1 Challenges in Lipid Management

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Challenges in Lipid Management

2
Objectives
Provide an overview of the effects of lipid-lowering drugs on lipoprotein levels and clinical results
Detail the effects of fibrates on lipoprotein levels, atherosclerotic disease, and coronary end points
Describe the mechanism of action of niacin and how it affects plasma lipids, lipoproteins, and its anti-inflammatory actions
Review the results of clinical trials of niacin alone or combined with colestipol or statins
Describe the side effects of niacin

3
Effects of Lipid-Lowering Drugs
Challenges in Lipid Management
4
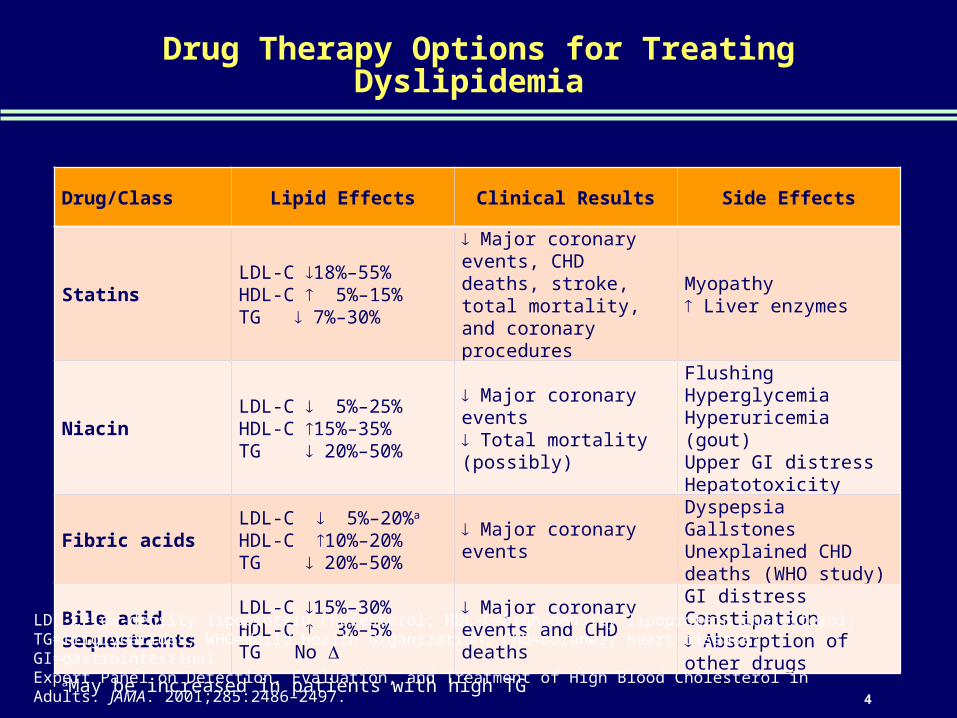
Drug Therapy Options for Treating Dyslipidemia
Drug/Class Lipid Effects Clinical Results Side Effects
StatinsLDL-C 18%–55%HDL-C 5%–15%TG 7%–30%
Major coronary events, CHD deaths, stroke, total mortality, and coronary procedures
Myopathy Liver enzymes
NiacinLDL-C 5%–25%HDL-C 15%–35%TG 20%–50%
Major coronary events Total mortality (possibly)
FlushingHyperglycemiaHyperuricemia (gout)Upper GI distressHepatotoxicity
Fibric acidsLDL-C 5%–20%a
HDL-C 10%–20%TG 20%–50%
Major coronary events
DyspepsiaGallstonesUnexplained CHD deaths (WHO study)
Bile acid sequestrants
LDL-C 15%–30%HDL-C 3%–5%TG No
Major coronary events and CHD deaths
GI distressConstipation Absorption of other drugs
aMay be increased in patients with high TGLDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; TG=triglycerides; WHO=World Health Organization; CHD=coronary heart disease; GI=gastrointestinalExpert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486–2497.

5
Fibrates and Their Benefits on Management of Lipids
MOA Fibrates inhibit fatty acid synthesis in the liver and increase the elimination of TG-rich particles from plasma. They also increase the synthetic rate of HDL-C.
Efficacy TC:
TG: (by 25%–45%)
LDL-C: (by 10%–20%)
HDL-C: (by 10%–15%)
LDL-C/HDL-C:
VLDL:
apo B:
Side effects Abnormal liver function tests, dyspepsia, gallstones, myopathy
Indications Treatment of hypercholesterolemia, hypertriglyceridemia
Contraindications Hypersensitivity to fenofibrate, hepatic or severe renal dysfunction, preexisting gallbladder disease
MOA=mechanism of action; TG=triglycerides; HDL-C=high-density lipoprotein cholesterol; TC=total cholesterol; LDL-C=low-density lipoprotein cholesterol; VLDL=very low-density lipoprotein cholesterol; apo B=apolipoprotein BYoung CE et al. Cardiol Rev. 2004;12:107–119; LOFIBRA® [package insert]; 2005.

6
Effects of Gemfibrozil on CHD Events: VA-HIT Trial
CHD=coronary heart disease; VA-HIT=Veterans Affairs HDL Intervention Trial; MI=myocardial infarctionRubins HB et al. N Engl J Med. 1999;341:410–418.
23%P=0.02
22%P=0.07
22%P=0.006
n=184 n=146 n=118 n=93 n=275 n=219
0
5
10
15
20
25
Nonfatal MI CHD Deaths Combined
CH
D E
ve
nts
, %
Placebo
Gemfibrozil
In a 5-year, randomized, double-blind placebo-controlled trial of 2531 CHD patients
7
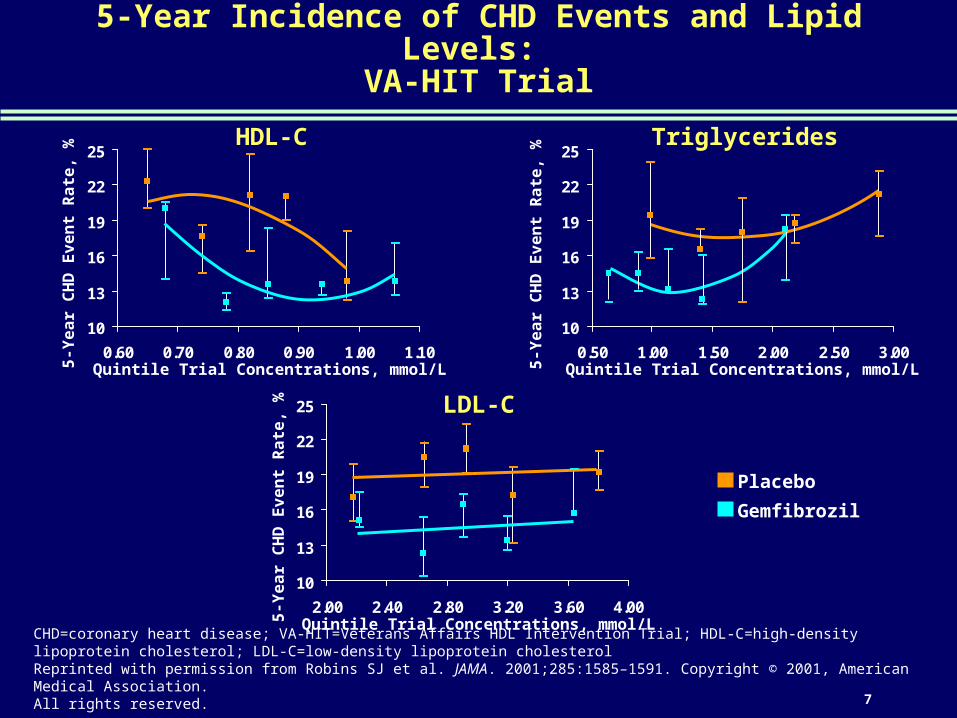
5-Year Incidence of CHD Events and Lipid Levels: VA-HIT Trial
CHD=coronary heart disease; VA-HIT=Veterans Affairs HDL Intervention Trial; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterolReprinted with permission from Robins SJ et al. JAMA. 2001;285:1585–1591. Copyright © 2001, American Medical Association. All rights reserved.
Placebo
Gemfibrozil
5-Y
ea
r C
HD
Ev
en
t R
ate
, %
5-Y
ea
r C
HD
Ev
en
t R
ate
, %
5-Y
ea
r C
HD
Ev
en
t R
ate
, %
Quintile Trial Concentrations, mmol/L
Quintile Trial Concentrations, mmol/L
HDL-C Triglycerides
LDL-C
Quintile Trial Concentrations, mmol/L
10
13
16
19
22
25
0.50 1.00 1.50 2.00 2.50 3.00
10
13
16
19
22
25
2.00 2.40 2.80 3.20 3.60 4.00
10
13
16
19
22
25
0.60 0.70 0.80 0.90 1.00 1.10

