1 Harnessing ICT-based Tool for Improving the Collaborative Health Planning Debate; the Case of Logan- Beaudesert, Australia Presenters: * Ori Gudes – Griffith University & QUT The study is Supervised by: Tan Yigitcanlar, Elizabeth Kendall and Virendra Pathak

1 Harnessing ICT-based Tool for Improving the Collaborative Health Planning Debate; the Case of Logan- Beaudesert, Australia Presenters: * Ori Gudes –
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Harnessing ICT-based Tool for Improving the Collaborative Health Planning Debate; the
Case of Logan- Beaudesert, Australia
Presenters:
* Ori Gudes – Griffith University & QUT
The study is Supervised by: Tan Yigitcanlar, Elizabeth Kendall and Virendra Pathak
2
Geospatial Revolution clip
Geospatial Revolution clip
http://www.youtube.com/watch?v=ZdQjc30YPOk&feature=channel
3
Aims of the Study
To examine the role of decision support systems as a mechanism to facilitate collaborative health decision-making
To develop a potential information management framework to underpin a health decision support system
To generate a participatory process to create an online tool for health planners using geographic information systems (GIS)
To measure and understand the impact and effectiveness of decision support systems on health decision-makers / health planners
4
Problems to address
Lack of an effective information in health planning Lack of collaboration in decision-making practice Lack of evidence in decision-making processes

5
Decision support systems (DSS) are set of solution mechanisms that help all forms of decision makers to assess complex decision-making processes and to solve problems faced by the help of ICT tools (Shim et al., 2002).
DSS aims to Improve efficiency of decisions made by stakeholders Optimise their overall performance Minimise judgemental biases
Turban, 1990
Decision Support Systems
Health Decision Support System
Knowledge Sharing
Public Participation
Evidence-based Policy

6
How our data collection efforts have been grounded?
Fundamental / macro level
most difficult to influence greatest benefits achieved
Intermediate / meso level more easily influenced
Proximate / micro level
level where we usually work least effective necessary for planning have been given greater scientific
attention in recent years
Individual level targeting disease not most successful influence the individual habitués.
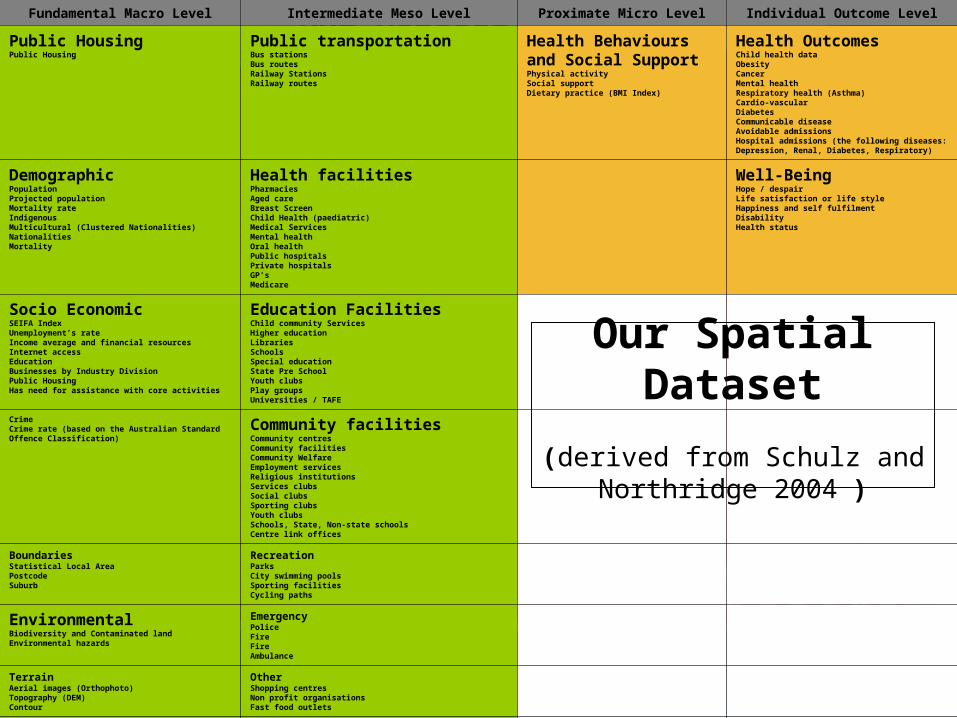
Health assessment framework Schulz and Northridge (2004)
This framework summarises thedifferent levels of factors that impact upon health and,therefore, should be considered in health planning initiatives.
