CASE REPORT 195 a Assistant Professor, Karadeniz Technical University, Department of Orthodontics, Trabzon, Turkey. b Assistant Professor, Karadeniz Technical University, Department of Oral Surgery, Trabzon, Turkey. Corresponding author: Mehmet Bayram. Karadeniz Technical University, Department of Orthodontics, Trabzon, Black Sea 61080, Turkey. +90 462 3774724; e-mail, [email protected]. Received January 26, 2010; Last Revision March 6, 2010; Accepted March 9, 2010. DOI:10.4041/kjod.2010.40.3.195 Zygoma-gear appliance for intraoral upper molar distalization Metin Nur, DDS, PhD, a Mehmet Bayram, DDS, PhD, a Alper Pampu, DDS, PhD b The aim of this report is to present an intraoral upper molar distalization system supported with zygomatic anchorage plates (Zygoma-gear Appliance, ZGA). This system was used for a 16-year-old female patient with a Class II molar relationship requiring molar distalization. The system consisted of bilateral zygomatic anchorage plates, an inner-bow and heavy intraoral elastics. Distalization of the upper molars was ach- ieved in 3 months and the treatment results were evaluated from lateral cephalometric radiographs. According to the results of the cephalometric analysis, the maxillary first molars showed a distalization of 4 mm, associated with a distal axial inclination of 4.5 o . The results of this study show that an effective upper molar distalization without anchorage loss can be achieved in a short time using the ZGA. We sug- gest that this new system may be used in cases requiring molar distalization in place of extraoral appliances. (Korean J Orthod 2010;40(3):195-206) Key words: Distalization, Zygomatic anchorage plate, Class II, Anchorage INTRODUCTION Several methods have been used for upper molar distalization including extraoral 1 and intraoral 2-10 appli- ances. The esthetic and social concerns of the use of headgear wear and the anchorage loss that occurs with the application of intraoral systems have stimulated many investigators to use skeletal anchorage. To over- come these anchorage problems, skeletal anchorage units applied to palatal regions, for example, osteointe- grated implants, miniscrews, and Graz type implant were combined with these tooth and tissue supported intraoral appliances. 11-18 Although anchorage loss has been eliminated in this way, different problems related with the proximity between the implant and the roots of teeth or the presence of a bulky acrylic Nance ap- pliance behind the upper incisors may become a prob- lem during the retraction of anterior teeth. The zygomatic process of the maxilla is another ap- propriate region for skeletal anchorage. 19 Recently, zy- gomatic anchorage systems have been used alternati- vely for upper molar distalization. 20,21 We designed an intraoral upper molar distalization system supported by the zygomatic region named as the Zygoma-Gear Ap- pliance (ZGA). The aim of this study is to present the use of ZGA for bilateral upper molar distalization in a 16-year-old female with a Class II molar relationship requiring molar distalization. The system consists of two zygomatic anchor plates (Multi Purpose Anchor MPI 1000, Tasarim Med, Istan- bul, Turkey), an inner-bow, and heavy intraoral elastics (Fig 1A). The effective distalizing force vector of the ZGA is illustrated in Fig 1B. The zygomatic anchor is a titanium miniplate with three holes, which continues into a round bar. The an- chor plates are placed at the zygomatic buttress of the maxillae under local anesthesia (Fig 2). The zygomatic

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CASE REPORT
195
aAssistant Professor, Karadeniz Technical University, Department
of Orthodontics, Trabzon, Turkey.bAssistant Professor, Karadeniz Technical University, Department
of Oral Surgery, Trabzon, Turkey.
Corresponding author: Mehmet Bayram.
Karadeniz Technical University, Department of Orthodontics,
Trabzon, Black Sea 61080, Turkey.
+90 462 3774724; e-mail, [email protected].
Received January 26, 2010; Last Revision March 6, 2010;
Accepted March 9, 2010.