8
Effects of Fibrates on Coronary End Points: Results of a Meta-analysis
-10
-5
0
5
10
15
20
25
30
MajorCoronaryEvents
CoronaryDeaths
CV Deaths Non-CVDeaths
All-CauseDeaths
Re
lati
ve
Ris
k R
ed
uc
tio
n,
%
NS=not significant; CV=cardiovascularBirjmohun RS et al. J Am Coll Cardiol. 2005;45:185–197.
P<0.001
53 trials/16,802 patientsusing fibrates or placebo
P=NSP=NS
P=NSP=NS
9
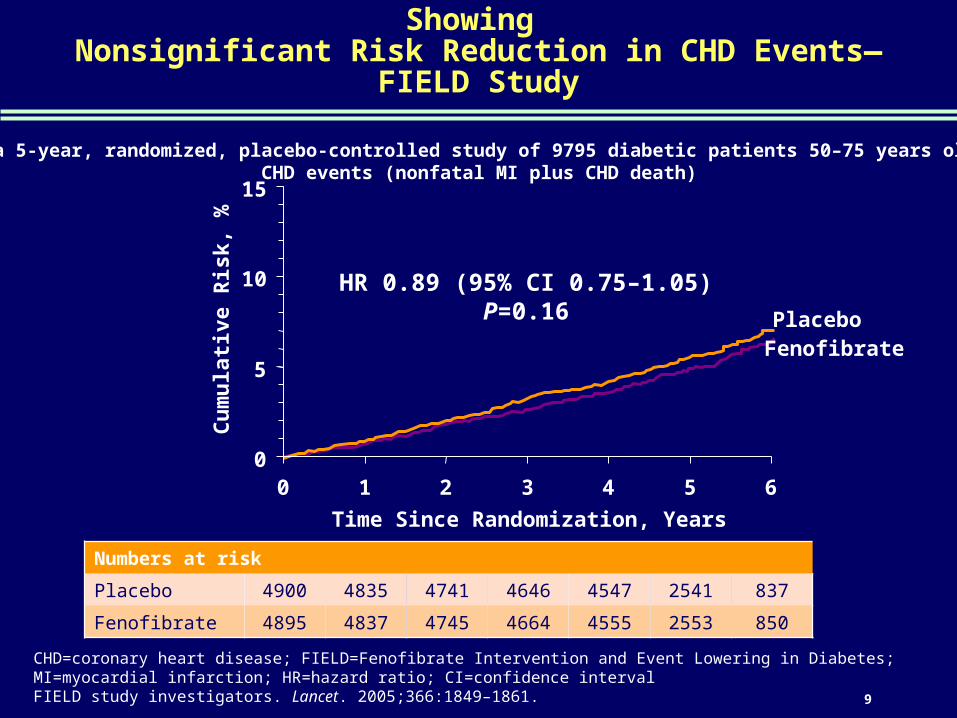
Cumulative Risk Curve of Time to First Event Showing Nonsignificant Risk Reduction in CHD Events—FIELD Study
CHD=coronary heart disease; FIELD=Fenofibrate Intervention and Event Lowering in Diabetes; MI=myocardial infarction; HR=hazard ratio; CI=confidence intervalFIELD study investigators. Lancet. 2005;366:1849–1861.
In a 5-year, randomized, placebo-controlled study of 9795 diabetic patients 50–75 years old, CHD events (nonfatal MI plus CHD death)
Numbers at risk
Placebo 4900 4835 4741 4646 4547 2541 837
Fenofibrate 4895 4837 4745 4664 4555 2553 850
PlaceboFenofibrate
HR 0.89 (95% CI 0.75–1.05)P=0.16
0
5
10
15
0 1 2 3 4 5 6
Time Since Randomization, Years
Cu
mu
lati
ve R
isk,
%
10
Challenges in Lipid Management
Niacin Effects on Lipids and Other Cardiovascular Disease (CVD) Risk Factors
11
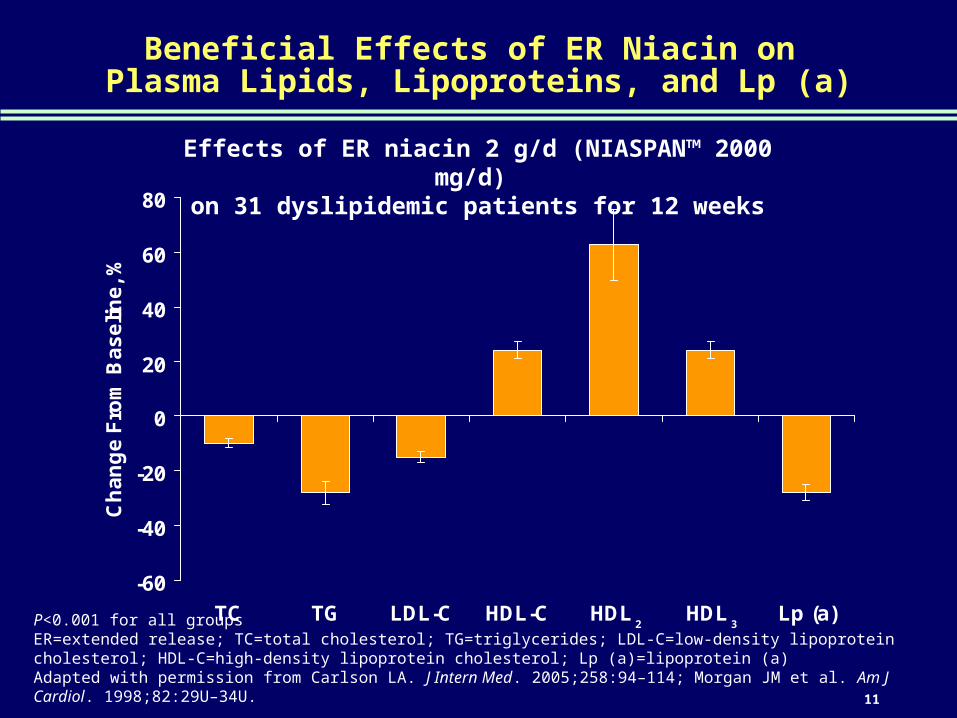
Beneficial Effects of ER Niacin on Plasma Lipids, Lipoproteins, and Lp (a)
P<0.001 for all groupsER=extended release; TC=total cholesterol; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; Lp (a)=lipoprotein (a)Adapted with permission from Carlson LA. J Intern Med. 2005;258:94–114; Morgan JM et al. Am J Cardiol. 1998;82:29U–34U.
-60
-40
-20
0
20
40
60
80
TC TG LDL-C HDL-C HDL HDL Lp (a)
Ch
an
ge
Fro
m B
as
eli
ne
, %
2 3
Effects of ER niacin 2 g/d (NIASPAN™ 2000 mg/d) on 31 dyslipidemic patients for 12 weeks
12
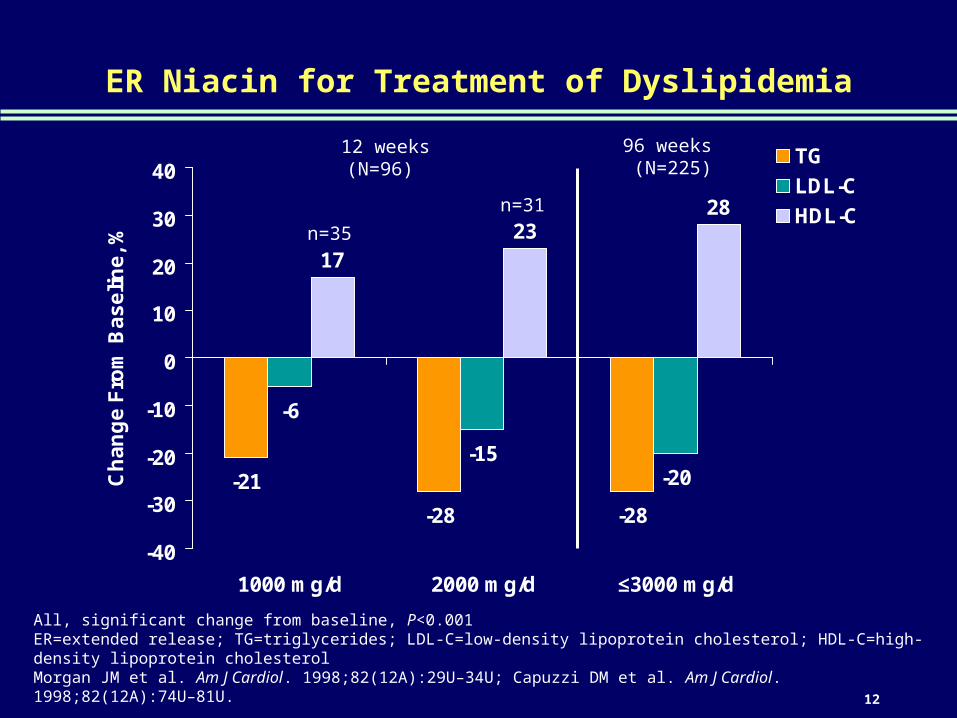
ER Niacin for Treatment of Dyslipidemia
-21
-28 -28
-6
-15-20
1723
28
-40
-30
-20
-10
0
10
20
30
40
1000 mg/d 2000 mg/d ≤3000 mg/d
Ch
an
ge
Fro
m B
as
eli
ne
, %
TG
LDL-C
HDL-C
12 weeks(N=96)
96 weeks (N=225)
All, significant change from baseline, P<0.001ER=extended release; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterolMorgan JM et al. Am J Cardiol. 1998;82(12A):29U–34U; Capuzzi DM et al. Am J Cardiol. 1998;82(12A):74U–81U.
n=35
n=31
13
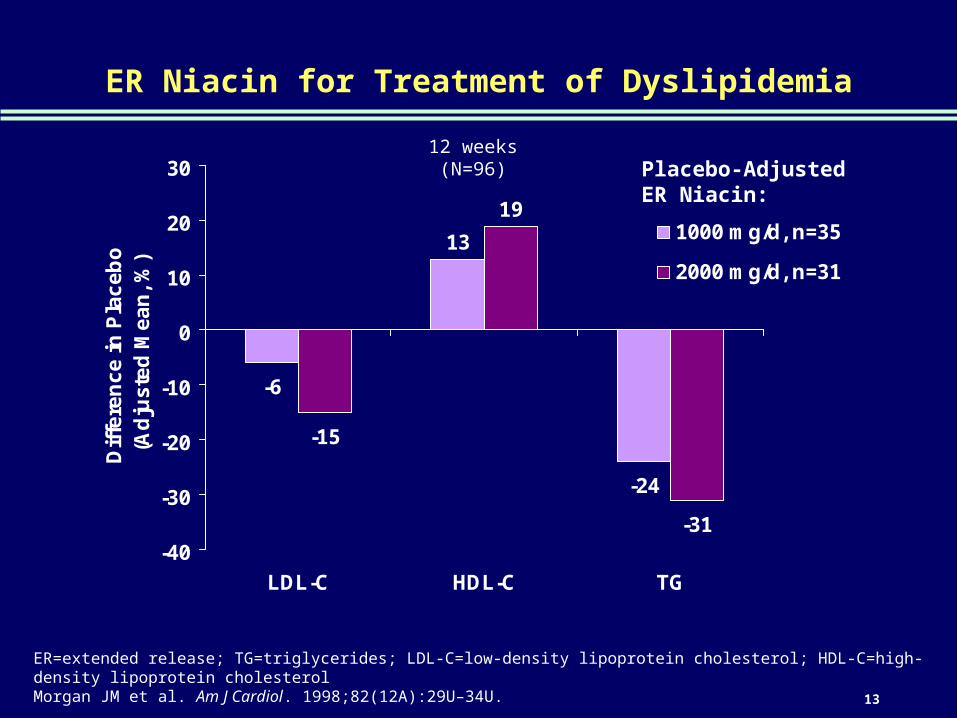
ER Niacin for Treatment of Dyslipidemia
-6
13
-24
-15
19
-31-40
-30
-20
-10
0
10
20
30
LDL-C HDL-C TG
Dif
fere
nc
e i
n P
lac
eb
o(A
dju
ste
d M
ea
n,
%)
1000 mg/d, n=35
2000 mg/d, n=31
12 weeks (N=96)
ER=extended release; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterolMorgan JM et al. Am J Cardiol. 1998;82(12A):29U–34U.
Placebo-Adjusted ER Niacin:

