8-ENDORPHIN ADMINISTRATION TO ACUTE SCHIZOPHRENIC PATIENTS: A DOUBLE BLIND STUDY Bertalan Petho,* LBszld Gr&f,t Istvh Karczag,* J h o s Borvendkg,t Istvhn Bitter,* Istvh Barna,t Ilona Hermann,t Judit Toha,* and Krisztina Baraczka * * Semmelweis Medical University Budopest, Hungary t Institute for Drug Research Budapest, Hungary Apparently incompatible experimental findings and considerations support the hypothesis that the endogenous opioids participate, in some way, in main- taining the psychic equilibrium. Terenius et al.18 first drew attention to the possible connection between disorders in the metabolism of endogenous opioids and the different psychoses. According to their investigations, the measurable concentration of partially purified Fraction I, an opioid peptide different from enkephalins and @-endorphin, is considerably higher in the CSF of schizo- phrenics than in that of control patients. This tendency was more marked in acute cases and parallel with the improvement of the clinical condition. Neuroleptic therapy reduced Fraction I levels that were initially above the control value.2 This recognition raised the possibility of treating schizophrenic patients with opiate antagonists (e.g., naloxone) ,s but most authors have reported on the failure of therapy.' Interpretation of the findings is greatly hampered by the fact that the opiate antagonists block the effect not only of Fraction I, but of all the other endogenous opioids, including those which other authors consider to play a psychopathological role antagonistic to that of Fraction I. This latter view is essentially based on two experimental obser- vations. Jacquet and Marks suggested a similarity between certain pharma- cological properties of &endorphin and the neuroleptics, while de Wied et al.B demonstrated neuroleptic activity for y-endorphin, one of the fragments of 8-endorphin also released under physiological condition^.^ After studying the complex psychiatric literature on alkaloid narcotics and endogenous opioids, Verebey et al.8 have proposed that the endogenous opioids contribute to maintaining psychic equilibrium through their anxiolytic, tran- quilizing, antidepressant, anger-, aggression-, and delusion-reducing effects, and their action in reducing insufficiency and suicidal tendencies. Consequently, reduction of the level of endogenous opioids would result in manifestations antagonistic to the above favorable effects (anxiety, hypersensitivity to average stress, reduced self-esteem, etc.) . it became possible to conduct clinical tests of the polypeptide. mine and LehmaM lo administered &endorphin in intravenous doses of 1.5-9.0 mg to 15 psychiatric patients on 42 occasions. On the basis of the nature and duration of the effects, the authors distinguished four phases in the action: I. autonomous (30-120 sec); 11. antidysphoric (1-6 hours); 111. inhibitory (2-3 hours); IV. therapeutic (1-10 days). Vegetative reactions appeared in phase I and With the successful chemical synthesis of human &endorphin 460 3011-8923/82/0398-0460 $01.15/0 0 1982. WAS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8-ENDORPHIN ADMINISTRATION TO ACUTE SCHIZOPHRENIC PATIENTS: A DOUBLE BLIND STUDY
Bertalan Petho,* LBszld Gr&f,t Is tvh Karczag,* J h o s Borvendkg,t Istvhn Bitter,* Istvh Barna,t Ilona Hermann,t Judit Toha,*
and Krisztina Baraczka * * Semmelweis Medical University
Budopest, Hungary t Institute for Drug Research
Budapest, Hungary
Apparently incompatible experimental findings and considerations support the hypothesis that the endogenous opioids participate, in some way, in main- taining the psychic equilibrium. Terenius et al.18 first drew attention to the possible connection between disorders in the metabolism of endogenous opioids and the different psychoses. According to their investigations, the measurable concentration of partially purified Fraction I, an opioid peptide different from enkephalins and @-endorphin, is considerably higher in the CSF of schizo- phrenics than in that of control patients. This tendency was more marked in acute cases and parallel with the improvement of the clinical condition. Neuroleptic therapy reduced Fraction I levels that were initially above the control value.2 This recognition raised the possibility of treating schizophrenic patients with opiate antagonists (e.g., naloxone) ,s but most authors have reported on the failure of therapy.' Interpretation of the findings is greatly hampered by the fact that the opiate antagonists block the effect not only of Fraction I, but of all the other endogenous opioids, including those which other authors consider to play a psychopathological role antagonistic to that of Fraction I. This latter view is essentially based on two experimental obser- vations. Jacquet and Marks suggested a similarity between certain pharma- cological properties of &endorphin and the neuroleptics, while de Wied et al.B demonstrated neuroleptic activity for y-endorphin, one of the fragments of 8-endorphin also released under physiological condition^.^
After studying the complex psychiatric literature on alkaloid narcotics and endogenous opioids, Verebey et al.8 have proposed that the endogenous opioids contribute to maintaining psychic equilibrium through their anxiolytic, tran- quilizing, antidepressant, anger-, aggression-, and delusion-reducing effects, and their action in reducing insufficiency and suicidal tendencies. Consequently, reduction of the level of endogenous opioids would result in manifestations antagonistic to the above favorable effects (anxiety, hypersensitivity to average stress, reduced self-esteem, etc.) .