DOI:10.4041/kjod.2010.40.3.195
Zygoma-gear appliance for intraoral upper molar distalization
Metin Nur, DDS, PhD,a Mehmet Bayram, DDS, PhD,
a Alper Pampu, DDS, PhD
b
The aim of this report is to present an intraoral upper molar distalization system supported with zygomatic anchorage plates (Zygoma-gear Appliance, ZGA). This system was used for a 16-year-old female patient with a Class II molar relationship requiring molar distalization. The system consisted of bilateral zygomatic anchorage plates, an inner-bow and heavy intraoral elastics. Distalization of the upper molars was ach-ieved in 3 months and the treatment results were evaluated from lateral cephalometric radiographs. According to the results of the cephalometric analysis, the maxillary first molars showed a distalization of 4 mm, associated with a distal axial inclination of 4.5o. The results of this study show that an effective upper molar distalization without anchorage loss can be achieved in a short time using the ZGA. We sug-gest that this new system may be used in cases requiring molar distalization in place of extraoral appliances. (Korean J Orthod 2010;40(3):195-206)
Key words: Distalization, Zygomatic anchorage plate, Class II, Anchorage
INTRODUCTION
Several methods have been used for upper molar
distalization including extraoral1 and intraoral2-10 appli-
ances. The esthetic and social concerns of the use of
headgear wear and the anchorage loss that occurs with
the application of intraoral systems have stimulated
many investigators to use skeletal anchorage. To over-
come these anchorage problems, skeletal anchorage
units applied to palatal regions, for example, osteointe-
grated implants, miniscrews, and Graz type implant
were combined with these tooth and tissue supported
intraoral appliances.11-18 Although anchorage loss has
been eliminated in this way, different problems related
with the proximity between the implant and the roots
of teeth or the presence of a bulky acrylic Nance ap-
pliance behind the upper incisors may become a prob-
lem during the retraction of anterior teeth.
The zygomatic process of the maxilla is another ap-
propriate region for skeletal anchorage.19
Recently, zy-
gomatic anchorage systems have been used alternati-
vely for upper molar distalization.20,21 We designed an
intraoral upper molar distalization system supported by
the zygomatic region named as the Zygoma-Gear Ap-
pliance (ZGA). The aim of this study is to present the
use of ZGA for bilateral upper molar distalization in
a 16-year-old female with a Class II molar relationship
requiring molar distalization.
The system consists of two zygomatic anchor plates
(Multi Purpose Anchor MPI 1000, Tasarim Med, Istan-
bul, Turkey), an inner-bow, and heavy intraoral elastics
(Fig 1A). The effective distalizing force vector of the
ZGA is illustrated in Fig 1B.
The zygomatic anchor is a titanium miniplate with
three holes, which continues into a round bar. The an-
chor plates are placed at the zygomatic buttress of the
maxillae under local anesthesia (Fig 2). The zygomatic

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
196
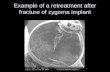
Fig 2. The zygomatic anchor plates adapted and fixed to the zygomatic buttress.
Fig 1. Schematic illustration of components (A) and the effective distalizing force vector of theZGA (Zygoma-Gear Appliance) (B).
buttress is palpated in the labial sulcus, and a 1- to
2-cm-high vertical incision is made starting at the mu-
cogingival junction while maintaining contact with the
bone. The lower aspect of the zygomatic process of
the maxilla is totally exposed by blunt dissection. The
anchor plate is adjusted to fit the contour of the lower
face of each zygomatic process and fixed by three
bone screws (length, 7.0 mm). The body portions of
them are positioned subperiosteally. The round bars are
intraorally exposed and positioned outside the denti-
tion, so that they never disturb the distalization of the
maxillary molars. After fixation, the incision site is
closed and sutured. The free intraoral parts of the min-
iplates are bent distally into hooks.
The inner-bow is made from stainless steel wire, 1.1
mm in diameter and designed like the inner part of a
conventional facebow. Two hooks are soldered onto
the inner-bow at the lateral teeth regions, and U bends
are bent bilaterally in front of the upper first molars.
The inner-bow is adjusted to the headgear tubes on the
upper first molar bands. A distally directed force is ap-
plied to the upper molar teeth via the heavy intraoral
elastics, which are placed between the zygomatic plate
and the inner-bow hooks.
DIAGNOSIS AND ETIOLOGY
A 16-year and 8 month-old female was diagnosed
with skeletal Class II, Division 1 malocclusion. She
was referred to our department for consultation about
her unerupted upper teeth. She had a well-balanced
face and a mild convex profile (Fig 3). The dental
midlines were concordant with each other and with her
face, and no mandibular shift was detected on closure.
