Acute Kidney Injury David T. Selewski, MD,* Jordan M. Symons, MD † Author Disclosure Drs Selewski and Symons have disclosed no financial relationships relevant to this article. This commentary does not contain a discussion of an unapproved/ investigative use of a commercial product/ device. Educational Gap The term acute kidney injury has replaced acute renal failure and represents a spectrum of clinically meaningful kidney damage. Objectives After completing this article, readers should be able to: 1. Recognize and define the spectrum of acute kidney injury (AKI). 2. Understand the diagnostic approach and be able to differentiate the main causes of AKI. 3. Understand the complications of AKI and the treatment of a child with AKI. Introduction Acute kidney injury (AKI), formerly called acute renal failure, is characterized by multiple abnormalities, including increases in serum creatinine and blood urea nitrogen, electrolyte abnormalities, acidosis, and difculties with uid management. We have come to realize that what was previously thought to be relatively minor damage to the kidney can have signicant short-term effects on morbidity and mortality and potential long-term implica- tions for the development of chronic kidney disease. Thus, the term acute kidney injury has replaced acute renal failure, suggesting the spectrum of kidney damage that can occur. Definition AKI is classically dened as an acute decrease in glomerular ltration rate, which results in an increase in serum creatinine. It is important to recognize the limitations of creatinine as a marker of AKI because an increase in creatinine can be delayed by as much as 48 hours after damage to the kidney has occurred. Despite this limitation, change in creatinine re- mains the gold standard for the diagnosis of AKI. An evolution in the denition of AKI to better understand, characterize, and study the disease spectrum, has occurred, which has sought to capture the clinical importance of even small variations in kidney function. In addition, previous denitions used in the literature were widely disparate; this lack of stan- dardization made the understanding of AKI challenging. These circumstances have led to the development of 2 sys- tems to dene pediatric AKI that rely on changes in creati- nine, estimated creatinine clearance, or urine output. The rst of these denitions is the pediatric Risk, Injury, Failure, Loss, and End-stage (RIFLE) criteria, (1) which are modi- ed from similar adult criteria. (2) The second is the Acute Kidney Injury Network (AKIN) denition, which relies on an increase in creatinine from a previous trough level. (3) The Kidney Disease: Improving Global Outcomes (KDIGO) consortium has put forth modications to recon- cile subtle differences in the adult AKIN and RIFLE criteria. (4) KDIGO is an international initiative composed of ex- perts who, based on systematic review of evidence, develop and standardize clinical practice guidelines for children and adults with a variety of kidney diseases (including AKI). At Abbreviations ACE: angiotensin-converting enzyme AKI: acute kidney injury AKIN: Acute Kidney Injury Network ANCA: antineutrophil cytoplasmic antibody ATN: acute tubular necrosis ECG: electrocardiogram FE urea : fractional excretion of urea FE Na : fractional excretion of sodium KDIGO: Kidney Disease: Improving Global Outcomes NSAID: nonsteroidal anti-inammatory drug RIFLE: Risk, Injury, Failure, Loss, and End-stage *Department of Pediatrics and Communicable Diseases, Division of Nephrology, C.S. Mott Children’s Hospital, University of Michigan, Ann Arbor, MI. † Department of Pediatrics, Division of Nephrology, University of Washington School of Medicine, Seattle, WA. Article nephrology 30 Pediatrics in Review Vol.35 No.1 January 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Acute Kidney InjuryDavid T. Selewski, MD,*
Jordan M. Symons, MD†
Author Disclosure
Drs Selewski and
Symons have disclosed
no financial
relationships relevant
to this article. This
commentary does not
contain a discussion of
an unapproved/
investigative use of
a commercial product/
device.
Educational GapThe term acute kidney injury has replaced acute renal failure and represents a spectrum of
clinically meaningful kidney damage.
Objectives After completing this article, readers should be able to:
1. Recognize and define the spectrum of acute kidney injury (AKI).
2. Understand the diagnostic approach and be able to differentiate the main causes of
AKI.
3. Understand the complications of AKI and the treatment of a child with AKI.
IntroductionAcute kidney injury (AKI), formerly called acute renal failure, is characterized by multipleabnormalities, including increases in serum creatinine and blood urea nitrogen, electrolyteabnormalities, acidosis, and dif!culties with "uid management. We have come to realizethat what was previously thought to be relatively minor damage to the kidney can havesigni!cant short-term effects on morbidity and mortality and potential long-term implica-tions for the development of chronic kidney disease. Thus, the term acute kidney injury hasreplaced acute renal failure, suggesting the spectrum of kidney damage that can occur.
DefinitionAKI is classically de!ned as an acute decrease in glomerular !ltration rate, which results inan increase in serum creatinine. It is important to recognize the limitations of creatinine asa marker of AKI because an increase in creatinine can be delayed by as much as 48 hoursafter damage to the kidney has occurred. Despite this limitation, change in creatinine re-mains the gold standard for the diagnosis of AKI. An evolution in the de!nition of AKI tobetter understand, characterize, and study the disease spectrum, has occurred, which hassought to capture the clinical importance of even small variations in kidney function. Inaddition, previous de!nitions used in the literature were widely disparate; this lack of stan-
dardization made the understanding of AKI challenging.These circumstances have led to the development of 2 sys-tems to de!ne pediatric AKI that rely on changes in creati-nine, estimated creatinine clearance, or urine output. The!rst of these de!nitions is the pediatric Risk, Injury, Failure,Loss, and End-stage (RIFLE) criteria, (1) which are modi-!ed from similar adult criteria. (2) The second is the AcuteKidney Injury Network (AKIN) de!nition, which relieson an increase in creatinine from a previous trough level.(3) The Kidney Disease: Improving Global Outcomes(KDIGO) consortium has put forth modi!cations to recon-cile subtle differences in the adult AKIN and RIFLE criteria.(4) KDIGO is an international initiative composed of ex-perts who, based on systematic review of evidence, developand standardize clinical practice guidelines for children andadults with a variety of kidney diseases (including AKI). At
Abbreviations
ACE: angiotensin-converting enzymeAKI: acute kidney injuryAKIN: Acute Kidney Injury NetworkANCA: antineutrophil cytoplasmic antibodyATN: acute tubular necrosisECG: electrocardiogramFEurea: fractional excretion of ureaFENa: fractional excretion of sodiumKDIGO: Kidney Disease: Improving Global OutcomesNSAID: nonsteroidal anti-in"ammatory drugRIFLE: Risk, Injury, Failure, Loss, and End-stage
*Department of Pediatrics and Communicable Diseases, Division of Nephrology, C.S. Mott Children’s Hospital, University ofMichigan, Ann Arbor, MI.†Department of Pediatrics, Division of Nephrology, University of Washington School of Medicine, Seattle, WA.
