ZYGOMATIC (MALAR) FRACTURES 129 CHAPTER 12 All fractures of the zygoma potentially involve the orbital floor. Minor discrepancies of zygomatic bone position can cause marked asymetry. Anatomical articulations FZ — Fronto-zygomatic ZT — Zygomatico- temporal ZMB — Zygomatico - maxillary buttress IO — Infraorbital Forms the lateral part of the orbit Provides lateral facial projection Protects the globe The zygomatic bone transmits 3 nerves Infraorbital Zygomaticofacial Zygomaticotemporal Anatomical articulation ZS — Zygomaticospenoid Zygomaticosphenoid junction is a key articulation when there is gross comminution of the other fracture articulations. Useful in cases of revision trauma. b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 129

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ZYGOMATIC (MALAR)FRACTURES
129
CH
AP
TE
R 1
2
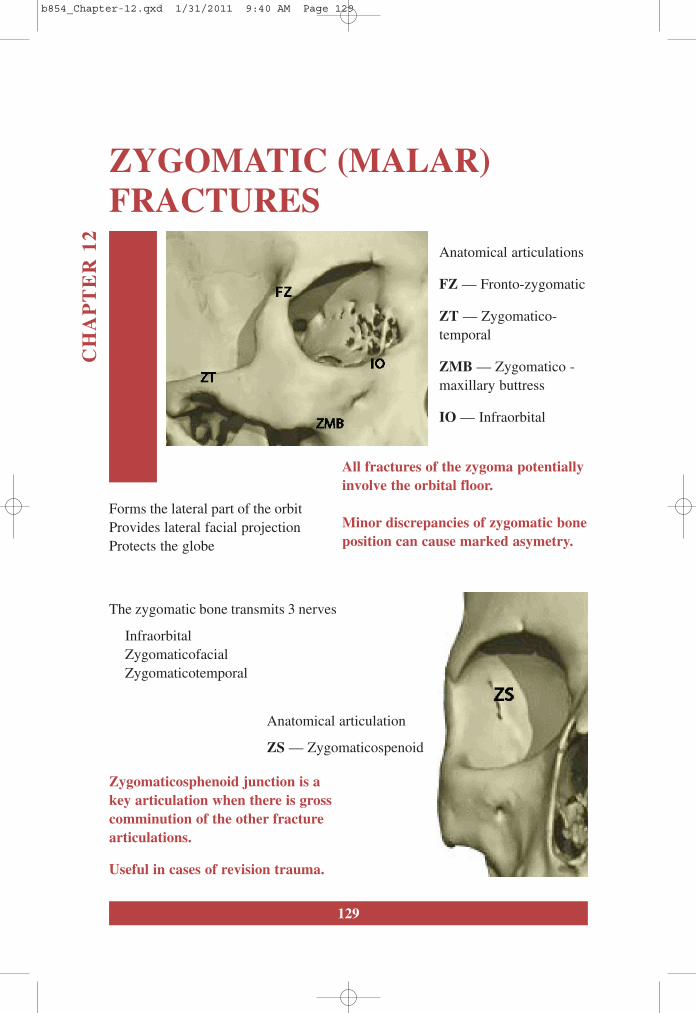
All fractures of the zygoma potentiallyinvolve the orbital floor.
Minor discrepancies of zygomatic boneposition can cause marked asymetry.
Anatomical articulations
FZ — Fronto-zygomatic
ZT — Zygomatico-temporal
ZMB — Zygomatico -maxillary buttress
IO — Infraorbital
Forms the lateral part of the orbit Provides lateral facial projectionProtects the globe
The zygomatic bone transmits 3 nerves
InfraorbitalZygomaticofacialZygomaticotemporal
Anatomical articulation
ZS — Zygomaticospenoid
Zygomaticosphenoid junction is akey articulation when there is grosscomminution of the other fracturearticulations.
Useful in cases of revision trauma.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 129
130
An Atlas of Craniomaxillofacial Trauma
ClassificationThere are several classifications of lateral facial fractures, the Henderson classifi-cation is the most useful.
Henderson Classification Description
Type 1 Undisplaced
Type 2 Zygomatic arch
Type 3 Tripod fracture — Intact FZ suture
Type 4 Tripod fracture — Distracted FZ suture
Type 5 Associated orbital floor fracture
Type 6 Orbital rim fracture
Type 7 Comminuted and other fracture
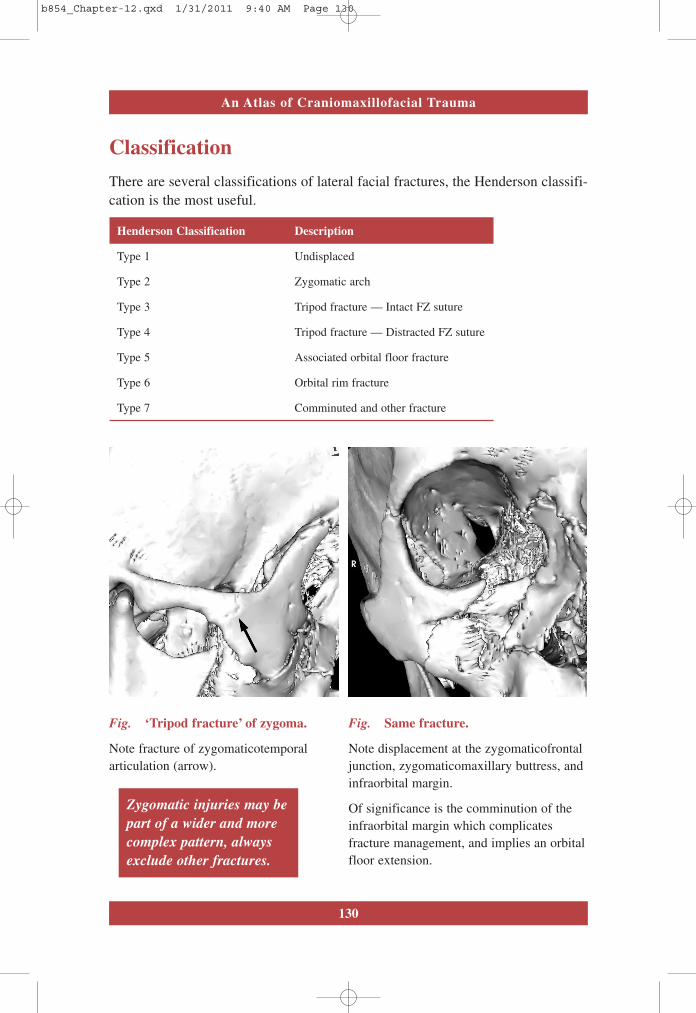
Fig. ‘Tripod fracture’ of zygoma.
