Hépatite B Fabien Zoulim Département d’hépatologie & INSERM U1052, Lyon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hépatite B
Fabien ZoulimDépartement d’hépatologie
& INSERM U1052, Lyon

EPIDEMIOLOGIE DE L’HÉPATITE B
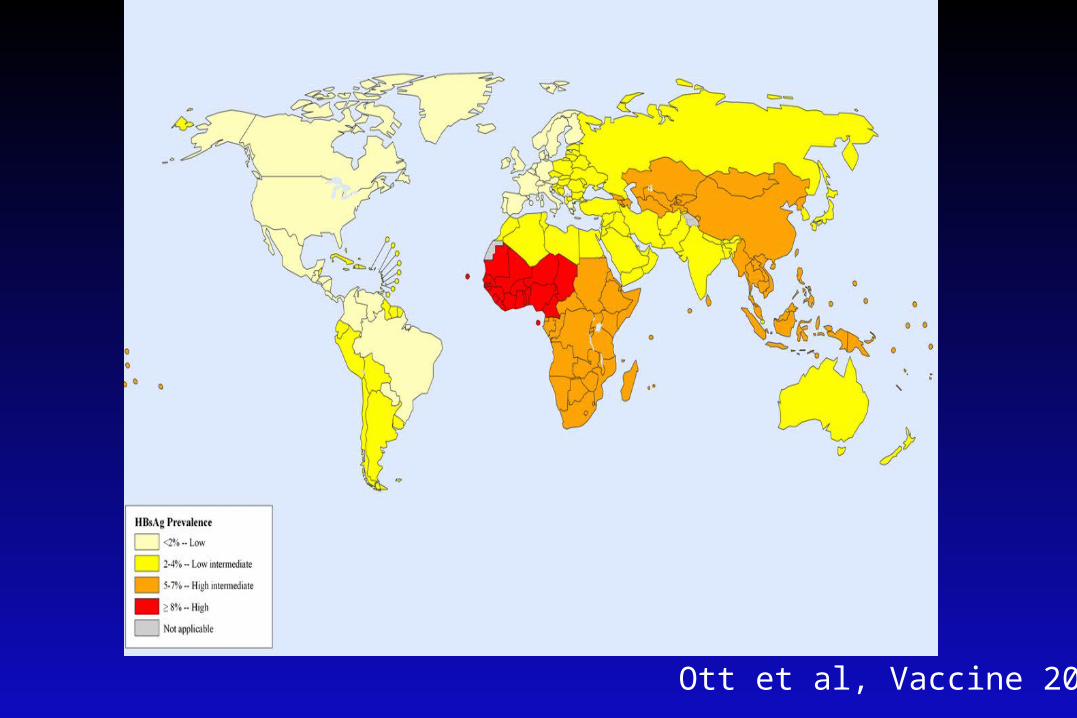
Ott et al, Vaccine 2012
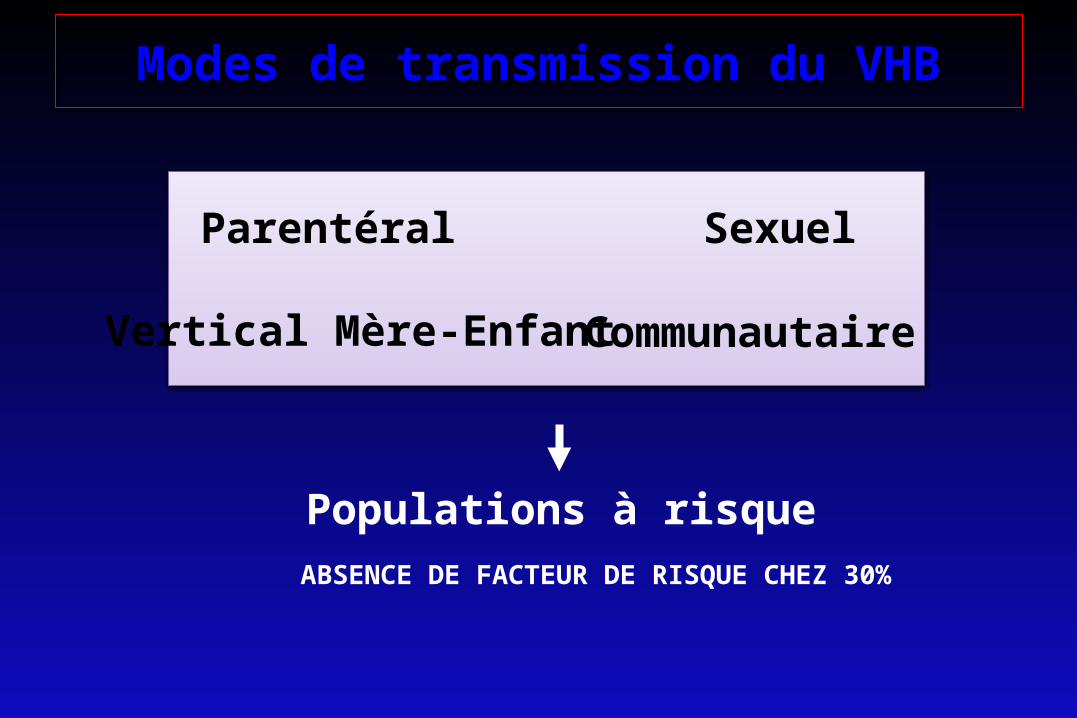
Modes de transmission du VHB
Parentéral Sexuel
Vertical Mère-Enfant Communautaire
Populations à risqueABSENCE DE FACTEUR DE RISQUE CHEZ 30%

MODES DE TRANSMISSION DU VIRUS DE L'HÉPATITE B EN EUROPE
sexuelle34%
hétéro23%
homo11%
drogue IV26%
inconnue31%
hémodialysés8%
transfusions2%
personnels de santé 2%
contact avecporteur du VHB
4%
AsieTransmission verticale

