www.metcardio.org LINEE GUIDA LINEE GUIDA SULLE SULLE DISLIPIDEMIE DISLIPIDEMIE Giuseppe Biondi Zoccai Giuseppe Biondi Zoccai Professore Aggregato Professore Aggregato Dipartimento di Medicina Interna Dipartimento di Medicina Interna Università di Torino Università di Torino Divisione di Cardiologia 1 Divisione di Cardiologia 1 A.O.U. San Giovanni Battista “Molinette” A.O.U. San Giovanni Battista “Molinette” Torino Torino

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.metcardio.org
LINEE GUIDA SULLE LINEE GUIDA SULLE DISLIPIDEMIEDISLIPIDEMIE
Giuseppe Biondi ZoccaiGiuseppe Biondi Zoccai
Professore AggregatoProfessore AggregatoDipartimento di Medicina InternaDipartimento di Medicina Interna
Università di Torino Università di Torino
Divisione di Cardiologia 1Divisione di Cardiologia 1A.O.U. San Giovanni Battista “Molinette”A.O.U. San Giovanni Battista “Molinette”
TorinoTorino

www.metcardio.org
E’ UTILE RIDURRE IL COLESTEROLO?
0 4 8 12 16 20 24 28 32 36–1,0
–0,8
–0,6
–0,4
–0,2
–0,0
Mortalità per CHD, p=0.012
Mortalità totale, p=0.04
Riduzione di colesterolo totale (%)
Ridu
zion
e di
mor
talit
à,
log
odds
ratio
Gould AL , Circulation 1998;97:946–952
Meta-analisi di 38 studi di prevenzione primaria e secondaria con più di 98.000 pazienti

www.metcardio.org
EFFETTI DEL TRATTAMENTO DELLE DISLIPIDEMIE
1% di riduzionedel C-LDL
riduce il rischio di CHD dell’1%
1% di aumentodel C-HDL riduce il rischio di CHD
del 3%

www.metcardio.org
INCIDENZA DI EVENTI IN FUNZIONE DI C-LDL NEI TRIAL CON STATINE
LDL-C, livelli raggiunti, mg/ dL (mmol/ L)
WOSCOPS – Placebo
AFCAPS - Placebo
ASCOT - PlaceboAFCAPS - Rx WOSCOPS - Rx
ASCOT - Rx
4S - Rx
HPS - Placebo
LIPID - Rx
4S - Placebo
CARE - Rx
LIPID - Placebo
CARE - Placebo
HPS - Rx
0
5
10
15
20
25
30
40(1.0)
60(1.6)
80(2.1)
100(2.6)
120(3.1)
140(3.6)
160(4.1)
180(4.7)
6
Prevenzione Secondaria
Prevenzione Primaria
Rx - Statin therapyPRA – pravastatinATV - atorvastatin
200(5.2)
PROVE-IT - PRATNT – ATV10
TNT – ATV80

www.metcardio.org
COSA FARE ALLORA?

