Focus on the Patient Experience. This month the Unit Council News is pleased to bring you a special issue on the Patient Ex‐ perience in healthcare. From first hand coverage of a landmark conference in Cleveland Ohio, to the expose’ on the new drugs that are hitting the market. This month the focus is on the experience of a person and how that experience impacts the individual , family, the commu‐ nity, and the world. Our experiences shape our futures and define our pasts. And so our charge, from the Caritas theory of Dr. Jean Watson, to the practicality of the Recov‐ ery movement; is to help the veterans experience the breath and width of life. And it is your responsibility as caring staff and partners in wellness to talk to talk of recovery, to walk the walk of recovery, and to help the people that come to our ward experience the life fulfilling promise of recovery and not the stigma of “mental Illness”. The recovery model takes us beyond just “managing” an illness. It brings us face to face with the experience of wellness. Welcome to the new face of the patient experience. Welcome to Unit Council News. this issue Letter from the Editor P.2 Employee of the Issue P.3 MedWatch : Special Focus P.6 Calling Volunteers P.19 Find out what our reporter had to say about what is in your local head‐ shop...the find‐ ings may sur‐ prise you. Page 11 in MedWatch K2: Incense, Legal Pot, or a Reason for Psychosis 6A Unit Council News Michael E DeBakey Veterans Administration Volume 3 July/August 2010 Does Marijuana with‐ drawal syndrome exist?

6A Unit Council News
Mar 25, 2016
About Patient Experience, focus on drugs and abuse/dependance
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Focus on the Patient Experience.
This month the Unit Council News is pleased to bring you a special issue on the Patient Ex‐
perience in healthcare. From first hand coverage of a landmark conference in Cleveland Ohio,
to the expose’ on the new drugs that are hitting the market. This month the focus is on the
experience of a person and how that experience impacts the individual , family, the commu‐
nity, and the world.
Our experiences shape our futures and define our pasts.
And so our charge, from the Caritas theory of Dr. Jean Watson, to the practicality of the Recov‐
ery movement; is to help the veterans experience the breath and width of life.
And it is your responsibility as caring staff and partners in wellness to talk to talk of recovery,
to walk the walk of recovery, and to help the people that come to our ward experience the life
fulfilling promise of recovery and not the stigma of “mental Illness”. The recovery model takes
us beyond just “managing” an illness. It brings us face to face with the experience of wellness.
Welcome to the new face of the patient experience. Welcome to Unit Council News.
this issue
Letter from the Editor P.2 Employee of the Issue P.3
MedWatch : Special Focus P.6 Calling Volunteers P.19
Find out what
our reporter had
to say about
what is in your
local head‐
shop...the find‐
ings may sur‐
prise you.
Page 11 in
MedWatch
K2: Incense, Legal Pot, or a Reason for Psychosis
6A Unit Council News Michael E DeBakey Veterans Administration
Volume 3 July/August 2010
Does Marijuana with‐
drawal syndrome exist?

2
Conference Coverage at the Cleveland Clinic
6A Unit Council News (UCN) is pro‐
duced as part of the Unit Council on
unit 6A. We are pleased to accept
submissions pertaining to the focus
of Nursing, health information, tech‐
nology, opinion, mental health is‐
sues, medical issues, medication
information, jokes, poems, photo‐
graphs, and scholarly writings.
Submission must include your name,
your credentials, and your unit. All
submissions become the property of
UCN news and publishing is at the
discretion of the editor.
Submissions must be submitted by
the last Wednesday of the Month
for inclusion into the next issue.
UCN is produced 10 times a year
with double issues and special in‐
serts at the discretion of the editor.
Nominations for “Employee of the
Issue” must be forwarded to Kevin
Badon as UCN does not pick the
winners.
Anyone who would like to write a
regular or guest column please send
letter of inquiry via email to:
Writers are not paid for articles, (all
we can do is make you famous), and
UCN accepts no responsibility for
non‐evidenced based information.
Please check your sources to ensure
accurate and fair reporting of your
event or idea or issue.
SUBMIT TO :
By Frances Hodgkins, RN, PMHN‐BC ,Editor of UCN
The Patient Experience Summit:
Empathy and Innovat ion .
Cleveland, Ohio May 2010.
Think of the biggest names in business today
and you have the line‐up at the Cleveland
Clinic’s landmark summit on the Patient Ex‐
perience. The CEO of Enterprise Rent a Car,
representatives from the Disney Institute,
The CEO of Key Bank. Siegfried (of Siegfried
and Roy), Press Ganey, Dr. Jean Watson, Dr.
Mary Bennett, and Gallup Polling were some
of the illustrious speakers.
Countless others from hospital magistrates,
working nurses, and concerned persons
filled the packed auditorium at the Intercon‐
tinental Hotel in Cleveland, Ohio.
The Focus?
The experience of the patient in
health care.
Many individual lectures and
panel discussions from some of
the worlds leading experts on
customer experiences were there.
Sharing their insights on the impact of the
customer experience.
But how does Enterprise Rent‐a‐car fit in
with all the healthcare guru’s? What about
the Disney institute? How does a giant in
the hospitality industry be asked to attend
and speak at a health care conference?
The Reason.
They are the experts in the experiences of
people.
And they are very good a making people
happy.
The Quiz
Here’s a one question quiz of your general
knowledge about experiences.
Why do hotels place mirrors in the eleva‐
tors lobbies?
(You’ve all seen them there...but is it just a
coincidence, or a shared decorating idea?)
It is there because the hospitality industry
knows something about waiting.
Waiting produces anxiety, and hotels do
not want you feeling anxious even the least
little but, because if you get anxious while
waiting for the elevator, that anxiety will
stay with you, and disturb the relaxation you
have gained by being at the hotel.
Now that’s customer
serv ice. Cri t ica l
thinking down to the
very last detail that
you d idn ’ t even
know was making
you anxious.
For me, that’s true
customer service.
Now, on the business end of customer ex‐
periences, Enterprise Rental has the insight
on the employees that provide great cus‐
tomer service.
Enterprise rental, (the largest car rental
company in the world), promotes the man‐
agers that have high customers satisfaction
scores, even though the manager down the
street may have more financial savvy.
There is a lesson there...saying, if you have a
total customer experience, then the rewards
(Continued on page 4)
UCN Editor‐In‐Chief goes to Cleveland Clinic to bring back the cutting
edge discussion in healthcare today. Empathy and Innovation
Submission Guidelines
Interactive Art at Cleveland Clinic
3
4
(One of the Gallery’s at Cleveland Clinic)
are personal such as pay and promotion,
and fiscal because you have repeat custom‐
ers throughout the organization. Repeat
customers means the business is growing.
Simple Math
The VA staff needs to
know and understand
the simple math. Our
patients can choose to
go anywhere they like.
But if they all go to
Methodist or Memorial
Herman, where are all
those dollars going? Not
into to your paycheck.
And now with health‐care reform and Presi‐
dent Obama giving citizens more control
over their healthcare options, it does not
take a fortune‐teller to understand that the
consequences might be disastrous for the
future of Government‐run health care, if
other options are more attractive to the
consumer, even if they cost the same.
(But I digress...)
Art and the Patient Experience
Included in the Cleveland Clinic’s patient
experience is the addition of interactive art.
The picture on page 2 is a “still shot” of an
interactive art instillation. The tree is com‐
puter generated and on the wall via a projec‐
tor mounted to the ceiling.
The tree twists and turns in the breeze ,and
the leaves rustle and turn colors in relation‐
ship to a “season” of time.
Cleveland Clinic has done research as to the
efficacy of interac‐
tive art and the
results are clear.
Art reduces anxiety.
6A already knows
that from our own
art experiments
with the veteran
space, and the vet‐
eran experiences on
6A. Our art projects
have met with myriad responses and most
always evoke a positive emotional response.
And that, my friends, is what we are good at;
emotions. And that is where the patient
experience lies.
In emotions.
The ability to appreciate music, art, card
playing, movies, bowling, outings, and learn‐
ing to laugh and play is just as important in
the patient experience, and recovery, as
going to groups, taking medications, and
being up for meals.
So how can you enhance your patient
experience, today?
(Continued on page 21)
Our “EYES” are on IT
Art Therapy on 6A
Submitted by: Sandra Brooks RN BSN Unit 6A
According to the American Art Therapy Association “The creative process in‐volved in making art is healing and life enhancing.” On 6A we strive to en‐hance the lives of our patient’s through Art Therapy, as one of many therapeu‐tic tools used by our staff. We use the creative process of art making, to im‐prove and enhance the physical, men‐tal and emotional well‐being of our veterans. The art activities are based on the belief that the creative process involved in artistic self‐expression helps people to resolve conflicts and problems, develop interpersonal skill, manage behavior, reduce stress, in‐crease self‐esteem, self‐awareness, and achieve insight. It is our belief that the creative processes involved in art making is healing and life enhancing. It is our mission to serve the veterans by providing and promoting knowledge in the area of art therapy.
(Human Figure made of Steel Letters on Natural Rock)
In Lobby of Cleveland Clinic
(Whispering Wall)
5
5 WAYS TO THINK LIKE A CHAMPION
I meet and learn from Champions every day.