Intraoral examination revealed that she had a bilateral
Class II molar and canine relationship with a posterior

Vol. 40, No. 3, 2010. Korean J Orthod Zygoma-gear appliance for intraoral upper molar distalization
197
Fig 3. Pretreatment facial and intraoral photographs of the case.
crossbite on the right side. The dental cast analysis
showed 2 mm of space deficiency in the upper arch,
1.5 mm of space excess in the lower arch, 4 mm over-
jet, and 6 mm overbite (Fig 4). The maxillary lateral
incisors were small, creating a tooth size discrepancy.
Bolton’s tooth size analysis revealed a maxillary ante-
rior deficiency of 2.1 mm.
Radiographic examination showed that all teeth, in-
cluding the third molars, were present (Fig 5). Initial
panoramic radiograph revealed that both maxillary can-
ines had well developed roots, were impacted at the
level of the roof of the palate, and were mesially angu-
lated near the roots of the maxillary lateral incisors.
Further detailed radiographic investigation disclosed no
significant resorption of the roots of the maxillary lat-
eral incisors. A horizontal tube shift technique with pe-
riapical radiographs and clinical palpation confirmed
that both impacted maxillary canines were in the pala-
tal position.
Cephalometric evaluation revealed a mild skeletal
Class II pattern due to a mild mandibular retrognatia.
The pre-treatment cephalometric parameters showed
that the maxilla was normal (SNA 82o), and in centric
occlusion the mandible was in a slightly retruded posi-
tion according to the cranial base (SNB 76o). The max-
illary incisors were slightly upright, while the man-
dibular incisors were normal. The mandibular plane
was normal relative to the cranial base (SN-GoGn
34.5o).

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
198
Fig 4. Pretreatment diagnostic models of the case.
Fig 5. Pretreatment radiographic records of the case.
TREATMENT OBJECTIVES
Treatment objectives, based on the clinical examina-
tion and cephalometric analysis, were to:
1. Align the palatally impacted maxillary canines.
2. Correct the unilateral posterior crossbite.
3. Obtain normal overjet and overbite.
4. Establish a well-intercuspated bilateral Class I ca-
nine and molar occlusion.
5. Constitute a good aesthetic smile.
TREATMENT ALTERNATIVES
There were four treatment alternatives for this case:
(1) align the palatally impacted maxillary canines and
distalization of upper molars; (2) extraction of the im-
pacted canines and closure of the extraction space or-
thodontically; (3) extraction of the impacted canines
and prosthetic rehabilitation with implants or bridge-
work; and (4) align the palatally impacted maxillary
canines with the extraction of two upper first pre-
molars.
Considering all aspects of the case in detail, during
the treatment-planning interview, the patient was told

Vol. 40, No. 3, 2010. Korean J Orthod Zygoma-gear appliance for intraoral upper molar distalization
199
Fig 6. Intraoral occlusal views of the mechanics for erupting of the impacted canines (A), and of the erupted canines(B).
Fig 7. Application of the ZGA (Zygoma-Gear Appliance) at the beginning of distalization (A), and the views of thepatient immediately after the distalization (B).
that the impacted canines might not respond to ortho-
dontic eruption; and if this were the case, they would
need to be extracted, and prosthetic rehabilitation with
implants or bridgework would be required. She chose
orthodontic eruption of the impacted canines with the
nonextraction approach, and informed consent was tak-
en to this effect.
TREATMENT PROGRESS
Preadjusted fixed appliances (0.022 × 0.028-in, MBT
system) were placed in both arches to achieve leveling
and alignment. Intraoral cross elastics were used for
the correction of crossbite at the right first molars.
After the leveling phase, the retained primary canines
were extracted and then both palatally impacted maxil-
lary canines were surgically exposed with the help of
an envelope flap. Bondable cleats were bonded to
them, and stainless steel ligature wires were braided
from these cleats. After soft tissue healing, an auxiliary
continuous 0.016-in Australian wire including vertical
loops with terminal eyelets was applied with a 0.016-in
stainless steel main archwire (Fig 6A). In the passive
state, the eyelets faced down occlusally. Torsion was
built up in the round wire, which was secured at its
distal ends as the vertical loops were bent through 90o
to tie them to the braided ligatures from the canines.