www.metcardio.org
RUOLO DELLA DIETA/STILE DI VITA
• Alimentazione sana frutta, vegetali, cereali, pesce, legumi, carni bianche
• Appropriato peso corporeorapporto corretto tra iapporto e consumo energetico
• Limitare grassi saturi e colesterolosostituire con grassi insaturi
• Smettere di fumare• Condurre vita attiva
www.metcardio.org
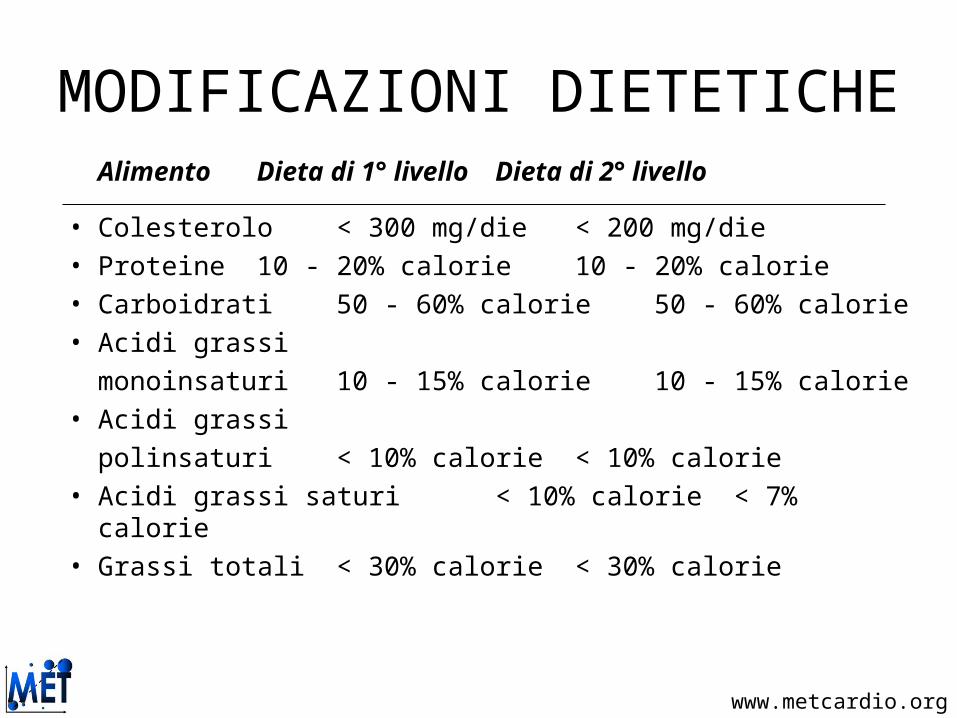
MODIFICAZIONI DIETETICHEAlimento Dieta di 1° livello Dieta di 2° livello
• Colesterolo < 300 mg/die < 200 mg/die• Proteine 10 - 20% calorie 10 - 20% calorie• Carboidrati 50 - 60% calorie 50 - 60% calorie• Acidi grassi
monoinsaturi 10 - 15% calorie 10 - 15% calorie• Acidi grassi
polinsaturi < 10% calorie < 10% calorie• Acidi grassi saturi < 10% calorie < 7% calorie• Grassi totali < 30% calorie < 30% calorie

www.metcardio.org
RUOLO DELL’ESERCIZIO FISICO
Thompson PD, Circulation 2003

www.metcardio.org
RUOLO DELL’ESERCIZIO FISICO
Attività fisica aerobica consigliata:•camminata a passo veloce per 30’, 5
volte a settimana•corsa di almeno 20’, 3 volte a
settimana

www.metcardio.org
COME POSSIAMO RAGGIUNGERE I TARGET DESIDERATI? AGGIUNGENDO, DOPO 3
MESI DI DIETA/STILE DI VITA, I FARMACI
C-LDL
basale
Riduzione richiesta
> 200 > 50%
180-200 45-50%
160-180 40-45%
140-160 30-40%
120-140 20-30%
Grundy SM, Circulation 2004; 110:227-239; Smith S, JACC 2006; 2130-2139; M. Bucci, A. Mezzetti, per conto della SISA sezione Abruzzo
RISCHIO ELEVATO:
TARGET C-LDL < 100 MG/DL
RISCHIO MOLTO ELEVATO:
TARGET C-LDL < 70 MG/DL
C-LDL
basale
Riduzione richiesta
> 200 > 50%
180-200 > 50%
160-180 > 50%
140-160 > 50%
120-140 40-50%