it became possible to conduct clinical tests of the polypeptide. mine and LehmaM lo
administered &endorphin in intravenous doses of 1.5-9.0 mg to 15 psychiatric patients on 42 occasions. On the basis of the nature and duration of the effects, the authors distinguished four phases in the action: I. autonomous (30-120 sec); 11. antidysphoric (1-6 hours); 111. inhibitory (2-3 hours); IV. therapeutic (1-10 days). Vegetative reactions appeared in phase I and
With the successful chemical synthesis of human &endorphin
460 3011-8923/82/0398-0460 $01.15/0 0 1982. W A S
Petho et al. : P-Endorphin and Schizophrenia 46 1
favorable therapeutic effects (improved mood, relief from anxieties, etc.) could be observed in phases 11-IV.10 The main technical shortcomings in these and in the investigations by Angst et al." giving rise to the possibility of error, were as follows: ( 1 ) the investigations were not carried out in blind design; (2) the authors did not use a structured evaluation; l2 and (3) the medication given at the same time as the treatment or its interruption could influence the effect of the 8-endorphin.
We report here studies on &endorphin treatment of six acute schizophrenic patients in a double-blind design. These patients did not receive any other medication during the trial period. During the preparation of our pre- liminary report l3 on these studies, double-blind clinical studies with &endorphin have also been reported by two other groups.14* l5
MATERIALS AND METHODS
Human @endorphin was produced by solid-phase peptide synthesis l8 in Prof. C. H. Li's laboratory (University of California, San Francisco). We checked the homogeneity of this /?-endorphin preparation with end-group and amino acid analyses and paper and gel electrophoreses (see ref. 16 for the methods). Following intracerebroventricular (i.c.v.) administration, the an- algesic effect determined by the rat tail-flick test was the same as that of pig 8-endorphin isolated from natural source.17
