2013 Bound Volume 2 Issue 1-4: 1-191 World Journal of Obstetrics and Gynecology World J Obstet Gynecol 2013 November 10; 2(4): 62-191 ISSN 2218-6220 (online) www.wjgnet.com www.wjgnet.com Volume End World Journal of Obstetrics and Gynecology World J Obstet Gynecol 2013 February 10; 2(1): 1-7 ISSN 2218-6220 (online) www.wjgnet.com www.wjgnet.com World Journal of Obstetrics and Gynecology World J Obstet Gynecol 2013 May 10; 2(2): 8-36 ISSN 2218-6220 (online) www.wjgnet.com www.wjgnet.com World Journal of Obstetrics and Gynecology ISSN 2218-6220 (online) World Journal of Obstetrics and Gynecology World J Obstet Gynecol 2013 August 10; 2(3): 37-61 ISSN 2218-6220 (online) www.wjgnet.com www.wjgnet.com www.wjgnet.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

2013 Bound Volume 2 Issue 1-4: 1-191
World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 November 10; 2(4): 62-191
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
Volume End
World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 February 10; 2(1): 1-7
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 May 10; 2(2): 8-36
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
World Journal of Obstetrics and Gynecology
ISSN 2218-6220 (online)
World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 August 10; 2(3): 37-61
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
www.wjgnet.com

World Journal ofObstetrics and GynecologyW J O G
EDITOR-IN-CHIEFBo Jacobsson, Gothenburg
GUEST EDITORIAL BOARD MEMBERSWing P Chan, TaipeiChie-Pein Chen, TaipeiShi-Yann Cheng, YulinSong-Nan Chow, TaipeiPeng-Hui Wang, Taipei
MEMBERS OF THE EDITORIAL BOARD
Australia
Ashwini Chand, MelbourneSteven D Fleming, BrisbaneAnkit Jain, Coffs HarbourMarjan Khajehei, ComoGavin Sacks, SydneyJing Sun, Brisbane
Austria
Susanne Huber, ViennaEdgar Petru, Graz
Belgium
Marc FD Baay, AntwerpChristophe Blockeel, BrusselsYves Jacquemyn, EdegemEkaterine Tskitishvili, LiegeJan Baptist Vermorken, Edegem
Brazil
Carlos KB Ferrari, Barra do GarçasWellington P Martins, Ribeirão PretoFernando M Reis, Belo HorizonteMaria Inês Rosa, CriciúmaCicero de Andrade Urban, Curitiba
Canada
Emmanuel Bujold, QuébecPaul James Hoskins, Vancouver
Chile
Patricio E Donoso, Santiago
China
Cherng-Jye Jeng, NanjingJian-Xin Li, NanjingErnest Hung Yu Ng, Hong KongDan Xie, Guangzhou
Egypt
Hesham E Abdel-Hady, MansouraAhmed S El Hefnawy, MansouraAhmed Nasr, Assiut
Finland
Johan O Fellman, Helsinki
Kari Juhani Syrjanen, Turku
France
Cherif Y Akladios, StrasbourgSouhail Alouini, Orleans
Germany
Safaa H Al-Hasani, Luebeck
Greece
Georgios P Artsinevelos, AthensByron Asimakopoulos, AlexandroupolisAnastasios Athanasopoulos, PatraPanagiotis Christopoulos, AthensChristos R Iavazzo, AthensIoannis E Messinis, LarissaAthanasios PG Papatsoris, AthensKitty Pavlakis, AthensKonstantinos A Toulis, ThessalonikiPanagiotis PT Tsikouras, AlexandroupolisMenelaos Zafrakas, Thessaloniki
Hungary
Jozsef Gabor Joo, Budapest
India
Chinmoy K Bose, KolkataPralhad Kushtagi, Mangalore
I
Editorial Board2012-2016
The World Journal of Obstetrics and Gynecology Editorial Board consists of 178 members, representing a team of worldwide experts in obstetrics and gynecology. They are from 40 countries, including Australia (6), Austria (2), Belgium (5), Brazil (5), Canada (2), Chile (1), China (9), Egypt (3), Finland (2), France (2), Germany (1), Greece (11), Hungary (1), India (3), Iran (3), Israel (6), Italy (13), Japan (6), Jordan (2), Lithuania (1), Malaysia (1), Mexico (1), Moldova (1), Netherlands (3), Nigeria (1), Norway (2), Poland (1), Portugal (1), Qatar (1), Saudi Arabia (3), Serbia (1), Slovenia (1), South Korea (3), Spain (4), Sweden (2), Thailand (3), Turkey (8), United Kingdom (10), United States (46), and Venezuela (1).
February 10, 2013WJOG|www.wjgnet.com

Niraj N Mahajan, Mumbai
Iran
Hossein Fallahzadeh, YazdAbbas A Ghaderi, ShirazRamesh Omranipour, Tehran
Israel
Zeev Blumenfeld, HaifaSorina Grisaru-Granovsky, JerusalemAlexander Ioscovich, JerusalemMarwan Odeh, NahariyaEyal Sheiner, Beer-ShevaJohnny S Younis, Tiberias
Italy
SML Chamayou, Sant’Agata Li BattiatiFederico Coccolini, BergamoErich Cosmi, PaduaVassilios Fanos, CagliariRoberta Granese, MessinaAnna Maria Marconi, MilanoFilippo Murina, MilanFelice Petraglia, SienaGiuseppe Rizzo, RomeEmilio Sacco, RomeGiulio Aniello Santoro, TrevisoAndrea Tinelli, LeceEmanuela Turillazzi, Foggia
Japan
Madoka Furuhashi, NagoyaTakeshi Maruo, KobeKaei Nasu, OitaYuzuru Niibe, SagamiahraKenzo Sonoda, FukuokaYoshihito Yokoyama, Hirosaki
Jordan
Moamar I Al-Jefout, MutahZouhair O Amarin, Irbid
Lithuania
Linas Rovas, Klaipeda
Malaysia
Geok Chin Tan, Kuala Lumpur
Mexico
Alfonso Dueñas-González, Mexico City
Moldova
Fanuel Lampiao, Blantyre
Netherlands
Marieke J Claas, UtrechtWendy Koster, UtrechtArnold-Jan Kruse, Maastricht
Nigeria
Chibuike O Chigbu, Enugu
Norway
Andrej M Grjibovski, OsloSvein Rasmussen, Bergen
Poland
Andrzej Wincewicz, Kielce
Portugal
Renato Manuel Natal Jorge, Porto
Qatar
Sajjad ur Rahman, Doha
Saudi Arabia
Ismail Al-Badawi, RiyadhMamdoh Eskandar, AbhaHans-Juergen Schulten, Jeddah
Serbia
Miroslava G Gojnic Dugalic, Belgrade
Slovenia
Spela Smrkolj, Ljubljana
South Korea
Kwang-Hyun Baek, SeongnamMin Hyung Jung, SeoulSue Kyung Park, Seoul
Spain
J de la Torre Fernandez de Vega, TenerifeAntonio Pinero Madrona, MurciaSantiago Palacios, Madrid
Faustino R Perez-Lopez, Zaragoza
Sweden
Eva Marie Wiberg-Itzel, Stockholm
Thailand
Pisake NA Lumbiganon, Khon KaenVorapong Phupong, BangkokViroj Wiwanitkit, Bangkok
Turkey
Metin Akbulut, DenizliCem Baykal, IstanbulHusnu Celik, ElazigCem Dane, IstanbulPolat Dursun, AnkaraErdin İlter, İstanbulMehmet Kefeli, SamsunKamile Kukulu, Antalya
United Kingdom
Mohamed Abdel-fattah, AberdeenSuha Deen, NottinghamStergios K Doumouchtsis, LondonMona A El-Bahrawy, LondonAlaa A El-Ghobashy, WolverhamptonAyman AA Ewies, BirminghamMyra S Hunter, LondonPaul D Losty, LiverpoolTim Mark Reynolds, Burton-on-TrentAriel Zosmer, London
United States
Muktar H Aliyu, NashvilleM Robyn Andersen, SeattlePriya R Bhosale, HoustonDonald P Braun, ZionChunxia Cao, GainesvilleWally A Carlo, BirminghamLinda R Chambliss, PhoenixTeresa P Diaz-Montes, BaltimoreSteven M Donn, Ann ArborOmar F Duenas, New YorkMarilyn B Escobedo, OklahomaRobert Freedman, DetroitSergio G Golombek, ValhallMichael P Goodman, DavisDiane M Harper, KansasMatthew H Ho, Los AngelesPatricia B Hoyer, TucsonMei-Hua Huang, Los AngelesWilliam W Hurd, ClevelandGabor B Huszar, New HavenAmer K Karam, Los AngelesJustin P Lavin, AkronLinda E May, KansasZaher Merhi, BronxNash S Moawad, GainesvilleLisa Eileen Moore, AlbuquerqueRobert D Moore, Atlanta
II February 10, 2013WJOG|www.wjgnet.com

III February 10, 2013WJOG|www.wjgnet.com
David Gardner Mutch, St. LouisNihar R Nayak, Palo AltoAnita L Nelson, Manhattan BeachFarr Nezhat, New YorkRobert W Powers, PittsburghWerner Schaefer, PittsburghGerald Phillip Schatten, PittsburghDanny Joseph Schust, Columbia
Hen Yitzhak Sela, New YorkElizabeth S Ginsburg, New YorkSherri Lynn Stewart, AtlantaRobert S Tan, HoustonPing Tang, RochesterIhab Mohammed Usta, New YorkJian-Jun Wei, ChicagoXiuquan Zhang, Salt Lake
Chengquan Zhao, PittsburghYulian Zhao, BaltimoreWenxin Zheng, Tucson
VenezuelaMaría E Aponte-Rueda, Caracas

World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 February 10; 2(1): 1-7
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
1 Burdenofgynaecologicalcancersindevelopingcountries
Iyoke CA, Ugwu GO
Contents
IWJOG|www.wjgnet.com February 10, 2013|Volume 2|Issue 1|
MINIREVIEWS
World Journal ofObstetrics and GynecologyW J O G
Quarterly Volume 2 Number 1 February 10, 2013

ContentsWorld Journal of Obstetrics and Gynecology
Volume 2 Number 1 February 10, 2013
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Shuai Ma Responsible Science Editor: Su-Xin GouResponsible Electronic Editor: Jun-Yao LiProofing Editor-in-Chief: Lian-Sheng Ma
World Journal of Obstetrics and GynecologyRoom 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected]://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza, 315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188Telephone: +852-31779906E-mail: [email protected]://www.wjgnet.com
PUBLICATIONDATEFebruary 10, 2013
COPYRIGHT© 2013 Baishideng. Articles published by this Open-Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial Li-cense, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in this journal represent the view-points of the authors except where indicated otherwise.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm.
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
IIWJOG|www.wjgnet.com
APPENDIX
ABOUT COVER
AIM AND SCOPE
FLYLEAF
February 10, 2013|Volume 2|Issue 1|
NAMEOFJOURNALWorld Journal of Obstetrics and Gynecology
ISSNISSN 2218-6220 (online)
LAUNCHDATEJune 10, 2012
FREQUENCYQuarterly
EDITOR-IN-CHIEFBo Jacobsson, MD, PhD, Professor, Department Obstetrics and Gynecology, Sahlgrenska University Hospital/Ostra, SE-416 85 Gothenburg, Sweden
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice Director
I-V Instructionstoauthors
WorldJournalofObstetricsandGynecology EditorialBoardMember,Danny
JosephSchust,MD,AssociateProfessor,CenterforReproductiveMedicineand
Fertility,DepartmentofObstetrics,GynecologyandWomen’sHealth,University
ofMissouriSchoolofMedicine,500NorthKeeneStreet,Suite203,Columbia,MO
65201,UnitedStates
World Journal of Obstetrics and Gynecology (World J Obstet Gynecol, WJOG, online ISSN 2218-6220, DOI: 10.5317) is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJOG covers topics concerning pregnancy complications, obstetric surgical procedures, diagnostic imaging, endoscopy, reproductive endocrinology, tumors, pelvic diseases, evidence-based medicine, epidemiology and nursing.
We encourage authors to submit their manuscripts to WJOG. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Obstetrics and Gynecology is now indexed in Digital Object Identifier.
I-III EditorialBoard
INDEXING/ABSTRACTING

Burden of gynaecological cancers in developing countries
Chukwuemeka Anthony Iyoke, George Onyemaechi Ugwu
Chukwuemeka Anthony Iyoke, Department of Obstetrics and Gynaecology, University Hospital of Wales, Heath Park, Cardiff CF14 4XN, United KingdomGeorge Onyemaechi Ugwu, Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu 4000001, NigeriaAuthor contributions: Iyoke CA conducted the literature re-view and drafted the manuscript; Ugwu GO reviewed and added intellectual content to the manuscript.Correspondence to: Dr. Chukwuemeka Anthony Iyoke, De-partment of Obstetrics and Gynaecology, University Hospital of Wales, Heath Park, Cardiff CF14 4XN, United Kingdom. [email protected]: +44-117-9043422 Fax: +44-117-9043444Received: June 22, 2012 Revised: November 7, 2012Accepted: December 15, 2012Published online: February 10, 2013
Abstract Approximately 1:4 of all cancers in women in develop-ing countries (excluding non-melanoma skin cancer) is a gynaecological cancer. The gynaecological cancer burden in developing countries is huge primarily due to the high incidence and mortality of cervical cancer. Cervical cancer accounts for over 60% of the gynaeco-logical cancer burden in developing countries despite being preventable by current technologies. This is due to the absence of effective nationally organized screening programmes in most developing countries. Institution of such programmes, therefore, has the potential to dramatically reduce gynaecological cancer burden in these countries. Subsidized human papil-loma virus (HPV) vaccine and HPV typing as well as cheap screening techniques such as visual inspection aided with acetic acid hold the key to effective preven-tion of cervical cancer in these countries. This is be-cause a significant proportion of patients in developing countries are unable to access and avail themselves of the few available preventive, diagnostic and treatment services because of poverty. Although, advocacy and the political will to invest in the development of human resources and healthcare infrastructure appear criti-
cal to gynaecological cancer control and reducing the burden of disease in many developing countries, the proposition assumes that resources are truly available for this investment. This may not be true. Many devel-oping countries rely on foreign aids for developmental programmes and these aids have dwindled significantly with the current global economic meltdown.
© 2013 Baishideng. All rights reserved.
Key words: Gynaecological cancer; Cancer burden; Can-cer mortality; Cancer morbidity; Cancer prevention
Iyoke CA, Ugwu GO. Burden of gynaecological cancers in developing countries. World J Obstet Gynecol 2013; 2(1): 1-7 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i1/1.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i1.1
INTRODUCTIONEmerging global trend in the burden of cancer Cancer is the second leading cause of death and disability worldwide, behind only heart disease[1]. More people die from cancer every year than human immunodeficiency virus (HIV), tuberculosis and malaria combined[1-4]. Con-trary to about three decades ago when cancer was more prevalent in the developed world, the burden is shifting significantly to the developing countries. According to estimates by the International Agency for Research on Cancer (IARC), in 2008, 53% of the 12.7 million new cases of cancer and 63% of the 7.6 million cancer deaths occurred in developing countries[3]. Three decades earlier, developing countries accounted for a mere 15% of global cancer burden[4]. A recent report based on the IARC/GLOBOCAN 2002 world cancer statistics estimated that by the year 2020, about 10.25 million new cases of cancer would be diagnosed in the developing countries com-pared to 5.94 million in the developed countries[1]. This trend is quite disturbing for many reasons including the fact that it will, no doubt, compound the already existing
MINIREVIEWS
� February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Online Submissions: http://www.wjgnet.com/esps/[email protected]:�0.53�7/wjog.v2.i�.�
World J Obstet Gynecol 20�3 February �0; 2(�): �-7ISSN 22�8-6220 (online)
© 20�3 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G

formidable health and human developmental challenges posed by poverty, weak economies and high prevalences of communicable diseases in developing countries.
Explanations given for the increasing burden of can-cer currently observed in developing countries have been based largely on epidemiological data and empirical ob-servations. Reasons often cited include a shift in develop-ing countries to Western lifestyle and behaviors such as cigarette smoking, low fiber/high fat diets and less physi-cal activity[5]; high prevalence of immunosuppressing conditions such as malnutrition, tuberculosis and HIV[6]; high prevalence of oncogenic infections such as hepatitis B virus, HIV, hepatitis C virus, human papilloma virus (HPV), Helicobacter pylori[5]. We observe that it is also pos-sible that increasing health awareness in these countries has facilitated resort to orthodox medical care resulting in more persons with cancer reporting to hospitals for care, rather than seeking care from herbalists and other forms of alternative health care. Whether the increased documentation of cancer in developing countries is due to actual increase in disease incidence or reporting bias, cancer has become a new challenge to the health systems in developing countries.
Definition of operative conceptsDeveloping countries: For the purpose of this review, the term developing countries refers to countries clas-sified by the World Bank as middle and low income countries in their classification of economies in 2009[7]. These countries had gross national income per capita of USD 12 275 or below[7]. Developing countries are by no means homogenous with respect to all indices of devel-opment. However, they are generally characterized by low standard of living (including poor access to health care, poor sanitation, poor access to safe drinking water and poor nutrition); underdeveloped industrial base and low human development index (including low level of literacy, low life expectancy, high infant and maternal mortality)[8]. They include most countries of sub-Saharan Africa, South and South East Asia, Latin and South America.
Burden of cancer: For the burden of cancer, the epide-miological definition of the burden of cancer as described by Sankaranarayanan et al[9] was used in this review. For economic burden, the economic definition described by Kim et al[10] was adopted. Accordingly, the epidemiological indices of burden of gynaecological cancer used in this review include cancer incidence, mortality and case fatality while the economic definition involves the economic cost of the cancer (including medical costs, nonmedical costs and the cost due to loss of productivity)[9,10].
Sources of dataThe information contained in this review were obtained through electronic literature search conducted in major data bases including PubMed, Medline, EMBASE, Sco-pus, Cochrane database and central register of controlled
trials using the following search terms individually and in combination: gynaecological cancer, cancer in develop-ing countries, burden of gynaecological cancer, cancer, cancer burden, cancer in sub-Saharan Africa, South Asia, Latin America, South America, the Caribbean, economic burden of cancer, cervical cancer, ovarian cancer, corpus cancer, vulval cancer, vaginal cancer, choriocarcinoma. All relevant peer-reviewed English language articles and publications were identified, retrieved and reviewed. We also obtained further articles by reviewing the bibliogra-phies of the relevant published documents obtained in the primary search of databases. In addition to these, we consulted the website of the IARC for the current ver-sion of the GLOBOCAN world cancer statistics.
Aetiology of gynaecological cancersIn view of the importance of causative factors to any disease burden, it is appropriate to review the aetiological basis of gynaecological cancers. Gynaecological cancers include cancers of the ovary, fallopian tube, uterine body, cervix, vagina and vulva as well as choriocarcinoma which primarily come under the care of gynaecologists and gynaecological oncologists. This review excludes breast cancer because it comes under the specialty of general surgery in most developing countries.
Gynaecological cancers can be epidemiologically grouped into two with respect to aetiology. On the one hand are cervical, vaginal and vulvar cancers which share similarities, first in having known premalignant stages before the development of invasive cancer and secondly in their link with high risk human papilloma virus infec-tion. Chronic infection with this virus is now known to induce premalignant changes in epithelial cells ultimately leading to cancer after several years[11-13]. Human papil-loma virus is a sexually transmitted disease. For cervical cancer, the relationship to HPV and the presence of a recognizable premalignant stage of the disease called cervical intraepithelial neoplasia (CIN) provide multiple planks for preventive efforts[14-17]. Several co- factors are known to modify the effect of chronic HPV infection in the causation of cervical cancer and these include high parity, prolonged use of oral contraceptive pills, multiple sexual partners, cigarette smoking and early age at sexual debut[11]. Vaginal and vulvar cancers are also known to evolve through premalignant phases called vaginal in-traepithelial neoplasia and vulvar intraepithelial neoplasia respectively, but screening for these stages in the popula-tion is not currently recommended[18-20].
On the other hand are ovarian, Fallopian tube and corpus cancers which do not have any known infective aetiology. Most cases of ovarian cancer occur sponta-neously although genetic predisposition is responsible for ovarian cancer in 10% of cases[21]. These hereditary ovarian cancers are associated with inherited germ line mutations in the BRCA-1 and BRCA-2 genes as well as the Lynch type 2 gene associated with hereditary non-polyposis colorectal cancer[21]. Epithelial ovarian cancer is associated with a number of risk factors including a
Iyoke CA et al . Gynaecological cancer in developing countries
2 February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com

family history of ovarian cancer, old age, postmenopausal status and use of hormone replacement therapy[21]. Ovar-ian cancer has been traditionally thought to occur more in developed countries due to the higher prevalence of these epidemiological risk factors[22]. However, it would appear that with recent global cancer estimates, the trend may be reversing[1].
On its part, corpus cancer refers to cancer of the uter-ine body and is mainly endometrial cancer although rarely uterine sarcoma (leiomyosarcoma) may occur. Endome-trial cancer is the third commonest gynaecological cancer in developing countries[1,2]. It is a hormone-dependent cancer and is associated with several epidemiological risk factors, the most significant of which include unopposed estrogen, sedentary lifestyle and obesity[23,24]. Endometrial cancer is thought to evolve through a premalignant stage called endometrial hyperplasia but the natural course of progression from endometrial hyperplasia to endometrial cancer is not clearly understood.
BURDEN OF GYNAECOLOGICAL CANCERSGeneral overviewThe burden of gynaecological cancers in developing countries appears huge. In these countries, gynaecologi-cal cancers account for 25% of all new cancers diag-nosed among women aged up to 65 years compared to 16% in the developed world[25]. According to a recent report, developing countries accounted for 820 265 cases (77.7%) of global estimates for new cases of the com-monest gynaecological cancers including cervical, corpus and ovarian cancer in 2009[1]. This constituted 12.1% of the 6.8 million cases of cancer in developing countries[1]. This review intends to explore the pattern, magnitude and significance of the current burden of gynaecological cancers in developing countries. Specific gynaecological cancers Cervical cancer: Cervical cancer is the commonest gyn-aecological malignancy in developing countries where or-ganized screening programmes do not exist[1,3]. According to the IARC, there were 453 531 cases of cervical cancer in developing countries in 2008 representing 89% of global estimates[3]. Also 273 000 deaths occur worldwide every year due to cervical cancer out of which 83% occur in developing countries[26]. Case fatality rates of cervical cancer are quite high in these countries with case fatalities up to 60% reported[1]. Conversely in developed countries where nationally organized screening programmes exist, cervical cancer is not as common and case fatality rates are as low as 32%[1]. About 80%-95% of cervical cancers are squamous cell carcinoma[9].
Across different regions of the world, developing countries individually report heavy burdens of high in-cidences and mortality from cervical cancer. The highest incidence rates are found in Sub Saharan Africa, Latin America and the Caribbean, South Central and South
East Asia[9]. A report from Nigeria gave the incidence of cervical cancer as 25/100 000 per year which translates to a disease burden for an estimated 32 million women in 2005 to about 8000 cases per year[27]. A recent hospital based study in Lagos Nigeria showed that, overall, cancer was the leading cause of death among gynaecological inpatients and that cervical cancer contributed over 44% to all gynaecological mortality[28]. South and South East Asia are thought to experience over 200 000 new cases of cervical cancer yearly (more than one-third of the global burden)[26]. Age-adjusted cervical cancer mortality rates exceed 15 per 100 000 in most developing countries, with rates as high as 35/100 000 in East Africa[9]. A na-tionwide survey in India published recently evaluated the cause of 122 429 deaths in 1.1 million randomly selected homes across the country between 2001 and 2003: cervi-cal cancer made the highest contribution to cancer deaths among women at 17.5%[29]. In Latin America and the Caribbean, Haiti, Nicaragua and Bolivia had the highest mortality due to cervical cancer with rates of 40, 28 and 22 percent respectively[26]. The very high mortality rates of cervical cancer in developing countries are due to the fact that most patients present at advanced clinical stages of the disease, and to the fact that a significant propor-tion of patients do not receive or complete prescribed courses of treatment due to deficiencies in treatment availability, accessibility, and affordability[9].
Ovarian and adnexal cancers: Fallopian tube cancers and extra ovarian primary peritoneal cancers are con-sidered along with ovarian cancer because their biology and clinical characteristics are similar to ovarian cancer[9]. Over 80% of cases of ovarian cancer are epithelial in ori-gin[22,30,31]. Ovarian cancer is the second commonest gyn-aecological cancer in developing countries[9]. It accounts for 18.8% of all gynaecological cancers in developing countries and 28.7% in developed countries[9]. Recent esti-mates indicated that of 240 476 cases of ovarian cancer in 2009, 155 835 (64.8%) occurred in developing countries compared to 84 641 in developed countries[1]. Accounts that ovarian cancer is commoner in developed countries than in developing countries may not, therefore, be sup-ported by the most current estimates. Ovarian cancer has a case-fatality rate of 59.2% in developing countries which is similar to the 54.8% in developed countries[1]. The high case fatality rate of ovarian cancer is primarily due to the fact that the disease only becomes manifest in advanced stages of the disease[30,31].
Corpus cancer: Corpus cancer is commoner in devel-oped countries than in developing countries[23]. In 2009, there were 236 643 cases worldwide out of which 113 486 occurred in developing countries representing ap-proximately 48% of the global burden[3]. Low incidences less than 4/100 000 are found in South Asia and Africa[9]. More than 90% occur in women aged 50 years and above[9]. It has a more favorable prognosis than Ovarian and Cervical cancers with 5-year survival rates around
3 February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Iyoke CA et al . Gynaecological cancer in developing countries

global population contributes 6.4% of new cancer cases and accounts for a mere 0.3% global cancer costs[1].
DISCUSSIONFrom the foregoing, it is clear than the burden of gyn-aecological cancer in developing countries is huge. Con-tending with this challenge demands two vital planks of intervention: generation of representative and accurate data on cancer and the introduction or scaling up of preventive programmes and early detection of cancer through increased funding by all stakeholders.
Population data on cancer from developing countries are prone to inaccuracies. For instance the IARC relies on data from population-based cancer registries to estimate cancer incidences and mortality globally. Such registries are available in only 5% of developing countries - in parts of the developing world where cancer registries exist, they are either regional or hospital registries[9]. In many countries of the developing world, data do not exist at all[9]. For such countries, estimates are usually made from neighbouring countries. Variations in validity and extent of data from different countries are therefore unavoid-able and the actual burden of cancers may be more or less than current quoted figures. Inaccurate data militates against accurate planning of policies and programmes for cancer care and control. It is therefore advocated that the establishment of population based cancer registries be made a priority policy for cancer control in developing countries.
Gynaecological cancer incidences are either be ex-pressed as an absolute number of cases per year which reflects the load of new patients diagnosed in a region or group, or as a rate in terms of number of new cases per 100 000 per year which represents the average risk of developing the disease in a population. Whichever way it is expressed, recent estimates of gynaecological cancer incidences in developing countries show that as much as 64% of the gynaecological cancer burden is due to cer-vical cancer[3]. Cervical cancer control, therefore, holds the key to the reduction in overall gynaecological cancer burden in developing countries. With an estimated case-fatality rate of 55.1%[1], cervical cancer is also the major contributor to gynaecological cancer mortality in devel-oping countries.
Cervical cancer is preventable and curable in the very early stages of the disease. Fortunately, it has a very well known natural history characterized by a long prema-lignant phase which provides a good opportunity for preventive interventions. And among all gynaecological cancers, cervical cancer offers the greatest potential for prevention, early detection and cure[9]. Evidence from the developed world shows that the high incidences of cervi-cal cancer in developing countries are due to lack of or inadequate/inefficient existing screening programmes[34,35].
The central role of HPV infection in the etiology of cervical cancer has led to the introduction of the HPV vaccine and HPV detection and typing in cervical screen-
70% in developing countries[9].
Vaginal cancer: Vaginal cancer is rare and constitutes less than 2% of gynaecological cancers worldwide[9]. Of 13 200 cases globally in 2002, 9000 (68%) occurred in developing countries[9]. Incidence rates do not exceed 0.8/100 000 in any region of the world[9]. Case fatality rate in developing countries is 44.7% compared to 15.4% in the developed world[1]. More than 75% of cases occur in women older than 60 years[9].
Vulva cancer: This constitutes 3% of gynaecological can-cers worldwide[9]. In 2002, there were 26 800 cases out of which 11 100 (41.4%) occurred in developing countries[9]. Incidence rate is less than 1/100 000 in developing coun-tries[9]. More than 50% are seen in women over 70 years and more than two-thirds occur in the labia majora[9].
Choriocarcinoma: This represents 0.6% of all gynae-cological cancers[9]. Approximately 5800 cases occurred worldwide in 2002 out of which 5400 (96.4%) occurred in developing countries[9]. Incidence rates are highest in South East Asia where rates of (0.43-1.7)/100 000 are quoted compared to 0.04/100 000 in Africa and Europe[9].
ECONOMIC BURDEN OF GYNAECOLOGICAL CANCERSThe economic burden of gynaecological cancers can be discussed at the level of individual patients and their families as well as the level of health systems and gov-ernment. Accurate estimation of the actual economic burden of gynecological cancers in developing countries is difficult because studies on the economic burden of gynaecological cancers in these countries are scanty. A few cross-sectional studies document the socio-economic impact of cervical cancer on individuals and families in some developing countries. Arrossi et al[32] in Argentina and Ohaeri et al[33] in Nigeria studied the socioeconomic and psychological impact of cervical cancer. The study in Argentina found that the socioeconomic impact of cervi-cal cancer was considerable and that it had negative con-sequences on treatment compliance[32]. It found that “in addition to facing pain, disability and fear of death, cervi-cal cancer patients had to deal with increased treatment related expenses, loss of employment and consequent income, and changes in household responsibilities”[32].
At the level of government and health systems, studies on the cost of cancer care and control are also scanty. A report based on calculations extrapolated from a study in Korea suggests a huge unmet need for funding of cancer care in developing countries. According to the report, the cost of new gynaecological cancers in developing coun-tries in 2009 totalled USD 1.087 billion[1]. This pales into insignificance when compared to the USD 11.913 billion spent in developed countries[1]. The report clearly shows a huge funding gap in developing countries compared to developed countries[1]. Africa which represents 15% of
� February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Iyoke CA et al . Gynaecological cancer in developing countries

ing[36,37]. Already HPV vaccine is licensed for use in many developing countries, although the cost of the vaccine makes it generally unaffordable. In Nigeria, for instance, it costs the equivalent of USD 100.00 for a course of trivalent HPV vaccine - a country where over 70% of the population live on less than USD 1.0 per day. On its part, HPV detection and typing also require expensive equip-ment and highly skilled manpower that are not gener-ally available in developing countries. Thus like cytology screening which requires a great input of human and ma-terial resources to sustain, nationally organized preventive programmes using HPV vaccine and detection may prove just too expensive for developing countries[38].
It would appear therefore, that cervical cancer control in developing countries will require active scaling up of cheaper screening techniques such as visual inspection with acetic acid which has similar CIN detection rates compared to HPV testing and cervical cytology[3]. Subsi-dizing the cost of HPV vaccine and HPV DNA testing by governments of these countries will go a long way to make them affordable to individuals. It has been sug-gested that linking testing or screening to treatment (screen and treat) without recourse to colposcopy or sophisticated laboratories would potentially prevent cervical cancer in large numbers of women in developing countries[15,39,40].
In the case of ovarian cancer, the burden in develop-ing countries appears to be rapidly evolving with recent estimates suggesting a greater burden than in developed countries[1]. Except in about 10% of cases, ovarian can-cer tends to occur spontaneously. The key to control of ovarian cancer appears to be early detection and treat-ment at the very early stages when cure may be theoreti-cally possible[13].
Screening for ovarian cancer has been evaluated re-cently by several large randomized controlled trials using assay of CA125 and transvaginal ultrasound[41-43]. Results of the prostate, lung, colorectal, and ovarian cancer screening trial in the United States already published in 2011 suggest that whereas screening may decreases the stage at detection[44] and thereby decrease case - specific mortality; it may not decrease disease specific mortality[45]. The methodological flaws in these conclusions have how-ever, been raised in a recent publication[46] and the world awaits the publishing of the final results of the UKC-TOCS trial in 2015 to draw a conclusion as to whether ovarian cancer screening decreases mortality from the disease.
Endometrial cancer is the third commonest gynaeco-logical cancer in developing countries. In order to be pro-active in addressing the current and future burden of this cancer in developing countries, the risk factors that are modifiable such as obesity, sedentary lifestyles and use of unopposed estrogen/estrogen agonists have to be active-ly discouraged[47,48]. Population screening for endometrial cancer is not yet recommended[24] although early detec-tion with transvaginal ultrasound scan using measure-ment of endometrial thickness in symptomatic women is practised in developed countries[49]. Such practice requires
provision of ultrasonography and hysteroscopic facilities and manpower which are not yet freely available in devel-oping countries.
The burden of vaginal and vulval cancers is small. Currently no evidence exists to support any screening tests[50] although their association with HPV provides a window of opportunity for preventive interventions through HPV vaccination or typing. The task for devel-oping countries in mounting early treatment or primary preventive interventions will be similar to the challenges faced with cervical cancer.
In conclusion, there is a high incidence and mortality from gynaecological cancers in developing countries due primarily to the failure of these countries to mount effec-tive nationally organized screening programmes for cervi-cal cancer. A huge unmet need for funding for cancer care and control exists in these countries. “The human right to life, to prevention of suffering, and to education are all key rights linked to improving the control of cervical can-cer in resource poor parts of the world”[51]. The resources needed to provide adequately for gynaecological cancer care in many developing countries demands that increased funding is critically needed[52]. Scaling up of cheap sustain-able and effective preventive interventions against cervical cancer will potentially decrease the burden of gynaecolog-ical cancer in developing countries. Nationally organized HPV vaccination and low cost screening programmes subsidized by funding from governments and donor agen-cies are key to this intervention.
REFERENCES � The Economist Intelligence Unit. Breakaway: The global
burden of cancer-challenges and opportunities. The Econo-mist, 2009
2 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statis-tics, 2002. CA Cancer J Clin 2005; 55: 7�-�08 [PMID: �576�078 DOI: �0.3322/canjclin.55.2.7�]
3 International Agency for Research on Cancer. GLOBO-CAN 2008 Fast stats. Available from: URL: http: //www.globocan.iarc.fr/. Accessed: April 2�, 20�2
� Boyle P, Levin B. World cancer report 2008. Lyon: Interna-tional Agency for Research on Cancer, 2008
5 Wilson CM, Tobin S, Young RC. The exploding worldwide cancer burden: the impact of cancer on women. Int J Gynecol Cancer 200�; 14: �-�� [PMID: ��76�02� DOI: �0.����/j.�0�8-89�x.200�.���78.x]
6 Price AJ, Ndom P, Atenguena E, Mambou Nouemssi JP, Ryder RW. Cancer care challenges in developing countries. Cancer 20�2; 118: 3627-3635 [PMID: 22223050 DOI: �0.�002/cncr.2668�]
7 World bank. World Development indicators. Available from: URL: http: //data.worldbank.org/data-catalog/world-development-indicators?cid=GDP_WDI. Accessed: April 2�, 20�2
8 United Nations Statistics Division. Composition of macro-geographical (continental) regions, geographical sub regions and selected economies and other groupings (“Footnote c”). United Nations, 2008
9 Sankaranarayanan R, Ferlay J. Worldwide burden of gyn-aecological cancer: the size of the problem. Best Pract Res Clin Obstet Gynaecol 2006; 20: 207-225 [PMID: �6359925 DOI: �0.�0�6/j.bpobgyn.2005.�0.007]
�0 Kim SG, Hahm MI, Choi KS, Seung NY, Shin HR, Park
5 February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Iyoke CA et al . Gynaecological cancer in developing countries

EC. The economic burden of cancer in Korea in 2002. Eur J Cancer Care (Engl) 2008; 17: �36-��� [PMID: �8302650 DOI: �0.����/j.�365-235�.2007.008�8.x]
�� Bosch FX, Manos MM, Muñoz N, Sherman M, Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R, Shah KV. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst �995; 87: 796-802 [PMID: 779�229 DOI: �0.�093/jnci/87.��.796]
�2 Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kum-mer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Muñoz N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol �999; 189: �2-�9 [PMID: �0�5��82 DOI: �0.�002/(SICI)�096-9896(�99909)�89]
�3 Bosch FX, Lorincz A, Muñoz N, Meijer CJ, Shah KV. The causal relation between human papillomavirus and cervical cancer. J Clin Pathol 2002; 55: 2��-265 [PMID: ��9�9208 DOI: �0.��36/jcp.55.�.2��]
�� Denny L. Cytological screening for cervical cancer preven-tion. Best Pract Res Clin Obstet Gynaecol 20�2; 26: �89-�96 [PMID: 2207�306 DOI: �0.�0�6/j.bpobgyn.20��.08.00�]
�5 Wright TC, Kuhn L. Alternative approaches to cervical cancer screening for developing countries. Best Pract Res Clin Obstet Gynaecol 20�2; 26: �97-208 [PMID: 22385539 DOI: �0.�0�6/j.bpobgyn.20��.��.00�]
�6 Bhatla N, Singla S, Awasthi D. Human papillomavirus deoxyribonucleic acid testing in developed countries. Best Pract Res Clin Obstet Gynaecol 20�2; 26: 209-220 [PMID: 22�5�228 DOI: �0.�0�6/j.bpobgyn.20��.��.003]
�7 Sankaranarayanan R, Nessa A, Esmy PO, Dangou JM. Visual inspection methods for cervical cancer prevention. Best Pract Res Clin Obstet Gynaecol 20�2; 26: 22�-232 [PMID: 22075��� DOI: �0.�0�6/j.bpobgyn.20��.08.003]
�8 American College of Obstetrics and Gynecology. ACOG Committee Opinion No. 509: Management of vulvar in-traepithelial neoplasia. Obstet Gynecol 20��; 118: ��92-��9� [PMID: 220�5906 DOI: �0.�097/AOG.0b0�3e3�823b�7c2]
�9 Jones RW, Rowan DM, Stewart AW. Vulvar intraepithe-lial neoplasia: aspects of the natural history and outcome in �05 women. Obstet Gynecol 2005; 106: �3�9-�326 [PMID: �63�9258 DOI: �0.�097/0�.AOG.0000�8730�.76283.7f]
20 Pearson JM, Feltman RS, Twiggs LB. Association of hu-man papillomavirus with vulvar and vaginal intraepithelial disease: opportunities for prevention. Womens Health (Lond Engl) 2008; 4: ��3-�50 [PMID: �90725�6 DOI: �0.22�7/�7�55057.�.2.��3]
2� Jelovac D, Armstrong DK. Recent progress in the diagnosis and treatment of ovarian cancer. CA Cancer J Clin 20��; 61: �83-203 [PMID: 2�52�830 DOI: �0.3322/caac.20��3]
22 Hennessy BT, Coleman RL, Markman M. Ovarian cancer. Lancet 2009; 374: �37�-�382 [PMID: �97936�0 DOI: �0.�0�6/S0��0-6736(09)6�338-6]
23 Fader AN, Arriba LN, Frasure HE, von Gruenigen VE. Endometrial cancer and obesity: epidemiology, biomark-ers, prevention and survivorship. Gynecol Oncol 2009; 114: �2�-�27 [PMID: �9�06�60 DOI: �0.�0�6/j.ygyno.2009.03.039]
2� Van den Bosch T, Coosemans A, Morina M, Timmerman D, Amant F. Screening for uterine tumours. Best Pract Res Clin Obstet Gynaecol 20�2; 26: 257-266 [PMID: 220787�9 DOI: �0�6/j.bpobgyn]
25 Ferlay J, Bray F, Norman D, Mathers C, Parkin DM. GLO-BOCAN 2008, Cancer incidence and mortality worldwide. International Agency for Research on Cancer, 2008
26 Ferlay J, Bray F, Pisani P, Parkin DM. Cancer incidence, mortality and Prevalence worldwide. GLOBOCAN 2002, IARC Cancer base 5(2.0). Lyon: IARC Press, 200�
27 Adewole IF, Benedet JL, Crain BT, Follen M. Evolving a strategic approach to cervical cancer control in Africa. Gyne-col Oncol 2005; 99: S209-S2�2 [PMID: �6202��5 DOI: �0.�0�6/j.ygyno.2005.07.086]
28 Anorlu RI, Obodo K, Makwe CC. Cancer mortality among patients admitted to gynecological wards at Lagos Universi-ty Teaching Hospital, Nigeria. Int J Gynaecol Obstet 20�0; 110: 268-269 [PMID: 205�0��5 DOI: �0.�0�6/j.ijgo.20�0.03.038]
29 Dikshit R, Gupta PC, Ramasundarahettige C, Gajalakshmi V, Aleksandrowicz L, Badwe R, Kumar R, Roy S, Suraweera W, Bray F, Mallath M, Singh PK, Sinha DN, Shet AS, Gelband H, Jha P. Cancer mortality in India: a nationally representative survey. Lancet 20�2; 379: �807-�8�6 [PMID: 22�603�6 DOI: �0.�0�6/S0��0]
30 Bast RC, Hennessy B, Mills GB. The biology of ovarian can-cer: new opportunities for translation. Nat Rev Cancer 2009; 9: ��5-�28 [PMID: �9�6�667 DOI: �0.�038/nrc26��]
3� Gubbels JA, Claussen N, Kapur AK, Connor JP, Patankar MS. The detection, treatment, and biology of epithelial ovar-ian cancer. J Ovarian Res 20�0; 3: 8 [PMID: 203503�3 DOI: �0.��86/�757-22�5-3-8]
32 Arrossi S, Matos E, Zengarini N, Roth B, Sankaranayananan R, Parkin M. The socio-economic impact of cervical cancer on patients and their families in Argentina, and its influence on radiotherapy compliance. Results from a cross-sectional study. Gynecol Oncol 2007; 105: 335-3�0 [PMID: �725880� DOI: �0.�0�6/j.ygyno.2006.�2.0�0]
33 Ohaeri JU, Campbell OB, Ilesanmi AO, Omigbodun AO. The psychosocial burden of caring for some Nigerian women with breast cancer and cervical cancer. Soc Sci Med �999; 49: �5��-�5�9 [PMID: �05�5635 DOI: �0.�0�6/S0277-9536(99) 00223-3]
3� Gustafsson L, Pontén J, Bergström R, Adami HO. Inter-national incidence rates of invasive cervical cancer before cytological screening. Int J Cancer �997; 71: �59-�65 [PMID: 9�39836 DOI: �0.�002/(SICI)�097-02�5(�9970��0)7�]
35 Gustafsson L, Pontén J, Zack M, Adami HO. International incidence rates of invasive cervical cancer after introduc-tion of cytological screening. Cancer Causes Control �997; 8: 755-763 [PMID: 9328�98]
36 Sankaranarayanan R, Nene BM, Shastri SS, Jayant K, Mu-wonge R, Budukh AM, Hingmire S, Malvi SG, Thorat R, Kothari A, Chinoy R, Kelkar R, Kane S, Desai S, Keskar VR, Rajeshwarkar R, Panse N, Dinshaw KA. HPV screening for cervical cancer in rural India. N Engl J Med 2009; 360: �385-�39� [PMID: �93397�9 DOI: �0.�056/NEJMoa08085�6]
37 Brown AJ, Trimble CL. New technologies for cervical cancer screening. Best Pract Res Clin Obstet Gynaecol 20�2; 26: 233-2�2 [PMID: 22��9058 DOI: �0.�0�6/j.bpobgyn.20��.��.00�]
38 Kulasingam S, Havrilesky L. Health economics of screen-ing for gynaecological cancers. Best Pract Res Clin Obstet Gynaecol 20�2; 26: �63-�73 [PMID: 22�38003 DOI: �0.�0�6/j.bpobgyn.20��.�0.0�3]
39 Armstrong EP. Prophylaxis of cervical cancer and related cervical disease: a review of the cost-effectiveness of vac-cination against oncogenic HPV types. J Manag Care Pharm 20�0; 16: 2�7-230 [PMID: 2033�326]
�0 Goldie SJ, Gaffikin L, Goldhaber-Fiebert JD, Gordillo-Tobar A, Levin C, Mahé C, Wright TC. Cost-effectiveness of cervi-cal-cancer screening in five developing countries. N Engl J Med 2005; 353: 2�58-2�68 [PMID: �629�985]
�� Buys SS, Partridge E, Greene MH, Prorok PC, Reding D, Riley TL, Hartge P, Fagerstrom RM, Ragard LR, Chia D, Izmirlian G, Fouad M, Johnson CC, Gohagan JK. Ovarian cancer screening in the Prostate, Lung, Colorectal and Ovar-ian (PLCO) cancer screening trial: findings from the initial screen of a randomized trial. Am J Obstet Gynecol 2005; 193: �630-�639 [PMID: �6260202 DOI: �0.�0�6/j.ajog.2005.05.005]
�2 Menon U, Gentry-Maharaj A, Hallett R, Ryan A, Burnell M, Sharma A, Lewis S, Davies S, Philpott S, Lopes A, God-frey K, Oram D, Herod J, Williamson K, Seif MW, Scott I, Mould T, Woolas R, Murdoch J, Dobbs S, Amso NN, Leeson S, Cruickshank D, McGuire A, Campbell S, Fallowfield L, Singh N, Dawnay A, Skates SJ, Parmar M, Jacobs I. Sensitiv-
6 February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Iyoke CA et al . Gynaecological cancer in developing countries

ity and specificity of multimodal and ultrasound screening for ovarian cancer, and stage distribution of detected can-cers: results of the prevalence screen of the UK Collabora-tive Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol 2009; 10: 327-3�0 [PMID: �92822�� DOI: �0.�0�6/S��70-20�5(09)70026-9]
�3 Kobayashi H, Yamada Y, Sado T, Sakata M, Yoshida S, Kawaguchi R, Kanayama S, Shigetomi H, Haruta S, Tsuji Y, Ueda S, Kitanaka T. A randomized study of screening for ovarian cancer: a multicenter study in Japan. Int J Gynecol Cancer 2008; 18: ���-�20 [PMID: �76�5503 DOI: �0.����/j.�525-��38.2007.0�035.x]
�� Pavlik EJ, van Nagell JR. Ovarian cancer screening--what women want. Int J Gynecol Cancer 20�2; 22 Suppl �: S2�-S23 [PMID: 225�39�5]
�5 Buys SS, Partridge E, Black A, Johnson CC, Lamerato L, Isaacs C, Reding DJ, Greenlee RT, Yokochi LA, Kessel B, Crawford ED, Church TR, Andriole GL, Weissfeld JL, Fouad MN, Chia D, O’Brien B, Ragard LR, Clapp JD, Rathmell JM, Riley TL, Hartge P, Pinsky PF, Zhu CS, Izmirlian G, Kramer BS, Miller AB, Xu JL, Prorok PC, Gohagan JK, Berg CD. Ef-fect of screening on ovarian cancer mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Randomized Controlled Trial. JAMA 20��; 305: 2295-2303 [PMID: 2�6�268� DOI: �0.�00�/jama.20��.766]
�6 Menon U. Ovarian cancer screening has no effect on disease-specific mortality: commentary on the mortality results of
the PLCO trial. Evid Based Med 20�2; 17: �7-�8 [DOI: �0.��36/ebm.20��.�00�63]
�7 Gehrig PA, Cantrell LA, Shafer A, Abaid LN, Mendivil A, Boggess JF. What is the optimal minimally invasive surgi-cal procedure for endometrial cancer staging in the obese and morbidly obese woman? Gynecol Oncol 2008; 111: ��-�5 [PMID: �869�588]
�8 Soliman PT, Oh JC, Schmeler KM, Sun CC, Slomovitz BM, Gershenson DM, Burke TW, Lu KH. Risk factors for young premenopausal women with endometrial cancer. Obstet Gy-necol 2005; 105: 575-580 [PMID: �5738027 DOI: �0.�097/0�.AOG.0000�5��5�.��5�6.f7]
�9 Havrilesky LJ, Maxwell GL, Myers ER. Cost-effectiveness analysis of annual screening strategies for endometrial cancer. Am J Obstet Gynecol 2009; 200: 6�0.e�-6�0.e8 [PMID: �9380�2�]
50 Eva LJ. Screening and follow up of vulval skin disorders. Best Pract Res Clin Obstet Gynaecol 20�2; 26: �75-�88 [PMID: 22�89088 DOI: �0.�0�6/J.BPOBGYN.20��.��.005]
5� Basile S, Angioli R, Manci N, Palaia I, Plotti F, Benedetti Panici P. Gynecological cancers in developing countries: the challenge of chemotherapy in low-resources setting. Int J Gynecol Cancer 2006; 16: ��9�-��97 [PMID: �688�356 DOI: �0.����/J.�525-��38.2006.008�9.x]
52 Cain JM, Ngan H, Garland S, Wright T. Control of cervical cancer: women’s options and rights. Int J Gynaecol Obstet 2009; 106: ���-��3 [PMID: �953507� DOI: �0.�0�6/j.ijgo.2009.03.027]
P- Reviewer Schust DJ S- Editor Gou SX L- Editor A E- Editor Li JY
7 February �0, 20�3|Volume 2|Issue �|WJOG|www.wjgnet.com
Iyoke CA et al . Gynaecological cancer in developing countries

GENERAL INFORMATIONWorld Journal of Obstetrics and Gynecology (World J Obstet Gynecol, WJOG, online ISSN 2218-6220, DOI: 10.5317) is a peer-reviewed open ac-cess (OA) academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
Aim and scopeWJOG covers topics concerning pregnancy complications, obstetric surgical procedures, diagnostic imaging, endoscopy, reproductive endocrinology, tumors, pelvic diseases, evidence-based medicine, epidemiology and nursing. We encourage authors to submit their manuscripts to WJOG. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance. WJOG is edited and published by Baishideng Publishing Group (BPG). BPG has a strong professional editorial team composed of science editors, language editors and electronic editors. BPG currently publishes 42 OA clinical medical journals, including 41 in English, has a total of 15 471 editorial board members or peer reviewers, and is a world first-class publisher.
ColumnsThe columns in the issues of WJOG will include: (1) Editorial: The editorial board members are invited to make comments on an im-portant topic in their field in terms of its current research status and future directions to lead the development of this discipline; (2) Frontier: The editorial board members are invited to select a highly cited cutting-edge original paper of his/her own to summarize ma-jor findings, the problems that have been resolved and remain to be resolved, and future research directions to help readers understand his/her important academic point of view and future research di-rections in the field; (3) Diagnostic Advances: The editorial board members are invited to write high-quality diagnostic advances in their field to improve the diagnostic skills of readers. The topic covers general clinical diagnosis, differential diagnosis, pathological diagnosis, laboratory diagnosis, imaging diagnosis, endoscopic diagnosis, bio-technological diagnosis, functional diagnosis, and physical diagnosis; (4) Therapeutics Advances: The editorial board members are invited to write high-quality therapeutic advances in their field to help improve the therapeutic skills of readers. The topic covers medication therapy, psychotherapy, physical therapy, replacement therapy, interventional therapy, minimally invasive therapy, endoscopic therapy, transplanta-tion therapy, and surgical therapy; (5) Field of Vision: The editorial board members are invited to write commentaries on classic articles, hot topic articles, or latest articles to keep readers at the forefront of research and increase their levels of clinical research. Classic articles refer to papers that are included in Web of Knowledge and have re-ceived a large number of citations (ranking in the top 1%) after being published for more than years, reflecting the quality and impact of papers. Hot topic articles refer to papers that are included in Web of Knowledge and have received a large number of citations after being published for no more than 2 years, reflecting cuttingedge trends in scientific research. Latest articles refer to the latest published high-quality papers that are included in PubMed, reflecting the latest re-search trends. These commentary articles should focus on the status quo of research, the most important research topics, the problems
that have now been resolved and remain to be resolved, and future research directions. Basic information about the article to be com-mented (including authors, article title, journal name, year, volume, and inclusive page numbers; (6) Minireviews: The editorial board members are invited to write short reviews on recent advances and trends in research of molecular biology, genomics, and related cut-ting-edge technologies to provide readers with the latest knowledge and help improve their diagnostic and therapeutic skills; (7) Review: To make a systematic review to focus on the status quo of research, the most important research topics, the problems that have now been resolved and remain to be resolved, and future research directions; (8) Topic Highlight: The editorial board members are invited to write a series of articles (7-10 articles) to comment and discuss a hot topic to help improve the diagnostic and therapeutic skills of readers; (9) Medical Ethics: The editorial board members are invited to write ar-ticles about medical ethics to increase readers’ knowledge of medical ethics. The topic covers international ethics guidelines, animal studies, clinical trials, organ transplantation, etc.; (10) Clinical Case Conference or Clinicopathological Conference: The editorial board members are invited to contribute high-quality clinical case conference; (11) Origi-nal Articles: To report innovative and original findings in obstetrics and gynecology; (12) Brief Articles: To briefly report the novel and innovative findings in obstetrics and gynecology; (13) Meta-Analysis: To evaluate the clinical effectiveness in obstetrics and gynecology by using data from two or more randomised control trials; (14) Case Report: To report a rare or typical case; (15) Letters to the Editor: To discuss and make reply to the contributions published in WJOG, or to introduce and comment on a controversial issue of general interest; (16) Book Reviews: To introduce and comment on quality monographs of obstetrics and gynecology; and (17) Autobiography: The editorial board members are invited to write their autobiography to provide readers with stories of success or failure in their scientific research career. The topic covers their basic personal information and information about when they started doing research work, where and how they did research work, what they have achieved, and their les-sons from success or failure.
Name of journalWorld Journal of Obstetrics and Gynecology
ISSNISSN 2218-6220 (online)
FrequencyQuarterly
Editor-in-ChiefBo Jacobsson, MD, PhD, Professor, Department Obstetrics and Gynecology, Sahlgrenska University Hospital/Ostra, SE-416 85 Gothenburg, Sweden
Editorial OfficeJin-Lei Wang, DirectorXiu-Xia Song, Vice DirectorWorld Journal of Obstetrics and GynecologyEditorial Department: Room 903, Building D, Ocean International Center,
IWJOG|www.wjgnet.com February 10, 2013|Volume 2|Issue 1|
INSTRUCTIONS TO AUTHORS
Online Submissions: http://www.wjgnet.com/esps/[email protected]
World Journal ofObstetrics and GynecologyW J O G
World J Obstet Gynecol 2013 February 10; 2(1): I-VISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.

