-
7/25/2019 Diseases of the Parathyroid Gland
1/48
PRIMARY HYPERPARATHYROIDISM:
ETIOLOGY:
SOLITARY ADENOMAS: ~80%: a single abnormal gland is the cause (benign neoplasm,
adenoma or a parathyroid carcinoma)
~15%: all glands are hyperfunctioning (chief cell parathyroid
hyperplasia) Others: double adenomas
MULTIPLE ENDOCRINE NEOPLASIA (MEN): MEN 1 (Wermerssyndrome): hyperparathyroidism, pituitary and
pancreatic tumors, gastric hypersecretion and PUD (Zollinger-Ellisonsyndrome)
MEN 2A: pheochromocytoma, medullary carcinoma of the thyroid,hyperparathyroidism
MEN 2B: multiple neuromas without hyperparathyroidism
-
7/25/2019 Diseases of the Parathyroid Gland
2/48
PRIMARY HYPERPARATHYROIDISM:PATHOLOGY:
ADENOMAS: Most often located in the inferior parathyroid glands
Usually 0.5 to 5 grams in size but may be as large as 10-20 grams (normalglands weigh 25 mg on average)
Chief cells are predominant in both hyperplasia and adenoma
PARATHYROID CARCINOMA may be: (1) non-aggressive-long-term survival without recurrence is common if at
initial surgery the entire gland is removed without rupture of the capsule
(2) aggressivewith distant metastases ( lung, liver, bone)
Hyperparathyroidism from a parathyroid carcinoma may be indistinguishablefrom other forms of primary hyperparathyroidism; a potential clue to thediagnosis is provided by the degree of calcium elevation (> 3.5 to 3.7mmol/Lor 14-15 mg/dL)
GENETIC CONSIDERATIONS:
As in many other types of neoplasia, 2 fundamental types of geneticdefects have been identified in parathyroid gland tumors:
(1) overactivity of protooncogenes (2) loss of function of tumor-suppressor genes
-
7/25/2019 Diseases of the Parathyroid Gland
3/48
PRIMARY HYPERPARATHYROIDISM:SIGNS and SYMPTOMS:
~80% of patients with hyperparathyroidism are asymptomatic
MANIFESTATIONS: 1. KIDNEYS:
Due either to deposition of calcium in the renal parenchyma or to recurrent nephrolithiasis
(60-70%)
Renal stones are usually composed of either calcium oxalate or calcium phosphate
Repeated episodes of nephrolithiasis or the formation of large calculi may lead to urinary
tract obstruction, infection and loss of renal function
Nephrocalcinosis may also cause decreased renal function and phosphate retention
2. BONE:
OSTEITIS FIBROSA CYSTICA- the distinctive bone manifestation
The pathognomonic histologic features are an increase in the giant multinucleated
osteoclasts in scalloped areas on the surface of the bone (HOWSHIPS LACUNAE) and thereplacement of the normal cellular and marrow elements by fibrous tissue
X-ray changes include resorption of the phalangeal tufts and replacement of the usually
sharp cortical outline of the bone in the digits by an irregular outline (SUBPERIOSTEAL
RESORPTION)
Cortical bone density is reduced while cancellous bone density, especially in the spine, is
relatively preserved
-
7/25/2019 Diseases of the Parathyroid Gland
4/48
PRIMARY HYPERPARATHYROIDISM:
3. CNS- neuropsychiatric manifestations
4. NEUROMUSCULAR MANIFESTATIONS: Proximal muscle weakness, easy fatigability, muscle atrophy
The distinguishing feature from a primary neuromuscular disorder isthe complete regression of neuromuscular disease after surgicalcorrection of the hyperparathyroidism
5. GASTROINTESTINAL MANIFESTATIONS Subtle or may present as vague abdominal complaints or as disorders
of the stomach and pancreas Duodenal ulcer in MEN 1 may be the result of associated pancreatic
tumors that secrete excessive quantities of gastrin (Zollinger-Ellisonsyndrome)
-
7/25/2019 Diseases of the Parathyroid Gland
5/48
PRIMARY HYPERPARATHYROIDISM:DIAGNOSIS:
Made by detecting an elevated immunoreactive PTH level in a patient withasymptomatic hypercalcemia
Serum phosphate is usually low, but may be normal especially if renal failure hasdeveloped
TREATMENT:
MEDICAL SURVEILLANCE vs. SURGICAL TREATMENT
SURGERYis mandatory if (+)severe hypercalcemia (3.7 to 4.5 mmol/L or 15-18mg/dL)
ASYMPTOMATIC HYPERPARATHYROIDISM:
Defined as documented (presumptive) hyperparathyroidism without signs or symptomsattributable to the disease
SURGERYis recommended by the National Institutes of Health (NIH) for the following: (1) patients 50 y/o
(2) if patient wishes to avoid surgery
(3)the guidelines recommending surgery were not present***
-
7/25/2019 Diseases of the Parathyroid Gland
6/48
PRIMARY HYPERPARATHYROIDISM:MEDICAL MANAGEMENT GUIDELINES for
ASYMPTOMATIC PRIMARY HYPERPARATHYROIDISMwho do not undergo parathyroid surgery: (1)Serum calcium measurement should be monitored
biannually
(2) Serum creatinine monitoring should be done annually
(3) Bone density measurement (lumbar spine, hip,forearm) should be undertaken annually