14
Effects on HDL-C, LDL-C, and TG Levels of Niacin in Combination With Colestipol or Statins
-50
-40
-30
-20
-10
0
10
20
30
40
50
HDL-C LDL-C TG
Ch
an
ge
Fro
m P
retr
ea
tme
nt,
%
Colestipol (30 g/d), IR Niacin (3–12 g/d), n=94
Colestipol (15–30 g/d), IR Niacin (0.25–4 g/d), n=36
Fluvastatin (20 mg/d), IR Niacin (<3 g/d), n=38
Pravastatin (20 mg/d), IR Niacin (3 g/d), n=27
Lovastatin (20 mg/d), IR Niacin (1.5 g/d), n=14
Simvastatin (10–20 mg/d), SR Niacin (2 g/d), n=33
HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; TG=triglycerides; IR=immediate release; SR=slow releaseCarlson LA. J Intern Med. 2005;258:94–114; Blankenhorn DH et al. JAMA. 1987;257:3233–3240; Brown G et al. N Engl J Med. 1990;323:1289–1298; Jacobson TA et al. Am J Cardiol. 1994;74:149–154; O’Keefe JH Jr et al. Am J Cardiol. 1995;76:480–484; Gardner SF et al. Pharmacotherapy. 1996;16:419–423; Brown BG et al. N Engl J Med. 2001;345:1583–1592.
15
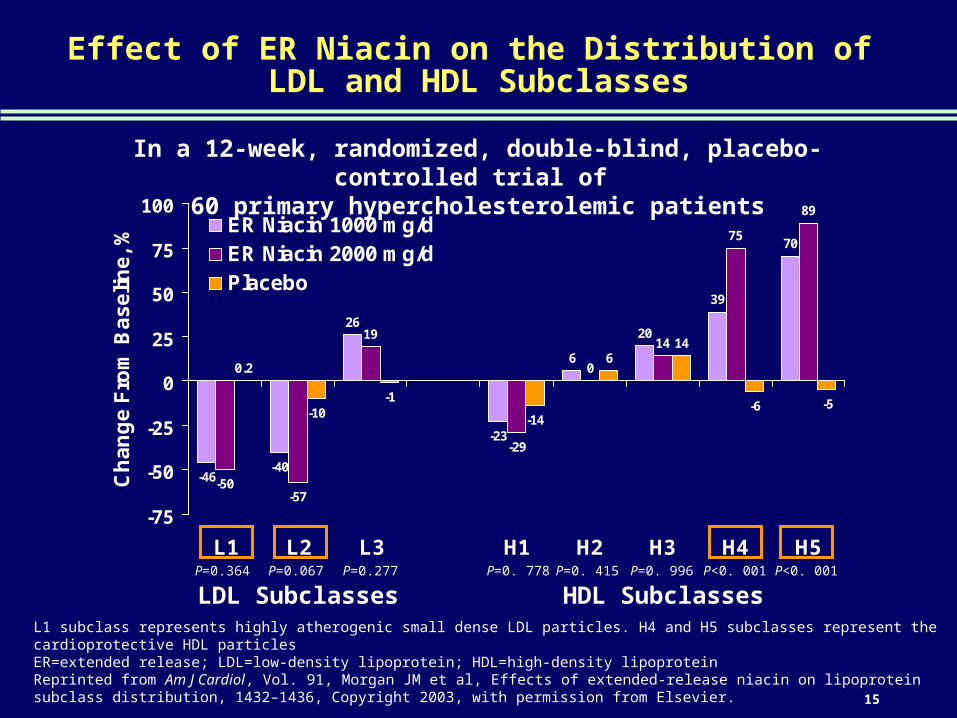
Effect of ER Niacin on the Distribution of LDL and HDL Subclasses
-46-40
26
-23
6
20
39
70
-50-57
19
-29
0
14
75
89
0.2
-10-1
-14
614
-6 -5
-75
-50
-25
0
25
50
75
100
L1 L2 L3 H1 H2 H3 H4 H5
Ch
an
ge
Fro
m B
as
eli
ne
, %
ER Niacin 1000 mg/dER Niacin 2000 mg/dPlacebo
L1 subclass represents highly atherogenic small dense LDL particles. H4 and H5 subclasses represent the cardioprotective HDL particlesER=extended release; LDL=low-density lipoprotein; HDL=high-density lipoprotein Reprinted from Am J Cardiol, Vol. 91, Morgan JM et al, Effects of extended-release niacin on lipoprotein subclass distribution, 1432–1436, Copyright 2003, with permission from Elsevier.
LDL Subclasses HDL SubclassesP=0.364 P=0.067 P=0.277 P=0. 778 P=0. 415 P=0. 996 P<0. 001 P<0. 001
In a 12-week, randomized, double-blind, placebo-controlled trial of 60 primary hypercholesterolemic patients
16
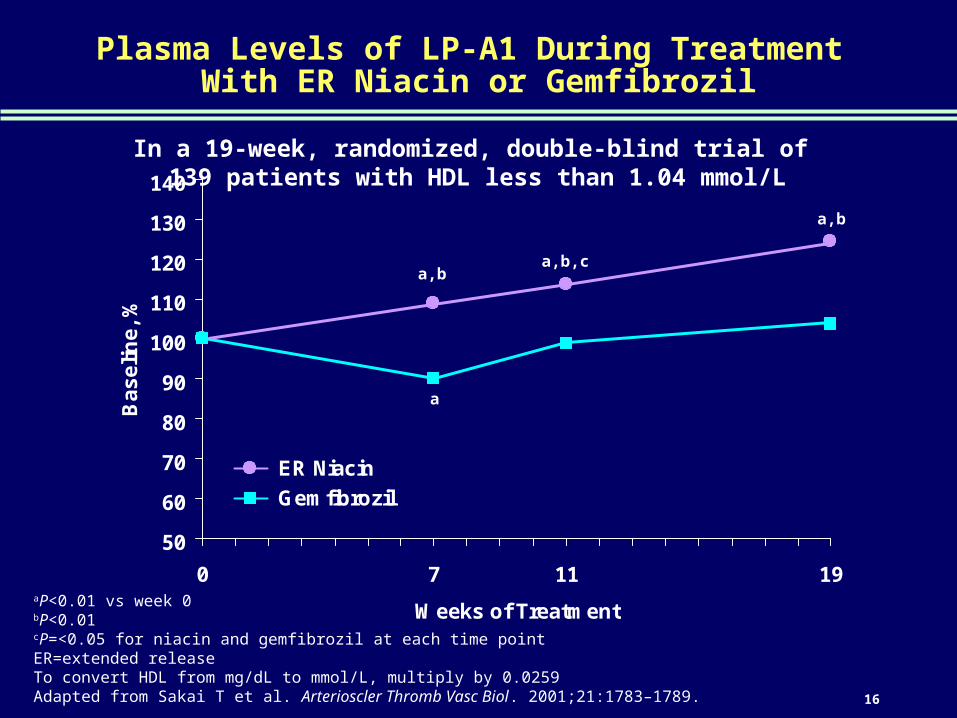
Plasma Levels of LP-A1 During Treatment With ER Niacin or Gemfibrozil
50
60
70
80
90
100
110
120
130
140
0 7 11 19
Weeks of Treatment
Ba
se
lin
e,
%
ER Niacin
Gemfibrozil
aP<0.01 vs week 0bP<0.01cP=<0.05 for niacin and gemfibrozil at each time pointER=extended releaseTo convert HDL from mg/dL to mmol/L, multiply by 0.0259Adapted from Sakai T et al. Arterioscler Thromb Vasc Biol. 2001;21:1783–1789.
a,ba,b,c
a,b
a
In a 19-week, randomized, double-blind trial of 139 patients with HDL less than 1.04 mmol/L

