ACID-BASE BALANCE & DISORDERS
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Water is the solvent of life.
Functions of Water:
Provides aqueous medium to organisms.
Water directly participates as a reactant in
several metabolic reactions.
Vehicle for transport of solutes.
Associated with regulation of body
temperature.
Distribution of Water:
Adult human body contains about 60% (42
litres) water.

Distributed in intracellular (28L) & extra
cellular (14L) compartments.
Water turnover and Balance:
Water intake:
Water is supplied to the body by
Exogenous Water.
Endogenous Water.
Ingested water & water content of solid
foods constitute the exogenous source of
water.
Ingestion of water is mainly controlled by
thirst centre located in the hypothalamus.
The metabolic water produced within the
body is the endogenous water.
This water (300-350 ml/day) is derived from the
oxidation of foodstuffs.
The elimination of water from the body
occurs through
Urine
Skin,
Lungs
Feces.

Electrolytes are the compounds which readily
dissociate in solution & exist as ions i.e.
positively & negatively charged particles.
Electrolytes are well distributed in the body
fluids in order to maintain the osmotic
equilibrium and water balance.

Cations:
Na+ =142
K+ =5
Ca2+ =5
Mg2+ =3
Total =155
Anions:
Cl- =103
HCO3- =27
HPO42- =2
SO42- =1
Proteins =16
Organic acids =6
Total =155
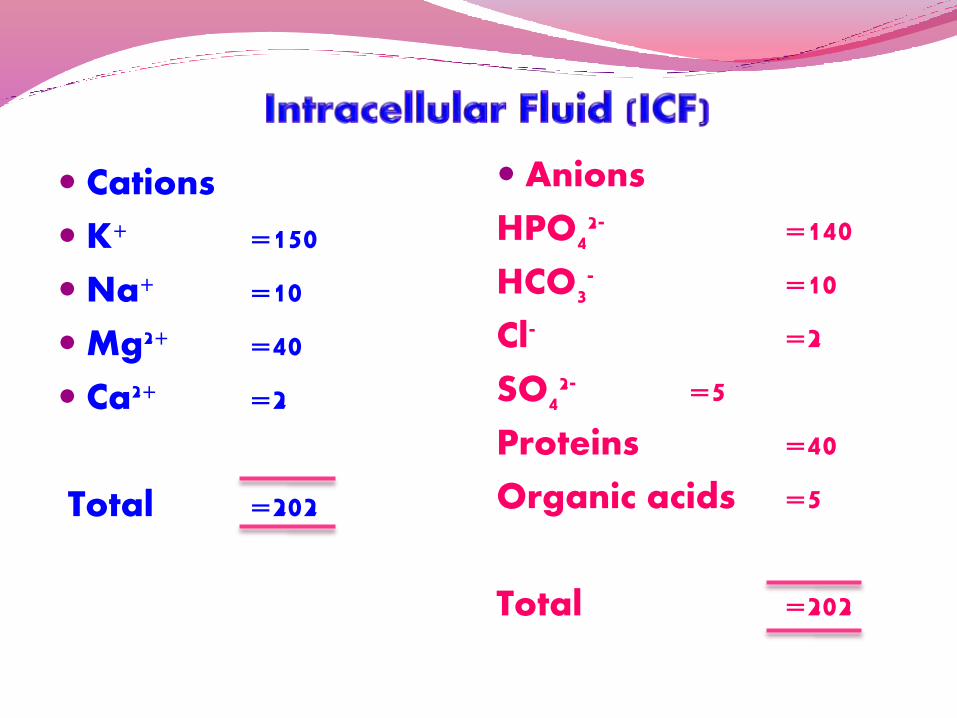
Cations
K+ =150
Na+ =10
Mg2+ =40
Ca2+ =2
Total =202
Anions
HPO42- =140
HCO3- =10
Cl- =2
SO42- =5
Proteins =40
Organic acids =5
Total =202
Na+ is the principal extracellular cation.
K+ is the intracellular cation.
Osmolarity:
The number of moles per liter of solution.
Osmolality:
The number of moles per kg of solvent.
Electrolyte & water balance are regulated
together.
Kidneys plays an important role.
Role of Hormones:
Aldosterone:
It is a mineralocorticoid produced by
adrenal cortex.
Aldosterone increases Na+ reabsorption by
renal tubules at the expense of K+ and H+
ions.
The net effect is the retention of Na+ to the
body.
An increase in the plasma osmolality
stimulates hypothalamus to release ADH.
ADH increases water reabsorption by renal
tubules.
The secretion of aldosterone is controlled by
renin-angiotensin system
Decrease in blood pressure is sensed by
juxtaglomerular apparatus of the nephron
which secrete renin.
Renin acts on angiotensinogen to produce
angiotensin I.
Angiotensin I is converted to Angiotensin II
which stimulates the release of aldosterone.
Aldosterone & ADH coordinate with each
other to maintain the normal fluid and
electrolyte balance.
Characterized by water depletion in the body.
It may be due to insufficient intake or
excessive water loss or both.
Causes of dehydration:
Occur as a result of diarrhea, vomiting,
excessive sweating, fluid loss in burns,
adrenocortical dysfunction, kidney diseases &
deficiency of ADH.
Acids:
Acid is a substance whose dissociation in
water releases hydrogen ions (H+)
Addition of an acid to a solution, increases
concentration of free H+ in the solution.
Produces more acidic solution & decrease in
pH

