51 Disorders of the Parathyroid Gland ANDREW ARNOLD AND ANDREW F. STEWART INTRODUCTION PARATHYROID HORMONE STRUCTURE, BIOSYNTHE- SIS, AND SECRETION The parathyroid hormone (PTH) gene is located on the short arm of chromosome 11. Its 3 exons encode mature PTH (84 amino acids), as well as its signal (25 amino acids) and "pro" (6 amino acids) peptides. The study of the structure and regulation of the PTH gene and the intricacies of PTH biosynthe- sis, posttranslational processing, and intracellular targeting have led to the accrual of a body of information that is as complete as that for any other peptide hormone. In the sections that follow, these areas are briefly reviewed as an introduction to the molecular disorders of the parathyroid gland. The reader is referred to several up-to-date extensive reviews at the end of this chapter for a more detailed treatment of the subject. The Extracellular Calcium-Sensing Receptor Increases in the serum ionized calcium inhibit the secretion of PTH. Con- versely, reductions in serum ionized calcium stimulate the cascade of events that lead to the secretion of PTH. This inverse sigmoidal relationship between serum calcium and PTH secretion is pre- cisely controlled, is the key physiologic feature of the parathyroid gland, and accounts for the tight minute-to-minute regulation of PTH secretion and the strict maintenance of serum calcium. Recently, the cloning of a parathyroid calcium receptor has been reported (Fig. 51-1). The calcium receptor is expressed in a restricted number of tissues (including the parathyroid gland, the thyroid C cell, the renal tubule, and the central nervous system [CNS]), is present on the surface of parathyroid cells, and is coupled by G proteins to the cytosolic calcium-inositol phosphate- phospholipase C intracellular signaling pathways. The receptor also has the structural features of a seven transmembrane spanning G-protein coupled receptor with a large extracellular domain and has been demonstrated using cRNA injection into Xenopus oocytes to serve as a receptor for calcium in that it can recognize extra- cellular calcium in physiologic concentrations and can couple extracellular calcium signals to appropriate intracellular signals. The gene encoding the calcium receptor has been localized to chromosome 3q. Transcriptional and Posttranscriptional Control PTH gene transcription is subject to both positive and negative regula- tion primarily through the combined regulatory effects of serum calcium concentration and of 1,25(0H)zD, the active form of vitamin D. Reductions in serum calcium and reductions in circu- From: Principles of Molecular Medicine (J. L. Jameson, ed.), ©1998 Humana Press Inc., Totowa, NJ. lating 1,25(0H)zD lead to activation of PTH gene transcription. Conversely, increases in serum calcium and in circulating 1,25(0H)zD inhibit PTH gene transcription. These effects occur during a period of hours to days and are viewed as being important in the long-term or tonic regulation of PTH secretion. PTH Biosynthesis PTH synthesis requires translation of the PTH mRNA on ribosomes, entry of the nascent preproPTH into the cistern of the endoplasmic reticulum (ER), cleavage of the signal peptide cotranslationally by signal peptidase on the lumenal side of the ER, passage of the immature peptide through the lamel- lae of the Golgi apparatus, targeting of the peptide into the secre- tory granules of the regulated secretory pathway, and cleavage of the "pro" segment of the peptide, presumably within the Golgi compartment. In addition, the quantity of stored hormone within secretory granules appears to be subject to regulation through deg- radation of mature PTH within secretory granules or within phagolysosomes, a process referred to as "crinophagy." Control of Secretion During the short term, PTH secretion is regulated by the serum ionized calcium concentration. Changes in serum calcium concentration lead to immediate (minutes) and opposite changes in PTH secretion. The key features of this acute regulation appear to be those observed in other neuroendocrine peptide secretory systems (i.e., storage of preformed, completely processed hormone in dense core secretory granules, with secre- tory granule fusion to the cell membrane leading to immediate secretion) with one important difference: in most neuroendocrine cell types, fusion of secretory granules with the cell membrane is triggered by an increase in cytosolic calcium. The reverse is true in the parathyroid. The cellular mechanisms governing this inverse secretion-stimulus coupling in the parathyroid gland are incom- pletely understood. FAMILIAL HYPOCALCIURIC HYPERCALCEMIA AND NEONATAL SEVERE HYPERPARATHYROIDISM Familial hypocalciuric hypercalcemia (FHH, also referred to as familial benign hypercalcemia or FBH) is a disorder that is typically discovered incidentally on routine serum calcium screen- ing. Thehypercalcemiais usually mild (i.e., in the 10.5-12.0 mg/dL range), is lifelong, is generally not associated with the symptoms of hypercalcemia, and is associated with a reduction in the urinary excre- tion of calcium. Historically, patients with FHH were confused with patients with primary hyperparathyroidism, with the unfortunate con- sequence that affected patients underwent unsuccessful partial par- athyroidectomy or complete parathyroidectomy with the development of surgical hypoparathyroidism. Since the initial description of the 475

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

51 Disorders of the Parathyroid Gland
ANDREW ARNOLD AND ANDREW F. STEWART
INTRODUCTION PARATHYROID HORMONE STRUCTURE, BIOSYNTHE
SIS, AND SECRETION The parathyroid hormone (PTH) gene is located on the short arm of chromosome 11. Its 3 exons encode mature PTH (84 amino acids), as well as its signal (25 amino acids) and "pro" (6 amino acids) peptides. The study of the structure and regulation of the PTH gene and the intricacies of PTH biosynthesis, posttranslational processing, and intracellular targeting have led to the accrual of a body of information that is as complete as that for any other peptide hormone. In the sections that follow, these areas are briefly reviewed as an introduction to the molecular disorders of the parathyroid gland. The reader is referred to several up-to-date extensive reviews at the end of this chapter for a more detailed treatment of the subject.