Synthetic human 8-endorphin was dissolved in physiological saline solu- tion, strained through a Millipore HA 0.22 p filter, and filled in ampules under sterile conditions. Each ampule contained 4.0 mg of 8-endorphin in 10 ml of physiological saline solution. The ampules were stored at -20°C.
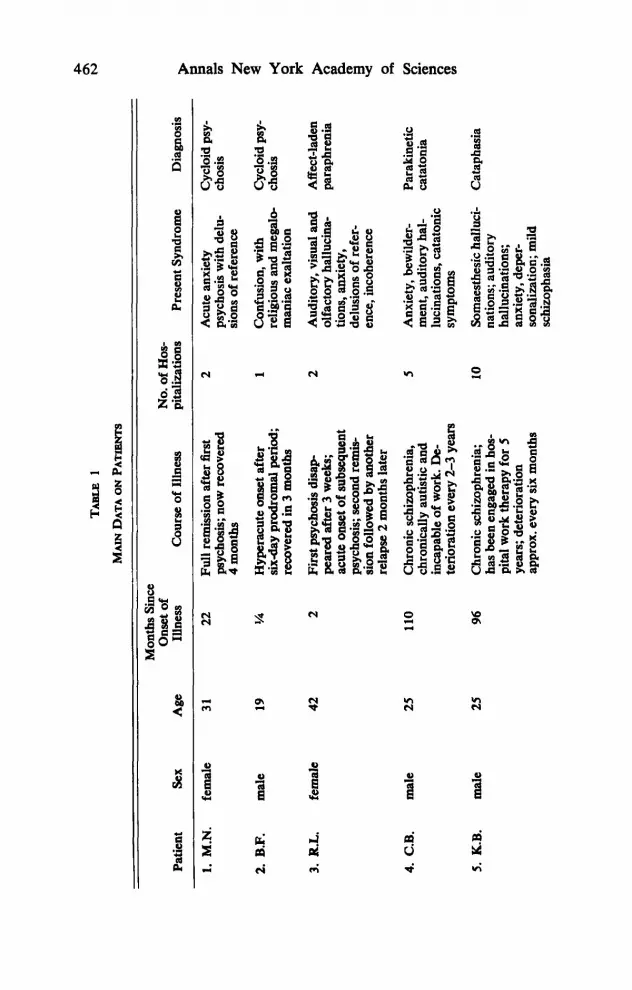
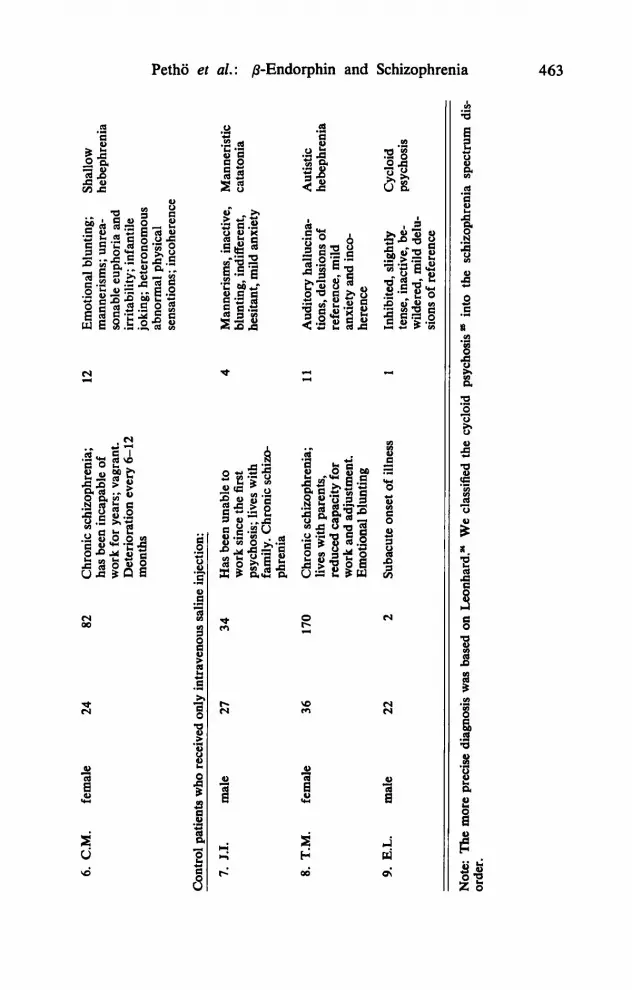
Since @-endorphin has not yet been administered to patients suffering from manifest psychosis, we selected such patients for our investigation (TABLE 1 ). Six patients each received 4 mg of 8-endorphin intravenously, while three patients were given the same volume of physiological saline solution. The injection lasted 5 minutes in all cases.
Our investigations were conducted in a double-blind design, with the psychopathological examination recorded according to the factor construct rating scale (FCRS) 18 in patients who had received no medication for a t least 10 days and who were not receiving any other medication during the course of the study. The injection was administered at 10 A.M. The psycho- pathological and pain sensation tests were conducted at the following times: (1) at 8:30 A.M. on the day of treatment; (2) in 15 minutes immediately following the treatment; (3) hourly on the day of treatment up to 5 P.M.; and (4) at 9 A.M. and 1 P.M. on the days following treatment for one week unless it became necessary before the end of this period to give other (neuro- leptic, anxiolytic) medication.
One hour before the 8-endorphin injection and at the same time on the third day, we took 9-10 ml of CSF by lumbar puncture with the patient in a seated position. After removal the CSF was immediately frozen and was then lyophilized and dissolved again in 0.9-1.0 ml distilled water in order to determine the &endorphin content by radioimmunoassay (RIA). For the details of the @-endorphin RIA method we refer to the description given by Borvendeg et al.lg We used a pig &endorphin antibody produced in rabbits in a dilution of 1 : 30,000; the lower limit of sensitivity, 20 pg b-endorphin, gave a 100% cross reaction with reference human 8-endorphin.
