Yair Edden, MD Department of Surgery Shaare-Zedek Medical Center The Hebrew University School of Medicine Jerusalem, Israel Sigmoid Diverticular Disease

Yair Edden , MD Department of Surgery Shaare-Zedek Medical Center
Jan 02, 2016
Sigmoid Diverticular Disease. Yair Edden , MD Department of Surgery Shaare-Zedek Medical Center The Hebrew University School of Medicine Jerusalem, Israel. Nomenclature. Diverticulum = sac-like protrusion of the colonic wall Diverticulosis = describes the presence of diverticuli - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Yair Edden, MD
Department of Surgery
Shaare-Zedek Medical Center
The Hebrew University School of Medicine
Jerusalem, Israel
Sigmoid Diverticular Disease

Nomenclature
• Diverticulum = sac-like protrusion of the colonic wall
• Diverticulosis = describes the presence of diverticuli
• Diverticulitis = inflammation of diverticuli

Nomenclature
• True Diverticulum = all layers of the GI wall (mucosa to serosa) e.g. Appendix, Meckel, Congenital
• False/Pseudo Diverticulum = Mucosa-submucosa herniates through the muscle layer (muscularis propria)
and then is only covered by serosa e.g. Acquired pathology

• Before the 20th century, diverticular disease was rare
• Prevalence has increased over time– 1907 First reported resection of complicated diverticulitis by Mayo– 1925 5-10%– 1969 35-50%
Epidemiology- Sigmoid diverticulosis
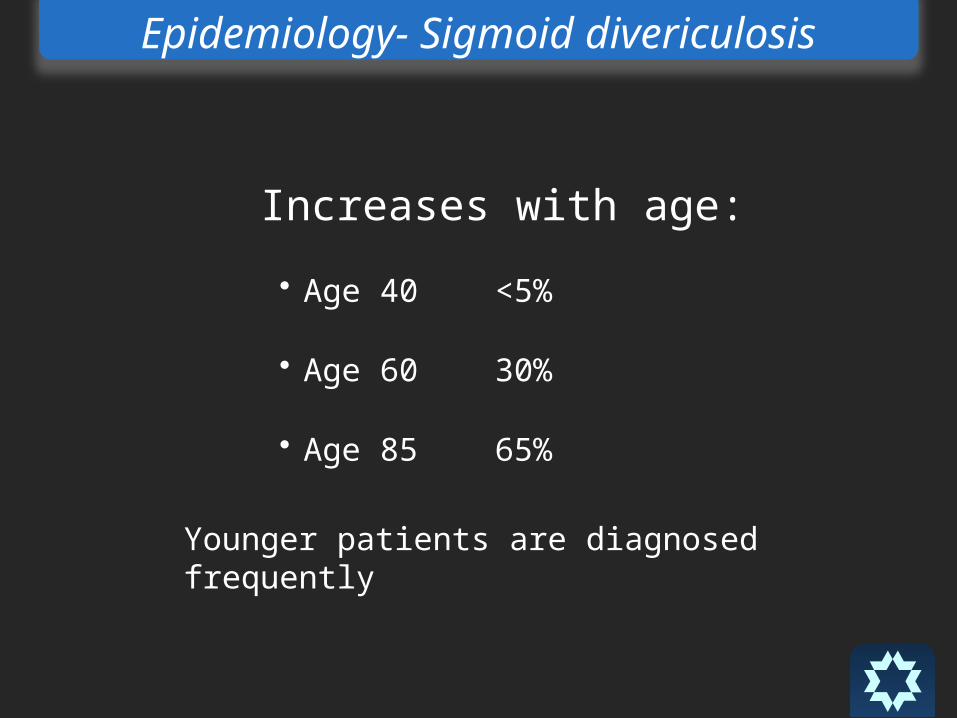
Increases with age:• Age 40 <5%
• Age 60 30%
• Age 85 65%
Younger patients are diagnosed frequently
Epidemiology- Sigmoid divericulosis