Article nephrology
30 Pediatrics in Review Vol.35 No.1 January 2014
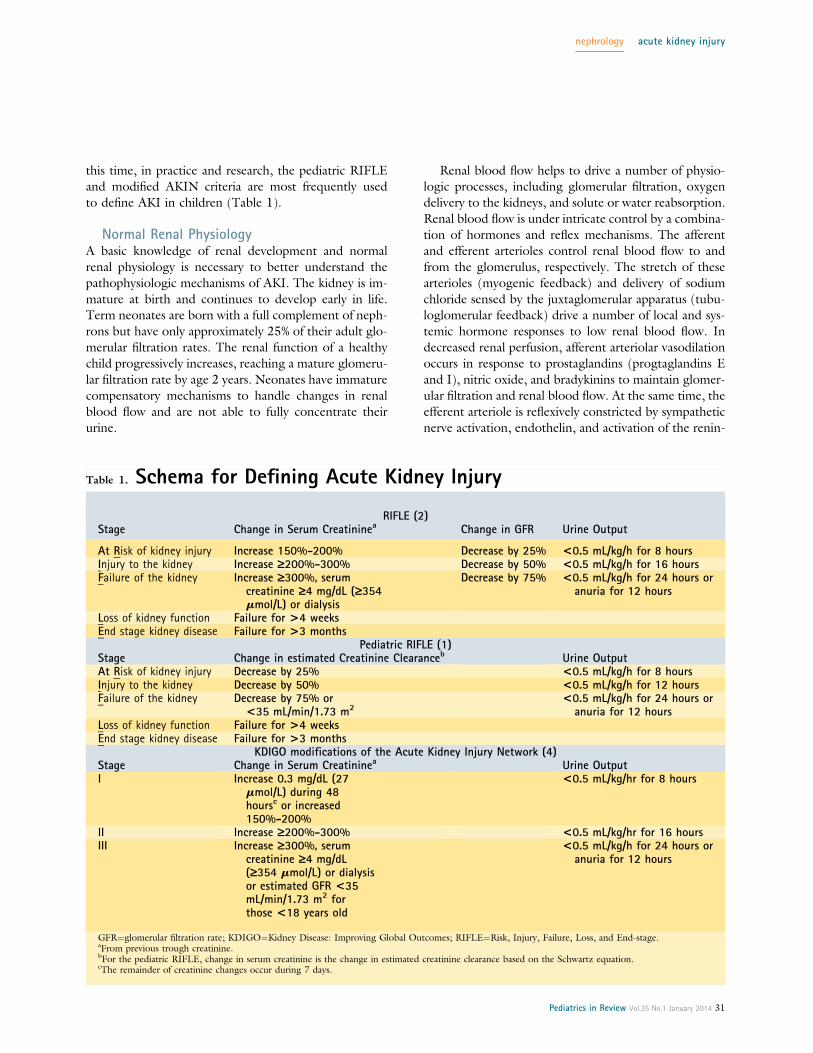
this time, in practice and research, the pediatric RIFLEand modi!ed AKIN criteria are most frequently usedto de!ne AKI in children (Table 1).
Normal Renal PhysiologyA basic knowledge of renal development and normalrenal physiology is necessary to better understand thepathophysiologic mechanisms of AKI. The kidney is im-mature at birth and continues to develop early in life.Term neonates are born with a full complement of neph-rons but have only approximately 25% of their adult glo-merular !ltration rates. The renal function of a healthychild progressively increases, reaching a mature glomeru-lar !ltration rate by age 2 years. Neonates have immaturecompensatory mechanisms to handle changes in renalblood "ow and are not able to fully concentrate theirurine.
Renal blood "ow helps to drive a number of physio-logic processes, including glomerular !ltration, oxygendelivery to the kidneys, and solute or water reabsorption.Renal blood "ow is under intricate control by a combina-tion of hormones and re"ex mechanisms. The afferentand efferent arterioles control renal blood "ow to andfrom the glomerulus, respectively. The stretch of thesearterioles (myogenic feedback) and delivery of sodiumchloride sensed by the juxtaglomerular apparatus (tubu-loglomerular feedback) drive a number of local and sys-temic hormone responses to low renal blood "ow. Indecreased renal perfusion, afferent arteriolar vasodilationoccurs in response to prostaglandins (progtaglandins Eand I), nitric oxide, and bradykinins to maintain glomer-ular !ltration and renal blood "ow. At the same time, theefferent arteriole is re"exively constricted by sympatheticnerve activation, endothelin, and activation of the renin-
Table 1. Schema for Defining Acute Kidney Injury
RIFLE (2)Stage Change in Serum Creatininea Change in GFR Urine Output
At Risk of kidney injury Increase 150%-200% Decrease by 25% <0.5 mL/kg/h for 8 hoursInjury to the kidney Increase ‡200%-300% Decrease by 50% <0.5 mL/kg/h for 16 hoursFailure of the kidney Increase ‡300%, serum
creatinine ‡4 mg/dL (‡354mmol/L) or dialysis
Decrease by 75% <0.5 mL/kg/h for 24 hours oranuria for 12 hours
Loss of kidney function Failure for >4 weeksEnd stage kidney disease Failure for >3 months
Pediatric RIFLE (1)Stage Change in estimated Creatinine Clearanceb Urine OutputAt Risk of kidney injury Decrease by 25% <0.5 mL/kg/h for 8 hoursInjury to the kidney Decrease by 50% <0.5 mL/kg/h for 12 hoursFailure of the kidney Decrease by 75% or
<35 mL/min/1.73 m2<0.5 mL/kg/h for 24 hours oranuria for 12 hours
Loss of kidney function Failure for >4 weeksEnd stage kidney disease Failure for >3 months
KDIGO modifications of the Acute Kidney Injury Network (4)Stage Change in Serum Creatininea Urine OutputI Increase 0.3 mg/dL (27
mmol/L) during 48hoursc or increased150%-200%
<0.5 mL/kg/hr for 8 hours
II Increase ‡200%-300% <0.5 mL/kg/hr for 16 hoursIII Increase ‡300%, serum
creatinine ‡4 mg/dL(‡354 mmol/L) or dialysisor estimated GFR <35mL/min/1.73 m2 forthose <18 years old
<0.5 mL/kg/h for 24 hours oranuria for 12 hours
GFR!glomerular !ltration rate; KDIGO!Kidney Disease: Improving Global Outcomes; RIFLE!Risk, Injury, Failure, Loss, and End-stage.aFrom previous trough creatinine.bFor the pediatric RIFLE, change in serum creatinine is the change in estimated creatinine clearance based on the Schwartz equation.cThe remainder of creatinine changes occur during 7 days.