Instructions to authors
No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaE-mail: [email protected]://www.wjgnet.comTelephone: +86-10-85381891Fax: +86-10-8538-1893
PublisherBaishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza, 315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188Telephone: +852-31779906E-mail: [email protected]://www.wjgnet.com
Production centerBeijing Baishideng BioMed Scientific Co., LimitedRoom 903, Building D, Ocean International Center,No. 62 Dongsihuan Zhonglu, Chaoyang District,Beijing 100025, ChinaTelephone: +86-10-85381892Fax: +86-10-85381893
Representative officeUSA Office8226 Regency Drive,Pleasanton, CA 94588-3144, United States
Instructions to authorsFull instructions are available online at http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm.
Indexed and Abstracted inDigital Object Identifier.
SPECIAL STATEMENTAll articles published in this journal represent the viewpoints of the authors except where indicated otherwise.
Biostatistical editingStatistical review is performed after peer review. We invite an ex-pert in Biomedical Statistics to evaluate the statistical method used in the paper, including t-test (group or paired comparisons), chi-squared test, Ridit, probit, logit, regression (linear, curvilinear, or stepwise), correlation, analysis of variance, analysis of covariance, etc. The reviewing points include: (1) Statistical methods should be described when they are used to verify the results; (2) Whether the statistical techniques are suitable or correct; (3) Only homoge-neous data can be averaged. Standard deviations are preferred to standard errors. Give the number of observations and subjects (n). Losses in observations, such as drop-outs from the study should be reported; (4) Values such as ED50, LD50, IC50 should have their 95% confidence limits calculated and compared by weighted probit analysis (Bliss and Finney); and (5) The word ‘significantly’ should be replaced by its synonyms (if it indicates extent) or the P value (if it indicates statistical significance).
Conflict-of-interest statementIn the interests of transparency and to help reviewers assess any poten-tial bias, WJOG requires authors of all papers to declare any compet-ing commercial, personal, political, intellectual, or religious interests in relation to the submitted work. Referees are also asked to indi-cate any potential conflict they might have reviewing a particular paper. Before submitting, authors are suggested to read “Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Ethical Considerations in the Conduct and Reporting of Research: Conflicts of Interest” from International Committee of Medical Journal Editors (ICMJE), which is available at: http://www.icmje.org/ethical_4conflicts.html.
Sample wording: [Name of individual] has received fees for serv-ing as a speaker, a consultant and an advisory board member for [names of organizations], and has received research funding from [names of organization]. [Name of individual] is an employee of [name of or-ganization]. [Name of individual] owns stocks and shares in [name of organization]. [Name of individual] owns patent [patent identification and brief description].
Statement of informed consentManuscripts should contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee or it should be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Authors should also draw attention to the Code of Ethics of the World Medi-cal Association (Declaration of Helsinki, 1964, as revised in 2004).
Statement of human and animal rightsWhen reporting the results from experiments, authors should follow the highest standards and the trial should conform to Good Clini-cal Practice (for example, US Food and Drug Administration Good Clinical Practice in FDA-Regulated Clinical Trials; UK Medicines Research Council Guidelines for Good Clinical Practice in Clinical Trials) and/or the World Medical Association Declaration of Hel-sinki. Generally, we suggest authors follow the lead investigator’s na-tional standard. If doubt exists whether the research was conducted in accordance with the above standards, the authors must explain the rationale for their approach and demonstrate that the institutional review body explicitly approved the doubtful aspects of the study.
Before submitting, authors should make their study approved by the relevant research ethics committee or institutional review board. If human participants were involved, manuscripts must be accompa-nied by a statement that the experiments were undertaken with the understanding and appropriate informed consent of each. Any per-sonal item or information will not be published without explicit con-sents from the involved patients. If experimental animals were used, the materials and methods (experimental procedures) section must clearly indicate that appropriate measures were taken to minimize pain or discomfort, and details of animal care should be provided.
SUBMISSION OF MANUSCRIPTSManuscripts should be typed in 1.5 line spacing and 12 pt. Book Antiqua with ample margins. Number all pages consecutively, and start each of the following sections on a new page: Title Page, Ab-stract, Introduction, Materials and Methods, Results, Discussion, Acknowledgements, References, Tables, Figures, and Figure Leg-ends. Neither the editors nor the publisher are responsible for the opinions expressed by contributors. Manuscripts formally accepted for publication become the permanent property of Baishideng Publishing Group Co., Limited, and may not be reproduced by any means, in whole or in part, without the written permission of both the authors and the publisher. We reserve the right to copy-edit and put onto our website accepted manuscripts. Authors should follow the relevant guidelines for the care and use of laboratory animals of their institution or national animal welfare committee. For the sake of transparency in regard to the performance and reporting of clinical trials, we endorse the policy of the ICMJE to refuse to pub-lish papers on clinical trial results if the trial was not recorded in a publicly-accessible registry at its outset. The only register now avail-able, to our knowledge, is http://www.clinicaltrials.gov sponsored by the United States National Library of Medicine and we encour-age all potential contributors to register with it. However, in the case that other registers become available you will be duly notified. A letter of recommendation from each author’s organization should be provided with the contributed article to ensure the privacy and secrecy of research is protected.
Authors should retain one copy of the text, tables, photo-graphs and illustrations because rejected manuscripts will not be returned to the author(s) and the editors will not be responsible for loss or damage to photographs and illustrations sustained dur-
IIWJOG|www.wjgnet.com February 10, 2013|Volume 2|Issue 1|

Instructions to authors
ing mailing.
Online submissionsManuscripts should be submitted through the Online Submission System at: http://www.wjgnet.com/2218-6220office. Authors are highly recommended to consult the ONLINE INSTRUC-TIONS TO AUTHORS (http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm) before attempting to submit online. For assistance, authors encountering problems with the Online Submission System may send an email describing the problem to [email protected], or by telephone: +86-10-85381891. If you submit your manuscript online, do not make a postal contribution. Repeated online submission for the same manuscript is strictly pro-hibited.
MANUSCRIPT PREPARATIONAll contributions should be written in English. All articles must be submitted using word-processing software. All submissions must be typed in 1.5 line spacing and 12 pt. Book Antiqua with ample mar-gins. Style should conform to our house format. Required informa-tion for each of the manuscript sections is as follows:
Title pageTitle: Title should be less than 12 words.
Running title: A short running title of less than 6 words should be provided.
Authorship: Authorship credit should be in accordance with the standard proposed by ICMJE, based on (1) substantial contribu-tions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the ver-sion to be published. Authors should meet conditions 1, 2, and 3.
Institution: Author names should be given first, then the complete name of institution, city, province and postcode. For example, Xu-Chen Zhang, Li-Xin Mei, Department of Pathology, Chengde Medical College, Chengde 067000, Hebei Province, China. One au-thor may be represented from two institutions, for example, George Sgourakis, Department of General, Visceral, and Transplantation Surgery, Essen 45122, Germany; George Sgourakis, 2nd Surgical Department, Korgialenio-Benakio Red Cross Hospital, Athens 15451, Greece
Author contributions: The format of this section should be: Author contributions: Wang CL and Liang L contributed equally to this work; Wang CL, Liang L, Fu JF, Zou CC, Hong F and Wu XM designed the research; Wang CL, Zou CC, Hong F and Wu XM performed the research; Xue JZ and Lu JR contributed new reagents/analytic tools; Wang CL, Liang L and Fu JF analyzed the data; and Wang CL, Liang L and Fu JF wrote the paper.
Supportive foundations: The complete name and number of sup-portive foundations should be provided, e.g. Supported by National Natural Science Foundation of China, No. 30224801
Correspondence to: Only one corresponding address should be provided. Author names should be given first, then author title, af-filiation, the complete name of institution, city, postcode, province, country, and email. All the letters in the email should be in lower case. A space interval should be inserted between country name and email address. For example, Montgomery Bissell, MD, Professor of Medicine, Chief, Liver Center, Gastroenterology Division, Universi-ty of California, Box 0538, San Francisco, CA 94143, United States. [email protected]
Telephone and fax: Telephone and fax should consist of +, coun-try number, district number and telephone or fax number, e.g. Tele-phone: +86-10-85381892 Fax: +86-10-85381893
Peer reviewers: All articles received are subject to peer review. Normally, three experts are invited for each article. Decision for acceptance is made only when at least two experts recommend an article for publication. Reviewers for accepted manuscripts are acknowledged in each manuscript, and reviewers of articles which were not accepted will be acknowledged at the end of each issue. To ensure the quality of the articles published in WJOG, review-ers of accepted manuscripts will be announced by publishing the name, title/position and institution of the reviewer in the footnote accompanying the printed article. For example, reviewers: Professor Jing-Yuan Fang, Shanghai Institute of Digestive Disease, Shang-hai, Affiliated Renji Hospital, Medical Faculty, Shanghai Jiaotong University, Shanghai, China; Professor Xin-Wei Han, Department of Radiology, The First Affiliated Hospital, Zhengzhou University, Zhengzhou, Henan Province, China; and Professor Anren Kuang, Department of Nuclear Medicine, Huaxi Hospital, Sichuan Univer-sity, Chengdu, Sichuan Province, China.
AbstractThere are unstructured abstracts (no less than 200 words) and struc-tured abstracts. The specific requirements for structured abstracts are as follows:
An informative, structured abstract should accompany each manuscript. Abstracts of original contributions should be struc-tured into the following sections: AIM (no more than 20 words; Only the purpose of the study should be included. Please write the Aim in the form of “To investigate/study/…”), METHODS (no less than 140 words for Original Articles; and no less than 80 words for Brief Articles), RESULTS (no less than 150 words for Original Articles and no less than 120 words for Brief Articles; You should present P values where appropriate and must provide relevant data to illustrate how they were obtained, e.g., 6.92 ± 3.86 vs 3.61 ± 1.67, P < 0.001), and CONCLUSION (no more than 26 words).
Key wordsPlease list 5-10 key words, selected mainly from Index Medicus, which reflect the content of the study.
Core tipPlease write a summary of less than 100 words to outline the most innovative and important arguments and core contents in your paper to attract readers.
TextFor articles of these sections, original articles and brief articles, the main text should be structured into the following sections: INTRO-DUCTION, MATERIALS AND METHODS, RESULTS and DISCUSSION, and should include appropriate Figures and Tables. Data should be presented in the main text or in Figures and Tables, but not in both.
IllustrationsFigures should be numbered as 1, 2, 3, etc., and mentioned clearly in the main text. Provide a brief title for each figure on a sepa-rate page. Detailed legends should not be provided under the figures. This part should be added into the text where the figures are applicable. Figures should be either Photoshop or Illustra-tor files (in tiff, eps, jpeg formats) at high-resolution. Examples can be found at: http://www.wjgnet.com/1007-9327/13/4520.pdf; http://www.wjgnet.com/1007-9327/13/4554.pdf; http://www.wjgnet.com/1007-9327/13/4891.pdf; http://www.wjgnet.com/1007-9327/13/4986.pdf; http://www.wjgnet.com/1007-9327/13/4498.pdf. Keeping all elements compiled is necessary in line-art image. Scale bars should be used rather than magnification factors, with the length of the bar defined in the leg-end rather than on the bar itself. File names should identify the fig-ure and panel. Avoid layering type directly over shaded or textured areas. Please use uniform legends for the same subjects. For exam-ple: Figure 1 Pathological changes in atrophic gastritis after treat-ment. A: ...; B: ...; C: ...; D: ...; E: ...; F: ...; G: …etc. It is our principle
IIIWJOG|www.wjgnet.com February 10, 2013|Volume 2|Issue 1|

to publish high resolution-figures for the printed and E-versions.
TablesThree-line tables should be numbered 1, 2, 3, etc., and mentioned clearly in the main text. Provide a brief title for each table. Detailed legends should not be included under tables, but rather added into the text where applicable. The information should complement, but not duplicate the text. Use one horizontal line under the title, a second under column heads, and a third below the Table, above any footnotes. Vertical and italic lines should be omitted.
Notes in tables and illustrationsData that are not statistically significant should not be noted. aP < 0.05, bP < 0.01 should be noted (P > 0.05 should not be noted). If there are other series of P values, cP < 0.05 and dP < 0.01 are used. A third series of P values can be expressed as eP < 0.05 and fP < 0.01. Other notes in tables or under illustrations should be expressed as 1F, 2F, 3F; or sometimes as other symbols with a superscript (Arabic numerals) in the upper left corner. In a multi-curve illustration, each curve should be labeled with ●, ○, ■, □, ▲, △, etc., in a certain se-quence.
AcknowledgmentsBrief acknowledgments of persons who have made genuine con-tributions to the manuscript and who endorse the data and conclu-sions should be included. Authors are responsible for obtaining written permission to use any copyrighted text and/or illustrations.
REFERENCESCoding systemThe author should number the references in Arabic numerals ac-cording to the citation order in the text. Put reference numbers in square brackets in superscript at the end of citation content or after the cited author’s name. For citation content which is part of the narration, the coding number and square brackets should be typeset normally. For example, “Crohn’s disease (CD) is associated with increased intestinal permeability[1,2]”. If references are cited directly in the text, they should be put together within the text, for example, “From references[19,22-24], we know that...”
When the authors write the references, please ensure that the order in text is the same as in the references section, and also ensure the spelling accuracy of the first author’s name. Do not list the same citation twice.
PMID and DOIPleased provide PubMed citation numbers to the reference list, e.g. PMID and DOI, which can be found at http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed and http://www.crossref.org/Sim-pleTextQuery/, respectively. The numbers will be used in E-version of this journal.
Style for journal referencesAuthors: the name of the first author should be typed in bold-faced letters. The family name of all authors should be typed with the ini-tial letter capitalized, followed by their abbreviated first and middle initials. (For example, Lian-Sheng Ma is abbreviated as Ma LS, Bo-Rong Pan as Pan BR). The title of the cited article and italicized journal title (journal title should be in its abbreviated form as shown in PubMed), publication date, volume number (in black), start page, and end page [PMID: 11819634 DOI: 10.3748/wjg.13.5396].
Style for book referencesAuthors: the name of the first author should be typed in bold-faced letters. The surname of all authors should be typed with the initial letter capitalized, followed by their abbreviated middle and first initials. (For example, Lian-Sheng Ma is abbreviated as Ma LS, Bo-Rong Pan as Pan BR) Book title. Publication number. Publication place: Publication press, Year: start page and end page.
FormatJournals English journal article (list all authors and include the PMID where applicable)1 Jung EM, Clevert DA, Schreyer AG, Schmitt S, Rennert J,
Kubale R, Feuerbach S, Jung F. Evaluation of quantitative con-trast harmonic imaging to assess malignancy of liver tumors: A prospective controlled two-center study. World J Gastroenterol 2007; 13: 6356-6364 [PMID: 18081224 DOI: 10.3748/wjg.13. 6356]
Chinese journal article (list all authors and include the PMID where applicable)2 Lin GZ, Wang XZ, Wang P, Lin J, Yang FD. Immunologic
effect of Jianpi Yishen decoction in treatment of Pixu-diar-rhoea. Shijie Huaren Xiaohua Zazhi 1999; 7: 285-287
In press3 Tian D, Araki H, Stahl E, Bergelson J, Kreitman M. Signature
of balancing selection in Arabidopsis. Proc Natl Acad Sci USA 2006; In press
Organization as author4 Diabetes Prevention Program Research Group. Hyperten-
sion, insulin, and proinsulin in participants with impaired glu-cose tolerance. Hypertension 2002; 40: 679-686 [PMID: 12411462 PMCID:2516377 DOI:10.1161/01.HYP.0000035706.28494. 09]
Both personal authors and an organization as author 5 Vallancien G, Emberton M, Harving N, van Moorselaar RJ;
Alf-One Study Group. Sexual dysfunction in 1, 274 European men suffering from lower urinary tract symptoms. J Urol 2003; 169: 2257-2261 [PMID: 12771764 DOI:10.1097/01.ju. 0000067940.76090.73]
No author given6 21st century heart solution may have a sting in the tail. BMJ
2002; 325: 184 [PMID: 12142303 DOI:10.1136/bmj.325. 7357.184]
Volume with supplement7 Geraud G, Spierings EL, Keywood C. Tolerability and safety
of frovatriptan with short- and long-term use for treatment of migraine and in comparison with sumatriptan. Headache 2002; 42 Suppl 2: S93-99 [PMID: 12028325 DOI:10.1046/j.1526-4610.42.s2.7.x]
Issue with no volume8 Banit DM, Kaufer H, Hartford JM. Intraoperative frozen
section analysis in revision total joint arthroplasty. Clin Orthop Relat Res 2002; (401): 230-238 [PMID: 12151900 DOI:10.1097/00003086-200208000-00026]
No volume or issue9 Outreach: Bringing HIV-positive individuals into care. HRSA
Careaction 2002; 1-6 [PMID: 12154804]
BooksPersonal author(s)10 Sherlock S, Dooley J. Diseases of the liver and billiary system.
9th ed. Oxford: Blackwell Sci Pub, 1993: 258-296Chapter in a book (list all authors)11 Lam SK. Academic investigator’s perspectives of medical
treatment for peptic ulcer. In: Swabb EA, Azabo S. Ulcer disease: investigation and basis for therapy. New York: Marcel Dekker, 1991: 431-450
Author(s) and editor(s)12 Breedlove GK, Schorfheide AM. Adolescent pregnancy.
2nd ed. Wieczorek RR, editor. White Plains (NY): March of Dimes Education Services, 2001: 20-34
Conference proceedings13 Harnden P, Joffe JK, Jones WG, editors. Germ cell tumours V.
Proceedings of the 5th Germ cell tumours Conference; 2001 Sep 13-15; Leeds, UK. New York: Springer, 2002: 30-56
Conference paper14 Christensen S, Oppacher F. An analysis of Koza's computa-
tional effort statistic for genetic programming. In: Foster JA, Lutton E, Miller J, Ryan C, Tettamanzi AG, editors. Genetic
IVWJOG|www.wjgnet.com
Instructions to authors
February 10, 2013|Volume 2|Issue 1|

VWJOG|www.wjgnet.com
Instructions to authors
February 10, 2013|Volume 2|Issue 1|
programming. EuroGP 2002: Proceedings of the 5th Euro-pean Conference on Genetic Programming; 2002 Apr 3-5; Kinsdale, Ireland. Berlin: Springer, 2002: 182-191
Electronic journal (list all authors)15 Morse SS. Factors in the emergence of infectious diseases.
Emerg Infect Dis serial online, 1995-01-03, cited 1996-06-05; 1(1): 24 screens. Available from: URL: http://www.cdc.gov/ncidod/eid/index.htm
Patent (list all authors)16 Pagedas AC, inventor; Ancel Surgical R&D Inc., assignee. Flex-
ible endoscopic grasping and cutting device and positioning tool assembly. United States patent US 20020103498. 2002 Aug 1
Statistical dataWrite as mean ± SD or mean ± SE.
Statistical expressionExpress t test as t (in italics), F test as F (in italics), chi square test as χ2 (in Greek), related coefficient as r (in italics), degree of freedom as υ (in Greek), sample number as n (in italics), and probability as P (in italics).
UnitsUse SI units. For example: body mass, m (B) = 78 kg; blood pres-sure, p (B) = 16.2/12.3 kPa; incubation time, t (incubation) = 96 h, blood glucose concentration, c (glucose) 6.4 ± 2.1 mmol/L; blood CEA mass concentration, p (CEA) = 8.6 24.5 mg/L; CO2 volume fraction, 50 mL/L CO2, not 5% CO2; likewise for 40 g/L formal-dehyde, not 10% formalin; and mass fraction, 8 ng/g, etc. Arabic numerals such as 23, 243, 641 should be read 23 243 641.
The format for how to accurately write common units and quantums can be found at: http://www.wjgnet.com/2218-6220/g_info_20100724062131.htm.
AbbreviationsStandard abbreviations should be defined in the abstract and on first mention in the text. In general, terms should not be abbrevi-ated unless they are used repeatedly and the abbreviation is helpful to the reader. Permissible abbreviations are listed in Units, Symbols and Abbreviations: A Guide for Biological and Medical Editors and Authors (Ed. Baron DN, 1988) published by The Royal Society of Medicine, London. Certain commonly used abbreviations, such as DNA, RNA, HIV, LD50, PCR, HBV, ECG, WBC, RBC, CT, ESR, CSF, IgG, ELISA, PBS, ATP, EDTA, mAb, can be used directly without further explanation.
ItalicsQuantities: t time or temperature, c concentration, A area, l length, m mass, V volume.Genotypes: gyrA, arg 1, c myc, c fos, etc.Restriction enzymes: EcoRI, HindI, BamHI, Kbo I, Kpn I, etc.Biology: H. pylori, E coli, etc.
Examples for paper writingAll types of articles’ writing style and requirement will be found in the
link: http://www.wjgnet.com/esps/NavigationInfo.aspx?id=15
RESUBMISSION OF THE REVISED MANUSCRIPTSAuthors must revise their manuscript carefully according to the re-vision policies of Baishideng Publishing Group Co., Limited. The revised version, along with the signed copyright transfer agreement, responses to the reviewers, and English language Grade A certificate (for non-native speakers of English), should be submitted to the online system via the link contained in the e-mail sent by the editor. If you have any questions about the revision, please send e-mail to [email protected].
Language evaluation The language of a manuscript will be graded before it is sent for revision. (1) Grade A: priority publishing; (2) Grade B: minor lan-guage polishing; (3) Grade C: a great deal of language polishing needed; and (4) Grade D: rejected. Revised articles should reach Grade A.
Copyright assignment formPlease download a Copyright assignment form from http://www.wjgnet.com/2219-2808/g_info_20100725073726.htm.
Responses to reviewersPlease revise your article according to the comments/suggestions provided by the reviewers. The format for responses to the reviewers’ comments can be found at: http://www.wjgnet.com/2218-6220/g_info_20100724061942.htm.
Proof of financial supportFor paper supported by a foundation, authors should provide a copy of the document and serial number of the foundation.
Links to documents related to the manuscript WJOG will be initiating a platform to promote dynamic interactions between the editors, peer reviewers, readers and authors. After a manuscript is published online, links to the PDF version of the submitted manuscript, the peer-reviewers’ report and the revised manuscript will be put on-line. Readers can make comments on the peer reviewer’s report, authors’ responses to peer reviewers, and the revised manuscript. We hope that authors will benefit from this feedback and be able to revise the manuscript accordingly in a timely manner.
Publication feeWJOG is an international, peer-reviewed, OA online journal. Ar-ticles published by this journal are distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium and format, provided the original work is properly cited. The use is non-commercial and is otherwise in compliance with the license. Authors of accepted articles must pay a publication fee. Publica-tion fee: 600 USD per article. All invited articles are published free of charge.

World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 May 10; 2(2): 8-36
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com

8 Newdevelopmentsoftheeffectofmelatoninonreproduction
Lampiao F, Du Plessis SS
16 Roleofbariatricsurgeryinthepelvicfloordisorders
Iavazzo C
21 Past,presentandfutureofprimarysystemictreatmentinbreastcancer
Alonso-Romero JL, Piñero-Madrona A
34 Prenatalincarcerationofcaputsuccedaneum:Acasereport
Okazaki A, Miyazaki K, Kihira K, Furuhashi M
Contents
IWJOG|www.wjgnet.com May 10, 2013|Volume 2|Issue 2|
REVIEW
World Journal ofObstetrics and GynecologyW J O G
Quarterly Volume 2 Number 2 May 10, 2013
MINIREVIEW
CASE REPORT

ContentsWorld Journal of Obstetrics and Gynecology
Volume 2 Number 2 May 10, 2013
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Shuai Ma Responsible Science Editor: Ling-Ling WenResponsible Electronic Editor: Xiao-Mei ZhengProofing Editor-in-Chief: Lian-Sheng Ma
World Journal of Obstetrics and GynecologyRoom 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected]://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza, 315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188Telephone: +852-31779906E-mail: [email protected]://www.wjgnet.com
PUBLICATIONDATEMay 10, 2013
COPYRIGHT© 2013 Baishideng. Articles published by this Open-Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial Li-cense, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in this journal represent the view-points of the authors except where indicated otherwise.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm.
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
IIWJOG|www.wjgnet.com
APPENDIX
ABOUT COVER
AIM AND SCOPE
FLYLEAF
May 10, 2013|Volume 2|Issue 2|
NAMEOFJOURNALWorld Journal of Obstetrics and Gynecology
ISSNISSN 2218-6220 (online)
LAUNCHDATEJune 10, 2012
FREQUENCYQuarterly
EDITOR-IN-CHIEFBo Jacobsson, MD, PhD, Professor, Department Obstetrics and Gynecology, Sahlgrenska University Hospital/Ostra, SE-416 85 Gothenburg, Sweden
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice Director
I-V Instructionstoauthors
EditorialBoardMemberofWorldJournalofObstetricsandGynecology,FanuelLampiao,PhD,DepartmentofBasicMedicalScience,PhysiologyDivision,P/Bag360,Blantyre3,Malawi
World Journal of Obstetrics and Gynecology (World J Obstet Gynecol, WJOG, online ISSN 2218-6220, DOI: 10.5317) is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJOG covers topics concerning pregnancy complications, obstetric surgical procedures, diagnostic imaging, endoscopy, reproductive endocrinology, tumors, pelvic diseases, evidence-based medicine, epidemiology and nursing.
We encourage authors to submit their manuscripts to WJOG. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Obstetrics and Gynecology is now indexed in Digital Object Identifier.
I-III EditorialBoard
INDEXING/ABSTRACTING

tonin, its effect on puberty, testicular and ova function, pregnancy, and oxidative stress. A growing body of scientific evidence is suggesting that melatonin plays an important role in reproductive function. It is there-fore imperative to highlight the beneficial effects of this hormone in improving the reproductive processes.
© 2013 Baishideng. All rights reserved.
Key words: Melatonin; Reproduction; Reactive oxygen species; Antioxidants; Pineal gland
Core tip: In recent years, many studies have been fo-cusing on the role melatonin plays in the process of reproduction. The low success rate in assisted reproduc-tive technologies due to the detrimental effects of oxi-dative stress has led to studies investigating the potency of melatonin as an antioxidant. Studies have shown that melatonin reduces oxidative stress and contributes to oocyte maturation, embryo development, and lutein-ization of granulosa cells. Clinical studies have demon-strated that melatonin treatment for infertile women increases intra-follicular melatonin concentrations, re-duces intra-follicular oxidative damage, and increases the chances of pregnancy. This review highlights the effects of melatonin in reproduction.
Lampiao F, Du Plessis SS. New developments of the effect of melatonin on reproduction. World J Obstet Gynecol 2013; 2(2): 8-15 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i2/8.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i2.8
INTRODUCTIONIn the past few decades, a lot of studies regarding the biochemistry and physiology of a hormone called mela-tonin (N-acetyl-5-methoxytryptamine) have taken place. This hormone is secreted during the dark hours at night by the pineal gland and is responsible for the regulation of a variety of important central and peripheral actions
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i2.�
World J Obstet Gynecol 2013 May 10; 2(2): �-15ISSN 221�-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
New developments of the effect of melatonin on reproduction
Fanuel Lampiao, Stefan S Du Plessis
Fanuel Lampiao, Division of Physiology, Department of Basic Medical Sciences, College of Medicine, Blantyre 3, MalawiStefan S Du Plessis, Division of Medical Physiology, Stellenbosch University, Tygerberg Campus, Tygerberg 19063, South AfricaAuthor contributions: Lampiao F and Du Plessis SS were in-volved in conception and designing, drafting, revising and final approval of the article.Correspondence to: Fanuel Lampiao, PhD, Division of Physi-ology, Department of Basic Medical Sciences, College of Medi-cine, PO Box 360, Blantyre 3, Malawi. [email protected]: +265-1878058 Fax: +265-111872644Received: January 5, 2013 Revised: April 18, 2013Accepted: May 8, 2013Published online: May 10, 2013
AbstractIn the past decades, a lot of advances in understand-ing the biochemistry and physiology of the pineal gland have been made. There is evidence that it interacts with many endocrine as well as non-endocrine tissues to influence their metabolic activity modulating many organs and functions. Melatonin is secreted by the pi-neal gland in the brain and plays an important role in regulating the neuroendocrine system. This hormone is one of the major role players in the regulation of the circadian sleep-wake cycle. It is normally released from the pineal gland during the night in response to environmental changes in light. Studies have shown that melatonin plays a role in the regulation of many reproductive processes such as puberty, gonadal func-tion, and pregnancy. Beside these, melatonin has been shown to be able to directly neutralize a number of free radicals and reactive oxygen and nitrogen species. The main objective of this review is to provide comprehen-sive information about the new developments in mela-tonin research regarding its role in reproduction. A re-view of international scientific literature was done and a question-and-answer format was used in an attempt to convey comprehensive information in a simple man-ner. This review discusses evidence currently available relating to the effect of melatonin on reproductive pro-cesses. It deliberates the mechanism of action of mela-
REVIEW
� May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com

related to circadian rhythms and reproduction[1]. Al-though melatonin is primarily synthesized and secreted by the pineal gland, it is has been reported that it is also formed in tiny amounts by other organs such as the retina, harderian gland, gastrointestinal tract, lympho-cytes, and the skin[2-5]. The role of melatonin in other animal species is related to seasonal reproductive cycles. In humans, melatonin secretion levels by the pineal gland can regulate the reproductive neuroendocrine axis[6]. The increase in reactive oxygen species (ROS) generation in in vitro fertilization (IVF) settings has been reported to negatively affect the success rate of IVF outcomes[7-9].
Melatonin has also been reported to have free radical scavenging properties[10,11] as well as stimulating several other antioxidant enzymes[12]. Can melatonin supplemen-tation during assisted reproductive technologies increase the success rate of these procedures? Since the body is capable of producing melatonin does endogenous mela-tonin production or exogenous melatonin supplemen-tation has any effect on the reproductive processes of humans and animals?
This review will provide comprehensive information about the new developments in melatonin research specif-ically regarding its role in the process of reproduction of both humans and animals. It will discuss the mechanism of action of melatonin, its effect on puberty, testicular and ovarian function, pregnancy, and oxidative stress.
CURRENT AVAILABLE EVIDENCE CONCERNING THE EFFECT OF MELATONIN ON THE REPRODUCTIVE PROCESSWhat is the effect of melatonin on seasonal reproduction?There is accumulation of evidence suggesting that the pattern of melatonin secretion, which is mediated by photoperiod, directly influences reproductive function. Much of the evidence has been generated from season-ally breeding mammals[13-16]. Long-day breeding animals such as rodents have been shown to be depressed during winter months (when elevated melatonin levels are at their longest nocturnal duration). The reproductive qui-escent period was also prevented by surgical removal of the pineal gland[17]. On the other hand, short-day breed-ers such as sheep, and white-tailed deer were shown to be sexually very active and capable during the shortest days of the year, when melatonin levels are highest in terms of their nocturnal duration[18,19]. These observa-tions suggest that melatonin is neither antigonadotrophic nor progonadotrophic. Thus, the changing duration of the nocturnal melatonin message is a passive signal that provides the hypothalamo-pituitary-gonadal (HPG)-axis information as to the time of year[20].
In a study involving male and female Syrian hamsters which were maintained under naturally occurring short days and reduced temperatures, it was observed that they developed gonadal regression. This regression was
reversed by surgical removal of the pineal gland[21]. This is evidence that the reproductive axis obviously uses the seasonally dependent melatonin rhythm to adjust testicu-lar and ovarian physiology accordingly.
Investigations using long-day and short-day breeding animals have enormously contributed to the understand-ing of the mechanisms whereby day length and melato-nin govern seasonal reproduction. These findings have led to the successful use of melatonin as a pharmacologi-cal agent to advance the breeding season of sheep and to induce estrous cycles and increase lambing during the interval when these animals would normally be experi-encing seasonal anestrus[22-24].
How does melatonin influence the selection of sexual mates?Some studies have demonstrated that melatonin may be involved in the selection of sexual partner. It was ob-served that administering melatonin to male zebra finches in the drinking fluid in combination with carotenoids en-hanced the brightness of the carotenoid-based pigmenta-tion in their bills[25]. Since males with brighter coloured bills are more likely to be selected as a mate by females, melatonin may aid in the selection of a mate. Colourful plumage generally signals superior genetic quality and is common ploy used by many bird species as a sexual at-tractant[26].
More evidence of the role of melatonin on the selec-tion of sexual mate has been demonstrated by the two-spotted goby fish[27]. Treating the skin explants of gobies with a combination of either melatonin and melanocyte-stimulating hormone or melatonin and prolactin, led to an exaggerated orange colouration and transparency of the belly skin. This colouration change induced by mela-tonin and other hormones would presumably benefit the individual in terms of attracting a sexual mate.
PINEAL MELATONIN BIOSYNTHESIS AND REGULATIONHow is melatonin synthesized and regulated?The production of melatonin by the pineal gland exhibits a circadian rhythm with low level of production during day time and high levels during the night[28,29]. During the process of melatonin synthesis, Tryptophan is hydroxyl-ated to 5-hydroxy-tryptophan and subsequently into se-rotonin. Serotonin is acetylated to form N-acetylserotonin and then converted into melatonin (Figure 1). The supra-chiasmatic nucleus (SCN) which is the major circadian oscillator that receives light input from the retina through the retino-hypothalamic tract is the one that regulate the circadian melatonin production[30]. When melatonin is formed in the pineal gland, it is not stored there, but re-leased immediately into the blood or into the cerebrospi-nal fluid. It is metabolized mainly in the liver.
What is the mechanism of action of melatonin?Melatonin exerts its actions through two types of recep-
� May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Lampiao F et al . Melatonin and reproduction

tors belonging to the super-family of G-protein coupled receptors. These receptors contain seven typical trans-membrane domains and are called the MT1 and MT2
[31,32]. The MT1 and MT2 are membrane bound receptors which are widely distributed in different organs of the body, in-cluding the brain and other peripheral organs.
When these receptors are activated they cause inhibi-tion of adenyl cyclase activity[33] and inhibition of for-skolin-induced cyclic adenosine monophosphate (cAMP) formation which result in the reduction in activated pro-tein kinase[34]. In mammals melatonin has been reported to affect the reproductive function by activation of mela-tonin receptor sites within the HPG-axis[35].
Neonatal pituitary cells have been shown to express MT1 and MT2 subtype of melatonin receptors. These re-ceptors when activated lead to a decrease in cAMP produc-tion and activity of protein kinase A, and attenuation of gonadotropic releasing hormone (GnRH)-induced gonado-tropin secretion[36].
EFFECT OF MELATONIN ON PUBERTYWhat is the effect of melatonin on the onset of puberty?During fetal life and the first year of life, the HPG-axis is active, but becomes quiescent thereafter until around 10 years. Its reactivation depends on the progressive in-crease in the levels of GnRH which subsequently lead to the pulsatile secretion of luteinizing hormone (LH) and follicle stimulating hormone[37]. It has been reported that melatonin secretion has an inhibitory influence on the hypothalamic secretion of GnRH in humans[38]. It is there-fore speculated that before puberty, melatonin concentra-tions are too high thus inhibiting the hypothalamic activa-tion. But prior to puberty, the levels of melatonin decline below the threshold value thus forming the trigger signals of GnRH from the hypothalamus which leads to the on-set of pubertal changes[39]. Therefore, it is the decline of melatonin levels that trigger puberty. Studies have demon-strated that high nocturnal melatonin secretion in children delays puberty[40] whereas low levels of melatonin have been shown to be associated with precocious puberty[41].
How does melatonin modulate sexual maturation?The mechanism by which the HPG-axis is inhibited by melatonin after the first year of life until puberty is not well elucidated. However, there are reports that point to the influence of melatonin on the HPG-axis. These include, the evidence that melatonin is involved in the control of pulsatile secretion of LH[42] and that there is a negative correlation between nocturnal melatonin and LH concentrations[43]. Furthermore, high levels of serum melatonin in women have been shown to be associated with amenorrhea accompanied with decreased GnRH/LH pulsatile secretion[44,45]. Similarly, increases in noc-turnal peak amplitude and duration of melatonin were reported in amenorrhoeic athletes who displayed irregu-larities in hypothalamic-pituitary-ovarian-axis function-ing[46,47]. In vitro studies have demonstrated that melatonin leads to the down-regulation of the GnRH gene expres-sion in a cell line containing GnRH secreting neurons[48].
MELATONIN AND GAMETE FUNCTIONWhat is the effect of melatonin on testicular function?In animal studies, it has been shown that melatonin may modulate testicular function. In mice and rats it was re-ported that melatonin has an inhibitory effect on Leydig cells[49,50]. The Leydig cells are responsible for the produc-tion of testosterone. Mel1a and Mel1b receptor mRNAs are expressed in epithelial cells of rat epididymis suggest-ing that melatonin has a role in the regulation of epididy-mal physiology[51]. The epididymis is important for the maturation and storage of spermatozoa before they are ejaculated into the female reproductive tract.
There are contradictory reports concerning the ef-fect of melatonin on spermatozoa function. It has been reported that long term administration of melatonin to healthy men is associated with decreased semen quality[52]. Sperm concentration, motility as well as testosterone levels were found to be significantly decreased in healthy men administered with melatonin. On the other hand, an in vitro study demonstrated that administration of melato-nin to human spermatozoa improved progressive motil-ity and reduced the number of static cells[53]. In another study in which melatonin levels were measured in fertile and infertile men, it was found that serum and semi-nal melatonin levels in infertile men were significantly reduced compared with the levels in the fertile men[54]. This demonstrated that melatonin may be involved in the modulation of the reproductive neuroendocrine axis in male infertility.
What is the effect of melatonin on ovary function?The role of melatonin in the production of female gam-etes is focused on its direct actions in the ovary. It is able to pass through all cell membranes and enter all tissues because of its lipophilic property, however, it specifically concentrates in the ovary when injected systemically[55]. Studies have shown that high levels of melatonin are found in human preovulatory follicular fluid at concen-
10 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Tryptophan
5-hydroxy-tryptophan
Serotonin
N-acetylserotonin
Melatonin
Tryptophan hydroxylase
5-HTP Decarboxylase
Serotonin-N-acetyltransferase
Hydroxyindole-O-methyl-transferase
Figure 1 Biosynthesis of melatonin. 5-HTP: 5-hydroxy-tryptophan.
Lampiao F et al . Melatonin and reproduction

trations which are much higher than those in serum[56,57]. It has been reported that the follicular fluid melatonin levels depend on the follicular growth[58]. The larger the follicle the higher the melatonin concentration. When oocytes are incubated in medium with melatonin supple-mentation during in vitro maturation, they have lower lev-els of ROS than control (without melatonin treatment) oocytes[59]. The ability of melatonin to promote embryo development in different species has correspondingly been reported. When mouse embryos were cultured in medium containing melatonin, increased blastocyst devel-opment rates were observed[60]. This suggests that mela-tonin may be involved in embryo development.
EFFECT OF MELATONIN ON PREGNANCYWhat role does melatonin play in human pregnancy?People living in the Arctic region have shown that their pituitary-gonadal function and conception rates are lower in the dark winter months than in the summer[61]. It has been further observed that during these dark periods of the winter season, the increases in serum melatonin con-centration correlate with reduced activity of the anterior pituitary-ovarian axis[62]. The precise role of melatonin in human pregnancy is not clear. However, it has been reported that serum melatonin levels are higher during pregnancy than in nonpregnant women[63]. Moreover, twin pregnancies have been reported to yield higher nocturnal melatonin levels than singleton pregnancies[63]. This suggests that melatonin might have a role to play in human pregnancy. Clinical studies have demonstrated that melatonin treatment for infertile women increases intra-follicular melatonin concentrations, reduces intra-follicular oxidative damage and elevates fertilization and pregnancy rates[8].
Does melatonin play a role in fetal development?Because melatonin is a small molecule, it gets transferred from the maternal circulation into that of the fetus through the placenta[64]. This means that the fetal circu-lation mirrors a circadian rhythm of plasma melatonin similar to that of the mother[65]. It has also been reported that there are melatonin receptors in the human fetal SCN. It is believed that melatonin is involved in the regu-lation of the circadian rhythm in the fetus. It has been observed that if maternal melatonin is suppressed, both MT1 gene and clock genes are affected, suggesting that maternal melatonin has a role in modulating fetal clock gene function[66]. The generation as well as maintenance of circadian clock function depends on clock genes[67].
What is the role of melatonin in parturition?In some mammals such as rats, parturition occurs during daytime[68]. Continuous darkness abolishes the photope-riodic timing of parturition[69]. If the pineal gland is re-moved in rats, the daytime delivery birth pattern is abol-ished and melatonin replacement therapy restores it[70]. It is well documented that the human myometrium has
functional melatonin receptors[71]. Administration of mel-atonin has been shown to modulate the strength of affin-ity of gap junctions found in the myometrium[72,73]. These gap junctions serve to coordinate individual myometrial cell contractions into powerful labor inducing forces[72], thus implicating melatonin as a possible role player in the mechanism underlying the initiation of parturition.
MELATONIN AND OXIDATIVE STRESSWhat are the sources of oxidative stress in the human reproductive system?In females ROS is locally produced during the ruptur-ing of the follicle at the time of ovulation[74]. It has been suggested that the ROS are involved in the ovulation process. There is a surge of LH during ovulation which induces dissolution of the basement membrane between the granulosa and theca internal layers and an expansion of the theca capillaries into the avascular granulosa cell layer to form a dense network of capillaries. These en-dothelial cell capillaries contribute to the generation of the free radicals[74]. Neutrophils and macrophages are also reported to reside in follicles[75]. These macrophages and neutrophils produce tremendous amounts of free radi-cals. The locally produced free radicals seems to have an important role on follicle rupture, since ROS have been shown to act as second messengers modulating the ex-pression of genes that govern physiological processes of oocyte maturation[76,77]. However, excess ROS is respon-sible for oxidative stress which can damage molecules and structures of oocyte and granulosa cells within the follicle. Hence the ROS must be continuously scavenged to keep only small amounts necessary to maintain normal cell function.
In the male reproductive system, the cellular compo-nent of semen is a huge source of ROS. Morphologi-cally abnormal and immature spermatozoa together with the presence of leukocytes can generate ROS in human ejaculates. Spermatozoa do generate ROS at the level of the plasma membrane and mitochondria[78]. Studies have shown that human spermatozoa generate superoxide (O2
.-), which spontaneously dismutates to hydrogen per-oxide (H2O2)[79].
In the male genital tract and the ejaculate, ROS are not only derived from the spermatozoa, but can also be generated by leukocytes, which physiologically produce even up to 1000 times more ROS than spermatozoa[80,81]. This high ROS production by leukocytes plays a major role in infections, inflammation and cellular defense mechanisms. Basically, the cellular mechanisms for the generation of ROS in leukocytes and spermatozoa are the same, yet in leukocytes it is a physiological necessity to release large amounts of O2
.- into phagocytic vesicles during the killing action of pathogens.
Considering the extraordinary high content of poly-unsaturated fatty acids in their membrane, the sperm plasma membrane is particularly susceptible to oxidative stress and the double bonds of the membrane lipids can
11 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Lampiao F et al . Melatonin and reproduction

easily be oxidized by excessive ROS levels present in the sperm cells' environment. These can either be produced in large amounts by leukocytes or the spermatozoa them-selves. In case of ROS attacking the plasma membrane lipids, a process called “lipid peroxidation” is initiated. Ultimately, this process decreases membrane fluidity of both plasma and organelle membranes and, as a result, damages membrane function, ion gradients, receptor-me-diated signal transduction, etc[82]. Hence, with the loss of membrane function, spermatozoa lose the ability to func-tion properly and therefore, fertilization is impaired[83].
Is melatonin a free radical scavenger?Usually melatonin exerts its effects through its receptors, but it can also act directly as a powerful free radical scav-enger by detoxifying the highly reactive hydroxyl radi-cal[84,85]. There are numerous other reports confirming the scavenging abilities of melatonin on ROS and reactive nitrogen species[86,87]. Some of the free radicals scavenged by melatonin include O2
-, H2O2, hydrochlorous acid, nitric oxide and the peroxynitrite anion[88-91]. The anti-oxidant properties of melatonin as a cell protector have been extensively studied and its scavenging ability have been reported to be higher than that of well known scav-engers such as vitamin C and vitamin E[86]. Apart from scavenging free radicals directly, melatonin has a high ca-pability to detoxify ROS and suppress its oxidative effects indirectly by enhancing the production of endogenous antioxidants. Melatonin has been shown to stimulate the scavenging activities and mRNA levels of antioxidant enzymes including superoxide dismutase, glutathione per-oxidase, and catalase[92,93].
CONCLUSIONIn recent years, a lot of research focused on the effect of melatonin as a direct free radical scavenger. This has greatly broadened our understanding of its multiple physiological roles. Melatonin’s role in the regulation of reproductive physiology has been demonstrated in photo-period dependent breeding mammals, and it seems to be receptor mediated mechanism in hypothalamus and pitu-itary gland. Currently, most of the research on melatonin is focusing on its local role as an antioxidant. The intra-follicular role of melatonin in the ovary has been demon-strated. Melatonin, secreted by the pineal gland, has been reported to be taken up into the follicular fluid from the blood. The free radicals produced within the follicles, especially during the ovulation process, are scavenged by melatonin, and reduced oxidative stress may be involved in oocyte maturation and embryo development. Evidence is pointing to the fact that melatonin treatment for infer-tility in women increases intra-follicular melatonin con-centrations which subsequently reduces intra-follicular oxidative damage and elevates fertilization and pregnancy rates. The safety of exogenous melatonin treatment has been demonstrated in many studies[94,95]. Animal studies have also shown that melatonin has no detrimental ef-
fects on mouse and rat embryo development both in vitro and in vivo[96,97]. Future studies will indicate whether mela-tonin treatment could become a new cure for improving oocyte and sperm quality in infertile patients.
REFERENCES1 Tamura H, Takasaki A, Taketani T, Tanabe M, Kizuka F, Lee L,
Tamura I, Maekawa R, Aasada H, Yamagata Y, Sugino N. The role of melatonin as an antioxidant in the follicle. J Ovarian Res 2012; 5: 5 [PMID: 22277103 DOI: 10.11�6/1757-2215-5-5]
2 Bubenik GA. Gastrointestinal melatonin: localization, func-tion, and clinical relevance. Dig Dis Sci 2002; 47: 2336-234� [PMID: 123�5�07 DOI: 10.1023/A: 1020107�15�1�]
3 Slominski A, Fischer TW, Zmijewski MA, Wortsman J, Semak I, Zbytek B, Slominski RM, Tobin DJ. On the role of melatonin in skin physiology and pathology. Endocrine 2005; 27: 137-14� [PMID: 16217127 DOI: 10.13�5/ENDO: 27: 2: 137]
4 Carrillo-Vico A, Calvo JR, Abreu P, Lardone PJ, García-Mauriño S, Reiter RJ, Guerrero JM. Evidence of melatonin synthesis by human lymphocytes and its physiological sig-nificance: possible role as intracrine, autocrine, and/or para-crine substance. FASEB J 2004; 18: 537-53� [PMID: 147156�6]
5 Cardinali DP, Rosner JM. Metabolism of serotonin by the rat retina in vitro. J Neurochem 1�71; 18: 176�-1770 [PMID: 5571113 DOI: 10.1111/j.1471-415�.1�71.tb03752.x]
6 Anderson RA, Lincoln GA, Wu FC. Melatonin potentiates testosterone-induced suppression of luteinizing hormone se-cretion in normal men. Hum Reprod 1��3; 8: 1�1�-1�22 [PMID: �2��743]
7 Eryilmaz OG , Devran A, Sarikaya E, Aksakal FN, Mollamahmutoğlu L, Cicek N. Melatonin improves the oocyte and the embryo in IVF patients with sleep disturbances, but does not improve the sleeping problems. J Assist Reprod Genet 2011; 28: �15-�20 [PMID: 2174�445 DOI: 10.1007/s10�15-011-�604-y]
� Tamura H, Takasaki A, Taketani T, Tanabe M, Kizuka F, Lee L, Tamura I, Maekawa R, Asada H, Yamagata Y, Sugino N. Melatonin as a free radical scavenger in the ovarian follicle. Endocr J 2013; 60: 1-13 [PMID: 23171705 DOI: 10.1507/endocrj.EJ12-0263]
� Kim MK, Park EA, Kim HJ, Choi WY, Cho JH, Lee WS, Cha KY, Kim YS, Lee DR, Yoon TK. Does supplementation of in-vitro culture medium with melatonin improve IVF out-come in PCOS? Reprod Biomed Online 2013; 26: 22-2� [PMID: 23177415 DOI: 10.1016/j.rbmo.2012.10.007]
10 Webb SM, Puig-Domingo M. Role of melatonin in health and disease. Clin Endocrinol (Oxf) 1��5; 42: 221-234 [PMID: 775�227 DOI: 10.1111/j.1365-2265.1��5.tb01�6�.x]
11 Zang LY, Cosma G, Gardner H, Vallyathan V. Scavenging of reactive oxygen species by melatonin. Biochim Biophys Acta 1���; 1425: 46�-477 [PMID: ��3�210 DOI: 10.1016/S0304-4165(��)000��-3]
12 Reiter RJ, Tan DX, Osuna C, Gitto E. Actions of melatonin in the reduction of oxidative stress. A review. J Biomed Sci 2000; 7: 444-45� [PMID: 110604�3 DOI: 10.1007/BF02253360]
13 Reiter RJ, Hester RJ. Interrelationships of the pineal gland, the superior cervical ganglia and the photoperiod in the regulation of the endocrine systems of hamsters. Endocrinology 1�66; 79: 116�-1170 [PMID: 5�51523 DOI: 10.1210/endo-7�-6-116�]
14 Reiter RJ. Comparative physiology: pineal gland. Annu Rev Physiol 1�73; 35: 305-32� [PMID: 4575164 DOI: 10.1146/an-nurev.ph.35.030173.001513]
15 Stetson MH, Elliott JA, Menaker M. Photoperiodic regula-tion of hamster testis: circadian sensitivity to the effects of light. Biol Reprod 1�75; 13: 32�-33� [PMID: 121�1�� DOI: 10.10�5/biolreprod13.3.32�]
16 Turek FW, Desjardins C, Menaker M. Melatonin-induced in-
12 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Lampiao F et al . Melatonin and reproduction

hibition of testicular function in adult golden hamsters. Proc Soc Exp Biol Med 1�76; 151: 502-506 [PMID: 1257250]
17 Wagner GC, Johnston JD, Clarke IJ, Lincoln GA, Hazlerigg DG. Redefining the limits of day length responsiveness in a seasonal mammal. Endocrinology 200�; 149: 32-3� [PMID: 17�01234 DOI: 10.1210/en.2007-065�]
1� Coelho LA, Rodrigues PA, Nonaka KO, Sasa A, Balieiro JC, Vicente WR, Cipolla-Neto J. Annual pattern of plasma mela-tonin and progesterone concentrations in hair and wool ewe lambs kept under natural photoperiod at lower latitudes in the southern hemisphere. J Pineal Res 2006; 41: 101-107 [PMID: 16�7�314 DOI: 10.1111/j.1600-07�X.2006.00333.x]
1� Chemineau P, Guillaume D, Migaud M, Thiéry JC, Pellicer-Rubio MT, Malpaux B. Seasonality of reproduction in mam-mals: intimate regulatory mechanisms and practical implica-tions. Reprod Domest Anim 200�; 43 Suppl 2: 40-47 [PMID: 1�63�103 DOI: 10.1111/j.143�-0531.200�.01141.x]
20 Reiter RJ. The melatonin rhythm: both a clock and a cal-endar. Experientia 1��3; 49: 654-664 [PMID: �3�540� DOI: 10.1007/BF01�23�47]
21 Reiter RJ. Pineal control of a seasonal reproductive rhythm in male golden hamsters exposed to natural daylight and temperature. Endocrinology 1�73; 92: 423-430 [PMID: 46�2�5� DOI: 10.1210/endo-�2-2-423]
22 Haresign W, Peters AR, Staples LD. The effect of melatonin implants on breeding activity and litter size in commercial sheep flocks in the UK. Anim Prod 1��0; 50: 111-121 [DOI: 10.1017/S0003356100004517]
23 Haresign W. Manipulation of reproduction in sheep. J Re-prod Fertil Suppl 1��2; 45: 127-13� [PMID: 1304027]
24 Abecia JA, Valares JA, Forcada F, Palacín I, Martín S, Mar-tino A. The effect of melatonin on the reproductive perfor-mance of three sheep breeds in Spain. Small Rumin Res 2007; 69: 10-16 [DOI: 10.1016/j.smallrumres.2005.12.01�]
25 Bertrand S, Faivre B, Sorci G. Do carotenoid-based sexual traits signal the availability of non-pigmentary antioxi-dants? J Exp Biol 2006; 209: 4414-441� [PMID: 1707�711 DOI: 10.1242/jeb.02540]
26 Roulin A, Jungi TW, Pfister H, Dijkstra C. Female barn owls (Tyto alba) advertise good genes. Proc Biol Sci 2000; 267: �37-�41 [PMID: 10�5373� DOI: 10.10��/rspb.2000.10�3]
27 Sköld HN, Amundsen T, Svensson PA, Mayer I, Bjelven-mark J, Forsgren E. Hormonal regulation of female nuptial coloration in a fish. Horm Behav 200�; 54: 54�-556 [PMID: 1�5�603� DOI: 10.1016/j.yhbeh.200�.05.01�]
2� Brzezinski A. Melatonin in humans. N Engl J Med 1��7; 336: 1�6-1�5 [PMID: ������� DOI: 10.1056/NEJM1��701163360306]
2� Pang SF, Li L, Ayre EA, Pang CS, Lee PP, Xu RK, Chow PH, Yu ZH, Shiu SY. Neuroendocrinology of melatonin in re-production: recent developments. J Chem Neuroanat 1���; 14: 157-166 [PMID: �704��4 DOI: 10.1016/S0��1-061�(��)0002�-5]
30 Berson DM, Dunn FA, Takao M. Phototransduction by retinal ganglion cells that set the circadian clock. Science 2002; 295: 1070-1073 [PMID: 11�34�35 DOI: 10.1126/science.1067262]
31 Reppert SM, Weaver DR, Ebisawa T. Cloning and character-ization of a mammalian melatonin receptor that mediates re-productive and circadian responses. Neuron 1��4; 13: 1177-11�5 [PMID: 7�46354 DOI: 10.1016/0��6-6273(�4)�0055-�]
32 Reppert SM, Godson C, Mahle CD, Weaver DR, Slaugen-haupt SA, Gusella JF. Molecular characterization of a second melatonin receptor expressed in human retina and brain: the Mel1b melatonin receptor. Proc Natl Acad Sci USA 1��5; 92: �734-�73� [PMID: 756�007 DOI: 10.1073/pnas.�2.1�.�734]
33 von Gall C, Stehle JH, Weaver DR. Mammalian melatonin receptors: molecular biology and signal transduction. Cell Tissue Res 2002; 309: 151-162 [PMID: 12111545 DOI: 10.1007/s00441-002-05�1-4]
34 Vanecek J, Klein DC. Melatonin inhibits gonadotropin-releasing hormone-induced elevation of intracellular Ca2+ in neonatal rat pituitary cells. Endocrinology 1��2; 130: 701-707
[PMID: 173371� DOI: 10.1210/en.130.2.701]35 Malpaux B, Migaud M, Tricoire H, Chemineau P. Biology
of mammalian photoperiodism and the critical role of the pineal gland and melatonin. J Biol Rhythms 2001; 16: 336-347 [PMID: 1150637� DOI: 10.1177/074�7300112�002051]
36 Balík A, Kretschmannová K, Mazna P, Svobodová I, Zem-ková H. Melatonin action in neonatal gonadotrophs. Physiol Res 2004; 53 Suppl 1: S153-S166 [PMID: 1511��46]
37 Sizonenko PC. Physiology of puberty. J Endocrinol Invest 1���; 12: 5�-63 [PMID: 26�134�]
3� Buchanan KL, Yellon SM. Delayed puberty in the male Djungarian hamster: effect of short photoperiod or melatonin treatment on the GnRH neuronal system. Neuroendocrinology 1��1; 54: �6-102 [PMID: 1766555 DOI: 10.115�/000125�57]
3� Silman R. Melatonin and the human gonadotrophin-releas-ing hormone pulse generator. J Endocrinol 1��1; 128: 7-11 [PMID: 1���677 DOI: 10.1677/joe.0.12�0007]
40 Cohen HN, Hay ID, Annesley TM, Beastall GH, Wallace AM, Spooner R, Thomson JA, Eastwold P, Klee GG. Serum immunoreactive melatonin in boys with delayed puberty. Clin Endocrinol (Oxf) 1��2; 17: 517-521 [PMID: 7172460]
41 Cavallo A. Melatonin and human puberty: current perspec-tives. J Pineal Res 1��3; 15: 115-121 [PMID: �106�56 DOI: 10.1111/j.1600-07�X.1��3.tb00517.x]
42 Brzezinski A, Lynch HJ, Wurtman RJ, Seibel MM. Possible contribution of melatonin to the timing of the luteinizing hormone surge. N Engl J Med 1��7; 316: 1550-1551 [PMID: 35�72�7 DOI: 10.1056/NEJM1��70611316241�]
43 Waldhauser F, Weiszenbacher G, Frisch H, Zeitlhuber U, Waldhauser M, Wurtman RJ. Fall in nocturnal serum mela-tonin during prepuberty and pubescence. Lancet 1��4; 1: 362-365 [PMID: 6141425 DOI: 10.1016/S0140-6736(�4)�0412-4]
44 Berga SL, Mortola JF, Yen SS. Amplification of nocturnal melatonin secretion in women with functional hypothalamic amenorrhea. J Clin Endocrinol Metab 1���; 66: 242-244 [PMID: 333560� DOI: 10.1210/jcem-66-1-242]
45 Brzezinski A, Lynch HJ, Seibel MM, Deng MH, Nader TM, Wurtman RJ. The circadian rhythm of plasma melatonin during the normal menstrual cycle and in amenorrheic women. J Clin Endocrinol Metab 1���; 66: ��1-��5 [PMID: 312�44� DOI: 10.1210/jcem-66-5-��1]
46 Laughlin GA, Loucks AB, Yen SS. Marked augmentation of nocturnal melatonin secretion in amenorrheic athletes, but not in cycling athletes: unaltered by opioidergic or dopami-nergic blockade. J Clin Endocrinol Metab 1��1; 73: 1321-1326 [PMID: 1�55514 DOI: 10.1210/jcem-73-6-1321]
47 Aleandri V, Spina V, Morini A. The pineal gland and repro-duction. Hum Reprod Update 1��6; 2: 225-235 [PMID: �07�415 DOI: 10.10�3/humupd/2.3.225]
4� Roy D, Belsham DD. Melatonin receptor activation regulates GnRH gene expression and secretion in GT1-7 GnRH neu-rons. Signal transduction mechanisms. J Biol Chem 2002; 277: 251-25� [PMID: 116�46�1 DOI: 10.1074/jbc.M10���0200]
4� Ng TB, Lo LL. Inhibitory actions of pineal indoles on ste-roidogenesis in isolated rat Leydig cells. J Pineal Res 1���; 5: 22�-243 [PMID: 2�41443 DOI: 10.1111/j.1600-07�X.1���.tb0064�.x]
50 Persengiev S, Kehajova J. Inhibitory action of melatonin and structurally related compounds on testosterone production by mouse Leydig cells in vitro. Cell Biochem Funct 1��1; 9: 2�1-2�6 [PMID: 1�07�5� DOI: 10.1002/cbf.2�00�0410]
51 Shiu SY, Li L, Wong JT, Pang SF. Biology of G protein-coupled melatonin receptors in the epididymis and prostate of mammals. Chin Med J (Engl) 1��7; 110: 64�-655 [PMID: �5�4273]
52 Luboshitzky R, Shen-Orr Z, Nave R, Lavi S, Lavie P. Mela-tonin administration alters semen quality in healthy men. J Androl 2002; 23: 572-57� [PMID: 12065466]
53 Ortiz A, Espino J, Bejarano I, Lozano GM, Monllor F, García JF, Pariente JA, Rodríguez AB. High endogenous melatonin
13 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Lampiao F et al . Melatonin and reproduction

14 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
concentrations enhance sperm quality and short-term in vi-tro exposure to melatonin improves aspects of sperm motil-ity. J Pineal Res 2011; 50: 132-13� [PMID: 20�64711]
54 Awad H, Halawa F, Mostafa T, Atta H. Melatonin hormone profile in infertile males. Int J Androl 2006; 29: 40�-413 [PMID: 1637110� DOI: 10.1111/j.1365-2605.2005.00624.x]
55 Wurtman RJ, Axelrod J, Potter LT. The uptake of H3-melato-nin in endocrine and nervous tissues and the effects of con-stant light exposure. J Pharmacol Exp Ther 1�64; 143: 314-31� [PMID: 14161142]
56 Brzezinski A, Seibel MM, Lynch HJ, Deng MH, Wurtman RJ. Melatonin in human preovulatory follicular fluid. J Clin Endocrinol Metab 1��7; 64: �65-�67 [PMID: 3�1��07 DOI: 10.1210/jcem-64-4-�65]
57 Rönnberg L, Kauppila A, Leppäluoto J, Martikainen H, Vakkuri O. Circadian and seasonal variation in human preovulatory follicular fluid melatonin concentration. J Clin Endocrinol Metab 1��0; 71: 4�2-4�6 [PMID: 23�0343 DOI: 10.1210/jcem-71-2-4�3]
5� Nakamura Y, Tamura H, Takayama H, Kato H. Increased endogenous level of melatonin in preovulatory human follicles does not directly influence progesterone produc-tion. Fertil Steril 2003; 80: 1012-1016 [PMID: 14556�25 DOI: 10.1016/S0015-02�2(03)0100�-2]
5� Jahnke G, Marr M, Myers C, Wilson R, Travlos G, Price C. Maternal and developmental toxicity evaluation of melato-nin administered orally to pregnant Sprague-Dawley rats. Toxicol Sci 1���; 50: 271-27� [PMID: 1047��64 DOI: 10.10�3/toxsci/50.2.271]
60 Ishizuka B, Kuribayashi Y, Murai K, Amemiya A, Itoh MT. The effect of melatonin on in vitro fertilization and embryo development in mice. J Pineal Res 2000; 28: 4�-51 [PMID: 10626601 DOI: 10.1034/j.1600-07�x.2000.2�0107.x]
61 Sawhney RC, Malhotra AS, Prasad R, Pal K, Kumar R, Bajaj AC. Pituitary-gonadal hormones during prolonged resi-dency in Antarctica. Int J Biometeorol 1���; 42: 51-54 [PMID: �7�0�46]
62 Kauppila A, Kivelä A, Pakarinen A, Vakkuri O. Inverse seasonal relationship between melatonin and ovarian activ-ity in humans in a region with a strong seasonal contrast in luminosity. J Clin Endocrinol Metab 1��7; 65: �23-�2� [PMID: 3667��0 DOI: 10.1210/jcem-65-5-�23]
63 Nakamura Y, Tamura H, Kashida S, Takayama H, Yamagata Y, Karube A, Sugino N, Kato H. Changes of serum melato-nin level and its relationship to feto-placental unit during pregnancy. J Pineal Res 2001; 30: 2�-33 [PMID: 1116��04 DOI: 10.1034/j.1600-07�X.2001.300104.x]
64 Yellon SM, Longo LD. Effect of maternal pinealectomy and reverse photoperiod on the circadian melatonin rhythm in the sheep and fetus during the last trimester of preg-nancy. Biol Reprod 1���; 39: 10�3-10�� [PMID: 321�3�2 DOI: 10.10�5/biolreprod3�.5.10�3]
65 Muñoz-Hoyos A, Jaldo-Alba F, Molina-Carballo A, Ro-dríguez-Cabezas T, Molina-Font JA, Acuña-Castroviejo D. Absence of plasma melatonin circadian rhythm during the first 72 hours of life in human infants. J Clin Endocrinol Metab 1��3; 77: 6��-703 [PMID: �3706�2 DOI: 10.1210/jc.77.3.6��]
66 Torres-Farfan C, Rocco V, Monsó C, Valenzuela FJ, Campi-no C, Germain A, Torrealba F, Valenzuela GJ, Seron-Ferre M. Maternal melatonin effects on clock gene expression in a nonhuman primate fetus. Endocrinology 2006; 147: 461�-4626 [PMID: 16�40546 DOI: 10.1210/en.2006-062�]
67 Hawkins GA, Meyers DA, Bleecker ER, Pack AI. Identifica-tion of coding polymorphisms in human circadian rhythm genes PER1, PER2, PER3, CLOCK, ARNTL, CRY1, CRY2 and TIMELESS in a multi-ethnic screening panel. DNA Seq 200�; 19: 44-4� [PMID: 17�52344]
6� Boer K, Lincoln DW, Swaab DF. Effects of electrical stimulation of the neurohypophysis on labour in the rat. J Endocrinol 1�75; 65: 163-176 [PMID: 1151202 DOI: 10.1677/
joe.0.0650163]6� Lincoln DW, Porter DG. Photoperiodic dissection of endo-
crine events at parturition. Anim Reprod Sci 1�7�; 2: �7-115 [DOI: 10.1016/037�-4320(7�)�0040-X]
70 Takayama H, Nakamura Y, Tamura H, Yamagata Y, Harada A, Nakata M, Sugino N, Kato H. Pineal gland (melatonin) affects the parturition time, but not luteal function and fetal growth, in pregnant rats. Endocr J 2003; 50: 37-43 [PMID: 12733707 DOI: 10.1507/endocrj.50.37]
71 Schlabritz-Loutsevitch N, Hellner N, Middendorf R, Mül-ler D, Olcese J. The human myometrium as a target for melatonin. J Clin Endocrinol Metab 2003; 88: �0�-�13 [PMID: 12574232 DOI: 10.1210/jc.2002-02044�]
72 Tamura H, Nakamura Y, Terron MP, Flores LJ, Manchester LC, Tan DX, Sugino N, Reiter RJ. Melatonin and pregnancy in the human. Reprod Toxicol 200�; 25: 2�1-303 [PMID: 1�4�5664 DOI: 10.1016/j.reprotox.200�.03.005]
73 Olecese J. Melatonin effects on uterine physiology. In: Pandi-Perumal SR, Cardinali DP, editors. Melatonin: from molecules to therapy. New York: Nova Science publishers, 2007: 205-225
74 Brännström M, Norman RJ. Involvement of leukocytes and cytokines in the ovulatory process and corpus luteum func-tion. Hum Reprod 1��3; 8: 1762-1775 [PMID: �300�42]
75 Nakamura Y, Smith M, Krishna A, Terranova PF. Increased number of mast cells in the dominant follicle of the cow: relationships among luteal, stromal, and hilar regions. Biol Reprod 1��7; 37: 546-54� [PMID: 3676403 DOI: 10.10�5/biol-reprod37.3.546]
76 Dröge W. Free radicals in the physiological control of cell function. Physiol Rev 2002; 82: 47-�5 [PMID: 1177360�]
77 Hensley K, Robinson KA, Gabbita SP, Salsman S, Floyd RA. Reactive oxygen species, cell signaling, and cell injury. Free Radic Biol Med 2000; 28: 1456-1462 [PMID: 10�2716� DOI: 10.1016/S0��1-5�4�(00)00252-5]
7� Gavella M, Lipovac V. NADH-dependent oxidoreductase (diaphorase) activity and isozyme pattern of sperm in infer-tile men. Arch Androl 1��2; 28: 135-141 [PMID: 152003� DOI: 10.310�/014�501�20���76�1]
7� Alvarez JG, Touchstone JC, Blasco L, Storey BT. Spontane-ous lipid peroxidation and production of hydrogen peroxide and superoxide in human spermatozoa. Superoxide dis-mutase as major enzyme protectant against oxygen toxicity. J Androl 1��7; 8: 33�-34� [PMID: 2�22642]
�0 Plante M, de Lamirande E, Gagnon C. Reactive oxygen spe-cies released by activated neutrophils, but not by deficient spermatozoa, are sufficient to affect normal sperm motility. Fertil Steril 1��4; 62: 3�7-3�3 [PMID: �0340��]
�1 de Lamirande E, Gagnon C. Capacitation-associated produc-tion of superoxide anion by human spermatozoa. Free Radic Biol Med 1��5; 18: 4�7-4�5 [PMID: �10123� DOI: 10.1016/0��1-5�4�(�4)0016�-K]
�2 Sikka SC, Rajasekaran M, Hellstrom WJ. Role of oxidative stress and antioxidants in male infertility. J Androl 1��5; 16: 464-46� [PMID: ��675�5]
�3 Riffo MS, Parraga M. Study of the acrosome reaction and the fertilizing ability of hamster epididymal cauda spermato-zoa treated with antibodies against phospholipase A2 and/or lysophosphatidylcholine. J Exp Zool 1��6; 275: 45�-46� [PMID: �7�52�0]
�4 Poeggeler B, Reiter RJ, Tan DX, Chen LD, Manchester LC. Melatonin, hydroxyl radical-mediated oxidative damage, and aging: a hypothesis. J Pineal Res 1��3; 14: 151-16� [PMID: �1021�0 DOI: 10.1111/j.1600-07�X.1��3.tb004��.x]
�5 Schindler AE, Christensen B, Henkel A, Oettel M, Moore C. High-dose pilot study with the novel progestogen dienoges-tin patients with endometriosis. Gynecol Endocrinol 2006; 22: �-17 [PMID: 1652252� DOI: 10.10�0/0�5135�05004314�2]
�6 Reiter RJ, Tan DX, Manchester LC, Qi W. Biochemical reac-tivity of melatonin with reactive oxygen and nitrogen spe-
Lampiao F et al . Melatonin and reproduction