Note fracture of zygomaticotemporalarticulation (arrow).
Fig. Same fracture.
Note displacement at the zygomaticofrontaljunction, zygomaticomaxillary buttress, andinfraorbital margin.
Of significance is the comminution of theinfraorbital margin which complicatesfracture management, and implies an orbitalfloor extension.
Zygomatic injuries may bepart of a wider and morecomplex pattern, alwaysexclude other fractures.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 130

131
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
CLINICAL FEATURES
Clinical Features Signs and Symptoms
Soft tissue Periorbital ecchymosisSubconjunctival haematomaChemosisBuccal Sulcus haematoma
Bone deformity Flattening of malar prominenceStep deformityCrepitusZygomatic arch depression
Eyes DiplopiaEnophthalmosIf associated orbital floor fracture
Nerves Infraorbital paraesthesia anaesthesiaZygomaticotemporal paraesthesiaZygomaticofacial paraesthesiaAlveolar nerve anaesthesia
Nasal EpistaxisNasal deformity (if fracture continuous with nose)
Occlusal Trismus (zygomatic arch)Occlusal disturbance (if fracture extends into alveolar process)
Fig. Classic ‘zygomatic facies’, periorbital ecchymosis.
Associated soft tissue swelling may make examination ofthe globe difficult.
Bone deformity and asymmetry may be demonstrated bycareful palpation.
Remember to always examine the globe.
Visual acuity and globe integrity mustbe documented.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 131
132
An Atlas of Craniomaxillofacial Trauma
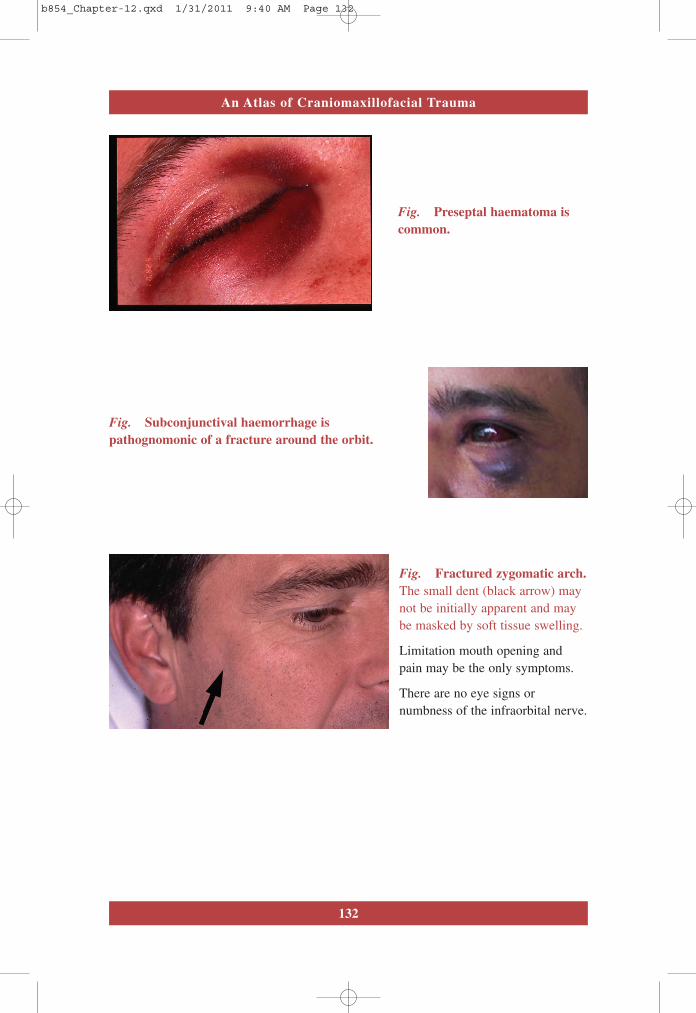
Fig. Preseptal haematoma iscommon.
Fig. Subconjunctival haemorrhage ispathognomonic of a fracture around the orbit.
Fig. Fractured zygomatic arch.The small dent (black arrow) maynot be initially apparent and maybe masked by soft tissue swelling.
Limitation mouth opening andpain may be the only symptoms.