MEDICAL TREATMENT OPTIONS: (1) RALOXIFENE (Evista)
the 1stof the SERMS has bone protective effects in osteoporotic subjectsand increased bone density at the same time lowering the incidence ofbreast cancer compared to estrogens
(2) CALCIMIMETIC DRUGS selectively stimulate the calcium sensor and suppress PTH secretion ,
decreasing calcium levels to normal and lower PTH levels by at least 50%for > 1year of continuous use
-
7/25/2019 Diseases of the Parathyroid Gland
7/48
PRIMARY HYPERPARATHYROIDISM:GUIDELINES for PARATHYROID SURGERY in ASYMPTOMATIC PRIMARY
HYPERPARATHYROIDISM:
(1) Serum calcium >0.3mmol/L (1.0 mg/dL) above upper limit of normal
(2) 24-h urinary calcium >400 mg
(3) Creatinine clearance reduced by 30%
(4) Bone mineral density T-score < 2.5 at any site
(5) Age 1 glandis abnormal
Another approach involves a combination of preoperative sestamibi imaging, cervicalblock anesthesia, minimal surgical incision and intraoperative PTH measurement whichhas allowed successful outpatient surgical management with a clear-cut cost benefitcompared to general anesthesia and more extensive neck surgery
When parathyroid carcinoma is encountered, the tissue should be widely excised; care
must be taken to avoid rupture of the capsule to prevent local seeding of tumor cells
-
7/25/2019 Diseases of the Parathyroid Gland
8/48
PRIMARY HYPERPARATHYROIDISM:
In multiple gland hyperplasia, 2 schemes have beenproposed for surgical management: (1) total removal of 3 glands with partial excision of the 4th
gland; care is taken to leave a good blood supply for theremaining gland
(2) total parathyroidectomy with immediate transplantation of aportion of a removed, minced parathyroid gland into themuscles of the forearm, with the view that surgical excision iseasier from the ectopic site in the arm if there is recurrenthyperfunction
When a 2ndparathyroid exploration is indicated, minimallyinvasive techniques such as UTZ, CT scan and isotopescanning may be combined with venous sampling and/orselective digital arteriography, with intraoperative PTH
monitoring to guide the surgery
-
7/25/2019 Diseases of the Parathyroid Gland
9/48
PRIMARY HYPERPARATHYROIDISM:HYPOCALCEMIA after PARATHYROID SURGERY:
A decline in serum calcium occurs within 24hrs after successful surgery
Blood calcium falls to low-normal values for 3-5days until the remainingparathyroid tissue resumes hormone secretion
Once hypocalcemia signifies successful surgery, patients can be put on a high-calcium intake or be given oral calcium supplements
If serum calcium falls to
-
7/25/2019 Diseases of the Parathyroid Gland
10/48
PRIMARY HYPERPARATHYROIDISM:
MAGNESIUM DEFICIENCY after PARATHYROID SURGERY:
Magnesium deficiency may also complicate the postoperative course
Magnesium deficiency impairs PTH secretion, so hypomagnesemia shouldbe corrected whenever detected
Because the depressant effect of magnesium on central and peripheralnerve functions does not occur at levels
-
7/25/2019 Diseases of the Parathyroid Gland
11/48
LITHIUM THERAPY:
Lithium, used in the management of bipolar depression and otherpsychiatric disorders, causes hypercalcemia in ~10% of treatedpatients
The hypercalcemia is dependent on continued lithium treatment,
remitting and recurring when lithium is stopped and restarted
Long-standing stimulation of parathyroid cell replication by lithiummay predispose to the development of adenomas
Parathyroid surgery should not be recommended unlesshypercalcemia and elevated PTH level persist after lithium isdiscontinued
-
7/25/2019 Diseases of the Parathyroid Gland
12/48
FAMILIAL HYPOCALCIURIC HYPERCALCEMIA (FHH):
Also called Familial Benign Hypercalcemia
Inherited as an autosomal dominant trait
Involves excessive secretion of PTH, but does not involve a primary growth disorder of the
parathyroids
PATHOPHYSIOLOGY:
The primary defect is abnormal sensing of the blood calcium by the parathyroid gland
and renal tubule, causing inappropriate PTH secretion and excessive renalreabsorption of calcium
Many different mutations in the calcium-sensing receptor have been identified- these
mutations lower the capacity of the sensor to bind calcium, and the mutant receptors
function as though blood calcium levels were low
Excessive PTH secretion occurs from an otherwise normal gland Few clinical signs or symptoms are present, and other endocrine abnormalities are not
present
Parathyroid surgery or medical treatment seem needed to lower the calcium
The exception to the rule against parathyroid surgery is NEONATAL SEVERE
HYPERCALCEMIA
-
7/25/2019 Diseases of the Parathyroid Gland
13/48
JANSENS DISEASE:
A rare autosomal dominant syndrome and variant of hyperparathyroidism