TA
BL
E 1
P
Q\
h)
MAIN DATA
ON P
ATIE
NTS
Mon
ths S
ince
O
nset
of
NO. O
f H
OS-
Pa
tient
Sex
Age
Il
lnes
s Course of
Illn
ess
pita
lizat
ions
Pr
esen
t Syn
drom
e D
iagn
osis
1. M.N.
fem
ale
31
22
Full
rem
issi
on a
fter
firs
t 2
Acu
te a
nxie
ty
Cyc
loid
psy-
c
psyc
hosi
s; n
ow r
ecov
ered
ps
ycho
sis w
ith d
elu-
ch
osis
v1 z
sixd
ay p
rodr
omal
per
iod;
re
ligio
us a
nd m
egal
o-
chos
is
4
4 m
onth
s si
ons of
ref
eren
ce
2. B.F.
mal
e 19
%
H
yper
acut
e ons
et a
fter
1
Con
fusi
on, w
ith
Cyc
loid
PSY
- 9 % b H g
reco
vere
d in
3 m
onth
s
3. R.L.
fem
ale
42
2 Fi
rst p
sych
osis
dis
ap
2 A
udito
ry, v
isua
l and
A
ffec
t-lad
en
pear
ed a
fter
3 w
eeks
; ol
fact
ory
hallu
cina
- pa
raph
reni
a ac
ute
onse
t of
subs
eque
nt
9 ps
ycho
sis;
sec
ond
rem
is-
sion
follo
wed
by
anot
her
ence
, inc
oher
ence
Y
E! re
laps
e 2
mon
ths
late
r
chro
nica
lly au
tistic
and
m
ent,
audi
tory
hal
- ca
tato
nia
inca
pabl
e of
wor
k. De-
lu
cina
tions
. cat
aton
ic
R te
rior
atio
n ev
ery
2-3
year
s sy
mpt
oms
I
man
iac
exal
tatio
n
tions
, anx
iety
, de
lusi
ons o
f re
fer-
110
Chr
onic
schi
zoph
reni
a,
5 A
nxie
ty, b
ewild
er-
Para
kine
tic
4. C.B.
mal
e 25
5. K.B.
mal
e 25
96
C
hron
ic sc
hizo
phre
nia;
10
So
mae
sthe
sic h
allu
ci-
Cat
apha
sia
has
been
eng
aged
in h
os-
natio
ns; au
dito
ry
pita
1 w
ork
ther
apy
for 5
ha
lluci
natio
ns;
year
s; d
eter
iora
tion
anxi
ety,
dep
er-
appr
ox. e
very
six
mon
ths
sona
lizat
ion;
mild
sc
hizo
phas
ia
6. C.M.
fem
ale
24
82
Chr
onic
schi
zoph
reni
a;
has b
een
inca
pabl
e of
w
ork
for y
ears
; vag
rant
. D
eter
iora
tion
ever
y 6-
12
mon
ths
Con
trol
pat
ient
s w
ho re
ceiv
ed o
nly
intra
veno
us s
alin
e inj
ectio
n:
7. J
.I.
mal
e 27
34
H
as b
een
unab
le to
w
ork
sinc
e th
e fir
st
psyc
hosi
s; li
ves
with
fa
mily
. Chr
onic
schi
m-
phre
nia
8. T
.M.
fem
ale
36
170
Chr
onic
schi
zoph
reni
a;
lives
with
par
ents
, re
duce
d ca
paci
ty f
or
wor
k an
d ad
just
men
t. E
mot
iona
l blu
ntin
g
12
Emot
iona
l blu
ntin
g;
Shal
low
m
anne
rism
s; u
nrea
- he
beph
reni
a so
nabl
e eu
phor
ia a
nd
irrita
bilit
y; in
fant
ile
joki
ng; h
eter
onom
ous
sens
atio
ns; i
ncoh
eren
ce
cd
abno
rmal
phy
sica
l (D
g b s .. 4
Man
neris
ms,
inac
tive,
M
anne
ristic
bl
untin
g, in
diff
eren
t, ca
tato
nia
hesi
tant
, mild
anx
iety
11
Aud
itory
hal
luci
na-
Aut
istic
tio
ns, d
elus
ions
of
hebe
phre
nia
g. re
fere
nce,
mild
an
xiet
y an
d in
co-
here
nce
WJ 9.
E.L.
mal
e 22
2
Suba
cute
ons
et o
f ill
ness
1
Inhi
bite
d, s
light
ly
Cyc
loid
0
wild
ered
, mild
del
u-
m T
2.
tens
e, in
activ
e, b
e-
psyc
hosi
s
sion
s of
refe
renc
e 0
(D
Note:
The
mor
e pr
ecis
e di
agno
sis
was
bas
ed on
Leon
hard
."
