DOI: 10.1542/peds.2013-0787 ; originally published online April 28, 2014; 2014;133;809 Pediatrics Chakkarapani, Hemmen Sabir and Marianne Thoresen John Dingley, James Tooley, Xun Liu, Emma Scull-Brown, Maja Elstad, Ela Encephalopathy: A Feasibility Study Xenon Ventilation During Therapeutic Hypothermia in Neonatal http://pediatrics.aappublications.org/content/133/5/809.full.html located on the World Wide Web at: The online version of this article, along with updated information and services, is of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at University of Bristol Library on September 30, 2014 pediatrics.aappublications.org Downloaded from at University of Bristol Library on September 30, 2014 pediatrics.aappublications.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DOI: 10.1542/peds.2013-0787; originally published online April 28, 2014; 2014;133;809Pediatrics
Chakkarapani, Hemmen Sabir and Marianne ThoresenJohn Dingley, James Tooley, Xun Liu, Emma Scull-Brown, Maja Elstad, Ela
Encephalopathy: A Feasibility StudyXenon Ventilation During Therapeutic Hypothermia in Neonatal
http://pediatrics.aappublications.org/content/133/5/809.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

Xenon Ventilation During Therapeutic Hypothermia inNeonatal Encephalopathy: A Feasibility Study
WHAT’S KNOWN ON THIS SUBJECT: Hypothermia treatment ofneonatal encephalopathy reduces death and disability from 66%to 50%; additional neuroprotective therapies are needed. Wepreviously found in animal models that adding 50% xenon to thebreathing gas during cooling doubled neuroprotection.
WHAT THIS STUDY ADDS: This clinical feasibility study used 50%xenon for 3 to 18 hours in 14 cooled infants with cardiovascular,respiratory, and amplitude-integrated EEG monitoring. Thisdepressed seizures, with no blood pressure reduction. Xenon isready for randomized clinical trials in newborns.
abstractBACKGROUND AND OBJECTIVES: Therapeutic hypothermia has becomestandard of care in newborns with moderate and severe neonatal en-cephalopathy; however, additional interventions are needed. In exper-imental models, breathing xenon gas during cooling offers long-termadditive neuroprotection. This is the first xenon feasibility study in cooledinfants. Xenon is expensive, requiring a closed-circuit delivery system.
METHODS: Cooled newbornswith neonatal encephalopathy were eligiblefor this single-arm, dose-escalation study if clinically stable, under 18hours of age and requiring less than 35% oxygen. Xenon duration in-creased stepwise from 3 to 18 hours in 14 subjects; 1 received 25%xenon and 13 received 50%. Respiratory, cardiovascular, neurologic(ie, amplitude-integrated EEG, seizures), and inflammatory (C-reactiveprotein) effects were examined. The effects of starting or stopping xenonrapidly or slowly were studied. Three matched control subjects perxenon treated subject were selected from our cooling database. Follow-up was at 18 months using mental developmental and physical devel-opmental indexes of the Bayley Scales of Infant Development II.
RESULTS: No adverse respiratory or cardiovascular effects, includingpost-extubation stridor, were seen. Xenon increased sedation and sup-pressed seizures and background electroencephalographic activity. Seiz-ures sometimes occurred during rapid weaning of xenon but not duringslow weaning. C-reactive protein levels were similar between groups.Hourly xenon consumption was 0.52 L. Three died, and 7 of 11 survivorshad mental and physical developmental index scores $70 at follow-up.
CONCLUSIONS: Breathing 50% xenon for up to 18 hours with 72 hoursof cooling was feasible, with no adverse effects seen with 18 months’follow-up. Pediatrics 2014;133:809–818
AUTHORS: John Dingley, MD,a James Tooley, MRCPH,b XunLiu, PhD,b Emma Scull-Brown,b Maja Elstad, PhD,c ElaChakkarapani, MD,b Hemmen Sabir, MD,b and MarianneThoresen, PhDb,c
aCollege of Medicine, Swansea University, Swansea, UnitedKingdom; bNeonatal Neuroscience, School of Clinical Sciences,University of Bristol, Bristol, United Kingdom; and cDepartment ofPhysiology, Institute of Basic Medical Sciences, University of Oslo,Oslo, Norway
KEY WORDShypoxic-ischemic encephalopathy, hypothermia, neonatalencephalopathy, newborn, quality of life, sedation, ventilation,xenon
ABBREVIATIONSaEEG—amplitude-integrated EEGBS—burst suppressionCRP—C-reactive proteinETCO2—end-tidal carbon dioxideFIO2—fraction of inspired oxygenHIE—hypoxic-ischemic encephalopathyHI—hypoxic-ischemicMABP—mean arterial blood pressureMDI—mental developmental indexNE—neonatal encephalopathyPDI—psychomotor developmental indexTcSO2—transcutaneous oxygen saturationTH—therapeutic hypothermiaXe—xenon
Dr Dingley was responsible for xenon administration andtechnical Medicines and Healthcare Products Regulatory Agencydocumentation, and contributed to drafting and reviewing of themanuscript; Dr Tooley was responsible for organizing outborntransport and early treatment of the infants, was clinicallyresponsible and contributed to administering the treatment,and contributed to drafting of the manuscript; Dr Liuadministered the study, collected and analyzed data, contributedto drafting and manuscript revisions, and created the figures;Mrs Scull-Brown organized the administration of the study andcollected data; Dr Elstad collected and analyzed data andcontributed to manuscript revisions; Dr Chakkarapani treatedthe infants, collected and analyzed data, and contributed to themanuscript; Dr Sabir treated the infants, entered and analyzeddata, created figures, and contributed to the manuscript; andDr Thoresen was the Principal Investigator of the study whoplanned the study protocol with Dr Dingley and secured thefunding for the study. Dr Thoresen also treated and organizedfollow-up of patients, supervised the data collection andanalysis, and participated in data analysis, manuscript drafting,and revision. All authors approved the final manuscript assubmitted.
This trial has been registered with the ISRCTN Register(ISRCTN75602528).
