A STUDY ON SIRAJA GRANTHI AND ITS MANAGEMENT WITH PUNARNAVADI GUGGULU AND NIMBADI GUGGULU-A COMPARATIVE STUDY. By Dr. NADAF A.N. Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Bengaluru, Karnataka In partial fulfillment of the requirements for the degree of AYURVEDA DHANWANTARI (MASTER OF SURGERY) In SHALYA TANTRA Under the guidance of Dr. B.A.VENKATESH BSAM, BAMS, MD (Ayu), FICA Professor & H.O.D. Dept. Of P.G. Studies in Shalya Tantra G.A.M.C, Bengaluru - 09 DEPARTMENT OF POST GRADUATE STUDIES IN SHALYA TANTRA GOVERNMENT AYURVEDIC MEDICAL COLLEGE Bengaluru - 560009 2009 - 2010 A STUDY ON SIRAJA GRANTHI AND ITS MANAGEMENT WITH PUNARNAVADI GUGGULU AND NIMBADI GUGGULU-A COMPARATIVE STUDY. Dr. NADAF A.N. 2009 - 2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A STUDY ON SIRAJA GRANTHI AND ITS MANAGEMENT WITH PUNARNAVADI GUGGULU AND NIMBADI GUGGULU-A
COMPARATIVE STUDY.
By
Dr. NADAF A.N. Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Bengaluru, Karnataka
In partial fulfillment of the requirements for the degree of
AYURVEDA DHANWANTARI (MASTER OF SURGERY)
In
SHALYA TANTRA
Under the guidance of
Dr. B.A.VENKATESH BSAM, BAMS, MD (Ayu), FICA
Professor & H.O.D. Dept. Of P.G. Studies in Shalya Tantra
G.A.M.C, Bengaluru - 09
DEPARTMENT OF POST GRADUATE STUDIES
IN SHALYA TANTRA
GOVERNMENT AYURVEDIC MEDICAL COLLEGE
Bengaluru - 560009
2009 - 2010
A STU
DY O
N SIR
AJA
GR
AN
THI A
ND
ITS MA
NA
GEM
ENT W
ITH PU
NA
RN
AVA
DI
GU
GG
ULU
AN
D N
IMB
AD
I GU
GG
ULU
-A C
OM
PAR
ATIVE STU
DY .
Dr. N
AD
AF A
.N.
2009 - 2010

A STUDY ON SIRAJA GRANTHI AND ITS MANAGEMENT WITH PUNARNAVADI GUGGULU AND NIMBADI
GUGGULU-A COMPARATIVE STUDY.
By
Dr. NADAF A.N. Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Bengaluru,
Karnataka
In partial fulfillment of the requirements for the degree of
AYURVEDA DHANWANTARI (MASTER OF SURGERY)
In
SHALYA TANTRA
Under the guidance of
Dr. B.A.VENKATESH BSAM, BAMS, MD (Ayu), FICA
Professor & H.O.D. Dept. Of P.G. Studies in Shalya Tantra
G.A.M.C, Bengaluru - 09
DEPARTMENT OF POST GRADUATE STUDIES
IN SHALYA TANTRA
GOVERNMENT AYURVEDIC MEDICAL COLLEGE
Bengaluru - 560009
2009 - 10
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
KARNATAKA, BENGALURU
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “A study on Siraja granthi and
its management with Punarnavadi guggulu and Nimbadi guggulu – Comparative
study, is a bonafide and genuine research work carried out by me under the guidance
of Dr.B.A.Venkatesh Professor and HOD of Dept of PG studies in Shalya Tantra,
GAMC Bangalore.
Date: Signature of the candidate Place:
Dr.NADAF. A.N
Department of Post Graduate Studies in Shalya Tantra.
Government Ayurvedic Medical College
Bengaluru : 560009
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A study on Siraja granthi and
its management with Punarnavadi guggulu and Nimbadi guggulu – Comparative
study” is a bonafide and genuine research work carried out by Dr.NADAF.A.N in
partial fulfillment of the requirement for the degree of “AYURVEDA
DHANWANTARI” [Shalya Tantra] – Master of Surgery [Ayu].
I recommend this dissertation for the above degree to the University for assessment
and approval.
Date: Dr.B.A.Venkatesh BSAM,BAMS,M.D (Ayu),FICA
Place: Professor and HOD Dept of PG Studies ShalyaTantra GAMC Bengaluru: 09

Department of Post Graduate Studies in Shalya Tantra.
Government Ayurvedic Medical College
Bengaluru: 560009
ENDORSEMENT BY HOD
This is to certify that the dissertation entitled “A study on Siraja granthi and
its management with Punarnavadi guggulu and Nimbadi guggulu – Comparative
study” is bonafide research work done by Dr.NADAF.A.N under the guidance of
Dr.B.A.VENKATESH. Professor and HOD, Dept of PG studies in Shalya Tantra.
I recommend this dissertation for the above degree to the University for Assessment
and approval.
Head of the Department Dr.B.A.Venkatesh Professor and HOD Dept of PG Studies in ShalyaTantra GAMC Bengaluru: 09

Department of Post Graduate Studies in Shalya Tantra.
Government Ayurvedic Medical College
Bengaluru: 560009
ENDORSEMENT BY PRINCIPAL
This is to certify that the dissertation entitled “A study on Siraja granthi and
its management with Punarnavadi guggulu and Nimbadi guggulu – Comparative
study” is a bonafide research work done by Dr. NADAF.A.N under the guidance of
Dr.B.A.VENKATESH. Professor and HOD, Dept of PG studies in Shalya Tantra.
I recommend this dissertation for the above degree to the University for Assessment
and approval.
Principal Govt.Ayurvedic Medical College
Bengaluru

COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Bengaluru, Karnataka, shall have the rights to preserve, use and
disseminate this dissertation in print or electronic format for
Academic / research purposes.
Signature of the candidate Dr. NADAF.A.N
@ Rajiv Gandhi University of Health Sciences, Bengaluru

No work is a result of individual effort. It is contributory effort of many
hearts, hands and heads. It gives me immense pleasure to offer my sincere thanks to
all those who have rendered their wholehearted support, guidance and Co-operation in
completing my thesis work.
I place on record my utmost gratitude to my adorable guide and HOD
Dr.B.A.Venkatesh, Professor and Head, Department of P.G.Studies in Shalyatantra
G.A.M.C. Bengaluru, for his incessant, untiring, round the clock guidance with all the
diligence, his sustained fostering and encouragement instilled considerable impetus in
me enabling to achieve this milestone which otherwise would have lacked this
particular finish.
I extend earnest thanks to Dr. H.T.Sreenivas, Principal, G.A.M.C, Bengaluru,
for unstinted help extended whenever solicited.
I express my sincere thanks to, Dr. Vijaya Sarathi .R, Professor,
Dr.R.KHibare, Professor, Dr.Ahalya, Professor and Dr. Narmada., Asst. Professor,
Dr.Sridhar Rao.A, Asst. Professor Dr. Shivu Arekeri, Dr. Srinivas, Dr.Durgesh,
lecturers, Dept. of P.G Studies in Shalya Tantra, G.A.M.C, Bengaluru, for their kind
suggestion and guidance throughout the course of my study.
I am at no words to explain the amount of gratitude and thanks to
Dr.Ravikumar, Gen.Surgeon, KCG Hospital for his dedicated professionalism,
indefatigable efforts and cheerful co-operation.
I sincerely thank my Senior colleagues for their tremendous suggestions and
support through out my work.
I acknowledge my gratitude to all my colleagues, Dr. Vishwanath sharma,
Dr. Ramya bhat, Dr. Veena koppal, Dr. Sweta, Dr. Abhinetri hegde and
Dr.Rajeshwari, who gave me unstinted support and stood solidly beside me
throughout my study.
I also profusely thank my junior colleagues, Jayanth, Laxman, Prashanth,
Manjunath Joshi, Vivek, Naveen, Jayashree and Divya lakshmi for their
continuous support and kind help.
ACKNOWLEDGEMENT

I would like to thank my friend Dr.Naveen, for his support.
I express my sincere gratitude to all the teaching fraternity, Physicians, library
staff, hospital and office staff of G.A.M.C, Bengaluru, for sincere advices and
assistance.
I am very much thankful to my department colleagues and friends for their
needful support to fulfill this task.
It fills joy in my heart to express my sincere gratitude to all my Teachers of
DGM Ayurvedic Medical College, Gadag, who designed my career in Ayurveda. I am
grateful to all the teachers who came in my life and taught me ‘the science of life’.
I sincerely thank Dr.Arun biradar for his utmost support and help during my
study period.
I thank Dr K.P.Suresh, Statistician, without whose help whole of my work
would have looked meaningless
I take this opportunity to appreciate the generous co-operation offered by my
patients by being supportive and compliant during the study period.
I express my thanks to all the persons who have helped me directly &
indirectly with apologies for my ability to identify them individually.
Dr. NADAF.A.N

ABSTRACT
Background: Siraja granthi (varicose veins) is one of the commonest
disorders in surgical practice. Ayurveda has given a great contribution in the
management of this disorder, while describing the management of Vata Vyadhi and
siraja granthi.
In Ayurveda there are various terminology for varicose veins such as Siraja
granthi, Siraakunchan, Sirakutilata and Siragata vata. Research works have been done
with both internal and external medicines along with conservative treatment such as
external application of Sahacharadi Taila, internal Basti and Para surgical procedure
such as Jaloukavacharana and Siravyadha.
A preliminary pilot study was conducted on a selective patient of varicose vein
for a period of 2 months where in selected subject were divided into 2 groups of 5
patients in each group. Group A was administrated with Punarnavadi guggulu vati in
dose of two vati twice daily for a period of 2 months. In-group B, Nimbadi guggulu
two vati twice daily was administered for a period of 2 months.
Objectives of the study:
• To evaluate the efficacy of the Punarnavadi guggulu in Siraja granthi.
• To evaluate the efficacy of the Nimbadi guggulu in Siraja granthi.
• To evaluate the comparative efficacies of Punarnavadi guggulu vati and
Nimbadi guggulu vati in Siraja granthi.
• To assess the management of varicose vein with that of conservative line
of treatment like control study with elastic stockings.

Study design:
This study was undertaken by selecting 20 patients in each group.
Group A- Internal administration of Punarnavadi guggulu in a dose of 2 vati, twice a
day.
Group B- Internal administration of Nimbadi guggulu in a dose of 2 vati, twice a day.
Group C-The management of varicose vein with conservative line of treatment i.e,
control study with Elastic stockings.
Ankle oedema, Skin changes and Tortuous dilated veins were taken as
objective parameters whereas itching was taken as subjective parameter.
In-Group A out of 20 patients, Mild improvement was observed in the 14
patients, Moderate Improvement was present in 3 patients.
In group B out of 20 patients, Mild Improvement was observed in 8 patients,
Moderate improvement was observed in 5 patients and Marker Improvement was
found in 2 patients.
In Group C out of 20 patients, Mild Improvement was observed in 9 patient
and Moderate Improvement was observed in 4 patients.
Key Words: Siraja granthi, Varicose vein, Elastic stockings, Punarnavadi guggulu
vati, Nimbadi guggulu vati.

List of Abbreviations
• Su.Su. – Sushruta Samhita Sutrasthana
• Su.Sha. - Sushruta Samhita Sharirasthana
• Su.U. - Sushruta Samhita Uttarasthana
• Su.Chi. - Sushruta Samhita Chikitsasthana
• Ch.Su. – Charaka Samhita Sutrasthana
• Ch.Vi. – Charaka Samhita Vimanasthana
• Ch.Chi. – Charaka Samhita Chikitsasthana
• A.Hr.Su. – Astanga Hrudyam Sutrasthana
• A.S.Su. – Astanga Sangraha Sutrasthana
• L.S.V. – Long Saphenous Vein
• S.S.V. – Short Shaphenous Vein
• B.P . – Bhavaprakasha
• A.T. – After Treatment
• B.T. – Before Treatment
• M.Ni – Madhava nidana
• B.R – Bhaishajya Ratnavali
• B B R – Bharatha Bhaishajya Ratnavali

CONTENTS
1. Introduction 1-2
2. Objectives 3
3. Review of Literature 4-55
• Disease review 4-47
• Drug review 48-55
4. Materials and Methods 56-60
5. Observation and Results 61-86
6. Discussion 87-93
7. Conclusion 94-95
8. Summary 96-98
9. References 99-101
10. Bibliography 102-104

List of Tables
Sl.No
Titles
Page.No
1. Study design 57
2. Grading of Itching 58
3. Grading of Ankle oedema 58
4. Grading of Skin changes 58
5. Grading of Tortuous dilated vein 59
6. Age wise Distribution of 60 patients of Siraja granthi 60
7. Sex wise Distribution of 60 patients of Siraja granthi 62
8. Distribution of Patients According to Occupation 62
9. Habitat-wise Distribution of 60 patients of Siraja granthi 63
10. Distribution of the Patients According to Agni 63
11. Distribution of Patients According to Involvement of Leg 64
12. Distribution of Patients According to Involvement of Vein 64 – 65
13. Distribution of Patients According to Site of Perforators 65
14 Incidence of Lakshanas in Trail groups 66
15. Effect of Punarnavadi guggulu vati on Itching 67
16. Effect of Nimbadi guggulu vati on Itching 68
17. Effect of the Elastic stocking on Itching 68
18. Effect of the Punarnavadi guggulu vati on the Ankle oedema. 69
19. Effect of the Nimbadi guggulu vati on the Ankle oedema 70
20. Effect of the Elastic stocking on the Ankle oedema 70
21. Effect of the Punarnavadi guggulu vati on the Skin changes 71
22. Effect of the Nimbadi guggulu vati on the Skin changes 72
23. Effect of the Elastic stocking on the Skin changes 73
24. Effect of Punarnavadi guggulu vati on Tortuous dilated vein 73
25. Effect of Nimbadi guggulu vati on the Tortuous dilated vein 74
26. Effect of Elastic stocking on the Tortuous dilated vein 74
27. Therapeutic effect of all the groups on Itching 75
28. Therapeutic effect of all the groups on Ankle oedema 75

29. Therapeutic effect of all the groups on Skin changes 76
30. Therapeutic effect of all the groups on Tortuous dilated vein 76
31 Overall response of the therapies on Siraja granthi 77
32. Co relation between Siraja granthi and varicose vein 88
List of Charts
Sl.No
Titles
Page
No.
1. Classification of the Granthi roga 42
2. Ingredients of Punarnavadi Guggulu. 48
3. General Properties of the Punarnavadi guggulu 48 – 49
4. Karma, Amayika prayoga and Chemical composition of
Punarnavadi guggulu.
49 – 50
5. Ingredients of the Nimbadi guggulu 50
6. General properties of Nimbadi guggulu 50 – 51
7. Karma, Amayika prayoga and Chemical composition of Nimbadi
guggulu.
51 - 52

List of Figure
Sl.No. Title Page No.
1 Leonardo’s drawing of superficial Veins of lower limb 4
2 Leonardo’s detailed drawing of L.S.V. 4
3 Communicating Veins of leg 10
4 Valve of vein 11
5 Incompetent Valve 12
6a Normal vein 16
6b Varicose vein caused by deformed valve 16
7 Communicating vein incompetence 17
8 Thigh and calf perforators 23
9 Crepe bandage 32
10 Ingredients of Punarnavadi guggulu 54
11 Ingredients of Nimbadi guggulu 55
12 Punarnavadi guggulu vati 60
13 Nimbadi guggulu vati 60
14 Elastic stocking 60
15 Photo showing effect of Punarnavadi guggulu 85
16 Photo showing effect of Nimbadi guggulu 85
17 Photo showing effect of Elastic stocking 86

List of Diagrams
Sl.No. Title Page No.
1 Age wise Distribution 78
2 Sex wise Distribution 78
3 Incidence of Occupational Status 79
4 Incidence of Habitat 79
5 Incidence of Agni 80
6 Incidence of Involved Leg 80
7 Incidence of Involved Veins 81
8 Incidence of Involved Perforators 81
9 Incidence of Lakshanas in Trail groups 82
10 Effect on Itching 82
11 Effect on Ankle oedema 83
12 Effect on Skin changes 83
13 Effect of all groups on tortuous dilated vein 84
14 Overall Response of therapies 84

Introduction _______________________________________________________
_____________________________________________________________________
INTRODUCTION
Siraja granthi (varicose veins) is one of the commonest disease in surgical
practice. It occurs in people who are habitual to standing for long periods.
The most important factors leading to the development of the varicose veins
includes heredity, prolonged standing, increasing age, heavy lifting, prior superficial
or deep vein clot, female gender, multiple pregnancies, less physical activities, high
blood pressure and obesity has also been linked with the presence of varicose veins in
females.
Ayurveda has given a great contribution in the management of such disorders,
while describing the management of vata vyadhi and Siraja granthi
In Ayurveda, there are many nomenclatures for varicose veins such as Siraja
granthi, Siraakunchana, Sirakutilata and SiragataVata. Research works have been
done including conservative treatment such as external application of Sahacharadi
Taila, internal Basti and Para surgical procedure such as Jaloukavacharana and
Siravyadha, by using animal Shringa as Sushruta had indicated cow’s horn for Vata
Dushita Rakta1 .
It is commonly assumed that, if varicose veins are left untreated they will
continue to enlarge and ‘varicose processes’ will spread to involve other previously
‘normal’ veins. There is evidence that long saphenous vein regress by sclerotherpy.
Other investigators have observed that simple ligation and division of the sapheno-
femoral junction causes regression of distal varices.
The influence of prolonged external elastic compression on the natural history
of varicosity is still not known to our knowledge, but it is interesting to note that
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 1

Introduction _______________________________________________________
_____________________________________________________________________
many patients with primary varicose veins who have been given elastic stocking to
wear while they await operation, they are so much better that they no longer required
treatment. This is progressive incurable disease that has satisfactorily symptomatic
relief.
It is frequently argued that varicose veins must be treated to prevent the
development of skin changes but little is known about the magnitude of risk that
patients with uncomplicated varicose veins will develop skin changes that may lead to
ulceration.
Based on the clinical experience of physician, Nimbadi guggulu vati and
Punarnavadi guggulu vati was successfully used in the management of varicose vein.
The Punarnavadi guggulu was also used for treating this condition with good result as
per the internet references 2
A preliminary pilot study was conducted on selective patients of varicose vein
for a period of 2 months where in selected subjects were divided into two groups of 5
patients in each group. In Group first, Punarnavadi guggulu vati was given twice a
day for a period of 2 months .In Group second, Nimbadi guggulu vati was given,
twice a day for a period of 2 months.
At the end of the treatment, satisfactory symptomatic improvement was
observed.
This formed basis for selection of these drugs in the management of varicose
vein (Siraja granthi). Hence, this study was undertaken by selecting 60 patients in
three groups
In Group A-Punarnavadi guggulu vati, in Group B- Nimbadi guggulu vati was
administered. In Group C- Patients were advised to wear the elastic stockings.
Hence, the study is undertaken to evaluate the efficacy of the treatment in all groups.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 2

Objectives of the study _______________________________________________________
OBJECTIVES OF THE STUDY
• To evaluate the efficacy of the Punarnavadi guggulu vati in Siraja granthi
• To evaluate the efficacy of the Nimbadi guggulu vati in Siraja granthi
• To evaluate the comparative efficacies of Punarnavadi guggulu vati and
Nimbadi guggulu vati in Siraja granthi.
• To assess the management of varicose vein with that of conservative line
of treatment like Elastic stockings as the control study.
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 3

Disease review _______________________________________________________
______________________________________________________
VARICOSE VEINS
Historical review
A.D. 130-200
Galen – the beginning of varicose vein surgery:
Galen of Pergamum describes the treatment of ulcer and varicose vein by
Venesection. He noticed that wall of the vein was always much thinner than the wall
of the arteries and that veins contain dark blood. He described the use of silk ligatures
and advised that varicose vein should treated by incision and tearing out with a blunt
hook.
The Anatomy of Veins as Seen by a great artist –
The masterly anatomical drawing of Leonardo da Vinci shows how clearly he
observed the venous system.
Fig-1 Fig-2
Leonardo’s drawing of superficial Leonardo’s detailed drawing of L.S.V
Veins of lower limb
1585:
A drawing of a Valve, at last is believed to be the first recorded drawing of
valve in vein. Saloman Alberti published it in 15853.
200 B.C.
Sushruta Samhita, the main textbook of Indian surgery describes about Siraja
granthi in nidana sthana and chikitsa sthana.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 4