Not just in locker rooms but in classrooms, hospitals, homeless shelters, homes and of-fice buildings. I've learned that to be a cham-
pion you must Think Like a Champion. Cham-pions think differently than everyone else.
They approach their life and work with a different mindset and belief system that sepa-rates them from the pack.
Champions Expect to Win - When they walk on the court, on the field,
into a meeting or in a classroom they expect to win. In fact they are surprised when they
don't win. They expect success and their positive beliefs often lead to positive actions and outcomes. They win in their mind first
and then they win in the hearts and minds of their customers, students or fans.
Champions Celebrate the Small Wins - By celebrating the small wins champions gain
the confidence to go after the big wins. Big wins and big success happen through the accumulation of many small victories. This
doesn't mean champions become compla-cent. Rather, with the right kind of celebra-tion and reinforcement, champions work
harder, practice more and believe they can do greater things.
Champions Don't Make Excuses When
They Don't Win -
They don't focus on the faults of others. They focus on what they can do better. They see their mistakes and defeats as opportuni-
By: Jon Gordon By: Jon Gordon ties for growth. As a result they become stronger, wiser and better.
Champions Focus on What They Get To
Do, Not What They Have To Do - They see their life and work as a gift not an obligation. They know that if they want to
achieve a certain outcome they must commit to and appreciate the process. They may not love every minute of their journey but their
attitude and will helps them develop their skill.
Champions Believe They Will Experi-
ence More Wins in the Future -
Their faith is greater than their fear. Their positive energy is greater than the chorus of negativity. Their certainty is greater than all
the doubt. Their passion and purpose are greater than their challenges. In spite of their
situation champions believe their best days are ahead of them, not behind them.
If you don’t think you have what it takes to be a champion, think again. Champions aren’t born. They are shaped and molded. And as
iron sharpens iron you can develop your mindset and the mindset of your team with
the right thinking, beliefs and expectations that lead to powerful actions.
A great example of this is John Wooden, the legendary UCLA basketball coach who passed away at the age of 99. He was one of
my heroes and someone who not only thought like a champion, but lived like a
champion, taught like a champion and devel-oped champions. Visit http://www.coachwooden.com/ to learn more.
Kudos and Congratu-lations to:
Emmanuel Ekhator for finishing his BSN;
Shirley Collins for getting her Board Certifi-cation in Psych!
The following excerpt is from a lar‐
ger article from NCPEA about the
theory of transformational leader‐
ship.
Transformational Leadership (TL) is
also in the GAP Analysis we worked
on with Kevin. 6A will be addressing
the GAPs that were observed in TL.
The theoretical framework for this
study is transformational leadership
theory, otherwise known as charismatic
leadership theory or social entrepre‐
neurship (Purdue, 2001). According to
Aldoory & Toth (20004) and
Mackenzie, Podsacoff and Rich (2001),
transformational leadership theory is
the most widely used, widely studied
and positively effective leadership the‐
ory. T
he skill‐set characteristic for these lead‐
ers is proficiency in articulating their
vision and/or missions verbally, and
particularly nonverbally, for resonance
and change in followers as described by
Axelsson, Kullen‐Engstrom and Edgren
(2000) and Bennis (2007).
Transformational leaders create trust
and enthusiasm to motivate followers
to change or persevere through dark
times by appealing to and sharing in
their high ideals, moral values and opti‐
mism about the future (Burns, 1978;
Mackenzie et al. 2001). There is an as‐
sumed promise that followers somehow
will be transformed by the leader’s vi‐
sion and/or mission, becoming some‐
what a spiritual product of the leader’s
collaborative purpose with which they
have identified and internalized.
For example, Senge (1990) states that
shared vision is not an idea but rather a
force in people’s hearts. The adoration
of Nelson Mandela and the slave gladia‐
tor Spartacus was not due to their
status as people but rather as icons or
symbols of liberation and autonomy –
core values – with which their followers
identified.
The transformational leader’s personal
integrity is critical in the process of
leading by example – walking the talk –
according to Burns (1978), Mackenzie et
al. (2001) and Wendt & Fairhurst (1994).
The transformational leader is always
visible and his or her attitudes and ac‐
tions model proper behavior to every‐
one else. Mackenzie et al. (2001); Bass,
(1995) and Popper (2004) state that the
transformational leader becomes an
image, identity or an appropriate role
model to guide and symbolize expected
values and behaviors of followers; es‐
sentially crafting a vision, which is a
symbolic process of lacing the message
with metaphors, stories and other col‐
orful emotional language, according to
Aldoory & Toth (2004); Axelsson et. al.
(2000); and Hoy & Miskel (2001).
Deal (1985) as cited in Hoy & Miskel
(2001) asserted that principals of effec‐
tive schools take up the hero or heroine
role that embodies core values. Takala
(1998) describes the transformational
style of leadership as “symbolic leading”
evoking patterns of meaning by creat‐
ing symbolic reality (p. 796). Hoy &
Miskel stress that leaders are managers
of meaning who exhibit “inspirational,
visionary and symbolic or less rational‐
istic aspects of behavior” (2001p.409);
for example:
“Leaders are managers of
meaning” (p.409)
“Meaning is transferred sym‐
bolically” (p.185)
“Leadership is a symbolic activ‐
ity” (p.437)
http://cnx.org/content/m26728/latest/
What is Transformational Leadership?
Four elements of transformational leadership:
Individualized Consideration – the degree to which the leader attends to each follower's needs, acts as a men‐tor or coach to the follower and lis‐tens to the follower's concerns and needs. The leader gives empathy and support, keeps communication open and places challenges before the fol‐lowers. This also encompasses the need for respect and celebrates the individual contribution that each follower can make to the team. The followers have a will and aspirations for self development and have intrin‐sic motivation for their tasks.
Intellectual Stimulation – the de‐gree to which the leader challenges assumptions, takes risks and solicits followers' ideas. Leaders with this style stimulate and encourage crea‐tivity in their followers. They nurture and develop people who think inde‐pendently. For such a leader, learning is a value and unexpected situations are seen as opportunities to learn. The followers ask questions, think deeply about things and figure out better ways to execute their tasks.
Inspirational Motivation – the de‐gree to which the leader articulates a vision that is appealing and inspiring to followers. Leaders with inspira‐tional motivation challenge followers with high standards, communicate optimism about future goals, and provide meaning for the task at hand. Followers need to have a strong sense of purpose if they are to be motivated to act. Purpose and meaning provide the energy that drives a group for‐ward. The visionary aspects of leader‐ship are supported by communica‐tion skills that make the vision un‐derstandable, precise, powerful and engaging. The followers are willing to invest more effort in their tasks, they are encouraged and optimistic about the future and believe in their abili‐ties.
Idealized Influence – Provides a
role model for high ethical behavior,
instills pride, gains respect and trust.
6
Old Drugs/New Drugs:Same Problems
MedWatch 2010
MICHAEL E DEBAKEY VA MEDICAL CENTER
Unit Council News
Dear Readers,
This month MedWatch is please to bring you the latest
news from the drug world. Heroin, meth, marijuana
and the newest kids on the block, K2 and meow meow.
Every special issue of MedWatch strives to bring you
breaking news from the pharma industry,
and you must be in tune to what your pa‐
tients are buying and experiencing on their
own.
Addiction is a severe problem with many
facets, and ones that are not always obvious.
Any addict can tell you what
makes them happy, and many
were not ever happy until they
started using drugs.
Our mission is to help them with Recovery, extending
hope in the darkness and ushering them toward well‐
ness. Drugs are powerful, but they can not stand up to
hope. You are the hope for our patients.
This month take the time to read the latest
from the street and walk a mile in your veter‐
ans shoes.
And please consider joining the National Alco‐
hol and drug addiction recovery month cele‐
bration planning committee.
We have lots of free materials to
get you started. Please see your
unit reps ,and till then,
Be Well.
Fran
7
Study Shows 111 Percent Increase in Emergency Department Visits In‐volving Nonmedical Use of Pre‐scription Opioid Pain Relievers in Five‐Year Period
From 2004 to 2008 the estimated number of emergency department visits linked to the nonmedical use of prescrip‐tion pain relievers rose from 144,644 visits to 305,885 visits a year.
Visits to hospital emergency departments involving non‐medical use of prescription narcotic pain relievers more than doubled, rising 111 percent, between 2004 and 2008, according to a study by the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Cen‐ters for Disease Control and Prevention. The study used data from SAMHSA's Drug Abuse Warning Network (DAWN) emergency department system. It examined emergency department visits for nonmedical use of legal drugs, such as using them without a prescription.
The dramatic rise in emergency department visits associ‐ated with nonmedical use of these drugs occurred among men and women, as well as among those younger than age 21 and those 21 and older.
"The abuse of prescription drugs is our nation's fastest‐growing drug problem. And this new study shows it is a problem that affects men and women, people under 21, and those over 21," said Office of National Drug Control Policy Director Gil Kerlikowske. "The newly released Na‐tional Drug Control Strategy contains specific steps that all of us can take to address this issue."