Caused by excessive biologic activity of the PTH receptor in targettissues
Does not involve a primary growth disorder of the parathyroid glands
Manifestations:
The disorder leads to short-limbed dwarfism due to abnormalregulation of the bone growth plate
In adult life, there are numerous abnormalities in bone, includingmultiple cystic resorptive areas resembling those seen inhyperparathyroidism
Hypercalcemia and hypophosphatemia with undetectable or low PTH
levels are typically seen
-
7/25/2019 Diseases of the Parathyroid Gland
14/48
MALIGNANCY-RELATED
HYPERCALCEMIA:CLINICAL SYNDROMES and MECHANISMS of HYPERCALCEMIA:
Previously, hypercalcemia associated with malignancy was thought to be due to localinvasion and destruction of bone by tumor cells
Many cases are now known to result from the elaboration by the malignant cells ofhumoral mediators of hypercalcemia
Parathyroid hormone related protein (PTHrP) is the responsible humoral agent
MECHANISMS OPERATIVE in CANCER HYPERCALCEMIA:
(1) many solid tumors associated with hypercalcemia (squamous cell and renal tumors)produce and secrete PTHrP that causes increased bone resorption and mediate thehypercalcemia through systemic actions on the skeleton Alternatively, direct bone marrow invasion occurs with hematologic malignancies (leukemia, lymphoma,
multiple myeloma)
Lymphokines and cytokines produced by cells involved in the marrow response to the tumors promotebone resorption through local destruction
(2) HUMORAL HYPERCALCEMIA of MALIGNANCY solid tumors (cancers of the lung and kidney) in which bone metastases are absent, minimal or not
detectable clinically, secrete PTHrP, which activates PTH1R, resulting in a pathophysiology resemblinghyperparathyroidism (hypercalcemia, hypophosphatemia);
elimination or regression of the primary tumor leads to disappearance of the hypercalcemia
-
7/25/2019 Diseases of the Parathyroid Gland
15/48
MALIGNANCY-RELATED HYPERCALCEMIA:DIAGNOSIS:
Clinical suspicion that malignancy is the cause of the hypercalcemia is heightened whenthere are other paraneoplastic signs or symptoms (weight loss, fatigue, muscle weakness,
unexplained skin rash) or when symptoms specific for a particular tumor are present
Squamous cell tumors are most frequently associated with hypercalcemia (lung, kidney,
head and neck, and urogenital tract)
Radiologic examinations should focus on squamous cell tumor locations when clinical
evidence is unclear
Bone scans are useful for detection of osteolytic metastases
Bone marrow biopsies are helpful in patients with anemia or abnormal PBS
TREATMENT:
Directed to control of tumor
Reduction of tumor mass usually corrects hypercalcemia
-
7/25/2019 Diseases of the Parathyroid Gland
16/48
VITAMIN D-RELATED HYPERCALCEMIA:
Can be due to excessive ingestion or abnormal metabolism of thevitamin
Vitamin D metabolism is carefully regulated, particularly the activityof renal 1--hydroxylase, the enzyme responsible for the production
of 1,25(OH)2D
The regulation of 1--hydroxylase and the normal feedbacksuppression by 1,25(OH)2D seem to work less well and operatepoorly in sites other than the renal tubule
These phenomena explain the occurrence of hypercalcemiasecondary to excessive 1,25(OH)2D3 production in infants withWilliams syndrome and in adults with sarcoidosis or lymphoma
-
7/25/2019 Diseases of the Parathyroid Gland
17/48
VITAMIN D INTOXICATION:
Chronic ingestion of 50-100x the normal physiologic requirement of vitamin D
(amounts>50,000 to 100,000 U/day)is required to produce significant hypercalcemia in
normal individuals
Vitamin D excess increases intestinal calcium absorption, and if severe, also increases
bone resorption
Hypercalcemia in vitamin D intoxication is due to an excessive biologic action of the
vitamin, the consequence of increased levels of 25(OH)2D rather than merely increasedlevels of the active metabolite 1,25(OH)2D
DIAGNOSIS:
substantiated by documenting elevated levels of 25(OH)D > 100ng/mL
TREATMENT: Hypercalcemia is controlled by restriction of dietary calcium intake and appropriate
attention to hydration
Vitamin D stores in fat may be substantial, and vitamin D intoxication may persist for
weeks after vitamin D ingestion is terminated
Glucocorticoids (Hydrocortisone) in doses of 100mg/day return serum calcium levelsto normal over several days
-
7/25/2019 Diseases of the Parathyroid Gland
18/48
SARCOIDOSIS and Other
GRANULOMATOUS DISEASES: In patients with sarcoidosis and other granulomatous diseases (TB,
fungal infections), excess 1,25(OH)2D is synthesized in macrophagesor other cells in the granulomas
The usual regulation of active metabolite production by calcium or
