NORTHWEST PORTLAND AREA INDIAN HEALTH BOARD Burns –Paiute Tribe Chehalis Tribe Coeur d’Alene Tribe Colville Tribe Coos, Suislaw & Lower Umpqua Tribe Coquille Tribe Cow Creek Tribe Cowlitz Tribe Grand Ronde Tribe Hoh Tribe Jamestown S’Klallam Tribe Kalispel Tribe Klamath Tribe Kootenai Tribe Lower Elwha Tribe Lummi Tribe Makah Tribe Muckleshoot Tribe Nez Perce Tribe Nisqually Tribe Nooksack Tribe NW Band of Shoshoni Tribe Port Gamble S’Klallam Tribe Puyallup Tribe Quileute Tribe Quinault Tribe Samish Indian Nation Sauk-Suiattle Tribe Shoalwater Bay Tribe Shoshone-Bannock Tribe Siletz Tribe Skokomish Tribe Snoqualmie Tribe Spokane Tribe Squaxin Island Tribe Stillaguamish Tribe Suquamish Tribe Swinomish Tribe Tulalip Tribe Umatilla Tribe Upper Skagit Tribe Warm Springs Tribe Yakama Nation 2121 SW Broadway Suite 300 Portland, OR 97201 Phone: (503) 228-4185 Fax: (503) 228-8182 www.npaihb.org December 1, 2015 Zero Suicide Model Training for NW IHS/Tribal Clinics The Northwest Portland Area Indian Health Board’s THRIVE project (Tribal Health: Reaching out InVolves Everyone) works to improve the capacity of tribal health programs to track, prevent, and treat suicide. In support of this goal, THRIVE is recruiting three IHS/Tribal Clinics to support their implementation of the Zero Suicide (ZS) Model. NW IHS/Tribal Clinics can request a 1-2 day Zero Suicide Model (ZS) training to be organized by THRIVE, which will take place at the Tribes’ clinic in 2016 (January – July). These trainings will be funded by the Methamphetamine and Suicide Prevention Initiative (MSPI – grant no. BH16IHS0016-01-00) from the Indian Health Service (IHS). ZS is a promising practice recognized by the 2012 National Strategy for Suicide Prevention (NSSP), which helps communities create systems-wide change to improve the identification of those at risk of suicide, and the quality of treatment services. Being versed in ZS can help clinics build the tools and support needed to adopt approaches that can dramatically reduce suicide among those served by the clinic. This is a model that helps coordinate care across the care continuum, from a phone call or referral to the actual appointment where the patient is seen. Coordinated care keeps suicidal persons from falling through the cracks in the healthcare system. The attached ZS document contains more information about the ZS Model. Tribes and tribal organizations who request this training will need to meet several eligibility requirements before submitting the Training Request Form. The trainings will be fulfilled on a first come, first served basis, as long as the eligibility requirements are met. Eligibility Tribes or tribal organizations with existing Meth and Suicide Prevention Initiative (MSPI), SAMHSA suicide prevention grants, or who are already implementing the ZS Model are not eligible to apply. Timeframe The clinic’s scope of work should be completed within 12 months of the 1-2 day ZS Training.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

