CANADIAN GUIDELINE FOR ACUTE BACTERIAL RHINOSINUSITIS Ruchmana Aga 112013319 Lia Trisna Pertiwi 1320221146

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CANADIAN GUIDELINE FOR ACUTE BACTERIAL RHINOSINUSITIS
Ruchmana Aga 112013319Lia Trisna Pertiwi 1320221146

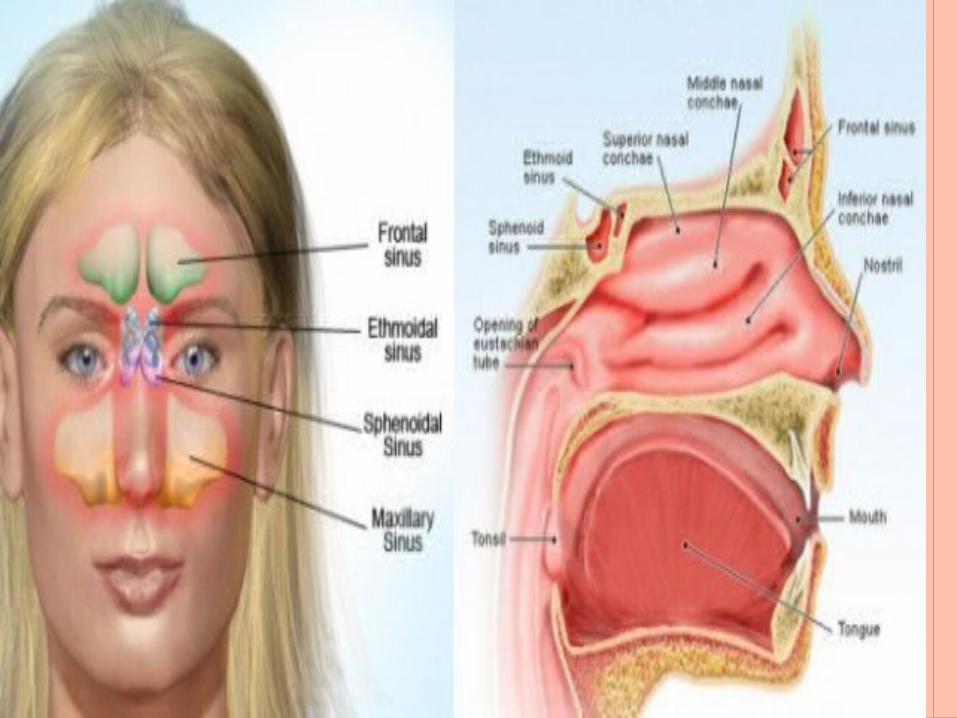
DEFINITION Rhinosinusitis is the inflammation of the
nasal passages and sinus cavities. It causes a combination of symptoms of rhinitis and sinusitis
Usually, rhinosinusitis caused by allergies or an infection

EPIDEMYOLOGY Rhinosinusitis is a common malady, afflicting
approximately 1 in 8 adults
America 11% (26 million) in 2007 to 13% (29.8 million) in 2010
Canada 3.5 million adults with acute rhinosinusitis annually

SinusitisEtiologic Organisms (& % incidence)
Bakteri Aerob:• Strep. pneumoniae (30%)• Hemophilus influenzae (25 to 30%• Moraxella catarrhalis (15 to 20%)• Alpha & beta hemolytic Strep (5%)• Staph. aureus (5%)• Escherichia coli (5%)

RADIOLOGY Axial image showing mucosal thicknening and an air-fluid level in the maxillary sinus (MS)
Bakteri Anerobes (10 % acute, 66 % chronic)
Peptostreptococcus,Propionobacterium, Bacteroides, FusobacteriumFungi (2 to 5%)Viruses (5 to 10%)

Acute Sinusitis Predisposing Conditions
Local–Allergic rhinitis–Nasal septal defects–Barotrauma (diving)–Nasal foreign bodies–Dental infections–Over use of topical decongestants–Nasal polyps or tumors–Aspiration of infected water–Smoking