We
clas
sifie
d th
e cy
cloi
d ps
ycho
sis
orde
r. in
to t
he s
chiz
ophr
enia
spe
ctru
m d
is-
rs
464 Annals New York Academy of Sciences
n + v
+ +
+ +
n n + +
+ h
v I I +
m - w - f - b - rn
+ ++ + h + + v
I + I +
I T + I I ,+
I + 1 + 1
IN I
Petho et al.: p-Endorphin and Schizophrenia
I T Y I I
I ' i l Y I
h + W
+ ? + Y
h
I Y
h + + I I v T I Y
465
466 Annals New York Academy of Sciences
RESULTS
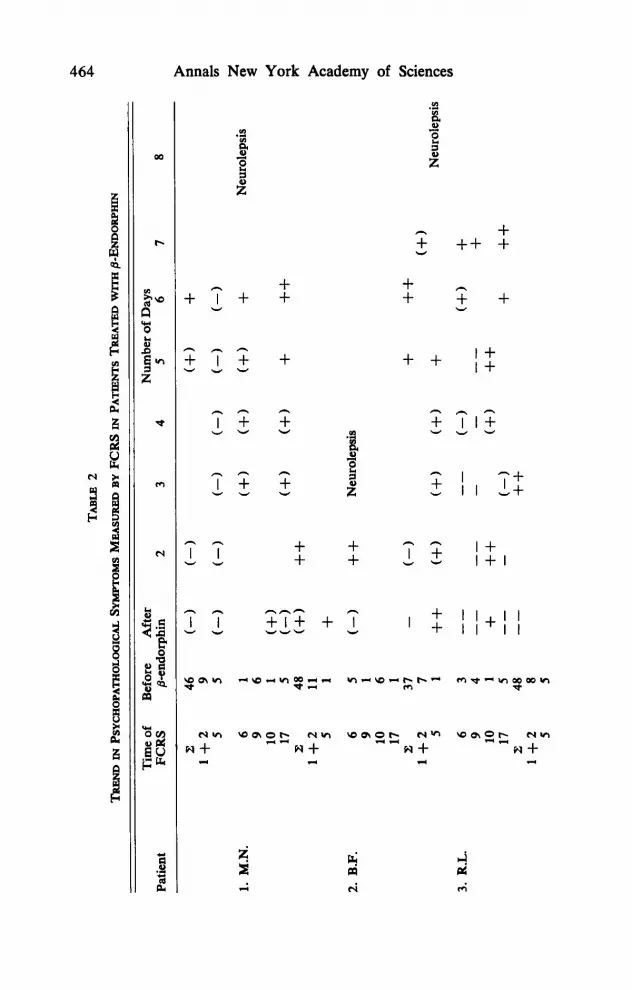
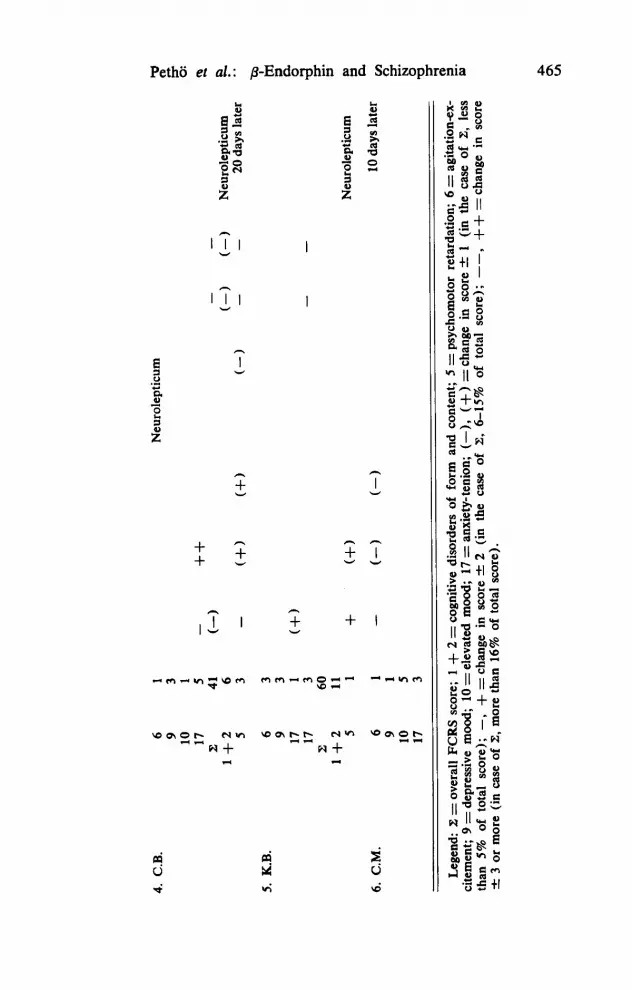
Marked and lasting somnolence developed in two patients (3 and 6) on the day of the &endorphin injection. A milder degree of somnolence could also be observed in the other four patients. We did not observe a reduction in the pain sensation in any of the patients when the skin was pricked with a needle. There was a change in the psychiatric symptoms in patients 1, 2, and 3 even within 30 minutes and one hour, particularly on the first day. The characteristic daily values for the FCRS scores are given in TABLE 2. Cogni- tive disorders showed a minimal improvement only in patient 6 and here too, only after days 6 and 7 following the treatment. With the exception of patient 4, psychomotor activity showed normalization in the first days. Where inhibition had been more marked before treatment with 8-endorphin it declined, and where agitation and excitement were more prominent, these were reduced. There was a similar reciprocal change in mood in patient 3 compared to the initial value before administration of &endorphin. Transient euphoria also occurred in two other patients (1 and 5 ) . Patients 2 and 6 were in such a state of prolonged euphoria prior to treatment that any further increase in euphoria would have been