Acute care toolkit 12 Acute kidney injury and intravenous fluid therapy

Acute care toolkit 12 Acute kidney injury and intravenous fluid therapy.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Acute care toolkit 12Acute kidney injury and intravenous fluid therapy
Definition and staging of AKI
• The term ‘acute kidney injury’ (AKI) replaces the term ‘acute renal failure’
• Even seemingly minor changes in serum creatinine levels are associated with a significant increase in mortality
• AKI should be regarded as a spectrum of injury that may progress to organ failure
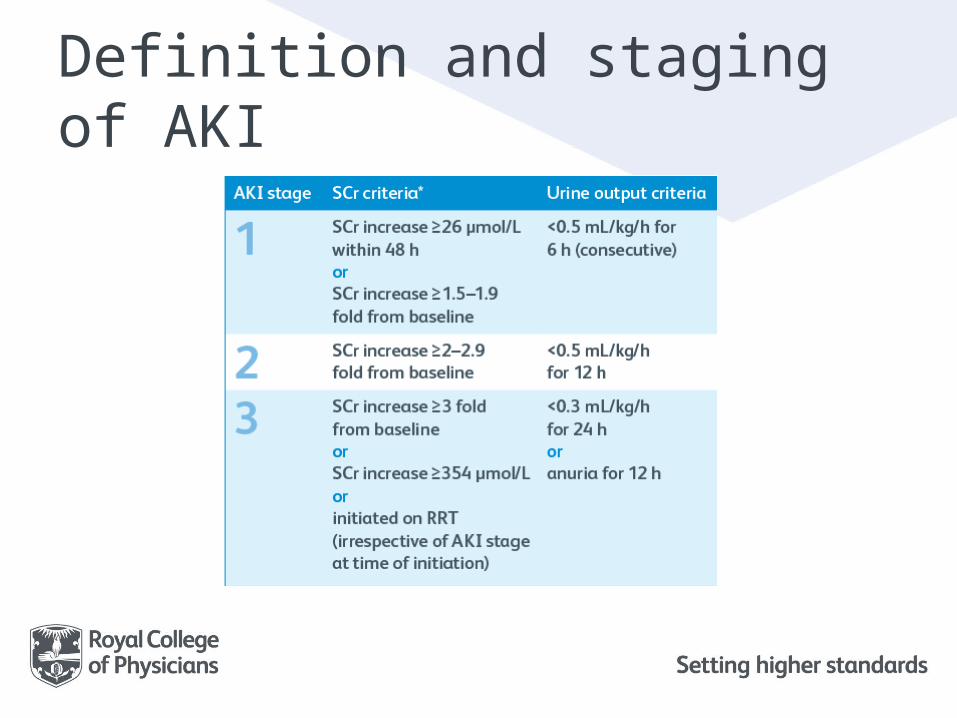
Definition and staging of AKI
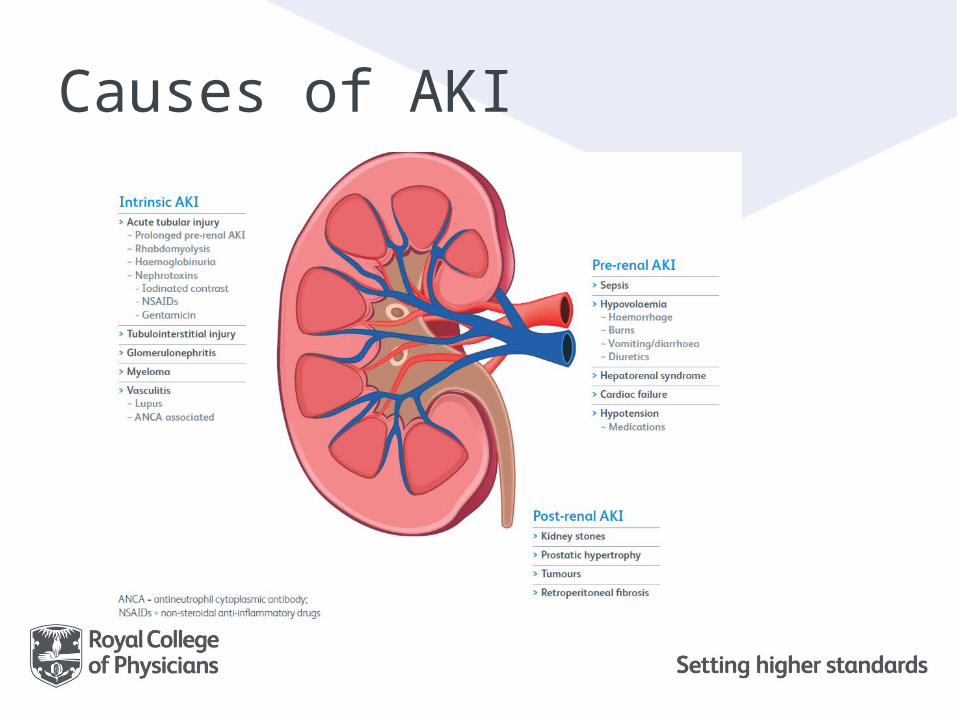
Causes of AKI

Risk factors for AKI• AKI occurs most commonly in patients who are
at risk, who either are acutely ill or have had major surgery
• Recognition of those at risk of AKI allows simple preventative measures, eg ensuring adequate hydration
• Patients at risk of AKI should be aware of the risk of AKI developing in certain situations and actions to be taken, eg temporary cessation of drugs that may exacerbate hypovolaemia and/or hypotension
AKI warning systems• In March 2015, NHS England mandated that all
NHS trusts in England must have biochemistry department laboratory systems that issue an AKI warning, based on rises in serum creatinine level, for patients in secondary care
• Each trust must determine how they communicate this AKI warning to clinicians caring for individual patients, eg e-alerts, AKI care bundles, AKI outreach teams