This was done to generate eruptive forces for the bi-

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
200
Fig 9. The system for retraction of the incisors.
Fig 8. Lateral cephalometric radiograph of the case taken immediately after the distalization.
laterally impacted teeth. After 2.5 months of traction,
it was observed that the maxillary canines were erupt-
ed sufficiently in crossbite. An elastic chain was ap-
plied to move the canines labially (Fig 6B). Bite-rais-
ers (Guray Bite Raiser, GAC International Inc, Bohem-
ia, NY) were adjusted on the upper first molar bands
for bite-opening to avoid possible interferences be-
tween the upper canines and lower teeth during the la-
bial movement of the upper canines.
When the maxillary canines had moved into the arch,
canine brackets were then bonded and a continuous
0.016-in superelastic nickel-titanium (NiTi) wire was
placed. After leveling, we decided to accomplish the
upper molar distalization with an extraoral appliance.
However, usage of an extraoral appliance was rejected
by the patient and her parents because the patient was
concerned about her facial appearance. Therefore, the
ZGA was designed and applied for distalization of the
upper molars (Fig 7A).
Three weeks after the zygomatic plate implantation
surgery, a distalization force of 400 g per side was ap-
plied to the upper molars. The patient was instructed
to wear her appliance for at least 20 hours a day and
to change intraoral elastics every 12 hours. After 3
months of distalization, super Class I molar relation-
ships were achieved on both sides (Figs 7B and 8).
The teeth located at the anterior of the upper molars
were also distalized together with the molar teeth,
spontaneously. Then fixed appliance treatment was pro-
gressed for other alignment problems. The maxillary
premolars and canines were completely distalized by
using power chains. After the Class I canine relation-
ship was obtained, the retraction of incisors was ac-
complished by using closed coils, which were placed
between the zygomatic anchor and 0.019 × 0.025-in
stainless steel posted archwire (Fig 9).
At the end of active treatment, finishing procedures
were used for the final alignment of the teeth and de-
tailing of the occlusion. The orthodontic appliances
were removed after active treatment was completed
(Figs 10 - 12). After debonding procedures, peg shaped
maxillary lateral incisors were restored with composite
resin (Fig 13) and a maxillary removable Hawley re-
tainer and a 3-3 mandibular fixed lingual retainer were
constructed for the patient and placed.
RESULTS
After 21 months of treatment with the ZGA and full
fixed orthodontic appliances, the impacted canines
were successfully aligned and Class I molar and canine
relationships were established with satisfactory inter-

Vol. 40, No. 3, 2010. Korean J Orthod Zygoma-gear appliance for intraoral upper molar distalization
201
Fig 10. Posttreatment facial and intraoral photographs of the case.
digitation of the posterior teeth. Acceptable overjet and
overbite were also achieved and the tooth size discrep-
ancy caused by the upper lateral incisors was managed
successfully.
Table 1 shows the cephalometric changes in all
stages of the treatment. A comparison of the pre- and
post-distalization cephalometric analysis revealed that
the maxillary first molars showed a distalization of 4
mm, associated with a distal axial inclination of 4.5o.
Non-significant changes were observed in vertical an-
gles (SN/GoGn, FMA, and ANS-PNS/GoGn) (Fig 14A).
According to the analysis of the posttreatment lateral
cephalometric radiograph, SNA, ANB, Wits appraisal,
interincisal angle, overjet, and overbite were decreased
(Fig 14B).
After the completion of active treatment, the centric
relation coincided with the centric occlusion, and the
patient reported no temporomandibular joint problems.
The final panoramic radiograph showed that minimal
root resorption had occurred during treatment and that
root parallelism was satisfactory. The patient has been
in retention for more than 12 months, and the occlu-
sion has been maintained very well during this time.
DISCUSSION
Nonextraction treatment of Class II malocclusion of-
ten requires distal movement of the upper molar teeth

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
202
Fig 13. Intraoral photographs of the case after restoring the peg shaped upper lateral incisors.
Fig 12. Posttreatment radiographic records of the case.