PTH does not operate in the above conditions- hypercalcemia doesnot lead to reduction in the blood levels of 1,25(OH)2D, and itsclearance from the blood may be decreased as well
TREATMENT:
Avoiding excessive sunlight exposure and limiting vitamin D andcalcium intake
Glucocorticoids (Hydrocortisone
-
7/25/2019 Diseases of the Parathyroid Gland
19/48
IDIOPATHIC HYPERCALCEMIA of INFANCY:
Also referred to as WILLIAMS SYNDROME
An autosomal dominant disorder due to abnormal sensitivity to Vitamin D
Characterized by multiple congenital development defects:
supravalvular AS, MR
an elfin facies hypercalcemia
Levels of 1,25(OH)2D are elevated ranging from 46 to 120 nmol/L (150-500pg/mL)
The mechanism of the abnormal sensitivity to vitamin D and of theincreased circulating levels of 1,25(OH)2D is still unclear
Studies suggest that mutations involving the elastin locus and perhaps othergenes on chromosome 7 may play a role in the pathogenesis
-
7/25/2019 Diseases of the Parathyroid Gland
20/48
HYPERCALCEMIA Associated with
HIGH BONE TURNOVER:1. HYPERTHYROIDISM:
~20% of hyperthyroid patients have high-normal or mildly elevated
serum calcium concentrations associated with hypercalciuria
The hypercalcemia is due to increased bone turnover, with boneresorption exceeding bone formation
Severe calcium elevations are not typical, and the presence of such
suggests a concomitant disease such as hyperparathyroidism
Hypercalcemia is managed by treatment of the hyperthyroidism
2. IMMOBILIZATION:
The mechanism appears to involve a disproportion between bone
formation and bone resorption
-
7/25/2019 Diseases of the Parathyroid Gland
21/48
HYPERCALCEMIA Associated with HIGH BONE TURNOVER:
3. THIAZIDES:
Administration of thiazides can cause hypercalcemia in patients with high rates of
bone turnover, such as patients with hypoparathroidism treated with high doses ofvitamin D
Chronic thiazide administration leads to reduction in urinary calcium; thehypocalciuric effect appears to reflect the enhancement of proximal tubularresorption of sodium and calcium in response to sodium depletion
The abnormal effects of thiazide on calcium metabolism disappear within days ofcessation of the drug:
4. VITAMIN A INTOXICATION:
Calcium levels can be elevated into the 3 to 3.5mmol/L (12-14mg/dL) range afterthe ingestion of 50,00100,000 units of vitamin A daily (10-20x the minimumdaily requirement)
Excess vitamin A intake is presumed to increase bone resorption
DIAGNOSIS:
established by history and by measurement of vitamin A levels in serum
skeletal x-rays reveal periosteal calcifications
TREATMENT:
withdrawal of the vitamin Hydrocortisone 100mg/d
-
7/25/2019 Diseases of the Parathyroid Gland
22/48
HYPERCALCEMIA Associated with RENAL FAILURE:
1. SEVERE SECONDARY HYPERPARATHYROIDISM:
Secondary hyperparathyroidism occurs when partial resistance to the metabolic actionsof PTH leads to excessive production of the hormone
Parathyroid gland hyperplasia occurs because resistance to the normal level of PTH leadsto hypocalcemia, which, in turn, is a stimulus to parathyroid gland enlargement
SYMPTOMS:
Bone pain, ectopic calcification, pruritus
RENAL OSTEODYSTROPHY- bone disease seen in patients with secondaryhyperparathyroidism and renal failure
OSTEOMALACIA -due to vitamin D and calcium deficiency
OSTEITIS FIBROSA CYSTICA -due to excessive PTH action on bone may also occur
TREATMENT: Reduction of excessive blood phosphate by restriction of dietary phosphate
The use of nonabsorbable antacids (CALCIUM CARBONATE ) is preferred overaluminum-containing antacids to prevent aluminum toxicity
CALCITRIOL(0.25 to 2.0ug/day)
TERTIARY HYPERPARATHYROIDISM- a state of severe hyperparathyroidism in patientswith renal failure that requires surgery
-
7/25/2019 Diseases of the Parathyroid Gland
23/48
HYPERCALCEMIA Associated with RENAL FAILURE:
2. ALUMINUM INTOXICATION: May occur in patients on chronic dialysis
MANIFESTATIONS: Acute dementia, unresponsive and severe osteomalacia, bone pain, multiple nonhealing
fractures (ribs, pelvis), proximal myopathy
Hypercalcemia develops when these patients are treated with vitamin D or calcitriolbecause of impaired skeletal responsiveness
PREVENTION: avoidance of aluminum excess in the dialysis regimen
TREATMENT: mobilizing aluminum through the use of the chelating agent
(DEFEROXAMINE)
3. MILK-ALKALI SYNDROME: Due to excessive ingestion of calcium and absorbable antacids (milk, use of
calcium carbonate in osteoporosis)
CLINICAL PRESENTATIONS: Hypercalcemia, alkalosis, renal failure
The cycle of mild hypercalcemia-> bicarbonate retention-> alkalosis-> renal calciumretention-> severe hypercalcemia perpetuates and aggravates hypercalcemia andalkalosis as long as calcium and absorbable alkali are ingested
