April 2005 WHO/STB/THD 1 World Health Organization "The international experience of DOTS- "The international experience of DOTS- Plus and Plus and the Green Light Committee mechanism" the Green Light Committee mechanism" Dr Ernesto Jaramillo Dr Ernesto Jaramillo Medical Officer, WHO/HTM/STB/THD Medical Officer, WHO/HTM/STB/THD

1 April 2005 WHO/STB/THD World Health Organization "The international experience of DOTS-Plus and the Green Light Committee mechanism" Dr Ernesto Jaramillo.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

April 2005 WHO/STB/THD 1World Health Organization
"The international experience of DOTS-Plus and "The international experience of DOTS-Plus and the Green Light Committee mechanism" the Green Light Committee mechanism"
Dr Ernesto JaramilloDr Ernesto JaramilloMedical Officer, WHO/HTM/STB/THD Medical Officer, WHO/HTM/STB/THD
April 2005 WHO/STB/THD 2
DOTS-PlusDOTS-Plus
The strategy designed to manage MDR-TB using
second-line anti-TB drugs within the DOTS strategystrategy in
low- and middle-income countries.
DISCLAIMER: DOTS-Plus means DOTS firstDISCLAIMER: DOTS-Plus means DOTS first
April 2005 WHO/STB/THD 3
The ‘Green Light Committee’ mechanism of the The ‘Green Light Committee’ mechanism of the Stop TB PartnershipStop TB Partnership
The mechanism of WHO and its partners of the Stop TB Partnership to
enabling access to second-line anti-TB drugs in low- and middle-
income countries to treat multidrug resistant tuberculosis under
programmatic conditions and following specific guidelines
(Guidelines for implementing DOTS-Plus projects for the
management of MDR-TB).

April 2005 WHO/STB/THD 4
The ‘Green Light Committee’ mechanism of the The ‘Green Light Committee’ mechanism of the Stop TB PartnershipStop TB Partnership
DOTS-Plus and the GLC mechanism: a comprehensive response to…
– Evidence that basic DOTS was not enough to control TB and MDR-
TB
– Global widespread misuse of second-line TB drugs
– Failure of the market of second-line TB drugs
– Lack of policy to manage and control MDR-TB

April 2005 WHO/STB/THD 5
A market failure: management of MDR-TB before A market failure: management of MDR-TB before the creation of the GLC mechanism the creation of the GLC mechanism
High Cost of Treatment
Insufficient response to demand
Lack of evidence on feasibility and cost-effectiveness
Lack of Policy
Lack of Drug Demand
Situation on low and middle income countries
April 2005 WHO/STB/THD 6
Response to MDR-TB by linking conceptsResponse to MDR-TB by linking concepts
GLCGLCmechanismmechanism
ACCESSACCESSPrice & qualityPrice & quality
RATIONAL RATIONAL USE OF USE OF DRUGSDRUGS
POLICY POLICY FOR TB FOR TB
CONTROLCONTROL