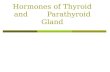
The Extracellular Calcium-Sensing Receptor Increases in the serum ionized calcium inhibit the secretion of PTH. Conversely, reductions in serum ionized calcium stimulate the cascade of events that lead to the secretion of PTH. This inverse sigmoidal relationship between serum calcium and PTH secretion is precisely controlled, is the key physiologic feature of the parathyroid gland, and accounts for the tight minute-to-minute regulation of PTH secretion and the strict maintenance of serum calcium. Recently, the cloning of a parathyroid calcium receptor has been reported (Fig. 51-1). The calcium receptor is expressed in a restricted number of tissues (including the parathyroid gland, the thyroid C cell, the renal tubule, and the central nervous system [CNS]), is present on the surface of parathyroid cells, and is coupled by G proteins to the cytosolic calcium-inositol phosphatephospholipase C intracellular signaling pathways. The receptor also has the structural features of a seven transmembrane spanning G-protein coupled receptor with a large extracellular domain and has been demonstrated using cRNA injection into Xenopus oocytes to serve as a receptor for calcium in that it can recognize extracellular calcium in physiologic concentrations and can couple extracellular calcium signals to appropriate intracellular signals. The gene encoding the calcium receptor has been localized to chromosome 3q.
Transcriptional and Posttranscriptional Control PTH gene transcription is subject to both positive and negative regulation primarily through the combined regulatory effects of serum calcium concentration and of 1,25(0H)zD, the active form of vitamin D. Reductions in serum calcium and reductions in circu-
From: Principles of Molecular Medicine (J. L. Jameson, ed.), ©1998 Humana Press Inc., Totowa, NJ.
lating 1,25(0H)zD lead to activation of PTH gene transcription. Conversely, increases in serum calcium and in circulating 1,25(0H)zD inhibit PTH gene transcription. These effects occur during a period of hours to days and are viewed as being important in the long-term or tonic regulation of PTH secretion.
PTH Biosynthesis PTH synthesis requires translation of the PTH mRNA on ribosomes, entry of the nascent preproPTH into the cistern of the endoplasmic reticulum (ER), cleavage of the signal peptide cotranslationally by signal peptidase on the lumenal side of the ER, passage of the immature peptide through the lamellae of the Golgi apparatus, targeting of the peptide into the secretory granules of the regulated secretory pathway, and cleavage of the "pro" segment of the peptide, presumably within the Golgi compartment. In addition, the quantity of stored hormone within secretory granules appears to be subject to regulation through degradation of mature PTH within secretory granules or within phagolysosomes, a process referred to as "crinophagy."
Control of Secretion During the short term, PTH secretion is regulated by the serum ionized calcium concentration. Changes in serum calcium concentration lead to immediate (minutes) and opposite changes in PTH secretion. The key features of this acute regulation appear to be those observed in other neuroendocrine peptide secretory systems (i.e., storage of preformed, completely processed hormone in dense core secretory granules, with secretory granule fusion to the cell membrane leading to immediate secretion) with one important difference: in most neuroendocrine cell types, fusion of secretory granules with the cell membrane is triggered by an increase in cytosolic calcium. The reverse is true in the parathyroid. The cellular mechanisms governing this inverse secretion-stimulus coupling in the parathyroid gland are incompletely understood.