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 31

angiotensin system, leading to the production of angio-tensin II. These mechanisms work in concert to maintainglomerular !ltration and renal blood "ow. Disease statesand certain medical interventions may interfere withthese mechanisms, leading to negative effects on glomer-ular !ltration. Further, some of these compensatorymechanisms, when stressed beyond normal parameters,may themselves lead to diminished urinary output andclinical !ndings one would associate with AKI.
With decreased renal perfusion, a number of thesecompensatory mechanisms also drive sodium and waterreabsorption to increase extracellular volume. Increasedactivity of the renin-angiotensin system and productionof angiotensin II (active in the proximal tubule) leadsto increased secretion of aldosterone (active in the distaltubule), resulting in increased sodium reabsorption. In-creased sympathetic nerve activity also drives sodium re-absorption. The reabsorption of urea and water is drivenby antidiuretic hormone. The activity of these re"exmechanisms explains a number of the changes in urineelectrolyte concentrations and clinical !ndings that helpto differentiate the causes of AKI. The immaturity ofthese mechanisms in the neonate also explains why thediagnosis and evaluation of the cause of AKI in the neo-nate differs from that in older children.
EpidemiologyThe epidemiology of AKI has evolved over the years andre"ects the patient population under study. In developingcountries the most common causes of AKI continue to bevolume depletion, infection, and primary renal diseases(hemolytic uremic syndrome, glomerulonephritis). In de-veloped countries, volume depletion and primary renal dis-ease remain common causes of AKI in previously healthychildren. In hospitalized children in developed countries,particularly in tertiary care centers, there has been a shift inthe etiology of AKI from primary renal disease to second-ary causes of AKI that are oftenmultifactorial in nature andoften complicate another diagnosis or its treatment (eg, heartdisease, sepsis, and nephrotoxic drug exposure). (5) Despitethis shift in epidemiology, an ordered approach to the diag-nosis of AKI divides the potential origins into prerenal, in-trinsic, and postrenal causes.
Pathophysiology of AKIPrerenal AKI
Prerenal AKI results from a decrease in renal blood "ow,leading to hypoperfusion (Table 2). The underlying path-ophysiologic states may be due to a decrease in effectivecirculating volume, loss of vascular tone, or decreased
cardiac output or blood delivery to the kidneys. Renallosses, gastrointestinal tract losses, or hemorrhage canlead to direct reduction in volume and decreased renalperfusion. Alternatively, a redistribution of "uid may oc-cur from either reduced oncotic pressure within theblood (low albumin from liver disease, nephrotic syn-drome, or protein losing enteropathy) or increased leakfrom vessels (systemic in"ammatory response syndromeor sepsis), leading to suboptimal renal perfusion. Systemicvasodilation or poor vascular tone complicates a numberof illnesses in critically ill children and may result in hy-poperfusion of the kidneys. Finally, there may be a de-crease in the delivery of blood to the kidneys becauseof an overall decrease in cardiac output (underlying heartdisease or myocarditis) or increased resistance to "ow(abdominal compartment syndrome or renal artery ste-nosis). In practice, previously healthy children frequentlypresent with a decreased effective circulating volumefrom a single cause, whereas chronically ill or hospitalizedchildren may have multifactorial processes.
As noted above, low renal blood "ow stimulates com-pensatory mechanisms, including increased sympathetictone, activation of the renin-angiotensin system, releaseof antidiuretic hormone, and local paracrine activities(prostaglandin release). In the prerenal state, the afferentarterioles vasodilate in response to the local effects ofprostaglandins in an effort to maintain renal blood "owand glomerular !ltration. Consequently, nonsteroidalanti-in"ammatory drugs (NSAIDs), such as ibuprofen,in volume-depleted children may worsen AKI by prevent-ing this compensatory afferent arteriolar vasodilation. Atthe same time, angiotensin II causes efferent arteriolarconstriction. Interruption of this compensatory mech-anism by angiotensin-converting enzyme (ACE) inhibi-tors predisposes patients to prerenal AKI. The effectsof renin-angiotensin system activation and antidiuretichormone release result in increased sodium and urea re-absorption, respectively. The reabsorption of sodium,urea, and water leads to oliguria and the characteristicurine !ndings in prerenal AKI (Table 3).
Neonates are a special group when considering prere-nal AKI. Neonates have increased insensible losses be-cause of a high body surface area to mass ratio, whichcan be exacerbated by the use of radiant warmers for crit-ically ill newborns. Neonates are further at risk for prere-nal AKI due to immature compensatory mechanisms,including poor urine concentrating abilities. This inabilityto concentrate urine explains why AKI in neonates is of-ten nonoliguric, making its recognition more dif!cult.
Patients with sickle cell disease are predisposed to pre-renal AKI because of a number of pathophysiologic
nephrology acute kidney injury
32 Pediatrics in Review Vol.35 No.1 January 2014

mechanisms inherent to the disease that may affect thekidney. The renal medulla represents an area of the kid-ney at risk in sickle cell disease because of a low oxygenconcentration and high tonicity; this predisposes patientsto sickling. Repeated episodes of sickling in the renalmedulla result in vascular congestion and the loss of vasa
recta of the juxtaglomerular nephrons, which can lead tochronic interstitial !brosis and urine concentrating de-fects. In early childhood, the urinary concentrating de-fects frequently are reversible with treatment of thesickle cell disease but can progress to chronic concentrat-ing defects over time.
Intrinsic AKIIntrinsic AKI refers to direct renal parenchymal damageor dysfunction. Categories include AKI associated withtubular, interstitial, glomerular, or vascular damage andnephrotoxin exposure (Table 4).
The most common cause of intrinsic AKI in tertiarycare centers is transformation of prerenal AKI to acutetubular necrosis (ATN) after prolonged hypoperfusion.The areas of the kidney that are most susceptible to dam-age with prolonged renal hypoperfusion include the thirdsegment of the proximal tubule (high energy require-ment) and the region of the thick ascending limb ofthe loop of Henle located within the medulla (low oxy-gen tension in the medulla). The damage seen from pro-longed hypoperfusion can range from mild tubular injuryto cell death. As cellular necrosis occurs, debris may buildup in the tubules and further block tubular "ow. Tubulardysfunction, a frequent hallmark of ATN, will not be ev-ident during periods of oliguria but may become appar-ent during the recovery phase.
In previously healthy children, glomerular and vascularcauses of intrinsic AKI are more common. Where thereis concern for glomerulonephritis, the clinical presentationand timing often suggest the origin, including isolated glo-merulonephritides (eg, postinfectious glomerulonephritis)and multisystem immune complex–mediated processesthat involve the kidney (eg, systemic lupus erythematosus).