April 2005 WHO/STB/THD 7
Advantages of applying to the WHO GLC mechanismAdvantages of applying to the WHO GLC mechanism
Access to quality-assured drugs following international accepted standards (including WHO)
Access to low-cost drugs
Access to a continuous drug supply, essential for treatment success
Access to technical assistance to ensure rational drug use
April 2005 WHO/STB/THD 8
Advantages of applying to the WHO GLC mechanismAdvantages of applying to the WHO GLC mechanism
Access to an external monitoring mechanism
Increased rational use of drugs
Creation of wide evidence base for national policy development
Ensures consolidation of DOTS as the strategy to control TB
April 2005 WHO/STB/THD 9
0
5
10
15
20
25
30
35
2000 2001 2002 2003 2004 2005
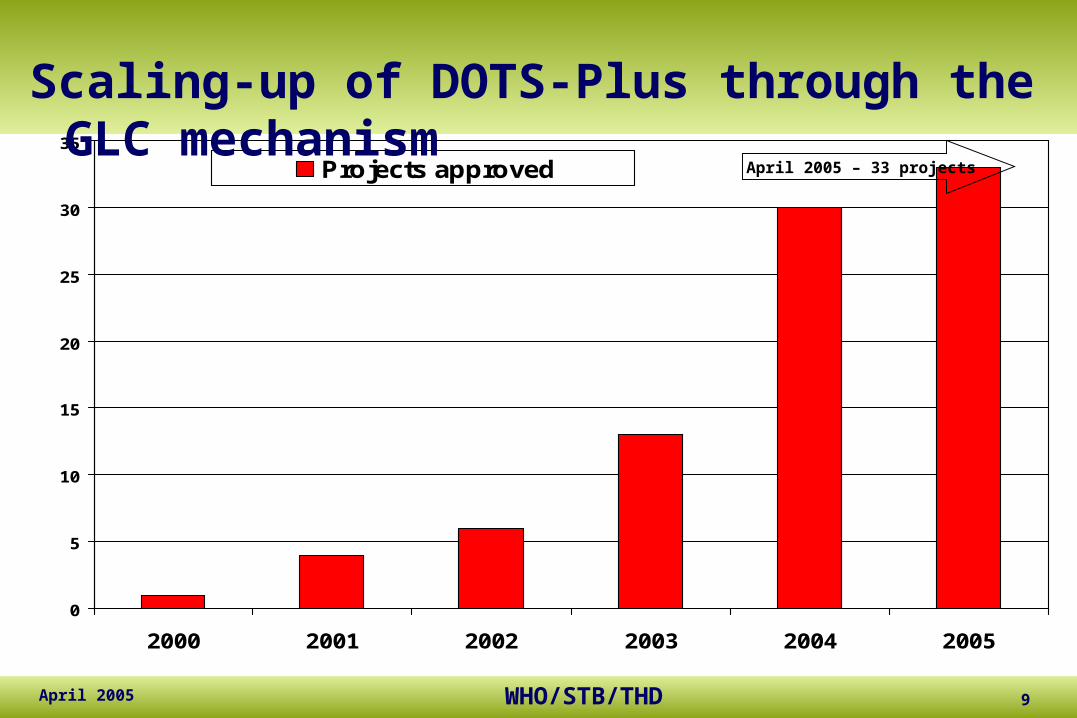
Projects approved April 2005 – 33 projects
Scaling-up of DOTS-Plus through the GLC mechanism
April 2005 WHO/STB/THD 10
0
2000
4000
6000
8000
10000
12000
2000 2001 2002 2003 2004 2005
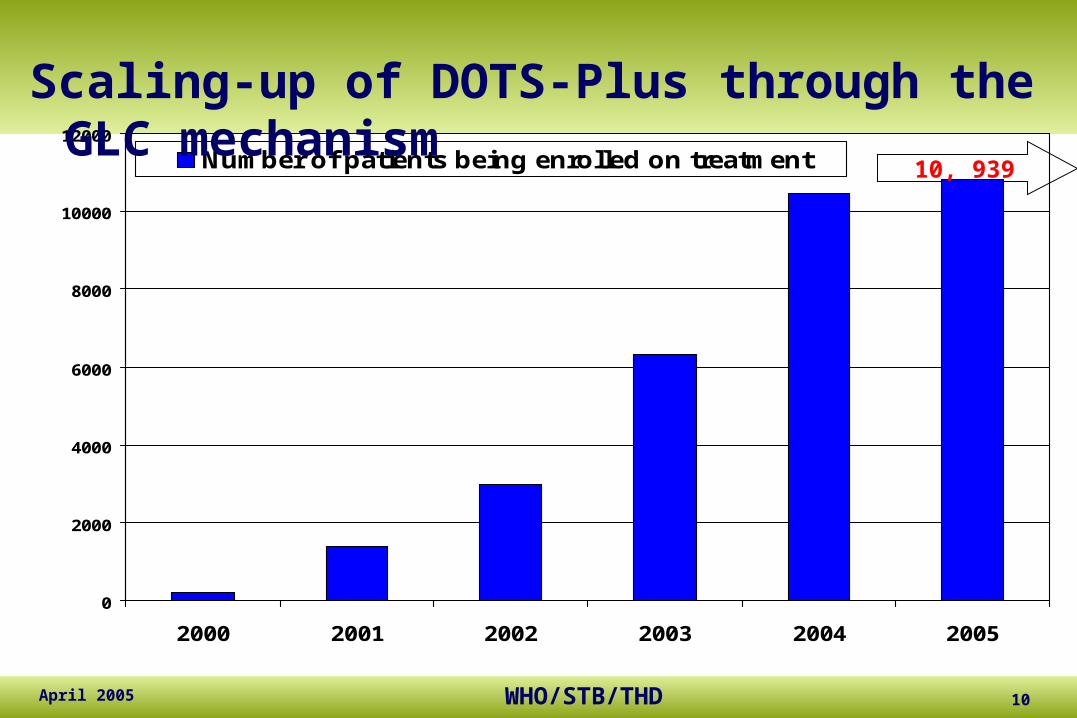
Number of patients being enrolled on treatment 10, 939
Scaling-up of DOTS-Plus through the GLC mechanism
April 2005 WHO/STB/THD 11
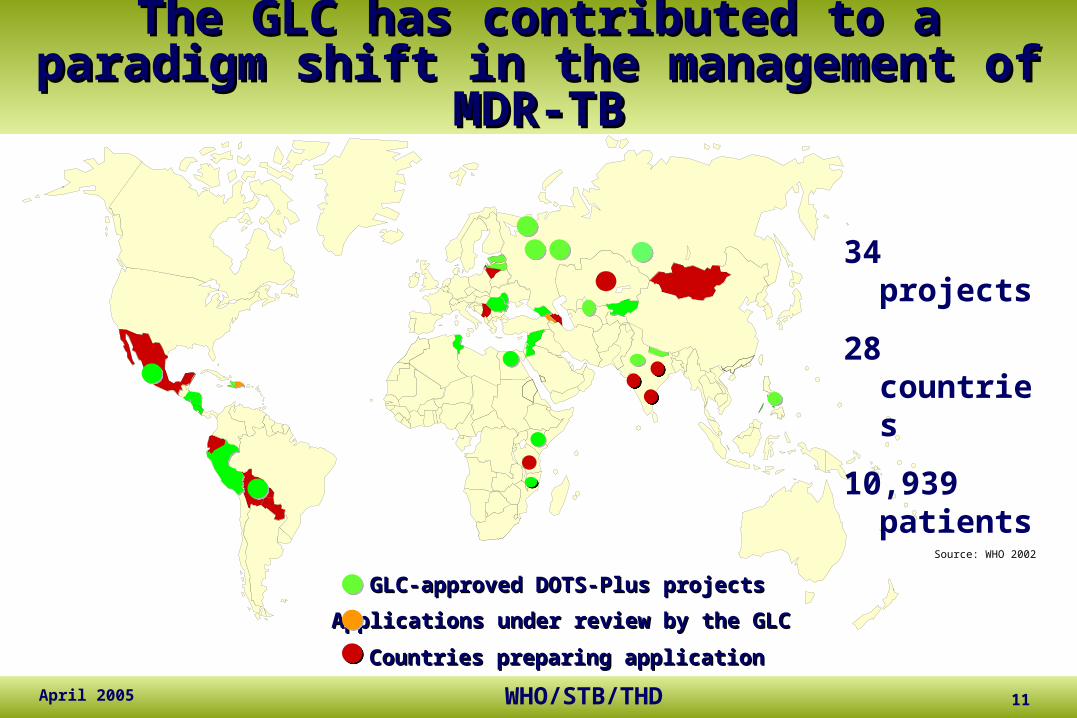
The GLCThe GLC has contributed to a paradigm shift has contributed to a paradigm shift in the management of MDR-TBin the management of MDR-TB
Source: WHO 2002
Applications under review by the GLCApplications under review by the GLC
GLC-approved DOTS-Plus projectsGLC-approved DOTS-Plus projects
Countries preparing applicationCountries preparing application
34 projects
28 countries
10,939 patients