There are no eye signs ornumbness of the infraorbital nerve.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 132
133
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
INVESTIGATIONS — Imaging
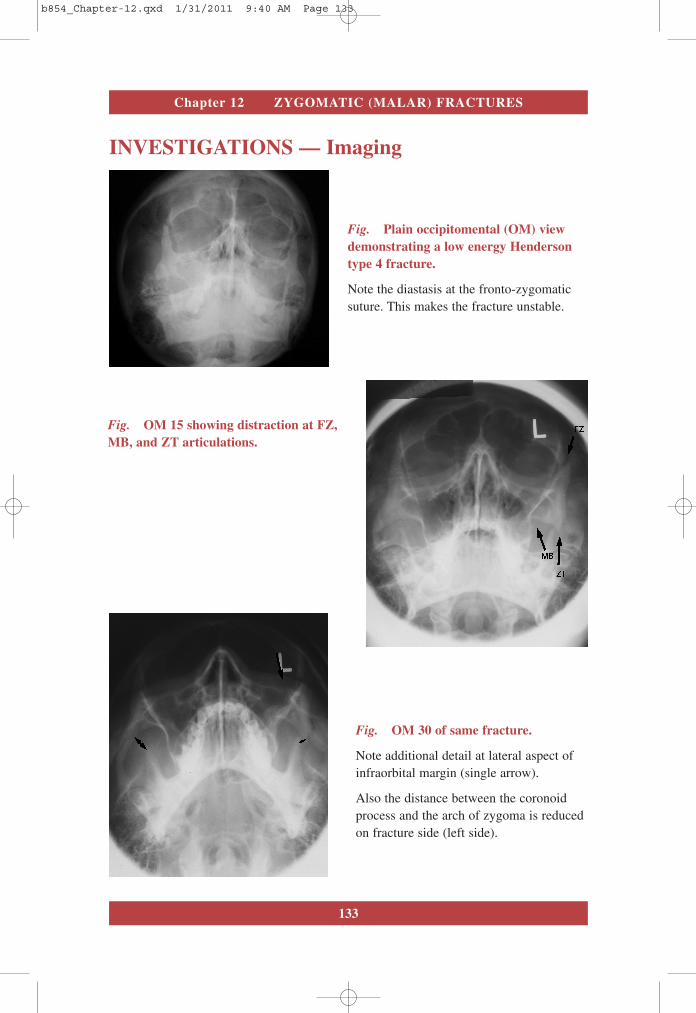
Fig. Plain occipitomental (OM) viewdemonstrating a low energy Hendersontype 4 fracture.
Note the diastasis at the fronto-zygomaticsuture. This makes the fracture unstable.
Fig. OM 15 showing distraction at FZ,MB, and ZT articulations.
Fig. OM 30 of same fracture.
Note additional detail at lateral aspect ofinfraorbital margin (single arrow).
Also the distance between the coronoidprocess and the arch of zygoma is reducedon fracture side (left side).
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 133
134
An Atlas of Craniomaxillofacial Trauma
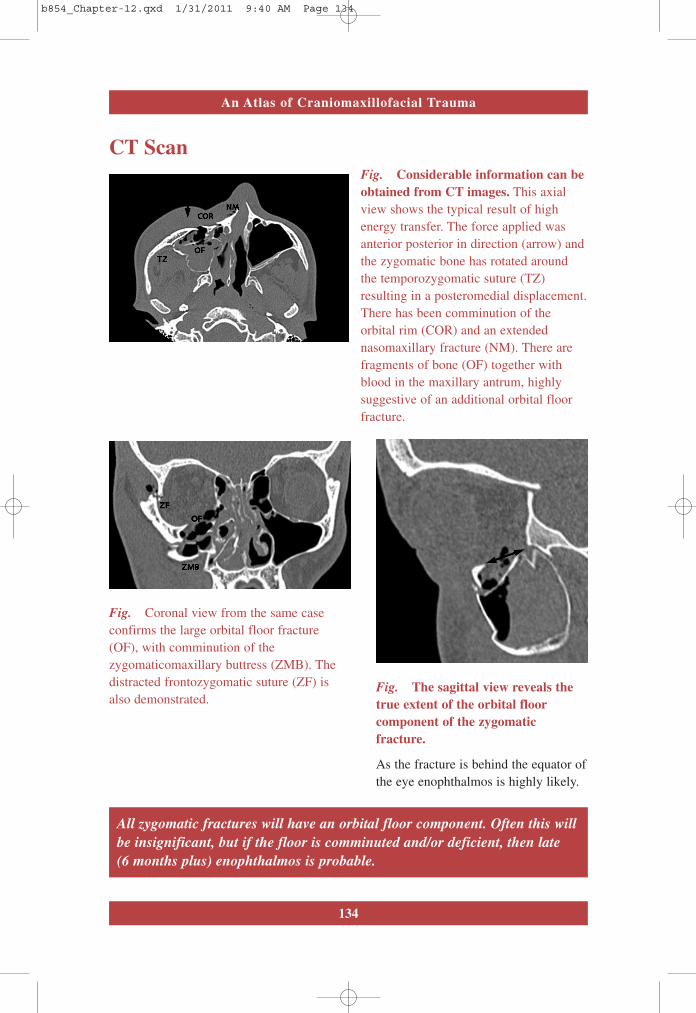
CT ScanFig. Considerable information can beobtained from CT images. This axialview shows the typical result of highenergy transfer. The force applied wasanterior posterior in direction (arrow) andthe zygomatic bone has rotated aroundthe temporozygomatic suture (TZ)resulting in a posteromedial displacement.There has been comminution of theorbital rim (COR) and an extendednasomaxillary fracture (NM). There arefragments of bone (OF) together withblood in the maxillary antrum, highlysuggestive of an additional orbital floorfracture.