www.metcardio.org
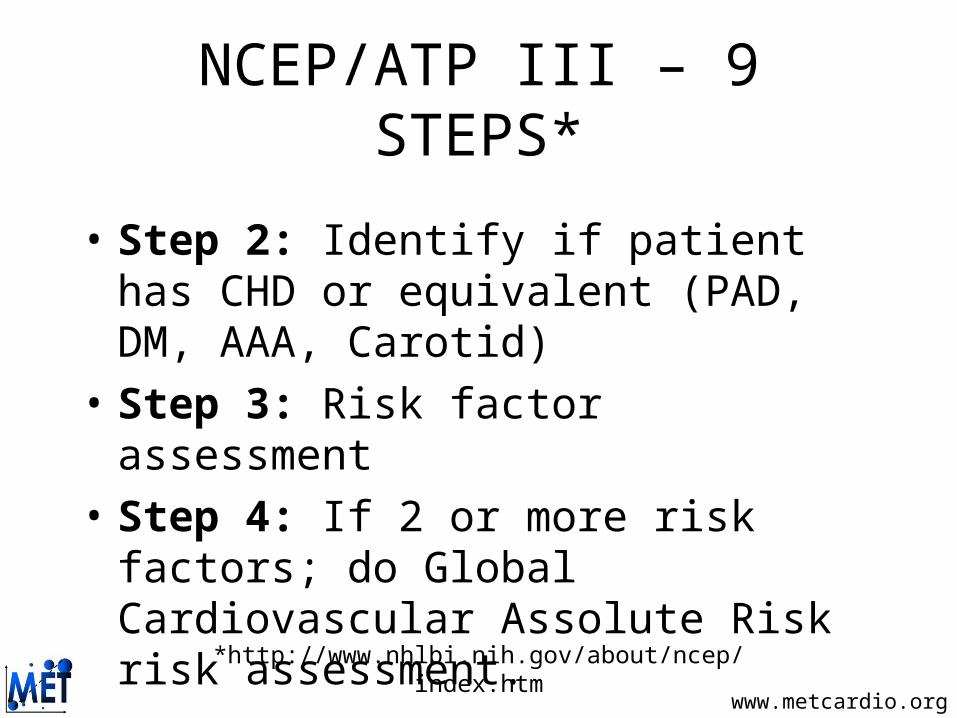
NCEP/ATP III – 9 STEPS*
• Step 1: Obtain, complete & fasting lipids• Interpret: LDL < 100mg/dl optimal LDL 100-129 near optimal LDL 130-159 borderline high LDL 160-189 high LDL >190 very high (mg/dl x 0.0259mmol/l = SI units)
*http://www.nhlbi.nih.gov/about/ncep/index.htm
www.metcardio.org
• Step 2: Identify if patient has CHD or equivalent (PAD, DM, AAA, Carotid)
• Step 3: Risk factor assessment• Step 4: If 2 or more risk factors; do Global
Cardiovascular Assolute Risk risk assessment.
NCEP/ATP III – 9 STEPS*
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
RISCHIO CARDIOVASCOLARE GLOBALE ASSOLUTO*
*http://www.cuore.iss.it/

www.metcardio.org
NCEP/ATP III – STEP 5*
Risk category LDL goal Start lifestyle changes
Start drug treatment
CHD/10yr risk>20%
(high)
<100mg/dl >100mg/dl >100 – 129mg/dl
2+RF or10yr<20%(Medium)
<130mg/dl >130mg/dl >130 – 160mg/dl
0-1 risk factors (low)
<160mg/dl >160mg/dl >160 – 190mg/dl
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
NCEP/ATP III – STEP 6*
• Initiate therapeutic lifestyle changes (TLC) – Diet– Soluble fiber 10-25gm/day– Plant sterols/Sitostanol– Increased exercise– Weight management
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
NCEP/ATP III – STEP 7*• Add drug therapy simultaneously to TLC in
patients with CHD or equivalent. Add drugs after 3 months if TLC not effective in other risk categories:
Ezetimibe, Fibrates, Niacin,
PUFA, Resins, Statins
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
NCEP/ATP III – STEP 8*
• Identify metabolic syndrome: (3 of 5)– SBP>130, FBS>110, TG>150, HDL<40 in men
and <50 in women, waist>40”men, 35”womenAggressively:– Treat underlying causes of overweight and
physical inactivity.– Treat HTN, use ASA for CHD patients
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
NCEP/ATP III – STEP 9*
• Treat elevated TG (>150mg/dl)– First lower LDL; if TG still >200 consider
adding/increasing drug therapy– But, if TG >500mg/dl, first lower triglycerides
to prevent pancreatitis. When they are <500 then return to LDL lowering
– Treat HDL <40 after lowering LDL.
*http://www.nhlbi.nih.gov/about/ncep/index.htm