15 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
cies: a review of the evidence. Cell Biochem Biophys 2001; 34: 237-256 [PMID: 11����66 DOI: 10.13�5/CBB: 34: 2: 237]
�7 Tan DX, Manchester LC, Reiter RJ, Plummer BF, Limson J, Weintraub ST, Qi W. Melatonin directly scavenges hydrogen peroxide: a potentially new metabolic pathway of melatonin biotransformation. Free Radic Biol Med 2000; 29: 1177-11�5 [PMID: 11121726 DOI: 10.1016/S0��1-5�4�(00)00435-4]
�� Hardeland R. Antioxidative protection by melatonin: multi-plicity of mechanisms from radical detoxification to radical avoidance. Endocrine 2005; 27: 11�-130 [PMID: 16217125 DOI: 10.13�5/ENDO: 27: 2: 11�]
�� Allegra M, Reiter RJ, Tan DX, Gentile C, Tesoriere L, Livrea MA. The chemistry of melatonin’s interaction with reactive species. J Pineal Res 2003; 34: 1-10 [PMID: 124�5365 DOI: 10.1034/j.1600-07�X.2003.02112.x]
�0 Reiter RJ, Tan DX, Gitto E, Sainz RM, Mayo JC, Leon J, Man-chester LC, Vijayalaxmi E, Kilic U. Pharmacological utility of melatonin in reducing oxidative cellular and molecular dam-age. Pol J Pharmacol 2004; 56: 15�-170 [PMID: 15156066]
�1 Tan DX, Manchester LC, Sainz RM, Mayo JC, Leon J, Hardeland R, Poeggeler B, Reiter RJ. Interactions between melatonin and nicotinamide nucleotide: NADH preserva-tion in cells and in cell-free systems by melatonin. J Pineal Res 2005; 39: 1�5-1�4 [PMID: 160��0�7 DOI: 10.1111/j.1600-07�X.2005.00234.x]
�2 Mayo JC, Sainz RM, Antoli I, Herrera F, Martin V, Rodriguez
C. Melatonin regulation of antioxidant enzyme gene expres-sion. Cell Mol Life Sci 2002; 59: 1706-1713 [PMID: 124751�1 DOI: 10.1007/PL000124��]
�3 Rodriguez C, Mayo JC, Sainz RM, Antolín I, Herrera F, Martín V, Reiter RJ. Regulation of antioxidant enzymes: a significant role for melatonin. J Pineal Res 2004; 36: 1-� [PMID: 14675124 DOI: 10.1046/j.1600-07�X.2003.000�2.x]
�4 Buscemi N, Vandermeer B, Hooton N, Pandya R, Tjosvold L, Hartling L, Vohra S, Klassen TP, Baker G. Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta-analysis. BMJ 2006; 332: 3�5-3�3 [PMID: 16473�5� DOI: 10.1136/bmj.3�731.532766.F6]
�5 Carr R, Wasdell MB, Hamilton D, Weiss MD, Freeman RD, Tai J, Rietveld WJ, Jan JE. Long-term effectiveness outcome of melatonin therapy in children with treatment-resistant cir-cadian rhythm sleep disorders. J Pineal Res 2007; 43: 351-35� [PMID: 17�10603 DOI: 10.1111/j.1600-07�X.2007.004�5.x]
�6 Chan WY, Ng TB. Development of pre-implantation mouse embryos under the influence of pineal indoles. J Neural Transm Gen Sect 1��4; 96: 1�-2� [PMID: 7531��1 DOI: 10.1007/BF01277�25]
�7 McElhinny AS, Davis FC, Warner CM. The effect of melato-nin on cleavage rate of C57BL/6 and CBA/Ca preimplanta-tion embryos cultured in vitro. J Pineal Res 1��6; 21: 44-4� [PMID: ��36�63 DOI: 10.1111/j.1600-07�X.1��6.tb0026�.x]
P- Reviewers Dane C, Martins WP, Zhang QX S- Editor Gou SX L- Editor A E- Editor Zheng XM
Lampiao F et al . Melatonin and reproduction
Key words: Obese women; Surgical treatment; Inconti-nence; Prolapse; Quality of life
Core tip: Pelvic floor disorders are very frequent among women. Weight loss can help them to achieve urinary and faecal continence again. In this narrative review, the possible mechanisms of pelvic floor disorders in obese women, their symptoms and the role of bariatric surgery in changing their quality of life are presented.
Iavazzo C. Role of bariatric surgery in the pelvic floor disorders. World J Obstet Gynecol 2013; 2(2): 16-20 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i2/16.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i2.16
INTRODUCTIONOverweight and obesity are defined as abnormal or exces-sive fat accumulation that presents a risk to health. Body mass index (BMI) is a simple index of weight-for-height that is commonly used to classify overweight and obesity in adults. It is defined as a person’s weight in kilograms di-vided by the square of his height in meters (kg/m2)[1]. Ac-cording to the World Health Organization, obesity is clas-sified as class Ⅰ for a BMI between 30 and 34.9 kg/m2, class Ⅱ for a BMI between 35 and 39.9 kg/m2, and class Ⅲ for a BMI ≥ 40 kg/m2[1,2]. Current data estimate that obesity is increasing worldwide especially in the devel-oped countries[1,2]. A rise is also noticed in the younger population (18 to 29 years) and especially in women[2]. The impact of obesity on quality of life is broad causing even pelvic floor disorders among other conditions.
Pelvic floor disorders (urinary or faecal incontinence and pelvic organ prolapse) are common conditions af-fecting many obese women today. The exact prevalence of pelvic floor disorders in the general population is ap-proximately 11%, but it should be higher in obese wom-en[3]. In the different studies, pelvic floor disorders affect between 2% and 42% of women, depending on the defi-nition of the condition and the study population[4-6].
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i2.16
World J Obstet Gynecol 2013 May 10; 2(2): 16-20ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Role of bariatric surgery in the pelvic floor disorders
Christos Iavazzo
Christos Iavazzo, Iaso, Maternity Hospital, 14231 Athens, GreeceAuthor contributions: Iavazzo C solely contributed to this paper.Correspondence to: Christos Iavazzo, MD, MSc, PhD, Iaso, Maternity Hospital, 38, Seizani Str., Nea Ionia, 14231 Athens, Greece. [email protected]: +30-694-8054119 Fax: +30-694-8054119Received: December 17, 2012 Revised: February 21, 2013Accepted: March 22, 2013Published online: May 10, 2013
AbstractPelvic floor disorders are very frequent among women. Weight loss can help them to achieve urinary and faecal continence again. In this narrative review, the possible mechanisms of pelvic floor disorders in obese women, their symptoms and the role of bariatric sur-gery in changing their quality of life are presented. We retrieved the included results of our study after per-forming a systematic, electronic search in PubMed (De-cember 17, 2012) and Scopus (December 17, 2012). The main mechanism causing the development of pelvic floor disorders is chronically increased abdominal pressure as it overts structural damage or neurologic dysfunction predisposing to prolapse and incontinence. The symptoms include a sensation of vaginal fullness or pressure, uterine descent, sacral back pain with stand-ing, vaginal spotting from ulceration of the protruding cervix or vagina, coital difficulty, lower abdominal dis-comfort, and voiding and defecatory difficulties. Evi-dence indicates that massive weight loss (45 to 50 kg) improves incontinence in morbidly obese women after bariatic surgery. Faecal incontinence is also improved after bariatric surgery. This review highlights the role of bariatric surgery in weight reduction of obese women that could act as a treatment for the pelvic floor disor-ders faced by those women offering improvement in incontinence as well as quality of life.
© 2013 Baishideng. All rights reserved.
MINIREVIEW
16 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com

The aim of this narrative review is to present the role of bariatric surgery operations in the improvement of the pelvic floor disorders that many obese women are facing, as well as the effect on the quality of life of obese women.
METHODSData sourcesWe retrieved the included results of our study after performing a systematic, electronic search in PubMed (December 17, 2012) and Scopus (December 17, 2012). Both PubMed and Scopus search strategy included the combination of the key words: (bariatric surgery or pelvic floor disorders) and incontinence and prolapse. Cochrane database (December 17, 2012) was also searched in order to look for any reviews on this argument. The reference list was also hand-searched for additional studies.
Study selection criteriaStudies reporting data on the role of bariatric surgery in pelvic floor disorders were included in this review. Abstracts in scientific conferences and studies published in languages other than English, German, French, Ital-ian and Spanish were excluded from this review. Studies which referred to male patients were also excluded.
ResultsThe search performed in PubMed and Scopus retrieved a total of 11 and 14 search results, respectively, among which 10 studies (7 retrospective studies, 1 letter to the editor and 2 reviews) which were identified as eligible for inclusion in this review. No additional studies were identi-fied through hand-searching of references.
Possible mechanisms explaining the correlation be-tween obesity and pelvic floor disorders.
The main mechanism causing the development of pelvic floor disorders is chronically increased abdominal pressure as it overts structural damage or neurologic dys-function predisposing to prolapse and incontinence[7-10]. Elevated abdominal and intravesical pressures are also found in patients with increased sagittal abdominal di-ameter and elevated BMI[1,2], while significant weight loss improves stress urinary incontinence[11,12]. Animal studies showed an association between obesity and urinary incontinence by evaluating urethral sphincter incontinence, urethral length or tone[13]. Some studies suggest that neurogenic disease caused by obesity might lead to pelvic floor disorders[11-13]. For example, a study proposed that the risk for abnormal median nerve con-duction was 3.5-fold greater in obese workers, while a higher incidence of lumbar disk herniation is also found in obese patients[14,15]. Other etiologic mechanisms are either the direct injury and denervation to the pelvic floor musculature or defects in the supporting system of the endopelvic fascia and ligaments[16]. Conditions such as menopausal status, chronic constipation, chronic cough, and heavy lifting major predisposing factors[17].
SymptomsMore than 90 percent of morbidly obese women experi-ence some degree of pelvic floor disorders, and 50 per-cent of these women report that symptoms adversely im-pact quality of their life[18]. In these women, obesity was found to be strongly correlated in predicting pelvic floor disorders in the same extent as obstetric history[18]. Al-though signs of pelvic organ prolapse are frequently ob-served, the condition seldom causes symptoms especially in younger ages[19]. However, vaginal or uterine descent at or through the introitus can become symptomatic. Symp-toms may also include a sensation of vaginal fullness or pressure, sacral back pain with standing, vaginal spotting from ulceration of the protruding cervix or vagina, coital difficulty, lower abdominal discomfort, and voiding and defecatory difficulties[19]. An association between obesity and urinary incontinence exists, while the association between obesity and other pelvic floor disorders is less clear. However, Chen et al[20] showed the presence of any pelvic floor disorder in 75% of the obese patients com-pared with 44% in non-obese (P < 0.0001). More obese patients experienced stress urinary incontinence, urge urinary incontinence, and anal incontinence, but not pel-vic organ prolapse. The severity of those symptoms were higher in more obese patients[20].
Bariatric surgeryBariatric surgery is suggested to be the only consistently-effective long-term treatment for morbid obesity[21]. The name “Bariatric surgery” is derived from the Greek words baros and iatriki denoting respectively “heavy weight” and “medicine”. In the United States, figures from 2010 indicate that the number of bariatric surgical operations carried out that year was 218000[22,23]. Bariatric surgery is associated with long-term weight loss and de-creased overall mortality. It could lead to a mean weight loss of between 14% and 25% (depending on the type of procedure performed) at 10 years, and a 29% reduction in all cause mortality when compared to standard weight loss measures[24]. Bariatric surgery includes a variety of procedures and its efficacy is based on both the restric-tion of the quantities of ingested food (vertical banded gastroplasty, adjustable gastric band, sleeve gastrectomy, gastric balloon and the malabsorption of the nutrients through the shunted gut (biliopancreatic diversion, endo-luminal sleeve)[25-35]. However, the main factor in the suc-cess of any bariatric surgery is still a strict post-surgical change of life attitude to a healthier pattern of eating. Since weight is a modifiable risk factor for incontinence, weight reduction may be an effective treatment. Studies of weight loss have examined its effects and explored the pathophysiologic mechanisms of improvement in pelvic floor disorders.
Role in urinary incontinenceA number of studies have shown improvements in uri-nary incontinence after bariatric surgery[8,12,36,37]. Evidence indicates that massive weight loss (45 to 50 kg) improves
17 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Iavazzo C. Bariatric surgery and pelvic floor disorders

incontinence in morbidly obese women after bariatic sur-gery[11,12]. Women who achieved a weight loss of 5%-10% or greater had at least a 50% reduction in incontinence frequency[38]. It is reported that an average weight loss of 69% of excess body weight could lead to significant changes in sagittal abdominal diameter (32 to 20 cm, P < 0.0001) and intravesical pressure (17 to 10 cmH2O, P < 0.001)[37]. In another study, a weight loss greater than 50% leads to a reduction in stress urinary incontinence from 61% to 11.6% (P < 0.001)[11]. Similar studies reported improvement in urodynamic parameters after bariatric surgery operations[8,12]. Greater weight loss was associ-ated with greater improvement of incontinence; as from the patients who lost more than 18 BMI points, 71% re-gained urinary continence[39].
Surgically induced weight loss has a beneficial effect on symptoms of pelvic floor disorders in morbidly obese women. In a questionnary based study, it was shown that the prevalence of pelvic floor disorders symptoms im-proved from 87% before surgery to 65% after surgery[40]. There was also a significant reduction in total mean dis-tress scores after surgery, which was attributed mainly to the significant decrease in urinary symptoms. Moreover, reductions in the scores were noted for the other pel-vic floor disorders, while quality of life total scores also improved. Age, parity, history of complicated delivery, percent excess body weight loss, BMI, type of weight loss procedure and presence of diabetes mellitus and hypertension had no predictive value for postoperative outcomes in the same study[40]. Cuicchi et al[41] evaluated clinically and instrumentally pelvic floor disorders before and after bariatric surgery in obese women and found that a clear association exists between BMI and urinary incontinence. Weight loss after bariatric surgery resulted in improved urinary incontinence, fecal incontinence, and symptoms of pelvic organ prolapse[41]. After a mean BMI reduction of 10 kg/m2, the prevalence of pelvic floor dis-orders decreased to 48%, with a significant improvement in quality of life. The prevalence of urinary incontinence decreased from 61% to 9.2% and was associated with the decrease in postoperative BMI (P = 0.04)[41]. A recent study also showed that weight loss after bariatric surgery can result in resolution of symptoms in nearly half of women with stress urinary incontinence and three quar-ters of women with overactive bladder and is associated with significant improvement in quality of life[42]. On the other hand, according to McDermott et al[43] the preva-lence of pelvic floor disorders did not improve greatly after surgery. More specifically, even with significant weight loss (BMI, 43.7 kg/m2 to BMI, 29 kg/m2), there was no significant difference in the prevalence of pelvic floor symptoms before and after surgery (94% to 81%, respectively) the first postoperative year. However, sig-nificant weight loss improved the degree of bother and quality of life related to these symptoms as it was shown by PFDI-20 and PFIQ-7 scores[43].
Role in faecal incontinenceThe role of obesity in faecal incontinence is less well
defined. The prevalence of faecal incontinence in the general population is reported to be 2% to 9%[5,44]. Obe-sity appears to be correlated with higher rates of faecal incontinence and diarrhoea. However, in morbidly obese patients undergoing evaluation for bariatric surgery, the prevalence of anal incontinence was notable at 32%, while incontinence of liquid stool was 21.1% and solid stool was 8.8%[45]. The effects of bariatric surgery on these conditions are not well defined. A systematic re-view showed that faecal incontinence improved after Roux-en-Y gastric bypass in studies with preoperative data, while the effects of bariatric surgery on diarrhoea were unclear[46]. It should be mentioned that one of the major disadvantages of the biliopancreatic diversion with duodenal switch operation is diarrhea. Although duode-nal switch is associated with more bowel episodes than gastric bypass, the difference is not statistically significant. More specifically, bowel habits were found to be similar in patients who achieved 50% estimated body weight loss with duodenal switch surgery or gastric bypass[47].
Quality of lifeRecently data were analyzed from 421 female patients undergoing bariatric surgery, based on a screening ques-tionnaire [“Minnesota Multiphasic Personality Inventory, 2nd ed., Restructured Form (MMPI-2-RF)”]. The women were dichotomized as those pelvic floor disorders (n = 121) and those without pelvic floor disorders (n = 300)[48]. Women with pelvic floor disorders were found to be more psychiatrically vulnerable. More specifically, they were significantly older and more likely to evidence a his-tory of substance abuse/dependence and depression. A trend was also found for previous inpatient hospitaliza-tion, outpatient behavioral health treatment, and psycho-tropic medication usage[48]. For this reason, one could understand that bariatric surgery could offer better conti-nence control, quality of life and psychological balance.
CONCLUSIONBariatric surgery can lead to significantly weight reduction of obese women. This method also acts as a treatment for the pelvic floor disorders that those women face by offering improvement in incontinence and quality of life.
REFERENCES1 World Health Organization. Obesity and overweight. Avail-
able from: URL: http://www.who.int/dietphysicalactivity/publications/facts/obesity/en/
2 Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks JS. Prevalence of obesity, diabetes, and obe-sity-related health risk factors, 2001. JAMA 2003; 289: 76-79 [PMID: 12503980 DOI: 10.1001/jama.289.1.76]
3 Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997; 89: 501-506 [PMID: 9083302 DOI: 10.1016/S0029-7844(97)00058-6]
4 Melville JL, Katon W, Delaney K, Newton K. Urinary in-continence in US women: a population-based study. Arch Intern Med 2005; 165: 537-542 [PMID: 15767530 DOI: 10.1001/
18 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Iavazzo C. Bariatric surgery and pelvic floor disorders

archinte.165.5.537]5 Kalantar JS, Howell S, Talley NJ. Prevalence of faecal in-
continence and associated risk factors; an underdiagnosed problem in the Australian community? Med J Aust 2002; 176: 54-57 [PMID: 11936284]
6 Morrill M, Lukacz ES, Lawrence JM, Nager CW, Contreras R, Luber KM. Seeking healthcare for pelvic floor disorders: a population-based study. Am J Obstet Gynecol 2007; 197: 86.e1-86.e6 [PMID: 17618770]
7 Noblett KL, Jensen JK, Ostergard DR. The relationship of body mass index to intra-abdominal pressure as measured by multichannel cystometry. Int Urogynecol J Pelvic Floor Dysfunct 1997; 8: 323-326 [PMID: 9609328 DOI: 10.1007/BF02765589]
8 Lara MD, Kothari SN, Sugerman HJ. Surgical management of obesity: a review of the evidence relating to the health benefits and risks. Treat Endocrinol 2005; 4: 55-64 [PMID: 15649101 DOI: 10.2165/00024677-200504010-00006]
9 Bouldin MJ, Ross LA, Sumrall CD, Loustalot FV, Low AK, Land KK. The effect of obesity surgery on obesity comorbid-ity. Am J Med Sci 2006; 331: 183-193 [PMID: 16617233 DOI: 10.1097/00000441-200604000-00004]
10 Lambert DM, Marceau S, Forse RA. Intra-abdominal pres-sure in the morbidly obese. Obes Surg 2005; 15: 1225-1232 [PMID: 16259876 DOI: 10.1381/096089205774512546]
11 Deitel M, Stone E, Kassam HA, Wilk EJ, Sutherland DJ. Gynecologic-obstetric changes after loss of massive excess weight following bariatric surgery. J Am Coll Nutr 1988; 7: 147-153 [PMID: 3361039]
12 Bump RC, Sugerman HJ, Fantl JA, McClish DK. Obesity and lower urinary tract function in women: effect of surgically induced weight loss. Am J Obstet Gynecol 1992; 167: 392-397; discussion 397-399 [PMID: 1497041]
13 Cummings JM, Rodning CB. Urinary stress incontinence among obese women: review of pathophysiology therapy. Int Urogynecol J Pelvic Floor Dysfunct 2000; 11: 41-44 [PMID: 10738933 DOI: 10.1007/s001920050008]
14 Nathan PA, Keniston RC, Myers LD, Meadows KD. Obesity as a risk factor for slowing of sensory conduction of the median nerve in industry. A cross-sectional and longitudinal study involving 429 workers. J Occup Med 1992; 34: 379-383 [PMID: 1564575]
15 Heliövaara M. Body height, obesity, and risk of herniated lum-bar intervertebral disc. Spine (Phila Pa 1976) 1987; 12: 469-472 [PMID: 3629398 DOI: 10.1097/00007632-198706000-00009]
16 Bidmead J, Cardozo LD. Pelvic floor changes in the older woman. Br J Urol 1998; 82 Suppl 1: 18-25 [PMID: 9883258 DOI: 10.1046/j.1464-410X.1998.0820s1018.x]
17 Lin SY, Tee YT, Ng SC, Chang H, Lin P, Chen GD. Changes in the extracellular matrix in the anterior vagina of women with or without prolapse. Int Urogynecol J Pelvic Floor Dysfunct 2007; 18: 43-48 [PMID: 16547686 DOI: 10.1007/s00192-006-0090-1]
18 Wasserberg N, Haney M, Petrone P, Ritter M, Emami C, Rosca J, Siegmund K, Kaufman HS. Morbid obesity adverse-ly impacts pelvic floor function in females seeking attention for weight loss surgery. Dis Colon Rectum 2007; 50: 2096-2103 [PMID: 17899277 DOI: 10.1007/s10350-007-9058-6]
19 Baden WF, Walker TA. Genesis of the vaginal profile: a cor-related classification of vaginal relaxation. Clin Obstet Gyne-col 1972; 15: 1048-1054 [PMID: 4649139 DOI: 10.1097/00003081-197212000-00020]
20 Chen CC, Gatmaitan P, Koepp S, Barber MD, Chand B, Schau-er PR, Brethauer SA. Obesity is associated with increased prevalence and severity of pelvic floor disorders in women considering bariatric surgery. Surg Obes Relat Dis 2009; 5: 411-415 [PMID: 19136310 DOI: 10.1016/j.soard.2008.10.006]
21 National Institute of Health. Gastrointestinal Surgery for Se-vere Obesity. March 25-27, 1991. Available from: URL: http://consensus.nih.gov/1991/1991GISurgeryObesity084html.htm
22 Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric
surgical procedures. JAMA 2005; 294: 1909-1917 [PMID: 16234497 DOI: 10.1001/jama.294.15.1909]
23 Buchwald H, Oien DM. Metabolic/bariatric surgery World-wide 2008. Obes Surg 2009; 19: 1605-1611 [PMID: 19885707 DOI: 10.1007/s11695-009-0014-5]
24 Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, Lystig T, Sullivan M, Bouchard C, Carlsson B, Bengtsson C, Dahlgren S, Gummesson A, Jacobson P, Karls-son J, Lindroos AK, Lönroth H, Näslund I, Olbers T, Stenlöf K, Torgerson J, Agren G, Carlsson LM. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007; 357: 741-752 [PMID: 17715408 DOI: 10.1056/NEJ-Moa066254]
25 Abell TL, Minocha A. Gastrointestinal complications of bar-iatric surgery: diagnosis and therapy. Am J Med Sci 2006; 331: 214-218 [PMID: 16617237 DOI: 10.1097/00000441-200604000-00008]
26 Intestinal ‘Sleeve’ Mimics Effects of Gastric Bypass. Health-Day News. December 4, 2008
27 http://www.medpagetoday.com/Endocrinology/Diabe-tes/17008
28 Schouten R, Rijs CS, Bouvy ND, Hameeteman W, Koek GH, Janssen IM, Greve JW. A multicenter, randomized efficacy study of the EndoBarrier Gastrointestinal Liner for presurgical weight loss prior to bariatric surgery. Ann Surg 2010; 251: 236-243 [PMID: 19858703 DOI: 10.1097/SLA.0b013e3181bdfbff]
29 Stanczyk M, Martindale R., Deveney C. Bariatric surgery overview. In: Berdanier CD, Feldman EB, Dwyer J. Hand-book of Nutrition and Food. Boca Raton, FL: CRC Press, 2007: 915-926
30 Shikora SA, Kim JJ, Tarnoff ME. Nutrition and gastrointesti-nal complications of bariatric surgery. Nutr Clin Pract 2007; 22: 29-40 [PMID: 17242452 DOI: 10.1177/011542650702200129]
31 Freitas A, Sweeney JF. Bariatric surgery. In: Banerjee B, editor. Nutritional Management of Digestive Disorders. Boca Raton, FL: CRC Press, 2010: 327-342 [DOI: 10.1201/9781420086553-21]
32 http://bariatrictimes.com/2009/06/18/laparoscopic-sleeve-gastrectomy/Bariatrictimes.com
33 Mathus-Vliegen EM. Intragastric balloon treatment for obe-sity: what does it really offer? Dig Dis 2008; 26: 40-44 [PMID: 18600014 DOI: 10.1159/000109385]
34 Rosenthal, Elisabeth (January 3, 2006). “Europeans Find Extra Options for Staying Slim”. The New York Times. Re-trieved April 26, 2010. Available from: URL: http://query.nytimes.com/gst/fullpage.html?res=9400EED61030F930A35752C0A9609C8B63&sec=health&pagewanted=all
35 http://thehealthclinic.org.uk/procedures-2/weight-loss-surgery/gastric-balloon
36 Gastrointestinal surgery for severe obesity. Consens Statement 1991; 9: 1-20 [PMID: 1760489]
37 Sugerman H, Windsor A, Bessos M, Kellum J, Reines H, De-Maria E. Effects of surgically induced weight loss on urinary bladder pressure, sagittal abdominal diameter and obesity co-morbidity. Int J Obes Relat Metab Disord 1998; 22: 230-235 [PMID: 9539191 DOI: 10.1038/sj.ijo.0800574]
38 Subak LL, Johnson C, Whitcomb E, Boban D, Saxton J, Brown JS. Does weight loss improve incontinence in moderately obese women? Int Urogynecol J Pelvic Floor Dysfunct 2002; 13: 40-43 [PMID: 11999205 DOI: 10.1007/s001920200008]
39 Burgio KL, Richter HE, Clements RH, Redden DT, Goode PS. Changes in urinary and fecal incontinence symptoms with weight loss surgery in morbidly obese women. Obstet Gyne-col 2007; 110: 1034-1040 [PMID: 17978117 DOI: 10.1097/01.AOG.0000285483.22898.9c]
40 Wasserberg N, Petrone P, Haney M, Crookes PF, Kaufman HS. Effect of surgically induced weight loss on pelvic floor disorders in morbidly obese women. Ann Surg 2009; 249: 72-76 [PMID: 19106678 DOI: 10.1097/SLA.0b013e31818c7082]
19 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Iavazzo C. Bariatric surgery and pelvic floor disorders

41 Cuicchi D, Lombardi R, Cariani S, Leuratti L, Lecce F, Cola B. Clinical and instrumental evaluation of pelvic floor disor-ders before and after bariatric surgery in obese women. Surg Obes Relat Dis 2013; 9: 69-75 [PMID: 21978747]
42 Whitcomb EL, Horgan S, Donohue MC, Lukacz ES. Impact of surgically induced weight loss on pelvic floor disorders. Int Urogynecol J 2012; 23: 1111-1116 [PMID: 22527554 DOI: 10.1007/s00192-012-1756-5]
43 McDermott CD, Terry CL, Mattar SG, Hale DS. Female pel-vic floor symptoms before and after bariatric surgery. Obes Surg 2012; 22: 1244-1250 [PMID: 22258196]
44 Nelson R, Norton N, Cautley E, Furner S. Community-based prevalence of anal incontinence. JAMA 1995; 274: 559-561 [PMID: 7629985 DOI: 10.1001/jama.1995.03530070057030]
45 Richter HE, Burgio KL, Clements RH, Goode PS, Redden DT, Varner RE. Urinary and anal incontinence in morbidly
obese women considering weight loss surgery. Obstet Gyne-col 2005; 106: 1272-1277 [PMID: 16319252 DOI: 10.1097/01.AOG.0000187299.75024.c4]
46 Poylin V, Serrot FJ, Madoff RD, Ikramuddin S, Mellgren A, Lowry AC, Melton GB. Obesity and bariatric surgery: a sys-tematic review of associations with defecatory dysfunction. Colorectal Dis 2011; 13: e92-103 [PMID: 21564470 DOI: 10.1111/j.1463-1318.2011.02584.x]
47 Wasserberg N, Hamoui N, Petrone P, Crookes PF, Kaufman HS. Bowel habits after gastric bypass versus the duodenal switch operation. Obes Surg 2008; 18: 1563-1566 [PMID: 18752029 DOI: 10.1007/s11695-008-9658-9.]
48 Merrell J, Brethauer S, Windover A, Ashton K, Heinberg L. Psychosocial correlates of pelvic floor disorders in women seeking bariatric surgery. Surg Obes Relat Dis 2012; 8: 792-796 [PMID: 22426031 DOI: 10.1016/j.soard.2012.01.019]
P- Reviewers Athanasopoulos A, F Duenas O, Papatsoris AG S- Editor Wen LL L- Editor A E- Editor Zheng XM
20 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Iavazzo C. Bariatric surgery and pelvic floor disorders

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i2.21
World J Obstet Gynecol 2013 May 10; 2(2): 21-33ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Past, present and future of primary systemic treatment in breast cancer
José L Alonso-Romero, Antonio Piñero-Madrona
José L Alonso-Romero, Antonio Piñero-Madrona, Depart-ment of Oncology and Surgery, “Virgen de la Arrixaca” Univer-sity Hospital, 30120 Murcia, SpainAuthor contributions: Alonso-Romero JL and Piñero-Madrona A contributed to the conception, design, writing and final ap-proval.Correspondence to: Antonio Piñero-Madrona, MD, PhD, Department of Surgery, “Virgen de la Arrixaca” University Hos-pital, Ctra Madrid-Cartagena s/n, 30120 Murcia, Spain. [email protected]: +34-968-369677 Fax: +34-968-395537Received: January 27, 2013 Revised: February 12, 2013Accepted: April 10, 2013Published online: May 10, 2013
AbstractPrimary systemic treatment is a fundamental part of breast cancer therapy, and it is applied to non-surgical and locally advanced tumours as well as surgical tu-mours to increase the likelihood of conservative treat-ment. Its aim is to achieve the best possible survival with better cosmetic results and with the lowest num-ber of treatment-related secondary effects. Before treatment is started, it is necessary to attain the best knowledge of the biological features and locoregional extension of the tumour. To do so, it is necessary to obtain a biopsy of the lesion with a wide bore needle, as well as good radiological knowledge of the disease. Therefore, currently, the use of a dynamic magnetic resonance imaging (MRI) of the breast should be in-cluded in all cases. In addition, before it is started, especially in those tumours in which conservative treatment is considered, one or several radiopaque markers should be put into place to make it possible to locate the area to be treated if there is a considerable or complete response. Systemic treatment is mainly based on combined chemotherapy with anthracyclins and taxanes, in addition to some biological agents with demonstrated efficiency for increasing the likelihood
of complete disease response (trastuzumab in patients with Her-2/neu overexpression). However, there is room for neoadjuvant hormone treatment, in patients with hormone receptor overexpression, especially in those cases in which chemotherapy is contraindicated as well as in elderly patients with a relatively short life expectancy. The assessment of preoperative treatment should be based on adequate radiological tests, and nowad these should include MRI before taking deci-sions about adequate surgical treatment. The objective of primary treatment is to be able to increase survival and improve the chances of local treatment in the case of locally advanced treatment, achieving results that are at least equal to those of adjuvant treatment in the case of surgical tumours, but with greater chances of conservative surgery. Although the objective is survival, achieving complete pathological response seems to be a reasonable related objective, although these are more closely linked in some tumour subtypes.
© 2013 Baishideng. All rights reserved.
Key words: Breast cancer; Breast carcinoma; Primary systemic therapy; Neoadjuvant chemotherapy; Neoad-juvant therapy
Core tip: Primary systemic treatment is a fundamental part of breast cancer therapy, and it is applied to non-surgical and locally advanced tumours as well as surgi-cal tumours to increase the likelihood of conservative treatment. As in any kind of tumour, an attempt should be made to include these patients in clinical trials to allow us to define the best and earliest individualised treatment strategy for our patients.
Alonso-Romero JL, Piñero-Madrona A. Past, present and future of primary systemic treatment in breast cancer. World J Obstet Gynecol 2013; 2(2): 21-33 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i2/21.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i2.21
MINIREVIEW
21 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com

Alonso-Romero JL et al . Primary systemic treatment in breast cancer
INTRODUCTIONIn the specific case of breast cancer, two overriding theo-ries of the biological behaviour of tumors in terms of their mechanisms of metastatic dissemination have pre-dominated over the past two centuries, paving the way for two opposing paradigms: Halsted’s mechanistic theory and Fisher’s systemic theory. However, observations and evidence from subsequent studies have revealed that an intermediate theory, Hellman’s spectrum theory, is more realistic and accounts for the differences observed in dif-ferent kinds of scenarios[1].
In light of this historical background, the treatment of most malignant tumours is complex and requires in-terdisciplinary teams of physicians who are specialists in various fields working holistically to control them.
Therefore, breast cancer should be considered as a systemic disease in order to achieve optimal management outcomes, at least from a conceptual point of view. This should be the case even when cancer is theoretically con-fined to this organ (localized breast cancer) and requires local and systemic treatment for its control.
Systemic adjuvant treatment (hormone therapy, che-motherapy, immunotherapy, biological therapy against a specific molecular target), used to control micrometastat-ic disease after curative intent surgery, has been proven to reduce recurrence risk by 0.77 and breast cancer mortal-ity by 0.83[2]. This benefit has been attained, although to a varying degree, regardless of axillary lymph node infiltra-tion, the state of the hormonal receptors, the histologi-cal subtype, the level of tumour differentiation, or the expression of other predictive response factors (Her-2/neu).
However, for some patients adjuvant treatment is not the best approach and the use of neoadjuvant chemo-therapy (primary or preoperative) is preferred before the local treatment of the disease.
Consequently, neoadjuvant treatment has transformed from a treatment for patients with locally advanced breast cancer (making surgery more likely in tumours in which local treatment with curative intent could not be guaran-teed), into the treatment used in initially surgical tumours to enable conservative breast surgery. Taking into ac-count that neoadjuvant and adjuvant chemotherapy pro-vide similar benefits in terms of overall and disease-free survival in operable tumours[3], neoadjuvant treatment is currently providing a greater knowledge of the in vivo ef-fects of modern treatment options in tumours prior to surgery.
PRELIMINARY TERMINOLOGICAL CONSIDERATIONSFrom chemotherapy to systemic therapyClassically, the systemic cancer treatment was based on the use of chemotherapy, that is, medication against neo-plastic tissues with greater or lesser sensitivity and speci-ficity, which directly influences the real achilles heel of
this treatment: morbidity associated with the secondary effects of the toxicity of non neoplastic cells and tissues. Nowad, other modalities must be considered which are not related to classical chemotherapy. This is the situation with hormone therapy, which has a fundamental role in the specific case of breast cancer, or with the application of molecular-targeted therapies, through monoclonal an-tibodies, or immune tolerance induction (or suppression) therapies through vaccines or antibodies. These therapies try to increase effectiveness against different types of cancers by attempting to increase the specificity of treat-ment and to avoid these secondary effects.
For all of these reasons, the most appropriate term we should adopt is "systemic therapy" given that it en-compasses the different therapeutic modalities, in addi-tion to chemotherapy.
From neoadjuvancy to primary therapyAt first glance the term neoadjuvant therapy was used to refer to the fact that the therapy is administered before other treatments considered as main ones, unlike adjuvant therapy which was assigned after these treatments. Thus, a temporal relationship was explicitly established, involv-ing an implicit subordination of importance between the treatments according to when they were applied. How-ever, two points should be made: firstly the treatment of any type of cancer is usually multimodal, as it should be, with aspects of the treatment targeted at treating the pri-mary tumour and others focussed more on avoiding or treating its dissemination, and which should generally be considered as having a complementary application. The second point refers to the importance of different treat-ment strategies used in cancer, which are determined by their effectiveness, efficacy (and even efficiency) and are not based on whether they are administered at an earlier or later stage. In this way, the sequencing of the differ-ent treatments is a secondary aspect and priority must be given to carrying out the most comprehensive treatment possible: it would be just as pointless to treat the primary tumour without worrying about the occurrence of dis-tant dissemination as it would be to treat the disease as a whole while underestimating the primary focus of the disease thus allowing the persistence or recurrence of locoregional disease which could contribute to a potential focus of future dissemination. Therefore, it would be convenient to sideline the terms referring to the connota-tions of “main role” or “adjuvancy” of treatment options and to keep to those that refer to temporal sequence (pri-mary).
HISTORY OF NEOADJUVANT CHEMOTHERAPY: THE REASON FOR PRIMARY TREATMENTNeoadjuvant chemotherapy was first reported in breast cancer in the 1970s as an early-stage treatment for inop-erable locally advanced tumours[4] and in several studies
22 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com

carried out between 1980-1990 which showed an im-provement in the surgery rates in these patients, as well as an improvement in their survival rate, so that it became established as part of the initial standard treatment in these patients.
As well as allowing for the surgery of these tumours that were initially non-surgical and improving the survival rate of these patients, it was found that primary chemo-therapy could play a role in reducing the initial size of tumours thus making it possible to perform conservative surgery in patients in which mastectomy had initially been established as the surgical treatment. In this situation, it had to be demonstrated that primary chemotherapy was able to achieve the same effects already shown by adjuvant chemotherapy in the reduction of recurrence and overall and disease-free survival[1], and also in the im-provement of the percentage of patients in which con-servative surgery could be performed.
Many non-randomised studies have investigated the ability of neoadjuvant chemotherapy to increase the possibilities of conservative treatment in surgical breast cancer. Generally, the results obtained in these studies us-ing this kind of chemotherapy achieved clinical response rates of between 67%-85%, with complete pathological responses of nearly 3% and conservative surgery rates of 85%[5-7].
Several studies have prospectively and randomly anal-ysed phase Ⅲ trials on the use of adjuvant chemotherapy compared with the same chemotherapy administered neoadjuvantly in patients with operable breast cancer without revealing any difference in overall survival or disease free survival and achieving a significant increase in the rates of conservative surgery of breast cancer. It is worth highlighting two studies due to their design and the number of patients included: NSABP B-18[8] and EORTC 10902[9].
In the NSABP B-18[8] study, 1523 patients diagnosed with surgical breast cancer (T1-3, N0-1) were randomly administered 4 cycles of chemotherapy with adriamycin and cyclophosphamide (60-600 mg/m2) as neoadju-vant or adjuvant chemotherapy. A clinical response was achieved in 79% of the patients treated with neoadjuvant chemotherapy, with 36% complete clinical responses and 13% complete pathological responses. What is more, 68% conservative surgeries were achieved in the neoad-juvant chemotherapy arm compared to 60% in the initial surgery arm, especially in patients with tumours greater than 5 cm in diameter.
With more than 15 years of follow-up no differences were found between both groups in terms of survival. An increase in local ipsilateral recurrence was observed in patients receiving primary chemotherapy (10.7 vs 7.6) especially in patients under 50 years, which was attributed to the fact that they were not treated with tamoxifen, although this absence of hormone treatment occurred equally in both treatment arms.
In addition, those patients that achieved complete pathological response had a significant improvement in
terms of disease-free survival and overall survival com-pared to those who had residual disease after neoadjuvant chemotherapy.
In the EORTC 10902[9] study, 698 patients diagnosed with breast cancer (T1-4, N0-1) were treated with 4 cy-cles of 5-fluorouracil, epirubicin and cyclophosphamide (600-60-600 mg/m2) administered adjuvantly and neoad-juvantly. The response obtained in patients treated with primary chemotherapy was 49% with 4% complete pa-thology responses. A 23% conservative surgery rate was achieved in patients initially programmed for mastectomy before neoadjuvant chemotherapy.
With a follow-up period of more than 4 years, there were no differences in disease-free survival, overall sur-vival or locoregional recurrence. Significantly, the patients treated with neoadjuvant chemotherapy with complete pathological response had a significant advantage in terms of survival compared to patients with residual dis-ease.
In 2005, Mauri et al[10] reported a meta-analysis of 9 randomised studies, including 3946 patients, that faced the same adjuvant and neoadjuvant systemic treatment administered for local treatment (surgery or radiotherapy). There were no differences in terms of survival [RR = 1.00 (95%CI: 0.90-1.12)], disease-free survival [RR = 0.99 (95%CI: 0.91-1.12)] or progression free survival [RR = 0.94 (95%CI: 0.83-1.06)], although there was an increased possibility of local recurrence in patients treated with neo-adjuvant chemotherapy [RR = 1.22 (95%CI: 1.04-1.43)], probably because in those patients in which it was admin-istered it was decided not perform surgery and to treat the patients exclusively with locoregional radiotherapy [RR = 1.53 (95%CI: 1.11-2.10)].
Therefore it can be concluded that neoadjuvant che-motherapy is fundamental for the primary treatment of locally advanced tumours, and that in surgical tumours it is an alternative to adjuvant chemotherapy, offering the same survival rate and a comparatively significant increase in conservative treatment rates.
CURRENT SITUATION OF PRIMARY THERAPY: CERTAINTIES AND CONTROVERSIESIndicationsThe use of primary systemic therapy is currently indi-cated in two situations:
The initial treatment of non-surgical locally advanced tumours, before locoregional treatment: (1) for patients with locally advanced or inflammatory tumours, initial sys-temic treatment allows for the use of subsequent locore-gional treatment, which would not have been possible in the first place, and it also provides an added improvement in survival and disease free survival. In these patients, no randomised studies have been carried out for compar-ing neoadjuvant and adjuvant treatment given that initial surgical treatment is impossible; and (2) in the treatment
23 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

of these patients we know that when complete pathologi-cal response is achieved there is an advantage in survival compared to when complete response is not attained[11,12].
The initial treatment of tumours in which conserva-tive treatment is considered this should be as a more like-ly option than radical surgery (mastectomy). In these pa-tients we know that there are similar survival and disease free survival rates in those treated with either neoadjuvant or adjuvant chemotherapy. This means that there is no clear disadvantage for neoadjuvant treatment in terms of locoregional recurrence when it allows for an increase in the possibilities of conservative treatment provided that it is followed by correct hormone treatment and locore-gional radiotherapy if required[10].
From a theoretical viewpoint there are advantages to neoadjuvant treatment compared to the adjuvant variety: (1) the possibility of demonstrating the in vivo efficacy of the therapeutic agents used by assessing tumour response, offering the theoretical advantage of being able to replace those treatment options that are not useful by others which display a better antitumoral response. However, these “made to measure” treatments have shown no ad-vantage in terms of survival or disease free survival; and (2) identifying biomarkers that allow us to obtain early infor-mation about the antitumor activity of the two treatment options would allow us to take faster decisions when we use survival as the fundamental variable.
However, the feasible use of primary systemic treat-ment could also have disadvantages for initial surgical treatment: It could delay the use of local curative-intent treatment in surgical tumours that could be resistant to systemic treatment. It has been confirmed that this re-sistance is uncommon but it accounts for around 5% in most studies[8,9,13,14]. It could lead to difficulties for carrying out a correct clinical locoregional staging prior to surgery, preventing the selection of an appropriate systemic treat-ment or leading to an incorrect disease prognosis being established at a later stage. Nowad, this is less important because initial systemic treatment is very homogeneous from the beginning (with the use of anthracyclines and taxanes) and is mainly based on known biological factors (e.g., the use of trastuzumab/lapatinib in patients with overexpressed Her-2/neu), and additionally we can make accurate locoregional staging through the study of the sentinel node prior to neoadjuvant chemotherapy.
Selection of patients who are candidates for primary treatmentThe following patients are candidates for this treatment: (1) patients diagnosed with non-surgical locally advanced breast cancer: tumours greater than 5 cm in diameter (T3), or attached to the thoracic wall (T4a), or with skin ulceration or satellite lesions (T4b), or both (T4c); axillary lymph nodes attached to each other (N2); supraclavicular lymph node involvement (N3); inflammatory tumours (T4d); (2) patients diagnosed with surgical breast cancer, to increase the chances of conservative surgery. Tradition-ally, a 3 cm tumour diameter has been accepted as the cut-
off point although some studies have included tumours of 2 cm. From a practical point of view this treatment can be offered to all patients who have an a priori dis-proportion between the tumor and breast size which presupposes mastectomy or a poor cosmetic result after initial conservative treatment; (3) patients contraindicated against surgery and in whom surgery should be delayed: a recent acute myocardial infarction, a recent cerebrovascu-lar accident, pregnancy, et al; and (4) fragile elderly patients in which surgery would involve too high a risk and who could benefit from initial medical treatment.
Diagnosis and staging in patients before systemic therapyInitial diagnosis should be carried out before starting pri-mary systemic treatment and preferably through biopsy using a wide bore needle rather than a fine needle, located either by palpation or, better still, guided by ultrasound. In addition to confirming the existence of tumor invasion, this biopsy should provide enough tissue for the study of estrogen, progesterone and Her-2/neu receptors, as well as other biological markers that could be used in other re-search studies.
Initial staging should make use of the TNM system, and the “c” prefix is advised in pretreatment staging and “y” in pathological staging after surgery. For the assess-ment of lymph node staging it is recommended to use the “c” when assessment is clinical or radiological, “f ” if it included fine needle aspirations and “sn” if a study of the sentinel gland has been carried out.
All the patients should have had a thorough physical examination, at least one bilateral mammography exam, a breast ultrasound analysis, and correct systemic staging, above all in the case of locally advanced tumours to rule out distant metastasis.
LOCOREGIONAL STAGINGAssessment of the primary tumourBefore beginning primary chemotherapy a locoregional analysis should be carried out which should include a physical examination, a bilateral breast analysis, a breast ultrasound study, and in addition, the lesion should be located with a radiopaque (clip) marker which makes it possible to locate the lesion after chemotherapy in prepa-ration for surgical treatment when there is a complete clinical response[15,16].
Magnetic resonance imaging (MRI) provides high defi-nition anatomical images of the breast and the tumour, as well as the dynamic study of the uptake and elimination of contrast making it possible to define the existence of other tumour foci not seen using conventional analyses (multicentricity and multifocality). In addition, it allows for a better definition of possible chest wall involvement. However, although its sensitivity is greater than that of other radiological techniques, its specificity is not so sharp, so that it identifies suspicious lesions that are not malign, often leading to overtreatment.
24 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

Currently, a histological analysis is recommended (tak-ing a biopsy with a fine or wide bore needle) of the po-tentially malignant lesions identified using MRI, if these findings alter the plan initially set out. These lesions could be located using guided ultrasound (second-look)[17] or otherwise using a MRI-guided biopsy, for which there are specific kits available[18].
The positioning of a radiopaque marker could be done at the time of the ultrasound-guided histological diagnosis, when the need for neoadjuvant treatment is ini-tially considered. Alternatively, it can be done at a second stage, before beginning treatment or once it has been started and treatment response has been seen, although in the latter case it is important to closely monitor the response to avoid the disappearance of the lesion before being marked. It is particularly useful for locating the area for carrying out conservative surgical treatment if a com-plete clinical and radiological response is achieved, and to guide the pathologist in the search for tumor remnants and to identify microscopic disease persistence or a truly complete pathological response[1,19].
Axillary lymph node assessmentIt is particularly important to carry out axillary lymph node assessment before the start of neoadjuvant chemo-therapy in those patients who are surgical from the out-set, although it can also be beneficial in selected cases for some patients with locally advanced disease.
Its utility is guaranteed because it allows for patient prognosis as well as the choice of chemotherapy for treatment (e.g., the addition of taxanes to the anthracy-clins if there is lymph node affectation).
However, this need could change in the years to come, especially if we take into account that the addition of taxanes seems to be beneficial to the adjuvant treatment of patients with negative lymph nodes. In addition, the prognostic and therapeutic assessment of the disease increasingly depends on biological factors analysed in the primary tumour rather than on classical prognostic fac-tors such as axillary lymph node infiltration.
This assessment can be carried out through physical examination, axillary radiological examination (mainly ul-trasound) and fine needle aspiration of the suspicious le-sions, but clearly the best assessment is achieved through selective analysis of the sentinel node. These techniques have a sensitivity of between 70% and 90%, but this is lower where axillary involvement is due to micrometasta-sis.
Selective analysis of the sentinel nodeIt is debatable whether the sentinel node should be stud-ied before or after chemotherapy in patients with operable breast tumours with clinically negative lymph nodes if they are going to be treated using primary systemic treat-ment[20].
The analysis of the sentinel node after neoadjuvant chemotherapy is made difficult by the fact that it is identi-fied to a lower extent, probably due to structural changes
in lymphatic drainage brought about by chemotherapy, and a greater percentage of false negatives due to chemo-therapy response.
The potential advantages of the analysis of the sen-tinel node before chemotherapy include the prevention of these confusions caused by the chemotherapy itself, together with the guarantee of the appropriate choice of systemic treatment and the correct subsequent locore-gional treatment after it has been completed, preventing unnecessary axillary lymph node dissections or reducing the volume of locoregional radiotherapy.
However, this procedure involves subjecting the pa-tient to two operations and only on a few occasions will it modify the type of chemotherapy that will be received; systemic treatment usually includes anthracyclins and tax-anes for achieving the best possible response and this is mainly decided upon according to the studies of biologi-cal markers in the biopsy of the primary tumour.
A systematic review of 27 studies including 2148 pa-tients subjected to a selective biopsy of the sentinel node after chemotherapy confirmed that the lymph node was identified in 91% of patients (95%CI: 88-93) and the false negatives were 10.5% (95%CI: 8.1-13.6)[21]. This study concluded that during surgery of the primary tumour and after neoadjuvant chemotherapy, the sentinel node is a useful tool for considering post chemotherapy treatment.
Few data are available comparing the pre and post chemotherapy procedure. In a series of cases in which the first 31 were carried out after chemotherapy and a further 58 before, it was found that in 99% vs 87% the sentinel node was identified and there were false negative rates of 0% vs 16% (pre vs post)[22].
No data are available for comparison of the biopsy before and after neoadjuvant chemotherapy over a pro-longed follow-up period making the treatment of choice a matter of opinion. While there are data that lead us to believe that this analysis is a useful tool after chemo-therapy, doing it beforehand is going to bring about a more precise knowledge of the situation and will allow for maximum subsequent locoregional treatment (axillary radiotherapy).
Systemic stagingIn addition to the locoregional staging (axillary and primary tumour) previously reported, before beginning treatment it is necessary to perform a correct systemic staging of the disease. As a general rule, and following the recommenda-tions of the published guidelines, it would be enough to test surgical tumours using adequate anamnesis, a thor-ough physical examination, radiography of the thorax and a comprehensive medical analysis including bone and hepatic biochemical tests. Analysis with computerized axial tomography, bone scintigraphy or even positron emission tomography (PET) or PET with computed axial tomog-raphy (PET/CAT) would be performed when considered necessary due to any alterations in the previous test results.
In the case of locally advanced tumours, and given that the possibilities of distant dissemination from diag-
25 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

nosis are higher, computerized axial tomography would be indicated from the beginning, leaving bone scintigraphy and PET/CAT for those situations in which it was con-sidered as a clinical recommendation or there were suspi-cious alterations in the tests previously carried out.
Choice of neoadjuvant treatmentThere are many possible treatment options with neo-adjuvant intent: hormone therapy, targeted therapeutic treatment, to name a few, but the treatment of choice is mostly going to be based on polychemotherapy.
Neoadjuvant hormone therapyMost of the studies published on primary systemic treat-ment are based on combination chemotherapy, but recent studies with neoadjuvant hormone therapy are being re-ported, especially in elderly patients or in those in which for some reason the chemotherapy is considered as an unacceptable treatment option.
Most of the studies carried out are about tamoxifen, although in recent years data is becoming available on studies with aromatase inhibitors.
In 2009, Syed et al[23] published a study in ASCO com-paring treatment with adjuvant tamoxifen after surgery or tamoxifen administered exclusively without surgery, in 1031 elderly patients with operable breast tumours. The 5-year survival rate was greater in those patients treated with surgery than in those that were only treated with tamoxifen (95% vs 85%) in patients between 70 and 80 years of age, but survival was the same in those over 80 years (90% for both), and it was concluded that in these patients with a short life expectancy exclusive ad-ministration of tamoxifen could prevent surgical treat-ment.
Few data are available comparing hormone therapy with neoadjuvant chemotherapy.
A randomized phase Ⅱ study compared 3 mo treat-ment with exemestane or anastrozol with 4 cycles of chemotherapy with adriamycin and paclitaxel in 121 post-menopausal patients with positive hormone receptors. There were no differences in median time until response (57 d vs 51 d), complete pathological response (3% vs 6%) or clinical response (67% and 62% in exemestane and anastrozol vs 63% in chemotherapy). No differences were found regarding conservative breast surgery (33% vs 24%) or locoregional recurrences (3.3% vs 3.4%)[24].
No differences were found in either premenoupausal patients in complete response or clinical response or in type of surgery when faced with exemestane and gosere-lin treatment with 4 cycles of epirubicin-cyclophospha-mide followed by 4 cycles of docetaxel[25].
In general and with the data available until now it could be said that the preference for neoadjuvant che-motherapy over hormone therapy is reserved for patients in which chemotherapy is not indicated and in which surgery is not the only initial option (patients with locally advanced or surgical tumours contraindicated for surgery and chemotherapy).
Hormone treatment is an alternative to surgery in tumours in elderly patients with a relatively short life ex-pectancy.
Among the hormone treatments available, the treat-ment of choice is aromatase inhibitors rather than tamox-ifen, given that there are data showing that the responses are more frequent and the possibilities of conservative treatment are higher, although it is not clear that this will lead to an increase in survival[26-29].
It is also unclear how long treatment should last, but in the absence of progression, most studies suggest between 3-4 mo, and it would seem to be reasonable to continue until month 6 or more if there is a response be-fore surgery, to later complete 5 years of adjuvant treat-ment.
Primary chemotherapyAs we have already seen, neoadjuvant chemotherapy achieves the same overall and disease free survival as the same schemes administered adjuvantly, with an increase in the possibilities of conservative breast surgery. How-ever, there are data pointing towards an increased possi-bility of local relapse, although they are not conclusive.
The treatment of choice is based on the principle that the chemotherapy that is efficient in adjuvant treatment has a similar efficacy in neoadjuvant treatment, and there-fore there is no reason to use different schemes.
In locally advanced non-surgical tumours and those surgical ones in which an increase in conservative sur-gery is sought after, obtaining a maximal response is a reasonable objective, and this is achieved by combining anthracyclins and taxanes[30-34], whether simultaneously or sequentially (Table 1).
It is generally recommended to administer all the planned chemotherapy before the surgical procedure, if there is no evidence of progression, to maximse clinical response or complete pathological response.
In those patients contraindicated for the use of an-thracyclins the exclusive use of taxanes or the combina-tion with capecitabine or vinorelbine could be a valid option.
It is not clear whether the schemes with increased dose density (the same dose of chemotherapy in shorter periods of time) could improve the data of the conven-tional schemes. Along these lines, the GerparDuo study randomized 913 patients with T1-3N0-2 breast cancer in 4 cycles of chemotherapy with adriamycin and docetaxel every 14 d and compared them with 4 cycles of AC every 21 d followed by 4 cycles of docetaxel every 21 d. The data were favourable for sequential treatment (in other words, with a lower dose density) with greater patho-logical responses and a higher level of conservative sur-gery[35].
There are data supporting the use of dose-dense treatments especially in patients with negative hormone receptors, given that in a published meta-analysis, these treatments, used adjuvantly or neoadjuvantly, could be associated with better overall and disease free survival
26 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

27 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
rates[36]. However, it would be necessary to gather data from well-designed phase Ⅲ studies to consider dose-dense treatments as a standard treatment.
Positive Her-2/neu tumorsThe addition of trastuzumab to patients with an overex-pression of Her-2/neu has demonstrated a survival ben-efit both in the context of adjuvant therapy as well as in advanced disease.
In the same way, the use of trastuzumab is recom-mended in the neoadjuvant treatment of Her-2/neu positive patients given that it increases the possibility of complete responses. There are phase Ⅲ studies comparing the addition of trastuzumab to neoadjuvant chemotherapy (NOAH[37], GeparQuattro[38]). In both cases the addition of trastuzumab significantly increases the chances of a complete pathological response (43% and 31.7% com-pared to 23% and 15.7% respectively), without any chang-es in the survival rate or percentage of patients treated with conservative surgery.
A meta-analysis has been carried out comparing the addition of trastuzumab to schemes without it, including 5 studies with 515 patients and the conclusion is similar to the previous one: a significant increase in the chances of achieving a complete pathological response without
adding toxicity or changing the likelihood of carrying out conservative treatment[39].
Lapatinib, a biological drug with anti thyrosin-kinase activity, achieves results that are similar to those of trastu-zumab when it is used in an isolated way and associated with chemotherapy, according to the results reported in ASCO in 2012. Both drugs achieve similar complete re-sponse rates, regardless of the status of the hormone re-ceptors. However, the addition of them does not increase the percentage of pathological responses[40].
The results of the Neo-ALTTO study, however, contradict the previous results, showing that the addition of trastuzumab and lapatinib to neoadjuvant paclitaxel significantly increases the percentage of complete patho-logical response (51.3% in combined treatment compared with 29.5% and 24.9% with trastuzumab and lapatinib as single treatments, respectively)[41], although with greater toxicity.
The addition of pertuzumab, another anti-Her2/neu antibody, to trastuzumab and docetaxel as a neoadjuvant treatment significantly increases the chances of patholog-ical responses by nearly 45.8% (according to the results of a randomized phase Ⅱ study), compared to trastu-zumab and docetaxel on their own[42].
The use of any of these drugs is still not recommend-
Table 1 Chemotherapy schemes used in neoadjuvant treatment, with category-1 evidence and that can be used in neoadjuvant treatment
Ref. Chemotherapy scheme Drugs/dose
Martin et al[70] CAT Docetaxel 75 mg/m2 iv on day 1Doxorubicin 50 mg/m2 iv on day 1Cyclophosphamide 500 mg/m2 iv on day 1Cycled every 21 d for 6 cycles (all cycles are with filgrastim support)
Citron et al[71] Non-trastuzumab containing regimens
Dose-dense AC followed by paclitaxel every 2 wk
Doxorubicin 60 mg/m2 iv on day 1Cyclophosphamide 600 mg/m2 iv on day 1Cycled every 14 d for 4 cyclesFollowed by paclitaxel 175 mg/m2 as a 3 h iv infusion on day 1Cycled every 14 d for 4 cycles (all cycles are with filgrastim support)
Henderson et al[72]
AC followed by weekly paclitaxel
Doxorubicin 60 mg/m2 on day 1Cyclophosphamide 600 mg/m2 iv on day 1Cycled every 21 d for 4 cyclesFollowed by paclitaxel 80 mg/m2 as a 1 h iv infusion weekly from day 1 for 12 wk
Jones et al[73] CT Docetaxel 75 mg/m2 on day 1Cyclophosphamide 600 mg/m2 iv on day 1Cycled every 21 d for 4 cycles(all cycles are with filgrastim support)
Romond et al[74]
Trastuzumab containing regimens
AC followed by weekly paclitaxel concurrent with trastuzumab
Doxorubicin 60 mg/m2 iv on day 1Cyclophosphamide 600 mg/m2 iv on day 1Cycled every 21 d for 4 cyclesFollowed by Paclitaxel 80 mg/m2 as a 1 h iv weekly for 12 wkWith Trastuzumab 4 mg/kg iv with first dose of paclitaxelFollowed by Trastuzumab 2 mg/kg iv weekly to complete 1 yr of treatmentCardiac monitoring at baseline, 3, 6, and 9 mo
Robert et al[75] TCH Docetaxel 75 mg/m2 iv day 1Carboplatin AUC 6 iv on day 1Cycled every 21 d for 6 cyclesWith Trastuzumab 4 mg/kg in week 1Followed by Trastuzumab 2 mg/kg for 17 wkFollowed by Trastuzumab 6 mg/kg iv every 3 wk to complete 1 yr of trastuzumab therapyCardiac monitoring at baseline, at 3, 6, and 9 mo
CAT: Docetaxel, doxorubicin and cyclophosfamide; AC: Doxorubicin plus cyclophosfamide; CT: Docetaxel plus cyclophosfamide; TCH: Docetaxel, cyclophosfamide plus trastuzumab.
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

28 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
ed (lapatinib or pertuzumab) as a standard treatment with neoadjuvant intent.
Triple negative tumoursAlthough many studies suggest that the percentage of complete pathological response is greater in triple nega-tive patients than in the rest, it remains unclear whether this produces some kind of benefit in these patients. In fact, in spite of the increase in complete response these patients still have a poor prognosis with lower expecta-tions in terms of survival.
There are no specific defined treatment schemes for these patients although there are data suggesting promis-ing results using derivates from platinum[43] PARP inhibi-tors (especially in patients with the BRCAs mutation) and antiEGFR1 drugs.
The current recommendations are to use the same treatments that are used for the rest of the patients, al-though this is undoubtedly a fertile area for specific clinical trials which are likely to change the treatment used in the near future.
Other biological treatmentsThe addition of bevacizumab (an anti VEGF antibody, with mainly antiangiogenic activity) to chemotherapy in negative Her-2/neu patients has revealed contradictory results. In the GeparQuinto[44] study, with 1948 patients, bevacizumab was able to increase the percentage of com-plete pathological responses in triple negative patients but not in patients with an overexpression of hormone recep-tors. However, the NSABP B-40 study[45] on 1206 patients achieved the opposite effect, producing an increase in pathological responses in patients with an overexpression of hormone receptors but not in triple negative patients.
Therefore, until more substantial results are obtained, its use is not recommended in this context.
TailoringIn spite of the advantage of neoadjuvant treatment for checking the in vivo sensitivity of certain drugs (so that a change in the chemotherapy scheme could provide advantages in the case of progressive disease or limited response), this benefit has not been demonstrated in the only phase Ⅲ study carried out with this objective.
In the GeparTrio[46] study on 2070 patients treated using the CAT scheme (cyclophosphamide, doxorubicin and docetaxel), those who do not achieve a response of at least a 50% reduction in tumour size are randomized to continue with CAT or to receive treatment with vinorel-bine and capecitabine, and do not achieve any differences in response according to ultrasound tests, complete path-ological responses or percentage breast conservation.
Another one of the issues to be taken into account within systemic treatment tailoring is to know if it makes sense to prolong this treatment once surgery has been per-formed and a partial response has been achieved, whether this is a result of the initial treatment or of an alternative type of treatment.
It might be thought that systemic treatment is not the most appropriate strategy and further treatment or an-other kind of treatment could increase efficacy, or alter-natively, that the limited response or the lack of response to the systemic treatment is a reflection of the fact that we are facing a tumour with a worse prognosis which is therefore less chemosensitive.
Until now, no study has demonstrated that the admin-istration of any kind of systemic treatment after standard preoperative treatment improves the prognosis of these patients.
Outside of a clinical trial no recommendation has been made for additional systemic treatment following surgery, after standard preoperative treatment.
Assessment of treatment responseThe assessment of treatment response involves the as-sessment of clinical response as much as pathological response after surgery. Both prognostic factors are related to survival.
It is vital to carry out an exhaustive clinical follow up during systemic treatment because although a change in systemic chemotherapy in the absence of treatment response has not proven to be useful[36], clinical disease progression or the absence of response is enough to postpone systemic treatment and to consider immediate adequate locoregional treatment.
The clinical and radiological response should be made according to the RECIST criteria[47,48], so that a bidimen-sional assessment of the lesions can be made. Complete clinical response can be defined as the disappearance of the tumour in both the breast and the axillary lymph node through physical examination and radiological tests.
The traditional methods for examining the breast (physical examination, mammogram and ultrasound) have a limited ability to assess response and are not very closely correlated with pathological response[49].
However, dynamic MRI has been better correlated with pathological response in many studies and in one meta-analysis[50]. In spite of its increased sensitivity com-pared to other techniques it has more false positives and overestimates the occurrence of residual disease after systemic treatment[51].
By carrying out early dynamic MRI after initiating che-motherapy it is possible to distinguish respondent patients (in whom there is an early-onset decrease in contrast enhancement compared to levels in previous tests), from non-respondents, in whom this enhancement is main-tained or increased[52].
MRI can also underestimate the result of chemo-therapy revealing residual disease or disease which is very unresponsive to treatment, and this seems to be espe-cially related to the use of taxanes in the chemotherapy regimes’[53].
Although MRI can provide underestimations or over-estimations of response to chemotherapy, currently it is undoubtedly the radiological method of choice for as-sessing neoadjuvant treatment response.
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

29 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
In those patients studied given MRI after systemic treatment, the possibility of overestimating the disease should be assessed before planning surgical treatment given that conservative surgery would become less likely in patients who could potentially receive this kind of sur-gery[54].
Pathological responseAlthough complete clinical response (disappearance of the tumour in the physical examination and radiological tests) and complete pathological response (the absence of a viable invasive tumour, depending on the accepted definition in the surgical sample) have been related with disease prognosis, there is no clear correlation between them, and approximately a third or more of the patients with complete clinical response have a viable tumour in the surgical sample[55].
In most of the initially reported studies, a significant reduction in tumour size was achieved making conserva-tive treatment more likely, but this had no correlation with disease-free or overall survival.
Achieving complete pathological response is a very important surrogate marker for determining the efficacy of preoperative treatment and it has been correlated in several studies and a recent meta-analysis[56] with better re-sults in disease survival and it is considered as a marker of systemic disease chemosensitivity.
The definition of complete pathological response var-ies among the reported studies. In some studies complete response has been considered as the absence of tumour cells in the primary tumour area and in the axillary node areas, whereas in other studies where it has been argued that the existence of a ductal tumour does not affect dis-ease-free or overall survival[57], it is defined as the persis-tence of a non-invasive tumour. Some studies go further separating complete response in the primary tumour and in the axillary lymph node.
Although there is disagreement over complete re-sponse in the literature, it is currently thought that obtain-ing complete pathological response is a predictive factor, independent of disease-free and overall survival in the multivariate analysis[7].
Furthermore, the persistence of residual disease in the lymph nodes is a factor of worse prognosis than disease persistence in the primary tumour[58].
The likelihood of achieving complete response varies according to tumour biology, so that tumours with Her-2/neu overexpression and negative receptors can achieve up to a 45% chance of complete response (defined as an absence of tumour invasion) compared to those that have hormone overexpression but no Her-2/neu receptors in whom only 9% attain a complete response[59] (without trastuzumab).
In addition, complete pathological response capacity or long term survival prognosis also appears to depend on the tumour subtype, so that, complete response is the best predictor of disease-free survival especially in pa-tients with positive hormone receptors[46].
Predictive response factorsSeveral predictive response factors related to achieving complete response have been reported, and therefore they are related to chemosensitivity, but they are currently still not recommended for selecting individualised systemic treatment.
We know that tumours that do not express hormone receptors or only express a few of them such as luminal B subtype and tumours with a high percentage of Ki67 expression according to immunohistochemistry, are as-sociated with greater chances of complete pathological response to chemotherapy, while those tumours that overexpress hormone receptors or lobular histologies are less likely to achieve complete pathological response with chemotherapy[60,61].
Alternatively, Her-2/neu overexpression is a clear predictive factor of response to trastuzumab, although we also know that it increases the chances of response to inhibitors of aromatase compared to tamoxifen, when endocrine treatment is chosen[62].
The genetic profile can predict pathological results, so that it is more likely for pathological response to occur in triple negative tumours or in those who have a luminal B profile[63-65].
A recent meta-analysis concluded that complete re-sponse with chemotherapy is more likely in patients with triple negative (31.1%) and positive Her-2/neu (38.9%) tumours than in tumours that only overexpress hormone recpetors (8.3%)[66].
However, it is not just biological factors that are re-lated with tumour chemosensitivity. Dynamic analysis, spectroscopic analysis with MRI[67], and positron emission tomography[68] can predict sensitivity to treatment if they are carried out early-on once systemic treatment has been undertaken. The differences regarding the baseline stud-ies of contrast uptake or SUV (in the case of PET) are related with the chances of systemic treatment response.
PET has a high sensitivity for evaluating neoadjuvant treatment response but with a low specificity, so that it cannot be recommended as an isolated technique for tak-ing decisions[69].
FUTURE OF PRIMARY SYSTEMIC THERAPYNeoadjuvant treatment is undoubtedly a realistic option in many scenarios, but it continues to be a treatment that has potential for development, with the introduction of new treatments or new indications or even as a substitute for surgery in certain patient subgroups.
In spite of the importance of local treatment in breast cancer, over time the aggressiveness of surgery has been diminishing, making procedures more and more conserva-tive, with less aggression against the axillary lymph node, improved cosmetic results and a reduction in secondary effects. This has all been possible thanks to the increase in the anti-tumour efficacy of systemic treatments.
Much research still needs to be done and improve-
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

