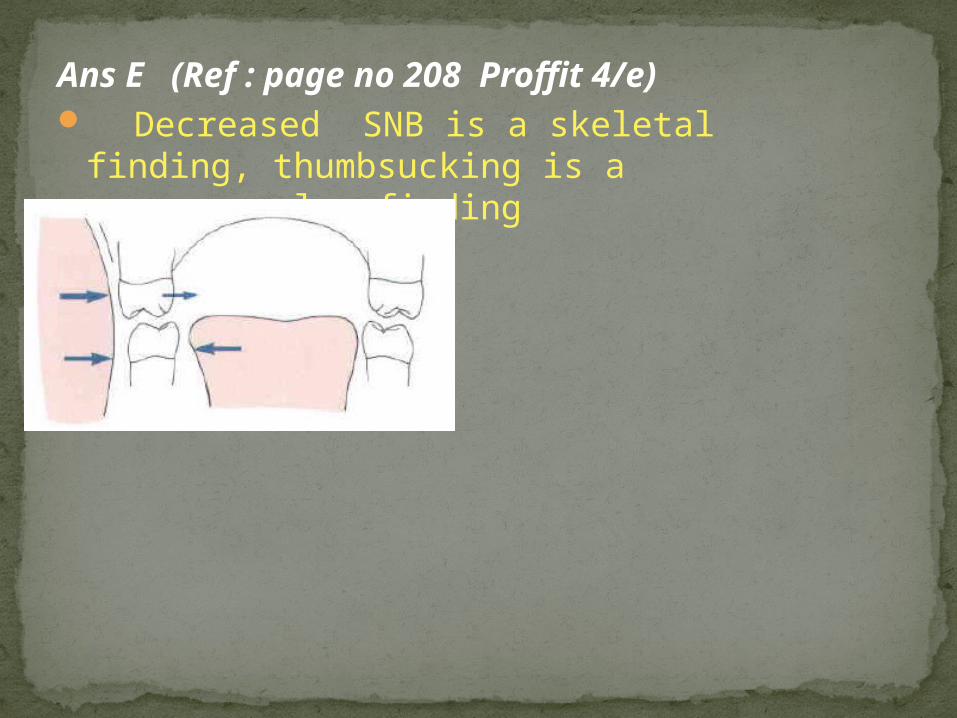
Ans E (Ref : page no 208 Proffit 4/e) Decreased SNB is a skeletal finding,
thumbsucking is a neuromuscular finding
21.Cephalometrics is used in orthodontics toA. treat malocclusions. B. study growth changes.C. aid in diagnosis and case analysis.D. B.and C. E. All of the above
22. Cephalometrics is useful in assessing which of the following relationships?
A. Tooth-to-tooth. B. Bone-to-bone.E. Tooth-to-bone. D. All of the above.
23. In cephalometric analysis of children with malocclusion, the angle ANB is frequently used. In
patients with severe Class~II malocclusion, this angle is
A. greater than the normal. B. less than the normal.C. normal. D. unrelated.
24.Which of the following congenital problems most often results in a malocclusion?
A. cleft palate. B. ectodermal dysplasia.C. Pierre Robin syndrome.D. cleidocranial dysostosis
Ans A The most common craniofacial congenital defect is cleftlip and palate. Its incidence is 1 per 600 -700 live births
25. Angle used the term "subdivision" to refer to a malocclusion in which the abnormal molar relationship was
A. bilateral. B.unilateral. C. only mildly abnormal.D. severely abnormal.E. coupled with labioversion of the maxillary
incisors.