Déclaration obligatoire de l’hépatite B en France :
résultats des 12 premiers mois de notification
Denise Antona, E Delarocque-Astagneau, D Lévy-Bruhldépartement des maladies infectieuses

Results
158 acute hepatitis cases
• Hospital doctor in 64% cases
• Sex ratio M/F : 2,95 (118/40)
• Median age: 37 yrs for males, 36yrs for females
• Jaundice : 69%
• Hospitalisation : 46%
• Fulminant hepatitis : 3 (2 death)

Risk exposure within 6 months preceding the acute case Source : obligatory declaration 2003-04
• Source: obligatory declaration march 03- february 2004 N=145– Sexual 59 40,6% No factor
43 29,6%– IVDU 9 6,2% >1 factor 38
26,3%– Invasive treatment 15 10,3%
– Tatoo, piercing 5 3,4%– Familial 14 9,7%– Perinatal 2 1,4%– Live in instiution 11 7,6%– Travel in endemic 21 14,5% areas91/145 patients (63 %) had a vaccine indication (2 vaccinated ≥
3 doses)
• Sentinel networks 91-96 N=195 – sexual
35% – IVDU
19%– « percutaneous »
15%– No factor
35%

Surveillance épidémiologique de l’infection HBV
• 14 446 adultes testés• Prévalence de l’AgHBs 0,65% (280 000 porteurs
chroniques du VHB)• Homme 1,1% versus 0,2% femme• Naissance en zone d’endémie 4% versus 0,5%• Précarité, séjour en institution, homosexualité,
usage de droguesMeffre et al, J. Med Virol 2004

Distribution géographiqueDonnées en France
InVS, 2004.
• Prévalence du portage de l'AgHBs : estimée à 0,65 %

Hépatites virales B: épidémiologie
- Vaccin mais 250 millions de porteurs chroniques dans le monde- 280 000 porteurs chroniques en France (INVS)- 45% ignorent leur statut- 1 300 décès par an en France- 60 000 avec hépatite chronique active- Environ 15 000 patients traités

VIROLOGIE

• FAMILLE : Hepadnaviridae, seul représentant humain
•VIRUS RESISTANT :- 7 jours dans l’environnement- pendant 5 mn à 100°C, 10 h à 60°C- à la congélation.
LE VIRUS DE L ’HEPATITE B

S small surface protein
M middle surface protein
L large surface protein
core capsid protein
HBeAg secreted e antigen
pol polymerase
HBx X protein (non-secreted)
v
v
v
spherefilament
Dane particle
HBeAg
HBsAg
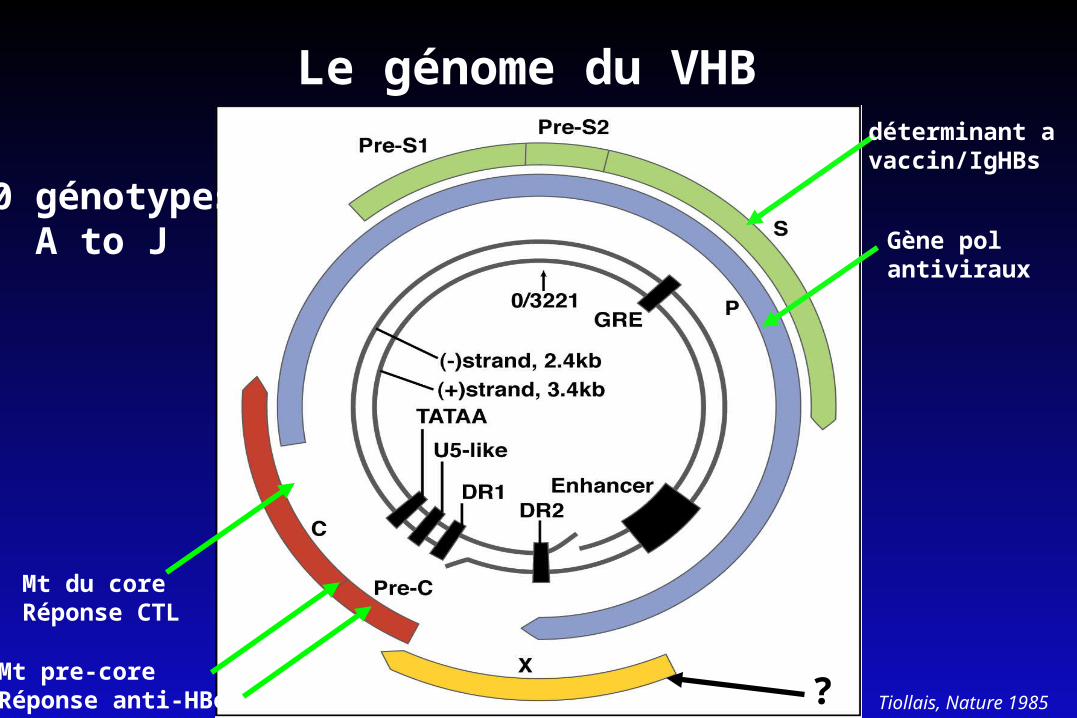
Le génome du VHB
Tiollais, Nature 1985
déterminant avaccin/IgHBs
Gène pol antiviraux
Mt pre-coreRéponse anti-HBe ?
Mt du coreRéponse CTL
10 génotypesA to J

Le cycle de réplication virale
Zoulim & Locarnini, Gastroenterology 2009
hNTCP

Model for sodium-dependent taurocholic cotransporting polypeptide (NTCP) binding to preS1
Seeger C , and Mason W S Gut 2013 in press; Yan H, et al. eLife 2012;1:e00049; Hu NJ, et al. Nature 2011;478:408–11.
• Sodium-dependent transporter for taurocholic acid • Expressed at the basolateral membrane of hepatocytes• Mediates the transport of conjugated bile acids • 349 amino acid-long glycosylated transmembrane protein. • Expression controlled by hepatocyte-specific transcription
factors, including HNF3 and C/EBP

Model for sodium-dependent taurocholic cotransporting polypeptide (NTCP) binding to preS1
Seeger C , and Mason W S Gut 2013 in press; Yan H, et al. eLife 2012;1:e00049; Hu NJ, et al. Nature 2011;478:408–11.