BURNETTS SYNDROME- the chronic form of the disease associated with irreversiblerenal damage
The acute syndromes reverse if the excess calcium and absorbable alkali arestopped
-
7/25/2019 Diseases of the Parathyroid Gland
24/48
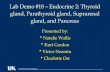
ALGORITHM for the EVALUATION of
PATIENTS with HYPERCALCEMIA:
-
7/25/2019 Diseases of the Parathyroid Gland
25/48
TREATMENT:1. HYDRATION, INCREASED SALT INTAKE and MILD and FORCED DIURESIS:
Many hypercalcemic patients are dehydrated because of vomiting, inanition,and/or hypercalcemia-induced defects in urinary concentrating ability
The resulting drop in GFR is accompanied by an additional decrease in renaltubular sodium and calcium clearance
Restoring a normal ECF volume corrects these abnormalities and increasesurine calcium excretion by 2.5-7.5 mmol/d (100-300mg/d)
Increasing urinary sodium excretion to 400-500 mmol/d increases urinary
calcium excretion even further than simple rehydration
After rehydration, saline can be administered or furosemide or ethacrynicacid can be given to depress the tubular reabsorptive mechanism for calcium
Precautions should be taken to prevent potassium and magnesium depletion;renal calculi are also a potential complication
-
7/25/2019 Diseases of the Parathyroid Gland
26/48
TREATMENT:
2. BIPHOSPHONATES: Analogues of pyrophosphate
High affinity for bone especially in areas of increased bone turnover
Powerful inhibitors of bone resorption
1stgeneration: Etidronate
2ndgeneration: Pamidronate 3rdgeneration: Zolendronate
3. CALCITONIN: Calcitonin acts through receptors on osteoclasts to block bone
resorption and to increase urinary calcium excretion by inhibition ofrenal tubular calcium reabsorption
Usual doses are 2-8U/kg BW IV, SC or IM q 6-12hrs
-
7/25/2019 Diseases of the Parathyroid Gland
27/48
TREATMENT:4. OTHER THERAPIES: PLICAMYCIN:
inhibits bone resorption but has been replaced by biphosphonates because of its toxicity
Given IV, either as a bolus or by slow infusion at a dose of 25ug/kg BW
GALLIUM NITRATE:
Exerts a hypocalcemic action by inhibiting bone resorption and altering the structure of bone crystals
GLUCOCORTICOIDS:
Increase urinary calcium excretion and decrease intestinal calcium absorption Malignancies in which hypercalcemia responds to glucocorticoids: multiple myeloma, leukemia,
Hodgkins disease, carcinoma of the breast
Glucocorticoids are also effective in treating hypercalcemia due to vitamin D intoxication andsarcoidosis
Prednisone 40-100mg daily in 4 divided doses
DIALYSIS: Treatment of choice for severe hypercalcemia complicated by renal failure
PHOSPHATE THERAPY:
Correcting hypophosphatemia lowers the serum calcium concentration
The usual oral dose is 1 to 1.5g phosphorus per day
IV phosphate is used only in severe hypercalcemia with cardiac or renal failure at a dose of >1500 mgover 6-8hrs leads to a decrease of serum calcium to 1.2-2.5mmol/L (5-10mg/dL)
-
7/25/2019 Diseases of the Parathyroid Gland
28/48
TREATMENT:SUMMARY:
The choice of treatment depends on the underlying disease, the
severity of the hypercalcemia, the serum inorganic phosphate level,and the renal, hepatic and bone marrow function
MILD HYPERCALCEMIA (3.7mmol/L or 15mg/dL): Calcitoningiven for its rapid blockade of bone resorption
IV biphosphonates- pamidronate or zolendronate
For the 1st24-48hrs, aggressive sodium-calcium diuresis with IV salineand large doses of furosemide or ethacrynic acid following initial
hydration while monitoring cardiac and renal function Dialysis
MODERATE HYPERCALCEMIA (3-3.7mmol/L or 12-15mg/dL):vigorous hydration plus the most appropriate selection for the
patient of the combinations used with severe hypercalcemia
-
7/25/2019 Diseases of the Parathyroid Gland
29/48
HYPOCALCEMIA:
SIGNS and SYMPTOMS: Paresthesia around the mouth, fingers and toes
Tetany: (+) Trousseau & Chvostek signs
Seizures
Dementia
Cataracts
Calcification of the basal ganglia
Epidermal changes (dry skin, coarse hair, brittle nails)
ECG abnormalities (prolonged QT intervals & QRS and ST changes which mimicMI)
FACTITIOUS HYPOCALCEMIA: Decrease in total Ca, but not ionized Ca
Majority is due to hypoalbuminemia caused by chronic Illness, psoriasis,malnutrition, volume expansion
-
7/25/2019 Diseases of the Parathyroid Gland
30/48
HYPOCALCEMIA:ETIOLOGIES:
1. ABSENCE of PTH or PARATHYTOID GLANDS A. Congenital
B. Postsurgical hypoparathyroidism
C. Infiltrative disorders (e.g., hemochromatosis)
D. Hypoparathyroidism secondary to radioactive iodine thyroid ablation
E. Autoimmune hypoparathyroidism (isolated or as part of Polyglandular Autoimmune Syndrome Type1)
2. IMPAIRED SECRETION of PTH