(Continued on last page)
PEDIATRICS Volume 133, Number 5, May 2014 809
ARTICLE
at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

Severe neonatal encephalopathy (NE),mostly of hypoxic-ischemic (HI) origin,leads to brain injury in term newborns,often causing lifelong motor and cog-nitive impairment. The primary insult isfollowed by a self-sustaining destruc-tive cascade1 that postinsult therapiesmight limit. No clinical interventionexcept therapeutic hypothermia (TH) isknown to improve the neurologic out-come.2–4 A meta-analysis of 7 largerandomized controlled cooling trialshas shown that poor outcome is re-duced from 66% to 50% in cooledinfants.4–7 Adding the anesthetic gasxenon (Xe) to TH for additional neuro-protection has been investigated insmall8–11 and large12 experimental invivo preclinical outcome studies by usas well as other researchers. Adding50% Xe to cooling immediately post-insult doubles the neuroprotectiveeffect,11,12 as measured by using his-tologic neuropathology scores, and Xeis effective even after a 2-hour delay.13
After HI, reperfusion leads to exces-sive glutamate release, N-methyl-D-aspartate receptor overactivation, andcalcium influx–mediated apoptoticneuronal death. Xe partially inhibits theN-methyl-D-aspartate receptor,14 andXe pretreatment up-regulates the pro-survival proteins Bcl-2 and brain-derived neurotrophic factor in rats.15
Xe is an almost inert elemental gas, 4times heavier than air and free of ad-verse physiologic effects or toxicity.16–18
It is eliminated unchanged via the lungswithin minutes when delivery is stop-ped and therefore is a potentially re-versible intervention. Xe is licensed foradult anesthesia in Europe19 (LENOXeTM, Air Liquide, Paris, France) andRussia (KseMed, Akela-P Medical GasesPvt. Ltd, Moscow, Russia; Russian Feder-ation license 64/0125-Л/02 of 19.12.2002),but the high cost ($30 per liter) andfixed annual production limit its use.The only previous neonatal experiencewith Xe was from 133Xe isotope stud-ies.20
An economical Xe delivery system wasdeveloped that recirculates exhaledgases, removes carbon dioxide, andadds oxygen/Xe to replace patient up-take. In preclinical pig studies,12,21 0.25L/h of Xe maintained a steady 50%Xe concentration after initial circuitpriming, minimizing costs comparedwith an open ventilator using up to180 L/h of Xe. Additional costs included$200 for the single-use ventilation cir-cuit and $80 for the cuffed endotra-cheal tube.
Adding50%Xe toTH inbothshort-term11
and long-term13 neonatal brain injurymodels doubles the neuroprotectioncompared with TH alone. Moving froma rodent to a larger whole-body HI pigsurvival model confirmed an additiveeffect between Xe and TH, resulting in75% protection in neuropathology.12 Ina newborn pig brain ischemia model,metabolic markers favored the Xe + THgroup compared with Xe or TH alone.22
Xe + TH improved cardiovascular stabilityand reduced inotropic requirements.23
There was no increased oxygen require-ment, no cuffed tracheal tube complica-tions, and no stridor or extubation delaysin either our experimental pig study12
(n = 120) or this clinical study. There areongoing concerns regarding neuro-apoptosis in the immature brain withinhalation anesthetic agents.24 Althoughatypical in mode of action, Xe is an in-halation anesthetic. Recently, we venti-lated newborn pigs for 24 hours with50% Xe, finding no increase in neuro-apoptosis over normal controls unlikethose ventilated with 2% isoflurane, inwhich there was a .10-fold increase.25
A study of 120 newborn pigs providedsafety data for all organ systems26 andsupported our use of 50% Xe in thisclinical feasibility study in term infantsundergoing TH.
METHODS
This was a single-arm, dose-escalationfeasibility study adding Xe ventilation to
14 cooled infants with NE. We used theSarnat clinical severity scoring sys-tem27 of hypoxic-ischemic encephalop-athy (HIE) (1: mild; 2: moderate; and 3:severe) and included grade 2 or 3 in-fants. The setting was a single tertiarycenter treating in- and outborn pa-tients fulfilling standard TH criteria.Approvals from the Medicines andHealthcare Products Regulatory Agencyfor the Xe delivery system21 (C1/2009/0043) as well as for off-license Xeuse (LenoXe, Air Liquide, Duesseldorf,Germany) (12893/0223/001-0001) wereobtained, as was ethics approval fromBristol University, United Kingdom (UK09/H0106/64). Recruitment was fromMarch2010 until April 2011.
Primary outcomes were technical fea-sibility and physiologic stability, partic-ularly with respect to cardiorespiratoryparameters and EEG. The regional eth-ical committee requested follow-up asin the ongoing cooling program, witha Bayley Scales of Infant DevelopmentII28 examination performed at 18 to 20months as a secondary safety analysis.The mental developmental index (MDI)and the psychomotor developmentalindex (PDI) are classified as mild delay(,1 SD below the mean) if values are,85 and as major delay if ,70. Theregional ethical committee also re-quested a limited data set of historicalcontrols from our institution; 3 cooledpatients per Xe-treated patient werematched for oxygen requirement andseverity of NE at entry. Signed informedparental consent was obtained foradding Xe to cooling, including re-placement of the standard uncuffedendotracheal tube with a cuffed tube(code 3511; Kimberly-Clark Health Care,Roswell, Georgia) of the same or 0.5 mmsmaller diameter. Minimum cuff pres-sures for a complete seal were moni-tored hourly (Portex, Hythe, UK) (Fig 1D).
The number of deaths that statisticallywould require trial suspension, pend-ing review, as calculated for patients 1
810 DINGLEY et al at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

through 14 based on a retrospectivecooling mortality of 25% is shown inTable 1. This stopping rule is such thatthe trial is stopped if the binomialprobability for the observed number ofdeaths is ,0.05 but continued if thisvalue is.0.05. These calculationsweremade by our study statistician basedon this principle and our cooling mor-tality data over the preceding 6 years.
After initial resuscitation and medicalmanagement following usual guide-lines for NE and cooling therapy, addi-tional inclusion criteria for Xe wereapplied:,18 hours old, weight greaterthan the second percentile for gesta-tional age, intubated and ventilated,sedated, being cooled, seizures undercontrol, stable cardiovascular param-eters, mean arterial blood pressure(MABP) .40 mm Hg, oxygen re-quirement via mechanical ventilator,0.35, positive end-expiratory pres-
sure #8 cm H2O, arterial/capillary/venous PCO2 ,7.0 kPa (ideally arte-rial), and absence of major congenitalabnormalities (in particular, imperfo-rate anus or any bowel obstruction).4,6
Thirteen infants were outborn and 1was inborn. All started “passive” cool-ing followed by active servo-controlledbody cooling by using Criticool (MTREAdvanced Technologies Ltd, Rehovot,Israel) (n = 12) or Tecotherm Neo (In-spiration Healthcare Ltd, Leicester, UK)(n = 2) machines. Umbilical arterial/venous catheters were inserted forarterial pressure, blood gas measure-ments, fluid infusions of dextrose withelectrolytes (n = 12), or total paren-teral nutrition (n = 2), sedatives, anti-convulsants, inotropes, and antibiotics.Routine sedation for ventilated infantswas 20 mg/kg per hour of morphine.Hourly neonatal facial coding scoringfor pain evaluation was performed,
and the dose adjusted accordingly.29
Clinical or subclinical seizures recog-nized on an amplitude-integrated EEG(aEEG) and an EEG (Olympic CFM 6000,Natus Medical Incorporated, San Carlos,California) lasting .3 minutes weretreated with anticonvulsants. The firstinfant who received Xe during coolingwas given 25% Xe for 3 hours; thefollowing infants received 50% Xe for3, 6, 12, or 18 hours (Table 2). Becauseno human neonate had previously re-ceived Xe, we gradually increased thetreatment duration to our target of 18hours, which is the amount shown tobe neuroprotective in the preclinicalstudy.12
Figure 1 shows the monitoring andbreathing system assembly.21 (seeSupplemental Video) The closed venti-lator circuit was partially flushed withfresh gas every 2 hours as a pre-caution. Cardiovascular, respiratory,
FIGURE 1Xe closed-circuit breathing system: A, Cuffed tracheal tube and mainstream infrared carbon dioxide (CO2) sensor with display (inset). B, Diagram of closedbreathing circuit: (a) inspiratory and (b) expiratory hoses, (c) Xe addition port, and (d) oxygen substitution valve. C, Breathing circuit assembled with Xecylinder. D, Median hourly cuff pressure during Xe inhalation.