NORTHWEST
PORTLAND
AREA
INDIAN
HEALTH
BOARD
Burns –Paiute Tribe
Chehalis Tribe
Coeur d’Alene Tribe
Colville Tribe
Coos, Suislaw &
Lower Umpqua Tribe
Coquille Tribe
Cow Creek Tribe
Cowlitz Tribe
Grand Ronde Tribe
Hoh Tribe
Jamestown S’Klallam Tribe
Kalispel Tribe
Klamath Tribe
Kootenai Tribe
Lower Elwha Tribe
Lummi Tribe
Makah Tribe
Muckleshoot Tribe
Nez Perce Tribe
Nisqually Tribe
Nooksack Tribe
NW Band of Shoshoni Tribe
Port Gamble S’Klallam Tribe
Puyallup Tribe
Quileute Tribe
Quinault Tribe
Samish Indian Nation
Sauk-Suiattle Tribe
Shoalwater Bay Tribe
Shoshone-Bannock Tribe
Siletz Tribe
Skokomish Tribe
Snoqualmie Tribe
Spokane Tribe
Squaxin Island Tribe
Stillaguamish Tribe
Suquamish Tribe
Swinomish Tribe
Tulalip Tribe
Umatilla Tribe
Upper Skagit Tribe
Warm Springs Tribe
Yakama Nation
2121 SW Broadway
Suite 300
Portland, OR 97201
Phone: (503) 228-4185
Fax: (503) 228-8182
www.npaihb.org
December 1, 2015
Zero Suicide Model Training for NW IHS/Tribal Clinics
The Northwest Portland Area Indian Health Board’s THRIVE project (Tribal
Health: Reaching out InVolves Everyone) works to improve the capacity of tribal
health programs to track, prevent, and treat suicide.
In support of this goal, THRIVE is recruiting three IHS/Tribal Clinics to support
their implementation of the Zero Suicide (ZS) Model. NW IHS/Tribal Clinics
can request a 1-2 day Zero Suicide Model (ZS) training to be organized by
THRIVE, which will take place at the Tribes’ clinic in 2016 (January – July).
These trainings will be funded by the Methamphetamine and Suicide Prevention
Initiative (MSPI – grant no. BH16IHS0016-01-00) from the Indian Health Service
(IHS).
ZS is a promising practice recognized by the 2012 National Strategy for Suicide
Prevention (NSSP), which helps communities create systems-wide change to
improve the identification of those at risk of suicide, and the quality of treatment
services. Being versed in ZS can help clinics build the tools and support needed to
adopt approaches that can dramatically reduce suicide among those served by the
clinic. This is a model that helps coordinate care across the care continuum, from
a phone call or referral to the actual appointment where the patient is seen.
Coordinated care keeps suicidal persons from falling through the cracks in the
healthcare system. The attached ZS document contains more information about
the ZS Model.
Tribes and tribal organizations who request this training will need to meet several
eligibility requirements before submitting the Training Request Form. The
trainings will be fulfilled on a first come, first served basis, as long as the
eligibility requirements are met.
Eligibility
Tribes or tribal organizations with existing Meth and Suicide Prevention
Initiative (MSPI), SAMHSA suicide prevention grants, or who are already
implementing the ZS Model are not eligible to apply.
Timeframe
The clinic’s scope of work should be completed within 12 months of the 1-2
day ZS Training.

Before submitting the Training Request Form:
Review the ZS toolkit online: http://zerosuicide.sprc.org/toolkit
Watch the recorded webinar - The Emerging Zero Suicide Paradigm:
http://zerosuicide.sprc.org/about
Obtain written approval from the Tribal Health Director and the Behavioral Health Director.
Select a primary contact person who will schedule the ZS training, facilitate a local
implementation team, and participate in monthly technical assistance calls with THRIVE
staff for 12 months following the ZS training.
To support implementation of the Zero Suicide Model, THRIVE will provide:
A free 1-2 day training at your clinic with a certified trainer (Dr. Ursula Whiteside).
Implementation team planning tools and templates.
Analysis and compilation of a local Workforce Survey Report.
Monthly technical assistance (or as requested by the clinic).
One follow-up conference call with THRIVE and Dr. Whiteside approximately 1-3 months
following the training.
$2,000 per site to host a ZS community kickoff event.
To support implementation, the IHS/Tribal Clinic will:
Complete the enclosed Organizational Self-Study with at least 3 clinic staff who would be
leaders in the ZS effort, including clinic decision-makers.
Circulate and return the enclosed Workforce Survey. The survey must be completed by at
least 75% of the medical and behavioral health workforce, including janitorial staff, medical
records, finance staff, etc. This step must be completed before the ZS Training can take
place.
Select dates (1-2 days) and a location for the ZS training. (Unfortunately, THRIVE’s grant
dollars cannot pay for meals, just light refreshments.) Ensure at least 15 clinic staff attend
the 1-2 day training. Decision-makers are important to the implementation process, and
should be present at the training if possible.
Create a local ZS Implementation Plan at the first implementation team meeting after the ZS
training. A template will be provided by THRIVE staff.
Host a ZS community kickoff event to get your community (and partnering programs)
excited about the ZS model and your clinic’s services. The implementation team will be
encouraged to announce the ZS initiative in their tribal paper.
Review and/or update the clinic’s current crisis response protocol, particularly surrounding
suicide and suicide attempts.