Disease review _______________________________________________________
______________________________________________________
Embryology and Radiographic Anatomy
Development and Congenital anomalies:
Initially the cardinal veins are the main venous drainage system of the
embryo. They consist of the anterior cardinal vein, which drain the cephalic part of
the embryo, and the posterior cardinal veins, which drain the remaining part of the
body of the embryo. The anterior and posterior cardinal vein join before entering the
sinus horn to form the short common cardinal veins. During the 4th week the cardinal
veins form a symmetrical system.
During the 5th to 7th week of embryonic life a number of additional veins are
formed, Subcardinal veins which mainly drain the kidneys; the Sacrocardinal veins
which drain the lower extremities; and the Supracardinal veins which drain the body
wall by the way of intercostal veins, there by taking over the function of the posterior
cardinal veins. Characteristic formation of the vena cava system is the appearance of
anastomosis between left and right so that blood from left is channeled to the right
side.
The anastomosis between the sacrocardial veins is formed by the left common
illiac vein. The right sacrocardinal vein finally becomes the sacrocardinal segment of
inferior vena cava. When the renal segment of the inferior vena cava connects with
the hepatic segment, which is derived from the right vitelline vein, the inferior
venacava is complete. It consists of a hepatic segment, a renal segment and a
sacrocardinal segment4.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 5

Disease review _______________________________________________________
______________________________________________________
Development of the Limb Veins:
The border vein appears in the arm and leg between the 6th and 8th week the
adult venous anatomy being outlined during the next 2 weeks. In the leg, tibial
continuation of primitive border vein disappears while the fibular segment largely
persists.
The long saphenous vein arises separately from the posterior cardinal vein,
gives off the femoral and posterior tibial veins and then incorporates the tibial border
vein at the level of the knee. Distally the border vein develops into the anterior tibial
and saphenous veins.
Structure of Veins:
The walls of the vein like those of the arteries are composed of three coats, the
tunica intima, the tunica media and the tunica adventitia. The main difference between
the wall of arteries and those of vein is that, in the latter, there is a comparative
weakness of the muscular layer and a much smaller proportion of elastic tissue. In
small veins these coats are difficult to distinguish.
Valves:
Unlike arteries, veins possess valves, through which the blood flow towards
the heart. The valves have two leaflets consisting of folds of intima reinforced with an
intervening layer of connective tissue.
There are no valves in the superior and inferior venae cavae but there are
valves in the tributaries from both upper and lower limbs, the number of valves
increasing towards the periphery of each limb. The valves in the lower limb play an
important role in controlling the direction of blood flow.
There are no valves in the sinusoidal veins of the soleal muscles but the
veins arcades that drain the soleal and gastronemius muscles have numerous valves.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 6

Disease review _______________________________________________________
______________________________________________________
All the deep veins of the calf are densely valved with the valves occurring at
approximately 2 cm. intervals.
The popliteal vein usually has two valves in the region of the knee joint;
damage to these valves may result serious consequences on the calf muscle pump.
There is a valve in the femoral vein just distal to its junction with the deep femoral
vein in 90% of all legs and a valve in the upper third of the popliteal vein just distal to
the adductor canal in 96% of the legs. There are eight to ten valves in the long and
short saphenous vein, which is thought to be important in preventing reflux down the
long saphenous vein.
The valves in the communicating vein between the superficial and deep
venous systems of the leg are arranged so that blood flows from the superficial to the
deep vein.
The common femoral and external iliac vein:
The common femoral vein is formed by the confluence of the superficial
femoral and deep femoral veins and becomes the external iliac vein as it passes
beneath the inguinal ligament.
The Common Iliac Veins:
These are short wide vessels, which ascend from the level of the sacroiliac
joints to unit on the right side of the 5th lumbar vertebrae to form the inferior vena
cava. The right common iliac vein and the inferior vena cava run upwards in an
almost straight line where as the left common iliac vein runs transversely to join the
left common iliac vein at right angle. Excessive compression at this site may
predispose to thrombosis.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 7

Disease review _______________________________________________________
______________________________________________________
The superficial veins of the lower limb:
The superficial venous system of the leg consists of two main veins, the long
and short saphenous veins and their tributaries
The Long Saphenous Vein:
The long saphenous vein is formed by the union of the veins from the medial
side of the sole of the foot with the medial dorsal vein. It runs upward in front of the
medial malleolus along the length of the anterior-medial aspect of the limb, gradually
inclining posteriorly to pass behind the medial condyles of the Tibia and Femur. It is
accompanied by the saphenous branches of the femoral nerve, which may be avulsed
if the vein is stripped below the knee in the thigh. The long saphenous vein runs in a
slight curve towards its junction with the femoral vein, the breadth of two fingers
(3cm) below and lateral to the pubic tubercle at the fossa ovalis just before it inter the
fossa, it is joined by superficial circumflex iliac. The superficial inferior epigastric
and superficial external pudendal vein together with as many as seven other
superficial unnamed veins. The long saphenous vein receives several tributaries in its
Course along the lower leg. The medial superficial vein from the sole joins it near its
anatomical origin and the posterior arch vein joints its posterior aspect in the upper
leg. The posterior arch vein is important because it is connected to the deep venous
system by at least two or three major medial ankle communicating veins. The anterior
superficial tibial vein joins the long saphenous vein at about the same level as the
posterior arch vein. There are many variations of anatomy in the region of the fossa
ovalis where the long saphenous joins the common femoral vein.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 8

Disease review _______________________________________________________
______________________________________________________
The Short Saphenous Vein:
The short saphenous vein begins at the outer border of the foot behind the
lateral malleolus as a continuation of the dorsal venous arch. It is joined above the
malleolus by a communicating vein, which may be important when ulcers are present
in this area. It enters the popliteal vein between the heads of the gastronemius muscle.
There are a number of variable connections between long and short saphenous vein in
the region of the knee and these may cause confusion when trying to decide whether
varices are connected to dorsal tributaries of the long saphenous vein or to the
tributaries of the short saphenous vein.
The short saphenous vein usually joins the posterior aspect of the popliteal
vein lateral to the tibial nerve producing a characteristic ‘S’ shaped loop on a
saphenogram. Approximately 60% of all short saphenous veins join the popilteal vein
in the popliteal fossa within 8cm. of the knee joint; 20% join the long saphenous vein
via postero- medial or antero- lateral superficial thigh veins at varying levels in the
thigh and the remainder join the superficial femoral vein, the deep femoral vein, or
even tributaries of the internal iliac veins.
The Communicating Veins:
The deep and superficial venous system of the lower extremities are separated
by fascia and joined by communicating veins with valves, which direct the blood from
superficial to deep venous system. These communicating veins are sometimes called
perforating veins because they pierce the deep fascia. The communicating veins have
been further divided into direct or indirect, when the connection is through one or
more sinusoids in the muscles. Direct communicating veins are generally more
constant in position, larger and haemodyamically more important than the indirect
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 9

Disease review _______________________________________________________
______________________________________________________
veins. The largest communicating veins are the termination of the long and short
saphenous veins where they join the deep venous system.
In the lower leg, there are medial and lateral communicating veins. On the
medial side there is one communicating vein just below the medial malleolus and
three or four above the malleolus behind the tibia. The medial lower leg
communicating veins, often called Cockett’s veins, connect the posterior arch vein
with the posterior tibial veins but do not drain directly into the long saphenous vein.
The lowest medial communicating vein is usually found at approximately 7cm, the
middle vein at 12cm, and the upper vein 18cm above the tip of the medial malleolus.
Another communicating vein, which may become incompetent, is situated on the
medial aspect of the calf 10cm below the knee joint. It joins the main trunk of the long
saphenous vein to the posterior tibial veins and is sometimes called Boyd’s vein.
Two more constant communicating veins also joining the short saphenous vein
with the peroneal veins are situated posteriorly approximately 5cm and 12cm above
the os calcis These are the two posterior and mid calf communicating veins which
sometime causes recurrent varicose veins.(Fig- 3)
(a) (b)
Fig.no 3: Communicating Veins of leg (a) medal view, (b) posterior lateral view
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 10

Disease review _______________________________________________________
______________________________________________________
In the thigh, there are several connections between the long saphenous vein
and femoral vein. The most important group, sometimes-called Dodd’s veins consist
of one or more veins, which pass through the subsartorial (Hunter’s) canal to join the
long saphenous vein with the superficial femoral vein. These veins are usually, but
not invariably, destroyed when the long saphenous vein is stripped out and so are an
important cause of recurrent varicose veins. After saphenous ligation, without
stripping an incompetent mid thigh communicating vein may be responsible for an
early recurrence of varicose veins on the medial aspect of the leg in the region of the
knee.
Physiology and Functional Anatomy
The Valves:
The direction of venous blood flow is controlled by the valves. Vein valves are
bicuspid. The cusps of the valves of the superficial vein lie with their free edges
parallel to the skin surface. (Fig- 4)
Fig- 4: Valve of vein
Nomenclature of the Valve
The inferior vena cava and common iliac veins have no valves and 75% of
external iliac veins have no valves, but only 25% of common femoral veins are
valveless. It has been suggested that the lack of the valves in the iliac and common.
Femoral vein is the starting point for the development of a progressive
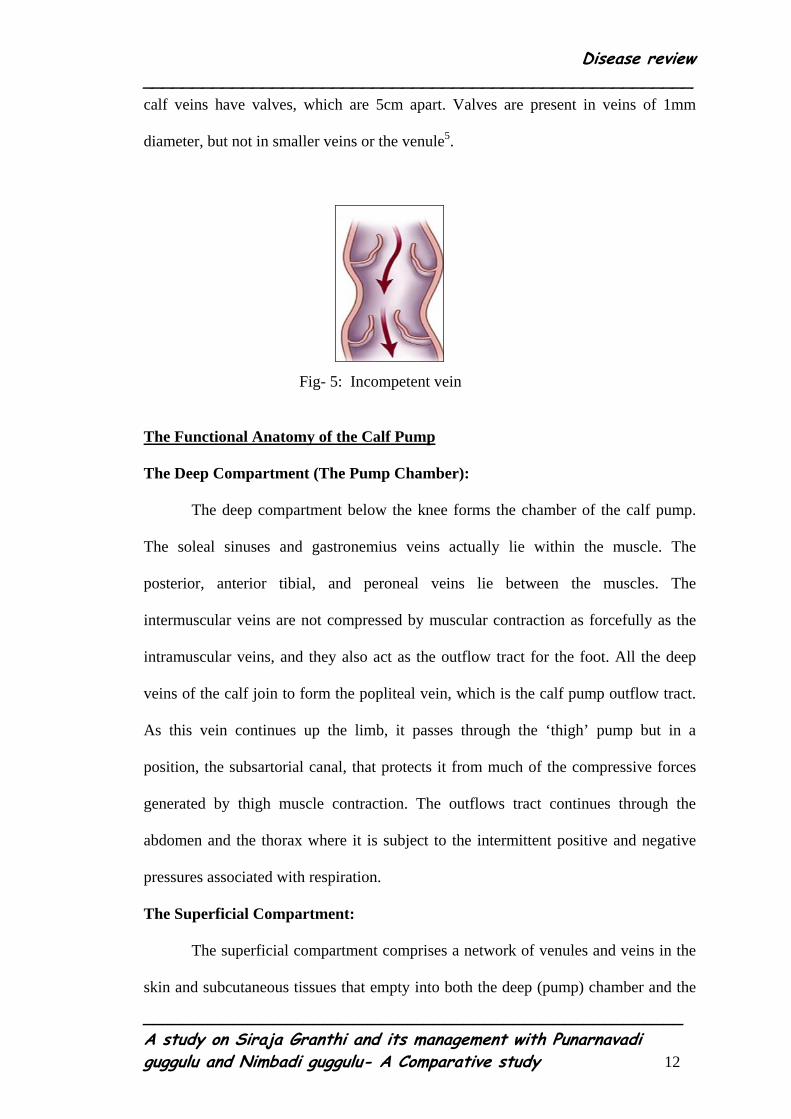
descending valvular incompetence that causes varicose veins (Fig- 5). Below the
inguinal ligament, the number of valves in each segment steadily increases so that the
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 11
Disease review _______________________________________________________
______________________________________________________
calf veins have valves, which are 5cm apart. Valves are present in veins of 1mm
diameter, but not in smaller veins or the venule5.
Fig- 5: Incompetent vein
The Functional Anatomy of the Calf Pump
The Deep Compartment (The Pump Chamber):
The deep compartment below the knee forms the chamber of the calf pump.
The soleal sinuses and gastronemius veins actually lie within the muscle. The
posterior, anterior tibial, and peroneal veins lie between the muscles. The
intermuscular veins are not compressed by muscular contraction as forcefully as the
intramuscular veins, and they also act as the outflow tract for the foot. All the deep
veins of the calf join to form the popliteal vein, which is the calf pump outflow tract.
As this vein continues up the limb, it passes through the ‘thigh’ pump but in a
position, the subsartorial canal, that protects it from much of the compressive forces
generated by thigh muscle contraction. The outflows tract continues through the
abdomen and the thorax where it is subject to the intermittent positive and negative
pressures associated with respiration.
The Superficial Compartment:
The superficial compartment comprises a network of venules and veins in the
skin and subcutaneous tissues that empty into both the deep (pump) chamber and the
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 12

Disease review _______________________________________________________
______________________________________________________
pump outflow tract. The two main superficial veins, the long and short saphenous
veins, drain directly into the outflow tract, but there are many other connections
between the superficial veins and the veins of the deep compartment.
The superficial tributaries of the saphenous systems collect blood from the
skin and subpapillary dermal plexus and then progressively unite to form the two
main veins. The saphenous veins themselves lie in a deeper layer of the subcutaneous
tissues underneath a thin but quite strong layer of connective tissue. The vein in the
dermal plexus and the subcutaneous fat are well situated for their role in
thermoregulation but are poorly supported against distending forces. The valves
ensure that blood flow into the pump and towards the heart. Blood leaves the
superficial compartment by flowing up the saphenous veins into the femoral or
popliteal veins or directly into the pump through the many communicating veins.
Communication between the Superficial and Deep Compartments:
The superficial compartment has two large constant connections with the
outflow tract, the sapheno-femoral and the sapheno-popliteal junctions. They are
protected by valves that normally prevent reflux from the deep to the superficial
compartments. The common femoral and popliteal veins are not inside the muscle
pumps. They lie relatively unsupported in the loose fatty connective tissue, which
surrounds the femoral and popliteal neurovascular bundles.
The named communicating veins on the medial aspect of the lower leg
connect the superficial veins with the posterior tibial veins. These veins do not
connect the long saphenous vein directly to the deep compartment but drain the whole
superficial system, including the long saphenous vein, into the pump indirectly
through their connection with the posterior arch vein.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 13

Disease review _______________________________________________________
______________________________________________________
The Physiology of the Calf Pump:
The calf pump has been called the peripheral heart. We have found it helpful
to develop this comparison because the left side of the heart is also a two-chamber
system. The calf pump is equivalent to the left ventricle. The venous outflow tract is
the equivalent of the aorta and its valve. The superficial compartment is equivalent to
left atrium, and the communicating veins are comparable to mitral valve.
The Pump:
Systole:
When calf muscles and the muscles in deep posterior compartment of the
lower leg contract, they raise the pressure in and around all structures contained
within the deep fascia. The muscles generate pressures of 200- 300 mmHg. These
pressures squeeze the blood out of the veins, the valves ensuring that the blood flows
only towards the heart. Flow from the deep to the superficial compartment is
prevented by the valves in the communicating veins.
The large veins within the gastronemius and soleus muscles form the main
chamber of the pump but all the other deep veins participate. The average volume of
the calf is 1500 – 2000 ml, and its contained calf blood volume is 60-70 ml. Normal
walking at 80 steps/min contract each calf 40 times/min so the pump can easily deal
with the high blood flow of exercise hyperemia.
Diastole:
The pump chamber is refilled by the arterial inflow and the flow from the
superficial compartment during diastole. Just as blood flows from the left atrium to
left ventricle during ventricular diastole, so blood flows from the superficial to the
deep compartment when the calf muscles relax.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 14
Disease review _______________________________________________________
______________________________________________________
Thus, calf pump activity performs two vital functions:
1. It ensures venous return from the lower limbs during exercise.
2. It reduces superficial vein pressure thus removing the damaging effect of the
hydrostatic pressure that is inseparable from men’s upright posture.
The causes of Calf Pump Failure:
The Pump:
Four abnormalities may reduce the efficiency of the pump itself.
Muscle weakness:
Weakness of the calf pump is the equivalent of heart failure. The calf muscle
rapidly waste and weaken with disuse. The absence of calf contractions exacerbates
the venous hypertension and its complications and causes calf muscle disuse atrophy.
A vicious circle develops as valve damage causes skin complications, which cause
pain and walking difficulties, which diminish pump function, which causes further
deterioration of the skin.
Pump Chamber contraction (Reduced End-Diastolic Volume):
Extensive deep vein thrombosis may leave many of the deep veins of the calf,
within and between the muscles, permanently occluded or thick, stiff and narrow with
incompetent valves. They cannot hold all the blood delivered to them during pump
diastole, so that pump vein pressure between calf contractions rises rapidly. The
undamaged patent veins dilate and their valves become incompetent. These secondary
changes, added to the damage caused by the deep vein thrombosis, cause the pump to
fail.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 15

Disease review _______________________________________________________
______________________________________________________
Pump Chamber Dilatation (Increased End-Diastolic Volume):
Obstruction to the outflow of blood from the pump caused by occlusion of
veins within the pump or in the main outflow tract causes the veins within the pump
to dilate and their valves to become secondarily incompetent. Valvular incompetence
of the intramuscular veins alone may not be particularly important but, if the
communicating veins become incompetent, calf pump efficiency is seriously reduced.
Pump Vein Valve Incompetence:
All veins lying along the axis of the limb need valves to prevent retrograde
flow. Not all the veins within the calf muscles have valves (e.g. the soleal sinuses),
but these particular vessels are U -shaped with both ends emptying towards the heart.
An absence of valves in the deep veins puts additional strain on the valves in the
communicating veins.(fig- 6 )
a b
Fig- 6: (a) -Normal vein. (b) - Varicose vein caused by deformed valve
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 16

Disease review _______________________________________________________
______________________________________________________
Communicating Veins Incompetence:
Their valves form an essential protection between the high pressure that
develop within the pump and the low pressures produced by the pump in the
subcutaneous compartment. If their valves fail, the pump pushes blood into the
superficial veins as well as into the outflow tract during systole. The situation is
analogous to mitral valve incompetence. (Fig- 7)
Varicose vein
Communicating vein
Deep vein
Fig –7: Communicating vein incompetence
The two causes of communicating vein valve incompetence are:-
• Valve cusp destruction by thrombosis and/or valve ring dilatation secondary to
a downstream post-thrombotic venous obstruction.
• The result of the progressive vein dilatation of the primary varicose vein
diathesis.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 17

Disease review _______________________________________________________
______________________________________________________
Superficial Veins Incompetence:
Superficial vein incompetence is mainly a cosmetic problem. Its only effect on
calf pump function is to increase the volume of blood that has to be pumped out of the
lower leg. Incompetence superficial veins (varicose veins) blood refluxing through
them may be considerable. Eventually, usually after very many years, this added load
can impair calf pump function and cause skin damage6.
Clinical Examination:
History:
Venous disease affects all age groups, though varicose veins in children are
likely to be associated with a congenital rather than an acquired abnormality and deep
vein thrombosis is rare in children. Pain, swelling and unsightliness are the dominant
symptoms. Superficial venous insufficiency causes a dull aching pain, which is
relieved by rest; deep vein thrombosis causes a persistent, more severe pain. Venous
outflow obstruction, whether acute (following a deep vein thrombosis) or chronic,
causes a bursting pain during muscle exercise. A patient with an acute thrombosis is
unlikely to try to walk because the muscles are also painful at rest. Night cramps are
less common.
Swelling of the leg may be localized, or general. General swelling may very
from a little oedema around the ankle to gross swelling of whole limb. There is no
difference between the swelling of deep vein thrombosis and that of chronic venous
insufficiency; it is a low protein oedema caused by the venous obstruction.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 18