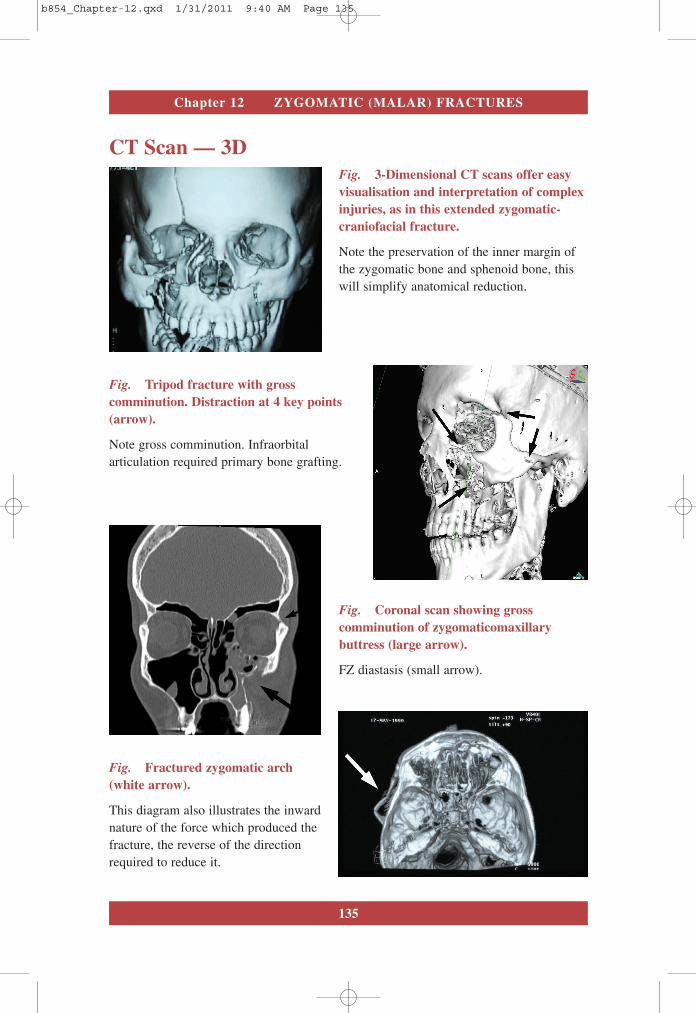
Fig. Coronal view from the same caseconfirms the large orbital floor fracture(OF), with comminution of thezygomaticomaxillary buttress (ZMB). Thedistracted frontozygomatic suture (ZF) isalso demonstrated.
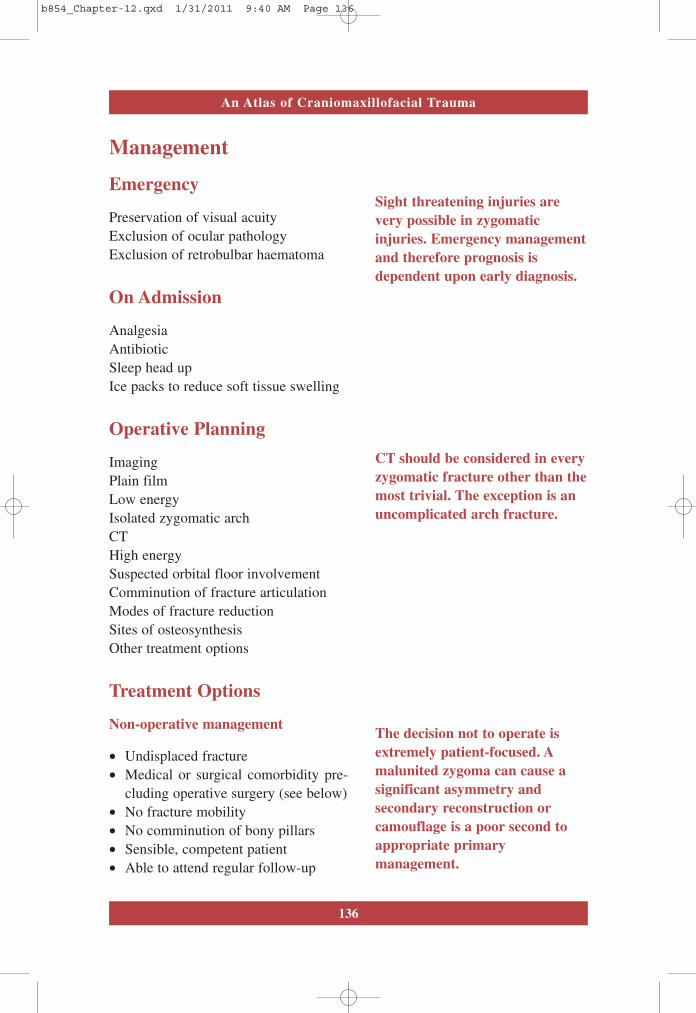
Fig. The sagittal view reveals thetrue extent of the orbital floorcomponent of the zygomaticfracture.
As the fracture is behind the equator ofthe eye enophthalmos is highly likely.
All zygomatic fractures will have an orbital floor component. Often this willbe insignificant, but if the floor is comminuted and/or deficient, then late(6 months plus) enophthalmos is probable.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 134
135
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
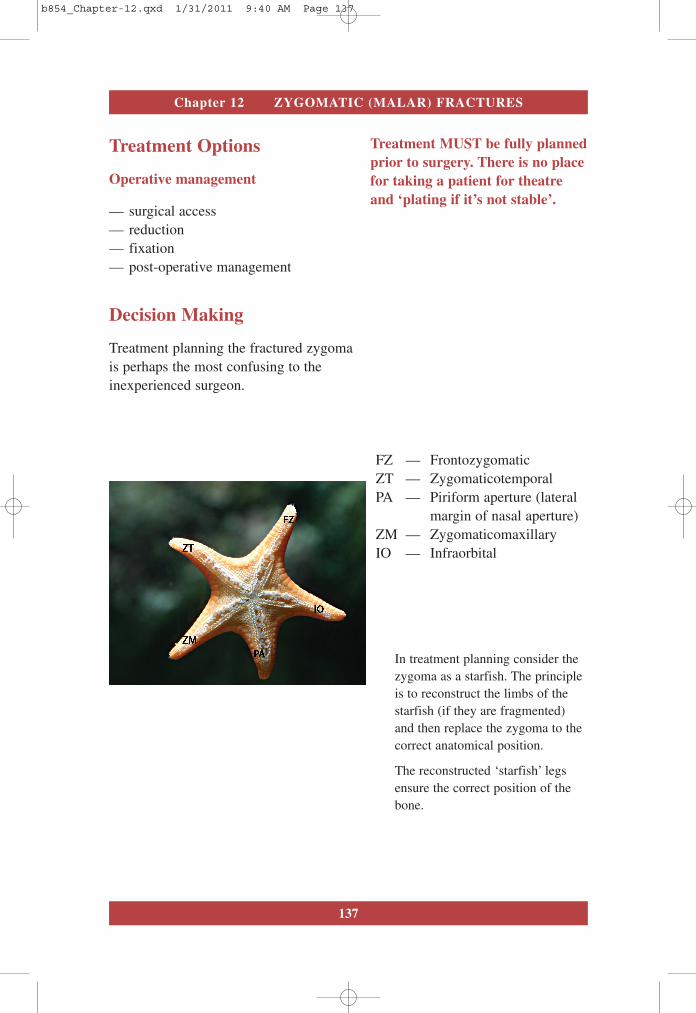
CT Scan — 3DFig. 3-Dimensional CT scans offer easyvisualisation and interpretation of complexinjuries, as in this extended zygomatic-craniofacial fracture.