26.Excessive forces used to move teeth will cause
1. a tooth to move faster. 2. a tooth to move slower.
3. root elongation.4. bone to be added uniformly on all
surfaces.5. damage to the periodontal tissues.A. (1)(3)(4) B. (2) and (4)C. (2) (4) (5) D. (2) and (5)
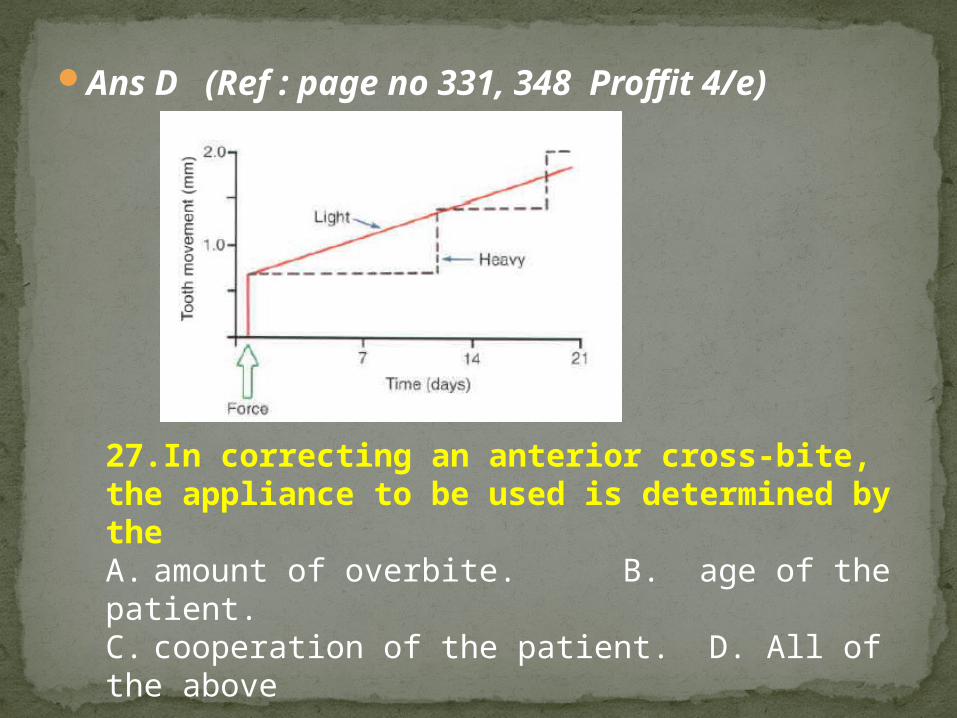
Ans D (Ref : page no 331, 348 Proffit 4/e)
27.In correcting an anterior cross-bite, the appliance to be used is determined by theA. amount of overbite. B. age of the patient.C. cooperation of the patient. D. All of the above
28.Which parameter is a CONTRAINDICATION for serial extraction?
A. Crowding of 7mm or more per quadrant.B. Class I molar relationship. C. Skeletal deepbite.D. Class I skeletal relationship.E. Coordinated dental arches.

Ans C (Ref : page no 490 Proffit 4/e) Serial extraction is directed toward severe
dental crowding.For this reason, it is best used when no skeletal problem exists and the space discrepancy is large-greater than l0mm per arch
29. A skeletal cross-bite always results from a discrepancy inA. eruption patterns.B. mandibular and maxillary bone
structure.C. tongue position (low posture).D. functional centric. E. facial
musculature patterns

Ans B (Ref : page no 437 Proffit 4/e)Skeletal crossbites, usually resulting from a narrow maxilla
but occasionally from an excessively wide mandible, generally are treated by heavy forces to open the midpalatal suture and make the maxilla wider.
30. The body of the mandible increases in length to
accommodate the second molar byA. apposition of bone in the condyle.B. resorption of bone along the anterior border of the
ramus and apposition of bone on the posterior border of the ramus.
C. apposition of bone on the alveolar margin and lower border of the body of the mandible.
D. apposition of bone at the symphysis and posterior border of the ramus of the mandible. E. anterior growth

Ans B (Ref : page no 47 Proffit 4/e
31. Dontrix gauze is used to:A. Measure strength of wire B. Measure force C. Measure wire distortion D. Measure wire deformation
32. In a patient with cleft palate alveolar bone grafting should be done a.After expansion of maxilla & correction of crossbite, but
before cuspid eruptionb.Before expansion of maxilla & correction of crossbite, but
after cuspid eruptionc.Before expansion of maxilla & correction of crossbite, after
cuspid eruption
d.After expansion of maxilla & correction of crossbite, & after before cuspid eruption
33.The last bone in the craniofacial complex to stop growing is the
A. frontal bone. B.nasal bone.C.maxilla.D.mandible.
34. The appliance best suited to achieve rapid maxillary expansion (palatine suture stretching) is a
A. removable appliance with an expansion screw.
B. Nance appliance.C. quad helix appliance. D. fixed Hyrax
appliance

Ans D (Ref : page no 561 Proffit 4/e)Appliance best suited to achieve rapid maxillary expansion (palatine suture stretching) is a fixed Hyrax appliance. Hyrax is an acronym for hygienic rapid expander. The screws have heavy gauge wire extensions that are adapted to follow the palatal contour
35. A labia frenum causes a diastema between the maxillary permanent central incisors. The lateral incisors and canines have not erupted. The most appropriate treatment is to
A. perform a frenectomy.B. close the space with an orthodontic
appliance.C. observe the case until the eruption of
maxillary permanent lateral incisors and canines.
D. close the space with an elastic band, close the space after the eruption of the lateral incisors