April 2005 WHO/STB/THD 12
The ‘Green Light Committee’ mechanismThe ‘Green Light Committee’ mechanism
…has contributed to demonstrate that:
– Market of SLDs can be increased and be rationally handled
– DOTS-Plus is feasible, effective and cost-effective
– Integration of DOTS-Plus into regular DOTS is feasible and
strengthens regular DOTS programmes
April 2005 WHO/STB/THD 13
DOTS-Plus and the ‘Green Light DOTS-Plus and the ‘Green Light Committee’ mechanism: a learning Committee’ mechanism: a learning
experience for all!experience for all! …by creatively sailing in non-chartered waters, the Working Group on DOTS-
Plus and its subgroups have contributed to demonstrate that:
– Market of SLDs can be increased and be rationally handled
– DOTS-Plus is feasible, effective and cost-effective
– Integration of DOTS-Plus into regular DOTS is feasible and
strengthens regular DOTS programmes
April 2005 WHO/STB/THD 14
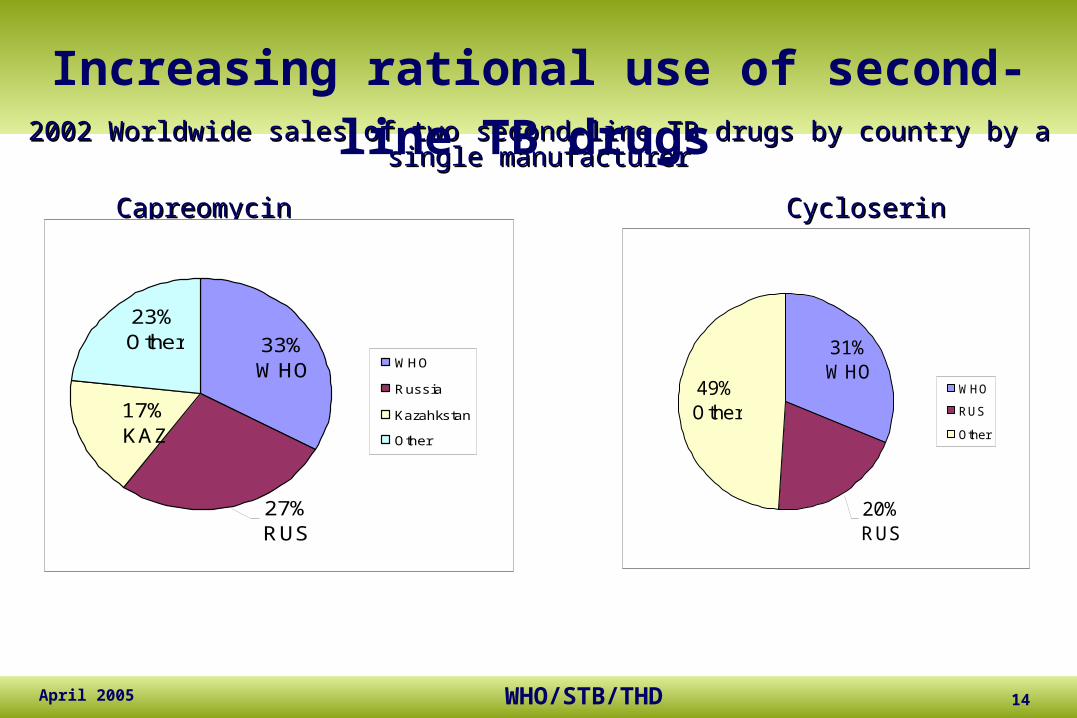
2002 Worldwide sales of two second-line TB drugs by country by a single manufacturer2002 Worldwide sales of two second-line TB drugs by country by a single manufacturer
Capreomycin Capreomycin Cycloserin Cycloserin
20% RUS
31% WHO
49% Other
WHO
RUS
Other
33% WHO
27% RUS
17% KAZ
23% Other
WHO
Russia
Kazahkstan
Other
Increasing rational use of second-line TB drugs

April 2005 WHO/STB/THD 15
Increased size and quality of the market of Increased size and quality of the market of second-line anti-TB drugssecond-line anti-TB drugs
Eli Lilly transfer of technology and effects on supply
Increasing production capacity in some manufacturers
Investments in some manufacturers to meet quality standards
April 2005 WHO/STB/THD 16
Main components of a DOTS-Plus projectMain components of a DOTS-Plus project
Plan (who will do what, when, how, where?)
Locating the project in the NTP structure
Case finding strategy
Treatment regimen
Drug management (including procurement plan)
April 2005 WHO/STB/THD 17
Main components of a DOTS-Plus projectMain components of a DOTS-Plus project
Role of hospital vs ambulatory treatment
Management of adverse reactions
Data collection and analysis
Laboratory functions
Training of health care workers
April 2005 WHO/STB/THD 18
Main components of a DOTS-Plus projectMain components of a DOTS-Plus project
Role of hospital vs ambulatory treatment
Management of adverse reactions
Data collection and analysis
Laboratory functions
Training of health care workers
April 2005 WHO/STB/THD 19
Lessons learned: main barriers to implement Lessons learned: main barriers to implement DOTS-Plus DOTS-Plus
Poor integration of the MDR-TB activities in the NTP Lack of drug registration of quality-assured drugs Poor understanding of drug side effects, its prevention and
management Poor TB laboratory capacity and/or performance (no quality
control system in place, lack of quality assurance for performing DST for first-line TB drugs)
April 2005 WHO/STB/THD 20
Lessons learned: main barriers to implement Lessons learned: main barriers to implement DOTS-Plus DOTS-Plus
Lack of experience in managing second-line drugs to treat MDR-TB under programmatic conditions
Inadequate facilities to hospitalize and/or treat MDR-TB patients
Absence of social support measures to facilitate adherence to treatment

April 2005 WHO/STB/THD 21
Lessons learned: different ways to implement Lessons learned: different ways to implement a single frameworka single framework
MDR-TB burden does not determine the decision to implement DOTS-Plus: from Latvia to Lebanon
Country-wide DOTS coverage does not determine the decision to implement DOTS-Plus: from Peru to the Philippines
High cost of treatment does not prevent to treat MDR-TB: from El Salvador to Estonia