HCL H+ + Cl-
Bases:
A base releases hydroxyl ions (OH-) in aqueous
solution & decreases its H+ concentration by accepting
or by binding with free H+.
This results in increase in pH of the solution.
NaOH Na+ + OH-
The OH-, accepts H+ & results in the formation of water.
Some substances, such as amino acids &
proteins, act acids as well as bases.
These substances are referred to as
Amphoteric substances.

The normal pH of the blood is maintained in
the narrow range of 7.35 - 7.45 (slightly
alkaline).
The body has developed three lines of
defense to regulate the body’s acid-base
balance.
Blood buffers
Respiratory mechanism
Renal mechanism
Blood buffers:
A buffer may be defined as a solution of a
weak acid & its salt with a strong base.
The buffer resists the change in the pH by the
addition of acid or alkali & the buffering
capacity is dependent on the absolute
concentration of salt & acid.
The buffer cannot remove H+ ions from the
body but it temporarily acts as a shock
absorbant to reduce free H+ ions.
Bicarbonate buffer
Phosphate buffer
Protein buffer
Bicarbonate buffer system:
Sodium bicarbonate & carbonic acid (NaHCO3-
H2CO3) is the most predominant buffer system
of ECF (plasma).
Carbonic acid dissociates into hydrogen and
bicarbonate ions.
H2CO3 H+ + HCO3-
By the law of mass action
Ka= -------(1)
Ka=Dissociation constant of H2CO3.
(H+) (HCO3-)
H2CO3

The equation may be rewritten as follows
= Ka -------(2)
pH=log1/H+
By taking the reciprocals & logarithms.
log1/H+ = log1/Ka + log -------(3)
(H+)(H2CO3)
(HCO3-)
HCO3-
(H2CO3)
Log1/Ka = pKa
The equation 3 may now written as
pH = pKa + log --------(4)
The above equation is referred as Henderson
– Hasselbalch equation for any buffer.
pH = pKa + log
(H2CO3)
(HCO3-)
(Acid)
(Base)
The plasma bicarbonate (HCO3-) concentration
is around 24 mmol/l (range 22-26 mmol/l).
Carbonic acid is a solution of CO2 in water.
Its concentration is given by the product of
pco2 (arterial partial pressure of CO2 = 40 mm
Hg) & the solubility constant of CO2 (0.03).