ARTICLE
PEDIATRICS Volume 133, Number 5, May 2014 811 at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
and aEEG/EEG responses, includingseizures, were monitored closely dur-ing Xe initiation (0% to 50%) andweaning (50% to 0%). Xe onset andoffset were initially performed slowlyover 45 minutes as a precautionarymeasure, then reduced gradually to 7minutes. On stopping Xe, conventionalventilation was resumed, the endotra-cheal tube cuff deflated, and the tubeleft in situ. Protocols for hypotension,hypoxemia, infection risk, abnormal
carbon dioxide levels, seizures, reintu-bation, and extubation followed stan-dard clinical practice.
RESULTS
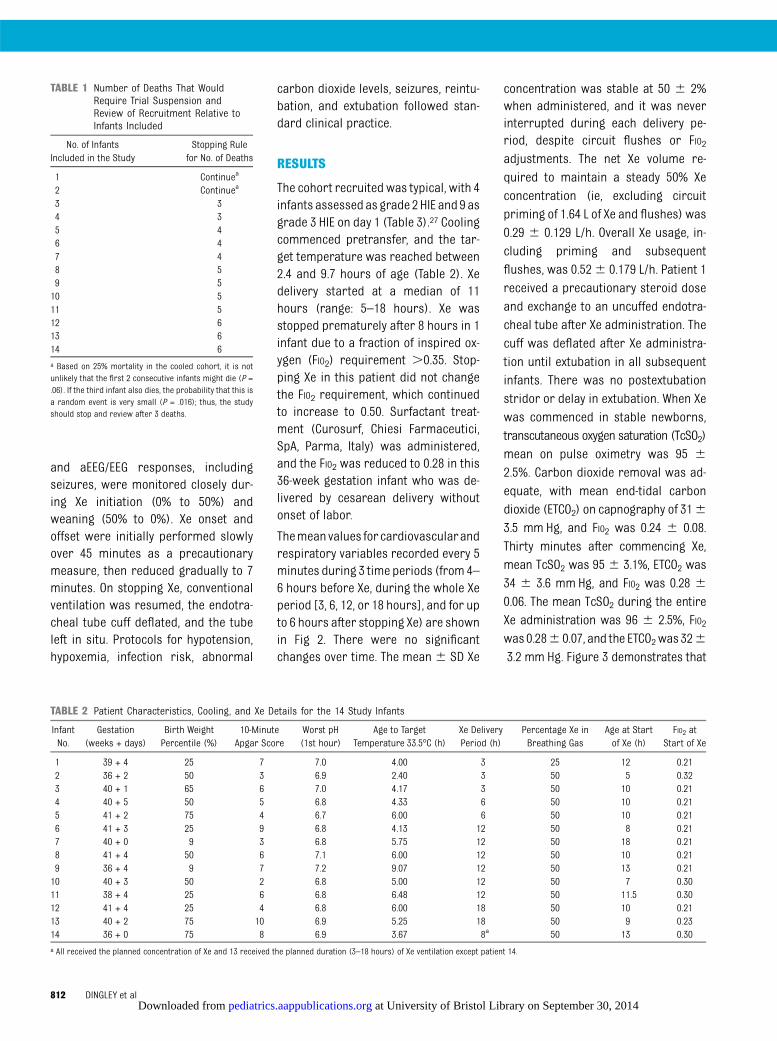
The cohort recruited was typical, with 4infants assessed as grade 2HIE and 9 asgrade 3 HIE on day 1 (Table 3).27 Coolingcommenced pretransfer, and the tar-get temperature was reached between2.4 and 9.7 hours of age (Table 2). Xedelivery started at a median of 11hours (range: 5–18 hours). Xe wasstopped prematurely after 8 hours in 1infant due to a fraction of inspired ox-ygen (FIO2) requirement .0.35. Stop-ping Xe in this patient did not changethe FIO2 requirement, which continuedto increase to 0.50. Surfactant treat-ment (Curosurf, Chiesi Farmaceutici,SpA, Parma, Italy) was administered,and the FIO2 was reduced to 0.28 in this36-week gestation infant who was de-livered by cesarean delivery withoutonset of labor.
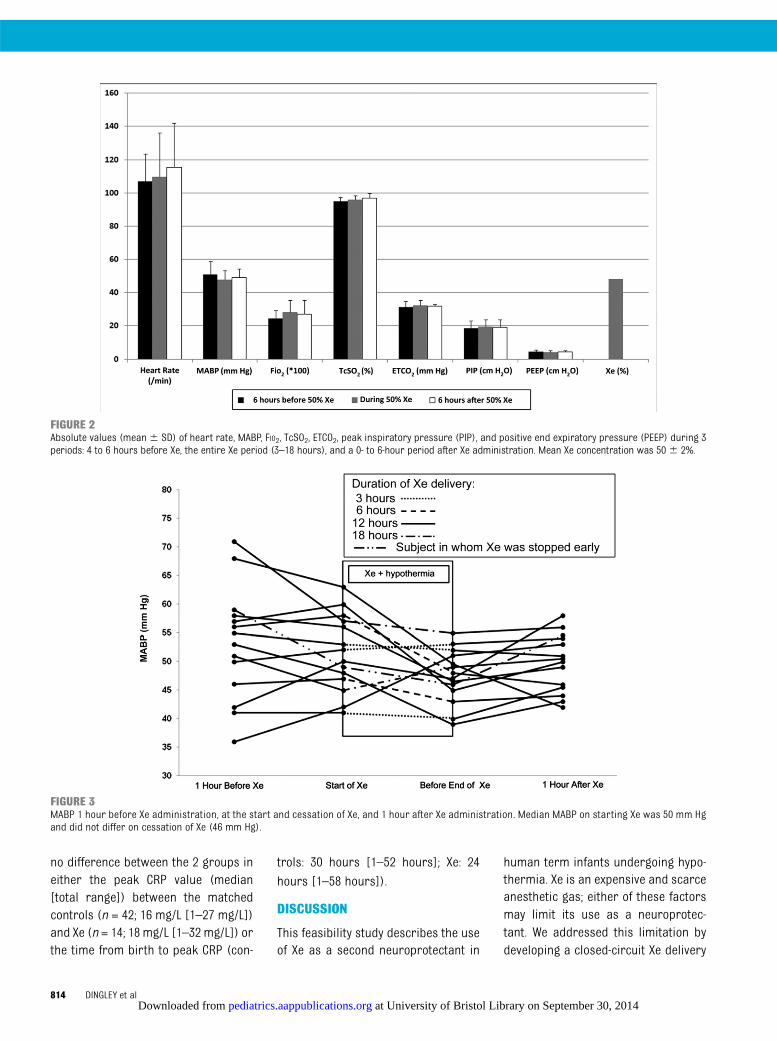
Themeanvalues forcardiovascularandrespiratory variables recorded every 5minutes during 3 time periods (from 4–6 hours before Xe, during the whole Xeperiod [3, 6, 12, or 18 hours], and for upto 6 hours after stopping Xe) are shownin Fig 2. There were no significantchanges over time. The mean6 SD Xe
concentration was stable at 50 6 2%when administered, and it was neverinterrupted during each delivery pe-riod, despite circuit flushes or FIO2adjustments. The net Xe volume re-quired to maintain a steady 50% Xeconcentration (ie, excluding circuitpriming of 1.64 L of Xe and flushes) was0.29 6 0.129 L/h. Overall Xe usage, in-cluding priming and subsequentflushes, was 0.526 0.179 L/h. Patient 1received a precautionary steroid doseand exchange to an uncuffed endotra-cheal tube after Xe administration. Thecuff was deflated after Xe administra-tion until extubation in all subsequentinfants. There was no postextubationstridor or delay in extubation. When Xewas commenced in stable newborns,transcutaneous oxygen saturation (TcSO2)mean on pulse oximetry was 95 6
2.5%. Carbon dioxide removal was ad-equate, with mean end-tidal carbondioxide (ETCO2) on capnography of 3163.5 mm Hg, and FIO2 was 0.24 6 0.08.Thirty minutes after commencing Xe,mean TcSO2 was 956 3.1%, ETCO2 was34 6 3.6 mm Hg, and FIO2 was 0.28 6
0.06. The mean TcSO2 during the entireXe administration was 96 6 2.5%, FIO2was 0.286 0.07, and the ETCO2was 3263.2 mm Hg. Figure 3 demonstrates that
TABLE 1 Number of Deaths That WouldRequire Trial Suspension andReview of Recruitment Relative toInfants Included
No. of InfantsIncluded in the Study
Stopping Rulefor No. of Deaths
1 Continuea
2 Continuea
3 34 35 46 47 48 59 510 511 512 613 614 6a Based on 25% mortality in the cooled cohort, it is notunlikely that the first 2 consecutive infants might die (P =.06). If the third infant also dies, the probability that this isa random event is very small (P = .016); thus, the studyshould stop and review after 3 deaths.