7
Our DatasetFundamental Macro Level Intermediate Meso Level Proximate Micro Level Individual Outcome Level
Public HousingPublic Housing
Public transportationBus stationsBus routesRailway StationsRailway routes
Health Behaviours and Social SupportPhysical activitySocial supportDietary practice (BMI Index)
Health OutcomesChild health dataObesityCancerMental healthRespiratory health (Asthma)Cardio-vascularDiabetesCommunicable diseaseAvoidable admissionsHospital admissions (the following diseases: Depression, Renal, Diabetes, Respiratory)
Demographic PopulationProjected populationMortality rateIndigenous Multicultural (Clustered Nationalities)NationalitiesMortality
Health facilitiesPharmaciesAged careBreast ScreenChild Health (paediatric)Medical ServicesMental healthOral healthPublic hospitalsPrivate hospitalsGP’sMedicare
Well-BeingHope / despairLife satisfaction or life styleHappiness and self fulfilmentDisabilityHealth status
Socio EconomicSEIFA IndexUnemployment’s rateIncome average and financial resourcesInternet accessEducationBusinesses by Industry DivisionPublic HousingHas need for assistance with core activities
Education FacilitiesChild community ServicesHigher educationLibrariesSchoolsSpecial educationState Pre SchoolYouth clubsPlay groupsUniversities / TAFE
CrimeCrime rate (based on the Australian Standard Offence Classification)
Community facilitiesCommunity centresCommunity facilitiesCommunity WelfareEmployment servicesReligious institutionsServices clubsSocial clubsSporting clubsYouth clubsSchools, State, Non-state schoolsCentre link offices