Fig 11. Posttreatment dental casts of the case.
into a Class I relationship. Conventional extraoral ap-
pliances such as headgear are frequently used for this
purpose.1 Despite their efficacy in tooth movement;
these appliances have the major disadvantage of a

Vol. 40, No. 3, 2010. Korean J Orthod Zygoma-gear appliance for intraoral upper molar distalization
203
Pretreatment Before distalization After distalization Posttreatment
SNA (o) 82 81 81 80.5
SNB (o) 76 76 76.5 77
ANB (o) 6 5 4.5 3.5
SN-GoGn (o) 34.5 34 34.5 34
FMA (o) 22.5 23 23 22.5
ANS-PNS/GoGn (o) 23 23 22.5 22.5
S-Go (mm) 72.5 73 73 73
N-Me (mm) 115 115.5 115 115
ANS-Me (mm) 62 61.5 61 61.5
S-Go/N-Me (%) 63 63.2 63.4 63.4
Wits appraisal (mm) 5.5 2.5 2 2
U1-NA (mm) 2 2.5 4 3.5
U1-NA (o) 13 16 20 20.5
U1-ANS-PNS (o) 106.5 107.5 108 112
L1-NB (mm) 5 4 2.5 4
L1-NB (o) 23 20 17 23
IMPA (o) 92.5 90 88 93.5
U1-PtV (mm) 60.5 60 60 60
U6-PtV (mm) 33.5 33 29 30
U6/ANS-PNS (o) 92 90.5 85 90
Interincisal angle (o) 138 140 139.5 133.5
Overjet (mm) 4 4.5 4.5 2.5
Overbite (mm) 6 4.5 5 4
Lower lip-E line (mm) 0 0.5 0.5 1
Upper lip-E line (mm) 1.5 4 4 4
Nasolabial angle (o) 111 114 114 112
Table 1. Cephalometric measurements of the patient
heavy dependence on patient cooperation. Additionally,
many patients reject headgear wear because of social
and esthetic concerns.
The difficulty in the use of headgear wear has
stimulated many investigators to develop intraoral de-
vices and techniques for the distal movement of
molars.2-10 Intraoral maxillary molar distalization appli-
ances, such as Wilson arches,2 repelling magnets,3
Hilgers pendulum appliances,4-6
the sectional jig assem-
bly,7 the distal jet,8 the Keles slider,9 and the first class
appliance10 do not require extensive cooperation from
patients. However, they have several disadvantages
such as mesialization of the maxillary premolars, pro-
trusion of the maxillary incisors, an increase in overjet,
and relapse of molars. Relapse of molar distalization is
commonly seen as the molars are used as anchorage
during distalization and retraction of the premolars and
incisors.
To remedy these anchorage problems of noncom-
pliant appliances, intraoral distalizing mechanics com-
bined with palatal implants have attracted attention,11-16
because it has become possible to distalize the maxil-
lary molars without anchorage loss by using absolute
anchorage more efficiently than ever. Although anchor-
age loss has been eliminated in this way, an important
problem still occurs during the retraction of anterior
teeth. Because of the proximity of palatal implant to
the roots of anterior teeth or the presence of a bulky
acrylic Nance appliance behind the upper incisors, the
retraction of the anterior teeth is limited. At this stage,

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
204
Fig 14. Superimpositions of pre- and post-distalization (A), and pre- and post-treatment cephalometric tracings (B).
the palatal implants must be removed and the dista-
lized molars are used as part of the anchorage during
retraction of the anterior teeth. Therefore, the reinforce-
ment of molar anchorage or the use of another anchor-
age area is required to prevent the relapse of molars.
The zygomatic process of the maxilla can be used for
this purpose because zygomatic anchors can be posi-
tioned at the zygomatic buttress, at a safe distance
from the roots of the maxillary molars and allow a full
unit buccal segment distalization.20,21 Sugawara et al.20
and Kaya et al.21 described their distalization systems
supported with the zygomatic anchor plates. They re-
ported that the en-masse distalization of maxillary buc-
cal segments was successfully accomplished by their
systems.
In the current study, we used the ZGA for upper mo-
lar distalization in a 16-year-old girl. The upper molars
were efficiently distalized to Class I relationships with-
out anchorage loss in a short time. The ZGA system
has more advantages than other intraoral distalization
appliances and combines the advantages of extraoral
and intraoral appliances.