Vascular causes of intrinsic AKI in-clude microangiopathic processes(hemolytic uremic syndrome andthrombotic thrombocytopenic pur-pura) and systemic vasculitides thatinvolve larger vessels.
Acute interstitial nephritis occursafter exposure to an offendingagent, such as certain medications,including antibiotics, proton pumpinhibitors, NSAIDs, and diuretics.Signs and symptoms may develop3 to 5 days after a second expo-sure to as long as weeks to monthsafter an initial exposure. Drugs cancause AKI in ways other than acuteinterstitial nephritis. Nephrotoxin
Table 2. Causes of Prerenal AcuteKidney Injury
Decreased effective circulating volumeReduction in blood volumeGastrointestinal losses (eg, gastroenteritis)Renal losses (eg, diabetes insipidus and diuretic
exposure)Hemorrhage (eg, gastrointestinal bleed and trauma)Increased losses through the skin (eg, burn patients)
Redistribution of blood volumeDecreased oncotic pressureCirrhosis or liver diseaseNephrotic syndromeMalnutritionProtein-losing enteropathy
Increased leak from vessels (systemic inflammatoryresponse syndrome/sepsis)
Loss of vascular tone (systemic vasodilation)SepsisAnaphylaxis
Decreased blood delivery to the kidneysDecreased cardiac outputHeart disease (congenital heart disease, heart
failure)Increased resistance to flowRenal artery stenosisAbdominal compartment syndrome
Table 3. Comparison of Laboratory Findings in AKI
Test Prerenal AKI Intrinsic AKI
Urine specific gravity >1.020 £1.010Urine sodium, mEq/L <20 >40Fractional excretionof sodium
<1% (neonates <2%) >2% (neonates >2.5%)
Fractional excretionof urea
<35% >50%
Urine osmolality,mOsm/kg
>500 <350
Urea nitrogen–creatinine ratio
>20 10-15
AKI!acute kidney injury.
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 33

exposure is an increasingly common cause of intrinsicAKI, particularly in hospitalized patients. As previouslymentioned, drugs such as NSAIDs and ACE inhibitorscan contribute to AKI by inhibiting renal vascular auto-regulation. Other common drugs implicated in AKI in-clude aminoglycosides, amphotericin, chemotherapeuticagents (cisplatin, ifosfamide, and methotrexate), andcalcineurin inhibitors (cyclosporine and tacrolimus). Ra-diocontrast agents are a signi!cant cause of nephrotoxin-related AKI; newer iso-osmolar agents are somewhat lessnephrotoxic, but the risk remains. In instances of massivehemolysis or rhabdomyolysis, endogenous elements,such as myoglobin and hemoglobin, can obstruct tubulesand/or cause direct toxic effects to the kidney.
Postrenal AKIPostrenal AKI results from obstructive processes thatblock urine "ow. Acquired causes of urinary tract ob-struction include those that result from local mass effect(bilateral ureteral obstruction by a tumor), renal calculi,or clots within the bladder.
The Renal Angina Concept and EarlyIdentification of AKI
An important developing paradigm in the study andtreatment of AKI is the idea of renal angina, a term usedto describe a high-risk state that occurs before AKI. (6)Earlier recognition of a prerenal state de!nes a periodbefore signi!cant parenchymal damage (eg, the develop-ment of ATN) where AKI can be reversed. Furthermore,patients who are identi!ed as being at risk may havenephrotoxic medications held or dosages adjusted to po-tentially prevent the development of intrinsic AKI. Re-search using renal angina scoring systems is an activearea that aims to identify patients at risk for AKI. Con-currently, investigation is under way to study novel bio-markers (urine neutrophil gelatinase–associated lipocalinand urine kidney injury molecule 1) that will allow forthe earlier identi!cation of kidney injury in critically illchildren (often up to 48 hours before an increase increatinine) to allow prevention and potentially earlierintervention.
Diagnosis of AKIA detailed history and physical examination are invaluablefor children who develop AKI. Quantifying the urineoutput during the previous several days may provide in-sight to the cause and severity of the episode of AKIand serves to categorize the event as oliguric (de!nedas urine output<1 mL/kg/h) or nonoliguric. Systematic
Table 4. Causes of Intrinsic AKI
Tubular injuryAcute tubular necrosisUrine microscopy: muddy brown granular castsCommonly from transformation of prerenal AKIDrugs associated with acute tubular necrosis:aminoglycosides, calcineurin inhibitors,amphotericin, chemotherapeutic agents(platinum based), methotrexate, intravenouscontrast
Toxin mediated: myoglobinuria, hemoglobinuria,heavy metals
GlomerulonephritisHematuria, proteinuria, red blood cell casts onurinalysis
Postinfectious glomerulonephritisClassically 2-3 weeks after upper respiratory tractinfection, 4-6 weeks after skin infection
Low C3, normal C4Dark brown or “smoky” urine
IgA nephropathyGross hematuria soon after (1-3 days) an upperrespiratory tract infection
Normal C3, C4Systemic lupus erythematosusAnti–double-stranded DNA associated with renaldisease; antinuclear antibody positive
Low C3 and low C4Associated systemic symptoms (eg, arthritis,discoid rash, malar rash, photosensitivity,serositis)
Membranoproliferative glomerulonephritisLow C3; normal or low C4Uncommon pediatric condition
Goodpasture syndromeHemoptysisAnti–glomerular basement membrane antibody
Granulomatosis with polyangiitis (formerly Wegenergranulomatosis)Respiratory tract involvement including upperairway (sinus) and lungs
Cytoplasmic antineutrophil cytoplasmic antibodyMicroscopic polyangiitisLung involvementPerinuclear antineutrophil cytoplasmic antibody
Eosinophilic granulomatosis (formerly Churg-Strausssyndrome)Associated with sinusitis, asthma, and skin findingsPeripheral eosinophiliaPerinuclear antineutrophil cytoplasmic antibody
Rapidly progressive glomerulonephritisProgressive loss of renal function over short periodof time
Medical emergency warranting renal biopsyTypified by crescents on renal biopsyPotentially caused by any of theglomerulonephritides
Continued
nephrology acute kidney injury
34 Pediatrics in Review Vol.35 No.1 January 2014

evaluation of potential prerenal, intrinsic, and postrenalcauses is key to diagnosing the origin of AKI. Frequently,the history will provide insight into causes or risk factorsfor prerenal AKI, including decreased circulatory volume(gastroenteritis and hemorrhage), redistribution of circu-latory volume (edematous states, nephrotic syndrome,and sepsis), decreased cardiac output (heart disease), orincreased resistance to blood "ow (abdominal compart-ment syndrome and renal artery stenosis). In previouslyhealthy children, the history and physical examinationmay offer clues (Table 4) to the underlying intrinsic re-nal origin, including volume depletion, recent viralillness or sore throat (possibly consistent with acute glo-merulonephritis), rashes, swollen joints (suggesting sys-temic disorders such as lupus), hematuria, or medicationexposures. In newborns with a suspected obstruction,a good prenatal history is important. For example, ab-normalities on fetal ultrasonogram, including enlarged
bladder, hydronephrosis, or decreased amniotic "uid,may suggest posterior urethral valves in a male infant.When evaluating AKI, it is important to remember thatan increase in creatinine typically occurs up to 48 hoursafter renal injury and may re"ect events that occurred 2 to3 days earlier. Therefore, it is important to review epi-sodes of hypotension, hypoxia, sepsis, surgery, contrastexposures, and drug exposures that occur 48 to 72 hoursbefore the episode of AKI becomes apparent.