17
Effect of ER Niacin vs Gemfibrozil on Lipid Parameters
-60
-40
-20
0
20
40
HDL-C LDL-C TG
ER=extended release; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; TG=triglycerides; apo A-1=apolipoprotein A-1; Lp (a)=lipoprotein (a)Adapted with permission from Guyton JR et al. Arch Intern Med. 2000;160:1177–1184. Copyright © 2000, American Medical Association. All rights reserved.
-25
-20
-15
-10
-5
0
LDL-C/HDL-C TG/HDL-C
ER Niacin 2000 mg
Gemfibrozil 600 mg BID
Ch
ang
e F
rom
Bas
elin
e, %
-15
-10
-5
0
5
10
15
apo A-1 apo B
-30
-20
-10
0
10
20
Lp (a) Fibrinogen
P<0.001
P=0.004P=0.02
P=0.001
P=0.06
P<0.001 P=0. 005
P=0.01
P<0.001
In a randomized, double-blind trial of 173 patients 21–75 years old

18
Challenges in Lipid Management
Niacin Mechanism of Action

19
Niacin Acts Through Nicotinic Acid Receptors on Multiple Tissues
Adipocytes Immune Cells (Spleen, Lymphoid Cells, Lung)
Epidermal Langerhans’ Cells
Niacin
Antilipolytic effects
Probableantiinflammatory
effectPLA2
Arachidonic acid
PGD2
GPR109A
Flushing
NiacinNiacin
PLA2=phospholipase A2; PGD2=prostaglandin D2
Adapted from Pike NB. 2005;115:3400–3403. Journal of Clinical Investigation. Online by Pike. Copyright 2005 by American Society for Clinical Investigation. Reproduced with permission of American Society for Clinical Investigation in the format presentation via Copyright Clearance Center; Yu BL et al. Med Hypotheses. 2007;69:90–94.
20
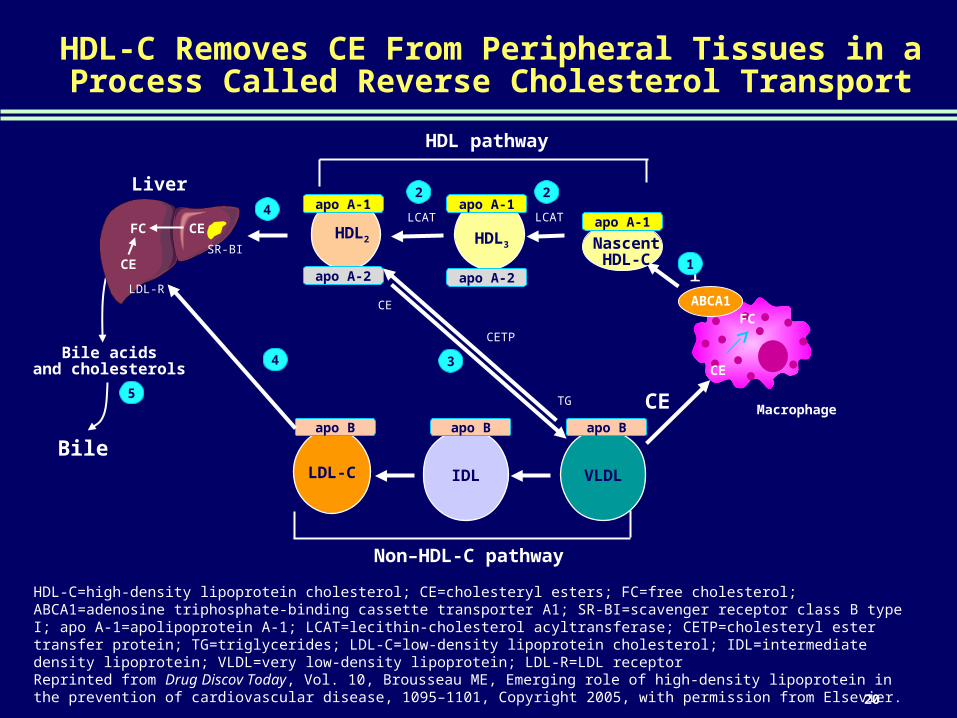
HDL-C Removes CE From Peripheral Tissues in a Process Called Reverse Cholesterol Transport
ABCA1
Macrophage
CE
FC
11HDL2 HDL3 Nascent
HDL-C
HDL pathway
apo A-1apo A-1apo A-1
apo A-2 apo A-2
LCATLCAT
22
CE
VLDLIDLLDL-C
Non–HDL-C pathway
apo B apo B apo B
CE
TG
CETP
3Bile acids
and cholesterols
Bile
5
HDL-C=high-density lipoprotein cholesterol; CE=cholesteryl esters; FC=free cholesterol; ABCA1=adenosine triphosphate-binding cassette transporter A1; SR-BI=scavenger receptor class B type I; apo A-1=apolipoprotein A-1; LCAT=lecithin-cholesterol acyltransferase; CETP=cholesteryl ester transfer protein; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; IDL=intermediate density lipoprotein; VLDL=very low-density lipoprotein; LDL-R=LDL receptorReprinted from Drug Discov Today, Vol. 10, Brousseau ME, Emerging role of high-density lipoprotein in the prevention of cardiovascular disease, 1095–1101, Copyright 2005, with permission from Elsevier.
4
Liver
CEFC
CE
LDL-R
4
SR-BI

21
Niacin Significantly Increases Cholesterol Exporter ABCA1
aP<0.05bP<0.01 ABCA1=adenosine triphosphate-binding cassette transporter A1; SEM=standard error of mean; dHDL=delipidated HDLReprinted from Biochem Pharmacol, Vol. 67, Rubic T et al, Stimulation of CD36 and the key effector of reverse cholesterol transport ATP-binding cassette A1 in monocytoid cells by niacin, 411–419, Copyright 2004, with permission from Elsevier.
0
50
100
150
200
250
300
Control Niacin
Co
ntr
ol
(SE
M),
%
3 h
48 h
0
20
40
60
80
100
120
Co
ntr
ol
(SE
M),
%
Baseline After Exposure to:
dHDL Niacin Both
a
aa
b
b
ABCA1 Cellular Cholesterol Content

22
Niacin and Reverse Cholesterol Transport
Bile acidsand cholesterols
Bile
HDL2 HDL3 Nascent HDL-C
HDL pathway
CE
Liver
CEFC
CE
ABCA1
Macrophage
VLDLIDLLDL-C
Non–HDL-C pathway
CE
FC
apo A-1apo A-1apo A-1
apo A-2 apo A-2
LCATLCAT
SR-BI
LDL-R
apo B apo B apo B
CE
TG
CETP
11
22
3
4
4
5
Nascent HDL-C
Nascent HDL-C
Niacinapo A-1
apo A-1
HDL-C=high-density lipoprotein cholesterol; CE=cholesteryl esters; FC=free cholesterol; ABCA1=adenosine triphosphate-binding cassette transporter A1; SR-BI=scavenger receptor class B type I; LDL-R=LDL receptor; apo A-1=apolipoprotein A-1; LCAT=lecithin-cholesterol acyltransferase; CETP=cholesteryl ester transfer protein; TG=triglycerides; LDL-C=low-density lipoprotein cholesterol; IDL=intermediate density lipoprotein; VLDL=very low-density lipoproteinReprinted from Drug Discov Today, Vol. 10, Brousseau ME, Emerging role of high-density lipoprotein in the prevention of cardiovascular disease, 1095–1101, Copyright 2005, with permission from Elsevier; Rubic T et al. Biochem Pharmacol. 2004;67:411–419; McKenney J. Am J Health-Syst Pharm. 2003;60:995–1005.
23
Effects of Niacin on Lipoprotein Metabolism Summary
Partial inhibition of release of FFAs from adipose tissue, leading to a decrease in TG synthesis by the liver
– Decreased TG synthesis reduces the synthesis of VLDL, the precursor of LDL-C, and eventually decreases LDL-C
Inhibition of synthesis of apo B, which is needed for the formation of VLDL particles and enhanced VLDL catabolism
Favorable LDL particle size transformation, with shift from small, dense to large, bouyant particles
Reduced extraction and catabolism of apo A-1 from HDL-C, maintaining structure and function of HDL-C particles
Stimulation of the expression of membrane cholesterol transporter ABCA1
FFAs=free fatty acids; TG=triglyceride; VLDL=very low-density lipoprotein; LDL-C=low-density lipoprotein cholesterol; apo B=apolipoprotein B; apo A-1=apolipoprotein A-1; HDL-C=high-density lipoprotein cholesterol; ABCA1=adenosine triphosphate-binding cassette transporter A1McKenney J. Am J Health-Syst Pharm. 2003;60:995–1005; Carlson LA. J Intern Med. 2005;258:94–114.

24
Antiinflammatory Actions of ER Niacin That May Be Beneficial Against Atherosclerosis
Emerging clinical studies suggest that ER niacin may reduce inflammation by a variety of mechanisms unrelated to its antiatherosclerotic lipid-altering effects
ER niacin appears to attenuate overexpression of NOS
ER niacin has been shown to reduce plasma CRP levels
ER niacin has been shown to decrease levels of lipoprotein-associated phospholipase A2
ER niacin has been shown to increase levels of the antiinflammatory adipokine, adiponectin
ER=extended release; NOS=nitric oxide synthase; CRP=C-reactive proteinYu BL et al. Med Hypotheses. 2007;69:90–94.