difficult to detect. Anxiety was defi- nitely reduced in four patients (1, 3, 4, and 5 ) but later-also in the case of patient 2-just because of the very marked increase in anxiety-neuroleptic- anxiolytic treatment had to be started. There was no substantial change in the other items of the FCRS. In four cases the intensity of the psychosis as reflected in the FCRS overall score first declined and then rose, in one case ( 5 ) it rose immediately and rapidly and in another one (6) it did not change.
Among the three control patients (whose FCRS scores are not shown), patient 7 improved suddenly and substantially after the psychological saline injection was given. For 3 days he was bright, active, and sociable, although his manneristic behavior remained unchanged. It was only in this case that the “blind” observer felt certain that the patient had received @endorphin. His symptoms returned after 3 days and he had to be given anxiolyticums for his acute anxiety. The psychosis of control patient 8 grew gradually and steadily worse until we administered a neuroleptic drug on day 4. The behavior of control patient 9 was slightly improved, but he also had to be given neuroleptics on day 3.
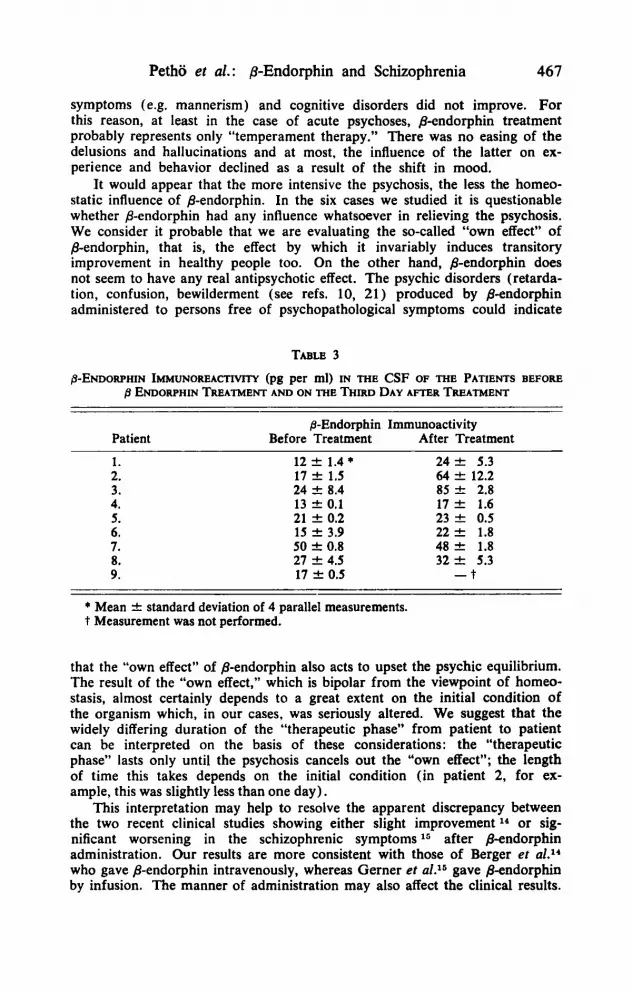
In agreement with the data in the literature,z0 the 8-endorphin immuno- reactivity in the CSF of the patients before the treatment gave a value in the range of 12-50 pg 8-endorphinlml. The CSF @-endorphin levels determined three days after treatment with @-endorphin in patients 4, 5, and 6 and in the two control patients examined (7 and 8), coincided with the initial values while in three patients (1, 2, and 3) we found a significant rise in the level (TABLE 3 ) .