FAMILIAL HYPOCALCIURIC HYPERCALCEMIA AND NEONATAL SEVERE HYPERPARATHYROIDISM
Familial hypocalciuric hypercalcemia (FHH, also referred to as familial benign hypercalcemia or FBH) is a disorder that is typically discovered incidentally on routine serum calcium screening. Thehypercalcemiais usually mild (i.e., in the 10.5-12.0 mg/dL range), is lifelong, is generally not associated with the symptoms of hypercalcemia, and is associated with a reduction in the urinary excretion of calcium. Historically, patients with FHH were confused with patients with primary hyperparathyroidism, with the unfortunate consequence that affected patients underwent unsuccessful partial parathyroidectomy or complete parathyroidectomy with the development of surgical hypoparathyroidism. Since the initial description of the
475

476 SECTION VII / ENDOCRINOLOGY
0 ~~~~
§ ~.J 2 X(4) X(S) X~
Hydrophobic
segment
~ X(10) 8 N M
8 0 ~ v ~ ~
M ~~xxxJf
~ ~~iiACXY~ n&~ca~~~~~eo~~xx~~~oo~oooxxx~~xx~xxooax~CM~~x~xxr.od
0 Cysteine 't= N-glycosylation
• Conserved residue s Stop mutation
... Acidic residue X Familial hypocalciuric hypercalcemia
4j) Protein kinase C site * Activating mutation
X(l) - Arg63Met
X(2) - Arg67Cys *(3) - Glu128Aia X(4) - Thr139Met
X(S) - Gly144Giu
X{6) - Arg186Gin
X{7) - Asp216Giu
X{8) - Tyr219Ser
X{9) - Arg228Gin
X{10) - Glu298Lys
S(11) - Ser608Stop
X{12)- Ser658Tyr X{13) - Gly678Arg
X{14)- Pro749Arg
X{15) - Arg796Trp
X{16)- Val81811e
Figure 51-1 The structure of the calcium receptor. This figure shows the structure of the bovine calcium receptor or sensor. The important structural features are the seven putative transmembrane-spanning domains, the extracellular amino-terminal domain, and the cytoplasmic carboxy-terminus. As can be seen from the key within the figure, both activating (causing hypoparathyroidism) and inactivating (causing familial hypocalciuric hypercalcemia) mutations can occur. (Reproduced with permission from Brown eta!. N Eng! J Med 1995;333:234-240.)
syndrome in the 1970s, it has become clear that these patients do have a mild form of primary hyperparathyroidism with slightly elevated or inappropriately normal serum PTH concentrations, that they have inappropriately efficient renal reabsorption of calcium, that the parathyroid glands appear to have a defective ability to sense the hypercalcemia, and that multiple family members are typically involved, usually in an autosomal dominant fashion.
Recently, several groups have demonstrated that inherited inactivating mutations in the parathyroid cell surface calcium receptor appear to be responsible for the features of the syn-
drome in most affected kindreds (Fig. 51-1). The responsible mutations generally involve either the extracellular domain (presumably adversely influencing calcium binding to the receptor) or one of the transmembrane loops (presumably interfering with conformational changes that in turn lead to the activation of signal transduction pathways). In general, affected patients have been heterozygous for the mutant calcium receptor allele. Interestingly, however, infants have been described who appear to have a particularly malignant form of the syndrome, characterized by severe hypercalcemia (sometimes in the 20-mg/dL range)

CHAPTER 51 / PARATHYROID DISORDERS 477
and prominent parathyroid hypercellularity. This form of the syndrome has been referred to as neonatal severe hyperparathyroidism (NSHPT). The syndrome in some of these infants has now been reported to result from a double dose of the mutant, inactivated calcium receptor gene, events that resulted in turn from consanguineous parentage.
In support of the concept that inactive mutant forms of the calcium receptor are responsible for the syndrome, it has been reported that expression in Xenopus oocytes of calcium receptors containing the same mutations as those encountered in humans with the disease results in impaired ability to sense extracellular calcium Also, an FHH-like phenotype is found in mice whose extracellular calcium receptor gene has been heterozygously knocked out, and a more severe phenotype similar to NSHPT is seen in mice with no functional copy of the gene. At the time of this writing, 15 mutations have been described in the calcium receptor in families with FHH (Fig. 51-1 ). In addition, other FHH families who map to the 3q region have been defined that do not display mutations in the coding region of the calcium receptor gene. These findings suggest that mutations in the intronic or regulatory regions of the calcium receptor gene may explain additional kindreds. Further, it is important to note that mutations in other genes will undoubtedly be demonstrated in the future; for some families with what appears to be standard FHH, the disease locus maps to chromosome 19p or other locations distinct from chromosomes 19 or 3. It is presumed that the genes at these other loci encode other proteins that play a role in the calcium sensing machinery.