25
Randomized Controlled Clinical Trials of Nicotinic Acid and Effect on HDL-C and Atherosclerosis
Nicotinic Acid and Atherosclerosis: A Positive Effect in Imaging Studies
SourceImaging Studies
Special Agent(s)
Patients Receiving Treatment n/Total (%)
Increase in HDL-C Levels
%
Follow-up
Duration y Outcomesa
CLAS I Niacin + colestipol 94/188 (50.0) 37 2 Decreased coronary atherosclerosis
CLAS II Niacin + colestipol 75/138 (54.3) 37 4 Decreased coronary atherosclerosis
FATS Niacin + colestipol 48/146 (32.9) 43 2.5 Decreased coronary atherosclerosis;Decreased death, MI, or revascularization (secondary outcome)
CLAS Fem Niacin + colestipol 80/162 (49.4) 38 2 Decreased femoral atherosclerosis
CLAS IMT Niacin + colestipol 39/78 (50.0) 38 4 Decreased carotid IMT (regression also observed at 1 and 2 y)
SCRIP Niacin + colestipol + gemfibrozil + lovastatin + aggressive lifestyle modification
145/300 (48.3) 12 4 Decreased coronary atherosclerosis; Decreased frequency of new coronary lesion formation
ARBITER 2 Niacin + statin 87/167 (52.1) 21 1 Decreased carotid IMT (P>0.05)
ARBITER 3 Niacin + statin 87/167 (52.1) 23 2 Decreased carotid IMT
ARBITER=Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol; CLAS=Cholesterol-Lowering Atherosclerosis Study; CLAS Fem=femoral atherosclerosis group of CLAS; CLAS IMT=carotid ultrasound group of CLAS; FATS=Familial Atherosclerosis Treatment Study; HDL-C=high-density lipoprotein cholesterol; IMT=intima-media thickness; MI=myocardial infarction; SCRIP=Stanford Coronary Risk Intervention ProjectaDeath indicates all-cause mortality
Adapted with permission from Singh IM et al. JAMA. 2007;298:786–798. Copyright © 2007, American Medical Association. All rights reserved.

26
CLAS: Changes in Carotid Artery Intima-Media Thickness
-0.06
-0.04
-0.02
0
0.02
0.04
0.06
0.08
Year 2 vs Baseline Year 4 vs Baseline Year 4 vs Year 2
Me
an
Ch
an
ge
, m
m
Placebo, n=22
Niacin + Colestipol, n=24
aVs drug groupCLAS=Cholesterol-Lowering Atherosclerosis StudyBlankenhorn DH et al. Circulation. 1993;88:20–28.
P<0.0001a
P<0.0001a
P=0.06a
In a randomized, placebo-controlled angiographic trial of 188 nonsmoking men with progressive atherosclerosis
27
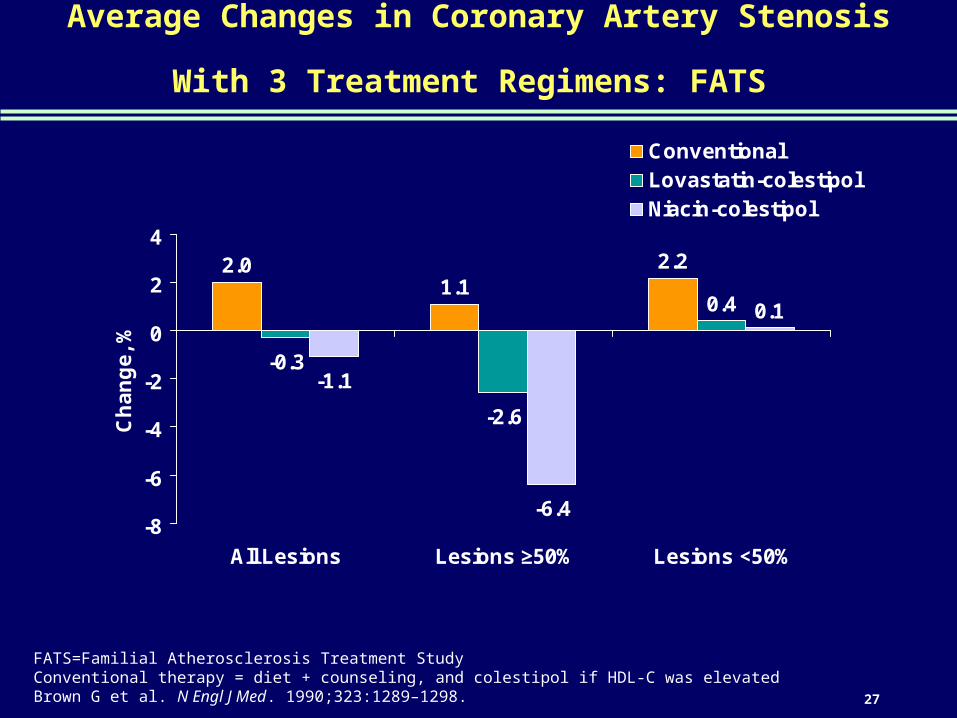
Average Changes in Coronary Artery Stenosis With 3 Treatment Regimens: FATS
2.01.1
2.2
-0.3
-2.6
0.4
-1.1
-6.4
0.1
-8
-6
-4
-2
0
2
4
All Lesions Lesions ≥50% Lesions <50%
Ch
an
ge
, %
ConventionalLovastatin-colestipolNiacin-colestipol