30 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
ments need to be made to the systemic treatment of localised breast cancer with neoadjuvant intent, but in the near future, the main improvement will be the availability of an individualised treatment, based on the patient's genetic profile and predictive biological response factors, using early response assessment methods that are prob-ably based on sufficiently sensitive image techniques and with few false positives.
An appropriate selection of systemic treatment, with local efficacy, and an adequate response assessment using imaging methods with false negatives could mean that in the future, in some patients, surgery could become un-necessary for treating localized breast cancer.
The current extensive biological knowledge about tumours is making it possible to use highly selective treat-ment options efficient for certain types of tumour (anti Her-2/neu drugs, for example). However, just as it has been shown in other tumours (melanoma, colon cancer, lung cancer…) shortly we will have very efficient systemic treatments for small groups of patients that could be eas-ily selected for this purpose.
Currently many studies are in progress on a range of agents (PARP inhibitors and other targeted agents) in the neoadjuvant context.
REFERENCES1 Hellman S. Karnofsky Memorial Lecture. Natural history of
small breast cancers. J Clin Oncol 1994; 12: 2229-2234 [PMID: 7931493]
2 Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365: 1687-1717 [PMID: 15894097 DOI: 10.1016/S0140-6736(05)66544-0]
3 Fisher B, Brown A, Mamounas E, Wieand S, Robidoux A, Margolese RG, Cruz AB, Fisher ER, Wickerham DL, Wol-mark N, DeCillis A, Hoehn JL, Lees AW, Dimitrov NV. Effect of preoperative chemotherapy on local-regional dis-ease in women with operable breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-18. J Clin Oncol 1997; 15: 2483-2493 [PMID: 9215816]
4 De Lena M, Zucali R, Viganotti G, Valagussa P, Bonadonna G. Combined chemotherapy-radiotherapy approach in lo-cally advanced (T3b-T4) breast cancer. Cancer Chemother Pharmacol 1978; 1: 53-59 [PMID: 373908]
5 Jacquillat C, Weil M, Baillet F, Borel C, Auclerc G, de Maublanc MA, Housset M, Forget G, Thill L, Soubrane C. Results of neoadjuvant chemotherapy and radiation therapy in the breast-conserving treatment of 250 patients with all stages of infiltrative breast cancer. Cancer 1990; 66: 119-129 [PMID: 2112976 DOI: 10.1002/1097-0142(19900701)66:1<119::AID-CNCR2820660122>3.0.CO;2-3]
6 Smith IE, Jones AL, O’Brien ME, McKinna JA, Sacks N, Baum M. Primary medical (neo-adjuvant) chemotherapy for operable breast cancer. Eur J Cancer 1993; 29A: 1796-1799 [PMID: 8398318]
7 Bonadonna G, Valagussa P, Brambilla C, Ferrari L, Moliterni A, Terenziani M, Zambetti M. Primary chemotherapy in op-erable breast cancer: eight-year experience at the Milan Can-cer Institute. J Clin Oncol 1998; 16: 93-100 [PMID: 9440728]
8 Fisher ER, Wang J, Bryant J, Fisher B, Mamounas E, Wol-mark N. Pathobiology of preoperative chemotherapy: find-ings from the National Surgical Adjuvant Breast and Bowel (NSABP) protocol B-18. Cancer 2002; 95: 681-695 [PMID:
12209710]9 van der Hage JA, van de Velde CJ, Julien JP, Tubiana-Hulin
M, Vandervelden C, Duchateau L. Preoperative chemother-apy in primary operable breast cancer: results from the Eu-ropean Organization for Research and Treatment of Cancer trial 10902. J Clin Oncol 2001; 19: 4224-4237 [PMID: 11709566]
10 Mauri D, Pavlidis N, Ioannidis JP. Neoadjuvant versus ad-juvant systemic treatment in breast cancer: a meta-analysis. J Natl Cancer Inst 2005; 97: 188-194 [PMID: 15687361 DOI: 10.1093/jnci/dji021]
11 Kuerer HM, Newman LA, Smith TL, Ames FC, Hunt KK, Dhingra K, Theriault RL, Singh G, Binkley SM, Sneige N, Bu-chholz TA, Ross MI, McNeese MD, Buzdar AU, Hortobagyi GN, Singletary SE. Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemo-therapy. J Clin Oncol 1999; 17: 460-469 [PMID: 10080586]
12 Feldman LD, Hortobagyi GN, Buzdar AU, Ames FC, Blu-menschein GR. Pathological assessment of response to in-duction chemotherapy in breast cancer. Cancer Res 1986; 46: 2578-2581 [PMID: 3697997]
13 Caudle AS, Gonzalez-Angulo AM, Hunt KK, Pusztai L, Kue-rer HM, Mittendorf EA, Hortobagyi GN, Meric-Bernstam F. Impact of progression during neoadjuvant chemotherapy on surgical management of breast cancer. Ann Surg Oncol 2011; 18: 932-938 [PMID: 21061075]
14 Osako T, Horii R, Matsuura M, Ogiya A, Domoto K, Miyagi Y, Takahashi S, Ito Y, Iwase T, Akiyama F. Common and discriminative clinicopathological features between breast cancers with pathological complete response or progressive disease in response to neoadjuvant chemotherapy. J Cancer Res Clin Oncol 2010; 136: 233-241 [PMID: 19685074 DOI: 10.1007/s00432-009-0654-9]
15 Kaufmann M, Hortobagyi GN, Goldhirsch A, Scholl S, Makris A, Valagussa P, Blohmer JU, Eiermann W, Jackesz R, Jonat W, Lebeau A, Loibl S, Miller W, Seeber S, Semiglazov V, Smith R, Souchon R, Stearns V, Untch M, von Minckwitz G. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of oper-able breast cancer: an update. J Clin Oncol 2006; 24: 1940-1949 [PMID: 16622270]
16 Schwartz GF, Hortobagyi GN. Proceedings of the consensus conference on neoadjuvant chemotherapy in carcinoma of the breast, April 26-28, 2003, Philadelphia, Pennsylvania. Cancer 2004; 100: 2512-2532 [PMID: 15197792 DOI: 10.1002/cncr.20298]
17 LaTrenta LR, Menell JH, Morris EA, Abramson AF, Dershaw DD, Liberman L. Breast lesions detected with MR imag-ing: utility and histopathologic importance of identification with US. Radiology 2003; 227: 856-861 [PMID: 12773685 DOI: 10.1148/radiol.2273012210]
18 Perlet C, Heywang-Kobrunner SH, Heinig A, Sittek H, Cas-selman J, Anderson I, Taourel P. Magnetic resonance-guid-ed, vacuum-assisted breast biopsy: results from a European multicenter study of 538 lesions. Cancer 2006; 106: 982-990 [PMID: 16456807]
19 Alonso-Bartolome P, Ortega Garcia E, Garijo Ayensa F, de Juan Ferre A, Vega Bolivar A. Utility of the tumor bed marker in patients with breast cancer receiving induction chemotherapy. Acta Radiol 2002; 43: 29-33 [PMID: 11972458]
20 Piñiero A, Giménez J, Vidal-Sicart S, Intra M. Selective sen-tinel lymph node biopsy and primary systemic therapy in breast cancer. Tumori 2010; 96: 17-23 [PMID: 20437852]
21 van Deurzen CH, Vriens BE, Tjan-Heijnen VC, van der Wall E, Albregts M, van Hilligersberg R, Monninkhof EM, van Diest PJ. Accuracy of sentinel node biopsy after neoadjuvant chemotherapy in breast cancer patients: a systematic re-view. Eur J Cancer 2009; 45: 3124-3130 [PMID: 19716287 DOI: 10.1016/j.ejca.2009.08.001]
22 Papa MZ, Zippel D, Kaufman B, Shimon-Paluch S, Yosepo-
Alonso-Romero JL et al . Primary systemic treatment in breast cancer
31 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
vich A, Oberman B, Sadetzki S. Timing of sentinel lymph node biopsy in patients receiving neoadjuvant chemother-apy for breast cancer. J Surg Oncol 2008; 98: 403-406 [PMID: 18683193 DOI: 10.1002/jso.21128]
23 Syed BM, Johnston SJ, Wong DWM, Morgan DAL, Ellis IO, Cheung KL. Surgery versus primary endocrine therapy for elderly women with estrogen receptor-positive early oper-able primary breast cancer: Survival analysis and correlation with oestrogen receptor positivity. J Clin Oncol 2009; 27: Abstr 612
24 Semiglazov VF, Semiglazov VV, Dashyan GA, Ziltsova EK, Ivanov VG, Bozhok AA, Melnikova OA, Paltuev RM, Kletzel A, Berstein LM. Phase 2 randomized trial of primary endocrine therapy versus chemotherapy in postmenopausal patients with estrogen receptor-positive breast cancer. Cancer 2007; 110: 244-254 [PMID: 17538978]
25 Alba E, Calvo L, Albanell J, De la Haba JR, Arcusa Lanza A, Chacon JI, Sanchez-Rovira P, Plazaola A, Lopez Garcia-Asenjo JA, Bermejo B, Carrasco E, Lluch A. Chemotherapy (CT) and hormonotherapy (HT) as neoadjuvant treat-ment in luminal breast cancer patients: results from the GEICAM/2006-03, a multicenter, randomized, phase-II study. Ann Oncol 2012; 23: 3069-3074 [PMID: 22674146 DOI: 10.1093/annonc/mds132]
26 Mouridsen H, Gershanovich M, Sun Y, Perez-Carrion R, Boni C, Monnier A, Apffelstaedt J, Smith R, Sleeboom HP, Jaenicke F, Pluzanska A, Dank M, Becquart D, Bapsy PP, Salminen E, Snyder R, Chaudri-Ross H, Lang R, Wyld P, Bhatnagar A. Phase III study of letrozole versus tamoxifen as first-line therapy of advanced breast cancer in postmeno-pausal women: analysis of survival and update of efficacy from the International Letrozole Breast Cancer Group. J Clin Oncol 2003; 21: 2101-2109 [PMID: 12775735 DOI: 10.1200/JCO.2003.04.194]
27 Smith IE, Dowsett M, Ebbs SR, Dixon JM, Skene A, Blohmer JU, Ashley SE, Francis S, Boeddinghaus I, Walsh G. Neo-adjuvant treatment of postmenopausal breast cancer with anastrozole, tamoxifen, or both in combination: the Immedi-ate Preoperative Anastrozole, Tamoxifen, or Combined with Tamoxifen (IMPACT) multicenter double-blind randomized trial. J Clin Oncol 2005; 23: 5108-5116 [PMID: 15998903]
28 Cataliotti L, Buzdar AU, Noguchi S, Bines J, Takatsuka Y, Petrakova K, Dube P, de Oliveira CT. Comparison of anas-trozole versus tamoxifen as preoperative therapy in post-menopausal women with hormone receptor-positive breast cancer: the Pre-Operative “Arimidex” Compared to Tamoxi-fen (PROACT) trial. Cancer 2006; 106: 2095-2103 [PMID: 16598749]
29 Ellis MJ, Suman VJ, Hoog J, Lin L, Snider J, Prat A, Parker JS, Luo J, DeSchryver K, Allred DC, Esserman LJ, Unzeitig GW, Margenthaler J, Babiera GV, Marcom PK, Guenther JM, Watson MA, Leitch M, Hunt K, Olson JA. Randomized phase II neoadjuvant comparison between letrozole, anas-trozole, and exemestane for postmenopausal women with estrogen receptor-rich stage 2 to 3 breast cancer: clinical and biomarker outcomes and predictive value of the baseline PAM50-based intrinsic subtype--ACOSOG Z1031. J Clin On-col 2011; 29: 2342-2349 [PMID: 21555689]
30 Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A, Margolese RG, Hoehn JL, Vogel VG, Dakhil SR, Tamkus D, King KM, Pajon ER, Wright MJ, Robert J, Paik S, Mamounas EP, Wolmark N. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol 2008; 26: 778-785 [PMID: 18258986 DOI: 10.1200/JCO.2007.15.0235]
31 Evans TR, Yellowlees A, Foster E, Earl H, Cameron DA, Hutcheon AW, Coleman RE, Perren T, Gallagher CJ, Quigley M, Crown J, Jones AL, Highley M, Leonard RC, Mansi JL. Phase III randomized trial of doxorubicin and docetaxel ver-sus doxorubicin and cyclophosphamide as primary medical
therapy in women with breast cancer: an anglo-celtic cooper-ative oncology group study. J Clin Oncol 2005; 23: 2988-2995 [PMID: 15860854]
32 Bear HD, Anderson S, Smith RE, Geyer CE, Mamounas EP, Fisher B, Brown AM, Robidoux A, Margolese R, Kahlenberg MS, Paik S, Soran A, Wickerham DL, Wolmark N. Sequential preoperative or postoperative docetaxel added to preop-erative doxorubicin plus cyclophosphamide for operable breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol 2006; 24: 2019-2027 [PMID: 16606972]
33 von Minckwitz G, Kümmel S, Vogel P, Hanusch C, Eidt-mann H, Hilfrich J, Gerber B, Huober J, Costa SD, Jackisch C, Loibl S, Mehta K, Kaufmann M. Neoadjuvant vinorelbine-capecitabine versus docetaxel-doxorubicin-cyclophospha-mide in early nonresponsive breast cancer: phase III ran-domized GeparTrio trial. J Natl Cancer Inst 2008; 100: 542-551 [PMID: 18398097]
34 Cuppone F, Bria E, Carlini P, Milella M, Felici A, Sperduti I, Nisticò C, Terzoli E, Cognetti F, Giannarelli D. Taxanes as primary chemotherapy for early breast cancer: meta-analysis of randomized trials. Cancer 2008; 113: 238-246 [PMID: 18470908]
35 von Minckwitz G, Raab G, Caputo A, Schütte M, Hilfrich J, Blohmer JU, Gerber B, Costa SD, Merkle E, Eidtmann H, Lampe D, Jackisch C, du Bois A, Kaufmann M. Doxorubicin with cyclophosphamide followed by docetaxel every 21 days compared with doxorubicin and docetaxel every 14 days as preoperative treatment in operable breast cancer: the GEPARDUO study of the German Breast Group. J Clin Oncol 2005; 23: 2676-2685 [PMID: 15837982]
36 Bonilla L, Ben-Aharon I, Vidal L, Gafter-Gvili A, Leibovici L, Stemmer SM. Dose-dense chemotherapy in nonmeta-static breast cancer: a systematic review and meta-analysis of randomized controlled trials. J Natl Cancer Inst 2010; 102: 1845-1854 [PMID: 21098761]
37 Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, Tjulandin S, Zambetti M, Vazquez F, Byakhow M, Lichinits-er M, Climent MA, Ciruelos E, Ojeda B, Mansutti M, Bozhok A, Baronio R, Feyereislova A, Barton C, Valagussa P, Baselga J. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet 2010; 375: 377-384 [PMID: 20113825]
38 Untch M, Rezai M, Loibl S, Fasching PA, Huober J, Tesch H, Bauerfeind I, Hilfrich J, Eidtmann H, Gerber B, Hanusch C, Kühn T, du Bois A, Blohmer JU, Thomssen C, Dan Costa S, Jackisch C, Kaufmann M, Mehta K, von Minckwitz G. Neoadjuvant treatment with trastuzumab in HER2-positive breast cancer: results from the GeparQuattro study. J Clin Oncol 2010; 28: 2024-2031 [PMID: 20308670]
39 Valachis A, Mauri D, Polyzos NP, Chlouverakis G, Mav-roudis D, Georgoulias V. Trastuzumab combined to neoad-juvant chemotherapy in patients with HER2-positive breast cancer: a systematic review and meta-analysis. Breast 2011; 20: 485-490 [PMID: 21784637]
40 Robidoux A, Tang G, Rastogi P, Geyer CE, Azar CA, Atkins JN, Fehrenbacher L, Bear HD, Baez-Diaz L, Kuebler JP, Mar-golese RG, Farrar WB, Brufsky A, Shibata HR, Bandos H, Paik S, Costantino JP, Swain SM, Mamounas EP, Wolmark N. Evaluation of lapatinib as a component of neoadjuvant therapy for HER2+ operable breast cancer: NSABP protocol B-41. J Clin Oncol 2012; 30: Abstr LBA506
41 Baselga J, Bradbury I, Eidtmann H, Di Cosimo S, de Azam-buja E, Aura C, Gómez H, Dinh P, Fauria K, Van Dooren V, Aktan G, Goldhirsch A, Chang TW, Horváth Z, Coccia-Por-tugal M, Domont J, Tseng LM, Kunz G, Sohn JH, Semiglazov V, Lerzo G, Palacova M, Probachai V, Pusztai L, Untch M,
Alonso-Romero JL et al . Primary systemic treatment in breast cancer
32 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Gelber RD, Piccart-Gebhart M. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a ran-domised, open-label, multicentre, phase 3 trial. Lancet 2012; 379: 633-640 [PMID: 22257673]
42 Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, Lluch A, Staroslawska E, de la Haba-Rodriguez J, Im SA, Pedrini JL, Poirier B, Morandi P, Semiglazov V, Sri-muninnimit V, Bianchi G, Szado T, Ratnayake J, Ross G, Valagussa P. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflam-matory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol 2012; 13: 25-32 [PMID: 22153890]
43 Chang HR, Glaspy J, Allison MA, Kass FC, Elashoff R, Chung DU, Gornbein J. Differential response of triple-negative breast cancer to a docetaxel and carboplatin-based neoadjuvant treatment. Cancer 2010; 116: 4227-4237 [PMID: 20549829]
44 von Minckwitz G, Eidtmann H, Rezai M, Fasching PA, Tesch H, Eggemann H, Schrader I, Kittel K, Hanusch C, Kreienberg R, Solbach C, Gerber B, Jackisch C, Kunz G, Blohmer JU, Huober J, Hauschild M, Fehm T, Müller BM, Denkert C, Loibl S, Nekljudova V, Untch M. Neoadjuvant chemotherapy and bevacizumab for HER2-negative breast cancer. N Engl J Med 2012; 366: 299-309 [PMID: 22276820]
45 Bear HD, Tang G, Rastogi P, Geyer CE, Robidoux A, Atkins JN, Baez-Diaz L, Brufsky AM, Mehta RS, Fehrenbacher L, Young JA, Senecal FM, Gaur R, Margolese RG, Adams PT, Gross HM, Costantino JP, Swain SM, Mamounas EP, Wol-mark N. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. N Engl J Med 2012; 366: 310-320 [PMID: 22276821]
46 von Minckwitz G, Kümmel S, Vogel P, Hanusch C, Eidt-mann H, Hilfrich J, Gerber B, Huober J, Costa SD, Jackisch C, Loibl S, Mehta K, Kaufmann M. Intensified neoadjuvant chemotherapy in early-responding breast cancer: phase III randomized GeparTrio study. J Natl Cancer Inst 2008; 100: 552-562 [PMID: 18398094]
47 Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sar-gent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: 228-247 [PMID: 19097774]
48 Husband JE, Schwartz LH, Spencer J, Ollivier L, King DM, Johnson R, Reznek R. Evaluation of the response to treatment of solid tumours - a consensus statement of the International Cancer Imaging Society. Br J Cancer 2004; 90: 2256-2260 [PMID: 15150551]
49 Chagpar AB, Middleton LP, Sahin AA, Dempsey P, Buzdar AU, Mirza AN, Ames FC, Babiera GV, Feig BW, Hunt KK, Kuerer HM, Meric-Bernstam F, Ross MI, Singletary SE. Ac-curacy of physical examination, ultrasonography, and mam-mography in predicting residual pathologic tumor size in patients treated with neoadjuvant chemotherapy. Ann Surg 2006; 243: 257-264 [PMID: 16432360]
50 Yuan Y, Chen XS, Liu SY, Shen KW. Accuracy of MRI in prediction of pathologic complete remission in breast cancer after preoperative therapy: a meta-analysis. AJR Am J Roent-genol 2010; 195: 260-268 [PMID: 20566826]
51 Kwong MS, Chung GG, Horvath LJ, Ward BA, Hsu AD, Carter D, Tavassoli F, Haffty B, Burtness BA. Postchemo-therapy MRI overestimates residual disease compared with histopathology in responders to neoadjuvant therapy for locally advanced breast cancer. Cancer J 2006; 12: 212-221 [PMID: 16803680]
52 Fangberget A, Nilsen LB, Hole KH, Holmen MM, Enge-braaten O, Naume B, Smith HJ, Olsen DR, Seierstad T. Neoadjuvant chemotherapy in breast cancer-response evalu-ation and prediction of response to treatment using dynamic
contrast-enhanced and diffusion-weighted MR imaging. Eur Radiol 2011; 21: 1188-1199 [PMID: 21127880]
53 Denis F, Desbiez-Bourcier AV, Chapiron C, Arbion F, Body G, Brunereau L. Contrast enhanced magnetic resonance imaging underestimates residual disease following neoadju-vant docetaxel based chemotherapy for breast cancer. Eur J Surg Oncol 2004; 30: 1069-1076 [PMID: 15522553]
54 Chen JH, Feig BA, Hsiang DJ, Butler JA, Mehta RS, Bahri S, Nalcioglu O, Su MY. Impact of MRI-evaluated neoadjuvant chemotherapy response on change of surgical recommenda-tion in breast cancer. Ann Surg 2009; 249: 448-454 [PMID: 19247033]
55 Hortobagyi GN, Ames FC, Buzdar AU, Kau SW, McNeese MD, Paulus D, Hug V, Holmes FA, Romsdahl MM, Fraschini G. Management of stage III primary breast cancer with pri-mary chemotherapy, surgery, and radiation therapy. Cancer 1988; 62: 2507-2516 [PMID: 3056604]
56 Kong X, Moran MS, Zhang N, Haffty B, Yang Q. Meta-anal-ysis confirms achieving pathological complete response after neoadjuvant chemotherapy predicts favourable prognosis for breast cancer patients. Eur J Cancer 2011; 47: 2084-2090 [PMID: 21737257 DOI: 10.1016/j.ejca.2011.06.014]
57 Mazouni C, Peintinger F, Wan-Kau S, Andre F, Gonzalez-Angulo AM, Symmans WF, Meric-Bernstam F, Valero V, Hortobagyi GN, Pusztai L. Residual ductal carcinoma in situ in patients with complete eradication of invasive breast can-cer after neoadjuvant chemotherapy does not adversely af-fect patient outcome. J Clin Oncol 2007; 25: 2650-2655 [PMID: 17602071]
58 Hennessy BT, Hortobagyi GN, Rouzier R, Kuerer H, Sneige N, Buzdar AU, Kau SW, Fornage B, Sahin A, Broglio K, Singletary SE, Valero V. Outcome after pathologic complete eradication of cytologically proven breast cancer axillary node metastases following primary chemotherapy. J Clin Oncol 2005; 23: 9304-9311 [PMID: 16361629]
59 Esserman LJ, Berry DA, DeMichele A, Carey L, Davis SE, Buxton M, Hudis C, Gray JW, Perou C, Yau C, Livasy C, Krontiras H, Montgomery L, Tripathy D, Lehman C, Liu MC, Olopade OI, Rugo HS, Carpenter JT, Dressler L, Chhieng D, Singh B, Mies C, Rabban J, Chen YY, Giri D, van ‘t Veer L, Hylton N. Pathologic complete response predicts recurrence-free survival more effectively by cancer subset: results from the I-SPY 1 TRIAL--CALGB 150007/150012, ACRIN 6657. J Clin Oncol 2012; 30: 3242-3249 [PMID: 22649152 DOI: 10.1200/JCO.2011.39.2779]
60 Bhargava R, Beriwal S, Dabbs DJ, Ozbek U, Soran A, John-son RR, Brufsky AM, Lembersky BC, Ahrendt GM. Immuno-histochemical surrogate markers of breast cancer molecular classes predicts response to neoadjuvant chemotherapy: a single institutional experience with 359 cases. Cancer 2010; 116: 1431-1439 [PMID: 20131351 DOI: 10.1002/cncr.24876]
61 Kaufmann M, von Minckwitz G, Bear HD, Buzdar A, Mc-Gale P, Bonnefoi H, Colleoni M, Denkert C, Eiermann W, Jackesz R, Makris A, Miller W, Pierga JY, Semiglazov V, Sch-neeweiss A, Souchon R, Stearns V, Untch M, Loibl S. Recom-mendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann Oncol 2007; 18: 1927-1934 [PMID: 17998286]
62 Ellis MJ, Coop A, Singh B, Mauriac L, Llombert-Cussac A, Jänicke F, Miller WR, Evans DB, Dugan M, Brady C, Quebe-Fehling E, Borgs M. Letrozole is more effective neoadjuvant endocrine therapy than tamoxifen for ErbB-1- and/or ErbB-2-positive, estrogen receptor-positive primary breast cancer: evidence from a phase III randomized trial. J Clin Oncol 2001; 19: 3808-3816 [PMID: 11559718]
63 Rouzier R, Perou CM, Symmans WF, Ibrahim N, Cristofanil-li M, Anderson K, Hess KR, Stec J, Ayers M, Wagner P, Mo-randi P, Fan C, Rabiul I, Ross JS, Hortobagyi GN, Pusztai L. Breast cancer molecular subtypes respond differently to pre-
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

33 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
operative chemotherapy. Clin Cancer Res 2005; 11: 5678-5685 [PMID: 16115903]
64 Hatzis C, Pusztai L, Valero V, Booser DJ, Esserman L, Lluch A, Vidaurre T, Holmes F, Souchon E, Wang H, Martin M, Cotrina J, Gomez H, Hubbard R, Chacón JI, Ferrer-Lozano J, Dyer R, Buxton M, Gong Y, Wu Y, Ibrahim N, Andreopou-lou E, Ueno NT, Hunt K, Yang W, Nazario A, DeMichele A, O’Shaughnessy J, Hortobagyi GN, Symmans WF. A genomic predictor of response and survival following taxane-anthra-cycline chemotherapy for invasive breast cancer. JAMA 2011; 305: 1873-1881 [PMID: 21558518]
65 Huober J, von Minckwitz G, Denkert C, Tesch H, Weiss E, Zahm DM, Belau A, Khandan F, Hauschild M, Thomssen C, Högel B, Darb-Esfahani S, Mehta K, Loibl S. Effect of neoad-juvant anthracycline-taxane-based chemotherapy in different biological breast cancer phenotypes: overall results from the GeparTrio study. Breast Cancer Res Treat 2010; 124: 133-140 [PMID: 20697801 DOI: 10.1007/s10549-010-1103-9]
66 Houssami N, Macaskill P, von Minckwitz G, Marinovich ML, Mamounas E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoad-juvant chemotherapy. Eur J Cancer 2012; 48: 3342-3354 [PMID: 22766518 DOI: 10.1016/j.ejca.2012.05.023]
67 Nagashima T, Sakakibara M, Nakamura R, Arai M, Kadowa-ki M, Kazama T, Nakatani Y, Koda K, Miyazaki M. Dynamic enhanced MRI predicts chemosensitivity in breast cancer patients. Eur J Radiol 2006; 60: 270-274 [PMID: 16926079]
68 Shimoda W, Hayashi M, Murakami K, Oyama T, Sunagawa M. The relationship between FDG uptake in PET scans and biological behavior in breast cancer. Breast Cancer 2007; 14: 260-268 [PMID: 17690502]
69 Cheng X, Li Y, Liu B, Xu Z, Bao L, Wang J. 18F-FDG PET/CT and PET for evaluation of pathological response to neo-adjuvant chemotherapy in breast cancer: a meta-analysis. Acta Radiol 2012; 53: 615-627 [PMID: 22734080 DOI: 10.1258/ar.2012.110603]
70 Martin M, Pienkowski T, Mackey J, Pawlicki M, Guastalla JP, Weaver C, Tomiak E, Al-Tweigeri T, Chap L, Juhos E, Guevin R, Howell A, Fornander T, Hainsworth J, Coleman R, Vinholes J, Modiano M, Pinter T, Tang SC, Colwell B, Prady C, Provencher L, Walde D, Rodriguez-Lescure A, Hugh J, Loret C, Rupin M, Blitz S, Jacobs P, Murawsky M, Riva A, Vogel C. Adjuvant docetaxel for node-positive breast cancer.
N Engl J Med 2005; 352: 2302-2313 [PMID: 15930421]71 Citron ML, Berry DA, Cirrincione C, Hudis C, Winer EP,
Gradishar WJ, Davidson NE, Martino S, Livingston R, Ingle JN, Perez EA, Carpenter J, Hurd D, Holland JF, Smith BL, Sartor CI, Leung EH, Abrams J, Schilsky RL, Muss HB, Nor-ton L. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol 2003; 21: 1431-1439 [PMID: 12668651]
72 Henderson IC, Berry DA, Demetri GD, Cirrincione CT, Goldstein LJ, Martino S, Ingle JN, Cooper MR, Hayes DF, Tkaczuk KH, Fleming G, Holland JF, Duggan DB, Carpenter JT, Frei E, Schilsky RL, Wood WC, Muss HB, Norton L. Im-proved outcomes from adding sequential Paclitaxel but not from escalating Doxorubicin dose in an adjuvant chemother-apy regimen for patients with node-positive primary breast cancer. J Clin Oncol 2003; 21: 976-983 [PMID: 12637460]
73 Jones S, Holmes FA, O’Shaughnessy J, Blum JL, Vukelja SJ, McIntyre KJ, Pippen JE, Bordelon JH, Kirby RL, Sand-bach J, Hyman WJ, Richards DA, Mennel RG, Boehm KA, Meyer WG, Asmar L, Mackey D, Riedel S, Muss H, Savin MA. Docetaxel With Cyclophosphamide Is Associated With an Overall Survival Benefit Compared With Doxorubicin and Cyclophosphamide: 7-Year Follow-Up of US Oncology Research Trial 9735. J Clin Oncol 2009; 27: 1177-1183 [PMID: 19204201 DOI: 10.1200/JCO.2008.18.4028]
74 Romond EH, Perez EA, Bryant J, Suman VJ, Geyer CE, Da-vidson NE, Tan-Chiu E, Martino S, Paik S, Kaufman PA, Swain SM, Pisansky TM, Fehrenbacher L, Kutteh LA, Vogel VG, Visscher DW, Yothers G, Jenkins RB, Brown AM, Dakhil SR, Mamounas EP, Lingle WL, Klein PM, Ingle JN, Wolmark N. Trastuzumab plus adjuvant chemotherapy for oper-able HER2-positive breast cancer. N Engl J Med 2005; 353: 1673-1684 [PMID: 16236738]
75 Robert NJ, Eiermann W, Pienkowski T, Crown J, Martin M, Pawlicki M, Chan A, Bee V, Slamon D, Au H. BCIRG 006: Docetaxel and trastuzumab-based regimens improve DFS and OS over AC-T in node positive and high risk node negative HER2 positive early breast cancer patients: Quality of life (QOL) at 36 months follow-up. J Clin Oncol 2007; 25: 19647
P- Reviewer Brufsky A S- Editor Gou SX L- Editor A E- Editor Zheng XM
Alonso-Romero JL et al . Primary systemic treatment in breast cancer

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i2.34
World J Obstet Gynecol 2013 May 10; 2(2): 34-36ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Prenatal incarceration of caput succedaneum: A case report
Atsuko Okazaki, Ken Miyazaki, Kana Kihira, Madoka Furuhashi
Atsuko Okazaki, Ken Miyazaki, Kana Kihira, Madoka Furu-hashi, Department of Obstetrics and Gynecology, Japanese Red Cross Nagoya Daiichi Hospital, Nagoya 453-8511, JapanAuthor contributions: All authors participated equally in the preparation of this case report by contributing their expertise; Furuhashi M designed and performed the research; Okazaki A provided patient’s data; Okazaki A, Miyazaki K, Kihira K and Furuhashi M managed the patient with PPROM; Furuhashi M wrote the manuscript; all authors approved the final manuscript.Correspondence to: Madoka Furuhashi, MD, PhD, Depart-ment of Obstetrics and Gynecology, Japanese Red Cross Nagoya Daiichi Hospital, 3-35 Michishita-cho, Nakamura-ku, Nagoya 453-8511, Japan. [email protected]: +81-52-4815111 Fax: +81-52-4827733Received: February 27, 2013 Revised: April 22, 2013Accepted: May 8, 2013Published online: May 10, 2013
AbstractCaput succedaneum is relatively common at birth but infrequently diagnosed in utero. We report the first case of a prenatal incarcerated caput succedaneum af-ter cervical cerclage in a patient with premature rupture of the membranes (PPROM). A 41-year-old woman was referred and admitted to our hospital due to PPROM at 19 wk of gestation. Aggressive therapy, including amnioinfusion, cervical cerclage, and administration of antibiotics and tocolysis, was initiated. At 24 wk of gestation, a thumb tip-sized and polyp-like mass, which was irreducible, was delineated with a vaginal examina-tion, vaginal speculum, and transvaginal ultrasonogra-phy, leading to the diagnosis of incarcerated caput suc-cedaneum. Under general anesthesia, the incarcerated caput succedaneum was repositioned with fingers after cutting the string to avoid necrosis, and then, place-ment of a McDonald cervical cerclage was undertaken again. At 26 wk of gestation, she delivered a 678 g girl through an emergency cesarean section performed due to profuse bleeding and prolonged decelerations. A slight bulge with hair was observed on the head by palpation at birth. Cephalic ultrasonography, X-ray, magnetic resonance imaging and electroencephalogram
confirmed no abnormality. Although the baby needed oxygen (0.2 L/min) at the time of hospital discharge, she has grown favorably at three years of corrected age.
© 2013 Baishideng. All rights reserved.
Key words: Caput succedaneum; Cervical cerclage; Pa-tient with premature rupture of the membranes; Ultra-sonography; Prenatal
Core tip: Caput succedaneum is relatively common at birth but infrequently diagnosed in utero. Furthermore, no case of incarceration of antenatal caput succedane-um has been reported in the literature. This is the first report of prenatal and incarcerated caput succedaneum after cervical cerclage in a patient with premature rup-ture of the membranes (PPROM). The presenting case makes obstetricians recognize that cerclage placement, especially in a patient with PPROM, may result in un-usual caput succedaneum in utero. When it develops to incarceration, earlier release should be considered to prevent the serious complication of necrosis.
Okazaki A, Miyazaki K, Kihira K, Furuhashi M. Prenatal incar-ceration of caput succedaneum: A case report. World J Obstet Gynecol 2013; 2(2): 34-36 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i2/34.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i2.34
INTRODUCTIONCaput succedaneum is a cranial subcutaneous serohemat-ic extravasation that can be differentiated from cephalhe-matoma by findings of extension over a suture line and definite palpable edges. It is more likely to form during a prolonged or difficult delivery and often resolves in sev-eral d without sequelae. Furthermore, it is relatively com-mon at birth but infrequently diagnosed in utero[1-4]. We present a case of caput succedaneum that was diagnosed
CASE REPORT
34 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com

Okazaki A et al . Prenatal incarceration of caput succedaneum
by ultrasonographic examination during the antepartum period.
CASE REPORTA 41-year-old woman, gravida 3, para 0, was referred and admitted to our hospital due to patient with premature rupture of the membranes (PPROM) at 19 wk and 6 d of gestation. Her surgical history was unremarkable, except for conization of the cervix at age 37 for carcinoma in situ. She had been on insulin therapy due to diabetes mel-litus. On admission, she was afebrile. The plasma level of C-reactive protein (CRP) and white blood cell count were 0.1 mg/dL and 9500/mm3, respectively. These find-ings showed that there was no clinical chorioamnionitis. Vaginal examination demonstrated 2 cm-dilated cervical os and amniotic fluid flowing out. Laboratory culture of the vaginal discharge was negative. She reported a history of intermittent staining since the first trimester of preg-nancy. Ultrasound showed that the cervical length was 28 mm, and the maximum cord-free amniotic pocket was 2.5 cm. Although we informed her that she might have a bad prognosis, she wanted to continue the pregnancy. A catheter was transabdominally indwelled in the amniotic cavity after introduction of a 21-gauge needle under con-tinuous ultrasound guidance. Although the amniotic cul-ture was negative, the amniotic fluid polymorphonuclear neutrophil leukocyte, glucose, lactate dehydrogenase, and neutrophil elastase levels were 371 cells/mm3, 20 mg/dL, 2575 IU/L, and 14.7 μg/mL, respectively, showing intra-amniotic inflammation[5]. She underwent placement of a McDonald cervical cerclage using polyester tape under intravenous anesthesia to prevent cervical dilation. Subse-quently, amnioinfusion was initiated, whose purpose was not retention of the fluid but lavage throuth perfusion. Approximately 1000 mL/d sterile and warm saline was spontaneously drip- infused into the amniotic cavity, and the corresponding volume of fluid flowed out every day. Magnesium sulfate and ritodrine were used for tocolysis. Antibiotic therapy was also given. Cefmetazole sodium (2 g/d iv), piperacillin sodium (4 g/d iv), anhydrous cef-triaxone sodium (2 g/d iv), and meropenem trihydrate (1 g/d iv) were administered in sequential order until delivery. The level of blood CRP and white blood cell was in the normal range. At 23 wk and 3 d of gestation, a small amount of outflow was unexpectedly observed, although a certain level of amniotic fluid was observed in utero by ultrasonography. The latter finding suggested obstruction of the cervical canal. Thus, saline inflow was kept at the level of outflow to prevent hydramnios. At 24 wk and 0 d of gestation, a thumb tip-sized and polyp-like mass, which was irreducible, was delineated with a vaginal examination. A vaginal speculum demonstrated a purple-black-colored mass with hair on the surface. These find-ings along with transvaginal ultrasonography (Figure 1A) led to the diagnosis of caput succedaneum. Because the most feared sequela was necrosis, we decided that the in-carceration should be released. Under general anesthesia,
the incarcerated caput succedaneum was repositioned with fingers after cutting the string, and then, placement of a McDonald cervical cerclage was undertaken again. The same treatment strategy as before was taken to al-low the fetus to become mature enough to survive. At 25 wk and 0 d of gestation, transvaginal ultrasonography showed an echogenic bulge within the soft tissue of the fetal head (Figure 1B). The estimated fetal weight was 598 g, corresponding to the weight for 23 wk and 3 d. At 26 wk and 1 d of gestation, profuse bleeding occurred, and prolonged decelerations were observed on fetal heart rate monitoring. Thus, an emergency cesarean section was performed, and she delivered a 678 g girl with an Ap-gar score of 1 (5-min). There was a true knot of the um-bilical cord. Placental pathology demonstrated histologic chorioamnionitis (Grade 3) and funisitis (Grade 2). The arterial blood gas analyses of the umbilical cord showed that the pH and base deficit were 7.04 and 17.9 mmol/L, respectively. Resuscitation was started without delay. The levels of CRP and immunoglobulin M were 5 μg/dL and 9 mg/dL, respectively. Arterial blood culture was nega-tive. The head of the newborn baby looked normal with hair by inspection, but a slight bulge was observed by palpation at birth. Cephalic ultrasonography, X-ray, and magnetic resonance imaging confirmed no abnormality, such as an intracranial hemorrhage, a skull fracture, or a bone defect. She had a normal electroencephalogram at 1 and 40 wk after birth. The newborn central hearing
35 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
h
c
B
h
A
Figure 1 Transvaginal ultrasonography. A: A bulge (arrowheads) with an echogenic core was identified outside the cervical string (arrows); B: The bulge (arrowheads) was observed within the contour of the fetal head but inside the cervical string (arrows) 7 d after re-operation. h: Fetal head; c: Cervix.

screening showed no abnormality. Meanwhile, she was af-fected with retinopathy of prematurity and received laser coagulation. She has grown favorably without alopecia and shows normal physical and neurological development at three years of corrected age.
DISCUSSIONThe common management in most centers of PPROM before 22 wk of gestation is termination of the preg-nancy or the expectant approach because expectant man-agement results in an increased rate of fetal and neonatal morbidity and mortality[6,7]. When a patient with previable PPROM desires continuation of the pregnancy, more aggressive interventions, such as amnioinfusion[8], cervi-cal cerclage, and intra-amniotic gelatin sponge[9], are not infrequently required in addition to the administration of antibiotics and tocolysis to prolong pregnancy until the fetus becomes viable. In such cases, our usual protocol is to supply continuous amnioinfusion, cervical cerclage, and the use of antibiotics and tocolysis after obtaining informed consent[10]. The aggressive intervention of pre-viable PPROM results in a high neonatal survival rate[10].
Caput succedaneum is a cranial subcutaneous serohe-matic extravasation that is more likely to form during a prolonged or difficult delivery and often resolves in sev-eral d without sequelae. Although it has been infrequently diagnosed in utero[1-4], no case of incarceration has been reported in the literature. It would appear that several factors are associated with incarceration of caput suc-cedaneum. Uterine contractions are primarily inevitable, as usual caput succedaneum is formed during delivery. In addition, PPROM might play a pivotal role because pressure is directly placed on the fetal scalp contiguous to the internal os of the uterus in the setting of oligohy-dramnios. This assumption is supported by the fact that a percentage of cephalhematoma and caput succedaneum in utero is involved in PPROM[2-4]. Cerclage placement is also a contributing factor. Even a successful cerclage may result in limited dilation of the cervix when uterine con-tractions are persistent because they may promote cervi-cal maturation and diminish its thickness. In that event, the opening encircled by the suture might induce pro-lapse of the caput succedaneum and form an incarcera-tion when it swells. Considering that only a slight bulge of the newborn head was observed at birth in our case, caput succedaneum in utero could spontaneously reduce but for incarceration.
One of the serious sequelae of perinatal scalp injury is halo scalp ring, which is annular scalp alopecia. Al-though it is usually a temporary defect, a necrotic caput succedaneum may result in scarring alopecia because deep ulceration can destroy hair follicles[11,12]. This con-cept suggests that incarceration of caput succedaneum
is harmful to the fetus. Because it is not difficult to diagnose prenatal incarceration of caput succedaneum through vaginal examination and ultrasonography, special attention should be paid to prevent undesirable necrosis.
In conclusion, obstetricians should recognize that cerclage placement, especially in a patient with PPROM, may result in unusual caput succedaneum in utero. When it develops to incarceration, earlier release should be con-sidered to prevent the serious complication of necrosis.
REFERENCES1 Sherer DM, Allen TA, Ghezzi F, Gonçalves LF. Enhanced
transvaginal sonographic depiction of caput succedaneum prior to labor. J Ultrasound Med 1994; 13: 1005-1008 [PMID: 7877201]
2 Petrikovsky BM, Schneider E, Smith-Levitin M, Gross B. Cephalhematoma and caput succedaneum: do they always occur in labor? Am J Obstet Gynecol 1998; 179: 906-908 [PMID: 9790368 DOI: 10.1016/S0002-9378(98)70187-5]
3 Bats AS, Senat MV, Mohlo M, Ville Y. [Discovery of caput succedaneum after premature rupture of the membranes at 28 weeks gestation]. J Gynecol Obstet Biol Reprod (Paris) 2003; 32: 179-182 [PMID: 12717309]
4 Gerscovich EO, McGahan JP, Jain KA, Gillen MA. Caput succedaneum mimicking a cephalocele. J Clin Ultrasound 2003; 31: 98-102 [PMID: 12539251 DOI: 10.1002/jcu.10138]
5 Kidokoro K, Furuhashi M, Kuno N, Ishikawa K. Amniotic fluid neutrophil elastase and lactate dehydrogenase: associa-tion with histologic chorioamnionitis. Acta Obstet Gynecol Scand 2006; 85: 669-674 [PMID: 16752257 DOI: 10.1080/01443610600604432]
6 Dewan H, Morris JM. A systematic review of pregnancy out-come following preterm premature rupture of membranes at a previable gestational age. Aust N Z J Obstet Gynaecol 2001; 41: 389-394 [PMID: 11787910]
7 Dinsmoor MJ, Bachman R, Haney EI, Goldstein M, Mack-endrick W. Outcomes after expectant management of ex-tremely preterm premature rupture of the membranes. Am J Obstet Gynecol 2004; 190: 183-187 [PMID: 14749657 DOI: 10.1016/S0002-9378(03)00926-8]
8 Locatelli A, Vergani P, Di Pirro G, Doria V, Biffi A, Ghidini A. Role of amnioinfusion in the management of premature rup-ture of the membranes at <26 weeks’ gestation. Am J Obstet Gynecol 2000; 183: 878-882 [PMID: 11035330 DOI: 10.1067/mob.2000.108873]
9 O’Brien JM, Barton JR, Milligan DA. An aggressive interven-tional protocol for early midtrimester premature rupture of the membranes using gelatin sponge for cervical plugging. Am J Obstet Gynecol 2002; 187: 1143-1146 [PMID: 12439492 DOI: 10.1067/mob.2002.127124]
10 Miyazaki K, Furuhashi M, Yoshida K, Ishikawa K. Aggres-sive intervention of previable preterm premature rupture of membranes. Acta Obstet Gynecol Scand 2012; 91: 923-929 [PMID: 22536879 DOI: 10.1111/j.1600-0412.2012.01432.x]
11 Tanzi EL, Hornung RL, Silverberg NB. Halo scalp ring: a case series and review of the literature. Arch Pediatr Adolesc Med 2002; 156: 188-190 [PMID: 11814382]
12 Siegel DH, Holland K, Phillips RJ, Drolet BA, Esterly NB, Frieden IJ. Erosive pustular dermatosis of the scalp after perinatal scalp injury. Pediatr Dermatol 2006; 23: 533-536 [PMID: 17155993 DOI: 10.1111/j.1525-1470.2006.00304.x]
P- Reviewers Inês Rosa M, Khajehei M, Li JX S- Editor Gou SX L- Editor A E- Editor Zheng XM
36 May 10, 2013|Volume 2|Issue 2|WJOG|www.wjgnet.com
Okazaki A et al . Prenatal incarceration of caput succedaneum

World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 August 10; 2(3): 37-61
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com

37 Thegeneralsurgeonininter-disciplinarygynaecologicalcancercare
Isichei MW, Ismaila BO
42 Intrapartumapplicationofthecontinuousglucosemonitoringsystemin
pregnanciescomplicatedwithdiabetes:Areviewandfeasibilitystudy
Harizopoulou VC, Tsiartas P, Goulis DG, Vavilis D, Grimbizis G, Theodoridis TD,
Tarlatzis BC
47 Laparoscopicsurgicalrepairofpelvicorganprolapseandfemalestress
urinaryincontinence
Mourmouris PI, Skolarikos A, Mitsogiannis IC, Migdalis V, Papatsoris AG
53 Smokingandgenitalhumanpapillomavirusinfectioninwomenattending
cervicalcancerscreeninginGreece
Chatzistamatiou K, Katsamagas T, Zafrakas M, Zachou K, Orologa A, Fitsiou F,
Theodoridis T, Konstantinidis T, Konstantinidis TC, Agorastos T
Contents
IWJOG|www.wjgnet.com August 10, 2013|Volume 2|Issue 3|
TOPIC HIGHLIGHT
World Journal ofObstetrics and GynecologyW J O G
Quarterly Volume 2 Number 3 August 10, 2013
MINIREVIEW
BRIEF ARTICLE

ContentsWorld Journal of Obstetrics and Gynecology
Volume 2 Number 3 August 10, 2013
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Xin-Xin Che Responsible Science Editor: Xiu-Xia SongResponsible Electronic Editor: Xiao-Mei ZhengProofing Editor-in-Chief: Lian-Sheng Ma
World Journal of Obstetrics and GynecologyRoom 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected]://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza, 315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188Telephone: +852-31779906E-mail: [email protected]://www.wjgnet.com
PUBLICATIONDATEAugust 10, 2013
COPYRIGHT© 2013 Baishideng. Articles published by this Open-Access journal are distributed under the terms of the Creative Commons Attribution Non-commercial Li-cense, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in this journal represent the view-points of the authors except where indicated otherwise.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm.
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
IIWJOG|www.wjgnet.com
APPENDIX
ABOUT COVER
AIM AND SCOPE
FLYLEAF
August 10, 2013|Volume 2|Issue 3|
NAMEOFJOURNALWorld Journal of Obstetrics and Gynecology
ISSNISSN 2218-6220 (online)
LAUNCHDATEJune 10, 2012
FREQUENCYQuarterly
EDITOR-IN-CHIEFBo Jacobsson, MD, PhD, Professor, Department Obstetrics and Gynecology, Sahlgrenska University Hospital/Ostra, SE-416 85 Gothenburg, Sweden
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice Director
I-V Instructionstoauthors
EditorialBoardMemberofWorld JournalofObstetricsandGynecology ,AthanasiosPapatsorisGPapatsoris,MD,MSc,PhD,FEBU,FES,AssistantProfessor,2ndDepartmentofUrology,UniversityofAthens,SismanoglioHospital,15126,Athens,Greece
World Journal of Obstetrics and Gynecology (World J Obstet Gynecol, WJOG, online ISSN 2218-6220, DOI: 10.5317) is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJOG covers topics concerning pregnancy complications, obstetric surgical procedures, diagnostic imaging, endoscopy, reproductive endocrinology, tumors, pelvic diseases, evidence-based medicine, epidemiology and nursing.
We encourage authors to submit their manuscripts to WJOG. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Obstetrics and Gynecology is now indexed in Digital Object Identifier.
I-III EditorialBoard
INDEXING/ABSTRACTING

Key words: General surgeon; Inter disciplinary; Diagno-sis; Treatment; Gynaecological; Cancer
Core tip: Gynaecologic cancers constitute a major can-cer burden. The general surgeon’s role in inter-disciplin-ary gynaecological cancer differs between developed and developing countries. The increased sub-special-ization in surgery in developed countries has obviated the need for the general surgeon in gynaecologic can-cer care. In developing countries the general surgeon plays an essential but variable role, depending on the medical infrastructure and available manpower, which is usually limited in this setting. Interdisciplinary care is an emerging concept aimed at improving outcomes in cancer management and may be useful irrespective of the setting.
Isichei MW, Ismaila BO. The general surgeon in inter-disciplinary gynaecological cancer care. World J Obstet Gynecol 2013; 2(3): 37-41 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i3/37.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i3. 37
INTRODUCTION Cancers which primarily affect women are a major contri-bution to the global cancer burden. When breast cancer is excluded, gynaecological cancers still constitute a sig-nificant part of the cancer burden worldwide. Gynaeco-logical cancer includes, but is not limited to, cancers of the cervix, uterus, ovary, vulva and vagina. Since cervical, uterine and ovarian cancers are the most common gynae-cological cancers, they will be the main ones considered in this review. Of the estimated 12.7 million new cancer cases in 2008, cancers of the cervix uterus and ovaries accounted for 529000 (4.2%), 287000 (2.3%) and 225000 (1.8%), respectively, and these cancers were responsible
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i3.37
World J Obstet Gynecol 2013 August 10; 2(3): 37-41ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
The general surgeon in inter-disciplinary gynaecological cancer care
Mercy Wakili Isichei, Bashiru Omeiza Ismaila
Mercy Wakili Isichei, Bashiru Omeiza Ismaila, Department of Surgery, University of Jos and Jos University Teaching Hospital, 930001 Plateau State, NigeriaAuthor contributions: Isichei MW designed and compiled the review article; Ismaila BO reviewed articles and performed final reading of the review.Correspondence to: Dr. Mercy Wakili Isichei, Department of Surgery, University of Jos and Jos University Teaching Hospital, Box 745 Jos, 930001 Plateau State, Nigeria. [email protected]: +234-73-610514 Fax: +234-73-460319Received: September 13, 2012 Revised: April 3, 2013Accepted: April 9, 2013Published online: August 10, 2013
AbstractGynaecological cancers pose a significant cancer bur-den globally. In 2008 cancers of the cervix, uterus and ovaries accounted for 529000 (4.2%), 287000 (2.3%) and 225000 (1.8%) cancers, respectively, and together were responsible for 486400 deaths. Inter-disciplinary gynaecological care is an emerging concept aimed at providing more effective care by integrating different disciplines into a team working together to perform the various aspects of management at one time. This mod-el has both advantages and potential shortcomings. In advanced healthcare systems there appears to be little role for the general surgeon. However in developing world, the general surgeon has a valuable, but comple-mentary role in inter-disciplinary gynaecological cancer care. This role depends on the available workforce and includes, but is not limited to, the establishment of a diagnosis and treatment, including the management of complications. There is however little evidence-based research to provide guidance on the general surgeon’s role in inter-disciplinary gynecologic cancer care and more research is needed.
© 2013 Baishideng. All rights reserved.
TOPIC HIGHLIGHT
37 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Chibuike O Chigbu, MD, Series Editor

for 486400 of the 7.6 million cancer deaths in the same year. These 3 gynaecological cancers alone are among the 10 most common cancers in women[1].
A general surgeon is difficult to define. Trunkey’s statement over 25 years ago provides an interesting but adequate description. He stated that a general surgeon is one who can treat the injured, the very sick patient and perform non-cardiac thoracic, general vascular, gut and gland surgery[2]. While there is currently increasing sub-specialization within general surgery, we would concern ourselves with those specialists trained in general surgery who can provide competent and high quality care across a broad range of conditions. A general surgeon may be involved in the management of patients with gynae-cological cancer for reasons including those related to diagnosis, treatment, and follow-up as well as workforce availability. Traditionally the general surgeon’s role in the management of gynaecological cancer depends strongly on the medical infrastructure and varies from country to country and from region to region. There is a major difference in the role of a general surgeon in interdisci-plinary gynaecological cancer care between developed and developing countries. While specialists and subspe-cialists are widely available in the developed world, with technology that aids accurate diagnosis and treatment, the reverse is the case in the developing world[3,4]. This review article will discuss the role of the general surgeon in interdisciplinary gynaecological cancer from these two perspectives.
Modern cancer care may be interdisciplinary or mul-tidisciplinary with different specialties contributing their knowledge and experience to improve patient outcome. It has become important for health workers to collaborate to achieve improved outcomes. They bring knowledge and expertise from their different disciplines which can be effectively channeled into better patient care. The vari-ous disciplines working together in a team complement each other[5]. Suitable definitions of interdisciplinary and multidisciplinary teams have been difficult[6]. An interdis-ciplinary team may be described as that which integrates separate disciplines into a single consultation. This is such that history taking, physical examination, diagnosis and management are conducted with the patient by the combined team at one time[7]. This should be differenti-ated from multidisciplinary care which also utilizes the skills and experience of individuals from different disci-plines but with each discipline approaching the patient from their own perspective. The consultations may be arranged for different times on a single day and the mul-tidisciplinary team meets frequently to discuss the man-agement, but in the absence the patient[8]. It is expected that each member of the interdisciplinary team should be individually knowledgeable, skillful, reliable, experienced, and able to communicate effectively sharing responsibil-ity in teamwork[9]. The general surgeon is no exception.
Advantages of interdisciplinary care are related to the patient, health workers and the health care system. Ad-vantages to the patient include better outcomes, reduced
waiting time and greater level of involvement in decision making. For the health worker, advantages are more equal workload distribution, increased learning opportunities and greater work satisfaction. On the whole, there is reduced cost and more efficient utilization of the health care system. Possible disadvantages include role confu-sion, differing values and interests, and sometimes lack of common purpose[6]. In addition, the views of quieter team member may be neglected. There is a paucity of literature on the role of a general surgeon in an interdis-ciplinary team.
In developed countries, current recommended man-agement for gynaecogical cancer is multidisciplinary[5]. The team is generally made up of a gynaecological oncologist, a site specialist oncologist, pathologist, gyn-aecological cancer nurse specialist, radiologist, palliative care specialist and a clinical geneticist. In addition, patient management is aided by advanced medical equipment including those used for imaging, thus pretreatment diag-nosis and staging is usually known and treatment planned accordingly.
DIAGNOSISGynaecological malignancies present in various ways. Pre-sentation depends on the type of cancer, site and stage. Classical presentation with vaginal bleeding and other symptoms related to the female reproductive tract are likely to present no difficulty to the primary care physi-cians or the gynecologists. Cancers detected by screening, like cervical cancer, are also relatively straightforward in terms of diagnosis.
Occasionally a general surgeon may encounter a gyn-aecological malignancy while managing surgical patients. If this occurs preoperatively it is recommended that the patient be referred to the gynaecological oncology team. However, if this occurs intraoperatively it is more dif-ficult to decide on treatment, but studies have shown that patient outcomes are better when gynaecological cancer surgeries are performed by gynaecogical oncologists[10,11].
In this context, the role of a general surgeon in an interdisciplinary setting may be to contribute in the initial clinical assessment of a patient with a gynaecological tu-mour which has progressed to involve other organs. This may be the case in a patient with ovarian cancer who has relapsed. However, it may be argued that rather than the general surgeon, the specific sub-specialists associated with the cancer sites should be part of the interdisciplin-ary team. In this context then, there will be little role if any for the general surgeon. In reality it may be that, in this context, there is little need for the specialist referred to as a general surgeon in any role.
The converse is the situation in the developing world, characterized by the absence of skilled manpower and equipment. The classical presentations of gynaecological malignancies will similarly present no major difficulty in diagnosis for the primary care physicians and gynaecolo-gists but precise diagnosis and staging may be challenging
38 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Isichei MW et al . General surgeon in gynaecological cancer

due to inadequate complementary diagnostic investiga-tions, such as modern imaging. There is greater reliance on the clinical evaluation in this setting, with the atten-dant difficulty in accurate staging[12]. Patients also tend to present at healthcare facilities later, with more advanced disease and attendant complications[13].
In this setting, the general surgeon as a part of in-terdisciplinary care may contribute in the process of history taking and examination by helping to determine or exclude involvement of other organs. Advanced gyn-aecological tumors presenting as intra abdominal masses, gastrointestinal or vascular obstruction, will require in-put from the general surgeon. Ovarian tumors are well known for their relatively late presentation[14] and compli-cations such as bowel obstruction are common[15]. This type of late presentation is common in less developed countries where there are limited investigation modalities and preoperative diagnosis may be difficult. Sometimes the exact diagnosis is determined during surgery. The general surgeon will provide knowledge and experience that would be useful to the interdisciplinary team in the evaluation of these cases. The presence of metastatic disease at sites remote from the female reproductive tract will be easier for the general surgeon to detect during the interdisciplinary evaluation of the patient. The general surgeon may also play a complementary role in the choice of investigations in the diagnostic work-up, enabling early, relevant and necessary investigations that will influ-ence further management. Involvement of neighboring structures, such as small and large bowel, and ureters are determined early. The presence of remote metastases and how this may affect treatment plans (curative versus pal-liative) is another area where the general surgeon’s exper-tise will be useful.
Some patients with gynaecological malignancies have hereditary cancers and may have or be at risk of other tumours outside the female reproductive tract. These include hereditary non-polyposis colorectal cancer syn-dromes (HNPCC) and BRCA mutations[16]. These are now largely managed by colorectal and breast surgeons as part of the interdisciplinary team in developed countries. However, the general surgeon replaces these sub-special-ists in developing countries, and may be able to advise on the possible need for further genetic evaluation.
A possible drawback in the interdisciplinary approach to these patients may be the loss of privacy involved in asking questions about, and evaluation of parts of the body that are normally concealed. Thus the patient may feel uncomfortable divulging information and exposing her body to examination by a group.
TREATMENTTreatment of gynaecological cancer is multimodal. Op-tions include surgery, radiotherapy, chemotherapy and hormonal therapy. It is not uncommon for patients to undergo extensive pelvic surgery with neoadjuvant or adjuvant chemotherapy as well as chemotherapy. The
multimodal treatment of these tumours already encour-ages multidisciplinary collaboration and has the potential to foster an interdisciplinary approach to patient care. Modern trends suggest that surgical treatment should be done by gynaecological oncologists for more favorable outcomes. However in the interdisciplinary setting, the treatment of the patient is individualized, recognizing the needs, condition and aim of treatment. Treatment with curative intent should be the goal but is not always possible and the interdisciplinary team has the potential to offer the best available form of care when the team brings their collective expertise to bear. For early tumors the gynaecological oncologist in conjunction with the team attempt to achieve a cure, but the radiologist and pathologist aid in determining accurately what constitutes early disease. Tumour involvement of adjacent organs may require the inclusion of other specialists like urolo-gists and colorectal surgeons, especially in more advanced tumors. As previously discussed, the role of the general surgeon is limited in advanced countries.
However in less advanced healthcare settings, as a re-sult of dearth of relevant manpower, the general surgeon can contribute to the decision on the type and extent of surgery and the need for other modalities of treatment. Issues such as the extent of resection, dealing with other involved organs and whether a stoma is required tempo-rarily or permanently, can be resolved preoperatively. The role of surgery in the management of early and advanced gynaecological cancer is established[17-20]. Even intraopera-tively, the presence of more extensive disease than antici-pated or detected preoperatively poses less of a challenge to the interdisciplinary team. Modifications to the opera-tive technique traditionally out of the purview of the gynecological oncologist can be carried out readily and competently without the need for further surgery. Issues such as bowel involvement and possible need for primary anastomosis or the creation of stoma, are addressed confidently as they arise and vascular involvement by the tumour need not be an indication for limiting the extent of surgery. Intraoperative complications, especially in ex-tensive surgeries, involving bowel, vessels and the urinary tract, can be repaired during a single surgery. Surgical management of advanced gynaecological malignancies poses a major challenge in oncological care[19]. The gen-eral surgeon will provide assistance in cytoreductive and palliative surgeries. It is important to note that oncologi-cal care in less developed countries at present largely in-volves management of advanced diseases. Closely related to advanced presentation is the treatment of recurrent disease either as a result of previous suboptimal or in-adequate treatment or of disease recurrence even in well treated cases.
Use of multimodal treatment options like radio-therapy for gynaecological malignancies increases the risk of bowel related complications such as fistulae and stric-tures[21]. Definition of the extent and location of these complications may require the expertise of a general sur-geon in the interdisciplinary team.
39 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Isichei MW et al . General surgeon in gynaecological cancer