HEREDITARY FORMS OF HYPOPARATHYROIDISM The majority of patients with hypoparathyroidism have surgi
cal or acquired autoimmune hypoparathyroidism. In contrast to these acquired forms of hypoparathyroidism, familial forms of congenital and acquired hypoparathyroidism have been described. These can be subdivided into familial syndromes in which hypoparathyroidism is accompanied by abnormalities in multiple other organ systems, and familial forms of hypoparathyroidism that are unaccompanied by other abnormalities (Table 51-1 ). These various syndromes are discussed below.
FAMILIAL VARIETIES OF HYPOPARATHYROIDISM ASSOCIATED WITH MULTIPLE ORGAN SYSTEM ABNORMALITIES These syndromes are of interest in that they represent genetic syndromes associated with hypoparathyroidism, but given their multisystem abnormalities, it is intuitive that the parathyroid gland abnormalities are not intrinsic to defects within the parathyroid gland but are in some fashion secondary to other developmental or regulatory abnormalities.
Hypoparathyroidism Associated With the Polyglandular Failure Syndrome This syndrome is composed of at least two subtypes. Hypoparathyroidism is most often associated with the pediatric variant of the syndrome, termed the HAM syndrome, an acronym for the hypoparathyroidism, Addison's disease, mucocutaneous candidiasis syndrome. The syndrome is an autoimmune disease that is associated with autoimmune destruction of the parathyroid glands and the adrenal glands, and is coupled with T-cell abnormalities that lead to mucocutaneous candidiasis. It is inherited in an autosomal recessive fashion, and is linked to chromosome 2lq22.3. Circulating antibodies directed against parathyroid surface antigens have been difficult to demonstrate. One recent preliminary report suggests that a cell surface target of circulating autoimmune antisera in some affected patients is the calcium receptor.
Table 51-1 Hereditary Forms of Hypoparathyroidism
Familial hypoparathyroidism associated with multiple organ system abnormalities
Polyglandular failure type I or HAM syndrome DiGeorge syndrome Renal dysgenesis/sensorineural deafness syndromes
Autosomal recessive Autosomal dominant
Isolated familial hypoparathyroidism syndromes X -linked hypoparathyroidism Autosomal recessive syndromes
PTH gene intron splice site mutation Others
Autosomal dominant syndromes Parathyroid hormone signal peptide mutation Constitutively activating calcium receptor mutations Others
The DiGeorge Syndrome The DiGeorge syndrome (see Chapter 120) is a complex of developmental disorders centered on the third and fourth branchial pouches that includes: (1) cardiac and conotruncal defects (such as ventricular septal defects, tetralogy of Fallot); (2) T-cell deficiency as a result of partial or incomplete development of the thymus gland; (3) craniofacial abnormalities; and (4) partial or complete hypoparathyroidism as a result of congenital absence or hypoplasia of the parathyroid glands. It may occur in both sporadic and inherited forms. The pattern of inheritance in the latter is consistent with an autosomal dominant mode of transmission. The vast majority of inherited and sporadic cases display deletions or translocations in the 22q 11 region. The broad spectrum of abnormalities in patients with the DiGeorge syndrome together with the large region of DNA typically affected by these deletions and rearrangements suggests that defects in multiple adjacent genes at 22q 11 may collectively account for the abnormalities observed. Candidate genes include DGCR2/LAN, which appears to encode a membrane-bound adhesion molecule; the CTP (human citrate transporter protein) gene; and DGCR3, which encodes what appears to be a DNA-binding protein. The last of these is particularly interesting for it appears to span the region of a 22q 11 rearrangement breakpoint, and therefore its disruption seems likely to be functionally important.
Hypoparathyroidism Associated With Renal Dysgenesis and Sensorineural Hearing Loss This syndrome has been reported by several groups. Both autosomal dominant and autosomal recessive patterns of inheritance have been described. Linkage studies defining chromosomal locations for the putative responsible gene or genes have not been described.