Recognised risk factors for AKI• Age >75 years• Pre-existing CKD (eGFR <60 mL/kg/1.73 m2)• Previous episode of AKI• Debility and dementia• Heart failure• Liver disease• Diabetes mellitus• Hypotension (Mean arterial pressure <65 mmHg,
systolic pressure <90 mmHg)• Sepsis• Hypovolaemia• Nephrotoxins, eg gentamicin, NSAIDs, iodinated contrast• Antihypertensives in setting of hypotension, eg ACE inhibitors,
loop diuretics
Initial investigation of AKI• Urea and electrolytes, and creatinine• Bicarbonate• Full blood count – if platelets low, request blood film/
lactate dehydrogenase (to diagnose haemolytic uraemic syndrome/ thrombotic thrombocytopenic purpura)
• Liver function tests (to diagnose hepatorenal syndrome)• Ca2+/PO4
3– (to diagnose myeloma)• Creatine kinase (to diagnose myeloma)• Blood cultures (if sepsis suspected)• Urinalysis – if blood, protein, leucocytes or nitrites, send midstream
urine• Ultrasound scan of renal tract and bladder
– if obstruction expected, scan within 24 h– if pyonephrosis suspected, scan within <6 h
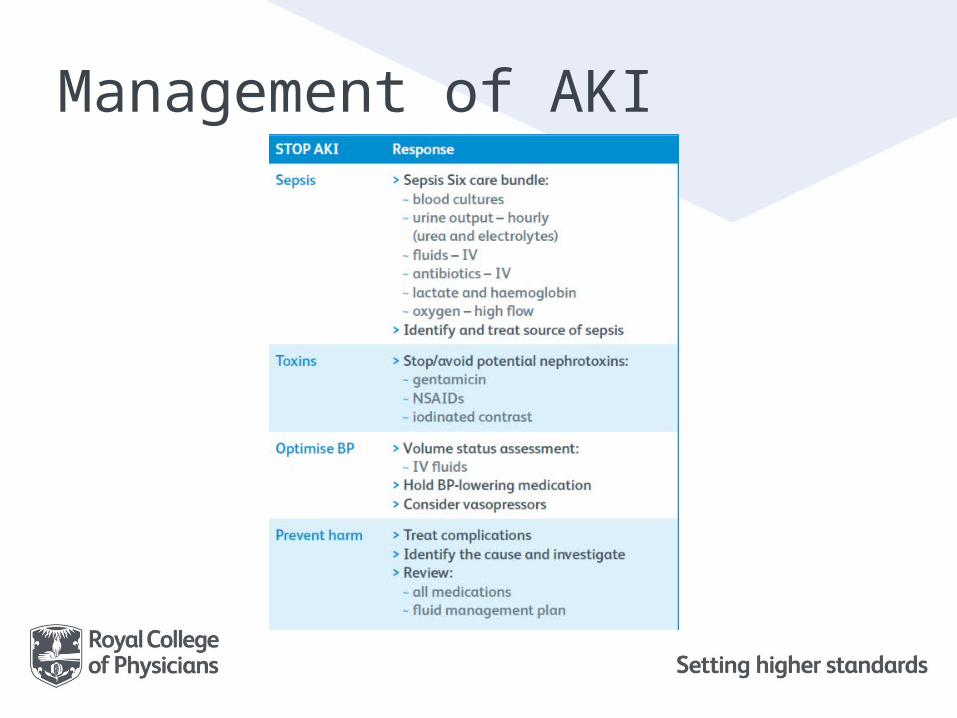
Management of AKI
Intravenous (IV) fluid therapy
• Any dehydrated patient is at risk of AKI, particularly in the setting of acute illness
• For any patient who is fasting for over 12 h or in whom losses of fluid cannot be matched by parenteral intake, parenteral fluids must be commenced
Assessing fluid status
Prior to any prescription of IV fluids, the patient should have a volume assessment that includes the following parameters
Classification of IV fluid therapy