Endoscopic appearance
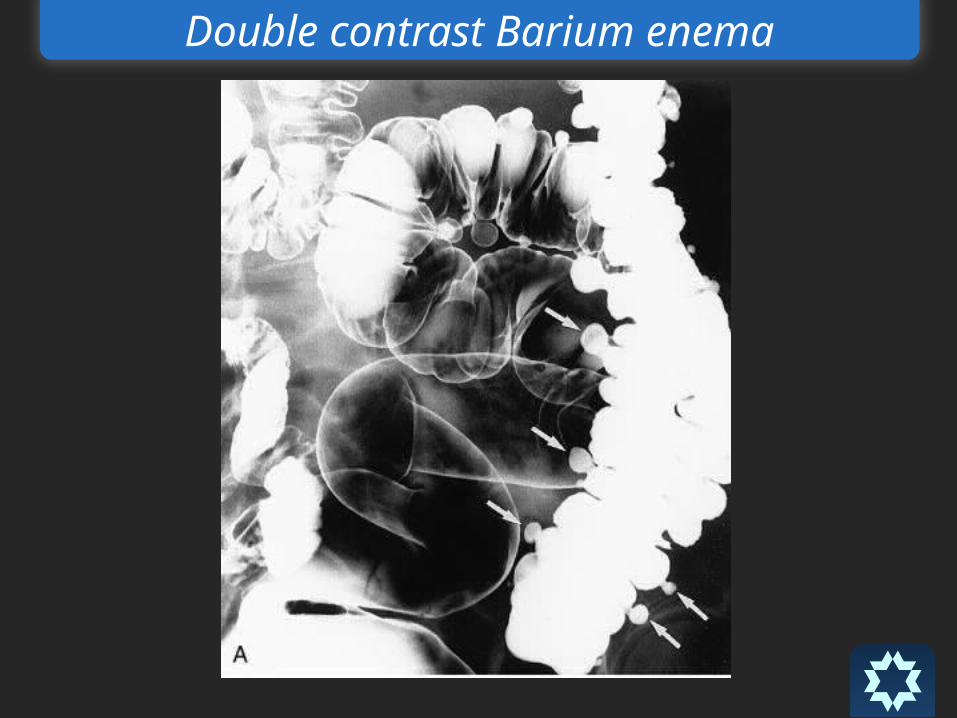
Double contrast Barium enema

CT Scan

CT Scan
From out side…

“Westernized” nations have predominantly left sided diverticulosis
– 95% diverticuli are in sigmoid colon
– 35% can also have proximal diverticuli
– 4% have only right sided diverticuli
Anatomic location of diverticuli varies with the geographic location

Asia and Africa diverticulosis in general is rare and usually right sided
– Prevalence < 0.2%
– 70% diverticuli in right colon in Japan
Anatomic location of diverticuli varies with the geographic location

Pathophysiology
• Diverticuli develop in ‘weak’ regions of the colon. Specifically, local hernias develop where the vasa recta penetrate the bowel wall
Pathophysiology
• Law of Laplace:• Pressure = K x Tension / Radius
• Sigmoid colon has the smallest diameter resulting in highest pressure zone

Pathophysiology
• Segmentation = motility process in which the segmental muscular contractions separate the lumen into chambers
• Segmentation increased intraluminal pressure mucosal herniation Diverticulosis
May explain why high fiber prevents diverticuli by creating a larger diameter colon and less vigorous segmentation

Pathophysiology

Lifestyle factors associated with diverticular disease
Low fiber diverticular disease
Not absolutely proven in all studies but strongly suggested
Western diet is low in fiber with high prevalence of diverticulosis
In contrast, African diet is high in fiber with a low prevalence of diverticulosis

Lifestyle factors associated with diverticular disease
• Obesity associated with diverticulosis – particularly in men under the age of 40
• Lack of physical activity
Lifestyle factors associated with diverticular disease
Do patients need to avoid foods with seeds or nuts?

Lifestyle factors associated with diverticular disease
NO!
In most cases diverticular disease is a-
symptomatic

A-symptomatic diverticulosis
• Considered ‘a-symptomatic’ • However, some patients will complain of
cramping, bloating, irregular BMs, narrow caliber stools
• Confused with IBS• Recent studies demonstrate motility
abnormalities in patients with ‘a-symptomatic’ uncomplicated diverticulosis