There have been reports that patients managed by gynaecological oncologists have better outcomes than those treated by general surgeons[10,11]. This may be re-lated more to the working environment rather than surgi-cal skill[22]. However, it is clear that multidisciplinary care results in better outcomes[23-27]. The role of a general sur-geon in interdisciplinary care will be complementary and useful even if there are doubts about the outcome when he/she manages the patient alone.
FOLLOW UPPatients with gynaelogical cancer may undergo multimod-al treatment with curative or palliative intent. They may be cured, or symptoms effectively palliated. At the other extreme, they may develop debilitating complications from the cancer or it treatment. Often the outcome falls between these two extremes, therefore consigning the patient to a lifetime of repeated evaluation to determine recurrence, manage symptoms and treat complications. The general surgeon’s skill is a useful part of the interdis-ciplinary management of these patients. Gastrointestinal symptoms and complications can be detected and man-aged accordingly.
Evaluation of the patient for evidence of recurrence or distant spread may enable earlier detection and appro-priate management.
WORKFORCEIn parts of the world where there is inadequate availabil-ity of health workers to manage gynaecological cancers, general surgeons may provide a readily available pool that can provide the knowledge and technical skill required to achieve better outcomes in an interdisciplinary setting. They also can be trained to fill any gaps that currently ex-ist in the provision of high quality gynaecological oncol-ogy services.
There is little evidence in the literature about the role of general surgeons in interdisciplinary health teams involved in the management of gynecological cancers. Research in this and related areas is required.
CONCLUSION Interdisciplinary healthcare is an emerging system which challenges the traditional paradigms. It has the potential to improve patient care and change the way gynaeco-logical cancer is managed. The general surgeon’s role in an interdisciplinary team for gynaecological care can be viewed from two perspectives; in an advanced healthcare setting in which his/her role is very limited due to the availability of the relevant subspecialists, and in a less advanced setting in which his/her role is complementary but important and useful. The general surgeon may be a valuable resource where there is inadequate manpower and should perhaps be trained in gynaecological oncol-ogy to provide optimal care.
REFERENCES1 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.
Estimates of worldwide burden of cancer in 2008: GLOBO-CAN 2008. Int J Cancer 2010; 127: 2893-2917 [PMID: 21351269 DOI: 10.1002/ijc.25516]
2 Irving M. The general surgeon. Br Med J (Clin Res Ed) 1986; 292: 741-742 [PMID: 3082420 DOI: 10.1136/bmj.292.6522.741]
3 Chinnock P, Siegfried N, Clarke M. Is evidence-based medi-cine relevant to the developing world? PLoS Med 2005; 2: e107 [PMID: 15916456 DOI: 10.1371/journal.pmed.0020107]
4 Jones SB. Cancer in the developing world: a call to action. BMJ 1999; 319: 505-508 [PMID: 10454408 DOI: 10.1136/bmj.319.7208.505]
5 Kidger J, Murdoch J, Donovan JL, Blazeby JM. Clinical de-cision-making in a multidisciplinary gynaecological cancer team: a qualitative study. BJOG 2009; 116: 511-517 [PMID: 19250362 DOI: 10.1111/j.1471-0528.2008.02066.x]
6 McCallin A. Interdisciplinary practice--a matter of teamwork: an integrated literature review. J Clin Nurs 2001; 10: 419-428 [PMID: 11822488 DOI: 10.1046/j.1365-2702.2001.00495.x]
7 Petoukhov K. Measuring the effectiveness of interdisciplin-ary health care teams in a primary care setting: a review of published evidence. IHCT Research Report
8 Jessup RL. Interdisciplinary versus multidisciplinary care teams: do we understand the difference? Aust Health Rev 2007; 31: 330-331 [PMID: 17669052 DOI: 10.1071/AH070330]
9 McCallin A. Interdisciplinary team leadership: a revisionist approach for an old problem? J Nurs Manag 2003; 11: 364-370 [PMID: 14641717 DOI: 10.1046/j.1365-2834.2003.00425.x]
10 Kehoe S, Powell J, Wilson S, Woodman C. The influence of the operating surgeon’s specialisation on patient survival in ovarian carcinoma. Br J Cancer 1994; 70: 1014-1017 [PMID: 7947077 DOI: 10.1038/bjc.1994.440]
11 Nguyen HN, Averette HE, Hoskins W, Penalver M, Sevin BU, Steren A. National survey of ovarian carcinoma. Part V. The impact of physician’s specialty on patients’ survival. Cancer 1993; 72: 3663-3670 [PMID: 8252483]
12 Ozsarlak O, Tjalma W, Schepens E, Corthouts B, Op de Beeck B, Van Marck E, Parizel PM, De Schepper AM. The correlation of preoperative CT, MR imaging, and clinical staging (FIGO) with histopathology findings in primary cervical carcinoma. Eur Radiol 2003; 13: 2338-2345 [PMID: 12802611]
13 Varughese J, Richman S. Cancer care inequity for women in resource-poor countries. Rev Obstet Gynecol 2010; 3: 122-132 [PMID: 21364864]
14 Monaghan JM. Malignant disease of the ovary. In: Edmonds DK, editor. Dewhurst's Textbook of Obstetrics and Gynae-cology for postgraduate. 6th ed. Oxford: Blackwell science Ltd., 1999: 590-601
15 Krouse RS, McCahill LE, Easson AM, Dunn GP. When the sun can set on an unoperated bowel obstruction: management of malignant bowel obstruction. J Am Coll Surg 2002; 195: 117-128 [PMID: 12113535 DOI: 10.1016/S1072-7515(02)01223-1]
16 Guillem JG, Wood WC, Moley JF, Berchuck A, Karlan BY, Mutch DG, Gagel RF, Weitzel J, Morrow M, Weber BL, Giardiello F, Rodriguez-Bigas MA, Church J, Gruber S, Of-fit K. ASCO/SSO review of current role of risk-reducing surgery in common hereditary cancer syndromes. J Clin Oncol 2006; 24: 4642-4660 [PMID: 17008706 DOI: 10.1200/JCO.2005.04.5260]
17 Aure JC, Hoeg K, Kolstad P. Clinical and histologic studies of ovarian carcinoma. Long-term follow-up of 990 cases. Ob-stet Gynecol 1971; 37: 1-9 [PMID: 4321469 DOI: 10.1097/00006254-197106000-00022]
18 Griffiths CT, Fuller AF. Intensive surgical and chemothera-peutic management of advanced ovarian cancer. Surg Clin North Am 1978; 58: 131-142 [PMID: 417410]
40 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Isichei MW et al . General surgeon in gynaecological cancer

19 Fader AN, Rose PG. Role of surgery in ovarian carcinoma. J Clin Oncol 2007; 25: 2873-2883 [PMID: 17617518]
20 Barakat RR. Contemporary management of endometrial cancer. In: Perry MC, editor. American Society of Clinical Oncology Educational Book. 38th Annual Meeting; Alexan-dria, VA, USA; 2002: 85-88
21 Baines M. The pathophysiology and management of malig-nant intestinal obstruction. In: Doyle D, Hanks GWC, Mac-Donald N, editors. Oxford Textbook of Palliative Medicine. 2nd ed. Oxford: Oxford University Press, 1998: 526-534
22 Münstedt K, Franke FE. Role of primary surgery in ad-vanced ovarian cancer. World J Surg Oncol 2004; 2: 32 [PMID: 15461788]
23 Junor EJ, Hole DJ, Gillis CR. Management of ovarian cancer: referral to a multidisciplinary team matters. Br J Cancer 1994; 70: 363-370 [PMID: 8054286 DOI: 10.1038/bjc.1994.307]
24 Junor EJ, Hole DJ, McNulty L, Mason M, Young J. Special-
ist gynaecologists and survival outcome in ovarian cancer: a Scottish national study of 1866 patients. Br J Obstet Gyn-aecol 1999; 106: 1130-1136 [PMID: 10549956 DOI: 10.1111/j.1471-0528.1999.tb08137.x]
25 Kiely BE, Friedlander ML, Milne RL, Stanhope L, Russell P, Jenkins MA, Weideman P, McLachlan SA, Grant P, Hopper JL, Phillips KA. Adequacy of risk-reducing gynaecologic sur-gery in BRCA1 or BRCA2 mutation carriers and other wom-en at high risk of pelvic serous cancer. Fam Cancer 2011; 10: 505-514 [PMID: 21424757 DOI: 10.1007/s10689-011-9435-0]
26 Messalli EM, Scaffa C, Mainini G, Rotondi M, Pecori E, Cobellis L. Third stage ovarian carcinoma--case report: the necessity of a multidisciplinary approach to treatment. Eur J Gynaecol Oncol 2006; 27: 291-293 [PMID: 16800262]
27 Mäkelä J, Kairaluoma MI, Kauppila A. Palliative surgery for intestinal complications of advanced, recurrent gynaecologic malignancy. Acta Chir Scand 1987; 153: 57-61 [PMID: 2437746]
P- Reviewer Hricak H S- Editor Wen LL L- Editor Hughes D E- Editor Zheng XM
41 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Isichei MW et al . General surgeon in gynaecological cancer

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i3.42
World J Obstet Gynecol 2013 August 10; 2(3): 42-46ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Intrapartum application of the continuous glucose monitoring system in pregnancies complicated with diabetes: A review and feasibility study
Vicentia C Harizopoulou, Panagiotis Tsiartas, Dimitrios G Goulis, Dimitrios Vavilis, Grigorios Grimbizis, Theodoros D Theodoridis, Basil C Tarlatzis
Vicentia C Harizopoulou, Dimitrios G Goulis, Dimitrios Vavi-lis, Grigorios Grimbizis, Theodoros D Theodoridis, Basil C Tarlatzis, Unit for Human Reproduction, First Department of Obstetrics and Gynaecology, Papageorgiou General Hospital, Ring Road, Nea Efkarpia, 54603 Thessaloniki, GreecePanagiotis Tsiartas, Department of Obstetrics and Gynecology, Sahlgrenska University Hospital, 41685 Göteborg, SwedenAuthor contributions: Harizopoulou VC and Tsiartas P con-tributed to analysis and interpretation of the data; Goulis DG contributed to the conception and design; Vavilis D contributed to critical revision of the article; Grimbizis G and Theodoridis TD contributed to the collection and assembly of data; Tarlatzis BC contributed to the final approval of the manuscript.Correspondence to: Vicentia C Harizopoulou, Midwife, MSc, PhDc, Unit for Human Reproduction, First Department of Ob-stetrics and Gynaecology, Papageorgiou General Hospital, Ring Road, Nea Efkarpia, 54603 Thessaloniki, Greece. [email protected]: +30-2313-323131 Fax: +30-2310-991520Received: December 23, 2012 Revised: April 21, 2013Accepted: May 18, 2013Published online: August 10, 2013
AbstractIntrapartum maternal normoglycemia seems to play an important role in the prevention of adverse perinatal, maternal and neonatal outcomes. Several glucose moni-toring protocols have been developed, aiming to achieve a tight glucose monitoring and control. Depending on the type of diabetes and the optimal or suboptimal glyc-emic control, the treatment options include fasting status of the parturient, frequent monitoring of capillary blood glucose, intravenous dextrose infusion and subcutane-ous or intravenous use of insulin. Continuous glucose monitoring system (CGMS) is a relatively new technology that measures interstitial glucose at very short time in-tervals over a specific period of time. The resulting pro-file provides a more comprehensive measure of glycemic
excursions than intermittent home blood glucose moni-toring. Results of studies applying the CGMS technology in patients with or without diabetes mellitus (DM) have revealed new insights in glucose metabolism. Moreover, CGMS have a potential role in the improvement of gly-cemic control during pregnancy and labor, which may lead to a decrease in perinatal morbidity and mortality. In conclusion, the use of CGMS, with its important tech-nical advantages compared to the conventional way of monitoring, may lead into a more etiological intrapartum management of both the mother and her fetus/infant in pregnancies complicated with DM.
© 2013 Baishideng. All rights reserved.
Key words: Diabetes mellitus; Pregnancy; Intrapartum management; Glucose monitoring protocols; Continu-ous glucose monitoring system
Core tip: In pregnancies complicated with diabetes, intrapartum maternal normoglycemia seems to play an important role in the prevention of adverse perinatal outcomes. Several glucose monitoring protocols have been developed, aiming to achieve a tight glucose monitoring and control intrapartum. The continuous glucose monitoring system is a relatively new technol-ogy; its intrapartum application in pregnancies com-plicated with diabetes is feasible, allows for a closer observation of glucose concentrations and is expected to lead to a more etiological management of both the mother and her fetus/infant.
Harizopoulou VC, Tsiartas P, Goulis DG, Vavilis D, Grimbizis G, Theodoridis TD, Tarlatzis BC. Intrapartum application of the continuous glucose monitoring system in pregnancies complicat-ed with diabetes: A review and feasibility study. World J Obstet Gynecol 2013; 2(3): 42-46 Available from: URL: http://www.
MINIREVIEW
42 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com

Harizopoulou VC et al . Intrapartum application of CGMS
wjgnet.com/2218-6220/full/v2/i3/42.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i3.42
INTRODUCTIONThe incidence of diabetes mellitus (DM) continues to rise worldwide[1,2]. Obviously, this increase affects the inci-dence of hyperglycemia in pregnancy[3]. The co-existence of DM and pregnancy, commonly encountered in clini-cal practice, is important both from a pathophysiology and clinical point of view as it is associated with short and long-term morbidity and mortality for the foetus/in-fant and the mother. Generally, it is accepted that tight glycemic control during pregnancy and labor leads to a decrease in perinatal morbidity and mortality. Pregnancies complicated with DM are treated intrapartum under this principle.
The continuous glucose monitoring system (CGMS) is a relatively new technology that measures interstitial glucose every 1 to 10 min for a maximum of 3 to 6 d, depending on the monitor used. The resulting profile provides a more comprehensive measure of glycemic excursions than in-termittent home blood glucose monitoring. Clinical indica-tions for CGMS use include conditions where tight control is crucial[4].
The aim of this review is to present the intrapartum glucose monitoring protocols in pregnancies complicated with DM. The potential role of CGMS as a tool in the achievement of the optimal glycemic control intrapartum is discussed in detail.
SIGNIFICANCE OF INTRAPARTUM NORMOGLYCEMIAAlthough the need for normoglycemia during pregnan-cies complicated with DM has been well established[5-8], the importance and need for intrapartum normoglycemia arise from epidemiological studies only[9-13]. Poor glycemic control intrapartum is associated with adverse maternal (hypoglycemia, ketoacidosis) and neonatal (hypoglyc-emia, ketoacidosis and respiratory distress syndrome) outcomes[14]. Neonatal hyperglycemia, specifically, has an impact not only on immediate morbidity but also seems to affect long-term neurological development[14].
It is generally accepted that the main target of intra-partum management in pregnancies complicated with DM is to achieve optimal glycemic control. On the other hand, the definition of “optimal” remains a matter of debate. In the literature, there is a great variance in the recommend-ed targets for blood glucose control during labor, ranging from 4.0-6.5 mmol/L[15] to 4.0-8.0 mmol/L[16] and 3.88- 6.5 mmol/L[17].
INTRAPARTUM GLUCOSE MONITORING PROTOCOLS Different protocols for glycemic control during labor
have been developed worldwide. The controversies in the literature concerning the management of pregnan-cies complicated with DM in the delivery room led to the adoption of different local policies[18-23]. Depending on the type of DM and the optimal or suboptimal glycemic control, the treatment options include fasting status of the parturient, frequent monitoring of capillary blood glucose, intravenous dextrose infusion and subcutaneous or intravenous use of insulin.
Most of the protocols are based on the intravenous dextrose and insulin infusion when the concentration of blood glucose is not maintained in the desired range. The insulin infusion rate usually depends on capillary blood glucose, which is monitored hourly during labor[17,23-25]. Specific algorithms that include simultaneous adjustment of both dextrose and insulin infusion rates during labor have been published. These are considered as the stand-ard of care since their efficacy and safety in reducing the risk for maternal hypoglycemia or ketoacidosis have been tested in many studies[23,26-28].
Insights into the pathophysiology and the intrapartum management of pregnancies complicated with insulin-re-quiring DM suggest that the amount of insulin required during the onset of labor is often zero; thus, it seems that the probability of ketoacidosis due to the prolonged fast-ing status constitutes a real problem[20-29].
CLINICAL INDICATION OF CGMS USEThe main clinical indications of the CGMS include: (1) adjustment of anti-diabetic treatment; (2) quantitative as-sessment of the effect of anti-diabetic therapy; (3) assess-ment of the effect of lifestyle changes in glycemic control; (4) situations where strict glycemic control is particularly important; (5) diagnosis and prevention of hypoglycemia, particularly during sleep; and (6) diagnosis and prevention of post-prandial hyperglycemia[4,30,31].
The most common use of CGMS is during the adjust-ment of anti-diabetic therapy towards a better glycemic control[30]. These adjustments include modification of insulin dosage before meals, change of the type of insu-lin administered, changes in the composition of the diet in carbohydrates, decrease in the dose of insulin during periods of intense physical exercise and changes in diet or DM treatment during the night in an attempt to avoid the “dawn phenomenon”[4,31]. CGMS have been also used in clinical trials concerning anti-diabetic agents in an attempt to obtain accurate data about their effect on patients’ glyc-emic profile[32]. CGMS have been used to monitor glucose levels not only in patients with DM, but also in other populations with high risk of hyperglycemia or hypoglyc-emia. Much attention has been paid to patients with cystic fibrosis[33,34] who face an increased risk of developing DM, in patients hospitalized in intensive care units[35] who are at a high risk of hypoglycemia[36,37] or hyperglycemia[35,38] and in patients with glycogen storage diseases[39] who also face an increased risk of hypoglycemia.
The aim of a very recent publication of a task force
43 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com

of experts appointed by the Endocrine Society was to formulate practice guidelines for determining settings where patients are most likely to benefit from the use of CGMS[40]. Indications and implications of the use of CGMS in the perinatal and intrapartum setting were not evaluated and so still need to be assessed.
USE OF CGMS IN PREGNANCYAlthough publications on the use of CGMS in pregnan-cies with or without DM are scarce, their significance is of great importance due to the proposed changes in the therapeutic approach.
The main research aims concerning the use of CGMS during pregnancy include comparison of CGMS to inter-mittent blood glucose monitoring (finger prick self-mon-itoring)[41-44], determination of the ideal time to measure post-prandial glucose concentrations[44-50] and day to day variability of the glycemic profile[41,51-54]. Additionally, some studies have evaluated the reliability, specificity and accuracy of the CGMS’s readings. In particular, the ability of CGMS to detect asymptomatic episodes of hypogly-cemia and hyperglycemia has been studied in pregnant women with DM type 1[41,42].
INTRAPARTUM APPLICATION OF CGMSIn 2008, two pilot studies concerning intrapartum appli-cation of CGMS were published. In a prospective study by Stenninger et al[55], a CGMS was used to monitor the glucose profile of fifteen pregnant women with insulin-treated DM in the last 120 min before delivery. The capil-lary plasma glucose concentrations were checked hourly and rapid-acting insulin analogues were injected subcuta-neously if these levels exceeded 7 mmol/L, in an attempt to reduce the frequency of early neonatal hypoglycemia. In their conclusions, researchers state that parturients with insulin-treated DM coped well with CGMS. They also emphasized the correlation between strict normogly-cemia and occurrence of postnatal hypoglycemia. Their suggestion was that CGMS is a feasible and valuable method for close glucose monitoring intrapartum. The interpretation emerges from the superiority of CGMS over intermittent blood glucose monitoring when maxi-mal information about glucose fluctuations is vital.
In the second study, Iafusco et al[56] used a real time CGMS to monitor the glucose profile of eighteen preg-nant women with DM type 1 in two phases: antenatal, during treatment with bethamethasone for fetal lung mat-uration and intrapartum. The main target in both phases was to achieve normoglycemia by using intravenous administration of insulin and glucose fluctuation moni-toring. In their conclusions, the researchers state that no infant experienced hypoglycemia or respiratory distress syndrome at the moment and within the first hours after birth. They also emphasized the importance of strict glycemic control in these two phases in pregnant women with DM type 1, considering the CGMS as an important tool to achieve it.
More recently, our group conducted a feasibility study[57] with the primary aim to assess the feasibility of the CGMS in the deliveries of pregnancies complicated with DM; a secondary aim was to examine CGMS acceptance by the women. The study involved twelve pregnant women with GDM. The minimally invasive microdialysis-based CGMS (Gluco-Day, Menarini Diagnostics) was used to record glucose profile during labor. The device was installed 6 h before delivery for a total of 48 h. As far as the primary aim is concerned, no pain was reported during sensor in-stallation and removal. Subcutaneous application into the abdominal wall did not affect the obstetric interventions. In the case of vaginal delivery, even an operative one, CGMS did not affect the continuous electronic fetal mon-itoring, the application of epidural analgesia, or the use of ultrasonography, when needed. In the case of caesarean section, the selection of the site for the placement of the sensor (far enough from the incision) and its careful im-mobilization guaranteed the successful recording. In two cases, the monitoring failed (breaking of the microdialysis fiber, device disconnection). As far as the secondary aim is concerned, the mode of delivery was associated with the acceptance of the device postpartum: all women that gave birth vaginally (n = 6) reported discomfort in contrast to the women that underwent caesarean section (n = 6). This can be attributed to different levels of postpartum mobility between the two groups. All women coped well with the CGMS and reported feeling secure by checking glucose concentrations in real-time.
CONCLUSIONIn pregnancies complicated with DM, both perinatal and intrapartum normoglycemia is an important milestone in the ultimate goal of reducing perinatal morbidity and mortality. Once diagnosed with DM, pregnancies receive special obstetric management by intense monitoring and adjustment of therapeutic interventions. Even then, the absolute absence of any complication is not guaranteed. Intrapartum glucose monitoring protocols were devel-oped in the name of strict glucose control, although there is still much to be elucidated in the pathophysiology of DM and its behavior intrapartum. CGMS is a tempting and promising technology, with its reliability, specificity and accuracy being evaluated and tested in recent clinical trials. The intrapartum application of CGMS in pregnan-cies complicated with DM allows for a closer observation of glucose concentrations and is expected to lead to a more etiological management of both the mother and her foetus/infant. As a future perspective, a large, pro-spective study is needed to determine the clinical implica-tions of intrapartum application of CGMS.
REFERENCES1 Burke JP, Williams K, Gaskill SP, Hazuda HP, Haffner SM,
Stern MP. Rapid rise in the incidence of type 2 diabetes from 1987 to 1996: results from the San Antonio Heart Study. Arch Intern Med 1999; 159: 1450-1456 [PMID: 10399896 DOI:
44 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Harizopoulou VC et al . Intrapartum application of CGMS

10.1001/archinte.159.13.1450]2 Wild S, Roglic G, Green A, Sicree R, King H. Global preva-
lence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27: 1047-1053 [PMID: 15111519 DOI: 10.2337/diacare.27.5.1047]
3 Hunt KJ, Schuller KL. The increasing prevalence of diabetes in pregnancy. Obstet Gynecol Clin North Am 2007; 34: 173-199, vii [PMID: 17572266 DOI: 10.1016/j.ogc.2007.03.002]
4 Klonoff DC. Continuous glucose monitoring technology de-livers detailed diabetes data. Point Care 2006; 5: 105-111 [DOI: 10.1097/01.poc.0000232577.13891.d3]
5 Adashi EY, Pinto H, Tyson JE. Impact of maternal eugly-cemia on fetal outcome in diabetic pregnancy. Am J Obstet Gynecol 1979; 133: 268-274 [PMID: 433986]
6 Skyler JS, O’Sullivan MJ, Robertson EG, Skyler DL, Hols-inger KK, Lasky IA, McLeod AG, Burkett G, Mintz DH. Blood glucose control during pregnancy. Diabetes Care 1980; 3: 69-76 [PMID: 6996971 DOI: 10.2337/diacare.3.1.69]
7 Yang X, Hsu-Hage B, Zhang H, Zhang C, Zhang Y, Zhang C. Women with impaired glucose tolerance during pregnancy have significantly poor pregnancy outcomes. Diabetes Care 2002; 25: 1619-1624 [PMID: 12196437 DOI: 10.2337/dia-care.25.9.1619]
8 Walkinshaw SA. Pregnancy in women with pre-existing diabetes: management issues. Semin Fetal Neonatal Med 2005; 10: 307-315 [PMID: 15927547 DOI: 10.1016/j.siny.2005.04.004]
9 Obenshain SS, Adam PA, King KC, Teramo K, Raivio KO, Räihä N, Schwartz R. Human fetal insulin response to sus-tained maternal hyperglycemia. N Engl J Med 1970; 283: 566-570 [PMID: 5450610 DOI: 10.1056/NEJM197009102831104]
10 Andersen O, Hertel J, Schmølker L, Kühl C. Influence of the maternal plasma glucose concentration at delivery on the risk of hypoglycaemia in infants of insulin-dependent dia-betic mothers. Acta Paediatr Scand 1985; 74: 268-273 [PMID: 3993374 DOI: 10.1111/j.1651-2227.1985.tb10963.x]
11 Carron Brown S, Kyne-Grzebalski D, Mwangi B, Taylor R. Ef-fect of management policy upon 120 Type 1 diabetic pregnan-cies: policy decisions in practice. Diabet Med 1999; 16: 573-578 [PMID: 10445833 DOI: 10.1046/j.1464-5491.1999.00124.x]
12 Jovanovic L. Glucose and insulin requirements during labor and delivery: the case for normoglycemia in pregnancies complicated by diabetes. Endocr Pract 2004; 10 Suppl 2: 40-45 [PMID: 15251639]
13 Balsells M, Corcoy R, Adelantado JM, García-Patterson A, Altirriba O, de Leiva A. Gestational diabetes mellitus: meta-bolic control during labour. Diabetes Nutr Metab 2000; 13: 257-262 [PMID: 11105967]
14 Stenninger E, Flink R, Eriksson B, Sahlèn C. Long-term neurological dysfunction and neonatal hypoglycaemia after diabetic pregnancy. Arch Dis Child Fetal Neonatal Ed 1998; 79: F174-F179 [PMID: 10194986 DOI: 10.1136/fn.79.3.F174]
15 Kline GA, Edwards A. Antepartum and intra-partum in-sulin management of type 1 and type 2 diabetic women: Impact on clinically significant neonatal hypoglycemia. Dia-betes Res Clin Pract 2007; 77: 223-230 [PMID: 17126946 DOI: 10.1016/j.diabres.2006.10.024]
16 Taylor R, Lee C, Kyne-Grzebalski D, Marshall SM, Davison JM. Clinical outcomes of pregnancy in women with type 1 diabetes(1). Obstet Gynecol 2002; 99: 537-541 [PMID: 12039106 DOI: 10.1016/S0029-7844(01)01790-2]
17 Guideline Development Group. Management of diabetes from preconception to the postnatal period: summary of NICE guidance. BMJ 2008; 336: 714-717 [PMID: 18369227 DOI: 10.1136/bmj.39505.641273.AD]
18 West TE, Lowy C. Control of blood glucose during labour in diabetic women with combined glucose and low-dose insu-lin infusion. Br Med J 1977; 1: 1252-1254 [PMID: 861562 DOI: 10.1136/bmj.1.6071.1252]
19 Nattrass M, Alberti KG, Dennis KJ, Gillibrand PN, Letch-worth AT, Buckle AL. A glucose-controlled insulin infusion
system for diabetic women during labour. Br Med J 1978; 2: 599-601 [PMID: 698607 DOI: 10.1136/bmj.2.6137.599]
20 Haigh SE, Tevaarwerk GJ, Harding PE, Hurst C. A method for maintaining normoglycemia during labour and delivery in insulin-dependent diabetic women. Can Med Assoc J 1982; 126: 487-490 [PMID: 7039797]
21 Lean ME, Pearson DW, Sutherland HW. Insulin manage-ment during labour and delivery in mothers with diabetes. Diabet Med 1990; 7: 162-164 [PMID: 2137758 DOI: 10.1111/j.1464-5491.1990.tb01352.x]
22 Lepercq J, Abbou H, Agostini C, Toubas F, Francoual C, Velho G, Dubois-Laforgue D, Timsit J. A standardized pro-tocol to achieve normoglycaemia during labour and delivery in women with type 1 diabetes. Diabetes Metab 2008; 34: 33-37 [PMID: 18069031 DOI: 10.1016/j.diabet.2007.08.003]
23 Caplan RH, Pagliara AS, Beguin EA, Smiley CA, Bina-Fry-mark M, Goettl KA, Hartigan JM, Tankersley JC, Peck TM. Constant intravenous insulin infusion during labor and de-livery in diabetes mellitus. Diabetes Care 1982; 5: 6-10 [PMID: 6754303 DOI: 10.2337/diacare.5.1.6]
24 Hawkins JS, Casey BM. Labor and delivery management for women with diabetes. Obstet Gynecol Clin North Am 2007; 34: 323-334, x [PMID: 17572275 DOI: 10.1016/j.ogc.2007.04.003]
25 ACE/ADA Task Force on Inpatient Diabetes. American College of Endocrinology and American Diabetes Associa-tion consensus statement on inpatient diabetes and glycemic control. Endocr Pract 2006; 12: 458-468 [PMID: 16983798]
26 Bowen DJ, Daykin AP, Nancekievill ML, Norman J. Insulin-dependent diabetic patients during surgery and labour. Use of continuous intravenous insulin-glucose-potassium infusions. Anaesthesia 1984; 39: 407-411 [PMID: 6375445 DOI: 10.1111/j.1365-2044.1984.tb07305.x]
27 Yeast JD, Porreco RP, Ginsberg HN. The use of continuous insulin infusion for the peripartum management of preg-nant diabetic women. Am J Obstet Gynecol 1978; 131: 861-864 [PMID: 686085]
28 Hadden DR. How to improve prognosis in type 1 diabetic pregnancy. Old problems, new concepts. Diabetes Care 1999; 22 Suppl 2: B104-B108 [PMID: 10097909]
29 Jovanovic L, Peterson CM. Insulin and glucose requirements during the first stage of labor in insulin-dependent diabetic women. Am J Med 1983; 75: 607-612 [PMID: 6353916 DOI: 10.1016/0002-9343(83)90441-2]
30 Clarke WL, Cox D, Gonder-Frederick LA, Carter W, Pohl SL. Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care 1987; 10: 622-628 [PMID: 3677983]
31 Klonoff DC. Continuous glucose monitoring: roadmap for 21st century diabetes therapy. Diabetes Care 2005; 28: 1231-1239 [PMID: 15855600 DOI: 10.2337/diacare.28.5.1231]
32 Abrahamian H, Francesconi M, Loiskandl A, Dzien A, Prag-er R, Weitgasser R. Evaluation of a new insulinotropic agent by using an innovative technology: efficacy and safety of nateglinide determined by continuous glucose monitoring. Diabetes Technol Ther 2004; 6: 31-37 [PMID: 15000767 DOI: 10.1089/152091504322783387]
33 Jefferies C, Solomon M, Perlman K, Sweezey N, Daneman D. Continuous glucose monitoring in adolescents with cystic fibrosis. J Pediatr 2005; 147: 396-398 [PMID: 16182684 DOI: 10.1016/j.jpeds.2005.05.004]
34 Brennan AL, Gyi KM, Wood DM, Hodson ME, Geddes DM, Baker EH. Relationship between glycosylated haemoglobin and mean plasma glucose concentration in cystic fibrosis. J Cyst Fibros 2006; 5: 27-31 [PMID: 16202666 DOI: 10.1016/j.jcf.2005.09.001]
35 Goldberg PA, Siegel MD, Russell RR, Sherwin RS, Halick-man JI, Cooper DA, Dziura JD, Inzucchi SE. Experience with the continuous glucose monitoring system in a medical in-tensive care unit. Diabetes Technol Ther 2004; 6: 339-347 [PMID: 15198837 DOI: 10.1089/152091504774198034]
45 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Harizopoulou VC et al . Intrapartum application of CGMS

36 Beardsall K, Ogilvy-Stuart AL, Ahluwalia J, Thompson M, Dunger DB. The continuous glucose monitoring sensor in neo-natal intensive care. Arch Dis Child Fetal Neonatal Ed 2005; 90: F307-F310 [PMID: 16036889 DOI: 10.1136/adc.2004.051979]
37 Chee F, Fernando TL, Savkin AV, van Heeden V. Expert PID control system for blood glucose control in critically ill pa-tients. IEEE Trans Inf Technol Biomed 2003; 7: 419-425 [PMID: 15000368 DOI: 10.1109/TITB.2003.821326]
38 Javid PJ, Halwick DR, Betit P, Thompson JE, Long K, Zhang Y, Jaksic T, Agus MS. The first use of live continuous glu-cose monitoring in patients on extracorporeal life support. Diabetes Technol Ther 2005; 7: 431-439 [PMID: 15929674 DOI: 10.1089/dia.2005.7.431]
39 Hershkovitz E, Rachmel A, Ben-Zaken H, Phillip M. Con-tinuous glucose monitoring in children with glycogen stor-age disease type I. J Inherit Metab Dis 2001; 24: 863-869 [PMID: 11916320 DOI: 10.1023/A:1013996325720]
40 Klonoff DC, Buckingham B, Christiansen JS, Montori VM, Tamborlane WV, Vigersky RA, Wolpert H. Continuous glucose monitoring: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2011; 96: 2968-2979 [PMID: 21976745 DOI: 10.1210/jc.2010-2756]
41 Yogev Y, Ben-Haroush A, Chen R, Kaplan B, Phillip M, Hod M. Continuous glucose monitoring for treatment adjust-ment in diabetic pregnancies--a pilot study. Diabet Med 2003; 20: 558-562 [PMID: 12823237 DOI: 10.1046/j.1464-5491.2003. 00959.x]
42 Yogev Y, Chen R, Ben-Haroush A, Phillip M, Jovanovic L, Hod M. Continuous glucose monitoring for the evaluation of gravid women with type 1 diabetes mellitus. Obstet Gyne-col 2003; 101: 633-638 [PMID: 12681863 DOI: 10.1016/S0029-7844(02)02714-X]
43 Chen R, Yogev Y, Ben-Haroush A, Jovanovic L, Hod M, Phillip M. Continuous glucose monitoring for the evalua-tion and improved control of gestational diabetes mellitus. J Matern Fetal Neonatal Med 2003; 14: 256-260 [PMID: 14738172 DOI: 10.1080/jmf.14.4.256.260]
44 Kestilä KK, Ekblad UU, Rönnemaa T. Continuous glu-cose monitoring versus self-monitoring of blood glucose in the treatment of gestational diabetes mellitus. Diabetes Res Clin Pract 2007; 77: 174-179 [PMID: 17234297 DOI: 10.1016/j.diabres.2006.12.012]
45 Huddleston JF, Cramer MK, Vroon DH. A rationale for omitting two-hour postprandial glucose determinations in gestational diabetes. Am J Obstet Gynecol 1993; 169: 257-262; discussion 262-264 [PMID: 8362934]
46 Moses RG, Lucas EM, Knights S. Gestational diabetes melli-tus. At what time should the postprandial glucose level be monitored? Aust N Z J Obstet Gynaecol 1999; 39: 457-460 [PMID: 10687763 DOI: 10.1111/j.1479-828X.1999.tb03132.x]
47 Leguizamón G, Krupitzki H, Glujovsky D, Olivera Ravasi M, Reece EA. Blood glucose monitoring in gestational dia-betes mellitus: 1- versus 2-h blood glucose determinations. J
Matern Fetal Neonatal Med 2002; 12: 384-388 [PMID: 12683648 DOI: 10.1080/jmf.12.6.384.388]
48 Sivan E, Weisz B, Homko CJ, Reece EA, Schiff E. One or two hours postprandial glucose measurements: are they the same? Am J Obstet Gynecol 2001; 185: 604-607 [PMID: 11568785 DOI: 10.1067/mob.2001.117184]
49 Ben-Haroush A, Yogev Y, Chen R, Rosenn B, Hod M, Langer O. The postprandial glucose profile in the diabetic pregnancy. Am J Obstet Gynecol 2004; 191: 576-581 [PMID: 15343240 DOI: 10.1016/j.ajog.2004.01.055]
50 Bühling KJ, Winkel T, Wolf C, Kurzidim B, Mahmoudi M, Wohlfarth K, Wäscher C, Schink T, Dudenhausen JW. Optimal timing for postprandial glucose measurement in pregnant women with diabetes and a non-diabetic pregnant population evaluated by the Continuous Glucose Monitor-ing System (CGMS). J Perinat Med 2005; 33: 125-131 [PMID: 15843262 DOI: 10.1515/JPM.2005.024]
51 Kerssen A, de Valk HW, Visser GH. Day-to-day glucose variability during pregnancy in women with Type 1 diabetes mellitus: glucose profiles measured with the Continuous Glucose Monitoring System. BJOG 2004; 111: 919-924 [PMID: 15327605 DOI: 10.1111/j.1471-0528.2004.00203.x]
52 Kerssen A, Evers IM, de Valk HW, Visser GH. Poor glucose control in women with type 1 diabetes mellitus and ‘safe’ hemoglobin A1c values in the first trimester of pregnancy. J Matern Fetal Neonatal Med 2003; 13: 309-313 [PMID: 12916680 DOI: 10.1080/jmf.13.5.309.313]
53 Kerssen A, de Valk HW, Visser GH. Forty-eight-hour first-trimester glucose profiles in women with type 1 diabetes mellitus: a report of three cases of congenital malforma-tion. Prenat Diagn 2006; 26: 123-127 [PMID: 16463292 DOI: 10.1002/pd.1340]
54 Yogev Y, Ben-Haroush A, Chen R, Rosenn B, Hod M, Langer O. Diurnal glycemic profile in obese and normal weight nondiabetic pregnant women. Am J Obstet Gynecol 2004; 191: 949-953 [PMID: 15467570 DOI: 10.1016/j.ajog.2004.06.059]
55 Stenninger E, Lindqvist A, Aman J, Ostlund I, Schvarcz E. Continuous Subcutaneous Glucose Monitoring System in diabetic mothers during labour and postnatal glucose adap-tation of their infants. Diabet Med 2008; 25: 450-454 [PMID: 18387079 DOI: 10.1111/j.1464-5491.2008.02416.x]
56 Iafusco D, Stoppoloni F, Salvia G, Vernetti G, Passaro P, Petro-vski G, Prisco F. Use of real time continuous glucose moni-toring and intravenous insulin in type 1 diabetic mothers to prevent respiratory distress and hypoglycaemia in infants. BMC Pregnancy Childbirth 2008; 8: 23 [PMID: 18593467 DOI: 10.1186/1471-2393-8-23]
57 Harizopoulou VC, Goulis DG, Vavilis DS, Grimbizis G, Tsakalis AV, Saranti ES, Tarlatzis BC. The intrapartum ap-plication of Continuous Glucose Monitoring System in preg-nancies complicated with diabetes. Proceedings of the 6th In-ternational Symposium on Diabetes and Pregnancy. Austria: Salzburg, 2011: 23-26
P- Reviewer Power RW S- Editor Zhai HH L- Editor Roemmele A E- Editor Zheng XM
46 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Harizopoulou VC et al . Intrapartum application of CGMS

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i3.47
World J Obstet Gynecol 2013 August 10; 2(3): 47-52ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Laparoscopic surgical repair of pelvic organ prolapse and female stress urinary incontinence
Panagiotis I Mourmouris, Andreas Skolarikos, Iraklis C Mitsogiannis, Vasileios Migdalis, Athanasios G Papatsoris
Panagiotis I Mourmouris, Andreas Skolarikos, Iraklis C Mitsogiannis, Athanasios G Papatsoris, 2nd Department of Urology, School of Medicine, University of Athens, Sismanoglio General Hospital, 14578 Athens, GreeceVasileios Migdalis, 1st Department of Urology, School of Medi-cine, University of Athens, Laiko General Hospital, 14578 Athens, GreeceAuthor contributions: Mourmouris PI, Skolarikos A, Mitsogi-annis IC, Migdalis V and Papatsoris AG contributed to this paper.Correspondence to: Dr. Athanasios G Papatsoris, 2nd De-partment of Urology, School of Medicine, University of Athens, Sismanoglio General Hospital, 1 Sismanogleiou Street, 14578 Athens, Greece. [email protected]: +30-210-8044703 Fax: +30-210-8044703Received: March 9, 2013 Revised: April 6, 2013Accepted: June 8, 2013Published online: August 10, 2013
AbstractPelvic organ prolapse (POP) occurs in a relatively big population of women which is continuously increasing and is associated with a variety of urinary bowel and sexual symptoms. As this problem magnifies, the need for surgical repair is increasing relatively. The main goals of surgical repair for POP include: no anatomic prolapse, no functional symptoms, patient satisfac-tion and avoidance of complications, goals that cannot always be fully achieved. The decision for the type of surgery depends of various factors such as patient characteristics and prolapsed compartment but also by the surgeon expertise. The laparoscopic approach is already the gold standard procedure for many urologic procedures and can also be used for the treatment of POP and stress urinary incontinence. Herein, we review the literature about the available data concerning lapa-roscopic surgery techniques for treating POP.
© 2013 Baishideng. All rights reserved.
Key words: Pelvic organ prolapse; Laparoscopic; Minimal invasive; Repair
Core tip: Laparoscopic approaches in urologic surgery have become over the years very popular. Novel lapa-roscopic expertise is continuously acquired in many different surgical fields such as pelvic organ prolapse (POP). We summarize the relevant literature upon the laparoscopic surgical repair of POP and female stress urinary incontinence.
Mourmouris PI, Skolarikos A, Mitsogiannis IC, Migdalis V, Papatsoris AG. Laparoscopic surgical repair of pelvic organ prolapse and female stress urinary incontinence. World J Obstet Gynecol 2013; 2(3): 47-52 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i3/47.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i3.47
INTRODUCTIONPelvic organ prolapse (POP) is defined as the descent of one or more of the following: anterior vaginal wall, pos-terior vaginal wall and apex of the vagina (cervix/uterus) or vault (cuff) after hysterectomy. Absence of prolapse is defined as POP stage 0, while POP can be staged from stage Ⅰ to stage Ⅳ. POP occurs in up to 50% of parous women and may be associated with a variety of urinary bowel and sexual symptoms[1]. The prevalence of POP is currently increasing and the lifetime risk of requiring surgery for POP is more than 10%[1]. The main goals of surgical repair for POP is to achieve no anatomic pro-lapse, no functional symptoms, patient satisfaction and avoidance of complications, goals that usually cannot be fully established[2]. The available surgical techniques in correlation with the relevant anatomical compartments are listed in Table 1.
Laparoscopic approach is the gold standard operation for many urological clinical entities. In POP the laparo-scopic approach has the advantage of allowing a very good view of the anterior and posterior compartments so that an overall approach for POP is possible by the
MINIREVIEW
47 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com

same surgical route[3]. There have been described over 100 different approaches for the repair of the POP. The decision for the type of surgery depends on the compart-ments that are affected and the patient characteristics. The laparoscopic approach for the surgical treatment of POP was introduced to treat the three compartment de-fects with the objectives of being less invasive than open surgery, of easier magnified access to the pelvis with less blood and shorter postoperative convalescence.
We performed a search at PubMed and Cochrane databases for articles concerning surgery repair of POP and laparoscopic approaches published between 1970 and 2013. We used as key words the terms: POP, laparo-scopic, minimal invasive techniques and robotic assisted laparoscopic techniques. We studied all the relevant ar-ticles and we analyzed the ones with the biggest series.
LAPAROSCOPIC RETROPUBIC SUSPENSIONLaparoscopic techniques for retropubic suspension were introduced by Vancaillie and Schuessler in 1991. They performed a Marshall Marchetti-Krantz urethropexy laparoscopically and since then laparoscopic techniques have been applied to both the Burch procedure and the paravaginal repair. Proposed advantages of the laparo-scopic approach include improved intraoperative visu-alization, less postoperative pain, shorter hospitalization and quicker recover times[4]. Disadvantages include great-er technical difficulty, longer operative times and higher operative costs[5]. The procedure may be performed extraperitoneally or transperitoneally and each approach has its proponents. Although extraperitoneal technique may be associated with shorter operating times, easier dissection and fewer bladder injuries[6] the transperitoneal approach provides a larger operating space and the ability to perform concomitant intraperitoneal procedures and apical prolapsed repair[5].
Paraiso et al[5] reviewed 13 studies of laparoscopic retropubic suspensions, reported success rates from 69% to 100% with follow up of 1 to 36 mo and these rates are comparable to the outcomes of open procedures. Both retrospective[7] and randomized prospective tri-als[8] between open and laparoscopic techniques have demonstrated similar short term success rates. However when following patients for a longer time, laparoscopic suspensions tend to fail in comparison with open surgery. McDougall et al[9] reported only 30% recovery of stress urinary incontinence (SUI) and 50% cure with a laparo-scopic Burch procedure after 45 mo of follow up.
Five trials summarized in a Cochrane review com-pared laparoscopic with open colposuspension[8,10-13]. Overall, there was a significantly higher success rate after open colposuspension (RR = 0.89; 95%CI: 0.82-0.98) equivalent to an absolute difference of an additional 9% risk of failure after laparoscopic surgery. No significant differences between the two groups were observed for
postoperative urgency, voiding dysfunction, or de novo detrusor overactivity. A trend was shown toward a higher complication rate, less postoperative pain, shorter hospi-tal stay, and more rapid return to normal function for lap-aroscopic colposuspension. The operating time tended to be longer, the intraoperative blood loss less, and the dura-tion of catheterization shorter for laparoscopic compared with open colposuspension. Carey et al[12] published a randomized trial upon 200 women during 1997 and 1998, with 2-year follow-up available for 83% of participants. The authors found no difference in urodynamic studies outcome, incidence of detrusor overactivity, or patient satisfaction at 6 mo, with an overall objective cure rate of 75%. Detrusor overactivity was recorded in 12% of the women. The overall satisfaction rate was 87%. At 24 mo after surgery there were no significant differences be-tween the two treatment groups with respect to reporting SUI, urgency, and urgency incontinence and a satisfaction score of greater than or equal to 80. Although follow-up information was only available on approximately 80% of all patients by 24 mo, a sensitivity analysis was per-formed assuming that all women who did not complete the 24-mo follow-up had either occasional or frequent SUI. With these assumptions, cure rates decreased to 61% for open colposuspension and 50% for laparoscopic colposuspension. There were no significant differences between the two treatment groups at 3 to 5 years after surgery. Mean operating time was approximately twice as long for laparoscopic colposuspension, but surgeon’s esti-mates of blood loss and patient’s estimates of immediate postoperative pain at rest were significantly less after the laparoscopic procedure with a return to normal activities, 5 d earlier (P = 0.01). Kitchener et al[14] also found no dif-ference in the objective cure rate (79% for laparoscopic vs 70% for open) or subjective cure rate (55% vs 54%) between the study arms. The intention-to-treat analysis indicated no significant difference in cure rates between open and laparoscopic surgery.
In a meta-analysis of all of the comparative stud-ies published between 1995 and 2006 of laparoscopic vs open colposuspension, 16 studies matched the selection criteria of 1807 patients, of whom 861 (47.6%) under-went laparoscopic and 946 (52.4%) underwent open colposuspension[15]. The length of hospital stay and re-turn to normal life were significantly reduced after lapa-roscopic surgery. These findings remained consistent on sensitivity analysis. Bladder injuries occurred more often in the laparoscopic group, but only with a marginal sta-tistical significance. Comparable bladder injury rates were found when studies were matched for quality, year, and randomized trials. Cure rates were similar between the two procedures at 2 years follow-up. Table 2 summarizes the available data in laparoscopic retropubic suspension.
The current evidence suggests that in adequately ex-perienced hands there is no difference in overall safety and efficacy between laparoscopic and open colposus-pension. Laparoscopic colposuspension shows compa-rable subjective outcome, but poorer objective outcome
48 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Mourmouris PI et al . Laparoscopic surgery repair of POP and female SUI

than both open colposuspension and tension-free vaginal tape procedure in the short to medium term follow.
LAPAROSCOPIC PROMONTOFIXATIONThe wide spectrum of open and laparoscopic surgical ap-proaches used to treat POP represented the complexity of managing this medical condition[16]. Irrespective of the route or repair chosen by the surgeon, a sound surgical judgment, complete understanding of the pelvic anatomy and the mechanisms involved in POP are required for a successful outcome[17].
Recently, Bacle et al[18] studied prospectively 501 con-secutive patients that underwent laparoscopic promon-tofixation (LP) for POP. They reported a 1.7% intra-operative compilations rate and after a mean follow up of 20.7 mo the complications rate was 17.8% and the recur-rence rate was 11.5%. Risk factors for recurrence were the prolypropylene mesh when compared with the polyester mesh (P < 0.0001), intra-operative hysterectomy (P = 0.02) and bleeding (P = 0.0049). The authors concluded in a statistically significant improvement in most of the symp-toms (P < 0.001). Ganatra et al[19] reviewed 11 laparoscopic studies that included 1197 patients and reported a 10% recurrence rate for POP. In this study the mean incidence of vaginal erosion was 2.7%. Sabbagh et al[20] performed a retrospective study of 186 consecutive women who un-derwent LP for POP. The median follow up was 60 mo with a success rate of 92.4%, complications rate up to 6% and satisfaction rate up to 91.1%.
Rivoire et al[21] performed LP in 138 patients with POP. The follow up was 33.7 mo with a recurrence rate at 11%, while 98% of patients were satisfied with the operation but the postoperative SUI rate was 46%. White
et al[22] in their study of 30 patients concluded that there was no significant difference with respect to the operative time, blood loss, pain score and duration of hospital-ization between laparoscopic and robotic assisted ap-proaches. They concluded that laparoscopic and robotic assisted sacral colpopexy offered comparable efficacy and superior cosmetic results compared to open approaches.
Recently, Maher et al[23] compared laparoscopic sacral colpopexy to total mesh placement for vaginal vault prolapsed. In this randomized study of 108 patients the laparoscopic group had a shorter hospitalization period and quicker return to work while the follow up of 2 years showed a 77% success rate at all vaginal site for laparo-scopic sacral colpopexy as compared with 43% for total vaginal mesh (P < 0.001). The re-operation rate was sig-nificantly higher after the vaginal mesh surgery (22%) as compared to the laparoscopic sacral colpopexy (5%) (P = 0.006). The authors concluded that laparoscopic sacral colpopexy provided higher success rates and lower peri-operative morbidity and re-operation rates in comparison with the total vaginal mesh procedure. The overview of the above results are summarized in Table 3.
LAPAROSCOPIC PLACEMENT OF THE ARTIFICIAL URINARY SPHINCTER FOR SUIThe first clinical report of laparoscopic transperitoneal artificial urinary sphincter (AUS) implantation in women was published by Ngninkeu et al[24]. In this study the authors reported their preliminary results (mean follow up 6 mo) of treating four women with SUI due intrin-sic sphincter deficiency (ISD) with implantation of the
49 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Table 1 Surgical repair of pelvic organ prolapse
Compartment Prolapsed organ Vaginal wall site Abdominal repair
Anterior Urethra Distal anterior vaginal wall Retropubic urethropexyAnterior Bladder (cystocele) Proximal and distal anterior vaginal wall Paravaginal repairMiddle Cervix Cervix Abdominal sacrocolpopexyMiddle Small bowel (enterocele) Ureterosacral scar Halban culdoplastyPosterior Small bowel AP (enterocele) Proximal posterior vaginal wall ColpoperineopexyPosterior RectumBp (rectocele) Proximal and distal posterior vaginal wall NAPosterior Perineal body Perineal Body NA
NA: Not available.
Table 2 Laparoscopic retropubic suspension overview
Ref. n Follow up (mo)
Objective cure rate (%)
Satisfaction rate (%)
Paraiso et al[5] 150 1-36 69-100 NAMcDougall et al[9] 45 30 NACarey et al[12] 200 24-60 50 87Kitchener et al[14] 291 24 79 NATan et al[15] 861 24 NA NA
NA: Not available.
Table 3 Laparoscopic promontofixation overview
Ref. n Mean follow up (mo)
Objective cure rate (%)
Recurrence rate (%)
Bacle et al[18] 501 20.7 NA 11.5Ganatra et al[19] 1197 24.6 NA 10Sabbagh et al[20] 186 60 92.4 NARivoire et al[21] 138 33.7 64 NAMaher et al[23] 108 24 77 5
NA: Not available.
Mourmouris PI et al . Laparoscopic surgery repair of POP and female SUI

AMS 800 AUS. The aim was to evaluate the efficacy and safety of the AMS 800 implanted by the transperitoneal laparoscopic approach. The primary inclusion criterion for this study was a negative Marshall test (urine leak-age on straining or coughing not corrected with vaginal elevation)[25]. Patients in whom bladder overactivity was diagnosed were excluded from the study. The age of the patients was 50 to 79 years old, while the same surgeon performed all the procedures. Three trocars were inserted into the left iliac fossa, at midline halfway between the umbilicus and the pubis and into the right iliac fossa. The first step was the anterior approach to the bladder followed by dissection of the periurethral fascia and of the bladder neck from the vagina. The next step was the placement of the cuff and the pump. Finally, the balloon was introduced at the left lateral space of the bladder. The connections were performed and the device was de-activated. The activation of the device took place after 6 to 8 wk. All the cases were successfully completed within 2-2.5 h except from one. The urethral catheter remained for 7 d, while in one patient the symptoms persisted and the AUS balloon was replaced. All the patients had functioning devices at the end of the study. None of the patients experienced any preoperative or postoperative complications.
Hoda et al[26] used an extraperitoneal laparoscopic ap-proach for the implantation of the AMS 800 sphincter in two women with high body mass index (BMI) and significant co-morbidities. The technique of the surgeon involved the placement of balloon trocars in the preperi-toneal space, complete mobilization of the bladder neck, placement of the cuff at the bladder neck, insertion from the same port of the AUS balloon and placement of the pump in a pocket in the right labia major. The urethral catheter remained 2 d but one patient after the catheter removal experienced urinary retention and for 1 wk he performed intermittent self catheterization. The mean operating time was 117 min and patients were discharged after 5-6 d. The activation of the AUS occurred 6 wk after surgery. One patient developed an abdominal wall hema-toma which resulted in protrusion of the tubes from the suprapubic incision and secondary healing. Nearly 5 to 8 mo postoperatively both patients were continent. The au-thors concluded that the laparoscopic AUS implantation is a feasible and safe method but in order to achieve optimal results a careful patient selection must occur.
Rouprêt et al[27] reported their preliminary results with the laparoscopic approach for AUS implantation in 12 women with SUI due to ISD. The inclusive criterion for this study was a negative Marshall test associated with a low urethral closure pressure. Nine cases underwent lapa-roscopic extraperitoneal implantation of AUS and three of them the transperitoneal approach. Three procedures were converted to open and one was abandoned. Eleven patients out of 12 had a history of an anti-incontinence surgery. The extraperitoneal approach was performed with two trocars placed medially to the anterior supe-rior iliac spines and one trocar placed at the midpoint
between the pubis and umbilicus. After identifying the bladder neck the surgeon entered the endopelvic fascia on both sides. The next step was the dissection of the bladder neck below the periurethral fascia and the cuff was positioned and pressurized. The balloon was intro-duced through the iliac fossa mini incision and placed at the right of the bladder and after that the pump was placed into the labia major. The last step was to make the connections and deactivate the device. The mean opera-tive time was 181 min with no significant blood loss. The mean hospital stay was 7 d. The AUS activation was done at a mean period of 40.6 d. During the mean follow up of 12 mo 11 patients had a functioning device and the SUI was resolved in 10 patients. The remaining woman improved, but had a persistent degree of SUI (1 pad/d). Urinary retention occurred in 5 out of 12 patients (45%) and in 3 patients the authors encountered intra-operative injuries (25%). No postoperative erosion or device mal-functions during the follow up. The authors concluded that the laparoscopic implantation of AUS in women ap-peared to be technically feasible and that the results were promising.
Recently, Mandron et al[28] published the results in 25 patients that underwent laparoscopic implantation of AUS for SUI with ISD. This study is the largest in terms of patients (25 patients) and follow up (26.1 mo). The mean BMI was 26.8 and all patients had a negative Mar-shall test. All patients had a history of anti-incontinence and or pelvic surgery. All operations started with the placement of one 10 mm trocar for the laparoscope fol-lowed by a 10 mm trocar midway between the umbilicus and the pubic symphysis, and two 5 mm trocars 2 cm medially to each superior iliac crest. The next step was the incision of the peritoneum and the dissection of the lateral attachments of the bladder neck. Next were the dissection of the urethra from the vaginal wall and the placement of the AUS measuring tape and cuff. After the placement of the cuff around the urethra the AUS bal-loon reservoir with the relevant volume of fluid was in-serted. Finally, after progressive dilatation (up to 14 F) the AUS control pump was pocketed in the major labia and after the connection were made and placed in the Retzius place, the device was deactivated. The authors significant-ly reduced the operative time (mean 92 min) and hospital stay (mean 4 d). The urethral catheter remained for 2 d and the success rate (92%) was comparable to the open AUS implantation. There were no perioperative compli-cations except for one vaginal perforation which was re-paired during the operation in two layers with absorbable sutures. The device was activated 6 wk after the surgery. Five out of 25 patients (20%) developed urinary reten-tion and after surgery four patients were diagnosed with a urinary tract infection. Vaginal erosion was diagnosed in two patients during the first appointment. There was no need for blood transfusion. Out of 25 patients, 23 reported continence and functional devices, 19 of which had no need for pads per day and 4 needed 1 pad/d.
The results of the above mentioned studies upon the
50 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Mourmouris PI et al . Laparoscopic surgery repair of POP and female SUI

laparoscopic implantation of the AUS are summarized in Table 4.
LAPAROSCOPIC AND ROBOTIC ASSISTED LAPAROSCOPIC SACROCOLPOPEXYSince sacral colpopexy is considered to be the most ef-fective operation for the treatment of vaginal vault pro-lapse it was inevitable that laparoscopic approach would be attempted in order to minimize morbidity and reach higher cure rates. The largest series on this approach was reported by Stepanian et al[29] who studied 446 patients. They formed 2 groups, one with patients undergoing concominant hysterectomy and one with history of hys-terectomy. The risk for mesh related complications was 1, while no differences were found between the two groups. The median follow up was 12 mo. Although the study was the largest in this type of procedure it was a cohort study that used questionnaires and chart reviews[29].
Robotic assisted laparoscopic procedures for the treat-ment of POP are relatively novel procedures. Although this type of procedure is performed transabdominally with increased morbidity compared with the vaginal re-pairs the complication and recurrence rates are low. Elliott et al[30] reported low complication rates and only one pa-tient with recurrent grade 3 rectocele but the mean follow up was relatively short (5 mo). Di Marco et al[31] followed 5 patients for 4 mo and found no relapse in any of the 3 compartments and no complications except one patient that experienced vaginal bleeding. They concluded that robotic assisted techniques may provide the same long term durability with open sacroclpopexy[31]. The need for largest randomized studies is important in order to reach safe results.
CONCLUSIONLaparoscopic surgical repair of POP is safe and efficient and it can be used from surgeons that are familiar with the anatomy of the pelvic floor. Many different laparoscopic techniques have been published with relatively good re-sults that are equal with open surgery. However, the num-ber of patients is these studies are still small and better studies with bigger number of patients are warranted.
REFERENCES1 Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S.
Surgical management of pelvic organ prolapse in women: a short version Cochrane review. Neurourol Urodyn 2008; 27: 3-12 [PMID: 18092333 DOI: 10.1002/nau.20542]
2 Lee U, Raz S. Emerging concepts for pelvic organ prolapse surgery: What is cure? Curr Urol Rep 2011; 12: 62-67 [PMID: 21140299 DOI: 10.1007/s11934-010-0160-2]
3 Wattiez A, Canis M, Mage G, Pouly JL, Bruhat MA. Promontofix-ation for the treatment of prolapse. Urol Clin North Am 2001; 28: 151-157 [PMID: 11277060 DOI: 10.1016/S0094-0143(01)80017-3]
4 Liu CY. Laparoscopic retropubic colposuspension (Burch procedure). A review of 58 cases. J Reprod Med 1993; 38: 526-530 [PMID: 8410846]
5 Paraiso MF, Falcone T, Walters MD. Laparoscopic surgery for enterocele, vaginal apex prolapse and rectocele. Int Urogynecol J Pelvic Floor Dysfunct 1999; 10: 223-229 [PMID: 10450821]
6 Frankel G, Kantipong M. Sixteen-month experience with video-assisted extraperitoneal laparoscopic bladder neck suspension. J Endourol 1995; 9: 259-264 [PMID: 7550270 DOI: 10.1089/end.1995.9.259]
7 Polascik TJ, Moore RG, Rosenberg MT, Kavoussi LR. Com-parison of laparoscopic and open retropubic urethropexy for treatment of stress urinary incontinence. Urology 1995; 45: 647-652 [PMID: 7716846 DOI: 10.1016/S0090-4295(99)80057-0]
8 Summitt RL. Laparoscopic-assisted vaginal hysterectomy: a review of usefulness and outcomes. Clin Obstet Gynecol 2000; 43: 584-593 [PMID: 10949761 DOI: 10.1097/00003081-200009000-00019]
9 McDougall EM, Heidorn CA, Portis AJ, Klutke CG. Lapa-roscopic bladder neck suspension fails the test of time. J Urol 1999; 162: 2078-2081 [PMID: 10569574 DOI: 10.1016/S0022-5347(05)68105-0]
10 Burton G. A three year prospectiverandomized urodynam-icstudy comparing open and laparoscopic colposuspension [Abstract]. Neurourol Urodyn 1997; 16: 353-354
11 Su TH, Wang KG, Hsu CY, Wei HJ, Hong BK. Prospective comparison of laparoscopic and traditional colposuspensions in the treatment of genuine stress incontinence. Acta Obstet Gynecol Scand 1997; 76: 576-582 [PMID: 9246967 DOI: 10.3109/00016349709024588]
12 Carey M, Rosamilia A, Maher C, Cornish A, Murray C, Ugo-ni A, Fynes M, Dwyer P. Laparoscopic versus open colposus-pension: a prospective multicentre randomised single-blind comparison [Abstract]. Neurourol Urodyn 2000; 19: 389-391
13 Fatthy H, El Hao M, Samaha I, Abdallah K. Modified Burch colposuspension: laparoscopy versus laparotomy. J Am Assoc Gynecol Laparosc 2001; 8: 99-106 [PMID: 11172123 DOI: 10.1016/S1074-3804(05)60557-9]
14 Kitchener HC, Dunn G, Lawton V, Reid F, Nelson L, Smith AR. Laparoscopic versus open colposuspension--results of a pro-spective randomised controlled trial. BJOG 2006; 113: 1007-1013 [PMID: 16956332 DOI: 10.1111/j.1471-0528.2006.01035.x]
15 Tan E, Tekkis PP, Cornish J, Teoh TG, Darzi AW, Khullar V. Laparoscopic versus open colposuspension for urodynamic stress incontinence. Neurourol Urodyn 2007; 26: 158-169 [PMID: 17252603 DOI: 10.1002/nau.20398]
16 McIntyre M, Goudelocke C, Rovner ES. An update on surgery for pelvic organ prolapse. Curr Opin Urol 2010; 20: 490-494 [PMID: 20827209 DOI: 10.1097/MOU.0b013e32833e4c94]
17 Dorsey JH, Sharp HT. Laparoscopic sacral colpopexy and oth-er procedures for prolapse. Baillieres Clin Obstet Gynaecol 1995; 9: 749-756 [PMID: 8821252 DOI: 10.1016/S0950-3552(05)80396-7]
18 Bacle J, Papatsoris AG, Bigot P, Azzouzi AR, Brychaet PE, Piussan J, Mandron E. Laparoscopic promontofixation for pelvic organ prolapse: a 10-year single center experience in a series of 501 patients. Int J Urol 2011; 18: 821-826 [PMID: 21917023]
19 Ganatra AM, Rozet F, Sanchez-Salas R, Barret E, Galiano M, Cathelineau X, Vallancien G. The current status of laparo-scopic sacrocolpopexy: a review. Eur Urol 2009; 55: 1089-1103 [PMID: 19201521 DOI: 10.1016/j.eururo.2009.01.048]
51 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Table 4 Results of the studies upon laparoscopic implantation of the artificial urinary sphincter
Ref. n Mean follow up
(mo)
Success rate (%)
Operative duration (min)
Hospital stay (d)
Ngninkeu et al[24] 4 6 80 150 8Hoda et al[26] 2 6 100 120 6Rouprêt et al[27] 12 12.1 88 180 7Mandron et al[28] 25 26.1 92 92 4
Mourmouris PI et al . Laparoscopic surgery repair of POP and female SUI