Transgenic miceHumanized mice
HumanChimpanzeeGibbonbaboons
Tupaïa
Woolley monkey
Ground squirrel
American woodchuck
Pekin DuckGrey Heron
Summers PNAS 1978, Mason J Virol 1981, Chisari Science 1985, Petersen PNAS 1998, Lanford PNAS 1998
The animal models of HBV infection

Cell culture models for HBV infection
Zeisel M et al, Gut 2015
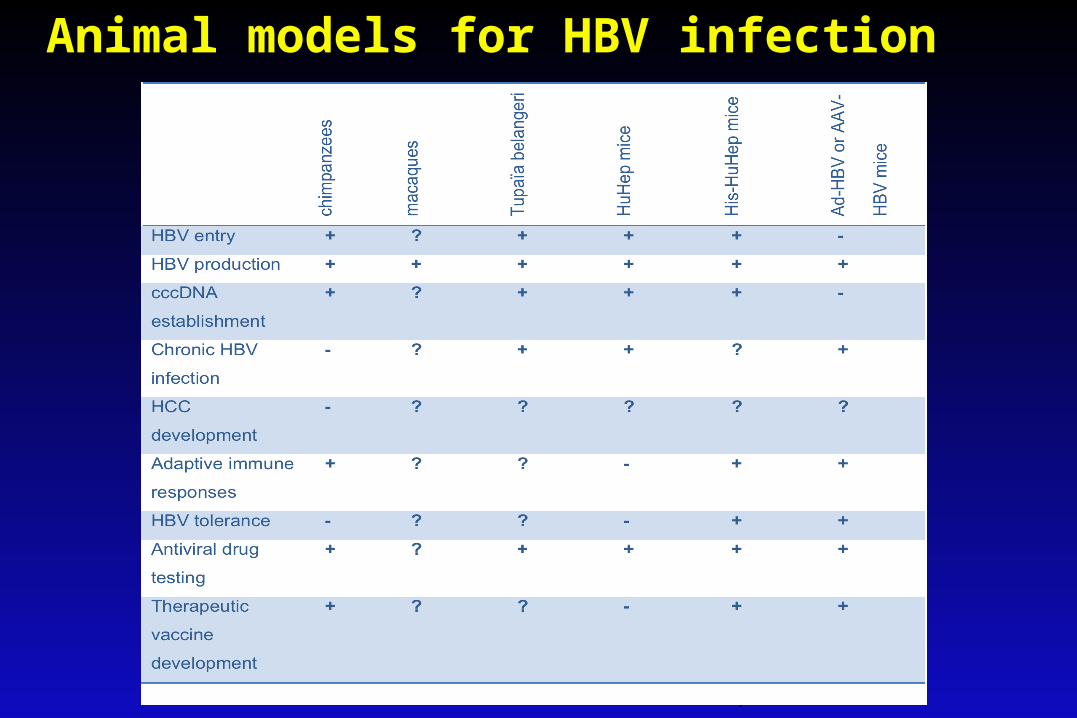
Animal models for HBV infection
Zeisel M et al , Gut 2015

Infection à VHB et risque de CHC
• Etude de Beasley à Taiwan– risque relatif = 100 chez les porteurs de l'AgHBs
• Etude de Tsukuma– risque cumumatif de CHC à 3 ans
• 12,5% chez 240 patients avec cirrhose• 3,8% chez 677 patients avec hépatite chronique
– risque x 7 si AgHBs +– risque X 4 si anti-HCV +
• Facteurs associés : alcool, tabac, aflatoxine• Diminution incidence avec la vaccination de masse (Chen,
NEJM 1995)
CARCINOME HEPATOCELLULAIRE ET VIRUS DE L'HEPATITE B
• Co-incidence de répartition géographique VHB / CHC• Porteurs AgHBs : RR x 100 pour le CHC• CHC dans les modèles animaux de l'hépatite B :
– marmotte– écureuil
• Présence d'ADN viral intégré dans les tumeurs

HBV replication and its role in HCC development
Wands, NEJM 2004

Role du VHB dans l’oncogénèse hépatique
VHBINFECTION CHRONIQUE
CARCINOGENESCO-FACTEURS
REACTION INFLAMMATOIRE CHRONIQUEREGENERATION HEPATIQUE
MUTAGENESE INSERTIONNELETRANSACTIVATION DE GENES CELLULAIRES
INTERACTIONS PROTEIQUESINACTIVATION DE GENES SUPPRESSEURS DE TUMEUR
CHC

PHYSIOPATHOLOGIE / IMMUNOPATHOLOGIE

HBV and the immune responses

Current model of HBV pathogenesis

IMMUNOPATHOLOGY OF HBV INFECTION
Immune tolerance
Clearance phaseChronic hepatitis
SeroconversionRemission
CD8+
HBV
CD8+ HBV
CD8+ HBV

Immunopathology
Fulminant hepatitis
CD8+
HBV

Hépatocyte infecté
HBV
Hépatocyte non infecté
Phase de « tolérance immunitaire »
MarqueursAgHBe +HBV DNA > 6 logALAT = NFoie = N
HBc/e Ag