Disease review _______________________________________________________
______________________________________________________
Examination:
Always examine the legs twice, first when the patient is standing and then
when the patient is lying down, except when muscle pain and discomfort are severe.
Inspection:
Three abnormalities may be visible on inspection: dilated superficial veins,
changes in the skin and swelling. Dilated veins may be large incompetence tortuous
subcutaneous veins (i.e. varicose veins) or fine intradermal venules (‘venous stars’).
The position of dilated veins may indicate their anatomical origin and connections.
Veins on the medial side of the thigh are most likely to be connected to the long
saphenous system but below the knee, the position of a varicose vein does not allow
its attribution to any particular system. A varicose vein on the medial side of the calf
may be connected to the long saphenous system but it could be connected to the short
saphenous system or it could be independent of both.
Skin changes range from mild eczema and pigmentation through thickening
and hardening of the skin and fat (lipodermatosclerosis) to weeping eczema and frank
ulceration. Although the majority of these skin changes are found on the lower medial
third of the lower leg, they can occur anywhere. Conversely, other forms of ulceration
more common on other parts of the leg can occur in the ‘gaiter’ area and so it should
never be assumed that skin changes are venous in origin just because of their site. The
presence of skin changes indicates a severe disturbance of calf pump function,
whereas quite large varicose veins may exist with little or no functional abnormality.
The extent of diffuse swelling caused by venous disease usually correlates
with the site and severity of the venous outflow obstruction. Localized swelling is
usually caused by local inflammatory changes (e.g. superficial thrombophlebitis).
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 19

Disease review _______________________________________________________
______________________________________________________
Palpation:
The size and tension of the veins can easily be assessed with the finger tips.
The presence of an expansile cough impulse indicates the absence of functioning
valves between the palpating finger and the thorax. Always examine for this impulse
at the sapheno – femoral junction, whether there be a palpable vein or not, and over
any other visible veins. Veins that cannot be seen, can often be felt, especially in the
thigh. A calf that is the site of a deep vein thrombosis will be warmer than the normal
calf. Recently thrombosed veins are firm, incompressible and tender. The tenderness
fades with the inflammation but the vein gets harder and the overlying skin often
becomes pigmented. The surface of an ulcer is painful if it is infected or necrotic.
Clean, healing chronic venous ulcers are usually neither painful nor very tender. The
oedema of venous obstruction is soft and ‘pits’ easily with firm pressure. The
thickening of lipodermatosclerosis some time looks like oedema but is hard and
incompressible and can even become calcified.
Percussion:
A dilated blood - filled vein will conduct a percussion impulse in the direction
of normal blood flow and retrogradely if the valves are incompetent. Thus tapping on
a vein and feeling downstream should be used as a method for detecting the course
and connections of a dilated vein, whereas tapping and feeling upstream should be
used as a way of testing for incompetent valves in the segment of vein between the
two hands.
Auscultation:
Do not forget to place a stethoscope over large bunches of varicosities,
especially if they are in an abnormal position. On rare occasions there will be a
machinery murmur indicating the presence of an arteriovenous fistula.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 20
Disease review _______________________________________________________
______________________________________________________
Elevation:
If the veins in a limb are distended when the patient is lying down, slowly
raise the limb until the veins collapse. The height to which the limb has to be raised
corresponds to the pressure in the veins and indicates the severity of the venous
obstruction.
Clinical classification:
C – for Clinical signs.
E – for Etiologic classification.
A – for Anatomical distribution.
P – for Pathophysiological dysfunction.
C: Clinical signs:
Class 0 – No visible or palpable signs of venous disease.
Class 1 – Telangiectases or reticular veins.
Class 2 – Varicose veins.
Class 3 – Edema.
Class 4 – Skin changes ascribed to venous disease (e.g. pigmentation, venous eczema,
and lipodermatosclerosis).
Class 5 – Skin changes as defined above with healed ulceration.
Class 6 – Skin changes as defined above with active ulceration.
E: Aetiology:
Congenital (Ec).
Primary (Ep) – with undetermined cause.
Secondary (Es) – with known cause of
Post thrombotic and Post traumatic
Other.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 21
Disease review _______________________________________________________
______________________________________________________
P: Pathophysiology:
Reflux (PR).
Obstruction (Po).
Reflux and obstruction (PRo).
A: Anatomy:
Superficial veins (As).
1- Telangiectases/reticular veins.
2- Greater (long) saphenous (GSV) – above knee.
3- Greater (long) saphenous (GSV) – below knee.
4- Lesser (short) saphenous (LSV).
5- Nonsaphenous.
Deep veins (AD)
6- Inferior vena cava.
7- Common iliac.
8- Internal iliac.
9- External iliac.
10- Pelvic- gonadal, broad ligament, other.
11- Common femoral.
12- Deep femoral.
13- Superficial femoral.
14- Popliteal.
15- Crural – anterior tibial, posterior tibial, peroneal (all paired).
16- Muscular- gastronemial, soleal, other.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 22

Disease review _______________________________________________________
______________________________________________________
17- Perforating veins (Ap) (Fig- 8 )
18- Thigh.
19- Calf
Fig-8: Thigh and calf Perforators
A few tests are performed to know the details of the varicose vein including
the sites of incompetent perforators7.
Brodie – Trendelenburg Test:
This test is performed to determine incompetence of the sapheno-femoral
valve and the other communicating system. This test can be performed in two ways.
In both the methods, the patient is first placed in recumbent position and his legs are
raised to empty the veins. The sapheno-femoral junction is now compressed with the
thumb of the clinician and the patient is asked to stand up quickly.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 23

Disease review _______________________________________________________
______________________________________________________
(1) In the first method, the pressure is released, if the varices fill very quickly
by a column of blood from above, it indicates incompetency of the sapheno-femoral
valve. This is called a positive Tredelenburg test.
(2) To test the communicating venous system, the pressure is not released but
maintained for about 1 minute. Gradual filling of the veins during the period
indicates incompetency of the communicating veins, mostly situated on the medial
side of the lower half of leg allowing the blood to flow from deep to the superficial
veins. This is also considered as a positive Trendelenburg test.
Tourniquet Test:
It can be called a variant of Trendelenburg test. In this test, the tourniquet is
tied around the thigh or leg at different levels after the superficial veins have been
made empty by raising the leg in recumbent position. The patient is now asked to
stand up. If the veins above the tourniquet fill up and those below it remain collapsed,
it indicates presence of incompetent communicating vein above the tourniquet.
Similarly, if the veins below the tourniquet fill rapidly whereas veins above the
tourniquet remain empty, the incompetent communicating veins must be below the
tourniquet. Thus by moving the tourniquet down the leg in steps one can determine
the position of the incompetent communicating vein.
Pratt’s Test:
This test is performed to know the position of the leg perforators. Firstly, in
Esmarch elastic bandage is applied from toes to the groin. A tourniquet is then applied
at the groin at the upper end of the elastic bandage. This causes emptying of the
varicose veins. The tourniquet is kept in position and the elastic bandage is taken off.
The same elastic bandage is now applied from the groin downwards. At the position
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 24

Disease review _______________________________________________________
______________________________________________________
of the perforator, a ‘blow out’ or a visible varix can be seen. This is marked with a
skin pencil.
Perthes’ Test (Modified):
This test is primarily intended to know whether the deep veins are normal or
not. A tourniquet is tied round the upper part of the thigh tight enough to prevent any
reflux down the vein. The patient is asked to walk quickly with the tourniquet in
place. If the communicating and the deep veins are normal the varicose veins will
shrink whereas if they are blocked the varicose veins will be more distended.
Schwartz Test:
In a long standing case if a tap is made on the long saphenous varicose vein in
the lower part of the leg an impulse can be felt at the saphenous opening with the
other hand.
Morrissey’s Cough Impulse Test:
In this test limb is elevated to empty the veins. The patient is asked to cough
forcibly. An expansile impulse, if felt in the long saphenous varicose vein, it may be
presumed that the sapheno-femoral valve is incompetent. Similarly, if the patient
coughs and the sapheno-femoral junction are incompetent a bruit may be heard on
auscultation.
Fegan’s Method to Indicate the Sites of Perforators:
In the standing position, the places of excessive bulges within the varicosities
are marked with a pencil. The patient now lies down. The affected limb is elevated
and the heel is kept supported. The palpates along the line of the marked varicosities
carefully, so that he can find gap or small pit in the deep fascia which transmits the
incompetent perforator. This is marked with ‘X’ this is the site of the perforator. It
should tally with the skin pencil mark of the venous bulge marked before8.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 25

Disease review _______________________________________________________
______________________________________________________
Varicose Vein:
Definition:
The world health organization (WHO) defines varicose veins as:
Saccular dilatation of the veins which are often tortuous.’
This definition specifically excludes:
• Dilatation of small intradermal subcutaneous veins called ‘venectasis’
• Any tortuous dilated veins that are secondary to previous thrombophlebitis or an
arteriovenous fistula.
The Basle study separated varicose veins into:
1. Dilated saphenous veins (trunk veins)
2. Dilated superficial tributaries (reticular veins)
3. Dilated venules (hyphenwebs).
Epidemiology:
The incidence of this condition is estimated in number of patients in whom the
condition has developed in a specified time period.
The USA National Surveys:
A subsequent survey between 1959 and 1961, of severe chronic disabling
conditions, produced an estimated rate (prevalence) of 2.25 patients with varicose
veins per 100 of the population per year, comprised of 0.8% in men and 3.5% in
women.
The UK Survey:
Showed that 1.41% of men and 3.74% of women had varicose veins.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 26

Disease review _______________________________________________________
______________________________________________________
The Sickness Survey of Denmark:
This survey of patients attending hospital with varicose veins found an
incidence of 1.7% of males and 2.0% females attending in 1 year.
Aetiology:
Valvular Deficiency:
Anatomical studies on the distribution of venous valves in cadavers have
shown that between 20 and 40% of apparently ‘normal’ individuals have an absent
valve in and above the common femoral vein on one or both sides. These studies
suggested that an absence of ilio-femoral valves exposes the highest valve in the long
saphenous vein to thoraco-abdominal pressures and that on standing upright the
hydrostatic pressure produced by the vertical column of venous blood between the
groin and the heart would be resisted only by a single important saphenous valve.
There are few patients who have a congenital absence of all venous valves
(congenital valve aplasia) who often do develop severe secondary varicose veins.
The complications of Varicose Veins:
The pathology of the complication such as superficial thrombophlebitis, eczema,
pigmentation, lipodermatosclerosis, haemorrhage, ulceration and an increased risk of
deep vein thrombosis9.
Diagnosis of Varicose veins:
Symptoms caused by varicose veins:
• Unsightliness
• Aches and pain
• Cramps
• Mild ankle oedema
• Itching
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 27

Disease review _______________________________________________________
______________________________________________________
• Superficial thrombophlebitis
• Hemorrhage
• Eczema
• Pigmentation
• Lipodermatosclerosis
• Ulceration
Unsightliness:
Many patients with varicose veins complain of the unsightliness produced by
tortuous dilated veins in their lower limbs.Patients concerned with the unsightly
appearance of their varicose veins often complain of discomfort but the severity of
this discomfort is difficult to assess and does not seem to be related to the size of the
varices.
Aches and Pain:
Many patients do however, experience considerable discomfort, which is
sometimes localized to the main varices, but is often a diffuse dull ache felt
throughout the legs, which gets worse as the day passes and is exacerbated by
prolonged standing. Worsening of the pain before a period is characteristic and pain
is sometimes accompanied by a severe ‘itch’ over the veins. Pain that is present at
rest or in bed is unlikely to be caused by varicose veins and another source must be
sought. The typical description of ‘venous’ pain is an ‘ache’ or ‘discomfort’. The
presence of a sharp or acute pain should suggest an alternative diagnosis.
Relief of the discomfort by wearing an elastic stocking provides good
circumstantial evidence that the pain is of venous origin. Elevation of the legs, bed
rest and walking all relieve venous pain, while standing still for prolonged periods
invariably makes it worse.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 28

Disease review _______________________________________________________
______________________________________________________
A history of a bursting pain during exercise (venous claudication) may
indicate venous outflow obstruction but is a rare symptom in patients with
uncomplicated varicose veins.
Night cramps are a common complaint and appear to be particularly frequent in
patients with varicose veins, especially after a long day of standing without exercise.
Ankle Edema:
Edema is not a common or prominent feature of varicose veins. It is usually
mild and only becomes noticeable at the end of the day. Incompetence of the lower
leg communicating veins in isolation or in association with post-thrombotic damage
of the deep veins can cause moderate oedema of the ankle and lower leg.
Superficial Thrombophlebitis:
This is common complication of varicose veins but must be differentiated
from superficial thromboplebitis caused by other conditions. Thrombophlebitis
usually presents as a tender, hot, red thickening on the course of a varicose vein.
Hemorrhage:
A varicose vein may bleed after injury and can occasionally bleed
spontaneously. Large veins are easily knocked or cut end, if this occurs, they can
bleed profusely for a short time.
Eczema, Pigmentation, Lipodermatosclerosis and Ulceration –
It is important to ask patients if they have ever had a deep vein thrombosis or
leg ulcer and to question them about the duration of skin discoloration or induration
around the ankle.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 29
Disease review _______________________________________________________
______________________________________________________
Physical signs of varicose veins:
Inspection:
The legs should be examined with the patient standing on a low stool or
platform, suitably undressed to expose the whole of both lower limbs from the groins
to the toes
The presence or absence of the following abnormalities should be recorded.
1. Both limbs must be inspected from all aspects (front, back and side) to ensure
varicosities in the short saphenous territory or abnormal axial veins are not
missed.
2. The presence of a saphena varix.
3. The presence of a capillary naevus.
4. The presence of a dilated intradermal venuls (‘spider veins, or ‘venous stars’)
5. The presence of any angiomatous malformations.
6. The presence of ankle oedema or limb swelling.
7. The presence of an ‘ankle flare’ (corona phlebectatica)
8. The presence of large varicosities, blow-out, over known sites of communicating
veins.
9. The presence of acute and chronic lipodermatosclerosis.
10. The presence of eczema.
11. The presence of ulceration.
12. The presence of atrophic blanche or livedo reticularis.
13. An increase in the length or circumference of the limb.
14. Shortening of the limb or muscle wasting.
15. Evidence of swollen or deformed knee or hip joints
16. Evidence of distended veins in the groin, pubic region or abdominal wall.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 30
Disease review _______________________________________________________
______________________________________________________
Palpation and Percussion:
Some varicose veins are more easily felt than seen. For example, the upper end
of a dilated long saphenous vein can often be felt along its course in the thigh between
the groin and a lower dilated visible varicose tributary, even when it cannot be seen.
After palpating the terminal segments of the long and short saphenous veins, the hand
should be gently passed over the inner side of the thigh and leg and up the posterior
surface of the calf to detect other sites of venous dilatation that might not have been
detected by inspection. Any difference in the temperature of the two limbs should also
be recorded, and any firm subcutaneous cords, which are usually felt if there have
been past episodes of superficial thrombophlebitis, should be noted.
Auscultation:
A bruit coming from a superficial vein usually indicates the presence of an
arteriovenous fistula10.
TREATMENT
1 Conservative treatment11
• Elastic crepe bandage application from below upwards or use of pressure
stockings to the limb pressure gradiant 30 to 40 mm of hg is provided
• Diosmin therapy increases the venous tone Elevation of the limb to relive
edema
• Unna boots provides nonelastic compressive mechanism. It comprises a gauge
compression dressings that contain zinc oxide , calamine and glycerine.
Pneumatic compression method provide dynamic sequential compression
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 31

Disease review _______________________________________________________
______________________________________________________
Fig-9: Crepe Bandages
STOCKINGS12
Compression stockings: are used to support the venous and lymphatic systems of the
leg. They offer graduated compression where maximum compression is achieved at
the ankle and decreases as you move up the leg. This compression, when combined
with the muscle pump effect of the calf, aids in circulating blood and lymph fluid
through the legs.
Today, compression stockings are available in a wide range of opacities,
colors, styles and sizes, making them virtually indistinguishable from regular hosiery
or socks.
Indications for use:
• Tired, aching legs
• Varicose vein
• Venous insufficiency
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 32

Disease review _______________________________________________________
______________________________________________________
• Oedema
• Lymph oedema
• Burn scar
• Prevention of Deep vein thrombosis (DVT) and the post-thrombotic
syndrome (PTS) following DVT
Compression classes:
Compression stockings are constructed using elastic fibers or rubber. These
fibers help compress the limb, aiding in circulation.
Compression stockings are offered in different levels of compression. The
unit of measure used to classify the pressure of the stockings in different mmHg. They
are often sold in one of the following pressure ranges:
Support - over-the-counter
• 10-15 mmHg
• 15-20 mmHg
With the advice or prescription of a physician or medical professional and
proper size from a trained fitter.
• 20-30 mmHg
• 30-40 mmHg
• 40-50 mmHg
• 50+ mmHg
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 33

Disease review _______________________________________________________
______________________________________________________
Compression levels used by some manufacturers for custom made, flat knitted
products in the US. Also used in Europe.
• 18-21 mmHg
• 23-32 mmHg
• 34-46 mmHg
• >50 mmHg
Styles
• Knee-high (AD)
• Thigh-high (AG)
• Pantyhose (AT)
Commonly used terms for compression stockings:
• Anti-embolism - Worn when non-ambulatory or post-surgical to help prevent
pooling of blood in the legs that could lead to a venous thrombosis.
• Custom - uniquely made for a specific individual.
• Circular Knit - Seamless stockings that offer greater aesthetic appeal.
• Flat Knit - Stockings made with a seam that can be constructed in virtually
any shape or size. Most often used in higher compression classes.
• Silver - Stockings constructed using special silver textile fibers. Silver offers
natural anti-microbial protection.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 34
Disease review _______________________________________________________
______________________________________________________
• Lymphedema - compression stockings used to manage edema resulting from
the onset of Lymphedema.
• Support - mild compression stockings sold over-the-counter and without a
physician's prescription .
2. Drugs used for varicose vein:13
• Calcium dobisilate 500 mg BD . Improves the lymph flow, macrophage
mediated proteolysis and reduces oedema.
• Doismin 450 mg +Hesperidin50 mg relive the night cramps.
• Toxerutin 500 mg BD or TID Antierothrocytic aggregation agent, which
improves capillary dynamics.
• Benefit of these entire drugs is doubtful.
3. Injection sclerotherapy:14
A detergent injected into the superficial veins, this destroys the lipid
membrane of endothelial cells causing to shed, leading to thrombosis, fibrosis and
obliteration. The commonly used detergent is sodium tetradecyle sulphate.
Fegan stressed to continued compression following sclerosant injections.
Scerotherapy was not found to be effective at eradicating varicosities in the
presence of major saphenous incompetence. It is however, useful for dealing with
minor varicosities and recurrence, especially in calf and lower leg.
Ultra sound guided foam sclerotherapy: 15
Ultra sound guided foam sclerotherpy used treat the main
saphenous trunk. A needle is inserted under duplex ultrasound guidance and
sclerosant made into foam. The top of the saohenous vein should be
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 35

Disease review _______________________________________________________
______________________________________________________
compressed by ultrasound probe to prevent the entrance of foam in deep
veins, until spasm in the main trunk develops.
Sclerosants used are16
• Sodium tetradecyle sulphate3%
• Sodium morrhuate
• Sodium oleate
• pilidocanol
Complications of sclerotherapy: 17
• Cutanious ulcerations
• Deep vein thrombosis
• Sever head ache
• Transient blindness
• Stroke
• Death
4. Surgery:
Varicose surgery is performed18
1. To relive symptoms
2. For cosmetic reasons
3. For prophylaxes
4. To reverse skin changes and effect ulcer healing
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 36

Disease review _______________________________________________________
______________________________________________________
a. Trendelene burg operation:
It is juxt-femoral flush ligation of long saphenous vein, after ligating
superficial circumflex, superficial external pudendal, superficial epigastric
vien, deep external pudendal vein and unnamed tributaries.
b. Stripping of vein:
Using Myers stripper vein is stripped off. Stripping from below to upwards
is technically easier. Stripping avulses the vein as well as obliterates the
tributaries. Babcock stripper and rigid metal pin stripper can also be used.
Stripping of the short saphenous vein is done from ankle below upwards
after passing stripper from above downwards. It obliterates the mild calf
perforator vein, which is the common reason for recurrence.
c. Subfecial ligation of Cockett and Dodd:
Perforators marked out by fegans method. Perforators are ligated deep to the
deep fascia through the incision in antero medial side of the leg.
d. Ligation of short saphenous vein at saphenopopleteal junction.
e. Removal of superficial varicose vein by hook phleboctomy.
f. Linton’s vertical approach – subfacial ligation of perforators.
g. Subfecial endoscopic perforator ligation surgery(SEPS)
h. Radiofrequency ablation method (RFA);
A catheter is passed into long/short saphenous vein near sapheno femoral or
saphenopopliteal junction under guidance. 850C temperature maintained to
cause endothelial damage collagen denaturation and venous constriction.
Phlebectomy is done while with drawing the catheter. Operation performed
under G.A.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 37

