NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies Tuesday 4 th September 2018, 2.30pm – 5.00pm The Conference Suite, Bridge Centre, Birches Head Road, Birches Head, ST2 8DD Agenda Agenda No Item description Enc./ Table / Pres. Decision / To Note / Discussion / Information Item Presenter 1 Welcome and Apologies for Absence: Verbal To Note RC 2.30pm (5 mins) 2 Declarations of Interest North Staffordshire CCG & Stoke-on-Trent CCG : If any member of the Committee or invited attendee has any pecuniary interest, in any contract, proposed contract or other matter under consideration at this meeting he/she shall disclose the fact to the Chairman and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it unless agreed by the Chairman and members of the committee 3 Confirmation of Quoracy (following consideration of interests declared pertaining to the agenda) North Staffordshire CCG Stoke-on-Trent CCG 4 Minutes from: Public Meeting In Common of The North Staffordshire and Stoke- on-Trent Clinical Commissioning Groups’ Governing Bodies held on Tuesday 7 th August 2018 Action List and Matters Arising Enc. 4.1 Enc. 4.2 To Note / Decision 5 North Staffordshire and Stoke-on-Trent CCGs Risk Register and Board Assurance Framework - 2017/18 Sally Young, Director of Corporate Services, Governance and Communications Enc. 5 Assurance SY (10 mins) 6 Strategic 2.45pm 6.1 Chairs Address Matters Discussed in the Closed Section Enc. 6.1 To Note AB (10 mins) 6.2 Accountable Officers Report Marcus Warnes, Accountable Officer Enc 6.2 To Note MW (10 mins)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes
NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Tuesday 4th September 2018, 2.30pm – 5.00pm The Conference Suite, Bridge Centre, Birches Head Road, Birches Head, ST2
8DD
Agenda
Agenda No
Item description Enc./ Table / Pres.
Decision / To Note / Discussion / Information
Item Presenter
1 Welcome and Apologies for Absence:
Verbal To Note
RC 2.30pm (5 mins)
2
Declarations of Interest North Staffordshire CCG & Stoke-on-Trent CCG :
If any member of the Committee or invited attendee has any pecuniary interest, in any contract, proposed contract or other matter under consideration at this meeting he/she shall disclose the fact to the Chairman and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it unless agreed by the Chairman and members of the committee
3
Confirmation of Quoracy (following consideration of interests declared pertaining to the agenda)
North Staffordshire CCG Stoke-on-Trent CCG
4
Minutes from: Public Meeting In Common of The North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies held on Tuesday 7
th August 2018
Action List and Matters Arising
Enc. 4.1 Enc. 4.2
To Note / Decision
5
North Staffordshire and Stoke-on-Trent CCGs Risk Register and Board Assurance Framework - 2017/18 Sally Young, Director of Corporate Services, Governance and Communications
Enc. 5
Assurance
SY
(10 mins)
6 Strategic 2.45pm
6.1 Chairs Address
Matters Discussed in the Closed Section
Enc. 6.1 To Note AB
(10 mins)
6.2
Accountable Officers Report Marcus Warnes, Accountable Officer
Enc 6.2 To Note MW
(10 mins)

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes
NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE
6.3
Urgent and Emergency Care
Staffordshire and Stoke-on-Trent Urgent and Emergency Care (UEC) Programme Briefing
Winter Plan Cheryl Hardisty, Director of Commissioning and Operations
Enc 6.3
Enc 6.3a
Assurance/To Note
CH (10 mins)
6.4 STP Update Marcus Warnes, Accountable Officer
Enc 6.4
To follow
Assurance/To Note
MW
(10 mins)
7 Quality 3.25pm
7.1 Quality Report Heather Johnstone, Director of Nursing and Quality
Enc. 7.1 Assurance/To
Note HJ
(15 mins)
8 Finance , Performance and Planning 3.40pm
8.1 Financial Update – North Staffordshire and Stoke-on-Trent CCGs Alistair Mulvey, Chief Finance Officer
Enc. 8.1 To Note AM
(15 mins)
8.2
Governing Board Performance Report Kara Lawrence, Deputy Director of Strategy, Planning and Performance
Enc. 8.2
To Note
KL (15 mins)
9 Committees - Reports and Matters for Decision 4.10pm
9.1
Primary Care Commissioning Committee in Common Report Peter Dartford / Margy Woodhead, Lay Members Patient and Public Involvement
Enc. 9.1 Decision/ Assurance
PD/MWo (5 mins)
9.2 Planning and Commissioning Committee in Common Report Dr Steve Fawcett, Medical Director
Enc. 9.2 Decision / Assurance
SF (5 mins)
9.3 Transforming Care Partnership Board Update Dr Waheed Abbasi, Clinical Director
Verbal Assurance WA
(5 mins)
10 Any Other Business 4.25pm
Questions from the Public Any other key issues
Verbal Verbal
Information RC
DATE/TIME OF NEXT MEETING:
Date Time Venue Chair
Tuesday 2nd
October 2018 2.30pm The Churnet Room, Moorlands House, Stockwell Street,
Leek, ST13 6HQ AB

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 1
Members:
Qu
ora
cy
10
/04
/20
18
01
/05
/20
18
07
/08
/20
18
04
/09
/20
18
02
/10
/20
18
06
/11
/20
18
04
/12
/20
18
Present:
North Staffordshire CCG Voting Members:
Dr Alison Bradley AB North Staffordshire CCG Clinical Chair (Chair) ✓ ✓ ✓
Peter Dartford PD Lay Member – Patient and Public Involvement ✓ ✓ x
Mike Edgley ME Lay Member ✓ ✓ ✓
Neil McFadden NMcF Lay Member – Governance ✓ ✓ ✓
Dr Doug Robertson DR Secondary Care Board Member x ✓ x
Stoke-on-Trent CCG Voting Members:
Dr Ruth Chambers OBE RC Stoke-on-Trent CCG Clinical Chair ✓ ✓ ✓
Tim Bevington TB Lay Member ✓ ✓ ✓
Dr John Gilby JG Clinical Director – Primary Care ✓ ✓ ✓
John Howard JH Lay Member – Governance ✓ ✓ ✓
Dr Simon Mellor SM Secondary Care Board Member x x ✓
Margy Woodhead MWo Lay Member – Patient and Public Involvement ✓ ✓ ✓
North Staffordshire and Stoke-on-Trent CCGs’ Voting Members:
Dr Waheed Abbasi WA Clinical Director – Mental Health and Specialist Groups
x ✓ ✓
Dr Lorna Clarson LC Clinical Director – Partnerships and Engagement ✓ ✓ ✓
Cheryl Hardisty CH Director of Commissioning and Operations ✓ ✓ ✓
Dr Latif Hussain LH Non-Executive GP Board Member x x ✓
Zara Jones ZJ Director of Strategy, Planning and Performance ✓ ✓ ✓
Dr Steve Fawcett SF Medical Director ✓ x ✓
Heather Johnstone HJ Director of Nursing and Quality ✓ ✓ ✓
Alistair Mulvey AM Chief Finance Officer ✓ ✓ ✓
Marcus Warnes MWa Accountable Officer ✓ ✓ x
In attendance:
North Staffordshire and Stoke-on-Trent CCGs:
Anna Collins AC Associate Director of Communications and Engagement
✓ ✓ ✓
Melanie Mahon MM Head of Primary Care Commissioning x x ✓
Stacey Thursfield ST Executive Assistant (Minutes) x x ✓
Paul Winter PW Deputy Director of Corporate Services, Governance and Communications
x x ✓
Staffordshire Single Leadership Team:
Lynn Millar LM Director of Primary Care ✓ ✓ x
Mark Seaton MS Managing Director – North ✓ ✓ ✓
Sally Young SY Director of Corporate Governance, Communications and Engagement
✓ ✓ ✓
Public/Observers
Simmy Akhtar SA Healthwatch Stoke-on-Trent x ✓ ✓
Jakob Oguntimehin JO Medical Student x x ✓
Dr Paul Scott PS North Staffordshire LMC Chair x ✓ x
5 members of public/press in attendance.
Public Meeting of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies held in Common Tuesday 7th August 2018, 2.30pm – 5.00pm
The Conference Suite, Bridge Centre, Birches Head Road, Birches Head, ST2 8DD
Unconfirmed Minutes

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 2
2018/AUG
/063
1. Welcome and Apologies for absence Action
AB welcomed members to the public meeting of the North Staffordshire and Stoke-on-Trent CCG Governing Bodies held in Common. Apologies were duly received and noted as above.
2018/AUG
/064
2. Members’ Declarations of Interest Action
No further declarations of interest made
2018/AUG
/065
3. Confirmation of Quoracy
The meeting was confirmed as quorate for North Staffordshire CCG and Stoke-on-Trent CCG.
2018/AUG
/066
4. Minutes, Action Sheet and Matters Arising
Minutes from the meeting held on Tuesday 1
st May 2018
The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies duly received and approved the minutes of the public session of the North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies held in common on Tuesday 1
st May 2018.
Minutes from the Annual General Meeting held on Tuesday 3
rd July 2018
The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies duly received and approved the minutes of the Annual General Meeting of the North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies held in common on Tuesday 3
rd July 2018.
Action List and Matters Arising Actions contained within the action list were agreed as complete. Action on page 6 of the minutes of the 1
st May to be included on the action list:
SY to present the Governing Bodies with the refreshed Risk Register in September 2018 – on agenda for 7
th August 2018.
2018/AUG
/067
5. North Staffordshire CCG and Stoke-on-Trent CCG Risk Register and Board Assurance Framework – 2017/18
SY presented the Governing Bodies with the latest update in relation to the Risk Register and Board Assurance Framework. The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to note the assurances for risks scoring 15 and above, review the content and layout of the risk register and note the work being undertaken to align the risk registers. Details presented as follows: SY explained that work is being undertaken to align the risk registers (clinical and non-clinical) across North Staffordshire CCG, Stoke-on-Trent CCG, East Staffordshire CCG, Cannock Chase CCG, Stafford and Surrounds CCG and South East Staffs and Seisdon Peninsula CCG. The Governance team is meeting on an individual basis with Executive Directors to look at the risk and residual risk reporting thereby identifying whether any risks can be reduced in scoring or recommended for closure. The Governance team are working closely with PWC to drive forward a risk culture across the organisation and are in the process of writing a new common Risk Strategy. This will incorporate best practice from across the three localities – North, South and East. SY explained that PWC would be attending one of the weekly Executive Management Team meetings to provide training around risk management, going forward, it is expected that the Executive Team will review the
NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 3
risk register on a monthly basis. JH thanked SY for the assurance around the progress of the Risk Register noting that members of the Audit Committee would like confirmation that current arrangements need to stay in place until the updated work is complete and ready to be implemented with ME supporting his statement. SY agreed and assured Governing Bodies that there is a robust transition plan in place. NMcF queried whether minutes are taken at the weekly Executive Management Team meeting for the purposes of an audit trail in relation to the risk register. SY confirmed that action notes are taken and a decision log kept so any discussion around risks will be logged, an update will also be included in the register itself. To conclude, North Staffordshire CCG Governing Body noted the assurances for risks scoring 15 and above, reviewed the content and layout of the risk register and noted the work being undertaken to align the risk registers; and Stoke-on-Trent CCG Governing Body noted the assurances for risks scoring 15 and above, reviewed the content and layout of the risk register and noted the work being undertaken to align the risk registers.
2018/AUG /068
6.1 Clinical Chairs’ Address
RC welcomed attendees of the meeting of the Governing Bodies acknowledging the efforts across the CCGs along with system partners to respond to pressures on urgent care, NHS constitutional standards, the financial position, planning requirements, delivery of the financial recovery plan and the Together We’re Better Sustainability and Transformation Partnership (STP) which continue to be our key priorities. The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the Chairs’ Address. Details presented as follows: The Integrated Care Record (ICR) procurement is progressing and will provide a revolutionary new way of providing health and care in Staffordshire and Stoke-on-Trent. This electronic system will link NHS and local government organisations more closely than ever before in order to provide the best possible care. The critical role that digital innovation and technology will play in the transformation of health and care in Staffordshire and Stoke-on-Trent was highlighted at a regional conference hosted by Together We’re Better. Health and care professionals from across the area attended the conference to learn about how digital can, and is being utilised to enhance services and improve peoples’ lives, the event was chaired by the Senior Responsible Officer(SRO) for the programme, Caroline Donovan. NHS staff across Staffordshire and Stoke-on-Trent celebrated the 70
th birthday of the NHS on
Thursday 5th July with over 30 events taking place across the area. RC noted that an example
of this was a van hosted on Tesco car park which encouraged members of the public to calculate their heart age; this was visited by 55 people. The Chairs of the Staffordshire CCGs continue to meet on a monthly basis along with MW to explore how work can be better joined up and done once where possible instead of six times. Decisions will also be made at a local level where applicable and it is important that this is maintained as we operate across a bigger system footprint. A much wider meeting which includes the lay members of the six CCGs now meets on a quarterly basis. RC noted that the Management of Change process has formally ended and staff are working to the new structures which seek to achieve economies of scale whilst maintaining local focus.
The clinical leadership is still under discussion; the Chairs along with SF and the clinical directors including LC are involved in this piece of work for the north locality to consider what clinical involvement the northern division needs. The North Staffordshire CCG and Stoke-on-Trent CCG Annual General Meeting in common was held on Tuesday 3
rd July at the Bridge Centre, Birches Head. Patients and members of the
public from across North Staffordshire and Stoke-on- Trent came together to celebrate the 70th

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 4
anniversary of the NHS and hear of future plans for improved healthcare. SA acknowledged the updates from RC in particular around the closer working between the CCGs and doing something once rather than six times and queried the progress around the Joint Strategic Commissioning Committee, what is the timeframe for this to be in place? SY confirmed that the aim is to have the first meeting in shadow form in September 2018; the Terms of Reference are being drafted and will be shared with the Governing Bodies. RC noted that the Governing Bodies of the six Staffordshire CCGs had met in July and it had been a very constructive meeting.
To conclude, the North Staffordshire CCG Governing Body received and noted the Clinical Chairs’ address; and Stoke-on-Trent CCG Governing Body received and noted the Clinical Chairs’ address.
2018/AUG/ 069
6.2 Accountable Officer’s Report
AM presented the Accountable Officer report in the absence of MW providing an update to the Governing Bodies around the current environment the CCGs have been operating in. In addition, the paper described progress with regards to the CCGs’ financial position, the Better Care Fund (BCF), STP and the Pre-Consultation Business Case. The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the August report. The report was taken as read by the Governing Bodies and details were presented as follows: After three months the CCGs are reporting an £8.5m adverse variance to plan, with actual performance being a combined deficit of £6.95m against a planned surplus of £1.65m. Within the overall position there is a pressure of a shortfall in QIPP plans of £2m with other pressures manifesting in increased costs of acute care provision most notably non-elective care. A&E performance has continued to improve since the Easter period; this is despite increased pressure resulting from the heatwave over recent weeks. The validated month two performance against the four hour standard was 83.8% (a 3.8% improvement on month one). The CCGs continue to work with partners to manage demand and to ensure that sufficient bed and home based capacity is in place to facilitate timely discharge. The Pre-Consultation Business Case (PCBC) in relation to the Future of Local Health Services in Northern Staffordshire was presented to the NHS England Assurance Panel on the 17
th July.
This was attended by CCG colleagues and Chief Executive colleagues from University Hospital North Midlands (UHNM), Midlands Partnership Foundation Trust (MPFT), Stoke-on-Trent City Council, Staffordshire County Council and Staffordshire and Stoke-on-Trent Sustainability and Transformation Partnership (STP). Formal feedback has been received from NHS England and a further meeting with them is planned for Friday 17
th August 2018.
The CCGs continue to work closely with STP colleagues, the STP Director, Simon Whitehouse, was in attendance at the confidential meeting of the Governing Bodies to discuss how to strengthen both clinical and patient engagement within the programme. Work has been taking place to strengthen clinical leadership and accountability within the partnership; this is being delivered through the STP Clinical Chairs and Lay Members meeting. Stoke-on-Trent CCG and the City Council have agreed and submitted the quarter one report template in relation to BCF progress. Performance for Stoke-on-Trent delayed transfers of care continues to improve; however the CCG and Stoke-on-Trent City Council continue to work closely with MPFT to ensure that the commissioned capacity continues to be available to carry on this reduction. There has been significant progress made in relation to the delivery of the improvement plan that resulted from local system review by the CQC. Stoke-on-Trent CCG and the City Council have agreed on a draft integrated commissioning strategy that will be overseen by a newly re-constituted Health and Wellbeing Board. A more detailed delivery plan is in development and expected to be presented at the Health and Wellbeing Board in September where the CCGs are represented by MS.

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 5
As previously reported, the Management of Change process concluded on 1
st May 2018.Staff
vacancies that resulted from this have now been advertised and recruitment commenced. Clinical leadership is still being discussed. The six Staffordshire CCGs’ Governing Bodies met in common on the 19
th July to discuss the
new governance arrangements. These discussions will continue in the coming weeks with Governing Body members fully engaged and driving the shape of future governance arrangements from both a corporate and clinical management governance perspective. TB made reference to paragraph 4.8 which relates to the planning gap identified by the STP and queried what impact that will have on the CCGs, in particular, in relation to the fines and penalties issue with UHNM. AM noted that this is not just a financial diagnostic but system wide and is a piece of work that CH is leading on for the CCGs. It will consolidate previous reviews to produce a cohesive shared view of the local issues of which it is expected fines and penalties will be one of them. System leaders will agree the list of issues and solutions and then map these through to the individual organisations. JH acknowledged the update around the Management of Change process and noted that this has also been monitored via the Organisational Development (OD) Committee. One of the unintended consequences of the process that has been noted by the OD Committee is that due to the number of vacancies across the organisations a number of staff are still doing work from their old role as well as their new. AM agreed and the Executive Team recognise the hard work of staff both during and after the process. Filling the vacancies is critically important and the message shared across the organisation is that work should be rationalised where possible, Directors are working closely with staff to ensure they are focused on the key organisational priorities. SY confirmed that she is working with Lisa Kelly, CSU Business Partner to write an end of process report which will include feedback from Unison; this will be shared with both the Governing Bodies and the OD Committee. To conclude, the North Staffordshire CCG Governing Body received and noted the Accountable Officer’s report; and Stoke-on-Trent CCG Governing Body received and noted the Accountable Officer’s report.
2018/AUG/ 070
6.3 Extended Access – Melanie Mahon, Head of Primary Care Commissioning in attendance
MM presented the report regarding the Extended Access Contract Award, North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to ratify the decision made at the Assurance Panel and to approve the issue of contracts for signature. The Governing Bodies were also asked to receive and note the details within the paper, including the assurance panel process. RC took over as Chair and advised that the practising clinical Board Members would stay in the meeting to discuss the item, but would not be able to provide an opinion and would then leave the room while the remaining members took a vote. MM explained that the purpose of the report was a follow up to the decision made by the Governing Bodies in February and to inform the Governing Bodies of the process taken for the award of the Extended Access Contract, including details around the Assurance Panel, finance and the outcome of the award and to obtain ratification for the panels’ decision to award. Following the decision taken in February 2018 an engagement and assurance process was developed, whereby the primary care localities across Staffordshire were asked to submit proposals for consideration by a non-conflicted panel. The aim of the panel was to obtain assurance that the submitted proposals will deliver the core criteria within the specification. The panel was assured that the North Staffordshire GP Federation would be able to meet the requirements of the Extended Access service specification for patients across both North Staffordshire CCG and Stoke-on-Trent CCG. The decision of the direct award was on the basis that local GP practices are the only providers who could ensure a level of additionality was

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 6
provided over and above the seven core requirements set nationally. The proposal from North Staffordshire GP Federation is for over 400 additional hours which is above the request of an additional 267, 400 hours would equate to approximately 1700 additional 15 minute appointments. SA queried what communications have been planned to get the message out to patients. MM confirmed that a communication plan had been developed and would go across Staffordshire to ensure that the communication for patients was consistent. Information should be included on all GP practice websites and NHS England will be performing spot checks to ensure this has been done. Conflicted clinical members left the meeting. AM asked if we were clear we were going to deliver all 7 requirements and what was the value of what we got for the direct award instead of going out to tender. MM responded that all 7 core requirements had been met. She confirmed that we were getting more hours and all 7 core requirements would be delivered. AM asked what the additionality was. MM stated that NHS England had brought the timeline forward with all services now being live by 1
st September. For the additionality, the contract will
ensure that a Service Development Improvement Plan (SIP) is written and agreed between the provider and the CCG by 31
st January with the proposals to be in place by April 2019. If a plan
is not agreed then there is a clause in the contract which could result in the contract being terminated.
AM queried how they will measure the principles around underpinning integrated working for the future to deliver new models of care, that delivery solutions are developed with the engagement and support of all practices and localities and, developing the workforce to help support the sustainability of primary care. MM confirmed they would measure the baseline now against what they would expect to see next year; this would be included in the contract to ensure they deliver against the baseline. JH queried what arrangements are in place for monitoring and MM confirmed that it would be managed in the same way as an acute contract including monthly KPIs and friends and family surveys. MWo noted the importance of a patient satisfaction survey. To conclude, the North Staffordshire CCG Governing Body and Stoke-on-Trent Governing Body were asked to: 1. Ratify the recommendation made at the Assurance Panel 2. Approve the issue of contracts for signature
In relation to recommendation one, North Staffordshire CCG ratified the recommendation made at the Assurance Panel and; Stoke-on-Trent CCG ratified the recommendation made at the Assurance Panel. In relation to recommendation two, North Staffordshire CCG approved the issue of contracts for signature and; Stoke-on-Trent CCG approved the issue of contracts for signature. Following discussions around additionality and patient satisfaction, North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies requested the following caveat North Staffordshire CCG and Stoke-on-Trent CCG approved the award of the contract subject to the additionality being quantified and measurable within the contract, and subject to regular patient feedback to ensure the service is fit for purpose.
2018/AUG/ 071
6.4 Appointment Process for the Stoke-on-Trent CCG Chair and Secondary Care Consultant
SY presented the report in relation to the appointment process for the Stoke-on-Trent CCG Chair and Secondary Care Consultant. The report relates to Stoke-on-Trent CCG only and Governing Body members were asked to be assured by the process outlined within the paper

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 7
for the recruitment of the CCG Chair and Secondary Care Consultant. SY confirmed to the Governing Bodies that the Chair of Stoke-on-Trent CCG has announced her intention not to seek a further term of office in her role as CCG Chair, as has the Stoke-on-Trent CCG Secondary Care Consultant. A Remuneration Committee meeting was held prior to the meeting of the Governing Bodies and both posts have been approved to be sent out to advert. The advert and job description for the Clinical Chair will be sent out to GPs in Stoke-on-Trent and they will have four weeks to respond. A provisional interview date has been agreed as the 18
th September but the final decision to recruit will be made by the Membership. Applications
must be supported by five GPs in line with the process set out in schedule 2 of the constitution. The role of the Secondary Care Consultant will be advertised on NHS jobs and will be subject to a formal interview process. The interview panel will include the Stoke-on-Trent CCG Chair, the Accountable Officer, a Lay Member and the Medical Director. The post has been reviewed and it has been agreed the number of sessions will now align to those done by the North Staffordshire CCG Secondary Care Consultant – 2 days per month instead of 2.5 days per month. To conclude, the Stoke-on-Trent CCG Governing Body was assured by the update in relation to the appointment process for the Stoke-on-Trent CCG Chair and Secondary Care Consultant report.
2018/AUG/ 072
7.1 Quality Report
HJ provided the Governing Bodies with an update in relation to quality issues across the North Staffordshire and Stoke-on-Trent areas. The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to note for assurance the items discussed at the May and 2018 Quality Committees in Common. Details were presented as follows: The quarter four and annual reports in relation to GP Event Reporting were received by the committee. Key points noted were that 72 out of 76 practices reported on the Datix system and the number of events reported increased by 5% in 17/18 from 16/17. The process in the north locality has been recognised as an example of good practice and this will be rolled out across the other localities. The Quality Committee continue to review the clinical risk register and noted that as work streams relating to HCAI have successfully reduced levels of avoidable HCAI to within nationally determined objectives, the two risk associated with this have been closed but continue to be monitored. HJ highlighted that the June 2018 Joint Quality Committee received the Provider Failure Standard Operating Procedure (SOP) for information and assurance. The SOP has been developed jointly between Staffordshire County Council and the Staffordshire CCGs. The CCGs have been involved with developing the procedure and will adhere to its requirements in the event of an urgent failure of a care home or care provider, where NHS funded patients are involved / placed. The SOP details the procedures that need to be followed in the event of an urgent / non-urgent closure of a care home, or home care provider, where the home has failed or is failing. Stoke-on-Trent City Council has also agreed to adopt the SOP. In July 2018 there was a pilot Single Joint Quality Committee which covered all six of the Staffordshire CCGs. Members are currently reviewing how effective the pilot meeting was and will feedback at the September meeting. Going forward, the meeting will be known as the Joint Quality and Safety Committee, there will still be an option for smaller divisional based meetings if there is a locality based issue that needs addressing.
HJ, on behalf of the CCGs, expressed condolences to the family, friends and colleagues of local midwife, Samantha Eastwood, following the recent tragic events reported in the news. HJ has offered her support to Liz Rix, Chief Nurse at University Hospital North Midlands and asked that this offer be extended to the rest of her team. The CCGs will also formally write to the Trust.