Hépatocyte infecté
HBV
CD8
Fasperforine
Hépatocyte non infecté
Phase de clairance immune(hépatite chronique)
MarqueursAgHBe+HBV DNA > 2000 IU/mLALAT +++Foie: Hépatite chronique
HBc/e Ag
HLAI
cytokines
Hépatocyte infecté
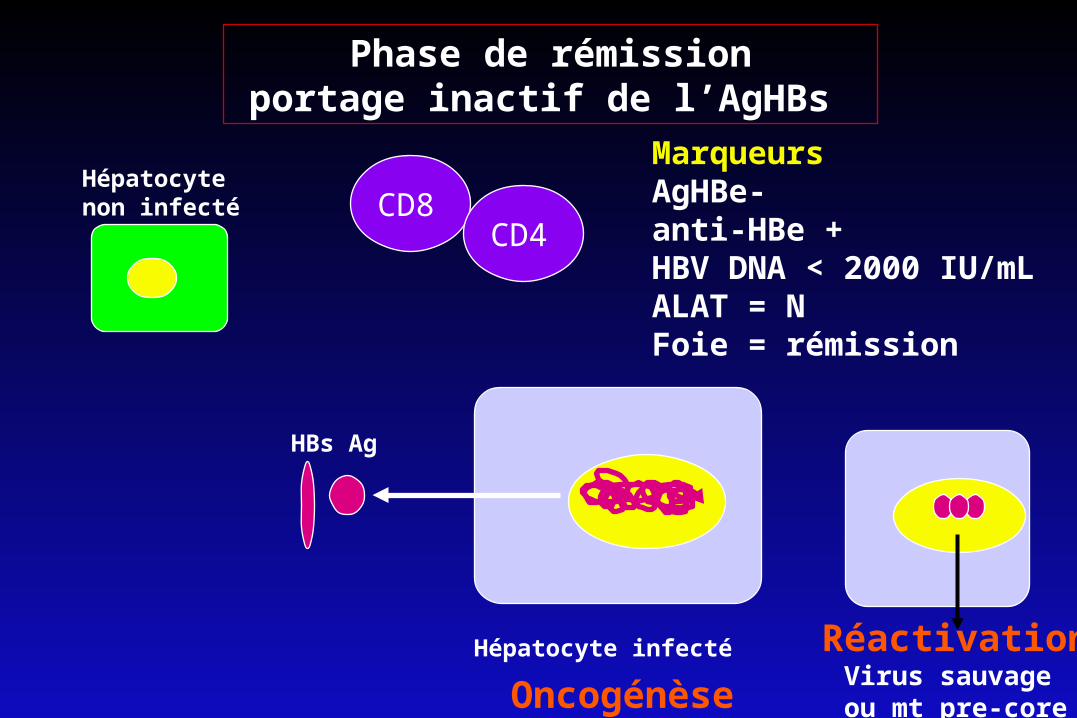
HBs Ag
Hépatocyte non infecté
MarqueursAgHBe-anti-HBe +HBV DNA < 2000 IU/mLALAT = NFoie = rémission
Phase de rémissionportage inactif de l’AgHBs
RéactivationVirus sauvage ou mt pre-coreOncogénèse
CD8CD4

Hépatocytes infectés
Hépatocytes non infectés
MarqueursHBsAg -
anti-HBc +Anti-HBs +/-
PCR sérum (-) / foie (+)
Clairance de l’AgHBs
Mutants d’échappementInfections occultesOncogénèse
CD8CD4
B

cccD
NA
(cop
ies/
cell)
Tota
l HB
V D
NA
(cop
ies/
cell)
cccDNA levels in the different phases of chronic HBV infection
• HBeAg+ patients had significantly higher cccDNA (90-fold) and total HBV DNA (147- fold) levels compared to HBeAg- patients. (p<0.001, Wilcoxon tests)
HBeAg+ (63)
Inact. Carrie
rs (10)
HBSAg- (7)
HBeAg- (18)
HBeAg+ (63)
Inact. Carrie
rs (10)
HBSAg- (7)
HBeAg- (18)
Werle et al, Gastroenterology 2004

Inactive HBV carrier● Not virologically inactive:
– low levels of viremia– episomal HBV DNA in the liver
LOW-REPLICATIVE STATE HIGH-REPLICATIVE STATE– spontaneously
– during immunosuppression
Low-replicative or latent infectionEpigenetic control
Histones
CBPPCAFp300
CBPPCAF
p300Sirt1
Sirt1HDAC1HDAC1
Histones
Pollicino et al., Gastroenterology 2006
Pollicino et al. Gastroenteroplogy 2006Levrero et al. J Hepatol, 2009
HISTOIRE NATURELLE ET VIROLOGIE CLINIQUE

Histoire Naturelle de l’hépatite BInfection aigue
Infection chronique
Tolérance immunitaire
Hépatite chroniquePortage inactif
Guérison5% nx-nés90% adultes
Virus sauvage (HBeAg+) Mutant pre-core (HBeAg-)
Cirrhose
Carcinome hépatocellulaire
Réactivation
30-50 ans
Seeger, Zoulim, Mason; Fields Virology; 2007
Seeger, Zoulim, Mason – Fields Virology 2007-2013

HEPATITE B AIGUE• Incubation 1 à 6 mois• Le plus souvent asymptomatique
– Évolution plus fréquente vers la chronicité• Prodromes:
– Maladie sérique : arthralgies, urticaire, acrodermatite etc. ..
• Formes ictériques : + graves que VHA et VHC– Durée de l’ictère : jusqu’à 4 mois
• Evolution : chronicité 5 à 10%• Hépatites fulminantes

Laboratory Diagnosis of Acute Hepatitis B
ALT
HBsAg
HBeAg
HBV DNA
Normal
Months After Exposure
ALT
and
HB
V D
NA
IU/L
and
mill
ion
copi
es/m
l
Symptoms
Anti-HBs AbAnti-HBe Ab
IgM anti-HBc
Total anti-HBc
Seeger, Zoulim, Mason, Fields Virology 2007