Disease review _______________________________________________________
______________________________________________________
i. Trivex method under subcutaneous illumination and local anesthesia:
A large quantity of fluid is injected percutaniously to identify the superficial
veins. Tumescent anaesthesia causes hydrodissection. Trivex and illuminator are
placed under the skin. Dissector gently extracts veins by suction and morcellation.
Further stages of tumescence flushes all blood and delivers vaso-constriction
solutions. Solution is passed through 18-gauze needle to clear all blood underneath
j. Endo venous laser ablation (EVLA):
Under USG guidance LSV is canulted above the knee and a guide wire is
passed beyond SFJ and 5 French catheter is passed over guide wire and tip is placed 1
cm distal to junction. 200 ml of .1 % lignocaine infiltrated. Laser fiber is inserted up
to the tip of the catheter, it is withdrawn 2 cm, and laser fiber protrudes for 2 cm
.Laser fiber is fired systematically.
Using diode laser, one mm withdrawal in 2-second 7290 to 10000 C heat
produced damages endothelium and leads occlusion of vein.
k. Transilluminated phlebectomy:
Is done by passing transilluminated light under the skin and passing a rotating
blade through another small incision. Veins are grasped by rotating movements.
l. Ambulatory phlebectomy:
This is done through tiny small incision using special phleboctomy instruments.
m. Electrodessication using weak electric current:
In this method, electrical is passed through a fine needle directly into the spider
veins.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 38

Disease review _______________________________________________________
______________________________________________________
Complications of surgery:
• Considerable bruising
• Small aria numbness may be associated with intense tingling pain
(saphenous neuralgia, sural nerve injury).
• Postoperative thrombosis.
• Superficial thrombophlebitis .
• Infection.
• Haematoma formation.
• Recurrence.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 39

Disease review _______________________________________________________
______________________________________________________
Review of Literature in Ayurveda
According to Charaka
Dhamanis are pulsating structures
Srotases are secreting structures
Siras are which allows the flow of blood through them19
SIRA:
Vagbhata says, ‘Those which are blue, yellow or black, warm to touch and
bleed quickly, carry rakta20.’
GRANTHI:
The granthi is so called because of its genuine quality if grathan that is the
property of accumulation or collection. It is as follows according to shabda kalpa
dhruma.
Gradh- Curved or curl in nature. Formation of knot or twist like structure by the
quality if curliness or coiling, rippling in action21
Gradhitam- To twist into ringlets.
Granthi: - Formation of knot like structure by way of accumulation.
It also means swelling and hardening of the vessels.
DEFINITION OR NIRUKTI:
Granthi can be defined as a round mass caused by vitiation of
treedosha,mamsa, meda and sira22
According to Vagbhta, Granthi is a round and huge mass like swelling caused
by vitiation of meda, mamsa and rakta23.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 40

Disease review _______________________________________________________
______________________________________________________
According to and Bhavamisra Granthi is a round mass like swelling caused by
vitiation of mamsa and rakta24
According to Sushruta, a round, knotty, elevated swelling which is caused by
mamsa, rakta, meda25
NIDANA26
The cause for the granthi can be anything, which vitiates all the thridosha at
time, there are some factors as follows which directly result in the vitiation of tridoshs
which in turn form the cause for the granthi.
Diets that of mixed variety, indigestion , improper timing of food, combination
of food stuffs of opposite quality, putrefied water and liquor and flesh, dried
vegetables especial moolaka, residue of oil, clay , too fresh liquor. Improper dieting,
abnormal variations, wind blow from east. Due to the exertion, weakness and
abhighata.
Granthi is also manifests due to exposure to sun and due to excessive smoking
and also due to coming contact with irritants.
CLASSIFICATION (BHEDAS)
The classification is based on the predominant dosha and the site of
manifestation.
Sushruta, Bhavamishra, Yogaratnakara, classified granthi into 5 types, Charaka
said 6 types granthi and Vagbhat explained 9 types granthi rogasa. They are displayed
in the chart.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 41

Disease review _______________________________________________________
______________________________________________________
Chart No.01 Classification of Granthi roga
No Types of the
granthi
Sushruta Bhavamishra Yogaratnakara Charaka Vagbhata
1 Vataj granthi + + + + +
2 Pittaja granthi + + + + +
3 Kaphaja
granthi
+ + + + +
4 Medaja granthi + + + + +
5 Siraja granthi + + + + +
6 Mamsaja
granthi
- - + +
7 Raktaja granthi - - - +
8 Asthija granthi - - - - +
9 Vranaja
granthi
- - - - +
SAMPRAPTI OF SIRAJA GRANTHI
All the three dosha are involved in the samprapti. Initially vitiated three
dosha by there own individual causes results in the involment of Mams and Rakta.
The charestrics of granthi is i.e. swelling. The shareerak vruddha dosha invades the
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 42
Disease review _______________________________________________________
______________________________________________________
mamsa, rakta and sira. Apart of from this stanika kapha will be greatly involved in the
disease process.
The localized Vata in the diseased area accounts for the dryness, blockage and
accumulation, where as pitta results in the transformation of the entities to increase in
there number. On the other hand, the kapha gives rise to Grathana, consistence and
shape. These mechanisms are being noticed on dooshya like Mamsa, Rakta, Sira,
meda. Thus, granthi that is formed out by above mechanism is no doubt involving all
the three doshas but still the Amshams Kalpana, the Vyadhi sambhava elicits that
Kaph, and Medas will be the dominant factor in most of the granthis.
These granthi normally do not under go the suppuration but may undergo
changes in relation to the Samkshobhaka Niadana and once the change becomes
evidential, growth becomes faster and size increases.
LAKSHANA (Clinical features)
SAMANYA LAKSHANA27
1. Granthi will be round in shape
2. Knotty
3. Elevated
VISHISTA LAKSHANA (Specific features)
According to Sushruta
In persons who are weak, indulging in more of physical exercises, vata
gets aggravated, invades the net work of veins, Squeezes, constricts and dries
up and give rise to an elevated, quick developing and round swelling of veins
(Siraja Granthi).28
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 43

Disease review _______________________________________________________
______________________________________________________
According to Vagabhata,
foot soldiers immersing themselves suddenly in to the water or other
persons getting exhausted by exertion, Vata getting increased invades Siras,
causing constriction, distortion and dryness in them give rise to granthi, which
is non pulsating and painless. This is Siraja granthi.29
SADHYA ASADHYATA
Vagbhata opines that out of 9 granthi he mentioned, the vataja granthi, pittaja
granthi, kaphaja granthi, raktaja grnthi and medoja granthi are said to be sadhya30
According to sushruta, yogaratnakara, madhavakara, and bhavamishra, are of
the opines that if Saraja granthi is painful and movable, then it is krucchrasadhya.
UPADRAVA31
If this disease is treated properly in initial stage, then there is no occurrence
complication. If not treated in proper time then leads to complication.
1. Weakness.
2. Vruna.
CHIKITSA
This granthi is treated according to the Pittaja granthi chikitsa except Siraja
granthi, remaining other Granthi should be treated surgically. In initial stage,
Sahachara taila should be administer internally. Along with the Vataghna dravya.
Basti karma can be adopted32.
PATHYA33
Ahara sambandhi
Amalaki, fibery fruits, vegetables, whole grains, black and blue berries and
cherries,carrot, lemon peel, onion, brahmi, garlic, ginger, pineapple egg, milk and
meat( not red meat)
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 44

Disease review _______________________________________________________
______________________________________________________
Vihar sambandhi
Healthy walking, swimming, and cycling.
APATHYA
Alcohol, strong coffee.
SIRAGATAVATA:
Varicose can be correlated with Siragatavata.
In SiragataVata, Sthanasamshraya (localizing the vitiated Dosha and Dhatu)
occurs in Siras of the lower limb; hence, the site of the disease is to be studied well
before the treatment. In the classics, “Siras and Dhamanis” are described separately as
the channels for circulation of blood. The differentiation of Sira and Dhamani can be
understood while the following description as “Sravanat Srotamsi” means through
which blood flows constantly without any pulsation. “Dhamanat Dhamani” means to
pulsate. From this description, it is very clear that Sira is veins and Dhamani is artery.
According to Ayurveda Sira is considered as Srotas, which comes under RasaVaha,
and RaktaVaha Srotas. The occurrence of a disease starts with Doshadushya
Sammurchana, which takes place in Srotas. Srotas can be regarded as the system
through which all the metabolites are transported.
According to Charaka, Dosha, Dhatu and Mala are depended on their
respective Srotas for their formation, conduction and destruction. When Srotas gets
deranged the physiological activity of Dosha, Dhatu and Mala also get deranged. The
derangement of Srotas is called “Kha vaigunya” – Kha means a space or cavity. In the
classics two Moolasthana, have been assigned to each Srotas. If the Moolasthana is
affected then the entire Srotas is deranged. The Moolasthana of Rasa Vaha Srotas is
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 45

Disease review _______________________________________________________
______________________________________________________
described as Hrudaya and the ten Sthoola Dhamani. The Moolasthana of RaktaVaha
is Yakrit and Pleeha34.
Srotho Vaigunya:
The Samprapti of the disease takes place when the Srotas is deformed
structurally and functionally. If there is only vitiation of Dosha without any deformity
in the Srotas, the Dosha will not find a place for Samoorchana and the disease will not
be manifested35. Hence, along with maintaining of the state of equilibrium of Dosha,
the normal functioning of Srotas is very important for the prevention of diseases. One
can prevent the vitiation of Srotas by avoiding such causes that derange the normal
functioning. Regarding Rasa Vaha Srotas, excessive intake of heavy, cold and fatty
foods and disturbed mental status are the causes of vitiation. The causes of vitiation of
Rakta Vaha Srotas are intake of food material, which causes Vidaha, Snigdha Ahara
and excessive exposure to sun.36
The normal property of Rakta is lost by excessive intake of Guru, Sheeta,
Vidaha and Snigdha Ahara. Charaka has described four general defects of Srotas.
They are Atipravrutti, Sanga, Siragranthi and Vimaraga Gamana37 That means by any
of these one can identify the vitiation of the particular Srotas. In chronic condition,
Vimaraga Gamana or regurgitation is noticed as an important symptom.
The Ashrayasthana of Siragata Vata is the Sira of the lower limbs. The
vitiation of Dosha particularly Vata occurs due to the above said Ahara and Vihara
causing obstruction of the flow of blood in Sira of the lower limb. Adho-Kaya is an
important seat of Vata, where the Kutila Sira is manifested. So Tulya Dosha and
Tulya Desha make the disease Durupakrama i.e., not easily curable and the duration
of the disease becomes prolonged.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 46

Disease review _______________________________________________________
______________________________________________________
Rakta moving in their own Sira performs function such as supplying
nutrition to the tissue, colour, tactile sensation and many other functions. When it
aggravates, Rakta accumulates in its own Siras, then many diseases caused by blood
developed in the body38.
A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 47

Materials and Methods _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 56
MATERIALS AND METHODS
The present study deals with critical evaluation and analysis of both
Punarnavadi guggulu vati and Nimbadi guggulu vati on Siraja granthi.
Selection of patients
The patients suffering from Siraja granthi were selected from the out-patient
and in-patient department of PG studies in Shalya Tantra, Government Ayurvedic
Medical college and hospital, Bangalore irrespective of their sex, religion, occupation.
Materials
Materials required for the study (Fig 12, 13, 14)
1. Punarnavadi guggulu vati
2. Nimbadi guggulu vati
3. Elastic stockings
Methodology
It is a comparative study, comprising of pre-test and post-test design. For this
study, 60 patients in three different groups were taken up, the signs and symptom
before and after the treatment were observed, and recorded in the clinical proforma,
exclusively designed for study.
Inclusive criteria
• Diagnosed cases presenting lakshanas of tortuous dilated vein, ankle oedema,
skin changes and itching in the lower limb.
• Primary varicose vein confined to veins of lower extremities.

Materials and Methods _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 57
Exclusion criteria
• Varicosity associated with complications like deep vein thrombosis,
calcification, equines deformity, venous ulcer.
STUDY DESIGN
Table No.01: Study design
Group Chikitsa Prayoga
avadi
Nireekshana
Avadi for
changes with
treatment
Follow up
for
recurrence
Group A
Internally two Punarnavadi guggulu vati twice a day each weighing 500 mg
90 days On 30th day, on 60th day and on
90th day
3 months
Group B
Internally two Nimbadi
guggulu vati twice a day
each weighing 500 mg
90 days On 30th day, on 60th day and on
90th day
3 months
Group C Wearing of Elastic
Stockings during day
time
90 days On 30th day, on 60th day and on
90th day
3 months
Assessment criteria
Changes with the treatment were observed on 30th ,60th and on 90th day. The
features considered for assessment criteria are

Materials and Methods _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 58
Subjective:
1. Itching
Objective:
1. Ankle oedema.
2. Skin Changes.
3. Tortuous dilated vein.
The above parameters have been graded for statistical evaluation and to express result criteria. Subjective parameters: Table No. 02. Grading of itching
SL.NO
ITCHING GRADINGS
01 Absent 00 02 Present 01
Objective parameters: Table No. 03. Grading of Ankle oedema
SL.NO ANKLE OEDEMA GRADINGS 01 Absent 00 02 Present 01
Table No. 04. Grading of Skin changes
SL.NO
SKIN CHANGES
GRADINGS
01 No color changes 00 02 Patchy hyper pigmentation 01 03 Hyper pigmentation with
eczema 02
04 Hyper pigmentation with lipodermatosclerosis
03

Materials and Methods _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 59
Table No. 05. Grading of Tortuous dilated vein
SL.NO TORTUOUS DILATED VIEN GRADINGS 01 Absent 00 02 Present 01
Result criteria:
The total sum point of all the parameters of assessment before and after treatment
were taken into consideration to assess the total effect of the treatment, it is assessed
as follows:
1. Marked improvement - relief of >60% in clinical parameters
2. Moderate improvement - 40 to 60% relief in clinical parameters.
3. Mild improvement - less than 40% relief in clinical parameters.
4. No change - 0% no relief in clinical parameters.

Materials and Methods _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 60
Fig.no.12: Punarnavadi guggulu Fig.no.13: Nimbadi guggulu
Fig.no.14: Stockings

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 61
OBSERVATIONS AND RESULTS
The periodical observation on different aspect of the study was documented
and studied under intervals via 30th day, 60th day and 90th day in all the groups. The
observations have been presented as follows.
• Distribution or surveillance:
A subsequent survey from 2008 – 2009 of all the patients attending OPD and
IPD of Shalya Tantra, incidence of Varicose vein cases was 1.04 % in one year.
• Age wise distribution
The cases of Siraja granthi were maximum in age group of 30-39 years
(36.33%) and minimum i.e. 15% in age group of 60-69 years.(Table No.06) ( Graph
No. 01) .
Table No. 06: Age wise distribution of 60 patients of Siraja granthi
Total Age in years Group A Group B Group C
No. %
30-39 9(45.0%) 8(40.0%) 5(25.0%) 22 36.33
40-49 6(30.0%) 5(25.0%) 4(20.0%) 15 25
50-59 2(10.0%) 2(10.0%) 10(50.0%) 14 23.33
60-69 3(15.0%) 5(25.0%) 1(5.0%) 9 15
Total 20(100.0%) 20(100.0%) 20(100.0%) 60 100
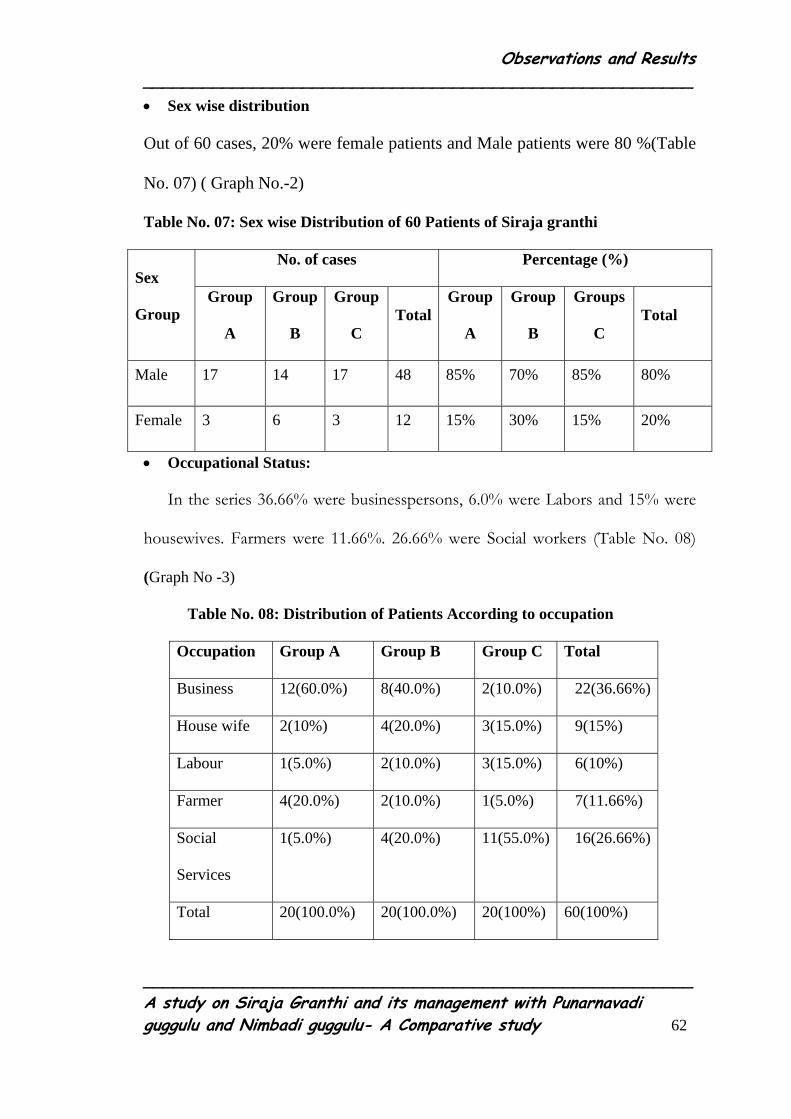
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 62
• Sex wise distribution
Out of 60 cases, 20% were female patients and Male patients were 80 %(Table
No. 07) ( Graph No.-2)
Table No. 07: Sex wise Distribution of 60 Patients of Siraja granthi
No. of cases Percentage (%) Sex
Group Group
A
Group
B
Group
C Total
Group
A
Group
B
Groups
C Total
Male 17 14 17 48 85% 70% 85% 80%
Female 3 6 3 12 15% 30% 15% 20%
• Occupational Status:
In the series 36.66% were businesspersons, 6.0% were Labors and 15% were
housewives. Farmers were 11.66%. 26.66% were Social workers (Table No. 08)
(Graph No -3)
Table No. 08: Distribution of Patients According to occupation
Occupation Group A Group B Group C Total
Business 12(60.0%) 8(40.0%) 2(10.0%) 22(36.66%)
House wife 2(10%) 4(20.0%) 3(15.0%) 9(15%)
Labour 1(5.0%) 2(10.0%) 3(15.0%) 6(10%)
Farmer 4(20.0%) 2(10.0%) 1(5.0%) 7(11.66%)
Social
Services
1(5.0%) 4(20.0%) 11(55.0%) 16(26.66%)
Total 20(100.0%) 20(100.0%) 20(100%) 60(100%)