www.metcardio.org
TARGET RACCOMANDATI: EUROPA VS. USA

www.metcardio.org
High Risk
CHD or CHD risk equivalents
(10-yr risk >20%)
LD
L-C
leve
l
100 -
160 -
130 -
190 -
Lower Risk
< 2 risk factors
Moderately High Risk
≥ 2 risk factors
(10-yr risk 10-20%)
Target 160
mg/dLTarget
130mg/dL
70 -
Target 100
mg/dL
or optional
70 mg/dL*
Moderate Risk
≥ 2 risk factors
(10-yr risk <10%)
Target 130
mg/dL
or optional
100 mg/dL**
Grundy SM et al. Circulation 2004;110:227-239.
ULTIMI TARGET
*Therapeutic option in very high-risk patients and in patients with high TG, non-HDL-C<100 mg/dL;**Therapeutic option; 70 mg/dL =1.8 mmol/L; 100 mg/dL = 2.6 mmol/L; 130 mg/dL = 3.4 mmol/L; 160 mg/dL = 4.1 mmol/L
www.metcardio.org
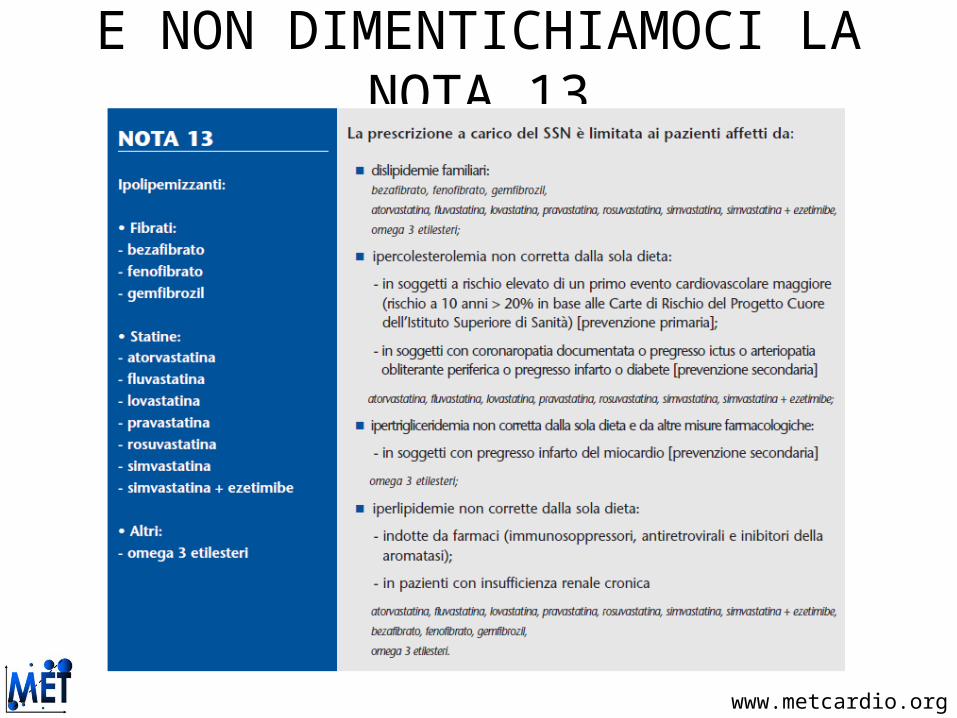
E NON DIMENTICHIAMOCI LA NOTA 13
www.metcardio.org
TAKE HOME MESSAGES
www.metcardio.org
TAKE HOME MESSAGES• Nei soggetti ad alto rischio1 con LDL < 150 mg/dL
(per i quali basta una riduzione di LDL del 35-40%) dopo >3 mesi di dieta, appare opportuno prescrivere statine a potenza moderata (ad esempio simvastatina 20-40 o pravastatina 40-80)
• Nei soggetti a rischio molto alto,2 o ad alto rischio ma con LDL > 150 mg/dL (per i quali è necessaria una riduzione di LDL > 35-40%) nonostante >3 mesi di dieta, è opportuno prescrivere statine a potenza elevata (ad esempio atorvastatina 20-80 o rosuvastatina 10-40)
1. rischio cardiovascolare globale a 10 anni >20%2. SCA, ictus recente, recente PTCA/CABG, o CHD+DM

www.metcardio.org
Grazie della Vostra attenzione
Per qualsiasi informazione: [email protected]
Queste e altre slides pertinenti sono disponibili sul sito web metcardio.org:
http://www.metcardio.org/slides.html
www.metcardio.org
RESERVE SLIDES