TABLE 2 Patient Characteristics, Cooling, and Xe Details for the 14 Study Infants
InfantNo.
Gestation(weeks + days)
Birth WeightPercentile (%)
10-MinuteApgar Score
Worst pH(1st hour)
Age to TargetTemperature 33.5°C (h)
Xe DeliveryPeriod (h)
Percentage Xe inBreathing Gas
Age at Startof Xe (h)
FIO2 atStart of Xe
1 39 + 4 25 7 7.0 4.00 3 25 12 0.212 36 + 2 50 3 6.9 2.40 3 50 5 0.323 40 + 1 65 6 7.0 4.17 3 50 10 0.214 40 + 5 50 5 6.8 4.33 6 50 10 0.215 41 + 2 75 4 6.7 6.00 6 50 10 0.216 41 + 3 25 9 6.8 4.13 12 50 8 0.217 40 + 0 9 3 6.8 5.75 12 50 18 0.218 41 + 4 50 6 7.1 6.00 12 50 10 0.219 36 + 4 9 7 7.2 9.07 12 50 13 0.2110 40 + 3 50 2 6.8 5.00 12 50 7 0.3011 38 + 4 25 6 6.8 6.48 12 50 11.5 0.3012 41 + 4 25 4 6.8 6.00 18 50 10 0.2113 40 + 2 75 10 6.9 5.25 18 50 9 0.2314 36 + 0 75 8 6.9 3.67 8a 50 13 0.30a All received the planned concentration of Xe and 13 received the planned duration (3–18 hours) of Xe ventilation except patient 14.
812 DINGLEY et al at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
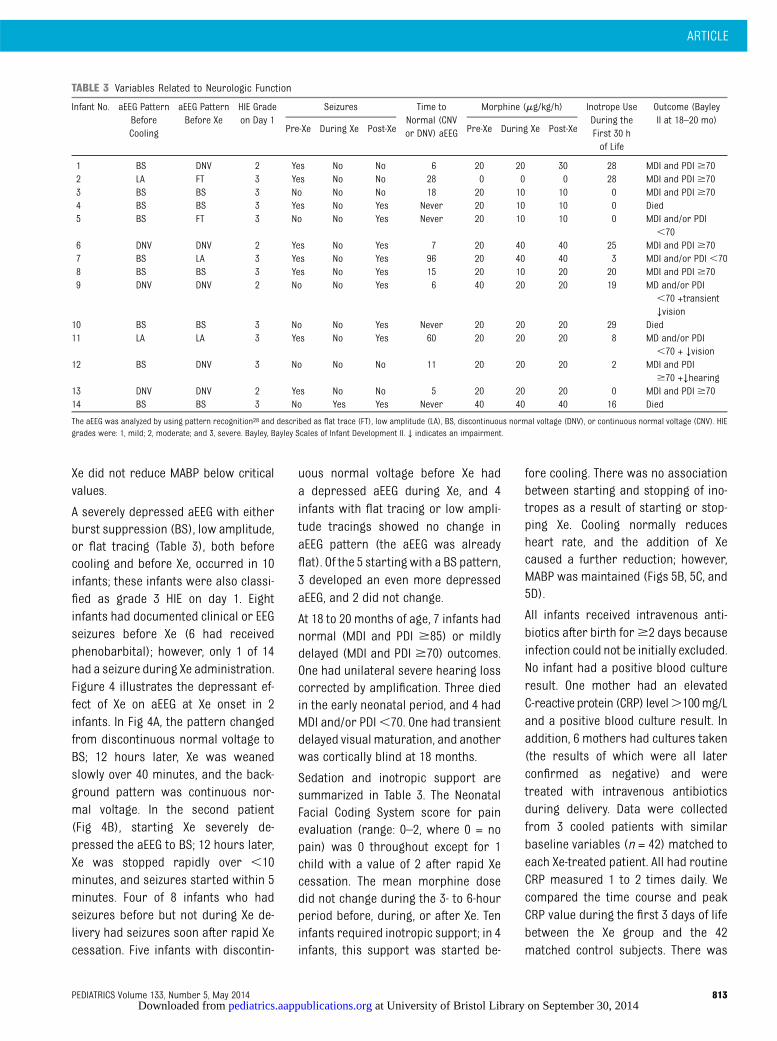
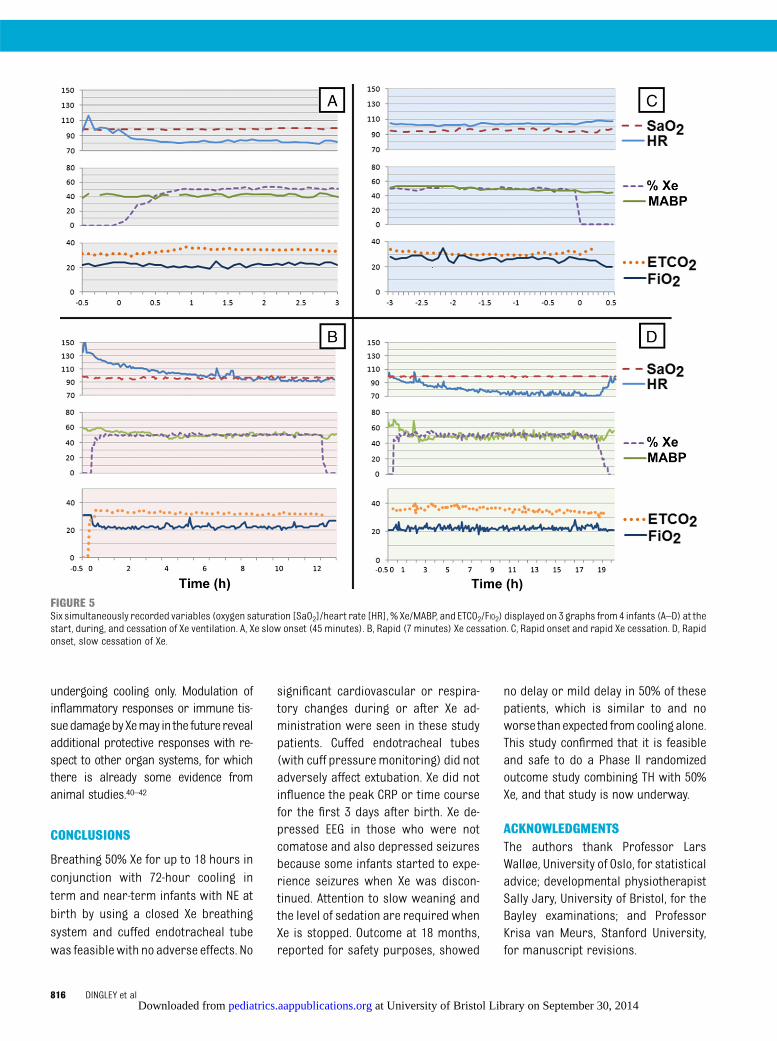
Xe did not reduce MABP below criticalvalues.