Thus H2CO3 = 40 x 0.03 = 1.2 mmol/l.
The Henderson-Hasselbalch equation for
bicarbonate buffer is
(H2CO3)
(HCO3-)pH = pKa + log
Substituting the values (blood pH = 7.4, pKa
for H2CO3 = 6.1; HCO3- = 24 mmol/l; H2CO3- = 1.2
mmol/l.
7.4 = 6.1 + log 24/1.2
= 6.1 + log 20
= 6.1 + 1.3
= 7.4
The blood pH 7.4, the ratio of bicarbonate to
carbonic acid is 20 : 1
The bicarbonate concentration is much higher
(20 times) than carbonic acid in the blood.
This is referred to as alkali reserve.
Sodium dihydrogen phosphate and
disodium hydrogen phosphate (NaH2PO4-
Na2HPO4) constitute the phosphate buffer
It is mostly an Intracellular buffer.
The plasma proteins & hemoglobin, constitute
the protein buffer.
The buffering capacity of proteins is
dependent on the pK of ionizable groups of
amino acids.
The imidazole group of histidine (pK=6.7) is
the most effective contributor of protein
buffer.
Respiratory system provides a rapid
mechanism for the maintenance of acid-base
balance.
This is achieved by regulating the
concentration of carbonic acid (H2CO3) in the
blood.
The large volumes of CO2 produced by the
cellular metabolic activity endanger the acid-
base equilibrium of the body.
All of this CO2 is eliminated from the body in
the expired air via the lungs
H2CO3 CO2 + H2O Carbonic anhydrase
The rate of respiration is controlled by a
respiratory centre, located in the medulla of
the brain
This centre is highly sensitive to changes in the
pH of blood.
Decrease in blood pH causes hyperventilation
to blow off co2 & reducing the H2CO3
concentration.
H+ ions are eliminated as H2O
Respiratory control of blood pH is rapid but
only a short term regulatory process, since
hyperventilation cannot proceed for long.
Hemoglobin binds to H+ ions & helps to
transport CO2 as HCO3- with a minimum change
in pH.
In the lungs, hemoglobin combines with O2, H+
ions are removed which combine with HCO3- to
form H2CO3 & is dissociates to release CO2 to be
exhaled.
Due to lack of aerobic metabolic pathways,
RBC produce very little CO2.
The plasma CO2 diffuses into RBC along the
concentration gradient, it combines with water
to form H2CO3 by Carbonic anhydrase.
In RBC, H2CO3 dissociates to produce H+ & HCO3-
The H+ ions are buffered by Hemoglobin.
As the concentration of HCO3- increases in the
RBC, it diffuses into plasma along with
concentration gradient, in exchange for Cl-
ions, to maintain electrical neutrality.
This is referred to as chloride shift, helps to
generate HCO3- .

