YOLANDA ROSS, LBSW LEAH DAVIES, LMSW CENTRAL TEXAS AFRICAN AMERICAN FAMILY SUPPORT CONFERENCE MARCH 27, 2015 Prenatal Alcohol Exposure: Lifelong Impacts

YOLANDA ROSS, LBSW LEAH DAVIES, LMSW CENTRAL TEXAS AFRICAN AMERICAN FAMILY SUPPORT CONFERENCE MARCH 27, 2015 Prenatal Alcohol Exposure: Lifelong Impacts.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
YOLANDA ROSS, LBSWLEAH DAVIES, LMSW
CENTRAL TEXAS AFRICAN AMERICAN FAMILY SUPPORT CONFERENCE
MARCH 27 , 2015
Prenatal Alcohol Exposure:Lifelong Impacts

Welcome and Thank you for coming!
FASD
Pregnancy
Choice?
Addiction
Mental Health Disabilit
y
HealthAlcohol Development
Support
Knowledge
Yolanda’s Story

ALCOHOL USE AMONG PREGNANT WOMEN
Understanding FASD
Women and Alcohol
Studies show that women with alcoholism are up to twice as likely as men to die from alcohol-related causes such as suicide, accidents, and illnesses.
Alcohol becomes more highly concentrated in a woman’s body.
Women who drink heavily are more prone to liver disease, heart damage, and brain damage than men.
The code of silence around women and substance abuse and women is harming women and their babies.
The Numbers
1 in 13 pregnant women drink (CDC, 2012)
47% of Texas pregnancies are unintended (PRAMS, 2009) Approximately 68% for women aged 19 and younger
44.3 % of Texas women report drinking any alcohol before pregnancy (PRAMS, 2009)
5.7 % reported drinking any alcohol during the 3rd trimester
34% of pregnant adolescents (age 12-14) report using one or substance in past 30 days (Salas-Wright, 2015)
Most commonly used: Alcohol (16%)
Most likely to report alcohol use during pregnancy in 2012 CDC MMWR report:
White Between the ages of 35 and 44 College graduates Employed
Drinking while pregnant?
Women may be unaware that they are pregnant
Women may know other women who drank during pregnancy and who have children who appear outwardly to be healthy
Women may use alcohol to cope with difficult life situations such as: poverty, violence, isolation, despair or depression
Women may be struggling with addiction.
STIGMA

FASD is not about the face, it’s about the brain!
Wattendorf, D. MAJ, MC, USAF, and Muenke, M, National Human Genome Research Institute, National Institutes of Health, Bethesda, Maryland. Am Fam Physician. 2005 Jul 15;72(2):279-285.
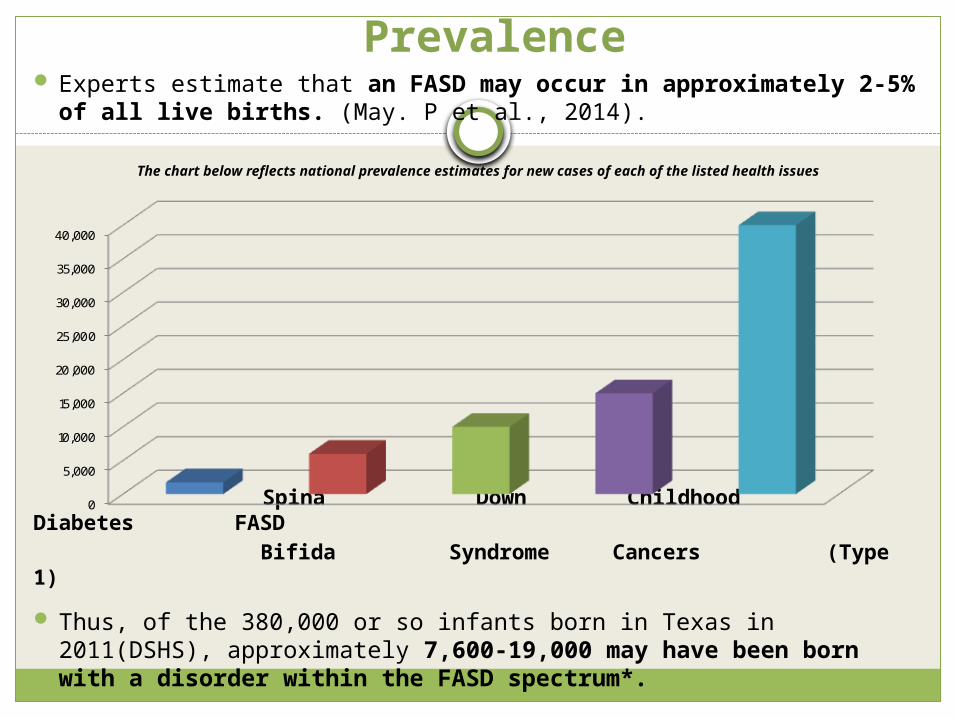
Prevalence Experts estimate that an FASD may occur in approximately 2-
5% of all live births. (May. P et al., 2014).
The chart below reflects national prevalence estimates for new cases of each of the listed health issues
Spina Down Childhood Diabetes FASD Bifida Syndrome Cancers (Type 1)
Thus, of the 380,000 or so infants born in Texas in 2011(DSHS), approximately 7,600-19,000 may have been born with a disorder within the FASD spectrum*.
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Characteristics of FASD Due to Brain Damage
Impaired executive function
Developmental delay
Mental Health Issues Attention deficits Increased stress
responseIncreased activity Sleep disturbances
Decreased visual focus
Decreased/increased response to noise or stimulation
Delayed speech development
Possible intellectual disability
Learning difficulties
FASD and well-being . . .
Oppositional Defiant Disorder (ODD)ADHD, ADDBipolar disorderIntermittent Explosive DisorderAutism Spectrum (including Asperger’s
Syndrome)Reactive Attachment DisorderTraumatic Brain InjuryAntisocial Personality DisorderConduct DisorderBorderline Personality DisorderDepression
Logic Model
Because FASD is a brain-based disability, seen mostly in behaviors . . .
Then providing accommodations for people with an FASD or other neurocognitive impairment is as
appropriate, effective and important as providing accommodations for people with other physical
disabilities