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 8
NMcF queried the reporting of never events and serious incidents going forward. HJ confirmed that a new dashboard is being developed; this will be across all six of the Staffordshire CCGs and will be a high level summary. The numbers and trends will be identified but the more specific detail will be limited in order to protect the patient. Due to the nature of the events too much detail could make them identifiable. To conclude, the North Staffordshire CCG Governing Body received and noted the Quality Report; and Stoke-on-Trent Governing Body received and noted the Quality Report.
2018/AUG/ 073
8.1 Financial Update
AM presented the current financial position to members of the Governing Bodies, North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the content of the report. Details were presented as follows: At the end of quarter one, the position for both CCGs combined is a £8.60m adverse variance against plan with a £6.96m in-year actual deficit reported (North Staffs £3.65m deficit, Stoke-on-Trent CCG £3.30m deficit). This compares to a planned position at month 3 of a £1.65m surplus (North Staffs £0.2m surplus, Stoke-on-Trent £1.45m surplus). AM explained that with the overall financial position the following key points should be noted, the CCG has concerns over the level of activity being reported by UHNM, non-elective figures have significantly changed since March 2018, SF has a meeting in place to look at the various emergency portals to determine whether there has been a change in the counting and coding of patients and a contract challenge has already been submitted in relation to this. Due to the slippage in the forecast financial positon the CCGs are in financial escalation with NHS England with the next meeting scheduled for Friday 17
th August. Preparation for the
meeting is underway and the CCGs will be expected to explain the current financial position in relation to the plan. JH noted that the report is in relation to 18/19 and queried the progress of 17/18 in relation to the fines and penalties dispute with UHNM. AM confirmed that the CCGs are entering into expert determination with UHNM in relation to financial year 2017/18 which includes disputes over CQUIN payments and fines and penalties, the paperwork has been submitted to NHS England and NHS Improvement this week. AM confirmed that the CCGs have applied the fines and penalties in line with the contract, auditors have reviewed the paperwork and agree that they have been applied appropriately. Following the external expert determination process if it is deemed that the fines were not appropriate this decision would impact on both last year’s accounts and this year as the terms of the contract are the same. AM noted that in 17/18 UHNM didn’t agree the control total, didn’t apply for the STF funding and therefore fines should be applicable. NMcF queried whether the CCGs are continuing to apply the fines and penalties in 18/19 given the dispute with UHNM. AM confirmed that the CCGs continue to apply the contract, the CCGs consider where to reinvest the money from fines and have invested significantly in community services and A&E, and the improvement in performance is highlighted in the Performance Report included with the Governing Body papers.
To conclude, the North Staffordshire CCG Governing Body received and noted the Finance Report; and Stoke-on-Trent Governing Body received and noted the Finance Report.
2018/AUG/ 074
8.2 Performance Report
ZJ presented the current performance to members of the Governing Bodies, North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the content of the report. Details were presented as follows:
NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 9
ZJ presented the report and stated that there has been a steady improvement in A&E performance and in May performance was 83.8% which was the highest since April 2017. There has been a reduction in the delayed transfers of care with schemes in place to improve flow. UHNM are planning to achieve 90% by September 2018 by redesigning flow through majors to allow greater in-reach, and then 95% by March 2019.
In relation to West Midlands Ambulance Service (WMAS) have achieved both the mean and the 90
th centile response targets for category 1, 2, 3 and 4 response targets in month two. There
have been issues around 111 which has seen a continuous deterioration but new national indicators are expected to be released shortly which will change the focus. Referral To Treatment (RTT) waiting times are similar to last month with the total 18 week backlog accounting to 25% of the total waiting list. For UHNM to achieve the 92% standard they would need to clear 8178 patients from the backlog which is 3 – 4 months’ work. Commissioners are meeting colleagues at UHNM fortnightly to support the management of the waiting lists. North Staffordshire CCG failed the standard in month two for diagnostic waits which are underperforming by 0.2%. East Cheshire NHS Trust was the main provider that contributed to this with 28/208 tests failing to be done within 6 weeks for the north Staffordshire cohort of patients.
The cancer performance in June for the 62 day from GP referral target is at 82.4% against the 85% target. Most recent data shows that they achieved 85% in July which is really positive but needs to be sustained. Confirmation has been received in relation to the CCGs’ Improvement and Assessment Framework (IAF) ratings. Both North Staffordshire CCG and Stoke-on-Trent CCG have gone
from ‘requires improvement’ to ‘good’ which is really positive but needs to be sustained. MWo referred to the RTT waiting times and queried the progress of the Medway system. SF agreed with the challenge around the backlog and that they are working closely with UHNM regarding how to tackle this and ensure patient safety. SF noted that Medway is not working as anticipated but it was never expected to be the solution to the backlog. SF has been invited to the UHNM Planned Care Board and following this will feedback to the Governing Bodies. JH noted this will be the last meeting of the Governing Bodies for ZJ and thanked her for her contributions during her time as Director of Strategy, Planning and Performance and commended the performance reports that are received by the Governing Bodies for the level of detail and the up to date information. RC commended the Executive Directors and their teams on the excellent IAF results. To conclude, the North Staffordshire CCG Governing Body received and noted the Performance Report; and Stoke-on-Trent Governing Body received and noted the Performance Report.
SF
2018/AUG/ 075
9.1 Primary Care Commissioning Committee in Common Report
The Governing Bodies received the Primary Care Commissioning Committee in Common Chairs’ report detailing the matters discussed at the July meeting. The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the report. MWo provided an update to the Governing Bodies in relation to the work of the Primary Care Commissioning Committee noting that in July they received a plan for the development of the Primary Care Commissioning Strategy which was approved. The Primary Care Discretionary Spending Plan has been developed to ensure that the available primary care budgets are spent appropriately and within the GMS statement of financial entitlements. The plan includes details around governance and confirmed that monitoring of the spend will sit with the Primary Care Commissioning Committee. The plan was approved by the

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 10
Committee. The Committee received an update on the implementation of social prescribing and noted that a social prescribing steering group has been convened and is leading on the development of the model to be used across North Staffordshire and Stoke-on-Trent. The model has been collaboratively developed with representatives from the CCGs, Local Authorities, Community Providers and Voluntary Sector. Progress will be reported to the Committee on a monthly basis. The Committee received an update in relation to progress made on the BMJ marketing campaign, work is taking place with the CCG, LMC and Northern Staffordshire GP Federation to encourage local GPs to get involved in a video detailing the benefit of working in Northern Staffordshire. The aim is for this to go live at the start of September. Feedback was received from the 360 Ipsos Mori Stakeholder Survey 2018. The Committee considered the results from General Practice, with a response rate of 49% for North Staffordshire CCG and 59% for Stoke-on-Trent CCG. Key findings were that GPs expressed they felt unable to influence decisions, lack of understanding of CCGs’ plans and delivery and that they cannot influence strategy in General Practice. The go-live date for the GP Extended Access has been brought forward to the 1
st September
from the 1st October. Extensive work has been done with practices to achieve this date. There
has been a level of national interest due to the Direct Award Procurement route taken but this has been worked through with the Mills and Reeve legal team. The Committee scrutinised the three risks highlighted on the Public Primary Care Risk Register as scoring 12 and above, following discussion by the Committee, two of the risks had their risk score reduced with mitigations put in place for the third. To conclude, the North Staffordshire CCG Governing Body received and noted the Primary Care Commissioning Committee in Common Report; and Stoke-on-Trent Governing Body received and noted the Primary Care Commissioning Committee in Common Report.
2018/AUG/ 076
9.2 Audit Committees in Common Report
NMcF presented the Governing Bodies with the Audit Committee in Common Chairs’ Report detailing the matters discussed at the July meeting. The North Staffordshire CCG and Stoke-on-Trent CCH Governing Bodies were asked to receive and note the contents of the Audit Committees Chairs Report and to be assured that the Audit Committees were discharging their duties as appropriate. Details presented as follows:
Progress against the 18/19 Internal Audit Plan – the Staffordshire wide internal audit plan continues to be discussed with the Chief Finance Officer. Both the CCGs’ Internal Audit Charter and Terms of Reference for an early risk management review have been drafted. NMcF noted that the report states that the Terms of Reference have not yet been received by the Audit Committee Chairs for review and approval and therefore requested that bullet point three be struck from the report.
External Audit – the annual audit letter was presented to the Committees to communicate the key issues arising. These included that Stoke-on-Trent CCG was classed as ‘unqualified’ for both financial statements and regularity of income and expenditure. North Staffs CCG was classed as ‘qualified’ for financial transactions.
Conflict of Interest Training – all staff should have completed module 1 of the conflict of interest training by 31
st May. A small number is still outstanding and work is being done
to ensure these are completed as soon as possible.
Single Tender Actions / Waivers – discussion took place around the need for STAs to be completed by exception, and for the full rationale to be provided for review. Work around this is ongoing and a further, more detailed, report is expected at the next meeting of the Audit Committees in Common.
To conclude, the North Staffordshire CCG Governing Body received and noted the Audit

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 11
Committee in Common Report; and Stoke-on-Trent Governing Body received and noted the Audit Committee in Common Report.
2018/AUG/
077 9.3 Planning and Commissioning Committee in Common Report
The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to note the summary of key issues and ratify the decisions made from the Joint Planning and Commissioning Committee in Common. SF took the report as read and presented details as follows: SF noted that the details of the meeting held on 17
th April have already been reported to the
Governing Bodies and asked members to focus on the updates in relation to the 8th May 2018
and 12th June 2018. Discussions on the 8
th May focused on extended access to primary care,
tier 2 community ophthalmology service, over the counter items, Future of Local Health Services – Options Evaluation process and reviewed the risk register. The meeting held on the 12
th June focused on the updates around the pre-consultation business
case programme of work, the Macmillan cancer initiatives update, extended access to primary care service specification, alcohol services and the Staffordshire area Medicine Optimisation Committee. SA noted that it had been agreed in principle that the preferred option to extend the contract for the commissioning of the Hanley Primary Care Access Hub by twelve months using a revised specification and queried what this means for patients. SF stated that this was more around registered vs non-registered patients and noted that non-registered patients have now been distributed more evenly across GP lists. There is concern if the service were to be decommissioned due to the number of homeless people in the Hanley area. To conclude, the North Staffordshire CCG Governing Body received and noted the content of the Planning and Commissioning Committees in Common Chairs’ report and; Stoke-on-Trent CCG Governing Body received and noted the content of the Planning and Commissioning Committees in Common Chairs’ report.
2018/AUG/ 078
9.4 Transforming Care Partnership Board Update
The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the content of the Transforming Care report. Details were presented by WA as follows: The Staffordshire Transforming Care Programme has not achieved the NHS England target trajectory for quarter one 18/19, and is in escalation with NHS England which involves monthly regulatory meetings. Performance has deteriorated but WA noted this is consistent across all CCGs. Many planned patient discharges were delayed during May and June for clinical and safety reasons. This group of patients will now be discharged to the community over the next 3-4 months when full assurance is in place that all the holistic needs of these patients can be met in the community. The CCGs have previously stated that they will not place patients outside of the Staffordshire area but the current situation means that if we may have to for safety reasons. A number of patients stepped down from a specialised commissioned bed in quarter one, these now form part of the CCGs’ cohort of patients and has impacted on the achievement of the CCGs’ trajectory. However, the benefit to the individual of a step down to a locked rehabilitation bed has been carefully evaluated and it has been agreed that this further period of treatment and risk testing in a less secure environment is the right pathway for these individuals. Additional funding has been provisionally allocated by NHS England to increase the capacity of the Transforming Care programme team and to commission additional capacity in the CAMHS

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 12
and Intensive Support services for young adults. NHS England are recruiting additional case workers to work alongside the Transforming Care programme teams to provide support in the discharge management of individuals currently in specialised commissioned beds into the community. One of these case workers will be allocated to the Staffordshire team. MWo commented that there appears to be a transitional gap between child and adult services, referring to the fourth paragraph on page three which relates to those young adults aged 18-25 that are presenting with a high incidence of behaviours that challenge. There is a lack of commissioned services which prevents this behaviour. CH acknowledged the comment and explained that commissioners have identified this gap and are completing an urgent review of CAMHS in partnership with the local authority. The transitional gap in particular around autism has also been discussed at the recently formed Joint Commissioning Board. To conclude, the North Staffordshire CCG received and noted the Transforming Care report and; the Stoke-on-Trent CCG received and noted the Transforming Care report.
2018/AUG/ 079
9.5 Communication and Engagement Committee Report
The North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies were asked to receive and note the verbal update in relation to the Communication and Engagement Committee. Details were presented by SY as follows: The Communications and Engagement Committee has been reviewed and a new Terms of Reference is being developed. The new committee will be called the Equality, Engagement and Employment Committee and will also encompass the work previously done by the Organisational Development Committee. The Corporate Services team have recognised the value of the LEAF meeting hosted by North Staffordshire CCG and Stoke-on-Trent CCG and wish to replicate this in the other localities. SY noted that AC now has a much wider remit and leads on communication for the CCGs and the STP which will ensure a more aligned approach going forward, with her new job title being Associate Director of Communications and Engagement. To conclude, the North Staffordshire CCG received and noted the Communications and Engagement Committee verbal update and; the Stoke-on-Trent CCG received and noted the Communications and Engagement Committee verbal update.
2018/AUG/ 080
10. Any Other Business
Questions and Comments from the Public 1. Ian Syme (IS) acknowledged that this is the last meeting of the Governing Bodies for ZJ
before she leaves the organisation. He thanked ZJ for her openness, transparency and integrity in relation to the Pre-Consultation Business Case and the significant improvement in the performance reports, commenting on their coherency. IS wished ZJ well in her new role.
2. IS referred to Vocare noting that they have failed standards with the NHS needing to take over part of their services and queried what the CCGs are doing about the situation. CH explained that following the failure of standards and the inspection from the CQC, there was a system wide decision to move the streaming element of the service to the Royal Stoke University Hospital. Vocare are working closely with the CCG and Royal Stoke colleagues to work through an action plan. There is a weekly system wide call to update against the plan with the intention being that Vocare take back the streaming element on 10
th September. CH wished to assure the members of the public and Governing Body
members that she has asked for early sight of a fully populated GP rota which she will be testing, if this isn’t in place the service will not go live with Vocare on 10
th September.
HJ commented that this has been escalated to NHS England and is being closely monitored

NS Accountable Officer: Marcus Warnes SOT Accountable Officer: Marcus Warnes NS Clinical Chair: Dr Alison Bradley SOT Clinical Chair: Dr Ruth Chambers OBE 13
All parties should note that the minutes of the meeting are for record purposes only. Any action required should be noted by the parties concerned during the course of the meeting and actions carried out promptly without waiting for the issue of the minutes. These minutes are signed as being a true record of the meeting, subject to any necessary amendments being made, which will, if any, be recorded in the following meeting’s minutes.
Signed: ..................................................................... Position: .................................. Date:.............................
by the Quality Surveillance Group meetings; the service is under enhanced surveillance currently which may move to routine dependent on the actions CH described.
3. IS noted that in June of this year, additional guidance was released in relation to Hearing Loss and queried whether the CCGs would be reviewing their policy CH stated there is a review planned and would confirm the date to IS.
4. IS commented that there are ten beds on the Scotia Ward at Haywood Hospital which are designated for rheumatology. He has received notification that these are to be shut and that since November 2017 they have been used as winter escalation beds, when did this change? CH confirmed that Scotia Ward is a 20 bed facility – 10 inpatient beds and 10 day beds. Best practice has identified that there are very few inpatient stays as the preference would be day services. Monitoring of Scotia Ward has highlighted that there are only ever two or three inpatient beds in use at any time and this figure might actually be less. Patients are being monitored in other wards with the same in reach rheumatology services. CH confirmed that In the winter of 2017 as mentioned by IS, 10 of the beds were used as winter escalation beds but 10 day beds remained. IS queried where the evidence is for the increase in day cases. CH to confirm to IS.
Any Other Key Issues The two CCG Chairs wished to formally acknowledge that this would be the last meeting of the Governing Bodies for ZJ and SM and thanked them for their contributions and achievements during their time with the organisations.
CH
CH
2018/AUG/ 081
Date and Time of Next Meeting
Tuesday 4
th September, 2.30pm-5pm, The Conference Suite, The Bridge Centre, Birches Head
Road, Birches Head, Stoke-on-Trent, ST2 8DD

1
Action Tracker from August 2018 Governing Body Meeting
Public Session
MEETING DATE
REF. Action Responsible
Officer Outcome / update
07/08/2018 2018/AUG/
074
SF to feedback to the Governing Bodies regarding the backlog reported at UHNM following his attendance at their Planned Care Board
SF
07/08/2018 2018/AUG/
080
CH to feedback to Mr Ian Syme the date of the planned review of hearing aids following the recently published guidance
CH
07/08/2018 2018/AUG/
080 CH to feedback to Mr Ian Syme figures in relation to the increase of day cases at Scotia Ward - Haywood
CH
Enc. 4.2

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 5
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Risk Register
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Sally Young, Director of Corporate Services, Governance & Communications
N Jane Chapman, Head of Governance
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
N/A N
Action Required (select):
Decision Discussion For Assurance / For Information
Purpose of the Paper (Key Points + Executive Summary):
This papers sets out to update the North Staffordshire and Stoke-on-Trent CCG Governing Bodies in Common the risk register for risks rated 15 and above as of the 20th August 2018 in respect of the following:
Finance Strategy, Planning and Performance Commissioning and Operations Nursing and Quality Primary Care
It should be noted that no new risks with a score of 15 or above has been reported for Corporate Services, Governance and Communication. The scores for two of the risks have been reduced from 15 to 12, they are included for completeness and will be removed next month The table below provides a summary of the number of risks scored 15-20 inclusive, which represents a reduction risks scoring 20, from 5 to 4.
No of risks Risk Score Risk Rating
4 20 High
3 16 High
3 15 High

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
CCG Corporate Risk Register The North Staffordshire and Stoke-on-Trent CCG Governing Bodies in Common is asked to note that work is progressing to align the risk registers (clinical and non-clinical) across (1) North Staffordshire CCG; (2) Stoke-on-Trent CCG; (3) Staffordshire and Surrounds CCG; (4) South East Staffordshire and Seisdon Peninsula CCG; (5) Cannock Chase CCG and (6) East Staffordshire CCG. Meetings between members of the Governance team and individual Directors, to look at the risk and residual risk reporting / monitoring, will be complete by 24th August. The draft combined risk register across the 6 CCGs’ will then be submitted to the Executive Team meeting for review / comments in the first instance and respective Committees thereon prior to a further update being provided to the North Staffordshire and Stoke-on-Trent CCG Governing Bodies in Common. The North Staffordshire and Stoke-on-Trent CCG Governing Bodies in Common is asked to: 1. Note that assurances for risks scoring 15 and above have been sought and the register has been
updated accordingly. 2. Review and make any comments regarding the content of the risk register and identify if they
require any further assurances in regard to the risks recorded. 3. Note the progress of the work to align the risk registers (clinical and non-clinical) across (1) North
Staffordshire CCG; (2) Stoke-on-Trent CCG; (3) Staffordshire and Surrounds CCG; (4) South East Staffordshire and Seisdon Peninsula CCG; (5) Cannock Chase CCG and (6) East Staffordshire CCG.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
Low risk of failure to align registers in timely fashion
Implications:
Legal and/or Risk Enables CCG to demonstrate that risks are assessed and managed.
CQC
Patient Safety Forms part of our approach to delivering safe services.
Patient Engagement
Financial Forms part of our approach to financial management
Sustainability
Workforce / Training In house training by Governance team to Directorates to ensure consistent & appropriate use of registers in the management of risks
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
N
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
N
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
N
Recommendations / Action Required:
The Governing Bodies in Common are asked to: Review the Risk Register and be Assured that the identified risks are being well managed or seek further Assurance.

2
Executive directors
24.8.18
DirectorateR
isk
Re
f
Da
te r
isk
reco
rde
d
Risk Owner Risk Description Trend Risk Proximity Actions Action Owner Completion Date for
Actions
Assurances Last reviewed
A unique coding
that allows the
risk to be easily
identified
Date risk
recorded
Job title of the person responsible for the
management, monitoring, control and
escalation where appropriate, of the
identified risk
A statement describing the risk event, cause and impact
Like
liho
od
Imp
act
RA
G S
tatu
s
The trend
indicates any
change in the
current risk
score in the
form of an
arrow
Timescale as to
when the risk will
occur
The actions and activities planned to take place that will when implemented or completed
reduce, eliminate or minimise the risk
Job title of the person
responsible for
completing the action
Each action should have
a completion date set
Like
liho
od
Imp
act
RA
G S
tatu
s
Internal assurance / evidence (e.g. Board reporting, sub-committee and programme
governance) and external assurance / evidence (e.g. planned or received audits or
reviews) that the risk is being effectively managed
Date when the risk was last reviewed and/or updated
Finance F5
02/11/2017
Chief Finance Officer That agreement with UHNM is not reached and an arbitration
process is required to conclude the year end financial position
5 4 R
↑ 3-6 months 1. The CCG and Trust have submitted a rec to month 6 of the base financial/contract position
as required by NHSE/I, this shows acceptance of fines however UHNM are understood to be
planning to raise an invoice at the year end. The CCG have raised this with NHSE and will also
include this issue as a potential arbitration issue. The key mitigation is that, without a
different contractual agreement, the CCG will follow the direction of NHSE on this matter and
the application of the national contract which both the CCG and UHNM have signed.
CFO 31/03/2018 5 4 R At the year end UHNM raised invoices to the CCG for repayment of fines and penalties,
this is outside of the contract, this shows as a different in the agreement of balances
position - the CCG do not recognise these invoices, a position accepted by external
audit. The invoices remain outstanding and there is no national process to address
these. The CCG have kept NHSE informed of the position and approach consistently and
the CCG expectation is that these invoices will be withdrawn in the future.
08.08.2018 agreed with Director of Finance to close down this risk. Following the management of
change and restructuring of the six CCGs, the risk registers are currently in transition and being aligned
with discussions taking place with each of the Directors to review the risks on the six risk registers to
align them into one register.
23/08/18 Risk continues to be manged as an operational issue. there is no change to the position.
Planning &
Performance
PP3 09/11/2017 Director of Strategy, Planning and
Performance
Pre Consultation Business Case - Risk that we cannot progress the
process due to external challenge
4 4 R ↔ 9-12 months 1. Close working with regulators and stakeholders
2. Robust comms and engagement plan to minimise opposition to our plans
3. Quality Assurance by the Consultation Institute
4. On SPP Directorate risk register.
5. Regular contact maintained with OSC Officers, MPs and lobbyists
6. Clinical Senate visits during May/ June to ensure clinician assurance of the proposed option
7. Reference Groups held throughout May involving key stakeholders
8. Attendance at Staffordshire County Council and Stoke-on-Trent City Council Informal
Cabinet Meetings to ensure LA engagement
1. Associate Director of
Strategic Commissioning
2. Associate Director of
Comms and Engagement
3. Associate Director of
Comms and Engagement
4. Associate Director of
Strategic Commissioning
5. Associate Director of
Comms and Engagement
6. Associate Director of
Strategic Commissioning
7. Associate Director of
Comms and Engagement
8. Head of Comms and
Engagement
1. Throughout process
2. Throughout process
3. Directorate risk
register discussed
ongoing at CCG audit
committee.
4. Complete
5. Throughout process
6. Complete
7. Complete
8. Throughout process
3 4 AR 11/6/2018 - Actions, action owner and completion dates updated. 13.08.2018 risk has been amended following discussions with Zara Jones. Clinical Senate review has
now been completed.
Planning &
Performance
PP4 09/11/2017 Director of Strategy, Planning and
Performance
Any proposed options may be formally challenged, for example
through judicial review or referral to Secretary of State. Impact:
A long, costly and potentially damaging legal process, resulting in
reputational damage.
4 4 R ↔ 9-12 months 1. The PID outlines the assurance process.
2. An engagement and evidence log will be kept and updated regularly.
3. NHSE leads have an open invite to Steering Group meetings.
4. Quality Assurance by the Consultation Institute.
5. Evidence including governance processes will be kept and provided as part of the assurance
process.
6. The NHSE best practice tests, including the Gunning principles, will be applied to the PCBC.
7. Engagement with stakeholders will be ongoing as part of the co-production of solutions.
8. Independent advice will be provided by the West Midlands Clinical Senate.
9. Options development process to be logged and documented 10. Extraordinary Governing
Body meeting Agenda to ensure that Board is publicly exercising its legal requirements and
duties 11. Issue regular newsletter to stakeholders 12. Microsite to be developed for formal
consultation
1. Associate Director of
Strategic Commissioning
2. Associate Director of
Comms and Engagement
3.Associate Director of
Strategic Commissioning
4.Associate Director of
Comms and Engagement
5. Associate Director of
Comms and Engagement
6. Associate Director of
Comms and Engagement
7. Associate Director of
Comms and Engagement
8. Associate Director of
Strategic Commissioning
9. Associate Director of
Strategic Commissioning
10. Associate Director of
Strategic Commissioning
11. Associate Director of
1. Complete.
2. Throughout process.
3. Complete.
4. Throughout process.
5. Throughout process.
6. Throughout process.
7. Throughout process.
8. 12/6/2018
9. Throughout process
10. Complete
11. Throughout process
12. 30/6/2018
1 2 G 11/6/2018 - Risk description update, actions, action owner, completion date updated,
anticipated risk score on completion of actions reduced.
13.08.2018 risk has been amended following discussions with Zara Jones.
Independent advice has been provided by the West Midlands Clinical Senate.
Reviewed at Extraordinary Governing Body.
Regular news letters to stakeholder.
Microsite developed for formal consultation.
Commissioning C2 22/09/2017 Director of Commissioning Pressures in Stoke-on-Trent City Council Social care funding will
directly impact upon health provision as a result of there being
insufficient packages of Care (POC) available to meet the needs
of patients who are Medically Fit for Discharge (MFFD)
4 5 R ↔ 3-6 months 1. Stoke CC have advised they are currently have 2000 hours deficit within domiciliary care.
Have provided assurance that they are undertaking a dynamic procurement starting mid Dec
2017 for completion end of June 2018 which is expected to close the gap, interim actions
offering off framework provision and purchasing sets of rotas.
2. Use of iBCF funding to cover off additional capacity
3. Undertake reviews of current PoC to release the capacity back into the system
4. Transfer of enablement to home first which will reduce demand for domiciliary care
5. Procure process too be complete February 2019,
6. Rollout to be completed February 2019
7.CCGs have agreed to joint tender with Stoke on Trent City Council to secure an additional
1000 hours of block rota capacity to support flow with a number of caveats to ensure that
patients are transitioned within 21 days into framework provision to free up block rotas to
deliver a POLR model for patients post assessment requiring domiciliary care.
1. Director of
Commissioning working in
collaboration with
Director of Adult Social
Care to support process
and interim measures
2.HoC aligned to Strategic
Manager for SOT CC
3.HoC aligned to Strategic
Manager for SOT CC
4. Joint H&SC funded
approach
1. Director of
Commissioning working in
collaboration with
Director of Adult Social
Care to support process
and interim
measures2.HoC aligned to
Strategic Manager for
SOT CC3.HoC aligned to
Strategic Manager for
SOT CC4. Joint H&SC
funded approach
4 4 R 9/4/18 update-Quarterly assurance statement completed - Actions updated, and dates,
existing controls recorded.
09/04/2018
13/06/18 CCG have worked closely with SCC to undertake co-commissioning of POLR capacity equating
to 1000 hours which is now within the system.
13.08.2018 - This risk has been reviewed in line with the proposed changes for the registers across the
six, it has been proposed by the Director of Commissioning and Operations that the risk should remain
as a PAN Staffordshire risk. This will form part of the work being undertaken to align the registers
including mitigating actions and will be report once final approval by the Single Leadership Team has
been agreed.
Commissioning C5 13/10/2015 Director of Commissioning The A&E Recovery Plan will not deliver the 95% 4 hour and 12
hour trolley breach having a direct effect on patient safety and
quality.
5 4 R ↔ 0-3 months 1. Quality visits to A&E to check on patient care.
2. A&E Delivery Board.
3. Track and Triage to promote flow in the system.
4. CQRM
5. Remedial Action Plans
6. D2A Steering Group
7. 12 hour trolley breach assurance report
8. Urgent care plan being pulled together SSOTP/UHNM and CCG
9. Acute /unplanned PMO being developed supported by all organisations. along with a
programme of governance around it
1. Director of Nursing &
Quality
2. Director of
Commissioning
3. Director of
Commissioning
4. Medical Director
5. Director of
Commissioning
6. Director of
Commissioning
7. Director of Nursing &
Quality
8.Director of
Commissioning
9. Director of
Commissioning
achievement expected by
March 2018
5 4 R 9/4/18 - Qtrly assurance statement completed risk remains the same- Risk already mitigated
13/06/18 Single plan has been developed with system partners which reflects the actions identified
within the recent Sir Neil McKay review, Newton Europe and internal plans within the acute trust.
This has been reviewed by West AEDB and in principle agreed. Milestones will be tracked through the
STP PMO with and underpinning governance and assurance framework.
10.08.2018 - UHNM are currently 36th in the country in terms of ED performance as a result of
sustained system actions which are impacting positively upon flow.
As part of the risk review it is proposed to re-assign this risk to the Director of Commissioning and
Operations as realted to Winter Plan, following a meeting with Zara Jones on 13.08.2018.
Commissioning C7 09/11/2017 Director of Commissioning Flow through the commissioned capacity and achievement of
DTOC trajectories in line with BCF
4 5 R ↔ 3-9 months 1. CCG dedicated resource to manage bed flow across the system
2. Trajectories agreed by NHSE/LAs with BCF potential penalties if not achieved
3. Additional bed base commissioned in line with the Winter Plan to support flow
4. Home First service commissioned from one p+K8rovider, with associated contract levers
which support the over-arching performance targets.
5. T&T team fully implemented directly supporting planning and decision making.
10.08.18 Agreement has been reached across all partners as to how to approach the counting
of DTOCs in a consistent way, which it is expected will mean that Stoke trajectories remain on
track.
1. Director of
Commissioning
2. HoC/Director of Social
Care (SOT
CC/Staffordshire CC)
3. Director of
Commissioning
4. Director of
Commissioning/ Director
of Operations SSOTP
5. Director of
Commissioning/Director
of Operations
1. complete
2. complete Nov 2017
3. Complete
4.Nov 2017 (stoke) April
(2018)
5. complete
4 4 R 9/4/18 - Quarterly assurance statement completed risk remains the same .
13/06/18 - Stoke DTOC trajectory has been achieved. SCC is due to achieve the required 3.5% in July &
is on track to do so.
10.08.2018 - As a result of a counting issue the figures submitted against the DTOC trajectory have
been revised, this has resulted in a shift against trajectory & resubmission to the region and national
teams. Agreement has now been acheived across all partners as to how to approach the counting of
DTOCs in a consistent way, which will it is expected mean that Stoke trajectories remain on track.
Current Risk
Score 1
Anticipated
Risk Score on
Completion of
Actions
Version Control Full Risk Register (covering Commissioning, Quality, Finance, Organisational Development, Primary Care and Planning & Performance)
Version
Author
Date