Agree to implement the ZS Model for at least one full year, through an active implementation
team that meets at least once a month. This will require using your clinic’s EHR and quality
improvement initiatives to achieve system-wide change.
Distribute THRIVE’s social marketing campaign: We Are Connected. We Need You Here.
Participate in 2 regional Tribal Zero Suicide virtual meetings or conference calls, to support
cross-site sharing and learning.
Optional: Host at least one additional suicide prevention training (i.e. QPR, ASIST,
safeTALK, etc.) for clinic staff and community members. THRIVE can support the cost of
QPR or ASIST participant booklets, and can facilitate the training if scheduled in advance.
(Unfortunately THRIVE cannot cover the cost of outside trainers.)
Please contact the THRIVE project manager, Colbie Caughlan, at [email protected] or
503.416.3284 if you plan to submit a request for the ZS Training or if you have any questions
about the application process.
Applications must be completed and submitted to the project manager by fax
(503.228.4801) or email ([email protected]) by January 22, 2016. We will continually
take applications until the three clinics have been identified. Please contact Colbie if you
would like to turn in your request after the January 22 due date.
Respectfully,
Colbie Caughlan, Stephanie Craig Rushing, Celena McCray
THRIVE Staff

THRIVE - Zero Suicide Model Training Request
Tribe:
Primary Contact:
Address, City, State, & Zip:
Email:
Phone Number:
Alternate contact name, number, and email:
Please answer the following questions. (All three must be NO to be eligible to apply)
Does your Tribe or IHS/Tribal Clinic currently having funding through the Meth & Suicide Prevention Initiative or a SAMHSA suicide prevention grant?
Circle one: Yes No
Has your Tribe or IHS/Tribal Clinic staff ever attended a Zero Suicide Academy?
Circle one: Yes No
Is your Tribe or IHS/Tribal Clinic currently implementing the Zero Suicide Model?
Circle one: Yes No
Please check those steps that your clinic has completed:
Reviewed the ZS toolkit online: http://zerosuicide.sprc.org/toolkit
Watched the recorded webinar - The Emerging Zero Suicide Paradigm:
http://zerosuicide.sprc.org/about
Obtained written approval from the Tribal Health Director and the Behavioral Health Director.
Selected a primary contact person who will schedule the ZS training, facilitate a local
implementation team, and participate in monthly technical assistance calls with THRIVE staff for 12
months following the 1-2 day ZS training.

Check this box to indicate that you agree to fulfill the following activities:
Complete the enclosed Organizational Self-Study with at least 3 clinic staff who would be
leaders in the ZS effort, including clinic decision-makers.
Circulate and return the enclosed Workforce Survey. This survey must be completed by at least
75% of the medical and behavioral workforce, including janitorial staff, medical records, finance
staff, etc. This step must be completed before the ZS Training can take place.
Select dates (1-2 days) and a location for the ZS training. (Unfortunately, THRIVE’s grant dollars
cannot pay for meals, just light refreshments.) Ensure at least 15 clinic staff attend the 1-2 day
training. Decision-makers are important to the implementation process, and should be present
at the training if at all possible.
Host a ZS community kickoff event to get your community excited about the program and your
clinic’s services. The implementation team will be encouraged to announce the ZS initiative in
their tribal paper.
Create a local ZS Implementation Plan at the first implementation team meeting after the ZS
training. A template will be provided by THRIVE staff.
Review and/or update the clinic’s current crisis response protocol, particularly surrounding
suicide and suicide attempts.
Agree to implement the ZS Model for at least one full year, through an active implementation
team that meets at least once a month. This will require using your clinic’s EHR and quality
improvement initiatives to achieve system-wide change.
Distribute THRIVE’s social marketing campaign: We Are Connected. We Need You Here.
Participate in 2 regional Tribal Zero Suicide virtual meetings or conference calls, to support
cross-site sharing and learning.
Optional - Host at least one additional suicide prevention training (i.e. QPR, ASIST, safeTALK,
etc.) for staff and community members by September 29, 2016.

Why does your clinic want to take on the Zero Suicide Model?
Briefly describe what changes your crisis response protocols/policies will need in the upcoming year, and how your ZS implementation team will be poised to achieve them.

Please have the Tribal Health Director and/or Behavioral Health Director (or equivalent) sign in the box and submit with your application. This signature indicates that your Tribe and IHS/Tribal Clinic are in support of the ZS implementation process and are committed to the time and energy that are needed to put this model into action. This process can be time intensive, and can ebb and flow based on the local plan and workforce implementing it. THRIVE staff will provide as much technical assistance as we can. This also indicates your understanding that the funds provided will only cover the costs of the ZS training and trainer; it will not cover your staff’s time.
In exchange for this subcontract, (Tribal Clinic Name) _______________________________ agrees to implement the Zero Suicide Model for at least one year following the provided training. The preferred month for the training is: ____________________ 2016. Primary Contact’s Signature: _____________________________________________________________ Printed Name & Date: __________________________________________________________________ Tribal Health Director Signature: _________________________________________________________ Printed Name & Date: __________________________________________________________________ Behavioral Health Director Signature (optional but preferred):___________________________________ Printed Name & Date: __________________________________________________________________
Requests must be completed and submitted to the project manager by fax (503.228.4801) or email ([email protected]) by January 22, 2016