Erythrocyte
CO2 + H2O
CAH2CO3
HHb
HCO3- + H+ Hb
Cl-
Plasma
CO2
HCO3-
Cl-
The kidneys plays an important role in the
regulation of pH
Normal urine has a pH around 6.
The pH of the urine vary from 4.5 to 9.8.
Excretion of H+ ions
Reabsorption of Bicarbonate
Excretion of titratable acid
Excretion of ammonium ions
Kidney is the only route through which the H+
can be eliminated from the body.
H+ excretion occurs in the proximal
convoluted tubules & is coupled with
generation of HCO3-.
Carbonic anhydrase catalyses the production
of carbonic acid (H2CO3) from CO2 & H2O in
renal tubular cells.
H2CO3 then dissociates to H+ & HCO3-
H+ ions are secreted into tubular lumen in
exchange for Na+
Na+ in association with HCO3- is reabsorbed into
blood
An effective mechanism to eliminate acids (H+)
from the body with a simultaneous generation of
HCO3-
H+ combines with non-carbonate base & excreted.
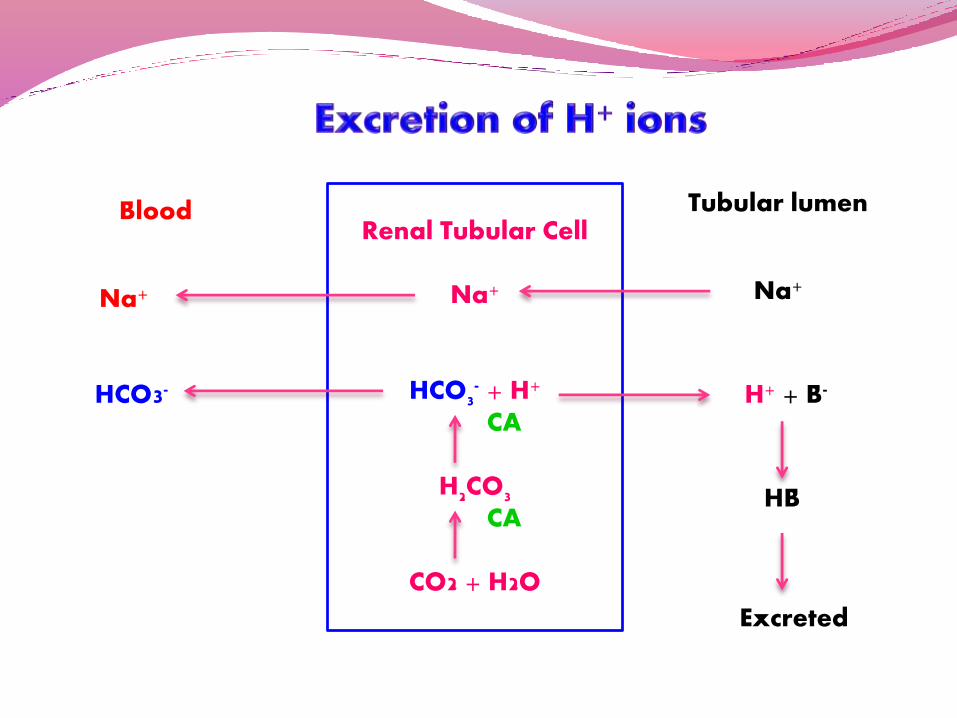
Renal Tubular Cell
Na+
HCO3- + H+
CA
H2CO3
CA
CO2 + H2O
Blood
Na+
HCO3-
Na+
H+ + B-
HB
Excreted
Tubular lumen
This mechanism is responsible to conserve blood
HCO3-, with simultaneous excretion of H+ ions.
Bicarbonate freely diffuses from plasma into
tubular lumen.
HCO3- combines with H+, secreted by tubular cells,
to form H2CO3.
H2CO3 is then cleaved to form CO2 and H2O.

As the CO2 concentration builds up in the
lumen, it diffuses into the tubular cells along
the concentration gradient.
In the tubular cell, CO2 again combines with
H2O to form H2CO3 which then dissociates into
H+ & HCO3-
The H+ is secreted into the lumen in exchange
for Na+.
The HCO3- is reabsorbed into plasma in
association with Na+.
Reabsorption of HCO3- is a cyclic process with
the net excretion of H+ or generation of new
HCO3-
This mechanism helps to maintain the steady
state & will not be effective for the elimination
of H+ or generation of new HCO3- .

Renal Tubular Cell
Na+
HCO3- + H+
H2CO3
CA
H2O + CO2
Blood
Na+
HCO3-
Na+
Tubular lumen
H+
HCO3-
Plasma
H2CO3
CO2 + H2O
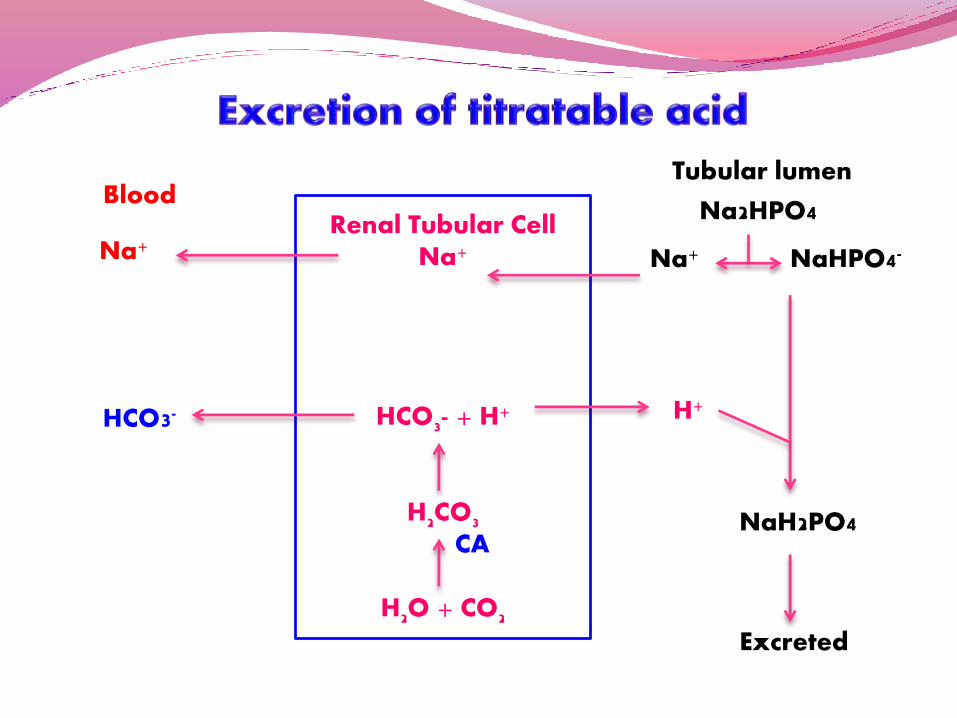
Titratable acidity is a measure of acid
excreted into urine by the kidney.
Titratable acidity refers to the number of
milliliters of N/10 NaOH required to titrate
1liter of urine to pH 7.4.
Titratable acidity reflects the H+ ions excreted
into urine.
H+ ions are secreted into the tubular lumen in
exchange for Na+ ion.
This Na+ is obtained from the base, disodium
hydrogen phosphate (Na2HPO4).
This combines with H+ to produce the acid,
sodium dihydrogen phosphate (NaH2PO4), in
which form the major quantity of titratable
acid in urine is present.