• NICE recommends that assessment of a patient’s fluid balance should be part of every ward round
• It also recommends that IV fluid therapy is classified as resuscitation, replacement or routine maintenance, and that any prescription should clearly identify which type of IV fluid therapy the patient is receiving
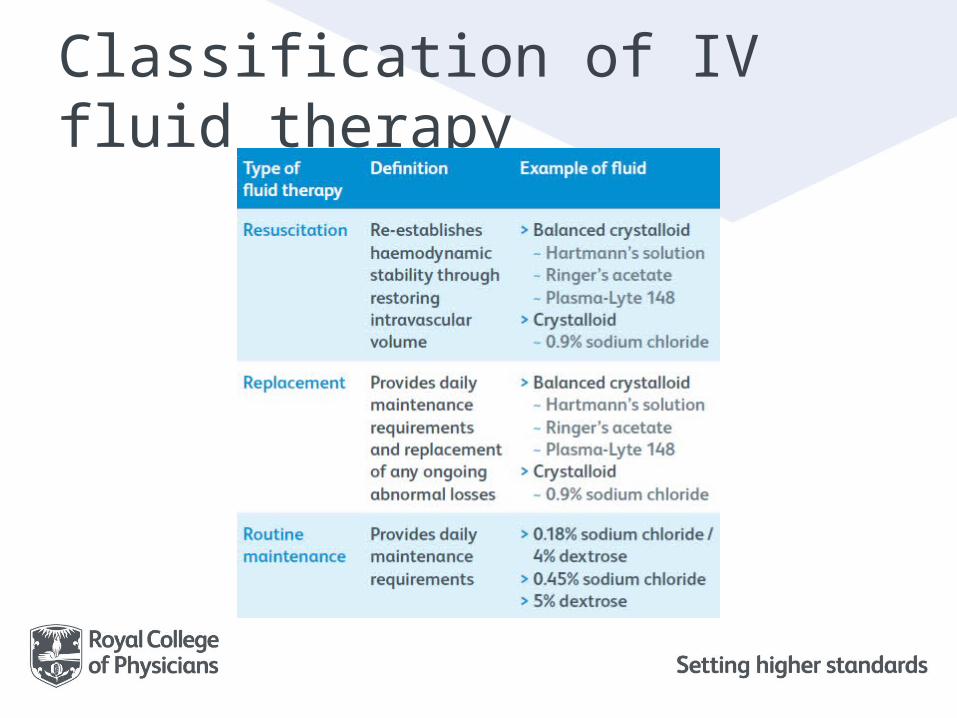
Classification of IV fluid therapy
Initial fluid resuscitation• NICE recommends that fluid resuscitation is best
approached with a crystalloid solution rather than a colloid
• Moat experts would recommend a balanced crystalloid (eg Hartmann’s, lactated Ringer’s or Plasma-Lyte 148), because excessive amounts of 0.9% sodium chloride can result in hyperchloraemic metabolic acidosis
• The only exception is rhabdomyolysis, when 0.9% sodium chloride would be preferred initially because of the risk of hyperkalaemia
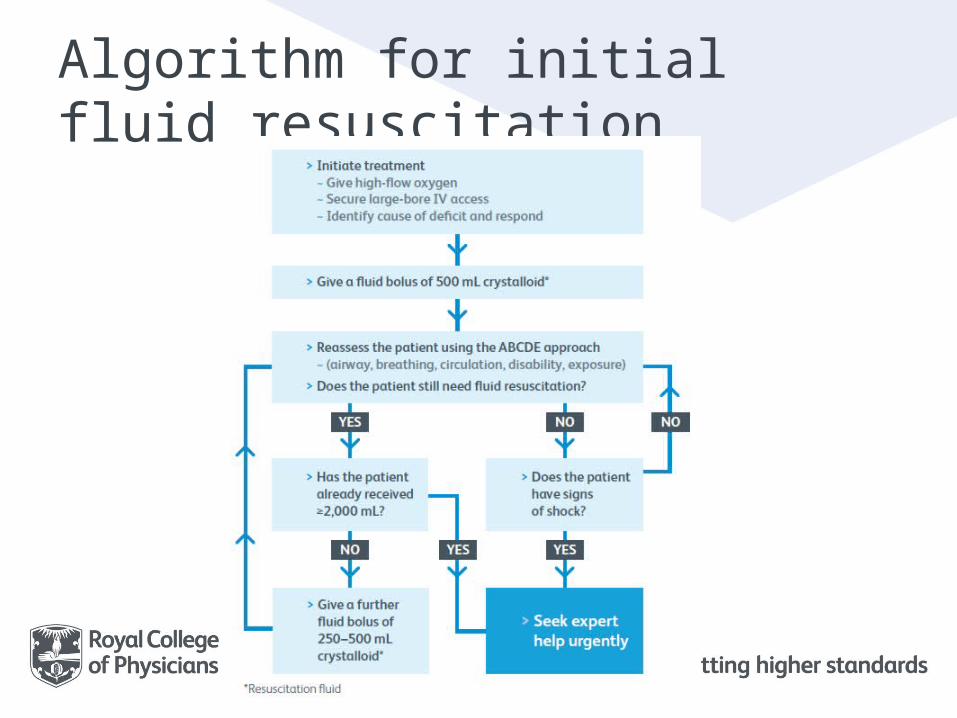
Algorithm for initial fluid resuscitation

Composition of IV fluids
It is important to know the electrolyte content of fluid prescribed

IV fluid challenges
• An IV cannula of adequate size to infuse the fluid at a high enough rate must be used (usually at least a 20G cannula and infusion of 250–500 mL over 5–15 minutes)
• Responsiveness to the fluid challenge should be assessed by regular monitoring of blood pressure and pulse rate
Responding to the fluid challenge• If there is an improvement in either blood
pressure or pulse rate that is poorly sustained, the fluid challenge should be repeated
• If haemodynamic stability is restored and the patient is deemed euvolaemic, the type of IV fluid prescribed should be reviewed