Quality Q8 Medical
Director
Director of
Nursing and
Quality
20/11/2017 There is a risk regarding 12 hour long waits in the Accident and
Emergency department at UHNM, during periods of pressure.
This is caused by overcrowding, bed blocking, patients being
medically fit for discharge but no social package in place and
demand/capacity at the Trust. The impact of the risk is that
patients could potentially come to harm as a result of 12 hr waits
and poor patient experience.
3 4 R ↔ 9-12 months 1. Quality visits to the provider over the year, escalation winter capacity visits (EMS level 4)
undertaken.
2. 12 hours Root Cause Analysis Reviews with CCG Quality team attendance.
3. Discussions at CQRM meetings with the provider to ensure patient safety.
4. There are weekly teleconferences between the CCGs, NHS England and NHS Improvement.
The teleconferences discusses patient flow and quality and safety.
5. Following the Risk Review meeting on the 9th March 2018, an action plan was produced for
all key stakeholders. The action plan will be overseen at the following meetings: Clinical
Quality Review Meeting, Joint Quality Committee, Accident and Emergency Delivery Board
and Quality Surveillance Group.
6. Care Excellence Framework visits
1. CCG Head of Quality
and CCG Strategic Lead for
Quality
2. CCG Strategic Lead for
Quality / NHS
England/UHNM Quality
Team
3. CCG Strategic Lead for
Quality
4. CCG Strategic Lead for
Quality
31/03/2019 3 2
A/G
UHNM to arrange additional 12 hour breach panels (CCG quality to attend) these panels are to be held
to try to clear the backlog of circa 200 now completed RCAs before the next QSG (28th June).
CCGs will work with UHNM to look at the existing process and how we can refine to make it less
bureaucratic whilst ensuring timely learning.
Current situation on 12 hr breaches - In April 2018 there were 2 validated 12 hr breaches, In May there
have been no reported 12 hour breaches.
13.08.2018 - The risk has been reviewed by the Director of Nursing and Quality as the risk currently
stands they are proposing that the risk is closed. This will form part of the work being undertaken to
align the registers including mitigating actions and will be report once final approval by the Single
Leadership Team has been agreed.
24.08.18 Safety Check List in place
Owing to the improvement in flow their is less crowding in the Dept. which supports improved care.
The risk is monitored through a planned cycle of announced and unannounced visits.
Quality Q10 Medical
Director
Director of
Nursing and
Quality
17/11/2015 There is a risk of that the CCGs will fail to achieve NHS
Constitutional Target of 18 week Referral to Treatment. This is
caused by a multitude of factors at the Trust, specifically around
demand and capacity. The impact of the risk is a potential poor
patient experience and potential delays in patients receiving
treatment.
3 5 R ↔ 9-12 months 1. Monitored at monthly CQRM meetings
2. For any patients that have breached the 18 week target, these are reviewed via the 52 week
breach RCA panel. The CCG quality team attend the 52 week RCA panel, the panel reviews if
any patients has come to patients as a result of the delay in treatment.
3.Liasing with Commissioning Teams to highlight quality issues
4. The Trust is working to set up an Planned Care Operational Group with CCG Executive
Attendance
1. CCG Director of Nursing
& Quality
2. CCG Strategic Lead for
Quality
3. CCG Director of Nursing
and Quality
4. CCG Medical Director
31/03/2019 3 2 A/G April 2018 update - UHNM have instituted a Planned Care Board with Executive lead to drive
improvement. The CCG is seeking agreement to attend the Operational Group.
There is an ongoing Intensive Training and Validation programme
There is a focus by the trust to tackle 40 and 52 week waiters (e.g. inline treatment)
13.08.2018 - The risk has been reviewed by the Director of Nursing and Quality as the risk currently
stands they are proposing that the risk is closed. This will form part of the work being undertaken to
align the registers including mitigating actions and will be report once final approval by the Single
Leadership Team has been agreed.
24.08.18 Trust carrying out harm reviews. no significant harm identified to date but awaiting more
information.
Quality Q12 1.Lead
Commissioner
for Cancer
2.Medical
Director
08/02/2016 There is a risk that the CCGs will fail to achieve the NHS
Constitutional wait time targets for cancer. This is caused by
demand and capacity at the Trust, the impact of this is potential
poor patient experience and potential delays to patients
receiving treatment.
3 4 R ↔ 9-12 months 1. Quality issues addressed through CQRM, Joint Quality Committee and the Governing Bodies
2. High Impact Action plan in place to drive cancer performance.
3.Fortnightly meetings between UHNM and the CCGs.
4. Commissioners have direct conference calls with NHSI and NHSE.
5. Quarterly CQRM reporting of 104+ cancer patients
6. Robust 104+ day RCA clinically led process, acknowledged by West Midlands Cancer Group
as a beacon of good practice.
7. Once the RCA process is completed a clinical governance panel is held internally by the
Trust to review all the 104 day patients.
1. CCG Director of Nursing
and Quality
2. CCG Director of Nursing
and Quality
3. CCG Director of
Commissioning and
Operations
4. CCG Director of
Commissioning and
Operations
5. CCG Strategic Lead for
Quality
6. UHNM Quality Team
7. UHNM Quality Team
31/03/2019 4 1 G May 2018 Update: As of 29/04/2018 - there are 6 patients that have breached the 104 + day cancer
wait time. These patients will be reviewed via the RCA clinically led process, to identify if any patients
have come to harm.
13.08.2018 - The risk has been reviewed by the Director of Nursing and Quality as the risk currently
stands they are proposing that the risk remains open and will be reviewed as part of the work being
undertaken to align the registers including mitigating actions and will be report once final approval by
the Single Leadership Team has been agreed.
24.08.18 Measures in place to manage harm appear effective and no evidence of significant harm
identified.
Quality Q13 Medical
Director
17/11/2015 There is a risk that the backlog of patients at UHNM have waited
longer than clinically required for their follow up appointment.
Spans across all specialties. Potential clinical risk to patients as
patients have exceeded their clinical review date.
3 5 R ↔ 6-9 months 1. Performance reported via the CRB and to Governing Body via the Assurance Report
(monthly).
2. Planned Care Operational Group.
3. Detailed speciality action plans in place by the provider to manage the risk, including clinical
validation, consultant specific meetings to discuss their individual positions, Junior Doctors
follow up protocols and actions to maximise clinic utilisation.
1. CCG Strategic Lead for
Quality
2. CCG Medical Director
3. UHNM
31/03/2019 3 2
A/G
May 2018 update:
1. Continued scrutiny and assurance sought at CQRM
2. Implementation of UHNM Planned Care Board with CCG representation
24.08.18 Paper recieved from UHNM at CQRM. however, this did not fully assure the committee and
further assurance is being sought.
3. Develop clinical audit programme Outpatient waiting list
4. 52 week RCA panel to assure no harm to patients from delays. The last 52 week breach panel was
held on 24/5/18 and attended by the Head of Quality. 36 RCAs were reviewed against the harm criteria
and no harm as a result of the long wait was identified. A report will be provided at the next CQRM.
5. UHNM to develop work programme to resolve IT problems with Medway
13.08.2018 - The risk has been reviewed by the Director of Nursing and Quality as the risk currently
stands they are proposing that the risk is moved to the directorate "Issues Log" which is being
developed for each directorate to monitor. This will form part of the work being undertaken to align
the registers including mitigating actions and will be report once final approval by the Single Leadership
Team has been agreed.
24.08.18 UHNM have presented a paper at the CQRM but it did not provide the committee with full
assurance and further information is being sought.
Quality Q14 Director of
Nursing and
Quality
11/07/2017 There is a risk that the Continuing Healthcare Team cannot
provide the CCGs with the assurance that reviews for continuing
healthcare funded patients are being undertaken in a timely
manner; including whether a DOLS is in place.
3 5 R ↔ 6-9 months 1. A review stratification project group has been established to identify specific areas of
reviews.
2. Each area of reviews is considered to determine new ways of working for nurse assessors
and timeframes with which to prioritise reviews.
3. A new method of reviewing fast track reviews commenced on the 1st January 2018.
4. A new resource for reviews of Physical Health High cost cases will commence on the 1st
May 2018.
5. Monthly updates provided at the CHC Programme Board, attended by either the CCG
Director of Nursing and Quality or Deputy Director of Nursing and Quality.
6. Quality Assurance reports provided to the Joint Quality Committee on a quarterly basis
1. CHC Team
2. CHC Team
3. CHC Team
4. CHC Team
5. CCG Deputy Director of
Nursing and Quality
6. CHC Team
31/03/2019 3 3 A May 2018 Update: It was reported at CHC Programme Board in April 2018 that, he CSU had been
advised by the CCG to put in a business case for the LD capacity, however the CHC have recently
informed the CCG that with the restructuring of the service they have been able to put in two LD Band
6 Nurse assessor posts into the LD team to help with the workload and are currently recruiting to these.
The CHC team also have the option of extending the Band 7 LD Bank Nurse if it is felt necessary.
However the CHC Team have maintained that they will monitor the capacity/workload and if it is
deemed necessary reinstate discussion with the CCG to complete a business case.
1. Initial work will be carried out to identify any reviews over 2 years which will be allocated to a nurse
working in that geographical area
2. Telephone reviews on Funded Nursing Care patients between 12 months and 2 years will commence
from June 2018 to reduce the number of overdue reviews in this category.
3. Of the 213 legacy overdue Fast Track packages reported in February 2018, this has now reduced to
185, of which 65 have been allocated for review, 29 have been scheduled to take place and 21 are
awaiting verification. Of the 21 awaiting verification, 16 are recommended as FNC and should these be
agreed a saving of £14,195 per week would be accrued.
4. Review stratification work now ensures that any offer of 1-2-1 care is reviewed initially by a Clinician
prior to acceptance. If agreed the 1-2-1 element of the care package is only awarded for an initial
period of 2 weeks after which the provider is responsible for ensuring suitable evidence is submitted to
request an extension.
13.08.2018 - This risk will remain and will be updated as a PAN Staffordshire risk and is part of the
ongoing development work to align the risk registers.
24.08.18 CHC Board meeting to manage risk. Quality have seat at table
Primary Care PC12 05/06/2018 Director of Primary Care Lack of a single, strategic, integrated plan for primary Care 4 4 R 0-2mths 1.Proposal to develop a single primary care strategy for Staffordshire including details of investment for
2018/19 and longer term investment approved by Primary Care Commissioning Committee 3/7/18
2. GPFV implementation plan in place and will continue to deliver transform primary care to deliver
sustainable general practice
3.Engagement process to develop the clinical model with stakeholders will commence September 2018
4.Primary Care Investment plan reviewing current and future funding will be presented to the Primary
Care Committee in September 2018
1. Director of Primary Care
2. Director of Primary Care
3. Heads of primary Care
Development &
Commissioning
4. Director of Primary Care
1. Ongoing
2. Ongoing
3. Ongoing
4. On-going
3 2 AG 13.06.18 new risk
9/07/2018 - commissioning plan has now been presented but now requires a delivery plan and
associated timeframes
22.08.2018 - Review of the risk taking place with Director of Primary Care as part of the alignment of
risks.


Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 6.1
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Chairs’ Address
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Dr Alison Bradley, Clinical Chair, North Staffordshire CCG Dr Ruth Chambers OBE, Clinical Chair, Stoke-on-Trent CCG
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
Dr Alison Bradley, Clinical Chair, North Staffordshire CCG Dr Ruth Chambers OBE, Clinical Chair, Stoke-on-Trent CCG
Action Required (select):
Decision Discussion For Assurance / For Information
Purpose of the Paper (Key Points + Executive Summary):
This report will provide an update to the North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies’ in common around the current environment in which the CCGs have been operating.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
N/A
Implications:
Legal and/or Risk
CQC
Patient Safety
Patient Engagement
Financial
Sustainability
Workforce / Training

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
N/A N/A
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
N/A N/A
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
N/A N/A
Recommendations / Action Required:
The North Staffordshire and Stoke-on-Trent CCG Governing Bodies’ are asked to:
Receive and note the contents of the Clinical Chairs’ Address

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
1. Introduction
1.1 The CCGs continue to work closely and effectively with system partners during this nationally difficult
time across the health and social care economy.
1.2 We would like to acknowledge the outstanding efforts across the CCGs and in collaboration with our
partners to respond to the pressures on urgent care, NHS constitutional standards, our financial
position, planning requirements, delivery of our financial recovery plan, and the Together We’re
Better Sustainability and Transformation Partnership (STP). These continue to be our key priorities.
1.3 We are, as always, grateful for the hard work and dedication of the CCG staff and front line staff in
primary, community, mental health and hospital settings, and would like to thank everyone for their
continued professionalism and support.
2. Engagement with the Sustainability and Transformation Partnership (STP)
2.1 The Chairs of the six Staffordshire CCGs meet on a monthly basis with the Chief Executives and
Chairs of key local organisations and on a quarterly basis the meeting is extended to also include lay
members. Following the meeting held on the 10th July 2018, Sir Neil McKay, Chair of the STP asked
all Chairs to consider what more can be done to achieve clinical and financial stability.
2.2 The CCGs’ response focused on promoting prevention across all health and social care settings –
spanning medication, falls, social prescribing, community outreach and much more. This should be
driven by joint working between our Health and Wellbeing Boards, STP, providers and commissioners
(attached as Appendix 1)
2.3 The feedback from this exercise will be discussed at the system wide Health and Care
Transformation Board in September.
2.4 The STP produce a monthly update report, the July update is attached as Appendix 2.
3. Health and Wellbeing Boards
3.1 Dr Alison Bradley has taken on an additional new role as Co-Chair of the Staffordshire Health and
Wellbeing Board. Dr Bradley has taken on this role following the retirement of Dr Charles Pidsley and
will Co-Chair the Board with Councillor Alan White. Councillor White is the Deputy Leader of
Staffordshire County Council and a Cabinet Member for Health, Care and Wellbeing.
3.2 The latest Staffordshire Health and Wellbeing Board meeting papers can be found here:
Agenda for Health and Wellbeing Board on Thursday, 6th September, 2018, 3.00 pm - Staffordshire
County Council
3.3 The latest Stoke-on-Trent Health and Wellbeing Board meeting papers can be found here:
Browse meetings - Health and Wellbeing Board | Stoke on Trent City Council

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
4. Update on Membership Vote and Constitution
4.1 Following the Membership meeting held on the 24th May 2018 and the proposed changes to the
Constitution, a voting slip will be sent to all GP practices by the end of August. The CCGs will request
that this is returned by 15th September 2018.
5. North Staffordshire CCG and Stoke-on-Trent CCG Lay Members
5.1 We are pleased to announce that Dr Latif Hussain has agreed to another term as one of GP lay
members until March 2020. We are delighted that Dr Hussain is to remain on the Governing Body.
5.2 Following his notification of his intention to not renew his tenure with Stoke-on-Trent CCG, September
will be the last month for Dr Simon Mellor in his role as Secondary Care Board Member. On behalf of
the Governing Body we would like to thank Dr Mellor for his contributions whilst fulfilling this role and
wish him all the best for the future.
5.3 The advert for the Stoke-on-Trent CCG Secondary Care Consultant is now live on NHS Jobs with a
closing date of 6th September 2018.
5.4 As previously reported, Dr Ruth Chambers OBE, Clinical Chair for Stoke-on-Trent CCG has
announced her intention to step down from this role. All GPs in the Stoke-on-Trent area have been
contacted if they wish to express an interest in applying for this role. The closing date for applicants is
Friday 7th September with a provisional interview date set as 18th September 2018.

1
Appendix 1
Staffordshire CCGs’ feedback on ‘our envisaged radical path for next 5-10 years to achieve clinical and financial
sustainability’ Following the meeting of STP chairs and chief executives on 10 July, the Staffordshire CCGs execs and non-execs considered the question posed at the meeting regarding what ‘radical’ things we need to do for the next 5-10 years to achieve clinical and financial sustainability across the system. The contributions received are non-attributed, have been edited together but are largely as provided and in some cases have been shared verbatim. In essence the imperative for clinical and financial sustainability is to focus our STP strategy and operations on prevention. Structurally that means:
Shifting a larger proportion of health and social care economy finances, resources and active support to primary and community care where new models of care and integrated care working can generate a reduction in the numbers of people with long term conditions or adverse lifestyle habits. Local authorities should reinstate efficient services to support people to redress adverse lifestyle habits such as smoking, being overweight, excessive alcohol consumption and illicit drug intake.
Implementing new models of care with an emphasis on prevention services, such as falls prevention and social prescribing.
Creating better service offers to enhance patient empowerment so that people taking greater responsibility for their own care and health condition with shared management of care between the patient and clinician is the norm. Greater emphasis on digital inclusion and the underpinning infrastructure, including the necessary equipment to relay biometric measurements from patient to clinician could help to facilitate this.
Systems and processes will need to change, for example:
Organising both Health and Wellbeing Boards to work jointly together to hold health and social care organisations to account for their investment decisions and the provision of care across the health and care economy.
Merging the six CCGs by 1st April 2020 so there is one strategic health commissioner with much stronger aligned and potentially integrated commissioning arrangements with the local authorities.
Ensuring closer working between MPFT, Combined Healthcare and the two local authorities
Revisiting the provider landscape and considering again whether we need two specialist providers of mental health and learning disabilities in Staffordshire and whether one fully integrated community provider of physical and mental health and health and social care services would make better sense.
The focus on prevention must be a priority:
We talk about being radical and while changing legislation is not going to happen soon, in Staffordshire we should be making a statement by paving the way for public health to come back under health direction, if not direct control initially.
The STP should have an overarching prevention agenda for the whole of the county to reduce health inequalities and focus prevention work on those conditions which have the biggest impact on individuals' quality of life and require most health interventions if not managed effectively.
The STP should require the two public health teams to work together to ensure the approach is consistent, with a single joint needs assessment for the whole county. Budgets should be pooled (virtually in the first instance) with commissioners and providers required to pool relevant overlapping resources, eg falls prevention, winter planning.
Short term benefits should see a reduction in the post code lottery access to prevention programmes and reversing short term decisions to cut funds or reduce access should have longer term benefits for individuals

2
and the Staffordshire health economy. Longer term there should be the obvious reduction in pressure on primary and secondary care.
In tandem with this the STP should be looking to have a unified approach to the Better Care Fund. We should have one BCF with one plan and set of proposals, even if they are presented as two BCF plans if statutorily we are required to keep them separate.
Tying the local authorities more directly into joint prevention and home care is the only way we are going to have any chance of avoiding these key areas being salami sliced into oblivion.
The overall theme for the STP should be on prevention and self-care, with targeted and assisted prevention for those most vulnerable and in need though to self-management and support through tech-enabled systems.
In terms of a consultation, I think if most residents were asked whether councils or the NHS managed health prevention they would get it wrong and probably support a change.
Sustainable general practice must be at the heart of the STP strategy:
Loss of GPs and partners in particular has accelerated with a loss of c500 GPs nationally in the last three months alone. If the current model of general practice becomes increasingly unsustainable in some parts of Staffordshire, there is an opportunity for providers such as MPFT and Combined Healthcare to step in and support practices or potentially to start providing GP services.
Traditional general practice with practice partners seems to be dying. Fewer doctors wish to become partners. There is now a preponderance of female doctors who wish to work part time to look after their families, which should be facilitated through more flexible working practices. Many younger doctors are interested in portfolio careers, rather than a lifetime in general practice. The Darzi review on larger, integrated practices offering many services must be revisited and implemented where possible, even if it means buying doctors out of unsustainable one and two handed practices.
Resource GP practices properly, not with short-term incentives, to develop their flexible workforce and to manage an integrated primary care team (not just general practice) effectively, and in doing so remove the many layers of management at MPFT that can get in the way of proactive, responsive, seamless, integrated working at practice and locality level. As part of an enhanced primary care offer, fund a full-time pharmacist for every average sized practice to improve prescribing and reduce medicines spend and arrange direct access physiotherapy and a mental health worker in every practice.
There must be a greater emphasis on integrated care, bringing together health and social care, prevention, physical and mental health community services and addressing the wider determinants of health:
Social Prescribing should be allowed to develop organically and relate to the needs of each locality. It is a concept which needs to be firmly embedded in the integrated care teams and hubs and wider locality working. The scope and benefits are evidenced and extensive if developed in line with locality needs. To work, it will require the coordination, via social prescribing link workers in each ICH area, of statutory, voluntary and community services to support the needs of local patients and the public. This concept also requires patients and the public to be more involved in their health and well-being status and to be more involved in their own health and care treatment plans (self-care). The long term benefits are profound and afford the scope for real long term transformational change.
Mental health link workers should be attached to each locality integrated care hub, with the remit to assess patients and offer a direct access link to appropriate MH support services. This concept was one of the recommendations emanating from the recent Citizen's Jury report in the north and accepted as an action by both Governing Bodies.
Community outreach health and social care buses/mobile units could provide opportunities to operate a partnership owned outreach support service to flex programmes and delivery as required, eg health promotion activities and events, screening services, local authority outreach services, voluntary agency advice and support services, etc.
For community and district nursing and social care, GPs, nurses and other care workers must agree on the skills needed in the community and ensure the nurses/care workers have them. The approach must be flexible, consistent and have demonstrable benefits to the patient.
3
Falls service – most patients who fall at home do not require hospitalization. If a fall occurs, the patient must be assessed at home by a suitable professional (OH, nurse, physio). If there is no evidence of fracture, can the cause of the fall be remediated quickly, such as clearing passageways, the use of non-slip mats, or would more major works such as handrails benefit patients.
Back pain is a huge cost to the community. The Startback concept must be embraced and commissioned across the whole of Staffordshire.
Many of the above strategies will reduce A&E attendance rates. However, it is clear that people attending A&E with easily definable and single problem conditions (heart attack, stroke) go into well-defined pathways very quickly. The trolley waits seem to concern multiple morbidity and vague presentations. This is where early consultant intervention to assess risk and make a plan is vital. Patients coming in from care homes with a vague deterioration must be turned round quickly if they are to return to the home.
In general we need to become more proactive rather than reactive. We need to work within more extensive partnership frameworks that include Fire, Police, Ambulance, clinicians, local authorities, voluntary and community services, etc so as to extend our reach into the diverse communities we operate in. This model of partnership working serves to reduce duplication of effort, enhances opportunities to effectively share limited resources, creates opportunities to collectively bid for new resources and to deliver services which better fit the needs and requirements of local populations.
There are things we should stop doing where the evidence tells us they are not effective and improving outcomes:
The Clinical Priorities Advisory Group (CPAG) should concentrate on refining pathways in common conditions. There is little point in arguing over the best measures in difficult to treat or rare conditions. The question there is whether we should stop commissioning in these areas.
Safe medication in care homes should be a priority, with patients in care homes the responsibility of a single practice to ensure consistency of treatment regimens. Care staff are easily confused by complex inconsistent medication regimens. Medications should be regularly reviewed and reduced to the absolute minimum, eg stop statins unless there is a proper indication.
If funded, for fertility services to achieve best results the care pathway must be seamless. Best results are achieved through single poc throughout the process. The worst way of doing this is by rationing IVF cycles.
However, should services such as IVF and gender reassignment be funded at all? A better solution may be to offer a grant (ultimately repayable) to those who cannot afford to pay but could benefit.
We must consider addressing anomalies in acute care funding, such as CAU, day case procedures, which are really outpatient clinic appointments, and the unbelievable medicines waste caused by pharmacies ordering “on behalf of” patients.
We cannot transact our way out of our current problems:
We should develop new payment and transactional mechanisms. PbR is the main cause of inflation in this system and moving away from a system of being payed to do more, to delivering better outcomes is long overdue. In the short term we should move to a block for acute contracts, which should be set at a level that shares financial risk between commissioners and providers whilst we agree a new payment mechanism, ideally in the form of incentivised population and outcome based capitated budgets. We’ve been talking about it for some time, but there are examples elsewhere we could consider and adopt. The new ICP contract could provide a vehicle for this and should be considered.
We need a shared control total across the system, rather than individual organisation control totals. Regulators need to get behind this and work with us accordingly.
We need a 3-5 year plan to get back into financial balance, rather than the annual deficit shifting exercise we usually resort to and are currently engaged in.

Page 1 of 2
Together We’re Better
Update for members of the partnership
1. Introduction
1.1. David Pearson, Vice Chair, opened July’s Health and Care Transformation Board (HCTB) meeting as Sir Neil McKay was unable to attend.
1.2. Partners agreed that the recent STP digital conference was a success, highlighting it was an inspirational and thought-provoking session.
1.3. Conference speakers included representatives from four other health economies, who shared their experiences and offered further help to Staffordshire and Stoke-on-Trent.
2. Pre-consultation update
2.1. Tracy Parker-Priest, STP Chief Operating Officer, reiterated the decision at the last HCTB that partners should take time to consider the scope of the planned engagement activity. TWB partners are committed to ensuring that when engagement with our public and stakeholders starts, discussions will include all areas of change that will help make our system clinically and financially viable.
2.2. Since the last board meeting a session with partners’ chairs, chief officers, lay members and non-executives was held to further the debate. An action was agreed that all partners would take this discussion to their respective boards. Partners will provide their updates to the HCTB next month.
2.3. Further risks were identified for consideration, including:
potential confusion for the public in running the formal consultation process on community hospitals in the North of the county alongside the wider pre-consultation engagement process
a need to balance competing priorities for senior leadership time; during expected winter pressures and planned engagement activity requiring intensive support
from a local authority perspective, there will be a requirement to engage on commissioning intentions during the latter part of the year and there are also local elections to consider.
2.4. Simon Whitehouse, STP Director, confirmed a diagnostic report has been commissioned, to bring together at a system level:
data from Rightcare, Getting it Right First Time, Model Hospital etc. that evidences improvements in outcomes for patients and the removal of potential system duplication
analysis of the key performance drivers across the system with recommendations on how performance can be improved.

Page 2 of 2
Simon confirmed that outputs from this are expected in approximately eight weeks and it would be a missed opportunity to not include this in the scope consideration.
2.5. David summarised the discussion above asking partners to also consider any quality and safety risks that could arise as an unintended outcome, whilst we are re-considering scope.
2.6. It was agreed that a more detailed paper would be brought back to the September H&CTB that would set out a revised timeline for consultation
3. Urgent and emergency care workstream update
3.1. Becky Scullion, CCGs’ Deputy Director of Commissioning and Operations, presented an update highlighting learning from good practice and how this has informed a whole system approach.
3.2. It was noted that explaining urgent and emergency care to the public would be the one of the next priorities for the programme. It was also acknowledged that this programme has many interdependencies with other programmes, in particular, the Enhanced Primary and Community Care workstream.
4. Locality working
4.1. Further to the CSU Strategy Unit’s presentation at the last HCTB, an update was given on the changes needed to bring together a range of providers to deliver locality working.
4.2. Partners reflected on the Organisational Development (OD) support needed to help staff work in a different way and enable true clinical leadership.
4.3. Caroline Donavan, Senior Responsible Officer for OD, confirmed that her programme would help by bringing together this workstream with EPCC and the Strategy Unit to agree how this can be done effectively. A further update would be brought to HCTB in September 2018.
5. Next meeting of the HCTB
5.1. Simon asked for confirmation of attendance in August 2018 to ensure quoracy. Members confirmed availability and it was decided this meeting will go ahead.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 6.2
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Accountable Officer’s Report
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Marcus Warnes, Accountable Officer N/A Marcus Warnes, Accountable Officer
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
Action Required (select):
Decision Discussion For Assurance / For Information
Purpose of the Paper (Key Points + Executive Summary):
This report provides an update to the governing bodies around the current environment that the CCGs are operating in. The report highlights
The first quarters financial performance including QIPP delivery
A & E performance including progress on Discharge to Assess (D2A)
An update on the Pre-Consultation Business Case (PCBC)
An update on the STP
The Better Care Fund (BCF)
CQC update
CCG Consolidation update
Progress on the development of the CCGs revised governanace arrangements The Governing Bodies are requested to:
Note the contents of the report.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
Implications:
Legal and/or Risk
CQC
Patient Safety

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Patient Engagement
Financial
Sustainability
Workforce / Training
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
Recommendations / Action Required:
The Governing Bodies are asked to: Note the content of the report

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
1.0 Financial and QIPP Position for 2018/9
1.1 At month 4 the year to date position for both CCGs combined is a £17.12m adverse variance against plan, with an £14.92m in-year actual deficit reported (North Staffs £8.37m deficit, Stoke on Trent £6.55m deficit). This compares to a planned position at month 4 of a £2.20m surplus (North Staffs £0.27m surplus, Stoke on Trent £1.93m surplus). Further detailed information is contained in the finance report later on the agenda.
1.2 Due to the current financial position the CCGs are in financial escalation with NHS England. We met
with Dr Paul Watson on Friday 17th August; one of the outcomes of this meeting was that we appoint a Turnaround Director and NHS England are supporting us with this process. The next planned meeting with NHS England is Friday 31st August 2018.
2.0 A&E Performance and Discharge to Assess (D2A) 2.1 Performance across the urgent care system has previously been reported as having improved
despite significant pressure resulting from the heatwave over the summer. Performance remains static with the validated M3 performance against the 4-hour standard being 82.8%. Detailed performance information is reported later in the agenda.
2.2 The CCGs continue to work with partners to manage demand and to ensure that sufficient bed and
home based capacity is in place to facilitate timely discharge. 2.3 Commissioners and providers have collaborated on the production of the Winter Plan for 2018/19
ensuring that all partners are committed to effectively manage expected demand. The deadline for submission of the latest draft plan to NHS England is 30th August. More detailed information on the Winter Plan including a draft copy is reported later in the agenda.
3.0 Pre Consultation Business Case – The Future of Local Health Services 3.1 As previously reported the Pre-consultation business case (PCBC) relating to the future of health
services in North Staffordshire was presented to the NHS England assurance panel on 17th July 2018.
3.2 A further assurance panel was held on 17th August, with a further panel at the end of September. 3.3 The feedback from the panels has been positive, with a number of areas that the CCGs will need to
work on for the PCBC to be consultation ready. The aim is to seek final approval from the panel in late September, after which the PCBC will be considered by the national investment committee in October. Once signed off, the CCGs can then begin formal consultation.
3.4 The Consultation Institute continue to work with the CCGs to quality assure the consultation process
to ensure compliance with our legal duties and best practice. 4.0 Staffordshire and Stoke-on-Trent Sustainability and Transformation Partnership (STP) 4.1 As the governing bodies are aware, Together We’re Better is the STP for Staffordshire and Stoke-
on-Trent. It is made up of NHS and local government organisations that are working closely together to transform health and care for people living and working in the area. The two local Healthwatch organisations also have a seat at the decision-making table.
4.2 Progress has been made in shaping proposals across a number of key areas including:

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
the prevention agenda
improving local primary and community care
increasing the effectiveness and efficiency of planned care
work to develop a simplified urgent and emergency care system
further improving local mental health services, and
improving children, young peoples’ and maternity services. 4.3 Work has also been taking place to strengthen clinical leadership and accountability within the
partnership. This is being delivered through the STP Clinical Chairs and Lay Members meeting, which was most recently held on 10th July.
4.4 Together We’re Better’s Independent Chair, Sir Neil McKay, recently shared some of the emerging
thinking taking place within the partnership, including an ambition for swift progress to be delivered in a number of areas.
4.5 These include implementing a greater number of integrated care teams across the area. These
would build on the work being done locally to bring together a range of physical and mental health services alongside social care professionals and the voluntary and community sector to enable a coordinated approach to improving population health.
4.6 Teams will provide care that:
helps more people lead healthy, active lives
enables more people to remain independent for longer
reduces the need to attend or stay in hospital
reduces the length of time people spend in hospital
predicts personal needs and plans care to prevent problems before they arise
makes greater use of technology and home adaptations, and
supports families and carers in their roles. 4.7 Over the coming months, there will be an increased focus on communications to enable the STP to
inform local people about what has been happening and prepare them for the consultation process that will begin next year.
4.8 The STP has identified a planning gap across Staffordshire relating to income expectations of
providers and expected levels of expenditure by commissioners. A joint diagnostic review is being undertaken by NHSE and NHSI, to provide a comprehensive and coherent diagnostic of the issues across the Staffordshire health system. The process is expected to take 6-8 weeks and commences in early August.
5.0 Better Care Fund (BCF) 5.1 Performance for Stoke-on-Trent delayed transfers of care (DTOCs) continues to improve and the
target that has been set nationally achieved. The CCGs and Stoke-on-Trent City Council continue to work closely with Midland Partnership Foundation Trust to ensure that commissioned capacity continues to be available to further reduce DTOCs.
5.2 Performance for Staffordshire DTOCs remains off trajectory, with more DTOCs occurring than
planned for. Daily calls with providers continue with individual patient discharges being micro-managed to ensure that patients are not delayed unnecessarily and that delays reduce.
5.3 Stoke-on-Trent CCG and the City Council have agreed and submitted the Q1 report template
relating to BCF progress. Further information is contained in the performance report.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
5
6.0 CQC Local System Review 6.1 Significant progress has been made on delivery of the improvement plan that resulted from the local
system review the CQC. 6.2 Stoke-on-Trent CCG and the City Council have agreed on a draft integrated commissioning strategy
that will be overseen by a newly re-constituted Health and Wellbeing Board. This high level agreement supports collaborative commissioning across health and social care where there are clear benefits to the local system in doing so. A more detailed delivery plan is in development and expected to be presented at the Health and Wellbeing Board in September.
7.0 CCG Reconfiguration Proposals 7.1 The Management of Change process concluded on 1st May 2018 as previously reported. 7.2 Staff vacancies that resulted from this process have now been advertised and recruitment
commenced, with a view to completing the recruitment process in the coming two months. Where necessary temporary appointments have been made to add additional capacity to support substantive staff and bridge the gaps until recruitments are concluded.
8.0 New Governance Arrangements 8.1 The six CCGs’ governing bodies met in common on 19th July to discuss the new governance
arrangements. These discussions will continue in the coming weeks with GB members fully engaged and driving the shape of future governance arrangements from both a corporate and clinical management governance perspective.
8.2 The draft terms of reference for the proposed northern Divisional Committee (North Staffs and
Stoke-on-Trent CCGs) are being shared with the CCG membership in September for endorsement and to ensure appropriate levels of clinical engagement are secured in the new arrangements.
9.0 Recommendations 9.1 The governing bodies are requested to: 9.1.1 Note the contents of the report.
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 6.3
Report to: North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies Public Meeting in Common
Title: Urgent and Emergency Care STP Programme
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
CHERYL HARDISTY Y Becky SCULLION
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
AIDEEN WALSH/STEVE FAWCETT URGENT AND EMERGENCY CARE
Action Required (select):
Decision Discussion For Assurance / For Information X
Purpose of the Paper (Key Points + Executive Summary):
1. This paper sets out a high level briefing for Governing Body Members regarding Staffordshire
and Stoke-on-Trent Urgent and Emergency Care (UEC) Programme.
2. The UEC programme is responsible for the delivery of simplified access to urgent and
emergency care services, developing services for people to use as an alternative to accident
and emergency and key delivery projects aimed at enabling patient flow. The programme is a
fundamental aspect of the Sustainability and Transformation Plan (STP) and all aspects of the
programme are aimed at supporting improved health and well-being.
3. Seven projects have been established within the UEC Programme. Key elements of these
include:
A revised NHS111 service offer including NHS11Online and a Clinical Assessment Service (CAS)
Urgent Treatment Centres (UTCs) made available across the Staffordshire footprint
Extensive series of changes internal to the local Emergency Departments.
Improving discharges from the acute trust bed base.
4. These changes are intended to improve individuals’ experience of urgent and emergency care,
reduce long waits and ensure that when individuals need access to emergency care, it is
immediately available.
5. UEC Programme progress includes:
The Urgent and Emergency Care Programme Board has been refreshed with revised Terms
of Reference and Membership. The Board now incorporates the East and West A&E

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Delivery Boards.
Clinical involvement in the programme is strong, with two identified STP Clinical Leads in place for the Staffordshire and Stoke-on-Trent UEC Programme covering Secondary and Primary Care and 6 out of the 7 UEC Projects are clinically led.
A Single Operational Delivery Plan for UEC programme covering UEC Transformation Programme and UEC (A&E) Delivery was submitted to the 19 July Health and Care Transformation Board (HCTB).
A comprehensive Demand and Capacity Model has been commissioned. The model commissioned is the first of its kind nationally, and will include primary and community care in its widest sense. The modelling is scheduled for final completion by April 2019.
An acute Demand and Capacity Plan is in place to support winter and has been developed with system partners, including regulators. The Winter Plan is based on physical beds being in place to support delivery. The financial implications of the Winter Plan are not yet resolved and have been escalated to CEOs of each organisation.
Development of a single whole system recognised UEC Dashboard is being overseen by the UEC Programme Board and an initial draft will be submitted to UEC Programme board on 5th September. The focus is on integrating the UEC Tracker (NHSE) into a single UEC Plan dashboard that reflects all national and locally agreed system targets.
6. UEC Projects will contribute to the achievement of:
Achieve and sustain the 4 hour wait target with all Emergency Departments
Reduce A&E attendances by 30%
Reduce emergency admissions by 23%
Reduce emergency admissions by frail elderly and/or patients with one or more LTC by
30%
Reduce Delayed Transfers Of Care (DTOCs) to 2.5%
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
Each project will identify risks and issues and escalate to UEC Board where above an agreed level. UEC Programme Risk Register identifies Programme Level Risks, these are escalated to Health and Care Transformation Board if cannot be mitigated at Programme Board Level. Any material risks will be identified on the CCGs Corporate Risk Register
Implications:
Legal and/or Risk
CQC
Patient Safety
Patient Engagement
Financial
Sustainability
Workforce / Training
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
X

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
X
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
x
Recommendations / Action Required:
The Governing Body is asked to note the briefing on the Urgent and Emergency Care Programme.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
Staffordshire and Stoke-on-Trent Urgent and Emergency Care (UEC)
Programme Briefing for CCGs Governing Body
1. Background
1.1. The Staffordshire and Stoke-on-Trent Urgent and Emergency Care (UEC) Programme is
responsible for the delivery of simplified access to urgent and emergency care services,
developing services for people to use as an alternative to accident and emergency. It also
includes some key delivery projects aimed at enabling patient flow (i) away from and through
acute hospital settings. The programme is a fundamental aspect of the Sustainability and
Transformation Plan (STP) and all aspects of the programme are aimed at supporting
improved health and well-being for our communities.
1.2. The NHS Five Year Forward View (1) articulates the need for integrated services and a radical
redesign of the urgent care system to one which is responsive to the changes in individual’s
health care needs and preferences and advances in care within the NHS that have been
made over the last 70 years.
(i) The term ‘flow’ describes the progressive movement of people, equipment and information through a sequence of processes.
In healthcare the term denotes the flow of patients between staff, departments and organisations along a pathway of care.
1.3. This paper provides an overview of local progress to date and discusses the anticipated risks
and benefits associated with proposed changes in the urgent and emergency care pathway.
2. Programme Principles and Vision
2.1. The UEC Programme is based upon three key guiding principles:
- Self-care and Prevention
- Right care, first time
- Easy to navigate with consistent offer
The vision of the programme is for simplified access for patients and their carers to a fully
developed integrated urgent care offer incorporating options for self-care. This vision and model
has been developed with clinicians, and is part of an ongoing iterative process to design the UEC
system for Staffordshire and Stoke-on-Trent.
Fig 1: Draft model for UEC (revised version currently in development)

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
2.2. The UEC programme is underpinned by the Enhanced Primary Care (EPCC) offer. This
includes the development of Primary Care Hubs which will be supporting an integrated
approach to care which is based around local need assisting individuals to self-care, access
voluntary care services and providing support for patients who have chronic, long term health
conditions or are frail entering the last years of life.
2.3. In addition to this offer there will be a revised NHS111 service offer. NHS England have
released a national specification (2) outlining the need for each service to have access to a
range of clinical support which will enhance the level of advice given over the telephone, and
on line, to both the public and clinicians. Another significant change is the ability for this
service to make direct appointments for individual callers to have a face to face consultation
with General Practice and the wider urgent and emergency care services. The Integrated
Urgent Care (IUC) service will become the gateway for the local population to access the right
service at the right time. The mandatory requirements must be in place by March 2019
(delivered through existing contracts) and full procurement of an integrated service will
conclude by March 2020.The key requirements are NHS111 online, the Clinical Assessment
Service and Direct Booking of appointments through NHS111.
2.4. The UEC Programme is also required to develop a plan which will see Urgent Treatment
Centres (UTCs) made available across the Staffordshire footprint. National Standards have
also been released by NHS England (3) which confirms that each UTC must provide access to
diagnostics, such as x-ray and blood testing, be open a minimum of 12 hours each day and
support “walk in” presentation alongside bookable appointments. All UTCs will provide a
multi-disciplinary service which is led by a GP. There is a national requirement to have
designated UTCs implemented by March 19. However, Staffordshire has been given approval
to have UTCs in place within the last phase (31.12.19).
2.5. The UEC is also proposing an extensive series of changes internal to the local Emergency
Departments. Through the use of improved referral mechanisms and tapping into digital
options, General Practitioners will have the ability to discuss and agree patients transfer into
speciality clinics where an urgent opinion is sought. This should prevent individuals attending

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
A&E with referral letters and having to wait significant periods of time to access the
appropriate clinical expertise.
2.6. There is also a tranche of work aligned to the UEC programme aimed at improving discharges
from the acute trust bed base. There is a significant amount of data and research which
highlights the debilitating effect of prolonged hospital stays on the most frail and vulnerable of
our population. This area of the programme strongly links with the EPCCs Discharge to
Assess (D2A) model of care.
2.7. Ultimately these changes are intended to improve individual’s experience of urgent and
emergency care, reduce long waits and ensue that when individuals need access to
emergency care, it is immediately available.
3. Impact
3.1. The UEC Programme has targets including :
Achieve and sustain the 4 hour wait target with all Emergency Departments
There have been issues with sustaining a level of performance within the local Emergency
Departments. It is expected by making access to alternative services easier and thereby
reducing attendances to the Emergency Departments front door, the UEC work stream will
support the local acute trusts to successfully achieve this target, thereby improving the
quality of patient’s experience.
Reduce A&E attendances by 30%
Nationally it is recognised that 40% of A&E attendances do not require urgent of
emergency intervention, which predominately represent frail and elderly individuals with
poorly managed LTCs.
Reduce emergency admissions by 23%
In addition the understanding from these findings is that 38% of those individuals could be
managed in a less clinical and acute environment and that at any one time within the acute
care system the equivalent of 8 wards across Staffordshire have people in them who no
longer require an acute care setting.
Reduce emergency admissions by frail elderly and/or patients with one or more LTC
by 30%
A local review of Staffordshire and Stoke-on-Trent accident and emergency activity
suggested that 83% of our non-elective admissions of over 65s have 1 or more long term
condition. There is also evidence to support that our most frail and elderly local residents
who are receiving care within a care home environment should receive an enhanced level
of care through Primary Care and Community Integrated Services ensuring that there is
support to meet needs in a care home setting and reduce attendances and admissions to
hospital where appropriate.
Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
Reduce Delayed Transfers Of Care (DTOCs) to 2.5%
Local services are required to reduce the number of people who are experiencing delays in
their discharges to 2.5%. The UEC is working in partnership with community and social
care providers and through the Better Care Fund to support the achievement of this
important milestone.
4. Progress with UEC Programme
4.1 Programme, Projects and Governance
To date seven projects have been established within the UEC Programme:
Transformation Projects
TR1 Simplified Access
TR2 Integrated Urgent and Emergency Care Offer
Delivery Projects
UEC 1 Working Together as One Health and Care System
UEC 2 Wider System Delivery
UEC 3 Hospital Front Door
UEC4 Hospital Flow
UEC5 Hospital Discharge
Each project has a project lead and a project manager and there are two STP Programme
Managers in place to support delivery of the Transformational Projects (TR1 and TR2) and
Delivery Projects (UEC1 to UEC5).
The projects will be managed through the governance process below:

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
5
Project Initiation Documents (PIDs) for all UEC Projects (7) are in draft and will be submitted
to September UEC Programme Board for formal sign off.
4.1.2 Urgent and Emergency Care Programme Board
The Urgent and Emergency Care Programme Board has been refreshed with revised
Terms of Reference and Membership. The Board now incorporates the East and West A&E
Delivery Boards in addition to STP UEC Programme.
The Urgent and Emergency Care Programme Board will provide the strategic and
operational leadership across the health and social care system for Staffordshire and be
accountable for the delivery of the Urgent and Emergency Care STP Programme.
The newly merged UEC Programme Board met 8 August 2018 and meetings will now take
place monthly.
4.1.3 Clinical Engagement and draft UEC Model
There are two identified STP Clinical Leads in place for the Staffordshire and Stoke-on-
Trent UEC Programme covering Secondary and Primary Care.
In addition 6 out of the 7 UEC Projects are clinically led. An outline draft model for UEC in
Staffordshire and Stoke-on-Trent has been developed with key clinicians. A clinically led
workshop was held (15 August 2018) to further develop this model and a revised model will

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
6
be widely shared as part of an iterative process to design the future system for
Staffordshire and Stoke-on-Trent.
A further workshop is planned to take place 12 September, focussing on Urgent Treatment
Centre development (UTCs).
4.1.4 UEC Operational Plan
A Single Operational Delivery Plan for UEC programme covering UEC Transformation
Programme and UEC (A&E) Delivery was submitted to the 19 July Health and Care
Transformation Board (HCTB).
The plan responds to the STP Transformational Plan of 2016, Newton Europe Report and
the Sir Neil McKay Urgent Care Review January 2018 and includes plans for each of the
UEC Projects identified at 4.1.
The Plan will support Urgent and Emergency Care services to achieve their constitutional
targets and to deliver the Five Year Forward View (and Next Steps) including national UEC
Deliverables.
The plan is a live document and as such continues to evolve. The Plan will be delivered
through detailed UEC Programme Project Plans and their delivery will be monitored
through UEC Programme governance and assurance processes and PM3 system.
4.1.5 Additional areas of Progress
- Refreshed data has been gathered to inform options appraisal for UTCs and heat maps
are in development.
- A progress report on Sir Neil McKay’s Urgent Care Review Recommendations completed
and reported to August Health and Social Care Transformation Board.
- STP Finance Lead confirmed.
- A comprehensive Demand and Capacity Model has been commissioned. The model
commissioned is the first of its kind nationally, and will include primary and community
care in its widest sense. The modelling is scheduled for final completion by April 2019.
- An acute Demand and Capacity Plan is in place to support winter and has been
developed with system partners, including regulators. The plan is accepted as robust and
well developed. However, the financial implications of the plan are not yet resolved and
are with CEOs of each partner organisation and the Chair and Director of the STP to
reach a system solution.
- Development of a single whole system recognised UEC Dashboard is being overseen by
the UEC Programme Board and an initial draft will be submitted to UEC Programme
board on 5th September. The focus is on integrating the UEC Tracker (NHSE) into a
single UEC Plan dashboard that reflects all national and locally agreed system targets.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
7
5. Risks and Mitigation
5.1. The UEC Programme has identified that there are a number of issues/risks that are
associated with the proposed transformational changes.The programme is working across a
number of STP programmes to mitigate through inter-dependency working. This is particularly
the case for ensuring:
Sufficient workforce within primary and community care to support the transfer of
activity away from the emergency departments;
Capacity built into services which will meet current and future demand;
Gathering support for change from all key stakeholders
Aligning consultation and engagement timescales with mandated delivery.
6. Summary
6.1. This briefing has been produced to provide an outline of the UEC Programme, the intended
outcomes and impacts and the key risks associated with the transformation of the urgent and
emergency care system.
6.2. The Governing Body is asked to note the briefing on the Urgent and Emergency Care
programme.
1. The Five Year Forward View (1) https://www.england.nhs.uk/wp-content/uploads/2014/10/5yfv-web.pdf
2. Integrated Urgent Care Specification https://www.england.nhs.uk/wp-content/uploads/2014/06/Integrated-Urgent-
Care-Service-Specification.pdf, August 2017
3. UTC National Standards - https://www.england.nhs.uk/wp-content/uploads/2017/07/urgent-treatment-
centres%E2%80%93principles-standards.pdf

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 6.3a
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Winter Plan
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
CHERYL HARDISTY Y MATT BEARDMORE
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
AIDEEN WALSH/STEVE FAWCETT Y (Urgent and Emergency Care)
Action Required (select):
Decision Discussion For Assurance / For Information Y
Purpose of the Paper (Key Points + Executive Summary):
This paper sets out a high level briefing for Governing Body Members regarding the Staffordshire and Stoke-on-Trent Winter Plans for 2018-19. The Staffordshire urgent care system has faced challenges for a number of years, consistently failing to deliver the 4 hour target. Winter 2017-18 was recognised as one of the worst on record for the Staffordshire and Stoke on Trent system, resulting in poor experiences and outcomes for patients. The STP commissioned Fusion 48 to review the 2017-18 Winter Plan and their report concluded that the system clearly did not work together to develop a coherent and deliverable plan. Key findings and recommendations were:
Use the STP framework for planning to ensure strategic objectives and programmes link;
Avoid long lists of winter schemes (Avoid long lists of winter schemes (there were c. 100 in 2017-18);
Adopt a more segmented approach to planning and use targeted KPIs;
Improve consistency of planning across the STP footprint;
Agree clear and consistent information flows. Further to these recommendations, NHS England wrote to Chief Executives, Accountable Officers and STP leads in June 2018 to detail their expected priorities:
25% reduction in the number of long stay patients in acute hospitals;
Holding or reducing length of stay for all other patients;
Reducing bed occupancy to manageable levels.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
The UEC system has acknowledged the report findings and has embraced the opportunity to ensure the lessons learned are in place for this year’s plan.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
The main risk will be the affordability of the winter plan. There are a number of initiatives that will need an investment, such as capital work at RSUH, and additional CCG commissioned care home capacity. All partners have shared financial plans and these are now being reviewed together as a system to come to an agreement on final costs and then how this will be financed.
Implications:
Legal and/or Risk
CQC
Patient Safety
Patient Engagement
Financial
Sustainability
Workforce / Training
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
No
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
No
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
No
Recommendations / Action Required:
The Governing Body is asked to note the briefing on the Winter Plan
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
1. Winter Planning 2018-19 1.1. Winter Planning began in June 2018, with weekly conference calls in place with all system partners to
discuss priorities and risks for the winter period.
1.2. The following areas were identified as the key focus areas, and agreement was reached between all organisations on the broad principles to ensure that each system partner’s plan has consistent assumptions built into it:
Demand and capacity plans;
Front door processes and primary care streaming;
Flow through the urgent care pathway;
Effective discharge processes;
Planning for surge in demand;
Workforce;
Adoption of best practice.
1.3. All system partners have developed organisational winter plans, covering the points above, which the
CCG has then used to form the system-wide winter plans for the East and West Staffordshire health economies. These plans were sent to each organisation for review/approval on 22nd August, with a deadline of 28th August for any comments received prior to submission to NHS England on 30th August.
1.4. Although there are submission deadlines, it is recognised that this is a live plan which will be reviewed and updated weekly from now through to April 2019 by local operational delivery teams in line with the milestones in the national timetable. More detail on this is provided in section 6 ‘Next Steps’.
2. Governance 2.1. There is a single Urgent and Emergency (UEC) Care Programme Board across Staffordshire. To
align with the STP Urgent and Emergency Care Programme, the two previous A&E Delivery Boards in Staffordshire agreed to merge to create the new Programme Board, with authorisation from both NHS England and NHS Improvement.
2.2. The UEC Programme Board is responsible for the oversight of the urgent and emergency care services delivered at the Royal Stoke University Hospitals, at Queen’s Hospital, Burton upon Trent and at County Hospital in Stafford; the latter operating a 14 hour day time service only with inpatient medical beds to support admissions.
2.3. The UEC Programme Board is accountable to the overall STP Health and Care Transformation Board. The Staffordshire STP has provided leadership to the development and implementation of the Winter Plans across Staffordshire. The UEC Programme Board will provide ongoing overview and assurance to implementation of this plan.
2.4. There will be weekly operational groups meeting to tactically manage the implementation and delivery
of the winter plan and A&E performance over winter. This will be complemented by ongoing daily system calls to resolve system blockages and highlight issues for the tactical meetings.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
2.5. The structure of this plan provides an overarching narrative around the key challenges facing the Staffordshire UEC system this winter, and the Delivery Boards have created their own respective plans which address their particular local circumstances. The Board will continue to be supported by the Staffordshire STP programme, but they will provide the ongoing day to day management of the plan and implementation.
3. Engagement
3.1. People are the key to ensuring the success of the winter plan. It is therefore imperative that everyone
within the health and social care system is aware of the contents of this plan and the implications of it for them to ensure ownership of the actions. If everyone understands their role on a day-to-day basis, the plan can be delivered.
3.2. Assurance will be sought from system leaders that their organisations support and own the content and delivery of the plan. Key tests/questions which will be asked of all system partners to ensure this has occurred will be:
Is the plan embedded to ‘service level’?
Is there ownership at service level / front-line level?
Sunderland System / cards – is this in place from top to bottom?
Role of leaders / visibility of leaders – not just at board level but on the wards / evidence that the plan is known at front-line level.
4. Finances 4.1. The CCG has worked closely with system partners to attach financial values to the delivery of the
Winter Plan for 2018-19.
4.2. All organisations have shared financial plans and these are now being reviewed together as a system to come to an agreement on final costs and then how this will be financed.
5. Next Steps
5.1. The final version of the Winter Plan will be submitted to NHS England today (30th August). It is expected that the plan will continue to evolve as a result of comments from NHS England, in addition to other national guidance expected over the next couple of months.
5.2. For example, we are anticipating further correspondence from Pauline Philips, National Urgent &
Emergency Care Director NHS England and NHS Improvement around winter plan expectations on 3rd September which may require further revision of the plan as it stands.
5.3. Furthermore, discussions around the financial affordability may also have an impact on the Winter
Plan. 5.4. As noted in section 4, further work will also be required to understand how the financial cost of the
plan will be funded. The table below details the next steps for the winter plan:

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
5
Fig. 2: Timetable for 2018/19 System Wide Winter Plan
Date Action
23-08-18 Operational Assurance and Risk Template to be issued to Providers by NHSI
30-08-18 Submit Final Integrated System Winter Plan to NHSE 17-09-18 Operational Assurance and Risk Template to be returned by Providers to NHSI 17-09-18 NHSE to complete formal Assurance
01-10-18 All plans and schemes to be in place and operational by 1 October 2018 in readiness for the start of Winter
Early Oct 2018
Winter Preparedness Assurance Visits undertaken by NHSI (Providers)

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 6.4
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Together We’re Better Update
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Marcus Warnes Y Anna Collins/Ruth Boyd
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
Y – all programmes
Action Required (select):
Decision X Discussion X For Assurance / For Information X
Purpose of the Paper (Key Points + Executive Summary):
To provide an update to Governing Body Members on:
The revised vision of Together We’re Better
The programmes
The current implementation priorities
The pre-consultation process
To agree how the Governing Bodies would like to receive future updates.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
Risks are held on the Together We’re Better risk log and summarised in the implications section below
Implications:
Legal and/or Risk Failure to engage the public in a robust way about any potential changes to services will attract a risk of legal challenge
CQC
Patient Safety Any potential changes will be subject to appropriate clinical scrutiny and a quality impact assessment
Patient Engagement Failure to engage the public in a robust way about any potential changes to services will attract a risk of legal challenge
Financial The key driver for potential changes is to achieve both clinical and financial sustainability for the Staffordshire and Stoke-on-Trent health and care system
Sustainability The key driver for potential changes is to achieve both clinical and financial

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
sustainability for the Staffordshire and Stoke-on-Trent health and care system
Workforce / Training Potential changes to achieve sustainability will include a programme of workforce development
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
X
Not at this stage
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
X
Drafted for the
engagement process and planned for each of the
programmes
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
X
Limited engagement
that is planned to significantly increase as we move
into the Pre-consultation
process
Recommendations / Action Required:
The Governing Body Members are asked to:
Note the contents of the presentation
Agree the format of future updates on progress of Together We’re Better programmes

Together
We’re Better

Final vision
“Working with you to
make Staffordshire and
Stoke-on-Trent the healthiest
places to live and work”
2
• People living well for longer
• Treating people and not a set of conditions
• Supporting and enabling you to stay well and
independent so we can be there when you need us
• More care delivered near to where you live
• Giving mental health equal priority to physical health
• Ensuring your experience of health and care is the
best it can be.
Together We’re Better is about..
3

Our
programmes

Overview
• Urgent and Emergency Care
• Planned Care
• Prevention
• Maternity, Children and Young People
• Mental Health
• Enhanced Primary and Community Care
• Digital
• Workforce
• Organisational Development and System Leadership
• Future of Stafford and Surrounds Health and Care Services
Urgent and emergency care
We want to make it easier for people to understand where they can go when they
have an urgent health need or healthcare emergency and ensure the treatment
they receive is timely and of high quality.
Priorities and projects
Self-care and prevention
Right care, first time
Easy to navigate with consistent offer
There are a number of projects in place aimed at improving every individual’s
experience of urgent and emergency care, reduce long waits and ensure that
when individuals need access to emergency care, it is immediately available.