Its core propositions are that suicide deaths for people under care are preventable,
and that the bold goal of zero suicides among persons receiving care is an aspirational
challenge that health systems should accept. The Zero Suicide approach aims to improve
care and outcomes for individuals at risk of suicide in health care systems. It represents
a commitment to patient safety—the most fundamental responsibility of health care—
and also to the safety and support of clinical staff, who do the demanding work of
treating and supporting suicidal patients.
The challenge of Zero Suicide is not one to be borne solely by those providing clinical
care. Zero Suicide relies on a system-wide approach to improve outcomes and close
gaps rather than on the heroic efforts of individual practitioners. This initiative in health
care systems also requires the engagement of the broader community, especially suicide
attempt survivors, family members, policymakers, and researchers. Thus, Zero Suicide
is a call to relentlessly pursue a reduction in suicide for those who come to us for care.
The programmatic approach of Zero Suicide is based on the realization that suicidal
individuals often fall through multiple cracks in a fragmented and sometimes distracted
health care system, and on the premise that a systematic approach to quality improvement
is necessary. The approach builds on work done in several health care organizations,
including the Henry Ford Health System (HFHS) in Michigan. Like other leading health
care systems, HFHS applied a rigorous quality improvement process to problems
such as inpatient falls and medication errors. HFHS realized that mental and behavioral
health care could be similarly improved. This insight led to the development of HFHS’s
Perfect Depression Care model, a comprehensive approach that includes suicide
prevention as an explicit goal. The approach incorporates both best and promising
practices in quality improvement and evidence-based care and has demonstrated stunning
results—an 80 percent reduction in the suicide rate among health plan members.
www.zerosuicide.com
2.10.15
Education Development Center, Inc. ©2015 All Rights Reserved.Suicide Prevention Resource CenterSPRC
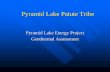
WHAT IS ZERO SUICIDE?Zero Suicide is a commitment to suicide prevention in health and behavioral health care systems, and also a specific set of tools and strategies. It is both a concept and a practice.
TRAIN
LEAD
IDENTIFY
ENGAGE
TREAT
TRANSITION
IMPROVE

Using these successful approaches as the basis for its
recommendations, the Clinical Care and Intervention
Task Force of the National Action Alliance for Suicide
Prevention identified essential elements of suicide
prevention for health care systems (i.e., health care
plans or care organizations serving a defined population
of consumers, such as behavioral health programs,
integrated delivery systems, and comprehensive primary
care programs). These elements include:
1 LEAD Create a leadership-driven, safety-oriented
culture committed to dramatically reducing suicide
among people under care. Include suicide attempt
and loss survivors in leadership and planning roles.
2 TRAIN Develop a competent, confident, and
caring workforce.
3 IDENTIFY Systematically identify and assess suicide
risk among people receiving care.
4 ENGAGE Ensure every person has a suicide care
management plan, or pathway to care, that is both
timely and adequate to meet his or her needs. Include
collaborative safety planning and restriction of lethal means.
5 TREAT Use effective, evidence-based treatments that
directly target suicidality.
6 TRANSITION Provide continuous contact and
support, especially after acute care.
7 IMPROVE Apply a data-driven quality improvement
approach to inform system changes that will lead to
improved patient outcomes and better care for those
at risk.
If we do not set big goals, we will never achieve them. In the
words of Thomas Priselac, president and CEO of Cedars-
Sinai Medical Center:
“It is critically important to design for zero even when
it may not be theoretically possible. When you design
for zero, you surface different ideas and approaches
that if you’re only designing for 90 percent may not
materialize. It’s about purposefully aiming for a higher
level of performance.”
Better performance and accountability for suicide prevention
and care should be core expectations of health care programs
and systems. While we do not yet have proof that suicide can
be eliminated in health systems, we do have strong evidence
that system-wide approaches are more effective.
To assist health and behavioral health plans and organizations,
the Suicide Prevention Resource Center (SPRC) offers an
evolving online toolkit that includes modules and resources
to address each of the elements listed above. SPRC also
provides technical assistance for organizations actively
implementing this approach.
Learn more at www.zerosuicide.com.
www.zerosuicide.com
FOR MORE INFORMATION, PLEASE CONTACT:
Julie Goldstein Grumet, PhD
Director of Prevention and Practice
Suicide Prevention Resource Center
Education Development Center, Inc.
1025 Thomas Jefferson Street, NW
Suite 700W
Washington, DC 20007
Phone: 202.572.3721
Email: [email protected]
Related Documents