Diverticulitis
• Diverticulitis = inflammation of diverticuli
• Most common complication of diverticulosis
• Occurs in 10-25% of patients with diverticulosis
Diverticulitis
• Micro or macroscopic perforation of the diverticulum
• Subclinical inflammation to generalized peritonitis
• Previously thought to be due to fecaliths causing
increased diverticular pressure; this is really rare
Diverticulitis
• Erosion of diverticular wall from increased
intraluminal pressure
• Inflammation
• Focal necrosis
• Perforation
• Usually inflammation is mild and microperforation is
walled off by peri-colonic fat and mesentery
Diagnosis of Diverticulitis
• Classic history: increasing, constant, LLQ abdominal
pain over several days prior to presentation with fever
• Crescendo quality – each day is worse
• Constant – not colicky
• Fever occurs in 57-100% of cases

Diagnosis of Diverticulitis
• Previous episodes of similar pain
• Associated symptoms• Nausea/vomiting 20-62%
• Constipation 50%
• Diarrhea 25-35%
• Urinary symptoms (dysuria, urgency, frequency) 10-15%
Diagnosis of Diverticulitis
• Diagnosis can be made with typical history and
examination
• Radiographic confirmation (CT) is often… (100%)
performed
• Rules out other causes of an acute abdomen
• Determines severity of the diverticulitis

CT Scan
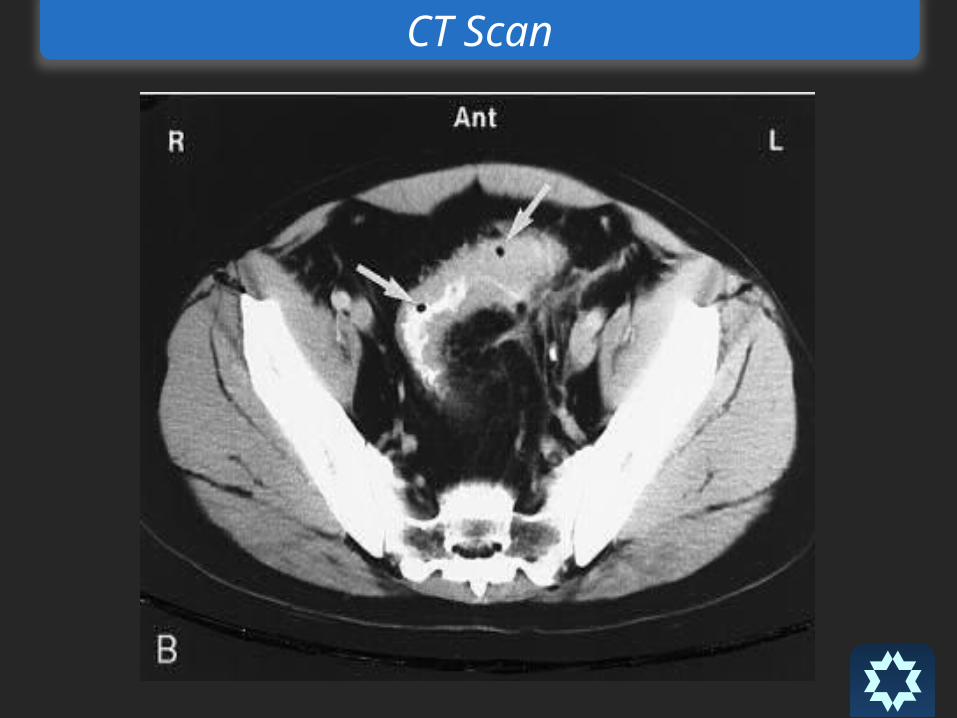
CT Scan

Simple vs. Complicated Diverticulitis
• Complicated diverticulitis = Presence of
macroperforation, obstruction, abscess or fistula
• Simple diverticulitis = Absence of the above
complications
Simple vs. Complicated Diverticulitis
• Complicated diverticulitis = Presence of
macroperforation, obstruction, abscess or fistula
• Simple diverticulitis = Absence of the above
complications

Simple Diverticulitis
Hospitalization !?