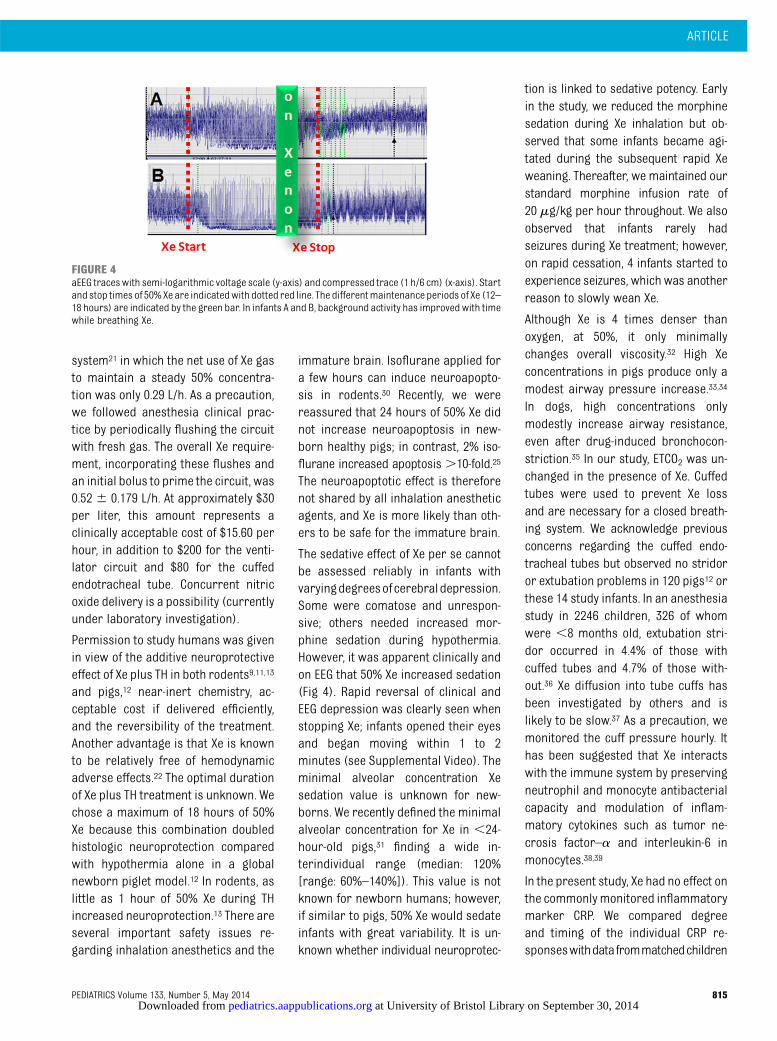
A severely depressed aEEG with eitherburst suppression (BS), low amplitude,or flat tracing (Table 3), both beforecooling and before Xe, occurred in 10infants; these infants were also classi-fied as grade 3 HIE on day 1. Eightinfants had documented clinical or EEGseizures before Xe (6 had receivedphenobarbital); however, only 1 of 14had a seizure during Xe administration.Figure 4 illustrates the depressant ef-fect of Xe on aEEG at Xe onset in 2infants. In Fig 4A, the pattern changedfrom discontinuous normal voltage toBS; 12 hours later, Xe was weanedslowly over 40 minutes, and the back-ground pattern was continuous nor-mal voltage. In the second patient(Fig 4B), starting Xe severely de-pressed the aEEG to BS; 12 hours later,Xe was stopped rapidly over ,10minutes, and seizures started within 5minutes. Four of 8 infants who hadseizures before but not during Xe de-livery had seizures soon after rapid Xecessation. Five infants with discontin-
uous normal voltage before Xe hada depressed aEEG during Xe, and 4infants with flat tracing or low ampli-tude tracings showed no change inaEEG pattern (the aEEG was alreadyflat). Of the 5 starting with a BS pattern,3 developed an even more depressedaEEG, and 2 did not change.
At 18 to 20 months of age, 7 infants hadnormal (MDI and PDI $85) or mildlydelayed (MDI and PDI $70) outcomes.One had unilateral severe hearing losscorrected by amplification. Three diedin the early neonatal period, and 4 hadMDI and/or PDI,70. One had transientdelayed visual maturation, and anotherwas cortically blind at 18 months.
Sedation and inotropic support aresummarized in Table 3. The NeonatalFacial Coding System score for painevaluation (range: 0–2, where 0 = nopain) was 0 throughout except for 1child with a value of 2 after rapid Xecessation. The mean morphine dosedid not change during the 3- to 6-hourperiod before, during, or after Xe. Teninfants required inotropic support; in 4infants, this support was started be-
fore cooling. There was no associationbetween starting and stopping of ino-tropes as a result of starting or stop-ping Xe. Cooling normally reducesheart rate, and the addition of Xecaused a further reduction; however,MABP was maintained (Figs 5B, 5C, and5D).