• If there is no improvement after two accurately performed fluid challenges, the patient should be reviewed and, when appropriate, their care should be escalated for senior review and possible involvement of critical care

Routine maintenance IV fluids• Rules for prescribing routine maintenance
IV fluid therapy include:– IV fluid should be given via volumetric pump if a
patient is on fluids for over 6 h or if the fluid contains potassium
– Always prescribe as mL/h, not ‘x hourly’ bags– Never give maintenance fluids at more than
100 mL/h– Never prescribe fluids for more than 24 h at a time
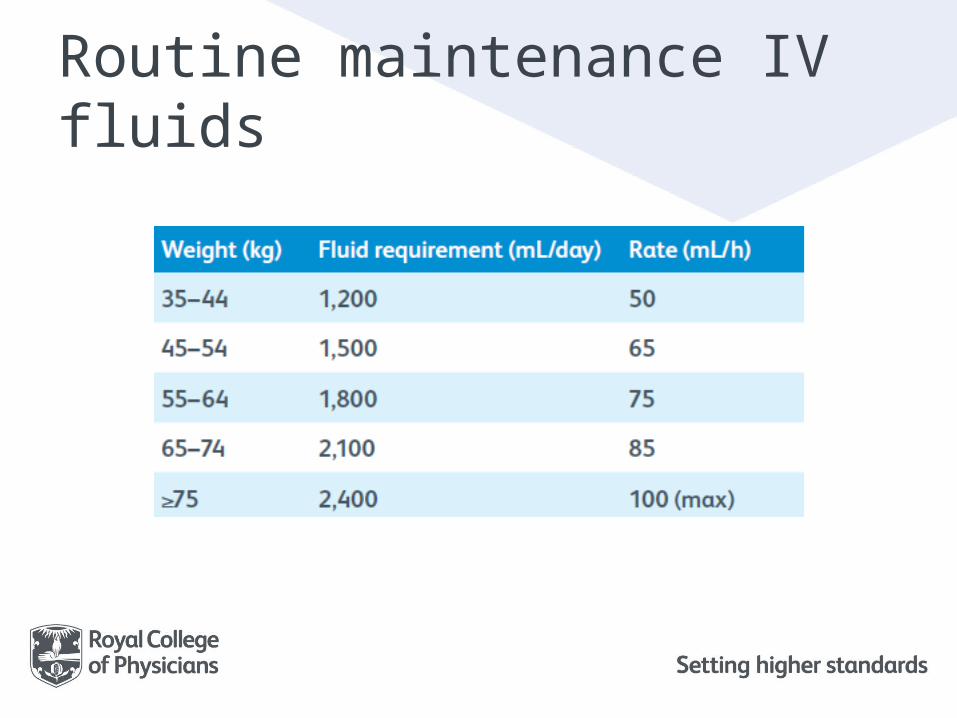
Routine maintenance IV fluids
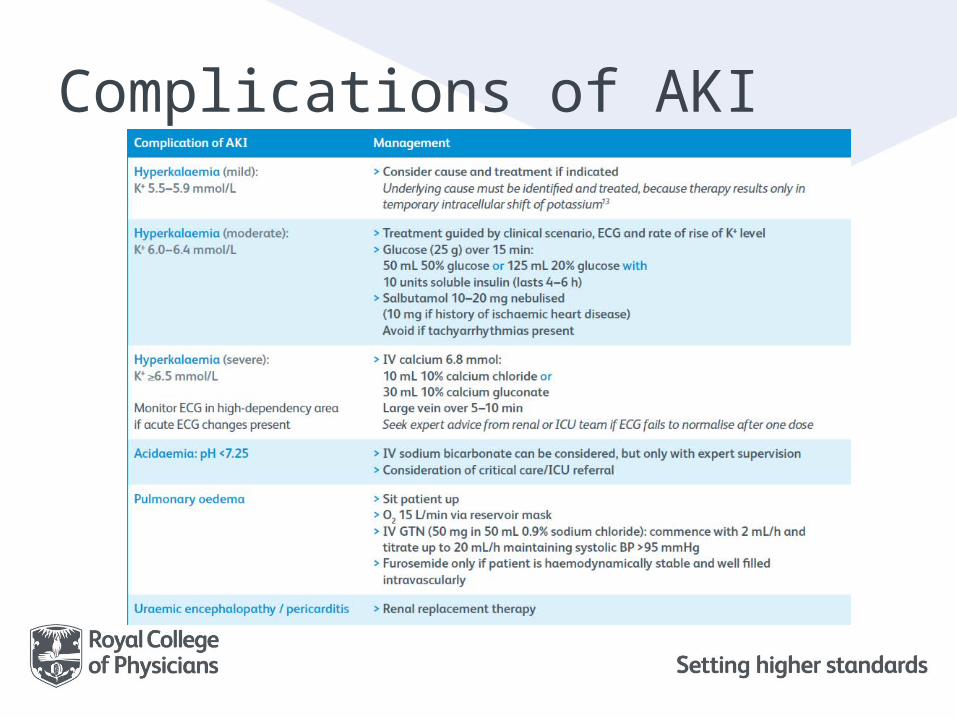
Complications of AKI

Referring to a nephrologist• Management of AKI should be discussed with a
nephrologist as soon as possible, and within 24 h of detection when one or more of the following is present– A possible diagnosis that may necessitate specialist
treatment (eg vasculitis, glomerulonephritis, tubulointerstitial nephritis or myeloma)
– AKI with no clear cause– Inadequate response to treatment– Complications associated with AKI– AKI stage 3– A renal transplant– Chronic kidney disease (CKD) stage 4 or 5
Patient recovery• Patients recovering from a significant episode of
AKI may develop profound diuresis, resulting in a free water deficit, hypernatraemia and/or hypokalaemia
• During this phase, maintaining patient hydration and replacing electrolytes are of paramount importance