20 Sabbagh R, Mandron E, Piussan J, Brychaert PE, Tu le M. Long-term anatomical and functional results of laparoscopic promontofixation for pelvic organ prolapse. BJU Int 2010; 106: 861-866 [PMID: 20089111 DOI: 10.1111/j.1464-410X.2009.09173.x]
21 Rivoire C, Botchorishvili R, Canis M, Jardon K, Rabischong B, Wattiez A, Mage G. Complete laparoscopic treatment of genital prolapse with meshes including vaginal promonto-fixation and anterior repair: a series of 138 patients. J Minim Invasive Gynecol 2007; 14: 712-718 [PMID: 17980331 DOI: 10.1016/j.jmig.2007.06.017]
22 White WM, Goel RK, Swartz MA, Moore C, Rackley RR, Kaouk JH. Single-port laparoscopic abdominal sacral col-popexy: initial experience and comparative outcomes. Urology 2009; 74: 1008-1012 [PMID: 19716594 DOI: 10.1016/j.urology.2009.02.086]
23 Maher CF, Feiner B, DeCuyper EM, Nichlos CJ, Hickey KV, O’Rourke P. Laparoscopic sacral colpopexy versus total vag-inal mesh for vaginal vault prolapse: a randomized trial. Am J Obstet Gynecol 2011; 204: 360.e1-360.e7 [PMID: 21306698]
24 Ngninkeu BN, van Heugen G, di Gregorio M, Debie B, Ev-ans A. Laparoscopic artificial urinary sphincter in women for type III incontinence: preliminary results. Eur Urol 2005; 47: 793-797; discussion 797 [PMID: 15925075 DOI: 10.1016/j.eururo.2005.01.010]
25 Costa P, Mottet N, Rabut B, Thuret R, Ben Naoum K, Wag-ner L. The use of an artificial urinary sphincter in women with type III incontinence and a negative Marshall test. J Urol 2001; 165: 1172-1176 [PMID: 11257664 DOI: 10.1016/S0022-5347(05)66459-2]
26 Hoda MR, Gauruder-Burmester A, Kümmel C, Nitzke T, Popken G. [Management of female stress urinary inconti-nence. Endoscopic extraperitoneal artificial urinary sphinc-ter--early experience]. Urologe A 2008; 47: 1004-1008 [PMID: 18461299 DOI: 10.1007/s00120-008-1739-9]
27 Rouprêt M, Misraï V, Vaessen C, Cardot V, Cour F, Richard F, Chartier-Kastler E. Laparoscopic approach for artificial urinary sphincter implantation in women with intrinsic sphincter deficiency incontinence: a single-centre prelimi-nary experience. Eur Urol 2010; 57: 499-504 [PMID: 19346059 DOI: 10.1016/j.eururo.2009.03.045]
28 Mandron E, Bryckaert PE, Papatsoris AG. Laparoscopic artificial urinary sphincter implantation for female genuine stress urinary incontinence: technique and 4-year experience in 25 patients. BJU Int 2010; 106: 1194-1198; discussion 1198 [PMID: 20132197]
29 Stepanian AA, Miklos JR, Moore RD, Mattox TF. Risk of mesh extrusion and other mesh-related complications after laparoscopic sacral colpopexy with or without concurrent laparoscopic-assisted vaginal hysterectomy: experience of 402 patients. J Minim Invasive Gynecol 2008; 15: 188-196 [PMID: 18312989 DOI: 10.1016/j.jmig.2007.11.006]
30 Elliott DS, Krambeck AE, Chow GK. Long-term results of robotic assisted laparoscopic sacrocolpopexy for the treat-ment of high grade vaginal vault prolapse. J Urol 2006; 176: 655-659 [PMID: 16813916 DOI: 10.1016/j.juro.2006.03.040]
31 Di Marco DS, Chow GK, Gettman MT, Elliott DS. Robotic-assisted laparoscopic sacrocolpopexy for treatment of vaginal vault prolapse. Urology 2004; 63: 373-376 [PMID: 14972496 DOI: 10.1016/j.urology.2003.09.03329]
P- Reviewers D Moore R, Sacco E, Wang PH S- Editor Wang JL L- Editor A E- Editor Zheng XM
52 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Mourmouris PI et al . Laparoscopic surgery repair of POP and female SUI
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i3.53
World J Obstet Gynecol 2013 August 10; 2(3): 53-61ISSN 2218-6220 (online)
© 2013 Baishideng. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Smoking and genital human papilloma virus infection in women attending cervical cancer screening in Greece
Kimon Chatzistamatiou, Taxiarchis Katsamagas, Menelaos Zafrakas, Konstantia Zachou, Anastasia Orologa, Fani Fitsiou, Thomas Theodoridis, Theocharis Konstantinidis, Theodoros C Konstantinidis, Theodoros Agorastos
Kimon Chatzistamatiou, Taxiarchis Katsamagas, Theodoros Agorastos, 4th Department of Obstetrics and Gynecology, Hip-pokrateio Hospital, Aristotle University of Thessaloniki, 54642 Thessaloniki, GreeceMenelaos Zafrakas, School of Health and Medical Care, Alex-ander Technological Educational Institute of Thessaloniki, 55134 Thessaloniki, GreeceKonstantia Zachou, Anastasia Orologa, Fani Fitsiou, Labo-ratory of Cytology, Hippokrateio Hospital, 54642 Thessaloniki, GreeceThomas Theodoridis, Center for Family Planning, Hippokrateio Hospital, 54642 Thessaloniki, GreeceTheocharis Konstantinidis, Peripheral Laboratory of Public Health, Hellenic Center for Disease Control and Prevention, Min-istry of Health, 68100 Alexandroupoli, GreeceTheodoros C Konstantinidis, Laboratory of Hygiene and Envi-ronmental Protection and Laboratory of Microbiology, Democri-tus University of Thrace, 68100 Alexandroupoli, GreeceAuthor contributions: Agorastos T conceived and co-ordinated the study; Chatzistamatiou K drafted the manuscript; Zafrakas M, Konstantinidis TC and Agorastos T revised the manuscript criti-cally for important intellectual content; all authors contributed in data acquisition, analysis and interpretation, as well as in drafting the article; all authors have read and approved the final version of the manuscript.Correspondence to: Menelaos Zafrakas, Associate Profes-sor of Obstetrics and Gynecology, School of Health and Medical Care, Alexander Technological Educational Institute of Thessa-loniki, Ethnikis Antistaseos 81, 55134 Thessaloniki, Greece. [email protected]: +30-2310-222792 Fax: +30-2310-222498Received: March 20, 2013 Revised: April 9, 2013Accepted: May 16, 2013Published online: August 10, 2013
AbstractAIM: To investigate whether smoking is associated with human papilloma virus (HPV) infection.
METHODS: HPV infection is considered to be a neces-
sary condition for cervical cancer development. The study population included 1291 women, aged 25-55 years, attending cervical cancer screening. All women had a Pa-panicolaou (Pap) test, with liquid-based cytology (Thin-prep®), an HPV-DNA test and an evaluation of smoking habits. The COBAS® 4800 system was used for HPV-DNA testing, enabling identification of the following high-risk HPV (hrHPV)-types: each of HPVs 16 and 18 separately, and HPVs 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68 as a cocktail. The evaluation of smoking habits was assessed using the smoking intensity index (SII), a vari-able formed as the product of cigarettes consumed per day by the days (years × 365) that a woman was a smoker, divided by 1000.
RESULTS: There were 136 smokers among 238 women tested positive for hrHPV-types (HPVs 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and/or 68), and 463 smokers among 1053 hrHPV-negative women (OR = 1.7, P < 0.001). This association was attributed to the youngest age group of women, aged 25-34 years (OR = 2.3, P < 0.001), while there was no association in other age groups. The intensity of smoking (increasing SII) showed no statistically significant association with hrH-PV infection. Cervical infection with HPV 16 and/or HPV 18 was also not associated with age or smoking habits. Finally, no association was found between Pap test sta-tus and smoking habits or smoking intensity.
CONCLUSION: Smoking appears to be associated with hrHPV infection of the uterine cervix, particularly in younger women. Further studies should investigate whether this association is based on causality and eval-uate the role of other possible co-factors.
© 2013 Baishideng. All rights reserved.
Key words: Human papilloma virus; High-risk human papilloma virus; Human papilloma virus-DNA test; Smok-ing; Cervical cancer; Screening
BRIEF ARTICLE
53 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com

Core tip: Human papilloma virus (HPV) infection is a prerequisite for cervical cancer development. We in-vestigated whether smoking can influence the course of HPV infection, in 1291 women attending cervical cancer screening. Smoking appeared to be associated with high-risk HPV (hrHPV) infection of the uterine cer-vix, particularly in younger women, aged 25-34 years. In addition, women in this younger age group with a negative Pap test were more likely to have hrHPV infec-tion if they were smokers than if they did not smoke. Further studies should investigate whether this associa-tion is based on causality and evaluate the role of other possible co-factors.
Chatzistamatiou K, Katsamagas T, Zafrakas M, Zachou K, Orologa A, Fitsiou F, Theodoridis T, Konstantinidis T, Konstantinidis TC, Agorastos T. Smoking and genital human papilloma virus infec-tion in women attending cervical cancer screening in Greece. World J Obstet Gynecol 2013; 2(3): 53-61 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i3/53.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i3.53
INTRODUCTIONGenital infection by human papilloma virus (HPV) is con-sidered to be a sine qua non condition for development of cervical cancer[1]. In general, HPVs are divided into two groups, according to their oncogenic potential: The first group consists of the so-called low-risk and the second of the high-risk HPV (hrHPV)-types. Specific types of hrHPV can cause cervical cancer, and more than 95% of cervical cancer biopsies contain DNA from hrHPV genomes[2].
There are, however, certain other factors that may influ-ence the probability of hrHPV infection or accelerate the carcinogenic processes leading to cervical cancer[3]. Trans-mission of HPV between sexual partners is influenced by the age of a woman and her partner, the number of sexual partners, the age at first sexual intercourse, use of barrier contraceptive methods, co-infections, male sexual behaviour, and male circumcision[4]. In some studies how-ever, age at first sexual intercourse was not identified as an independent risk factor in multivariate analysis[5-7]. Other factors that have similar impact on disease progression include high parity, long-term oral contraceptive use, and smoking[8-10].
Many studies have shown that cigarette and tobacco smoking in general have a moderate and statistically sig-nificant association with cervical cancer and cervical in-traepithelial neoplasia (CIN)[10-19], although the latter is not supported by other studies[20]. In detail, Syrjänen et al[20], by using multivariate analysis, found that cigarette smok-ing was not an independent risk factor for CIN2 or more advanced lesions; however, there is evidence that suggests a potential role of passive smoking on invasive cervical cancer[21,22]. There is also evidence suggesting an associa-tion between smoking and an increased risk of high grade vaginal intraepithelial neoplasia (high grade VAIN)[23].
It is not quite clear though, if tobacco smoking, apart from increasing the risk for invasive cervical cancer and its precursors, may also influence HPV infection, particu-larly persistent HPV infection. Recent research focusing on the possible association between tobacco smoking and HPV infection has shown a positive association in women[18,24,25], as well as in men[26]. In the present study, this possible association has been investigated in an ur-ban population of women participating in cervical cancer screening in Greece.
MATERIALS AND METHODSParticipants and specimen collectionWomen attending cervical cancer screening in two outpa-tient clinics of the Hippokrateio Hospital in Thessaloniki, Greece, were recruited for the present study, as well as for an ongoing multi-center study dealing with screening for cervical cancer based on hrHPV-DNA detection as primary test, using the Cobas® 4800 HPV Test. In total, 1291 women were recruited for the present study be-tween August 2011 and January 2013. Participants were 25-55 years old, living in the urban area of Thessaloniki. The following exclusion criteria were used: pregnancy, treatment for CIN during the previous 5 years, history of hysterectomy, and use of conventional cytology.
Every woman was informed about all aspects and the rationale of the study, and signed a consent-form in order to participate. After recruitment, women answered certain questions about their smoking habits; if they smoked, and if yes, how many cigarettes per day and for how many years. According to this information, the num-ber of cigarettes per day, multiplied by years of smoking [n (cig/d) × 365 × n (years) divided by 1000] was cal-culated, creating a new variable, the smoking intensity index (SII), by which the sample was stratified. Following completion of the questionnaire, all women were exam-ined by a specially trained healthcare professional (either a gynecologist or a midwife), who took cell samples from both the ecto- and the endocervix, using the Cervex brush® (Rovers® Medical Devices, B.V. Oss, The Nether-lands). Brushes were inserted in Thinprep® vials contain-ing PreservCyt® Solution (Hologic, Inc, Marlborough, MA, United States), and were discarded after handling according to the instructions of the manufacturer.
CytologyPapanicolaou (Pap) smears were prepared using the Thinprep® liquid-based methodology, as previously de-scribed[27] and examined by a specially trained cytologist. The cytological assessment was performed according to the Bethesda 2001 classification[28]. The remaining liquid sample was then sent to the Peripheral Laboratory of Public Health of the Hellenic Center for Disease Control and Prevention and Laboratory of Hygiene and Envi-ronmental Protection/Laboratory of Microbiology of the Democritus University of Thrace in Alexandroupoli, Greece, where it was tested for HPV-DNA, using the
54 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Chatzistamatiou K et al . Smoking and genital HPV infection
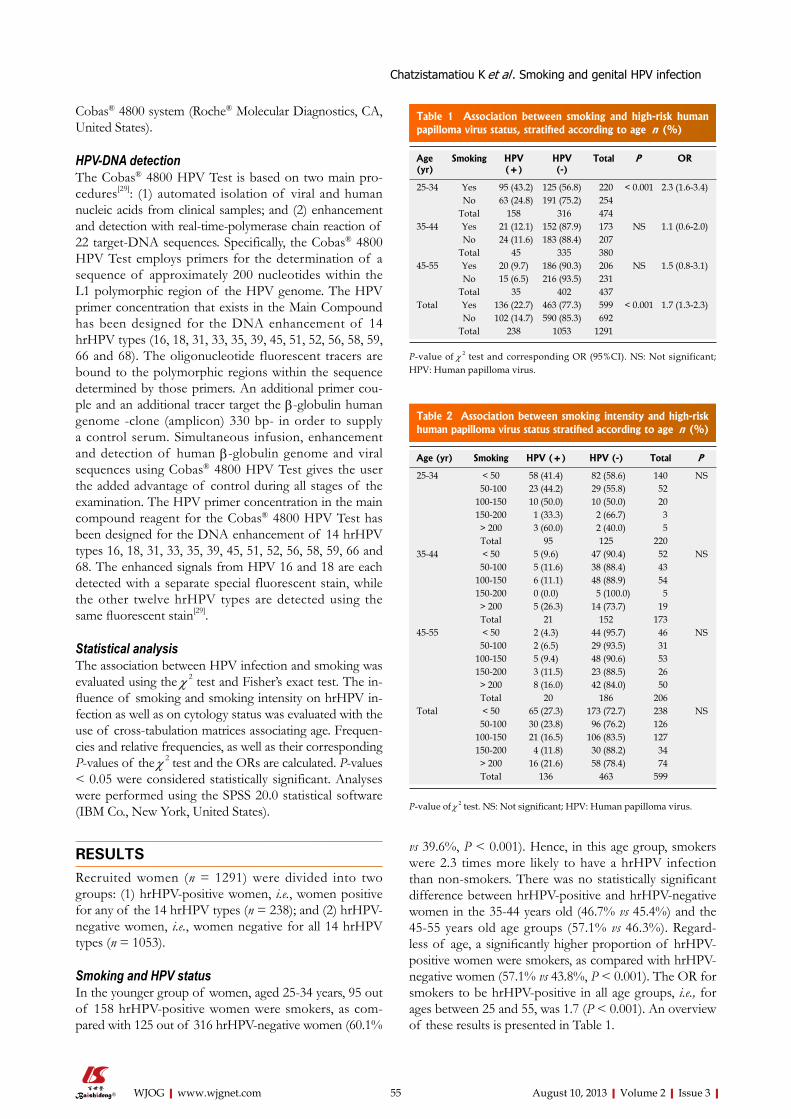
Cobas® 4800 system (Roche® Molecular Diagnostics, CA, United States).
HPV-DNA detection The Cobas® 4800 HPV Test is based on two main pro-cedures[29]: (1) automated isolation of viral and human nucleic acids from clinical samples; and (2) enhancement and detection with real-time-polymerase chain reaction of 22 target-DNA sequences. Specifically, the Cobas® 4800 HPV Test employs primers for the determination of a sequence of approximately 200 nucleotides within the L1 polymorphic region of the HPV genome. The HPV primer concentration that exists in the Main Compound has been designed for the DNA enhancement of 14 hrHPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68). The oligonucleotide fluorescent tracers are bound to the polymorphic regions within the sequence determined by those primers. An additional primer cou-ple and an additional tracer target the β-globulin human genome -clone (amplicon) 330 bp- in order to supply a control serum. Simultaneous infusion, enhancement and detection of human β-globulin genome and viral sequences using Cobas® 4800 HPV Test gives the user the added advantage of control during all stages of the examination. The HPV primer concentration in the main compound reagent for the Cobas® 4800 HPV Test has been designed for the DNA enhancement of 14 hrHPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68. The enhanced signals from HPV 16 and 18 are each detected with a separate special fluorescent stain, while the other twelve hrHPV types are detected using the same fluorescent stain[29].
Statistical analysisThe association between HPV infection and smoking was evaluated using the χ 2 test and Fisher’s exact test. The in-fluence of smoking and smoking intensity on hrHPV in-fection as well as on cytology status was evaluated with the use of cross-tabulation matrices associating age. Frequen-cies and relative frequencies, as well as their corresponding P-values of the χ 2 test and the ORs are calculated. P-values < 0.05 were considered statistically significant. Analyses were performed using the SPSS 20.0 statistical software (IBM Co., New York, United States).
RESULTSRecruited women (n = 1291) were divided into two groups: (1) hrHPV-positive women, i.e., women positive for any of the 14 hrHPV types (n = 238); and (2) hrHPV-negative women, i.e., women negative for all 14 hrHPV types (n = 1053).
Smoking and HPV status In the younger group of women, aged 25-34 years, 95 out of 158 hrHPV-positive women were smokers, as com-pared with 125 out of 316 hrHPV-negative women (60.1%
vs 39.6%, P < 0.001). Hence, in this age group, smokers were 2.3 times more likely to have a hrHPV infection than non-smokers. There was no statistically significant difference between hrHPV-positive and hrHPV-negative women in the 35-44 years old (46.7% vs 45.4%) and the 45-55 years old age groups (57.1% vs 46.3%). Regard-less of age, a significantly higher proportion of hrHPV-positive women were smokers, as compared with hrHPV-negative women (57.1% vs 43.8%, P < 0.001). The OR for smokers to be hrHPV-positive in all age groups, i.e., for ages between 25 and 55, was 1.7 (P < 0.001). An overview of these results is presented in Table 1.
55 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Table 1 Association between smoking and high-risk human papilloma virus status, stratified according to age n (%)
Age (yr)
Smoking HPV (+)
HPV (-)
Total P OR
25-34 Yes 95 (43.2) 125 (56.8) 220 < 0.001 2.3 (1.6-3.4)No 63 (24.8) 191 (75.2) 254
Total 158 316 47435-44 Yes 21 (12.1) 152 (87.9) 173 NS 1.1 (0.6-2.0)
No 24 (11.6) 183 (88.4) 207Total 45 335 380
45-55 Yes 20 (9.7) 186 (90.3) 206 NS 1.5 (0.8-3.1)No 15 (6.5) 216 (93.5) 231
Total 35 402 437Total Yes 136 (22.7) 463 (77.3) 599 < 0.001 1.7 (1.3-2.3)
No 102 (14.7) 590 (85.3) 692Total 238 1053 1291
P-value of χ 2 test and corresponding OR (95%CI). NS: Not significant; HPV: Human papilloma virus.
Table 2 Association between smoking intensity and high-risk human papilloma virus status stratified according to age n (%)
Age (yr) Smoking HPV (+) HPV (-) Total P
25-34 < 50 58 (41.4) 82 (58.6) 140 NS 50-100 23 (44.2) 29 (55.8) 52100-150 10 (50.0) 10 (50.0) 20150-200 1 (33.3) 2 (66.7) 3> 200 3 (60.0) 2 (40.0) 5Total 95 125 220
35-44 < 50 5 (9.6) 47 (90.4) 52 NS 50-100 5 (11.6) 38 (88.4) 43100-150 6 (11.1) 48 (88.9) 54150-200 0 (0.0) 5 (100.0) 5> 200 5 (26.3) 14 (73.7) 19Total 21 152 173
45-55 < 50 2 (4.3) 44 (95.7) 46 NS 50-100 2 (6.5) 29 (93.5) 31100-150 5 (9.4) 48 (90.6) 53150-200 3 (11.5) 23 (88.5) 26> 200 8 (16.0) 42 (84.0) 50Total 20 186 206
Total < 50 65 (27.3) 173 (72.7) 238 NS 50-100 30 (23.8) 96 (76.2) 126100-150 21 (16.5) 106 (83.5) 127150-200 4 (11.8) 30 (88.2) 34> 200 16 (21.6) 58 (78.4) 74Total 136 463 599
P-value of χ 2 test. NS: Not significant; HPV: Human papilloma virus.
Chatzistamatiou K et al . Smoking and genital HPV infection

No association was found between smoking intensity and hrHPV status. These results are presented in detail in Table 2. Figure 1 shows an overview of hrHPV-positive women stratified according to age and smoking intensity. The latter is defined according to the calculated smoking intensity index (SII = cigarettes/d × 365 × years of smok-ing divided by 1000), and a woman is classified as non-smoker if she had never smoked or if she had stopped smoking at least 1 year earlier. Smokers were classified into one of the following categories according to the previously described variable: SII < 50, if she had smoked less than 50000 cigarettes during her life as a smoker, SII = 50-100, if she had smoked between 50000 and 100000 cigarettes, SII = 100-150 if she had smoked between 100000 and 150000 cigarettes, SII = 150-200 if she had smoked be-tween 150000 and 200000 cigarettes, and SII > 200 if she had smoked more than 200000 cigarettes.
There was no statistically significant association be-tween smoking habits (i.e., smokers vs non-smokers) or smoking intensity (increasing SII) and infection from HPV types 16 or 18 in any age group. Table 3 show an overview
of the association between smoking and HPV-16 and HPV-18 status, respectively, stratified according to age.
Smoking and cervical cytology resultsRegarding cervical cytology results, women were divided into two groups: (1) Women with a negative (normal) Pap-smear (n = 1246); and (2) women with abnormal Pap smear [atypical squamous cells of uncertain significance (ASCUS) or worse] (n = 45). Comparisons according to smoking habits (smokers vs non smokers) or smoking intensity between women with normal and women with abnormal cytology results, using the χ 2 test, did not show any statistically significant differences between different age groups (data not shown).
Smoking, HPV status and cervical cytology resultsComparisons according to smoking habits between the two groups of women regarding cervical cytology and the two groups regarding hrHPV status showed that women with a negative Pap test were more likely to have hrHPV infection if they were smokers than if they did
56 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
100.0
80.0
60.0
40.0
20.0
0.0
HPV HR negativeHPV HR positive
%
SII 25-34 SII 25-34 SII 25-34
P < 0.001 P = NS P = NS
0 > 50
50-100
100-150
150-200
> 200
0 > 50
50-100
100-150
150-200
> 200
0 > 50
50-100
100-150
150-200
> 200
Figure 1 Stratification of human papilloma virus-positive and human papilloma virus-negative women according to age and smoking intensity. There was no statistically significant association between smoking intensity and (h) human papilloma virus (HPV) status. SII: Smoking intensity index. HR: High risk; NS: Not sig-nificant.
Age (yr) Smoking HPV-16 HPV-18
(+) (-) Total P OR (+) (-) Total P OR
25-34 Yes 24 (10.9) 196 (89.1) 220 NS 1.5 (0.8-2.8) 8 (3.6) 212 (96.4) 220 NS 1.3 (0.5-3.7)No 19 (7.5) 235 (92.5) 254 7 (2.8) 247 (97.2) 254
Total 43 431 474 15 459 47435-44 Yes 4 (2.3) 169 (97.7) 173 NS 0.8 (0.2-2.9) 1 (0.6) 172 (99.4) 173 NS 0.4 (0.1-3.8)
No 6 (2.9) 201 (97.1) 207 3 (1.4) 204 (98.6) 207Total 10 370 380 4 376 380
45-55 Yes - 206 (100) 206 - - 206 (100.0) 206No - 231 (100) 231 - 231 (100.0) 231
Total 437 437 - 437 437Total Yes 28 (4.7) 571 (95.3) 599 NS 1.3 (0.8-2.3) 9 (1.5) 590 (98.5) 599 NS 1.0 (0.4-2.6)
No 25 (3.6) 667 (96.4) 692 10 (1.4) 682 (98.6) 692Total 53 1238 1291 19 (1.5) 1272 (98.5) 1291
Table 3 Association between smoking and human papilloma virus-16, human papilloma virus-18 status stratified according to age n (%)
P-value of χ 2 test and corresponding OR (95%CI). NS: Not significant; HPV: Human papilloma virus.
Chatzistamatiou K et al . Smoking and genital HPV infection

not smoke (OR = 1.7, P = 0.001). This was not the case if cervical cytology showed ASCUS or worse; however the number of these women was rather low, given that the study was conducted among women attending screen-ing. These findings are presented in Table 4.
On the other hand, similar comparisons for smoking intensity between the two groups of women regarding cervical cytology and the two groups regarding hrHPV status showed, based on very low numbers, that smok-ing intensity (increasing SII) was associated with a higher probability of a positive (P = 0.045), but not a negative Pap test (Table 5).
Finally, stratification of all these associations between smoking habits, Pap smear results and hrHPV status ac-cording to age showed that only younger women (25- 34 years old) with a negative Pap test were more likely to have hrHPV infection if they were smokers than if they did not smoke (OR = 2.3, P = 0.001). These findings are presented in Table 6.
DISCUSSIONIn the present study, smokers were more likely to be test-ed positive for hrHPV types among women 25-55 years of age in an urban area of Greece. Similar results were found in a population of young women in Brazil: cer-tain HPV types were significantly more frequent in cur-rent smokers than non-smokers[30]. Likewise, in a study conducted in Portugal, the CLEOPATRE study group showed that smoking was associated with an increased risk of HPV infection[25]. The association between HPV infection and smoking has also been a consistent finding in other studies, conducted in various countries, including Russia, Belarus and Latvia[20], Germany[31], Costa Rica[7], and Canada[32].
With respect to smoking intensity, the International Agency for Research on Cancer (IARC), in a pooled analysis demonstrated that smoking intensity played a significant role in HPV infection risk[24]. Furthermore, similar results to the IARC study were found in a cohort of Tuscan women[33]. In contrast, Collins et al[12] found no evidence linking the risk of acquiring an HPV infection with the intensity of smoking. Likewise, in the present study, there was no association between smoking intensity (expressed by a Smoking Intensity Index) and hrHPV in-fection of the uterine cervix. These contradictory findings may be due to geographic variations in the prevalence of HPV-types[34], as well as due to differences in study design and methods used.
Despite the fact that smoking is a well established risk factor for cervical cancer, there are still contradicting reports regarding the association between tobacco use and hrHPV infection. In a study conducted in Denmark, current smokers were found to have similar HPV preva-lence as compared with women who had never smoked, whereas past smokers had a decreased prevalence of HPV[35]. A significant association between HPV preva-lence and smoking was found for HIV positive but not for HIV negative women, in a study comparing these two groups[36]. In a nested case control study, smoking was as-sociated with CIN3, but not with HPV infection[37]. In, a study conducted in the United States and Venezuela, risk factors for cervical cancer development appeared to vary
57 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Table 4 Association between smoking habits and high-risk human papilloma virus status according to Papanicolaou test results n (%)
Cytology Smoking HPV (+) HPV (-) Total P OR
Pap (+) Yes 18 (69.2) 8 (30.8) 26 NS 1.6 (0.5-5.6)No 11 (57.9) 9 (42.1) 19
Total 29 16 45Pap (-) Yes 118 (20.6) 455 (79.4) 573 0.001 1.7 (1.2-2.2)
No 91 (13.5) 582 (86.5) 673Total 209 1037 1246
Total Yes 136 (22.7) 463 (77.3) 599 < 0.001 1.7 (1.3-2.3)No 102 (14.7) 590 (85.3) 692
Total 238 1053 1291
P-value of χ 2 test and corresponding OR (95%CI). Papanicolaou (Pap) test (+) = atypical squamous cells of uncertain significance or worse; Pap test (-) = Normal. NS: Not significant; HPV: Human papilloma virus.
Table 5 Association between smoking intensity and high-risk human papilloma virus status according to Papanicolaou test results n (%)
Cytology Smoking HPV (+) HPV (-) Total P
Pap (+) < 50 8 (66.7) 4 (33.3) 12 0.045 50-100 4 (80.0) 1 (20.0) 5100-150 5 (100.0) 0 (0.0) 5150-200 0 (0.0) 3 (100.0) 3> 200 1 (100.0) 0 (0.0) 1Total 18 8 26
Pap (-) < 50 57 (25.2) 169 (74.8) 226 NS 50-100 26 (21.5) 95 (78.5) 121100-150 16 (13.1) 106 (86.9) 122150-200 4 (12.9) 27 (87.1) 31> 200 15 (20.5) 58 (79.5) 73Total 118 455 573
Total < 50 65 (27.3) 173 (72.7) 238 NS 50-100 30 (23.8) 96 (76.2) 126100-150 21 (16.5) 106 (83.5) 127150-200 4 (11.8) 30 (88.2) 34> 200 16 (21.6) 58 (78.4) 74Total 136 463 599
P-value of χ 2 test and corresponding OR (95%CI). Papanicolaou (Pap) test (+) = atypical squamous cells of uncertain significance or worse; Pap test (-) = Normal. NS: Not significant; HPV: Human papilloma virus.
Chatzistamatiou K et al . Smoking and genital HPV infection

between the two countries[38], and this might be possible for HPV infection as well. Therefore, studies evaluating risk factors for HPV infection should be conducted in various places around the world. An interesting finding in the present study was that younger women (25-34 years old) with a negative Pap test were more likely to have hrHPV infection if they were smokers as compared with non-smokers. This finding may suggest that smoking might enhance HPV-infection in its early stages, before development of pre-invasive lesions. On the other hand, it might be argued that this is a casual rather than a causal association, since younger women are more likely to smoke, as well as to be HPV-positive.
The exact biological mechanisms by which tobacco use is associated with HPV infection, are not clearly un-derstood yet. Persistence of an HPV infection might have been enhanced, leading to an increased risk of progression to cancer, coupled by the carcinogenic effect of polycyclic aromatic hydrocarbons contained in tobacco smoke[21]. These known carcinogens exert a transformation effect
on the epithelium of the cervix uteri[21,39,40]. Smoking may also act by increasing cell-turnover in the transformation zone of the cervix[41]. Finally, another possible mechanism might be aberrant, HPV-induced DNA methylation[42].
HPV infections are usually transient. On the other hand, persistence of HPV infection and progression to high grade lesion are probably facilitated by smoking, due to a local immunosuppression that it causes[21,38,43]. This local immune dysfunction results in prolonged dura-tion of oncogenic HPV infections, as well as a decreased probability of clearing the oncogenic infection[44,45]. Fur-thermore, smoking appears to decrease the capability of the immune system to develop HPV-16/18 antibodies or maintain HPV-16/18 antibody positivity over time, after a natural HPV infection[46]. In addition, smoking has been also associated with a higher baseline HPV-16 and HPV-18 DNA load[47]. In our study, however, smok-ing did not seem to be associated with cervical HPV-16 and/or HPV-18 infection. Finally, another possible factor that appears to play a role in the persistence of HPV in-
58 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Table 6 Association between smoking habits and high-risk human papilloma virus status according to Papanicolaou test result and stratified according to age n (%)
Age (yr) HPV (cytology) Smoking HPV (+) HPV (-) Total P OR
25-34 Pap (+) Yes 13 (76.5) 4 (23.5) 17 NSNo 9 (64.3) 5 (35.7) 14
Total 22 9 31Pap (-) Yes 82 (40.4) 121 (59.6) 203 < 0.001 2.3 (1.5-3.5)
No 54 (22.5) 186 (77.5) 240Total 136 307 443
Total Yes 95 (43.2) 125 (56.8) 220 < 0.001 2.3 (1.6-3.4)No 63 (24.8) 191 (75.2) 254
Total 158 (33.3) 316 (66.7 47435-44 Pap (+) Yes 3 (75.0) 1 (25.0) 4 NS
No 1 (100.0) 0 (0.0) 1Total 4 1 5
Pap (-) Yes 18 (10.7) 151 (89.3) 169 NSNo 23 (11.2) 183 (88.8) 206
Total 41 334 375Total Yes 21 (12.1) 152 (87.9) 173 NS
No 24 (11.6) 183 (88.4) 207Total 45 (11.8) 335 (88.2) 380
45-55 Pap (+) Yes 2 (40.0) 3 (60.0) 5 NSNo 1 (25.0) 3 (75.0) 4
Total 3 6 9Pap (-) Yes 18 (9.0) 183 (91.0) 201 NS
No 14 (6.2) 213 (93.8) 227Total 32 396 428
Total Yes 20 (9.7) 186 (90.3) 206 NSNo 15 (6.5) 216 (93.5) 231
Total 35 402 437All ages Pap (+) Yes 18 (69.2) 8 (30.8) 26 NS
No 11 (57.9) 8 (42.1) 19Total 29 16 45
Pap (-) Yes 118 (20.6) 455 (79.4) 573 0.001 1.7 (1.3-2.3)No 91 (13.5) 582 (86.5) 673
Total 209 1037 1246Total Yes 136 (22.7) 463 (77.3) 599 NS
No 102 (14.7) 590 (85.3) 692Total 238 1053 1291
P-value of χ 2 test and corresponding OR (95%CI). Papanicolaou (Pap) test (+) = atypical squamous cells of uncertain significance or worse; Pap test (-) = Normal. NS: Not significant; HPV: Human papilloma virus.
Chatzistamatiou K et al . Smoking and genital HPV infection

59 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
fection, as well as in its progression to high-grade lesions and invasive cervical cancer, is the interaction between smoking and the genetic background of an individual, which determines her susceptibility to infection and dis-ease progression[43].
A limitation of the present study, as well as of most relevant publications, is that HPV-DNA-testing was done only once for each woman. Sequential HPV genotyp-ing of all participants, at certain intervals, could possibly show if smoking might also influence the course of HPV infection. Another limitation of the present study and most relevant publications is that possible co-factors in-cluding age at first intercourse, number of sexual partners and oral contraceptive use have not been considered, and thus the possibility of bias cannot be ruled out.
In conclusion, smoking has a well-documented syner-gistic role with HPV infection, leading to cervical cancer development[48,49]. Furthermore, smoking seems to be as-sociated with an increased prevalence of HPV, a finding confirmed by the present study. Further studies should investigate whether this association is based on causality and evaluate the role of other possible co-factors. In any case, current smokers with either HPV infection or CIN lesion should be managed cautiously, and they should be advised to quit smoking.
COMMENTSBackgroundHuman papilloma virus (HPV) infection is considered to be a necessary condi-tion for cervical cancer development. High-risk HPV (hrHPV) types can cause cervical cancer, and more than 95% of tumour samples contain DNA from hrHPV genomes. Many studies have shown that smoking is associated with cervical cancer and its precursors.Research frontiersSeveral studies in various countries, including Brazil, Portugal, Russia, Belarus, Latvia, Germany, Costa Rica, and Canada, have shown that smoking is as-sociated with an increased risk of HPV infection. Regarding smoking intensity, results have been contradictory. Innovations and breakthroughsIn the present study, smokers were more likely to be tested positive for hrHPV types, among women 25-55 years of age, in an urban area of Greece. In re-spect to smoking intensity, no association with hrHPV infection of the uterine cervix was found in the present study.ApplicationsThe association between smoking and hrHPV infection is useful for planning cervical cancer prevention strategies. Furthermore, this association may help to clarify or identify new mechanisms of carcinogenesis. TerminologyHPVs are divided into two groups, according to their oncogenic potential: low-risk HPVs, usually leading to genital warts or low-grade intraepithelial lesions, and hrHPV types, with high oncogenic potential. Peer reviewThe paper is interesting and well written. The reviewers encourage authors to continue to explore this issue, improving their analysis with information on gen-eral habits of investigated young women and to discover the further correlations with HPV infection/co-infections and other factors, a part smoking.
REFERENCES1 Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kum-
mer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Muñoz N.
Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999; 189: 12-19 [PMID: 10451482]
2 zur Hausen H. Papillomaviruses in the causation of human cancers - a brief historical account. Virology 2009; 384: 260-265 [PMID: 19135222 DOI: 10.1016/j.virol.2008.11.046]
3 Arends MJ, Buckley CH, Wells M. Aetiology, pathogenesis, and pathology of cervical neoplasia. J Clin Pathol 1998; 51: 96-103 [PMID: 9602680]
4 Schiffman M, Kjaer SK. Chapter 2: Natural history of ano-genital human papillomavirus infection and neoplasia. J Natl Cancer Inst Monogr 2003; 14-19 [PMID: 12807940]
5 Vaccarella S, Franceschi S, Herrero R, Muñoz N, Snijders PJ, Clifford GM, Smith JS, Lazcano-Ponce E, Sukvirach S, Shin HR, de Sanjosé S, Molano M, Matos E, Ferreccio C, Anh PT, Thomas JO, Meijer CJ. Sexual behavior, condom use, and human papillomavirus: pooled analysis of the IARC human papillomavirus prevalence surveys. Cancer Epidemiol Biomark-ers Prev 2006; 15: 326-333 [PMID: 16492924]
6 Roura E, Iftner T, Vidart JA, Kjaer SK, Bosch FX, Muñoz N, Palacios S, Rodriguez MS, Morillo C, Serradell L, Torcel-Pagnon L, Cortes J, Castellsagué X. Predictors of human pap-illomavirus infection in women undergoing routine cervical cancer screening in Spain: the CLEOPATRE study. BMC Infect Dis 2012; 12: 145 [PMID: 22734435]
7 Herrero R, Castle PE, Schiffman M, Bratti MC, Hildesheim A, Morales J, Alfaro M, Sherman ME, Wacholder S, Chen S, Rodriguez AC, Burk RD. Epidemiologic profile of type-specific human papillomavirus infection and cervical neopla-sia in Guanacaste, Costa Rica. J Infect Dis 2005; 191: 1796-1807 [PMID: 15871111]
8 Castellsagué X, Bosch FX, Muñoz N. Environmental co-fac-tors in HPV carcinogenesis. Virus Res 2002; 89: 191-199 [PMID: 12445659]
9 Ylitalo N, Sørensen P, Josefsson A, Frisch M, Sparén P, Pon-tén J, Gyllensten U, Melbye M, Adami HO. Smoking and oral contraceptives as risk factors for cervical carcinoma in situ. Int J Cancer 1999; 81: 357-365 [PMID: 10209949]
10 Castellsagué X, Muñoz N. Chapter 3: Cofactors in human papillomavirus carcinogenesis--role of parity, oral contracep-tives, and tobacco smoking. J Natl Cancer Inst Monogr 2003; 20-28 [PMID: 12807941]
11 Appleby P, Beral V, Berrington de González A, Colin D, Franceschi S, Goodill A, Green J, Peto J, Plummer M, Sweet-land S. Carcinoma of the cervix and tobacco smoking: col-laborative reanalysis of individual data on 13,541 women with carcinoma of the cervix and 23,017 women without carcinoma of the cervix from 23 epidemiological studies. Int J Cancer 2006; 118: 1481-1495 [PMID: 16206285]
12 Collins S, Rollason TP, Young LS, Woodman CB. Cigarette smoking is an independent risk factor for cervical intraepi-thelial neoplasia in young women: a longitudinal study. Eur J Cancer 2010; 46: 405-411 [PMID: 19819687 DOI: 10.1016/j.ejca.2009.09.015]
13 Kapeu AS, Luostarinen T, Jellum E, Dillner J, Hakama M, Koskela P, Lenner P, Löve A, Mahlamaki E, Thoresen S, Tryggvadóttir L, Wadell G, Youngman L, Lehtinen M. Is smoking an independent risk factor for invasive cervical can-cer? A nested case-control study within Nordic biobanks. Am J Epidemiol 2009; 169: 480-488 [PMID: 19074773 DOI: 10.1093/aje/kwn354]
14 Kjaer SK, Engholm G, Dahl C, Bock JE. Case-control study of risk factors for cervical squamous cell neoplasia in Denmark. IV: role of smoking habits. Eur J Cancer Prev 1996; 5: 359-365 [PMID: 8972255]
15 Ho GY, Kadish AS, Burk RD, Basu J, Palan PR, Mikhail M, Romney SL. HPV 16 and cigarette smoking as risk factors for high-grade cervical intra-epithelial neoplasia. Int J Cancer 1998; 78: 281-285 [PMID: 9766558]
16 Tolstrup J, Munk C, Thomsen BL, Svare E, van den Brule AJ,
COMMENTS
Chatzistamatiou K et al . Smoking and genital HPV infection

60 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
Grønbaek M, Meijer C, Kjaer Krüger S. The role of smoking and alcohol intake in the development of high-grade squa-mous intraepithelial lesions among high-risk HPV-positive women. Acta Obstet Gynecol Scand 2006; 85: 1114-1119 [PMID: 16929418]
17 Jensen KE, Schmiedel S, Frederiksen K, Norrild B, Iftner T, Kjær SK. Risk for cervical intraepithelial neoplasia grade 3 or worse in relation to smoking among women with persistent human papillomavirus infection. Cancer Epidemiol Biomarkers Prev 2012; 21: 1949-1955 [PMID: 23019238]
18 Guarisi R, Sarian LO, Hammes LS, Longatto-Filho A, Der-chain SF, Roteli-Martins C, Naud P, Erzen M, Branca M, Tatti S, Costa S, Syrjänen S, Bragança JF, Syrjänen K. Smok-ing worsens the prognosis of mild abnormalities in cervical cytology. Acta Obstet Gynecol Scand 2009; 88: 514-520 [PMID: 19308752 DOI: 10.1080/00016340902846072]
19 Simen-Kapeu A, La Ruche G, Kataja V, Yliskoski M, Bergeron C, Horo A, Syrjänen K, Saarikoski S, Lehtinen M, Dabis F, Sasco AJ. Tobacco smoking and chewing as risk factors for multiple human papillomavirus infections and cervical squa-mous intraepithelial lesions in two countries (Côte d’Ivoire and Finland) with different tobacco exposure. Cancer Causes Control 2009; 20: 163-170 [PMID: 18814048 DOI: 10.1007/s10552-008-9230-x]
20 Syrjänen K, Shabalova I, Petrovichev N, Kozachenko V, Zakharova T, Pajanidi J, Podistov J, Chemeris G, Sozaeva L, Lipova E, Tsidaeva I, Ivanchenko O, Pshepurko A, Zakha-renko S, Nerovjna R, Kljukina L, Erokhina O, Branovskaja M, Nikitina M, Grunberga V, Grunberg A, Juschenko A, Santopietro R, Cintorino M, Tosi P, Syrjänen S. Smoking is an independent risk factor for oncogenic human papillomavirus (HPV) infections but not for high-grade CIN. Eur J Epidemiol 2007; 22: 723-735 [PMID: 17828436]
21 Louie KS, Castellsague X, de Sanjose S, Herrero R, Meijer CJ, Shah K, Munoz N, Bosch FX. Smoking and passive smoking in cervical cancer risk: pooled analysis of couples from the IARC multicentric case-control studies. Cancer Epidemiol Bio-markers Prev 2011; 20: 1379-1390 [PMID: 21610224]
22 Natphopsuk S, Settheetham-Ishida W, Sinawat S, Pientong C, Yuenyao P, Ishida T. Risk factors for cervical cancer in north-eastern Thailand: detailed analyses of sexual and smoking behavior. Asian Pac J Cancer Prev 2012; 13: 5489-5495 [PMID: 23317205]
23 Sherman JF, Mount SL, Evans MF, Skelly J, Simmons-Arnold L, Eltabbakh GH. Smoking increases the risk of high-grade vaginal intraepithelial neoplasia in women with oncogenic human papillomavirus. Gynecol Oncol 2008; 110: 396-401 [PMID: 18586314 DOI: 10.1016/j.ygyno.2008.05.015]
24 Vaccarella S, Herrero R, Snijders PJ, Dai M, Thomas JO, Hieu NT, Ferreccio C, Matos E, Posso H, de Sanjosé S, Shin HR, Sukvirach S, Lazcano-Ponce E, Muñoz N, Meijer CJ, Frances-chi S. Smoking and human papillomavirus infection: pooled analysis of the International Agency for Research on Cancer HPV Prevalence Surveys. Int J Epidemiol 2008; 37: 536-546 [PMID: 18316350 DOI: 10.1093/ije/dyn033]
25 Pista A, de Oliveira CF, Cunha MJ, Paixao MT, Real O. Risk factors for human papillomavirus infection among women in Portugal: the CLEOPATRE Portugal Study. Int J Gynaecol Obstet 2012; 118: 112-116 [PMID: 22608026 DOI: 10.1016/j.ijgo.2012.03.028]
26 Schabath MB, Villa LL, Lazcano-Ponce E, Salmerón J, Qui-terio M, Giuliano AR. Smoking and human papillomavirus (HPV) infection in the HPV in Men (HIM) study. Cancer Epi-demiol Biomarkers Prev 2012; 21: 102-110 [PMID: 22016473]
27 Hutchinson ML, Cassin CM, Ball HG. The efficacy of an au-tomated preparation device for cervical cytology. Am J Clin Pathol 1991; 96: 300-305 [PMID: 1877527]
28 Solomon D, Davey D, Kurman R, Moriarty A, O’Connor D, Prey M, Raab S, Sherman M, Wilbur D, Wright T, Young N. The 2001 Bethesda System: terminology for reporting results of
cervical cytology. JAMA 2002; 287: 2114-2119 [PMID: 11966386]29 Stoler MH, Wright TC, Sharma A, Apple R, Gutekunst K,
Wright TL. High-risk human papillomavirus testing in wom-en with ASC-US cytology: results from the ATHENA HPV study. Am J Clin Pathol 2011; 135: 468-475 [PMID: 21350104]
30 Roteli-Martins CM, Panetta K, Alves VA, Siqueira SA, Syrjänen KJ, Derchain SF. Cigarette smoking and high-risk HPV DNA as predisposing factors for high-grade cervical in-traepithelial neoplasia (CIN) in young Brazilian women. Acta Obstet Gynecol Scand 1998; 77: 678-682 [PMID: 9688248]
31 Remschmidt C, Kaufmann AM, Hagemann I, Vartazarova E, Wichmann O, Deleré Y. Risk factors for cervical human papillomavirus infection and high-grade intraepithelial le-sion in women aged 20 to 31 years in Germany. Int J Gynecol Cancer 2013; 23: 519-526 [PMID: 23360813 DOI: 10.1097/IGC.0b013e318285a4b2]
32 Sellors JW, Mahony JB, Kaczorowski J, Lytwyn A, Bangura H, Chong S, Lorincz A, Dalby DM, Janjusevic V, Keller JL. Prevalence and predictors of human papillomavirus infec-tion in women in Ontario, Canada. Survey of HPV in Ontario Women (SHOW) Group. CMAJ 2000; 163: 503-508 [PMID: 11006760]
33 Confortini M, Carozzi F, Zappa M, Ventura L, Iossa A, Car-iaggi P, Brandigi L, Franchini M, Mirri F, Viacava P, Scarfan-toni A, Bazzanti D, Sani C. Human papillomavirus infection and risk factors in a cohort of Tuscan women aged 18-24: results at recruitment. BMC Infect Dis 2010; 10: 157 [PMID: 20529280 DOI: 10.1186/1471-2334-10-157]
34 Agorastos T, Lambropoulos AF, Sotiriadis A, Mikos T, Togaridou E, Emmanouilides CJ. Prevalence and distribu-tion of high-risk human papillomavirus in Greece. Eur J Cancer Prev 2009; 18: 504-509 [PMID: 19741545 DOI: 10.1097/CEJ.0b013e32832abd5e]
35 Kjaer SK, van den Brule AJ, Bock JE, Poll PA, Engholm G, Sherman ME, Walboomers JM, Meijer CJ. Determinants for genital human papillomavirus (HPV) infection in 1000 ran-domly chosen young Danish women with normal Pap smear: are there different risk profiles for oncogenic and nononco-genic HPV types? Cancer Epidemiol Biomarkers Prev 1997; 6: 799-805 [PMID: 9332762]
36 Minkoff H, Feldman JG, Strickler HD, Watts DH, Bacon MC, Levine A, Palefsky JM, Burk R, Cohen MH, Anastos K. Relationship between smoking and human papillomavirus infections in HIV-infected and -uninfected women. J Infect Dis 2004; 189: 1821-1828 [PMID: 15122518]
37 Deacon JM, Evans CD, Yule R, Desai M, Binns W, Taylor C, Peto J. Sexual behaviour and smoking as determinants of cervical HPV infection and of CIN3 among those infected: a case-control study nested within the Manchester cohort. Br J Cancer 2000; 83: 1565-1572 [PMID: 11076670]
38 Sierra-Torres CH, Tyring SK, Au WW. Risk contribution of sexual behavior and cigarette smoking to cervical neoplasia. Int J Gynecol Cancer 2003; 13: 617-625 [PMID: 14675345]
39 Moore TO, Moore AY, Carrasco D, Vander Straten M, Arany I, Au W, Tyring SK. Human papillomavirus, smoking, and cancer. J Cutan Med Surg 2001; 5: 323-328 [PMID: 11907844]
40 Olsen AO, Dillner J, Skrondal A, Magnus P. Combined effect of smoking and human papillomavirus type 16 infection in cervical carcinogenesis. Epidemiology 1998; 9: 346-349 [PMID: 9583429]
41 Harris TG, Kulasingam SL, Kiviat NB, Mao C, Agoff SN, Feng Q, Koutsky LA. Cigarette smoking, oncogenic human papillomavirus, Ki-67 antigen, and cervical intraepithelial neoplasia. Am J Epidemiol 2004; 159: 834-842 [PMID: 15105176]
42 Fonseca-Moutinho JA. Smoking and cervical cancer. ISRN Obstet Gynecol 2011; 2011: 847684 [PMID: 21785734 DOI: 10.5402/2011/847684]
43 Hussain SK, Madeleine MM, Johnson LG, Du Q, Malkki M, Wilkerson HW, Farin FM, Carter JJ, Galloway DA, Daling JR, Petersdorf EW, Schwartz SM. Cervical and vulvar cancer risk
Chatzistamatiou K et al . Smoking and genital HPV infection

61 August 10, 2013|Volume 2|Issue 3|WJOG|www.wjgnet.com
in relation to the joint effects of cigarette smoking and genetic variation in interleukin 2. Cancer Epidemiol Biomarkers Prev 2008; 17: 1790-1799 [PMID: 18628433 DOI: 10.1158/1055-9965.EPI-07-2753]
44 Giuliano AR, Sedjo RL, Roe DJ, Harri R, Baldwi S, Papen-fuss MR, Abrahamsen M, Inserra P. Clearance of oncogenic human papillomavirus (HPV) infection: effect of smoking (United States). Cancer Causes Control 2002; 13: 839-846 [PMID: 12462549]
45 Koshiol J, Schroeder J, Jamieson DJ, Marshall SW, Duerr A, Heilig CM, Shah KV, Klein RS, Cu-Uvin S, Schuman P, Celentano D, Smith JS. Smoking and time to clearance of hu-man papillomavirus infection in HIV-seropositive and HIV-seronegative women. Am J Epidemiol 2006; 164: 176-183 [PMID: 16775041]
46 Simen-Kapeu A, Kataja V, Yliskoski M, Syrjänen K, Dillner J, Koskela P, Paavonen J, Lehtinen M. Smoking impairs hu-man papillomavirus (HPV) type 16 and 18 capsids antibody
response following natural HPV infection. Scand J Infect Dis 2008; 40: 745-751 [PMID: 19086247 DOI: 10.1080/00365540801995360]
47 Xi LF, Koutsky LA, Castle PE, Edelstein ZR, Meyers C, Ho J, Schiffman M. Relationship between cigarette smoking and human papilloma virus types 16 and 18 DNA load. Cancer Epidemiol Biomarkers Prev 2009; 18: 3490-3496 [PMID: 19959700]
48 Gunnell AS, Tran TN, Torrång A, Dickman PW, Sparén P, Palmgren J, Ylitalo N. Synergy between cigarette smok-ing and human papillomavirus type 16 in cervical cancer in situ development. Cancer Epidemiol Biomarkers Prev 2006; 15: 2141-2147 [PMID: 17057029]
49 Ndisang D, Khan A, Lorenzato F, Sindos M, Singer A, Latch-man DS. The cellular transcription factor Brn-3a and the smoking-related substance nicotine interact to regulate the activity of the HPV URR in the cervix. Oncogene 2010; 29: 2701-2711 [PMID: 20190800 DOI: 10.1038/onc.2010.33]
P- Reviewers Cao C, Celik H, Iavazzo CR, Kruse AJ, Tinelli A, Yokoyama Y S- Editor Gou SX L- Editor A
E- Editor Zheng XM
Chatzistamatiou K et al . Smoking and genital HPV infection

World Journal of Obstetrics and GynecologyWorld J Obstet Gynecol 2013 November 10; 2(4): 62-191
ISSN 2218-6220 (online)
www.wjgnet.comwww.wjgnet.com
Volume End

62 Whymoreattentionstofetusincasesofintrahepaticcholestasisofpregnancy?
Zhang XQ, Ding YL, Zhang LJ
65 Mirabegron,anovel,non-antimuscarinicdrugfortheoveractivebladder:An
up-to-datedreview
Sacco E, Bientinesi R
74 Femaleurinaryincontinenceduringpregnancyandafterdelivery:Clinical
impactandcontributingfactors
Mannella P, Palla G, Pérez-Roncero G, López-Baena MT, Pérez-López FR
80 Individualizedmisoprostoldosingforlaborinductionoraugmentation:A
review
Cheng SY
87 Folicacidsupplementation:Thenewdawnforpostmenopausalwomenwith
hotflushes
Ewies AAA
94 Cytoreductivesurgeryandhyperthermicintraperitonealchemotherapyin
epithelianovariancancer:Stateoftheart
Eskander RN, Ansaloni L, Bristow RE, Coccolini F
101 Cytoreductivesurgeryafterrecurrentepithelialovariancancerandatother
timepoints
Sammartino P, Cornali T, dei Malatesta MF, Piso P
108 Comprehensivemanagementofepithelialovariancancerwithperitoneal
metastases
Frigerio L, Ansaloni L, Poiasina E, Coccolini F, Sugarbaker PH
116 Cytoreductivesurgeryinprimaryadvancedepithelialovariancancer
Ansaloni L, Coccolini F, Catena F, Frigerio L, Bristow RE
124 CriticalitiesinrandomizedcontrolledtrialsonHIPECforovariancancer
Coccolini F, Ansaloni L, Corbella D, Lotti M, Glehen O
Contents
IWJOG|www.wjgnet.com November 10, 2013|Volume 2|Issue 4|
EDITORIAL
World Journal ofObstetrics and GynecologyW J O G
Quarterly Volume 2 Number 4 November 10, 2013
FRONTIER
THERAPEUTIC ADVANCES
TOPIC HIGHLIGHT

ContentsWorld Journal of Obstetrics and Gynecology
Volume 2 Number 4 November 10, 2013
129 Anestheticmanagementofcytoreductivesurgeryandhyperthermic
intraperitonealchemotherapyprocedures
Corbella D, Piraccini E, Finazzi P, Brambillasca P, Prussiani V, Corso MR,
Germandi C, Agnoletti V
137 Naturalhistoryofepithelialovariancanceranditsrelationtosurgicaland
medicaltreatment
De Iaco P, Perrone AM, Procaccini M, Pellegrini A, Morice P
143 Pharmacologyofcancerchemotherapydrugsforhyperthermicintraperitoneal
peroperativechemotherapyinepithelialovariancancer
Van der Speeten K, Stuart AO, Sugarbaker PH
153 Neoadjuvantchemotherapyandcytoreductivesurgeryinepithelialovarian
cancer
Tangjitgamol S, Hanprasertpong J, Cubelli M, Zamagni C
167 CytoreductivesurgeryandHIPECafterneoadjuvantchemotherapyfor
advancedepithelialovariancancer
Lotti M, Busci LM, Campanati L, Catena F, Coccolini F, Bakrin N, De Iaco P,
Ercolani G, Grosso G, Pisano M, Poiasina E, Rossetti D, Rossi M, Zamagni C, Bertoli P,
Pinna AD, Frigerio L, Ansaloni L
176 Surgicalrepairofpelvicorganprolapseandfollow-up:Aninstitutional
multi-centerexperience
Gustapane S, Leombroni M, Falò E, Santarelli A, Frondaroli F, Liberati M, Perrone E,
Tinelli A
181 CharacteristicsofsemenparametersofMalawianmenfromcouplesseeking
assistedreproduction
Lampiao F, Kutengule A
185 Pelvicarterialembolizationinobstetrichemorrhage
Chaudhary V, Sachdeva P, Arora R, Kumar D, Karanth P
IIWJOG|www.wjgnet.com November 10, 2013|Volume 2|Issue 4|
BRIEF ARTICLE

ContentsWorld Journal of Obstetrics and Gynecology
Volume 2 Number 4 November 10, 2013
EDITORS FOR THIS ISSUE
Responsible Assistant Editor: Xin-Xin Che Responsible Science Editor: Xiu-Xia SongResponsible Electronic Editor: Dan-Ni ZhangProofing Editor-in-Chief: Lian-Sheng Ma
World Journal of Obstetrics and GynecologyRoom 903, Building D, Ocean International Center, No. 62 Dongsihuan Zhonglu, Chaoyang District, Beijing 100025, ChinaTelephone: +86-10-85381891Fax: +86-10-85381893E-mail: [email protected]://www.wjgnet.com
PUBLISHERBaishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza, 315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188Telephone: +852-31779906E-mail: [email protected]://www.wjgnet.com
PUBLICATIONDATENovember 10, 2013
COPYRIGHT© 2013 Baishideng Publishing Group Co., Limited. Articles published by this Open-Access journal are dis-tributed under the terms of the Creative Commons At-tribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non com-mercial and is otherwise in compliance with the license.
SPECIALSTATEMENTAll articles published in this journal represent the view-points of the authors except where indicated otherwise.
INSTRUCTIONSTOAUTHORSFull instructions are available online at http://www.wjgnet.com/2218-6220/g_info_20100722175812.htm.
ONLINESUBMISSIONhttp://www.wjgnet.com/esps/
IIIWJOG|www.wjgnet.com
APPENDIX
ABOUT COVER
AIM AND SCOPE
FLYLEAF
November 10, 2013|Volume 2|Issue 4|
NAMEOFJOURNALWorld Journal of Obstetrics and Gynecology
ISSNISSN 2218-6220 (online)
LAUNCHDATEJune 10, 2012
FREQUENCYQuarterly
EDITOR-IN-CHIEFBo Jacobsson, MD, PhD, Professor, Department Obstetrics and Gynecology, Sahlgrenska University Hospital/Ostra, SE-416 85 Gothenburg, Sweden
EDITORIALOFFICEJin-Lei Wang, DirectorXiu-Xia Song, Vice Director
I-V Instructionstoauthors
WorldJournalofObstetricsandGynecologyEditorialBoardMember,EmilioSacco,PhD,AssistantProfessor,Urologia,PoliclinicoAgostinoGemelli,LargoGemelli8,00168Roma,Italy
World Journal of Obstetrics and Gynecology (World J Obstet Gynecol, WJOG, online ISSN 2218-6220, DOI: 10.5317) is a peer-reviewed open access academic journal that aims to guide clinical practice and improve diagnostic and therapeutic skills of clinicians.
WJOG covers topics concerning pregnancy complications, obstetric surgical procedures, diagnostic imaging, endoscopy, reproductive endocrinology, tumors, pelvic diseases, evidence-based medicine, epidemiology and nursing.
We encourage authors to submit their manuscripts to WJOG. We will give priority to manuscripts that are supported by major national and international foundations and those that are of great basic and clinical significance.
World Journal of Obstetrics and Gynecology is now indexed in Digital Object Identifier.
I-III EditorialBoard
INDEXING/ABSTRACTING