All infants received intravenous anti-biotics after birth for$2 days becauseinfection could not be initially excluded.No infant had a positive blood cultureresult. One mother had an elevatedC-reactive protein (CRP) level.100mg/Land a positive blood culture result. Inaddition, 6 mothers had cultures taken(the results of which were all laterconfirmed as negative) and weretreated with intravenous antibioticsduring delivery. Data were collectedfrom 3 cooled patients with similarbaseline variables (n = 42) matched toeach Xe-treated patient. All had routineCRP measured 1 to 2 times daily. Wecompared the time course and peakCRP value during the first 3 days of lifebetween the Xe group and the 42matched control subjects. There was
TABLE 3 Variables Related to Neurologic Function
Infant No. aEEG PatternBeforeCooling
aEEG PatternBefore Xe
HIE Gradeon Day 1
Seizures Time toNormal (CNVor DNV) aEEG
Morphine (mg/kg/h) Inotrope UseDuring theFirst 30 hof Life
Outcome (BayleyII at 18–20 mo)
Pre-Xe During Xe Post-Xe Pre-Xe During Xe Post-Xe
1 BS DNV 2 Yes No No 6 20 20 30 28 MDI and PDI $702 LA FT 3 Yes No No 28 0 0 0 28 MDI and PDI $703 BS BS 3 No No No 18 20 10 10 0 MDI and PDI $704 BS BS 3 Yes No Yes Never 20 10 10 0 Died5 BS FT 3 No No Yes Never 20 10 10 0 MDI and/or PDI
,706 DNV DNV 2 Yes No Yes 7 20 40 40 25 MDI and PDI $707 BS LA 3 Yes No Yes 96 20 40 40 3 MDI and/or PDI ,708 BS BS 3 Yes No Yes 15 20 10 20 20 MDI and PDI $709 DNV DNV 2 No No Yes 6 40 20 20 19 MD and/or PDI
,70 +transient↓vision
10 BS BS 3 No No Yes Never 20 20 20 29 Died11 LA LA 3 Yes No Yes 60 20 20 20 8 MD and/or PDI
,70 + ↓vision12 BS DNV 3 No No No 11 20 20 20 2 MDI and PDI
$70 +↓hearing13 DNV DNV 2 Yes No No 5 20 20 20 0 MDI and PDI $7014 BS BS 3 No Yes Yes Never 40 40 40 16 Died
The aEEG was analyzed by using pattern recognition28 and described as flat trace (FT), low amplitude (LA), BS, discontinuous normal voltage (DNV), or continuous normal voltage (CNV). HIEgrades were: 1, mild; 2, moderate; and 3, severe. Bayley, Bayley Scales of Infant Development II. ↓ indicates an impairment.
ARTICLE
PEDIATRICS Volume 133, Number 5, May 2014 813 at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
no difference between the 2 groups ineither the peak CRP value (median[total range]) between the matchedcontrols (n = 42; 16 mg/L [1–27 mg/L])and Xe (n = 14; 18 mg/L [1–32 mg/L]) orthe time from birth to peak CRP (con-
trols: 30 hours [1–52 hours]; Xe: 24
hours [1–58 hours]).
DISCUSSION
This feasibility study describes the useof Xe as a second neuroprotectant in
human term infants undergoing hypo-thermia. Xe is an expensive and scarceanesthetic gas; either of these factorsmay limit its use as a neuroprotec-tant. We addressed this limitation bydeveloping a closed-circuit Xe delivery
FIGURE 2Absolute values (mean6 SD) of heart rate, MABP, FIO2, TcSO2, ETCO2, peak inspiratory pressure (PIP), and positive end expiratory pressure (PEEP) during 3periods: 4 to 6 hours before Xe, the entire Xe period (3–18 hours), and a 0- to 6-hour period after Xe administration. Mean Xe concentration was 506 2%.
FIGURE 3MABP 1 hour before Xe administration, at the start and cessation of Xe, and 1 hour after Xe administration. Median MABP on starting Xe was 50 mm Hgand did not differ on cessation of Xe (46 mm Hg).
814 DINGLEY et al at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
system21 in which the net use of Xe gasto maintain a steady 50% concentra-tion was only 0.29 L/h. As a precaution,we followed anesthesia clinical prac-tice by periodically flushing the circuitwith fresh gas. The overall Xe require-ment, incorporating these flushes andan initial bolus to prime the circuit, was0.52 6 0.179 L/h. At approximately $30per liter, this amount represents aclinically acceptable cost of $15.60 perhour, in addition to $200 for the venti-lator circuit and $80 for the cuffedendotracheal tube. Concurrent nitricoxide delivery is a possibility (currentlyunder laboratory investigation).
Permission to study humans was givenin view of the additive neuroprotectiveeffect of Xe plus TH in both rodents9,11,13
and pigs,12 near-inert chemistry, ac-ceptable cost if delivered efficiently,and the reversibility of the treatment.Another advantage is that Xe is knownto be relatively free of hemodynamicadverse effects.22 The optimal durationof Xe plus TH treatment is unknown. Wechose a maximum of 18 hours of 50%Xe because this combination doubledhistologic neuroprotection comparedwith hypothermia alone in a globalnewborn piglet model.12 In rodents, aslittle as 1 hour of 50% Xe during THincreased neuroprotection.13 There areseveral important safety issues re-garding inhalation anesthetics and the
immature brain. Isoflurane applied fora few hours can induce neuroapopto-sis in rodents.30 Recently, we werereassured that 24 hours of 50% Xe didnot increase neuroapoptosis in new-born healthy pigs; in contrast, 2% iso-flurane increased apoptosis.10-fold.25
The neuroapoptotic effect is thereforenot shared by all inhalation anestheticagents, and Xe is more likely than oth-ers to be safe for the immature brain.
The sedative effect of Xe per se cannotbe assessed reliably in infants withvaryingdegreesofcerebraldepression.Some were comatose and unrespon-sive; others needed increased mor-phine sedation during hypothermia.However, it was apparent clinically andon EEG that 50% Xe increased sedation(Fig 4). Rapid reversal of clinical andEEG depression was clearly seen whenstopping Xe; infants opened their eyesand began moving within 1 to 2minutes (see Supplemental Video). Theminimal alveolar concentration Xesedation value is unknown for new-borns. We recently defined the minimalalveolar concentration for Xe in ,24-hour-old pigs,31 finding a wide in-terindividual range (median: 120%[range: 60%–140%]). This value is notknown for newborn humans; however,if similar to pigs, 50% Xe would sedateinfants with great variability. It is un-known whether individual neuroprotec-
tion is linked to sedative potency. Earlyin the study, we reduced the morphinesedation during Xe inhalation but ob-served that some infants became agi-tated during the subsequent rapid Xeweaning. Thereafter, we maintained ourstandard morphine infusion rate of20 mg/kg per hour throughout. We alsoobserved that infants rarely hadseizures during Xe treatment; however,on rapid cessation, 4 infants started toexperience seizures, which was anotherreason to slowly wean Xe.
Although Xe is 4 times denser thanoxygen, at 50%, it only minimallychanges overall viscosity.32 High Xeconcentrations in pigs produce only amodest airway pressure increase.33,34
In dogs, high concentrations onlymodestly increase airway resistance,even after drug-induced bronchocon-striction.35 In our study, ETCO2 was un-changed in the presence of Xe. Cuffedtubes were used to prevent Xe lossand are necessary for a closed breath-ing system. We acknowledge previousconcerns regarding the cuffed endo-tracheal tubes but observed no stridoror extubation problems in 120 pigs12 orthese 14 study infants. In an anesthesiastudy in 2246 children, 326 of whomwere ,8 months old, extubation stri-dor occurred in 4.4% of those withcuffed tubes and 4.7% of those with-out.36 Xe diffusion into tube cuffs hasbeen investigated by others and islikely to be slow.37 As a precaution, wemonitored the cuff pressure hourly. Ithas been suggested that Xe interactswith the immune system by preservingneutrophil and monocyte antibacterialcapacity and modulation of inflam-matory cytokines such as tumor ne-crosis factor–a and interleukin-6 inmonocytes.38,39
In the present study, Xe had no effect onthe commonlymonitored inflammatorymarker CRP. We compared degreeand timing of the individual CRP re-sponseswithdatafrommatchedchildren
FIGURE 4aEEG traceswith semi-logarithmic voltage scale (y-axis) and compressed trace (1 h/6 cm) (x-axis). Startand stop times of 50%Xe are indicatedwith dotted red line. The differentmaintenance periods of Xe (12–18 hours) are indicated by the green bar. In infants A and B, background activity has improvedwith timewhile breathing Xe.