Note the preservation of the inner margin ofthe zygomatic bone and sphenoid bone, thiswill simplify anatomical reduction.
Fig. Tripod fracture with grosscomminution. Distraction at 4 key points(arrow).
Note gross comminution. Infraorbitalarticulation required primary bone grafting.
Fig. Coronal scan showing grosscomminution of zygomaticomaxillarybuttress (large arrow).
FZ diastasis (small arrow).
Fig. Fractured zygomatic arch(white arrow).
This diagram also illustrates the inwardnature of the force which produced thefracture, the reverse of the directionrequired to reduce it.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 135
136
An Atlas of Craniomaxillofacial Trauma
Management
Emergency
Preservation of visual acuityExclusion of ocular pathology Exclusion of retrobulbar haematoma
On Admission
AnalgesiaAntibioticSleep head upIce packs to reduce soft tissue swelling
Operative Planning
ImagingPlain filmLow energyIsolated zygomatic archCTHigh energySuspected orbital floor involvementComminution of fracture articulationModes of fracture reductionSites of osteosynthesisOther treatment options
Treatment Options
Non-operative management
• Undisplaced fracture• Medical or surgical comorbidity pre-
cluding operative surgery (see below)• No fracture mobility• No comminution of bony pillars• Sensible, competent patient• Able to attend regular follow-up
Sight threatening injuries arevery possible in zygomaticinjuries. Emergency managementand therefore prognosis isdependent upon early diagnosis.
CT should be considered in everyzygomatic fracture other than themost trivial. The exception is anuncomplicated arch fracture.
The decision not to operate isextremely patient-focused. Amalunited zygoma can cause asignificant asymmetry andsecondary reconstruction orcamouflage is a poor second toappropriate primarymanagement.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 136
137
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
Treatment Options
Operative management
— surgical access— reduction— fixation— post-operative management
Decision Making
Treatment planning the fractured zygomais perhaps the most confusing to theinexperienced surgeon.
Treatment MUST be fully plannedprior to surgery. There is no placefor taking a patient for theatreand ‘plating if it’s not stable’.
FZ — FrontozygomaticZT — ZygomaticotemporalPA — Piriform aperture (lateral