A. Hypomagnesemia B. Respiratory alkalosis
C. Activating mutations of the Ca sensor
3. TARGET ORGAN RESISTANCE to PTH A. Hypomagnesemia
B. Pseudohypoparathyroidism (Type I and II)
4. VITAMIN D RELATED A. Vitamin D deficiency
B. Accelerated vit D loss C. Impaired 25-hydroxylation
D. Impaired 1-alpha-hydroxylation (e.g., renal failure)
E. Target-organ resistance
5. OTHERS A. Chelation with drugs
B. Pancreatitis
C. Septic shock
D. Hungry bone disease
HYPOCALCEMIA
-
7/25/2019 Diseases of the Parathyroid Gland
31/48
HYPOCALCEMIA: ACUTE HYPOCALCEMIA:
Patients have rapid decrease in serum Ca (
-
7/25/2019 Diseases of the Parathyroid Gland
32/48
FUNCTIONAL CLASSIFICATION of HYPOCALCEMIA:I. PTH ABSENT:
A. Hereditary hypoparathyroidism
B. Acquired hypoparathyroidism
C. Hypomagnesemia
II. PTH INEFFECTIVE:
A. Chronic renal failure
B. Active vitamin D lacking: 1. Decreased dietary intake or sunlight
2. Defective metabolism Anticonvulsant therapy
Vitamin D-dependent rickets type I
C. Active vitamin D ineffective 1. Intestinal malabsorption
2. Vitamin D-dependent rickets type II
D. Pseudohypoparathyroidism
III. PTH OVERWHELMED:
A. Severe, acute hyperphosphatemia 1. Tumor lysis
2. Acute renal failure
3. Rhabdomyolysis
B. Osteitis fibrosa after parathyroidectomy
-
7/25/2019 Diseases of the Parathyroid Gland
33/48
PTH ABSENT:
1. HEREDITARY HYPOPARATHYROIDISM: Onset is gradual and associated with other developmental defects
of the thymus or failure of other endocrine organs (adrenal, thyroid,ovary)
Manifest within the 1stdecade but may appear later
MANIFESTATIONS: Basal ganglia calcification and extrapyramidal syndromes are more
common and earlier in onset than in acquired hypoparathyroidism
Papilledema and raised ICP may occur in both hereditary and acquiredhypoparathyroidism, as do chronic changes in the fingernails and hairand lenticular cataracts
Skin manifestations: alopecia, candidiasis
-
7/25/2019 Diseases of the Parathyroid Gland
34/48
PTH ABSENT:IDIOPATHIC HYPOPARATHYROIDISM :Hereditary hypoparathyroidism occuring as an isolated entity
without other endocrine or dermatologic manifestations
DiGEORGE SYNDROME (Velocardiofacial Syndrome):
A rare form of hypoparathyroidism associated with defective development of both the thymus andthe parathyroid glands
Congenital cardiovascular, facial and other developmental defects are present, and most patientsdie in early childhood with severe infections, hypocalcemia and seizures, or cardiovascularcomplications
Most cases are sporadic, but an autosomal dominant form has been described
POLYGLANDULAR AUTOIMMUNE TYPE 1 DEFICIENCY:
Hypoparathyroidism occurs in association with a complex hereditary autoimmune syndromeinvolving failure of the adrenals, the ovaries, the immune system, and the parathyroids inassociation with recurrent mucocutaneous candidiasis, alopecia, vitiligo and pernicious anemia
AUTOSOMAL DOMINANT HYPOCALCEMIA:
Due to gain-of-function mutations in the calcium-sensing receptor The activated receptor suppresses PTH secretion leading to hypocalcemia: receptor activation in
the kidney results in excessive calcium excretion
HYPOPARATHYROIDISM associated with MITOCHONDRIAL DYSFUNTION and MYOPATHY:
1. KEARNS-SAYRE SYNDROME (KSS)associated with ophthalmoplegia and pigmentaryretinopathy
2. MELAS SYNDROMEMitochondrial Encephalopathy, Lactic Acidosis and Stroke-like episodes
-
7/25/2019 Diseases of the Parathyroid Gland
35/48
PTH ABSENT:2. ACQUIRED HYPOPARATHYROIDISM:
Usually the result of inadvertent surgical removal of all the parathyroid glands
The most frequent cause in the past was surgery for hyperthyroidism; hypoparathyroidismnow usually occurs after surgery for hyperparathyroidism
Rare causes:
Radiation-induced damage subsequent to radioiodine therapy of hyperthyroidism
Glandular damage in patients with hemochromatosis or hemosiderosis after repeatedblood transfusions
TRANSIENT HYPOPARATHYROIDISMoccurs following surgery for hyperparathyroidismafter normal parathyroid function returns to normal due to hyperplasia or recovery ofremaining tissue
TREATMENT: Treatment of acquired and hereditary hypoparathyroidism involves :
(1) Replacement with Vitamin D (40,000 to 120,000 U/day)
(2) 1,25(OH)2D (calcitriol) at 0.5 to 1.0 ug
(3) High oral calcium intake
(4) Thiazides- diuretics lower urine calcium by as much as 100mg/day in
hypoparathyroid patients on Vitamin D, provided they are maintained on a low sodiumdiet
-
7/25/2019 Diseases of the Parathyroid Gland
36/48
PTH ABSENT:
3. HYPOMAGNESEMIA: Severe hypomagnesemia (
-
7/25/2019 Diseases of the Parathyroid Gland
37/48
PTH INEFFECTIVE:
PTH is ineffective when:
(1) the hormone receptor-guanyl nucleotide-bindingprotein complex is defective (PHP) resulting in failure of
PTH to increase intracellular cAMP
(2) PTH action to promote calcium absorption from thediet is impaired due to Vitamin D deficiency or becausevitamin D is ineffective (receptor or synthesis defects)
(3) CRF where the calcium-elevating action of PTH isimpaired
PTH INEFFECTIVE
-
7/25/2019 Diseases of the Parathyroid Gland
38/48
PTH INEFFECTIVE:1. MECHANISMS of HYPOCALCEMIA in CHRONIC RENAL FAILURE (CRF):
Phosphate retention and impaired production of 1,25(OH)2D are the principal factors that cause
calcium deficiency, secondary hyperparathyroidism and bone disease
Low levels of 1,25(OH)2D due to hyperphosphatemia and destruction of renal tissue are
critical in the development of hypocalcemia
Hyperphosphatemia in renal failure lowers blood calcium levels by the following mechanisms:
(1) Extraosseous deposition of calcium and phosphate
(2) Impairment of the bone-resorbing action of PTH
(3) Reduction in 1,25(OH)2D production by remaining renal tissue
The uremic state also causes impairment of intestinal absorption by mechanisms other than
defects in vitamin D metabolism
TREATMENT: Phosphate restriction in the diet
Avoidance of aluminum-containing phosphate-binding antacids to prevent aluminum intoxication
Oral calcium supplementation (1-2g/day) and Calcitriol (0.25-1.0 ug/day)
The aim of therapy is to restore normal calcium balance to prevent osteomalacia and secondary
hyperparathyroidism, and to prevent secondary from becoming autonomoushyperparathyroidism.
-
7/25/2019 Diseases of the Parathyroid Gland
39/48
PTH INEFFECTIVE:
2. VITAMIN D DEFICIENCY due to INADEQUATE DIET and/or SUNLIGHT: PTH hypersecretion compensates for the tendency for the blood calcium to
fall but also induces renal phosphate wasting and results in osteomalacia
3. DEFECTIVE VITAMIN D METABOLISM:
A. ANTICONVULSANT THERAPYinduces vitamin D deficiency by increasingthe conversion of Vitamin D to inactive compounds
B. VITAMIN D-DEPENDENT RICKETS TYPE I (Pseudo-vitamin D-resistantrickets)
Due to the resistance to the action of vitamin D as well as to vitamin D deficiency
Autosomal recessive caused by mutations in the gene encoding 25(OH)D-1-alpha-
hydroxylase Differs from true vitamin D-resistant rickets in that it is less severe and the
biochemical and radiographic abnormalities can be reversed with appropriatedoses of vitamin D or its active metabolite 1,25(OH)2D3
CLINICAL FEATURES:hypocalcemia, often with tetany and convulsions,hypophosphatemia, secondary hyperparathyroidism and osteomalacia associatedwith skeletal deformities and increased alkaline phosphatase
-
7/25/2019 Diseases of the Parathyroid Gland
40/48
PTH INEFFECTIVE:4. VITAMIN D INEFFECTIVE:
A. INTESTINAL MALABSORPTION: Mild hypocalcemia, secondary hyperparathyroidism, severe
hypophosphatemia, and a variety of nutritional deficiencies occur with GIdiseases
Hepatocellular dysfunction (portal or biliary cirrhosis of the liver) can lead toreduction in 25(OH)D levels
Malabsorption of vitamin D and its metabolites (1,25(OH)2D) may occur in avariety of bowel diseases, hereditary or acquired
Hypocalcemia can lead to steatorrhea due to deficient production ofpancreatic enzymes and bile salts
B. VITAMIN D-DEPENDENT RICKETS TYPE II: Results from end-organ resistance to the active matabolite 1,25(OH)2D
CLINICAL FEATURES: hypocalcemia, hypophosphatemia, secondaryhyperparathyroidism, rickets, and partial or total alopecia
All of the genetically characterized genotypes have mutations in the gene forthe vitamin D receptor
-
7/25/2019 Diseases of the Parathyroid Gland
41/48
PTH INEFFECTIVE:5. PSEDOHYPOPARATHYROIDISM (PHP):
A hereditary disorder characterized by symptoms and signs of hypoparathyroidism inassociation with distinctive skeletal and developmental defects
The hypoparathyroidism is due to a deficient end-organ response to PTH
Hyperplasia of the parathyroids, a response to hormone resistance, causes elevation of PTHlevels
CLASSIFICATION:
1. PHP-Ia
2. PHP-Ib
3. PHP-II 4. PPHP
TREATMENT:
Treatment is similar to that of hypoparathyroidism, except that the doses of vitamin Dand calcium are usually lower than those required in true hypoparathyroidism,presumably because the defect in PHP is only partial because of imprinting in specifictissues
-
7/25/2019 Diseases of the Parathyroid Gland
42/48
CLASSIFICATION of PHP and PPHP:
-
7/25/2019 Diseases of the Parathyroid Gland
43/48
PTH OVERWHELMED:
The loss of calcium from the ECF is so severe that PTHcannot compensate
Situations in which there is rapid efflux of calcium:
Acute pancreatitis
Severe acute hyperphosphatemia in association with renalfailure