FAMILIAL ISOLATED HYPOPARATHYROIDISM In contrast to the syndromes described above, several forms of familial hypoparathyroidism have been described in which hypoparathyroidism is the sole abnormality. These syndromes will certainly prove to represent a group of several disorders with differing molecular pathogenesis. Some are still poorly defined in molecular terms such as most autosomal recessive forms of the disorder and certain autosomal dominant forms. Others are partially defined in molecular terms, such as the X-linked form of the syndrome, which has recently been mapped to the Xq26-q27 region. Still others, including an autosomal dominant form, are well-understood in genetic and biochemical terms. In this situa-

478 SECTION VII I ENDOCRINOLOGY
Break-PTH Coding PTH Coding
PTH 5' Regulatory
Break- PTH 5' Regulatory
PRA01/Cyclin 01 PRA01/Cyclin 01
Normal Inverted
Figure 51-2 Schematic diagram illustrating the pericentromeric inversion of chromosome 11 deduced to have caused the observed rearrangement involving the PTH gene and the PRADJ gene in a subset of parathyroid adenomas. The tumor's other copy of chromosome 11, which contains an intact PTH gene, is not shown. (Reproduced with permission from Arnold A. Genetic basis of endocrine disease 5: molecular genetics of parathyroid gland neoplasia. J Clin Endocrinol Metab 1993;77: 1108-1112.)
tion hypoparathyroidism results from a mutation that causes a Cys to Arg substitution in the middle of the hydrophobic core of preproPTH's signal peptide. The resultant mutant form of preproPTH is unable to be processed with normal efficiency. One curious aspect of this disorder is the question as to why a disabling mutation in only one allele of the PTH gene should lead to hypoparathyroidism. It is possible that accumulation of bound but poorly processed mutant preproPTH molecules in the endoplasmic reticulum might deny access of the normal allele's product to the processing apparatus, or otherwise interfere with the function of the parathyroid cell. Interestingly, this preproPTH mutation was the first signal peptide mutation reported to cause human disease, and signal peptide mutations have subsequently been found in preprovasopressin (causing diabetes insipidus) and in Factor X (causing a coagulopathy).
A family has been described with autosomal recessive hypoparathyroidism that appears to be caused by a splice junction mutation in intron 2 of the PTH gene. The resulting mRNA would have the sequences derived from exon 2, which contains the signal peptide, spliced out, and thereby lead to the production of a PTH species that could not enter the secretory pathway.
Recently, another mechanism underlying familial isolated hypoparathyroidism has been described. With the demonstration that familial hypocalciuric hypercalcemia may result from inactivating mutations in the extracellular calcium-sensing receptor (discussed above), it was logical to speculate that some cases of hereditary hypoparathyroidism might result from activating mutations in the calcium receptor. This type of syndrome has now been reported (Fig. 51-1). As would be expected, this kindred displays an autosomal dominant pattern of inheritance, and expression of the mutant calcium receptor in oocytes leads to constitutive activation of the inositol phosphate signal transduction pathway. The host parathyroid cell, therefore, behaves as though it were being exposed to higher than normal concentration of extracellular calcium and appropriately fails to secrete PTH. Similar mutations have also been identified in cases of sporadic hypoparathyroidism.
MOLECULAR GENETICS OF PARATHYROID GLAND NEOPLASIA
Primary hyperparathyroidism is caused by excessive secretion of PTH, resulting in hypercalcemia. Patients with primary hyperparathyroidism have both an excessive parathyroid cell mass and a resetting of the setpoint by which PTH secretion is tightly coupled to the parathyroid cell's ambient calcium level. In the large majority (>80%) of patients with primary hyperparathyroidism, a single benign parathyroid tumor (adenoma) is responsible, whereas multiple hypercellular glands are present in about 15% (primary hyperplasia). Parathyroid carcinoma is extremely rare, as is the ectopic secretion of PTH from nonparathyroid tumors. A comprehensive molecular description of parathyroid tumorigenesis will eventually need to fully explain the development of these types of tumors, as well as a variety of other special features such as the increased incidence of parathyroid tumors after exposure to neck irradiation and the disease's epidemiologic weighting toward postmenopausal women. Detailed molecular understanding will likely yield information of diagnostic, prognostic, preventative, or therapeutic importance, and recent progress gives cause for optimism in this regard.