The upper molar distalization with the ZGA system
is completely different from previous intraoral molar
distalization methods. The difference in the appliance
design enables the first and second premolars to drift
distally freely with the help of the transeptal fibers.
The distalized molars are never required as part of the
anchorage during the retraction of the premolars and
the anterior teeth, because the orthodontic force can be
directly provided from the zygomatic anchor plates.
Additionally, this system is more esthetic than extra-
oral appliances and is well tolerated by the patient.
The other advantages of this system are the simple
and hygienic design, easy application, short chair time,
minimal laboratory procedures, controllable force mag-
nitude, and easy repair. The force magnitude can be
adjusted according to need to achieve treatment objec-
tives. A different amount of distalization can be ach-
ieved on each side. When needed, all parts of the ap-
pliance (molar bands, elastics, and inner-bow) can be
easily repaired or changed except the zygomatic anchor
plates. This new system also allows the use of fixed
orthodontic appliances during the molar distalization,
simultaneously. On the other hand, the minor surgical
operation to place the anchorage plates on the zygo-
matic buttress was the main disadvantage of this ap-
pliance. The necessity of a second operation for the re-
moval of these plates and additional cost appears to be
another disadvantage.
From a clinical point of view, the choice of force
system and the optimum force magnitude are the deci-
sive factors for obtaining the desired tooth movement.22
Achieving the bodily movement of molars is also an
important strategy in modern orthodontics during dis-
talization. For this purpose, an effective force vector

Vol. 40, No. 3, 2010. Korean J Orthod Zygoma-gear appliance for intraoral upper molar distalization
205
must be passed through the center of the resistance
(CR) of teeth. In our case, the vector for an effective
distalizing force was located occlusally close to the CR
of the upper first molars. The force vector of ZGA
could be adjusted to obtain bodily molar movements
by changing the level of the zygomatic anchor hooks
and the height of the inner bow hooks. Additionally,
we used heavy intra oral elastics to gain orthodontic
force. As is known, this type of force is intermittent
in character. A continuous force is desirable for pro-
viding more efficient tooth movement. Thus, the force
characteristic of the ZGA could be converted to a con-
tinuous form with the usage of NiTi closed coils in-
stead of elastics. The appliance can be modified ac-
cording to the treatment objectives. In further studies,
the effects of the ZGA on dentofacial structures could
be assessed with large samples.
CONCLUSION
In conclusion, the results demonstrated that for this
case the ZGA was an effective system to distalize up-
per molars without anchorage loss. Absolute anchorage
control was provided by using zygomatic anchorage
plates during the distalization of molars and the re-
traction of incisors. The main disadvantage of this sys-
tem was the minor surgical operations to place and re-
move the plates. We suggest that this new system can
be used in nonextraction Class II treatment in place of
extraoral and intraoral distalization appliances.
-국문 록 -
Zygoma-gear를 이용한 구치부 후방이동을 통한
비발치 치험례
Metin Nur, Mehmet Bayram, Alper Pampu
본 증례보고에서는 골격성 II 계를 보이는 16세 여자 환자에서 zygomatic-anchorage plates (Zygoma-gear Appli-ance, ZGA)를 이용하여 상악 구치를 후방 이동시킨 구내 장치를 소개하고자 한다. 이 장치는 양측성 zygomatic anchor-age plates, inner-bow와 강한 힘을 내는 구강 내 고무 로
구성되어 있다. 3개월 내에 상악 구치의 후방 이동이 이루어졌으며, 측모 두부 방사선 사진 분석 결과, 상악 구치는 4
mm 후방 이동, 4.5o 후방 경사되었다. 본 연구 결과 ZGA 장치를 이용해 고정원 소실 없이 단기간에 상악 구치의 후방
이동이 효과 으로 이루어졌음이 확인되었으며, 이를 통해 구치의 후방 견인이 요하는 증례에서 구외 장치 신 사용될
수 있을 것으로 단된다.
주요 단어: 구치 후방이동, 골격성 고정원, 2 부정교합,
비발치 치료
REFERENCES
1. Cangialosi TJ, Meistrell ME Jr, Leung MA, Ko JY. A cepha-
lometric appraisal of edgewise Class II nonextraction treatment
with extraoral force. Am J Orthod Dentofacial Orthop 1988;
93:315-24.