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 63
• Habitat wise distribution:
Cases were analyzed in view of their habitat. Out of 60 cases of Siragatavata
maximum i.e. 78.33%, patients were from urban area while 21.66% patients were
reported from rural area (Table. No 09) (Graph No.-4)
Table. No. 09: Habitat wise Distribution of 60 Patients of Siraja granthi
Habitat No. of Cases Percentage
Rural 13 21.66%
Urban 47 78.33%
Total 60 100%
• Distribution of patients according to Agni
The present study showed that maximum 41% of patients had Mandagni,
38% had Samagni and 20% had Vishamagni. (Table No .10) (Graph No.5)
Table. No. 10: Distribution of the Patients According to Agni
Group A Group B Group C Total Agni
No. % No. % No. % No. %
Sama 9 45% 7 35% 7 35% 23 38.33%
Manda 4 20% 12 60% 9 45% 25 41.66%
Vishama 7 35% 1 5% 4 20% 12 20%
Total 20 100 20 100% 20 100% 60 100%
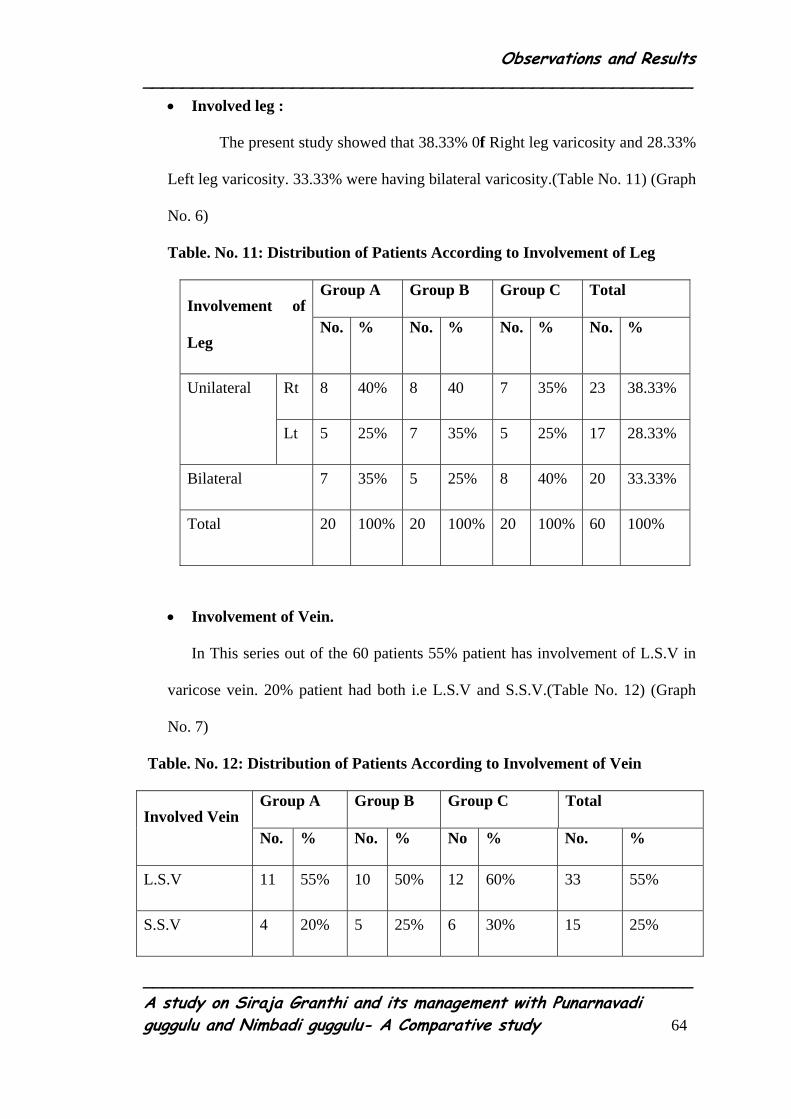
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 64
• Involved leg :
The present study showed that 38.33% 0f Right leg varicosity and 28.33%
Left leg varicosity. 33.33% were having bilateral varicosity.(Table No. 11) (Graph
No. 6)
Table. No. 11: Distribution of Patients According to Involvement of Leg
Group A Group B Group C Total Involvement of
Leg No. % No. % No. % No. %
Rt 8 40% 8 40 7 35% 23 38.33% Unilateral
Lt 5 25% 7 35% 5 25% 17 28.33%
Bilateral 7 35% 5 25% 8 40% 20 33.33%
Total 20 100% 20 100% 20 100% 60 100%
• Involvement of Vein.
In This series out of the 60 patients 55% patient has involvement of L.S.V in
varicose vein. 20% patient had both i.e L.S.V and S.S.V.(Table No. 12) (Graph
No. 7)
Table. No. 12: Distribution of Patients According to Involvement of Vein
Group A Group B Group C Total Involved Vein
No. % No. % No % No. %
L.S.V 11 55% 10 50% 12 60% 33 55%
S.S.V 4 20% 5 25% 6 30% 15 25%
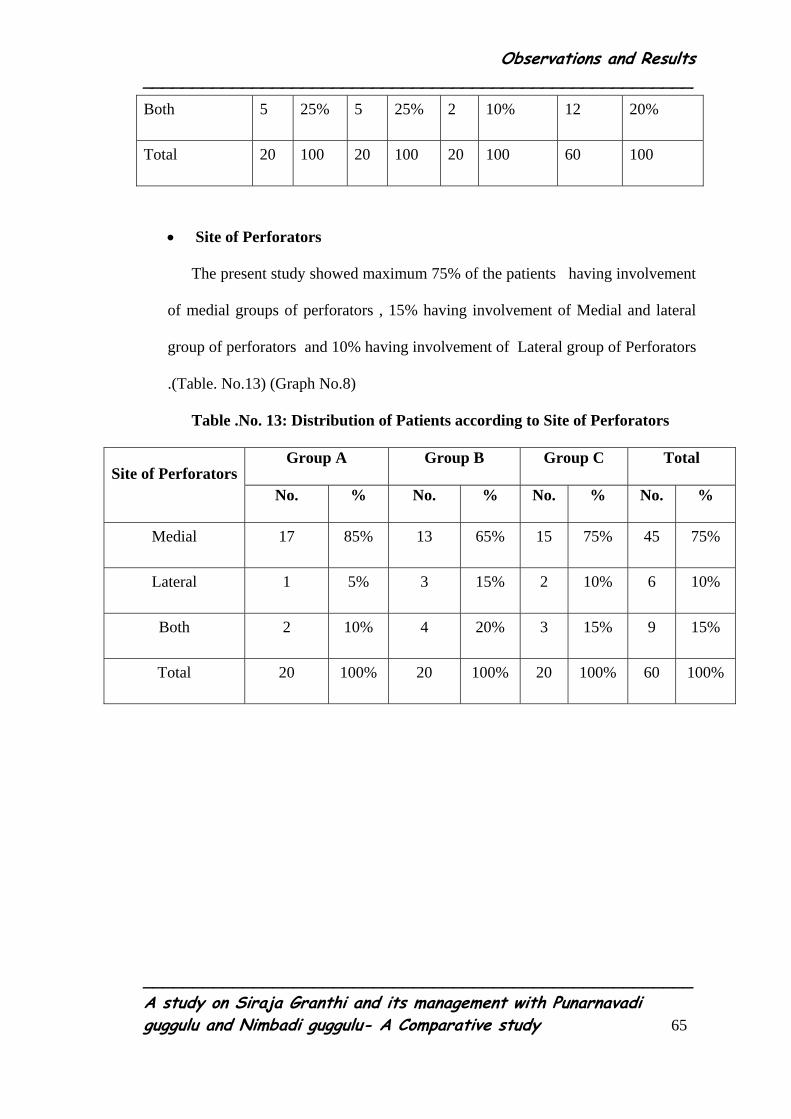
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 65
Both 5 25% 5 25% 2 10% 12 20%
Total 20 100 20 100 20 100 60 100
• Site of Perforators
The present study showed maximum 75% of the patients having involvement
of medial groups of perforators , 15% having involvement of Medial and lateral
group of perforators and 10% having involvement of Lateral group of Perforators
.(Table. No.13) (Graph No.8)
Table .No. 13: Distribution of Patients according to Site of Perforators
Group A Group B Group C Total Site of Perforators
No. % No. % No. % No. %
Medial 17 85% 13 65% 15 75% 45 75%
Lateral 1 5% 3 15% 2 10% 6 10%
Both 2 10% 4 20% 3 15% 9 15%
Total 20 100% 20 100% 20 100% 60 100%

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 66
• Incidence of lakshanas in Trail groups
In Group A, 60% patients had itching, in Group B-70% patient had itching and
in Group C 70% patient had itching.
In Group A, 80% patients had ankle oedema, in Group B-65% patients had
ankle oedema and in Group C 80% patient had ankle oedema.
In Group A, 95% patients had skin changes, in Group B-65% patients had skin
changes and in Group C-95% patients had skin changes.
In Group A, Group B and Group C-100% patients tortuous dilated vein(Table
No.14) (Graph No. 9)
Table.No. 14 Incidence of Lakshanas in trail groups
Lakshanas Group A Group B Group C
Itching 60% 70% 70%
Ankle oedema 80% 65% 80%
Skin changes 95% 65% 95%
Tortuous
dilated vein
100% 100% 100%

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 67
• Effect of Punarnavadi guggulu vati on the Itching
Before the treatment, Itching was 60%, which was reduced to the 45% on the
60th day and at the end of the treatment, it remained 45%. The relief was 15% (P
Value is 0.0186). Thus, the effect of Punarnavadi guggulu vati on the itching was not
significant. (Table No 15).
Table .No. 15: Effect of the Punarnavadi guggulu vati on Itching.
Group A
Before
treatment
30th day 60th day After
treatment
%
change
P
value
Itching
absent
8(40.0%) 8(40.0%) 11(55.0%) 12(60.0%) +20.0%
Itching
present
12(60.0%) 12(60.0%) 9(45.0%) 9(45.0%) -15.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
0.186
• Effect of Nimbadi guggulu vati on the itching.
Before the treatment, itching was 70% and after 30th day it reduced to 60%
and at the end of the treatment, it was reduced to 25%. The relief was 45% (P value is
0.021) .Thus, the effect of the Nimbadi guggulu vati on itching was moderately
significant. (Table No 16).

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 68
Table .No. 16: Effect of Nimbadi guggulu vati on itching.
Group B
Before
treatment
30th day 60th day After
treatment
%
change
P
value
Itching
absent
6(30.0%) 8(40.0%) 10(50.0%) 15(75.0%) +45.0%
Itching
present
14(70.0%) 12(60.0%) 10(50.0%) 5(25.0%) -45.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
0.021*
• Effect of the elastic stocking on itching.
Before the treatment, the itching was 70%, which after the 30th day reduced to 65%,
and at the end of the treatment, it was reduced to 45%. The relief was 25% (P value is
0.112) .Thus the effect of the Elastic stocking on the itching is statistically non-
significant. (Table No. 17).
Table .No. 17: Effect of the elastic stocking on the itching.
Group C
Before
treatment
30th day
60th day
After
treatment
%
change
P
value
Itching
absent
6(30.0%) 7(35.0%) 10(50.0%) 11(55.0%) +25.0%
Itching
present
14(70.0%) 13(65.0%) 10(50.0%) 9(45.0%) +25.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
0.112
P value 0.833 1.0000 1.000 0.367 -
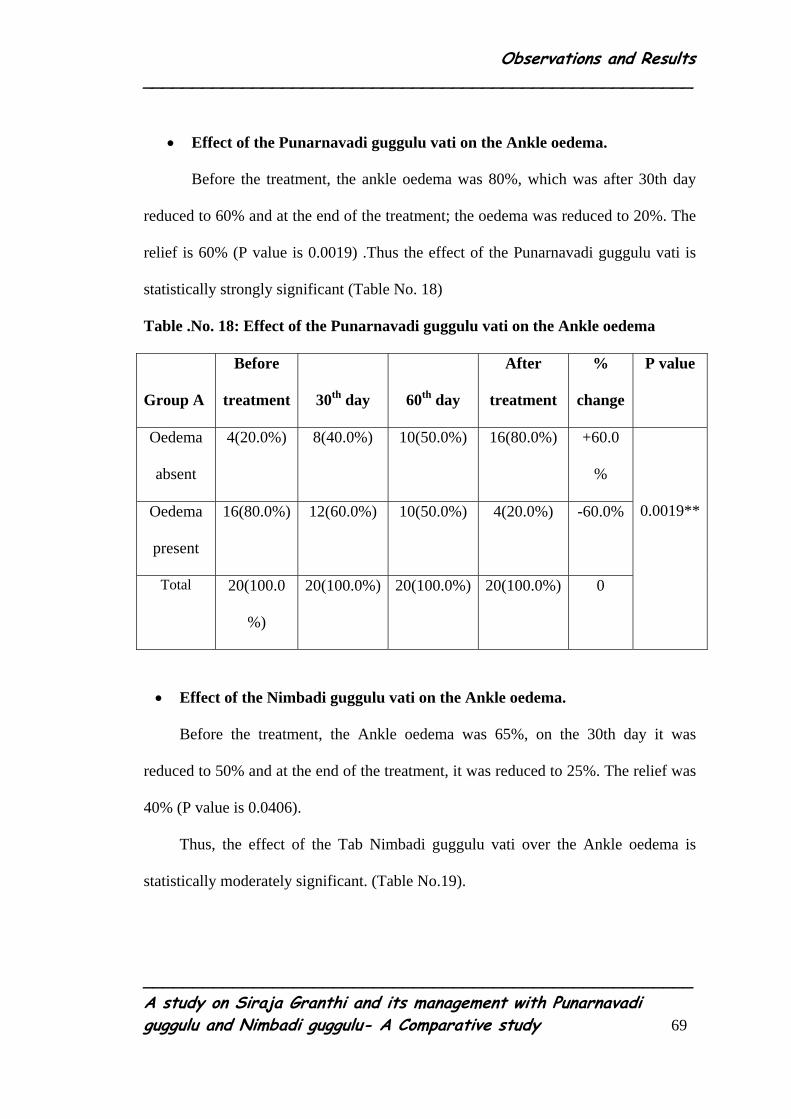
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 69
• Effect of the Punarnavadi guggulu vati on the Ankle oedema.
Before the treatment, the ankle oedema was 80%, which was after 30th day
reduced to 60% and at the end of the treatment; the oedema was reduced to 20%. The
relief is 60% (P value is 0.0019) .Thus the effect of the Punarnavadi guggulu vati is
statistically strongly significant (Table No. 18)
Table .No. 18: Effect of the Punarnavadi guggulu vati on the Ankle oedema
Group A
Before
treatment
30th day
60th day
After
treatment
%
change
P value
Oedema
absent
4(20.0%) 8(40.0%) 10(50.0%) 16(80.0%) +60.0
%
Oedema
present
16(80.0%) 12(60.0%) 10(50.0%) 4(20.0%) -60.0%
Total 20(100.0
%)
20(100.0%) 20(100.0%) 20(100.0%) 0
0.0019**
• Effect of the Nimbadi guggulu vati on the Ankle oedema.
Before the treatment, the Ankle oedema was 65%, on the 30th day it was
reduced to 50% and at the end of the treatment, it was reduced to 25%. The relief was
40% (P value is 0.0406).
Thus, the effect of the Tab Nimbadi guggulu vati over the Ankle oedema is
statistically moderately significant. (Table No.19).

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 70
Table. No. 19: Effect of the Nimbadi guggulu vati on the Ankle oedema.
Group B
Before
treatment
30th day
60th day
After
treatment
%
change
P value
Oedema
absent
7(35.0%) 10(50.0%) 14(70.0%) 15(75.0%) +40.0%
Oedema
present
13(65.0%) 10(50.0%) 6(30.0%) 5(25.0%) +40.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
0.0406*
• Effect of the Elastic stocking wearing over the Ankle oedema.
Before wearing Elastic stocking, the Ankle oedema was 80%,and after
wearing it, Ankle oedema was reduced to 30% on the 30th day. At the end of the
treatment, it was reduced to 25%. The relief was 55 %( P value is 0.0035)(Table No.
20).
Table .No. 20: Effect of the Elastic stocking on the Ankle oedema
Group C
Before
treatment
30th day
60th day
After
treatment
%
change
P value
Oedema
absent
4(20.0%) 8(40.0%) 15(75.0%) 15(75.0%) +55.0%
oedema
present
16(80.0%) 12(60.0%) 5(25.0%) 5(25.0%) -55.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
0.0035*
P value 0.602 0.720 0.179 1.000 -
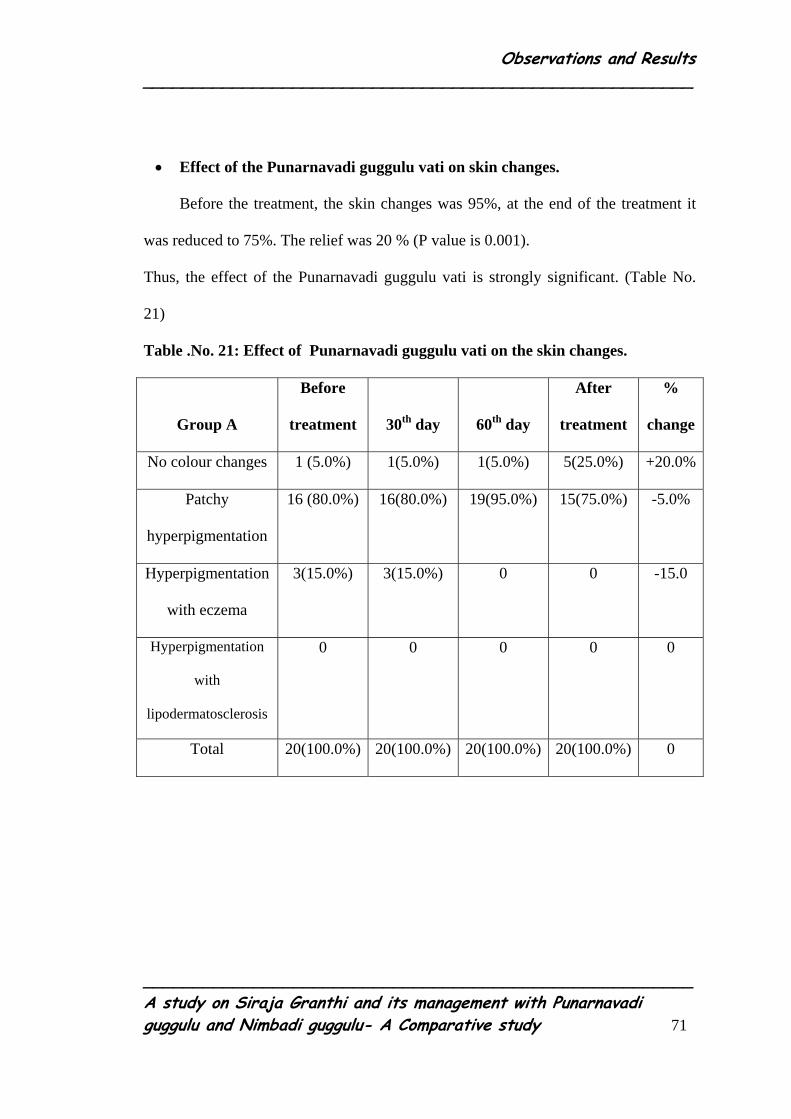
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 71
• Effect of the Punarnavadi guggulu vati on skin changes.
Before the treatment, the skin changes was 95%, at the end of the treatment it
was reduced to 75%. The relief was 20 % (P value is 0.001).
Thus, the effect of the Punarnavadi guggulu vati is strongly significant. (Table No.
21)
Table .No. 21: Effect of Punarnavadi guggulu vati on the skin changes.
Group A
Before
treatment
30th day
60th day
After
treatment
%
change
No colour changes 1 (5.0%) 1(5.0%) 1(5.0%) 5(25.0%) +20.0%
Patchy
hyperpigmentation
16 (80.0%) 16(80.0%) 19(95.0%) 15(75.0%) -5.0%
Hyperpigmentation
with eczema
3(15.0%) 3(15.0%) 0 0 -15.0
Hyperpigmentation
with
lipodermatosclerosis
0 0 0 0 0
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 72
• Effect of the Nimbadi guggulu vati on the skin changes.
Before the treatment, skin changes was 65%. At the end of the treatment, this
was reduced to the 60%. The relief was 5% (P value is 0.015) .Thus, the effect of the
Nimbadi guggulu vati is moderately significant. (Table No. 22)
Table .No. 22 Effect of the Nimbadi guggulu vati on the skin changes.
Group B
Before
treatment
30th day
60th day
After
treatment
%
change
No colour changes 7(35.0%) 7(35.0%) 7(35.0%) 8(40.0%) +5.0%
Patchy
hyperpigmentation
3(15.0%) 4(20.0%) 6(30.0%) 6(30.0%) +15.0%
Hyperpigmentation
with eczema
7(35.0%) 6(30.0%) 4(20.0%) 4(20.0%) -15.0%
Hyperpigmentation
with
lipodermatosclerosis
3(15.0%) 3(15.0%) 3(15.0%) 2(10.0%) -5.0%
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
• Effect of the Elastic stocking on the skin changes.
Before wearing of the Elastic stockings, the skin changes was 95%. At the
end of the treatment, it was reduced to the 65%. The relief was 30% (P Value is
<0.001). (Table No. 23)
Thus, the effect of the Elastic stocking on the skin changes is strongly
significant.
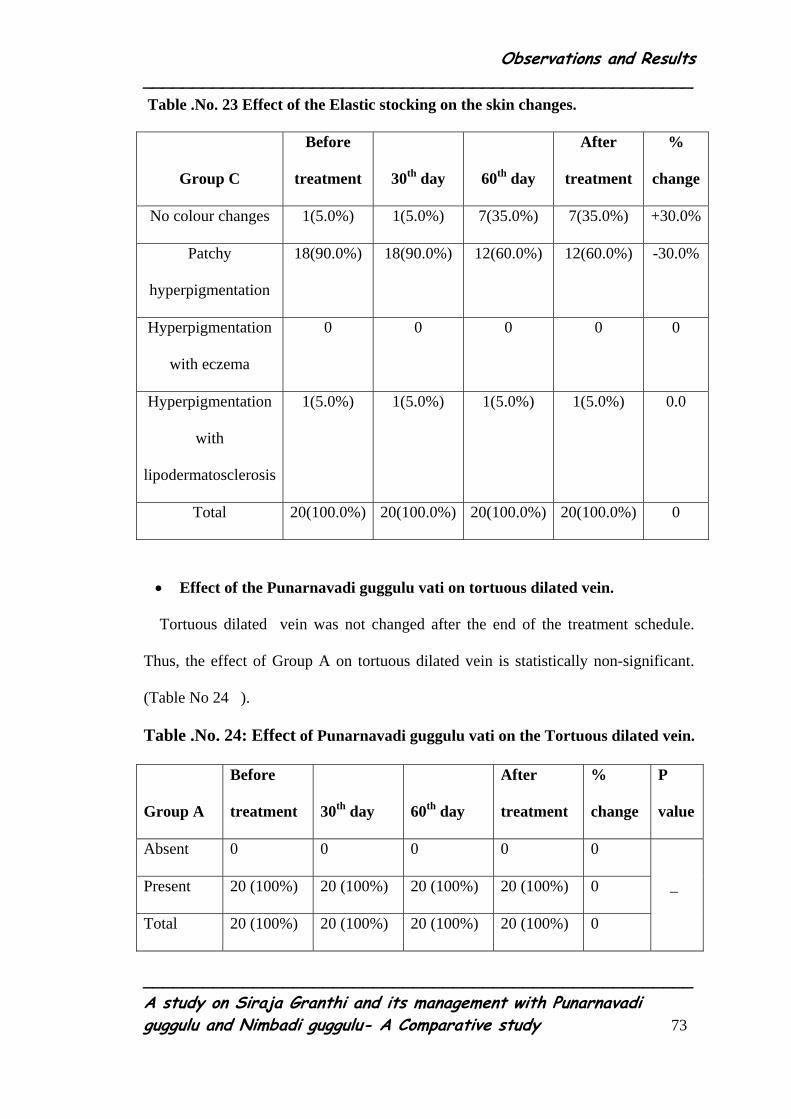
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 73
Table .No. 23 Effect of the Elastic stocking on the skin changes.
Group C
Before
treatment
30th day
60th day
After
treatment
%
change
No colour changes 1(5.0%) 1(5.0%) 7(35.0%) 7(35.0%) +30.0%
Patchy
hyperpigmentation
18(90.0%) 18(90.0%) 12(60.0%) 12(60.0%) -30.0%
Hyperpigmentation
with eczema
0 0 0 0 0
Hyperpigmentation
with
lipodermatosclerosis
1(5.0%) 1(5.0%) 1(5.0%) 1(5.0%) 0.0
Total 20(100.0%) 20(100.0%) 20(100.0%) 20(100.0%) 0
• Effect of the Punarnavadi guggulu vati on tortuous dilated vein.
Tortuous dilated vein was not changed after the end of the treatment schedule.
Thus, the effect of Group A on tortuous dilated vein is statistically non-significant.
(Table No 24 ).
Table .No. 24: Effect of Punarnavadi guggulu vati on the Tortuous dilated vein.
Group A
Before
treatment
30th day
60th day
After
treatment
%
change
P
value
Absent 0 0 0 0 0
Present 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
Total 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
_

