A New Face for Old Antibiotics: Tetracyclines in Treatment of Amyloidoses Tatiana Stoilova, † Laura Colombo, † Gianluigi Forloni, † Fabrizio Tagliavini, ‡ and Mario Salmona* ,† † IRCCS-Istituto di Ricerche Farmacologiche “Mario Negri”, Via Giuseppe La Masa 19, 20156 Milano, Italy ‡ Fondazione IRCCS Istituto Neurologico “Carlo Besta”, Via Celoria 11, 20133 Milano, Italy ABSTRACT: The use of tetracyclines has declined because of the appearance of resistant bacterial strains. However, the indications of nonantimicrobial activities of these drugs have considerably raised interest and triggered clinical trials for a number of different pathologies. About 10 years ago we first reported that tetracyclines inhibited the aggregation of prion protein fragments and Alzheimer’s β peptides, destabilizing their aggregates and promoting their degradation by proteases. On the basis of these observations, the antiamyloidogenic effects of tetracyclines on a variety of amyloidogenic proteins were studied and confirmed by independent research groups. In this review we comment on the data available on their antiamyloidogenic activity in preclinical and clinical studies. We also put forward that the beneficial effects of these drugs are a result of a peculiar pleiotropic action, comprising their interaction with oligomers and disruption of fibrils, as well as their antioxidant, anti-inflammatory, antiapoptotic, and matrix metalloproteinase inhibitory activities. I. INTRODUCTION The term amyloidosis comprises more than 25 unrelated human pathologies, all of which are characterized by extensive misfolding and assembly of normally soluble proteins followed by inappropriate deposition of fibrils that disrupt the structure and function of tissues and organs. 1,2 These diseases include both systemic amyloidoses in which protein aggregates may occur in any part of the body and localized amyloidoses in which deposits are presented in a single organ. Systemic amyloidosis is usually fatal and causes about 1 death per 1000 individuals in developed countries. 3 To date, 14 human amyloid proteins with respective precursors are known to cause systemic amyloidoses. 2 These include, but are not limited to, immunoglobulin light chain (LC), serum AA, β2-microglobulin (β2M), transthyretin (TTR), apolipoprotein A-I, apolipopro- tein A-II, gelsolin, and lysozyme amyloid proteins. 2 The most common representatives of localized amyloidoses are Alz- heimer’s, Parkinson’s, and prion protein diseases, characterized by accumulation and deposition of amyloid β (Aβ), α- synuclein, and prion protein (PrP), respectively. These pathologies affect the nervous system and cause dementia and/or motor disturbances, gradually destroying a person’s ability to move and function independently and ultimately leaving them vulnerable to fatal infections. Amyloidogenic proteins fold independently of their primary structure and molecular weight. This stands in contrast to natively folded proteins that fold to a specific three-dimensional structure strongly dependent on their amino acid sequence, while amyloidogenic proteins under certain conditions can aggregate and form fibrils with a very similar ultrastructure and properties. 4 In tissue deposits all amyloid fibrils present themselves as rigid, nonbranching structures of approximately 10 nm in diameter, which bind the dye Congo red and exhibit green birefringence when viewed under cross-polarized light. 2 In addition to Congo red, which specifically binds to β-sheet rich structure resulting in characteristic red shift in the absorption band of the dye, thioflavin T (ThT) is also widely used for the identification of amyloid fibrils. This dye fluoresces strongly when it is added to samples containing β-sheet rich structure. When isolated and analyzed by X-ray diffraction, amyloid fibrils demonstrate a typical cross-β diffraction pattern with two characteristic reflections: a relatively sharp and Received: January 31, 2013 Perspective pubs.acs.org/jmc © XXXX American Chemical Society A dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXX

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A New Face for Old Antibiotics: Tetracyclines in Treatment ofAmyloidosesTatiana Stoilova,† Laura Colombo,† Gianluigi Forloni,† Fabrizio Tagliavini,‡ and Mario Salmona*,†
†IRCCS-Istituto di Ricerche Farmacologiche “Mario Negri”, Via Giuseppe La Masa 19, 20156 Milano, Italy‡Fondazione IRCCS Istituto Neurologico “Carlo Besta”, Via Celoria 11, 20133 Milano, Italy
ABSTRACT: The use of tetracyclines has declined because of the appearance of resistant bacterial strains. However, theindications of nonantimicrobial activities of these drugs have considerably raised interest and triggered clinical trials for a numberof different pathologies. About 10 years ago we first reported that tetracyclines inhibited the aggregation of prion proteinfragments and Alzheimer’s β peptides, destabilizing their aggregates and promoting their degradation by proteases. On the basisof these observations, the antiamyloidogenic effects of tetracyclines on a variety of amyloidogenic proteins were studied andconfirmed by independent research groups. In this review we comment on the data available on their antiamyloidogenic activityin preclinical and clinical studies. We also put forward that the beneficial effects of these drugs are a result of a peculiar pleiotropicaction, comprising their interaction with oligomers and disruption of fibrils, as well as their antioxidant, anti-inflammatory,antiapoptotic, and matrix metalloproteinase inhibitory activities.
I. INTRODUCTION
The term amyloidosis comprises more than 25 unrelatedhuman pathologies, all of which are characterized by extensivemisfolding and assembly of normally soluble proteins followedby inappropriate deposition of fibrils that disrupt the structureand function of tissues and organs.1,2 These diseases includeboth systemic amyloidoses in which protein aggregates mayoccur in any part of the body and localized amyloidoses inwhich deposits are presented in a single organ. Systemicamyloidosis is usually fatal and causes about 1 death per 1000individuals in developed countries.3 To date, 14 human amyloidproteins with respective precursors are known to cause systemicamyloidoses.2 These include, but are not limited to,immunoglobulin light chain (LC), serum AA, β2-microglobulin(β2M), transthyretin (TTR), apolipoprotein A-I, apolipopro-tein A-II, gelsolin, and lysozyme amyloid proteins.2 The mostcommon representatives of localized amyloidoses are Alz-heimer’s, Parkinson’s, and prion protein diseases, characterizedby accumulation and deposition of amyloid β (Aβ), α-synuclein, and prion protein (PrP), respectively. Thesepathologies affect the nervous system and cause dementiaand/or motor disturbances, gradually destroying a person’s
ability to move and function independently and ultimatelyleaving them vulnerable to fatal infections.Amyloidogenic proteins fold independently of their primary
structure and molecular weight. This stands in contrast tonatively folded proteins that fold to a specific three-dimensionalstructure strongly dependent on their amino acid sequence,while amyloidogenic proteins under certain conditions canaggregate and form fibrils with a very similar ultrastructure andproperties.4 In tissue deposits all amyloid fibrils presentthemselves as rigid, nonbranching structures of approximately10 nm in diameter, which bind the dye Congo red and exhibitgreen birefringence when viewed under cross-polarized light.2
In addition to Congo red, which specifically binds to β-sheetrich structure resulting in characteristic red shift in theabsorption band of the dye, thioflavin T (ThT) is also widelyused for the identification of amyloid fibrils. This dye fluorescesstrongly when it is added to samples containing β-sheet richstructure. When isolated and analyzed by X-ray diffraction,amyloid fibrils demonstrate a typical cross-β diffraction patternwith two characteristic reflections: a relatively sharp and
Received: January 31, 2013
Perspective
pubs.acs.org/jmc
© XXXX American Chemical Society A dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXX
intensive meridional reflection at 4.7−4.8 Å and a more diffusesignal on the equator at approximately 10 Å, corresponding tothe β-strand and β-sheet distances, respectively.2,4,5 Themeridional reflection, which is derived from the fairly constantdistance between hydrogen bonded β-chains, is highlyconserved among all amyloidogenic proteins. This indicates avery similar core structure of the fibrils. By contrast, theequatorial reflection, which comes from the polypeptidesequence and side chain dependent distance between β-platedsheets, can vary from 8.8 to 14.6 Å.6
Amyloid fibrils, a principal component of plaques, wereregarded for many years as the primary cause of cellulardegeneration and pathogenesis of amyloidoses.7 However, anumber of studies strongly suggest that cytotoxicity andinitiation of degenerative cascades are rather caused by thesmall soluble oligomeric species that precede fibril forma-tion.8−10 This can explain the little to no correlation betweenthe density of amyloid deposits and disease manifestationobserved in Alzheimer’s and prion diseases, as well as in type 2diabetes mellitus and familial amyloid polyneuropathy(FAP).11−14 In fact, abundant amyloid deposits that character-ize Alzheimer’s disease (AD) were detected in some cognitivelynormal individuals who did not show any neurodegenerativesymptoms.15 A strong correlation was observed, however,between soluble amyloid β oligomer levels and the extent ofsynaptic loss and severity of cognitive impairment.13
Similarly, islet amyloid deposits associated with type 2diabetes have been detected in nondiabetic humans. Intransgenic mice carrying human amylin/islet amyloid polypep-tide genes, the load of fibrillar amyloid did not correlate withtheir lifespan.16,17 This has led some researchers to hypothesizethat the sequestration of misfolded protein in final amyloidfibrils and plaques has a protective function.18 However,formation of large amyloid deposits that impair thephysiological functioning of cells and tissues can hardly beconsidered beneficial in patients affected by amyloidoses. Thus,it was recently shown that fibrillar β2M was cytotoxic tomonocytes and chondrocytes and impaired osteoclast for-mation and viability. The result was decreased resorption of oldbones, altered cartilage formation, and bone remodeling.19
Lipid membrane disruption caused by β2M fibrils and leakageof toxic species from mature fibrils were also described.20
To date, while the exact mechanism behind cellulardegeneration remains unclear, several potential mechanismsof toxicity have been proposed. They were summarized in areview18 as follows: (1) tissue architecture destruction andorgan dysfunction caused by deposition of large amounts offibrils;21 (2) permeabilization and destabilization of mitochon-drial and plasma membrane by oligomeric species;22 (3)oxidative damage produced by reactive oxygen species causedby the incorporation of redox metals into amyloids;23 (4)general disorganization of cellular protein homeostasis essentialfor cell viability by sequestration of numerous proteins, mostlymetastable ones, in a “chaperone-like” manner.24,25
Virok et al. have used a protein array approach to discoverAβ interaction patterns, and more than 324 cellular proteinswere identified as possible interactors with oligomeric forms ofAβ.24 Among them, 24 proteins were found to be involved inprotein translation processes, suggesting that this might be theprimary target of Aβ toxicity.24 In a recent paper, Manzoni et al.reported that Aβ bound to a variety of membrane proteins and,to a lesser extent, cytosolic proteins. This finding confirms theidea of the existence of multiple molecular targets of amyloidoligomers as opposed to a single specific receptor.25
Despite a great number of hypotheses, the exact mechanismof amyloid toxicity remains elusive. It is still unclear whichpathway should be targeted for therapeutic intervention. Thecurrent search for disease-modifying therapies includes thefollowing key strategies: (i) reduction of amyloid production;(ii) inhibition of amyloid aggregation and/or destabilization ofaggregated species; (iii) promoting of its clearance.26
The first strategy, aimed at inhibition of amyloid formation,frequently produces a halt in disease progression. This strategyis based on decrease of the respective amyloid precursorprotein production or its stabilization. For example, in serum Aamyloidosis administration of anti-inflammatory and immuno-suppressive drugs suppresses inflammation and decreasesproduction of serum amyloid A protein, thereby slowingdisease progression.1 In another type of systemic amyloidosis,the light-chain amyloidosis, the reduction of amyloidproduction is achieved by hematopoietic stem cell trans-plantation and administration of melphalan and dexametha-sone, which are directed against the plasma cells responsible forthe precursor protein synthesis.27 However, these drugs areoften ineffective and poorly tolerated, producing a number of
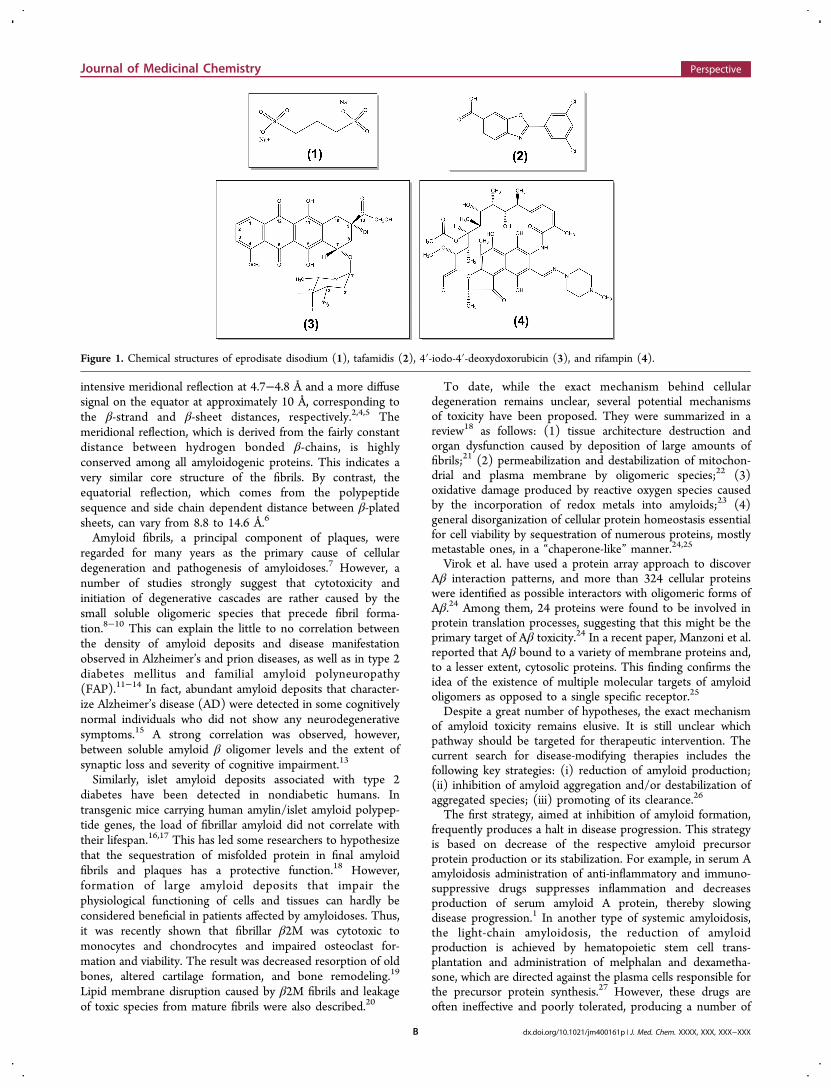
Figure 1. Chemical structures of eprodisate disodium (1), tafamidis (2), 4′-iodo-4′-deoxydoxorubicin (3), and rifampin (4).
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXB
side effects like diminished production of blood cells,gastrointestinal problems, and increased risk of infection.27 Inhereditary transthyretin amyloidosis, production of amyloido-genic mutant TTR in the liver is abolished by orthotopic livertransplantation.28 At the same time, it was found that inpatients carrying some types of TTR mutation, liver trans-plantation may cause acceleration of amyloid cardiomyopathydue to the deposition of wild-type TTR fibrils in the heart.29 Itis worth noting that amyloid fibrils isolated from patients afterliver transplantation show a predominance of wild-type overmutant TTR, at variance with amyloid deposits from untreatedpatients.30 In patients with combined heart and liver trans-plantation, amyloid deposition in the heart did not occur.However, progression of amyloid formation in other tissues,such as peripheral nerves, kidneys, and adipose tissue, wasobserved.30 The cause of this side effect is still not understood.One hypothesis is that the presence of preformed amyloiddeposits (nidus) in the heart and other organs of patients
before liver transplantation can lead to efficient recruitment ofwild-type TTR in these deposits after orthotopic livertransplantation.30 In AD the most desirable approach, targetingthe β- and γ-secretases to reduce amyloid β production, provesto be challenging. These enzymes have protein substrates otherthan amyloid precursor protein (e.g., neuregulin-1 for β-secretase, Notch1 for γ-secretase), and inhibiting the cleavageof these substrates has detrimental effects.31
Another therapeutic strategy is purposeful interference withthe amyloid aggregation process. For example, eprodisatedisodium (Figure 1, compound 1) is now in phase III clinicaltrial for the treatment of AA amyloidosis (ClinicalTrials.govidentifier NCT01215747). Compond 1 is a small sulfonatedmolecule which competes with sulfated glycosaminoglycans inbinding to amyloidogenic proteins, a process that interfereswith fibril formation and deposition. A phase IIa clinical trial forthe treatment of type 2 diabetes has been completed as well(ClinicalTrials.gov identifier NCT00675857). However, the
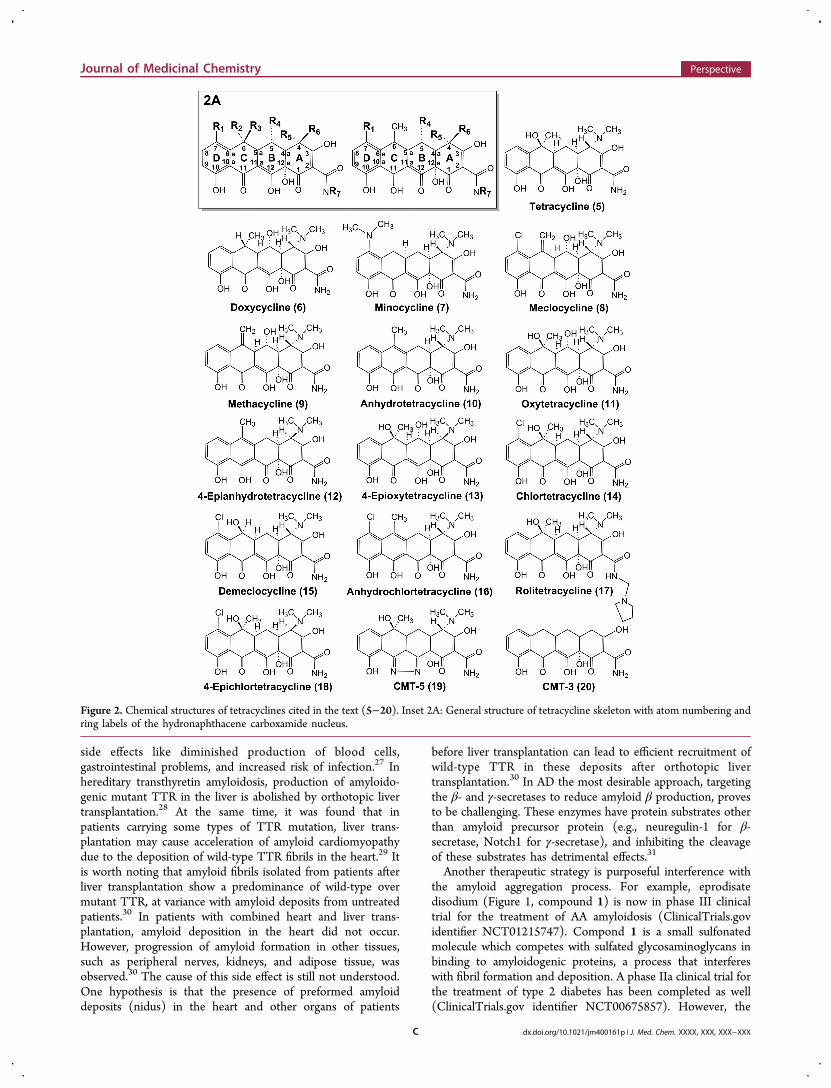
Figure 2. Chemical structures of tetracyclines cited in the text (5−20). Inset 2A: General structure of tetracycline skeleton with atom numbering andring labels of the hydronaphthacene carboxamide nucleus.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXC

observed side effects such as myocardial infarction, myocardialischemia, transient ischemic attack, and angina pectoris haveprompted further review of this therapeutic approach.32 In aphase III trial on a large AD population the use of the Aβ ligandtramiprosate as an inhibitor of Aβ aggregation demonstrated noclear benefits.33 This result was in spite of the efficacy inpreclinical animal studies, suggesting that great care is neededin attempting to extrapolate results from model organisms andcomputational models to the human situation. Overall,considerable effort in the design of Aβ targeting moleculeshas been useful, providing several classes of compounds withdifferent modes of activity.33 The drugs selected for clinicaltrials, however, have produced unsatisfactory results or causedadverse side effects.In past decades efforts aimed at generating other small
inhibitors of aggregation were also made. Thus, short β-sheetbreaker peptides, iPrP13 and iAβ5, were developed for thetreatment of prion and Alzheimer’s diseases, respectively.34 Inanimal models these peptides have been shown to inhibitfibrillogenesis and to induce disassembly of fibrillar amyloiddeposits in vivo, resulting in a substantial delay in the diseaseonset. However, proteolytic degradation, generation ofimmunoreactive response, and the poor permeability of thesepeptides at the blood−brain barrier impede their application inmedicine.34 Among other inhibitors, tafamidis (Figure 1,
compound 2) was found to prevent the TTR proteinmisfolding as a result of its stabilization into the nativetetrameric conformation. It inhibits formation of TTR amyloidfibrils and halts disease progression in patients with TTRamyloid polyneuropathy.35 In a pivotal phase II/III random-ized, double-blind, placebo-controlled trial, neuropathy did notprogress in 60% of patients who received 2 versus 38% ofpatients of the placebo group.36
Finally, generation of antibodies against amyloid fibrils andamyloid-like aggregates represents the third type of approachand is aimed at clearance of preformed amyloid deposits. Thisapproach is based on active immunization with aggregated Aβor passive administration of anti-Aβ antibodies. It was shown tobe effective in mouse models of AD in which there were noadverse events.37 However, when AD patients were vaccinated,6% developed severe meningoencephalitis.38 Clinical trials withpassive immunotherapy are currently underway. Initial assess-ment of a limited number of patients with PET imaging using11C-labeled Pittsburgh compound B showed that the peripheraladministration of a humanized anti-Aβ monoclonal antibodywas associated with 25% reduction in cortical fibrillar Aβ loadover 78 weeks compared with a placebo.31 However, nobeneficial effect on memory and the mental functions as well asactivities of daily living has been found in a recently completedclinical trial on mild to moderate AD.39
Table 1. Recently Completed and Ongoing Clinical Trials for Nonantimicrobial Activities of TCs
drug disease effect current statusClinicalTrials.gov
identifier
Doxycycline Inflammation in cystic fibrosis MMP-9 inhibitory Phase IV completed NCT01323101Anti-inflammatory
Minocycline, doxycycline Cerebral arteriovenous malformations and aneurysms MMPs inhibitory Phase I NCT00243893Doxycycline Lymphangioleiomyomatosis MMPs inhibitory Phase IV NCT00989742Doxycycline Abdominal aortic aneurism MMP-9 inhibitory Phase II completed NCT00538967Doxycycline Post myocardial infarction remodeling MMPs inhibitory Phase III NCT00469261
Anti-inflammatoryDoxycycline Inflammation and insulin resistance in type II diabetes
and obesityMMPs inhibitory Phase IV completed NCT01375491
Anti-inflammatoryDoxycycline Persistent symptoms postneuroborreliosis Immunomodulatory Completed NCT01205464CMT-3b Kasposi’s sarcoma MMPs inhibitory Phase II completed NCT00020683CMT-3b Recurrent brain tumors NSa Phase I/II completed NCT00004147CMT-3b Advanced solid tumors NSa Phase I completed NCT00003721CMT-3b Refractory metastatic cancer MMPs inhibitory Phase I completed NCT00001683Doxycycline Transthyretin amyloidosis NSa Phase II NCT01171859Minocycline Huntington disease NSa Phase II/phase III NCT00277355Minocycline Parkinson’s disease NSa Phase II completed NCT00063193Minocycline Alzheimer’s disease NSa Phase II NCT01463384Doxycycline Systemic and localized amyloidosis Antiamyloidogenic Phase II NCT01677286Doxycycline Alzheimer’s disease (biomarkers evaluation) Antiamyloidogenic MMPs
inhibitoryPhase III NCT00439166
Anti-inflammatoryMinocycline Amyotrophic lateral sclerosis Antioxidant Phase II completed NCT00355576
Anti-inflammatoryAntiapoptotic
Minocycline Acute hemorrhagic stroke Neuroprotective Not yet recruiting NCT01388127Minocycline Reduction of chemoradiation effects NSa Phase II NCT01636934Minocycline Schizophrenia Anti-inflammatory Phase III NCT01403662
AntidepressantMinocycline Atrial fibrillation after cardiac surgery Anti-inflammatory Recruiting NCT01422148Minocycline Retinal vein occlusion Anti-inflammatory Phase I/II NCT01468831Minocycline Retinal detachment surgery Neuroprotective Phase II NCT01297816
aNot specified. b6-Deoxy-6-demethyl-4-dedimethylaminotetracycline.115
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXD

Purified intravenous immunoglobulin (IVIg) obtained fromthe plasma of healthy humans contains naturally occurringantibodies against Aβ peptides. IVIg has been shown toameliorate AD pathology in mildly affected patients, and someclinical trials have been conducted to evaluate the effect of IVIgin patients with mild to moderate AD (ClinicalTrials.govidentifiers NCT00818662, NCT01561053, NCT01736579)and mild cognitive impairment (ClinicalTrials.gov identifierNCT01300728).The nonfibrillar plasma glycoprotein serum amyloid P
component (SAP) was found to be a component of amyloiddeposits and might contribute to their persistence andresistance to proteolysis.1 The combination of the SAP-bindingmolecule (R-1-[6-[R-2-carboxypyrrolidin-1-yl]-6-oxohexanoyl]-pyrrolidin-2-carboxylic acid) with anti-SAP antibodies wasproposed as an antiamyloidogenic strategy. In this way theSAP-binding molecule depletes rapidly circulating SAP, whileanti-SAP antibodies reach residual SAP in the amyloid depositsand promote their clearance.1,40 Phase I clinical trial to assessthe pharmacokinetics of GSK2315698 (SAP depleter) andGSK2398852 (anti-SAP monoclonal antibody) and circulatingSAP concentrations is now ongoing (ClinicalTrials.govidentifier NCT01777243).About 10 years ago tetracyclines (TCs), a well-known class
of antibiotics (Figure 2, compounds 5−20), were found toinhibit the aggregation of prion protein fragments (PrP106−126 and PrP82−146) and Aβ peptides. Furthermore, TCsdestabilized scrapie prion protein (PrPSc) and Aβ aggregatesand promoted their in vitro degradation by proteases.41,42
Later, the antiamyloidogenic effects of TCs on TTR,W7FW14F apomyoglobin, amylin, Huntingtin, α-synuclein,α2-macroglobulin, and poly-(A) binding protein nuclear 1 werestudied and confirmed.43 Although the exact mechanism ofantiamyloidogenic activity of TCs is still unknown, it is likelyrelated to their ability to interfere with the formation of β-sheetstructure. This is characteristic of all amyloidogenic proteins, aquality that makes them potentially effective against most typesof amyloidoses.43,44 TCs have an advantage over other newlyproposed antiamyloidogenic drugs because of their wellcharacterized pharmacological and pharmacokinetic propertiesand relatively low toxicity. Some of them (for example,minocycline (Figure 2, compound 7)) efficiently cross theblood−brain barrier.45 This old class of antibiotics was nearlyabandoned as a result of the development of resistant bacterialstrains. Today, however, TCs are involved in more than 130clinical trials unrelated to their antimicrobial activity.46 Amongothers, these include clinical trials focused on the beneficialeffects of tetracycline derivatives (in particular doxycycline (6)and 7) on the outcomes of amyloidogenic disorders, includingAlzheimer’s, Parkinson’s, and Huntington’s diseases and TTRamyloidosis (Table 1). An increase in the number ofpublications regarding successful application of TCs for thetreatment of amyloidoses indicates a growing interest in thistherapeutic approach. Moreover, the use of 6 as an orphan drugfor the treatment of hereditary amyloid polyneuropathy causedby β2M was recently approved by the European Committee forOrphan Medicinal Products (http://www.emea.europa.eu/docs/en_GB/document_library/Orphan_designation/2012/05/WC500127736.pdf).In this review, we first summarize data available in the
literature regarding the antiamyloidogenic activity of TCs incell-free, in vitro, and in vivo studies. We also give a brief insightinto the chemical properties of these molecules, paying special
attention to the structural features involved in theirantiamyloidogenic activity. We discuss putative mechanismsunderlying the beneficial effects of TCs on amyloidosesobserved in vivo. Finally, we examine evidence of the possiblesynergic effect of pleiotropic nonantimicrobial activities of TCson different pathological pathways of amyloidogenic disorders.The ultimate purpose of this review is to bring to the attentionof scientists and clinicians the versatility of properties of TCs.We argue that the versatility of these properties should be takeninto careful consideration in both preclinical and clinicalstudies.
II. CHEMICAL STRUCTURE AND PHYSICOCHEMICALPROPERTIES OF TETRACYCLINES
Tetracyclines are a group of structurally related antibioticsdiscovered in the late 1940s (Figure 2). The first members ofthis family, chlortetracycline (14) and oxytetracycline (11),were isolated from Streptomyces aureofaciens and Streptomycesrimosus. They were later followed by the discovery of othernatural TCs.47 Further chemical modifications of naturalstructures and synthesis of new compounds produced anumber of novel TCs, including two of the more commonsemisynthetic clinical antibiotics 7 and 6.46
The basic chemical structure of TCs is represented by thepartially saturated naphthacene carboxamide nucleus, com-posed of four linear fused six-membered carbocyclic rings A, B,C, and D (Figure 2, inset 2A). This structure is required forbioactivity in both prokaryotic and eukaryotic systems. Bothnatural TCs and many of their synthetic derivatives possess fiveasymmetric centers: C4, C4a, C5a, C6, and C12a. They havevarious functional groups attached to the periphery of themolecule.47,48 The lower and the upper peripheral regions aredistinguished. Structure−activity relationships studies demon-strate that modifications along the lower periphery, rich inoxygen functional groups, cause a decrease in both antimicro-bial and nonantimicrobial activities. Changes along the upperperiphery, particularly in positions C7 and C9 of the D-ring,mostly result in increased activity against various biologicaltargets. Modifications of the upper peripheral region influencebasic physicochemical properties such as shape, electronicconfiguration, charge density and distribution, and polarity.Consequently these changes lead to changes in solubility inbiological fluids and lipophilicity.48 The C4-dimethylaminogroup has proven to be necessary for antimicrobial activity.However, it is not involved in the biological effects oneukaryotic targets such as matrix metalloproteinases (MMPs).48
The presence of the phenol ring in the chemical structure ofTCs makes them effective scavengers of reactive oxygen species(ROS), similar to α-tocopherol and other phenolic antiox-idants. The reaction of TCs with free radicals results information of phenol-derived radicals. The latter radicals arerelatively stable and unreactive due to their resonance and stericstabilization by phenol ring side groups.49
The scavenging potency strongly depends on the numberand size of phenol ring substituents. In fact, in cell-free assays itwas demonstrated that the presence of dimethylaminosubstituent at the C7 atom of 7 strongly improved itsscavenging capacity of radicals compared to tetracycline(5).49 At the same time, under a variety of conditions, TCscan generate free radical species that damage surroundingmacromolecules.48 Thus, in a biological environment TCs canauto-oxidize in the presence of divalent cations such as Co2+.This process generates electronically reactive species and
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXE

cytotoxins like O2•−, HO•, H2O2, and singlet oxygen 1O2. This
reaction occurs in the dark and involves the electron-rich lowerperipheral region.48
Tetracycline molecules, because of the flexible connectionbetween ring A and ring B, may adopt two main conformations:an extended conformation and a folded conformation. It isgenerally assumed that in basic or nonaqueous solutions themolecule adopts an extended one. In this conformation, the B,C, and D rings approximately lie on the same plane and the C1,C2, C3, and amide carbons lie above this plane.50 In neutral toacidic solutions TCs adopt a folded conformation. This isderived from the extended conformation by the rotation aroundthe C4a−C12a bond, causing the A-ring to be more foldedtoward the B-ring.50 The type of conformation is principallydependent on the protonation state of the molecule. In general,TCs possess some groups with acid−base properties (the C1−C3 tricarbonylmethane, the two C10−C12 ketophenolichydroxyls, and the C4 dimethylammonium group) which canbe subject to protonation−deprotonation equilibria. Thisresults in formation of various protonation states, 3Dconformations, and tautomers.51 The protonation scheme ofTCs has been the subject of disagreements and intensediscussion. Initially it was thought that TCs can only undergothree deprotonations. According to different research groups,the first deprotonation occurred at C3-OH, whereas the secondand the third deprotonations affected 4-dimethylamino groupor C10-OH or C12-OH.51
The semiempirical studies of TCs provide theoretical andexperimental evidence that TCs can undergo four deprotona-tions, adopting 64 different tautomeric forms.51 The deproto-nation of C10-OH (pK = 11.8) requires strongly basicconditions, far from the biological pH. But the ionizablegroups of TCs may participate in the coordination of metalions, particularly transition metal ions. The binding of metalions to ionizable groups facilitates their deprotonation, givingrise to observed pK values shifted as much as several unitstoward lower values. It means that in the presence of complexmultiligand and multimetal systems like biological fluids, theproton release of C10-OH cannot be excluded.In aqueous solution, the first deprotonation of the fully
protonated species occurs at C3-OH. This results in formationof a neutral compound, represented by nonionized andzwitterionic tautomers (deprotonation constant pK1 ≈ 3.1−3.5). The second and the third deprotonations affect the C12-OH (pK2 ≈ 7.2−8.5) and C4-NMe2H
+ (pK3 ≈ 9.0−10.8),respectively. Finally, the fourth acidic group that undergoesdeprotonation is represented by the C10-OH (pK4 ≈ 11.8).51
In solution, TCs are an equilibrium of different tautomers,which can be shifted by varying the pH, the dielectric constantof the medium, and the metal ion presence.On the basis of the generally accepted attribution of the pKa
values to specific functional groups, 5 in aqueous solution atneutral pH presents two different forms. The first is thezwitterionic form with a positive charge on the C4-NMe2 groupand a negative charge on the C3-OH group. The second is theanionic form in which the C12-OH hydroxyl group isdeprotonated (Figure 2).50 In addition, circular dichroismspectra of 11 demonstrate a solvent-dependent shift of theequilibrium between the zwitterionic and the nonionized forms.The zwitterionic form clearly predominates in aqueoussolutions, while in organic solvents like ethanol, chloroform,and 1-octanol the nonionized form prevails.52 This nonionized,more lipophilic form of TCs easily crosses biological and model
membranes.52 The conformational flexibility of TCs makes itvery difficult both to establish the structure−function relation-ship and to define their chemical behavior in a complexbiological environment. On the other hand, the range ofconformations and protonation states adopted by TCs indifferent chemical environments confers activity against manybiological targets.The presence of different electron-donating groups in the
chemical structures of TCs makes them powerful chelatingagents. It is generally assumed that chelation sites include thedeprotonated functional groups, primarily along the lowerperipheral region.48,53 TCs bind with high affinity numerouspolyvalent metallic cations, including Fe2+, Fe3+, Al3+, Ca2+, andMg2+.48 In general, the affinity of TCs for different metalsdecreases in the following order: Fe3+ > Al3+ = Cu2+ > Co2+ =Fe2+ > Zn2+ > Mn2+ > Mg2+ > Ca2+ cations. For a given metalthis ranking can vary, depending on pH, protonation state, thepresence of other metal ions, and the presence of lateralsubstituents bound to the molecular tetracyclic skeleton.48,54
The results reported in the literature regarding thestoichiometries of complexes of TCs with metals, in particularwith physiologically relevant Ca2+ and Mg2+ cations, arenumerous and quite controversial. For both metal ions,stoichiometries of 1:1, 1:2, and 2:1 ions bound per 5 havebeen reported in aqueous solutions between pH 6.5 and pH8.5.54 The results of the isothermal titration calorimetry studiessuggest a distinct binding mode of TCs to Mg2+ as compared toCa2+ cation.54 Moreover, it was shown that the molar ratioswere distinct for the two ions, namely, 1:1 for the Ca2+/tetracycline complex and 2:1 for the Mg2+/tetracycline.54
Metal chelation is relevant for a number of biologicalproperties and activities of TCs. In blood TCs circulateprimarily as complexes of calcium and magnesium.53 In thegastrointestinal tract TCs bind to polyvalent metal cations.They are normally present in biological fluids or ingested withfood to form poorly absorbable complexes. This interaction, onone hand, may affect the biovailability of essential trace metalions. On the other hand, it alters the biovailability of theantibiotics themselves. In fact, simultaneous ingestion of TCswith milk and other dairy products that contain metal cationssuch as calcium, magnesium, iron, and zinc may impair theabsorption of the drug by 50−90%.55 TCs form a stablecomplex with calcium in any bone-forming tissue, tending todeposit in areas of calcification in bones and teeth. Thisaccumulation may be associated with adverse effects such aspermanent teeth pigmentation, especially in young individuals.Moreover, treatment of pregnant women with TCs mayproduce permanent brown discoloration of the deciduous andpermanent teeth in their children because the drug passes theplacental barrier. Importantly, this effect depends on the dosebut not on the duration of theraphy.56 At the same time, thetendency of TCs to deposit in areas where new bones aremineralizing can be useful for studies of bone formation andturnover in vivo.57 Thus, microscopic observation offluorescence, derived from tetracycline−calcium orthophos-phate complexes at sites of new bone formation, permits one todistinguish osteoid tissue from the mineralized bone. Moreover,observing the distribution of fluorescence derived from variousTCs in different regions of the bone affords insight into the rateand extent of bone formation in vivo. This approach has foundan application in clinical practice for characterization ofdynamic changes in bone turnover in both normal and certainpathological conditions including hyper- and hypothyroidism,58
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXF

postmenopausal osteoporosis, and myelodysplastic syndrome.59
Compound 5 labeling was also used for quick and easyintraoperative localization of the lesions to be resected inpatients affected by osteoid osteoma.60
Chelated TCs can act as ionophores and transport boundcalcium cations across biological membranes.48 This propertyhas important biological implications because on one hand itcan affect the release of calcium from storage organelles such assarcoplastic reticulum, endoplastic reticulum, and mitochon-dria.48 On the other hand, once transported inside the cell byTCs, Ca2+ can act as a secondary messenger, affecting variousbiological pathways such as metabolic and secretory processes,cell division, receptor activation, and membrane transport.Metal chelation plays an important role in antimicrobial
activity of TCs as well. Compound 5 chelates magnesium ionsituated near the acceptor site for aminoacyl-tRNA of the 30Ssubunit of bacterial ribosomes. Such chelation interferes withthe binding of aa-tRNA to ribosome by direct sterichindrance.61 As a result, protein biosynthesis is blocked,causing bacterial cell death. On the other hand, magnesiumcomplexes of 5 play a crucial role in the mechanisms ofbacterial resistance to the antibiotic. In complex withmagnesium, the drug binds to the tetracycline repressor TetRand triggers its conformational changes, resulting in theexpression of the gene tetA. The latter encodes for themembrane-bound tetracycline efflux pump, which exports theantibiotic out of the cell, thereby preventing bacterial death.48
In addition, inhibition of matrix metalloproteinase, a non-antimicrobial activity of TCs, is also strictly dependent on theirmetal chelation capacity.To summarize, it is clear that TCs possess pleiotropic
biological properties. By means of a rational chemicalmodification of their structure, it is possible to generatecompounds with low antimicrobial activity with enhancedtherapeutic potential against nonbacterial biological targets. Asubstantial body of data available in the current literatureprovides a detailed description of structural and conformationalbehavior of TCs in various environments. However, to date,there is no consensus about what makes them efficient againstsuch a variety of different targets. Elevated conformationalversatility of TCs upon changes in surrounding conditions (pH,metal ion presence, dielectric constant of the medium, etc.)makes it very difficult to characterize them. It is likewisedifficult to define the exact structure−activity relationships. Atthe same time, structural flexibility appears to be a key factorthat confers activity against so many different targets. The highlipophilicity of some derivatives (i.e., compound 7) permitsthem to cross blood−brain barriers with relative ease. Anotherimportant feature is their chelation property, implicated in theirinteractions with various macromolecules of both bacterial andmammalian origin. Taken together, all these features provideTCs with great pharmacological potential for a variety ofmolecular targets and have given rise to numerous preclinicaland clinical studies unrelated to their antimicrobial activity.
III. ANTIAMYLOIDOGENIC ACTIVITY OFTETRACYCLINES
The interest in antiamyloidogenic activity of TCs arises fromthe observation that a structural homologue of 5, theanthracycline anticancer drug 4′-iodo-4′deoxydoxorubicin(IDOX, Figure 1), produced clinical benefits in patientsaffected by immunoglobulin light-chain amyloidosis. Thus, abrief course (for about a month) of 3 (IDOX) inhibited
progression of amyloidosis and improved the clinical conditionof five patients over the course of several months.62
Furthermore, in vitro studies have demonstrated that 3bound strongly to five natural amyloid fibrils including amyloidA, LC, TTR, Aβ, and β2M but did not bind to native amyloidprecursor.63 In vivo in experimental murine reactive amyloi-dosis 3 specifically accumulated in amyloid deposits. Takentogether, these data suggested that the drug targeted certainstructural features of amyloid fibrils, like cross-β-sheetquaternary structure.63 Quantitative binding studies onsynthetic fibrils made of human recombinant insulin showedthat 3 recognized with high affinity two unrelated binding sites(dissociation constants KD = 5.9 × 10−11 M and KD = 3.4 ×10−9 M, respectively) along the amyloid fibril.63
Compound 3 also bound to PrP amyloid in brain sectionsfrom scrapie-infected hamsters and patients with Creutzfeldt−Jakob disease (CJD). It reduced the infectivity of prion-infectedbrains, resulting in prolonged survival with experimentalscrapie.64 In patients with FAP, 3 colocalized with amyloiddeposits and in vitro disrupted TTR fibrils obtained frompatients into an amorphous precipitate.65 Doxorubicin, whichdiffers from 3 by the presence of the hydroxyl group at C-4′ ofthe amino sugar instead of iodine, showed much lower affinityfor amyloid fibrils. However, the reason of the targeting of 3 toamyloid fibrils was not the presence of the iodine atom per sebut the substantially increased hydrophobicity of 3 as comparedto doxorubicin.63 All these data indicate the existence of auniversal mechanism of action of 3 against amyloidosis andmake it a potential antiamyloidogenic drug, feasible in all typesof amyloidosis. However, because of the high toxicity (inparticular, cardiotoxicity) of 3, attempts have been made toidentify structurally similar compounds, possessing antifibrillo-genic activity with a better safety/toxicological profile, alreadytested in clinical practice. The resemblance of the polycyclicconjugated structure of TCs with the aglycone moiety of 3prompted an initial study to hinder the pathologic aggregationand the propagation of the prion protein.41,66 The advantagesof TCs rely on their well characterized pharmacological andpharmacokinetic properties, relatively low toxicity, and theability of some congeners to cross the blood−brain barrier.45
The first studies of antiamyloidogenic activity of TCs werecarried out on fibrils generated by synthetic peptidescorresponding to residues 82−146 and 106−126 of humanPrP.41 These fragments have a high propensity to forminsoluble fibrils with extensive β-sheet conformation. They areultrastructurally similar to those found in patients withGerstmann−Straussler−Sheinken (GSS) and carry the proteaseresistant core of PrPSc.42,67,68 The interaction of 5 with PrPpeptides was first established by fluorescence spectroscopicanalysis, demonstrating a shift in the emission spectra of 5 inthe presence of the peptides.41 This interaction resulted ininhibition of peptide aggregation into fibrils, causing an increasein protease sensitivity. It also abolished neurotoxicity andastroglial proliferation, induced by PrP 106−126 in vitro.41
Further studies showed that, like 5, 6 was able to revert theprotease resistance of PrPSc protein from patients with CJD in adose-dependent manner, reaching almost 80% at 1 mM.66 Thepretreatment of scrapie−brain homogenates with 5 or 6 at 1mM, followed by injection in Syrian hamsters, resulted insignificant delay in disease onset and increased survival time.66
In addition, the ameliorations in pathological conditions intetracycline-treated animals were associated with a delay in theaccumulation of PrPSc in the brain. These findings were
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXG

revealed by immunohistochemistry and Western blot analysis inthe post-mortem brains. These data were also confirmed bymagnetic resonance imaging (MRI) studies in animal models ofprion disease, demonstrating that the extent of PrPSc
accumulation in the brain was remarkably more abundant inthe positive controls than in tetracycline-treated hamsters. Theobserved differences between the two groups were paralleled bya difference in the severity of spongiform changes andastrogliosis in the cerebral cortex and subcortical graystructures.66 Compound 5 was found to bind not only to PrPaggregates but also to oligomeric−monomeric forms ofPrP106−126,41 as revealed by fluorescence microscopy andnuclear magnetic resonance (NMR) spectroscopy. In particular,NMR data provided evidence for through-space interactionsbetween the aromatic protons of 5 and hydrophobic peptidedomains. This included the side chains of Ala117−119,Val121−122, and Leu125, all involved in the formation of β-sheet secondary structure.41 At the same time, fluorescenceexperiments, together with docking calculations and moleculardynamics simulations, suggested that antibiotics can alsointeract with the solvent-exposed C-terminal helix 2 ofhuman PrP. This fragment of PrP is a potential nucleationsite of the conversion from the cellular to the scrapie form ofPrP. Furthermore, it can adopt both α- and β-structure withouta definitive preference.69 These data suggest that TCs not onlyinhibit protein aggregation and fibrillization through interactionwith β-sheet forming domains but also stabilize the fluctuatingconformation of the C-terminal part of helix 2 and preventconformational transition of PrP to the pathological isoform.69
In addition, circular dichroism studies showed that 6 and 5prevented formation of β-sheet structures by human recombi-nant PrP91−230, a starting event of the conversion ofamyloidogenic proteins into fibrils.70 Finally, the anti-prionactivity of TCs has been studied in a small group of patientsaffected by CJD. These patients received compassionate dailytreatment with 6 at 100 mg/kg.71 Retrospective analysisshowed significantly longer survival in these patients, whichin turn gave rise to the ongoing phase II, multicenter,randomized, double-blind, placebo-controlled efficacy study of6 in CJD patients funded by the Italian Drug Agency.71
Antiamyloidogenic activity of both 5 and 6 has also beentested on synthetic peptide amyloid β 1−42 (Aβ 1−42),representing the major component of amyloid plaques in AD.42
Electron microscopy studies, together with quantitative ThTassay and trypsin digestion studies, have shown that equimolarconcentrations of TCs not only inhibited amyloid fibrillo-genesis but also disrupted preformed amyloid fibrils.42 Twobiophysical methods that permit following of the interactionbetween ligand and proteins, NMR and Fourier transforminfrared spectroscopy (FTIR), have demonstrated that 5 bindsto the Aβ peptide in a nonspecific manner. This was evidencedby the absence of a well-defined binding site on the peptide.44
Atomic force microscopy (AFM) and dynamic light scatteringanalysis showed that the supermolecular complexes betweenthe drug and Aβ formed immediately after their co-dissolution.The resulting aggregates formed by peptide with 5 were largerthan those detected in the absence of the drug (peptide alone1.56 nm vs peptide−5 2.94 nm) and increased slowly with timeto reach a maximum after 24 h. In fact, after 120 h of incubationwith 5, larger clusters of about 17 nm were observed. Thesecolloidal particles were very stable and did not show any later-stage evolution. They sequestered oligomers and preventedfurther progression of the amyloid fibril growth, resulting in
significant reduction of peptide toxicity as shown by 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT)assay in vitro.44 Compounds 5, 6, and 7 (50 μM) delayed theAβ-induced paralysis in transgenic Caenorhabditis elegansstrains, which express human Aβ 1−42 and represent asimplified invertebrate model of AD.72 This effect was dose-dependent and similar for all three congeners. The beneficialeffect on paralysis was associated with a strong decrease in thesoluble oligomeric Aβ forms and reduced deposition of fibrils inmuscle cells. Moreover, FTIR spectroscopy was used tocharacterize amyloid aggregates conformation at the molecularlevel in Caenorhabditis elegans and it was shown that TCshinder protein aggregation. In particular, worms treatment withTCs significantly reduced the absorption in the amide I regionof second derivative FTIR spectra (band at 1623 cm−1), whichcharacterizes the intermolecular β-sheet structure of proteinaggregates.72
The therapeutic role of 6 in combination with anotherantibiotic, rifampin (Figure 1, compound 4), that was shown toinhibit Aβ aggregation and in vitro neurotoxicity has beenassessed in patients with AD in a randomized, placebo-controlled, multicenter clinical trial.73,74 It has been shown thata 3-month course therapy of 6 (200 mg) and 4 (300 mg)significantly reduced cognitive worsening at 6 months offollow-up in patients with mild to moderate AD.73 There wasalso less dysfunctional behavior at 3 months. This decrease wasnot, however, observed at 6 and 12 months in the treatmentgroup with respect to the placebo group.73 Since Chlamydiapneumonia infection is thought to be implicated in AD, thecombined treatment with compounds 4 and 6 on Chlamydiapneumonia IgA or IgG antibody titers in patients wasperformed. However, the laboratory results did not show anysignificant reduction of Chlamydia pneumonia IgA or IgGantibody titers between treatment groups at 6-month follow-up.Considering previously reported antiamyloidogenic activity ofboth 6 and 4, authors suggested that the effect of the drugs oncerebral amyloid deposition could explain the clinicalfindings.73 However, the subsequent multicenter, blinded,randomized, 2 × 2 factorial controlled trial, conducted by thesame group and involving 406 patients, demonstrated that 12months of treatment with 6 (100 mg twice a day) or 4 (300mg/day) had no beneficial effects on cognition or function inAD.74 Currently, there are two ongoing clinical trials studyingthe effect of TCs in patients with AD (Table 1).These results attracted the interest of the research
community and gave rise to various in vitro and modelorganism studies using amyloidogenic proteins including butnot limited to human amylin, huntingtin, W7FW14F,apomyoglobin, poly-(A) binding protein nuclear 1, α-synuclein,β2M, and LC. Thus, Aitken et al. found that 5 decreased fibrilformation by the pancreatic hormone amylin, representing thepancreatic islet amyloid in advanced type II diabetes mellitus.75
In vitro studies showed that the presence of 20-fold molarexcess of 5 caused a gradual reduction in ThT binding toamylin with a half-life of 3.4 h. This indicates the drug’s capacityto hinder amylin assembly. Transmission electron microscopyexperiments have complemented these data, showing thatincubation of synthetic human amylin with 20-fold molar excessof 5 for approximately 20 h resulted in the formation of smallglobular structures and short fibril fragments. In the absence ofthe drug, however, longer and more dense characteristic amylinfibrils were observed.75 Successive in vivo studies were carriedout on transgenic hA/hIAPP mice that spontaneously develop
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXH

diabetes and produce human amylin (hA)/islet amyloidpoypeptide (hIAPP), thereby forming amyloid deposits inpancreatic islets.75 In this model, low doses of 5 (0.03 mg/mLdrinking water) for 60 days partially suppressed the progressionof diabetes. However, it did not influence the disease onset.Administration of 5 at a higher dosage (0.5 mg/mL drinkingwater) for 60 days significantly delayed both diseaseprogression and onset. In particular, 5 dose-dependentlyameliorated both hyperglycemia and polydipsia, resulting inan increase in median survival of 254% compared with controlanimals.75 The authors suggest that the observed ameliorationswere likely linked to the interaction of 5 with soluble nascentprefibrillar aggregates of hA/hIAPP rather than to any putativeextrapancreatic effects.75
Similarly, 5-fold molar excess of 5 inhibited fibrillogenesis ofthe amyloid forming protein W7FW14F apomyoglobin.76
AFM, ThT fluorescence, and dynamic light scattering studieshave demonstrated that incubation of the protein for 7 days inthe presence of 5 inhibited the formation of fibrils from earlyaggregates. In fact, in the presence of 5 only globular oligomericstructures were observed, while control samples presentedmostly mature fibrils. It is worth noting that, once formed,mature fibrils of W7FW14F apomyoglobin could not bedisrupted by 5 even at high drug to protein molar ratios (up to25:1) or long incubation time (up to 15 days). This was atvariance with previously reported results for Aβ 1−42, PrPSc,and TTR.42,66,77 According to the authors only few segments ofW7FW14F apomyoglobin are involved in the formation cross-β-sheet structure. Therefore, the core of the fibril might havelow accessibility for the noncovalent interactions with 5, thuspreventing fibril disaggregation by the drug.76 It was also foundthat the persistent globular aggregates of W7FW14Fapomyoglobin forming in the presence of 5 were able tointeract with cell membranes and cause cytotoxicity. In thisregard, authors suggest the careful usage of 5 as fibrilinhibitor.76
Compounds 5, 6, 7 and rolitetracycline (17) are all able todisrupt fibrils of TTR Leu55Pro protein, associated with one ofthe most aggressive forms of FAP and composing ofextracellular amyloid deposits.77 Thus, after 17 days ofincubation at 37 °C with the drugs, the samples clearly showedan abundance of small round particles. In these conditions 6was revealed as the most effective of the tested derivatives, asno fibrils were visible after incubation while in the cases of 5, 7,and 17 very few fibrils were present, similar to those found incontrol samples.77
Fibril disrupting activity of 6 has been confirmed in vivo intransgenic mice caring the Val30Met mutant of TTR.78 Thus,animals treated with 40 mg kg−1 day−1 6 in drinking water for 3months did not present mature TTR fibrils in deposits, asestablished by the lack of green birefringence in tissues stainedwith Congo red. At the same time, levels of nonfibrillar TTRload in tissues of treated animals were comparable to thosedetected in the control group. This suggests that while 6 wasvery efficient at disrupting already formed fibrils, it could notinhibit fibril formation until they reach a certain length.78
However, combined administration of 6 and an antioxidantcompound, tauroursodeoxycholic acid (TUDCA), in transgenicmice produced a synergic beneficial effect on both TTRamyloid deposition and all biomarkers associated with FAP.79
This stands in contrast to single individual drug administrationwhich did not affect biomarkers.79 On the basis of theseobservations, Obici et al. designed a phase II, open-label study
(Clinicaltrials.gov identifier NCT01171859) to evaluate theefficacy, tolerability, safety, and pharmacokinetics of 6 (100 mgtwice a day) and TUDCA (250 mg three times a day)administrated continuously in patients with TTR-relatedamyloidosis.80 The results of the 12-month follow-up showthat coadministration of 6 (100 mg twice a day) and TUDCA(250 mg three times a day) stabilized the disease for at least 1year in the majority of patients treated to date. No clinicalprogression of cardiac involvement was observed. Theneuropathy, as well, remained substantially stable for over 1year. The treatment was well tolerated and feasible for agedpatients with advanced diseases.80
Human α-synuclein is a highly conserved presynapticprotein. When aggregated, it represents the major fibrillarcomponent of cytosolic filamentous inclusions in α-synucleo-pathies, including Parkinson’s disease (PD).81 Thioflavin Sfluorescence and electron microscopy studies have shown that5 dose-dependently inhibited fibrillogenesis of α-synuclein anddestabilized preformed fibrils in vitro.81 Compound 7 wasshown to be protective in animal models of PD, induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine, providing dopa-mine depletion.82 It was also tested in an 18-month double-blind futility clinical trial for its potential to alter the short-termcourse of PD to a predetermined threshold.83 This approachpermits minimizing the number of subjects required for thestudy and provides indications of whether or not to proceedwith further large-scale trials. The results of the 12-monthevaluation of the clinical progression of PD suggest that 7should be considered for definitive phase III trials to determineif it alters the long-term progression of the disease.83
Beneficial effects of 7 in a mouse model of Huntington’sdisease (HD), characterized by formation of Huntingtinaggregates in autopsy brains, were first reported in 2000 byChen et al.84 Thus, in R6/2 transgenic mice, expressing exon-1of human huntingtin, daily treatment with 5 mg/kg of 7resulted in improvement of rotarod performance and extendedsurvival rates by 14%. These ameliorations were stronglyassociated with minocycline-induced inhibition of caspase-1and caspase-3 up-regulation and reduced activity of induciblenitric oxide synthase (iNOS).84 Later, Smith et al. investigatedthe ability of TCs to inhibit Huntingtin aggregation both invitro in a hippocampal slice culture and in vivo using the samemouse model. This was done in order to estimate thecontribution of antiamyloidogenic activity of TCs in neuro-protection.85 It was found that 5, 6, and 7 drastically reducedaggregation of huntingtin at 30 μM in organotypic slice culturemodel. They were also well tolerated and reduced hyper-glycemia in aged R6/2 mice by an unknown mechanism.However, in contrast to previous studies, the drugs neitherreduced aggregate load in R6/2 brains nor produced anyimprovement in the behavioral phenotype of mice.85 Anothermouse model of HD (strain N171-82Q) also reported noimprovements in survival, weight loss, or motor function aftertreatment with 7.86 Finally, to assess the safety and futility of 7at 200 mg/day in HD, an 18-month randomized, double-blindstudy using a futility design was conducted by the HuntingtonStudy Group.87 This study demonstrated that while not entirelyfutile, treatment with 7 provided minimum clinically relevantbenefit. In conclusion, the results suggested that it would not beadvisable to continue with the larger trial.87
Oculopharyngeal muscular dystrophy (OPMD) is anautosomal dominant progressive disease. It is associated withaccumulation of fibrils, formed by the mutant poly-(A) binding
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXI

protein nuclear 1 (PABPN1) within the nuclei of skeletalmuscle cells. In a mouse model of OPMD, 6 not only delayeddisease onset and attenuated disease phenotype but alsodecreased formation of PABPN1 aggregates in muscles.88 Sinceprevious studies have demonstrated the positive correlationbetween the decrease in aggregation of PABPN1 and reducedcytotoxicity, authors suggested that the antiamyloidogenicproperties of 6 likely contributed to its beneficial effects.Additionally, proapoptotic processes, such as Bax expression,cytochrome c release, and caspase-3 activation, were attenuatedin response to the treatment with 6. This indicates that togetherwith antiamyloidogenic properties, antiapoptotic activity of thedrug could also play an important role in protection againstOMPD.88
The most commonly diagnosed form of systemic amyloidosisresults from the aggregation and deposition of LC, produced byclonal plasma cells in the bone marrow.89 About 26% oftransgenic mice CMV-λ6, expressing human λ LC protein,developed amyloid deposits in the stomach within 6 months.Treatment with 0.5 mg/mL 6 in drinking water, starting from 3to 6 months and lasting at least 7 months, resulted in reducedamyloid deposits. Thus, only 23% of the treated mice hadamyloid deposits in the stomach, compared to 69% in theuntreated control group.89 Electron microscopy studies havedemonstrated that 6 not only inhibited fibrillogenesis of therecombinant LC protein in vitro but also disaggregated maturefibrils from patients ex vivo. Thus, after 5 days of incubation ofthe recombinant LC protein in water, EM images revealed thepresence of mature fibrils. On the other hand, after co-incubation with 6, fibrils were disorganized, broken, and leftwith frayed ends. Numerous large aggregates were also detectedafter incubation of tissue-extracted fibrils with 6, confirming adirect interaction between the drug and the fibrils.89
Abnormal aggregation and accumulation of a mutant αB-crystallin protein in myocytes is a key feature of desmin-relatedcardiomyopathy.90 Transgenic mice, producing a well charac-terized mutant of human αB-crystallin, CryABR120G, were usedto test its therapeutic effect in cardiac proteinopathies. It wasfound that the administration of 6 mg/mL 6 with drinkingwater, starting at 8−16 weeks of age, significantly delayed thepremature death of treated animals compared to control andattenuated cardiac hypertrophy. These ameliorations wereassociated with a decrease in accumulation of CryABR120G
aggregates in the hearts of treated mice. Similarly, a dose-dependent inhibition of aberrant protein aggregation by 6 wasobserved in culture cells infected with recombinant adenovirusexpressing CryABR120G protein.90
Amyloid deposits formed in patients subjected to long-termhemodialysis are mostly composed of full length β2M and itsN-terminal truncated species ΔN6β2m.91 Compound 5 and itsderivatives were able to inhibit fibrillogenesis and, uponprolonged exposure, disaggregated β2M fibrils. This wasshown by significantly reduced ThT fluorescence and completeloss of fibrillar structure observed by electron microscopy.Moreover, 6 at equimolar concentrations to β2M (100 μM)fully abrogated the toxicity of soluble β2M oligomers in SH-SY5Y neuroblastoma cell line.The effect on the cytotoxicity of the mature β2M fibrils was
more complex. In particular, the exposure of originally nontoxicfibrils to 6 elicited a transient dose-dependent cytotoxic effectin the range 100−300 μM. At 300 μM 6 this effect reachedmaximum levels after 3 days of incubation and disappearedafter 7 days of incubation.91 Cytotoxicity was directly related to
the doxycycline-induced evolution of fibril morphology imagedby AFM. In fact, exposure to 6 gave rise to fibril disaggregationinto smaller oligomeric species. These accumulations peakedafter 3 days of incubation. At longer incubation times, theseoligomers reassembled into more complex structures.91
Curiously, among 13 tetracycline congeners tested, only 7derivatives were able to inhibit β2M fibril growth, as establishedby ThT assay. According to these data, antifibrillogenic activityof these derivatives decreases in the following order: 6 ∼ 4-epioxytetracycline (13) > 11 ∼ methacycline (9) >meclocycline (8) > 17 ∼ anhydrochlortetracycline (16).Compounds 5, 7, 14, demeclocycline (15), 4-epichlortetracy-cline (18), and 4-epianhydrotetracycline (12), on the otherhand, were not active.91 Interestingly, according to differentstudies, antiamyloidogenic activity of TCs varies significantly.By estimation of the ability of 15 TCs to reduce the resistanceof preformed PrP106−126 fibrils to proteinase K, 11 and 17were identified as the most active derivatives. Compounds 5, 6,anhydrotetracycline (10), 13, and 15 were less potent, while 7and some other analogues were not active.92 Another study,based on Aβ-fibril specific immunoassay, showed that only one(17) out of eight compounds was able to inhibit formation ofAβ 1−40 fibrils.93 The immunoassay, based on estimation ofthe reduction of anti-Aβ antibodies binding to Aβ 1−42 fibrilsin the presence of TCs, demonstrated that 11 and 14 bindmore efficiently to Aβ fibrils compared to 5. Compounds 6 and17 did not affect the binding.94 Electron microscopy images,obtained from TTR fibrils after 17 days of incubation with fourTCs, revealed that 6 was the most effective compound.Compound 7 also demonstrated significant disrupter activity,apparently higher than both 5 and 17. The last one was theleast potent fibril disrupter.77 However, in these studiesdifferent experimental conditions (such as initial state ofaggregation, protein concentration, buffer, time of incubation),and approaches for detection of the effect were used. Therefore,it is difficult to explain the discordant results and to defineunequivocally the structural features responsible for theantiamyloidogenic activity. On one hand, inhibition ofamyloidogenesis could be a function of a specific proteinstructure, as was suggested by Giorgetti et al.91 On the otherhand, false positive/negative results can be derived from thechoice of an inappropriate method of screening. Thus, ThTbinding assay is one of the most common approaches forstudying amyloid aggregation. Recent NMR data, however,showed that 5 competes with ThT for the binding to protein,44
and hence, the use of another screening approach is preferable.For example, X-ray diffraction,5 ELISA-based assay,94 andMALDI MS based method95 for screening the efficiency ofpotential inhibitors of amyloid aggregation have all beenutilized.At present, there are no clear data regarding the relationship
between the structures of TCs and their antiamyloidogenicactivity. The results of molecular mechanics investigationsshowed that despite the flexibility between the extended andfolded conformations of TCs, there was no relevance to theobserved activity. In fact, in solution TCs acquire differentconformations and tautomeric forms that essentially depend onthe solvent, pH, and metal ions such as Ca2+, Mg2+, Cu2+, Co2+,and Ni2+. This confers to the hydronapthacene moiety anextraordinary conformational flexibility, and as a consequence,QSAR studies could not identify any geometrical pharmaco-phore.50 Furthermore, three-dimensional quantitative struc-ture−activity relationship (3D-QSAR) investigation has
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXJ

revealed that hydroxyl groups at positions 5 and 6 areimportant factors in determining antifibrillogenic activity.This is due to their ability to provide donor sites for putativeH-bond interactions with PrP peptides.92 These results are inagreement with data reported by Giorgetti et al. that suggest therelevance of the C5 oxidryl group for the interaction of TCswith β2M.91 A second relevant factor, according to 3D-QSARcalculations, is that the presence of electron-donor substituentson the D-ring enhances the π-electronic configuration of thearomatic ring and favors π-stacking interactions with electrondeficient peptide sites. The correct spatial orientation of thepositively charged C4-NMe2 group contributes to activity,ensuring electrostatic interactions with negatively charged sites.Alkylamine substituent at the amidic group in position 2, as inthe case of 17, was indicated as another factor enhancingantiamyloidogenic activity, while the keto−enolic switchbetween positions 11 and 12 decreases this activity.92
To conclude, numerous studies have demonstrated theantiamyloidogenic activity of TCs both in vitro and in vivo. Inparticular, it has been established that (i) TCs bind to the β-sheet forming domain of all amyloidogenic proteins,independent of their primary structure, by nonspecificinteractions,41,44,91 (ii) inhibition of fibrillogenesis is a resultof the immediate interaction of amyloidogenic protein with thedrug, resulting in formation of stable globular oligomericspecies and preventing further fibril growth,44 (iii) TCs alsoaffect mature fibrils, resulting in their complete or partialdisaggregation,42,75−77,81,85,89−91 (iv) treatment with TCsreduces amyloid-induced toxicity in cell culture,41,44,66,72,79,84
(v) treatment with TCs is often associated with reducedamyloid load in tissues and provides both ameliorations inpathological symptoms and prolonged survival in animalmodels of amyloidoses,17,82,84,88−90 (vi) several preliminaryand ongoing clinical trials demonstrate improvements in clinicaloutcomes in patients affected by different types of amyloidosesin response to treatment with TCs.73,80,83,87
IV. OTHER NONANTIMICROBIAL ACTIVITIES OFTETRACYCLINES AND THEIR POSSIBLEIMPLICATION IN THE TREATMENT OFAMYLOIDOSES
It is well-known that extracellular deposition of protein fibrillaraggregates is the main hallmark of amyloidogenic disorders.Since a variety of studies have demonstrated the ability of TCsto disrupt and/or inhibit formation of amyloid fibrils, thismechanism was initially thought to be responsible for thebeneficial effects of TCs in amyloidoses.17,66,88,90 At the sametime, these diseases are also associated with other commonpathological features such as inflammation,10,80,96 ROSgeneration causing oxidative stress,10,97 dysregulation of metalhomeostasis,98 mitochondrial dysfunction,99 and apoptosis.100
TCs have been recognized as therapeutic agents affecting avariety of pathological targets.46,100 These include matrixmetalloproteinases, apoptotic and inflammatory pathways, andoxidative stress. Therefore, in order to gain a betterunderstanding of the mechanisms underlying the beneficialeffects of TCs in amyloidoses, it is necessary to first summarizethe main features of nonantimicrobial activities of TCs.46
1. Inhibition of Matrix Metalloproteinases. Inhibition ofMMPs is probably the best characterized nonantimicrobialproperty of TCs. MMPs are a family of zinc-dependentextracellular matrix remodeling endopeptidases. They are
involved in a variety of physiological and pathologicalprocesses, including wound healing, tissue repair andremodeling, embryogenesis, inflammation, vascular and auto-immune disorders, cancer progression, and metastasis.46,101−103
Elevated expression of MMPs is also strongly associated withamyloidogenic diseases. Thus, significantly increased levels ofserum MMP-3 have been detected in hemodialysis patientswith dialysis-related amyloidosis.104 Moreover, serum MMP-3levels correlated with serum levels of β2-microglobulin,suggesting a direct stimulation of MMP-3 by β2M.104 In FAPthe elevated expression of MMP-9, colocalized with TTRdeposits, was detected by immunostaining salivary glandbiopsies from patients affected by FAP. In control biopsiesMMP-9 staining was absent.105 The overexpression of MMP-9was observed only at a later stage of disease, when theextracelluar deposits of amyloid fibrils were already present.105
In patients with cardiac amyloidosis due to LC protein, theincreased levels of serum MMP-2 and MMP-9 correlated withdiastolic dysfunction.106 Aberrant and chronic overexpressionof MMPs is also associated with the pathophysiology ofneuroinflammatory processes accompanying most centralnervous system disease. In particular, up-regulation of MPPs(MMP-9, MMP-3, and MMP-2) was detected in the plaque-affected brains and blood plasma of AD patients.107,108 Theoverexpression of MMPs in AD is likely a part of aninflammatory response and can be induced endogeneously byamyloid.107 In vitro studies have shown that both MMP-2 andMMP-9 could degrade Aβ. It is thus believed that both MMP-2and MMP-9 play a beneficial role in the extracellular Aβcatabolism and clearance in vivo. In a mouse model of ADMMP-9 is capable of degrading compact amyloid plaques inbrain sections.109 Excessive activation of MMPs, however, couldcause damage to the blood−brain barrier by attacking theextracellular matrix, basal lamina, and tight junctions inendothelial cells, thus promoting neurodegeneration.107,108 Inaddition, MMPs may act as signal molecules in both neuronalapoptotic processes and inflammation.110 For example, MMP-3participates in neuronal apoptotic signaling by activation ofcaspase-3 followed by DNA fragmentation.110 In neuro-inflammation MMP-3 activates microglia, leading to the releaseof proinflammatory cytokines such as IL-1β and tumor necrosisfactor α (TNF-α).108 These molecules in turn contribute to thedeath and removal of damaged neurons under physiologicalconditions. In contrast, under pathological conditions, theoverexpression of MMP-3 likely causes the death of nearby andundamaged neurons. An increase in MMP-3 levels has beenobserved in various experimental models of PD in the plasma,cerebrospinal fluid, and around senile plaques of AD patients. Italso appears elevated in blood mononuclear cells of multiplesclerosis patients.108
Taking these facts into account, down-regulation of MMPs isexpected to produce beneficial effects in a number ofpathological conditions. A considerable effort has been madeto develop safe and effective synthetic compounds targetingMMPs. Nearly 60 MMP inhibitors, including peptidomimetics,nonpeptidomimetics, and various natural compounds, havebeen developed and tested in clinical trials over the past severalyears. With the noteworthy exception of 6, however, all MMPsinhibitors were abandoned at early stages of clinical trialsbecause of low water solubility, lack of efficacy, and severe sideeffects. This failure is mainly due to the broad spectrum ofaction of MMPs inhibitors and complex biology of theenzymes.101
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXK

In 1983 Golub et al. first reported their finding that TCs arecapable of inhibiting collagenase-mediated breakdown ofconnective tissue in periodontitis that is associated with typeI diabetes.111 Later, Greenwald et al. found that 7 could reduceexcessive collagenase activity in diseased joints of patients withrheumatoid arthritis.112 While the precise mechanism under-lying the inhibitory effect of TCs on MMPs is not yet clear, it isbelieved that TCs act by direct inhibition of the enzymes andby down-regulation of their expression.46
Direct inhibition of the MMPs activity is likely mediated byTC chelation of metal ions associated with the enzyme. Thisprocess can, in fact, be reversed by the addition of micromolarconcentrations of zinc or millimolar concentrations of calciumions.113 Moreover, it was demonstrated that a chemicallymodified derivative of 5 (tetracycline pyrazole, CMT-5,115
compound 19) incapable of metal chelation did not inhibitMMPs.114 It was initially thought that 5 binds catalytic Zn2+.Further structural studies, however, indicated that themechanism of inhibitory effect involves drug interaction withthe structural zinc and/or calcium atoms within the proteinrather than with the catalytic zinc ions.113,115,116 In fact, Garciaet al. demonstrated that 6 binds matrilysin (MMP-7) proximalto the structural metal center of the protein, containing bothzinc and calcium ions, and destabilizes the tertiary structure ofthe enzyme.116 Moreover, studies of the effect of 6 on MMP-8activity and susceptibility to proteolytic digestion indicate thatthe destabilization of the enzyme is due to binding of TCs tocalcium rather than to zinc ion.117 In fact, the inhibitory effectof 6 on MMP-8 was duplicated by calcium and zinc chelatorEDTA. This effect was not duplicated, however, by 1,10-phenanthroline, a selective chelator of zinc.117
Compound 6 is now the only inhibitor of MMPs approvedfor systemic use by the U.S. Food and Drug Administration andregulatory agencies in Europe and Canada.118 The beneficialeffects of TCs as MMPs inhibitors are now being studied in anumber of clinical trials (Table 1).Various clinical studies evaluating beneficial effects of TCs in
rheumatoid arthritis demonstrated mild to moderate beneficialeffects.119 In a very recent paper, however, Greenwald affirmsthat the road forward in rheumatoid arthritis treatment nolonger involves 6 or 7. He pointed instead to other, morepowerful drugs. His conclusions do not exclude the possibilitythat a more effective chemically modified nonantimicrobialchemically modified derivative of tetracycline (CMT) mayprove to be useful.119
2. Scavenging of Reactive Oxygen Species. Oxidativestress is associated with increased formation of ROS, resultingin DNA damage, lipid peroxidation, protein modification, andother effects. It is also a typical feature of numerous diseasesincluding cancer, cardiovascular disease, diabetes, atheroscle-rosis, neurological disorders (AD, PD etc.), and chronicinflammation.120 Reactive oxygen species, including superoxide(O2), hydrogen peroxide (H2O2), peroxynitrite (ONOO−),hydroxyl radical (OH•), and nitric oxide (NO), are moleculeswith unpaired electrons in their outer orbit. This makes themvery unstable and highly reactive, disposed to initiate chainreactions with surrounding biomolecules. For example,peroxynitrite and its decomposition products can modify thestructure and function of proteins by nitration of tyrosineresidues or methionine sulfoxidation.121 At lower concen-trations NO acts as a neurotransmitter and signalingmolecule.122 It is estimated that generally 5% of oxygen takenup by a tissue is transformed into ROS. In order to overcome
the potential toxicity of ROS under physiological conditions,they are neutralized by endogenous enzymatic free radicalscavengers such as superoxide dismutase, glutathione perox-idase, and catalase.120 Under pathological conditions, anexcessive production of ROS overwhelms the defense capacityof endogenous antioxidants and may produce injurious radical-mediated reactions causing cell apoptosis. In order to reducethe oxidative stress and ameliorate the pathological conditionsof some ROS-related diseases, antioxidant therapeutics havebeen proposed. These include small ROS scavengers, inhibitorsof ROS generating enzymes, and antioxidative enzymes.120
Induction of inducible nitric oxide synthase (iNOS), respon-sible for excessive nitric oxide and peroxynitrite production, hasbeen observed in animal models of AD and HD, as well as inhumans affected by FAP, AD, and HD.84,122,123 Some dataindicate that mitochondrial dysfunction likely underliesoxidative damage in AD brains.97,124 Those neurons immunor-eactive-positive for oxidative damage (8-hydroxyguanosine)also showed an increased cytochrome oxidase in the brains ofAD patients, suggesting that mitochondrial dysfunction mightlead to oxidative damage in AD.The antioxidant potential of TCs was first reported about 25
years ago.125 At that time it was shown that 5, 6, and 7 inhibitedproduction of O2
−, H2O2, and OH• by zymosan-stimulatedleukocytes. Compound 7 was the only derivative able toscavenge free radicals directly in the cell-free xanthine−xanthineoxidase assay.125 Later, Akamatsu et al. demonstrated that 6 wasalso an efficient antioxidant in both cell-based and cell-freesystems.126 In vitro studies have shown that TCs can protectbiological macromolecules against damage induced by reactivenitrogen species, especially peroxynitrite. Moreover, recentstudies showed that 7 acts as a direct and highly selectivescavenger of peroxynitrite.121 The same study demonstratedthat 5, however, did not. According to the authors,peroxynitrite might be a direct target of 7 in vivo. They alsosuggested that peroxynitrite neutralization by 7 represents themechanism that protects biological targets from oxidativedamage.121 At the same time, the antioxidant potential of 7against other free radicals such as 6-hydroxydopamine, NO, andglutamate has also been observed in vitro.49
In vitro in a rat model of cardiac ischemia−reperfusion, 7produced a cardioprotective effect in part due to the reductionof oxidative stress.127 Antioxidant properties of 6 have also beenreported. Thus, in diabetic animal models and diabetic humansthe presence of high glucose levels induced a significantincrease in ROS production and impaired antioxidant defenses,causing severe cardiovascular dysfunction. Treatment ofdiabetic rats with 6 resulted in significant reduction in oxidativestress markers in plasma. It also preserved endothelial vascularfunctioning directly affecting endothelium, smooth muscle, orboth.128 Moreover, 6 was shown to alleviate doxorubicin-imposed oxidative stress on the heart tissue in mice byinhibiting ROS generation and stimulating endogenousantioxidant enzymes (superoxide dismutase and glutathioneperoxidase).129
The mechanism of the antioxidant activity of TCs remainselusive. On one hand, the presence of a multiple-substitutedphenol ring in the chemical structure of TCs makes them directradical scavengers, similar to vitamin E.49,121,125 Reaction of thephenol ring with free radicals results in the formation of arelatively unreactive phenol-derived free radical.48 Stability ofthese radicals depends on the number and size of phenol ringsubstituents as well as the extent of resonance stabilization. In
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXL

fact, 7, which has a dimethylamino substituent at the C7position of the D-ring, demonstrated superior scavengingactivity in both lipid peroxidation and 2,2-diphenyl-1-picrylhydrazyl (DPPH) assays with respect to the otherTCs.49 The effective concentrations of TCs in cell-free assayswere much higher (5−25 μM) than those providing protectiveeffects in cell-based assays (1−20 nM). From this one gathersthat direct antioxidant activity probably does not represent theprimary mechanism of protection against oxidative injury to acell.49 Therefore, several alternative mechanisms involvingdifferent intracellular pathways have been proposed. Forexample, in vitro and in vivo studies have shown that 7 and6 can inhibit iNOS, which is responsible for the generation ofexcessive NO amounts in inflammatory and autoimmuneprocesses.130,131 In murine macrophages and human cartilageaffected by osteoarthritis, compounds 7 and 6 inhibit iNOSexpression at the level of iNOS mRNA and protein expression.This implies a down-regulation of its specific activity.132
Another study suggests that the decrease in iNOS levels inLPS-stimulated cells treated with 7 was mediated by 7-inducedTNF-α inhibition. Finally, implication of p38 MAPK pathwayin the protective effect of TCs against oxidative stress has alsobeen proposed.130
3. Anti-Inflammatory Effects. Acute inflammation is atemporary and self-limiting response to infection or injury. Itultimately serves to remove damaged tissue and generate newtissue. This results in restoration of tissue homeostasis and,subsequently, healing. By contrast, chronic inflammation, whichis a result of immune dysregulation, plays a central role in themaintenance of pathological conditions. Chronic inflammationis characterized by an escalating cycle of tissue damage,resulting in autoimmunity, malignant transformation, ordeleterious changes in tissue morphology and function.46
Proinflammatory cytokines, produced during inflammatoryprocesses by activated immune effector cells, stimulate releaseof ROS and activation of MMPs. This results in direct injury tothe surrounding healthy tissue.As previously discussed, TCs can both inhibit MMPs and
protect from oxidative stress. Therefore, they are capable ofexerting anti-inflammatory actions. In addition, it was foundthat TCs can reduce elevated levels of proinflammatorycytokines. Thus, in a murine model of LPS-induced lethalendotoxemia, TCs significantly reduced TNF-α and IL-1βlevels in serum, producing a protective effect against LPS-induced shock.133 Since TCs did not affect directly theexpression of cytokines by LPS-induced macrophages in vitro,the authors deduced that TCs likely modulated some upstreampathway implicated in the production of TNF-α and IL-1β.133
Conversely, Krakauer and Buckley demonstrated that 6 directlyinhibited production of cytokines (IL-1β, IL-6, TNF-α, andIFN-γ) and chemokines (MCP-1, MIP-1α, and MIP-1β) byhuman peripheral blood mononuclear cells stimulated withstaphylococcal exotoxins.134 In neuroinflammation, the effectsof TCs are wide-ranging and include suppression of differentinflammatory factors. These include TNF-α, cycloxygenase-2,interleukins (IL-2, IL-6, IL-1β), iNOS, MMPs, and kinases(apoptosis signaling kinase-1, c-jun N-terminal kinase, p38mitogen-activated protein kinase).100
In vivo in a mouse model of induced acute or chronic colitis,treatment with 7 significantly reduced the levels of cytokinesIL-1β, TNF-α, and IL-6 and iNOS expression in colonictissues.131 Similarly, in a murine model of Kawasaki disease,associated with inflammatory response focused at the coronary
arteries, 6 inhibited T cell activation and TNF-α production inperipheral immune cells.135 Enzymatic activity of MMP-9induced by TNF-α also decreased after treatment with 6,reducing the elastin breakdown in coronary vessels andimproving coronary outcome.135
Aortic aneurysm is another pathology strongly associatedwith inflammation and increased MMPs expression. Animalstudies of 6 for abdominal aortic aneurysm treatment providedsignificant evidence of a beneficial effect. In mice with inducedaneurysm a treatment with 6 produced a dose-dependentattenuation in the progression of aneurysmal dilatation.136 Inhumans there was a significant attenuation of vascularinflammation. This consisted of a reduction of neutrophil andcytotoxic T-cell content in the aortic wall, selective suppressionof inflammatory cytokines (IL-6 and IL-8), transcriptionalfactors (AP-1, C/EBP, STAT3), and a reduction of neutrophil-derived proteases (MMP-9). However, there was no amelio-ration in patients’ outcome.137 The conflicting evidenceproduced by human and animal studies regarding the beneficialeffects of 6 on aneurysm progression is likely due to the poorquality of current clinical studies. It is expected that furtherclinical trials, involving large subject numbers with longer 6exposure and prolonged follow-up, could help clarify thismatter.At the same time, TCs were shown to produce beneficial
effects in a number of inflammation-related pathologies. In apatient affected by pulmonary, ocular, and muscular sarcoidosis,4-month treatment with 7 (200 mg/day) reduced both themuscle symptoms and the levels of IL-12 and interferon-inducible protein-10 (IP-10), generated by granuloma macro-phages at the inflamed sites and the bloodstream.138 Moreover,it was noted that during the treatment with 7 the levels ofcirculating cytokines and chemokines associated with T helpertype 1 response decreased. Levels of Th2-associated chemo-kines remained elevated. The disease rapidly relapsed afterdiscontinuation of the 7 administration. Subsequent 7readministration resulted in prompt improvement of symptomsagain, indicating the immunomodulatory mechanism ofaction.138 Similarly, some patients with persistent postneur-oborreliosis symptoms improved during 6 treatment butrelapsed after completed treatment (ClinicalTrials.gov identifierNCT01205464).In dermatology 6 and 7 were shown to be effective for the
treatment of acne and rosacea, resulting in a significantreduction in inflammatory lesions.46 Two randomized,double-blind, placebo-controlled, multicenter trials havedemonstrated the efficacy and excellent risk−benefit ratio of6 (40 mg/day) in the treatment of rosacea.139 Bipolar disorderis characterized by reduced monoaminergic signaling and otherneural changes. Such changes include dendritic remodeling,demyelination, and glial and neuronal cell loss deriving fromchronic inflammation. Phase III clinical trial of 7 efficacy forbipolar depression treatment is currently ongoing. This trial hasthe specific aim of investigating the correlation between theexpression levels of inflammatory cytokines and depressionratings in response to 7 (ClinicalTrials.gov identifierNCT01429272).In patients with adult and chronic periodontitis the oral
administration of subantimicrobial doses of 6 also producedsignificant improvements in clinical parameters. These improve-ments include tooth attachment, probing depth, clinicalattachment level, gingival index, plaque index, and decreasedproinflammatory cytokines levels.140
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXM

4. Antiapoptotic Effects. Apoptosis is a tightly regulatedcell death program. It involves many factors and is important inmaintaining tissue hemostasis. Activation of caspases is a keyevent in apoptotic cascades and may occur via extrinsic orintrinsic pathways. Extrinsic pathways are triggered by bindingof death signal proteins to their cell surface receptor. This stepis followed by activation of initiator caspase (caspase-8) whichin turn activates downstream effector caspases. Intrinsicpathways can be activated by various types of intracellularand extracellular stress stimuli (for example, excessive intra-cellular levels of Ca2+). Such pathways involve permeabilizationof the mitochondrial membrane and release of cytochrome cinto the cytoplasm. Cytochrome c then forms a multiproteincomplex known as the “apoptosome” and initiates activation ofthe caspase cascade through caspase-9.46,141 Caspase-independ-ent apoptosis involves Smac/DIABLO (mitochondria-derivedactivator of caspases/direct inhibitor of apoptosis proteinbinding protein with low pI) and apoptosis-inducing factor(AIF) proteins that are released from the intermembrane spaceinto cytosol.TCs were shown to possess antiapoptotic activity, which is
believed to involve the reduction of caspase expression.46 Thus,in a mouse model of HD, treatment with 7 resulted in down-regulation of both caspase-1 and caspase-3.84 Neuroprotectionby 7, associated with a reduction in caspase-1 and/or caspase-3expression, has also been observed in animal models oftraumatic brain injury, cerebral ischemia, and PD.46 The factthat 7 could not directly affect enzymatic activity of thecaspases in the enzymatic assay84 indicates that there might bean upstream mechanism that results in caspase down-regulation. One of the known physiological stimuli forcaspase-9 and caspase-3 activation is cytochrome c releasefrom mitochondria into the cytoplasm. In fact, several groupshave reported that in rodent models of amyotrophic lateralsclerosis, HD, and spinal cord injury, 7 inhibited cytochrome crelease from mitochondria. Besides that, it likely affectedmitochondrial permeability transition (MPT) and reduced theexpression levels of initiator caspases.142 In addition tocytochrom c, the decrease in release of other proapoptoticfactors, such as AIF and Smac/Diablo in response to treatmentwith 7, has been observed both in vitro and in a mouse modelof HD.142 Later, Antonenko et al. demonstrated that the effectof 7 was more likely related to the direct interaction of the drugwith mitochondrial membrane in complex with Ca2+, resultingin formation of ion channels and prevention of excessive Ca2+
accumulation in the mitochondrial matrix.143 Moreover, theselective activity of TCs against mammalian cell mitochondriahas also been previously described. Thus, it was shown thatTCs not only selectively accumulate in mitochondria144 butalso depolarize membrane potential, decrease respiratorycontrol, and inhibit synthesis of mitochondrial DNA-encodedproteins.145 In fact, in human liver epithelial cells treatmentwith micromolar concentrations of 5, 6, and 7 decreased levelsof a mitochondrial DNA-encoded protein (complex IV-subunit1). They did not, however, decrease those of a nuclear DNA-encoded protein (complex V-α subunit).146 As antibiotics, TCstarget protein synthesis on bacterial ribosomes.61 Consideringthe structural similarity between bacterial ribosomes andeukaryotic mitochondrial ribosomes, it is not surprising thatTCs can also selectively inhibit synthesis of mtDNA-encodedproteins. It is believed that impairment of mitochondrialbiogenesis is also implicated in immunosuppressive propertiesof TCs. Mitogen-induced blasts formation requires ATP
generated in mitochondria. Since 6 is able to impairmitochondrial biogenesis, it inhibits blast formation andhence produces an immunosuppressive effect.147
TCs apparently exert the antiapoptotic activity by amechanism involving mitochondrial stabilization. This mecha-nism ultimately results in a reduced release of cytochrome c andother proapoptotic proteins. At the same time, proapoptoticactivity of 6 has been observed in human cancer cell culture. Itwas also associated with reduction of mitochondrial trans-membrane potential and an increased cytochrome c releasewith attendant caspase-8 and caspase-9 activation.141 Curiously,the observed inhibitory effect on the growth of human andmouse cancer cells was observed for 6 but not for its analogue7.148 Moreover, it was found that 6, toxic to human and mousemelanoma cells, did not affect normal cell growth of rat aorticvascular smooth muscle cells. This indicates that the effect of 6may differ for normal and cancer cells.148 The mechanism ofpossible proapoptotic activity of 6 on cancer cells remains apoint of investigation and study. The possible mechanisms thathave been proposed include JNK activation mediatedapoptosis148 and caspase independent mitochondrial apoptoticpathway.141
V. CONCLUSIONS
Brown et al. first started to treat patients suffering fromrheumatoid arthritis with 14 and described their beneficialeffects in several papers.149 Although the mechanism of actionof TCs was then unknown, there was general agreement on thepossibility that their antimicrobial properties were responsiblefor the observed therapeutic effect. Subsequently, Paulus raisedthe question of whether various nonantimicrobial activities ofTCs (such as MMPs inhibitory, anti-inflammatory, immuno-suppressant) were involved in the clinical benefits inrheumatoid arthritis.150
Since then, ample evidence has been provided of theimportant role of TC nonantimicrobial activities in a variety ofpathologies, suggesting that their protective effects coulddepend on a combination of pathological pathways.46,53,100,152
As discussed above, the pleiotropic chemical properties ofTCs make them efficient against a variety of biological targetsand underlie both nonantimicrobial and antimicrobial activities.To shed light on the possibility of distinguishing the
therapeutic targets of TCs, we compared the treatmentschedules and dosages used in different clinical trials. In almostall these trials the doses of TCs were very similar, with very fewexceptions (acne, rosacea, and periodontal disease). Thedosages generally used are 250−1000 mg/day for 5, 100−200mg/day for 6, and 50−100 mg/day for 7. This is true for bothshort- and long-term treatments.45 The same dosages aregenerally recommended for the treatment of bacterialinfections.45 Tetracycline blood levels at these dosages showdose related linearity, regardless of the pathological state of thepatients.45 Two hours after a single oral dose of 100−200 mg of6, peak serum concentrations range from 1.7 to 5.7 mg/L,falling to 1.45 mg/L at 24 h.45 After intravenous infusion of thesame dose, peak plasma concentrations range from 5 to 10 mg/L, falling slowly and persisting for 24 h at 1−2 mg/L.45
According to in vitro studies, 3−20 μg/mL concentrations ofTCs, which can be achieved in patients after administration of200 mg of the drug, are enough to exert MMPs inhibitory, anti-inflammatory,130 antiapoptotic,151 and antioxidant49,121 activ-ities.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXN

In conclusion, considering the TCs doses given to patientsfor different pathologies, it is hard to establish specificity of thetarget affected by the drug. The final beneficial clinical outcomeof TCs therapy is most likely a result of targeting multiplepathological events leading to a combination and/or synergy ofeffects (Figure 3). The use of TCs to treat amyloidoses mayaffect the main pathological target, such as aggregation anddeposition of the misfolded proteins. They may also contributeto improving other pathological events, concurrent withamyloid deposit formation, including inflammation, ROSgeneration causing oxidative stress, apoptosis, and uncouplingof metal homeostasis. Our analysis of the literature indicatesthat there is very likely room for improving the therapeuticindex of TCs in various diseases and a more rational approachin new treatment schedules would be welcome. Clinical trialsneed to be designed specifically to reassess the therapeuticactivity of TCs, closely monitoring plasma levels in patients. Onthis basis only, it will be possible to rationally re-evaluate thepotential of this family of molecules.
■ AUTHOR INFORMATION
Corresponding Author*Telephone: +390239014447. E-mail: [email protected].
NotesThe authors declare no competing financial interest.Biographies
Tatiana Stoilova received her Ph.D. from the Lomonosov MoscowState Academy, Russian Academy of Sciences, in 2001 followed by apostdoc at the Department of Biochemistry, Biophysics, and
Macromolecular Chemistry, University of Trieste, Trieste, Italy. Atpresent she is attending the Advanced School of AppliedPharmacology at the Istituto di Ricerche Farmacologiche “MarioNegri”, Milan, Italy. She is involved in studies aimed at developing newpeptides with antiamyloidogenic activity using structure and ligandbase drug design. She also carries out structural analysis ofamyloidogenic proteins by means of X-ray and neutron diffraction.
Laura Colombo. Since 1985 she has been a Research Scientist in theDepartment of Molecular Biochemistry and Pharmacology at theIstituto di Ricerche Farmacologiche “Mario Negri”, Milan, Italy. Herresearch efforts focus on the development of physicochemicalapproaches for the identification of small molecules hindering theformation of soluble toxic oligomers and amyloid fibrils, with particularregard to prion-related encephalopathies and Alzheimer’s andParkinson’s diseases. She has carried out the original preclinicalstudies that enabled doxycycline to enter phase II clinical studies as anantiamyloidogenic drug.
Gianluigi Forloni. Since 2002, he has been the Head of theDepartment of Neuroscience at the Istituto di Ricerche Farm-acologiche “Mario Negri”, Milan, Italy. His scientific interests arefocused on the biological and genetic bases of aging-related disorderswith particular regard to prion-related encephalopathies andAlzheimer’s and Parkinson’s diseases. He has investigated the role ofprotein misfolding in neurodegneration in experimental models toidentify new pharmacological targets. His main achievements wereobtained in the following fields: the identification of new pathogenicmutations in Alzheimer’s and Parkinson’s disease; the characterizationof the apoptotic mechanism mediating the neurotoxicity of peptidesderived from prion protein, β-amyloid, and α-synuclein; thedevelopment of animal models to investigate the pathogenesis of
Figure 3. Layout of the possible mechanism of action of tetracylines (rectangles) against a variety of pathogenic effects concurrent with amyloiddeposition in amyloidoses (gray ellipses). The use of tetracyclines in amyloidoses therapy may affect the main pathological targets, such asaggregation and deposition of the misfolded proteins and ameliorate other pathological mechanisms associated with formation of amyloid deposits,including inflammation, ROS generation, apoptosis, and uncoupling of metal homeostasis. Tetracycline moieties known to display their therapeuticeffect on each of these pathological events are indicated in bold. The absence of side chains R3 and R6 (dashed circles, metal chelation) increasesMMPs inhibition.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXO

neurodegenerative diseases; the identification of compounds hinderingprotein misfolding.
Fabrizio Tagliavini. Since 2003, he has been the Head of theDepartment of Neurodegenerative Diseases and Director of theDivision of Neuropathology−Neurology at the Istituto “Carlo Besta”Milan, Italy. He has been working in the field of neurodegenerativedementias associated with protein misfolding, in particular Alzheimer’sdisease and prion-related encephalopathies with particular regard tothe early stages of neuropathological changes and the biologicalproperties of disease-associated proteins. His main achievements wereobtained in the following fields: the identification of new pathogenicmutations linked to degenerative dementias; the identification andcharacterization of the early stages of neuropathological changes andnew disease phenotypes; the development and characterization ofrelevant in vitro and in vivo models for pathogenesis studies; theidentification of compounds that interact with misfolded proteins.
Mario Salmona. Since 1997, he has been Head of the Department ofMolecular Biochemistry and Pharmacology at the Istituto di RicercheFarmacologiche “Mario Negri”, Milan, Italy. His research projects arefocused on the structural and functional studies of specific,pharmacologically important gene products. Potential interactionsbetween drugs and proteins were pursued at the molecular level by avariety of approaches ranging from animal studies to computersimulations. Particular attention was given to the relationship betweenprotein misfolding and neurodegeneration. His main achievementswere obtained in the following fields: identification and physicochem-ical characterization of a new pathogenic mutation in the Aβ peptide;biochemical, biophysical, and molecular modeling studies of neuro-toxic peptides; identification of tetracyclines that specifically interactwith misfolded proteins and inhibit amyloidogenesis.
■ ACKNOWLEDGMENTSThe critical reading of the manuscript by Dr. Vittorio Bertele,Dr. Barbara La Ferla, and Dr. Enrico Monzani is gratefullyacknowledged. This paper was supported by Banca IntesaSanpaolo, Grant 2012-2013, and the Italian Ministry of Health,Grant RF-2009-1473239.
■ ABBREVIATIONS USED3D-QSAR, three-dimensional quantitative structure−activityrelationship; AFM, atomic force microscopy; AIF, apoptosis-inducing factor; β2M, β2-microglobulin; CJD, Creutzfeldt−Jakob disease; CMT, chemically modified derivative oftetracycline; CryAB, αB-crystallin; DPPH, 2,2-diphenyl-1-picrylhydrazyl; FAP, familial amyloidotic polyneuropathy;FTIR, Fourier transform infrared; GSS, Gerstmann−Strauss-ler−Sheinken; HD, Huntington’s disease; hIAPP, humanamylin/islet amyloid poypeptide; IDOX, 4′-iodo-4′deoxydox-orubicin; IVIg, intravenous immunoglobulin; LC, immunoglo-bulin light chain; MPT, mitochondrial permeability transition;MTT, 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazoliumbromide; OPMD, oculopharyngeal muscular dystrophy;PABPN1, poly-(A) binding protein nuclear 1; PrP, prionprotein; SAP, serum amyloid P component; TC, tetracycline;ThT, thioflavin T; TTR, transthyretin; TUDCA, taurourso-deoxycholic acid
■ REFERENCES(1) Gillmore, J. D.; Hawkins, P. N. Drug insight: emerging therapiesfor amyloidosis. Nat. Clin. Pract. Nephrol. 2006, 2, 263−270.(2) Sipe, J. D.; Benson, M. D.; Buxbaum, J. N.; Ikeda, S.; Merlini, G.;Saraiva, M. J.; Westermark, P. Amyloid fibril protein nomenclature:
2010 recommendations from the nomenclature committee of theInternational Society of Amyloidosis. Amyloid 2010, 17, 101−104.(3) Pepys, M. B. Amyloidosis. Annu. Rev. Med. 2006, 57, 223−241.(4) Sunde, M.; Serpell, L. C.; Bartlam, M.; Fraser, P. E.; Pepys, M. B.;Blake, C. C. Common core structure of amyloid fibrils by synchrotronX-ray diffraction. J. Mol. Biol. 1997, 273, 729−739.(5) Kirschner, D. A.; Gross, A. A.; Hidalgo, M. M.; Inouye, H.;Gleason, K. A.; Abdelsayed, G. A.; Castillo, G. M.; Snow, A. D.; Pozo-Ramajo, A.; Petty, S. A.; Decatur, S. M. Fiber diffraction as a screen foramyloid inhibitors. Curr. Alzheimer Res. 2008, 5, 288−307.(6) Dobson, C. M. Protein folding and misfolding. Nature 2003, 426,884−890.(7) Hardy, J. A.; Higgins, G. A. Alzheimer’s disease: the amyloidcascade hypothesis. Science 1992, 256, 184−185.(8) Bucciantini, M.; Giannoni, E.; Chiti, F.; Baroni, F.; Formigli, L.;Zurdo, J.; Taddei, N.; Ramponi, G.; Dobson, C. M.; Stefani, M.Inherent toxicity of aggregates implies a common mechanism forprotein misfolding diseases. Nature 2002, 416, 507−511.(9) Kayed, R.; Head, E.; Thompson, J. L.; McIntire, T. M.; Milton, S.C.; Cotman, C. W.; Glabe, C. G. Common structure of solubleamyloid oligomers implies common mechanism of pathogenesis.Science 2003, 300, 486−489.(10) Glabe, C. G. Common mechanisms of amyloid oligomerpathogenesis in degenerative disease. Neurobiol. Aging 2006, 27, 570−575.(11) Ferreira, S. T.; Vieira, M. N.; De Felice, F. G. Soluble proteinoligomers as emerging toxins in Alzheimer’s and other amyloiddiseases. IUBMB Life 2007, 59, 332−345.(12) Budka, H. Neuropathology of prion diseases. Br. Med. Bull.2003, 66, 121−130.(13) Haass, C.; Selkoe, D. J. Soluble protein oligomers inneurodegeneration: lessons from the Alzheimer’s amyloid beta-peptide. Nat. Rev. Mol. Cell Biol. 2007, 8, 101−112.(14) Cooper, G. J.; Aitken, J. F.; Zhang, S. Is type 2 diabetes anamyloidosis and does it really matter (to patients)? Diabetologia 2010,53, 1011−1016.(15) Klein, W. L.; Krafft, G. A.; Finch, C. E. Targeting small Abetaoligomers: the solution to an Alzheimer’s disease conundrum? TrendsNeurosci. 2001, 2, 219−224.(16) Zhao, H. L.; Lai, F. M.; Tong, P. C.; Zhong, D. R.; Yang, D.;Tomlinson, B.; Chan, J. C. Prevalence and clinicopathologicalcharacteristics of islet amyloid in Chinese patients with type 2diabetes. Diabetes 2003, 52, 2759−2766.(17) Aitken, J. F.; Loomes, K. M.; Scott, D. W.; Reddy, S.; Phillips, A.R.; Prijic, G.; Fernando, C.; Zhang, S.; Broadhurst, R.; L’Huillier, P.;Cooper, G. J. Tetracycline treatment retards the onset and slows theprogression of diabetes in human amylin/islet amyloid polypeptidetransgenic mice. Diabetes 2010, 59, 161−171.(18) Bhak, G.; Choe, Y. J.; Paik, S. R. Mechanism of amyloidogenesis:nucleation-dependent fibrillation versus double-concerted fibrillation.BMB Rep. 2009, 42, 541−551.(19) Porter, M. Y.; Routledge, K. E.; Radford, S. E.; Hewitt, E. W.Characterization of the response of primary cells relevant to dialysis-related amyloidosis to β2-microglobulin monomer and fibrils. PLoSOne 2011, 6, e27353.(20) Stefani, M. Structural features and cytotoxicity of amyloidoligomers: implications in Alzheimer’s disease and other diseases withamyloid deposits. Prog. Neurobiol. 2012, 99, 226−245.(21) Merlini, G.; Bellotti, V. Molecular mechanisms of amyloidosis.N. Engl. J. Med. 2003, 349, 583−596.(22) Lashuel, H. A.; Hartley, D.; Petre, B. M.; Walz, T.; Lansbury, P.T., Jr. Neurodegenerative disease: amyloid pores from pathogenicmutations. Nature 2002, 418, 291.(23) Huang, X.; Atwood, C. S.; Hartshorn, M. A.; Multhaup, G.;Goldstein, L. E.; Scarpa, R. C.; Cuajungco, M. P.; Gray, D. N.; Lim, J.;Moir, R. D.; Tanzi, R. E.; Bush, A. I. The Ab peptide of Alzheimer’sdisease directly produces hydrogen peroxide through metal ionreduction. Biochemistry 1999, 38, 7609−7616.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXP
(24) Virok, D. P.; Simon, D.; Bozso, Z.; Rajko, R.; Datki, Z.; Balint,E.; Szegedi, V.; Janaky, T.; Penke, B.; Fulop, L. Protein array basedinteractome analysis of amyloid-β indicates an inhibition of proteintranslation. J. Proteome Res. 2011, 10, 1538−1547.(25) Manzoni, C.; Colombo, L.; Bigini, P.; Diana, V.; Cagnotto, A.;Messa, M.; Lupi, M.; Bonetto, V.; Pignataro, M.; Airoldi, C.; Sironi, E.;Williams, A.; Salmona, M. The molecular assembly of amyloid Aβcontrols its neurotoxicity and binding to cellular proteins. PLoS One2011, 6, e24909.(26) Aguzzi, A.; O’Connor, T. Protein aggregation diseases:pathogenicity and therapeutic perspectives. Nat. Rev. Drug Discovery2010, 9, 237−248.(27) Gertz, M. A.; Zeldenrust, S. R. Treatment of immunoglobulinlight chain amyloidosis. Curr. Hematol. Malig. Rep. 2009, 4, 91−98.(28) Suhr, O. B.; Herlenius, G.; Friman, S.; Ericzon, B. G. Livertransplantation for hereditary transthyretin amyloidosis. Liver Trans-plant. 2000, 6, 263−276.(29) Liepnieks, J. J.; Benson, M. D. Progression of cardiac amyloiddeposition in hereditary transthyretin amyloidosis patients after livertransplantation. Amyloid 2007, 14, 277−282.(30) Liepnieks, J. J.; Zhang, L. Q.; Benson, M. D. Progression oftransthyretin amyloid neuropathy after liver transplantation. Neurology2010, 75, 324−327.(31) Hamaguchi, T.; Ono, K.; Yamada, M. Anti-amyloidogenictherapies: strategies for prevention and treatment of Alzheimer’sdisease. Cell. Mol. Life Sci. 2006, 63, 1538−1552.(32) Dember, L. M.; Hawkins, P. N.; Hazenberg, B. P.; Gorevic, P.D.; Merlini, G.; Butrimiene, I.; Livneh, A.; Lesnyak, O.; Puechal, X.;Lachmann, H. J.; Obici, L.; Balshaw, R.; Garceau, D.; Hauck, W.;Skinner, M. Eprodisate for the treatment of renal disease in AAamyloidosis. N. Engl. J. Med. 2007, 356, 2349−2360.(33) Galimberti, D.; Scarpini, E. Disease-modifying treatments forAlzheimer’s disease. Ther. Adv. Neurol. Disord. 2011, 4, 203−216.(34) Soto, C.; Kascsak, R. J.; Saborío, G. P.; Aucouturier, P.;Wisniewski, T.; Prelli, F.; Kascsak, R.; Mendez, E.; Harris, D. A.;Ironside, J.; Tagliavini, F.; Carp, R. I.; Frangione, B. Reversion of prionprotein conformational changes by synthetic beta-sheet breakerpeptides. Lancet 2000, 355, 192−197.(35) Ratner, M. Spotlight focuses on protein-misfolding therapies.Nat. Biotechnol. 2009, 27, 874.(36) Plante-Bordeneuve, V.; Said, G. Familial amyloid polyneurop-athy. Lancet Neurol. 2011, 10, 1086−1097.(37) Weiner, H. L.; Lemere, C. A.; Maron, R.; Spooner, E. T.;Grenfell, T. J.; Mori, C.; Issazadeh, S.; Hancock, W. W.; Selkoe, D. J.Nasal administration of amyloid-beta peptide decreases cerebralamyloid burden in a mouse model of Alzheimer’s disease. Ann.Neurol. 2000, 48, 567−579.(38) Birmingham, K.; Frantz, S. Set back to Alzheimer vaccinestudies. Nat. Med. 2002, 8, 199−200.(39) Mullard, A. Sting of Alzheimer’s failures offset by upcomingprevention trials. Nat. Rev. Drug Discovery 2012, 11, 657−660.(40) Bodin, K.; Ellmerich, S.; Kahan, M. C.; Tennent, G. A.; Loesch,A.; Gilbertson, J. A.; Hutchinson, W. L.; Mangione, P. P.; Gallimo, J.R.; Millar, D. J.; Minogue, S.; Dhillon, A. P.; Taylor, G. W.; Bradwell,A. R.; Petrie, A.; Gillmore, J. D.; Bellotti, V.; Botto, M.; Hawkins, P.N.; Pepys, M. B. Antibodies to human serum amyloid P componenteliminate visceral amyloid deposits. Nature 2010, 468, 93−97.(41) Tagliavini, F.; Forloni, G.; Colombo, L.; Rossi, G.; Girola, L.;Canciani, B.; Angeretti, N.; Giampaolo, L.; Peressini, E.; Awan, T.; DeGioia, L.; Ragg, E.; Bugiani, O.; Salmona, M. Tetracycline affectsabnormal properties of synthetic PrP peptides and PrP(Sc) in vitro. J.Mol. Biol. 2000, 300, 1309−1322.(42) Forloni, G.; Colombo, L.; Girola, L.; Tagliavini, F.; Salmona, M.Anti-amyloidogenic activity of tetracyclines: studies in vitro. FEBS Lett.2001, 487, 404−407.(43) Forloni, G.; Salmona, M.; Marcon, G.; Tagliavini, F.Tetracyclines and prion infectivity. Infect. Disord.: Drug Targets 2009,9, 23−30.
(44) Airoldi, C.; Colombo, L.; Manzoni, C.; Sironi, E.; Natalello, A.;Doglia, S. M.; Forloni, G.; Tagliavini, F.; Del Favero, E.; Cantu, L.;Nicotra, F.; Salmona, M. Tetracycline prevents Aβ oligomer toxicitythrough an atypical supramolecular interaction. Org. Biomol. Chem.2011, 9, 463−472.(45) Saivin, S.; Houin, G. Clinical pharmacokinetics of doxycyclineand minocycline. Clin. Pharmacokinet. 1988, 15, 355−366.(46) Griffin, M. O.; Fricovsky, E.; Ceballos, G.; Villarreal, F.Tetracyclines: a pleiotropic family of compounds with promisingtherapeutic properties. Review of the literature. Am. J. Physiol.: CellPhysiol. 2010, 299, C539−C548.(47) Chopra, I.; Roberts, M. Tetracycline antibiotics: mode of action,applications, molecular biology, and epidemiology of bacterialresistance. Microbiol. Mol. Biol. Rev. 2001, 65, 232−260.(48) Nelson, M. L. Chemical and biological dynamics of tetracyclines.Adv. Dent. Res. 1998, 12, 5−11.(49) Kraus, R. L.; Pasieczny, R.; Lariosa-Willingham, K.; Turner, M.S.; Jiang, A.; Trauger, J. W. Antioxidant properties of minocycline:neuroprotection in an oxidative stress assay and direct radical-scavenging activity. J. Neurochem. 2005, 94, 819−827.(50) Cosentino, U.; Varí, M. R.; Saracino, A. A.; Pitea, D.; Moro, G.;Salmona, M. Tetracycline and its analogues as inhibitors of amyloidfibrils: searching for a geometrical pharmacophore by theoreticalinvestigation of their conformational behavior in aqueous solution. J.Mol. Model. 2005, 11, 17−25.(51) Duarte, H. A.; Carvalho, S.; Paniago, E. B.; Simas, A. M.Importance of tautomers in the chemical behavior of tetracyclines. J.Pharm. Sci. 1999, 88, 111−120.(52) Hughes, L. J.; Stezowski, J. J.; Hughes, R. E. Chemical−structural properties of tetracycline derivatives. 7. Evidence forcoexistence of the zwitterionic and nonionized forms of the freebase in solution. J. Am. Chem. Soc. 1979, 101, 7655−7657.(53) Sapadin, A. N.; Fleischmajer, R. Tetracyclines: nonantibioticproperties and their clinical implications. J. Am. Acad. Dermatol. 2006,54, 258−265.(54) Jin, L.; Amaya-Mazo, X.; Apel, M. E.; Sankisa, S. S.; Johnson, E.;Zbyszynska, M. A.; Han, A. Ca2+ and Mg2+ bind tetracycline withdistinct stoichiometries and linked deprotonation. Biophys. Chem.2007, 128, 185−196.(55) Neuvonen, P. J. Interactions with the absorption of tetracyclines.Drugs 1976, 11, 45−54.(56) Weinstein, L. The Tetracyclines. In The Pharmacological Basis ofTherapeutics, 4th ed.; Goodman, L. S., Gilman, A., Eds.; TheMacmillan Co.: New York, 1970; pp 1253−1268.(57) Canalis, R. F.; Lechago, J. Tetracycline bone labeling: animproved technique using incident fluorescence. Ann. Otol., Rhinol.,Laryngol. 1982, 91, 160−162.(58) Melsen, F.; Mosekilde, L. Trabecular bone mineralization lagtime determined by tetracycline double-labeling in normal and certainpathological conditions. Acta Pathol. Microbiol. Scand., Sect. A 1980, 88,83−88.(59) Mellibovsky, L.; Diez, A.; Serrano, S.; Aubia, J.; Perez-Vila, E.;Marinoso, M. L.; Nogues, X.; Recker, R. R. Bone remodelingalterations in myelodysplastic syndrome. Bone 1996, 19, 401−405.(60) Ayala, A. G.; Murray, J. A.; Erling, M. A.; Raymond, A. K.Osteoid-osteoma: intraoperative tetracicline-fluorescence demonstra-tion of the nidus. J. Bone Jt. Surg., Am. Vol. 1986, 68, 747−751.(61) Brodersen, D. E.; Clemons, W. M., Jr.; Carter, A. P.; Morgan-Warren, R. J.; Wimberly, B. T.; Ramakrishnan, V. The structural basisfor the action of the antibiotics tetracycline, pactamycin, andhygromycin B on the 30S ribosomal subunit. Cell 2000, 103, 1143−1154.(62) Gianni, L.; Bellotti, V.; Gianni, A. M.; Merlini, G. New drugtherapy of amyloidoses: resorption of AL-type deposits with 4′-iodo-4′-deoxydoxorubicin. Blood 1995, 86, 855−861.(63) Merlini, G.; Ascari, E.; Amboldi, N.; Bellotti, V.; Arbustini, E.;Perfetti, V.; Ferrari, M.; Zorzoli, I.; Marinone, M. G.; Garini, P.;Diegoli, M.; Trizio, D.; Ballinari, D. Interaction of the anthracycline 4′-
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXQ
iodo-4′-deoxydoxorubicin with amyloid fibrils: inhibition of amyloido-genesis. Proc. Natl. Acad. Sci. U.S.A. 1995, 92, 2959−2963.(64) Tagliavini, F.; McArthur, R. A.; Canciani, B.; Giaccone, G.;Porro, M.; Bugiani, M.; Lievens, P. M.; Bugiani, O.; Peri, E.; Dall’Ara,P.; Rocchi, M.; Poli, G.; Forloni, G.; Bandiera, T.; Varasi, M.; Suarato,A.; Cassutti, P.; Cervini, M. A.; Lansen, J.; Salmona, M.; Post, C.Effectiveness of anthracycline against experimental prion disease inSyrian hamsters. Science 1997, 276, 1119−1122.(65) Palha, J. A.; Ballinari, D.; Amboldi, N.; Cardoso, I.; Fernandes,R.; Bellotti, V.; Merlini, G.; Saraiva, M. J. 4′-Iodo-4′-deoxydoxorubicindisrupts the fibrillar structure of transthyretin amyloid. Am. J. Pathol.2000, 156, 1919−1925.(66) Forloni, G.; Iussich, S.; Awan, T.; Colombo, L.; Angeretti, N.;Girola, L.; Bertani, I.; Poli, G.; Caramelli, M.; Grazia Bruzzone, M.;Farina, L.; Limido, L.; Rossi, G.; Giaccone, G.; Ironside, J. W.; Bugiani,O.; Salmona, M.; Tagliavini, F. Tetracyclines affect prion infectivity.Proc. Natl. Acad. Sci. U.S.A. 2002, 99, 10849−10854.(67) Forloni, G.; Angeretti, N.; Chiesa, R.; Monzani, E.; Salmona, M.;Bugiani, O.; Tagliavini, F. Neurotoxicity of a prion protein fragment.Nature 1993, 362, 543−546.(68) Fioriti, L.; Angeretti, N.; Colombo, L.; De Luigi, A.; Colombo,A.; Manzoni, C.; Morbin, M.; Tagliavini, F.; Salmona, M.; Chiesa, R.;Forloni, G. Neurotoxic and gliotrophic activity of a synthetic peptidehomologous to Gerstmann−Straussler−Scheinker disease amyloidprotein. J. Neurosci. 2007, 27, 1576−1583.(69) Ronga, L.; Langella, E.; Palladino, P.; Marasco, D.; Tizzano, B.;Saviano, M.; Pedone, C.; Improta, R.; Ruvo, M. Does tetracycline bindhelix 2 of prion? An integrated spectroscopical and computationalstudy of the interaction between the antibiotic and alpha helix 2human prion protein fragments. Proteins 2007, 66, 707−715.(70) Georgieva, D.; Schwark, D.; von Bergen, M.; Redecke, L.;Genov, N.; Betzel, C. Interactions of recombinant prions withcompounds of therapeutical significance. Biochem. Biophys. Res.Commun. 2006, 344, 463−470.(71) De Luigi, A.; Colombo, L.; Diomede, L.; Capobianco, R.;Mangieri, M.; Miccolo, C.; Limido, L.; Forloni, G.; Tagliavini, F.;Salmona, M. The efficacy of tetracyclines in peripheral andintracerebral prion infection. PLoS One 2008, 3, e1888.(72) Diomede, L.; Cassata, G.; Fiordaliso, F.; Salio, M.; Ami, D.;Natalello, A.; Doglia, S. M.; De Luigi, A.; Salmona, M. Tetracyclineand its analogues protect Caenorhabditis elegans from β amyloid-induced toxicity by targeting oligomers. Neurobiol. Dis. 2010, 40, 424−431.(73) Loeb, M. B.; Molloy, D. W.; Smieja, M.; Standish, T.;Goldsmith, C. H.; Mahony, J.; Smith, S.; Borrie, M.; Decoteau, E.;Davidson, W.; McDougall, A.; Gnarpe, J.; O’Donnell, M.; Chernesky,M. A randomized, controlled trial of doxycycline and rifampin forpatients with Alzheimer’s disease. J. Am. Geriatr. Soc. 2004, 52, 381−387.(74) Molloy, D. W.; Standish, T. I.; Zhou, Q.; Guyatt, G.; TheDARAD Study Group.. A multicenter, blinded, randomized, factorialcontrolled trial of doxycycline and rifampin for treatment ofAlzheimer’s disease: the DARAD trial. Int. J. Geriatr. Psychiatry 2013,28, 463−470.(75) Aitken, J. F.; Loomes, K. M.; Konarkowska, B.; Cooper, G. J.Suppression by polycyclic compounds of the conversion of humanamylin into insoluble amyloid. Biochem. J. 2003, 374, 779−784.(76) Malmo, C.; Vilasi, S.; Iannuzzi, C.; Tacchi, S.; Cametti, C.; Irace,G.; Sirangelo, I. Tetracycline inhibits W7FW14F apomyoglobin fibrilextension and keeps the amyloid protein in a pre-fibrillar, highlycytotoxic state. FASEB J. 2006, 20, 346−347.(77) Cardoso, I.; Merlini, G.; Saraiva, M. J. 4′-Iodo-4′-deoxydoxor-ubicin and tetracyclines disrupt transthyretin amyloid fibrils in vitroproducing noncytotoxic species: screening for TTR fibril disrupters.FASEB J. 2003, 17, 803−809.(78) Cardoso, I.; Saraiva, M. J. Doxycycline disrupts transthyretinamyloid: evidence from studies in a FAP transgenic mice model.FASEB J. 2006, 20, 234−239.
(79) Cardoso, I.; Martins, D.; Ribeiro, T.; Merlini, G.; Saraiva, M. J.Synergy of combined doxycycline/TUDCA treatment in loweringtransthyretin deposition and associated biomarkers: studies in FAPmouse models. J. Transl. Med. 2010, 8, 74.(80) Obici, L.; Cortese, A.; Lozza, A.; Lucchetti, J.; Gobbi, M.;Palladini, G.; Perlini, S.; Saraiva, M. J.; Merlini, G. Doxycycline plustauroursodeoxycholic acid for transthyretin amyloidosis: a phase IIstudy. Amyloid 2012, 19, 34−36.(81) Ono, K.; Yamada, M. Antioxidant compounds have potent anti-fibrillogenic and fibril-destabilizing effects for α-synuclein fibrils invitro. J. Neurochem. 2006, 97, 105−115.(82) Du, Y.; Ma, Z.; Lin, S.; Dodel, R. C.; Gao, F.; Bales, K. R.;Triarhou, L. C.; Chernet, E.; Perry, K. W.; Nelson, D. L.; Luecke, S.;Phebus, L. A.; Bymaster, F. P.; Paul, S. M. Minocycline preventsnigrostriatal dopaminergic neurodegeneration in the MPTP model ofParkinson’s disease. Proc. Natl. Acad. Sci. U.S.A. 2001, 98, 14669−14674.(83) NINDS NET-PD Investigators.. A pilot clinical trial of creatineand minocycline in early Parkinson disease: 18-month results. Clin.Neuropharmacol. 2008, 31, 141−150.(84) Chen, M.; Ona, V. O.; Li, M.; Ferrante, R. J.; Fink, K. B.; Zhu,S.; Bian, J.; Guo, L.; Farrell, L. A.; Hersch, S. M.; Hobbs, W.;Vonsattel, J. P.; Cha, J. H.; Friedlander, R. M. Minocycline inhibitscaspase-1 and caspase-3 expression and delays mortality in a transgenicmouse model of Huntington disease. Nat. Med. 2000, 6, 797−801.(85) Smith, D. L.; Woodman, B.; Mahal, A.; Sathasivam, K.; Ghazi-Noori, S.; Lowden, P. A.; Bates, G. P.; Hockly, E. Minocycline anddoxycycline are not beneficial in a model of Huntington’s disease. Ann.Neurol. 2003, 54, 186−196.(86) Mievis, S.; Levivier, M.; Communi, D.; Vassart, G.; Brotchi, J.;Ledent, C.; Blum, D. Lack of minocycline efficiency in genetic modelsof Huntington’s disease. Neuromol. Med. 2007, 9, 47−54.(87) Huntington Study Group DOMINO Investigators.. A futilitystudy of minocycline in Huntington’s disease. Mov. Disord. 2010, 25,2219−2224.(88) Davies, J. E.; Wang, L.; Garcia-Oroz, L.; Cook, L. J.; Vacher, C.;O’Donovan, D. G.; Rubinsztein, D. C. Doxycycline attenuates anddelays toxicity of the oculopharyngeal muscular dystrophy mutation intransgenic mice. Nat. Med. 2005, 11, 672−677.(89) Ward, J. E.; Ren, R.; Toraldo, G.; Soohoo, P.; Guan, J.; O’Hara,C.; Jasuja, R.; Trinkaus-Randall, V.; Liao, R.; Connors, L. H.; Seldin,D. C. Doxycycline reduces fibril formation in a transgenic mousemodel of AL amyloidosis. Blood 2011, 118, 6610−6617.(90) Zheng, H.; Tang, M.; Zheng, Q.; Kumarapeli, A. R.; Horak, K.M.; Tian, Z.; Wang, X. Doxycycline attenuates protein aggregation incardiomyocytes and improves survival of a mouse model of cardiacproteinopathy. J. Am. Coll. Cardiol. 2010, 56, 1418−1426.(91) Giorgetti, S.; Raimondi, S.; Pagano, K.; Relini, A.; Bucciantini,M.; Corazza, A.; Fogolari, F.; Codutti, L.; Salmona, M.; Mangione, P.;Colombo, L.; De Luigi, A.; Porcari, R.; Gliozzi, A.; Stefani, M.;Esposito, G.; Bellotti, V.; Stoppini, M. Effect of tetracyclines on thedynamics of formation and destructuration of β2-microglobulinamyloid fibrils. J. Biol. Chem. 2011, 286, 2121−2131.(92) Cosentino, U.; Pitea, D.; Moro, G.; Saracino, G. A.; Caria, P.;Varì, R. M.; Colombo, L.; Forloni, G.; Tagliavini, F.; Salmona, M. Theanti-fibrillogenic activity of tetracyclines on PrP 106−126: a 3D-QSARstudy. J. Mol. Model. 2008, 14, 987−994.(93) Howlett, D. R.; George, A. R.; Owen, D. E.; Ward, R. V.;Markwell, R. E. Common structural features determine theeffectiveness of carvedilol, daunomycin and rolitetracycline asinhibitors of Alzheimer β-amyloid fibril formation. Biochem. J. 1999,343, 419−423.(94) Inbar, P.; Bautista, M. R.; Takayama, S. A.; Yang, J. Assay toscreen for molecules that associate with Alzheimer’s related β-amyloidfibrils. Anal. Chem. 2008, 80, 3502−3506.(95) Zovo, K.; Helk, E.; Karafin, A.; Tougu, V.; Palumaa, P. Label-free high-throughput screening assay for inhibitors of Alzheimer’samyloid-β peptide aggregation based on MALDI MS. Anal. Chem.2010, 82, 8558−8565.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXR
(96) Galimberti, D.; Fenoglio, C.; Scarpini, E. Inflammation inneurodegenerative disorders: friend or foe? Curr. Aging Sci. 2008, 1,30−41.(97) Ferreiro, E.; Baldeiras, I.; Ferreira, I. L.; Costa, R. O.; Rego, A.C.; Pereira, C. F.; Oliveira, C. R. Mitochondrial- and endoplasmicreticulum-associated oxidative stress in Alzheimer’s disease: frompathogenesis to biomarkers. Int. J. Cell Biol. 2012, 2012, 735206.(98) Bolognin, S.; Messori, L.; Zatta, P. Metal ion physiopathology inneurodegenerative disorders. Neuromol. Med. 2009, 11, 223−238.(99) Lim, Y. A.; Rhein, V.; Baysang, G.; Meier, F.; Poljak, A.; Raftery,M. J.; Guilhaus, M.; Ittner, L. M.; Eckert, A.; Gotz, J. Ab and humanamylin share a common toxicity pathway via mitochondrialdysfunction. Proteomics 2010, 10, 1621−1633.(100) Noble, W.; Garwood, C. J.; Hanger, D. P. Minocycline as apotential therapeutic agent in neurodegenerative disorders charac-terised by protein misfolding. Prion 2009, 3, 78−83.(101) Gialeli, C.; Theocharis, A. D.; Karamanos, N. K. Roles ofmatrix metalloproteinases in cancer progression and their pharmaco-logical targeting. FEBS J. 2011, 278, 16−27.(102) Manicone, A. M.; McGuire, J. K. Matrix metalloproteinases asmodulators of inflammation. Semin. Cell Dev. Biol. 2008, 19, 34−41.(103) Nagase, H.; Visse, R.; Murphy, G. Structure and function ofmatrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562−573.(104) Naganuma, T.; Sugimura, K.; Uchida, J.; Tashiro, K.;Yoshimura, R.; Takemoto, Y.; Nakatani, T. Increased levels of serummatrix metalloproteinase-3 in haemodialysis patients with dialysis-related amyloidosis. Nephrology (Carlton) 2008, 13, 104−108.(105) Sousa, M. M.; do Amaral, J. B.; Guimaraes, A.; Saraiva, M. J.Up-regulation of the extracellular matrix remodeling genes, biglycan,neutrophil gelatinase-associated lipocalin, and matrix metalloprotei-nase-9 in familial amyloid polyneuropathy. FASEB J. 2005, 19, 124−126.(106) Biolo, A.; Ramamurthy, S.; Connors, L. H.; O’Hara, C. J.;Meier-Ewert, H. K.; Soo Hoo, P. T.; Sawyer, D. B.; Seldin, D. C.; Sam,F. Matrix metalloproteinases and their tissue inhibitors in cardiacamyloidosis: relationship to structural, functional myocardial changesand to light chain amyloid deposition. Circ.: Heart Failure 2008, 1,249−257.(107) Rosenberg, G. A. Matrix metalloproteinases and their multipleroles in neurodegenerative diseases. Lancet Neurol. 2009, 8, 205−216.(108) Kim, E. M.; Hwang, O. Role of matrix metalloproteinase-3 inneurodegeneration. J. Neurochem. 2011, 116, 22−32.(109) Yan, P.; Hu, X.; Song, H.; Yin, K.; Bateman, R. J.; Cirrito, J. R.;Xiao, Q.; Hsu, F. F.; Turk, J. W.; Xu, J.; Hsu, C. Y.; Holtzman, D. M.;Lee, J. M. Matrix metalloproteinase-9 degrades amyloid-β fibrils invitro and compact plaques in situ. J. Biol. Chem. 2006, 281, 24566−24574.(110) Choi, D. H.; Kim, E. M.; Son, H. J.; Joh, T. H.; Kim, Y. S.; Kim,D.; Flint Beal, M.; Hwang, O. A novel intracellular role of matrixmetalloproteinase-3 during apoptosis of dopaminergic cells. J.Neurochem. 2008, 106, 405−415.(111) Golub, L. M.; Lee, H. M.; Lehrer, G.; Nemiroff, A.; McNamara,T. F.; Kaplan, R.; Ramamurthy, N. S. Minocycline reduces gingivalcollagenolytic activity during diabetes. Preliminary observations and aproposed new mechanism of action. J. Periodontal Res. 1983, 18, 516−526.(112) Greenwald, R. A.; Golub, L. M.; Lavietes, B.; Ramamurthy, N.S.; Gruber, B.; Laskin, R. S.; McNamara, T. F. Tetracyclines inhibithuman synovial collagenase in vivo and in vitro. J. Rheumatol. 1987, 14,28−32.(113) Golub, L. M.; Evans, R. T.; McNamara, T. F.; Lee, H. M.;Ramamurthy, N. S. A non-antimicrobial tetracycline inhibits gingivalmatrix metalloproteinases and bone loss in Porphyromonas gingivalis-induced periodontitis in rats. Ann. N.Y. Acad. Sci. 1994, 732, 96−111.(114) Ryan, M. E.; Usman, A.; Ramamurthy, N. S.; Golub, L. M.;Greenwald, R. A. Excessive matrix metalloproteinase activity indiabetes: inhibition by tetracycline analogues with zinc reactivity.Curr. Med. Chem. 2001, 8, 305−316.
(115) Seftor, R. E.; Seftor, E. A.; De Larco, J. E.; Kleiner, D. E.;Leferson, J.; Stetler-Stevenson, W. G.; McNamara, T. F.; Golub, L. M.;Hendrix, M. J. Chemically modified tetracyclines inhibit humanmelanoma cell invasion and metastasis. Clin. Exp. Metastasis 1998, 16,217−225.(116) Garcia, R. A.; Pantazatos, D. P.; Gessner, C. R.; Go, K. V.;Woods, V. L., Jr.; Villarreal, F. J. Molecular interactions betweenmatrilysin and the matrix metalloproteinase inhibitor doxycyclineinvestigated by deuterium exchange mass spectrometry. Mol.Pharmacol. 2005, 67, 1128−1136.(117) Smith, G. N., Jr.; Mickler, E. A.; Hasty, K. A.; Brandt, K. D.Specificity of inhibition of matrix metalloproteinase activity bydoxycycline: relationship to structure of the enzyme. Arthritis Rheum.1999, 42, 1140−1146.(118) Golub, L. M. Introduction and background. Pharmacol. Res.2011, 63, 99−101.(119) Greenwald, R. A. The road forward: the scientific basis fortetracycline treatment of arthritic disorders. Pharmacol. Res. 2011, 64,610−613.(120) Fang, J.; Seki, T.; Maeda, H. Therapeutic strategies bymodulating oxygen stress in cancer and inflammation. Adv. DrugDelivery Rev. 2009, 61, 290−302.(121) Schildknecht, S.; Pape, R.; Muller, N.; Robotta, M.; Marquardt,A.; Burkle, A.; Drescher, M.; Leist, M. Neuroprotection byminocycline caused by direct and specific scavenging of peroxynitrite.J. Biol. Chem. 2011, 286, 4991−5002.(122) Kummer, M. P.; Hermes, M.; Delekarte, A.; Hammerschmidt,T.; Kumar, S.; Terwel, D.; Walter, J.; Pape, H. C.; Konig, S.; Roeber,S.; Jessen, F.; Klockgether, T.; Korte, M.; Heneka, M. T. Nitration oftyrosine 10 critically enhances amyloid beta aggregation and plaqueformation. Neuron 2011, 71, 833−844.(123) Sousa, M. M.; Du Yan, S.; Fernandes, R.; Guimaraes, A.; Stern,D.; Saraiva, M. J. Familial amyloid polyneuropathy: receptor foradvanced glycation end products-dependent triggering of neuronalinflammatory and apoptotic pathways. J. Neurosci. 2001, 21, 7576−7586.(124) Manczak, M.; Park, B. S.; Jung, Y.; Reddy, P. H. Differentialexpression of oxidative phosphorylation genes in patients withAlzheimer’s disease: implications for early mitochondrial dysfunctionand oxidative damage. Neuromol. Med. 2004, 5, 147−162.(125) Miyachi, Y.; Yoshioka, A.; Imamura, S.; Niwa, Y. Effect ofantibiotics on the generation of reactive oxygen species. J. Invest.Dermatol. 1986, 86, 449−453.(126) Akamatsu, H.; Asada, M.; Komura, J.; Asada, Y.; Niwa, Y. Effectof doxycycline on the generation of reactive oxygen species: a possiblemechanism of action of acne therapy with doxycycline. Acta Derm.-Venereol. 1992, 72, 178−179.(127) Romero-Perez, D.; Fricovsky, E.; Yamasaki, K. G.; Griffin, M.;Barraza-Hidalgo, M.; Dillmann, W.; Villarreal, F. Cardiac uptake ofminocycline and mechanisms for in vivo cardioprotection. J. Am. Coll.Cardiol. 2008, 52, 1086−1094.(128) Zeydanli, E. N.; Kandilci, H. B.; Turan, B. Doxycyclineameliorates vascular endothelial and contractile dysfunction in thethoracic aorta of diabetic rats. Cardiovasc. Toxicol. 2011, 11, 134−147.(129) Lai, H. C.; Yeh, Y. C.; Ting, C. T.; Lee, W. L.; Lee, H. W.;Wang, L. C.; Wang, K. Y.; Lai, H. C.; Wu, A.; Liu, T. J. Doxycyclinesuppresses doxorubicin-induced oxidative stress and cellular apoptosisin mouse hearts. Eur. J. Pharmacol. 2010, 644, 176−187.(130) Hoyt, J. C.; Ballering, J.; Numanami, H.; Hayden, J. M.;Robbins, R. A. Doxycycline modulates nitric oxide production inmurine lung epithelial cells. J. Immunol. 2006, 176, 567−572.(131) Huang, T. Y.; Chu, H. C.; Lin, Y. L.; Lin, C. K.; Hsieh, T. Y.;Chang, W. K.; Chao, Y. C.; Liao, C. L. Minocycline attenuatesexperimental colitis in mice by blocking expression of inducible nitricoxide synthase and matrix metalloproteinases. Toxicol. Appl.Pharmacol. 2009, 237, 69−82.(132) Amin, A. R.; Attur, M. G.; Thakker, G. D.; Patel, P. D.; Vyas, P.R.; Patel, R. N.; Patel, I. R.; Abramson, S. B. A novel mechanism of
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXS

action of tetracyclines: effects on nitric oxide synthases. Proc. Natl.Acad. Sci. U.S.A. 1996, 93, 14014−14019.(133) Milano, S.; Arcoleo, F.; D’Agostino, P.; Cillari, E. Intra-peritoneal injection of tetracyclines protects mice from lethalendotoxemia downregulating inducible nitric oxide synthase in variousorgans and cytokine and nitrate secretion in blood. Antimicrob. AgentsChemother. 1997, 41, 117−121.(134) Krakauer, T.; Buckley, M. Doxycycline is anti-inflammatoryand inhibits staphylococcal exotoxin-induced cytokines and chemo-kines. Antimicrob. Agents Chemother. 2003, 47, 3630−3633.(135) Lau, A. C.; Duong, T. T.; Ito, S.; Wilson, G. J.; Yeung, R. S.Inhibition of matrix metalloproteinase-9 activity improves coronaryoutcome in an animal model of Kawasaki disease. Clin. Exp. Immunol.2009, 157, 300−309.(136) Prall, A. K.; Longo, G. M.; Mayhan, W. G.; Waltke, E. A.;Fleckten, B.; Thompson, R. W.; Baxter, B. T. Doxycycline in patientswith abdominal aortic aneurysms and in mice: comparison of serumlevels and effect on aneurysm growth in mice. J. Vasc. Surg. 2002, 35,923−929.(137) Lindeman, J. H.; Abdul-Hussien, H.; van Bockel, J. H.;Wolterbeek, R.; Kleemann, R. Clinical trial of doxycycline for matrixmetalloproteinase-9 inhibition in patients with an abdominalaneurysm: doxycycline selectively depletes aortic wall neutrophilsand cytotoxic T cells. Circulation 2009, 119, 2209−2216.(138) Miyazaki, E.; Ando, M.; Fukami, T.; Nureki, S.; Eishi, Y.;Kumamoto, T. Minocycline for the treatment of sarcoidosis: Is themechanism of action immunomodulating or antimicrobial effect? Clin.Rheumatol. 2008, 27, 1195−1197.(139) Del Rosso, J. Q.; Webster, G. F.; Jackson, M.; Rendon, M.;Rich, P.; Torok, H.; Bradshaw, M. Two randomized phase III clinicaltrials evaluating anti-inflammatory dose doxycycline (40-mg doxycy-cline, USP capsules) administered once daily for treatment of rosacea.J. Am. Acad. Dermatol. 2007, 56, 791−802.(140) Golub, L. M.; McNamara, T. F.; Ryan, M. E.; Kohut, B.;Blieden, T.; Payonk, G.; Sipos, T.; Baron, H. J. Adjunctive treatmentwith subantimicrobial doses of doxycycline: effects on gingival fluidcollagenase activity and attachment loss in adult periodontitis. J. Clin.Periodontol. 2001, 28, 146−156.(141) Sagar, J.; Sales, K.; Seifalian, A.; Winslet, M. Doxycycline inmitochondrial mediated pathway of apoptosis: a systematic review.Anti-Cancer Agents Med. Chem. 2010, 10, 556−563.(142) Wang, X.; Zhu, S.; Drozda, M.; Zhang, W.; Stavrovskaya, I. G.;Cattaneo, E.; Ferrante, R. J.; Kristal, B. S.; Friedlander, R. M.Minocycline inhibits caspase-independent and -dependent mitochon-drial cell death pathways in models of Huntington’s disease. Proc. Natl.Acad. Sci. U.S.A. 2003, 100, 10483−10487.(143) Antonenko, Y. N.; Rokitskaya, T. I.; Cooper, A. J.; Krasnikov,B. F. Minocycline chelates Ca2+, binds to membranes, and depolarizesmitochondria by formation of Ca2+-dependent ion channels. J.Bioenerg. Biomembr. 2010, 42, 151−163.(144) Du Buy, H. G.; Showacre, J. L. Selective localization oftetracycline in mitochondria of living cells. Science 1961, 133, 196−197.(145) Riesbeck, K.; Bredberg, A.; Forsgren, A. Ciprofloxacin does notinhibit mitochondrial functions but other antibiotics do. Antimicrob.Agents Chemother. 1990, 34, 167−169.(146) Nadanaciva, S.; Dillman, K.; Gebhard, D. F.; Shrikhande, A.;Will, Y. High-content screening for compounds that affect mtDNA-encoded protein levels in eukaryotic cells. J. Biomol. Screening 2010, 15,937−948.(147) Van der Bogert, C.; Melis, T. E.; Kroon, A. M. Mitochondrialbiogenesis during the activation of lymphocytes by mitogens: theimmunosuppressive action of tetracyclines. J. Leukocyte Biol. 1989, 46,128−133.(148) Shieh, J. M.; Huang, T. F.; Hung, C. F.; Chou, K. H.; Tsai, Y.J.; Wu, W. B. Activation of c-Jun N-terminal kinase is essential formitochondrial membrane potential change and apoptosis induced bydoxycycline in melanoma cells. Br. J. Pharmacol. 2010, 160, 1171−1184.
(149) Brown, T. M.; Clark, H. W.; Bailey, J. S.; Gray, C. W.Relationship between mycoplasma antibodies and rheumatoid factors.Arthritis Rheum. 1970, 13, 309−310.(150) Paulus, H. E. Minocycline treatment of rheumatoid arthritis.Ann. Intern. Med. 1995, 122, 147−148.(151) Ossola, B.; Lantto, T. A.; Puttonen, K. A.; Tuominen, R. K.;Raasmaja, A.; Mannisto, P. T. Minocycline protects SH-SY5Y cellsfrom 6-hydroxydopamine by inhibiting both caspase-dependent and-independent programmed cell death. J. Neurosci. Res. 2012, 90, 682−690.(152) Yong, V. W.; Wells, J.; Giuliani, F.; Casha, S.; Power, C.; Metz,L. M. The promise of minocycline in neurology. Lancet Neurol. 2004,3, 744−751.
Journal of Medicinal Chemistry Perspective
dx.doi.org/10.1021/jm400161p | J. Med. Chem. XXXX, XXX, XXX−XXXT
Related Documents