CLONALITY IN PARATHYROID TUMORIGENESIS The monoclonality or polyclonality of human tumors is an informative reflection of their underlying pathogenetic mechanism. Early data measuring isoforms of the X-chromosome-encoded protein G6PD in parathyroid adenomas in heterozygous women had indicated that apparently single parathyroid adenomas were polyclonal growths, likely to result solely from a generalized growth stimulus. These results, however, proved to be misleading, since modern molecular methods have now solidly established the monoclonality of typical parathyroid adenomas, both by X-chromosome inactivation analysis and by the direct demonstration of monoclonal genetic alterations in parathyroid adenomas (see below). Monoclonality highlights the concept that parathyroid adenomas are true neoplasms, consistent with clinical experience that surgical removal of the enlarged gland is generally curative. Neoplasia is a genetic disease, with most relevant DNA damage occurring somati-

CHAPTER 51 / PARATHYROID DISORDERS 479
Normal:
-----5-'-re_g_u-la_t_o-~--re_g_i_o_n_o_f_P_T_H __ G_e_n_e--------------~~-----
t PTH Exons
No PTH gene transcription in ovarian tissue
Rearranged:
New regulato~ DNA from a distant locus
t PTH Exons
Significant transcription of PTH gene is activated/permitted in ovarian tissue
Figure 51-3 Molecular pathology of the ectopic production of PTH by an ovarian cancer. Schematic diagram of the normal PTH gene region (top) and the rearranged, amplified PTH gene region (bottom) in a PTH-secreting ovarian tumor. The bold "X" represents the breakpoint of the DNA rearrangement. (Reproduced with permission from Arnold A. Genetic basis of endocrine disease 5: molecular genetics of parathyroid gland neoplasia. J Clin Endocrinol and Metab 1993;77: 1108- 1112.)
cally. Monoclonality implies that the necessary accumulation of multiple mutations in a tumor progenitor cell occurs only rarely in a large population of cells within a tissue, conferring a selective growth advantage critical in tumor outgrowth or clonal evolution. The search is now on for the specific oncogenes and tumor suppressor genes that are clonally activated or inactivated, respectively, in parathyroid tumors. Two notable successes and several important leads, described below, have already emerged in this search.
The clonal status of parathyroid tumors other than adenomas has also been investigated. As expected, parathyroid carcinomas, like all cancers, are monoclonal. Much more surprisingly, however, a substantial percentage of parathyroid tumors in the setting of primary hyperplasia and severe secondary hyperparathyroidism of uremia has recently been shown to be monoclonal, indicating that clonal somatic mutations have given selected cells a growth advantage over their already hyperplastic neighbors. Monoclonality in the majority of MEN -!- associated parathyroid tumors examined suggests a similar process in this syndrome. It is quite conceivable that the "conversion" from polyclonality to monoclonality may be a key factor in the increasing autonomy of PTH secretion that develops in many hemodialysis patients, making them refractory to standard medical therapy. Future identification of the specific molecular culprits in such clonal outgrowths may lead to rational new therapy or preventative measures for this important clinical problem.
GENETIC DERANGEMENTS IN BENIGN PARATHYROID TUMORS
THE CYCLIN D1/PRAD1 ONCOGENE CyclinD1/PRAD1, to date the only oncogene implicated in sporadic parathyroid neoplasia, was discovered by virtue of its proximity to a clonal chromosomal breakpoint in a subset of parathyroid adenomas. Fig. 51-2 is a diagram of this chromosomal inversion, which causes overexpression of the cyclin D liP RAD 1 gene by placing it in proximity to the strong tissue-specific enhancer of the PTH gene.
Cyclin D1/PRAD1 is recognized to have a crucial role in regulating progression through the G 1 phase of the cell division cycle. To do so, the cyclin Dl protein is believed to act as an activating regulatory subunit for its partner cyclin-dependent kinase(s), cdk4 or cdk6. One action of active cdk4 or cdk6 may be phosphorylation
of the retinoblastoma gene product pRB, moving the cell toward S phase, but this mechanism has not yet been established in parathyroid tissue. A still-uncertain fraction of parathyroid adenomas contain an activated form of the cyclin D1/PRAD 1 oncogene; one recent study showed overexpression of the cyclin D 1 protein in about 20% of adenomas. Cyclin Dl activation has also been incriminated in a variety of other human tumors, including B-cell lymphoma, breast, and esophageal cancers.
PUTATIVE TUMOR SUPPRESSOR GENES Inactivation of both alleles of a tumor suppressor gene is typically necessary to sufficiently eliminate its antioncogenic product, and somatic deletion of a sometimes large stretch of DNA that includes the relevant gene is a common inactivating mechanism. Thus, identification of genomic regions that are clonally and nonrandomly lost in parathyroid adenomas can point to the locations of putative parathyroid tumor suppressor genes. A growing proportion, now more than 70%, of parathyroid adenomas can be shown to bear at least one such clonal chromosomal defect.