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 74
• Effect of the Nimbadi guggulu vati on tortuous dilated vein.
Tortuous dilated vein was not changed after the end of the treatment schedule.
Thus, the effect of Group B on tortuous dilated vein is statistically non-significant.
(Table No 25 ).
Table .No. 25: Effect of Nimbadi guggulu vati on the Tortuous dilated vein.
Group B
Before
treatment
30th day
60th day
After
treatment
%
change
P
value
Absent 0 0 0 0 0
Present 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
Total 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
_
• Effect of Elastic stockings on tortuous dilated vein.
Tortuous dilated vein was not changed after the end of the treatment schedule.
Thus, the effect of Group C on tortuous dilated vein is statistically non-significant.
(Table No 26 ).
Table .No. 26: Effect of Elastic stockings on the tortuous dilated vein.
Group C
Before
treatment
30th day
60th day
After
treatment
%
change
P
value
Absent 0 0 0 0 0
Present 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
Total 20 (100%) 20 (100%) 20 (100%) 20 (100%) 0
_
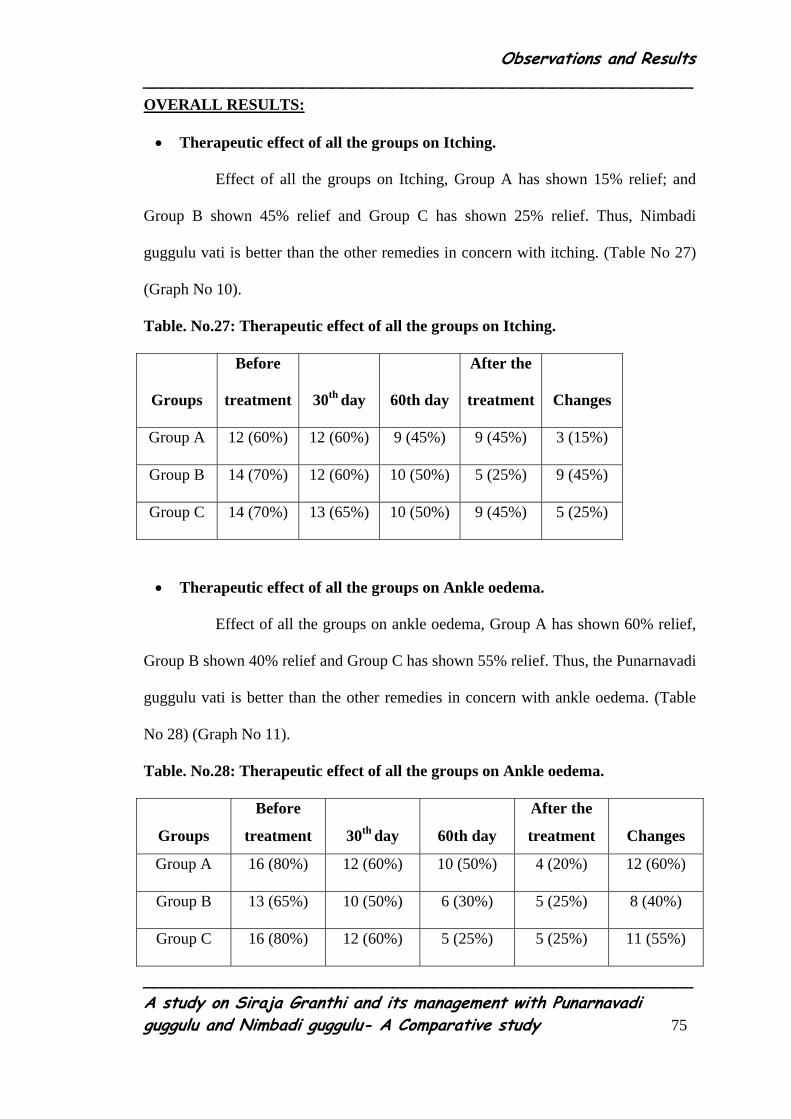
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 75
OVERALL RESULTS:
• Therapeutic effect of all the groups on Itching.
Effect of all the groups on Itching, Group A has shown 15% relief; and
Group B shown 45% relief and Group C has shown 25% relief. Thus, Nimbadi
guggulu vati is better than the other remedies in concern with itching. (Table No 27)
(Graph No 10).
Table. No.27: Therapeutic effect of all the groups on Itching.
Groups
Before
treatment
30th day
60th day
After the
treatment
Changes
Group A 12 (60%) 12 (60%) 9 (45%) 9 (45%) 3 (15%)
Group B 14 (70%) 12 (60%) 10 (50%) 5 (25%) 9 (45%)
Group C 14 (70%) 13 (65%) 10 (50%) 9 (45%) 5 (25%)
• Therapeutic effect of all the groups on Ankle oedema.
Effect of all the groups on ankle oedema, Group A has shown 60% relief,
Group B shown 40% relief and Group C has shown 55% relief. Thus, the Punarnavadi
guggulu vati is better than the other remedies in concern with ankle oedema. (Table
No 28) (Graph No 11).
Table. No.28: Therapeutic effect of all the groups on Ankle oedema.
Groups
Before
treatment
30th day
60th day
After the
treatment
Changes
Group A 16 (80%) 12 (60%) 10 (50%) 4 (20%) 12 (60%)
Group B 13 (65%) 10 (50%) 6 (30%) 5 (25%) 8 (40%)
Group C 16 (80%) 12 (60%) 5 (25%) 5 (25%) 11 (55%)

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 76
• Therapeutic effect of all the groups on Skin changes.
Effect of all the groups on skin changes, Group A has shown 20% relief,
Group B shown 5% relief and Group C has shown 30% relief. Thus, Wearing of
Elastic stockings is better than the other remedies in concern with skin changes.
(Table No 29) (Graph No 12).
Table .No. 29: Therapeutic effect of all the groups on skin changes.
Skin changes
Before
treatment
30th day
60th day
After
treatment
%
change
Group A 19 (95%) 19 (95%) 19 (95%) 15 (75%) 4 (20%)
Group B 13 (65%) 13 (65%) 13 (65%) 12 (60%) 1 (5%)
Group C 19 (95%) 19 (95%) 13 (65%) 13 (65%) 6 (30%)
• Therapeutic effect of all the groups on Tortuous dilated vein.
There was no change found in tortuous dilated vein. Therefore, the action of the
drugs and Elastic stocking was statistically non-significant. (Table No 30). (Graph No
13)
Table. No. 30: Therapeutic effect of all the groups on Tortuous dilated vein.
Grossly dilated
tortuous Vein
Before
treatment
30th day
60th day
After
treatment
%
change
Group A 20 (100%) 20(100%) 20(100%) 20 (100%) 0.0%
Group B 20 (100%) 20(100%) 20(100%) 20 (100%) 0.0%
Group C 20 (100%) 20(100%) 20(100%) 20 (100%) 0.0%

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 77
Overall response of the therapies on Siraja granthi:
• Overall effect of the Punarnavadi guggulu vati on Siraja granthi.
Considering the overall response of the patients to the therapy with
Punarnavadi guggulu vati, 14 patients got mild improvement and 3 patients got
moderate improvement. 3 patients showed no changes.
• Overall effect of the Nimbadi guggulu vati on Siraja granthi.
Considering the overall response of the patients to the therapy with
Nimbadi guggulu vati, 8 patients got mild improvement and 5 patients got
moderate improvement and 2 patients showed marked improvement. No changes
were observed in 5 patients.
• Overall effect of the Elastic stockings on Siraja granthi.
Considering the overall response of the patients to the therapy with Elastic
stockings, 9 patients got mild improvement and 4 patients got moderate improvement.
No changes were observed in 7 patients.
• Hence, Group A was best of all the groups. Group B is better than the Group C.
(Table No. 31) (Graph No.14 )
Table No.31: Overall response of the therapies on Siraja granthi.
Percentage of relief Group A Group B Group C Total
>60% 0 2 0 2
40 to 60 % 3 5 4 12
<40 % 14 8 9 31
No changes 3 5 7 15
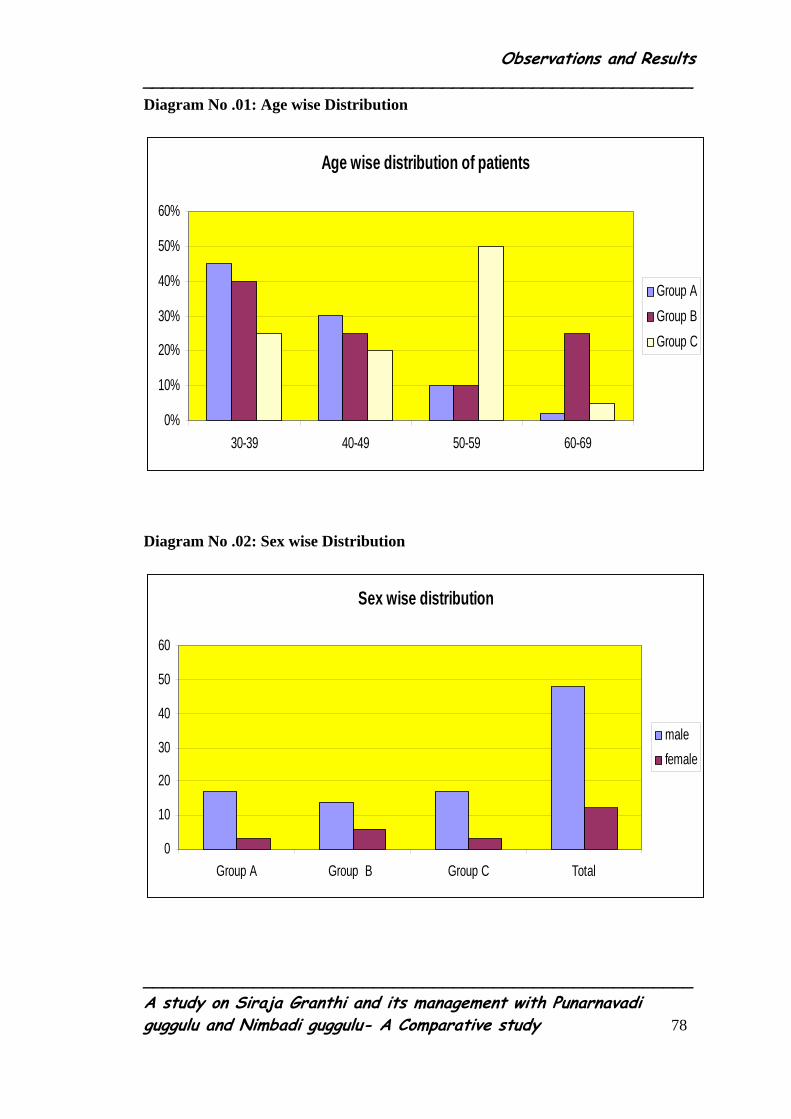
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 78
Diagram No .01: Age wise Distribution
Age wise distribution of patients
0%
10%
20%
30%
40%
50%
60%
30-39 40-49 50-59 60-69
Group AGroup BGroup C
Diagram No .02: Sex wise Distribution
Sex wise distribution
0
10
20
30
40
50
60
Group A Group B Group C Total
male female

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 79
Diagram No .03: Incidence of Occupational Status
0%
10%
20%
30%
40%
50%
60%
70%
Buisiness House wife Labor Farmer Socialworkers
Group AGroup BGroup CTotal
Diagram No .04: Incidence of Habitat
Rural Urban
Incidence of Habitat
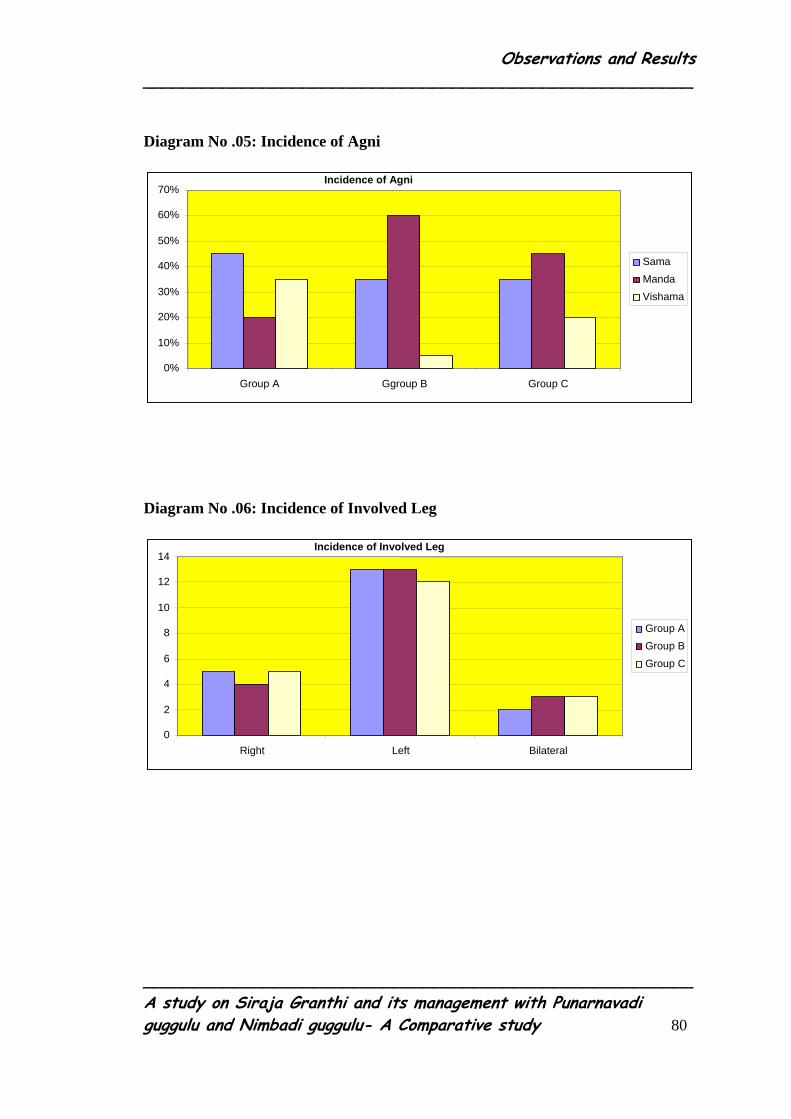
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 80
Diagram No .05: Incidence of Agni
0% 10% 20% 30% 40% 50% 60% 70%
Group A Ggroup B Group C
SamaMandaVishama
Incidence of Agni
Diagram No .06: Incidence of Involved Leg
0
2
4
6
8
10 12 14
Right Left Bilateral
Group AGroup BGroup C
Incidence of Involved Leg