FATS=Familial Atherosclerosis Treatment StudyConventional therapy = diet + counseling, and colestipol if HDL-C was elevatedBrown G et al. N Engl J Med. 1990;323:1289–1298.
28
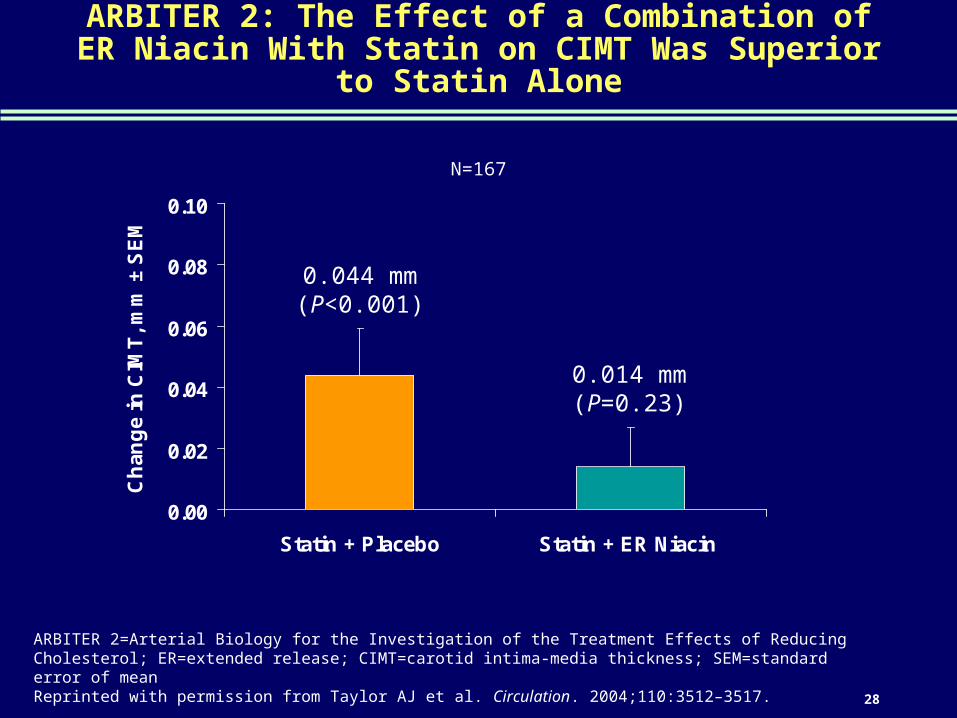
ARBITER 2: The Effect of a Combination of ER Niacin With Statin on CIMT Was Superior to Statin Alone
0.00
0.02
0.04
0.06
0.08
0.10
Statin + Placebo Statin + ER Niacin
Ch
ang
e in
CIM
T,
mm
± S
EM
0.044 mm(P<0.001)
0.014 mm(P=0.23)
ARBITER 2=Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol; ER=extended release; CIMT=carotid intima-media thickness; SEM=standard error of meanReprinted with permission from Taylor AJ et al. Circulation. 2004;110:3512–3517.
N=167
29
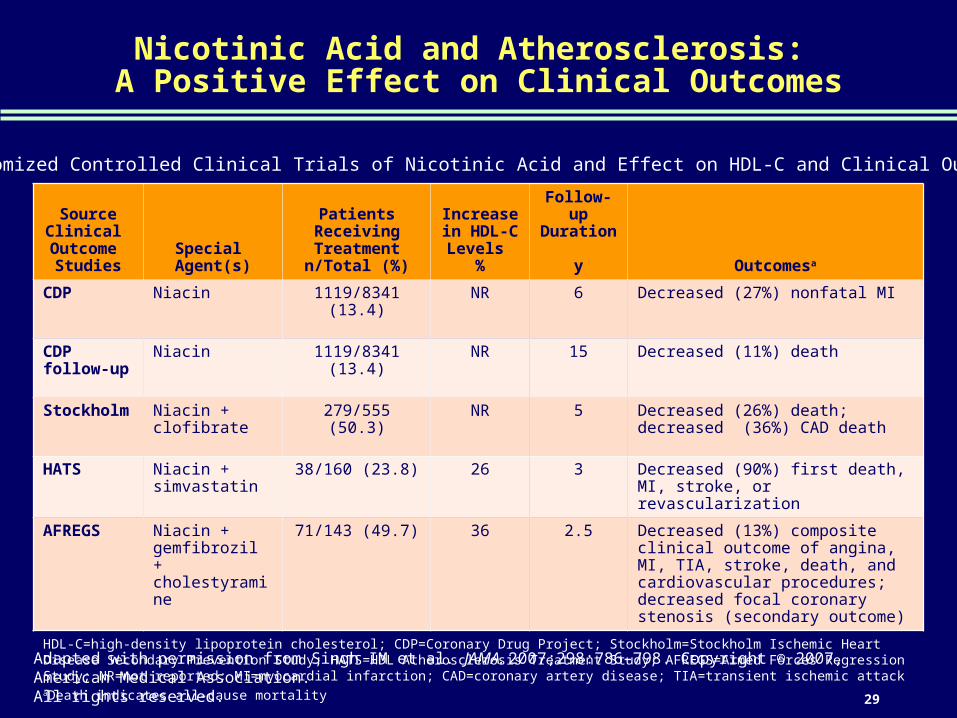
Nicotinic Acid and Atherosclerosis: A Positive Effect on Clinical Outcomes
Randomized Controlled Clinical Trials of Nicotinic Acid and Effect on HDL-C and Clinical Outcomes
SourceClinical
Outcome Studies
Special Agent(s)
Patients Receiving Treatment n/Total (%)
Increase in HDL-C Levels
%
Follow-up Duration
y Outcomesa
CDP Niacin 1119/8341 (13.4) NR 6 Decreased (27%) nonfatal MI
CDP follow-up
Niacin 1119/8341 (13.4) NR 15 Decreased (11%) death
Stockholm Niacin + clofibrate
279/555 (50.3) NR 5 Decreased (26%) death; decreased (36%) CAD death
HATS Niacin + simvastatin
38/160 (23.8) 26 3 Decreased (90%) first death, MI, stroke, or revascularization
AFREGS Niacin + gemfibrozil + cholestyramine
71/143 (49.7) 36 2.5 Decreased (13%) composite clinical outcome of angina, MI, TIA, stroke, death, and cardiovascular procedures; decreased focal coronary stenosis (secondary outcome)
HDL-C=high-density lipoprotein cholesterol; CDP=Coronary Drug Project; Stockholm=Stockholm Ischemic Heart Disease Secondary Prevention Study; HATS=HDL Atherosclerosis Treatment Study; AFREGS=Armed Forces Regression Study; NR=not reported; MI=myocardial infarction; CAD=coronary artery disease; TIA=transient ischemic attackaDeath indicates all-cause mortality
Adapted with permission from Singh IM et al. JAMA. 2007;298:786–798. Copyright © 2007, American Medical Association. All rights reserved.
30
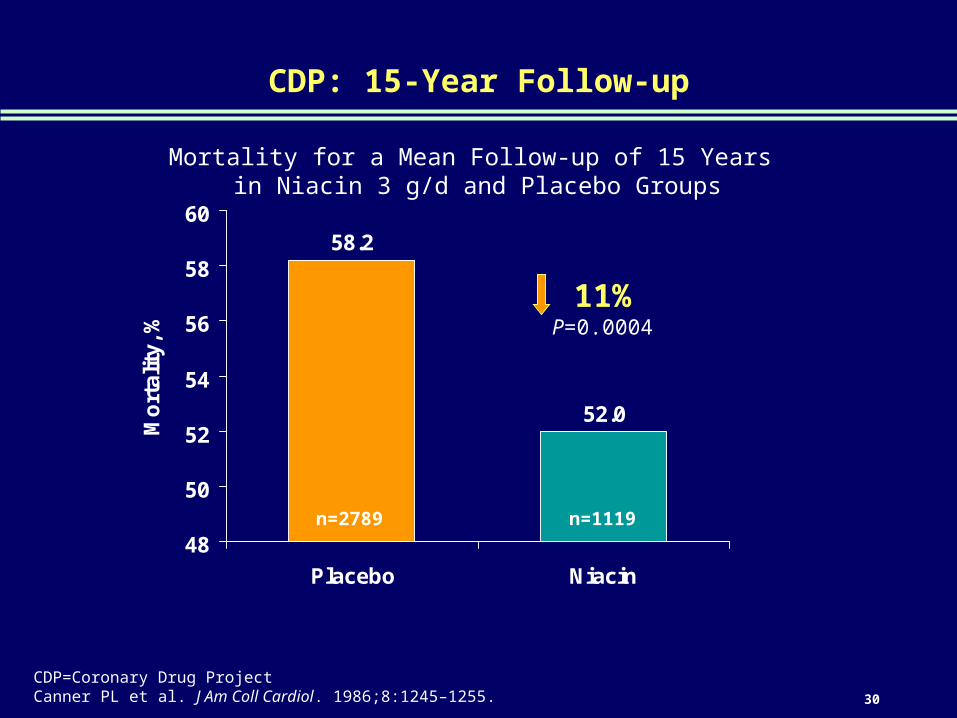
CDP: 15-Year Follow-up
Mortality for a Mean Follow-up of 15 Years in Niacin 3 g/d and Placebo Groups
CDP=Coronary Drug ProjectCanner PL et al. J Am Coll Cardiol. 1986;8:1245–1255.
58.2
52.0
48
50
52
54
56
58
60
Placebo Niacin
Mo
rta
lity
, %
11%P=0.0004
n=2789 n=1119