BoundariesStatistical Local AreaPostcodeSuburb
RecreationParksCity swimming poolsSporting facilitiesCycling paths
EnvironmentalBiodiversity and Contaminated landEnvironmental hazards
EmergencyPolice FireFireAmbulance
TerrainAerial images (Orthophoto)Topography (DEM)Contour
OtherShopping centresNon profit organisationsFast food outlets
RoadsMajor roadsStreets
Our Spatial Dataset
(derived from Schulz and Northridge 2004 )
8
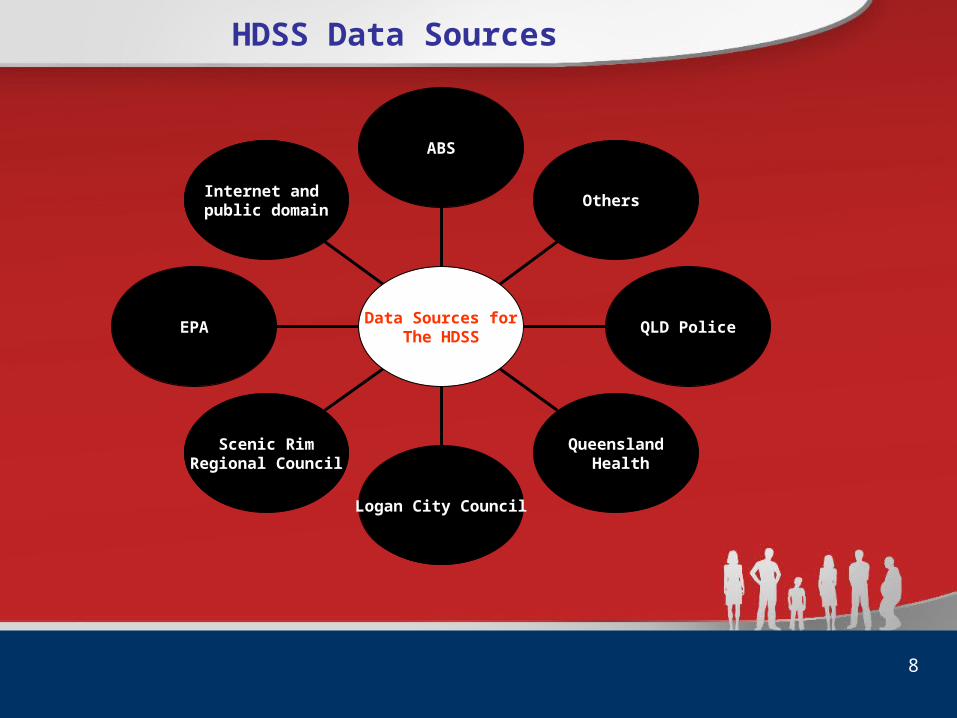
HDSS Data Sources
Internet and public domain
EPA
Scenic RimRegional Council
Logan City Council
Queensland Health
QLD Police
Others
ABS
Data Sources forThe HDSS
9
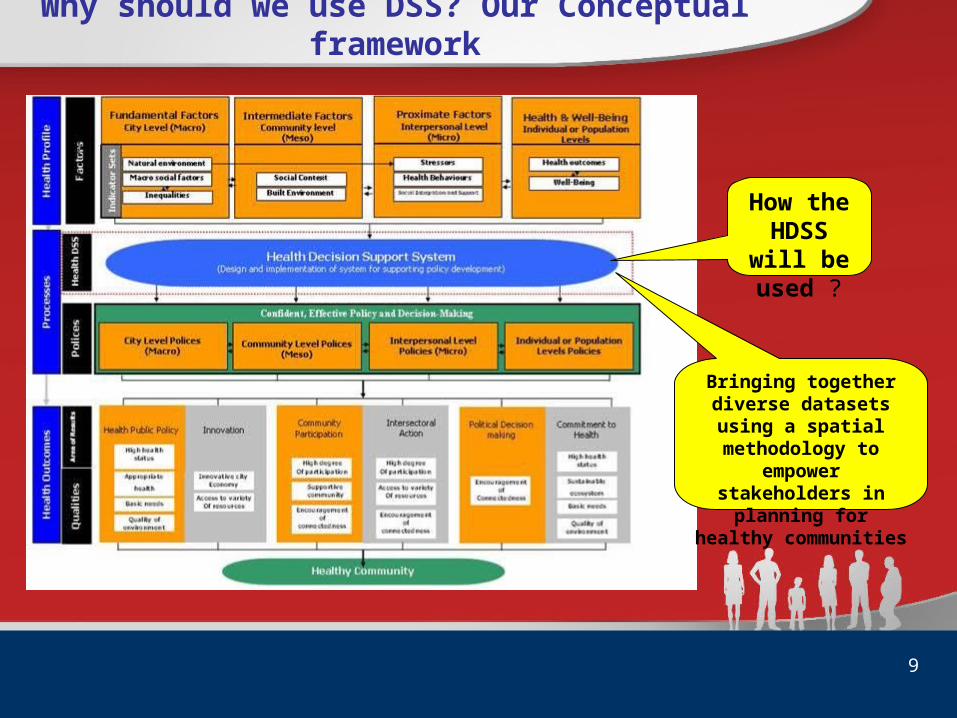
Why should we use DSS? Our Conceptual framework
Bringing together diverse datasets using a spatial methodology
to empower stakeholders in
planning for healthy communities
How the HDSS will be used ?

Pre DSS intervention survey
The quantitative data was collected using a 31-item survey based on several decision-making scales (Dean & Sharfman, 1993; Flood et al, 2000; Bennet et al, 2010; Parnell & Bell, 1994). The items measured the following dimensions of decision-making:
Evidence-based decision-making; Perceived consensus; Participation in decision-making; Perceived satisfaction of decision-making;Perceived importance of decision-making Perceived effectiveness of decision-making; andPerceived equity of decision-making;

11
Where are we?