DISCUSSION
All of our six patients given 8-endorphin treatment showed a certain improvement for a shorter or longer period. This improvement was restricted to the area of mood and activity. The nature of the improvement depended on the initial symptoms; in all cases they indicated a tendency to restore the homeostasis. Contrary to the earlier data in the literature,los l1 the formal
Petho et al. : ,&Endorphin and Schizophrenia 467
symptoms (e.g. mannerism) and cognitive disorders did not improve. For this reason, at least in the case of acute psychoses, &endorphin treatment probably represents only “temperament therapy.” There was no easing of the delusions and hallucinations and at most, the influence of the latter on ex- perience and behavior declined as a result of the shift in mood.
It would appear that the more intensive the psychosis, the less the homeo- static influence of 8-endorphin. In the six cases we studied it is questionable whether &endorphin had any influence whatsoever in relieving the psychosis. We consider it probable that we are evaluating the so-called “own effect” of &endorphin, that is, the effect by which it invariably induces transitory improvement in healthy people too. On the other hand, &endorphin does not seem to have any real antipsychotic effect. The psychic disorders (retarda- tion, confusion, bewilderment (see refs. 10, 21) produced by &endorphin administered to persons free of psychopathological symptoms could indicate
TABLE 3
p ENDORPHIN TREATMENT AND ON THE THIRD DAY AFTER TREATMENT ENDORPHIN IMMUNOREACTIWTY (pg per ml) IN THE CSF OF THE PATIENTS BEFORE
Patient p-Endorphin Immunoactivity
Before Treatment After Treatment 1. 2. 3. 4. 5. 6. 7. 8. 9.
12 f 1.4 * 17 -C 1.5 24 & 8.4 13 -C 0.1 21 f 0.2 15 2 3.9 50 2 0.8 27 f 4.5 17 -C 0.5
24 rt 5.3 64 k 12.2 85 k 2.8 17 f 1.6 23 k 0.5 22 f 1.8 48 2 1.8 32 k 5.3
- t
* Mean -C standard deviation of 4 parallel measurements. t Measurement was not performed.
that the “own effect” of 8-endorphin also acts to upset the psychic equilibrium. The result of the “own effect,” which is bipolar from the viewpoint of homeo- stasis, almost certainly depends to a great extent on the initial condition of the organism which, in our cases, was seriously altered. We suggest that the widely differing duration of the “therapeutic phase” from patient to patient can be interpreted on the basis of these considerations: the “therapeutic phase” lasts only until the psychosis cancels out the “own effect”; the length of time this takes depends on the initial condition (in patient 2, for ex- ample, this was slightly less than one day).
This interpretation may help to resolve the apparent discrepancy between the two recent clinical studies showing either slight improvement l4 or sig- nificant worsening in the schizophrenic symptoms l6 after B-endorphin administration. Our results are more consistent with those of Berger et d . 1 4
who gave @-endorphin intravenously, whereas Gerner et al.15 gave @endorphin by infusion. The manner of administration may also affect the clinical results.
468 Annals New York Academy of Sciences
As regards the change in the B-endorphin level measured in the CSF (TABLE 3) it is striking that we observed a marked rise in level only in the three ( 1-3) schizophrenic syndromes accompanied by strong affective symp- toms (“schizo-affective” psychosis). Since according to Foley et a1.,22 the half-life of human &endorphin administered to humans intravenously and intracerebroventricularly is 37 and 93 minutes, respectively, it is improbable that the 8-endorphin immunoactivity measured on the third day would be caused by the exogenous polypeptide. However, the possibility arises that p-endorphin introduced could stimulate the biosynthesis or release of cerebral (or hypophyseal?) pendorphin through some, as yet unknown, mechanism. If confirmed, this observation could give a new angle to the investigation of the pathogenesis of the schizo-affective psychoses. The selective susceptibility of the schizophrenic subgroups is also an open question.23
In drawing our conclusions, not only the small number of patients but also the experience with the control patients point to the need for increased cau- tion. As the example of patient 7 shows, the intravenous placebo injection can result in a transitory remission of the patient that misleadingly resembles the “temperament therapy” that can be expected from /%endorphin.
ACKNOWLELXMENT
We are grateful to Professor C. H. Li (University of California, San Francisco) for supplying us with synthetic human p-endorphin.
REFERENCES
1.
2.
3.
4.
5. 6.
7.
8.
9.
10.
11.
TERENIUS, L., A. WAHLSTROM, I. LINDSTROM & E. WIDERLOV. 1976. Neurosci. Letters 3: 157-162.