36. Which of the following represents the correct patient position for the left lateral cephalogram.
a.Mid sagittal plane should be 5 feet from the tube.
bRight ear should be 5 feet from the tube.c.Left ear should be 6 feet from the tube.d.Left ear should be 5 feet from the tube.
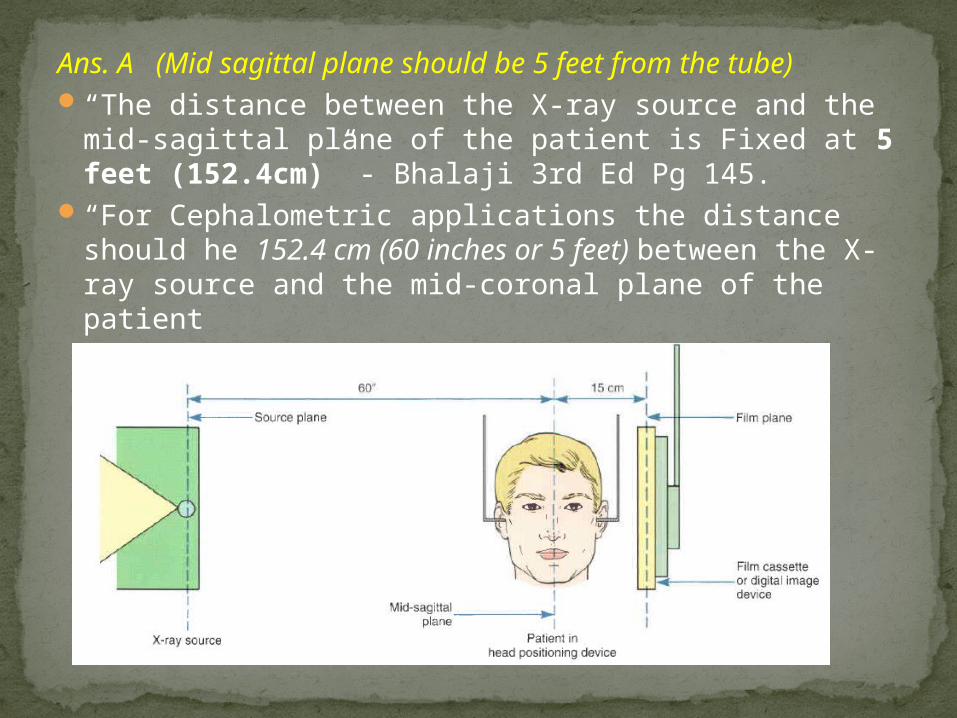
Ans. A (Mid sagittal plane should be 5 feet from the tube)
“The distance between the X-ray source and the mid-sagittal plane of the patient is Fixed at 5 feet (152.4cm)” - Bhalaji 3rd Ed Pg 145.
“For Cephalometric applications the distance should he 152.4 cm (60 inches or 5 feet) between the X-ray source and the mid-coronal plane of the patient

37. Which occlusal parameter is the most useful to determine if a posterior crossbite is of skeletal or dental origin?
A. Anterior overbite. B. Sagittal molar relationship.
C. Lack of space in the maxillary anterior area.
D. Lack of space in the mandibular arch.E. Buccolingual angulation of affected
teeth
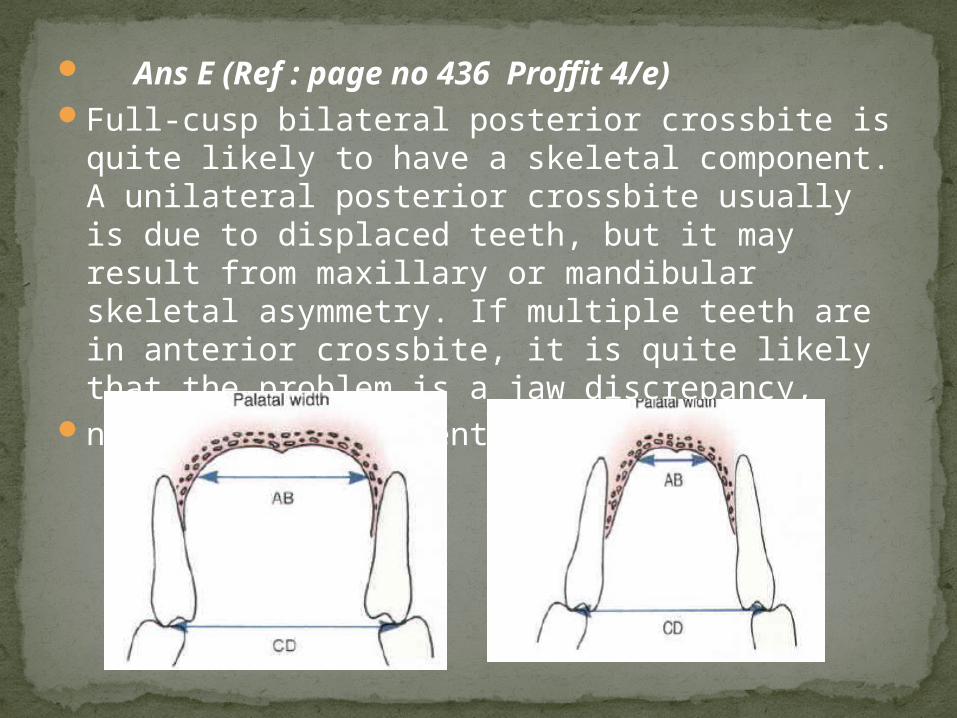
Ans E (Ref : page no 436 Proffit 4/e)Full-cusp bilateral posterior crossbite is quite
likely to have a skeletal component. A unilateral posterior crossbite usually is due to displaced teeth, but it may result from maxillary or mandibular skeletal asymmetry. If multiple teeth are in anterior crossbite, it is quite likely that the problem is a jaw discrepancy,
not just displacement of teeth.