ARTICLE
PEDIATRICS Volume 133, Number 5, May 2014 815 at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
undergoing cooling only. Modulation ofinflammatory responses or immune tis-suedamagebyXemay in the futurerevealadditional protective responses with re-spect to other organ systems, for whichthere is already some evidence fromanimal studies.40–42
CONCLUSIONS
Breathing 50% Xe for up to 18 hours inconjunction with 72-hour cooling interm and near-term infants with NE atbirth by using a closed Xe breathingsystem and cuffed endotracheal tubewas feasiblewith no adverse effects. No
significant cardiovascular or respira-tory changes during or after Xe ad-ministration were seen in these studypatients. Cuffed endotracheal tubes(with cuff pressuremonitoring) did notadversely affect extubation. Xe did notinfluence the peak CRP or time coursefor the first 3 days after birth. Xe de-pressed EEG in those who were notcomatose and also depressed seizuresbecause some infants started to expe-rience seizures when Xe was discon-tinued. Attention to slow weaning andthe level of sedation are required whenXe is stopped. Outcome at 18 months,reported for safety purposes, showed
no delay or mild delay in 50% of thesepatients, which is similar to and noworse thanexpected fromcooling alone.This study confirmed that it is feasibleand safe to do a Phase II randomizedoutcome study combining TH with 50%Xe, and that study is now underway.
ACKNOWLEDGMENTSThe authors thank Professor LarsWalløe, University of Oslo, for statisticaladvice; developmental physiotherapistSally Jary, University of Bristol, for theBayley examinations; and ProfessorKrisa van Meurs, Stanford University,for manuscript revisions.
FIGURE 5Six simultaneously recorded variables (oxygen saturation [SaO2]/heart rate [HR], % Xe/MABP, and ETCO2/FIO2) displayed on 3 graphs from4 infants (A–D) at thestart, during, and cessation of Xe ventilation. A, Xe slow onset (45 minutes). B, Rapid (7 minutes) Xe cessation. C, Rapid onset and rapid Xe cessation. D, Rapidonset, slow cessation of Xe.
816 DINGLEY et al at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

REFERENCES
1. Volpe JJ. Perinatal brain injury: frompathogenesis to neuroprotection. MentRetard Dev Disabil Res Rev. 2001;7(1):56–64
2. Thoresen M, Whitelaw A. Therapeutic hy-pothermia for hypoxic-ischaemic encepha-lopathy in the newborn infant. Curr OpinNeurol. 2005;18(2):111–116
3. Nelson KB, Ellenberg JH. Antecedents ofcerebral palsy. Multivariate analysis ofrisk. N Engl J Med. 1986;315(2):81–86
4. Gluckman PD, Wyatt JS, Azzopardi D, et al.Selective head cooling with mild systemichypothermia after neonatal encephalopa-thy: multicentre randomised trial. Lancet.2005;365(9460):663–670
5. Shankaran S, Laptook AR, Ehrenkranz RA,et al; National Institute of Child Health andHuman Development Neonatal ResearchNetwork. Whole-body hypothermia forneonates with hypoxic-ischemic encepha-lopathy. N Engl J Med. 2005;353(15):1574–1584
6. Azzopardi DV, Strohm B, Edwards AD, et al;TOBY Study Group. Moderate hypothermiato treat perinatal asphyxial encephalop-athy. N Engl J Med. 2009;361(14):1349–1358
7. Jacobs SE, Berg M, Hunt R, Tarnow-MordiWO, Inder TE, Davis PG. Cooling for new-borns with hypoxic ischaemic encephalop-athy. Cochrane Database Syst Rev. 2013;(1):CD003311
8. Petzelt C, Blom P, Schmehl W, Müller J, KoxWJ. Prevention of neurotoxicity in hypoxiccortical neurons by the noble gas xenon.Life Sci. 2003;72(17):1909–1918
9. Ma D, Hossain M, Chow A, et al. Xenon andhypothermia combine to provide neuro-protection from neonatal asphyxia. AnnNeurol. 2005;58(2):182–193
10. Dingley J, Tooley J, Porter H, Thoresen M.Xenon provides short-term neuroprotectionin neonatal rats when administered afterhypoxia-ischemia. Stroke. 2006;37(2):501–506
11. Hobbs C, Thoresen M, Tucker A, Aquilina K,Chakkarapani E, Dingley J. Xenon and hy-pothermia combine additively, offeringlong-term functional and histopathologicneuroprotection after neonatal hypoxia/is-chemia. Stroke. 2008;39(4):1307–1313
12. Chakkarapani E, Dingley J, Liu X, et al. Xenonenhances hypothermic neuroprotection inasphyxiated newborn pigs. Ann Neurol. 2010;68(3):330–341
13. Thoresen M, Hobbs CE, Wood T, ChakkarapaniE, Dingley J. Cooling combined with imme-diate or delayed xenon inhalation providesequivalent long-term neuroprotection after
neonatal hypoxia-ischemia. J Cereb BloodFlow Metab. 2009;29(4):707–714
14. Franks NP, Dickinson R, de Sousa SL, HallAC, Lieb WR. How does xenon produce an-aesthesia? Nature. 1998;396(6709):324
15. Ma D, Hossain M, Pettet GK, et al. Xenonpreconditioning reduces brain damagefrom neonatal asphyxia in rats. J CerebBlood Flow Metab. 2006;26(2):199–208
16. Rossaint R, Reyle-Hahn M, Schulte Am EschJ, et al; Xenon Study Group. Multicenterrandomized comparison of the efficacy andsafety of xenon and isoflurane in patientsundergoing elective surgery. Anesthesiol-ogy. 2003;98(1):6–13
17. Lane GA, Nahrwold ML, Tait AR, Taylor-BuschM, Cohen PJ, Beaudoin AR. Anesthetics asteratogens: nitrous oxide is fetotoxic, xenonis not. Science. 1980;210(4472):899–901
18. Burov NE, Arzamastsev EV, Kornienko LI,Kudimova LA. Investigation of the terato-genic and embryotoxic action of xenon [inRussian]. Anesteziol Reanimatol. 2002;(4):69–70
19. Air Liquide. Air Liquide launches LENOXe™.Available at: www.airliquide.com/en/rss/air-liquide-launches-lenoxe.html. AccessedDecember 19, 2013
20. Altes TA, Rehm PK, Harrell F, Salerno M,Daniel TM, De Lange EE. Ventilation imagingof the lung: comparison of hyperpolarizedhelium-3 MR imaging with Xe-133 scintig-raphy. Acad Radiol. 2004;11(7):729–734
21. Chakkarapani E, Thoresen M, Hobbs CE,Aquilina K, Liu X, Dingley J. A closed-circuitneonatal xenon delivery system: a technicaland practical neuroprotection feasibilitystudy in newborn pigs. Anesth Analg. 2009;109(2):451–460
22. Faulkner S, Bainbridge A, Kato T, et al. Xenonaugmented hypothermia reduces earlylactate/N-acetylaspartate and cell death inperinatal asphyxia. Ann Neurol. 2011;70(1):133–150