ALT
HBsAg
HBeAg
HBV DNA
Normal
Months After Exposure
ALT
and
HB
V D
NA
IU/ L
or m
il lio
n co
pies
/ml
Laboratory Diagnosis of Chronic Hepatitis B associated with wild type virus infection
Seeger, Zoulim, Mason, Fields Virology 2007

ALT
``HBsAg
HBeAg
HBV DNA
Normal
Months After Exposure
ALT
and
HB
V D
NA
IU/L
and
mill
ion
copi
es/m
l
Anti-HBe
Laboratory Diagnosis of Transition of Chronic Hepatitis B to The inactive Carrier State
0
100
200
300
400
500
600
700
800
0 1 2 3 4 5 6 12 24 36 48 60 72 80 92 104
Seeger, Zoulim, Mason, Fields Virology 2007

ALT
HBsAg
HBV DNA
Normal ALT levels
Months
ALT
and
HB
V D
NA
IU/L
and
mill
ion
copi
es/m
l Anti-HBeHBeAg
Laboratory Diagnosis of HBeAg negative Chronic Hepatitis B
Seeger, Zoulim, Mason, Fields Virology 2007

HBeAg(+) HBeAg(-) / anti-HBe(+)
ALAT
HBV DNA
Minimal CH Moderate to severe CH Moderate to severe CHRemission
Cirrhosis
Immunotolerantphase
Immuno-activephase
Inactive phaseLow replication Reactivation phase
Cirrhosis
109-1012 IU/mL >2000-<109 IU/mL <2000 IU/mL >2000 IU/mL
Inactive cirrhosis
Adapted from Fattovich G. Sem Liver Dis. 2003
HBsAgOccult infection

Formes cliniques

MANIFESTATIONS EXTRAHEPATIQUES DU VHB
• PAN– Complexes immuns circulants HBs/anti-HBs– Dépots artères moyens et petit calibre– Traitement : plasmaphéreses, corticoides, antiviraux
(vidarabine / IFN / famciclovir / lamivudine)• Glomérulonéphrites• Cryoglobulinémies• Guillain-Barré• Myocardite

TRANSMISSION VERTICALE DU VHB
• mère AgHBe +– transmission : 90%
• mère anti-HBe +– transmission : 10-20%– VHB muté pré-C (-) : hépatites fulminantes
• chronicité chez l’enfant : 90%

PRESENTATION CLINIQUE• INFECTION PERI-NATALE
– ALT normales ou subnormales– ADN-VHB > 1000 pg/ml– histologie : lésions minimes
• INFECTION POST-NATALE– ALT élevées– ADN-VHB < 1000 pg/ml– histologie : hépatite modérée à sévère
• CARCINOME HEPATOCELLULAIRE : 30 ANS

Pathophysiologic Cascade of Chronic HBV Infection
HBV Replication(Measured by
Serum HBV DNA)
Liver Inflammation
Worsening Histology• Necroinflammation• Fibrosis• Cirrhosis
Disease Progression• Liver Failure• Liver Cancer• Transplant• Death
Adapted from: Lavanchy D. Journal of Viral Hepatitis, 2004, 11, 97–107. Chen JC, et al. JAMA. 2006;295:65-73. Iloeje U. H, et al. Gastroenterology. 2006;130:678-86.
ALT Elevation

Charge virale et incidence de la cirrhose
R.E.V.E.A.L. – HBV StudyAnnée de suivi
Inci
denc
e cu
mul
ativ
e de
ci
rrho
se
.2
.1
0 1 2 3 4 5 6 7 8 9 10 11 12 130
.4
.3
P <0.001
n=37741.0 x 106 n=6271.0-9.9x105 n=3441.0-9.9x104 n=649300-9.9x103 n=1210<300 n=944
5.2%6.3%
10.0%
23.0%
37.1%
Iloeje UH et al. Gastroenterology 2006; 130: 678-686

Charge virale et incidence du CHC
Chen et al; JAMA 2006

Relationship Between Persistent Viremia and HCC: Argument For Antiviral Therapy
• Persistent replication associated with greater risk of HCC• Decreased risk when viral replication declines
Chen, et al. JAMA 2006
Baseline HBV DNA, (copies/mL) < 104 105 105 105
Follow-up HBVDNA, copies/mL --- < 104 104 to <105 105
Adjusted RR (95% CI)
1.0(ref)
3.6(1.7-7.6)
6.9(3.4-13.8)
9.1(5.8-14.1)
P Value -- < 0.001 < 0.001 < .001
HC
C In
cide
nce
Rat
e Pe
r 100
,000
0
1473
5882
873010,108
2.0x103
4.0x103
6.0x1038.0x1031.0x104
1.2x104