Tubular fluid moves down the renal tubules,
more and more H+ ions are added, resulting
in the acidification of urine.
Causes a fall in the pH of urine as low as 4.5.
Renal Tubular CellNa+
HCO3- + H+
H2CO3
CA
H2O + CO2
Blood
Na+
HCO3-
Na+
Tubular lumen
H+
Na2HPO4
NaHPO4-
NaH2PO4
Excreted
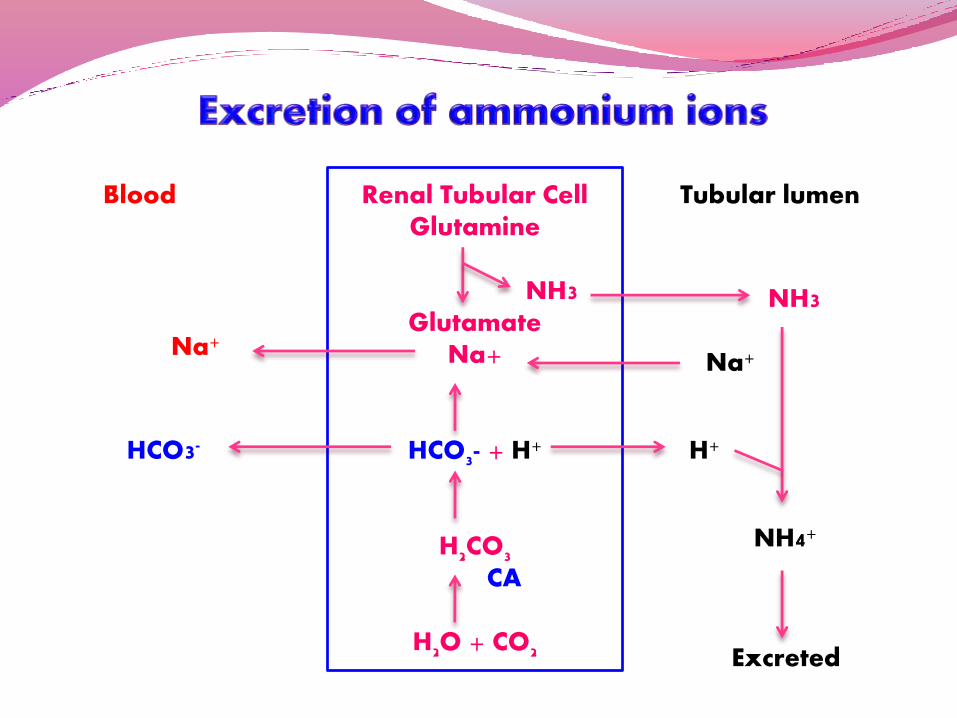
The H+ ion combines with NH3 to form
ammonium ion (NH4+).
The renal tubular cells deaminate glutamine
to glutamate and NH3 by the action of
enzyme glutaminase.
The liberated NH3 diffuses into the tubular
lumen where it combines with H+ to form
NH4+.
Ammonium ions cannot diffuse back into
tubular cells and excreted into urine.
Renal Tubular CellGlutamine
NH3 Glutamate
Na+
HCO3- + H+
H2CO3
CA
H2O + CO2
Blood
Na+
HCO3-
Na+
Tubular lumen
H+
Excreted
NH3
NH4+