The three prescription opioid pain relievers most fre‐quently involved in hospital emergency department visits from 2004 to 2008 were:
Oxycodone products – ED visits involving non‐medical use rose 152 percent, to 105,214.
Hydrocodone products – emergency department visits involving nonmedical use rose 123 percent, to 89,051.
Methadone products – emergency department visits involving nonmedical use rose 73 percent, to 63,629.
"These alarming findings provide one more example of how the misuse of prescription pain relievers is impacting lives and our health care system," said SAMHSA Adminis‐trator Pamela S. Hyde. "This public health threat requires an all‐out effort to raise awareness of the public about proper use, storage, and disposal of these powerful drugs."
The numbers of emergency department visits involving nonmedical use of other types of prescription pain reliev‐ers such as morphine, fentanyl and hydromorphone were lower, but they also showed sharp rises during this period – for example, hydromorphone‐related nonmedical use visits rose 259 percent from 2004, to 12,142 in 2008. These upward trends reflect in part dramatic increases in the rate at which these drugs are prescribed in the United States.
"We urgently need to take action," said CDC director Dr. Thomas Frieden. "Emergency department visits involving non‐medical use of these prescription drugs are now as common as emergency department visits for use of illicit drugs. These prescriptions medicines help many people, but we need to be sure they are used properly and safely."
The study is being co‐released in SAMHSA's survey report, Trends in Emergency Department Visits Involving Non‐medical Use of Narcotic Pain Relievers and CDC's MMWR "Emergency Department Visits Involving Nonmedical Use of Selected Prescription Drugs – United States, 2004‐2008." The reports are based on data from SAMHSA's Drug Abuse Warning Network (DAWN) for 2004 to 2008. DAWN is a public health information system that moni‐tors drug‐related ED visits throughout the United States.
The full reports are available at: CDC MMWR www.cdc.gov/mmwr. The SAMHSA report can also be obtained by calling the SAMHSA Health Information Net‐work at 1‐877‐SAMHSA‐7 (1‐877‐726‐4727). For related publications and information, visit http://www.samhsa.gov/.
CDC recently released an issue brief, "Unintentional Drug
Poisoning in the United States," showing more than
26,000 deaths from unintentional drug poisoning in the
United States in 2006 – more than 70 each day. The issue
brief provides recommendations on how health care pro‐
viders, private insurance providers, and state and federal
agencies can work to prevent unintentional drug over‐
doses. For a copy of the issue brief, please visit http://
www.cdc.gov/HomeandRecreationalSafety/Poisoning/
brief.htm
8
9
Does Marijuana
Withdrawal
Syndrome Exist?
By Elena M. Kouri, Ph.D. | February 1, 2002
The question of whether a clinically significant
marijuana (cannabis) withdrawal syndrome
exists remains controversial. In spite of the
mounting clinical and preclinical evidence sug‐
gesting that such a syndrome exists (Beardsley
et al., 1986; Budney et al., 2001; Holson et al.,
1989; Huestis et al., 2001), the DSM‐IV does not
include marijuana withdrawal as a diagnostic
category. The clinical syndrome has been char‐
acterized by restlessness, anorexia, irritability
and insomnia that begin less than 24 hours after
discontinuation of marijuana, peak in intensity
on days 2 to 4, and last for seven to 10 days
(Budney et al., 1999; Haney et al., 1999; Mendel‐
son et al., 1984).
The question of whether this syndrome is clini‐
cally significant is important, not only because
marijuana is the most commonly used illicit
drug in the United States (Johnston et al., 2001),
but also because marijuana has been shown to
produce dependence at rates comparable to
other drugs of abuse (Kandel et al., 1997; Kessler
et al., 1994) and because relapse rates among
individuals seeking treatment for marijuana
dependence are similar to those with other
drugs of abuse (Budney et al., 1998; Stephens et
al., 1993). Furthermore, many violent crimes are
committed by individuals undergoing with‐
drawal from drugs of abuse, including mari‐
juana (Kouri et al., 1997; Peters and Kearns,
1992). If a clinically significant marijuana with‐
drawal syndrome does exist, the omission of
this syndrome from the DSM‐IV might contrib‐
ute to the perception that behavioral or phar‐
macological treatment regimens for marijuana
dependence are not necessary.
We conducted two studies in our laboratory to
determine whether abstinence from marijuana
after long‐term use results in withdrawal symp‐
Dr. Kouri is assistant professor of psychiatry at
Harvard Medical School in Boston, Mass.
Dr. Kouri is assistant professor of psychiatry at
Harvard Medical School in Boston, Mass.
toms, to identify those symptoms and to quan‐
tify their severity (Kouri and Pope, 2000; Kouri
et al., 1999). The first study focused specifically
on whether abrupt discontinuation of mari‐
juana following chronic use results in changes
in aggressive behavior (Kouri et al., 1999). To
measure aggressive behavior, we used the Point
Subtraction Aggression Paradigm (PSAP). This
computer test has been used to detect changes
in aggressive responses following acute admini‐
stration of a number of drugs, and its external
validity has been demonstrated in a number of
studies of male and female parolees with histo‐
ries of violent behavior (Cherek and Lane, 1999;
Cherek et al., 1996).
Subjects in our study were long‐term heavy
users of marijuana who reported a history of at
least 5,000 separate episodes of marijuana use
in their lifetime (the equivalent to smoking
once per day for 13.7 years), were smoking at
least once daily at the time of recruitment and
met DSM‐IV criteria for marijuana dependence
without meeting criteria for a current Axis I
disorder. Subjects were excluded if they re‐
ported that they had used another class of drugs
more than 100 times in their lifetimes or had
consumed more than five alcoholic drinks per
day continuously for one month or more in
their lifetimes.
The controls were composed of two groups: 1)
individuals who had not smoked marijuana
more than 50 times in their lives and had not
smoked more than once per month in the last
year and 2) individuals who had formerly
smoked marijuana on a daily basis but who had
not smoked more than once per week during
the last three months. The rationale for using
infrequent or former smokers rather than mari‐
juana‐naive subjects as controls was to mini‐
mize possible confounding variables that might
(Continued on page 10)
10
differentiate individuals who had never tried
marijuana from those who had. We based this
decision on data from our laboratory demon‐
strating that heavy marijuana users do not differ
from occasional users in a wide range of demo‐
graphic and psychiatric measures (Kouri et al.,
1995).
During the study, subjects were required to
abstain from smoking marijuana and using any
other drugs for 28 consecutive days. To verify
abstinence, subjects had to come to the labora‐
tory every day to provide supervised urine sam‐
ples that we analyzed quantitatively for tetrahy‐
drocannabinol (THC) metabolites. We meas‐
ured aggressive responses with the PSAP on
study days 0 (before abstinence), 1 (after 24
hours of abstinence), 3, 7 and 28.
Subjects were told they would be playing a com‐
puter game against an anonymous same‐sex
subject from the study. In fact, however, this
second subject was actually a computer. During
the course of each 20‐minute computer session,
subjects had the option of pressing one of two
buttons on the PSAP response panel (labeled
"A" or "B"). Pressing button A resulted in the
accumulation of points that were exchanged for
money at the end of the study. Pressing this
button was defined as a non‐aggressive re‐
sponse. By pressing button B, subjects could
subtract points from the fictitious opponent.
Points taken from the opponent, however, were
not added to the subject's counter, and pressing
button B was defined as an aggressive response.
Aggressive responding was provoked by random
subtractions of the subject's points, which were
attributed to the fictitious opponent.