April 2005 WHO/STB/THD 22
Lessons learned: different ways to implement Lessons learned: different ways to implement a single frameworka single framework
Flexibility to adapt DOTS-Plus to local resources:
– Control of infection risk: from Estonia to Bolivia– Social support: from Peru to Latvia– Implementer: from Haiti to Honduras– Treatment strategy: from Mexico to Malawi– Delivery of treatment: from Nepal to Nicaragua
April 2005 WHO/STB/THD 23
Lessons learned: DOTS-Plus Lessons learned: DOTS-Plus preparation takes time!preparation takes time!
DOTS-Plus does not necessarily mean MDR-TB diagnosis and treatment in all regions and all districts from the very beginning !
Slow steps should be taken in order to pilot, adjust and expand a rational and feasible capacity to manage drug resistant TB
April 2005 WHO/STB/THD 24
Stepwise implementation of DOTS-Plus includes:
– Assessment of drug resistance situation (DRS data, risk groups, laboratory capacity, SLD use )
– Relevance of DOTS-Plus in the context of TB control
– From pilot phase to country-wide expansion: many scenarios, good to start to with national/provincial centres of excellence
Lessons learned: DOTS-Plus Lessons learned: DOTS-Plus preparation takes time!preparation takes time!

April 2005 WHO/STB/THD 25
Preliminary results of DOTS-Plus projectsPreliminary results of DOTS-Plus projects
More than 5,000 patients have been enrolled and 3,100 have completed treatment
MDR-TB among new cases in projects assessed range from 1.5-17.1%
57% of the MDR-TB cases treated are resistant to all first line-drugs and also to second-line anti-TB drugs
Treatment success rates range from 61-82% Only 2% of patients have stopped treatment due to adverse
events

April 2005 WHO/STB/THD 26
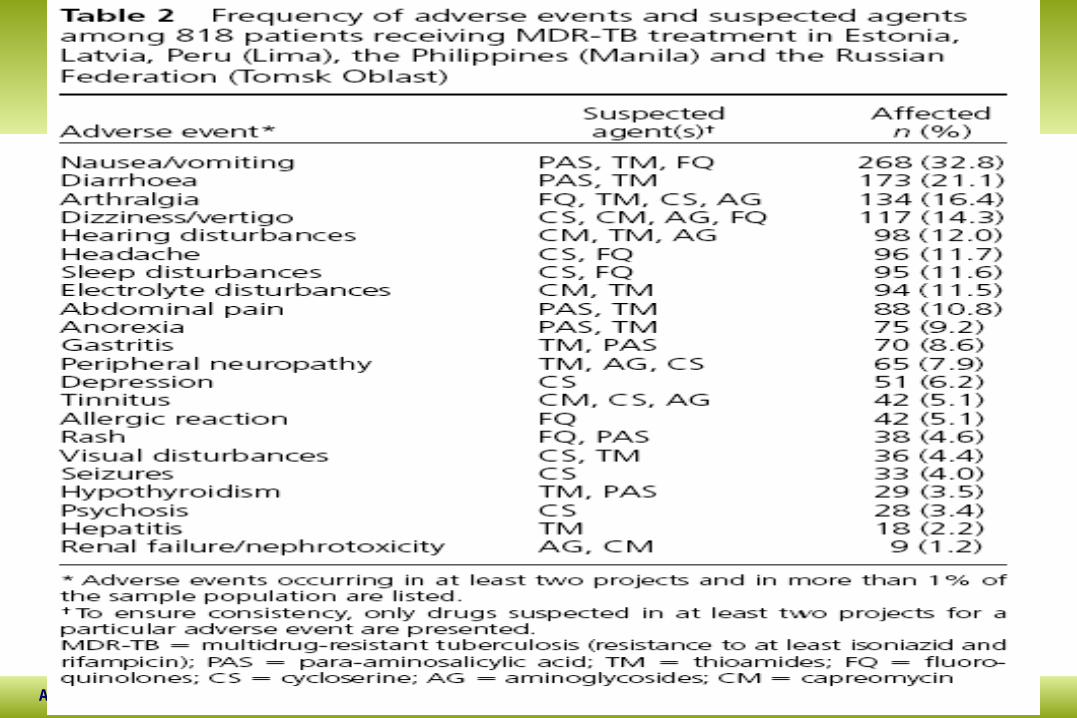
Adverse events (1)Adverse events (1)
Data in 924 patients from Estonia, Latvia, Russia and Philippines show that only 2% (17patients)
have stopped treatment due to side effects
April 2005 WHO/STB/THD 27
Adverse events (1)Adverse events (1)