In addition, high total BA can result in chorionic vein constriction and impaired fetal adrenal function.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Intrahepatic cholestasis of pregnancy; Bile acid; Perinatal outcome; Fetal lung; Fetal heart
Core tip: Fetal outcomes for patients diagnosed with intrahepatic cholestasis of pregnancy can be devastat-ing with serious complications. Advances in our un-derstanding of the reasons that can cause severe fetal complications, such as sudden fetal death, slowed fetal lung maturity, perinatal nervous system injury, distress, and neonatal asphyxia, will provide some hints towards the basic etiology of this disorder. We look forward to a time that early diagnosis will be made and laboratory tests will be carried out to monitor these fetal condi-tions. I would suggest that more attention should be paid to the fetus which contributes to improve fetal out-comes.
Zhang XQ, Ding YL, Zhang LJ. Why more attentions to fetus in cases of intrahepatic cholestasis of pregnancy? World J Obstet Gynecol 2013; 2(4): 62-64 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/62.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.62
INTRODUCTIONIntrahepatic cholestasis of pregnancy (ICP) is a maternal metabolic disease affecting up to 5% of pregnancies[1]. It occurs in the second and third trimester, and is character-ized by intense pruritus and an elevation in serum bile acid (BA) concentrations. Maternal outcomes for patients diagnosed with ICP are usually good. However, fetal outcomes can be devastating with complications of pre-
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.62
World J Obstet Gynecol 2013 November 10; 2(4): 62-64ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Why more attentions to fetus in cases of intrahepatic cholestasis of pregnancy?
Xiu-Quan Zhang, Yi-Lin Ding, Li-Juan Zhang
Xiu-Quan Zhang, Department of Obstetrics and Gynecology and Reproductive Genetics, University of Utah School of Medi-cine, Salt Lake City, UT 84132, United StatesYi-Lin Ding, Li-Juan Zhang, Department of Obstetrics and Gy-necology, the Second Xiangya Hospital, Central South Univer-sity, Changsha 410011, Hunan Province, ChinaAuthor contributions: Zhang XQ, Zhang LJ and Ding YL solely contributed to this paper.Correspondence to: Xiu-Quan Zhang, MD, PhD, Department of Obstetrics and Gynecology and Reproductive Genetics, Uni-versity of Utah School of Medicine, 50 North Medical Drive, Salt Lake City, UT 84132, United States. [email protected]: +1-801-5853117 Fax: +1-801-5853885Received: June 27, 2013 Revised: August 29, 2013Accepted: September 3, 2013Published online: November 10, 2013
AbstractIntrahepatic cholestasis of pregnancy (ICP) is a peculiar disease in middle-late pregnancy with the pathological characteristics of hepatic capillary bile duct silts and is accompanied by clinical presentations of pruritus and bile acid (BA) elevation in serum. Maternal outcomes for patients diagnosed with ICP are usually good. However, fetal outcomes can be devastating with high frequencies of perinatal complications. Patients with ICP generally have an early delivery due to fetal complications. The current hypothesis is that ICP has higher frequencies of fetal complications due to high concentrations of BA which has toxic cellular effects to many organs. In lungs, it destroys the AT-II cells, decreasing phospholip-ids synthesis leading to the alveolar capillary permeabil-ity to increase and pulmonary surfactant to decrease. In heart, cholate can cross into the fetal compartment and causing fetal arrhythmias and decreased contractil-ity. In the nervous system, high BAs can cause nerve cell denaturation and necrosis, mitochondria edema and membrane dissolve. In the placenta, high BA concentra-tion can cause edema of the villous, decrease number of villous, intervillous thickening and balloon formation.
EDITORIAL
62 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Zhang XQ et al . More attention to fetus in ICP
mature delivery, fetal distress, neonatal asphyxia, neonatal respiratory distress syndrome, neonatal multi-system damage, and fetal death[2,3]. Thus, early recognition, treat-ment, and timely delivery are imperative. From the mater-nal viewpoint, the main symptom is the intense pruritus, which may become intolerable leading to an early deliv-ery[4]. On the fetal viewpoint, it is more concerning since the high risk of perinatal complications which can result in fetal demise. Thus, many doctors would advocate in-duction at 37 wk[5].
SEVERE INFLUENCES OF ICP TO FETUSSudden fetal deathOne of the most worrisome aspects of ICP is the pos-sibility of sudden fetal death[6]. Possible explanations for sudden fetal death are taurocholate crossing into the fetal compartment and causing fetal arrhythmias and decreased contractility[7]. Other studies have noted an in-creased P-R interval in human fetuses affected by ICP[8].Intrauterine fetal demise is also associated with ICP, espe-cially when the total BA (TBA) level is critically elevated, but it rarely occurs prior to 36 weeks’ gestation. With the risk for sudden fetal death, it becomes a dilemma how to monitor and when to deliver. Since fetal death rarely occurs before 36 weeks’ gestation, many doctors favor delivery when it reaches to 37 wk gestation[9].
Lung maturityICP usually accompanied with slowed lung maturity. It is associated with fetal distress, neonatal asphyxia, neonatal respiratory distress syndrome, and cholic acid pneumo-nia[10]. In Glantz’s study, fetal asphyxia was related to BA concentration with the critical level of 40 mmol/L or greater[11]. The pulmonary pathological changes consist with neonatal pulmonary hyaline membrane disease, light transmittance of the lung reducing, swelling, widely atel-ectasis, diffuse pulmonary hyaline membrane disease[12,13]. In one of our case control studies, amniotic fluid surfac-tant and lamellar body was significantly decreased and fe-tal lung area/body weight ratio was significantly reduced in ICP patients. In addition, fetal blood TBA showed a negative correlation to the surface active substances-phospholipids production. In Shi et al[14] study, cholic acid can cause a dysfunction in the synthesis of surface active substances in the lung. He found that high BA can lead to immature fetal rat lung with the pulmonary morpho-logical changes of smaller alveolar cavities, thickening alveolar intervals, local atelectasis, and most cells fall off from the wall. Furthermore, pulmonary tissue was found to have heavy density and diffuse bleeding lesions.
Nervous systemSevere and moderate ICP can cause perinatal nervous system injury and the severity of injury is associated with the TBA level. Pathological changes include immaturity of the hepatoencephalic barrier and presents with en-dothelial holes, thinning of the base membrane leading to an increase in permeability[15]. Animal experiments
demonstrated that high BAs can cause nerve cell denatur-ation and necrosis, mitochondria edema and membrane damage[16]. By measuring umbilical artery blood pH, lactic acid, and color Doppler on fetal cerebral artery blood flow, it was found that ICP can cause fetal acidemia and reduced fetal cerebral blood flow[17].
Fetal distress and neonatal asphyxiaICP has higher frequencies of fetal distress and neonatal asphyxia. It is considered these may be associated with the pathological changes in the placenta. The morphology of placentas from the rodent model of ICP is markedly abnormal. Human and rodent studies have shown that transplacental transfer of BAs is impaired in ICP. High BA concentration results in placental alteration with increased syncytial knots, reduced collagen, edema of the villous, decreased number of villous, intervillous thickening and balloon formation[18]. Geenes found that ICP placentas have an increase in the number of syncytial knots, and that these can be reproduced in an in vitro model exposed to the BAs taurocholic acid and taurochenodoexycholic acid[19]. Ding studied the morphologic ultrastructure of human placental syncytial cells and reported that ICP placenta has impaired cellular organelle, resulting in the abnormal physiological function of syncytial cells, and affecting the synthesis and transportation functions of the placenta[20].
Vascular systemIn addition, high TBAs can increase the intracellular cal-cium concentration resulting in chorionic vein constric-tion and can lead to the increase of placental circulation resistance[21]. It can cause fetal adrenal dysfunction and influence the production of vascular aldosterone and corticosterone[22].
LABORATORY MONITORING OF ICPMany laboratory abnormalities can be seen in ICP. The most specific and sensitive marker of ICP is TBA levels greater than 10 μmol/L[23]. In addition, the cholic acid level is significantly increased while the chenodeoxycholic acid level is mildly increased, resulting in an elevation in the cholic/chenodeoxycholic acid level ratio[24,25].
Recommended laboratory studies for the diagnosis of ICP include monitoring total serum BA levels, cholic acid, chenodeoxycholic acid (to evaluate the cholic/chenode-oxycholic acid ratio), total bilirubin, transaminases, GGT, PT, PTT, and INR. These laboratory studies are used in conjunction with physical examination and symptoms to make a diagnosis of ICP. Once a diagnosis of ICP has been made, TBA levels can be followed every 2-3 wk to guide therapy and timing of delivery. In addition, coagula-tion studies and transaminase levels should be monitored to measure progression of the disease.
MANAGEMENT OF FETUSMore attention should be placed on the fetus. Tests for the fetus, including umbilical artery Doppler studies, bio-
63 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

physical profile, and nonstress tests, should be performed to reduce the risk of stillbirth[26]. One study demonstrated that increased fetal testing and scheduled induction with documentation of fetal lung maturity in patients with ICP lessened perinatal mortality rates compared with patients who were not tested[27]. Delivery should be induced at 37 wk. If deliver prior to 37 wk occurs, amniocentesis for fetal lung maturity is necessary. If meconium is present at the time of amniocentesis, delivery is indicated regardless of the fetal lung maturity results. Delivery should proceed without an amniocentesis if the fetal monitoring is nonre-assuring.
REFERENCES1 Abedin P, Weaver JB, Egginton E. Intrahepatic cholestasis of
pregnancy: prevalence and ethnic distribution. Ethn Health 1999; 4: 35-37 [PMID: 10887460 DOI: 10.1080/13557859998173]
2 Pan C, Perumalswami PV. Pregnancy-related liver dis-eases. Clin Liver Dis 2011; 15: 199-208 [PMID: 21112001 DOI: 10.1016/j.cld.2010.09.007]
3 Wikström Shemer E, Marschall HU, Ludvigsson JF, Stepha-nsson O. Intrahepatic cholestasis of pregnancy and associ-ated adverse pregnancy and fetal outcomes: a 12-year pop-ulation-based cohort study. BJOG 2013; 120: 717-723 [PMID: 23418899 DOI: 10.1111/1471-0528.12174]
4 Pathak B, Sheibani L, Lee RH. Cholestasis of pregnancy. Ob-stet Gynecol Clin North Am 2010; 37: 269-282 [PMID: 20685553 DOI: 10.1016/j.ogc.2010.02.011]
5 Mays JK. The active management of intrahepatic cholestasis of pregnancy. Curr Opin Obstet Gynecol 2010; 22: 100-103 [PMID: 20124899 DOI: 10.1097/GCO.0b013e328337238d]
6 Shao Y, Yao Z, Lu J, Li H, Wu W, Ding M. [Change of heart rate power spectrum and its association with sudden death in the fetuses of rats with intrahepatic cholestasis of pregnancy]. Shengwu Yixue Gongchengxue Zazhi 2007; 24: 1215-1219 [PMID: 18232463]
7 Favre N, Abergel A, Blanc P, Sapin V, Roszyk L, Gallot D. Un-usual presentation of severe intrahepatic cholestasis of preg-nancy leading to fetal death. Obstet Gynecol 2009; 114: 491-493 [PMID: 19622974 DOI: 10.1097/AOG.0b013e3181a0a81a]
8 Strehlow SL, Pathak B, Goodwin TM, Perez BM, Ebrahimi M, Lee RH. The mechanical PR interval in fetuses of women with intrahepatic cholestasis of pregnancy. Am J Obstet Gy-necol 2010; 203: 455.e1-455.e5 [PMID: 20684945 DOI: 10.1016/j.ajog.2010.05.035]
9 Williamson C, Hems LM, Goulis DG, Walker I, Chambers J, Donaldson O, Swiet M, Johnston DG. Clinical outcome in a series of cases of obstetric cholestasis identified via a patient support group. BJOG 2004; 111: 676-681 [PMID: 15198757]
10 Zecca E, De Luca D, Barbato G, Marras M, Tiberi E, Romag-noli C. Predicting respiratory distress syndrome in neonates from mothers with intrahepatic cholestasis of pregnancy. Early Hum Dev 2008; 84: 337-341 [PMID: 17928172]
11 Glantz A, Marschall HU, Mattsson LA. Intrahepatic cholesta-sis of pregnancy: Relationships between bile acid levels and fetal complication rates. Hepatology 2004; 40: 467-474 [PMID: 15368452]
12 Zecca E, De Luca D, Marras M, Caruso A, Bernardini T, Rom-
agnoli C. Intrahepatic cholestasis of pregnancy and neonatal respiratory distress syndrome. Pediatrics 2006; 117: 1669-1672 [PMID: 16651322]
13 Grabowski M, Kasran A, Seys S, Pauwels A, Medrala W, Dupont L, Panaszek B, Bullens D. Pepsin and bile ac-ids in induced sputum of chronic cough patients. Respir Med 2011; 105: 1257-1261 [PMID: 21592756 DOI: 10.1016/j.rmed.2011.04.015]
14 Shi Y, Qi HB. [Effects of intrahepatic cholestasis on morphol-ogy of fetal lungs in pregnant rat]. Zhonghua Fuchanke Zazhi 2010; 45: 283-286 [PMID: 20646541]
15 EQUEN M. The alnico magnet, an aid to bronchoscopy and esophagoscopy. Bull Fulton Cty Med Soc 1945; 19: 11 [PMID: 21003624]
16 Lin S, Li X, Yan G. [Bilirubin induced apoptosis of cerebel-lar granule neurons]. Zhonghua Yixue Zazhi 1999; 79: 125-128 [PMID: 11601019]
17 Yang X, Ding YL. [Relationship of the occurrence of fetal dis-tress and change of umbilical cord and expression of vasoac-tive substance in umbilical vein in intrahepatic cholestasis of pregnancy]. Zhonghua Fuchanke Zazhi 2008; 43: 85-89 [PMID: 18683743]
18 Wikström Shemer E, Thorsell M, Östlund E, Blomgren B, Marschall HU. Stereological assessment of placental morphol-ogy in intrahepatic cholestasis of pregnancy. Placenta 2012; 33: 914-918 [PMID: 23020907 DOI: 10.1016/j.placenta.2012.08.005]
19 Geenes VL, Lim YH, Bowman N, Tailor H, Dixon PH, Cham-bers J, Brown L, Wyatt-Ashmead J, Bhakoo K, Williamson C. A placental phenotype for intrahepatic cholestasis of preg-nancy. Placenta 2011; 32: 1026-1032 [PMID: 22015023 DOI: 10.1016/j.placenta.2011.09.006]
20 Ding YL, Tang LL. [Stereological study on syncytial cell of human placenta and determinations of total bile acid in cord blood of intrahepatic cholestasis of pregnancy]. Zhonghua Fuchanke Zazhi 2005; 40: 453-456 [PMID: 16080870]
21 Sepúlveda WH, González C, Cruz MA, Rudolph MI. Vasocon-strictive effect of bile acids on isolated human placental cho-rionic veins. Eur J Obstet Gynecol Reprod Biol 1991; 42: 211-215 [PMID: 1773876]
22 Wang C, Chen X, Zhou SF, Li X. Impaired fetal adrenal func-tion in intrahepatic cholestasis of pregnancy. Med Sci Monit 2011; 17: CR265-CR271 [PMID: 21525808]
23 Palma J, Reyes H, Ribalta J, Hernández I, Sandoval L, Al-muna R, Liepins J, Lira F, Sedano M, Silva O, Tohá D, Silva JJ. Ursodeoxycholic acid in the treatment of cholestasis of preg-nancy: a randomized, double-blind study controlled with placebo. J Hepatol 1997; 27: 1022-1028 [PMID: 9453428]
24 Pass LJ, Schloerb PR, Chow FT, Graham M, Pearce FJ, Frank-lin MW, Drucker WR. Liver adenosine triphosphate (ATP) in hypoxia and hemorrhagic shock. J Trauma 1982; 22: 730-735 [PMID: 7120524]
25 Lee NM, Brady CW. Liver disease in pregnancy. World J Gastroenterol 2009; 15: 897-906 [PMID: 19248187]
26 Zimmermann P, Albäck T, Koskinen J, Vaalamo P, Tuimala R, Ranta T. Doppler flow velocimetry of the umbilical ar-tery, uteroplacental arteries and fetal middle cerebral artery in prolonged pregnancy. Ultrasound Obstet Gynecol 1995; 5: 189-197 [PMID: 7788494]
27 Rioseco AJ, Ivankovic MB, Manzur A, Hamed F, Kato SR, Parer JT, Germain AM. Intrahepatic cholestasis of pregnan-cy: a retrospective case-control study of perinatal outcome. Am J Obstet Gynecol 1994; 170: 890-895 [PMID: 8141222]
P- Reviewer: Furuhashi M S- Editor: Qi Y L- Editor: A E- Editor: Zheng XM
64 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Zhang XQ et al . More attention to fetus in ICP

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.65
World J Obstet Gynecol 2013 November 10; 2(4): 65-73ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Mirabegron, a novel, non-antimuscarinic drug for the overactive bladder: An up-to-dated review
Emilio Sacco, Riccardo Bientinesi
Emilio Sacco, Riccardo Bientinesi, Urologic Clinic, “Agostino Gemelli” Hospital, Catholic University Medical School of Rome, 00168 Rome, ItalyAuthor contributions: Sacco E wrote the paper; Bientinesi R contributed to literature review and drafting the manuscript.Correspondence to: Emilio Sacco, MD, PhD, Urologic Clinic, “Agostino Gemelli” Hospital, Catholic University Medical School of Rome, Largo F Vito 1, 00168 Rome, Italy. [email protected]: +39-6-30155290 Fax: +39-6-30155975Received: May 14, 2013 Revised: June 29, 2013Accepted: July 4, 2013Published online: November 10, 2013
AbstractMirabegron opened a new era in the treatment of over-active bladder (OAB). For the first time physicians deal-ing with OAB have an effective alternative to the phar-macological mainstay of the therapy for this disorder, the antimuscarinic drugs. This first-in-class, potent β3-adrenoceptors agonist has recently received approval by regulatory authorities in Japan, United States and Europe, based on the favourable efficacy-tolerability profile demonstrated in multiple randomized, multi-national, controlled trials, both short and long-term. There is substantial consistency through the studies in reporting the cardiovascular safety of treatment with mirabegron. The main advantage of mirabegron is the placebo-like incidence of classic adverse effects caused by antimuscarinics, dry mouth and constipation, that is expected to improve long-term adherence of patients to treatment. Mirabegron can be used in patients with contraindications to antimuscarinics and in those who discontinued previous antimuscarinic therapy. Herein, we reviewed the published literature on mirabegron, focusing on the rationale of β3-agonism for OAB treat-ment and on the preclinical and clinical evidence of ef-ficacy and safety available on this new pharmacological principle.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Mirabegron; β3-adrenoceptor agonist; Anti-muscarinics; Overactive bladder; Urinary incontinence
Core tip: Mirabegron is a first-in-class, potent β3-adreno-ceptors agonist that has been proven effective in the treatment of overactive bladder (OAB) based on mul-tiple randomized multinational trials. The safety-toler-ability profile of treatment with mirabegron has been extensively studied. The placebo-like incidence of classic adverse effects caused by antimuscarinics should im-prove long-term adherence to treatment with this new drug. Mirabegron can be an alternative in patients with contraindications to antimuscarinics or that discontinued previous antimuscarinic therapy. An updated review of the rationale of β3-agonism for OAB treatment and evi-dence of efficacy and safety of mirabegron is presented.
Sacco E, Bientinesi R. Mirabegron, a novel, non-antimuscarinic drug for the overactive bladder: An up-to-dated review. World J Obstet Gynecol 2013; 2(4): 65-73 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/65.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.65
INTRODUCTIONOveractive bladder (OAB) is a syndrome characterized by the key symptom of urinary urgency, with or without urinary incontinence, usually associated with urinary fre-quency and nocturia[1]. Detrusor muscle overactivity (DO) is often, but not always, the underlying condition[2]. The differential diagnosis with stress or mixed urinary incon-tinence, based on clinical examination and urodynamic investigations, is of utmost importance in order to plan the more appropriate therapeutic strategy[3].
The prevalence of OAB is high in western countries and increases with age[4]. This bothersome and multifac-
EDITORIAL
65 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Sacco E et al . Review on mirabegron for overactive bladder
torial bladder disorder that significantly impairs patient’s health-related quality of life (HRQL), is also associated to significant comorbidities[5] and high socioeconomic costs[6].
The treatment of OAB is aimed to achieve symptom relief and improvement of HRQL. First-line treatment relies mainly on lifestyle advice and bladder training, functional electrical stimulation, clean intermittent cathe-terization and pharmacological treatment. Neuromodula-tion, intradetrusor botulinum toxin injection and surgery represent more invasive, second-line treatment options.
Antimuscarinics are the mainstay in the pharmacologi-cal treatment of OAB[7]. However, these drugs are merely symptomatic and patients with unsatisfactory response due to lack of efficacy are frequent. Moreover, antimusca-rinics are not completely bladder-selective causing bother-some adverse effects (AEs), including dry-mouth, nausea, constipation and central nervous system AEs. Because of these limitations, long-term adherence to treatment with antimuscarinics is low[7-10].
The limitations of antimuscarinics prompted the research of novel pharmacological principles with a dis-tinct mechanism of action and aimed to improve bladder storage phase symptoms, without affecting the voiding phase, and with a better tolerability profile[11]. Among in-novative peripherally acting compounds, several selective β3-adrenoceptors (β3-ARs) agonists have undergone clinical proof-of-concept studies including ritobegron (also known as KUC-7483 and as KUC-7322 for its ac-tive metabolite), solabegron (also known as GW427353) and mirabegron (also known as YM178).
Mirabegron reached the final stages of pharmacologi-cal development and has been recently granted market-ing approval in Japan, United States (Myrbetriq™) and Europe (Betmiga™). The drug is formulated as Oral Controlled Absorption System (OCAS) tablets. OCAS is a hydrophilic gel-forming matrix tablet, a modified release system (also referred as extended-release or prolonged-re-lease) that allows a release of drug from the tablets for an extended period, with more steady absorption, and avoids high peak-to-trough fluctuations in plasma concentration and the considerable food effect of immediate-release formulations. The drug product is available in two dosage strengths of 50 mg (recommended to-be-marketed, once daily dose, orally with or without food) and 25 mg (for pa-tients with severe renal or moderate hepatic impairment).
Thereafter we reviewed experimental and clinical data on mirabegron by searching English-language full papers and abstracts published by May 2013 in MEDLINE, clinicaltrials.gov, controlled-trials.com, clinicaltrialsfeeds.org, and proceedings of international scientific meetings.
RATIONALE OF β3-AGONISM FOR OAB TREATMENTThe fixation of noradrenalin to β-ARs activates the molecular pathway of cyclic adenosine monophosphate (cAMP) that is the most important mediator of detrusor
muscle compliance and relaxation in mammalian spe-cies, although there is evidence suggesting that a cAMP-independent, potassium channels-mediated mechanism may play an important role[12-15].
β1-, β2- and β3-ARs have been demonstrated in both animal and human urinary bladder, although, β3-ARs rep-resent the far most abundant subtype in the human blad-der[16,17]. β3-ARs have been found to be highly and prefer-entially expressed on bladder tissues including urothelium, interstitial cells, and detrusor smooth muscle[12,18-21].
Detrusor muscle relaxes in response to β-AR agonists in a dose-dependent manner and human studies showed that this effect is mediated mainly through β3-AR[17,22-25]. Targeting β3-ARs has a significant effect on reducing spontaneous uncoordinated detrusor contractile activity in human bladder[23]. Interestingly, preliminary research showed that 49% of patients with idiopathic DO have a tryptophan 64 arginine mutation of the β3-AR gene that may be a useful genetic marker[26].
Animal studies demonstrated that both non-selective and selective β3-AR agonists were able to increase blad-der capacity and inhibit neurogenic or experimentally-induced DO and bladder outlet obstruction (BOO)-asso-ciated OAB, without changing voiding detrusor pressure or increasing residual volume[17,21,27-30].
Although β3-ARs on detrusor muscle cells were be-lieved to be the main site of action of β3-AR agonists in treating OAB, the main in vivo effect of these compounds could be on the afferent side of the micturition reflex, by a direct inhibition of afferent nerves or of the myogenic/urotheliogenic mechanisms involved in the promotion of afferent activity. In fact, there is evidence that selective β3-AR agonists can (1) inhibit the bladder filling-induced activity of mechanosensitive Aδ-fibers (and C-fibers at higher doses inducing retention) in rats[31], and (2) reduce autonomous bladder non-voiding contractions of myo-genic origin[27] that can generate localized microcontrac-tions facilitating afferent nerves activity[32]. It has been also reported that a direct influence on urothelial functions, such as the release of NO and urothelial-derived inhibi-tory factor, can contributes to the promotion of detrusor relaxation via the inhibition of C-fiber activity[33-35]. Finally, experiments in spinal cord transected rats showed that β3-AR agonists can directly inhibit bladder afferent activity[36].
As the main effect of β3-AR agonists in vivo remains unclear, so the detailed mechanism of action by which these drugs exert their beneficial effect in DO and OAB has not been completely established and further studies are needed. However, taken together, the available experi-mental evidence supports β3-AR agonism as a novel phar-macological principle intended for the treatment of OAB, including storage symptoms secondary to BOO[37,38].
PRECLINICAL EVIDENCE ON MIRABEGRONMirabegron is a novel, once-daily, orally active, first-in-class, potent and selective β3-AR agonist. Cellular studies
66 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

showed that mirabegron stimulates the intracellular cAMP accumulation by acting with full agonistic activity and high efficacy on human β3-ARs; on the other hand, its efficacy on β1- and β2-ARs was very low (446 times less selective for these receptors in Chinese hamster ovary cells)[30,39].
Affinity for human β3-AR did not appear to be al-tered by several gene variants of the receptor[40]. Studies on isolated strips of human detrusor muscle demonstrat-ed an efficacy of mirabegron comparable to that of iso-prenaline, a non-selective β3-AR agonist[30]; this efficacy of mirabegron was maintained in isolated detrusor strips obtained from control patients and patients with BOO or BOO-associated DO[41]. More interestingly, mirabegron induced a dose-dependent reduction of the frequency of rhythmic bladder contractions when given intravenously to urethane-anesthetized rats; however, unlike anticolin-ergics, it did not significantly decrease the contraction amplitude[30]. In rat model of bladder dysfunctions, mi-rabegron was effective in improving storage-phase uro-dynamic parameters, without affecting voiding-phase pa-rameters, such as micturition pressure, threshold pressure and residual volume; this pharmacological profile should decrease the risk of causing urinary retention[39,42,43]. While mirabegron reduced the frequency of non-voiding bladder contractions, anticolinergics mainly reduced their amplitude[44].
In vivo experiments also showed that, during bladder filling, mirabegron can directly inhibit in a dose-dependent manner the mechanosensitive bladder afferent nerves fir-ing of both Aδ- and C-fibers, that was more remarkable for Aδ-fibers[45]; in this study, mirabegron also inhibited both bladder microcontractions and Aδ-fibers activity at doses that do not decrease bladder pressure, suggesting a possible additional action of β3-AR agonists as therapeu-tic agents for OAB or other bladder sensory disorders.
The aforementioned findings prompted several trials aimed to investigate efficacy, safety, tolerability and dis-continuation rate of mirabegron in the clinical setting of OAB patients. In particular, the development of mirabe-gron by Astellas Pharma Inc. (Ibaraki, Japan) involved an extensive clinical development and clinical pharmacology programs including 41 studies[46].
CLINICAL EVIDENCE OF EFFICACYProof-of-concept and dose-finding studiesMirabegron has been extensively studied in more than 10000 individuals and about 40 clinical studies have been performed over the last 10 years. Safety and efficacy in OAB patients were evaluated in 5 global, 12-wk trials: two phase Ⅱ (Clinicaltrials.gov number: NCT01604928 and NCT00337090) and three pivotal phase Ⅲ (NCT00689104, NCT00662909, NCT00912964) studies that compared mirabegron with placebo and with tolterodine (a com-monly prescribed oral anti-muscarinic agent). A further safety study (NCT00688688) evaluated long-term (12 mo) results.
A proof-of-concept, randomized, double-blind, paral-
lel group, phase Ⅱa dose-ranging trial (BLOSSOM trial, NCT01604928) was conducted in six European countries including 260 OAB patients that were assigned to four treatment arms: placebo (n = 66), mirabegron 100 mg bid (n = 65), mirabegron 150 mg bid (n = 65), and tolterodine 4 mg extended-release (ER) once-daily (n = 64), for a 4-wk period[47]. With regard to mean micturition frequency, mirabegron was significantly superior to placebo and tolt-erodine: 2.2 micturitions/24 h vs 1.2 micturitions/24 h for both doses (adjusted P ≤ 0.01 for both comparisons). Compared with placebo, mirabegron was also superior with respect to mean volume voided per micturition, mean number of incontinence episodes, nocturia epi-sodes, urgency incontinence episodes, urgency episodes per 24 h and HRQL variables. No difference in efficacy was observed between the 100 and 150 mg twice-daily doses, leading to the conclusion that a total daily dose of 200 mg provides maximum therapeutic efficacy.
An European, dose-finding, phase Ⅱb randomized trial (DRAGON trial, NCT00337090) enrolled 919 OAB patients (mean age 57.2 years, 89.3% female) assigned to six study arms: placebo (n = 166), mirabegron 25 mg (n = 167), 50 mg (n = 167), 100 mg (n = 168), 200 mg (n = 166) and tolterodine 4 mg ER (n = 85), for a 12-wk pe-riod[48]. In this study a once-daily OCAS formulation of mirabegron was used. Statistically significant, dose-de-pendent reductions in the mean number of micturitions per 24 h (primary endpoint) were seen with mirabegron 50 (-2.1), 100 (-2.1) and 200 (-2.2) mg, compared with placebo (-1.4). Mirabegron significantly increased mean volume voided per micturition and decreased mean num-ber of urgency and urgency incontinence episodes per 24 h, level of urgency (at doses of 100 and 200 mg) and nocturia episodes (at doses of 50 mg): about half of the incontinent patients in each mirabegron group was dry at the end of treatment. Similarly to previous studies evalu-ating antimuscarinics[49], the difference in response vs pla-cebo was evident after 1 wk of treatment and the maxi-mum effect was achieved and sustained from 8 to 12 wk. Although the study was not powered for head-to-head comparison with tolterodine, the authors observed that the magnitude of improvements in efficacy outcomes in the mirabegron groups was within the same range as that of the tolterodine group.
Randomized large-scale pivotal trialsBased on the aforementioned results, three subsequent large-scale, phase Ⅲ, randomized studies were conducted by Astellas (Table 1)[50-52]. Efficacy analyses of these stud-ies were based on two co-primary efficacy endpoints: (1) the change from baseline to endpoint in the mean num-ber of incontinence episodes per 24 h; and (2) the mean change from baseline to endpoint in the mean number of micturitions per 24 h.
An European-Australian multicentre, randomised, double-blind, parallel-group, placebo and active controlled phase Ⅲ trial (SCORPIO trail, NCT00689104) enrolled 1978 OAB patients (mean age 59.1 years, 72.2% female)
67 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Sacco E et al . Review on mirabegron for overactive bladder

that were assigned to four arms: placebo, mirabegron 50 mg, mirabegron 100 mg or tolterodine slow-release (SR) 4 mg once-daily, for a 12-wk period (Table 1)[50]. Compared to placebo, statistically significant reductions were observed with 50 and 100 mg of mirabegron in both co-primary efficacy measures. Although improve-ments in both co-primary endpoints were also observed with tolterodine SR, they did not reach statistical sig-nificance. Compared with placebo, all active treatment groups achieved statistically significant improvements from baseline in mean volume voided per micturition; the mirabegron 50 mg group achieved a statistically significant improvement also in the mean number of episodes with urgency (grade 3 or 4) per 24 h. No statistical comparison with tolterodine SR was performed in this study, however the magnitude of effect with mirabegron was at least as good as that observed with tolterodine SR.
Another multicentre, randomised, double-blind, paral-lel-group, placebo-controlled phase Ⅲ trial (ARIES trial, NCT00662909) was conducted in the United States and Canada[51]. This study enrolled 1328 OAB patients (mean age 60.1 years, 74.3% female) randomly assigned to three treatment arms: placebo, mirabegron 50 mg, mirabegron 100 mg once-daily, for a 12-wk period (Table 1). Com-pared to placebo, statistically significant decreases from baseline were observed with 50 and 100 mg mirabegron in the number of incontinence episodes and in the number of micturitions per 24 h. Significantly greater improve-ments vs placebo were observed for both mirabegron treatment groups also in mean level of urgency, mean number of urgency incontinence episodes per 24 h, mean number of urgency episodes (grade 3 or 4) per 24 h and mean number of nocturia episodes per 24 h.
The third pivotal phase Ⅲ study is an European-North American, randomized, double-blind, placebo-controlled trial (CAPRICORN trial, NCT00912964), including 1306 eligible patients (mean age 59.0 years, 68.7% female) randomly assigned to receive placebo, mirabegron 25 mg or mirabegron 50 mg, for a 12-wk period (Table 1). The
results of this trial, submitted to regulatory authorities by Astellas and presented as meeting abstract, are still un-published in peer-review journals[52]. Both mirabegron 25 and 50 mg groups demonstrated statistically significant improvements for the co-primary efficacy endpoints, providing evidence that the lower dose also results in a clinically meaningful benefit, although greater efficacy was observed with mirabegron 50 mg.
Recently, a pooled analysis of data from the above-mentioned three pivotal randomised phase Ⅲ studies has been reported as abstract; the efficacy of mirabegron (50 or 100 mg) was compared with placebo (Table 1)[53]. This pooled analysis demonstrated similar statistically significant and clinically meaningful improvements for mirabegron 50 and 100 mg compared with placebo based on co-primary efficacy endpoints; the reduction with mirabegron of the micturition frequency per 24 h and the number of incontinence episodes per 24 h compared with placebo was of about 0.55 and 0.40, respectively.
Long-term efficacy dataA multinational randomised, double-blind, parallel group, active-controlled, phase Ⅲ trial has been conducted in North America, Europe and other countries (TAURUS trial, NCT00688688) assessing long-term safety (primary outcome) and efficacy of mirabegron. In this study 2444 OAB patients were randomised to three study arms: mi-rabegron 50 mg (n = 812) and 100 mg (n = 820) and tolt-erodine SR 4 mg (n = 812), once daily for 12 mo[54]. The study was not designed to demonstrate a statistically sig-nificant difference in efficacy between treatment groups and was not placebo-controlled. The authors reported that, for both doses of mirabegron, improvements in OAB symptoms were observed by month 1 and were maintained throughout the follow-up period, as mea-sured by the change from baseline for mean number of micturitions per 24 h, mean number of incontinence epi-sodes per 24 h and mean volume voided/micturition[54]. Overall, data from this safety study provide evidence
68 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Coprimary efficacy variables in 12-wk phase Ⅲ pivotal randomized controlled trials
Trials Patients (n ) Arms (n ) Change from baseline in incontinence episodes/d1 (FAS-I)
Change from baseline in micturitions/d1 (FAS)
Ref.
SCORPIO 1978 Placebo (494) -1.17 -1.34 [50]Mirabegron 50 mg (493) -1.57a -1.93a
Mirabegron 100 mg (496) -1.46a -1.77a
Tolterodine 4 mg ER (495) -1.27 (NS) -1.59 (NS)ARIES 1328 Placebo (454) -1.13 -1.05 [51]
Mirabegron 50 mg (442) -1.47a -1.66a
Mirabegron 100 mg (433) -1.63a -1.75a
CAPRICORN 1302 Placebo (433) - - [52]Mirabegron 25 mg (433) -0.40a -0.47a
Mirabegron 50 mg (440) -0.42a -0.42a
Pooled analysis 3542 Placebo (1328) -1.10 -1.20 [53]Mirabegron 50 mg (1324) -1.49a -1.75a
Mirabegron 100 mg (890) -1.50a -1.74a
aP < 0.05 vs placebo. 1Mean adjusted changes from baseline to final visit. FAS: Full analysis set; FAS-I: Full analysis set-incontinence (all FAS patients with ≥ incontinence grade at baseline); NS: Not significant; ER: Extended release.
Sacco E et al . Review on mirabegron for overactive bladder

demonstrating the durability of effect for mirabegron in the treatment of OAB and support the results of previ-ous studies showing that the β3-AR, unlike other β-AR subtypes, is not prone to desensitization[55].
QUALITY OF LIFE MEASURES AND TREATMENT SATISFACTIONIn the DRAGON trial[48], the International Consulta-tion on Incontinence Questionnaire-Overactive Bladder (ICIQ-OAB) and the ICIQ-OABqol questionnaires were used for HRQL assessment. Dose-dependent improve-ments from baseline to the end of treatment were ob-served with the ICIQ-OAB questionnaire and were sta-tistically significant vs placebo for all mirabegron groups. Improvements from baseline to the end of treatment were also observed with the ICIQ-OABqol questionnaire, although only the comparison between the mirabegron 200-mg group and placebo was statistically significant. Patient-reported benefit was also evaluated with the ques-tion “has the treatment been of any benefit to you?” (“no”, “yes, a little”, or “yes, very much”). The percent-age of patients classified as “responders” (improvement of ≥ 1 category from baseline) at the end of treatment was 59.0%, 65.0%, 65.8% and 70.8% for the mirabegron 25-mg, 50-mg, 100-mg, and 200-mg groups, respectively, compared with 51% for placebo and 55% of the toltero-dine groups.
All three active treatment groups (mirabegron 50 and 100 mg, tolterodine ER 4 mg) demonstrated a statistically significant improvement from baseline to final visit com-pared with placebo on the three HRQL measures used in the SCORPIO trial[50]: OAB-Questionnaire (OAB-q), Patient Perception of Bladder Condition (PPBC), and Treatment Satisfaction-Visual Analog Scale (TS-VAS).
These results were replicated in the ARIES trial[51]; both mirabegron treatment groups demonstrated signifi-cantly greater improvements from baseline to final visit vs placebo in OAB-q (symptom bother, HRQL total score and dimensions of coping, concern and sleep), TS-VAS and PPBC.
In the CAPRICORN trial both mirabegron groups (25 and 50 mg) demonstrated statistically significant improve-ments vs placebo for the TS-VAS; for the OAB-q, the mirabegron 50 mg group demonstrated statistically sig-nificant improvements vs placebo in the Symptom Bother scale[52].
Long-term data on both doses of mirabegron, 50 and 100 mg, also showed numerical improvements on the OAB-q (symptom bother and HRQL total score), PPBC scale, and TS-VAS, similar to those seen using a well-established antimuscarinic treatment for OAB[54].
SUBPOPULATION ANALYSESClinical data in specific subpopulations of OAB patients are still scant in published literature.
With regard to the influence of gender, it must be
noted that most of patients enrolled in phase Ⅲ trials were females and limited data are available on the ef-ficacy of mirabegron in males, especially in those with benign prostatic hyperplasia (BPH). A non-randomized study, focusing on males, reported that mirabegron was effective in male patients with OAB and improved not only OAB symptoms, but also voiding symptoms in BPH men, without increasing post-voiding residual urine[56]. In this study, with a small number of participants, a greater improvement of urgency urinary incontinence based on OAB Symptom Questionnaire was observed in BPH patients treated with α1-blocker compared to those not treated with α1-blocker, suggesting that combining mirabegron with α1-blocker might benefit males with wet OAB. Accordingly, pooled pivotal trial efficacy data reported by the FDA showed that mirabegron 50 mg and 100 mg were effective for both male and female subjects, although a larger reduction vs placebo in mean number of incontinence episodes was observed in female subjects compared to male subjects; however, it was suggested that this observation could be due to a lower baseline lev-el of incontinence in males, overlapping symptomatology with male co-morbid conditions (e.g., BPH), increased mirabegron exposure in females, or some combination of all 3 factors[57]. The same document reports that mirabe-gron 50 and 100 mg did not appear effective in decreas-ing the mean number of incontinence episodes in men with BPH[57]. In a phase Ⅱ, double-blind, parallel-group, placebo-controlled urodynamic study (NCT00410514) including 200 men with LUTS and BOO, Nitti et al[58] re-ported that 50 and 100 mg mirabegron do not adversely affect Qmax, detrusor pressure at Qmax and bladder con-tractility index, and are well tolerated in these patients. However, because of the limited number of men with BPH included in available studies, it is not possible to draw meaningful conclusions.
A non-randomized, active-controlled study reported that mirabegron is effective for those whose OAB is unresponsive to antimuscarinic drugs, although its ef-fectiveness was less in these patients compared to newly diagnosed OAB patients[56]. In this study, 38.4% of OAB patients did not respond to mirabegron as well as to anti-muscarinics; as noted by the authors, this subject deserves further elucidation. Accordingly, a post-hoc analysis of the SCORPIO trial[59] showed that both mirabegron 50 and 100 mg once-daily were effective in improving both mean number of incontinence episodes and micturitions per 24 h vs placebo, not only in antimuscarinic-treatment-naïve patients but also in those patients who failed prior OAB antimuscarinic therapy, regardless of the reason for discontinuation.
With regard to the effect of the age, the pooled data from the three pivotal randomised studies were analysed in the OAB population aged ≥ 65 years in order to in-vestigate the benefit of mirabegron in elderly OAB pa-tients[60]. Approximately 38% of patients were ≥ 65 years of age (placebo n = 504; mirabegron 50 mg n = 499; mi-rabegron 100 mg n = 340). Mirabegron 50 and 100 mg re-
69 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Sacco E et al . Review on mirabegron for overactive bladder

sulted in reduction in incontinence episodes per 24 h and micturitions per 24 h in patients ≥ 65 years of age, with an adjusted mean difference vs placebo of -0.66 and -0.68, respectively, and of -0.62 and -0.75, respectively. These re-sults are of great value, given the increasing prevalence of OAB with age and the common adverse events associated with antimuscarinics in the aging population[7].
SAFETY, TOLERABILITY AND DISCONTINUATION There is substantial consistency through the studies in reporting safety and tolerability of treatment with mira-begron.
Despite a small increase in pulse rate, mirabegron demonstrated good safety and tolerability in the BLOS-SOM trial[47]. An incidence of treatment-emergent adverse effects (TEAEs) of 39.2% with mirabegron vs 36.4% with placebo and 48.4% with tolterodine has been re-ported. AEs in the mirabegron group were mild or mod-erate in intensity, the most commonly reported class of TEAEs being gastrointestinal disorders (13.8%), followed by headache (6.9%), with a lower incidence compared to tolterodine group (23.4%, 9.4%, respectively). Treatment-related dizziness and palpitations were more common with mirabegron compared to placebo and tolterodine. Of note, no episodes of acute urinary retention were re-ported. Discontinuation rates due to AEs were 4.6% and 7.7% with mirabegron 100 and 150 mg, respectively, 1.5% with placebo and 3.1% with tolterodine.
In the DRAGON trial, one or more TEAEs were reported by 43.8%-47.9% of patients in the mirabegron groups (25, 50, 100 and 200 mg) vs 43.2% in the placebo group[48]. Again, the most common reported TEAEs were gastrointestinal disorders (7.2%-8.3% with mirabegron vs 5.3% with placebo), including constipation, dry mouth, dyspepsia and nausea. Of note, the incidence of dry mouth, reported to be an important factor for determin-ing persistence with antimuscarinic agents[10], was higher with tolterodine ER 4 mg (3.5%) than with mirabegron (1.8% to 3.0%, depending on dose). Again, no episodes of acute urinary retention were reported with mirabegron. A statistically significant, dose-dependent increase from baseline in mean pulse rate vs placebo was detected with 100 and 200 mg mirabegron (1.6 and 4.1 bpm, respec-tively, AM; 2.7 and 4.7 bpm PM); however, this change in pulse rate was not associated with an increase in car-diovascular AEs and no differences between treatment groups were observed in ECG parameters and blood pressure. Discontinuation owing to AEs was low at 3.0% with placebo, 2.4%-5.3% with mirabegron, and 1.2% with tolterodine.
An incidence of TEAEs similar across the placebo, mirabegron 50 mg, mirabegron 100 mg, and tolterodine SR groups (43.3%, 42.8%, 40.1% and 46.7%, respec-tively) was reported in the SCORPIO trial[50]. The most common TEAEs in this study were hypertension (7.7%, 5.9%, 5.4% and 8.1%), dry mouth (2.6%, 2.8%, 2.8%
and 10.1%), headache (2.8%, 3.7%, 1.8% and 3.6%), and nasopharyngitis (1.6%, 2.8%, 2.8% and 2.8%). At the final visit, mirabegron was associated with small dose-dependent, not clinically meaningful increases in pulse rates compared with placebo, that were similar to those seen with tolterodine; the overall incidence of adjudicated cardiovascular events was similar in placebo- and mirabe-gron-treated patients, and slightly higher in tolterodine-treated patients. The discontinuation rate owing to TEAE was low, at 2.6%, 4.9%, 3.2%, and 4.4%, respectively.
The ARIES trial[51] confirmed a similar incidence of TEAEs across placebo, mirabegron 50 mg and 100 mg groups (50.1%, 51.6% and 46.9%, respectively). In this study, the incidence of hypertension was 6.6%, 6.1% and 4.9%, and headache 2.0%, 3.2% and 3.0% in the placebo, mirabegron 50 mg and 100 mg groups, respectively. An increase incidence of urinary tract infections was noted with mirabegron 50 mg (12%) and 100 mg (16%), com-pared with placebo (8%). Changes in laboratory assess-ments, vital signs, physical examination, ECG and post-void residual volume were small and consistent across treatment groups. No AEs of QTc prolongation and no proarrhythmic events were observed. Discontinuation rates due to AEs were 3.8%, 4.1% and 4.4% in the pla-cebo, mirabegron 50 mg and 100 mg groups.
In the CAPRICORN trial, common TEAEs included hypertension in 5.3%, 6.9%, and 7.0%, and headache in 2.1%, 0.9% and 0.9%, in the placebo, mirabegron 25 mg and mirabegron 50 mg groups, respectively[52].
In compliance with abovementioned studies, long-term safety and tolerability have been confirmed by the results of the TAURUS trial (Table 2)[54]. The most fre-quent TEAEs were hypertension, dry mouth, constipa-tion and headache, which occurred at a similar incidence across all treatment groups, while the incidence of dry mouth was more than three fold higher in the tolterodine group. A higher incidence of neoplasms (benign, ma-lignant, and unspecified including cysts and polyps) was seen in the mirabegron 100 mg group (1.3%) compared with mirabegron 50 mg (0.1%) or tolterodine ER 4 mg (0.5%), but was not considered to be treatment-related. Discontinuations due to AEs were comparable across treatment groups, occurring in only 6.4%, 5.9%, and 6.0% of patients on mirabegron 50 mg, mirabegron 100 mg, and tolterodine ER 4 mg, respectively.
ONGOING STUDIES AND AWAITED RESULTSSeveral studies are ongoing in order to evaluate efficacy and safety of mirabegron in selected groups of patients or in comparison with other drugs. Some of these stud-ies are still recruiting patients, while others have been completed and their results should be published on peer-review journals. Many studies are also ongoing focusing on several pharmacokinetic features of mirabegron and pharmacological interactions.
A randomized, phase Ⅱ, double-blind, factorial, paral-
70 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Sacco E et al . Review on mirabegron for overactive bladder

71 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
lel-group, active and placebo-controlled, multicenter, dose-ranging study (SYMPHONY trial, NCT01340027) has been conducted to evaluate efficacy, safety and tolerability of six dose combinations of solifenacin and mirabegron compared to mirabegron and solifenacin monotherapies in the treatment of OAB.
The BEYOND trial (NCT01638000) is an ongoing double-blind, randomized, multi-center, phase Ⅲ study of mirabegron vs solifenacin in 1692 subjects with OAB treated with antimuscarinics and dissatisfied due to lack of efficacy.
A post-marketing study (NCT01745094) is recruiting patients in order to evaluate safety and efficacy of con-comitant use (add-on-therapy) of mirabegron in patients with OAB under treatment with solifenacin.
CONCLUSIONAfter 30 years of predomination of antimuscarinics, a new compound, with a novel mechanism of action, is for the first time available in the pharmacological armamen-tarium aimed to treat OAB. Mirabegron has proven ef-fective across multiple randomized controlled trials, both short and long-term, and showed a favourable safety profile with a placebo-like dry mouth incidence. Mirabe-
gron can be used for patients with contraindications to antimuscarinics and its effectiveness has been confirmed in patients who discontinued previous antimuscarinic therapy. Although the tolerability profile of mirabegron offers the potential to improve adherence to OAB treat-ment, this optimal efficacy-tolerability balance is to be demonstrated in clinical real-world every day practice.
REFERENCES1 Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten
U, van Kerrebroeck P, Victor A, Wein A. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Con-tinence Society. Neurourol Urodyn 2002; 21: 167-178 [PMID: 11857671 DOI: 10.1002/nau.10052]
2 Sacco E. [Physiopathology of overactive bladder syndrome]. Urologia 2012; 79: 24-35 [PMID: 22287269]
3 Papatsoris AG, Chrisofos M, Antoniou N, Gekas A, Deliveli-otis C. An overview of stress urinary incontinence treatment in women. Aging Clin Exp Res 2007; 19: 334-340 [PMID: 17726366]
4 Irwin DE, Milsom I, Hunskaar S, Reilly K, Kopp Z, Her-schorn S, Coyne K, Kelleher C, Hampel C, Artibani W, Abrams P. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol 2006; 50: 1306-1314; discussion 1314-1315 [PMID: 17049716 DOI: 10.1016/j.eururo.2006.09.019]
5 Brown JS, McGhan WF, Chokroverty S. Comorbidities as-sociated with overactive bladder. Am J Manag Care 2000; 6: S574-S579 [PMID: 11183900]
6 Sacco E, Tienforti D, D’Addessi A, Pinto F, Racioppi M, To-taro A, D’Agostino D, Marangi F, Bassi P. Social, economic, and health utility considerations in the treatment of overac-tive bladder. Open Access J Urol 2010; 2: 11-24
7 Chapple CR, Khullar V, Gabriel Z, Muston D, Bitoun CE, Weinstein D. The effects of antimuscarinic treatments in over-active bladder: an update of a systematic review and meta-analysis. Eur Urol 2008; 54: 543-562 [PMID: 18599186 DOI: 10.1016/j.eururo.2008.06.047]
8 Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overac-tive bladder and how are they managed? A population-based prevalence study. BJU Int 2001; 87: 760-766 [PMID: 11412210 DOI: 10.1046/j.1464-410x.2001.02228.x]
9 D'Souza AO, Smith MJ, Miller LA, Doyle J, Ariely R. Persis-tence, adherence, and switch rates among extended-release and immediate-release overactive bladder medications in a regional managed care plan. J Manag Care Pharm 2008; 14: 291-301 [PMID: 18439051]
10 Wagg A, Compion G, Fahey A, Siddiqui E. Persistence with prescribed antimuscarinic therapy for overactive bladder: a UK experience. BJU Int 2012; 110: 1767-1774 [PMID: 22409769 DOI: 10.1111/j.1464-410X.2012.11023.x]
11 Sacco E, Pinto F, Bassi P. Emerging pharmacological targets in overactive bladder therapy: experimental and clinical evi-dences. Int Urogynecol J Pelvic Floor Dysfunct 2008; 19: 583-598 [PMID: 18196198 DOI: 10.1007/s00192-007-0529-z]
12 Andersson KE, Chapple CR, Cardozo L. Pharmacological treatment of urinary incontinence. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence, 4th International Consultation on Incontinence. Plymouth: Plymbridge Dis-tributors Ltd., 2009: 631-699
13 Frazier EP, Peters SL, Braverman AS, Ruggieri MR, Michel MC. Signal transduction underlying the control of urinary bladder smooth muscle tone by muscarinic receptors and beta-adrenoceptors. Naunyn Schmiedebergs Arch Pharma-col 2008; 377: 449-462 [PMID: 18060543 DOI: 10.1007/
MedDRA (v.9.1), preferred term
Mirabegron 50 mg
(n = 812)
Mirabegron 100 mg
(n = 820)
Tolterodine ER 4 mg
(n = 812)
Any AE 485 (59.7) 503 (61.3) 508 (62.6)Hypertension 75 (9.2) 80 (9.8) 78 (9.6)Urinary tract infection 48 (5.9) 45 (5.5) 52 (6.4)Dry mouth 23 (2.8) 19 (2.3) 70 (8.6)Nasopharyngitis 32 (3.9) 35 (4.3) 25 (3.1)Headache 33 (4.1) 26 (3.2) 20 (2.5)Influenza 21 (2.6) 25 (3.0) 28 (3.4)Constipation 23 (2.8) 25 (3.0) 22 (2.7)Back pain 23 (2.8) 29 (3.5) 13 (1.6)Dizziness 22 (2.7) 13 (1.6) 21 (2.6)Diarrhea 15 (1.8) 24 (2.9) 16 (2.0)Sinusitis 22 (2.7) 18 (2.2) 12 (1.5)Arthralgia 17 (2.1) 19 (2.3) 16 (2.0)Tachycardia 8 (1.0) 19 (2.3) 25 (3.1)Cystitis 17 (2.1) 11 (1.3) 19 (2.3)Adverse events of interest Corrected QT interval prolongation2
3 (0.4) 2 (0.2) 3 (0.4)
Hypertension2 89 (11.0) 83 (10.1) 86 (10.6) Cardiac arrhythmia2 32 (3.9) 34 (4.1) 49 (6.0) Urinary retention 1 (0.1) 1 (0.1) 3 (0.4) Acute urinary retenction 0 1 (0.1) 1 (0.1) Hypersensitivity 45 (5.5) 44 (5.4) 42 (5.2) Sincope/seizure 1 (0.1) 0 1 (0.1) Hepatotoxicity2 17 (2.1) 19 (2.3) 15 (1.8)
Table 2 Most frequent (> 2% in any treatment group) treat-ment emergent adverse events and adverse events of interest1 n (%)
1In the safety analysis set; 2Definition based on standardized medical dictionary for regulatory activities (MedDRA) query. Adverse event not based on standardized MedDRA queries were predefined. Reprinted from reference[54], with permission. AE: Adverse Event; ER: Extended release.
Sacco E et al . Review on mirabegron for overactive bladder

72 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
s00210-007-0208-0]14 Hudman D, Elliott RA, Norman RI. K(ATP) channels medi-
ate the beta(2)-adrenoceptor agonist-induced relaxation of rat detrusor muscle. Eur J Pharmacol 2000; 397: 169-176 [PMID: 10844111 DOI: 10.1016/S0014-2999(00)00229-6]
15 Uchida H, Shishido K, Nomiya M, Yamaguchi O. Involve-ment of cyclic AMP-dependent and -independent mecha-nisms in the relaxation of rat detrusor muscle via beta-adrenoceptors. Eur J Pharmacol 2005; 518: 195-202 [PMID: 16054622 DOI: 10.1016/j.ejphar.2005.06.029]
16 Takeda M, Obara K, Mizusawa T, Tomita Y, Arai K, Tsutsui T, Hatano A, Takahashi K, Nomura S. Evidence for beta3-adrenoceptor subtypes in relaxation of the human urinary bladder detrusor: analysis by molecular biological and pharmacological methods. J Pharmacol Exp Ther 1999; 288: 1367-1373 [PMID: 10027879]
17 Nomiya M, Yamaguchi O. A quantitative analysis of mRNA expression of alpha 1 and beta-adrenoceptor subtypes and their functional roles in human normal and obstructed blad-ders. J Urol 2003; 170: 649-653 [PMID: 12853849]
18 Andersson KE, Arner A. Urinary bladder contraction and re-laxation: physiology and pathophysiology. Physiol Rev 2004; 84: 935-986 [PMID: 15269341 DOI: 10.1152/physrev.00038.2003]
19 Limberg BJ, Andersson KE, Aura Kullmann F, Burmer G, de Groat WC, Rosenbaum JS. β-Adrenergic receptor subtype expression in myocyte and non-myocyte cells in human female bladder. Cell Tissue Res 2010; 342: 295-306 [PMID: 20953633 DOI: 10.1007/s00441-010-1053-x]
20 Otsuka A, Shinbo H, Matsumoto R, Kurita Y, Ozono S. Ex-pression and functional role of beta-adrenoceptors in the hu-man urinary bladder urothelium. Naunyn Schmiedebergs Arch Pharmacol 2008; 377: 473-481 [PMID: 18311486 DOI: 10.1007/s00210-008-0274-y]
21 Fujimura T, Tamura K, Tsutsumi T, Yamamoto T, Nakamura K, Koibuchi Y, Kobayashi M, Yamaguchi O. Expression and possible functional role of the beta3-adrenoceptor in human and rat detrusor muscle. J Urol 1999; 161: 680-685 [PMID: 9915482]
22 Badawi JK, Uecelehan H, Hatzinger M, Michel MS, Hafer-kamp A, Bross S. Relaxant effects of beta-adrenergic agonists on porcine and human detrusor muscle. Acta Physiol Scand 2005; 185: 151-159 [PMID: 16168009 DOI: 10.1111/j.1365-201X.2005.01474.x]
23 Biers SM, Reynard JM, Brading AF. The effects of a new se-lective beta3-adrenoceptor agonist (GW427353) on spontane-ous activity and detrusor relaxation in human bladder. BJU Int 2006; 98: 1310-1314 [PMID: 17026593 DOI: 10.1111/j.1464-410X.2006.06564.x]
24 Igawa Y, Yamazaki Y, Takeda H, Hayakawa K, Akahane M, Ajisawa Y, Yoneyama T, Nishizawa O, Andersson KE. Functional and molecular biological evidence for a pos-sible beta3-adrenoceptor in the human detrusor muscle. Br J Pharmacol 1999; 126: 819-825 [PMID: 10188996 DOI: 10.1038/sj.bjp.0702358]
25 Igawa Y, Michel MC. Pharmacological profile of β3-adrenoceptor agonists in clinical development for the treat-ment of overactive bladder syndrome. Naunyn Schmiedebergs Arch Pharmacol 2013; 386: 177-183 [PMID: 23263450 DOI: 10.1007/s00210-012-0824-1]
26 Yamaguchi O. Beta3-adrenoceptors in human detrusor muscle. Urology 2002; 59: 25-29 [PMID: 12007519]
27 Woods M, Carson N, Norton NW, Sheldon JH, Argent-ieri TM. Efficacy of the beta3-adrenergic receptor agonist CL-316243 on experimental bladder hyperreflexia and detru-sor instability in the rat. J Urol 2001; 166: 1142-1147 [PMID: 11490313]
28 Kaidoh K, Igawa Y, Takeda H, Yamazaki Y, Akahane S, Mi-yata H, Ajisawa Y, Nishizawa O, Andersson KE. Effects of selective beta2 and beta3-adrenoceptor agonists on detrusor hyperreflexia in conscious cerebral infarcted rats. J Urol 2002;
168: 1247-1252 [PMID: 12187276]29 Hicks A, McCafferty GP, Riedel E, Aiyar N, Pullen M,
Evans C, Luce TD, Coatney RW, Rivera GC, Westfall TD, Hieble JP. GW427353 (solabegron), a novel, selective beta3-adrenergic receptor agonist, evokes bladder relaxation and increases micturition reflex threshold in the dog. J Pharmacol Exp Ther 2007; 323: 202-209 [PMID: 17626794 DOI: 10.1124/jpet.107.125757]
30 Takasu T, Ukai M, Sato S, Matsui T, Nagase I, Maruyama T, Sasamata M, Miyata K, Uchida H, Yamaguchi O. Ef-fect of (R)-2-(2-aminothiazol-4-yl)-4’-{2-[(2-hydroxy-2-phenylethyl)amino]ethyl} acetanilide (YM178), a novel selective beta3-adrenoceptor agonist, on bladder function. J Pharmacol Exp Ther 2007; 321: 642-647 [PMID: 17293563 DOI: 10.1124/jpet.106.115840]
31 Aizawa N, Igawa Y, Nishizawa O, Wyndaele JJ. Effects of CL316,243, a beta 3-adrenoceptor agonist, and intravesical prostaglandin E2 on the primary bladder afferent activity of the rat. Neurourol Urodyn 2010; 29: 771-776 [PMID: 19816919 DOI: 10.1002/nau.20826]
32 Drake MJ, Harvey IJ, Gillespie JI, Van Duyl WA. Localized contractions in the normal human bladder and in urinary urgency. BJU Int 2005; 95: 1002-1005 [PMID: 15839921]
33 Murakami S, Chapple CR, Akino H, Sellers DJ, Chess-Williams R. The role of the urothelium in mediating bladder responses to isoprenaline. BJU Int 2007; 99: 669-673 [PMID: 17407521 DOI: 10.1111/j.1464-410X.2005.05455.x]
34 Yamaguchi O, Chapple CR. Beta3-adrenoceptors in urinary bladder. Neurourol Urodyn 2007; 26: 752-756 [PMID: 17600372 DOI: 10.1002/nau.20420]
35 Birder LA, Apodaca G, De Groat WC, Kanai AJ. Adrenergic- and capsaicin-evoked nitric oxide release from urothelium and afferent nerves in urinary bladder. Am J Physiol 1998; 275: F226-F229 [PMID: 9691011]
36 Kanai A, Wyndaele JJ, Andersson KE, Fry C, Ikeda Y, Zab-barova I, De Wachter S. Researching bladder afferents-deter-mining the effects of β(3) -adrenergic receptor agonists and botulinum toxin type-A. Neurourol Urodyn 2011; 30: 684-691 [PMID: 21661014 DOI: 10.1002/nau.21102]
37 Sacco E, Pinto F, Tienforti D, Marangi F, Destito A, Racioppi M, Gardi M, Volpi A, Bassi PF. [Investigational drug therapies for overactive bladder syndrome: the potential alternatives to anticolinergics.] Urologia 2009; 76: 161-177 [PMID: 21086288]
38 Igawa Y, Aizawa N, Homma Y. Beta3-adrenoceptor agonists: pos-sible role in the treatment of overactive bladder. Korean J Urol 2010; 51: 811-818 [PMID: 21221199 DOI: 10.4111/kju.2010.51.12.811]
39 Hatanaka T, Ukai M, Watanabe M, Someya A, Ohtake A, Su-zuki M, Ueshima K, Sato S, Sasamata M. In vitro and in vivo pharmacological profile of the selective β3-adrenoceptor agonist mirabegron in rats. Naunyn Schmiedebergs Arch Pharmacol 2013; 386: 247-253 [PMID: 23239087 DOI: 10.1007/s00210-012-0821-4]
40 Vrydag W, Alewijnse AE, Michel MC. Do gene polymor-phisms alone or in combination affect the function of hu-man beta3-adrenoceptors? Br J Pharmacol 2009; 156: 127-134 [PMID: 19133996 DOI: 10.1111/j.1476-5381.2008.00014.x]
41 Svalø J, Nordling J, Bouchelouche K, Andersson KE, Korstanje C, Bouchelouche P. The novel β3-adrenoceptor agonist mirabegron reduces carbachol-induced contractile activ-ity in detrusor tissue from patients with bladder outflow obstruction with or without detrusor overactivity. Eur J Pharmacol 2013; 699: 101-105 [PMID: 23246623 DOI: 10.1016/j.ejphar.2012.11.060]
42 Hatanaka T, Ukai M, Watanabe M, Someya A, Ohtake A, Suzuki M, Ueshima K, Sato S, Kaku S. Effect of mirabe-gron, a novel β3-adrenoceptor agonist, on bladder function during storage phase in rats. Naunyn Schmiedebergs Arch Pharmacol 2013; 386: 71-78 [PMID: 23224420 DOI: 10.1007/s00210-012-0814-3]
43 Tyagi P, Tyagi V. Mirabegron, a β3-adrenoceptor agonist
Sacco E et al . Review on mirabegron for overactive bladder