The most common molecular defect described to date in parathyroid tumors is allelic loss on chromosome arm 1 p, found in about 40% of adenomas; the putative tumor suppressor gene in this region has not yet been isolated. About 25% of adenomas contain allelic losses of chromosome 11 DNA, the region to which the MEN-1 gene has been mapped. The gene responsible for MEN-1 has been cloned using positional cloning techniques. The gene product, menin, is a 61 0-amino acid protein that lacks both a signal sequence and nuclear localization signal. Mutations in the affected individuals predict loss of function of the protein, suggesting that the MEN-1 gene is a tumor suppressor gene. In a recent study of parathyroid tumors not associated with MEN-1 , somatic mutations in MEN-1 were present in 4 of 24 adenomas. All of the tumors with mutations in MEN-I exhibited loss of heterozygosity on llq 13 at the MEN-1 locus. Thus, the tumors were hemizygous for the mutant allele. Still other regions of nonrandom clonal allelic loss in parathyroid adenomas, highlighting the locations of novel tumor suppressor genes, have been found on chromosome arms lq, 6q, 9p, and 15q. These data emphasize the molecular heterogeneity underlying parathyroid adenomatosis.
OTHER GENETIC ASPECTS Some genes responsible for rare inherited predispositions to certain tumors have also proved

480 SECTION VII / ENDOCRINOLOGY
important in more common, sporadic forms of the same tumors. The MEN-I gene, as mentioned above, is an example. The recent discovery of Ret proto-oncogene germline mutation in MEN-2A made this gene a candidate for involvement in nonfamilial hyperparathyroidism. However, studies have so far failed to document somatic Ret mutations in sporadic parathyroid adenomas. Similarly, inactivating mutations of the extracellular calcium-sensing receptor have been sought but not found in sporadic adenomas. It remains possible that somatic mutation in other genes involved in the calcium-sensing pathway may contribute to adenoma development, with the primary clonal setpoint defect driving the proliferative response. Finally, the gene responsible for an autosomal dominant predisposition to recurrent parathyroid adenomas and benign jaw tumors has been mapped to the long arm of chromosome 1; its ultimate identification may also provide insight into more common forms of hyperparathyroidism.
MOLECULAR PATHOGENESIS OF PARATHYROID CARCINOMA
The discovery that the cell-cycle regulator cyclin DJ/PRADl can be involved in parathyroid tumorigenesis has raised the possibility that other cell-cycle regulatory genes may also contribute to parathyroid neoplasia. One example, the RB tumor suppressor gene implicated in retinoblastoma and a narrow spectrum of often aggressive malignancies, may be a key factor in the pathogenesis of many parathyroid carcinomas, although a neighboring gene on 13q might be the target of the frequent DNA deletions in this region. Genetic lesions that are confirmed to be enriched in malignant as opposed to benign parathyroid tumors could be clinically useful in molecular diagnosis, given the difficulties in making such distinctions histopathologically.
ECTOPIC SECRETION OF PTH The ectopic secretion of PTH by nonparathyroid tumors is a
rare cause of primary hyperparathyroidism. The molecular basis of ectopic PTH production in one such case, an ovarian carcinoma, was found to be a DNA rearrangement in the regulatory region of the tumor's PTH gene (Fig. 51-3). Similar detailed molecular pathology has yet to be described in other examples of human ectopic hormone excess, and might involve analogous DNA rearrangements or, alternatively, a change in the tumor tissue's characteristic DNA-binding proteins.
SELECTED REFERENCES Aaltonen J, Bjorses P, Sandkuijl L, Perheentupa J, Peltonen L. An auto
somal locus causing autoimmune disease: autoimmune polyglandular disease type I assigned to chromosome 21. Nat Genet 1994;8:83-87.
Agarwal SK, Kester MB, Debelenko LV, et a!. Germline mutations ofthe MEN 1 gene in familial multiple endocrine neoplasia type 1 and related states. Hum Mol Genet 1997;6: 1169-1175.
Ahn TG, Antonarakis SE, Kronenberg HM, Igarashi T, Levine MA. Familial isolated hypoparathyroidism: a molecular genetic analysis of 8 families with 23 affected persons. Medicine 1986;65:73-81.
Arnold A. The cyclin D 1/PRAD 1 oncogene in human neoplasia. J Invest Med 1995;43:543-549.
Arnold A. Genetic basis of endocrine disease 5: molecular genetics of parathyroid gland neoplasia J Clin Endocrinol Metab 1993 ;77: II 08-1112.
Arnold A, Brown MF, Urena P, Gaz RD, Sarfati E, Drueke TB. Monoclonality of parathyroid tumors in chronic renal failure and in primary parathyroid hyperplasia J Clin Invest 1995;95:2047-2053.
Arnold A, Horst SA, Gardella TJ, Baba H, Levine MA, Kronenberg HM. Mutation of the signal peptide-encoding region of the preproparathyroid hormone gene in familial isolated hypoparathyroidism. J Clin Invest 1990;86: 1084-1087.