• PREVENTION
• INTERVENTION
So what should we do?

Prevention is key!
Screening
Brief Intervention(if positive)
Referral to Treatment(if necessary)


Shift in Thinking
From believing the individual with an FASD…
To understanding the individual possibly…
Won’t Can’t
Annoying Frustrated, challenged
Lies Fills in the blanks
Irritable Overstimulated
Trying to get attention Needs contact, support
Inappropriate Displays behaviors of a child, is developmentally younger
IS the problem HAS a problem
Adapted from Malbin, 2002
Developing Accommodations
Identify what was going on
just before
behavior = the need
Adapt teaching and/or
environment,carefully monitor progress
Ask: What can I do to help meet this child in his/her need?

So what works?Hannah’s experience
MHMRA of Harris CountyEarly Childhood Intervention (ECI)Pasadena Independent School District (PISD)NOFASUniversity of Washington The Council on Alcohol and Drugs Houston
(Cradles Project)K.I.N.D.E.R. Clinic through Memorial
Hermann Hospital (No longer in existence)No Place Like Here

Strategies for Success
Stable routineLimit (but provide,) choices and instructionCelebrate successes (even small ones)Teach social skills and emotionsProvide supports in school (to individual,
teachers, and classmates.)Repetition!ConsistencyUse concrete language and explanationsTeach self-advocacy
What doesn’t work
Rewards or punishments that will happen “in the future.”
Independence as a goal.
Viewing inability to follow through as a lack of motivation.
Zero Tolerance policies.
Approaches that rely heavily on verbal processing – like MI.
“We must move from viewing the individual as failing if s/he does not do well in a program to viewing the program as not providing what the individual needs in order to succeed.”
—Dubovsky, 2000
For more information
The Texas Office for Prevention of Developmental Disabilities http://www.topdd.state.tx.us Leah Davies: [email protected]
The CDC http://www.cdc.gov/ncbddd/fasd/index.html
The FASD Center for Excellence (SAMHSA) http://www.fasdcenter.samhsa.gov/
Questions/Thoughts
There is also no safe time during pregnancy to drink and no safe
kind of alcohol. We urge pregnant women not to drink alcohol at
any time during pregnancy.”
– Centers for Disease Control and Prevention, 2011
“There is no known safe amount of alcohol to drink while
pregnant.
“LIKE” US ON FACEBOOK
FOLLOW US ON TWITTER “TOPDD@PREVENT DD”
Thank you!
Related Documents