• Accurate fluid balance with daily weights is very important to prevent patients from becoming dehydrated as they recover from AKI
Discharge planning• Patients who have had AKI are at risk of developing CKD in the long
term (this risk depends on the severity of the episode of AKI)• Patients’ kidney function should be checked prior to discharge• Refer patients to nephrology if they are discharged with an eGFR
<30 mL/min/1.73 m2
• Medications should be reviewed prior to discharge, with a plan to reintroduce medications that may have been held during the acute illness (this may require an early follow-up with the patient’s GP)
• Discharge letters to the GP should include:– severity of AKI– cause of AKI– risk factors for AKI– kidney function on discharge– advice on whether medications need to be reviewed or reintroduced
Educational resources• An app developed by the Royal College of
Physicians of Edinburgh that is free to download www.rcpe.ac.uk/policy-standards/acute-kidney-injury-app
• An AKI core competency framework for healthcare professionals, endorsed by the Academy of Medical Royal Collegeswww.aomrc.org.uk/doc_details/9503-acute-kidney-injury-a-competency-framework
• The RRAPID app and e-book, which contain an AKI risk calculator and a NEWS calculatorhttp://rrapid.leeds.ac.uk
The RCP produces a series of acute care toolkits on a range of topics including
All the toolkits, including the full version of Acute toolkit 12: Acute kidney injury and intravenous fluid therapy, can be accessed atwww.rcplondon.ac.uk/resources/acute-care-toolkits

Related Documents