31
HATS—Niacin and Statin Outcome Trial
aComposite of coronary death, nonfatal MI, revascularization, hospitalization for confirmed ischemiaHATS=HDL Atherosclerosis Treatment StudyBrown BG et al. N Engl J Med. 2001;345:1583–1592.
12
1
11
6
0
2
4
6
8
10
12
14
Placebo Simvastatin-Niacin
AntioxidantVitamins
Simvastatin-Niacin Plus
Antioxidants
Ev
en
ts,
n
P=0.003vs Placebo
a
n=38 n=38 n=42 n=42
32
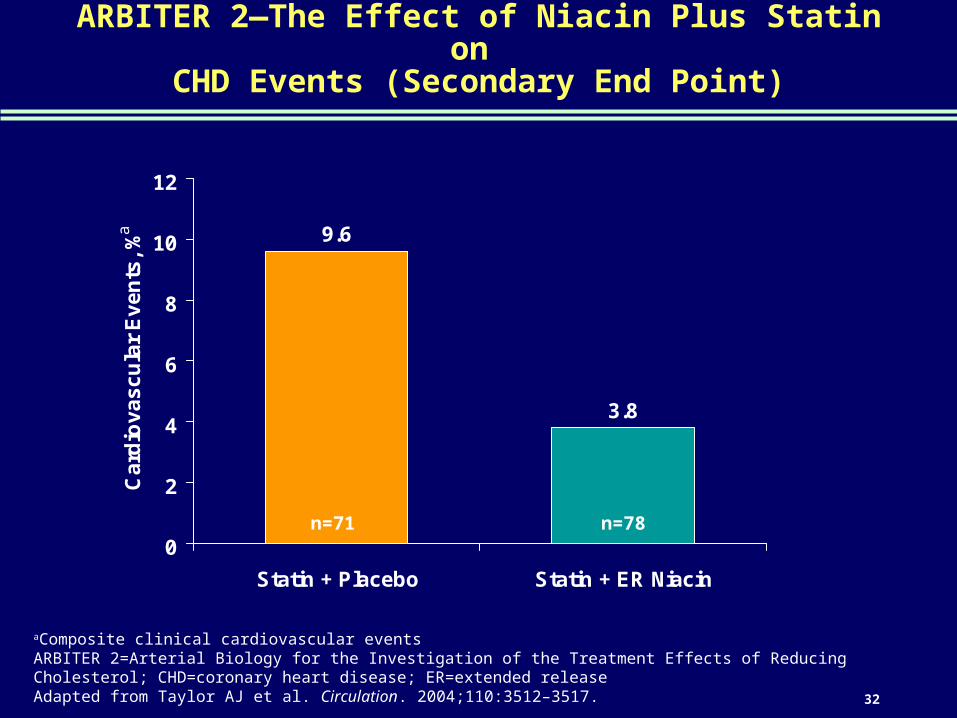
ARBITER 2—The Effect of Niacin Plus Statin on CHD Events (Secondary End Point)
aComposite clinical cardiovascular eventsARBITER 2=Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol; CHD=coronary heart disease; ER=extended releaseAdapted from Taylor AJ et al. Circulation. 2004;110:3512–3517.
9.6
3.8
0
2
4
6
8
10
12
Statin + Placebo Statin + ER Niacin
Ca
rdio
va
sc
ula
r E
ve
nts
, %
a
n=71 n=78