margin of nasal aperture)ZM — ZygomaticomaxillaryIO — Infraorbital
In treatment planning consider thezygoma as a starfish. The principleis to reconstruct the limbs of thestarfish (if they are fragmented)and then replace the zygoma to thecorrect anatomical position.
The reconstructed ‘starfish’ legsensure the correct position of thebone.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 137
138
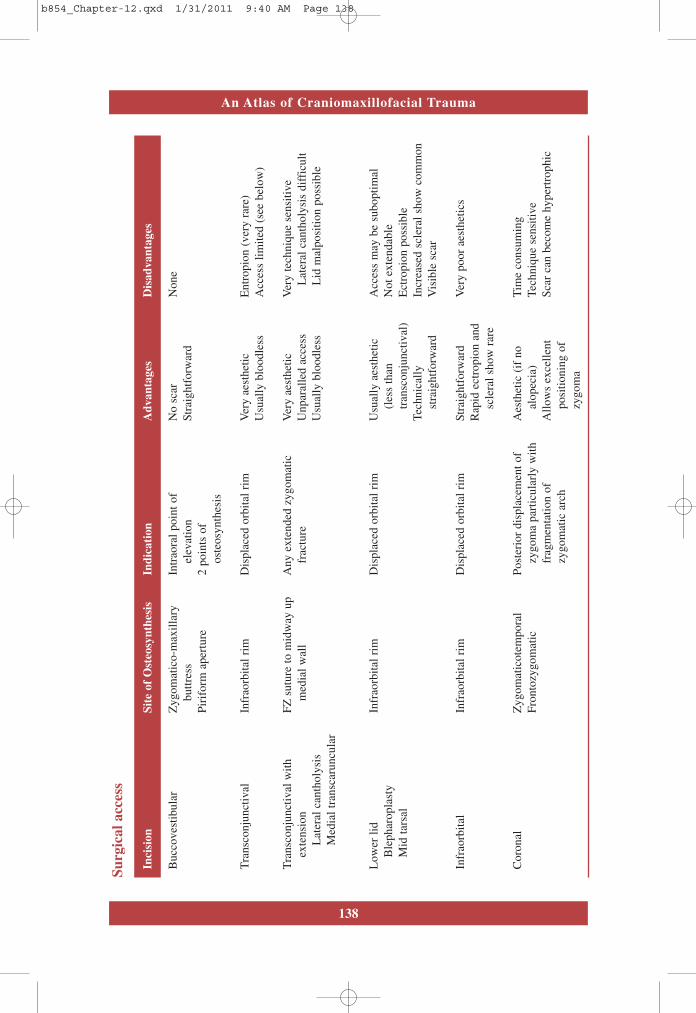
An Atlas of Craniomaxillofacial TraumaSu
rgic
al a
cces
s
Inci
sion
Site
of
Ost
eosy
nthe
sis
Indi
cati
onA
dvan
tage
sD
isad
vant
ages
Buc
cove
stib
ular
Zyg
omat
ico-
max
illar
yIn
trao
ral p
oint
of
No
scar
Non
ebu
ttres
sel
evat
ion
Stra
ight
forw
ard
Piri
form
ape
rtur
e2
poin
ts o
fos
teos
ynth
esis
Tran
scon
junc
tival
Infr
aorb
ital r
imD
ispl
aced
orb
ital r
imV
ery
aest
hetic
Ent
ropi
on (
very
rar
e)U
sual
ly b
lood
less
Acc
ess
limite
d (s
ee b
elow
)
Tran
scon
junc
tival
with
FZ s
utur
e to
mid
way
up
Any
ext
ende
d zy
gom
atic
Ver
y ae
sthe
ticV
ery
tech
niqu
e se
nsiti
veex
tens
ion
med
ial w
all
frac
ture
Unp
aral
led
acce
ssL
ater
al c
anth
olys
is d
iffi
cult
Lat
eral
can
thol
ysis
Usu
ally
blo
odle
ssL
id m
alpo
sitio
n po
ssib
leM
edia
l tra
nsca
runc
ular
Low
er li
dIn
frao
rbita
l rim
Dis
plac
ed o
rbita
l rim
Usu
ally
aes
thet
icA
cces
s m
ay b
e su
bopt
imal
Ble
phar
opla
sty
(les
s th
anN
ot e
xten
dabl
eM
id ta
rsal
tran
scon
junc
tival
)E
ctro
pion
pos
sibl
eTe
chni
cally
Incr
ease
d sc
lera
l sho
w c
omm
onst
raig
htfo
rwar
dV
isib
le s
car
Infr
aorb
ital
Infr
aorb
ital r
imD
ispl
aced
orb
ital r
imSt
raig
htfo
rwar
dV
ery
poor
aes
thet
ics
Rap
id e
ctro
pion
and
sc
lera
l sho
w r
are
Cor
onal
Zyg
omat
icot
empo
ral
Post
erio
r di
spla
cem
ent o
fA
esth
etic
(if
no
Tim
e co
nsum
ing
Fron
tozy
gom
atic
zygo
ma
part
icul
arly
with
alop
ecia
)Te
chni
que
sens
itive
frag
men
tatio
n of
Allo
ws
exce
llent
Scar
can
bec
ome
hype
rtro
phic
zygo
mat
ic a
rch
posi
tioni
ng o
fzy
gom
a
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 138
139
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
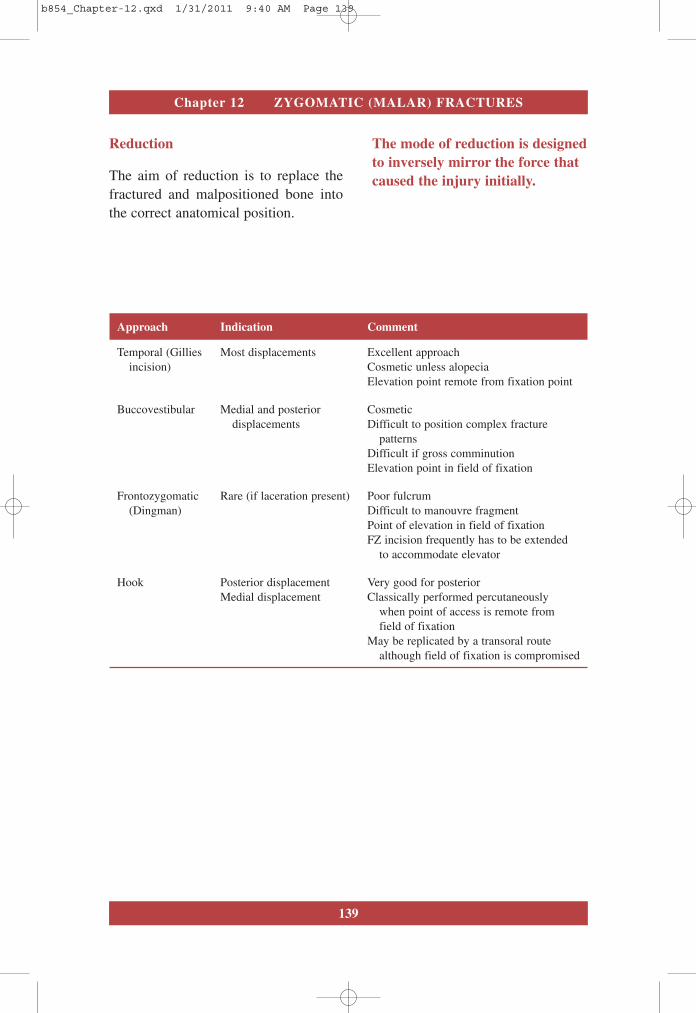
Reduction
The aim of reduction is to replace thefractured and malpositioned bone intothe correct anatomical position.
The mode of reduction is designedto inversely mirror the force thatcaused the injury initially.