38. The most appropriate time for surgical treatment in a female patient with mandibular prognathism is
A. just before the beginning of the prepubertal growth spurt.
B. just after the end of the prepubertal growth spurt.
C. just before eruption of the second permanent molars.
D. just after eruption of the second permanent molars.
E. after the completion of growth

39.If interincisal distance is 131 degree, it implicates.
a.Maxillary incisors are retroclinedb.Incisors are proclined c Incisors are crowdedd.Incisors are retroclined
40. In cephalometric analysis, Y axis is formed by
a.Angle formed by plane joining sella to gnathion & FH plane.
b.Angle formed by plane joining nasion to gnathion & FH plane.
c.Angle formed by mandibular plane & FH plane.d.It is another name for IMPA
41. The most common clinical characteristic/s of a buccolingual functional crossbite is/are
A. mandibular shift from initial contact to maximum intercuspation with midline deviation.
B. asymmetrical arches. C. several missing teeth
42. The most damaging characteristic of a Class II, Division 2 (Angle) malocclusion is the
A. deep overbite.B. crowding of the mandibular incisors.C. Class II relationship of the molars.D. impaction of the maxillary canines.E. malposition of the maxillary lateral incisors

43. Which of the following malocclusions should be corrected as soon as it is diagnosed?
A. A severe Class II, Division 1.B. A severe Class II, Division 2.C. A cross-bite with a lateral functional shift.D. A diastema between the maxillary central incisors
44. A maxillary posterior buccal crossbite in the deciduous dentition will most likely
A. be present when the permanent teeth erupt.B. correct itself when the permanent teeth erupt.C. be self-correcting with the discontinuance of
an associated habit.D. be associated with inadequate arch length.

45. A bimaxillary protrusion occurs whenA. a large overjet of the maxillary central incisors exists.B. the maxillary dentition is in a forward position to the
basal bone.C. the maxillary and mandibular incisors are in a forward
position to the basal bone.D. None of the above.
46. A clinical diagnostic indication of palatal impaction of maxillary permanent canines does NOT include
A. proclined and laterally flared permanent lateral incisors.
B. delayed exfoliation of primary canines.C. midline central diastema.D. lack of canine buccal bulges in a 10 year old patient
47. To prevent mesial migration of permanent 1st molar tooth, what is the ideal time to give space maintainer in case of premature loss of primary 2nd molar ?
A. After healing of the extraction socket B. Immediately after extraction of the tooth C. After the permanent 2nd molar has
erupted D. After the tooth pierces the gingival tissue48. In patients with cleft palates there may beA. an increase in supernumerary teeth.B. an increase in congenitally missing teeth.C. a higher incidence of crown defects.D. All of the above.

49.Which two muscles are involved in sucking?A. Caninus and depressor angularis.B. Risorius and buccinator.C. Buccinator and orbicularis oris.D. Levator labii superioris and zygomaticus major.
50. In clinical dentistry, stiffness of wire is a function of
A. length of the wire segment.B. diameter of the wire segment. C. alloy
omposition.D. All of the above. E. None of the above.
Related Documents