23. Chakkarapani E, Thoresen M, Liu X, WalloeL, Dingley J. Xenon offers stable haemody-namics independent of induced hypother-mia after hypoxia-ischaemia in newbornpigs. Intensive Care Med. 2012;38(2):316–323
24. Reddy SV. Effect of general anesthetics onthe developing brain. J Anaesthesiol ClinPharmacol. 2012;28(1):6–10
25. Sabir H, Bishop S, Cohen N, et al. Neitherxenon nor fentanyl induces neuroapoptosisin the newborn pig brain. Anesthesiology.2013;119(2):345–357
26. Thoresen M, Liu X, Tooley J, Chakkarapani E,Dingley J. First human use of 50% xenon
inhalation during hypothermia for neonatalhypoxic-ischemic encephalopathy: the “Coolxenon”Feasibility Study. Platform Presentation:Pediatric Academic Society Meeting; April30–May 3 2011; Denver, CO
27. Sarnat HB, Sarnat MS. Neonatal encepha-lopathy following fetal distress. A clinicaland electroencephalographic study. ArchNeurol. 1976;33(10):696–705
28. Bayley N. Bayley Scales of Infant Devel-opment II.. San Antonio, TX: PsychologicalCorporation/Harcourt, Brace & Co; 1993
29. Grunau RV, Craig KD. Pain expression inneonates: facial action and cry. Pain. 1987;28(3):395–410
30. Yon JH, Daniel-Johnson J, Carter LB, Jevtovic-Todorovic V. Anesthesia induces neuronalcell death in the developing rat brainvia the intrinsic and extrinsic apoptoticpathways. Neuroscience. 2005;135(3):815–827
31. Liu X, Dingley J, Elstad M, Scull-Brown E,Steen PA, Thoresen M. Minimum alveolarconcentration (MAC) for sevoflurane andxenon at normothermia and hypothermiain newborn pigs. Acta Anaesthesiol Scand.2013;57(5):646–653
32. Goto T, Saito H, Nakata Y, et al. Effects ofxenon on the performance of various re-spiratory flowmeters. Anesthesiology. 1999;90(2):555–563
33. Baumert JH, Reyle-Hahn M, Hecker K,Tenbrinck R, Kuhlen R, Rossaint R. Increasedairway resistance during xenon anaes-thesia in pigs is attributed to physicalproperties of the gas. Br J Anaesth. 2002;88(4):540–545
34. Calzia E, Stahl W, Handschuh T, et al. Re-spiratory mechanics during xenon anesthe-sia in pigs: comparison with nitrous oxide.Anesthesiology. 1999;91(5):1378–1386
35. Zhang P, Ohara A, Mashimo T, Imanaka H,Uchiyama A, Yoshiya I. Pulmonary re-sistance in dogs: a comparison of xenonwith nitrous oxide. Can J Anaesth. 1995;42(6):547–553
36. Weiss M, Dullenkopf A, Fischer JE, Keller C,Gerber AC; European Paediatric Endotra-cheal Intubation Study Group. Prospectiverandomized controlled multi-centre trial ofcuffed or uncuffed endotracheal tubes insmall children. Br J Anaesth. 2009;103(6):867–873
37. Ishiguro Y, Saito H, Nakata Y, et al. Effect ofxenon on endotracheal tube cuff. J ClinAnesth. 2000;12(5):371–373
38. De Rossi L, Gott K, Horn N, Hecker K,Hutschenreuter G, Rossaint R. Xenon pre-serves neutrophil and monocyte function in
ARTICLE
PEDIATRICS Volume 133, Number 5, May 2014 817 at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

human whole blood. Can J Anaesth. 2002;49(9):942–945
39. de Rossi LW, Brueckmann M, Rex S,Barderschneider M, Buhre W, Rossaint R.Xenon and isoflurane differentially modu-late lipopolysaccharide-induced activationof the nuclear transcription factor KB andproduction of tumor necrosis factor-alpha
and interleukin-6 in monocytes. AnesthAnalg. 2004;98(4):1007–1012
40. Ma D, Lim T, Xu J, et al. Xenon precon-ditioning protects against renal ischemic-reperfusion injury via HIF-1alpha activation.J Am Soc Nephrol. 2009;20(4):713–720
41. Irani Y, Pype JL, Martin AR, et al. Noble gas(argon and xenon)-saturated cold storage
solutions reduce ischemia-reperfusion in-jury in a rat model of renal transplantation.Nephron Extra. 2011;1(1):272–282
42. Baumert JH, Hein M, Gerets C, Baltus T,Hecker KE, Rossaint R. The effect of xenonanesthesia on the size of experimentalmyocardial infarction. Anesth Analg. 2007;105(5):1200–1206
(Continued from first page)
www.pediatrics.org/cgi/doi/10.1542/peds.2013-0787
doi:10.1542/peds.2013-0787
Accepted for publication Feb 12, 2014
Address correspondence to Marianne Thoresen, PhD, Professor of Neonatal Neuroscience Department of Neonatal Neuroscience Level D, St Michael’s Hospital,Southwell Street, Bristol BS2 8EG UK. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Dingley is a director (unpaid) of a university startup company interested in the development of efficient gas delivery systems. Thecompany owns intellectual property in this field that the researchers were permitted to include in the xenon breathing system design. The company did notmanufacture, pay for, or provide any equipment for this study. The other authors have indicated they have no financial relationships relevant to this article todisclose.
FUNDING: This research was funded by SPARKS (Sport Aiding Medical Research for Kids) (05BTL01).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
818 DINGLEY et al at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-0787; originally published online April 28, 2014; 2014;133;809Pediatrics
Chakkarapani, Hemmen Sabir and Marianne ThoresenJohn Dingley, James Tooley, Xun Liu, Emma Scull-Brown, Maja Elstad, Ela
Encephalopathy: A Feasibility StudyXenon Ventilation During Therapeutic Hypothermia in Neonatal
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/133/5/809.full.htincluding high resolution figures, can be found at:
Supplementary Material
2/peds.2013-0787.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2014/04/2Supplementary material can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/133/5/809.full.htat:This article cites 39 articles, 6 of which can be accessed free
Subspecialty Collections
_disorders_subhttp://pediatrics.aappublications.org/cgi/collection/neurologicNeurologic Disorders
_subhttp://pediatrics.aappublications.org/cgi/collection/neurologyNeurology
gy_subhttp://pediatrics.aappublications.org/cgi/collection/neonatoloNeonatology
orn_infant_subhttp://pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infantthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at University of Bristol Library on September 30, 2014pediatrics.aappublications.orgDownloaded from
Related Documents