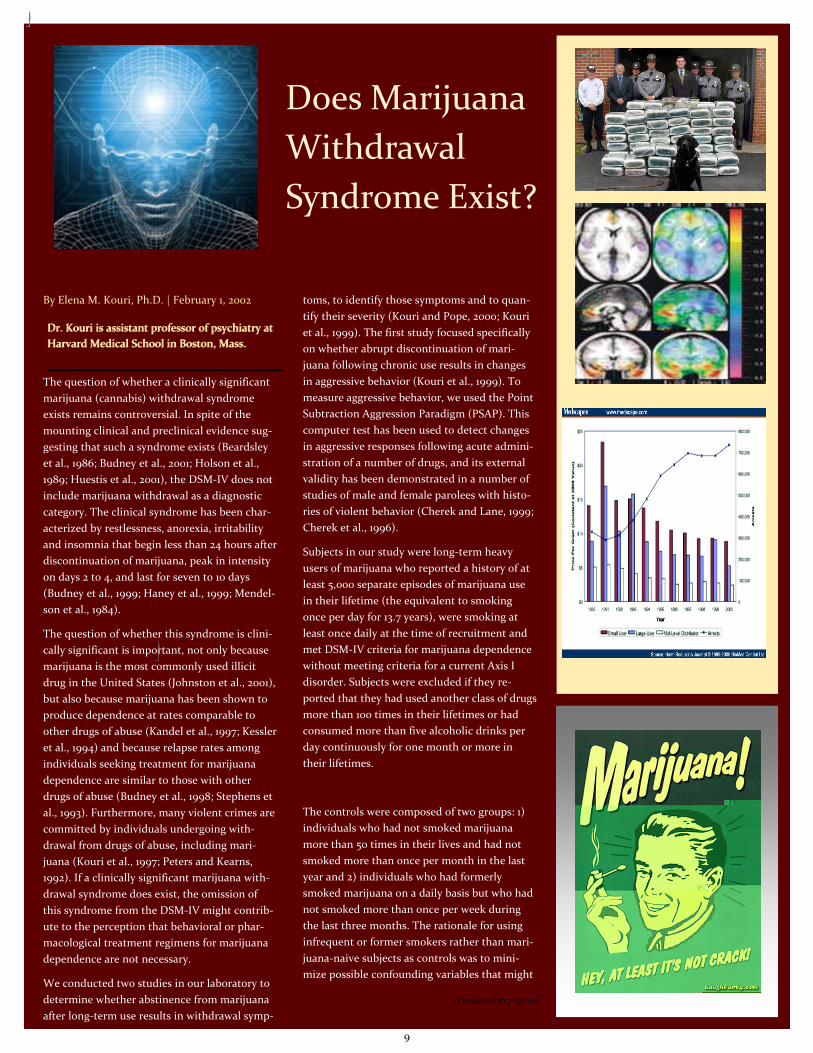
On study day 0 (before marijuana abstinence)
and study day 1 (24 hours of marijuana absti‐
nence), the current marijuana users did not
differ from past heavy users or light users in the
number of aggressive or non‐aggressive re‐
sponses they made. However, current marijuana
users were significantly more aggressive on days
3 and 7 of marijuana abstinence compared to
their pre‐withdrawal levels of aggression and
compared to the controls. By day 28, the num‐
ber of aggressive responses from the current
marijuana users was not different from their pre
‐withdrawal baseline levels or the controls
(Figure).
These data demonstrate that abstinence from
marijuana after chronic use is associated with
increases in aggressive responding following
provocation. Specifically, during the first week
of abstinence, current marijuana users dis‐
played levels of aggression that were signifi‐
cantly higher than before abstinence and higher
than the levels displayed by matched controls.
Interestingly, the increases in aggressive re‐
sponding followed a specific time course and
then returned to pre‐withdrawal levels after 28
days of abstinence. The transient nature of
these changes is consistent with other reports of
marijuana withdrawal.
The second study was designed to further char‐
acterize symptoms of marijuana withdrawal and
to quantify their magnitude (Kouri and Pope,
2000). We used the same study entry criteria as
in the first study and subjects were required to
come to the laboratory every day to provide
urine samples and to fill out a daily diary.
The items assessed in the daily diaries were:
mood, appetite, sleep, anxiety, irritability,
physical tension or agitation, physical symp‐
toms, ability to concentrate, desire to use mari‐
juana, and desire to resume using marijuana at
the end of the study. The questions were pre‐
sented on a 10‐point Likert scale with the quali‐
fiers "extremely low" at the zero end of the scale
and "extremely high" at the 10‐point end of the
scale. We obtained pre‐withdrawal baseline
levels for all of the diary items via a personal
interview with each subject before the begin‐
ning of the withdrawal period.
Thirty current marijuana users and 30 controls
(16 former heavy users and 14 light users) par‐
ticipated in the study. Before the beginning of
the abstinence period, the current marijuana
users were not different from the former users
or the light users on any of the items assessed in
the diaries except for the ability to concentrate
item. The current users reported a lower ability
to concentrate than the controls. Interestingly,
the former heavy users were not different from
the light users on any of the diary scores during
the course of the study. In contrast, the current
users reported increases in irritability, anxiety,
physical tension and physical symptoms, and
decreases in mood and appetite starting on day
1 and peaking between days 7 and 10 of mari‐
juana abstinence.
It is important to note that although, as a
group, the current marijuana users experienced
an increase in withdrawal symptoms compared
to the controls, only 60% of the subjects in the
current users group reported a change in symp‐
toms of at least three points in magnitude. The
fact that 40% of subjects who had used mari‐
juana regularly for an average of 22 years did
not report experiencing severe withdrawal
symptoms during abstinence might suggest that
physical dependence on marijuana is not as
strong as that observed with other drugs of
abuse. This may be due, at least in part, to the
long half‐life of THC. However, many subjects
reported that when trying to remain abstinent
in the past, the presence of withdrawal
symp
toms had played an important role in
their relapse. Thus, alleviation of absti‐
nence symptoms may contribute to the
maintenance of daily marijuana use in
chronic users.
Another significant finding is that after
28 days of marijuana abstinence, all of
the symptoms returned to pre‐
withdrawal levels except for irritability
and physical tension. It is possible that
these two symptoms remained slightly
elevated because they represented a
premorbid characteristic of the current
users and were not a result of marijuana
withdrawal. If this is the case, the fact
that the former users did not have ele‐
vated scores on these two items may
reflect a characteristic that potentially
differentiates individuals with a history
of heavy marijuana use who have suc‐
cessfully stopped from individuals who
continue to smoke regularly.
Taken together, the data from these two
studies provide further evidence of the
existence of a marijuana withdrawal
syndrome. An important aspect of both
of our studies is that we used two con‐
trol groups: 1) former heavy marijuana
users and 2) individuals who had rarely
smoked marijuana during their lives.
It is noteworthy that these control
groups were indistinguishable from one
another in diary scores or number of
aggressive responses on the PSAP,
whereas both were significantly distin‐
guishable from the current marijuana
users. This observation argues that the
elevated diary scores and aggressive
responses of the current marijuana us‐
ers were attributable to marijuana with‐
drawal, rather than a mere history of
marijuana use or some other aspect of
subject selection or study design. Future
studies should focus not on whether a
marijuana withdrawal syndrome exists
but rather on determining the clinical
significance of this syndrome and the
role withdrawal symptoms play in per‐
petuating marijuana use. Acknowledgement:These studies were supported by NIDA grants
DA10346, DA03994, DA00343. References:Beardsley PM, Balster RL,
Harris LS (1986), Dependence on tetrahydrocannabinol in rhesus
monkeys. J Pharmacol Exp Ther 239(2):311‐319.iBudney AJ, Hughes
JR, Moore BA, Novy PL (2001), Marijuana abstinence effects n
marijuana smokers maintained in their home environment. Arch
Gen Psychiatry 58(10):917‐924.Budney AJ, Novy PL, Hughes JR
(1999), Marijuana withdrawal among adults seeking treatment for
marijuana dependence. Addiction 94(9):1311‐1322.Budney AJ,
Radonovich KJ, Higgins ST, Wong CJ (1998), Adults seeking
treatment for marijuana dependence: a comparison with cocaine‐
dependent treatment seekers. Exp Clin Psychopharmacol 6(4):419‐
426.
“K2,” the brand name for a product that’s been sold since
2008 and marketed as incense, is a dried herb that has been
sprayed with a chemical compound that when smoked cre‐
ates a high similar to inhaling marijuana.
And in spite of the claims made on the multiple Internet
sites where it’s sold that is it is “the perfect incense mixture”
and is not meant for human consumption, law enforcement
calls it fake weed.
The problem? It’s legal in most states, including Michigan.
Kalamazoo Department of Public Safety Capt. Joseph Taylor,
commander of the Kalama‐
zoo Valley Enforcement
Team, which targets illegal
drug use in Kalamazoo
County, said his agency has‐
n’t come into contact with
K2. But it’s effects concern
him.
“There is no legitimate pur‐
pose for this,” Taylor said.
“It appears only to have
negative results and seems
intended on trying to surpass marijuana laws. The only real
design seems to be in the form of a drug.”
K2, also known as “Mr. Smiley” and “Spice,” is manufactured
in China and South Korea and is sprayed with a chemical
compound similar to THC, the psychoactive ingredient in
marijuana.
Sold over the Internet and in some head shops across the
state, K2 can be purchased for $30 to $50 for 3 grams. Web
sites that sell K2, which comes in blends called “Summit,”
“Sex,” “Blonde” and “Ultra,” claim that it is purely an incense
product.
“K2 incense smoke blends are a mix of hand‐selected herbs
and proprietary synthetic ingredients that create the perfect
incense mixture,” states a description of K2 on a wholesaler
website. “Each of the unique blends … create a robust smoke
coupled with a bouquet of unique aromas. These aromatic
scents are so flawless, consumers long to enjoy the K2 prod‐
uct time and time again.”
“Like playing Russian Roullette”
John Huffman, a professor of organic chemistry at Clemson
University, developed the chemical substances found in K2,
JWH‐018 and JWH‐073, in 1995 while doing research on the
effects of cannabinoids on brain.
He’s not sure how the recipes got picked‐up, but he is taken
aback in how they are being used.
“The real problem is that we really don’t know anything
about it,” he said during a phone interview from his office in
Clemson, S.C. Consuming it “is like playing Russian Roul‐
lette.”