T~RENIUS, L., A. WAHLSTROM & L. JOHANSSON. 1979. I n Endorphins in Mental Health Research. E. Usdin, W. E. Bunney & N. S. Kline, Eds.: 553- 560. MacMillan Press. London.
1977. J. Neural. Transm. 40: GUNNE, L. M., I. LINDSTROM & L. TERENIUS. 13-19.
DAVIS, G. C., W. E. BU”EY, E. G. DE FWmS, J. E. K L E I ” , D. P. VAN KAMMEN, R. M. POST & R. J. WYAIT. 1977. Science 197: 74-77.
JACQUET, Y. F. & N. MARKS. 1976. Science 194: 632-635. DE WIED, D., G. L. KOVACS, B. Boms, J. M. VAN REE & H. M. GREVEN.
BURBACH, I. P. H., J. G. LOEBER, J. VERHOEF, V. M. WIEOANT, E. R. UOET 1978.
& D. DE WED. 1980. Nature 283: 96-97.
Eur. J. Pharmacol. 49: 427-436.
VEREBEY, K., J. VOLAVKA & D. CLoueT. 1978. Arch. Gen. Psychiatry 35: 877-888.
LI, C. H., D. YAMASHIRO, L.-F. TSENG & H. H. LOH.
KLINE, N. S. & H. E. LEHMA”.
1977. I. Med. Chem.
1979. I n Endorphins in Mental Health Re- search. E. Usdin, W. E. Bunney & N. S. Kline, Eds.: 500-517. Macmillan Press. London.
ANGST, J., V. AUTENRIEW, F. BREM, M. KoUKKou, H. MeYeR, H. H. STASSEN & U. STOCK. 1979. I n Endorphins in Mental Health Research. E. Usdin, W. E. Bunney & N. S. Kline, Eds.: 518-528. Macmillan Press. London.
10 325-328.
Petho et al. : /+Endorphin and Schizophrenia 469
12. WATSON, S. J., H. AKIL. P. A. BERGER & J. D. BARCIIAS. 1979. Arch. Gen.
13. PETHO, B.. L. G&, I. KARCUG, I. B ~ R , J. TOLNA, K. BAXACZKA & C. H. LI.
14. BERGER. P. A., S. J. WATSON, H. AKIL. G. R. ELLIOTT. R. T. RUBIN, A. 1980. Arch. Gen.
15. GERNER, R. H., D. H. C A ~ I N , D. A. GORELICK, K. S. HUI & C. H. LI. 1980.
16. GI&, L., A. KENESSEY, A. PATIHY, A. GRYNBAUM, N. MARKS & A. LNRIA.
17. S ~ Y , J. I., A. Z. R~NAI. Z. DUNAI-KOV~CS, E. MIGLECZ, I. BERZ~TEI, S.
18. OVERALL, J. E, B. W. HENRY & J. R. MARKEYT. 1972. Psychiat. Res. 9 87-99. 19. BORVENDEG, J., L. G&, I. HERMANN, M. PALKOVITS & K. MERETEY. 1978.
In Endorphins 78. L. GrBf, M. Palkovits & A. Z. Ronai, Eds.: 177-186. Akademiai Kiado. Budapest.
20. EMRICH, H. W., C. CORDING & S. PIREE. 1977. Pharmakopsychiatr. Neuro- psychopharmakol. 10: 265-270.
21. OYAMA. T., T. FIN, R. YAMAYA, N. LING & R. GUILLEMIN. 1980. Lancet, Janu- ary 19: 122.
22. FOLEY, K. M., I. A. KOURIDES, C. E. INTURRISI, R. F. KAIKO, C. G. ZAROULIS, J. B. POSNER, R. W. HOUDE & C. H. LI. 1979. Proc. Natl. Acad. Sci. USA
23. VAN PRAAG, H. M. & W. M. A. VERHOEVEN. 1981. Comprehensive Psychiat.
24. LEONHARD, K. 1979. The Classification of Endogenous Psychoses. Irvington.
25. PEWS, C. 1974. Cycloid Psychosis. Munksgaard. Copenhagen.
Psychiatry 36: 3541.
1981. Lancet, January 24.: 212-213.
PFEFFERBAUM. K. L. DAVIS, J. D. BARCHAS & C. H. LI. Psychiatry 37: 635640.
37: 642647.
1979. Arch. Biochem. Biophys. 193: 101-109.
BAJUSZ & L. G ~ F . 1977. Eur. J. Pharmacol. 4j: 293-294.
76: 5377-5381.
22: 125-146.
New York.
Related Documents