Severe hypocalcemia can occur quickly; PTH rises inresponse to hypocalcemia but does not return bloodcalcium to normal
-
7/25/2019 Diseases of the Parathyroid Gland
44/48
PTH OVERWHELMED:A. SEVERE ACUTE HYPERPHOSPHATEMIA:
Severe hyperphosphatemia is associated with extensive tissue damage or celldestruction
The combination of increased release of phosphate from muscle and impaired ability toexcrete phophorus because of renal failure causes moderate to severehyperphosphatemia, the latter causing calcium loss from the blood and mild tomoderate hypocalcemia
Hypocalcemia is usually reversed with tissue repair and restoration of renal function asphosphorus and creatinine values return to normal
Other causes of hyperphosphatemia: hypothermia, massive hepatic failure, hematologicmalignancies
TREATMENT: Directed toward lowering of blood phosphate by the administration of phosphate-
binding antacids or dialysis
Although calcium replacement may be necessary if hypocalcemia is severe andsymptomatic, calcium administration during the hyperphosphatemic period tends toincrease extraosseous calcium deposition and aggravate tissue damage
-
7/25/2019 Diseases of the Parathyroid Gland
45/48
PTH OVERWHELMED:
B. OSTEITIS FIBROSIS after PARATHYROIDECTOMY:
Hypocalcemia can persist for days afterparathyroidectomy if calcium replacement isinadequate
Treatment:
parenteral calcium calcitriol and oral calcium supplementation is
sometimes needed for weeks to a month or two untilbone defects are filled
-
7/25/2019 Diseases of the Parathyroid Gland
46/48
DIFFERENTIAL DIAGNOSIS: CHRONIC HYPOCALCEMIA:
Can be ascribed to disorders associated with absent or ineffective PTH Characterized by LOW CALCIUM and LOW PHOSPHORUS
Important clinical criteria include: duration of the illness, sings or symptoms of associated disorders,presence of features that suggest a hereditary abnormality, nutritional history, history of excessive alcoholintake (magnesium deficiency)
HYPOPARATHYROIDISM and PHP:
Typically lifelong illnesses, usually appearing by adolescence Characterized by a LOW CALCIUM and HIGH PHOSPHORUS in the absence of renal failure or massive tissue
destruction
A recent onset of hypocalcemia that results in deficient or ineffective vitamin D in an adult: NUTRITIONAL DEFICIENCIES, RENAL FAILURE or INTESTINAL DISORDERS
POSTOPERATIVE HYPOPARATHYROIDISM- follows neck surgery
A history of SEIZURE DISORDER raises the issue of ANTICONVULSANT THERAPY
RICKETS and a variety of neuromuscular syndromes and deformities may indicate ineffectivevitamin D action, either due to defects in vitamin D metabolism or to vitamin D deficiency
-
7/25/2019 Diseases of the Parathyroid Gland
47/48
DIAGNOSIS: LABORATORY TESTS:
(1) Serum Ca (ionized Ca is the preferred measurement) (2) Albumin:
Hypoalbuminemia may result in false hypocalcemia if total serum calcium is measured
For each 1g/dL decrease in albumin below 4g/dL, subtract 0.8g/dL from the total serum Ca
(3) Phosphorus, PTH, Mg and if available, 25(OH)D and 1,25(OH)2D
PARATHYROID-RELATED DISORDERS: low serum Ca, high serum phosphate, low 1,25(OH)2D, low PTH
VITAMIN D-RELATED DISORDERS: hypocalcemia, hypophosphatemia, high PTH, low 1,25(OH)2D in vitamin D-
deficient patients
Failure to detect elevated PTH levels in the presence of hypocalcemia establishes the diagnosis ofHYPOPARATHYROIDISM; elevated levels suggest the presence of SECONDARY HYPERPARATHYROIDISM
Low or normal 25(OH)D indicates VITAMIN D DEFICIENCY due to lack of sunlight, inadequate vitamin D intake
or intestinal malabsorption
A low level of 1,25(OH)2D in the presence of elevated PTH suggests ineffective PTH action (CRF, severevitamin D deficiency, vitamin D-dependent rickets type I, PHP)
-
7/25/2019 Diseases of the Parathyroid Gland
48/48
TREATMENT: (1) VITAMIN D ANALOGS:
May be necessary in cases of vitamin D deficiency or resistance, dialysis patients, hypocalcemia fromsubtotal parathyroidectomy
Vitamin D 200 U (5ug/d) or Calcitriol 0.25 to 1.0 ug/drequired to prevent rickets in normal individuals
40,000 to 120,000 U (1-3mg) of vitamin D2 or D3required in hypoparathyroidism; calcitriol dosage isunchanged since the defect is in hydroxylation
(2) CALCIUM (PO or IV): Patients with hypoparathyroidism should also be given 2-3g elemental calcium by mouth daily
Patients who present with signs and symptoms of acute hypocalcemia need to be treated with rapidparenteral administration of calcium; chronic, asymptomatic hypocalcemia may be treated with Ca (PO)
(3) MAGNESIUM (PO or IV): Mg (IV) is administered if acute hypocalcemia is associated with hypomagnesemia, to be replaced as
soon as possible by Mg (PO) to replace body stores since Mg (IV) is excreted in the urine