USA Today in a report on K2
quoted Anthony Scalzo, director
of the Missouri Poison Center in
St. Louis, as saying that since he
notified poison centers nation‐
wide about K2 in early February
following reports of sick patients
in Missouri, poison centers na‐
tionwide have had more than 350
reports of illnesses from it. Pa‐
tients often have a rapid heart
rate, dangerously high blood pressure and sometimes hallu‐
cinations or paranoia, the USA Today story said.
Huffman said the active ingredient in K2 can be 10 times as
potent as marijuana, and in large doses can cause hallucina‐
tions and disorientation that can last for days. He said he got
an e‐mail from a young woman who smoked K2 and said she
was disoriented for a week and felt electric shocks pulsating
up and down her back.
Huffman said he’s been in touch with the U.S. Drug Enforce‐
ment Agency, the U.S. Dept. of Homeland Security and the
National Institutes of Health, advising the agencies on the
substance in K2.
And as much as he created the substance for research, he’s
not surprised that it’s gotten into the hands of those who
want to make a quick buck. The active substance in K2 is
easy to make, the raw materials are cheap and the profit
margin is high.
(Continued on page 12)
K2: Substance on the Street
11
“If I were a young entrepreneur in China and I knew enough
science, this would be a way to make good money,” Huff‐
man said. “These people are sophisticated. They’re coming
up with compounds we’ve never seen.”
Regulation sought
Richard Tooker, Kalamazoo County’s chief medical officer,
said that K2 has a “real potential for danger.”
“Anytime you’ve got something like this that’s unregulated,
you just don’t know what it is,” he said. “It’s not controlled,
it’s not licensed. There’s no question that it’s dangerous.”
Tooker likened K2 to Ecstacy, a drug that was once legal but
was eventually outlawed after its negative effects were made
known.
“Adolescents want to experiment,” he said. “So there’s the
potential for injury. This (K2) needs to be quickly regulated
and controlled.”
Michigan is one of 11 states across the nation that have ei‐
ther banned K2 or have legislation introduced that aims to
ban it. So far, Kansas and Kentucky are the only states to
outlaw K2.Republican State Rep. Rick Jones, of Grand
Ledge, introduced a bill in April that would make K2 illegal
in Michigan. His office said that a hearing on the measure
could take place this fall.
K2, which has been banned on U.S. military bases, is not on
the DEA’s Schedule I list of controlled substances, such as
cocaine, heroin, mescaline and several others, but the
agency does consider it a “drug or chemical of concern.”
For his part, KVET’s Taylor would like to see the drug out‐
lawed.
“Do kids really know what they’re putting in their bodies?,”
the drug unit commander said of K2. “They try these things
without being aware of the final outcome.”
Greg Francisco, executive director of the Michigan Medical
Marijuana Association, acknowledged that K2 is a poten‐
tially dangerous substance to consume, but said there
would not even be a discussion about it if marijuana were
legal.
“This is one more artifact of prohibition,” Francisco said.
“It’s no different than during prohibition when people
turned to wood alcohol. So what we now see is people turn‐
ing to inferior substitutions. It’s another example of why we
should legalize marijuana so we can finally control it.”
Store refuses to sell K2
From dried herbs to glass pipes to homemade soy candles,
the husband and wife team of Angel and Jeff Justice sell
several eccentric items at their Allegan store, Cloud 10, on
M‐40.
K2 isn’t one of them.
Employees at the Glass Onion, a popular head shop on
West Main Street in Kalamazoo, said K2 isn’t sold there
either.
Jeff Justice said he gets about three to four calls per week
from wholesalers looking to sell him K2. He always declines,
he said.
“It’s got chemicals in it or whatever else is in it,” Justice said.
“People don’t know what hell it is and no one wants to give
up the
ghost.”
This picture is from an actual web‐
site selling the K2 product.
http://www.k2cafe.org/
Consider the stereotypical represen‐
tation of a drug dealer, and ask
yourself, how does this relate with incense?
To me the message is
clear, this is not mark‐
ing incense, it is mar‐
keting a drug lifestyle.
What do you think?
Check it for yourself.
12
WINFIELD, Mo. — Mexican drug smugglers are increasingly
peddling a form of ultra‐potent heroin that sells for as little
as $10 a bag and is so pure it can kill unsuspecting users in‐
stantly, sometimes before they even remove the syringe from
their veins.
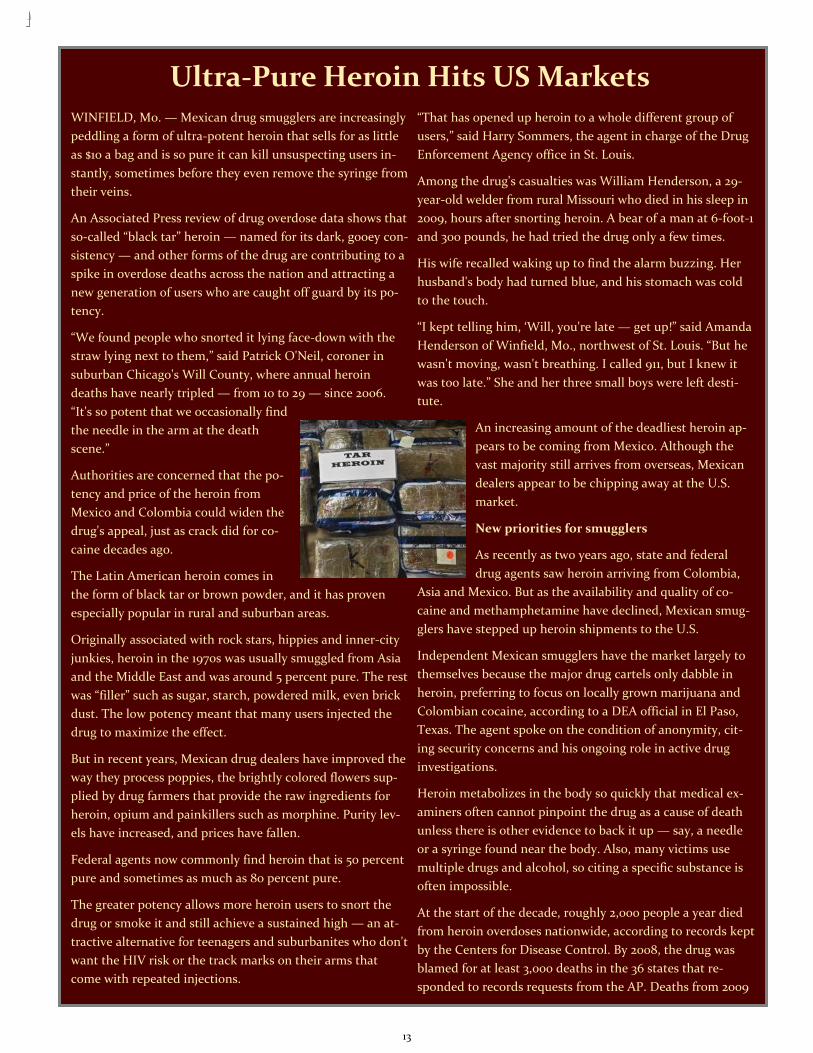
An Associated Press review of drug overdose data shows that
so‐called “black tar” heroin — named for its dark, gooey con‐
sistency — and other forms of the drug are contributing to a
spike in overdose deaths across the nation and attracting a
new generation of users who are caught off guard by its po‐
tency.
“We found people who snorted it lying face‐down with the
straw lying next to them,” said Patrick O'Neil, coroner in
suburban Chicago's Will County, where annual heroin
deaths have nearly tripled — from 10 to 29 — since 2006.
“It's so potent that we occasionally find
the needle in the arm at the death
scene.”
Authorities are concerned that the po‐
tency and price of the heroin from
Mexico and Colombia could widen the
drug's appeal, just as crack did for co‐
caine decades ago.
The Latin American heroin comes in
the form of black tar or brown powder, and it has proven
especially popular in rural and suburban areas.
Originally associated with rock stars, hippies and inner‐city
junkies, heroin in the 1970s was usually smuggled from Asia
and the Middle East and was around 5 percent pure. The rest
was “filler” such as sugar, starch, powdered milk, even brick
dust. The low potency meant that many users injected the
drug to maximize the effect.
But in recent years, Mexican drug dealers have improved the
way they process poppies, the brightly colored flowers sup‐
plied by drug farmers that provide the raw ingredients for
heroin, opium and painkillers such as morphine. Purity lev‐
els have increased, and prices have fallen.
Federal agents now commonly find heroin that is 50 percent
pure and sometimes as much as 80 percent pure.
The greater potency allows more heroin users to snort the
drug or smoke it and still achieve a sustained high — an at‐
tractive alternative for teenagers and suburbanites who don't
want the HIV risk or the track marks on their arms that
come with repeated injections.
“That has opened up heroin to a whole different group of
users,” said Harry Sommers, the agent in charge of the Drug
Enforcement Agency office in St. Louis.
Among the drug's casualties was William Henderson, a 29‐
year‐old welder from rural Missouri who died in his sleep in
2009, hours after snorting heroin. A bear of a man at 6‐foot‐1
and 300 pounds, he had tried the drug only a few times.
His wife recalled waking up to find the alarm buzzing. Her
husband's body had turned blue, and his stomach was cold
to the touch.