33
Niacin Side Effects
Challenges in Lipid Management

34
Major Side Effects of Niacin
ER=extended releaseCarlson LA. J Intern Med. 2005;258:94–114; Niaspan® [package insert]; 2007.
A temporary, dose-dependent skin flush—pronounced cutaneous vasodilation—induced by niacin occurs shortly after oral dosing– The niacin flush is thought to be the side effect that has limited
niacin’s clinical use
An increase in plasma uric acid levels is also seen regularly during niacin treatment– This effect is most clinically significant in patients with joint
problems and/or high pretreatment urate levels
Gastrointestinal side effects (gastritis-like) may occur in patients taking niacin
Other adverse events that have been reported with ER niacin in ≥5% of patients include– Headache – Rhinitis – Rash
– Pain (myalgia) – Pruritis

35
ER Niacin—Contraindications and Warnings
ER=extended release; IR=immediate release; HMG-CoA=hepatic hydroxymethyl glutaryl coenzyme ANiaspan® [package insert]; 2007.
Contraindicated in patients with
– Known hypersensitivity to niacin or its components
– Significant or unexplained hepatic dysfunction
– Active peptic ulcer disease
– Arterial bleeding
Warnings
– ER niacin should not be substituted for equivalent doses of IR niacin
– Cases of severe hepatic toxicity have occurred in patients substituting sustained release niacin products for IR niacin at equivalent doses
– Patients should be warned against substantial quantities of alcohol intake
– ER niacin should be used with caution in patients with a past history of liver disease
– Liver tests should be performed on all patients during therapy
– Rare cases of rhabdomyolysis have been associated with concomitant administration of niacin and HMG-CoA reductase inhibitors

36
Effect of ER Niacin on Glycemic Control in Diabetes Mellitus
0
2
4
6
8
10
Placebo ER Niacin 1000 mg/d ER Niacin 1500 mg/d
Baseline Week 4 Week 8 Week 12 Week 16aP=0.05ER=extended release; HbA1C=glycosylated hemoglobinReprinted with permission from Grundy SM et al. Arch Intern Med. 2002;162:1568–1576. Copyright © 2002, American Medical Association. All rights reserved.
Hb
A1C
, %
a
n=49 n=45 n=52
37
Summary
Niacin decreases FFA release and stimulates RCT, resulting in decreased triglycerides and LDL-C and increased HDL-C
Niacin also favorably affects HDL and LDL particle size and has antiinflammatory effects
These varied effects make niacin unique in its ability to broadly modify lipoprotein levels in a way that is beneficial for CVD risk
An important drawback to niacin use is the skin flush that occurs in some patients shortly after dosing
FFA=free fatty acid; RCT=reverse cholesterol transport; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; CVD=cardiovascular disease
38
Bibliography

39
Bibliography (continued)
40
Challenges in Lipid Management
Before prescribing, please consult the manufacturers’ prescribing information.
Merck does not recommend the use of any product in any different manner than as described
in the prescribing information.
Copyright © 2008 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved. 12-08 M524A-2007-W-1245907-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT WWW.MERCK.COM
41
Back-up
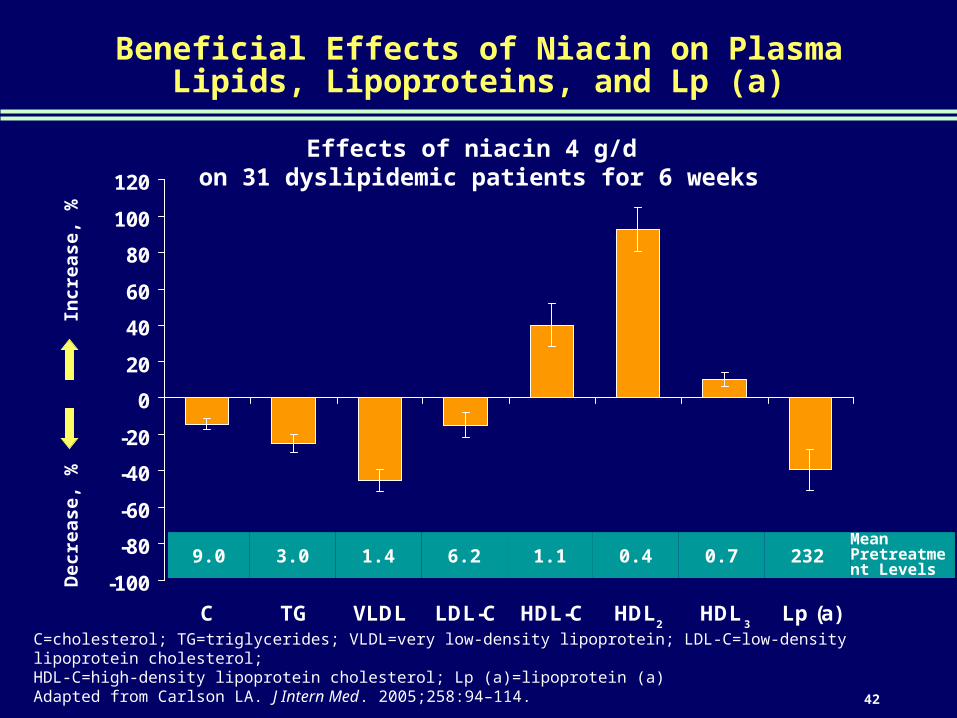
42
Beneficial Effects of Niacin on Plasma Lipids, Lipoproteins, and Lp (a)
-100
-80
-60
-40
-20
0
20
40
60
80
100
120
C TG VLDL LDL-C HDL-C HDL HDL Lp (a)
Effects of niacin 4 g/d on 31 dyslipidemic patients for 6 weeks
C=cholesterol; TG=triglycerides; VLDL=very low-density lipoprotein; LDL-C=low-density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; Lp (a)=lipoprotein (a)Adapted from Carlson LA. J Intern Med. 2005;258:94–114.
Incr
ease
, %
Dec
reas
e, %
9.0 3.0 1.4 6.2 1.1 0.4 0.7 232Mean Pretreatment Levels
2 3
Related Documents