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 81
Diagram No .07: Incidence of Involved Veins.
0% 10% 20% 30% 40% 50% 60% 70%
Group A Group B Group C Total
L.S.VS.S.VBoth
Incidence of Involved Vein
Diagram No. 8: Incidence of Involved Perforators
Site of Perforators
02468
1012141618
Medial Lateral Both
Group AGroup B Group C
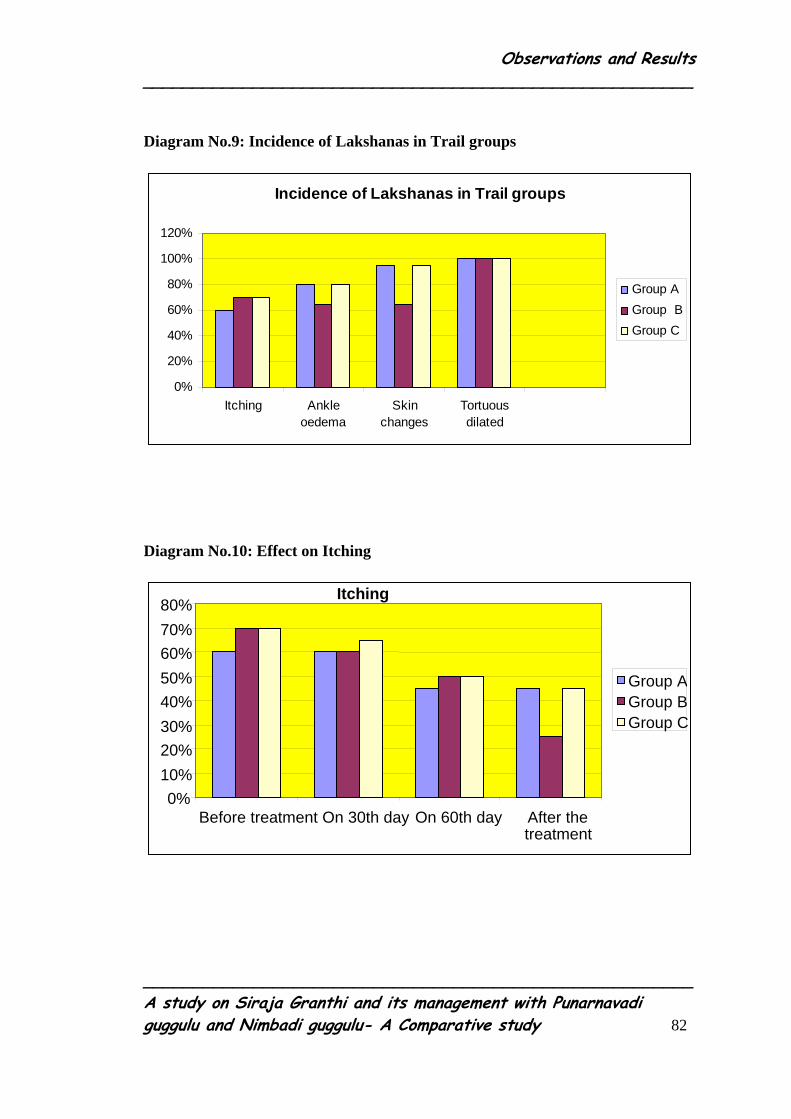
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 82
Diagram No.9: Incidence of Lakshanas in Trail groups
Incidence of Lakshanas in Trail groups
0%
20%
40%
60%
80%
100%
120%
Itching Ankleoedema
Skinchanges
Tortuousdilated
Group AGroup BGroup C
Diagram No.10: Effect on Itching
0%10% 20% 30% 40% 50% 60% 70% 80%
Before treatment On 30th day On 60th day After the treatment
Group A Group BGroup C
Itching

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 83
Diagram No.11: Effect on ankle oedema
Ankle oedema
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Before treatment On 30th day On 6oth day After thetreatment
Group A
Group B
Group C
Diagram.No.12: Effect on skin changes
Therapeutic effect in three groups on skin changes
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
Before treatment 30th day 60th day After treatment
Group AGroup B GroupC

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 84
Diagram No.13: Effect of all groups on tortuous dilated vein
Effect of all groups on Tortuous dilated vein
0 0.2 0.4 0.6 0.8
1 1.2
Before treatment 30th day 60th day After treatment
Group AGroup B Group C
Diagram No.14: Overall Response of the Therapies
Overall Response of the Therapies
0 2 4 6 8
10 12 14 16
No changes Mild Improvement
ModerateImprovement
MarkedImrovement
Group AGroup B Group C
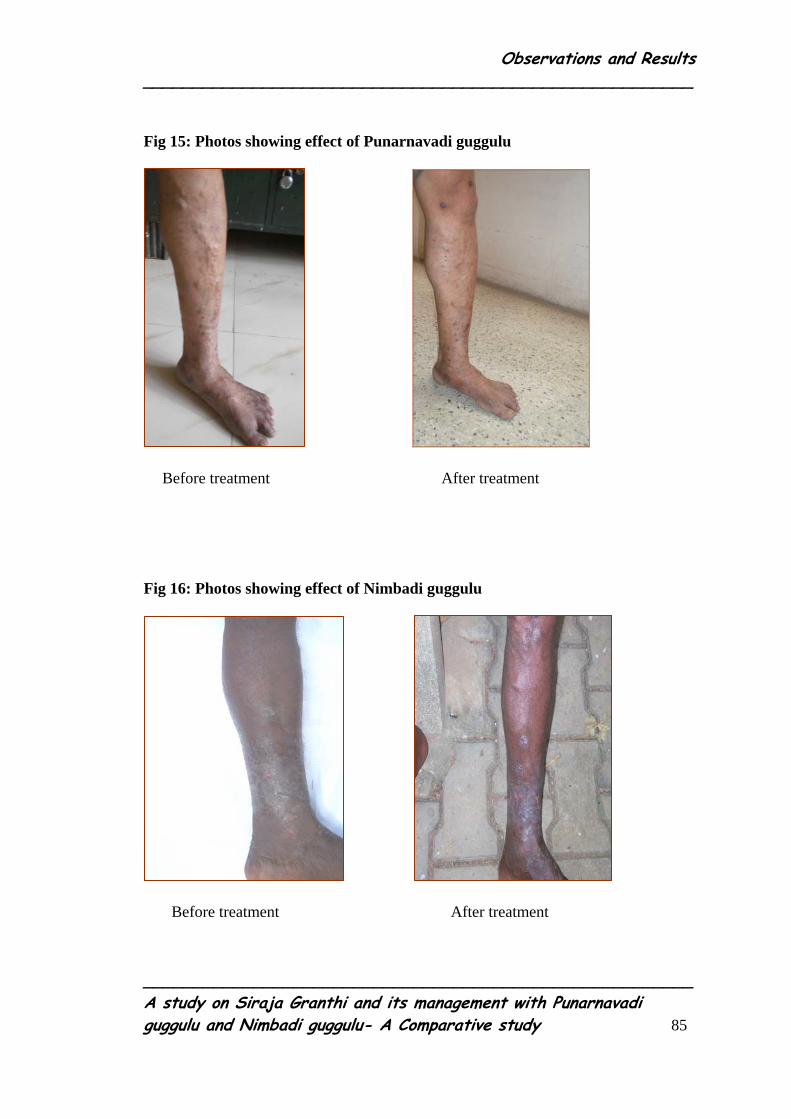
Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 85
Fig 15: Photos showing effect of Punarnavadi guggulu
Before treatment After treatment
Fig 16: Photos showing effect of Nimbadi guggulu
Before treatment After treatment

Observations and Results _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 86
Fig 17: Photos showing effect of Elastic stocking
Before treatment After treatment

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 87
DISCUSSION
Discussion constitutes the proper interpretation of different aspects of the
comparative study. A scientific and critical discussion always enriches the sciences by
adding facts to it. In the present study, discussions were made on three main headings
namely:
Discussion on Review of literature
Discussion on Methodology
Discussion on Observation and Results
Discussion on review of literature:
Siraja granthi one among the granthi rogas described in various ayurvedic
classics, denotes a pathological condition characterized by an elevated, quick
developing and round swelling of veins, which are non pulsating and painless. It
would have given a clear-cut picture of the varicose vein if there is a crystal clear
description of its related anatomy and pathology.
To add to the confusion and controversy the various misinterpretations,
additions of new coined recent authors have enumerated terms and new visions,
which are based on present contemporary science. However, it is important to
understand the sciences of Ayurveda based on its basic description of principles.
The disease Siraja granthi is described in the context of Granthi-apachi-arbuda
-galaganda chapter by Sushruta and Vaghbata.

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 88
Siraja granthi
Symptomatologies of Siraja granthi indicate the correlation towards the
Varicose veins. The following points can clarify it.
Table.No.32: Co relation between Siraja granthi and varicose vein
Siraja granthi Varicose vein
Involved
structure
Sira
Vein
Symptoms Sampeedya, Nispuram,
Nirujam.
Diffuse dull ache pain.
Signs Sankochya, Vrutta, Unnata,
Vakrikrutya, Shopham.
Dilated, elongated and tortuous vein,
Superficial thrombophlebitis.
The co-related disorder pattern is equivocal in both Siraja granthi and varicose
vein.
The main aims of the treatment in contemporary science are to strengthen the
veins wall and valves, to achieve the good venous flow from the lower extremities
and to avoid the complications of varicose vein. The treatment principle described in
the Ayurveda like external application of Sahacharadi taila, internal vatahara basti,
and Para surgical procedures such as Jaloukavacharana and Siravyadha serves the
above aim of the treatment.

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 89
Discussion on the Methodology:
Various formulations have been described in Ayurvedic classics for the
management of the Siraja granthi. Handful of researches mainly on external
application of the Sahacharadi taila and internal Administration of the Lashunadi vati
and Para surgical procedures were carried in different centers. It’s the matter of
interest to explore a simple formulation like Punarnavadi guggulu vati or Nimbadi
guggulu vati in the management of the varicose vein supported by Pilot study. Hence,
the study was taken up to see the efficacy of the Punarnavadi guggulu and Nimbadi
guggulu. Both being the Drug trail groups, it was important to have a control group to
compare the results. Hence, a control group in the form of the conservative line of
treatment, through application of Elastic stocking was advised.
The selected patients were assigned into 3 groups. Group A and Group B were
prescribed specific drugs for 90 days and Group C was advised to wear the Elastic
stockings
The symptoms and signs were assessed by observational facts, before, during
and after the treatment. The obtained results were statistically analyzed and
interpreted.
Discussion on Observational study:
• Age:
Out of 60 patients, the cases of Siraja granthi were maximum in age group of
30-39 years (36.33%) and minimum in age group of 60-69 years (15%). Age has no
relevance with that of treatment procedures as similar type of manifestation were
elicited in all the age group (Vide on Table No. 06).

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 90
• Sex:
Out of 60 cases, 20% of them were female patients and 80% of them were
male patients. Sex has no relevance with that of treatment procedures as similar
type of manifestation were elicited in all group (Vide on Table No 07).
• Occupational Status:
In the series, 36.66% were businesspersons, 6.0% were Laborers and 15% were
housewives, 11.66% were Farmers, 26.66% were Social workers. Businesspersons are
more prone to have this disease due to the continuous standing work. (Vide on Table
No 08).
• Habitat:
Cases were analyzed in view of their habitat. Out of 60 cases of Siraja granthi
78.33% patients were from urban area while 21.66% patients were reported from rural
area. Habitat has no relevance with that of treatment. (Vide on Table No 09).
• Agni:
The present study showed that maximum 41% of patients had Mandagni,
38% had Samagni and 20% had Vishamagni. Deepana , Pachana drugs were
given to correct the Agni before commencement of the clinical trail Agni . (Vide
On Table No 10).
• Involved leg :
In the present study, 38.33% had Right leg varicosity and 28.33% had
Left leg had varicosity. 33.33% were having bilateral varicosity. Involvement of
limbs is not related to the occurrence of the disease. (Vide on Table No 11).

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 91
• Involved vein:
In this series, out of the 60 patients,55% patient had varicosity of L.S.V ,
20% patient had both i.e. varicosity of L.S.V and S.S.V . This reveals that L.S.V
is most affected by varicosity. (Vide on Table No 12).
• Perforators:
The present study showed maximum 75% of the patients having
involvement of medial groups of perforators, 15% having involvement of Medial
and lateral group of perforators and 10% having involvement of Lateral group of
Perforators. The maximum number of patients (75%) suffered from the medial
group of perforators. (Vide on Table No 13)
• Lakshanas :
With regards to the lakshanas, it is evident that tortuous dilated veins were
present in all the cases while the remaining lakshanas were present between 60% -
80%. However, skin changes were present in all the cases. The response to the
treatment was more conspicuous as far as skin changes are concerned. On the
other hand appreciable changes were seen in other lakshanas like itching and
ankle oedema while no notable changes was seen in the tortuous dilated veins.
(Vide on Table No 14)
• Follow up study:
The patients were advised to attend the OPD after completion of three months.
No changes was reported within three months of follow up period as they had
been instructed not to stand continuously for long periods and advised to keep the
foot elevated while sleeping.

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 92
Discussion on Results
• Probable mode of action of Punarnavadi guggulu vati on Siraja granthi :
By virtue of its Pittakapha shonita nashana, kandu hara, kustha hara,
varnya, Shopha hara, and Anti-inflammatory properties, it effectively reduces the
pigmentation of skin over Siraja granthi pradesha. The skin attains smoothness, looses
the dark pigmentation, itching and vicharchikavat lakshana are reduced. Swelling
around the Ankle joint is reduced which is suggestive of good venous flow.
• Probable mode of action Nimbadi guggulu on the Siraja granthi :
By virtue of its Kapha-pitta hara, Shotha hara, Kustha hara, Udarda
prashamana, Kandoohara, Varnya and Anti-inflammatory properties, it effectively
removes the Kupita dosha from the twacha, which helps in achieving the Prakruta
varna of twacha. It also reduces the eczematous changes and Ankle swelling.
• Probable mode of action of Elastic Stockings on the Siraja granthi : Compression stockings are used to support the veins of the leg. They offer
graduated compression where maximum compression is achieved. This
compression, when combined with the muscle pump effect of the calf, helps in
movement of blood. The External support to the vein reduces the hydrostatic
pressure of the vein lumen. It prevents the venous stasis. By the virtues of these
properties, it helps in the reduction of swelling, itching, and restores the normalcy
of the skin.

Discussion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 93
• Over all effects of the treatment in all three groups :
In Group A, Mild improvement was observed in 14 patients, Moderate
improvement was present in 3 patients.
In Group B, Mild Improvement was observed in 8 patients, Moderate
improvement was observed in 5 patients and Marked Improvement was found in 2
patients.
In Group C, Mild Improvement was observed in 9 patients and Moderate
Improvement was observed in 4 patients. (Vide on Table No 31)
Hence,
The Punarnavadi guggulu group was best of all three groups.
The Nimbadi guggulu group was better than Elastic stocking group.
The Punarnavadi guggulu was better than the Nimbadi guggulu group.

Conclusion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 94
CONCLUSION
• A subsequent survey from 2008 – 2009 of all the patients attending OPD and
IPD of Shalya Tantra, incidence of Varicose vein cases was 1.04 % in one
year.
• The cases of Siraja granthi were maximum in age group of 30-39 years.
• Incidence of male was more as far as sex distribution is concerned.
• Incidence of varicose veins was more in people belonging to the occupation
that involved standing for longer duration.
• Almost all the lakshanas were present in all patients, predominantly skin
changes.
• Long saphenous vein was predominantly involved in all the cases.
• The Punarnavadi guggulu group was best of all three groups.
• The Nimbadi guggulu group was better than Elastic stocking group.
• The Punarnavadi guggulu was better than the Nimbadi guggulu group.
Scope for further study:
• The administration of the Nimbadi guggulu vati and Punarnavadi guggulu vati
can be studied on large number of cases for observing synergistic benefits of
the treatment
• The administration of the Punarnavadi guggulu with Elastic stocking wear can
be studied in large number of cases.

Conclusion _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 95
• The administration of the Nimbadi guggulu vati with Elastic stocking wear
can be studied in large number of cases.
• The administration of the Nimbadi guggulu and Punarnavadi guggulu along
with elastic stocking can be studied in large number of cases
• This study can be taken for multi centre study.

Summary _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 96
SUMMARY
The present study entitled “A study on Siraja granthi and its management with
Punarnavadi guggulu vati and Nimbadi guggulu vati a comparative study” is mainly
based on clinical observation. The dissertation comprises of literary review, clinical
study discussion, conclusion and summary.
The first part deals with the literary aspect of the disease i.e. Siraja Granthi.
After describing Siraja granthi in detail, Siragata vata is also explained briefly and
later the varicose veins described in modern science was also reviewed.
At the outset of the second part named as clinical study, materials and
methods adopted for this study has been explained in detail. There after general
observations were made on 60 patients of Siraja granthi and results recorded in three
groups. Treatments have been presented in tabular form along with brief description
of each finding. The statistical analysis and geographical presentation of the results
also have been presented. The results obtained in the clinical study have been
discussed in the third part of dissertation designated as discussion to draw the logical
conclusion.
1. Study design
Out of 60 patients of Siraja granthi studied in the series, 20 patients were treated
with Punarnavadi guggulu vati under Group A, 20 patients were treated with
Nimbadi guggulu vati under group B and In Group C, 20 patients were advised to
wear the Elastic stockings.

Summary _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 97
Out of 60 patients of Siraja granthi (Varicose Veins) maximum were belonging to
30-39 years of age group 36.33% because of their occupation , male sex 71.66%,
urban area 78.33%, occupation businessman 31.36%, Mandagni 41.66%, bilateral
varicosity 33.33%.
2. Significant effect of Punarnavadi guggulu vati :
Punarnavadi guggulu vati has provided significant relief in Ankle oedema (60%)
and Skin changes (20%)
3. Significant effect of Nimbadi guggulu vati :
Nimbadi guggulu vati has provided moderately significance in restoring the
normalcy of the affected skin (5%) and reducing the ankle oedema (55%).
4. Significant effect of Elastic Stockings:
The wearing of Elastic stockings has provided strongly significant relief in the
Skin changes (30%), moderately significant in the relief of Ankle oedema (55%).
5. Comparison of Effect of Both the Groups:
The above results have shown the effect of treatment by Punarnavadi guggulu
vati to be more pronounced in reducing the Ankle oedema and Skin changes. Effect
of treatment by Nimbadi guggulu vati showed moderate reduction in Skin changes,
Ankle oedema and Itching. Elastic stockings were strongly significant on the Skin
changes.
Thus, the total effect of Punarnavadi guggulu vati was better than Nimbadi
guggulu vati.

Summary _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 98
6. Over all effects of the treatment in all three groups:
In Group A, mild improvement was observed in 14 patients, Moderate
Improvement was present in 3 patients.
In Group B, mild Improvement was observed in 8 patients, Moderate
improvement was observed in 5 patients and Marked Improvement was found in 2
patients.
In Group C, Mild Improvement was observed in 9 patients and Moderate
Improvement was observed in 4 patients.

References _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 99
REFERENCES
1. Su.Su 13/4
2. Http://google/sin.com varicose-vein-treatment-ayurvedic-and-home-
Remedies
3 Diseases of the veins by Norman L Browse – Chapter -1
4 Diseases of the veins by Norman L Browse – Chapter -2
5 Diseases of the veins by Norman L Browse – Chapter -2
6 Diseases of the veins by Norman L Browse – Chapter -3
7 Diseases of the veins by Norman L Browse – Chapter -4
8 A Concise text book of Surgery by S. Das Chapter -16
9 Diseases of the veins by Norman L Browse – Chapter -5
10 Diseases of the veins by Norman L Browse – Chapter -6
11 SRB’s Manual of Surgery By Sriram Bhat M. 2nd Edition Page No.198
12 http://en.wikipedia. org/ wiki /file ( varicose vein.jpg)
13 SRB’s Manual of Surgery By Sriram Bhat M. 2nd Edition Page No.198
14 Bailey and Love’s Short Practice of Surgery 25th Edition, Chapter 54,
Page No929
15 Bailey and Love’s Short Practice of Surgery 25th Edition, Chapter 54,
Page No 930
16 SRB’s Manual of Surgery By Sriram Bhat M. 2nd Edition Page No.198
17 Atlas of General surgery, compiled by sir David carte. RCG Russel,
Henry pitt. Page No1144.
References _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 100
18 Atlas of General surgery, compiled by Sir David carte,RCG
Russel,Henry pitt, Page No 1107
19 Ch. Su.30/12
20 A. S. Su. 6/8
21 Shabda Kalpa Druma by Radha kanta deva, 2nd volume, Page No 372
22 M.Ni 37/11
23 A.S.U 34/2
24 B.P. Chikitsa prakarana 9/44/11
25 Su. Ni.11/3
26 Su. Ni. 11/3
27 Su. Ni. 26/3
28 Su. U. 11/34
29 A. S. Ni. 11/8
30 A. S.U.34/3
31 Su. Ni. 11/4
32 A.S.Chi 23/46
33 http://www.varicose vein-help.com/diet-for-varicose-veins-html
34 Ch. Vi.5/8
35 Ch. Vi. 5/6
36 Ch.Vi. 5/14
37 Ch .Vi. 5/24
38 Su. Sha.7/4-5

References _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 101
39 B R 42/135
40 B B R, vol- 3,Page No 179

Bibliography _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 102
BIBLIOGRAPHY
• . Agnivesha, Charaka Samhita, Revised By Charaka and Dridhabala with
Vidyothini Hindi commentary By Pt Kashinath Shastri, Dr Gorakhanath
Chaturvedi, part II, Chaukambha Bharati Academy Varanasi, Reprint 1998
• Bailey & Love’s Short Practice of Surgery, revised by Charles V. Mann, R. C.
G. Russell, 24th Edition, 1991, ELBS with Chapman and Hall
• Bhava Mishra. Bhava Prakasha – including Nighantu portion, with Vidyotini
Hindi Commentary, edited in Hindi by Sri Bramha Shankara Mishra and Sri
Rupalalaji Vaisya, 11th ed. Varanasi: Chaukhambha Sanskrit Sansthan; 2004.
Part 1 and 2
• Charaka, Vidyotini Hindi commentary by Pt. Kashinath Sharma and Dr.G.N.
Chaturvedi, Chaukhambha Sanskrit Sansthan, Varanasi (1975).
• David C Sabiston , Jr., M.D, Essential of surgery
• Dr. Ananta Rama Sharma, Sushruta Samhita edited with Sushruthvimarshini
Hindi commentary volume I & II, Chaukambha Surabharati Prakashana,
Varanasi, First edition 2001
• Dr. Rajgopal Shenoy K, Manipal Manual of Surgery, CBS Publishers &
Distributors New Delhi, Second Edition, 2005.
• Harsh Mohan, Text Book of Pathology, Fifth Edition, Reprint 2006
• Kaviraj Govind Das Sena. Bhaishajya Ratnavali- with ‘siddhiprad’ Hindi
commentary edited by prof. Siddhi Nandan Mishra. 1st ed. Chaukambha
Surabharati prakashana ; 2005.