“I kept telling him, ‘Will, you're late — get up!” said Amanda
Henderson of Winfield, Mo., northwest of St. Louis. “But he
wasn't moving, wasn't breathing. I called 911, but I knew it
was too late.” She and her three small boys were left desti‐
tute.
An increasing amount of the deadliest heroin ap‐
pears to be coming from Mexico. Although the
vast majority still arrives from overseas, Mexican
dealers appear to be chipping away at the U.S.
market.
New priorities for smugglers
As recently as two years ago, state and federal
drug agents saw heroin arriving from Colombia,
Asia and Mexico. But as the availability and quality of co‐
caine and methamphetamine have declined, Mexican smug‐
glers have stepped up heroin shipments to the U.S.
Independent Mexican smugglers have the market largely to
themselves because the major drug cartels only dabble in
heroin, preferring to focus on locally grown marijuana and
Colombian cocaine, according to a DEA official in El Paso,
Texas. The agent spoke on the condition of anonymity, cit‐
ing security concerns and his ongoing role in active drug
investigations.
Heroin metabolizes in the body so quickly that medical ex‐
aminers often cannot pinpoint the drug as a cause of death
unless there is other evidence to back it up — say, a needle
or a syringe found near the body. Also, many victims use
multiple drugs and alcohol, so citing a specific substance is
often impossible.
At the start of the decade, roughly 2,000 people a year died
from heroin overdoses nationwide, according to records kept
by the Centers for Disease Control. By 2008, the drug was
blamed for at least 3,000 deaths in the 36 states that re‐
sponded to records requests from the AP. Deaths from 2009
Ultra‐Pure Heroin Hits US Markets
13
have not yet been compiled.
The AP contacted agencies in all 50 states, as well as offi‐
cials in the District of Columbia and New York City, includ‐
ing medical examiners, coroners and health departments.
The survey showed that heroin deaths rose 18.2 percent
from 2007 to 2008, and 20.3 percent from 2006 to 2008.
Law enforcement officials and drug‐treatment experts be‐
lieve those statistics woefully undercount the actual number
of deaths. And they fear the problem is getting worse: Sei‐
zures of heroin along the U.S.‐Mexico border quadrupled
from 2008 to 2009, from about 44 pounds (20 kilograms) to
more than 190 pounds (86 kilograms).
In the Minneapolis‐St. Paul area, more than 20 deaths were
blamed on heroin in 2009. DEA analysis of heroin pur‐
chased undercover found the drug was nearly 60 percent
pure — the highest average purity in the U.S. At the same
time, the price was among the lowest.
Like the rise of crack
“This is consistent with how crack cocaine was introduced
in the 1970s, when it was a high‐purity product sold at a low
price,” said Carol Falkowski, director of the alcohol and
drug abuse division for the Minnesota Department of Hu‐
man Services.
To hook new users, dealers are selling heroin cheap — often
around $10 a bag. The new users included Billy Roberts, the
19‐year‐old son of a retired Chicago police officer. Last Sep‐
tember, he slumped over dead of a heroin overdose at a
friend's house.
John Roberts had moved his family to Will County when
Billy was just entering high school.
“I thought I was moving away from problems like that,”
Roberts said. “These kids out here are being introduced to
real serious drugs, dirt cheap, and they don't know how
pure and dangerous they are.”
Roberts now speaks to high school and civic groups about
the dangers of heroin.
Independent Mexican smugglers like Jose Antonio Medina
Arreguin pay the cartels for access to lucrative trade routes
used to sneak drugs across the border and along U.S. high‐
ways.
Medina, also known as “Don Pepe,” was arrested earlier this
year in Mexico on suspicion of running a $10 million‐a‐
month heroin smuggling business from the western Mexico
state of Michoacan. With the permission of the area's pow‐
erful La Familia cartel, he is believed to have shipped as
much as 440 pounds a month into the U.S. for street
sales from San Diego to San Jose.
Glendale, Calif., often ranks among the safest cities of
its size. But police are concerned about a growing her‐
oin problem tied to Mexican street gangs from nearby
Los Angeles. Gang members make the quick drive up
Interstate 5 to deliver heroin straight to high school
kids.
“They tell them, ‘Just smoke it. It's just like smoking a
cigarette. It's just like smoking marijuana,'” said Glen‐
dale police Sgt. Tom Lorenz. Once the kids are hooked,
“they've got a customer forever.”
The trip up I‐5 also leads to Oregon, where state Medi‐
cal Examiner Karen Gunson said the heroin problem is
worst in communities along the interstate. The state
had 131 heroin‐related overdose deaths last year — 42
more than three years earlier.
The dead simply didn't know the risks of the heroin
they used, she said.
“We're seeing it sometimes 80 percent pure,” Gunson
said. “There's no FDA approval on this stuff. If you're
using it every day, your chances grow and grow that it's
going to kill you.”
That's what happened to Nikki Tayon. A decade ago,
she helped lead the high school softball team from
Winfield to second place in the state. But it wasn't long
after high school that she began using drugs such as
marijuana and meth. A couple of years ago, she turned
to heroin.
Last April, her mother, Sue Tayon, got a call from a
ranger at Cuivre River State Park. Nikki's purse and cell
phone had been found, and rangers were looking for
her. Hours later came the gruesome news: Nikki's body
was discovered in a ditch. She was 28.
She had overdosed on heroin that was 90 percent pure,
her mother said. Police said her boyfriend panicked and
dumped Nikki from the car. No charges were filed.
“I know she was doing it,” Sue Tayon said. “But she did‐
n't deserve to die this way.”
14
4‐methylmethcathinone [Mephedrone, 4‐MMC, meow meow, m‐CAT, bounce, bubbles, mad cow]
July 2010 DEA/OD/ODE
Introduction
4-Methylmethcathinone (mephedrone) is a designer drug of the phenethylamine class and shares substantial structural similari-ties with methcathinone (Schedule I). Evidence of mephedrone use and associated toxicity has been increasing, in 2009 and 2010, particularly in the United Kingdom and other European countries. To date, one confirmed and several suspected deaths related to mephedrone have been reported by Europol-EMCDDA Joint report on mephedrone 2010. In recent years, law en-forcement agencies have documented seizures (Oregon, Illinois and Alabama) associated with mephedrone in the United States.
Licit Uses
Mephedrone is not approved for medical use in the United States.
Chemistry
The core chemical structure of mephedrone identifies it as a phenethylamine, and is related in chemical structure to meth-cathinone differing only by a methyl group (CH3) on the ring. It is a solid at room temperature.
Pharmacology
Structure-activity relationship studies allow to predict that the pharmacology of mephedrone is similar to methcathinone as well as other substances of phenethylamine chemical class. The compounds having similar structure (e.g., methampheta-mine, methylone, 3,4-methylenedioxymethamphetamine, cathinone and methcathinone) have been used to assess the phar-macological profile of mephedrone. This class of compounds is known to produce central nervous system stimulation, psy-choactivity and hallucinations.
The adverse health effects caused by mephedrone are broadly similar to those seen with other stimulant drugs. Adverse ef-fects produced by phenethylamines are increased heart rate, chest pain, agitation, irritability, dizziness, delusions, nose bleed-ing, nausea and vomiting. Consistent with the above discussion, mephedrone was reported to produce agitation, dilated pu-pils, increased heart rate and blood pressure in a 22-year-old man who used it for recreational purpose.
User Population
It is predominantly used by youth population (15-24 years), higher in males than females, from urban areas, who frequent clubs, discos and dance events (Europol-EMCDDA Joint report on Mephedrone, 2010).
Illicit Distribution
Mephedrone is sold over the internet and is promoted as a “research chemical”, “bath salts” or “plant food.”
Control Status
Mephedrone is not scheduled under Controlled Substance Act (CSA). However, it can be considered an analogue of methcathi-none (schedule I substance) under the analogue provision of the CSA (Title 21 United States Code 813). Therefore, law enforce-ment cases involving mephedrone can be prosecuted under the Federal Analog Act of the CSA. Comments and additional infor-mation are welcomed by the Drug and Chemical Evaluation Section, Fax 202-353-1263, Telephone 202-307-7183, or E-mail [email protected].
New Drugs on
the Horizon
Freely available on
the internet...you
must call for pricing
15

Methamphetamine Availability From mid-2008 through 2009, methamphetamine availability increased in the United States. Drug availability indicator data show that methamphetamine prices, which peaked in 2007, declined significantly during 2008 and 2009, while metham-
phetamine purity increased.