As part of the initial evaluation for AKI, patientsshould have the following tests performed: basic electro-lyte panel, serum creatinine measurement, urinalysis,urine sodium measurement, urine urea measurement,urine creatine measurement, urinalysis, and a renal ultra-sound study. Frequently, urine studies will allow differen-tiation between prerenal AKI and intrinsic AKI (eg,ATN). Typical laboratory !ndings for prerenal AKI in-clude a normal urinalysis result, concentrated urine (os-molality >500 mOsm/kg [>500 mmol/kg]), fractionalexcretion of sodium (FENa) less than 1% (<2% in neo-nates), fractional excretion of urea (FEurea) less than 35%,urine sodium less than 20 mEq/L (<20 mmol/L),and urea nitrogen to creatinine ratio greater than 20(Table 3). A loss of urine concentrating ability is classi-cally seen in ATN and results in the characteristic urinestudies that differentiate it from prerenal AKI (Table3). Urinalysis with accompanying urine microscopy canbe illuminating and point toward particular diagnosticcategories. Muddy granular casts on microscopy suggestATN; red blood cell casts suggest glomerulonephritis.A urinalysis positive for blood on dipstick evaluationwithout evidence of red blood cells on microscopy shouldraise concerns for hemoglobinuria (hemolysis) or myo-globinuria (rhabdomyolysis).
The presence of hematuria, proteinuria, and/or redblood cell casts in the right clinical scenario should raiseconcern for possible glomerulonephritis. In the contextof a recent upper respiratory tract infection, one shouldconsider the diagnosis of postinfectious glomerulone-phritis (classically with pharyngitis 2-3 weeks earlier orskin infections 4-6 weeks earlier) and should evaluate se-rum complements (low C3 and normal C4). In patientswith a more recent upper respiratory tract infection (2-3days) with gross hematuria on urinalysis, one must con-sider IgA nephropathy (normal complement levels). Aurinalysis consistent with glomerulonephritis in the con-text of the appropriate systemic symptoms (eg, rash andarthritis) may point toward systemic lupus erythematosus(low C3 and low C4) and may warrant further antibodytesting (antinuclear and anti–double-stranded DNA anti-bodies). If there is involvement of the pulmonary system
Table 4. (Continued)
Interstitial nephritisAllergic interstitial nephritisFrequently drug induced (classically antibiotics;
proton pump inhibitors an increasing cause)Classic triad (fever, eosinophilia, and rash) in only
15%Urinalysis may reveal eosinophils, white blood cell
casts, or red blood cell casts or may be blandMay also result from systemic disease capable of
causing acute interstitial nephritis, includingsarcoidosis, Sjogren disease, infections, and renaltransplant rejection
Hemolytic uremic syndromeMicroangiopathic hemolytic anemia (schistocytes onperipheral smear), thrombocytopenia, elevatedlactate dehydrogenase
Diarrhea-positive, classic, Shiga toxin–producingEscherichia coli hemolytic uremic syndromeOccurs within several days after infection with
toxin-producing organismColitis or bloody diarrheaUsually self-resolves
Diarrhea-negative hemolytic uremic syndromeNonintestinal infections (Streptococcus
pneumoniae and human immunodeficiency virus)Medication or therapy related (calcineurin
inhibitors, radiation therapy, and stem celltransplantation)
Disorders of complement regulation (deficiencies offactor H, factor I, and membrane cofactorprotein)
AKI!acute kidney injury.
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 35

(cough, in!ltrate on radiographs, and hemoptysis) andevidence of active glomerulonephritis, the pulmonary re-nal syndromes should be considered. These syndromesinclude granulomatosis with polyangiitis (formerly Wege-ner granulomatosis and cytoplasmic antineutrophil cyto-plasmic antibody [ANCA]), microscopic polyangiitis(perinuclear ANCA), eosinophilic granulomatosis (for-merly Churg-Strauss Syndrome and perinuclear ANCA),and Goodpasture syndrome (anti–glomerular basementmembrane antibody). A more detailed description of glo-merulonephritides is beyond the scope of this review. Inthe setting of a classic clinical and laboratory presentationof postinfectious glomerulonephritis, a renal biopsy is notwarranted, but to con!rm the diagnosis and guide treat-ment of the remaining glomerulonephritides, a biopsy isnecessary. Each of the glomerulonephritides is capable ofcausing rapidly progressive glomerulonephritis, which isde!ned by rapidly increasing blood urea nitrogen andcreatine levels. In this scenario, a renal biopsy and treat-ment are immediately warranted because irreversible re-nal injury may develop without prompt intervention.
The classic triad for allergic interstitial nephritis of fe-ver, rash, and eosinophilia is not often seen in the modernera and is observed in less than 15% of patients. This isdue to a change over time in the most common offendingagents. In patients with suspected interstitial nephritis,there is frequently bland urine sediment that does nothave red blood cell casts but may have white blood cellcasts present. The classic !nding is urine eosinophils, al-though this is not universal. There can be varying degreesof proteinuria; NSAID-associated interstitial nephritis iscapable of causing nephrotic range proteinuria. A renalbiopsy is necessary to con!rm the diagnosis.
If a patient has a recent history of diarrheal illness, lowplatelet counts, and hemolytic anemia with AKI, oneshould consider hemolytic uremic syndrome. In the appro-priate setting, a peripheral blood smear with schistocytes iscon!rmatory. In recent years there has been an increase inthe recognition of atypical hemolytic uremic syndromecaused by nondiarrheal infections (eg, Streptococcus pneu-monia or human immunode!ciency virus) or genetic ab-normalities in complement regulatory components (eg,factor H or factor I); a high index of suspicion is necessary,and specialty consultation is warranted.