Baron J, Winer KK, Yanovski JA, eta!. Mutations in theCa (2+ )-sensing receptor gene cause autosomal dominant and sporadic hypoparathyroidism. Hum Mol Genet 1996;5:601-606.
Bilous RW, Murty G, Parkinson DB, eta!. Brief report: autosomal dominant familial hypoparathyroidism, sensorineural deafness, and renal dysplasia. N Eng! J Med 1992;327:1069-1074.
Bjorses P, Aaltonen J, Vikman A, eta!. Genetic homogeneity of autoimmune polyglandular disease type I. Am J Hum Genet 1996;59:879-886.
Brown EM, Gamba G, Riccardi D, eta!. Cloning and characterization of an extracellular Ca2+ -sensing receptor from bovine parathyroid. Nature 1993;366:575-580.
Brown EM, Pollak M, Seidman CE, eta!. Calcium-sensing cell-surface receptors. N Eng! J Med 1995;333:234-240.
Budarf ML, Collins J, Gong W, eta!. Cloning a balanced translocation associated with DiGeorge syndrome and identification of a disrupted candidate gene. Nat Genet 1995;10:269-278.
Chandrasekharappa SC, Guru SC, Manickam P, eta!. Positional cloning of the genefor multiple endocrine neoplasia-type 1. Science 1997 ;276: 404--407.
Cryns VL, Yi SM, Tahara H, Gaz RD, Arnold A. Frequent loss of chromosome arm lp DNA in parathyroid adenomas. Genes Chromosomes Cancer 1995;13:9-17.
Dotzenrath C, The BT, Farnebo F, eta!. Allelic loss ofthe retinoblastoma tumor suppressor gene: a marker for aggressive parathyroid tumors? J Clin Endocrinol Metab 1996;81:3194-3196.
De Luca F, Ray K, Mancilla EE, et a!. Sporadic hypoparathyroidism caused by de novo gain-of-function mutations of the Ca2+-sensing receptor. J Clin Endocrinol Metab 1997;82:2710-2715.
Glover TW. CATCHing a break on 22. Nat Genet 1995;20:257,258. HeppnerC, Kester MB, Agarwal SK, eta!. Somatic mutation of the MEN!
gene in parathyroid tumours. Nat Genet 1997;16:375-378. Ho C, Conner DA, Pollak MR, et a!. A mouse model of human familial
hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Nat Genet 1995;11:389-394.
Kronenberg HM, Bringhurst FR, Segre GV, Potts JT. Parathyroid hormone biosynthesis and metabolism. In: Bilezikian JP, Marcus R, Levine MA, eds. The Parathyroids. New York; Raven, 1994; pp. 125-138.
Li Y, Song YH, Rais N, eta!. Autoantibodies to the extracellular domain of the calcium sensing receptor in patients with acquired hypoparathyroidism. J Clin Invest 1996;15:910-914.
Motokura T, Bloom T, Kim HG, eta!. A novel cyclin encoded by a belllinked candidate oncogene. Nature 1991;350:512-515.
Parkinson DB, Thakker RV. A donor splice site mutation in the parathyroid hormone gene is associated with autosomal recessive hypoparathyroidism. Nat Genet 1992;1:149-153.
Pearce SH, Williamson C, Kifor 0, et a!. A familial syndrome of hypocalcemia with hypercalciuria due to mutations in the calcium-sensing receptor. N Eng! J Med 1996; 10:1115-1122.
Pollak MR, Brown EM, Chou Y -HW, eta!. Mutations in the human Ca2+sensing receptor gene cause familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism. Ce111993;75:1297-1303.
Pollak MR, Brown EM, Estep HL, et a!. Autosomal dominant hypocalcaemia caused by a Ca2+-sensing receptor gene mutation. Nat Genet 1994;8:303-307.
Potts JT, Bringhurst FR, Gardella T, Nussbaum S, Segre GV, Kronenberg HM. Parathyroid hormone: physiology, chemistry, biosynthesis, secretion, metabolism, and mode of action. In: DeGroot LJ, ed. Endocrinology, 3rd ed. Philadelphia: WB Saunders, 1995; pp. 920-966.
Thakker RV. Molecular genetics of hypoparathyroidism. In: Bilezikian JP, Marcus R, Levine MA, eds. The Parathyroids. New York: Raven, 1994;pp. 765-779.
Szabo J, Heath B, Hill VM, et a!. Hereditary hyperparathyroidism-jaw tumor syndrome: the endocrine tumor gene HRPT2 maps to chromosome lq21-q31. Am J Hum Genet 1995;56:944-950.
Related Documents