Urgent and emergency care
SRO
Aideen Walsh
Programme Director
Cheryl Hardisty
Programme Manager
Christina Wigfall (Transformation)
Amanda Locke (A&E delivery)
Clinical leads
Dr Gulshan Kaul (Primary care - all)
Dr Zia Din (Secondary care - all)

Planned care
The aim of this programme is to deliver high quality and effective services safely in the right setting, at the right time and with the right professional. By 2020, the majority of people living in Staffordshire and Stoke-on-Trent will be able to access high quality elective care that is both clinically and financially sustainable, with the majority of services being provided through NHS trusts. Furthermore, alliances of local providers working across organisational boundaries will deliver efficient integrated care.
Priorities and projects
Utilise seven-day elective centres to ensure improvements in productivity, efficiency
and quality of care
Cancer - increase self-care and screening uptake, early access and intervention
Develop a Staffordshire and Stoke-on-Trent-wide sustainable model for outpatient
and day case provision
Efficiency – speciality focus
Consolidate diagnostics
The principles of a well-managed care system will be introduced, where there is
absolute clarity of the service offer and expectations for delivery
People will be empowered and supported to self-care and will feel confident in
choosing NHS services within Staffs and Stoke-to-Trent to receive their care

Planned care
SRO
Paula Clark
Programme Director
Mark Seaton
Programme Manager
Fleur Fernando
Clinical leads
Dr Steve Fawcett (Primary care)
Dr Vijay Jeganath (Secondary care)

Prevention
Enabling you and your family to take control of, and manage your own health and
wellbeing so that we can be there when you really need us.
Priorities and projects
Preventative pathways – Simplifying and connecting services for greater
wellness focused care creating a health and care system culture that promotes
self-reliance and wellbeing
Supportive communities – Creating a culture of ‘think family and community
first’ so that you family are able to live independently and manage your care
needs with support from families and communities
Digital and voice – Connecting and giving people their data, insights and
information to support wellbeing lifestyle choices and healthier lifestyles
Healthy environments – Improving where and how we live, enabling you to
make improvements to your environment and reducing risks to wellbeing

Prevention
SRO
Paul Edmondson-Jones
Programme Director
Karen Bryson
Programme Manager
Vicky Probyn
Clinical leads
Dr Gulshan Kaul (Primary care)

Maternity, children and young people
The Pan Staffordshire Maternity Transformation Programme is tasked with
implementing the recommendations arising from NHS England’s Better Births report,
and is working in partnership with Together We’re Better and parents and parents-to-be
to develop local maternity services. NHS England is providing additional funding for this
work and is helping to shape and improve the care we offer women and their families
now and for the future.
Priorities and projects
Improving the quality and safety of maternity and newborn services – Working with hospitals from surrounding areas to learn and share best practice
Engagement and co-production with women and their families – Maternity Champions are being recruited to work with women and families in co-producing and improving services
Configuration of maternity services – Run by senior midwives to develop new ways of working; e.g. increasing personalised care planning
Improving health and wellbeing of women and babies – Working in partnership with Public Health to undertake a wide variety of improvements; e.g. increase breastfeeding rates
Improving access to perinatal mental health services – Seek to increase capacity in order to see more women early and help to destigmatise mental health issues

Maternity, children and young people
SRO
Helen Riley
Programme Director
Heather Johnstone
Programme Manager
Stephen Casbolt
Clinical leads
Dr John James (Primary care)
Dr Simon Cunningham (Secondary care)

Mental health
Older people, adults, young people and children in Staffordshire and Stoke-on-Trent will
feel supported whether they find themselves in need of help in crisis or to maintain their
day-to-day mental health and wellbeing. We will work in an integrated and collaborative
way to ensure your mental health is given equal priority to your physical health needs
and also ensure you receive the help and support you need closer to home and family.
Priorities and projects
Children and young people – Children will not unnecessarily be admitted to
hospital; those children with an eating disorder will receive a responsive
service, while more children will be able to access services
Integrated physical and mental health – People with both physical and mental
health care needs will experience integrated services built around their needs,
with services co-located with primary community care and social care
Suicide prevention – There will be an ambition for zero suicides
Out of area placement – People will receive care closer to home and there will
be a reduction in overall out of area placements
Mental health crisis/ urgent care – People with a mental health condition will be
able to access support 24/7 in a crisis and they will know where to access this
support

Mental health
SRO
Caroline Donovan
Programme Director
Jonathan O’Brien
Programme Manager
Fleur Fernando
Clinical leads
Dr Waheed Abbasi (Primary care)
Dr Abid Khan (Secondary care)

Enhanced primary and community care
This programme is developing localities across Staffordshire and Stoke-on-Trent that provide networks of fully integrated health and care services. It seeks to enable frail elderly and those with long term conditions to live more independent lives and avoid unnecessary, costly and upsetting emergency episodes and is also leading on improving end of life care.
Priorities and projects
Integrated Care Teams – Bringing together primary, community and mental health
services, alongside social care professionals and the voluntary and independent
sector – serving populations of 30-70,000 people and based around neighbouring
GP practices, with Alliance Boards as the delivery vehicles
• Early adopter ICT sites in Leek/Biddulph, Lichfield (frailty hub)/Burntwood,
Longton/Meir and Stafford
Extended access to General Practice – Due to go live from September 2018, with
more than 2,350 extra appointments to be delivered per week
Review of Community Hospitals South
Care Navigation – Reception staff at GP practices being trained to ask patients
simple questions about why an appointment is needed. Patients may then be
signposted to an alternative if appropriate, helping to free up more time for GPs to
spend with patients who need it most

Enhanced primary and community care
SRO
Marcus Warnes
Programme Director
Steve Grange
Programme Manager
Jo Wilkes (New models of care/ Community hospitals)
Clinical leads
Dr Bhushan Rao (Primary care - Frailty/ Long term conditions/ End of life, Integrated Care Teams)
Dr John Oxtoby (Secondary care - all)

Digital
Digital technology has been identified as a key enabler to deliver new models of
care across health and social care organisations in Staffordshire and Stoke-on-
Trent. By supporting in the transformation of local health and care services, digital
has the power to support individuals to live healthier lives, manage their own health
and wellbeing and reduce the demand on local services.
Priorities and projects
Your Care Connected – New digital shared care record linking NHS and local
government organisations to benefit patients and health/care professionals
Universal capabilities – A set of digital standards to enable more efficient and
equitable access to health and care across Staffs and Stoke-on-Trent
Information sharing
Business intelligence and healthcare analytics – supporting the development of
population health and care management across Staffs and Stoke-on-Trent
Model architecture – Establishing a robust, future proof and state-of-the-art
information technology infrastructure
Technology enabled care services (TECS) – Improving frontline health and care
services through the use of innovative apps and digital technologies
Sharing best practice via a Staffordshire and Stoke-on-Trent informatics network

Digital
SRO
Caroline Donovan
Programme Director
TBC
Programme Managers
Andrew Brown
Marc Talbot
Clinical leads
Dr Paddy Hannigan (Primary care)
Dr Zia Din (Secondary care)

Workforce
This programme collaborates with health and social care provider organisations
across Staffordshire and Stoke-on-Trent to deliver the strategy’s three core
workforce priorities.
Priorities and projects
Sustainability – Focussing on recruitment initiatives (e.g. UK/international
recruitment, retention, flexible working) and improving temporary staff utilisation
(collaborative staff bank, system-wide coordination for agency spend)
Future workforce – Focussing on widening participation (e.g. nursing
apprenticeships, work experience, train the trainer) and new roles (training
hubs, voluntary/independent sector)
Transformation – Focussing on STP clinical pathway workforce planning
(workforce modelling, preparing for public engagement), integration of health
and social care, transforming primary care workforce (introducing new roles,
implementing a primary care workforce plan) and delivering Health Education
England’s ‘Facing the Facts, Shaping the Future’ health and care workforce
strategy for England

Workforce
SRO
Neil Carr
Programme Director
Greg Moores
Programme Managers
Mish Irvine
Clinical leads
Primary care - TBC
Dr Ingrid Britton (Secondary care)

Organisational development & system leadership
Leaders need the skills and resilience to operate effectively across integrated systems.
As well as great leaders we need great engagement - systematic engagement and
empowerment of frontline staff is crucial for success. In addition, staff need the tools
and techniques to continuously improve care and to evidence their practice. There is
also the need for enhanced partnership working and joint accountability for delivery of
robust credible plans.
Priorities and projects Identify and develop aspiring talent, ensuring we are spoilt for choice for future
senior level vacancies
Generate greater system leadership capacity
Support TWB’s engagement of health and care professionals
Develop a leadership approach which adopts an engaging approach to the system and behaviours and improves culture
As a consequence, this will deliver a more assured and confident workforce
Continue to support compassion recognition schemes
Primary Care Leadership programme – Provided local clinical leads with the opportunity to develop system leadership skills via dedicated tailored programme
Black, Asian and Minority Ethnic (BAME) Leadership Programme – Seeks to address imbalances in BAME representation in leadership roles at every level, with 120 places available for NHS staff band 5-7
Organisational development & system leadership
SRO
Caroline Donovan
Programme Director
Alex Brett
Programme Managers
Jane Rook
Clinical leads
Dr John James (Primary care)
Mr Roger Wade (Secondary care)

Future of Stafford and surrounds health and care services
Scope currently being agreed. This is a new programme
Priorities and projects
To be added

Future of Stafford and surrounds health and care services
SRO
Richard Harling
Programme Director
Andrew Butters
Programme Managers
TBC
Clinical leads
Dr Paddy Hannigan (Primary care)
Mr Roger Wade (Secondary care)

1. Two exemplar frailty hubs running in Staffordshire and Stoke-on-
Trent by the end of June 2018
2. Clear social prescribing proposals worked up and ready to roll out
3. Early adopter of Integrated Care Teams (4) in place by July
4. Supported GP federations / networks to be established with a focus
on sustainable GP services
5. Significant reduction in out of area placements in mental health
6. Develop Outwoods as an exemplar community health and care
campus
7. Full implementation of all recommendations in the Urgent Care
Review
8. Detailed delivery plan of elective shift of activity to County Hospital.
Implementation priorities

Our pre-
consultation
process

Leading the changes
Clinical Commissioning Groups have the statutory
legal responsibility for any formal public consultation
process and will be the body/bodies that makes the
decisions informed by any consultation process.
The core team of Together We’re Better
will co-ordinate and deliver the process,
with members of the partnership, on their behalf.
28

Simplifying the Urgent and Emergency Care offer; community based urgent care services, Acute Urgent and Emergency Care proposals and New Care Model.
New vision for health and care in Staffordshire and Stoke-on-Trent, specifically current configuration of services at County Hospital.
Reviewing Community Hospitals (South; Sir Robert Peel Community Hospital in Tamworth and Samuel Johnson Community Hospital Lichfield).
Additional priorities to be identified to deliver clinical and financial stability.
1.
2.
3.
4.
Draft engagement scope
29

Proposed
timeline
Linear assurance processes (seeking Clinical Senate sign-off
prior to NHS Assurance Sessions)
The following diagram sets out the proposed timeline
minimum for the Pre-Consultation activities.
NHSE Assurance
Process Review
Month 6-9 Month 10-13 Month 14-17 Month 1-3 Month 4-5
Production of
the PCBC
12 Weeks
Pre-Consultation
engagement
Clinical Senate
Review Public
Consultation
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
North Staffordshire Clinical Commissioning Group and Stoke-on-Trent Clinical Commissioning Group
Enclosure: 7.1
Report to: North Staffordshire CCG and Stoke-on-Trent CCG Governing Bodies (Open Session)
Title: Quality & Safety Assurance Report
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Heather Johnstone, Director of Nursing and Quality.
Y Quality Leads – Lindsey Boughey, Nigel Williams, Mary Barlow, Kellie Johnson and Allison Heseltine
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
Heads of Quality and Patient Safety, Deputy Director of Nursing and Quality, and Director of Nursing and Quality
Y – University Hospital of North Midlands Risk Review Action Plan is linked to the Sustainability and Transformation Partnership Urgent and Emergency Care (STP UEC) operational plan.
Action Required (select):
Decision Discussion For Assurance x
Purpose of the Paper
1.0 Introduction:
1.1 This monthly report is intended to provide the Governing Bodies with assurance in respect of the on-going monitoring of quality and safety with all key providers. This assurance is obtained as a result of day to day quality and safety monitoring and regular proactive interaction with providers.
1.2 Key quality information is reported monthly to the Joint Quality and Safety Committee, which has delegated responsibility from all 6 of the Staffordshire CCGs for providing assurance on the quality of services commissioned and delivery of improved outcomes for patients.
1.3 The Joint Quality and Safety Committee on behalf of the Governing Bodies provides thorough detailed scrutiny and analysis of all information received and currently declares itself to have received one of the following levels of assurance:
Full Assurance Partial Assurance Limited Assurance Not Assured
1.4 Governing Body members are advised that as previously discussed the format of this report has been changed. This is the new report format which brings together the aspects of previous report formats for all 6 CCGs utilising the best aspects of each to ensure a strong but concise assurance report.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
2 .0 Key Risk/Assurance Areas
2.1 A pilot Joint Quality and Safety Committee meeting took place on 12th July 2018, and the scoring to determine the level of assurance was undertaken in line with the scoring system used previously in the South Staffordshire Joint Quality Committee for which training is being arranged for North Staffordshire and Stoke on Trent representatives. This is subject to review as the newly formed committee evolves.
2.2 Providers were reviewed at Joint Quality and Safety Committee on the 12th July 2018. The assurance levels illustrated in the body of the report reflected the challenges that the individual Providers are managing. The Governing Bodies are advised of specific actions being taken with each relevant provider in respect of this as follows:
University Hospital of North Midlands
A&E 4hr Waiting - There was an improvement as the Trust exceeded the NHSI submitted trajectory of 76% for April 2018 with a performance of 80%. There has been significant improvement in the 12 hour trolley wait figures.
RTT 18 & 52 Week Referral - The number of incomplete pathways remains fairly static at circa 48,300 patients but the number of over 18 week patients has reduced by some 300. A Planned Care Board has been set up to provide the necessary governance and oversight.
Falls: Type of Harm Reported as a SI - The patient falls that resulted in harm have decreased with 113 falls with harm compared to 116 in March 2018. The level of harm is reducing in those incidents being classified as moderate harm or above.
Midlands Partnership Foundation Trust
Care Quality Commission (CQC) Inspection Update – As part of the due diligence ahead of the acquisition the CQC re-inspected the two service areas where warning notices had been issued in 2016 on the 18th & 19th April 2018; Community Health Services for Adults and End of Life Care. The reports were published by the CQC on 2nd July 2018 and both service areas achieved a rating of ‘Good’ in every domain. The full reports are in the process of being received at Community Nursing Assurance Group, Clinical Quality Review Meeting and Quality Committee.
North Staffs Combined Healthcare NHS Trust
Waiting times for CAMHS Services have increased slightly month on month for the last three months which is being closely monitored via the Contract Review Board.
The SI category shows the largest increase of deaths reported under the category ‘pending review’ refer to the deaths of people known to substance misuse services. The initial change in commissioning arrangements for drugs and alcohol Services meant that SI’s detailed within One Recovery Services were being recorded under NSCHT and the addition of Stoke Community Drug and Alcohol Services (CDAS) has made an impact on the number of SIs reported from substance misuse services.
The sharp increase in self-harm incidents is as a direct result of the Trust’s change in recording data from the Mental Health Liaison Team based within UHNM. From April the Mental Health Liaison Team is now submitting activity through the Community Mental Health Teams to ensure that the relevant Community Team is briefed on awareness and action for their patient.
The Trust are implementing a new ‘Integrated Locality Working Project’ to align leadership, management and clinical staff in a way that supports the integrated, locality based, out of hospital services.
EZEC – Non Urgent Patient Transport
Concerns have been escalated from UHNM to the CCG relating to excessive waits that patients are experiencing. An escalation call was undertaken on 27th June 2018 between CCG contract and commissioner leads and E-zec to discuss the significant delays in the service provision. Subsequent to this the CCG Director of Commissioning and Operations has spoken with E-zec’s
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
Director of Operations and requested an immediate action plan to increase capacity.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
Corporate Risk Register Reference No: Q8, Q10, Q12 and Q13.
Implications:
Legal and/or Risk Risks identified and managed via the CCG Risk Register and Board Assurance Framework.
CQC Updates contained within the report.
Patient Safety Levels of Assurance agreed within the Joint Quality and Safety Committee
Patient Engagement Priority agenda item at Joint Quality and Safety Committee
Financial Aligned to CCG financial recovery plan.
Sustainability
Workforce / Training Details contained within the report relating to Providers by exception.
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed? x
2. Has an Equality Impact Assessment been completed? x
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
x
Recommendations / Action Required:
The Governing Bodies is asked to be:
Assured that where full assurance cannot be offered at this time that the Staffordshire
CCGs Professional Quality Team under the leadership of the Director of Nursing & Quality
have appropriately identified key areas of risk and are taking the correct steps with
Providers and other Lead Commissioners to ensure that our local population continues to
have access to high quality and safe care
Assured that the Director of Nursing & Quality has acted appropriately to address any
immediate quality and safety concerns included within the exception reports.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1 Director of Nursing & Quality
4th September 2018 Governing Body Report
Quality and Safety Assurance Report – July/August 2018
LEAD COMMISSIONER REPORTING:
1.0 University Hospitals of North Midlands NHS Trust
ACUTE - 1500 beds across 2 sites Acute/major Trauma Centre
Joint Quality and Safety Committee Levels of Assurance
Month Quality Safety
July 2018 6 (Partial Assurance) 6 (Partial Assurance)
August 2018 NA – no committee meeting NA – no committee meeting
LEAD- Stoke-on Trent & North Staffordshire Clinical Commissioning
Group UHNM
Target Trend Mar Apr May
CQC Rating N/A N/A Requires Improvement (Caring domain- Outstanding)
Safety
Never Events 0 2 0 0
Serious Incidents Reported 0 23 21 19
Falls with harm per 1000 bed days 0 0.09 0.18 0.21
Pressure Ulcers avoidable 0 10 7 4
Avoidable C’DIff 0 = 0 0 0
MRSA 0 = 0 0 0
Safety-Thermometer Harm free care – NEW HARM (%)
0 = 97.8% 96.7% 96.87%
Patient Experience
EMSA Breaches No. Patients affected NA NA NA
F&F score – in patient % No target = 98% 98% 98%
F & F Number of responses = 3004 2209 3308
Effectiveness
12 hour Trolley Breaches (Validated) 0 61 2 0
104 day breaches 0 12 9 4
Hospital Standard Mortality Ratio (HSMR.) Year to Date (YTD)
National average > 100
102.8 (Apr17-Mar18)
1.1 Key Quality Issues / Concerns for the attention of the Governing Bodies related to the metrics:
1.1.2 12 hour Trolley Breaches – The 12 hour Quality Root Cause Analysis (RCA) backlog update – all RCAs have now been completed. 2017/18 breaches were 512 (1/4/17 - 31/3/18) 2018/19 breaches is 2 (April 2018) to date. This is a marked improvement.
Effectiveness Experience and Safety:
The outcomes of the Root Causes Analysis (RCA) and panel reviews identified that no patients had sustained any harm due to their long wait in the Emergency Department (ED), however there were a number of lessons learnt and actions taken:
Ensure Sepsis screen and pathway documentation is comprehensively completed.
To improve completion of the sepsis tool is being incorporated into ED documentation.
Ensure timely comfort rounds and comprehensive documentation.
Ensure incidents are recorded for all patients attending ED with existing skin damage.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2 Director of Nursing & Quality
4th September 2018 Governing Body Report
Current Actions in place:
The Trust has appointed a new ED Clinical Lead and a change in Directorate Manager from June 2018.
The Risk Review action plan will be monitored monthly by the Accident and Emergency Delivery Board. UHNM CQRM will receive the action plan each month along with any escalations.
A follow up Joint Quality Visit (CCG’s/NHSE/NHSI) is being arranged.
A safety check list has been introduced into the ED; this specifies 2 hour comfort checks and an hourly check of O2 cylinders.
A further 12 hour breach review panel is scheduled for the 21st August 2018, to review those patients who sadly passed away whist in the Emergency Department.
Over the last 3 months there has been a decline in 12 hour trolley breaches.
1.1.3 104 day breaches- The 104 day breaches change on a weekly basis the data cited in the above table are the number of patients waiting as of the week ending the 17th August 2018 across all 6 CCG’s.
Current Actions in place: The RCA process for 104 day breaches are led by the clinical and operational teams in conjunction with the cancer pathway co-ordinators. This is an intensive process (acknowledged as good practice by the West Midlands Cancer Group).
Once the RCA is completed a clinical governance panel is held to review all the 104 day patients. A 104 day wait report was received at July 2018 Clinical Quality Review Meeting, the report stated that no patients had been identified as coming to harm.
The Trust has embarked on a communications campaign to encourage patients to attend cancer appointments. Data shows that up to a third of appointments are lost due to patients either cancelling or not accepting appointments for their care due to social factors such as holidays etc. The BBC reported the situation in June 2018 on the local televised news and website. Further communications under the title ‘Cancer doesn’t take a holiday’ are being developed for widespread use in the Trust and other care providers.
1.1.4 Hospital Standardised Mortality Ratios (HSMR): Latest HSMR (April 2017-March 2018) is reported at 102.54 and Summary Hospital Mortality Indicator (SHMI) (October 2016-September 2017) is reported at 1.04 (band 2) are within the expected ranges.
Mortality Outlier Alerts – At July CQRM UHNM gave an update on the Dr. Foster/ Imperial College Mortality Outlier Alerts received for: Excision of colon and or rectum (received 31/10/17), Therapeutic operations on jejunum and ileum (received 16/1/18). There were no systemic issues identified from the review of these deaths. The Trust has submitted the review to the CQC and is awaiting a response.
1.1.5 Serious Incidents (SI’s): During May there were 19 SI’s reported, of these 9 were pressure ulcers and 9 were falls. The rate of SIs per 1000 bed days has an average rate at 0.41 SIs per 1000 bed days since Bradwell Hospital was reopened in December 2017. The Quarter One 2018/19 rate is 0.42, which is higher than the previous quarter rate of 0.38, but similar to the Quarter One rate of 2017/18 of 0.41. The rates have varied with the exception of February 2018, which had a lower reporting rate, the variation has always been within the control limits.
1.1.6 Falls: The total falls increased slightly during May 2018 compared to the previous month and the rate per 1000 bed days has also increased. When reviewing the data for all individual sites there have been increases across the Royal Stoke University Hospital and County Hospital. The target rate of 5.6 falls per 1000 bed days continues to be achieved across UHNM with 5.51 YTD, although May 2018 recorded at 5.87. Falls Bundle compliance remains above the 90% target at RSUH but County was at 85.6%. UHNM overall was at 91.9% All the SIs that are reported have a full RCA undertaken and are reviewed at either specialist forums such as Tissue Viability, Falls Steering Group, Safe Medications or at the Trust’s Risk Management Panel. The RCA’s are then reviewed by the CCG Quality team.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3 Director of Nursing & Quality
4th September 2018 Governing Body Report
1.1.7 Avoidable Pressure ulcers: The Trust is currently under trajectory for avoidable pressure ulcers.
Current actions in place: The Corporate Nursing Team is working collaboratively with the Tissue Viability Team to support the top 5 reporting areas on a monthly basis with required improvements. On-going awareness campaigns include the following: Incontinence Associated Dermatitis Pathway Launch February/March 2018, the re-launch of Continence Link Nurse Training and a planned Stop the Pressure Week scheduled for October 2018. These are to be carried out as part of the UHNM commitment to the national Sign up to Safety Campaign.
1.2 Key Quality Issues/Concerns for the attention of the Governing Bodies not captured in the metrics:
1.2.1 Coroners Regulation 28: The Trust has received a Regulation 28 sent by the Coroner on the 29th
May 2018, following the death of a lady post discharge. The cause of death was determined as being from
natural causes exacerbated by an unexpected reaction to opiate medication, which had previously been
tolerated. Although the Trust did not prescribe this medication as it occurred in the Community, the Trust
have been requested to formulate an action plan to ensure that discharge letters have the appropriate
information on regarding medication and any changes made.
1.2.2 NHS Constitutional Standards Referral to treatment Time (RTT) & 52 week- The performance in
May 2018 was 74.98%. The number of confirmed patients over 52 weeks is 78. The majority of these
patients are General Surgery (Upper GI, Colorectal), Urology and Spinal Surgery.
Effectiveness Experience and Safety:
52 week Breach Review Panels are now well established with representation from CCG Quality team and
reports provided at Clinical Quality Review Meetings. Whilst to date no harm has been identified by the
breach panel, all parties acknowledge that this is a poor patient experience. The most recent panel was held
on the 24th May 2018, 36 RCAs were reviewed and no harm was identified as a result of the breach.
Current Actions in place:
The Medical Director has recently written out to all Consultants regarding the amount of overdue follow up
appointments, requesting that each Consultant reviews their waiting list to ensure the following:
All patients waiting are genuine
That there is no clinical risk to these patients
Plans to address the backlog
Following the May 2018 CQRM a follow-up overdue appointments paper detailing actions by specialty was
shared with members.
The Trust has appointed a RTT Recovery Manager to work with the Planned Care lead to implement the
RTT recovery. The Trust has also put in place sustainable solutions for training and validation, as well as
Patient tracking list (PLT) management.
Quality and Safety Assurance Report: July 2018

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4 Director of Nursing & Quality
4th September 2018 Governing Body Report
LEAD COMMISSIONER REPORTING:
3.1 Burton 2.0 Midlands Partnership Foundation Trust (Previously South Staffordshire and Shropshire NHS Foundation Trust and Staffordshire & Stoke-on-Trent Partnership Trust)
Community/Physical Health Services – Community Services Focus
Joint Quality and Safety Committee Levels of Assurance
Month Quality Safety
July 2018 8 (Full Assurance) 8 (Full Assurance)
LEAD Pan Staffordshire CCGs
MPFT
Target Trend March April May
CQC Rating N/A N/A Good Good Good
Safety
Never Events 0 = 0 0 0
Serious Incidents Reported 0 = 2 1 1
Falls with harm = 16 10 7
Pressure Ulcers - Avoidable 0 = 2 1 1
Avoidable C’DIff 0 = 0 0 0
MRSA 0 = 0 0 0
Safety-Thermometer Harm free care - ALL (%) 0 = 90.1% 89.0% 90.2%
Safety-Thermometer Harm free care – NEW HARM (%)
0 = 96.6% 96.7% 97.0%
Patient Experience
EMSA Breaches No. Patients affected 0 = 0 0 0
F&F score – in patient % N/A = 97.0 97.0 98.0
F & F Number of responses N/A = 2642 2369 2390
2.1 Key Quality Issues / Concerns for the attention of the Governing Bodies related to the metrics:
2.1.1 Falls: There was 1 incident of a fall in May 2018 that caused moderate harm. This was reported by
Homefirst Stoke and was in regard to patient who had an unwitnessed fall prior to the visit. No other falls
categorised as Moderate Harm or above were recorded for Community or Hospital Services Pan
Staffordshire.
Current actions in place:
Falls are reviewed at the Trusts Falls Review Group which the Clinical Quality Improvement Manger
attends.
2.1.2 Pressure Ulcers: There have been 6 Grade 4 Pressure Ulcers (3 April and 3 May 2018) identified for
South Staffordshire Community Patients. These will be reviewed and if unavoidable will be investigated
under the Serious Incident framework, There is no commonality across the areas. There have been
increases in Grade 3 pressure ulcers in Community Hospitals, Lichfield, Cannock and Stafford areas.
Current Actions in place:
Avoidability will be reviewed by the Trust and reported through their Pressure Ulcer Review Group
(PURG).