Impact on Health and
Health Care Systems
In 2008, NSDUH estimated that 7 million individu-als aged 12 and older were dependent on or had abused illicit drugs in the past year, compared with 6.9 million in 2007. The drugs with the highest dependence or abuse levels were marijuana, pre-scription pain relievers, and cocaine. The number of individuals reporting past year marijuana abuse or dependence was 4.2 million in 2008, compared with 3.9 million in 2007; the number of individuals re-porting past year prescription pain reliever abuse or dependence was 1.7 million in both 2007 and 2008; and the number of individuals reporting past year cocaine abuse or dependence was 1.4 million in 2008, compared with 1.6 million in 2007. Many individuals who become dependent on illicit
drugs eventually seek treatment. The Treatment Episode Data Set (TEDS) provides information regarding the demographics and substance abuse patterns of treatment admissions to state-licensed treatment facilities for drug dependence. In 2007, there were approximately 1.8 million admissions to state-licensed treatment facilities for illicit drug dependence or abuse. The highest percent-age of admissions reported opiates as the primary drug of choice (31%, primarily heroin) followed by marijuana/hashish (27%), cocaine (22%), and stimulants (13%). Although approaches to treatment vary by drug, more than half of the admissions were to ambulatory (outpatient, intensive outpatient, and detox) facilities rather than residential facilities. (See Table B2 in Appendix B for data on admissions for specific drugs.) Individuals often experience adverse reactions to drugs--including nonfatal overdoses--that require them to go to the hospital. In 2006, the Drug Abuse Warning Network (DAWN) reported that of 113 million hospital ED visits--1,742,887 (1.5%)--were related to drug misuse or drug abuse. An estimated 31 percent of these visits involved illicit drugs only, 28 percent involved CPDs, and 13 percent involved illicit drugs in combination with alcohol. When drug misuse or abuse plays a role in these ED visits, the most commonly reported substances are cocaine, marijuana, heroin, and stimulants (typically amphetamines or methamphetamine).A 2007 DAWN survey of 63 metropolitan areas found an average of 12.1 deaths per 100,000 persons related to drug use.5 Rates of drug-related deaths range from 1.1 per 100,000 in Sioux Falls, South Dakota, to 26.1 per 100,000 in the New Orleans area. DAWN also records the number of drug-related suicide deaths. In 2007, the number of drug-related suicides per 100,000 persons ranged from less than one in several jurisdictions (including Chicago, Dallas-Fort Worth, and Minneapolis) to 6.2 per 100,000 in Fargo, North Dakota. To put these statistics in perspective, the Centers for Disease Control and Prevention (CDC) reports other nonnatural death rates as follows: Motor vehicle accidents, 15.1 per 100,000; nontransport accidents (e.g., falls, accidental drownings), 24.4 per 100,000; suicide, 11.1 per 100,000; and homicides, 6.2 per 100,000. The consequences of drug use usually are not limited to the user and often extend to the user's family and the greater community. According to SAMHSA, combined data from 2002 to 2007 indicate that during the prior year, an estimated 2.1 million American children (3%) lived with at least one parent who was dependent on or abused illicit drugs, and 1 in 10 children under 18 lived with a substance-addicted or substance-abusing parent.6 Moreover, the U.S. Department of Health and Human Services estimated in 1999 that substance abuse was a factor in two-thirds of all foster care placements.Many states have enacted drug-endangered children laws to protect children from the consequences of drug production, trafficking, and abuse. Typically associated with methampheta-mine production, drug-endangered children are exposed not only to abuse and neglect but also to fires, explosions, and physical health hazards such as toxic chemicals. In 2009, 980 children were reported to the El Paso Intelligence Center (EPIC) as present at or affected by methamphetamine laboratories, including 8 who were injured and 2 who were killed at the laboratories. These statis-tics do not include children killed by random gunfire associated with drug activity or who were physically or sexually abused by a "caretaker" involved in drug trafficking or under the influence of drugs.
16
SAMHSA Joins Together with National Behavioral Health
Provider Associations to Promote Health Recovery
The Substance Abuse and Mental Health Services Administration (SAMHSA) recently approved awards to five national behavioral healthcare provider associations to hasten awareness, acceptance, and adoption of recovery-based practices in the delivery of mental health services. The five awards represent a major new outreach by SAMHSA to directly engage key behavioral health professional groups in its on-going efforts to fundamentally improve the provision of behavioral healthcare services. The following national profes-sional organizations will receive funding for the next 5 years to develop recovery-oriented educational materials and train thousands of psychiatrists, psychologists, psychiatric nurses, social workers, and peer specialists:
American Psychiatric Association American Psychological Association American Psychiatric Nurses Association
Council on Social Work Education National Association of Peer Specialists
The five awards are part of SAMHSA’s new Recovery to Practice project that is in support of the agency’s strategic initiative to enhance the nation’s behavioral health workforce. “Through this new initiative we are retooling the behavioral health workforce by applying the principles of recovery to direct care practice,” said SAMHSA Administrator Pamela S. Hyde, J.D. “Critical components of mental health recovery such as peer support and self-empowerment will be expanded in the workforce to help clients build on their own strengths and create positive life changes.” In addition to material development and professional training, the Recovery to Practice effort will establish an on-line recovery resource center for behavioral health professionals that will enable them to access important research and practical information on mental health recovery-based practices and receive publications and participate in periodic web-based training seminars to enhance their clinical practices.
The project builds on SAMHSA’s National Consensus Statement on Mental Health Recovery (http://mentalhealth.samhsa.gov/
Call for Volunteers!
6A is looking for volunteers that would like to help promote the 21st Annual Recov-ery Month here at the VA.
If you would like to see what is going on, please talk to Fran Hodgkins , or Hal Sykes, or Daisy Coleman.
We have lots of free materials for you to get started.
We will be having a planning meeting soon!...September is only 3 months away! Sign up now!
17
18
Non‐Recovery Based Interactions
Practice Scripts for July
1.PRAISING APPROPRIATE BEHAVIOR
“When we reinforce adaptive behav‐
iors, they are more likely to occur.”
•Positive Verbal's
•Example: “You did a great job!”
•Example: “It’s great to see you see
you doing that!”
•Positive Non‐verbal's
•Example: smiling, thumbs up, nod‐
ding of head.
2. PROMPTING
•Instead of using Activity Demand or
Limit Setting.
Used when behavior maladaptive to
context or content (e.g., talking
loudly, making demands, odd behav‐
ior, etc.). Gives Veterans CHOICES.
• Example: “Specify X, if X then
something bad happens. However, if
Y, something good happens.”
• Example: Joe yells during a conver‐
sation.
• Staff: “Joe, you are yelling. If you
continue to yell, I can’t talk to you;
however, if you speak more softly,
I’ll be happy to keep talking.”
Next month 2 more practice scripts
will be featured for you to practice.
If you want to learn more, please
see the ARTE book at the nurses’
stations. Thank You...Fran
From a PowerPoint by: Dr. Justin Springer PhD
1) Negative Non‐Verbals—
Frowning, grimacing, scowling. If we demon‐
strate a negative affect, we are modeling
this behavior for Veterans.
2) Job Irrelevant Activity—
Engaging in behaviors that are not related to
treatment services. This takes away opportu‐
nities to assist and to interact with Veterans.
3) Ignoring Veterans with Appropriate Re‐
quests—
When we provide timely responses to Vet‐
eran requests, we encourage Veterans to ask
appropriately and model professionalism.
4) Negative Group References—
Statements with negative reference to a
group to which the individual belongs. Exam‐
ple: "You all are just so loud today.“
5) Negative Statements—
Giving negative expectations before the be‐
havior occurs. Example: "You can't do that
by yourself.“
6) Negative Verbals—
Any comment given in a negative, sarcastic,
or condescending tone; reprimands. Exam‐
ples: “That's a lousy idea;” “Can’t you see
that I’m busy.”
7) Activity Demand (do)/Limit Setting (stop)
Any request or demand requiring the Vet‐
eran to perform some sort of activity or to
stop doing something. Can be stated in a
positive or negative way [LS = 64% of aggres‐
sive indicents; AD = 34% aggressive incidents
(see Cheung, et al., 1996; Bjorkly, 1999;
Marth, 2009)].
Examples: “Lets take a walk down the hall‐
way and talk,”
“You need to go and take your medication
now.”
“Come here, I need to check your vitals.”
“Please don’t do that anymore.”
“You need to take your jacket off.”
From the Editor,
Remember, changing patters of communica‐
tion takes a focused effort. However, if you
can master the communication skills that are
needed in the ARTE then you will be able to
communicate in a recovery oriented way
that helps the veterans and supports their
wellness. AND you will be a better communi‐
cator with your friends and your family. It is
a win/win situation. Try it, you’ll like it!....Ed.
Things not to do when working with our veterans in the recovery environment
Recovery Model Behaviors
19
Parts of MH Handbook on Recovery
EYE ON IT:
Relapse Prevention
Recovery Moment
Monthly Pick
Recovery Is...
“What people believe because of a
diagnosis of a mental illness is often
more disabling than the illness itself.”
“It is about serving America’s Veterans
and partnering with them to restore
and improve their lives.”
Recovery is not “something else to do.”
Recovery is the point and organizing
principle of all our work.
5Patient Care ServicesDepartment of Veterans Affairs
…A Continuum of Care
Uniform MH Services Handbook
General specifications state:Mental health is essential to overall health…, andmental health services must be recovery oriented.