Simple Diverticulitis
• IV Antibiotics
• Bowel rest, clear liquids for 2-3 days
• Based on clinical findings advance diet (low residue)
and PO antibiotics

Simple Diverticulitis
After resolution of attack - high fiber diet
with supplemental fiber
Simple Diverticulitis
• Follow-up: Colonoscopy in 4-6 weeks• Purpose
• Exclude neoplasm
• Evaluate extent of the diverticulosis
Simple Diverticulitis
Prognosis after resolution
• 30-40% of patients will remain asymptomatic
• 30-40% of patients will have episodic abdominal
cramps without frank diverticulitis
• 20-30% of pts will have a second attack
Simple vs. Complicated Diverticulitis
• Complicated diverticulitis = Presence of
macroperforation, obstruction, abscess or fistula
• Simple diverticulitis = Absence of the above
complications

Complicated Diverticulitis
Hinchey classification1. Pericolic abscess
2. Distal abscess
3. Purulent peritonitis
4. Fecal peritonitis
Hinchey EJ et al. Treatment of perforated diverticular disease of the colon. Adv Surg. 1978

Complicated Diverticulitis
Hinchey classification1. Pericolic abscess
2. Distal abscess
CT guided drainage

Complicated Diverticulitis
Hinchey classification3. Purulent peritonitis
4. Fecal peritonitis
Surgery

Complicated Diverticulitis
Hartman’s Procedure

Complicated Diverticulitis
Other clinical presentation
1.Bleeding
2.Stricture
3.Fistula

Complicated Diverticulitis
Other clinical presentation
Bleeding

Complicated Diverticulitis

Complicated Diverticulitis

Complicated Diverticulitis
• Most only have symptoms of bloating and diarrhea but no significant abdominal pain – Painless hematochezia– Start – stop pattern; “water faucet”
• Diverticulitis rarely causes bleeding• Right > Left

Complicated Diverticulitis
Other clinical presentation
Stricture

Complicated Diverticulitis
• Chronic inflammation
• Bloating
• Constipation

Complicated Diverticulitis
Other clinical presentation
Stricture
Surgery

Complicated Diverticulitis
Other clinical presentation
Fistula
Complicated Diverticulitis
• Chronic inflammation• Small Bowel
• Bladder
• Vagina (s/p Hysterectomy)
• Retro – peritoneum

Complicated Diverticulitis
Other clinical presentation
Fistula
Surgery
Re-operative Surgery for Crohn’s Disease
Open vs. Lap?.
WhatWill Be Your
Approach?

Re-operative Surgery For Crohn’s Disease

Re-operative Surgery For Crohn’s DiseaseRe-operative Surgery For Crohn’s Disease

Re-operative Surgery For Crohn’s Disease
Sometimes it looks like this:

Re-operative Surgery For Crohn’s Disease

Less pain
Shorter stay
Less morbidity compared with open ?!
Faster return to normal activity
Immunologic & metabolic benefits
Adhesion formation, reduced SBO
Lower recurrence in Crohn’s ?
Cosmesis
So, Why Bother?
Port of entry & pneumoperitoneum
Adhesions & limited exposure
Anatomical orientation due to previous
resection / procedure
Anticipated Problems 1

Identification of pathology
Potential Intra-operative complications
(bleeding, enterotomies, adjacent organs i.e.
ureter)
Anticipated Problems 2
Get complete information & understanding
of the previous procedure
Plan surgical strategy: Port sites position,
complete Lap, Lap assisted, hand assisted
How to Avoid the Pitfalls

Positioning: both arms tucked in,
Lithotomy - team positioning flexibility
Room setup: 2 TV monitors!
How to Avoid the Pitfalls

Open technique for insufflation
First port placement away from scars
(a-traumatic Trocars / Visual ports)
Finger adhesiolysis (to create initial work space)
Angled scope – only!
A-traumatic intestinal graspers & dissectors
(Technical Considerations)
How to Avoid the Pitfalls

Adhesiolysis and additional port placement
Reestablish / confirm Anatomy
Identify pathology (tattoo in CRC, IOUS for solid
organs)
Urethral stents (depending procedure)
HALS?
Sound judgment & low threshold for conversion
How to Avoid the Pitfalls(Technical Considerations)