Imaging plays a small role in the diagnosis of intrinsicrenal disease. Kidney size, measured by renal ultrasonog-raphy, can provide information about the duration of thedisease. Larger kidneys point toward an acute processthat involves active in"ammation. Kidneys that are partic-ularly small for age may suggest a more chronic process.Often the kidneys will demonstrate increased echogenicity
in the setting of AKI, which is a nonspeci!c !nding. ADoppler evaluation of the renal vasculature is an importantinitial step if there are concerns of renal artery stenosis, butif the result of the evaluation is negative and concern ofrenal artery stenosis remains, further studies should beconsidered in consultation with a pediatric nephrologist.Imaging by renal ultrasonography to demonstrate hydro-nephrosis is the most important initial step in the diagnosisof an obstructive process and may provide clues to the an-atomical location of the obstruction. For example, bilateralhydronephrosis suggests a more distal obstruction. If anobstructive process is diagnosed, one should relieve theobstruction immediately.
Management of AKIThe most important management principle for childrenwith AKI is prevention. In both the outpatient settingsand the hospital this can be achieved by identifying chil-dren who are at risk for developing AKI. In outpatientpediatrics it is important to ensure adequate hydrationand be mindful of medications children may take in theshort term (NSAIDs) or long term (diuretics and ACEinhibitors) that increase the risk of AKI. In hospitalizedpatients, it is also important to be mindful of daily volumestatus, nephrotoxic medications, or nephrotoxic expo-sures. For patients at risk for developing AKI, it is impor-tant that the team evaluates all potentially nephrotoxicmedications, reviews prescribed doses, actively considersalternatives, and monitors levels of medications such asgentamicin and vancomycin.
Fluid and Electrolyte ManagementThe initial step in the treatment of children who presentwith oliguria, hypotension, or instability is to restore intra-vascular volume. An initial 20-mL/kg bolus of isotonic"uids should be given rapidly (in minutes if necessary inthe setting of shock). Isotonic "uids that may be usedfor short-term volume expansion include normal saline,lactated Ringer solution, albumin, and packed red bloodcells. The choice of "uid depends on the clinical scenario,but normal saline is most commonly used. This treatmentshould be repeated according to the Pediatric AdvancedLife Support algorithms. (7) In children with underlyingor suspected cardiac disease, smaller initial "uid boluses(10mL/kg)may be given repeatedly, as indicated, for lon-ger periods; this will permit appropriate resuscitation whilereducing the risk of unintentional volume overload, whichcould be problematic in the setting of heart disease. Dur-ing the "uid resuscitation process, repeated reevaluation isnecessary for all children to monitor for signs of "uid
nephrology acute kidney injury
36 Pediatrics in Review Vol.35 No.1 January 2014

overload (pulmonary or peripheral edema) and response(improved vital signs and urine output).
After adequate "uid resuscitation, early initiation ofvasopressor support may be indicated; vasopressor sup-port may be required sooner for a child who presents withobvious "uid overload. Studies in adults evaluating lowrenal dose dopamine have found no bene!t; dopamineat these low doses does not increase or preserve urineoutput or improve the outcome of AKI. Vasopressor sup-port should be provided to ensure adequate renal perfu-sion with the choice of vasopressor based on the clinicalscenario. Once the patient has been adequately "uid re-suscitated, one may consider a trial of diuretics (furose-mide) if the patient remains oliguric. The literaturereports mixed results for diuretics in patients with oligu-ria. The literature surrounding the use of mannitol is in-conclusive, and this medication may be associated withserious adverse effects (increased serum osmolarity, pul-monary edema, and AKI). The use of mannitol to ensureurine output is not recommended.
In children who remain oliguric after intravascular vol-ume resuscitation, conservative "uid management maybe necessary. In these children, one may restrict "uid toinsensible "uid losses (300-500 mL/m2/d). Individualswith AKI are subject to a number of electrolyte disturbances,including dysnatremias, hyperkalemia, acidosis, andhyperphosphatemia. Typical sodium requirements inhealthy children are 2 to 3 mEq/kg/d, but managementshould be individualized in children with AKI, with ad-justments made based on frequent monitoring. Excessivesodium input should be avoided to prevent hypertensionand other complications of sodium overload. Potassiumand phosphorous should be withheld from "uids in thesepatients to avoid the risks of iatrogenic overload. Potas-sium and phosphorous will need to be replaced intermit-tently as necessary because low levels of potassium(cardiac conduction abnormalities) and phosphorous(poor muscle contraction) can have detrimental implica-tions in critically ill children. Inability to maintain bio-chemical or "uid balance in AKI patients represents anindication for renal replacement therapy.
Hyperkalemia remains one of the most recognizedcomplications of AKI. The presenting symptoms of hy-perkalemia are frequently nonspeci!c, including fatigue,weakness, tingling, nausea, and even paralysis. For thisreason, limiting potassium intake and diligent monitoringof laboratory test results in children with AKI are impor-tant. The most serious manifestation of hyperkalemia iscardiac conduction abnormalities and arrhythmias. Elec-trocardiographic (ECG) changes may be noted when po-tassium levels are 6.5 to 7 mEq/L (6.5-7 mmol/L), but
there can be signi!cant variability, depending on the clin-ical circumstances. In pathophysiologic states of increasedpotassium release from cells (tumor lysis syndrome andrhabdomyolysis), ECG changes may occur at lower levels.The potassium levels that result in ECG changes "uctuatewith the underlying pathophysiologic mechanisms, acuity,and associated electrolyte abnormalities (hypocalcemia).The ECG changes are typi!ed !rst by peaked T waves.Other ECG changes may include widened QRS, "attenedp waves, and prolonged PR interval. Untreated hyperkale-mia may lead to life-threatening arrhythmias.
In patients with potassium levels greater than 6 mEq/L(>6 mmol/L), one should obtain an ECG. If potassiumlevels are 5.5 to 6.5 mEq/L (5.5-6.5 mmol/L) and thepatient has an appropriate urine output without any abnor-malities on ECG, one may consider treatment with a resinthat binds potassium in the gut (sodium polystyrene sulfo-nate) or a saline bolus with furosemide to reverse any up-ward trend and slowly bring the potassium back to a morenormal range. If there are changes on ECG, a potassiumlevel greater than 7 mEq/L (>7 mmol/L), or a rapidlyincreasing potassium level in a child with high cell turnoverstates (eg, tumor lysis and rhabdomyolysis), hyperkalemiashould be viewed as life threatening and treated accord-ingly. Initial rapid treatment measures include calcium glu-conate, which acts to stabilize the cardiac membranepotential and limit the risk of arrhythmia but does notlower potassium levels. This may be followed by the ad-ministration of sodium bicarbonate, b2-agonists, and/orinsulin with glucose, all of which cause intracellularmovement of potassium and subsequent reduction ofblood levels, but these do not remove potassium fromthe body. Sodium bicarbonate may be considered if thereis an acidosis associated with the hyperkalemia. Recenttrials evaluating sodium bicarbonate therapy in adultswith hyperkalemia have not reported ef!cacy, but thishas not been studied in children. Although sodium bicar-bonate may be given as part of treatment for hyper-kalemia, it should not be the sole therapy. Sodiumbicarbonate theoretically acts by shifting potassium intra-cellularly as it is exchanged for hydrogen ions. b2-agonists,such as albuterol, can be given via nebulizer. This therapyhas been reported to lower potassium by 1 mEq/L(1 mmol/L) and is well tolerated but may need to beavoided in children with cardiac issues because tachycar-dia is a common adverse effect of b2-agonist therapy. In-sulin given with glucose drives potassium into cells byincreasing sodium and potassium adenosine triphospha-tase activity. In conjunction with these various methods,efforts should be made to remove potassium from thebody, including loop diuretics with "uid bolus and
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 37

sodium polystyrene sulfonate. Sodium polystyrene sulfo-nate should be avoided in neonates or children with un-derlying bowel disease. If these measures fail, renalreplacement therapy should be considered.