Impact Clinique de la Variabilité du Génome Viral
VARIABILITE GENETIQUE DU VHB
• Multiplication virale» taux d'erreur de la transcriptase inverse
• Pression de sélection» réponse immunitaire cellulaire / humorale» antiviraux-> possibilité de variants d'échappement
• Conséquences cliniques» diagnostic sérologique» traitements antiviraux
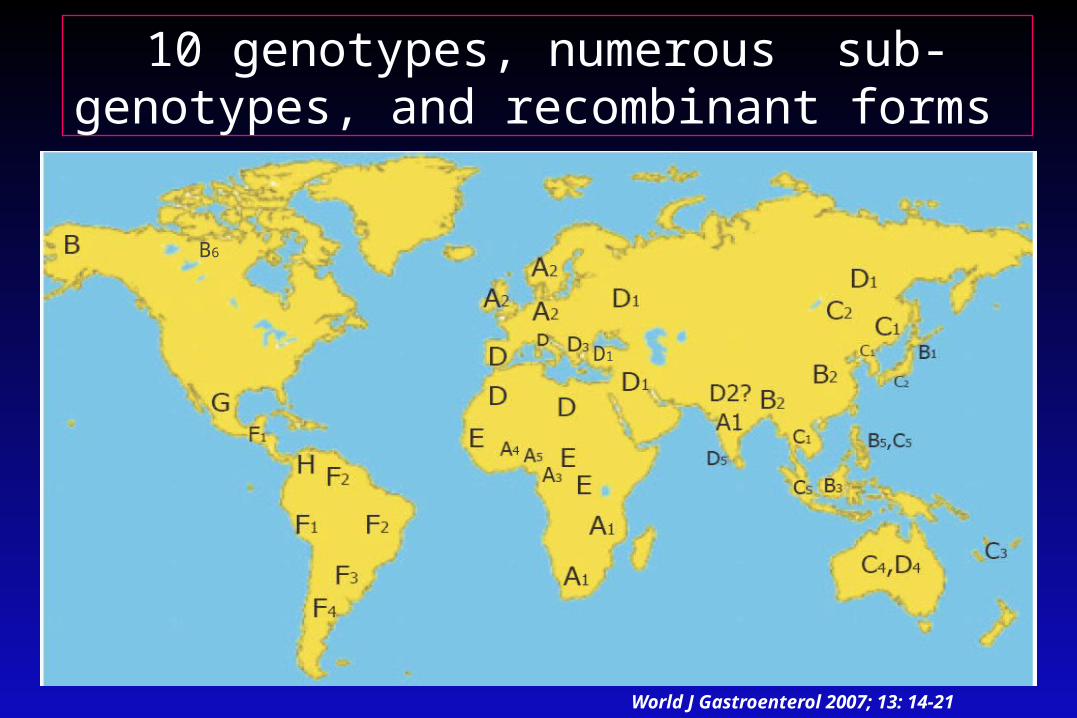
10 genotypes, numerous sub-genotypes, and recombinant forms
World J Gastroenterol 2007; 13: 14-21
B6
D1

Génotypes VHB chez les patients atteints d’hépatite chronique en France
Num
ber o
f sub
ject
s
F GA B C D E0
10
20
30
40
50
60
70
80
90100
30.2%
7.9%
12.5%
37.4%
11.3%
0.4 % 1.1%
Zoulim et al J Viral Hepatitis 2006

Impact du génotype sur la séroconversion Hbe/HBs
1 Janssen, Lancet 2005; 2 Flink, Am J Gastro 2006
PEG-IFN a-2bHBeAg Loss 1
0
10
20
30
40
50
A n=90
28%
47%44%
25%
Bn=23
C n=39
D n=103
Perc
enta
ge o
f pat
ient
s (%
)
HBV genotype
0
3
6
9
12
15
A n=90
5%
8%
0%
Bn=23
C n=39
D n=103
1815%
Perc
enta
ge o
f pat
ient
s (%
) 21
HBV genotype
PEG-IFN a-2bHBsAg Loss 2

LES MUTANTS DU GÉNOME DU VHB
déterminant avaccin/HBIg
polyméraseantiviraux
Mt pré-coreRéponse anti-e ?
Mt coreRéponse CTL

ROLE DE LA RÉGION PRÉ-C ET DE L’AgHBe
• Non nécessaire à la réplication du VHB– Culture cellulaire– Modèles in vivo
• Marmotte• Canard
• Modulation de la réponse immune– Tolérogène : souris transgéniques– Cible de la réponse anti-capside
Chang et al, J. Virol 1987; Schlicht et al J. Virol 1987; Chen J. Virol 1992; Millich et al PNAS

LES MUTANTS PRÉ-C (-)• codon stop / région pré-C
TGG -> TAG en pos. 1896
– génotypes B à E (A : exceptionnel)
– arrêt traduction protéine pré-C/C
– AgHBe négatif
• mutation dans promoteur pré-C
TTAAAGG -> TTAATGA en pos. 1762 /1764
– génotypes A à E
– transcrits pré-C/C :
– synthèse d'AgHBe :
Carman et al Lancet 1989, Okamoto et al J Virol 1990/1994, Tong et al Virology 1990

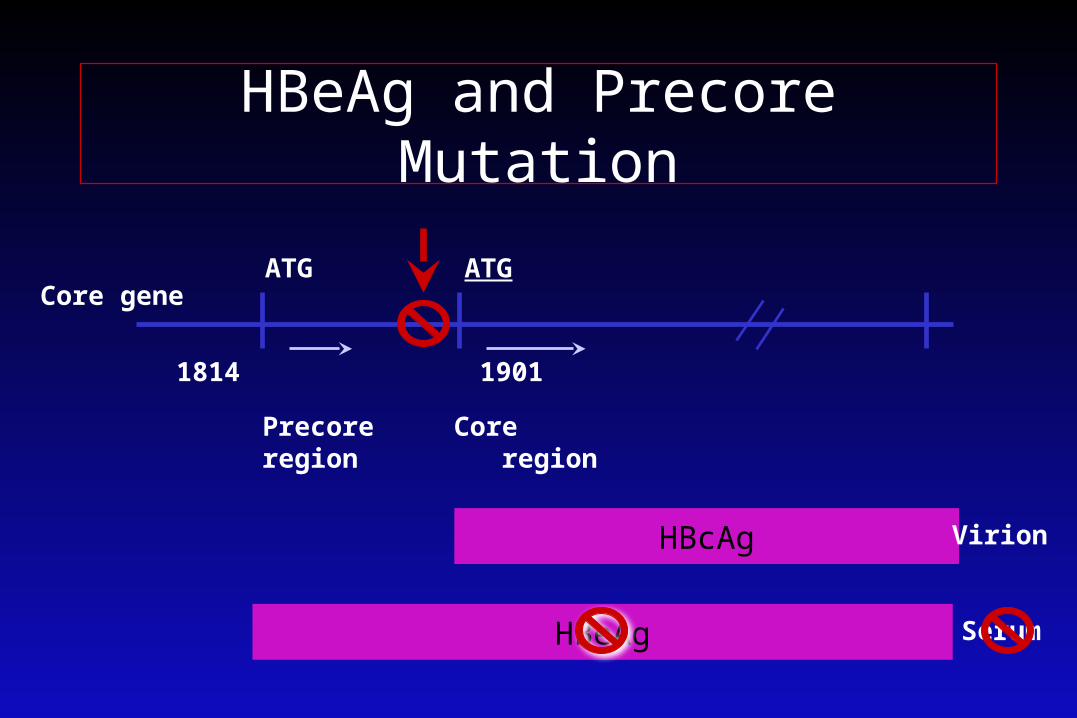
HBeAg and Precore Mutation
1814 1901
Precore Coreregion region
HBcAg
HBeAg
G 1896A = stop codon, TAG
ATG ATG
Virion
Serum
Core gene
HBeAg and Precore Mutation
1814 1901
Precore Coreregion region
HBcAg
HBeAg
ATG ATG
Virion
Serum
Core gene