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
5 Director of Nursing & Quality
4th September 2018 Governing Body Report
2.1.3 Incidents: During April and May 2018 there was an increase in reported incidents across the Trust. An
increase in reported incidents is not always an area for concern – often this is an indicator of a positive
reporting culture. The category of incidents showing an increase was acquired pressure ulcers. This will be
discussed at the Trusts next Pressure Ulcer Steering Group (PUSG). Community Hospitals record that Slips,
Trips and Falls are the largest number of incidents reported (46.9%). Other Incident Themes to note were:
Community Services have reported 2 Deaths which have been referred to the Mortality review group & an
overdose of an oral opiate which is being investigated by the Trust Adult Safeguarding team. Community
Hospital reported that during May 2018 there was a VTE event reported at Jackfield Ward. Appropriate
chemical thromboprophylaxis was in place and action was taken to commence treatment therapy once
health deterioration was noted.
2.1.4 Serious Incidents: There was one Pressure Ulcer that met the SI criteria for April and also 1 in May
2018 (2 in total). The Investigation will be submitted to the CCG for review and sign off as per the SI
process.
2.1.5 Friends and Family Test (FFT): The average FFT score from June 2017 to May 2018 is 99% for the
North Division, 99% for the Community Hospitals and 98% for the South Division and these continue to
exceed the national target of 90%.
2.2 Key Quality Issues / Concerns for the attention of the Governing Bodies not captured in the metrics:
2.2.1 The inaugural MPFT Clinical Quality Review Meeting took place on the 2nd August 2018. Members from the CCG and MPFT Quality Teams met to align reporting from the residual SSOTP/SSSFT contracts, to ensure that a meaningful discussion takes place to monitor and promote the quality agenda. MPFT will be reporting national metrics as one trust from the 1st August 2018 and quarterly reports will be aligned through governance process from October 2018 (Quarter 3). 2.2.2 Care Quality Commission (CQC) Inspection Update – As part of the due diligence ahead of the acquisition the CQC re-inspected the two service areas where warning notices had been issued in 2016 on the 18th & 19th April 2018; Community Health Services for Adults and End of Life Care. The reports were published by the CQC on 2nd July 2018 and both service areas achieved a rating of ‘Good’ in every domain. The full reports are in the process of being received at Community Nursing Assurance Group, Clinical Quality Review Meeting and Quality Committee.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
6 Director of Nursing & Quality
4th September 2018 Governing Body Report
Quality and Safety Assurance Report July 2018
LEAD COMMISSIONER REPORTING:
3.1 Burton 3.0 North Staffordshire Combined Health Care Trust [NSCHT]
N/A
Joint Quality Committee Levels of Assurance
Month Quality Safety
July 2018 Partial Assurance Partial Assurance
LEAD North Staffordshire Combined Health Care Trust [NSCHT]
Target Trend April May June
CQC Rating N/A N/A Good Good Good
Safety
Never Events 0 = 0 0 0
Serious Incidents Reported 0 9 12 7
Falls serious incident 0 1 1
Pressure Ulcers avoidable 0 0 0 0
Avoidable C’DIff 0 = 0 0 0
MRSA 0 = 0 0 0
Patient Experience
EMSA Breaches No. Patients affected 0 0 0
F&F score – in patient % No target N/A 95% 96%
F & F Number of responses 95% 96%
3.1 Key Quality Issues / Concerns for the attention of the Governing Bodies related to the metrics:
3.1.1: Serious Incidents: The Serious Incident (SI) category shows the largest increase of deaths reported under the category ‘pending review’ refer to the deaths of people known to substance misuse services. The initial change in commissioning arrangements for Drugs and Alcohol Services meant that SI’s detailed within One Recovery Services were being recorded under NSCHT and the addition of Stoke Community Drug and Alcohol Services (CDAS) has made an impact on the number of SIs reported from substance misuse services.
The reporting period shows an increase of SIs with the category showing the largest increase as ‘Pending review’, which is used when the situation around the death does not immediately give rise to a rational suspicion of death by suicide. The majority of deaths reported under this category refer to the deaths of people known to substance misuse services.
The Adult Community directorate reported the largest number of SI’s. The investigations in these cases evidenced substance misuse tended to result in unpredictable and chaotic behaviours, including self-harm. The North Staffordshire Combined Health Care Trust [NSCHT] Trust began delivering community substance misuse services in Stoke-on-Trent in June 2017 following the commissioning of Stoke Community Drug and Alcohol Services (CDAS). The number of deaths reported for people known to One Recovery Services remains largely unchanged, although there have been significant changes to service delivery due to budget cuts in 2017/18, the full impact of these changes is not yet fully known.
The category of apparent/actual abuse was used by the Trust for the first time in 2017/18, when 5 incidents were reported under this category. Four incidents were reported following the identification of errors in

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
7 Director of Nursing & Quality
4th September 2018 Governing Body Report
Mental Health Assessment documentation which resulted in unlawful detention and one incident of a service user physically assaulting staff was also reported.
3.1.2: Falls: The majority of categorised minor falls were reported from the Neuro Old Age Psychiatry [NOAP] wards. In order to reduce/prevent falls resulting in harm a number of actions were taken across the Trust. These actions included the establishment of a falls rapid improvement task group, which reviewed the trust falls policy and developed a multi-factorial risk assessment which was later incorporated into the risk assessments available on Lorenzo. Also, working in collaboration with the Advancing Quality Alliance (AQuA), the Trust aimed to reduce the number of falls in the Neuro Old Age Psychiatry NOAP inpatient areas by initiating locally developed falls reduction projects
The Commissioning Strategic Services Improvement Group for Child Adolescent Mental Health Services (CAMHS) continues to meet monthly and is closely monitoring the 18 week waiting initiatives.
3.2 Key Quality Issues/Concerns for the attention of the Governing Bodies not captured in the metrics:
Current Actions in place: Over the last two years, the Trust has made incredible progress in ensuring children and young people are seen in a timely manner for an initial assessment, they receive a good quality risk assessment and care plan. However unfortunately waiting times for CAMHS have started to increase slightly month on month for the last three months which is being closely monitored via the Contract Review Board.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
8 Director of Nursing & Quality
4th September 2018 Governing Body Report
Quality and Safety Assurance Report July 2018
LEAD COMMISSIONER REPORTING:
3.1 Burton 4.0 EZEC
Non Urgent Patient Transport
Joint Quality and Safety Committee Levels of Assurance
Month Quality Safety
July 2018 6 (Partial Assurance) 5 (Partial Assurance)
LEAD
Pan Staffordshire CCGs EZEC
Target Trend Feb Mar Apr
CQC Rating N/A N/A
Safety
Never Events 0 = 0 0 0
Serious Incidents Reported 0 0 1 0
Patient Experience
F & F - Score (% Would Recommend) No target = 100% 100% 100%
4.1 Key Quality Issues / Concerns for the attention of the Governing Bodies related to the metrics:
4.1.1 Serious Incidents: No serious incidents have been reported by E-zec for April 2018. RCAs for two previous SI’s relating to patient injuries have been closed through the CCG SI closure process and necessary recommendations made. 4.1.2 Patient Experience: During April 2018 the number of patient experience surveys completed demonstrated that 100% of patients were likely to recommend the service to friends and family. This is based on a small sample of 60 responses which is less than 1% of the total journeys for the month. The provider is regularly reminded that the data is not statistically valid to give a full overview of the service. E-zec had advised that they were pursuing alternative options but advise that this is pending due to staff capacity. In view of the same number of responses being issued for April 2018 this will be discussed further at the Contract Review Board.
4.2 Key Quality Issues / Concerns for the attention of the Governing Bodies not captured in the metrics:
4.2.1 Significant delays in service provision Concerns have been escalated from UHNM leads to the CCG relating to the excessive waits that patients are experiencing. Actions taken An escalation call was undertaken on 27th June 2018 between CCG contract and commissioner leads and E-zec to discuss the significant delays in the service provision. Subsequent to this the CCG Director of Commissioning and Operations has spoken with E-zec’s Director of Operations and requested an immediate action plan to address workforce, their allocation of resources and plans to reduce aborts and cancellations

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
9 Director of Nursing & Quality
4th September 2018 Governing Body Report
which would increase capacity. CCG leads have considered that in view of a number of these issues a joint protocol and joint working between E-zec and UHNM will be explored. This will be discussed in a further multidisciplinary meeting.
Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
10 Director of Nursing & Quality
4th September 2018 Governing Body Report
5.0 Quality Directorate Report – 12th July 2018 This section of the report provided by the Director of Nursing and Quality is to briefly share with the Governing Bodies the additional work being undertaken by the team locally, as well as informing on any initiatives affecting the CCG locally, regionally and nationally. The quality team works to continue to ensure the consistent provision of safe, effective, person-centred outcomes for patients across Staffordshire. 5.1 Joint Quality and Safety Committee (JQC) for the 12th July 2018 This meeting was the pilot for a single meeting for the JQC for; Cannock Chase CCG, East Staffordshire CCG, North Staffordshire CCG, South East Staffordshire and Seisdon Peninsula CCG, Stafford and Surrounds CCG and Stoke-on-Trent CCG Lay members, GPs, Directors and the quality team members from the North and South of the County came together. The Director of Nursing and Quality has produced a proposal which has been shared with the whole committee and feedback is currently being collated. Terms of reference for the new Joint Quality and Safety Committee are currently being finalised and will be presented to the next meeting on 13th September. Once these are approved they will be submitted to all Governing Body meetings for final ratification. The terms of reference have been amended to incorporate key feedback from the pilot meeting in July and will be subject to early review as the new committee evolves. This section includes a summary of other reports received by the JQC not pertaining to the Providers and is intended to provide further assurance (not detail) to members of the Governing Body in relation to key quality activity. 5.2 Items Approved at Joint Quality and Safety Committee for Ratification There were no items for approval by the Committee in July 2018. 5.3 Escalation to Governing Bodies ‘In Common’ from the Joint Quality and Safety Committee in July 2018. There were no items to escalate to the Governing Bodies from the Joint Quality and Safety Committee in July 2018.
5.4 Patient Engagement Report The Joint Quality and Safety Committee received briefings regarding key patient engagement activity including a summary of patient stories highlighted at the Patient District Groups. Members were assured that the information and any soft intelligence highlighted had previously been escalated to the quality team and action was underway to address this in line with normal processes. 5.5 UHNM Risk Review Action Plan The UHNM Risk Review Action Plan was presented to the Joint Quality and Safety Committee to provide assurance on the current developments regarding the A&E department. This was developed following a multiagency visit to UHNM January 2018.
Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
11 Director of Nursing & Quality
4th September 2018 Governing Body Report
Actions relating to the UHNM Risk Review have been incorporated into the Sustainability and Transformation Partnership Urgent and Emergency Care (STP UEC) operational plan, which is reported at A&E Delivery Board. The actions from the Risk Review have now been allocated to one of the seven work streams that sit under the STP UEC Programme. The (STP UEC) operational plan will provide a stand-alone update to the Joint Quality and Safety Committee on the specific actions from that review for assurance. Detailed plans for each STP Urgent and Emergency Care work stream and allocation of leads for specific actions are being finalised. 5.6 Clinical Risk Register The 3 current risk registers were received and reviewed by the Joint Quality and Safety Committee with information and assurance regarding the most significant quality risks currently facing the 6 Staffordshire CCGs. The Quality Team is working with the Governance Team to bring together and align the quality risks across the 6 CCGs. 5.7 Primary Care The Primary Care Report was presented and reviewed with a quarterly report in regard to primary care quality. The key Points included:
CQC Inspection ratings.
Primary Care quality quarterly review meeting outcome.
Upheld complaints.
Friends and Family test (FFT).
Learning and education including PLT and Peer reviews.
Quality visit programme for 2018/19.
Five GP practices (1 North Staffordshire and 4 Stoke-on-Trent) received a ‘Requires Improvement’ rating for the safety domain from their CQC inspection. The Joint Quality and Safety Committee received assurances regarding the actions being taken by the practices to improve their rating and the support given by the CCG primary care team. 5.8 GP 60 Second Reporting This is a section of the agenda used to enable GPs to share member concerns in respect of any emerging issues. This has proved to be an innovative method of highlighting such trends and will be continued in the new committee.
Feedback relating to discharge processes including letters will feed into the
dedicated discharge work stream and individual organisations.
The UHNM Access Policy 2015 was raised as patients who DNA the first time are
discharged back to their GP in line with the trust policy, with the exception of
vulnerable adults, obstetric patients, paediatrics. The Head of Quality and Safety
will be investigating this.
Differences in commissioning for paediatric phlebotomy between County Hospital
and the Royal Stoke University Hospital were highlighted; this will be raised with
the commissioners.

Cannock Chase Clinical Commissioning Group East Staffordshire Clinical Commissioning Group North Staffordshire Clinical Commissioning Group South East Staffordshire & Seisdon Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
12 Director of Nursing & Quality
4th September 2018 Governing Body Report
5.9 Serious Incident Report The regular monthly Serious Incident report was received by the Committee to appraise the committee of serious incidents occurring in local main providers along with independent providers. The report outlines immediate actions taken to ensure patient /staff safety, and to provide assurances to the Committee that all appropriate actions are being undertaken. 5.10 Quality Impact Assessment Sub-Group Summary Report The paper was received by the Committee with the purpose of updating members on the Quality Impact Assessments (QIAs) that have been submitted to Sub-Group for Review and the outcomes presented. In total there were 6 QIAs considered at the North QIA Panel in May/June 2018 of which the following outcomes were achieved:
Approved (with no recommendations or conditions) = 1
Approved with recommendations = 4
Approved with conditions = 1
Rejection – not approved = 0
The quality teams have worked closely with the QIPP PMO to ensure that all QIPP schemes have a completed QIA at the earliest opportunity and that it is presented to the panel for scrutiny and a decision on the outcome. The quality team has organised extra panels in order to assist the QIPP PMO to ensure that all QIPP schemes have a QIA that has been reviewed by the panel. Work is currently underway to integrate the North and South QIA process and sub- groups into a single sub-group with lay member representation from the North and South. A proposal paper is currently being developed and will be presented to the Director of Nursing and Quality prior to being finalised. 5.11 Patient Engagement Written and verbal reports were received by the Committee from all of the 6 CCGS describing the engagement and meetings held across the area. All patient stories/accounts are logged onto the soft intelligence system. 5.12 Quality Accounts The Committee has received Quality Accounts from the main providers, which are signed off by the Committee and Director of Nursing and Quality prior to insertion of CCG supporting statements by providers into their published quality accounts. 5.13 Research Update A Research paper was presented to the Committee describing the research projects currently being undertaken. A draft Strategy for the future of research in Staffordshire was shared with the Committee. The strategy presented proposed that a new Directorate of Research, Development and Innovation be created within the CCG. This would establish a separate formal governance structure for research within the CCG and is a change to existing arrangements as historically research has been under the Nursing and Quality directorate.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent
Clinical Commissioning Groups’ Governing Bodies
Enclosure: 8.1
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Month 4 Financial Position
Meeting Date: Tuesday 4th
September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Alistair Mulvey, CFO David Skelton, Financial Controller
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
Action Required (select):
Decision Discussion For Assurance / For Information
Purpose of the Paper (Key Points + Executive Summary):
This paper provides a summary of the CCGs financial performance as at the end of July 2018 (Month 4).
At month 4 the year to date position for both CCGs combined is a £17.12m adverse variance against plan, with an £14.92m in-year actual deficit reported (North Staffs £8.37m deficit, Stoke on Trent £6.55m deficit). This compares to a planned position at month 4 of a £2.20m surplus (North Staffs £0.27m surplus, Stoke on Trent £1.93m surplus).
Plan to Month 4
Actual to Month 4
Variance to Month 4
Full Year Plan
Full Year Forecast
Full Year Variance
CCG
£'000 £'000 £'000 £'000 £'000 £'000
North Staffordshire
268 -8,369 -8,637 800 800 0
Stoke on Trent
1,933 -6,547 -8,480 5,800 5,800 0
Total 2,201 -14,916 -17,117 6,600 6,600 0
Surplus/(Deficit)
Within the overall financial position the following key points should be noted:
The QIPP plan totals £35.82m (North Staffs £14.32m, Stoke on Trent £21.50m). As at Month 4 there is slippage in the QIPP programme of £2.45m (North Staffs £0.25m, Stoke on Trent £2.2m) against planned levels which is expected to be recovered and so the CCGs are forecasting full delivery of the programme.
The CCG’s have seen adverse movements to plan at month 4, the largest movements were reported in UHNM and Nuffield North Staffs although it should be noted that this is based on a small sample size of data.
The CCG’s are reporting net financial risk at month 4 of £25.8m (Stoke on Trent CCG £10.3m, North Staffs CCG £15.5m). This is due to gross risk of £6.1m attached to the QIPP programme, £22.9m credit forecast adjustment which is required in order to forecast a breakeven position against the plan and

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
emerging risks relating to Bradwell, prior year UHNM and winter totalling £7.6m, this is partially mitigated by the release of the £3.49m contingency and £7.2m UHNM fines and penalties.
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
The CCGs have a planned QIPP programme of £35.82m (North Staffs £14.32m, Stoke on Trent £21.50m). Of this an element of risk is attached to delivery, at month 4 this is reported as £6.1m (North Staffs £2.36m, Stoke on Trent £3.74m)
Additional risk includes a £22.9m credit forecast adjustment which is required in order to forecast a breakeven position against the plan and emerging risks relating to Bradwell, prior year UHNM and winter totalling £7.6m, this is partially mitigated by the release of the £3.49m contingency and £7.2m UHNM fines and penalties
Residual Net Risk of £25.8m is reported at month 4
Implications:
Legal and/or Risk
CQC
Patient Safety
Patient Engagement
Financial
Sustainability
Workforce / Training
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
Recommendations / Action Required:
The Governing Body is asked to note:-
I. The contents of this report and executive summary regarding the combined CCG performance
against 2018-19 financial duties to the end of Month 4; II. The key drivers of risk that have impacted upon the financial position;
III. The mitigations identified to reduce the level of net risk to £25.788m. IV. The performance against the other financial metrics

1
Month 4 Financial Position 2018/19
1. Background North Staffordshire CCG & Stoke on Trent CCG report achievement against their key financial duties and plans both monthly and annually. This report discusses the position to the end of July 2018 (Month 4) and the forecast for the remainder of the financial year 2018/19.
2. Executive Summary At month 4 the year to date position for both CCGs combined is a £17.12m adverse variance against plan, with an £14.92m in-year actual deficit reported (North Staffs £8.37m deficit, Stoke on Trent £6.55m deficit). This compares to a planned position at month 4 of a £2.20m surplus (North Staffs £0.27m surplus, Stoke on Trent £1.93m surplus).
The high level dashboard below provides performance detail against each key metric. This report further outlines the key drivers of the adverse financial performance, areas of mitigation and a summary of the year end position.
Plan to
Month 4
Actual to
Month 4
Variance to
Month 4
Full Year
Plan
Full Year
Forecast
Full Year
Variance
CCG £'000 £'000 £'000 £'000 £'000 £'000
North Staffordshire 268 -8,369 -8,637 800 800 0
Stoke on Trent 1,933 -6,547 -8,480 5,800 5,800 0
Total 2,201 -14,916 -17,117 6,600 6,600 0
Surplus/(Deficit)
North Staffordshire CCG
High Level Targets & RAG Rating
Total Revenue Allocation notified -£316.11m
Programme Allocation notified -£311.49m
Running Cost Allocation notified -£4.62m
Capital Allocation notified - Nil
G
G
G
A
Stoke-on-Trent CCG
High Level Targets & RAG Rating
Total Revenue Allocation notified - £442.94m
Programme Allocation notified - £436.97m
Running Cost Allocation notified - £5.97m
Capital Allocation notified - Nil
G
G
G
A
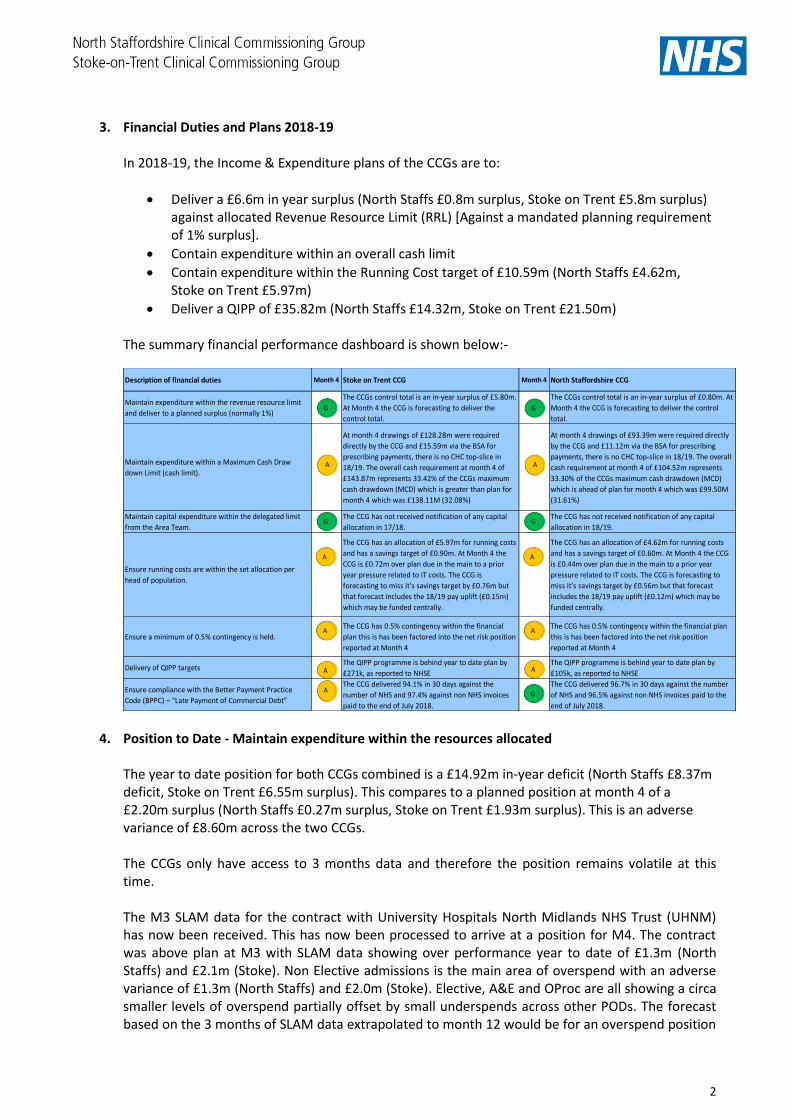
2
3. Financial Duties and Plans 2018-19
In 2018-19, the Income & Expenditure plans of the CCGs are to:
Deliver a £6.6m in year surplus (North Staffs £0.8m surplus, Stoke on Trent £5.8m surplus) against allocated Revenue Resource Limit (RRL) [Against a mandated planning requirement of 1% surplus].
Contain expenditure within an overall cash limit
Contain expenditure within the Running Cost target of £10.59m (North Staffs £4.62m, Stoke on Trent £5.97m)
Deliver a QIPP of £35.82m (North Staffs £14.32m, Stoke on Trent £21.50m)
The summary financial performance dashboard is shown below:-
4. Position to Date - Maintain expenditure within the resources allocated The year to date position for both CCGs combined is a £14.92m in-year deficit (North Staffs £8.37m deficit, Stoke on Trent £6.55m surplus). This compares to a planned position at month 4 of a £2.20m surplus (North Staffs £0.27m surplus, Stoke on Trent £1.93m surplus). This is an adverse variance of £8.60m across the two CCGs.
The CCGs only have access to 3 months data and therefore the position remains volatile at this time.
The M3 SLAM data for the contract with University Hospitals North Midlands NHS Trust (UHNM) has now been received. This has now been processed to arrive at a position for M4. The contract was above plan at M3 with SLAM data showing over performance year to date of £1.3m (North Staffs) and £2.1m (Stoke). Non Elective admissions is the main area of overspend with an adverse variance of £1.3m (North Staffs) and £2.0m (Stoke). Elective, A&E and OProc are all showing a circa smaller levels of overspend partially offset by small underspends across other PODs. The forecast based on the 3 months of SLAM data extrapolated to month 12 would be for an overspend position
Description of financial duties Month 4 Stoke on Trent CCG Month 4 North Staffordshire CCG
Maintain expenditure within the revenue resource limit
and deliver to a planned surplus (normally 1%)
The CCGs control total is an in-year surplus of £5.80m.
At Month 4 the CCG is forecasting to deliver the
control total.
The CCGs control total is an in-year surplus of £0.80m. At
Month 4 the CCG is forecasting to deliver the control
total.
Maintain expenditure within a Maximum Cash Draw
down Limit (cash limit).
At month 4 drawings of £128.28m were required
directly by the CCG and £15.59m via the BSA for
prescribing payments, there is no CHC top-slice in
18/19. The overall cash requirement at month 4 of
£143.87m represents 33.42% of the CCGs maximum
cash drawdown (MCD) which is greater than plan for
month 4 which was £138.11M (32.08%)
At month 4 drawings of £93.39m were required directly
by the CCG and £11.12m via the BSA for prescribing
payments, there is no CHC top-slice in 18/19. The overall
cash requirement at month 4 of £104.52m represents
33.30% of the CCGs maximum cash drawdown (MCD)
which is ahead of plan for month 4 which was £99.50M
(31.61%)
Maintain capital expenditure within the delegated limit
from the Area Team.
The CCG has not received notification of any capital
allocation in 17/18.
The CCG has not received notification of any capital
allocation in 18/19.
Ensure running costs are within the set allocation per
head of population.
The CCG has an allocation of £5.97m for running costs
and has a savings target of £0.90m. At Month 4 the
CCG is £0.72m over plan due in the main to a prior
year pressure related to IT costs. The CCG is
forecasting to miss it's savings target by £0.76m but
that forecast includes the 18/19 pay uplift (£0.15m)
which may be funded centrally.
The CCG has an allocation of £4.62m for running costs
and has a savings target of £0.60m. At Month 4 the CCG
is £0.44m over plan due in the main to a prior year
pressure related to IT costs. The CCG is forecasting to
miss it's savings target by £0.56m but that forecast
includes the 18/19 pay uplift (£0.12m) which may be
funded centrally.
Ensure a minimum of 0.5% contingency is held.
The CCG has 0.5% contingency within the financial
plan this is has been factored into the net risk position
reported at Month 4
The CCG has 0.5% contingency within the financial plan
this is has been factored into the net risk position
reported at Month 4
Delivery of QIPP targetsThe QIPP programme is behind year to date plan by
£271k, as reported to NHSE
The QIPP programme is behind year to date plan by
£105k, as reported to NHSE
Ensure compliance with the Better Payment Practice
Code (BPPC) – “Late Payment of Commercial Debt”
The CCG delivered 94.1% in 30 days against the
number of NHS and 97.4% against non NHS invoices
paid to the end of July 2018.
The CCG delivered 96.7% in 30 days against the number
of NHS and 96.5% against non NHS invoices paid to the
end of July 2018.
A
A
G
A
A
G
A
A
G
G
A
A
G
A
3
of £6.1m (North Staffs) and £8.5m (Stoke), however, it is assumed that QIPP delivery and contract challenges will mitigate this. The CCGs have investigated the high levels of emergency activity, and, in line with contract timescales, contested payment challenges have been raised for month 1 relating to increased zero length of stay admissions and increased costs of general medicines and geriatric admissions (at the time of writing, the month 2 contested payments deadline has not yet passed). In addition to the contested payment challenges, a formal activity query notice and a counting and coding challenge has been raised to UHNM in line with contractual mechanisms. Furthermore, a clinical visit of urgent care by the CCGs’ Medical Director, Dr Steve Fawcett, was undertaken in early August. The Midlands Partnership Foundation Trust (Community) data for month 3 is showing an overspend of £744k (North Staffs) and an underspend of £388k (Stoke) which have been extrapolated in the forecast to an adverse variance of £2.9m in North Staffs and a favourable variance of £1.5m in Stoke. However, it should be noted that the contract with this provider for North Staffs and Stoke CCGs is currently showing an incorrect split between the 2 CCGs, therefore the large overspend against the North Staffs contract value is partially mitigated by an underspend of £1.5m in Stoke CCG, resulting in an overall £1.5m pressure across the 2 CCGs. Data quality issues and a number of challenges are currently being discussed with the provider.
The West Midlands Ambulance Trust data for month 3 is showing an overspend of £37k (North Staffs) which has been extrapolated in the forecast to an adverse variance of £154k. This is a similar theme across the Staffordshire patch and is being reviewed by contract management colleagues. The contract with Stoke CCG is in line with plan. Other material year to date variances from plan based on the limited 3 months’ worth of data include over performance at Derby Teaching Hospitals NHS FT (£132k North Staffs), Nuffield North Staffs (£125k North Staffs and £289k Stoke) and Mid Cheshire (£94k North Staffs and £50k Stoke). Prescribing has an over spend of £0.5m in each CCG relating to the brought forward impact of the final month 12 PMD position being higher than the year end accrual. PMD data for month 2 is now available and the QIPP delivery for month 2 has been used as a proxy for month 3 and 4 to estimate the YTD position.
Continuing Care information has now been received for expenditure up to July. The M4 position is an overall under spend of circa £1m across the 2 CCGs. This is partially driven by the phasing of the budget which included an assumption that QIPP delivery would be later in the year, but the schemes have started to deliver from April. The forecast position on CHC is breakeven with an assumption of full QIPP delivery and a deep dive is taking place into the CHC financial information in order to validate the year to date position. On the 1st April 2017 the CCG was granted authority for the delegated commissioning of Primary Care, in 2018/19 the allocation is £28.68m. The year to date performance is outlined below, the CCG is reporting a £130k (North Staffs) and £51k (Stoke) under spend positions year to date and is currently forecasting to plan:
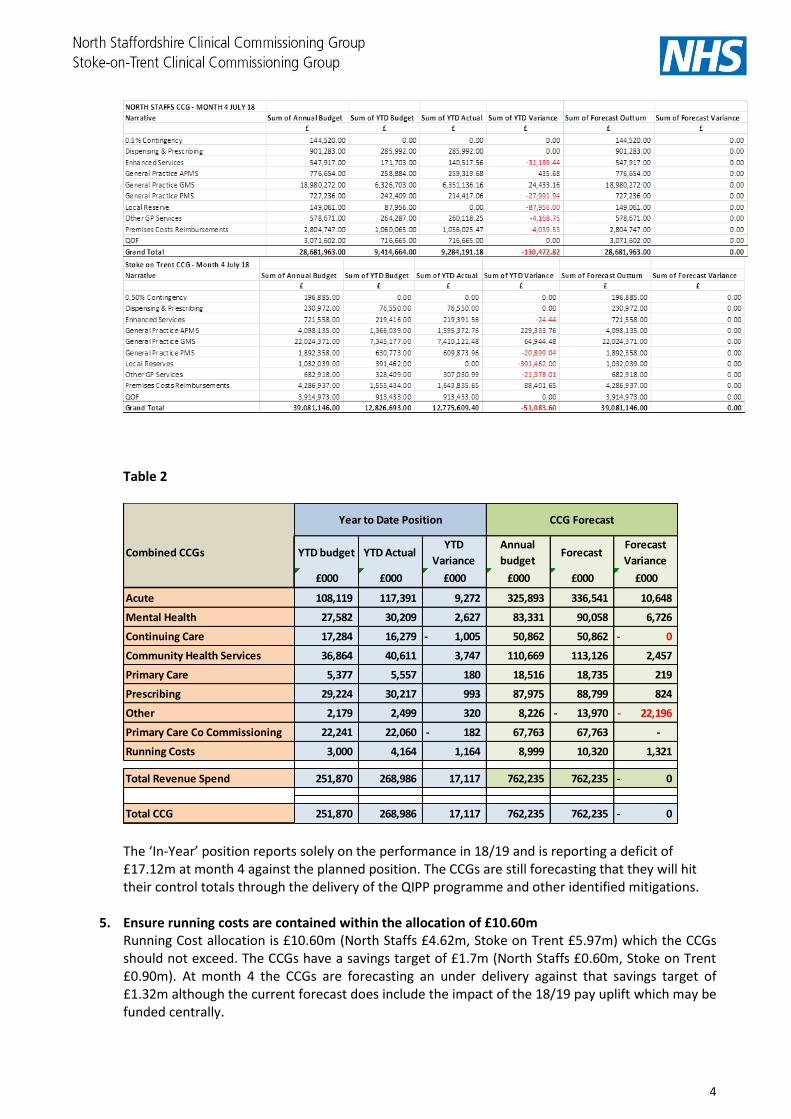
4
Table 2
The ‘In-Year’ position reports solely on the performance in 18/19 and is reporting a deficit of £17.12m at month 4 against the planned position. The CCGs are still forecasting that they will hit their control totals through the delivery of the QIPP programme and other identified mitigations.
5. Ensure running costs are contained within the allocation of £10.60m
Running Cost allocation is £10.60m (North Staffs £4.62m, Stoke on Trent £5.97m) which the CCGs should not exceed. The CCGs have a savings target of £1.7m (North Staffs £0.60m, Stoke on Trent £0.90m). At month 4 the CCGs are forecasting an under delivery against that savings target of £1.32m although the current forecast does include the impact of the 18/19 pay uplift which may be funded centrally.
Combined CCGs YTD budget YTD ActualYTD
Variance
Annual
budget Forecast
Forecast
Variance
£000 £000 £000 £000 £000 £000
Acute 108,119 117,391 9,272 325,893 336,541 10,648
Mental Health 27,582 30,209 2,627 83,331 90,058 6,726
Continuing Care 17,284 16,279 1,005- 50,862 50,862 0-
Community Health Services 36,864 40,611 3,747 110,669 113,126 2,457
Primary Care 5,377 5,557 180 18,516 18,735 219
Prescribing 29,224 30,217 993 87,975 88,799 824
Other 2,179 2,499 320 8,226 13,970- 22,196-
Primary Care Co Commissioning 22,241 22,060 182- 67,763 67,763 -
Running Costs 3,000 4,164 1,164 8,999 10,320 1,321
Total Revenue Spend 251,870 268,986 17,117 762,235 762,235 0-
Total CCG 251,870 268,986 17,117 762,235 762,235 0-
CCG Forecast Year to Date Position