South East Queensland
South of Brisbane City
---------------
Population: 270,000
31 SLAs
1 in 4 smokers
13% high risk alcohol
66% overweight

LBHC structure
A collaborative arrangement
between government
and non-government agencies, the
private sector and community to develop and deliver health programs and
services

13
Accessibility to hospitals based on
travel time
14
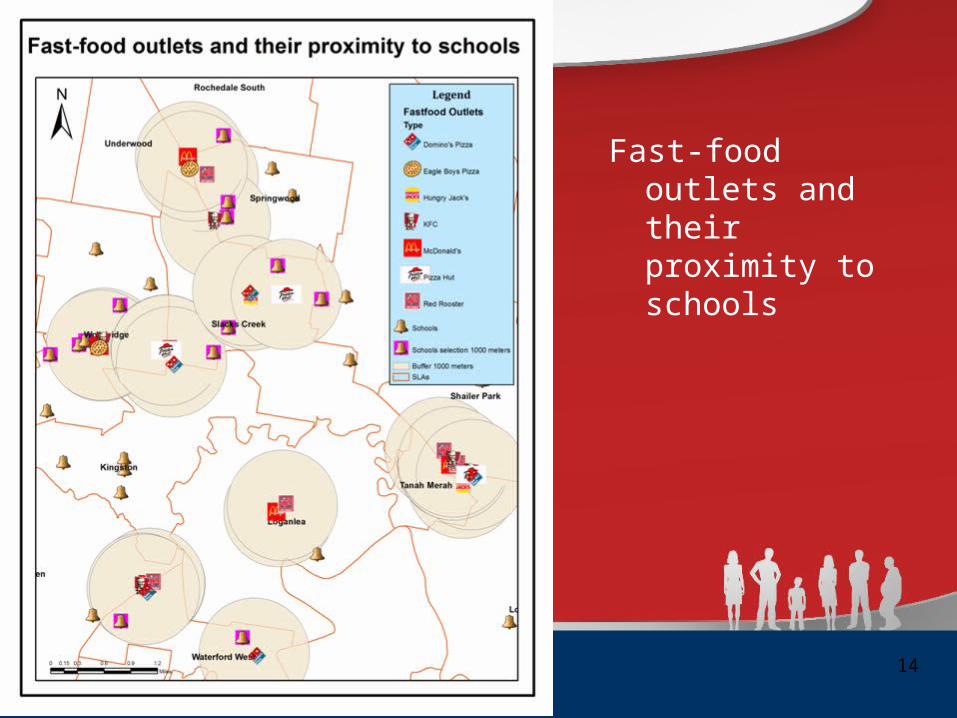
Fast-food outlets and their proximity to schools

15
Hotpot analysis based on people who admitted to hospitals with diabetes
* (Based on Logan-Beaudesert Hospitals data 2005-2007)
16
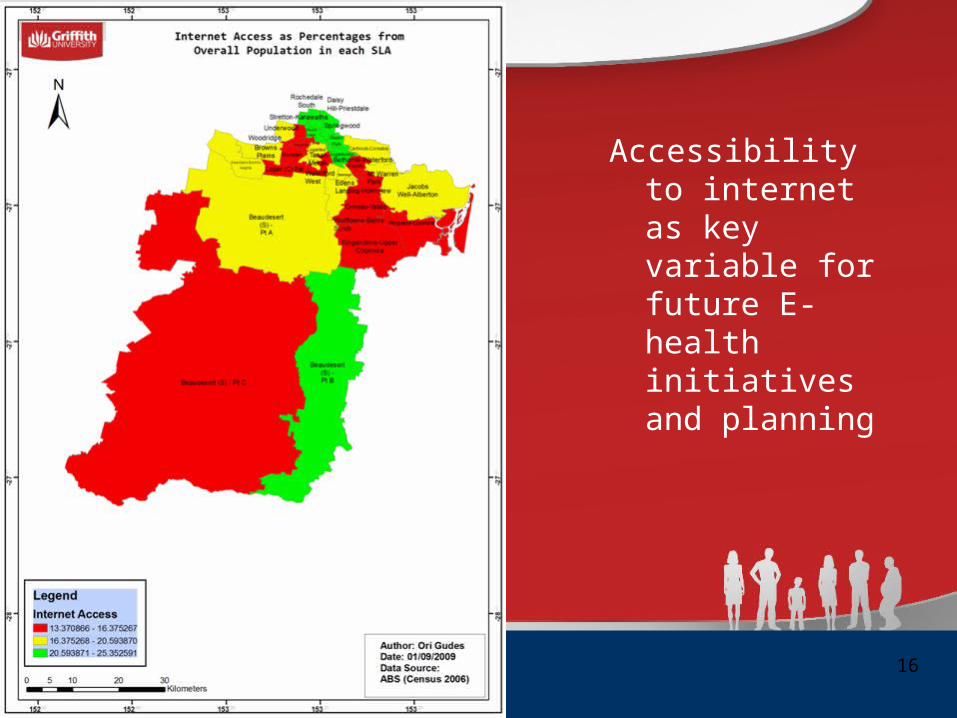
Accessibility to internet as key variable for future E-health initiatives and planning
Preliminary findings from the Pre DSS survey
• Low levels of satisfaction with the decision-making processes across the LBHC.