1443 Lap. Colorectal procedures
Oct. 2002 - Oct. 2010
42 Reop (2.8%) :
31 IBD (27 Rec Crohn’s, 4 UC)
7 Rec. CRC
4 Benign disease
26M, 16F, 21-79y old
1-13y - time from last procedure
Re-operative Laparoscopic Colorectal Surgery
Our Experience
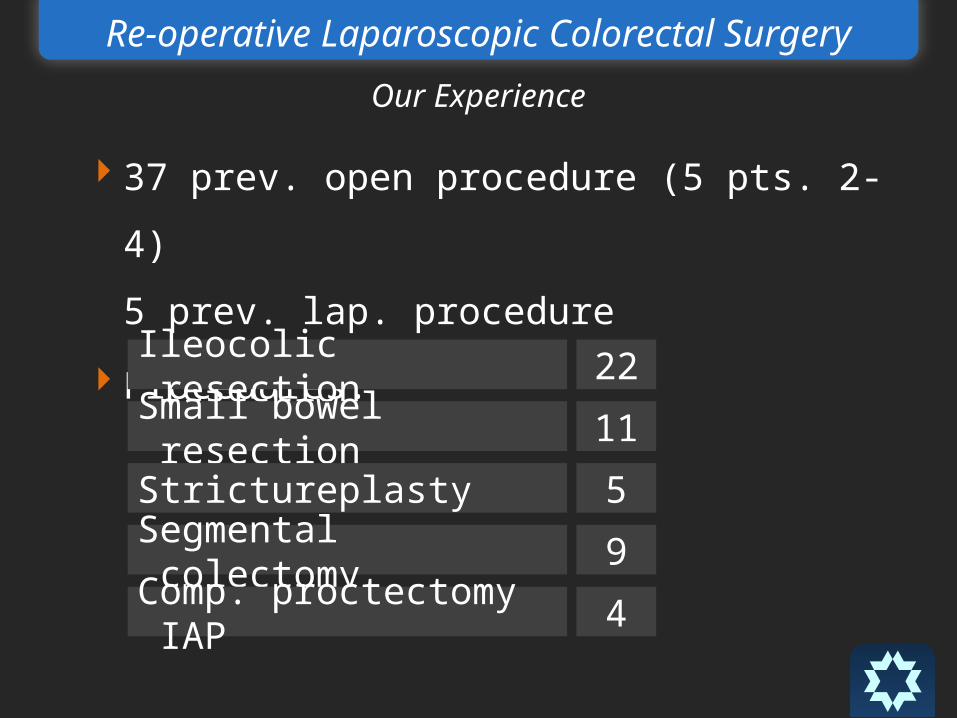
37 prev. open procedure (5 pts. 2-4)
5 prev. lap. procedure
Procedures: Ileocolic resection 22
Small bowel resection 11
Strictureplasty 5
Segmental colectomy 9
Comp. proctectomy IAP 4
Re-operative Laparoscopic Colorectal Surgery
Our Experience

Conversion rate 12% (n=6)
exposure & adhesions - 5
bleeding - 1
Morbidity 19% (n=8):
prolonged ileus - 6
post op intestinal bleeding - 2 (1 relaparotomy)
LOS mean 9 (6-21) days
Results:
Re-operative Laparoscopic Colorectal Surgery
Our Experience
Literature Review
The Role of Re-operative Laparoscopic Surgery
Anti reflux
Colorectal (IBD mostly Crohn’s disease, CRC)
Morbid obesity
SBO (adhesion related)
Re-operative Laparoscopic Surgery
70 – ileocolic resection
28/70 – previous ileocolic resection
1 – conversion ( in redo group)
7- complications (leak, stricture, hemorrhage, PE,
SBO, line sepsis, UTI) all in primary group
Canin J, Salky B, Edye M 1999 Surg Endosc
Re-operative Laparoscopic Surgery For Crohn’s Disease
Conclusion:
Experience required for successful laparoscopic
management in complicated Crohn’s
Canin J, Salky B, Edye M 1999 Surg Endosc
Re-operative Laparoscopic Surgery For Crohn’s Disease

23 patients underwent laparoscopic reoperation
for recurrent Crohn’s.
Conversion rate - 69% (n=16(
Complication, length of operation
were the same
Re-operative Laparoscopic Resection for Crohn’s Disease
Uchikoshi et al, Surg Endosc October 2004
168 laparoscopic-assisted ileocolic resections.
78.4% (n=124) redo
Previous resection was not a predictor
of conversion to laparotomy
Laparoscopic Assisted Ileocolic Resectionfor Crohn’s Disease
Edden Y. et al. JSLS 2008
Laparotomy vs. Laparoscopy?
Major Complication post
Laparoscopic Surgery
Requiring
Re-Exploration

510 patients
5.2% reoperation (n=27)
65% anastomotic leak (n=15)
Lap. approach 17 pts. (13/17 anast leak)
Open approach 10 pts. (2/10 anast leak)
Is a Laparoscopic Approach Useful for Treating Complication
After Primary Laparoscopic Colorectal Surgery?
Rotholz NA, Laporte M, et al. Dis Colon Rect 2009