2. Wilson WL, Wilson RC. Modular 3D appliances. Problem
solving in edgewise, straightwire and lightwire treatment. J
Clin Orthod 1984;18:272-81.
3. Blechman AM. Magnetic force systems in orthodontics.
Clinical results of a pilot study. Am J Orthod 1985;87:201-10.
4. Hilgers JJ. The pendulum appliance for Class II non-com-
pliance therapy. J Clin Orthod 1992;26:706-14.
5. Byloff FK, Darendeliler MA. Distal molar movement using the
pendulum appliance. Part 1: clinical and radiological evalua-
tion. Angle Orthod 1997;67:249-60.
6. Taner TU, Yukay F, Pehlivanoglu M, Cakirer B. A com-
parative analysis of maxillary tooth movement produced by
cervical headgear and pend-x appliance. Angle Orthod
2003;73:686-91.
7. Haydar S, Uner O. Comparison of Jones jig molar distalization
appliance with extraoral traction. Am J Orthod Dentofacial
Orthop 2000;117:49-53.
8. Carano A, Testa M. The distal jet for upper molar distali-
zation. J Clin Orthod 1996;30:374-80.
9. Keles A, Pamukcu B, Tokmak EC. Bilateral maxillary molar
distalization with sliding mechanics: keles slider. World J
Orthod 2002;3:57-66.
10. Fortini A, Lupoli M, Giuntoli F, Franchi L. Dentoskeletal ef-
fects induced by rapid molar distalization with the first class
appliance. Am J Orthod Dentofacial Orthop 2004;125:697-705.
11. Kärcher H, Byloff FK, Clar E. The Graz implant supported
pendulum, a technical note. J Craniomaxillofac Surg 2002;30:
87-90.
12. Keles A, Erverdi N, Sezen S. Bodily distalization of molars
with absolute anchorage. Angle Orthod 2003;73:471-82.
13. Gelgör IE, Büyükyilmaz T, Karaman AI, Dolanmaz D,
Kalayci A. Intraosseous screw-supported upper molar distali-
zation. Angle Orthod 2004;74:838-50.
14. Kircelli BH, Pektas ZO, Kircelli C. Maxillary molar distaliza-
tion with a bone-anchored pendulum appliance. Angle Orthod
2006;76:650-9.
15. Kinzinger GS, Diedrich PR, Bowman SJ. Upper molar dis-
talization with a miniscrew-supported distal jet. J Clin Orthod
2006;40:672-8.
16. Escobar SA, Tellez PA, Moncada CA, Villegas CA, Latorre

Metin Nur, Mehmet Bayram, Alper Pampu 대치교정지 40권 3호, 2010년
206
CM, Oberti G. Distalization of maxillary molars with the
bone-supported pendulum: a clinical study. Am J Orthod
Dentofacial Orthop 2007;131:545-9.
17. Bayram M, Nur M, Kilkis D. The frog appliance for upper
molar distalization: a case report. Korean J Orthod 2010;40:
50-60.
18. Kim SJ, Chun YS, Jung SH, Park SH. Three dimensional anal-
ysis of tooth movement using different types of maxillary mo-
lar distalization appliances. Korean J Orthod 2008;38:376-87.
19. De Clerck H, Geerinckx V, Siciliano S. The zygoma anchor-
age system. J Clin Orthod 2002;36:455-9.
20. Sugawara J, Kanzaki R, Takahashi I, Nagasaka H, Nanda R.
Distal movement of maxillary molars in nongrowing patients
with the skeletal anchorage system. Am J Orthod Dentofacial
Orthop 2006;129:723-33.
21. Kaya B, Arman A, Uckan S, Yazici AC. Comparison of the
zygoma anchorage system with cervical headgear in buccal
segment distalization. Eur J Orthod 2009;31:417-24.
22. Burstone CJ. Application of bioengineering to clinical ortho-
dontics. In: Graber TM, Vanarsdall RJ editors. Orthodontics.
Current principles and techniques. 3rd ed. St Louis: CV
Mosby; 2000. p. 259-92.
Related Documents