5
6. Quality, Innovation, Productivity and Prevention (QIPP) At month 4 performance is £2m below target across the 6 Staffordshire CCGs, with a current forecast of £8.8m below target. However within this figure there remain some delivery risks as a number of QIPP schemes are scheduled to commence later in the financial year. Overall the estimated total non-delivery risk is £20.1m across the 6 CCGs. For North Staffs CCG this represents a year to date under delivery on the QIPP target of £105k and a forecast of £250k under delivery. Within this forecast there are a number of schemes yet to commence giving a total financial risk of £2.4 million against achieving the target of £14.3 million. Delivery against the Stoke target of £21.5 million is under by £271k year to date and forecast to be £2.2 million under. Similar to North Staffs there are a number of schemes yet to start giving a total financial risk of £3.7 million potential under delivery.
7. Cash Flow - Maintain expenditure within a maximum cash drawdown limit The CCGs had drawings to the end of July 2018 of £248.39m (North Staffs £104.52m, Stoke on Trent £99.50m) against its planned requirement of £281.98m (North Staffs £99.50m, Stoke on Trent £138.11m), for the same period, including the requirements notified from the Business Services Authority.
8. Ensure compliance with the Better Payment Practice Code (BPPC)
The CCGs are expected to comply with the Confederation of British Industry (CBI) Prompt Payment Code. This requires the CCGs to pay 95% of valid invoices within 30 days of receipt. North Staffs CCG performance up to 31st July stood at 96.7% based on count for NHS payables . For non NHS payables the position was 96.5% based on count. Stoke on Trent CCG performance up to 31st July stood at 94.1% based on count for NHS payables. For non NHS payables the position was 97.4% based on count. The CCGs met the target in terms of numbers of invoices for all areas except Stoke on Trent CCG in respect of NHS payables albeit performance improved in July itself.
9. Strategic Support Under the NHS planning guidance, the CCGs are required to set aside an uncommitted 0.5% contingency in their financial plans. For the North CCGs, this equates to £3.492m (£1.472m North Staffordshire CCG and £2.020m Stoke-on-Trent CCG. In addition, the CCGs are required to ensure that the CCGs invest a cumulative £3 per head of population non-recurrently in primary care over 17/18 to 18/19, in line with the Five Year Forward View.
10. Balance Sheet
The CCGs individual Statements of Financial Position as at 31st July 2018 (Appendix 2) shows the level of inter-indebtedness between the CCGs and other parties (mainly NHS providers). Significant entries include the value of Accounts Payable at £44.44m (North Staffs £18.08m, Stoke on Trent £26.36m) and Accounts Receivable £7.75m (North Staffs £2.08m, Stoke on Trent £5.67m).
11. Financial Risks
The CCG’s are reporting net financial risk at month 4 of £25.8m (Stoke on Trent CCG £10.3m, North Staffs CCG £15.5m). This is due to gross risk of £6.1m attached to the QIPP programme, £22.9m credit forecast adjustment which is required in order to forecast a breakeven position against the plan and emerging risks relating to Bradwell, prior year UHNM and winter totalling £7.6m, this is partially mitigated by the release of the £3.49m contingency and £7.2m UHNM fines and penalties. Risks will continue to be critically reviewed as more data becomes available through the financial year, in addition mitigations will be continually sought to provide further headroom where possible.
Recommendation: The Governing Body is asked to note:-

6
I. The contents of this report and executive summary regarding the combined CCG
performance against 2018-19 financial duties to the end of Month 4; II. The key drivers of risk that have impacted upon the financial position;
III. The mitigations identified to reduce the level of net risk to £23.8m. IV. The performance against the other financial metrics

7
Appendix 1
North Staffordshire & Stoke on Trent CCGs - Combined QIPP Delivery April to July 2018/19
Combined QIPP Delivery April to July – 2018/19

8
Appendix 2 North Staffs - Statement of Financial Position Stoke on Trent - Statement of Financial Position As at 30th June 2018 As at 30th June 2018
Statement of Financial Position £
Non-Current Assets 235,200
Cash 377,170
Accounts Receivable 2,077,245
Current Assets 2,454,415
TOTAL ASSETS 2,689,615
Accounts Payable 18,080,135
Accrued Liabilities 42,666
Current Liabilities 18,122,801
Long Term Liabilities -
Retained Earnings incl. In Year (15,433,186)
Total Taxpayers Equity (15,433,186)
TOTAL EQUITY + LIABILITIES 2,689,615
Statement of Financial Position £
Non-Current Assets 198,796
Cash (703,079)
Accounts Receivable 5,671,265
Current Assets 4,968,186
TOTAL ASSETS 5,166,982
Accounts Payable 26,364,607
Accrued Liabilities 64,000
Current Liabilities 26,428,606
Long Term Liabilities -
Retained Earnings incl. In Year (21,261,625)
Total Taxpayers Equity (21,261,625)
TOTAL EQUITY + LIABILITIES 5,166,982

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 8.2
Report to: North Staffordshire and Stoke-on-Trent CCGs Governing Body in Common
Title: Month 3, 2018/19 Performance Report
Meeting Date: 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Zara Jones N Naomi Bentley
Clinical Lead(s) Reviewer: Links to the STP Y/N (if Y, which programme):
N
Action Required (select):
Decision Discussion For Assurance / For Information x
Purpose of the Paper (Key Points + Executive Summary):
The purpose of the month 3 performance report is to provide a summary of performance and activity across North Staffordshire (NS) and Stoke-on-Trent (SOT) Clinical Commissioning Groups (CCG). NHS Constitution at Month 3 The following constitutional standards are not achieving at Month 3. Month 2 performance is shown in brackets as a comparison.
Accident and Emergency 4 hour wait has improved – 82.8% (83.8%).
18 weeks from referral to treatment has seen an improvement in performance – SOT 77.8% (77.7%) and NS 78.9 % (78.6%).
52 week breach - numbers have increased for SOT to 37 (34) and increased for NS to 32 (27).
Cancer access standards SOT only:
31 day subsequent treatment surgery – 81.8% (90.9%)
NS only: Cancer Breast Symptoms 2 week wait – 73.9% (90.9%)
Both CCGs Cancer 62 day screening – 75% (100%) NS and 71.4% (90.9%) SOT

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Other Performance at Month 3 WMAS
Category 1 to 4 – At M3 Both SOT and NS have achieved both the mean and the 90th centile response targets for category 1, 2, 3 and 4.
Hear and Treat; All CCGs across the region failed to meet the Hear and Treat standard (>7%). SOT and NS have seen a decline in M3 with SOT performing at 3.10% (10/20 regionally) and NS performing at 2.70% (17/20 regionally).
See and Treat; Both CCGs have met the See and Treat standard (>37%) in M3, and SOT achieved 40.1% (9/20 regionally) and NS achieved 41.3% (6/20 regionally).
See and Convey; SOT CCG struggled to meet the See and Convey standard (<56%) in M3 at 56.8% (9/20 regionally). However, NS achieved the standard in M3 at 56.0% (6/20 regionally) (meeting the standard for the first time since Dec’17).
Summary of risks relating to the proposal (inc. Ref. No. of risk it aligns to on Risk Register):
The mitigating actions being taken to address areas of non-delivery of constitutional targets and IAF indicators could have an impact on levels of CCG contracted activity. Where non-delivery of NHS Constitutional Standards indicates an adverse impact on patient safety this is investigated by the CCG Quality Team and pursued through the Clinical Quality Review Meeting (CQRM.
Implications:
Legal and/or Risk Monitoring performance is a statutory duty of the CCG as stated in their respective constitutions.
CQC
Patient Safety Quality Team reviewing potential harm and managing risk.
Patient Engagement
Financial
Sustainability
Workforce / Training
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
Please provide detail within the body of the report
x
2. Has an Equality Impact Assessment been completed?
Please provide detail within the body of the report as to these considerations:
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
x

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
Please provide detail within the body of the report
x
Recommendations / Action Required:
The North Staffordshire and Stoke-on-Trent CCGs Governing Body Meeting in Common is asked to:
Receive and Note:
The contents of the performance report and key messages
Key actions against each indicator

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
1
North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
Month 3 Performance Report
2018/19

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
2
North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
Contents Page
1. Executive Summary Page 3
2. Performance Overview Page 4
3. Activity v Plan Page 5
4. Urgent and Emergency Care Pages 6 - 13
- UHNM A&E
- NHS 111
- Ambulance – WMAS
- DTOCS
- Stranded and Super-stranded patients
4. Planned Care Pages 14 - 17
- Referral to Treatment and Patients Waiting over 52 weeks
- Long Waits and Waiting List Management
- Diagnostic Waits
5. Cancer Services Pages 18 - 20
6. Appendix: Focus on Planned Care at UHNM Pages 21 - 24

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
EXECUTIVE SUMMARY
3
Key Messages • The ‘performance overview’ (page 4) shows the latest validated data against the constitutional targets and a more detailed overview of
performance against the specific targets and the associated actions to manage performance is included in the body of this report.
• The latest available unvalidated performance data will be shared at the Finance and Performance Committee and Governing Body, and below is
a summary of the key actions taken since the last respective meetings over the past month.
Urgent & Emergency
Care
• In the past month the focus on UHNM’s A&E internal recovery plan continued with the following actions;
• Development of an Emergency Floor Model to take patients out of the Department and discharge them more quickly, with a view to
implementing before winter;
• Primary Care referrals model - right place, first time, admission avoidance and controlling flow with GP visibility of UHNM assessment
capacity;
• IT modelling and portal construction has been commissioned by UHNM & the CCGs and is underway, aiming for August/September
completion.
• A significant level of work both internally and at a system level on the recovery improvement plan, but the sizeable scale of improvement
necessary to deliver this step change in performance remains.
• System-wide Winter Plans and Surge Plans have been discussed by all partners within their organisations to ensure confidence in the plans.
Final versions of plans are to be submitted to NHS England by the 30th August 2018.
• In July 2018 UHNM and MPFT (Midlands Partnership Foundation Trust) began reporting higher numbers of delayed transfers of care (DTOCs).
Following scrutiny UHNM and MPFT discovered that an incorrect methodology to count DTOCs since April 2017.
• Issues at UHNM with the incorrect reporting of DTOCs due to a change in methodology in April 2017 have been resolved. A DTOC
counting workshop on the 24th July reviewed the issues and a new methodology was agreed by all partners effective from 1st August
2018. The new methodology was circulated to system leaders.
• Proposals to increase the DTOC baseline for quarter 3 2017 to give accurate numbers have been agreed and the correct DTOC
reporting methodology is now in use by both Trusts.
Planned Care • Referral to Treatment (RTT) performance at UHNM is gradually improving and has done for several months, but is still short of the 92%
standard.
• The Trust continues to progress validation, training and capacity work in order to define a credible recovery plan for elective care to address the
52 week issue and provide a clear path to recovering the 92% constitutional standard for RTT.
• There are still ongoing issues with the Trust’s PAS system. The Trust have developed an action plan and are working through it. However, this
involves changes to internal processes as well as validation of waiting lists.
• UHNM is working currently with KPMG to undertake an 18 week diagnostic sustainability review with the speciality teams. This piece of work is
informing recovery and improvement plans, as well as work on data quality and waiting lists. This will also include in-depth Demand and
Capacity work, which will eventually then put UHNM in a position to forecast a recovery trajectory.
Cancer • Over the past month underlying improvements to cancer performance have continued, as a result of reducing timed pathways and turnaround
times for diagnostics.
• UHNM have achieved the 62 days from GP referral treatment standard for June – 85.9% (in line with the improvement trajectory) and are on
track to achieve in July. UHNM plan to keep up the momentum around this and will be continuing to campaign on the importance of patients
keeping their appointments.
• Additional monies from the West Midlands Cancer Alliance have been used to extend the contracts of existing patient trackers during the
summer holiday period, and to sustain improvements in operational grip.

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
PERFORMANCE OVERVIEW M3
4
Indicator Target Apr May June YTD Trend Target Apr May June YTD Trend Target Apr May June YTD Trend
Referral To Treatment times
RTT incompletes92% 77.9% 78.6% 78.9% 78.4% 92% 76.6% 77.7% 77.8% 77.3% 92% 73.7% 75.0% 75.2% 74.6%
Zero tolerance of over 52 week
waiters (Snapshot)0 22 27 32 NA 0 27 34 37 NA 0 66 78 114 NA
Diagnostic test waiting times
Diagnostics 6 weeks+99% 99.1% 98.8% 98.7% 98.9% 99% 99.3% 99.4% 99.4% 99.1% 99% 99.2% 99.4% 99.2% 99.3%
Cancer waits
Cancer 2 week wait93% 96.9% 95.9% 95.8% 96.2% 93% 96.8% 97.6% 95.0% 96.5% 93% 96.4% 96.9% 94.8% 96.1%
Cancer Breast Symptoms 2 week
wait93% 96.2% 90.9% 73.9% 87.8% 93% 95.2% 97.8% 95.5% 96.4% 93% 93.9% 91.8% 88.3% 91.8%
Cancer 31 day first definitive
treatment96% 94.6% 95.7% 99.2% 96.7% 96% 95.5% 97.2% 98.4% 97.1% 96% 95.4% 97.2% 98.9% 97.3%
Cancer 31 day subsequent
treatment - surgery94% 88.0% 83.3% 94.1% 87.9% 94% 94.1% 90.9% 81.8% 90.0% 94% 95.2% 90.0% 87.8% 91.2%
Cancer 31 day subsequent
treatment - drug98% 100.0% 100.0% 100.0% 100.0% 98% 100.0% 100.0% 100.0% 100.0% 98% 100.0% 100.0% 100.0% 100.0%
Cancer 31 day subsequent
treatment - radiotherapy94% 97.2% 100.0% 94.1% 97.1% 94% 94.9% 98.1% 97.9% 97.1% 94% 96.2% 98.0% 94.8% 96.5%
Cancer 62 day standard85% 79.6% 79.7% 87.1% 82.1% 85% 80.9% 88.1% 90.0% 86.5% 85% 82.1% 82.4% 86.0% 83.5%
Cancer 62 day screening90% 100.0% 100.0% 75.0% 90.0% 90% 66.7% 90.9% 71.4% 81.0% 90% 86.4% 95.0% 80.0% 86.3%
Cancer 62 day upgradeNo Target 96.7% 87.5% 97.6% 94.8% No Target 84.4% 87.5% 93.2% 88.8% No Target 91.0% 89.5% 95.7% 92.3%
Ambulance
Category 1 (mean)00:07:00 00:07:13 00:06:25 00:06:53 00:06:51 00:07:00 00:06:13 00:06:05 00:06:06 00:06:08 00:07:00 00:06:50 00:06:51 00:06:59 00:06:53
Category 1 (90th centile)00:15:00 00:11:45 00:10:28 00:12:58 00:11:54 00:15:00 00:09:44 00:09:38 00:09:43 00:09:42 00:15:00 00:12:04 00:11:50 00:12:03 00:11:58
Category 2 (mean)00:18:00 00:11:28 00:12:17 00:12:08 00:11:58 00:18:00 00:09:18 00:09:35 00:09:49 00:09:34 00:18:00 00:11:24 00:12:00 00:12:28 00:11:58
Category 2 (90th centile)00:40:00 00:20:35 00:21:26 00:20:21 00:20:52 00:40:00 00:14:38 00:15:30 00:15:15 00:15:10 00:40:00 00:20:24 00:19:31 00:22:22 00:21:28
Category 3 (90th centile)02:00:00 00:39:29 00:44:38 00:52:40 00:45:42 02:00:00 00:41:00 00:39:14 00:49:21 00:42:46 02:00:00 00:55:17 01:08:13 01:17:02 01:06:51
Category 4 (90th centile)03:00:00 01:12:00 01:15:22 01:20:48 01:14:33 03:00:00 01:07:32 01:31:31 01:22:33 01:21:34 03:00:00 01:32:40 02:02:22 02:08:26 01:54:41
HCAI
HCAI measure (MRSA)0 0 0 1 0 0 0 0 0 0 NA NA NA NA NA NA
HCAI measure (Clostridium
difficile infections)60 5 1 3 6 86 6 6 3 12 NA NA NA NA NA NA
Mixed Sex Accommodation
Mixed Sex Accommodation
Breaches0 2 2 0 4 0 0 0 0 0 NA NA NA NA NA NA
A&E Waits (UHNM)
A&E 4 Hour TargetNA NA NA NA NA NA NA NA NA NA NA NA 95% 80.0% 83.8% 82.8% 82.3%
12 hour trolley breachesNA NA NA NA NA NA NA NA NA NA NA NA 0 2 0 0 2
UHNM
ProviderNorth Staffordshire CCG
WMAS
UHNM
UHNM
UHNM
Stoke on Trent CCG

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
5
ACTIVITY V PLAN (NHSE PLANNING INDICATORS - EM NUMBERS)
Planned Care Indicators (Referrals, Outpatients and Electives)
• GP Referrals are 5.8% under plan in M3 bringing the YTD performance
to -3.1%.
• The 10% over performance at M1 in Other Referrals continued into M2,
and reduced to a 3.4% over performance in M3. This is being followed
up with UHNM to understand the change in referral pattern.
• Outpatient First activity in June is performing 2.6% below plan and
Follow Ups 1.2% above plan, both within the 2.5% YTD tolerance used
by NHSE.
• Elective activity continues to trend below plan in June at around 6.6% for
both North Staffs CCG and Stoke on Trent CCG. Year to date, the
CCGs are approximately 5% below plan.
Unscheduled Care Indicators (Non Elective, A&E)
• A&E activity has continued to over perform in June being 5.9% above
plan in month. This is being investigated internally to understand the
change in attendance numbers. Recent changes to the Front of
House suggest there may be an increase in patients due to those
previously being streamed and redirected now being seen at UHNM.
• Non Elective (NEL) admissions at UHNM also continue to increase.
An 8.6% over performance to plan in June continues the similar
performance from April and May. According to UHNM, the volume of
patients seen in CDU (0-1 Length of Stay patients) has increased due
to the efficiency of simply and timely discharges, thus increasing the
flow and 4 hour A&E performance. A NEL task and finish group has
been set up internally within the CCGs to investigate the issues, and
pursue contractual challenges to UHNM.
Ref Indicator2017/2018
YTD Actual
2018/19 YTD
Plan
2018/19
YTD Actual
Variance
(Plan v
Actual)
2018/19
2017/2018
YTD Actual
2018/19
YTD Plan
2018/19
YTD Actual
Variance
(Plan v
Actual)
2018/19
2017/2018
YTD Actual
2018/19
YTD Plan
2018/19
YTD Actual
Variance
(Plan v
Actual)
2018/19
% Var
EM7 Total Referrals (G&A) 26849 26412 26639 227 19922 19571 20200 629 46771 45983 46839 856 1.86%
EM7a GP Referrals (G&A) 9346 14337 13759 -578 6995 10924 10719 -205 16341 25261 24478 -783 -3.10%
EM7b Other Referrals (G&A) 7955 12075 12880 805 5815 8647 9481 834 13770 20722 22361 1639 7.91%
EM8 Cons Led OP 1st Att (Specific Acute) 20409 21842 21334 -508 16414 16779 17302 523 36823 38621 38636 15 0.04%
EM9 Cons Led OP FU Att (Specific Acute) 28865 29367 29443 76 24872 25234 25490 256 53737 54601 54933 332 0.61%
EM10 Total Elective Admissions (Specific Acute) 9144 9364 8936 -428 7552 7618 7206 -412 16696 16982 16142 -840 -4.95%
EM11 Total NEL Admissions (Spells) (Specific Acute) 9474 9831 10405 574 6355 6396 6945 549 15829 16227 17350 1123 6.92%
EM12 Total A&E Att (excluding planned follow ups) 19327 21042 22199 1157 12236 12655 13943 1288 31563 33697 36142 2445 7.26%
North Staffordshire CCGStoke on Trent CCG Both
North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
6
Urgent & Emergency Care

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
7
UHNM A&E • In June UHNM A&E
performance has
slightly dipped since
the previous month to
82.8%. This equates
to 19,076 attendances
that were seen within
the 4 hour standard
out of 23,044 total
attendances.
• YTD performance
currently stands at
82.3%.
• UHNM had zero 12
hour trolley breaches
for a second
consecutive month.
Indicator Target Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
A&E Standard 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
A&E Performance
95% 84.72% 79.48% 81.07% 80.88% 79.77% 76.45% 78.45% 77.85% 71.54% 69.10% 74.74% 76.03% 80.00% 83.80% 82.80%
12 Hour Trolley Breaches
0 0 0 0 0 0 4 0 13 98 272 60 61 2 0 0
Q4 Q1
2018/19
Q3Q1 Q2
2017/18

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
8
UHNM A&E Mitigating Actions
Reducing Demand
• UHNM continued to be above trajectory for A&E 4 hour performance and saw a rise in the number of attendances coming into the Trust with an increase
of 4.4% compared from July 2017 and July 2018. The A&E performance trajectory remains ambitious and is consistent with the national expectation of
90% by September and 95% by March. Initiatives to reduce demand include; Streaming, UCC relocation, Primary Care Patient Pathways Management &
Service Staffing.
• System-wide Winter Plans and Surge Plans discussed by all partners within their organisations to ensure confidence in the plans and surge capacity
contingency with final versions of plans to be submitted to NHSE by the 30th August 2018.
Improving Flow through A&E
• The UHNM A&E internal recovery plan includes the following actions;
• Continue to develop an Emergency Floor Model to take patients out of the Department and discharge them more quickly, with a view to
implementing before winter;
• Primary Care referrals model - right place, first time, admission avoidance and controlling flow with GP visibility of UHNM assessment capacity
(AMU/SAU/FEAU/AECU/ED);
• IT modelling and portal construction has been commissioned by UHNM & CCG and is underway, aiming for August/September completion
• IT Boards in situ to support visibility of ED wait by area.
Reducing Length of Stay and Increasing Discharges
• ED flow and Stranded Patient Improvements, includes, a Royal Stoke University Hospital ED flow model developed to optimise flow based on
attendance/admission cycle times.
• An Acute Flow Programme has also been developed with ward enabler and discharge work streams supporting improved WIS board utilisation for
tracking of LOS and escalation KPI for MFFD to monitor discharge performance.
• Introduction of a ‘Staffordshire and Stoke-on-Trent Choice Policy to avoid long hospital stays’ and support patient’s timely, effective discharge from NHS
funded beds, to a setting which meets their needs. It applies to all adult residents of Staffordshire and Stoke-on-Trent in NHS acute hospitals and NHS
funded community beds, and needs to be utilised before and during admission to ensure that those who are assessed as ready for transfer can leave in a
safe and timely way.
Monitoring and Assurance
• Delivery of a whole-system Information-Sharing workshop in August focusing on admission avoidance, portfolio of services, measures of performance
and feedback.
• The Pan-Staffordshire UEC Programme Board will meet for the first time in September.

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
9
NHS 111
*All Commissioners - this data related to all Staffordshire CCGs and the data cannot be broken down by individual CCG
Issues
• The main contributing factors contributing to the issues have
been;
• Calls within forecast but large influx of calls at concentrated
times.
• Clinicians unable to front-end calls to support peaks as more
calls have now been validated by clinicians.
• Mutual aid and Pin management was in place at points
during the week across the business to support the demand
on the services. This was managed by national on call and
the intra-day analyst team.
• W/C 25th June saw an increase in sickness levels.
Actions
• The CCGs continue to monitor performance at Contract Review
Meetings (CRM) and continue with Contract Performance Notices
(CPNs) and Remedial Actions Plans (RAPs).
• The resubmitted RAP is not agreed as National UIC KPIs have been
issued, which alter the existing KPIs.
• Answered in 60 seconds remains within the revised KPIs and the
provider presented changes they have implemented and CRM have
requested a briefing paper detailing these changes.
• The mutual aid information request remains outstanding and a new
information request was issued W/C 6th August 2018 requesting a
Quality Impact Assessment.
• The Clinical Assessment Service Business case continues to be
developed with Vocare and commissioners, however, further
engagement is required with clinicians and other stakeholders over the
next couple of months.
Indicator Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Trend
Plan 29,130 36,590 29,413 29,555 37,121 30,904 29,978 37,661 30,280 30,429 30,578 38,411 29,131 28,320 22,759
Actual 26,964 25,234 22,747 25,215 23,399 23,245 25,331 24,192 31,142 29,748 26,343 27,583 25,320 25,663 23,181
Plan <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9% <=9%
All commissioners 9.58% 10.11% 12.83% 12.43% 12.50% 13.52% 13.50% 13.55% 12.63% 13.02% 12.95% 13.01% 12.36% 13.55% 13.57%
NS 9.64% 11.02% 14.61% 13.26% 13.42% 14.27% 14.13% 15.35% 13.55% 13.90% 13.66% 14.40% 13.04% 13.04% 15.14%
SOT 9.83% 9.89% 13.27% 13.11% 13.41% 14.32% 14.37% 14.28% 13.04% 13.47% 13.44% 13.25% 12.57% 12.57% 14.05%
Plan <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5%
All commissioners 5.43% 6.49% 8.59% 8.30% 8.10% 8.19% 8.03% 8.02% 6.78% 7.49% 7.68% 7.93% 7.94% 8.46% 9.16%
NS 5.52% 6.32% 8.25% 8.16% 7.62% 8.65% 9.11% 7.49% 6.54% 7.66% 7.82% 8.30% 8.34% 9.18% 9.98%
SOT 5.27% 6.29% 8.15% 8.47% 8.20% 7.68% 7.30% 7.89% 6.73% 7.15% 7.39% 7.58% 7.76% 8.30% 9.22%
Plan <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5% <=5%
All commissioners 1.60% 1.91% 2.29% 1.28% 1.48% 2.28% 2.72% 2.59% 3.34% 2.59% 5.28% 5.84% 3.03% 1.65% 2.68%
Plan >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95% >=95%
All Commissioners 89.60% 86.01% 85.77% 90.26% 88.67% 85.59% 84.56% 86.19% 81.64% 81.11% 71.83% 69.09% 82.91% 87.30% 82.05%
2018/192017/18
LQR_017 Calls answered within
60 seconds
LQR_005 Referral to ambulance
services
Calls answered (all
commissioners
LQR_016 Abandoned calls
LQR_006 Referral to Emergency
Dispositions