• There was some diversity across the components of the LBHCSome groups within the LBHC were more satisfied than others (i.e., those who were over 40 years). There was also a tendency for LBHC board members, males, new members and veterans to be more satisfied with information and perceive higher levels of consensus, participation and evidence-based decision-making.
• There was an overall sense that decisions were ineffective, presumably because they were not based on information or evidence.
Conclusion from the Pre DSS survey findings
• New members are enthusiastic, but become more critical of decision-making over time and then eventually resolve this situation in some way – either by withdrawing or seeking other sources of information).
• Age of members had an important influence on the way decision-making was perceived. It is possible that younger people could be more demanding in terms of their need for involvement in the decision-making processes, whereas veterans are likely to have access to more intrinsic sources of information based on years of experience in the region. As a result, they may be less demanding of the decision-making processes.
Overall discussion
In summary, our findings have shown that: There was considerable diversity in the way decision-making were perceived, this, in turn, may require different approaches to health planning across different groups. The findings have also highlighted the need for a comprehensive information framework and collaborative process to underpin planning for healthy cities, thus enabling health coalitions to make effective decisions that engage all stakeholders equitably. The framework proposed in this paper would not only encourage planners to engage with evidence and information about the entire range of health determinants, but would also provide a platform for collaboration and shared engagement in the decision-making process.
Future Research
Unanswered questions:
• How the suggested framework and method are actually applied in local communities
• The impact of the HDSS on decision-making and its ability to facilitate collaborative-based health planning debate
These important research questions shall be addressed as we conduct the next phases in this ongoing project.
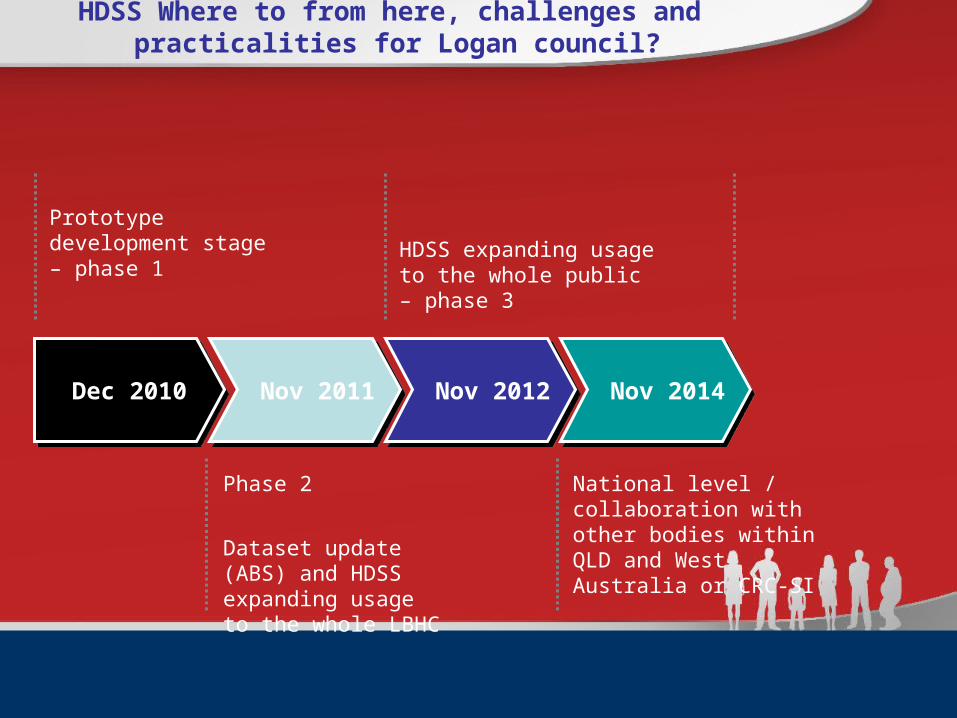
HDSS Where to from here, challenges and practicalities for Logan council?
Prototype development stage – phase 1 HDSS expanding usage to the
whole public – phase 3
Phase 2
Dataset update (ABS) and HDSS expanding usage to the whole LBHC
National level / collaboration with other bodies within QLD and West Australia or CRC-SI
Dec 2010Dec 2010 Nov 2011Nov 2011 Nov 2012Nov 2012 Nov 2014Nov 2014
22
“”Maps can show you where you are.
But a good map can also show you where you want to go, and what needs to happen so that you can get there”
(http://www.mappingforchange.org.uk/, 2009)
`
Related Documents