Approach Indication Comment
Temporal (Gillies Most displacements Excellent approachincision) Cosmetic unless alopecia
Elevation point remote from fixation point
Buccovestibular Medial and posterior Cosmeticdisplacements Difficult to position complex fracture
patternsDifficult if gross comminutionElevation point in field of fixation
Frontozygomatic Rare (if laceration present) Poor fulcrum(Dingman) Difficult to manouvre fragment
Point of elevation in field of fixationFZ incision frequently has to be extended
to accommodate elevator
Hook Posterior displacement Very good for posteriorMedial displacement Classically performed percutaneously
when point of access is remote fromfield of fixation
May be replicated by a transoral routealthough field of fixation is compromised
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 139
140
An Atlas of Craniomaxillofacial Trauma
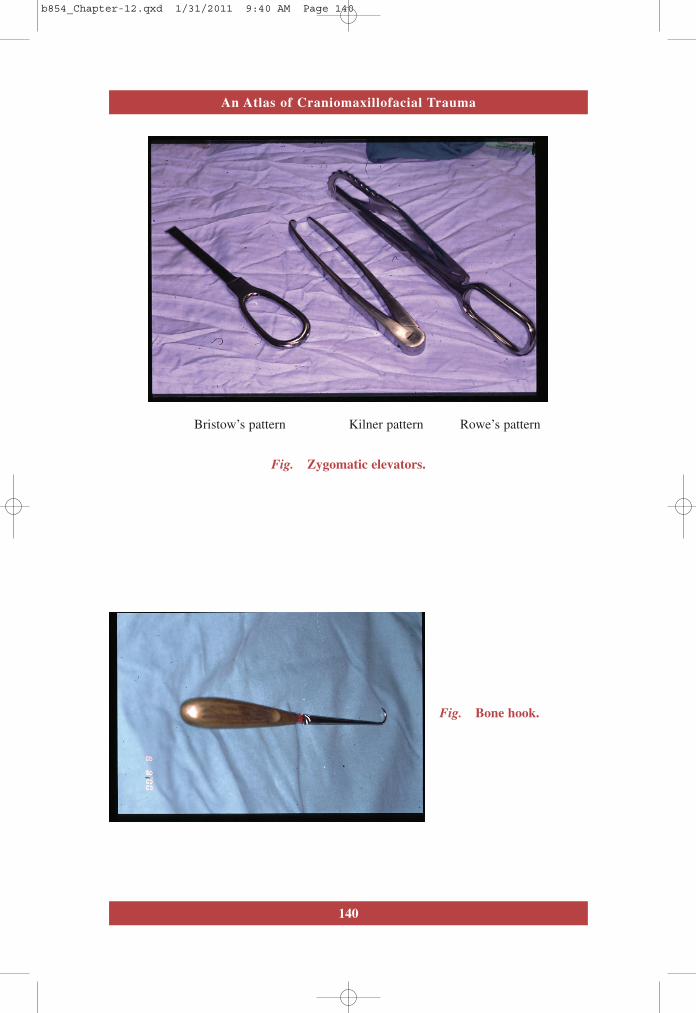
Bristow’s pattern Kilner pattern Rowe’s pattern
Fig. Zygomatic elevators.
Fig. Bone hook.
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 140
141
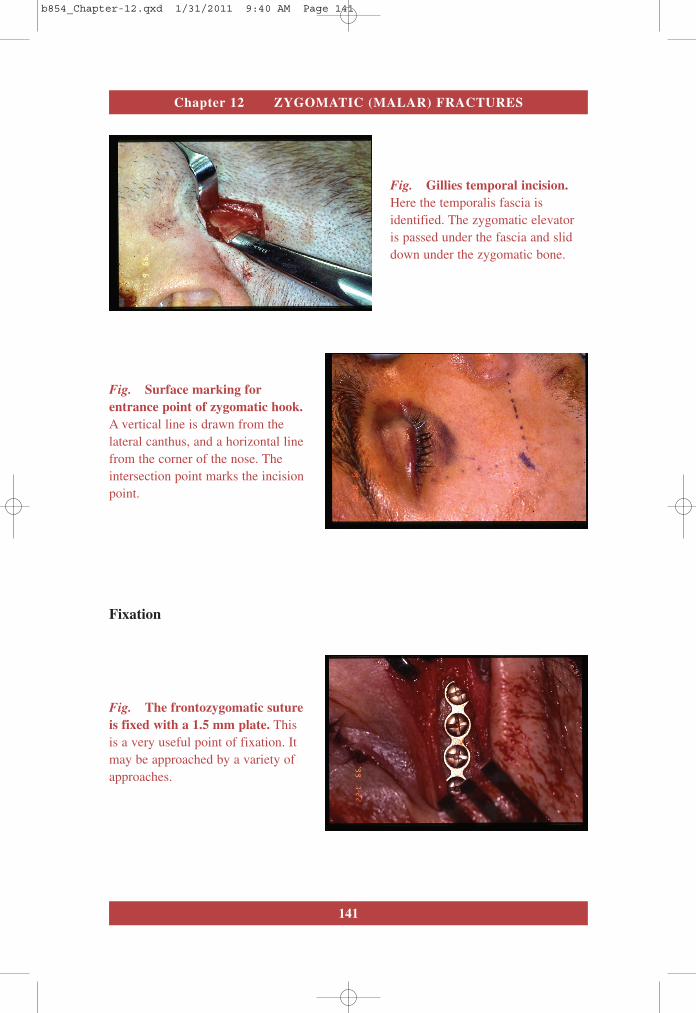
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
Fig. Gillies temporal incision.Here the temporalis fascia isidentified. The zygomatic elevatoris passed under the fascia and sliddown under the zygomatic bone.
Fig. The frontozygomatic sutureis fixed with a 1.5 mm plate. Thisis a very useful point of fixation. Itmay be approached by a variety ofapproaches.
Fig. Surface marking forentrance point of zygomatic hook.A vertical line is drawn from thelateral canthus, and a horizontal linefrom the corner of the nose. Theintersection point marks the incisionpoint.