April 2005 WHO/STB/THD 28
Adverse events (2)Adverse events (2)
Adverse events are manageable in the treatment of MDR-TB in resource-limited settings provided that standard management strategies are applied including:
• altering dosages when appropriate• ancillary drugs to treat adverse events• discontinuation of some drugs if indicated• special training on adverse events to second-line
drugs• standard protocols for registration
April 2005 WHO/STB/THD 29
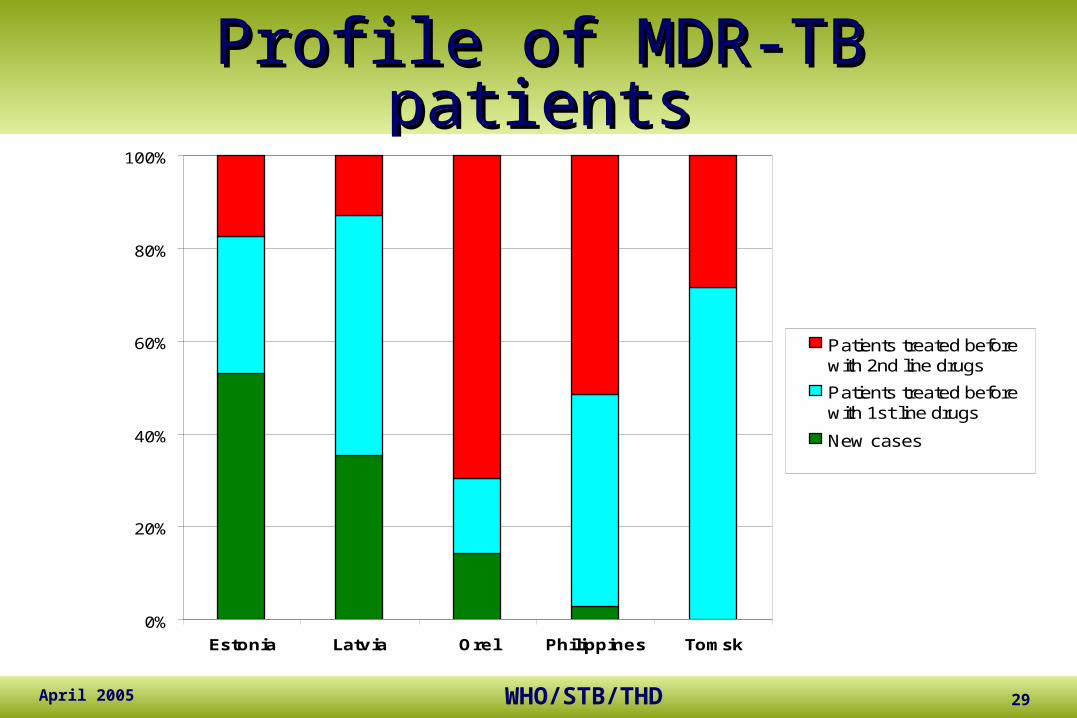
Profile of MDR-TB patientsProfile of MDR-TB patients
0%
20%
40%
60%
80%
100%
Estonia Latvia Orel Philippines Tomsk
Patients treated beforewith 2nd line drugs
Patients treated beforewith 1st line drugs
New cases
April 2005 WHO/STB/THD 30
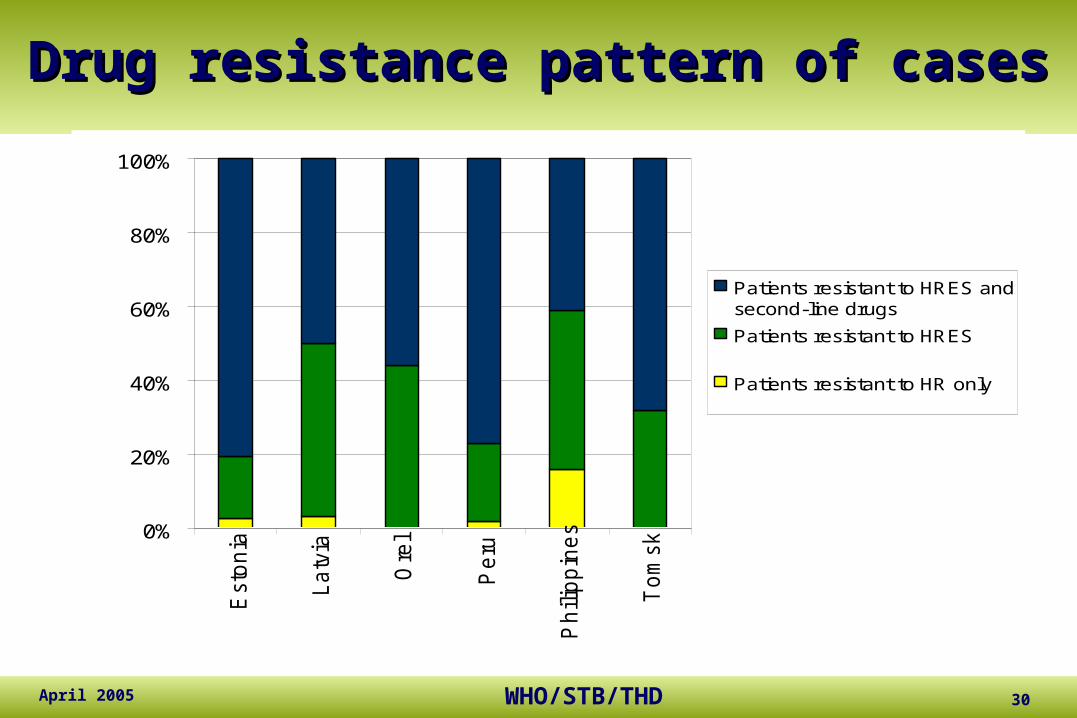
Drug resistance pattern of casesDrug resistance pattern of cases
0%
20%
40%
60%
80%
100%
Esto
nia
La
tvia
Ore
l
Pe
ru
Ph
ilip
pin
es
To
msk
Patients resistant to HRES andsecond-line drugs
Patients resistant to HRES
Patients resistant to HR only
April 2005 WHO/STB/THD 31
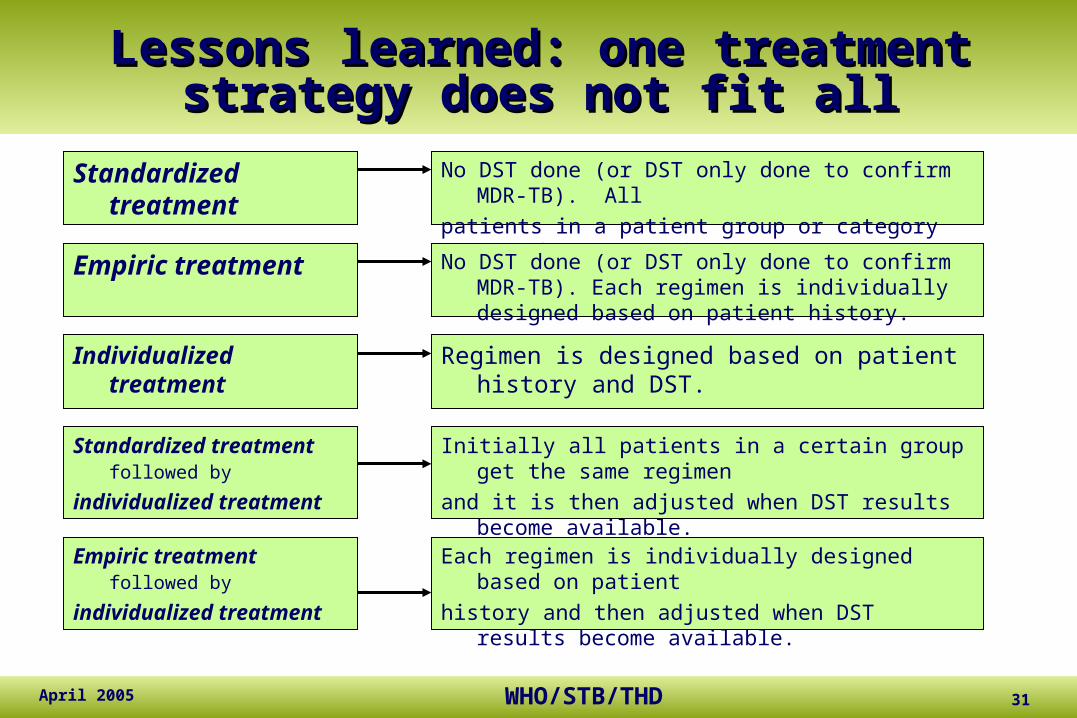
Lessons learned: one treatment strategy Lessons learned: one treatment strategy does not fit alldoes not fit all
Standardized treatment
Empiric treatment
Individualized treatment
Standardized treatment followed by
individualized treatment
No DST done (or DST only done to confirm MDR-TB). All
patients in a patient group or category get the same regimen.
Regimen is designed based on patient history and DST.
Initially all patients in a certain group get the same regimen
and it is then adjusted when DST results become available.
No DST done (or DST only done to confirm MDR-TB). Each regimen is individually designed based on patient history.
Empiric treatment followed by
individualized treatment
Each regimen is individually designed based on patient
history and then adjusted when DST results become available.
April 2005 WHO/STB/THD 32
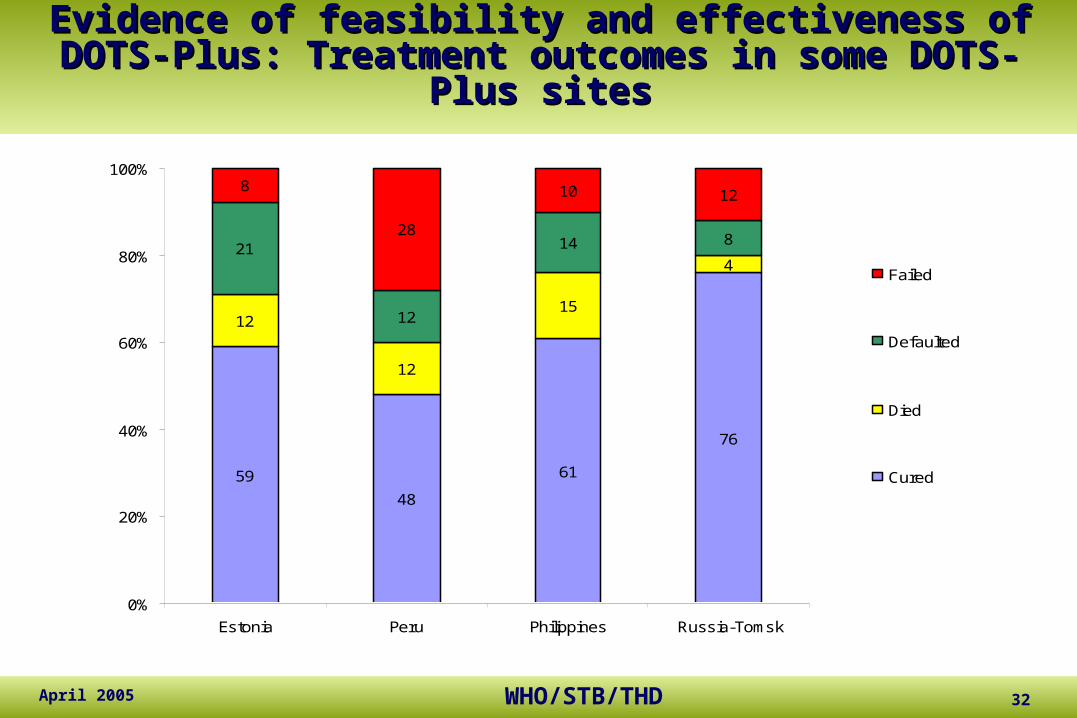
Evidence of feasibility and effectiveness of DOTS-Plus: Evidence of feasibility and effectiveness of DOTS-Plus: Treatment outcomes in some DOTS-Plus sitesTreatment outcomes in some DOTS-Plus sites