Bibliography _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 103
• Linda.G.Philips, David C. Sabiston (et al), Text Book of Surgery. The
Biological Basis of Modern Surgical Practice, 16th Edition, Volume I,
W.B.Saunders Company Publication.
• Madhavakara, Madhava Nidana with Madhukosha Sanskrit commentary, with
Vimala – Madhudhara Hindi commentary By Brahmanand Tripathi, Volume
II Chaukambha Surabharati Prakashana, Varanasi, Reprint 2005
• Norman L. Browse, Kevin G. Burnand, Allan T. Irvine and Nicholas M.
Wilson, Diseases of the Veins, Second Edition 1999
• R.C.G Russells (et al), Bailey & Love’s Short Practice of Surgery, Arnold
International Student edition London, 24th Edition.
• S.Das, A Concise Text Book of surgery, Dr S Das Publication Calcutta, First
Edition, Reprint 1996.
• Shabda kalpa druma, Radha kanta deva, vol 2, Naga publishers, Delhi
• Somen Das, A Manual on clinical surgery, Dr S Das Publication Calcutta,
Fourth edition Reprint 1998.
• Shri Naginadas Chaganalal. Shaha; Bharat Bhaishajya Ratnakar- edited by
Pandit Gopinath gupt. Reprint ed. New delhi B. Jain. Publishers ; 2005 vol 3 .
• Sri Ram Bhat M, SRB’s Manual of Surgery, Jaypee Brothers Publication, First
Edition 2004.
• Sushruta, Sushruta Samhita with Nibandha Sangraha commentary of Sri
Dalhanacharya. edited by Vaidya Yadavaji Trikamji Acharya, Chaukambha
Surabharati Prakashana, Varanasi, Reprint - 2003

Bibliography _______________________________________________________
_______________________________________________________ A study on Siraja Granthi and its management with Punarnavadi guggulu and Nimbadi guggulu- A Comparative study 104
• T.N.Patel, A System of Surgical Diagnosis, Jaypee Brothers Publication, Third
Edition, 1997.
• Vagbhata, Ashtanga Hridaya edited with Nirmala Hindi commentary By Dr.
Brahmanand Tripathi, Chaukambha Sanskrit Pratishthana, Varanasi
• Vagbhata, Ashtanga Sangraha with Hindi commentary volume II, By Kaviraj
Atridev Gupta, Krishnadas Academy Varanasi, reprint 1993
• Yogaratnakara – with ‘vidyotini’ Hindi commentary by Vaidya Lakshmipati
Shastri, Edited by Bhishagratna Bramhananda Shastri, 7th ed. Varanasi:
Chaukhambha Sanskrit Sansthan; 1999.

RESEARCH PROFORMA
DEPARTMENT OF P. G. STUDIES IN SHALYA TANTRA
GOVERNMENT AYURVEDIC MEDICAL COLLEGE,
BANGALORE – 560 009.
A STUDY ON SIRAJA GRANTHI AND ITS MANAGEMENT WITH PUNARNAVADI GUGGULU AND NIMBADI GUGGULU – A
COMPARATIVE STUDY Guide: Dr. B. A. Venkatesh B.S.A.M., B.A.M.S., M.D(Ayu), FICA Scholar : Dr. Nadaf A. N. Pt. Name Sl. No. & Group
OPD No. Address
IPD No
Age DOA
Sex DOD
Religion Education
Occupation Socio-economic status
Habitat Dietary Habits
Marital Status
A. PRADHANA VEDANA Duration: 01. Swelling in the lower extremities : Duration: 1) Present 2) Absent
If present – Nature of swelling – 1) Pitting 2) Non-Pitting 3) Unilateral 4) Bilateral 02. Skin changes : Duration:
1) Present 2) Absent
specify _ _ _ _ _ _ _ _ _ _
03. Itching : Duration:
1) Present 2) Absent
If pain present – Type of pain
1) Constant 2) Intermittent

B. ANUBANDHI VEDANA
1) Eczema 2) Dermatitis 3) Scaling
4) If other, specify _ _ _ _ _ _ _ _ _ _.
C. PRADHANA VEDANA VRUTTANTA
Onset of the disease in order with chronicity –
D. POORVA VYADHI VRUTTANTA History of similar previous complaints – Present / Absent
1) Hypertension 2) Diabetes 3) Tuberculosis
4) Asthma 5) COPD 6) Vericose ulcer
Give details –
History of other diseases, if any –
E. POORVA CHIKITSA VRUTTANTA Whether patient has taken treatment for present complaints?
Yes / No. If yes, give details _ _ _
History of any surgical procedures – Yes / No.
If Yes, give details –
Give the details of the management of previous similar complaints –
F. KAUTUMBIKA VRUTTANTA
Any history of similar complaints in the family Yes / No.
1) Maternal Family 2) Paternal Family
Details –
H/o of any other disease –
G. VAIYAKTIKA VRUTTANTA
01. Appetite i) Normal ii) Reduced iii) Increased
02. Bowel i) Regular ii) Irregular
04. Micturation i) Normal ii) Nocturia iii) Dysuria
05. Sleep i) Normal ii) Disturbed
06. Ahara i) Vegetarian ii) Non-vegetarian
1) Regular 2) Irregular
3) Proportionate 4) Dis-proportionate
5) Timely 6) Irrespective of time schedule
07. Vyasana – Smoking / Tobacco Chewing / Alcohol / Tea / Coffee/ others
H. GENERAL EXAMINATION
01. Pulse – / Min 02. Blood pressure – / mm of Hg
03. Temperature – 0F / Afrebrile 04. Respiratory rate – / Min
05. Conjunctiva – 06. Tongue –
07. Prakriti – 08. Satwa –
I. SYSTEMIC EXAMINATION
a) Respiratory system –
b) Cardio-vascular system –
c) Per abdomen –
J. LOCAL EXAMINATION
INSPECTION
1. Involvement of leg
2. Involvement of vein
3. Site of tortuous dilated vein

PALPATION
01. Temperature 1) Present 2) Absent
02. Cough impulse Test 1) Present 2) Absent
03. Trendelenburg Test (a) 1) Present 2) Absent
04. Trendelenburg Test (b) 1) Present 2) Absent
05. Perthe’s Test 1) Present 2) Absent
06. homan`s sign 1) Present 2) Absent
07. Tenderness 1) Present 2) Absent
08. Schwartz test 1) Present 2) Absent
K. INVESTIGATIONS
Doppler study (If necessary)
L. FINAL DIAGNOSIS
M. CHIKITSA
Group A : Punarnavadi Guggulu 500 mg Internally Two tablets twice
daily after food.
Group B : Nimbadi Guggulu 500 mg – Internally Two tablets twice
daily after food.
Group C : Advise to wear elastic stockings
SELF GRADE SCORING FOR RESULT ASSESSMENT PARAMETERS
SL. PARAMETER DESCRIPTION GRADEAbsent 0 01. Itching Present 1 Absent 0 02. Ankle Oedema Present 1 No colour changes 0 Patchy hyperpigmentation 1 Complete hyperpigmentation with eczema 2
03. Skin changes
Complete hyperpigmentation with lipodermatosclerosis
3
Absent 0 04. Tortuous dilated veins Present 1
N. ASSESSMENT OF THE THERAPY
During Treatment AT ASSESSMENT PARAMETERS BT 30 60 90 FU1 FU2 FU3
01. Itching 02. Ankle oedema 03. Skin changes
04. Tortuous dilated veins
RESULT
1) No Improvement 2) Mild Improvement 3) Moderate Improvement
4) Marked Improvement
Signature of the guide Signature of the PG Scholar

MASTER CHART
GROUP – A
GROUP – A Observational Data Clinical Data
Subjective Objective
Itching Ankle
Oedema
Skin
Changes TartuousityS. No Name O.P.No Age Sex Occup
BT AT BT AT BT AT BT AT
Follow up
1. N Prasanna 002000 34 M S 1 1 1 0 1 0 1 1 NR
2. Thiru J 000579 31 M B 0 0 1 1 1 1 1 1 NR
3. Kasturi 004072 46 F Hw 0 0 1 0 0 0 1 1 NR
4. Shankara L 000184 46 M S 1 1 1 0 1 1 1 1 NR
5. Lakshmana S 059095 66 M Fa 1 0 1 0 2 1 1 1 NR
6. Tiruvalla H 059184 39 M B 0 0 0 0 1 1 1 1 NR
7. Katta Shrihari 004072 50 M B 1 1 1 0 1 1 1 1 NR

8. Chandru D 024924 34 M Fa 1 0 1 1 2 1 1 1 NR
9. Shamalakshmi 024932 48 F Hw 1 1 1 0 1 0 1 1 NR
10. Ramachandra S 054307 35 M B 1 0 0 1 1 1 1 NR
11. P R Nagaraj 041133 32 M B 1 1 1 0 1 1 1 1 NR
12. Shrinivasa J 000492 32 M La 1 1 1 0 1 1 1 1 NR
13. Ramesh R 011663 40 M B 0 0 0 0 1 1 1 1 NR
14. N Satish 054621 47 M Fa 0 0 1 1 2 1 1 1 NR
15. Majara Mulla 054620 45 M B 1 1 1 0 1 1 1 1 NR
16. Ramadevi M 050298 60 F Hw 1 0 0 0 1 1 1 1 NR
17. Arun B 055034 32 M B 0 0 1 0 1 1 1 1 NR
18. Bharth. A 055032 32 M B 0 0 1 0 1 1 1 1 NR
19. Manimeh G 055103 60 M B 1 1 1 1 1 0 1 1 NR
20. Muniyappa J 014987 50 M Fa 0 0 1 0 1 0 1 1 NR
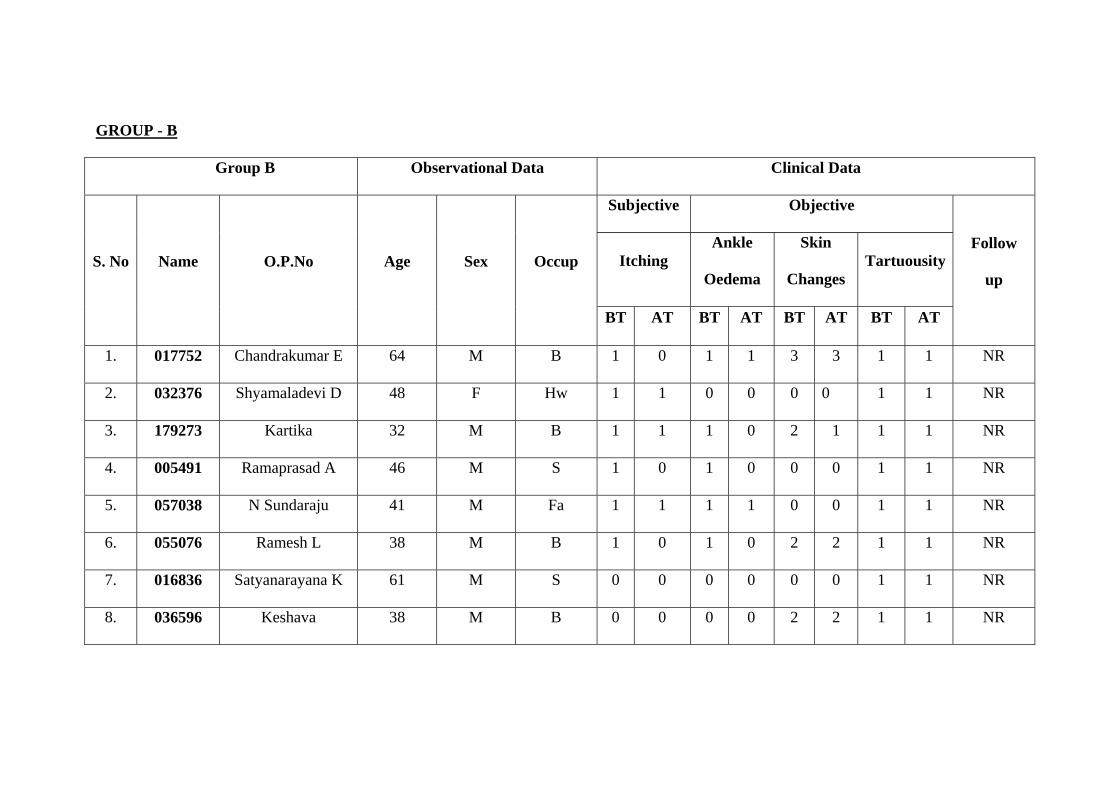
GROUP - B
Group B Observational Data Clinical Data
Subjective Objective
Itching Ankle
Oedema
Skin
Changes TartuousityS. No Name O.P.No Age Sex Occup
BT AT BT AT BT AT BT AT
Follow
up
1. 017752 Chandrakumar E 64 M B 1 0 1 1 3 3 1 1 NR
2. 032376 Shyamaladevi D 48 F Hw 1 1 0 0 0 0 1 1 NR
3. 179273 Kartika 32 M B 1 1 1 0 2 1 1 1 NR
4. 005491 Ramaprasad A 46 M S 1 0 1 0 0 0 1 1 NR
5. 057038 N Sundaraju 41 M Fa 1 1 1 1 0 0 1 1 NR
6. 055076 Ramesh L 38 M B 1 0 1 0 2 2 1 1 NR
7. 016836 Satyanarayana K 61 M S 0 0 0 0 0 0 1 1 NR
8. 036596 Keshava 38 M B 0 0 0 0 2 2 1 1 NR

9. 033712 Keshvacharya C 35 M La 0 0 1 1 1 0 1 1 NR
10. 009433 Ravindra S 51 M La 1 0 0 0 2 1 1 1 NR
11. 034614 Krishnaveni M 34 F Hw 1 0 1 1 2 1 1 1 NR
12. 038074 Gouri G 68 F B 1 0 1 0 3 3 1 1 NR
13. 037439 Mohini B 35 F Hw 1 0 0 0 2 2 1 1 NR
14. 003504 Shobha L 35 F Hw 0 0 1 0 1 1 1 1 NR
15. 004184 Shantakumara 60 M S 1 1 1 0 0 0 1 1 NR
16. 091704 Ajit R 47 M B 1 0 1 0 1 1 1 1 NR
17. 043063 Shrimant A 38 M B 0 0 0 0 3 2 1 1 NR
18. 032944 Ramalinga Reddy 56 M S 1 0 0 0 0 0 1 1 NR
19. 010662 Renuka Acharya L 46 M B 1 1 1 1 0 0 1 1 NR
20. 011065 Shrinivas E 36 M Fa 0 0 1 0 2 1 1 1 NR
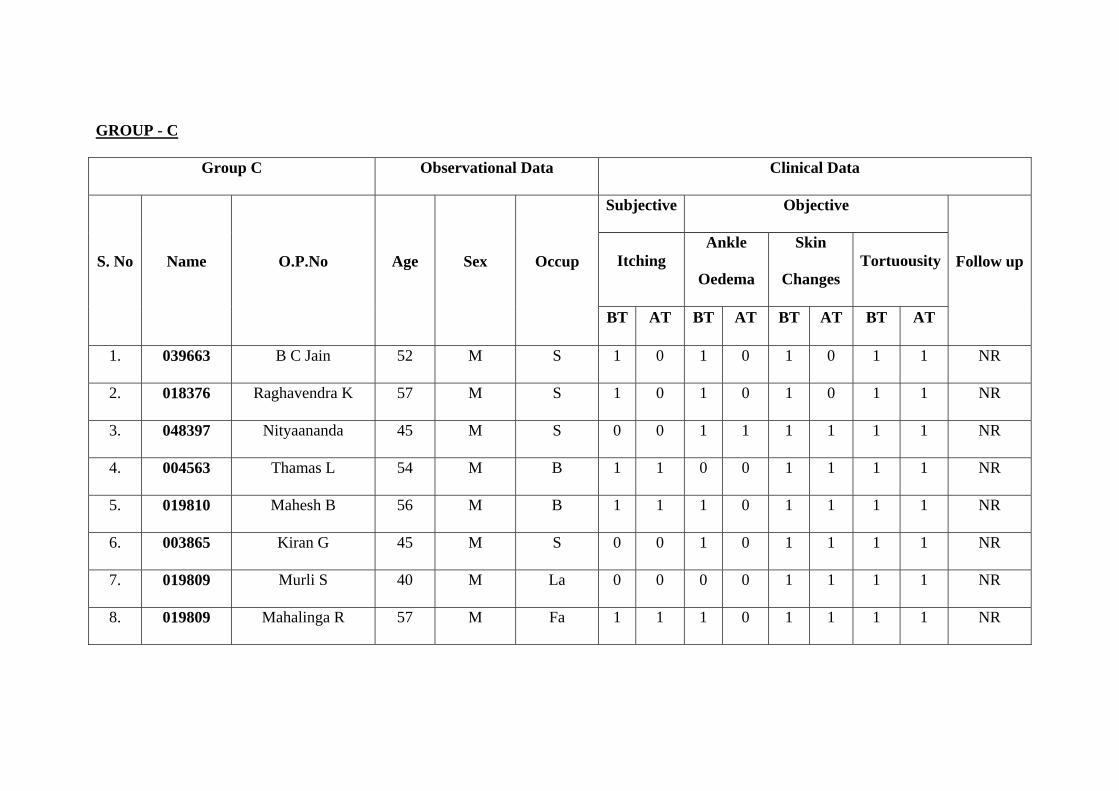
GROUP - C
Group C Observational Data Clinical Data
Subjective Objective
Itching Ankle
Oedema
Skin
Changes TortuousityS. No Name O.P.No Age Sex Occup
BT AT BT AT BT AT BT AT
Follow up
1. 039663 B C Jain 52 M S 1 0 1 0 1 0 1 1 NR
2. 018376 Raghavendra K 57 M S 1 0 1 0 1 0 1 1 NR
3. 048397 Nityaananda 45 M S 0 0 1 1 1 1 1 1 NR
4. 004563 Thamas L 54 M B 1 1 0 0 1 1 1 1 NR
5. 019810 Mahesh B 56 M B 1 1 1 0 1 1 1 1 NR
6. 003865 Kiran G 45 M S 0 0 1 0 1 1 1 1 NR
7. 019809 Murli S 40 M La 0 0 0 0 1 1 1 1 NR
8. 019809 Mahalinga R 57 M Fa 1 1 1 0 1 1 1 1 NR

9. 014263 Nagesh A 49 M La 0 0 1 0 1 1 1 1 NR
10. 35900 Radha 37 F Hw 1 1 1 1 1 1 1 1 NR
11. 39650 Guruprakash 30 M S 1 0 1 1 1 1 1 1 NR
12. 46658 Savitri 53 F Hw 1 1 1 0 1 0 1 1 NR
13. 11075 D.Vasadeva 50 M S 1 1 0 0 1 1 1 1 NR
14. 475600 Sayed Njira 58 M La 0 0 1 1 0 0 1 1 NR
15. 50404 Shekhara 55 M S 1 1 1 0 1 1 1 1 NR
16. 41027 Siddlingayya 35 M S 1 1 1 0 1 0 1 1 NR
17. 49772 Shalini 38 F Hw 1 1 1 1 3 3 1 1 NR
18. 019865 Shridhara 38 M S 1 0 1 0 1 1 1 1 NR
19. 19815 Ashwatha Nrayana 60 M S 0 0 0 0 1 0 1 1 NR
20. 19825 Govinndappa 52 M S 1 0 1 0 1 0 1 1 NR
M –Male; F – Female; Hw – House wives; La – Labour; B – Businessmen; S – Social service; Fa – Farmer; NR – No Relapses












Related Documents