The acidosis seen in AKI is characterized by an ele-vated anion gap, which re"ects an inability of the kidneysto excrete acid or reabsorb bicarbonate. With the ex-ception of the treatment of hyperkalemia, use of bicar-bonate should be reserved for severe acidosis andadministered with great care. Correction of acidosiswith bicarbonate can lead to a lowering of ionized cal-cium (functional hypocalcemia) as hydrogen ions areexchanged on plasma proteins for calcium, which can re-sult in tetany.
Because of a suboptimal glomerular !ltration rate inthe setting of AKI, hyperphosphatemia can develop, par-ticularly with increased cell turnover (tumor lysis syn-drome and rhabdomyolysis). In most circumstances,hyperphosphatemia can be managed conservatively bylimiting intake. In patients with hyperphosphatemia, itis important to diligently monitor calcium and ionizedcalcium levels because ionized hypocalcemia may occuras a result of intravascular binding to excess phosphorus.
MedicationsIn children with AKI drug clearance may be reduced;daily evaluation of patient medication lists is imperativeto avoid iatrogenic drug overdose. Once the kidney func-tion decreases to 50% of normal, most renally excreteddrugs will require dose adjustment. Early in episodes ofevolving AKI, bedside estimates of kidney function canlead to overestimation of the glomerular !ltration rate;careful clinical judgment is required. One should evaluatethe appropriateness of administering nephrotoxic medi-cations on a daily basis, consider alternatives, and closelymonitor drug levels as able when nephrotoxic medica-tions are unavoidable. When children begin renal replace-ment therapy, many medication doses must be adjustedfurther (particularly antibiotics). During episodes ofAKI, it is important to manage medication adjustmentsin a team-based approach that involves pediatric nephrol-ogists and specialized pharmacists.
NutritionTypically, AKI is marked by a catabolic state, particularlyin critically ill children. The protein requirements in thesechildren may be as high as 3 g/kg/d of amino acids withan accompanying caloric need of 125% to 150% that ofhealthy children and infants. One should not limit proteindelivery as a method to control blood urea nitrogen levels;to ensure adequate protein intake, one may accept
a blood urea nitrogen level of 40 to 80 mg/dL (14.3-28.6 mmol/L). If adequate nutrition and metabolic bal-ance cannot be obtained through conservative measures,this may be an indication for renal replacement therapy.
Renal Replacement TherapyRenal replacement therapy is considered when conserva-tive measures to manage AKI have failed or are unlikelyto be suf!cient. Indications for renal replacement therapyinclude volume overload (10%-20% "uid excess), severeacidosis, hyperkalemia, uremia (typically blood urea ni-trogen >100 mg/dL [>35.7 mmol/L] or symptom-atic), or an inability to provide adequate nutrition inpatients with renal dysfunction. In recent years the im-portance of volume overload in critically ill children hasbecome apparent, and the degree of "uid overload atthe initiation of renal replacement therapy has beenfound to be associated with increased mortality. (8)(9)
Modalities of renal replacement therapy include peri-toneal dialysis, hemodialysis, and continuous renal re-placement therapy. The correct choice of modality isa re"ection of center-speci!c expertise, patient character-istics, and clinical situation. Peritoneal dialysis is well tol-erated in critically ill children and relatively easy toperform but does not provide the same rate of clearanceor ability to manage volume as other modalities. Inter-mittent hemodialysis performed during 3 to 4 hours pro-vides better clearance but is generally not as well toleratedin critically ill children or children with unstable disease;total daily "uid removal during a short intermittent ses-sion can be challenging in these patients. There has beena shift toward continuous renal replacement as the mo-dality of choice in critically ill children. This mode allowsfor continuous volume and metabolic control spread dur-ing 24 hours. Bene!ts include increased tolerance of "uidremoval and improved ability to provide nutrition. Inter-mittent hemodialysis and peritoneal dialysis remain viableoptions for those patients who require renal replacementbut are not critically ill.
Progression to Chronic Kidney Disease andFollow-up
Recent literature has indicated that critically ill childrenwho are discharged after an episode of AKI are at in-creased risk of chronic kidney disease later in life. (10)(11) Long-term follow-up of these patients is important.The optimal follow-up plan for these children is not clear.In more severe cases of AKI that require renal replacementtherapy, follow-up should initially be with specialists. Inmilder cases, one may consider yearly blood pressurechecks and urinalysis.
nephrology acute kidney injury
38 Pediatrics in Review Vol.35 No.1 January 2014

References1. Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK,Jefferson LS, Goldstein SL. Modi!ed RIFLE criteria in criticallyill children with acute kidney injury. Kidney Int. 2007;71(10):1028–10352. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P; AcuteDialysis Quality Initiative workgroup. Acute renal failure - de!nition,outcome measures, animal models, "uid therapy and informationtechnology needs: the Second International Consensus Conference ofthe Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204–R2123. Mehta RL, Kellum JA, Shah SV, et al; Acute Kidney InjuryNetwork. Acute Kidney Injury Network: report of an initiative toimprove outcomes in acute kidney injury. Crit Care. 2007;11(2):R314. Kidney Disease: Improving Global Outcomes (KDIGO)Acute Kidney Injury Work Group. KDIGO clinical practiceguideline for acute kidney injury. Kidney Int Suppl. 2012;2(8):1–1385. Hui-Stickle S, Brewer ED, Goldstein SL. Pediatric ARF epide-miology at a tertiary care center from 1999 to 2001. Am J KidneyDis. 2005;45(1):96–1016. Basu RK, Chawla LS, Wheeler DS, Goldstein SL. Renal angina:an emerging paradigm to identify children at risk for acute kidneyinjury. Pediatr Nephrol. 2012;27(7):1067–10787. Pediatric Advanced Life Support Provider Manual. Dallas, Texas:American Academy of Pediatrics, American Heart Association;20118. Goldstein SL, Currier H, Graf Cd, Cosio CC, Brewer ED,Sachdeva R. Outcome in children receiving continuous venovenoushemo!ltration. Pediatrics. 2001;107(6):1309–13129. Sutherland SM, Zappitelli M, Alexander SR, et al. Fluidoverload and mortality in children receiving continuous renalreplacement therapy: the prospective pediatric continuous renalreplacement therapy registry. Am J Kidney Dis. 2010;55(2):316–32510. Mammen C, Al Abbas A, Skippen P, et al. Long-term risk ofCKD in children surviving episodes of acute kidney injury in theintensive care unit: a prospective cohort study. Am J Kidney Dis.2012;59(4):523–53011. Askenazi DJ, Feig DI, Graham NM, Hui-Stickle S, GoldsteinSL. 3-5 year longitudinal follow-up of pediatric patients after acuterenal failure. Kidney Int. 2006;69(1):184–189
Summary• On the basis of research evidence and consensus, the
term acute kidney injury (AKI) has replaced acuterenal failure, suggesting the spectrum of kidneydamage that can occur (Table 1). (1)(2)(3)(4)
• On the basis of research evidence, in developingcountries the most common causes of AKI continue to bevolume depletion, infections, and primary renal diseases.