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
10
AMBULANCE – West Midlands Ambulance Service (WMAS)
Category 1 - 4; NS and SOT CCG have achieved both the mean and the 90th centile response targets for category 1, 2, 3 and 4
response targets in M3.
Hear and Treat; All CCGs across the region failed to meet the Hear and Treat standard (>7%). SOT 3.10% (10/20 regionally) and NS 2.70% (17/20
regionally).
See and Treat; All CCGs across the region achieved the See and Treat standard (>37%). SOT 40.1% (9/20 regionally) and NS 41.3%
(6/20 regionally).
See and Convey; Performance was mixed across the region for See and Convey. SOT failed to achieve the standard in M3 at 56.8% (9/20
regionally) however NS achieved the standard at 56.0% (6/20 regionally).
18 mins 40 mins
CCGIncidents
TotalMean
90th
Centile
NS CCG 1,215 00:12:08 00:20:21
SOT CCG 2,127 00:09:49 00:15:15
WMAS 38,309 00:12:28 00:22:22
England 342,640 00:21:38 00:44:35
Category 2 Target
7 mins 15 mins
CCGIncidents
TotalMean
90th
Centile
NS CCG 160 00:06:53 00:12:58
SOT CCG 263 00:06:06 00:09:43WMAS 4,983 00:06:59 00:12:03
England 55,658 00:07:37 00:13:19
Category 1 Target
n/a 120 mins
CCGIncidents
TotalMean
90th
Centile
NS CCG 1,342 00:23:32 00:52:40
SOT CCG 2,190 00:21:56 00:49:21
WMAS 34,041 00:34:58 01:17:02
England 178,146 01:00:15 02:20:01
Category 3 Target
n/a 180 mins
CCGIncidents
TotalMean
90th
Centile
NS CCG 77 00:35:31 01:20:48
SOT CCG 101 00:36:08 01:22:33
WMAS 1,832 00:55:04 02:08:26
England 17,353 01:28:44 03:15:38
Category 4 Target
Hear and Treat (H&T) Local Target Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Trend
NS CCG >7% 3.10% 3.20% 3.60% 2.70% 3.20% 2.30% 3.10% 2.60% 2.30% 2.70% 2.30% 2.60% 2.70%
SOT CCG >7% 3.20% 3.10% 3.20% 2.70% 3.30% 2.90% 2.80% 3.20% 2.90% 3.10% 2.60% 3.30% 3.10%
Regional CCG >7% 4.1% 4.0% 4.2% 3.2% 3.5% 3.7% 4.20% 3.40% 3.70% 4.00% 3.20% 3.50% 3.60%
England Average* >7% 5.1% 4.7% 5.7% 6.70% 5.60% 5.40% 5.70% 5.20% 5.45% 5.50%
See and Treat (S&T) Local Target Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Trend
NS CCG >37% 40.40% 41.60% 39.50% 37.80% 39.70% 39.50% 41.60% 40.90% 41.10% 39.50% 41.30% 39.70% 41.30%
SOT CCG >37% 40.20% 39.50% 38.80% 36.80% 38.20% 36.70% 41.90% 40.50% 39.50% 39.00% 40.20% 41.70% 40.10%
Regional CCG >37% 37.2% 37.5% 37.2% 38.6% 37.1% 37.1% 37.50% 38.00% 37.40% 37.50% 38.10% 38.00% 37.90%
England Average* >37% 57.5% 27.5% 27.8% 30.1% 29.9% 29.6% 29.7% 29.3% 29.6% 29.9%
See and Convey (S&C) Local Target Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Trend
NS CCG <56% 56.50% 55.10% 56.90% 59.50% 57.10% 58.20% 55.30% 56.50% 56.60% 57.80% 56.30% 57.70% 56.00%
SOT CCG <56% 56.60% 57.40% 58.00% 60.50% 58.50% 60.40% 55.30% 56.30% 57.60% 57.90% 57.30% 55.00% 56.80%
Regional CCG <56% 58.8% 58.5% 58.7% 58.2% 59.4% 59.2% 58.20% 58.10% 58.90% 58.50% 58.70% 58.60% 55.70%
England Average* <56% 37.4% 67.9% 66.5% 63.1% 64.5% 65.0% 64.6% 65.5% 64.9% 64.6%
*Change in methodology and unable to calculate as numerator and denominator not provided prior to Sep-17

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
11
AMBULANCE – WEST MIDLANDS AMBULANCE SERVICE (WMAS)
Issues
• The provider are achieving all 4 categories of response standards region wide and locally within NS and Stoke.
• Contracted activity is over YTD for NS at 2.84% but as planned for Stoke, regionally the contract is over by 2.74%.
• Clarity sought regarding H&T, S&T, and S&C as these targets are reported locally but not discussed in regional meetings. The response was;
• There are no regional or local targets for the increase of H&T and S&T. The CQUIN scheme for the 17/19 contract set out the requirements
• Year 1 (17/18) – Maintain Hear and Treat and Set and Treat Rates - achieved.
• Year 2 (18/19) - Reducing Conveyance to ED by 2% from the baseline of 57.5%. Success will be achieving 2 months in quarter four
(rather than a trajectory), below 55.5% - you can track how we are doing here - https://www.england.nhs.uk/statistics/statistical-
work-areas/ambulance-quality-indicators/ambulance-quality-indicators-data-2018-19/
Actions
• Handover Delays at Royal Stoke – financial penalties cannot be applied to the Trust, however, through the Contract meetings the CCG can ask for
this issue to be addressed through an action plan
• Global Digital Exemplar programme has been agreed nationally and commissioners have received a summary of what this programme will include,
however, there is still further discussions to take place regarding match funding.
• Agreed that the next regional service development meeting in September will review all West Midland CCGs services that paramedics can access.
Through this process commissioners and providers can establish how to improve utilisation of the services.
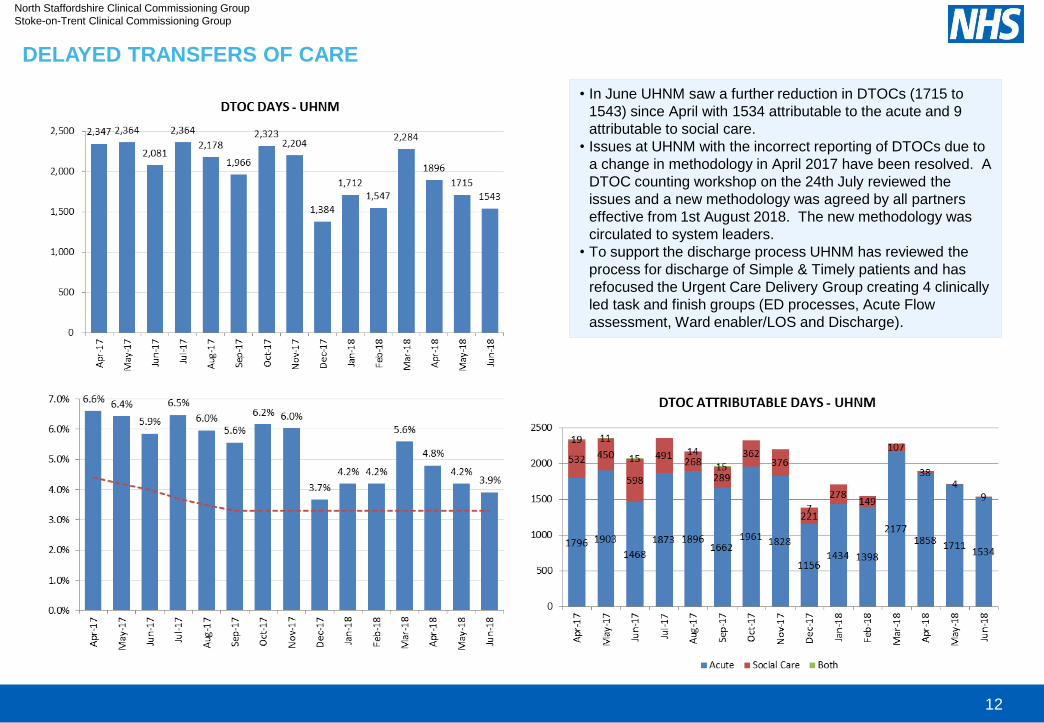
North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
12
DELAYED TRANSFERS OF CARE
• In June UHNM saw a further reduction in DTOCs (1715 to
1543) since April with 1534 attributable to the acute and 9
attributable to social care.
• Issues at UHNM with the incorrect reporting of DTOCs due to
a change in methodology in April 2017 have been resolved. A
DTOC counting workshop on the 24th July reviewed the
issues and a new methodology was agreed by all partners
effective from 1st August 2018. The new methodology was
circulated to system leaders.
• To support the discharge process UHNM has reviewed the
process for discharge of Simple & Timely patients and has
refocused the Urgent Care Delivery Group creating 4 clinically
led task and finish groups (ED processes, Acute Flow
assessment, Ward enabler/LOS and Discharge).

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
13
STRANDED PATIENTS AND SUPER STRANDED PATIENTS
• There is a growing focus on reducing length of
stay, particularly in the number of patients with a
length of stay over seven days (stranded patients)
and a length of stay over 21 days (super stranded
patients).
• A proportion of these patients will legitimately need
to be in hospital for that length of time however, a
significant proportion will have spent 7 or more
days in hospital because of unnecessary waits in
the system. Many are internal, including waiting for
a decision, diagnostic test, intervention, referral
etc.
• There is an expectation that providers and
commissioners work together to focus on reducing
their length of stay to release capacity for patients
who are legitimately waiting for a hospital bed as
identified in the stranded patients metric, to ensure
sufficient capacity will be available to meet planned
activity growth.
• Stranded patients and super stranded patients at
UHNM for NS and Stoke have remained relatively
flat in the last 12 months with peaks seen in spring
and summer months.

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
14
Planned Care

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
15
REFERRAL TO TREATMENT & PATIENTS WAITING OVER 52 WEEKS
UHNM Specialty Performance
* ‘Other’ ;the collection of specialities that are not required to be individually defined in the RTT
data by the DoH. It is not possible to further interrogate this category within the data
**Small volume of patients on waiting list
Measure Target SOT M3 Trend from
M2 YTD NS M3
Trend from
M2 YTD
% of incomplete pathways waiting less than 18 weeks 92% 77.8% ↑ 77.3% 78.9% ↑ 78.4%
Zero tolerance for patients waiting over 52 weeks 0 37 ↑ N/A 32 ↑ N/A
RTT waiting times
• 16 out of 18 reportable specialties at UHNM are not achieving
the 18 week target as at M3.
• In M3 most improvement can be seen in Cardiothoracic surgery
(+8.5%), T&O (+2.5%) and General Surgery (+2%). With a
number of other specialties showing marginal improvements,
although still performing below the standard.
• The specialty with the largest reduction in performance is
Neurosurgery (-2.8%),
Actions
• Given the CCG are unable to support the reinvestment of
contractual penalties into the validation of data and the
subsequent improvement plan for planned care, UHNM have
revisited their plans. UHNM have developed a short term
improvement plan, which the CCG have requested is shared.
• The CCGs have requested that they become members of the
UHNM Planned Care Board, and one of the CCG’s Medical
Directors will be attending.
• CPNs were issued for UHNM on 2nd August 2018 for both 18
weeks and 52 weeks.
• The CCGs are also focusing on a 52 week recovery trajectory
given the increasing number of breaches at UHNM. The CCGs
are working with providers to identify patients waiting more than
52 weeks and seek a method to offer them an alternative
provider. NS focus is around General Surgery and Urology
specialties, and SOT around General Surgery and T&O.
Treatment Function
NameM3
% variation
since M2Trend
Backlog
clearance
required to
achieve 92% at
M3
Increase/
Decrease in
backlog
since M2
Backlog
as of M2
General Surgery 64.3% +2.0% 1,747 -73 1,820
Urology 59.6% -0.6% 1,039 +71 968
Trauma & Orthopaedics 75.4% +2.5% 455 -86 541
ENT 91.7% +0.9% 8 -22 30
Ophthalmology 92.4% +0.1% 8
Oral Surgery 84.7% -0.1% 147 -2 149
Neurosurgery 77.5% -2.8% 49 +6 43
Plastic Surgery 89.9% -1.3% 16 +11 5
Cardiothoracic Surgery 90.1% +8.5% 4 -16 20
General Medicine** 94.4% -2.4%
Gastroenterology 88.4% -0.9% 118 +118
Cardiology 84.8% +0.6% 213 -25 238
Dermatology 73.8% +0.4% 309 +5 304
Thoracic Medicine 54.2% -0.3% 1,433 -72 1,505
Neurology 72.8% +0.1% 559 -31 590
Geriatric Medicine** 85.4% -12.0% 5 5
Gynaecology 70.4% -0.4% 532 -25 507
Other* 77.1% -0.5% 1,369 +28 1,341
Total 75.2% +0.3%

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
16
PLANNED CARE – LONG WAITS & WAITING LIST MANAGEMENT
UHNM overall total waiting list has seen a slight decrease in M3 with the total 18 week backlog decreasing to 11844, now accounting for 25% of the
total waiting list. For UHNM to achieve the 92% standard they would need to clear 8178 patients from the backlog.
• 52 week waits - Both CCGs continue to see an increase in the number of 52 weeks waits. 52 week Breach Review Panels are now well established
with representation from the CCGs quality team and reporting to CQRM.

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
17
DIAGNOSTIC WAITS
• NS failed the standard in M3 underperforming by 0.26%.
• East Cheshire NHS Trust continued to be the provider that contributed to this failure with 37/209 (17.7%) tests failing to be completed within 6
weeks for the NS cohort of patients.
Measure Target SOT M3 Trend from
YTD NS M3 Trend from
YTD M2 M2
Diagnostics 6 weeks + 99% 99.4% ↑ 99.2% 98.7% ↓ 98.9%
Issues
• Limited Clinician availability to pick up 'dropped lists' in the
Endoscopy Treatment Unit (associated with clinical leave).
• An increase in the Echocardiography backlog from 111 to 129.
• Cessation of weekend work.
• Increase in cancer and urgent referrals (16% increase in 2ww and
50% increase in urgent patients to be seen within 4 weeks which
means that these have been prioritised above routine patients).
• Transfer of cystoscopy was delayed until May due to estate issues.
• 2WW and urgent patients have been booked and standards met but
this prioritisation has resulted in an increased backlog of routine and
surveillance patients.
Actions
• Maintain productivity as close to 276 per week.
• Prioritise Echocardiography backlog patients in July. The Trust are
also exploring additional capacity to reduce the backlog in
echocardiography.
• Sub-contracting to Wilmslow Health Centre.
• Cytoscopy lists have now been removed from the endoscopy unit to
create additional capacity.
• Sustain compliance with access policy and maintain DNA rate
below 6%.
• Audit validation of surveillance patients to reduce inappropriate
scoping.
• The CCGs have asked the host commissioning CCG to provide a
detailed update on the complete diagnostic performance and
subsequent recovery plan and trajectory.

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
18
Cancer

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
19
CANCER SERVICE ACCESS
Breach Analysis
To note: breach reasons currently unavailable due to migration to new cancer
reporting repository – CCGs should have access from next month
Issues
• UHNM June’s performance for the 62 day from GP referral target is at
86.0% against the 85% target. July’s performance is on track to
achieve.
Actions
• Urology: to address access to diagnostic issue MRI hot reporting has
commenced. This should mean that some TRUS (Transrectal
Ultrasound Guided) biopsies are not required and appropriate patients
may be able to be taken off pathway at that point which will improve
efficiency of the pathway. The longer term plan to train more nurses is
in progress.
• Focused work continues by the trackers to identify patients on the
pathway most at risk of breaching.
• Rotas are being agreed for the Summer.
• Dermatology are phasing in the ‘see and treat’ model.
Stoke on Trent
No of patients that breached
the standard
31 day first definitive treatment surgery 2/11
62 day treatment from screening 2/7
Target
No of patients that breached
the standard
Breast symptoms 2 week wait 6/23
62 day treatment from screening 2/8
Indicator Target Apr May June Q1 YTD YTD Trend Target Apr May June Q1 YTD YTD Trend Target Apr May June Q1 YTD YTD Trend
Cancer waits
Cancer 2 week wait93% 96.9% 95.9% 95.8% 96.2% 96.2% 93% 96.8% 97.6% 95.0% 96.5% 96.5% 93% 96.4% 96.9% 94.8% 96.1% 96.1%
Cancer Breast Symptoms 2 week
wait93% 96.2% 90.9% 73.9% 87.8% 87.8% 93% 95.2% 97.8% 95.5% 96.4% 96.4% 93% 93.9% 91.8% 88.3% 91.8% 91.8%
Cancer 31 day first definitive
treatment96% 94.6% 95.7% 99.2% 96.7% 96.7% 96% 95.5% 97.2% 98.4% 97.1% 97.1% 96% 95.4% 97.2% 98.9% 97.3% 97.3%
Cancer 31 day subsequent
treatment - surgery94% 88.0% 83.3% 94.1% 87.9% 87.9% 94% 94.1% 90.9% 81.8% 90.0% 90.0% 94% 95.2% 90.0% 87.8% 91.2% 91.2%
Cancer 31 day subsequent
treatment - drug98% 100.0% 100.0% 100.0% 100.0% 100.0% 98% 100.0% 100.0% 100.0% 100.0% 100.0% 98% 100.0% 100.0% 100.0% 100.0% 100.0%
Cancer 31 day subsequent
treatment - radiotherapy94% 97.2% 100.0% 94.1% 97.1% 97.1% 94% 94.9% 98.1% 97.9% 97.1% 97.1% 94% 96.2% 98.0% 94.8% 96.5% 96.5%
Cancer 62 day standard85% 79.6% 79.7% 87.1% 82.1% 82.1% 85% 80.9% 88.1% 90.0% 86.5% 86.5% 85% 82.1% 82.4% 86.0% 83.5% 83.5%
Cancer 62 day screening90% 100.0% 100.0% 75.0% 90.0% 90.0% 90% 66.7% 90.9% 71.4% 81.0% 81.0% 90% 86.4% 95.0% 80.0% 86.3% 86.3%
Cancer 62 day upgrade
No
Target96.7% 87.5% 97.6% 94.8% 94.8% No Target 84.4% 87.5% 93.2% 88.8% 88.8% No Target 91.0% 89.5% 95.7% 92.3% 92.3%
North Staffordshire CCG Stoke on Trent CCG UHNM

North Staffordshire Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
20
CANCER SERVICE ACCESS – LONG WAITS (62 DAY AND 104 DAY PERFORMANCE)
• As of 05/08/2018 there
were 90 patients recorded
on the PTL list as waiting in
excess of 62 days.
• This is an increase of 12
patients since the previous
week. This remains slightly
below the 2017/18 weekly
average of 91 patients,
however this has seen a
marked increase since May.
• As at 05/08/2018 there were
5 x 104 day breaches on the
UHNM Cancer Patient
Tracking List (PTL).
• 2 x NS CCG
• 1 x SOT CCG
• 2 x Other CCGs
• This is an increase of 2
patients since the previous
week.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 9.1
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Summary of matters discussed at the Primary Care Commissioning Committees in Common meeting on Tuesday 7th August 2018
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Margy Woodhead – Lay Member for Patient and Public Involvement SOTCCG Peter Dartford – Lay Member for Patient and Public Involvement
Y Jessica Chaplin – Primary Care Administrator
Clinical Lead(s) Reviewer: Links to the STP:
N/A N/A
Action Required (select):
Decision Discussion For Assurance / For Information X
Purpose of the Paper:
The report provides a summary of the main issues considered by the North Staffordshire and Stoke-on-Trent CCGs’ Primary Care Commissioning Committees meeting in common on Tuesday 7th August 2018.
Areas discussed included: Finance Update Primary Care Commissioning Strategy Plan Discretionary Spending Plan Social Prescribing Implementation Plan BMJ GP Recruitment Marketing Campaign Update GP Forward View Milestone Report
Summary of risks relating to the proposal:
Implications:
Legal and/or Risk N/A
CQC N/A
Patient Safety N/A
Patient Engagement N/A

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Financial N/A
Sustainability N/A
Workforce / Training N/A
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
x
2. Has an Equality Impact Assessment been completed?
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
x
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
x
Recommendations / Action Required:
The Governing Bodies of North Staffordshire and Stoke-on-Trent CCGs’ are asked to: Receive and note the matters discussed at the Primary Care Commissioning Committee held in
Common on Tuesday 7th August 2018.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
North Staffordshire CCG and Stoke-on-Trent CCG Primary Care Commissioning Committees Meeting in Common
CHAIRS REPORT TO THE NORTH STAFFORDSHIRE CCG AND STOKE-ON-TRENT CCG GOVERNING BODIES
This briefing summarises the key items discussed at the North Staffordshire and Stoke-on-Trent CCGs’ Primary Care Commissioning Committees in Common on 7
th August 2018. The CCGs’ established the
Primary Care Commissioning Committees following the delegation of Primary Care to the CCGs with effect from 1
st April 2017 and the Committee has now been in operation for over 12 months. The main matters
considered at the August meetings which the Committees wish to draw the Governing Bodies attention to are as follows:
1. Primary Care Risk Register The Committees received the Primary Care Risk Register. There were a total of eight risks presented to the Committees, four of which were high scoring risks – there have been no new risks since the Committees received the register in June 2018. The Committees identified a number of issues in the Risk Register presented, with a number of due dates passed with no update and mitigating actions that had not been refreshed. It was agreed that the issue will be escalated by the chair of the Audit Committee, as assurance had been obtained that the risk registers were refreshed with meaningful mitigations, risk assessment and ownership of risks. Subsequently, the Committees were not assured and refreshed risk registers would be presented back to the September meeting.
2. Finance Update – Primary Care Delegated Budgets
The meeting received the month three financial position for North Staffordshire CCG and Stoke-on-Trent CCG Delegated Budgets. As at month 3 both CCGs were reporting an underspend with North Staffordshire CCG reporting an underspend of £156,000 and Stoke-on-Trent CCG were reporting an underspend of £94,000 – although the CCGs were reporting an underspend in the overall delegated budgets, there were cost pressures on APMS contracts and rent costs. Due to the underspend it has been identified that a robust plan needs to be developed to ensure that if there was an underspend at year end, funding will be suitably allocated to support the CCGs GP Five Year Forward View strategic vision. This plan is to be presented back to the October Committee and a verbal update to be presented back in September to update on progress made.
3. Primary Care Commissioning Strategy Plan – Update The meeting were presented with an update on the progress on the development of the Primary Care Commissioning Strategy Plan. The plan has now been presented to all Six Staffordshire CCGs’ Governing Bodies. A stakeholder Group will be convened including LMC representation to provide robust input in to the development of the plan. A further update to be presented to the September meeting.
4. Other The committees also received an update on the following items: BMJ Marketing Campaign – The Committees requested that the BMJ Marketing Campaign progressed at
pace to support the recruitment in to Primary Care; Workforce Update –The Committees were presented with a verbal update on General Practice Workforce.
As at the time of the meeting CCGs’ are 18% under their trajectory for GP whole time equivalent posts (WTE) across Staffordshire and 2% behind trajectory for other General Practice clinical staff. The Staffordshire Workforce plan outlines a clear commitment for retention with c£162,000 allocated for resilience. General Practice has submitted bids to support workforce to access the funding and there was a focus on the issues in retaining female GPs and an engagement plan is being developed to address the issues and in addition there is work taking place regionally to support international GP recruitment.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
Rebecca Woods, Head of Primary Care for NHS England is due to present a formal written update to the September meeting to provide an accurate position for North Staffordshire and Stoke-on-Trent and Staffordshire, including benchmarking.
Social Prescribing Implementation Plan – MWo to provide a verbal update to the Governing Bodies.
Margy Woodhead Peter Dartford Lay Member for PPI – Stoke-on-Trent CCG Lay Member for PPI – North Staffordshire CCG Co-Chair of the Primary Care Co-Chair of the Primary Care Commissioning Committee Commissioning Committee

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
1
REPORT TO:
Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Enclosure: 9.2
Report to: Public Meeting in Common of the North Staffordshire and Stoke-on-Trent Clinical Commissioning Groups’ Governing Bodies
Title: Summary of matters discussed at the Planning and Commissioning Committee – July Meeting
Meeting Date: Tuesday 4th September 2018
Executive Lead(s): Exec Sign-Off Y/N Author(s):
Dr Steve Fawcett – Medical Director Y Jessica Chaplin – Primary Care Administrator
Clinical Lead(s) Reviewer: Links to the STP:
N/A N/A
Action Required (select):
Decision X Discussion For Assurance / For Information
Purpose of the Paper:
The North Staffordshire and Stoke-on-Trent CCGs’ Governing Bodies Meeting in Common are asked to Note the summary of key issues and ratify the decisions made from the Planning and Commissioning Committee in Common held in July 2018.
Approved for Chairs Action to take place to award the contract for the Orthotics Service to the preferred provider for a 3 year contract, subject to a successful presentation demonstrating deliverability and quality of service
Noted the Healthy Lifestyle Budget update Noted the update on the Acute Visiting Service Noted the contentment of the End of Life presentation for Stoke-on-Trent and Staffordshire
and the palliative care coordination centre and acknowledged the next steps moving forward to develop the proposal following the outcome of the Government Life Chances Fund End of Life bid
Agreed that (1) that North Staffordshire CCG enters into a formal joint commissioning arrangement with Staffordshire County Council for non NHS Children and Young Peoples emotional wellbeing services with a current value of £100,134 per annum to be transferred for the duration of the contract and (2) that North Staffordshire CCG continues the joint commissioning arrangement with Staffordshire County Council for specialist emotional wellbeing support for Looked After Children. Current value £54,000 per annum to be transferred for the duration of the contract

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
2
Summary of risks relating to the proposal:
Implications:
Legal and/or Risk N/A
CQC N/A
Patient Safety N/A
Patient Engagement N/A
Financial N/A
Sustainability N/A
Workforce / Training N/A
Key Requirements: Yes No
1. Has a Quality Impact Assessment been completed?
x
2. Has an Equality Impact Assessment been completed?
Can you confirm an Equality Impact & Risk Assessment (EIRA: stage 1 & 2) has been completed; if not, what is the rationale for non-completion?
Which if any of the nine Protected Groups were targeted for engagement and feedback to CCGs, and why those?
Summarise any disaggregated feedback from local Protected Group reps about any negative impacts arising / recommendations (e.g. service improvements)
What mitigation / re-shaping of services resulted for people from local Protected Groups (along the lines of ‘You Said: We Listened, We Did’?)
Explain any ‘objective justification’ considerations, if applicable
x
Key Requirements: Yes No
3. Has Engagement activity taken place with Stakeholders / Practices / Communities / Public and Patients
x
Recommendations / Action Required:
The Governing Bodies of North Staffordshire and Stoke-on-Trent CCGs’ are asked to: Ratify the decisions made at the July Planning and Commissioning Committee.

Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
3
North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee
CHAIRS REPORT TO THE NORTH STAFFORDSHIRE CCG AND STOKE-ON-TRENT CCG
GOVERNING BODIES
1. Orthotics The Committee received a paper detailing the positon of the orthotics procurement. Three bids were received, with evaluation and moderation taking place in June 2018. Due to weighting calculations and the focus to ensure quality of service, the highest scoring bidder was invited back to demonstrate their model of delivery for one day, one week and one month based on activity information provided. The process delayed the process but ensured full assurance to the CCGs that all reasonable steps had been taken to appoint a bidder that is able to a good quality safe service. Due to the timescale, the July Committee were asked to approve for a Chairs action to be taken to award the three year contract – with the option of a two year extension. The North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee agreed for Chairs Action to take place to award the contract for the Orthotics Service to the preferred provider for a 3 year contract, subject to a successful presentation demonstrating deliverability and quality of service.
2. Healthy Lifestyle Budget
The Committee received an update on Staffordshire County Council Public Health spend and an overview of future Public Health commissioning intentions – whereby members were advised that Public Health were trying to target resources in the best way and developing a programme of work to compliment the traditional approach of investment in specialist services and to achieve the outcomes shared by both the CCGs and Public Health with aligned assets and lifestyle assets. The North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee noted the Healthy Lifestyle Budget update.
3. Acute Visiting Service (AVS) The Committee were provided with an update on the Acute Visiting Service operating across North Staffordshire and Stoke-on-Trent CCGs. A contact extension has been agreed with a view for a further extension for the service to operate until February 2019 to support the anticipated winter pressures. Work is taking place to incorporate the AVS in to the CCGs’ Urgent Care work stream, with a view to potentially commissioning an AVS scheme across Staffordshire, in line with the work taking place with Out of Hours and the Front of House Service. The North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee noted the update on the Acute Visiting Service.
4. End of Life Staffordshire and Stoke-on-Trent/Government Life Chances Fund The meeting received a presentation detailing the current position for end of life, details around the paper review around Palliative Care Coordination Centre and detail around an application to be submitted for the Government Life Chances fund for end of life innovation – with a vision to help patients to die with dignity in their placed of choice through good planning and good care with an inclusive approach tailored to individual needs.
Cannock Chase Clinical Commissioning Group East Staffs Clinical Commissioning Group North Staffs Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford & Surrounds Clinical Commissioning Group Stoke-on-Trent Clinical Commissioning Group
4
A series of working groups have been established to take forward the priorities and actions identified through the End of Life Programme Board and progress against actions to the Enhanced Primary and Community Care Committee. Details were provided around the application for Government Life Chances Fund, which outlined a bid to take forward element within the pathway across Staffordshire for £2m per year over a five year period based on a social finance proposal supported by Marie Curie and Macmillan funding and work will take place to work up the outcome measures, with financial caveats to be presented back to the Committee. The North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee noted the contentment of the End of Life presentation for Stoke-on-Trent and Staffordshire and the palliative care coordination centre and acknowledged the next steps moving forward to develop the proposal following the outcome of the Government Life Chances Fund End of Life bid.
5. Joint Commissioning of non NHS CAMHS Services (Tier 2) in North Staffordshire The Committee were presented with an overview of the proposal for commissioning non NHS (Tier 2) Child and Adolescent Mental Health Services and services for Looked After Children across Staffordshire. The services are presently aligned but with separate commissioning arrangements through North Staffordshire CCG and Staffordshire County Council. The current framework ends in March 2019 and there was a proposal that North Staffordshire CCG will enter in to a joint commissioning arrangement with Staffordshire County Council for the provision of Tier 2 services. The North Staffordshire CCG and Stoke-on-Trent CCG Planning and Commissioning Committee agreed that (1) that North Staffordshire CCG enters into a formal joint commissioning arrangement with Staffordshire County Council for non NHS Children and Young Peoples emotional wellbeing services with a current value of £100,134 per annum to be transferred for the duration of the contract and (2) that North Staffordshire CCG continues the joint commissioning arrangement with Staffordshire County Council for specialist emotional wellbeing support for Looked After Children. Current value £54,000 per annum to be transferred for the duration of the contract.
Related Documents