59
48
61
76
12
12
15
421
12
14 8
8
28
10 12
0%
20%
40%
60%
80%
100%
Estonia Peru Philippines Russia-Tomsk
Failed
Defaulted
Died
Cured
April 2005 WHO/STB/THD 33
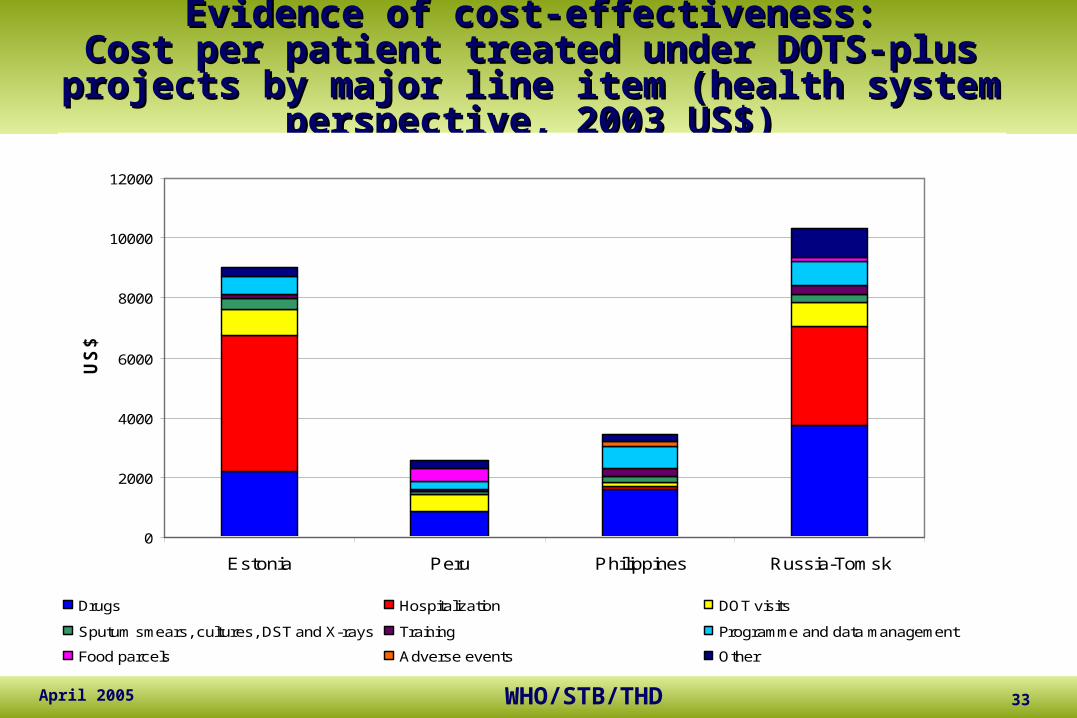
Evidence of cost-effectiveness:Evidence of cost-effectiveness:Cost per patient treated under DOTS-plus projects by Cost per patient treated under DOTS-plus projects by major line item (health system perspective, 2003 US$)major line item (health system perspective, 2003 US$)
0
2000
4000
6000
8000
10000
12000
Estonia Peru Philippines Russia-Tomsk
US
$
Drugs Hospitalization DOT visits
Sputum smears, cultures, DST and X-rays Training Programme and data management
Food parcels Adverse events Other
9020
3432
2544
10319
April 2005 WHO/STB/THD 34
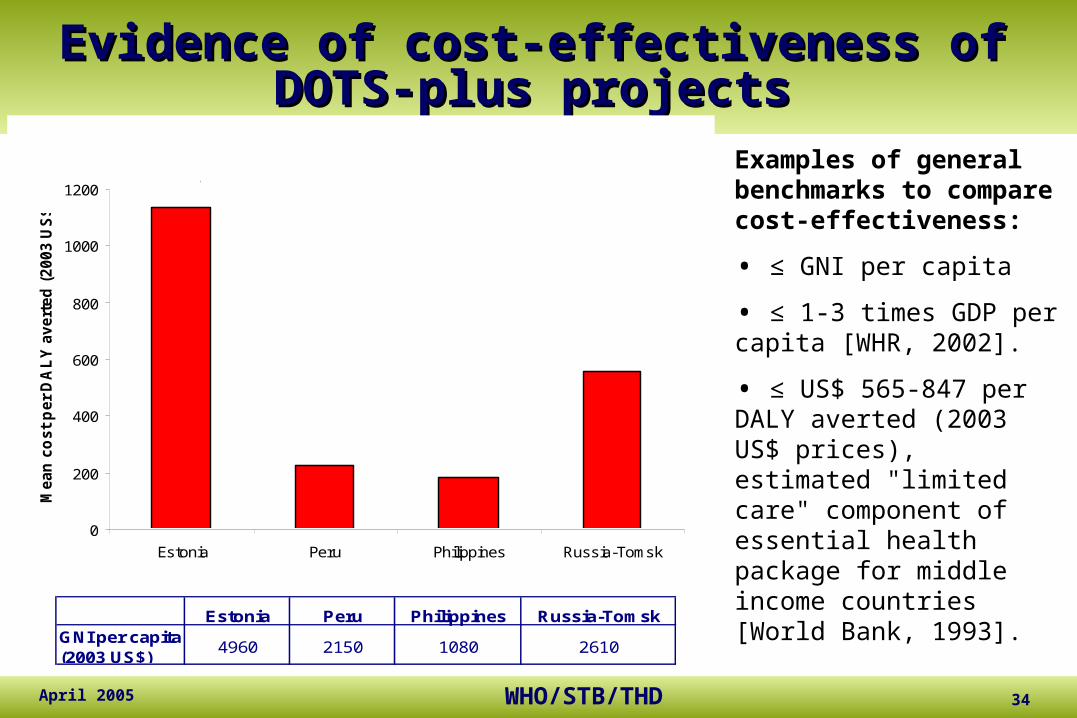
Evidence of cost-effectiveness of DOTS-Evidence of cost-effectiveness of DOTS-plus projectsplus projects
Examples of general benchmarks to compare cost-effectiveness:
• ≤ GNI per capita
• ≤ 1-3 times GDP per capita [WHR, 2002].
• ≤ US$ 565-847 per DALY averted (2003 US$ prices), estimated "limited care" component of essential health package for middle income countries [World Bank, 1993].
0
200
400
600
800
1000
1200
Estonia Peru Philippines Russia-Tomsk
Mean
co
st
per
DA
LY
avert
ed
(2003 U
S$)
1135
183225
556
Estonia Peru Philippines Russia-TomskGNI per capita (2003 US$)
4960 2150 1080 2610
April 2005 WHO/STB/THD 35
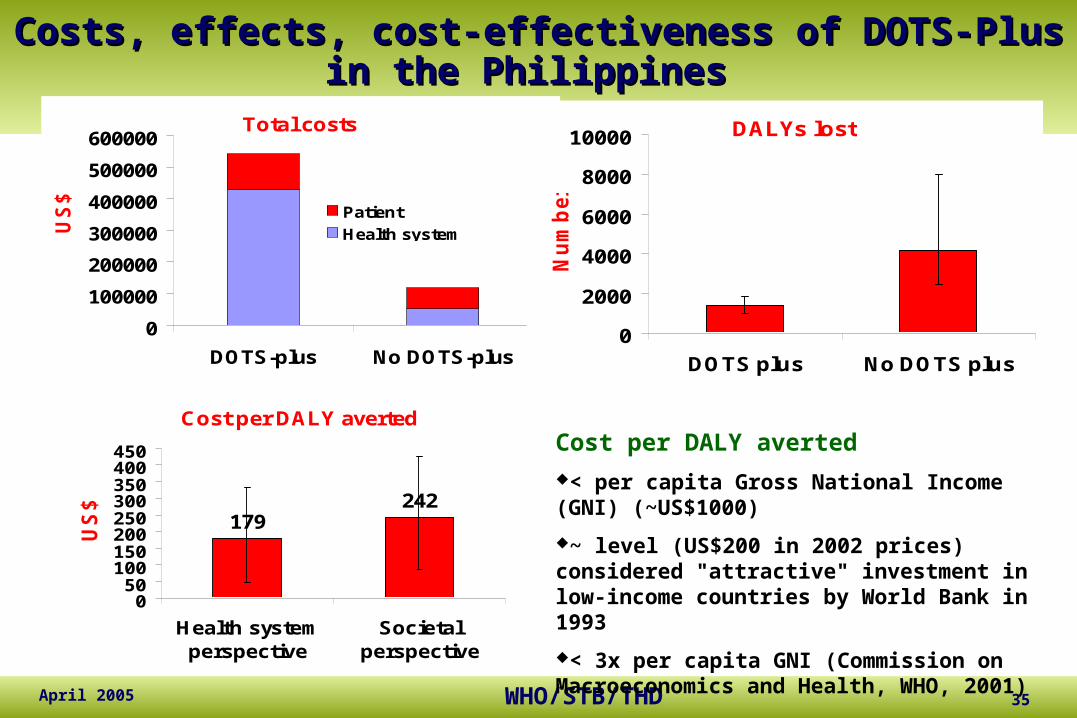
Costs, effects, cost-effectiveness of DOTS-Plus in the Costs, effects, cost-effectiveness of DOTS-Plus in the PhilippinesPhilippines
Total costs
0
100000
200000
300000
400000
500000
600000
DOTS-plus No DOTS-plus
US
$
Patient
Health system
DALYs lost
0
2000
4000
6000
8000
10000
DOTS plus No DOTS plus
Nu
mb
er
Cost per DALY averted
179242
050
100150200250300350400450
Health systemperspective
Societalperspective
US
$
Cost per DALY averted
< per capita Gross National Income (GNI) (~US$1000)
~ level (US$200 in 2002 prices) considered "attractive" investment in low-income countries by World Bank in 1993
< 3x per capita GNI (Commission on Macroeconomics and Health, WHO, 2001)