• On the basis of research evidence and expert opinion,in developed countries volume depletion and primaryrenal disease remain common causes of AKI inpreviously healthy children.
• On the basis of research evidence, in hospitalizedchildren, particularly in tertiary care centers, there hasbeen a shift in the etiology of AKI from primary renaldisease to secondary causes of AKI that are oftenmultifactorial in nature and often complicate anotherdiagnosis or its treatment (heart disease, sepsis, andnephrotoxic drug exposure). (1)(5)
• On the basis of expert opinion, an ordered approach tothe diagnosis of AKI divides the potential origins intoprerenal, intrinsic renal, and postrenal causes.
• On the basis of research evidence, expert opinion, andconsensus, patients with AKI are subject to a numberof fluid and electrolyte disturbances, includinghypervolemia, dysnatremias, hyperkalemia, acidosis,and hyperphosphatemia.
• On the basis of research evidence, expert opinion, andconsensus, indications for renal replacement therapyinclude volume overload (10%-20% fluid excess),acidosis, hyperkalemia, uremia (typically blood ureanitrogen >100 mg/dL [>35.7 mmol/L] orsymptomatic), or an inability to provide adequatenutrition in patients with renal dysfunction. (8)(9)
• On the basis of research evidence and expert opinion,recent literature has reported that critically ill childrenwho are discharged after an episode of AKI are atincreased risk for chronic kidney disease later in life.Long-term follow-up of these patients is important, butthe optimal follow-up plan remains unclear. (10)(11)
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 39
PIR Quiz RequirementsTo successfully complete 2014 Pediatrics in Review articles for AMA PRA Category 1 CreditTM, learners must demonstrate a minimum performancelevel of 60% or higher on this assessment, which measures achievement of the educational purpose and/or objectives of this activity. If you scoreless than 60% on the assessment, you will be given additional opportunities to answer questions until an overall 60% or greater score is achieved.NOTE: Learners can take Pediatrics in Review quizzes and claim credit online only at: http://pedsinreview.org.
1. An 8-month-old, 8-kg infant is brought in by his parents to the emergency department because of reduced urineoutput after viral gastroenteritis. On examination, the patient is mildly tachycardic and has dry mucous membranes butnormal capillary refill. You prescribe oral rehydration but admit the patient for observation andmonitor urine output for12 hours. Of the following, which criterion would be sufficient to diagnose acute kidney injury in this infant?
A. Serum creatinine level of 0.4 mg/dL (35 mmol/L) on baseline assessment.B. Urine output of 150 mL in 12 hours.C. Blood urea nitrogen level of 12 mg/dL (4.3 mmol/L) after 12 hours of observation.D. Urine output of 40 mL in 12 hours.E. Blood urea nitrogen level of 15 mg/dL (5.4 mmol/L) at baseline assessment.
2. You are evaluating a male newborn in the nursery. The neonatal nurse notes reduced urine output in the first12 hours of life. On reviewing the medical record, you note that child had a prenatal ultrasonogram thatdemonstrated an enlarged bladder. Of the following, which diagnosis best explains the findings above?
A. Infantile nephrotic syndrome.B. Juvenile nephronophthisis.C. Posterior urethral valves.D. Renal artery stenosis.E. Ureteropelvic junction obstruction.
3. A patient with cystic fibrosis is transferred to the intensive care unit with pneumonia and respiratory distress.Previously, the patient had received ketorolac and tobramycin. In the intensive care unit, you documenta markedly reduced urine output. Of the following, which finding is more consistent with intrinsic acute kidneyinjury as opposed to prerenal azotemia?
A. Blood urea nitrogen to creatinine ratio of 25.B. Fractional excretion of sodium of 0.5%.C. Urine osmolality of 800 mOsm/kg (800 mmol/kg).D. Urine sodium of 60 mEq/L (60 mmol/L).E. Urine specific gravity of 1.030.
4. A 12-year-old boy has been admitted to the ward for abdominal pain and a creatinine level of 2.0 mg/dL (177mmol/L). He underwent a liver transplantation 1 year ago and since that time has had multiple admissions forinfection and rejection. He is taking several medications. On examination, he is in no acute distress, althoughhe has mild jaundice. Laboratory studies demonstrate the following: creatinine, 2.0 mg/dL (177mmol/L); bloodurea nitrogen, 20 mg/dL (7.1 mmol/L); alanine aminotransferase, 80 U/mL; hematocrit, 37% (0.37); and whiteblood count, 8,900/mL (8.9 3 109/L). His urine sodium level is 60 mEq/L (60 mmol/L), and urine microscopyreveals granular casts. Of the following, which medication is most likely to cause the presentation above?
A. Azathioprine.B. Cyclosporine.C. Fluconazole.D. Furosemide.E. Prednisone.
5. An 8-year-old girl presents with headache and reddish urine. On further questioning, you note she hada respiratory infection and sore throat 3 weeks ago, but the symptoms resolved and she never came in forevaluation. On examination of the urine, you note gross hematuria. Microscopic examination demonstrates red
nephrology acute kidney injury
40 Pediatrics in Review Vol.35 No.1 January 2014

blood cell casts. Of the following tests, which would be the most consistent with a diagnosis ofpoststreptococcal glomerulonephritis?
A. Low blood urea nitrogen level.B. Low C3 level.C. Low C4 level.D. Low urine sodium level.E. Low serum IgA level.
nephrology acute kidney injury
Pediatrics in Review Vol.35 No.1 January 2014 41
Related Documents