Fixation
b854_Chapter-12.qxd 1/31/2011 9:40 AM Page 141
142
An Atlas of Craniomaxillofacial Trauma
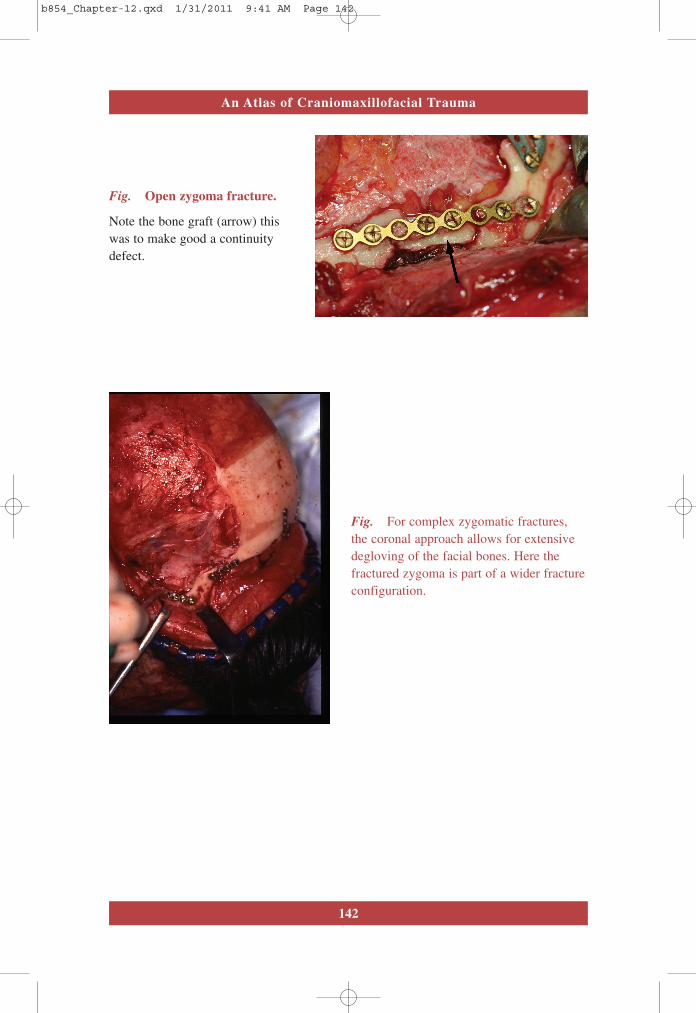
Fig. Open zygoma fracture.
Note the bone graft (arrow) thiswas to make good a continuitydefect.
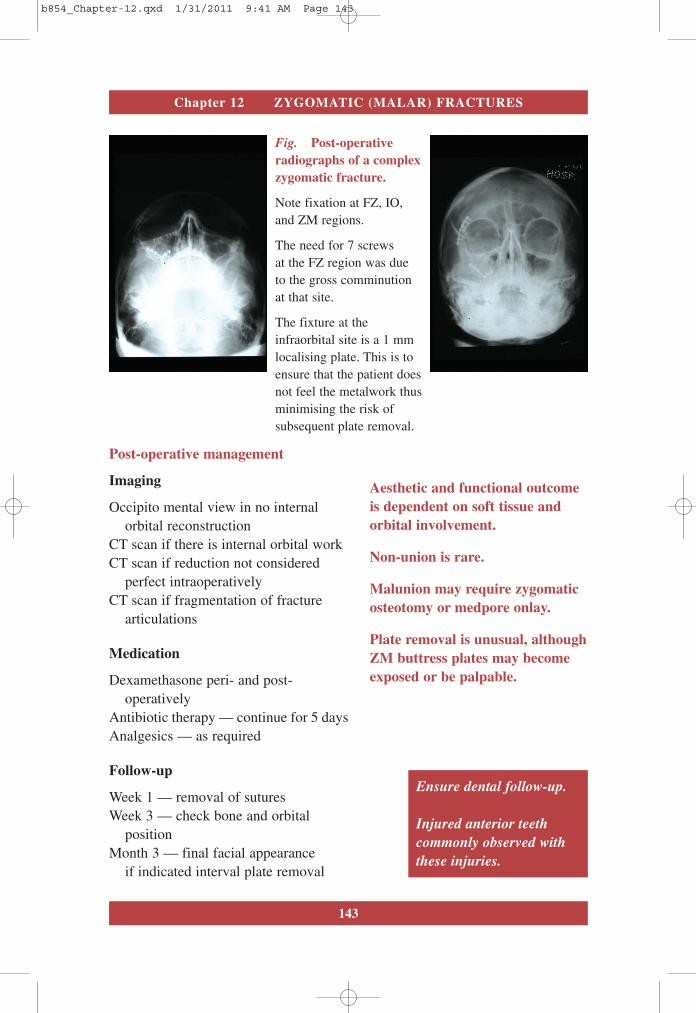
Fig. For complex zygomatic fractures,the coronal approach allows for extensivedegloving of the facial bones. Here thefractured zygoma is part of a wider fractureconfiguration.
b854_Chapter-12.qxd 1/31/2011 9:41 AM Page 142
143
Chapter 12 ZYGOMATIC (MALAR) FRACTURES
Fig. Post-operativeradiographs of a complexzygomatic fracture.
Note fixation at FZ, IO,and ZM regions.
The need for 7 screwsat the FZ region was dueto the gross comminutionat that site.
The fixture at theinfraorbital site is a 1 mmlocalising plate. This is toensure that the patient doesnot feel the metalwork thusminimising the risk ofsubsequent plate removal.
Post-operative management
Imaging
Occipito mental view in no internalorbital reconstruction
CT scan if there is internal orbital workCT scan if reduction not considered
perfect intraoperatively CT scan if fragmentation of fracture
articulations
Medication
Dexamethasone peri- and post-operatively
Antibiotic therapy — continue for 5 daysAnalgesics — as required
Follow-up
Week 1 — removal of suturesWeek 3 — check bone and orbital
positionMonth 3 — final facial appearance
if indicated interval plate removal
Aesthetic and functional outcomeis dependent on soft tissue andorbital involvement.
Non-union is rare.
Malunion may require zygomaticosteotomy or medpore onlay.
Plate removal is unusual, althoughZM buttress plates may becomeexposed or be palpable.
Ensure dental follow-up.
Injured anterior teethcommonly observed withthese injuries.
b854_Chapter-12.qxd 1/31/2011 9:41 AM Page 143
b854_Chapter-12.qxd 1/31/2011 9:41 AM Page 144
Related Documents