Results: LOS 12d vs. 18d (P=NS)
Complications 1/17 vs. 3/10 (P=NS)
Is a Laparoscopic Approach Useful for Treating Complication
After Primary Laparoscopic Colorectal Surgery?
Rotholz NA, Laporte M, et al. Dis Colon Rect 2009

Trocar sites are the most common cause of bowel
obstruction in the early post operative period
Reoperation Following Minimally Invasive Surgery:
Are the ‘Rules’ Different?
McCormick JT.& Simmang CL. Clin Colon Rectal Surg 2006
Results comparable/similar to primary
laparoscopic resection
Late in the learning curve, experienced team
Patients selection
Concluding Comments

Expect higher conversion and longer OR time
Surgeon’s sound judgment to ensure
patients safety
Concluding Comments


LAP HAND ASSISTED RIGHT COLECTOMY

Angled scope
Intestinal Graspers & Dissectors
Tissue and Vascular division:
Harmonic Scalpel (LCS)
Ligasure
Endo Staplers
Endoclips
SURGICAL INSTRUMENTS AND EQUIPMENT
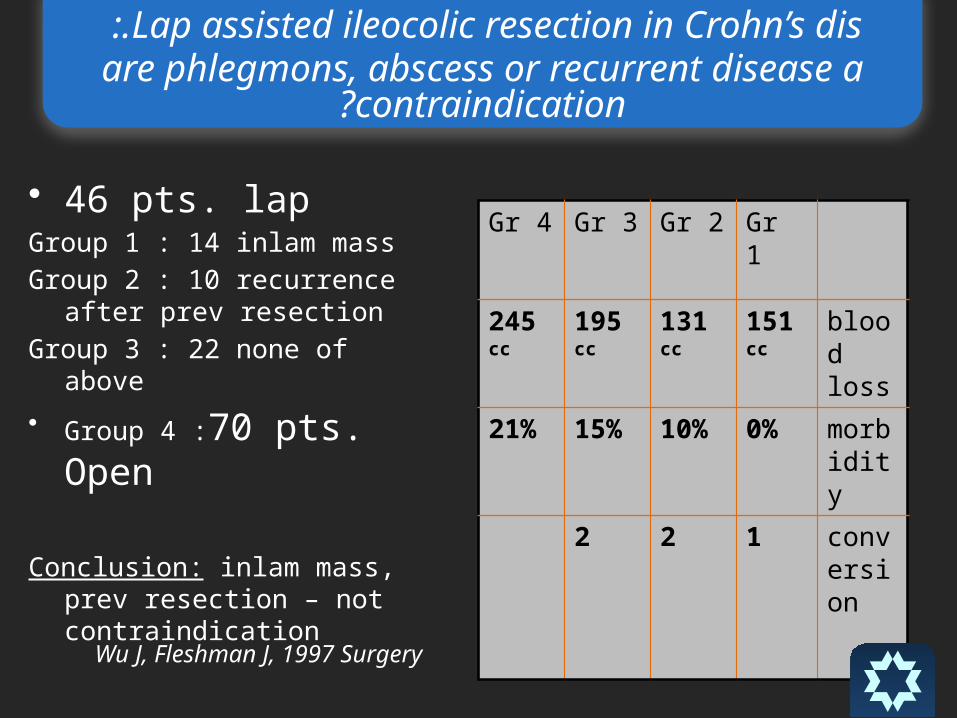
• 46 pts. lapGroup 1 : 14 inlam mass
Group 2 : 10 recurrence after prev resection
Group 3 : 22 none of above
• Group 4 :70 pts. Open
Conclusion: inlam mass, prev resection – not contraindication
Gr 4 Gr 3 Gr 2 Gr 1
245 cc
195 cc
131 cc
151 cc
blood loss
21% 15% 10% 0% morbidity
2 2 1 conversion
Lap assisted ileocolic resection in Crohn’s dis :.are phlegmons, abscess or recurrent disease a
contraindication?
Wu J, Fleshman J, 1997 Surgery
61 laparoscopic procedures,26.2% (n=16)
redo
No differences in the rate of postoperative
complications
Hasegawa H. et al. Br J Surg 2003
LAPAROSCOPIC SURGERY FOR RECURRENT CROHN’S DIS.

Related Documents