/ 33 1 mmon Psychiatric Proble mmon Psychiatric Proble in Family Practice in Family Practice omatoform Disorder omatoform Disorder Saudi Diploma in Family Medicine Center of Post Graduate Studies in Family Medicine Dr. Zekeriya Aktürk [email protected] www.aile.net

10 Somatoform
Jan 24, 2016
bhbhj765675rf t67t 67 uyg y gy gyg yjg
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

/ 331
CoCommon Psychiatric Problemsmmon Psychiatric Problemsin Family Practice in Family Practice
Somatoform DisordersSomatoform Disorders
Saudi Diploma in Family Medicine Center of Post Graduate Studies in Family Medicine
Dr. Zekeriya Aktü[email protected]
www.aile.net

/ 332
Your most difficult
patients ?Pain everywhe
reNot
improving
Comming every day

/ 333
• At the end of this session, the trainees will increase their knowledge in managing somatoform disorders– Explain the pathopysiology
– List symptoms which might be somatic
– List diagnostic criteria of somatoform disorders
– Explain the management principles of somatisation
– Categorize the somatoform disorders
Aim-Objectives

/ 334
somatization
desomatization
resomatization

/ 335
Bodily symptoms without any organic, physical cause
Definition
Lipowsky 1988

/ 336
• No explanatory organic cause can be found in 20-84% of patients presenting with bodily symptoms.
Why important?

/ 337
More common among less More common among less educated and less incomeeducated and less income
Epidemyology

/ 338
I. Increased bodily sensitivity Physical symptoms perceived are normal
for most individuals
Pathopysiology

/ 339

/ 3310
II. Defined patient Stress within the
family stabilizes after the member bocomes “sick”
Pathopysiology

/ 3311
III. Need to be sick
Becoming physically sick is less stressfull than being unsuccessfull
Barsky,1997
“There is no medicine or surgery to remove the
need to be sick”BARSKY,1997
Pathopysiology

/ 3312
IV. Dissociation
Perceiving a stimulus which is not present
• Phantom pain
• Depersonalization
• Flashback
Pathopysiology

/ 3313
• Somatization
• Conversion disorder
• Hypochondriasis
• Pain disorder
• Body dysmorphic disorder
Somatoform Disorders

/ 3314
• Resemples a neurological problemResemples a neurological problem
• Motor or sensorial symptomsMotor or sensorial symptoms
• Not explainable by neuroanatomyNot explainable by neuroanatomy
• ““La belle indiference” La belle indiference”
• Females 10-35 years,Females 10-35 years,
• Lower socioeconomic classLower socioeconomic class
Conversion

/ 3315
• “Disease of having disease”
• Severe anxiety
• M/F=1
• No insight
• Resistant, causing functional losses
Hypochondirasis

/ 3316
• Main symptom is pain
• M/F=1/2
• Pain increases with stressPain increases with stress
• Not explainable with nouroanatomyNot explainable with nouroanatomy
• Organic problem may be superimposedOrganic problem may be superimposed
Pain disorder

/ 3317
• Belives that there is a problem with appearance
• Obsessive
• M/F=1
• Frequent cosmetic surgery
Body Dysmorphic Disorder

/ 3318
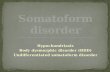
Organic cause?Substance abuse?
Other psychiatric dis.?
Neurological symptom conversion
Pain predominant
Too busy with disease Hypochondriasis
Pain disorder
Somatization dis.Many symptoms
Intentional symptoms Malingering
yok
I
II
III
IV
V
VI

/ 3319
SYMPTOMS WHICH MIGHT BE SOMATIC
GIS
Nausea
Abdominal pain
Diarrhea
Belching
Bloating
Food intolerance
CVS
Chest pain
Palpitations
Dyspnea
UROGENITAL
Burning
Dysparonia
Dysmenorrhea
Irregular menstruation
Vomiting
PAIN
Generalized pain
Extremity pain
Back pain
Joint pain
Headache
Dysuria
PSEUDONEUROLOGICAL
Amnesia
Swallowing difficulty
Loss of voice
Blurred vision, blindness
Fainting
Muscle weakness
Difficulty in walking
SYNDROMES
Atipical chest pain
Temporomandibular joint s.
“hypoglycemia”
Premenstruel symdrome
Unidentified “food allergy”
Unidentified “vitamin deficiency”

/ 3320
• At least three symptoms of uknown cause (generally in different systems)
• Chronic course (more than two years)
Since too long
Too many systems
Too many symptoms
Diagnostic Criteria

/ 3321
Symptoms might be exaggerated and
irrational for us but they are
REAL for the patient!

/ 3322
“We counldn’t find anything serious after the exam or investigations. But htere is something bothering you. Although the reason is not clear, this is a situation we face frequently…”
Management – Discuss the diagnosis

/ 3323
“Better we should discuss how we can help you instead of the name. However, although there are a lot of names given, we frequently call this situation as “Somatoform disorder”
What is my diagnosis:
Chronique fatigue
syndrome
Fibromyalgia
Management – Discuss the diagnosis

/ 3324
• Frequent visits (15 min/month)
• Short PE
• Aim: o Prevent new symptomso Decrease admissions to ER
• Discuss open ended questions
Management – Regular visits

/ 3325
• Don’t try to loose the symptoms, better try to teach how to deal with them
• Patients expect more “care” than “cure”.
• Patients expect continuous relationship.
Management – Regular visits

/ 3326
B ackgroundHow is your life going?
A ffectWhat do you feel?
T roubleWhat is the most important problem?
H andleWhat can help you?
E mpathy I understand you. This is a tough situation...
Stuart MR, Lieberman JA, 1993
Management – BATHE’ing the patient

/ 3327
• No specific medicine
• Treat concomittant psychiatric problem
• Deal with domiant symptom:o Pain Amitriptillineo Fatigue Bupropiono Anxiety, sleep dist SSRI, TCA
Management - Pharmacological

/ 3328
• Stress - somatic symptom relationship
• Symptom diary
• Group therapy
Management - Psychotherapy

/ 3329
• Light exercises (3x20 min/w)
• Increases self esteem
• Yoga, meditation, walks
• Non harmful methods: cold-warm applications, acupuncture, vitamins…
Management – Life style changes

/ 3330
• Dont put goals you can not meet
• Co-morbidity
• Diagnositc requests
• Emergency admissions
• Phone calls
Management - Problems

/ 3331
Concentrating on symptoms
Unnecessary Referrals / cons.Tests
or Rx without Dx
It’s just in your mind, take it
easy..

/ 3332
Frequent, short visits
Allow patient roleConcentrate on
functions
Single doctor

/ 3333
What did we learn?
Related Documents