April 2005 WHO/STB/THD 36
Preliminary results of DOTS-Plus projectsPreliminary results of DOTS-Plus projects
Strengthened DOTS: quality, consolidation and expansion
Training of human resources for management of drug resistant TB
Laboratory capacity strengthened
Size and quality of market of second-line TB drugs
Commitment of GFATM to fund management of MDR-TB
April 2005 WHO/STB/THD 37
Preliminary results of DOTS-Plus projectsPreliminary results of DOTS-Plus projects
DOTS-Plus is creating, fixing and strengthening DOTS– Makes DOTS the default option to control TB: Moldova– Ensures political commitment: Estonia– Strengthen laboratory capacity: Peru – Contributes to a comprehensive TB control policy: the Philippines– Highlights the importance of drug management in TB control: all– Improves the skills of health care workers: Latvia – Improves understanding of local TB and MDR-TB epidemiology: all
April 2005 WHO/STB/THD 38
DOTS-Plus frameworkDOTS-Plus framework
1. Sustained Political commitment
2. Diagnosis of MDR-TB through quality-assured culture and drug susceptibility testing (DST).
3. Appropriate treatment strategies that utilize second line drugs under proper management conditions.
4. Uninterrupted supply of quality assured reserve antituberculosis drugs.
5. Recording and reporting system designed for DOTS-Plus programs