This applies to all VA mental health services Built upon the 2003 President’s New Freedom
Commission Report, and the 2004 VA Comprehensive Mental Health Strategic Plan
Lays a strong foundation for current goals of providing Veteran-centric, results-driven, and forward-looking services
8
Uniform MH Services Handbook
Emphasizes rehabilitation and recovery for all, and everywhere (inpatient, outpatient, residential)
Strongly encourages the formation of local Veterans Mental Health Councils to give input about local needs and operations
Includes a special section outlining core psychosocial rehab principles and services including:
Local Recovery Coordinators PRRC
Peer Support Services Family Involvement
CWT: TWE and SE MHICM
12
Recovery
“Mental health recovery is a journey of healing and transformation enabling a person with a mental health problem to live a meaningful life in a community of the person's choice while striving to achieve ... full potential.”
Relapse Prevention: A cognitive‐
behavioral therapy developed for the
treatment of problem drinking and
adapted later for cocaine addicts. Cog‐
nitive‐behavioral strategies are based
on the theory that learning processes
play a critical role in the development
of maladaptive behavioral patterns. In
Relapse Prevention Therapy, individu‐
als learn to identify and correct prob‐
lematic behaviors. RPT encompasses
several cognitive‐behavioral strategies
that facilitate abstinence as well as
provide help for people who experi‐
ence relapse.
“Hope is Faith
holding out it’s
hand in the
dark.” ~George Iles~
20
(OAKBROOK TERRACE, Ill. – June 3, 2010) FOR IMMEDIATE RELEASE
A new Joint Commission Sentinel Event Alert warns that health care facilities today are being confronted with steadily increasing rates of crime, including
assault, rape and murder.
The Sentinel Event Alert urges greater attention to the issue of violence and to controlling access to facilities to protect patients, staff and visi‐
tors, noting that assault, rape and homicide are consistently in the top 10 types of serious events reported to The Joint Commission. The Alert
cautions that the actual number of violent incidents is significantly under‐
reported and ad‐ vises organizations to mandate the reporting of all real
or perceived threats.
To prevent vio‐ lence in health care facilities, The Joint Commission’s
Sentinel Event Alert newsletter suggests that facilities take a series of
13 specific steps, including the following:
Evaluate the facil‐ ity’s risk for violence examining the campus, reviewing
crime rates and surveying employees about their perceptions of risk.
Take extra security precautions in the emergency department, especially if
the facility is in an area with a high crime rate or gang activity. Precau‐
tions might include uniformed security guards, scanning people entering
the building for weapons and inspecting bags.
Conduct thorough background checks of prospective employees and staff.
Report crime to law enforcement.
“Health care facilities should be places of healing, not harm. But, unfortunately, health care settings are not immune from the types of vio‐
lence that are found in the other areas of our lives,” says Mark R. Chassin, M.D., M.P.P., M.P.H., president, The Joint Commission. “The recom‐
mendations in this Alert give health care institutions and caregivers specific strategies to take action that will keep everyone safer.”
In addition to the specific recommendations contained in the Alert, The Joint Commission urges hospitals to comply with the requirements
described in its accreditation standards to prevent violence. The standards require accredited health care facilities to have a security plan as
well as conduct violence risk assessments, develop strategies to prevent violence and have a response plan when a violent episode occurs. The
Joint Commission’s standards also are clear that patients have a right to be free from neglect, exploitation, and verbal, mental, physical and
sexual abuse.
The warning about violence in health care facilities is part of a series of Alerts issued by The Joint Commission. Much of the information
and guidance provided in these Alerts is drawn from The Joint Commission’s Sentinel Event Database, one of the nation’s most comprehensive
voluntary reporting systems for serious adverse events in health care. The database includes detailed information about both adverse events
and their underlying causes. Previous Alerts have addressed maternal deaths, health care technology, anticoagulants, wrong‐site surgery,
medication mix‐ups, health care‐associated infections, and patient suicides, among others. The complete list and text of past issues of Sentinel
Event Alert can be found on The Joint Commission Web site at www.jointcommission.org.
NEWS RELEASE Media Contact: FOR IMMEDIATE RELEASE
Elizabeth Eaken Zhani
Media Relations Manager
630.792.5914
Joint Commission Alert: Violence Rising at Health Care Facilities
Controlling access, greater staff vigilance urged
For more information on violence in the workplace and for questions about annual training for the prevention and management of disruptive behaviors:
Please See: Diane Toca, 6A Staff Trainer for PMDB
21
I’ll take care of you...
I’ll help you find the right per‐
son...
That sounds really rough...
Today, let’s see if we can make
that different...
What do you think will help
make you feel better?
When would you like to get this
done?
Your nurse is “…”, but we all
take care of everyone around
here.
Today is a good day for you!
Are you warm enough?
Would you like a beverage and
a snack while you are waiting?
Are you comfortable?
Do you need anything else?
These comments and many others
like these are the basis of good cus‐
tomer service and the reason for
CARITALK.
When focusing on the “YOU”, the
concepts of the Acute Recovery
Treatment Environment is realized.
We are not here to be control freaks.
We are not here to judge.
We ARE here to teach and to heal;
through the experiences of each
other.
Follow the guidelines from Dr. Springer. And
use them for CARITALK.
CARITALK
You can start with improving your patient
experience by using talking with your heart.
I call it CARITALK©.
CARITALK is the synthesis of the Caritas The‐
ory, Recovery interventions, and Heart‐
Math™ all rolled into one. It is an easy way
to communicate empathy, attunement, and
caring to your veterans and to each other.
How many times have you heard a veteran
say to you
“I’m in pain...I need more medications!”
You respond,
“Where is it? Rate your pain on a scale
of One to Ten, and /or I’ll call the doc‐
tor.”
Your response is not wrong, but it does not
convey caring and warmth the patients need
or expect. That’s because you were talking
out of your “headspace” and not your
heartspace”.
A CARITALK response would start with an
empathetic reflection:
“That must be so uncomfortable for
you.” (Reflecting with your heart)
Can you tell me Where is it? Rate your
pain on a scale of One to Ten, and I’ll
get you some medicine or call the doc‐
tor.” (Head = Assessment)
Then close it with another heart statement
like,
(Continued from page 4) “I will take care of you, so let me find
out what we can do.” (Cooperative
Planning with reassurance from the
heart)
I this manner the patient “feels” the caring
from the heart, not just the impersonal
“head” content.
Every wonder why doctors used to be so
bad at bedside manners and why nurses are
getting worse all the time? Because of all
the intellectual “head” statements they use.
For this month I challenge you to try some
CARITALK, as see what it does for you, and
your veterans.
In the end, it’s all about the veteran experi‐
ence here at the VA. It’s all about the ability
to decrease anxiety as much as possible to
help the veterans heal.
And the message from Cleveland was loud
and clear...the patient experience heals. We
are but one isolated incident in the lives of
our veterans, and yet a momentous person
in the extended stay of a hospitalization.
You have the control over the experience
your patient receives.
You are the healers, and you are the gate‐
keepers of the human experience on this
locked ward.
You are the secretaries and nurses, doctors
and technicians, food service workers and
service chiefs of the VA.
You are the experience of the VA., and with‐
out you the VA is merely a big empty build‐
ing.
What you fill it with … is up to you.
Namaste` …………………………………...Fran
CARITALK Phrases
Conference Coverage at the Cleveland Clinic
Continued from

22
A note from the internet @
VAnursescare.com
From: andrea Message: I met Jean Watson. She is caring and noted the spirit in me immediately. I am
so happy that nurses are remembering the way to nourish our own souls from the souls within the wrecked bodies of our
patients. We receive gifts of this from the patients, and they receive our gift. So grateful to be of sound enough mind and body to be the caretaker/caregiver...of the bodies which may be close to death....within the hands of suffer‐ing.....maybe even unrecognizable to their loved ones......so grateful to be able to witness and advocate......so grateful to recieve the gifts of wisdom from the bar‐dos of hell...so grateful to irm the hu‐manity and the god within all of us. The patient nurse relationship is a sacred bond. I pray I may execute it with the fullest prescence every day. ( It would also be nice to spell correctly some‐times).......I love you all...........
Join the American Psychiatric Nurses Association (APNA)
Fran Hodgkins is on the Board of Directors for APNA‐Texas and invites all interested nurses to join APNA.
APNA‐Texas has revitalized this year, and now working with APNA National in Arlington, VA., have created a
wonderful on‐line website designed to help you, the practicing nurse, with networking, advocacy, and more.
Membership information is available from Fran or on the web at APNA.org
This year to be held in Louisville ,Kentucky. October 13‐16
American Psychaitric Nurses Association National Conference
To see an instillation of Dale Chihuly glass sculpture in person is like falling through the looking
glass and landing in a kaleidoscope of color. His organic and flowing designs installed in the
Creekwood Botanical Garden, (just outside of Nashville, TN), are a compliment to the famous
garden built by the heiress of the Maxwell House fortune.
If you are able to travel to Nashville this summer, I suggest that you take the time to see this
amazing instillation. I really has an inspirational quality.
Dale Chihuly at Creekwood
Upcoming Events
2002 Holcombe Blvd
Houston, Texas 77586
713‐791‐1414 ph
Extension 6804
www.vanursescare.com
Related Documents