VARIANTS NÉGATIFS POUR L ’AgHBe
mRNA
Protéinepré-C/C
PRE-C CPROMOTEUR
TAG***
1762-1764 1896
arrêt des synthèses protéiques
Diminution de l’expression de l ’AgHBe

Sélection des mutants pré-core au cours de l’histoire naturelle de l’hépatite B chronique
ALAT
ADN-VHB
AgHBe Anti-HBe
sauvage
Mt pré-C
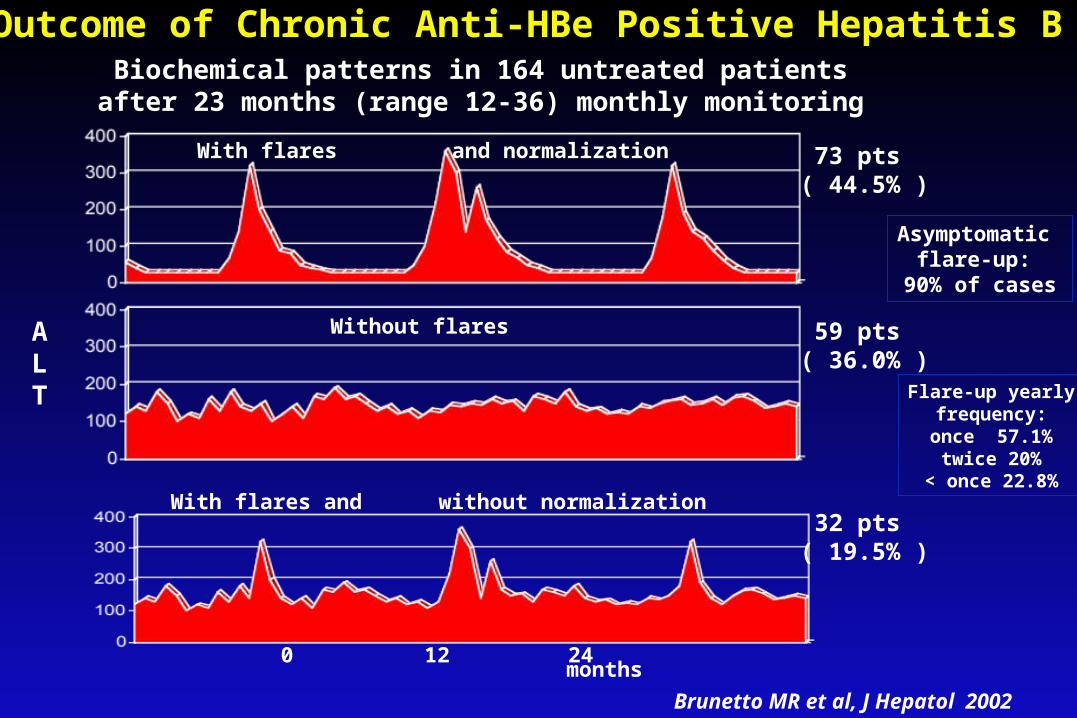
Outcome of Chronic Anti-HBe Positive Hepatitis BBiochemical patterns in 164 untreated patients
after 23 months (range 12-36) monthly monitoring
0 12 24months
With flares and normalization
Without flares
With flares and without normalization
73 pts ( 44.5% )
59 pts ( 36.0% )
32 pts ( 19.5% )
Asymptomatic flare-up:
90% of cases
ALT Flare-up yearly
frequency:once 57.1%twice 20%
< once 22.8%
Brunetto MR et al, J Hepatol 2002