www.metcardio.org
EFFETTI BENEFICI DELLA DIETA

www.metcardio.org
TIPO DI DIETA
www.metcardio.org
TIPO DI DIETA

www.metcardio.org
LINEE GUIDA PERTINENTI

www.metcardio.org
NCEP-ATP III

www.metcardio.org
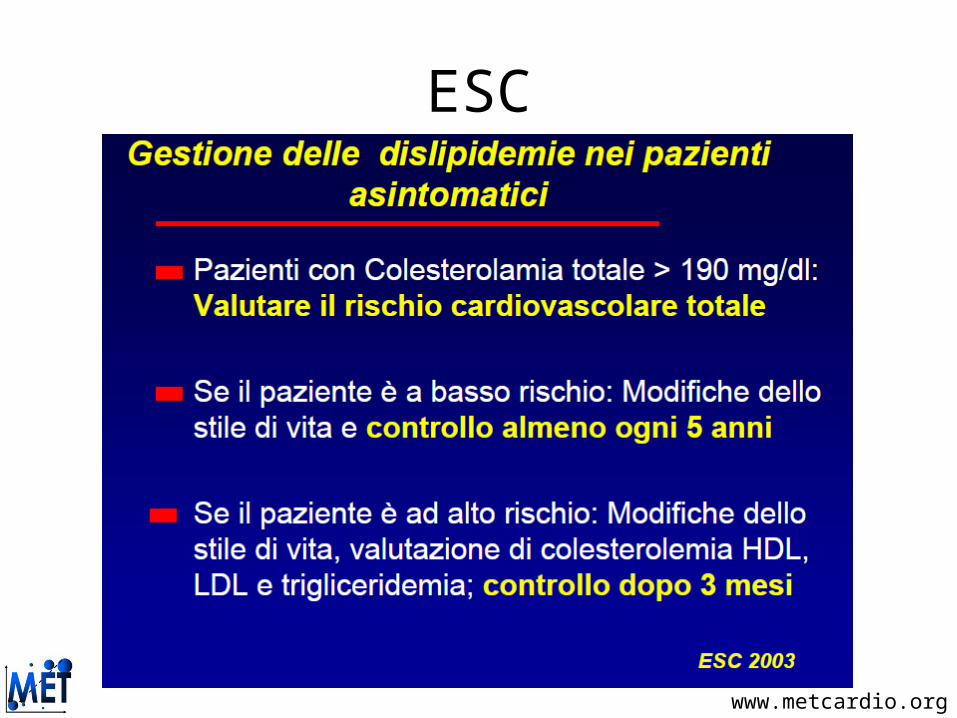
ESC
www.metcardio.org
ESC

www.metcardio.org
ESC

www.metcardio.org
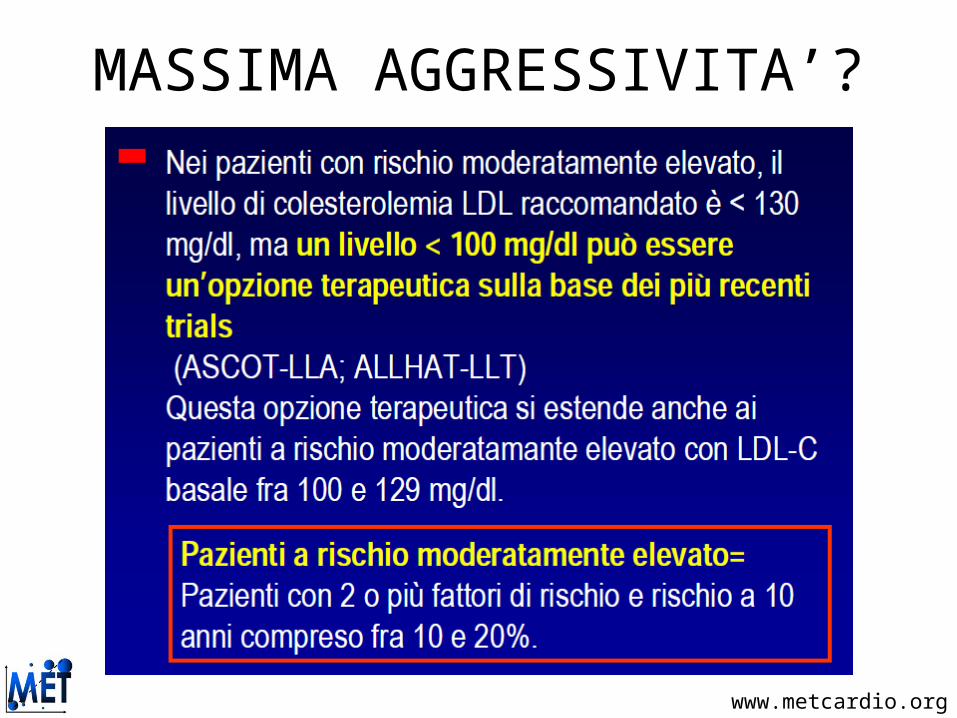
MASSIMA AGGRESSIVITA’?
www.metcardio.org
MASSIMA AGGRESSIVITA’?
Related Documents