April 2005 WHO/STB/THD 39
Framework Component 1:Framework Component 1:
Sustained Political commitmentSustained Political commitment
Long term investment of resources (human and financial)
Addressing the factors leading to the emergence of MDR-TB
A well functioning DOTS program !! Procurement of quality-assured drugs and
legislation to assure rational use Effective coordination between community, local
governments, and international agencies
April 2005 WHO/STB/THD 40
Framework Component 2:Framework Component 2: Diagnosis of MDR-TB through quality-assured culture and drug Diagnosis of MDR-TB through quality-assured culture and drug
susceptibility testing (DST)susceptibility testing (DST)
Proper triage of patients into susceptibility testing and the DOTS-Plus component of the DOTS program.
– Some programs can do drug susceptibility testing for all patients
– Most programs will use DST strategies that target MDR risk groups (failures, chronics)
– Some enrol patients based on representative DRS data (Nepal)
– But, all programs need access to quality assured drug smear microscopy, culture and susceptibility testing
April 2005 WHO/STB/THD 41
Framework Component 3:Framework Component 3: Appropriate treatment strategies that utilize second-line drugs under Appropriate treatment strategies that utilize second-line drugs under
proper management conditionsproper management conditions
Appropriate regimens Directly observed therapy (DOT) throughout Monitoring and early management of side
effects Adequate human resources (both quantity and
quality)
April 2005 WHO/STB/THD 42
Framework Component 3:Framework Component 3: Appropriate treatment strategies that utilize second-line drugs under Appropriate treatment strategies that utilize second-line drugs under
proper management conditionsproper management conditions (continued)(continued)
Monitoring and management of side effects
–Management algorithms provided in guidelines
–Ability to refer when indicated–Active monitoring (clinical ! and laboratory) –Ancillary medicines at no cost to patient
April 2005 WHO/STB/THD 43
Framework Component 4:Framework Component 4: Uninterrupted supply of quality assured second-line anti-Uninterrupted supply of quality assured second-line anti-
tuberculosis drugstuberculosis drugs
Many challenges of drug procurement– Individualized regimens are frequently being
adjusted (due to side-effects, drug susceptibility testing results, and lack of treatment response)
– Short shelf life (18 – 36 months)– Global production of quality-assured drugs is limited– Drug registration may be lengthy and costly

April 2005 WHO/STB/THD 44
Framework Component 5:Framework Component 5: Recording and reporting system designed for DOTS-Plus Recording and reporting system designed for DOTS-Plus
programsprograms
Enables – patient registration– monitoring (including culture, DST, laboratory
tests…etc)– interim indicators – final outcome analysis– comparison of different cohorts
Related Documents