The acid-base disorders are mainly two
types
Acidosis-a decline in blood pH.
Metabolic acidosis-due to a decrease in
bicarbonate
Respiratory acidosis-Due to an increase in
carbonic acid.
Alkalosis-a rise in blood pH.
Metabolic alkalosis-due to an increase in
bicarbonate.
Respiratory alkalosis-due to a decrease in
carbonic acid.
Metabolic acidosis:
Occur due to DM (ketoacidosis).
Lactic acidosis & renal failure.
Respiratory acidosis:
Severe asthama
Cardiac arrest
Metabolic alkalosis:
Vomiting
Hypokalemia
Respiratory alkalosis- due to
Hyperventilation
Severe anemia

The total concentration of cations & anions is
equal in the body fluids.
It is required to maintain electrical neutrality.
The commonly measured electrolytes are Na+,
K+, Cl- & HCO3-.
Na+ & K+ together constitute about 95% of the
plasma cations.
Cl- & HCO3- are the major anions, contributing
to about 80% of plasma anions.
The remaining 20% of plasma anions include
proteins, phosphate, sulfate, urate and
organic acids.
Anion gap is defined as the difference
between the total concentration of measured
cations (Na+ & K+) and that of measured anion
(Cl- & HCO3-).
The anion gap (A-) in fact represents the
unmeasured anions in the plasma which may
be calculated as follows, by substituting the
normal concentration of electrolytes (mEq/l).
Na+ + K+ = Cl- + HCO3- + A-
136 + 4 = 100 + 25- + A-
A- = 15 mEq/l
• Anion gap in healthy individual is 15 mEq/l.
• Acid-Base disorders associated with alteration in
anion gap.

Reduction in bicarbonate leads to fall in blood
pH.
This is due to excessive production of organic
acids which can combine with NaHCO3- and
deplete the alkali reserve
NaHCO3- + Organic acid Na salts of
organic acids + CO2
Commonly seen in DM.

The primary defect is due to a retention of CO2
(Increased H2CO3)
Causes for respiratory acidosis are
depression of respiratory centre, pulmonary
disorders & breathing air with high content of
CO2
This is due to increase in HCO3- concentration
Occur due to excessive vomiting or an
excessive intake of sodium bicarbonate for
therapeutic purposes.
Respiratory mechanism initiates
compensation by hypoventilation to retain
CO2, this is taken over by renal mechanism
which excrete more HCO3- and retain H+
This is due to decrease in H2CO3
concentration.
This is due to prolonged hyperventilation
resulting in increased exhalation of CO2 by
the lungs
Renal mechanism tries to compensate by
increasing the urinary excretion of HCO3-
Plasma potassium concentration (normal 3.5-
5.0 mEq/l) is very important as it affects the
contractility of the heart.
Hyperkalemia (high plasma K+) or
hypokalemia (low plasma K+) can be life-
threatening.

Insulin increases K+ uptake by cells.
The patient of severe uncontrolled diabetes (i.e. with
metabolic acidosis) is usually with hypokalemia.
When such a patient is given insulin, it stimulates K+
entry into cells.
The result is that plasma K+ level is further depleted.
Hypokalemia affects heart functioning and is life
threatening.
Low plasma concentration of K+
(hypokalemia) leads to an increased
excretion of hydrogen ions, and thus may
cause metabolic alkalosis.
Conversely, metabolic alkalosis is associated
with increased renal excretion of K+.
Textbook of Biochemistry – U Satyanarayana
Related Documents