DIAGNOSTICS DIFFICILES
I. Porteur inactifII. Exacerbation
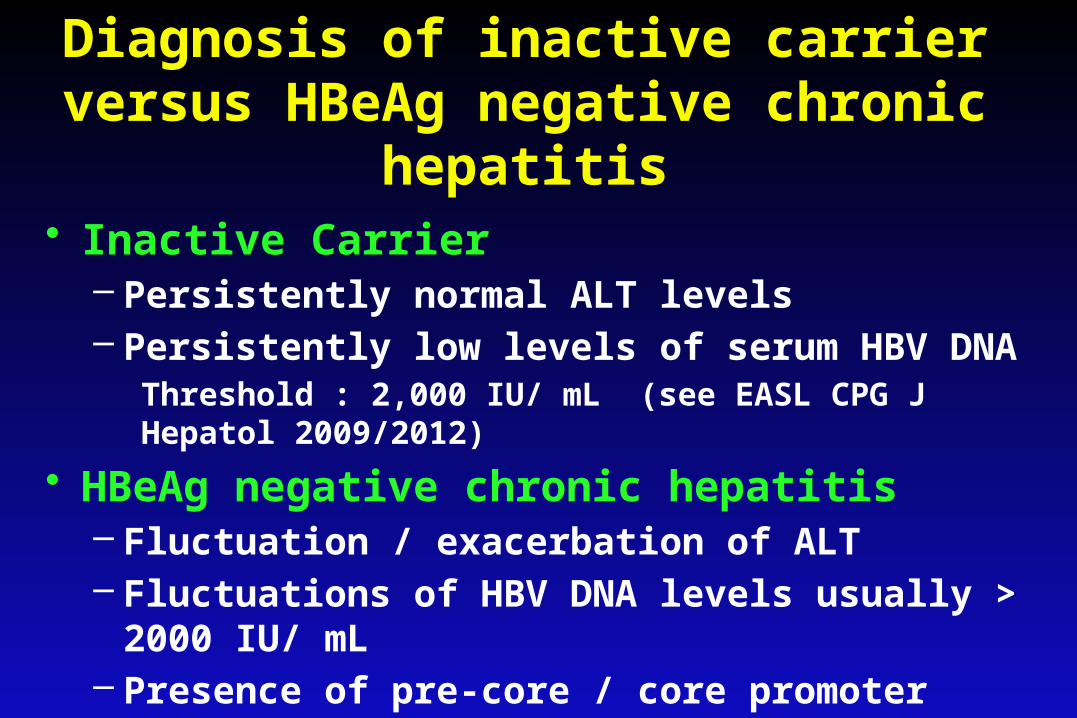
Diagnosis of inactive carrier versus HBeAg negative chronic hepatitis
• Inactive Carrier– Persistently normal ALT levels– Persistently low levels of serum HBV DNA
Threshold : 2,000 IU/ mL (see EASL CPG J Hepatol 2009/2012)• HBeAg negative chronic hepatitis
– Fluctuation / exacerbation of ALT– Fluctuations of HBV DNA levels usually > 2000 IU/ mL– Presence of pre-core / core promoter mutations

DIAGNOSTIC D'UNE EXACERBATION AIGUE SUR HEPATITE B CHRONIQUE
• Définition : poussée cytolytique≠ réactivation virale
• Ag HBe + initialement– rupture de tolérance immunitaire– séroconversion anti-HBe– très fréquent chez patients asiatiques
• Anti-HBe + initialement– réactivation virus sauvage : -> AgHBe +– réactivation virus muté pré-C (-)– Corticothérapie, biothérapie, chimiothérapie– surinfection delta / VHC

COOH
137149107
99 NH2
S - S
S - S S - SS- S
S-S
138139
147
Tiollais P. et al., Nature 1985. Torresi J., J. Clin Virol 2002; Dryden KA. et al., Mol Cell 2006
« a » determinant
HBs Ag
« a » determinant induces the synthesis of anti-HBs neutralizing antibodies
sG145R
sP120T
sD144H/A/E
PreS1 PreS2
SPol
Pré-C
C
Brin(+) 2,4kb
Brin(-) 3,2kb
X
TATAAU5-like
DR1DR2
Enh1Enh2
GRE0/322
1
SHBs (S)MHBs (preS2+S)LHBs (preS2+preS2+S)

Variants de l'Ag HBs
• échappement à la réponse humorale anti-HBs– naturelle– vaccination (transmission mère-enfant)– immunoprophylaxie (transplantation
hépatique)• infection active malgré Ac anti-HBs• sérologie AgHBs faussement négative
Risques : transmission virale + infections occultes

VARIANTS DE L'AgHBs
• Mutations ponctuelles dans le déterminant a de l'AgHBs (124-147)– aa 145 : Gly -> Arg – aa 126 : Ile -> Ser / Thr -> Asn
• transmission mère-enfant malgré la serovaccination (3%)
• infection du greffon hépatique malgré Immunoglobulines anti-HBs
• hépatites chroniques avec anti-HBc et anti-HBs +
Presence of HBV DNA in the liver ( serum) of
individuals testing HBsAg negative by currently
available assays
Occult HBV Infection (OBI)
Raimondo et al, J Hepatol 2008

Reported Prevalence of Occult HBV Infection in HIV Positive Patients
Study Country N° ofpatients
Occult HBV
N° (%)Methods
Hofer, 1998 Switzerland 57 51 (89%) “nested” PCR(serial evaluation)
Torres-Baranda, 2006 Mexico 35 7 (20%) “nested” PCR
Filippini, 2006 Italy 86 17 (20%) single step PCR
Mphahlele, 2006 South Africa 140 31 (22.%) “nested” PCR
Pogany, 2005 Netherlands 93 4 (4%) single step PCR
Neau, 2005 France 160 1 (0.6%)
Santos, 2003 Brazil 101 16 (16%) single step PCR
Wagner, 2004 France 30 11 (37%) “nested” PCR
Goncales, 2003 Brazil 159 8 (5%) “nested” PCR
Nunez, 2002 Spain 85 0 Cobas Amplicor HBV Monitor (Roche)
Piroth, 2000 France 37 13 (35%) single step PCR
Raffa, 2007 Italy “nested” PCR (liver)
Cobas Amplicor HBV Monitor (Roche)
101 42 (41%)
Raimondo et al, J Hepaol 2007, modified
OBI
Cause(s) for the failure of HBsAg detection
Suppression ofHBV replication and
gene expression
Infection byS gene Variants
“false” OBI

Occult HBV infection
HBV cccDNA Integrated HBV DNA
HBV mutants Epigenetic control
HBV replication
Immune surveillanceViral co-infections
Related Documents