Acute Sinusitis Predisposing Conditions
Systemic :–Diabetes–Immunocompromise (AIDS)–Malnutrition–Chemotherapy–Long term steroid Rx

CLASSIFICATION
By the duration of an inflammatory episode
Acute (up to 4 weeks) Subacute (4–12 weeks) Chronic (> 12 weeks) Recurrent acute rhinosinusitis ( ≥ four episodes
per year without evidence of chronic rhinosinusitis)

7-14 days to 1 month of symptoms
Infectious etiology Viral Bacterial
Symptoms:Purulent nasal drainage +
facial pain / pressure + nasal obstruction
>12 weeks
Etiology: Often not infectious, however bacterial profile differs from acute , culture-directed antimicrobial therapy is essential, can also be fungal
Symptoms: Chronic Purulent nasal drainage + facial pain/pressure + nasal obstruction + hyposmia
Acute Rhinosinusitis
Chronic Rhinosinusitis

DIAGNOSIS
P : Facial Pain, pressure/fullness
O : Nasal Obstruction D : Nasal purulence /
discoloured postnasal Discharge
S : Hyposmia or anosmia (Smell)
• Headache• Halitosis• Fatigue• Dental pain• Cough• Ear pain or pressure
Major Symptoms Minor Symptomps




TREATMENT The goal of therapy : improve symptoms by
- controlling infection,- reducing edema- reversing sinus ostial obstruction
Guidelines recommend using disease severity to help direct therapy.
Severity is based on the duration and intensity of symptoms, coupled with the effect of the disease on patient quality of life

TREATMENT For mild to moderate ABRS
- intranasal corticosteroids (INCSs) can be used to reducing inflammation
In a clinical study, mometasone furoate for 15 days significantly improved symptoms scores, beginning at day 2, compared with amoxicillin for 10 days (P = .002) or placebo (P < .001)
Compared with placebo treatment, mometasone furoate was associated with significantly improved quality of life for patients with ABRS

THE EFFICACY OF INCSS USED WITH ANTIBIOTIC SIGNIFICANT BENEFIT OF 15 TO 21 DAYS OF INCS THERAPY ADDED TO
ANTIBIOTIC IN PATIENTS WITH ABRS
patients with moderate to severe ABRS who receivedamoxicillin-
clavulanate plus mometasone
furoatereported significantly improved
symptom scores (days 1 to 15 averaged) versus
patients taking antibiotic monotherapy (P ≤ .017)
patients with ABRS and history of recurrent sinusitis or chronic rhinitis, patients receiving cefuroxime axetil plus fluticasone propionate spray reported significantly
higher rate of clinical success (93.5% vs 73.9%, P = .009) and shorter duration
of symptoms (6 days to clinical success vs 9.5 days,
P < .01)

ANTIBIOTICS First line: Amoxicillin; for ß-lactam allergy use
TMP-SMX combinations or a macrolide
Second line: Fluoroquinolones or amoxicillin–clavulanic acid combinations use with first-line failures and in patients for whom the
risk of bacterial resistance is high or consequences of therapy failure are
greatest Bacterial resistance should be considered when selecting
therapy
ADJUNCT THERAPY Although clinical trial evidence is sparse for
adjunct therapies in the treatment of ABRS, these therapies might help alleviate symptoms associated with ABRS
Analgesic Decongestant (oral & topikal) Saline

FOLLOW UPIf failure
occurs after a second course of antibiotic therapy, specialist assessment is warranted
When to refer No response to second-line
therapy Suspected chronicity Persistent severe symptoms More than 3 recurrences per year Immunocompromised host Allergic rhinitis evaluation for
immunotherapy Anatomic defects causing
obstruction infection or neoplasms

CONCLUSION The Canadian guidelines provide up-to-date
recommendations for diagnosis and treatment of ABRS that reflect an evolving understanding of the disease
Although lacking in specificity, using duration-based symptoms for the diagnosis of uncomplicated cases of ABRS is the best available approach for diagnosis in the office setting
Intranasal corticosteroids have emerged as modestly beneficial as adjunct therapy or as monotherapy, with antibiotics reserved for severe cases of disease in otherwise healthy adults
TERIMA KASIH
Related Documents