73 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
for the potential treatment of urinary frequency, urinary incontinence or urgency associated with overactive bladder. IDrugs 2010; 13: 713-722 [PMID: 20878594]
44 Gillespie JI, Palea S, Guilloteau V, Guerard M, Lluel P, Korstanje C. Modulation of non-voiding activity by the mus-carinergic antagonist tolterodine and the β(3)-adrenoceptor agonist mirabegron in conscious rats with partial outflow ob-struction. BJU Int 2012; 110: E132-E142 [PMID: 22734512 DOI: 10.1111/j.1464-410X.2012.11240.x]
45 Aizawa N, Homma Y, Igawa Y. Effects of mirabegron, a novel β3-adrenoceptor agonist, on primary bladder affer-ent activity and bladder microcontractions in rats compared with the effects of oxybutynin. Eur Urol 2012; 62: 1165-1173 [PMID: 22981677 DOI: 10.1016/j.eururo.2012.08.056]
46 Sacco E, Bientinesi R. Mirabegron: a review of recent data and its prospects in the management of overactive bladder. Ther Adv Urol 2012; 4: 315-324 [PMID: 23205058 DOI: 10.1177/1756287212457114]
47 Chapple CR, Amarenco G, López Aramburu MA, Everaert K, Liehne J, Lucas M, Vik V, Ridder A, Snijder R, Yamaguchi O; on behalf of the BLOSSOM Investigator Group. A proof-of-concept study: Mirabegron, a new therapy for overactive bladder. Neurourol Urodyn 2013; Epub ahead of print [PMID: 23424164 DOI: 10.1002/nau.22373]
48 Chapple CR, Dvorak V, Radziszewski P, Van Kerrebroeck P, Wyndaele JJ, Bosman B, Boerrigter P, Drogendijk T, Ridder A, Van Der Putten-Slob I, Yamaguchi O. A phase II dose-rang-ing study of mirabegron in patients with overactive bladder. Int Urogynecol J 2013; 24: 1447-1458 [PMID: 23471546 DOI: 10.1007/s00192-013-2042-x]
49 Madhuvrata P, Cody JD, Ellis G, Herbison GP, Hay-Smith EJ. Which anticholinergic drug for overactive bladder symp-toms in adults. Cochrane Database Syst Rev 2012; 1: CD005429 [PMID: 22258963]
50 Khullar V, Amarenco G, Angulo JC, Cambronero J, Høye K, Milsom I, Radziszewski P, Rechberger T, Boerrigter P, Drogendijk T, Wooning M, Chapple C. Efficacy and toler-ability of mirabegron, a β(3)-adrenoceptor agonist, in pa-tients with overactive bladder: results from a randomised European-Australian phase 3 trial. Eur Urol 2013; 63: 283-295 [PMID: 23182126 DOI: 10.1016/j.eururo.2012.10.016]
51 Nitti VW, Auerbach S, Martin N, Calhoun A, Lee M, Her-schorn S. Results of a randomized phase III trial of mirabe-gron in patients with overactive bladder. J Urol 2013; 189: 1388-1395 [PMID: 23079373 DOI: 10.1016/j.juro.2012.10.017]
52 van Kerrebroeck P, Barkin J, Castro-Díaz D, Espuña-Pons M, Frankel J, Gousse A, Martin N, Stolzel M, Gunther A, Herschorn S. Randomised, Double-blind, Placebo-controlled Phase III Study to Assess the Efficacy and Safety of Mira-begron 25 mg and 50 mg Once-daily in Overactive Bladder
(OAB). 42nd ICS meeting, October 2012, Poster 35953 Nitti V, Herschorn S, Khullar V, Cambronero J, Angulo J,
Blauwet MB, Dorrepaal C, Siddiqui E, van Kerrebroeck P, Martin N. Efficacy of mirabegron in patients with overactive bladder (OAB): Pre-specified analysis of three randomised, double-blind, placebo-controlled, Phase III studies. 42nd ICS meeting, October 2012, Poster 222
54 Chapple CR, Kaplan SA, Mitcheson D, Klecka J, Cummings J, Drogendijk T, Dorrepaal C, Martin N. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a β(3)-adrenoceptor ago-nist, in overactive bladder. Eur Urol 2013; 63: 296-305 [PMID: 23195283 DOI: 10.1016/j.eururo.2012.10.048]
55 Nantel F, Bouvier M, Strosberg AD, Marullo S. Functional effects of long-term activation on human beta 2- and beta 3-adrenoceptor signalling. Br J Pharmacol 1995; 114: 1045-1051 [PMID: 7780639]
56 Otsuki H, Kosaka T, Nakamura K, Mishima J, Kuwahara Y, Tsukamoto T. β3-Adrenoceptor agonist mirabegron is effec-tive for overactive bladder that is unresponsive to antimus-carinic treatment or is related to benign prostatic hyperplasia in men. Int Urol Nephrol 2013; 45: 53-60 [PMID: 23212147 DOI: 10.1007/s11255-012-0343-5]
57 Food and Drug Administation. Summary of safety and ef-ficacy as basis for Advisory Committee briefing document for mirabegron, 5 April 2012. Division of Reproductive and Urologic Products, Office of New Drugs Center for Drug Evaluation and Research of Food and Drug Administration. 2012. Available from: URL: http://www.fda.gov/down-loads/AdvisoryCommittees/CommitteesMeetingMateri-als/Drugs/ReproductiveHealthDrugsAdvisoryCommittee/UCM298284.pdf. Accessed May 2, 2013
58 Nitti VW, Rosenberg S, Mitcheson DH, He W, Fakhoury A, Martin NE. Urodynamics and Safety of the β3-Adrenoceptor Agonist Mirabegron in Males with Lower Urinary Tract Symptoms and Bladder Outlet Obstruction. J Urol 2013; 190: 1320-1327 [PMID: 23727415 DOI: 10.1016/j.juro.2013.05.062]
59 Khullar V, Cambronero J, Angulo J, Wooning M, Blauwet MB, Dorrepaal C, Martin NE. Efficacy of mirabegron in patients with and without prior antimuscarinic therapy for overactive bladder (OAB): Post-hoc analysis of a prospective, randomised European-Australian phase III trial. Presented at the 27th Annual Congress of the European Urological As-sociation, Paris 2012, Abstract 684
60 Khullar V, Cambronero J, Angulo J, Nitti V, Herschorn S, Van Kerrebroeck P, Blauwet MB, Dorrepaal C, Siddiqui E, Martin N. Age-related efficacy of the selective β3-adrenoceptor agonist mirabegron for the treatment of overactive bladder (OAB): Pooled analysis of three prospective, randomised phase iii studies in patients aged > = 65 years. 42nd ICS meeting, Octo-ber 2012, Poster 331
P- Reviewers: Athanasopoulos A, Papatsoris AG S- Editor: Gou SX L- Editor: A E- Editor: Zheng XM
Sacco E et al . Review on mirabegron for overactive bladder

Female urinary incontinence during pregnancy and after delivery: Clinical impact and contributing factors
Paolo Mannella, Giulia Palla, Gonzalo Pérez-Roncero, María T López-Baena, Faustino R Pérez-López
Paolo Mannella, Giulia Palla, Division of Obstetrics and Gyne-cology, Center of Pelvic Disorders, University of Pisa, Hospital of Pisa, 56100 Pisa, Italy Gonzalo Pérez-Roncero, María T López-Baena, Faustino R Pérez-López, Red de Investigación de Ginecología, Obstetricia y Reproducción, Instituto Aragonés de Ciencias de la Salud, 50009 Zaragoza, SpainFaustino R Pérez-López, Department of Obstetrics and Gyne-cology, University of Zaragoza School of Medicine, 50009 Zara-goza, SpainAuthor contributions: All authors contributed to this paper.Correspondence to: Faustino R Pérez-López, Professor, De-partment of Obstetrics and Gynecology, University of Zaragoza School of Medicine, Domingo Miral s/n, 50009 Zaragoza, Spain. [email protected]: +34-976-761734 Fax: +34-976-761735Received: March 6, 2013 Revised: September 18, 2013Accepted: October 16, 2013Published online: November 10, 2013
AbstractUrinary incontinence (UI) is a common condition af-fecting adult women of all ages and it could have a negative influence on quality of life. The etiology of UI is multifactorial, but some of the most important risk factors are obesity and ageing, as well as adverse ob-stetric events. Pregnancy and delivery per se have been implicated in the etiology of UI. Although several stud-ies have demonstrated a direct association between UI and vaginal delivery in short, medium and long-term, the role of childbirth on the risk of UI remains con-troversial. The mechanical strain during delivery may induce injuries to the muscle, connective and neural structures. Vaginal birth can be associated with relax-ation or disruption of fascial and ligamentous supports of pelvic organs. Parity, instrumental delivery, prolonged labor and increased birth weights have always been considered risk factors for pelvic floor injury. Also ge-netic factors have been recently raised up but still there are not appropriate guidelines or measures to reduce
significantly the incidence of UI. The role of pelvic floor muscle training (PFMT) in the prevention and treatment of UI is still unclear. However, PFMT seems to be useful when supervised training is conducted and it could be incorporated as a routine part of women’s exercise pro-grammes during pregnancy and after childbirth.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Urinary incontinence; Pregnancy; Delivery; Cesarean section; Forceps; Episiotomy; Obesity; Colla-gen; Pelvic floor muscle training
Core tip: The mechanical strain during delivery may induce injuries to the muscle, connective and neural structures. Vaginal birth can be associated with re-laxation or disruption of fascial and ligamentous sup-ports of pelvic organs. Parity, instrumental delivery, prolonged labor and increased birthweight have always been considered risk factors for pelvic floor injury. Also genetic factors have been recently raised up but still there are not appropriate guidelines or measures to re-duce significantly the incidence of urinary incontinence.
Mannella P, Palla G, Pérez-Roncero G, López-Baena MT, Pérez-López FR. Female urinary incontinence during pregnancy and after delivery: Clinical impact and contributing factors. World J Obstet Gynecol 2013; 2(4): 74-79 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/74.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.74
INTRODUCTIONPelvic floor dysfunctions include a wide range of ana-tomic and functional disorders (e.g., hypo-function: uri-nary incontinence, fecal incontinence and pelvic organ prolapse; hyper-function: defecatory dysfunction, sexual
EDITORIAL
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.74
World J Obstet Gynecol 2013 November 10; 2(4): 74-79ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
74 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

dysfunction and voiding dysfunction). In women over 45 years old, prevalence of urinary (urge or stress) incon-tinence ranges from 17% to 45%, anal (faecal or flatus) incontinence (AI) from 0.5% to 17%, and urogenital prolapse between 20% to 30%. These prevalences could be therefore underestimated since most of the epidemio-logical investigations are obtained by self-report which could confound the real incidence of pelvic floor dys-functions[1-4] (Table 1).
Epidemiological evidences demonstrate that adverse obstetric events are related to pelvic floor dysfunction. Lower urinary tract symptoms (LUTSs) during pregnancy and postpartum have been associated to physiological and anatomical changes of pregnancy. LUTSs were pres-ent in 63.8% of Brazilian pregnant women, and the main risk factors were multiparity and pre-pregnancy LUTSs, smoking, constipation, and regular coffee consumption[5]. However, those symptoms are transient and disappear some months after delivery and they do not request fur-ther investigations.
According to the most recent definition of the Inter-national Continence Society (ICS), urinary incontinence (UI) is defined as “the complaint of any involuntary leak-age of urine”. Although UI is not a life threatening status, it is a common, annoying and expensive condition, and it deeply affects a woman’s quality of life[6]. In a subset of population, UI during pregnancy has been reported to be 19.9% among nulliparous and 24.1% among primiparous women[7]. In the last years, clinicians and health research-ers have extensively investigated the factors influencing prevalence of UI in order to ameliorate the management and treatment of affected patients. However, accurate prevalence data are difficult to obtain from the literature since noteworthy differences among the studies in terms of methodologies[8,9]. The fact that UI is more common in women than in men indicates the contribution of fac-tors such as pregnancy to UI.
PREVALENCE OF UI DURING PREGNANCY AND AFTER DELIVERYIt is well known that, during pregnancy, women can ex-perience urogynaecological problems which includes not only urinary incontinence, but also urinary tract infection, filling and voiding disorders, pelvic organ prolapse and AI[10]. The development of these conditions determinate physiological changes that occur in pregnancy but it can be also linked to previous pregnancies. In fact, during pregnancy, supporting structures are supposed to be overloaded due to the fetus weight and the progressive growth of the uterus, both in weight and size[11,12]. Ad-ditionally, pregnant uterus increases the angle between the bladder neck and urethra, which can participate to urinary symptoms. Hormonal changes due to pregnancy can also cause changes in tissue, in the support and in the continence mechanism[7,13].
During pregnancy and after delivery, both UI and AI are frequent complaints. The cumulative incidence during
pregnancy was 39.1% and 10.3%, respectively[14]. Accord-ing to a recent systematic review, it has been reported a prevalence of UI at the first trimester of 8.3%, at the second of 31.8% and at the third of 34.8%[14]. The most prevalent type of UI is the stress urinary incontinence (SUI), affecting up to 79.2% at the third trimester which is prompted by a physical movement or activity, such as coughing, sneezing, running or heavy lifting, that puts pressure (stress) on the bladder[15,16]. In a systematic re-view of population-based studies, in order to investigate the prevalence of UI within the first year postpartum, during the first 3 mo postpartum, the pooled prevalence of any postpartum incontinence was 33% in all women. The mean prevalence was double in the vaginal delivery group (31%) compared to the cesarean section group (15%)[17].
RISK FACTORS OF DEVELOPING UI DURING PREGNANCY AND AFTER DELIVERYRisk factors of developing UI after delivery have been related to the characteristics of mother and baby them-selves. Pregnancy per se has been reported to be a risk factor for postpartum UI especially if the incontinence started during the first trimester[18,19]. That is supported by the increase in the rate of SUI with an increased num-ber of abortions, which suggests that pregnancy by itself may have promoting effects on UI.
It has been found that the main risk factors of UI in pregnancy are maternal age more than 35 years[20], pre-gestational maternal body mass index (BMI) and family history of UI[16]. The prevalence of UI increases with maternal age and there is an annual increase in UI preva-lence of 3% per year[21]. Moreover, the first delivery is considered to exert the greatest increase in risk for UI, even if subsequent deliveries contribute to a further in-crease in the risk of UI[22].
The relationship between maternal weight and sub-sequent development of incontinence has been diffusely investigated. Higher pregestational BMI is known to be associated with postpartum UI[23]. It has been demon-strated an increased risk of UI (8%) proportionally to the increase of BMI unit, and this risk is not related to the type of delivery, vaginally or by caesarian section[21]. Pregnant women at term with body weight equal or more than 75 kg appear to double the risk of SUI[24]. UI during pregnancy and still persistent at 3 mo is usually associated to women with higher BMI[25]. The Norwegian Mother and Child Cohort Study studied 12679 primiparous
Mannella P et al . Urinary incontinence during pregnancy and after delivery
75 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Pelvic floor dysfunctions
Hypo-function Hyper-function
Urinary incontinence Voiding dysfunctionFecal incontinence Defecatory dysfunctionPelvic organ prolapse Sexual dysfunction

women, continent before pregnancy, at weeks 15 and 30 of pregnancy and 6 mo postpartum. Weight gain greater than the 50th percentile weeks 0-15 was weakly related with higher incidence of UI at week 30 when compared with weight gain less than or equal to the 50th percentile. In addition, weight increase greater than 50th percentile during pregnancy was not associated with higher inci-dence of UI, 6 mo postpartum[26].
Most of the interest is given to the impact of obstet-ric factors on UI after childbirth. In women who deliv-ered vaginally, the risk of incontinence increases with increasing fetal birthweight (especially for children with birthweight ≥ 4000 g[25,27,28], and probably in women who received oxytocin[28]. Shoulder dystocia and associated obstetrical maneuvers for its relief have not detrimental effects on perineum and do not increase UI incidence after delivery[29]. The vaginal delivery of two successive fetuses does not seem to be a cause of SUI as compared to cesarean, although its rate was higher in the “twin” group (40%) than in the “singleton” group (20%) which appears to be related to total intrauterine weight[30].
Another important contributing factor in developing UI after delivery is the presence of urinary leakage before pregnancy[23]. Thus, previous UI was a significant risk fac-tor for period prevalent UI during pregnancy, explaining 34% and 83% of pregnancy UI for nulliparous and pri-miparous, respectively[7]. In addition, in nulliparous wom-en prepregnancy UI is a strong herald for the increased prevalence of UI 4-12 years postpartum[21].
Cesarean section seemed to be followed by less post-natal UI than vaginal delivery[28,31]. It has been found that the risk is 67%-71% higher after vaginal delivery than after caesarean section[21], but this advantage given by cesarean delivery seems to disappear after the second cesarean section[16]. A systematic review reported that ce-sarean section reduced the risk of postpartum SUI from 16% to 10%, and the number needed to prevent SUI is 15 in 6 cross-sectional studies. In the same report, from the analysis of 12 cohort studies, the incidence of SUI in cesarean section patient decreased from 22% to 10% and the number needed to prevent SUI was 10%[31]. Nev-ertheless, a prospective multicenter study do not show a significant difference of risk for bothersome UI between women delivered by one or more vaginal deliveries and women delivered by one or more caesarean sections[32].
Concerning the type of cesarean sections, it has been found no difference in the prevalence of UI, or UI persisting for more than 10 years[21], between women delivered by acute or elective caesarean section (elective caesarean is defined as the caesarean section performed before the onset of labour, while caesarean section per-formed during labour are denoted as acute caesarean sections). That one indicates that it is the later stages of delivery, when the fetus passes through the pelvic floor that leads to the increased risk of UI. However, it should be clear that one has to perform eight or nine caesarean sections to avoid one case of UI. Moreover, operative delivery by caesarean section also involves a degree of
risk for morbidity and mortality over and above that of vaginal delivery.
One area of considerable controversy is the role of episiotomy and spontaneous perineal lacerations[33]. Al-most 80 years ago, episiotomy was proposed as a strategy to prevent spontaneous lacerations and to thereby re-duce “pelvic relaxation”. However, more recent studies have suggested that episiotomy may increase the odds of pelvic floor disorders. Thus, the role of episiotomy is uncertain. Episiotomy is not significantly associated with any of the pelvic floor disorders considered. In con-trast, women who had experienced multiple spontaneous perineal lacerations were significantly more likely to have prolapse to or beyond the hymen, and were significantly less likely to have overactive bladder (OAB)[34]. In 2005, a systematic review concluded that the effect of episiotomy on the development of pelvic floor disorders remains un-known[35].
Also controversial is the association between opera-tive delivery and pelvic floor disorders. While some re-search has suggested that operative delivery substantially increases the odds for pelvic floor disorders[23,28,36], other research suggests that operative birth is not a strong predictor of urinary incontinence[19,37-39] or pelvic organ prolapse[40]. Recently, it has been demonstrated that wom-en with at least one forceps delivery are more likely to report stress incontinence, OAB, AI, prolapse symptoms and prolapse to or beyond the hymen on examination, although this association is statistically significant only for OAB[34]. Preventing obstetric trauma needs changes in current obstetric practice: reduction in the episiotomy rate, use of vacuum extractor in preference to forceps.
Anal sphincter injuries showed a significantly higher risk of fecal incontinence 10 wk after delivery in women with these injuries, as well as in women with a second-stage labor of more than 50 min[41].
MOLECULAR AND GENETIC MECHANISMSPelvic floor disorders, such as SUI and pelvic organ pro-lapse, may have common pathophysiological processes related to pelvic floor tissue laxity and loss of support. Those changes could be relevant most of all during pe-riod of important modifications, such as pregnancy and delivery. However, the molecular mechanisms responsible for tissue changes in UI are poorly understood yet. Lin et al[42] have studied 22000 genes from the urethral tis-sue of a parturition-induced stress urinary incontinence (SUI) rat model. The expression of 42 urethral genes was different between continent and incontinent rats. Genes important in inflammation, collagen breakdown, and smooth muscle inhibition are upregulated in the urethras from rats with parturition-related incontinence.
Using the same model, muscle, collagen Ⅰ/Ⅲ and reticular fibers in the urethra of SUI rats were also sig-nificantly decreased, besides fragmentation and disorgani-zation. Transforming growth factor (TGF) beta 1, metal-
76 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Mannella P et al . Urinary incontinence during pregnancy and after delivery

limit the incidence of postpartum UI. A good manage-ment of pre-pregnancy BMI and weight gain during pregnancy, proper management especially of the second and third stage of labor, fetal weight < 4.0 kg, and finally a good awareness of their own pelvic floor and its train-ing to strengthen those muscles, constitute the elements on which we can work to significantly reduce the possi-bility of developing UI after pregnancy.
REFERENCES1 Sandvik H, Hunskaar S, Vanvik A, Bratt H, Seim A, Herm-
stad R. Diagnostic classification of female urinary inconti-nence: an epidemiological survey corrected for validity. J Clin Epidemiol 1995; 48: 339-343 [PMID: 7897455 DOI: 10.1016/0895-4356(94)00147-I]
2 Sandvik H, Hunskaar S. General practitioners’ management of female urinary incontinence. Medical records do not reflect patients’ recall. Scand J Prim Health Care 1995; 13: 168-174 [PMID: 7481168 DOI: 10.3109/02813439508996757]
3 Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, Assassa RP, Shaw C, Cheater F. Systematic review and evaluation of methods of assessing urinary in-continence. Health Technol Assess 2006; 10: 1-132, iii-iv [PMID: 16487456]
4 van Leijsen SA, Hoogstad-van Evert JS, Mol BW, Vierhout ME, Milani AL, Heesakkers JP, Kluivers KB. The correlation between clinical and urodynamic diagnosis in classifying the type of urinary incontinence in women. A systematic review of the literature. Neurourol Urodyn 2011; 30: 495-502 [PMID: 21298721 DOI: 10.1002/nau.21047]
5 Martins G, Soler ZA, Cordeiro JA, Amaro JL, Moore KN. Prevalence and risk factors for urinary incontinence in healthy pregnant Brazilian women. Int Urogynecol J 2010; 21: 1271-1277 [PMID: 20502875 DOI: 10.1007/s00192-010-1185-2]
6 Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, Van Kerrebroeck P, Victor A, Wein A. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Con-tinence Society. Urology 2003; 61: 37-49 [PMID: 12559262 DOI: 10.1016/S0090-4295(02)02243-4]
7 Hvidman L, Hvidman L, Foldspang A, Mommsen S, Bugge Nielsen J. Correlates of urinary incontinence in pregnancy. Int Urogynecol J Pelvic Floor Dysfunct 2002; 13: 278-283 [PMID: 12355285 DOI: 10.1007/s001920200061]
8 Abrams P, Andersson KE, Birder L, Brubaker L, Cardozo L, Chapple C, Cottenden A, Davila W, de Ridder D, Dmo-chowski R, Drake M, Dubeau C, Fry C, Hanno P, Smith JH, Herschorn S, Hosker G, Kelleher C, Koelbl H, Khoury S, Madoff R, Milsom I, Moore K, Newman D, Nitti V, Norton C, Nygaard I, Payne C, Smith A, Staskin D, Tekgul S, Thuroff J, Tubaro A, Vodusek D, Wein A, Wyndaele JJ. Fourth Inter-national Consultation on Incontinence Recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 2010; 29: 213-240 [PMID: 20025020 DOI: 10.1002/nau.20870]
9 Buckley BS, Lapitan MC. Prevalence of urinary incontinence in men, women, and children--current evidence: findings of the Fourth International Consultation on Incontinence. Urology 2010; 76: 265-270 [PMID: 20541241 DOI: 10.1016/j.urology.2009.11.078]
10 Law H, Fiadjoe P. Urogynaecological problems in pregnancy. J Obstet Gynaecol 2012; 32: 109-112 [PMID: 22296415 DOI: 10.3109/01443615.2011.635227]
11 Ashton-Miller JA, DeLancey JO. Functional anatomy of the female pelvic floor. Ann N Y Acad Sci 2007; 1101: 266-296 [PMID: 17416924 DOI: 10.1196/annals.1389.034]
loproteinase (MMP) 9, and phosphorylated Smad2 were expressed significantly higher in parturition-associated SUI than in continent rats[43]. Birth appears to activate elastin expression by TGF-beta 1 signals while estrogen interferes with this mechanism, resulting in improper as-sembly of elastic fibers. The TGF-beta family also con-tributes in the regulation of myometrial activation at term integrating mechanical and endocrine signals for success-ful labor contraction[44].
In humans, there is a three-fold prevalence of SUI among first-degree relatives of female patients with SUI[45] which suggests a genetic factor involved in the predisposition of connective tissue injury. Allen-Brady et al[46] have studied the relationship between predisposing gene and pelvic flood disorders, including UI, on chro-mosome 9q21. In a large sample of twins, it has been demonstrated a genetic component for the aetiology of SUI, although environmental factors equally contributed to variation liability[47]. Further research into the genetic basis of UI may provide a comprehensive understanding of the biological basis of the disorder.
PREVENTION OF URINARY INCONTINENCE DURING PREGNANCY AND AFTER DELIVERYMost pregnant women had no information about pelvic floor, and a little number of women could only local-ize to the region. Several studies have demonstrated that antenatal pelvic floor muscle training (PFMT) taught in a general exercise class, during pregnancy, could be help-ful in the prevention of postpartum UI in primiparous women without UI during pregnancy[48]. The utility of regular pelvic floor muscle exercises is due to the ability of the muscles that support the pelvic organs, to become stronger and to help to use the muscles more effectively. Pregnant and postpartum women who do PFMT have significantly less urine leakage[49], even if PFMT does not affect labor and birth outcomes or complication rates[50,51]. In addition, PFMT applied in pregnancy is ef-fective in the treatment and prevention of urinary incon-tinence during pregnancy, and this effect may persist to postpartum period[50,52].
On the other hand, an Australian prospective ran-domised controlled trial, among women 3 mo after de-livery, has compared women which had PFMT or a usual postpartum care[27]. At 3 mo after delivery, the prevalence of UI was respectively 31% and 38%. After one year, there was no significant difference in continence status between both groups[53]. Even if there was no significant difference in continence status, women in the interven-tion group were more motivated than those in the con-trol group in practicing pelvic floor exercises at adequate frequencies.
In conclusion, there are no specific techniques or treatments to prevent the development of postpartum UI but there are correct behaviors to follow that severely
77 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Mannella P et al . Urinary incontinence during pregnancy and after delivery

12 Lukacz ES, Lawrence JM, Contreras R, Nager CW, Luber KM. Parity, mode of delivery, and pelvic floor disorders. Obstet Gynecol 2006; 107: 1253-1260 [PMID: 16738149 DOI: 10.1097/01.AOG.0000218096.54169.34]
13 Herbert J. Pregnancy and childbirth: the effects on pelvic floor muscles. Nurs Times 2009; 105: 38-41 [PMID: 19326654]
14 Solans-Domènech M , Sánchez E, Espuña-Pons M. Urinary and anal incontinence during pregnancy and postpartum: incidence, severity, and risk factors. Obstet Gynecol 2010; 115: 618-628 [PMID: 20177295 DOI: 10.1097/AOG.0b013e3181d04dff]
15 Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiol-ogy of Incontinence in the County of Nord-Trøndelag. J Clin Epidemiol 2000; 53: 1150-1157 [PMID: 11106889 DOI: 10.1016/S0895-4356(00)00232-8]
16 Cerruto MA, D’Elia C, Aloisi A, Fabrello M, Artibani W. Prevalence, incidence and obstetric factors’ impact on female urinary incontinence in Europe: a systematic review. Urol Int 2013; 90: 1-9 [PMID: 22868349 DOI: 10.1159/000339929]
17 Thom DH, Rortveit G. Prevalence of postpartum urinary incontinence: a systematic review. Acta Obstet Gynecol Scand 2010; 89: 1511-1522 [PMID: 21050146 DOI: 10.3109/00016349.2010.526188]
18 Milsom I, Ekelund P, Molander U, Arvidsson L, Areskoug B. The influence of age, parity, oral contraception, hysterectomy and menopause on the prevalence of urinary incontinence in women. J Urol 1993; 149: 1459-1462 [PMID: 8501788]
19 Gyhagen M, Bullarbo M, Nielsen TF, Milsom I. The preva-lence of urinary incontinence 20 years after childbirth: a na-tional cohort study in singleton primiparae after vaginal or caesarean delivery. BJOG 2013; 120: 144-151 [PMID: 22413831 DOI: 10.1111/j.1471-0528.2012.03301.x]
20 Rortveit G, Hannestad YS, Daltveit AK, Hunskaar S. Age- and type-dependent effects of parity on urinary incontinence: the Norwegian EPINCONT study. Obstet Gynecol 2001; 98: 1004-1010 [PMID: 11755545 DOI: 10.1016/S0029-7844(01)01566-6]
21 Brown SJ, Donath S, MacArthur C, McDonald EA, Krastev AH. Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, and associated risk factors. Int Urogynecol J 2010; 21: 193-202 [PMID: 19834637 DOI: 10.1007/s00192-009-1011-x]
22 MacArthur C, Glazener CM, Wilson PD, Lancashire RJ, Herbison GP, Grant AM. Persistent urinary incontinence and delivery mode history: a six-year longitudinal study. BJOG 2006; 113: 218-224 [PMID: 16412001 DOI: 10.1111/j.1471-0528.2005.00818.x]
23 Eason E, Labrecque M, Marcoux S, Mondor M. Effects of car-rying a pregnancy and of method of delivery on urinary in-continence: a prospective cohort study. BMC Pregnancy Child-birth 2004; 4: 4 [PMID: 15053837 DOI: 10.1186/1471-2393-4-4]
24 Diez-Itza I, Ibañez L, Arrue M, Paredes J, Murgiondo A, Sarasqueta C. Influence of maternal weight on the new on-set of stress urinary incontinence in pregnant women. Int Urogynecol J Pelvic Floor Dysfunct 2009; 20: 1259-1263 [PMID: 19499157 DOI: 10.1007/s00192-009-0923-9]
25 Glazener CM, Herbison GP, MacArthur C, Lancashire R, McGee MA, Grant AM, Wilson PD. New postnatal urinary incontinence: obstetric and other risk factors in primiparae. BJOG 2006; 113: 208-217 [PMID: 16412000 DOI: 10.1111/j.1471-0528.2005.00840.x]
26 Wesnes SL, Hunskaar S, Bo K, Rortveit G. Urinary inconti-nence and weight change during pregnancy and postpartum: a cohort study. Am J Epidemiol 2010; 172: 1034-1044 [PMID: 20729349 DOI: 10.1093/aje/kwq240]
27 Chiarelli P, Cockburn J. Promoting urinary continence in women after delivery: randomised controlled trial. BMJ 2002; 324: 1241 [PMID: 12028976 DOI: 10.1136/bmj.324.7348.1241]
28 Casey BM, Schaffer JI, Bloom SL, Heartwell SF, McIntire DD, Leveno KJ. Obstetric antecedents for postpartum pelvic floor dysfunction. Am J Obstet Gynecol 2005; 192: 1655-1662 [PMID: 15902173 DOI: 10.1016/j.ajog.2004.11.031]
29 Mazouni C, Menard JP, Porcu G, Cohen-Solal E, Heckenroth H, Gamerre M, Bretelle F. Maternal morbidity associated with obstetrical maneuvers in shoulder dystocia. Eur J Obstet Gynecol Reprod Biol 2006; 129: 15-18 [PMID: 16338049 DOI: 10.1016/j.ejogrb.2005.11.006]
30 Legendre G, Tassel J, Salomon LJ, Fauconnier A, Bader G. [Impact of twin gestation on the risk of postpartum stress incontinence]. Gynecol Obstet Fertil 2010; 38: 238-243 [PMID: 20362483 DOI: 10.1016/j.gyobfe.2010.02.004]
31 Press JZ, Klein MC, Kaczorowski J, Liston RM, von Dadel-szen P. Does cesarean section reduce postpartum urinary incontinence? A systematic review. Birth 2007; 34: 228-237 [PMID: 17718873 DOI: 10.1111/j.1523-536X.2007.00175.x]
32 McKinnie V, Swift SE, Wang W, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, Schaffer J. The effect of pregnan-cy and mode of delivery on the prevalence of urinary and fe-cal incontinence. Am J Obstet Gynecol 2005; 193: 512-57; discus-sion 512-57; [PMID: 16098879 DOI: 10.1016/j.ajog.2005.03.056]
33 da Silva FM, de Oliveira SM, Bick D, Osava RH, Tuesta EF, Riesco ML. Risk factors for birth-related perineal trauma: a cross-sectional study in a birth centre. J Clin Nurs 2012; 21: 2209-2218 [PMID: 22646921 DOI: 10.1111/j.1365-2702.2012.04133.x]
34 Handa VL, Blomquist JL, McDermott KC, Friedman S, Mu-ñoz A. Pelvic floor disorders after vaginal birth: effect of episiotomy, perineal laceration, and operative birth. Obstet Gynecol 2012; 119: 233-239 [PMID: 22227639 DOI: 10.1097/AOG.0b013e318240df4f]
35 Viswanathan M, Hartmann K, Palmieri R, Lux L, Swinson T, Lohr KN, Gartlehner G, Thorp J. The use of episiotomy in obstetrical care: a systematic review. Evid Rep Technol Assess (Summ) 2005; (112): 1-8 [PMID: 15910014]
36 Handa VL, Blomquist JL, Knoepp LR, Hoskey KA, McDer-mott KC, Muñoz A. Pelvic floor disorders 5-10 years after vaginal or cesarean childbirth. Obstet Gynecol 2011; 118: 777-784 [PMID: 21897313]
37 Schytt E, Lindmark G, Waldenström U. Symptoms of stress incontinence 1 year after childbirth: prevalence and predic-tors in a national Swedish sample. Acta Obstet Gynecol Scand 2004; 83: 928-936 [PMID: 15453888]
38 Fritel X, Schaal JP, Fauconnier A, Bertrand V, Levet C, Pigné A. [Pelvic floor disorders four years after first delivery: a comparative study of restrictive versus systematic episioto-my]. Gynecol Obstet Fertil 2008; 36: 991-997 [PMID: 18801690 DOI: 10.1016/j.gyobfe.2008.07.009]
39 Thom DH, Brown JS, Schembri M, Ragins AI, Creasman JM, Van Den Eeden SK. Parturition events and risk of urinary in-continence in later life. Neurourol Urodyn 2011; 30: 1456-1461 [PMID: 21780171 DOI: 10.1002/nau.21166]
40 Tegerstedt G, Miedel A, Maehle-Schmidt M, Nyrén O, Ham-marström M. Obstetric risk factors for symptomatic prolapse: a population-based approach. Am J Obstet Gynecol 2006; 194: 75-81 [PMID: 16389012 DOI: 10.1016/j.ajog.2005.06.086]
41 Lal M, Pattison HM, Allan TF, Callender R. Postcesarean pel-vic floor dysfunction contributes to undisclosed psychosocial morbidity. J Reprod Med 2009; 54: 53-60 [PMID: 19301567]
42 Lin G, Shindel AW, Banie L, Deng D, Wang G, Hayashi N, Lin CS, Lue TF. Molecular mechanisms related to parturition-induced stress urinary incontinence. Eur Urol 2009; 55: 1213-1222 [PMID: 18372098 DOI: 10.1016/j.eururo.2008.02.027]
43 Li GY, Cui WS, Zhou F, Gao ZZ, Xin H, Liu T, Li WR, Gong YQ, Bai GY, Guo YL, Xin ZC. Pathology of urethral fibromus-cular system related to parturition-induced stress urinary incontinence and TGF-β1/Smad pathway. Mol Cell Biochem 2012; 364: 329-335 [PMID: 22307744 DOI: 10.1007/s11010-012-1234-x]
78 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Mannella P et al . Urinary incontinence during pregnancy and after delivery

44 Shynlova O, Tsui P, Dorogin A, Langille BL, Lye SJ. The expression of transforming growth factor beta in pregnant rat myometrium is hormone and stretch dependent. Repro-duction 2007; 134: 503-511 [PMID: 17709568 DOI: 10.1530/REP-07-0004]
45 Mushkat Y, Bukovsky I, Langer R. Female urinary stress incontinence--does it have familial prevalence? Am J Obstet Gynecol 1996; 174: 617-619 [PMID: 8623794 DOI: 10.1016/S0002-9378(96)70437-4]
46 Allen-Brady K, Norton PA, Farnham JM, Teerlink C, Can-non-Albright LA. Significant linkage evidence for a predis-position gene for pelvic floor disorders on chromosome 9q21. Am J Hum Genet 2009; 84: 678-682 [PMID: 19393595 DOI: 10.1016/j.ajhg.2009.04.002]
47 Altman D, Forsman M, Falconer C, Lichtenstein P. Genetic influence on stress urinary incontinence and pelvic organ prolapse. Eur Urol 2008; 54: 918-922 [PMID: 18155350 DOI: 10.1016/j.eururo.2007.12.004]
48 Pelaez M, Gonzalez-Cerron S, Montejo R, Barakat R. Pel-vic floor muscle training included in a pregnancy exercise program is effective in primary prevention of urinary incon-tinence: A randomized controlled trial. Neurourol Urodyn 2013; Epub ahead of print [PMID: 23389863 DOI: 10.1002/
nau.22381]49 Mørkved S, Bø K. Effect of pelvic floor muscle training
during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. Br J Sports Med 2013; Epub ahead of print [PMID: 23365417 DOI: 10.1136/bjsports-2012-091758]
50 Bø K, Fleten C, Nystad W. Effect of antenatal pelvic floor muscle training on labor and birth. Obstet Gynecol 2009; 113: 1279-1284 [PMID: 19461423]
51 Dias LA, Driusso P, Aita DL, Quintana SM, Bø K, Ferreira CH. Effect of pelvic floor muscle training on labour and newborn outcomes: a randomized controlled trial. Rev Bras Fisioter 2011; 15: 487-493 [PMID: 21860990 DOI: 10.1590/S1413-35552011005000011]
52 Harvey MA. Pelvic floor exercises during and after pregnan-cy: a systematic review of their role in preventing pelvic floor dysfunction. J Obstet Gynaecol Can 2003; 25: 487-498 [PMID: 12806450]
53 Chiarelli P, Murphy B, Cockburn J. Promoting urinary conti-nence in postpartum women: 12-month follow-up data from a randomised controlled trial. Int Urogynecol J Pelvic Floor Dysfunct 2004; 15: 99-105; discussion 105 [PMID: 15014936 DOI: 10.1007/s00192-004-1119-y]
P- Reviewers: Akdemir N, Ishizuka O S- Editor: Zhai HH L- Editor: A E- Editor: Zhang DN
79 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Mannella P et al . Urinary incontinence during pregnancy and after delivery

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.80
World J Obstet Gynecol 2013 November 10; 2(4): 80-86ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Individualized misoprostol dosing for labor induction or augmentation: A review
Shi-Yann Cheng
Shi-Yann Cheng, Department of Obstetrics and Gynecology, China Medical University Beigang Hospital, Yunlin County 65152, TaiwanAuthor contributions: Cheng SY solely contributed to this paper.Correspondence to: Shi-Yann Cheng, MD, Department of Obstetrics and Gynecology, China Medical University Beigang Hospital, 123 Shinder Road, Beigang Town, Yunlin County 65152, Taiwan. [email protected]: +886-5-7837933 Fax: +886-5-7836439Received: March 18, 2013 Revised: June 3, 2013Accepted: July 18, 2013Published online: November 10, 2013
AbstractCesarean birth rates are greater than 20% in many de-veloped countries. The main diagnoses contributing to the high rate of cesarean births in nulliparous women are dystocia and prolonged labor. Traditionally, a policy of vaginal dinoprostone for the treatment of unripe cervix or early amniotomy with oxytocin administration for a ripened cervix has been associated with a mod-est reduction in the rate of cesarean births due to arrest disorders. However, the course of vaginal dinoprostone is tedious and oxytocin should be administered through an infusion pump, which may be inconvenient in certain settings. Because misoprostol has powerful uterotropic and uterotonic effects, and has become a common agent used in the practice of obstetrics and gynecology, the United States Food and Drug Administration removed the absolute contraindication of the drug during pregnancy from its label in April 2002. However, excessive uterine contractility resulting in tachysystole or fetal distress is always a concern with the oral or vaginal use of fixed-dosage misoprostol. Therefore, misoprostol should be ad-ministered with caution to ensure that fetal hypoxia does not occur. A pilot trial examining the use of very small, frequent, titrated oral misoprostol dosages administered every 2 h was first conducted by Hofmeyr et al in 2001. Given women’s different metabolisms and responses to
misoprostol, another method of titrating individualized oral misoprostol with dosing administered every hour rel-ative to uterine response was then developed by Cheng in 2006. Based on previous studies, this titration method is potentially an ideal alternative to traditional dinopros-tone, oxytocin or the previously established misoprostol dosing method for labor induction or augmentation.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Cervix; Misoprostol; Oxytocin; Labor induc-tion; Labor augmentation
Core tip: Avoiding uterine tachysystole and fetal hy-poxia is the critical consideration when implementing labor induction or augmentation with misoprostol. Ti-trated oral misoprostol is potentially an ideal alternative to traditional dinoprostone, oxytocin or the previously established misoprostol dosing method for labor induc-tion or augmentation.
Cheng SY. Individualized misoprostol dosing for labor in-duction or augmentation: A review. World J Obstet Gynecol 2013; 2(4): 80-86 Available from: URL: http://www.wjg-net.com/2218-6220/full/v2/i4/80.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.80
BIOGRAPHYShi-Yann Cheng received his MD degree from National Yang-Ming University, Taipei, Taiwan. He completed an extensive 5-year obstetrics residency in Taiwan in the De-partment of Obstetrics and Gynecology, Veteran General Hospital, Kaohsiung. He is presently the Director of the Department of Obstetrics and Gynecology and Medi-cal Education and Research at Medical China University Beigang Hospital and Lecturer in the School of Medicine
FRONTIER
80 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Cheng SY. Individualized misoprostol dosing for laboring women
at Medical China University, Taichung, Taiwan. His re-search interests cover clinical obstetrics and interdisciplin-ary collaborative care education, and his most notable contribution is the development of the concept of labor induction with titrated misoprostol solution with a focus on dosing interval and uterine responses according to the pharmacokinetics of misoprostol. His CV lists 16 peer-re-viewed publications, 2 book chapters, prestigious medical education devotion awards, and presentations at national and international meetings.
INTRODUCTIONThere are many indications for term labor inductions and more than 15% of all gravid women require aid in cervi-cal ripening. A labor course longer than that of spontane-ous labor is the most commonly encountered problem associated with labor induction. Additionally, prolonged spontaneous labor in nulliparous women is another com-mon problem that can result in a negative birth experi-ence[1,2] and can be associated with a non-reassuring fetal heart rate (FHR) resulting in emergency cesarean deliv-ery[3,4]. Considering the root cause of these problems, the unripe cervix is the greatest barrier to spontaneous birth, which results in great concern and unnecessary cesarean deliveries. Therefore, overcoming an unripe cervix is a critical issue. Misoprostol, a synthetic prostaglandin E1 analogue, was initially used to treat peptic ulcers caused by prostaglandin synthetase inhibitors. Because misopro-stol has been used off-label for a variety of indications in the practice of obstetrics and gynecology, including medication abortion, medical management of miscar-riage, induction of labor, cervical ripening before surgical procedures, and the treatment of postpartum hemor-rhage, the absolute contraindication of the use of miso-prostol during pregnancy was removed from the label by the United States Food and Drug Administration in April 2002[5]. Because misoprostol has powerful uterotropic and uterotonic effects, many studies have been conducted since 1992 to learn how to administer the drug while tak-ing into consideration safety during labor induction[6-9]. Fetal hypoxia resulting from uterine tachysystole is always an obstetrical concern[10-16]. The recommended dosage of misoprostol is 50 µg every 4 h via the oral route or 25 µg every 4 h via the vaginal route[17] until adequate la-bor commences, but the induction duration is prolonged. Because the risk of inducing fetal hypoxia is incurred by using a fixed dosage of misoprostol, a pilot trial using very small, frequent, titrated oral misoprostol doses every 2 h was first conducted by Hofmeyr et al[18,19] in 2001. It was concluded that this new approach to oral misopros-tol administration was successful in minimizing the risk of uterine hyperstimulation, which has been a feature of misoprostol use for labor induction, at the expense of a somewhat slower response in women with intact membranes and unfavorable cervices[19]. Given women’s different metabolic rates and responses, another method of titrating individualized oral misoprostol with dosing
administered every hour relative to uterine response was developed[20-23]. It was observed that a higher success rate of vaginal delivery within 24 h, not accompanied by a higher rate of uterine hyperstimulation, was achieved us-ing the 1-h oral misoprostol titration method (Table 1). According to the results of titration studies, misoprostol is the ideal candidate agent for labor induction and aug-mentation due to its convenience of administration and cervical ripening characteristics.
PRINCIPLE OF TITRATED ORAL MISOPROSTOL ADMINISTRATIONAfter misoprostol is absorbed, it undergoes rapid de-esterification to its free acid, which is responsible for its clinical activity and is detectable in the blood plasma[26]. Because misoprostol’s effects on and toxicity to the uterus based on serum concentrations of misoprostol acid at term are unknown, the rationale for titrated administra-tion stems from the proven efficacy and pharmacokinetics of misoprostol, and the extreme inter- and intra-individ-ual variation in uterine sensitivity[20]. To avoid uterine hy-perstimulation and shorten the labor course, misoprostol should be administered in small, frequent doses (one dose per hour, generally) titrated against the uterine response. This approach is analogous to the conventional, titrated use of oxytocin. Currently, misoprostol is available as an oral tablet of 100 or 200 µg and is water-soluble. Oral ad-ministration is easier and has greater acceptability among women than vaginal administration. Because the drug ab-sorption is more rapid and more predictable, with a peak serum concentration after oral administration of 34 min and a half-life of 20-40 min[26], a 1-h interval between oral administrations and an increase in dosage of 20 µg every 4 h from the initial 20-µg dosage were determined to be optimal, based on a mathematical model that takes these drug characteristics into consideration[20]. This method maintains a virtually steady serum level of misoprostol acid, thus avoiding large fluctuations and increases the peak serum concentration of the 20-µg absorptive miso-prostol dose every 4 h by a factor of 1.33. This math-ematical model is described in Table 2.
CLINICAL PHARMACOLOGY OF MISOPROSTOLMisoprostol does not affect the hepatic mixed-function oxidase enzyme systems. In patients with varying degrees of renal impairment, there is an approximate doubling of the T1/2, peak serum concentration (Cmax), and area under the serum concentration curve compared with those of normal patients, but no clear correlation between the degree of impairment and area under the serum concen-tration curve has been shown. No routine dosage adjust-ment is recommended in older patients or patients with renal impairment[27,28]. Misoprostol does not produce clinically significant effects on the serum levels of prolac-
81 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

tin, gonadotropin, thyroid-stimulating hormone, growth hormone, thyroxine, cortisol, gastrointestinal hormones, creatinine or uric acid. Furthermore, gastric emptying, immunological competence, platelet aggregation, pul-monary function and the cardiovascular system are not modified by the recommended doses of misoprostol[28].
Therefore, the use of misoprostol is not contraindicated in patients with renal disease, severe anemia, systemic lu-pus erythematosus, hypertension or heart disease.
RISKS OF MISOPROSTOL ADMINISTRATIONUterine rupture is an unwanted risk of labor regardless of whether a woman has had a previous caesarean deliv-ery. Most studies suggest that the use of misoprostol in women with a previous caesarean delivery increases the frequency of uterine scar disruption, either described as uterine dehiscence or overt uterine rupture[29-31]. There are even sporadic reports of uterine rupture in women without prior cesarean surgeries[32,33]. Grand multiparity appears to be a risk factor for uterine rupture in the pres-ence of misoprostol, although there is a report of uterine rupture in a primigravida[34]. Therefore, the indications for labor induction or augmentation must be carefully evaluated prior to misoprostol administration.
PREPARING ORAL MISOPROSTOL SOLUTIONS AND GUIDELINES FOR ADMINISTRATIONMisoprostol is manufactured as an oral tablet and is water-soluble. The uterine activity produced by an oral solution is faster and stronger than that produced by an oral tablet or when administered via the rectal or vaginal route[35]. One 200-µg tablet of misoprostol may be dissolved in 200 mL of drinking water in a medicine bottle. The misoprostol solution needs to be used completely within 24 h after preparation or discarded. Women are induced with one basal unit of 20 mL of misoprostol solution (1 µg/mL) prepared as described above. The determined volume of misoprostol solution is poured according to the obstetrician’s discretion at each dosing, following the guidelines of labor induction[21] or augmentation[22]. Ini-tially, the determined volume may be given upon request by an obstetrician according to the guidelines when regu-lar uterine contractions are not achieved. Once regular uterine contractions are achieved, the obstetrician is called to visit the patient and make a decision regarding the next dose or dosage adjustment, if any. Such individualized administration of misoprostol decreases the accidental fetal hypoxia resulting from uterine hyperstimulation. The flowchart of administration is shown in Figure 1. The
82 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Comparison of titrated oral misoprostol in labor induction between studies
Ref. Year No. of women
Initial dosage (µg)
Dosing interval
Efficacy Adverse effects Cesarean rate (%)
Hofmeyr et al[18] 2001 25 20 q2h 72% VD within 32 h 8% UH 20.0Hofmeyr et al[19] 2001 346 20 q2h 62% VD within 24 h 4% UH 16.0Matonhodze et al[24] 2003 176 20 q2h 60.2% VD within 24 h 4% UH, 8% UT 14.0Cheng et al[20] 2006 77 20 q1h 93.5% VD within 24 h 0% UH, 9.1% UT 3.9Bricker et al[25] 2008 375 20 q2h 76% VD within 24 h 2% UH, 5% UT 14.0Cheng et al[21] 2008 101 20 q1h 94.1% VD within 24 h 0% UH, 6.9% UT 4.0Ho et al[22] 2010 112 20 q1h 94.6% VD within 24 h 0% UH, 7.1% UT 3.6Souza et al[23] 2010 30 20 q1h 80% VD within 24 h 13.3% UT 20.0
VD: Vaginal delivery; UH: Uterine hyperstimulation; UT: Uterine tachysystole.
Table 2 Mathematical model of titrated oral misoprostol
Times t = 34 + 60n , n = 0, 1, 2, 3, --- (min)
Dosage (mcg) 34 94 154 214 274 20 P 20 P(1/40 + 1/41) 20 P(1/40 + 1/41 + 1/42) 20 P(1/40 + 1/41 + 1/42 + 1/43) 40 P + P(1/40 + 1/41 + 1/42 + 1/43 + 1/44) …
Set the function C = f(t), where C: Concentration of misoprostol acid (pg/mL) in plasma; t: Times during the whole process, t = 34 + 60n (min), when taking misoprostol at n = 0, 1, 2, 3, --- (h); Tmax (the time to peak plasma concentration of misoprostol acid after absorption): 34 min; T1/2 (the half-life of misoprostol acid): 30 min as determined by a pharmacokinetics study. When n = 0, intake 20 µg, t = 34 min, set the peak plasma concentration of misoprostol acid, C = P; When n = 1, intake 20 µg, t = 34 + (60 × 1) = 94 min, and C = P(1/40 + 1/41); When n = 2, intake 20 µg, t = 34 + (60 × 2) = 154 min, and C = P(1/40 + 1/41 + 1/42); When n = 3, intake 20 µg, t = 34 + (60 × 3) = 214 min, and C = P(1/40 + 1/41 + 1/42 + 1/43); When n = 4, intake 40 µg, t = 34 + (60 × 3) = 214 min, and C = P + P(1/40 + 1/41 + 1/42 + 1/43 + 1/44) and so on. Therefore, C = f(t) is a convergent series in which the upper limit = P/(1 - 1/4) + P/(1 - 1/4) + --- = (4/3)P + (4/3)P + ---.
Cheng SY. Individualized misoprostol dosing for laboring women
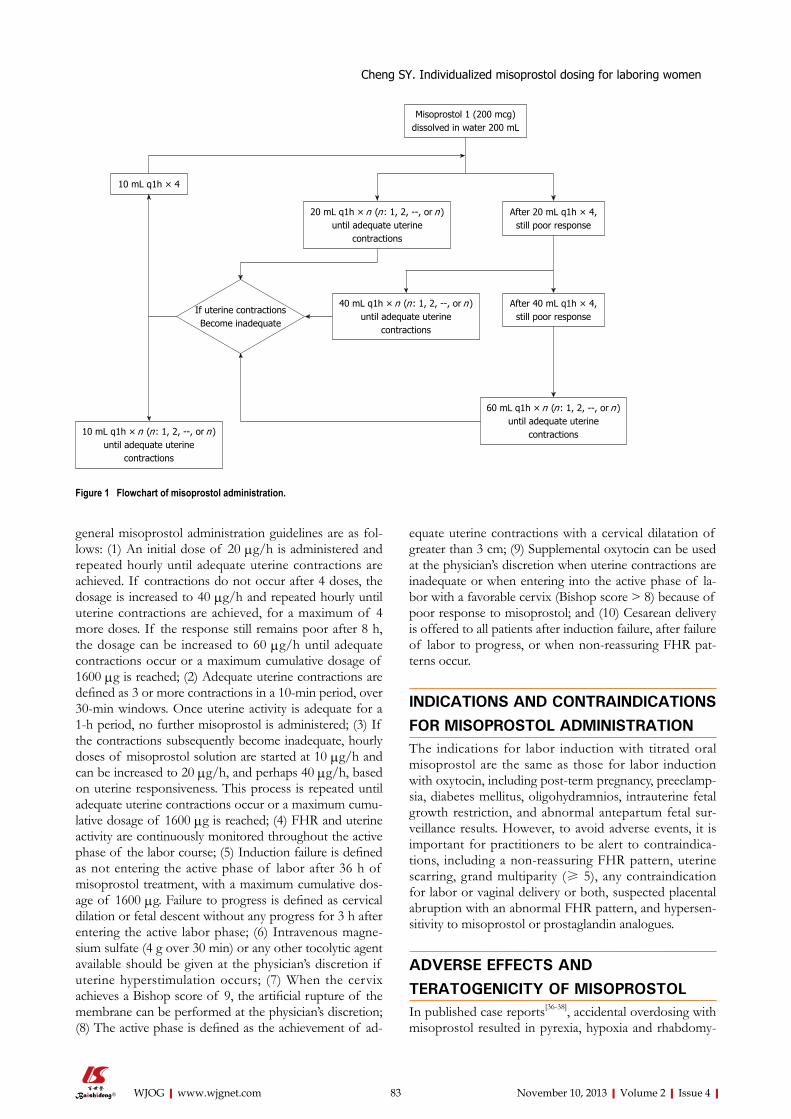
general misoprostol administration guidelines are as fol-lows: (1) An initial dose of 20 µg/h is administered and repeated hourly until adequate uterine contractions are achieved. If contractions do not occur after 4 doses, the dosage is increased to 40 µg/h and repeated hourly until uterine contractions are achieved, for a maximum of 4 more doses. If the response still remains poor after 8 h, the dosage can be increased to 60 µg/h until adequate contractions occur or a maximum cumulative dosage of 1600 µg is reached; (2) Adequate uterine contractions are defined as 3 or more contractions in a 10-min period, over 30-min windows. Once uterine activity is adequate for a 1-h period, no further misoprostol is administered; (3) If the contractions subsequently become inadequate, hourly doses of misoprostol solution are started at 10 µg/h and can be increased to 20 µg/h, and perhaps 40 µg/h, based on uterine responsiveness. This process is repeated until adequate uterine contractions occur or a maximum cumu-lative dosage of 1600 µg is reached; (4) FHR and uterine activity are continuously monitored throughout the active phase of the labor course; (5) Induction failure is defined as not entering the active phase of labor after 36 h of misoprostol treatment, with a maximum cumulative dos-age of 1600 µg. Failure to progress is defined as cervical dilation or fetal descent without any progress for 3 h after entering the active labor phase; (6) Intravenous magne-sium sulfate (4 g over 30 min) or any other tocolytic agent available should be given at the physician’s discretion if uterine hyperstimulation occurs; (7) When the cervix achieves a Bishop score of 9, the artificial rupture of the membrane can be performed at the physician’s discretion; (8) The active phase is defined as the achievement of ad-
equate uterine contractions with a cervical dilatation of greater than 3 cm; (9) Supplemental oxytocin can be used at the physician’s discretion when uterine contractions are inadequate or when entering into the active phase of la-bor with a favorable cervix (Bishop score > 8) because of poor response to misoprostol; and (10) Cesarean delivery is offered to all patients after induction failure, after failure of labor to progress, or when non-reassuring FHR pat-terns occur.
INDICATIONS AND CONTRAINDICATIONS FOR MISOPROSTOL ADMINISTRATIONThe indications for labor induction with titrated oral misoprostol are the same as those for labor induction with oxytocin, including post-term pregnancy, preeclamp-sia, diabetes mellitus, oligohydramnios, intrauterine fetal growth restriction, and abnormal antepartum fetal sur-veillance results. However, to avoid adverse events, it is important for practitioners to be alert to contraindica-tions, including a non-reassuring FHR pattern, uterine scarring, grand multiparity (≥ 5), any contraindication for labor or vaginal delivery or both, suspected placental abruption with an abnormal FHR pattern, and hypersen-sitivity to misoprostol or prostaglandin analogues.
ADVERSE EFFECTS AND TERATOGENICITY OF MISOPROSTOLIn published case reports[36-38], accidental overdosing with misoprostol resulted in pyrexia, hypoxia and rhabdomy-
83 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Misoprostol 1 (200 mcg) dissolved in water 200 mL
After 20 mL q1h × 4, still poor response
After 40 mL q1h × 4, still poor response
40 mL q1h × n (n : 1, 2, --, or n ) until adequate uterine
contractions
60 mL q1h × n (n : 1, 2, --, or n ) until adequate uterine
contractions
20 mL q1h × n (n : 1, 2, --, or n ) until adequate uterine
contractions
10 mL q1h × n (n : 1, 2, --, or n ) until adequate uterine
contractions
10 mL q1h × 4
If uterine contractionsBecome inadequate
Figure 1 Flowchart of misoprostol administration.
Cheng SY. Individualized misoprostol dosing for laboring women

olysis; all occurred with a single drug intake at a dosage exceeding 3000 µg. These adverse effects are signs of misoprostol toxicity and can be easily monitored when administering misoprostol. The other common side ef-fects are nausea, vomiting and diarrhea, but these side ef-fects rarely occur in the course of labor induction or aug-mentation with titrated oral misoprostol. Furthermore, these side effects are easily relieved by medication.
First trimester exposure to misoprostol is associated with facial paralysis[39], limb defects or vascular disruption defects[40,41] in newborns. In the Latina American Col-laborative Study of Congenital Malformations of 4673 malformed infants and 4980 control infants, increased frequencies of transverse limb defects, ring-shaped con-strictions of the extremities, arthrogryposis, hydrocepha-lus, holoprosencephaly and bladder exstrophy, but not Mobius syndrome, were observed in the infants exposed to misoprostol in utero[42]. There are no known reports of teratogenicity upon misoprostol ingestion when taken after the first trimester.
EFFICACY OF TITRATED ORAL MISOPROSTOLThe 1-h interval between titrated oral misoprostol ad-ministration based on pharmacokinetics has been proven to be effective in previous studies. One randomized con-trolled trial of titrated misoprostol compared titrated oral with vaginal misoprostol for labor induction[21]. Women between 34 and 42 wk of gestation with an unfavorable cervix (Bishop score ≤ 6) and an indication for labor in-duction were randomly assigned to receive titrated oral or vaginal misoprostol. The titrated oral misoprostol group received a basal unit dose of 20 mL of misoprostol solu-tion (1 µg/mL) every hour for 4 doses, then with titration based on individual uterine responses. The vaginal group received 25 µg every 4 h until attaining a more favorable cervix. Vaginal delivery within 12 h was the primary out-come. The data were analyzed on an intention-to-treat basis. Titrated oral misoprostol and vaginal misoprostol were given to 101 (48.8%) and to 106 (51.2%) women, respectively. Completed vaginal delivery occurred within 12 h in 75 (74.3%) women in the titrated oral group and 27 (25.5%) women in the vaginal group (P < 0.01; RR = 8.44; 95%CI: 4.52-15.76). Four women (4.0%) in the titrated oral group and 18 (17.0%) women in the vaginal group underwent cesarean deliveries (P < 0.01; RR = 0.20; 95%CI: 0.07-0.62). The incidence of hyperstimula-tion was 0.0% in the titrated oral group compared with 11.3% in the vaginal group (P < 0.01; RR = 0.08; 95%CI: 0.01-0.61). Although more women experienced nausea (10.9%) in the titrated oral group (P < 0.01; RR = 27.07; 95%CI: 1.57-465.70), fewer infants had Apgar scores of less than 7 at 1 min in the titrated oral group compared with the vaginal group (P < 0.01; RR = 0.10; 95%CI: 0.01-0.76). The conclusion was that titrated oral miso-prostol was associated with a lower incidence of uterine hyperstimulation and a lower cesarean delivery rate than
vaginal misoprostol for labor induction in patients with unfavorable cervix.
Another randomized controlled trial compared oral titrated misoprostol with intravenous oxytocin for labor augmentation in women at 36-42 wk of gestation with spontaneous onset of active labor[22]. Women meeting the general selection criteria of having regular contrac-tions, an effaced cervix dilated between 3 and 9 cm, and inadequate uterine contractions (2 or fewer contractions every 10 min) during the first stage of labor, were ran-domly assigned to titrated oral misoprostol or intravenous oxytocin. The augmentation-to-vaginal delivery interval and occurrence of vaginal delivery within 12 or 24 h were the primary outcomes. The data were analyzed on an intention-to-treat basis. Of the 231 women, 118 (51.1%) and 113 (48.9%) were randomized to titrated oral miso-prostol and titrated intravenous oxytocin, respectively. The median interval from the start of augmentation to vaginal delivery was 5.22 h (3.77-8.58 h, 25th-75th percentile) in the misoprostol group, and 5.20 h (3.23-6.50 h, 25th-75th percentile) in the intravenous oxytocin group (P = 0.019). Complete vaginal delivery occurred within 12 h for 92 (78.0%) women in the misoprostol group and 97 (85.8%) women in the oxytocin group (P = 0.121; RR = 0.91; 95%CI: 0.80-1.03). There were no significant differences between the 2 groups who delivered vaginally within 24 h. Twelve (10.2%) women in the misoprostol group and 13 (11.5%) women in the oxytocin group underwent cesar-ean deliveries (P = 0.744; RR = 0.88; 95%CI: 0.42-1.85). The side effects and neonatal outcomes also did not differ between the two groups. The conclusion was that labor augmentation with titrated oral misoprostol or intrave-nous oxytocin resulted in similar rates of vaginal delivery within 12 and 24 h.
A retrospective review of the medical records of all patients between 37 and 42 wk of gestation with a Bishop score ≤ 6 who underwent labor induction with titrated oral misoprostol solution[43] has also been conducted. The women were allocated into two groups: nulliparous and multiparous. The women received one basal unit of miso-prostol solution (20 mL, 1 µg/mL) every hour for four doses; additional doses were titrated based on individual uterine responses. The latent and active phase intervals and occurrence of vaginal delivery within 12 h were the primary outcomes. Of the 112 women included in the study, 49 (43.8%) nulliparae and 63 (56.2%) multiparae underwent labor induction with titrated oral misopros-tol solution. Although fewer women delivered vaginally within 12 h in the nulliparous group than in the multipa-rous group (42.9% vs 85.7%; P < 0.01; RR = 0.54; 95%CI: 0.39-0.76), there was no significant difference between the two groups regarding vaginal delivery within 24 h (87.8% vs 100.0%; P = 0.09; RR = 0.96; 95%CI: 0.90-1.02). Four (8.2%) women in the nulliparous group and none (0.0%) of the women in the multiparous group underwent cae-sarean deliveries (P = 0.02; RR = 1.09; 95%CI: 1.00-1.18). All induction durations, including the latent and active phases, were significantly shorter in the multiparous
84 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Cheng SY. Individualized misoprostol dosing for laboring women

group (P < 0.01). Induction failure did not occur in any patient in either of the groups. There was no instance of hyperstimulation, which was defined as tachysystole or hypertonus with a non-reassuring FHR pattern, although tachysystole, defined as the presence of at least 6 contrac-tions in 10 min over at least 2 10-min windows, occurred in 4 (8.2%) nulliparous women and 4 (6.3%) multiparous women. Hypertonus, defined as a single contraction last-ing more than 2 min, did not occur in either group. None of the neonates in either group had Apgar scores of < 7 at 1 min. The conclusion was that titrated oral misopro-stol solution was a promising method of labor induction for both nulliparous and multiparous women.
SUMMARY AND FUTURE PROSPECTSCesarean birth rates are greater than 20% in many devel-oped countries[44]. The main diagnoses contributing to the high rate of cesarean births in nulliparous women are dystocia and prolonged labor. Traditionally, a policy of vaginal dinoprostone for the treatment of an immature cervix or early amniotomy with oxytocin administration for mature cervices for the prevention of a delay in labor progress is associated with a modest reduction in the rate of cesarean births[45]. However, the course of vaginal dinoprostone or misoprostol is tedious, and excessive uterine contractility resulting in fetal distress is always a concern with the oral or vaginal use of fixed-dosage misoprostol. Oxytocin administration through the intra-venous route needs to be under the control of an intrave-nous pump and may be inconvenient in certain settings. Because titrated oral misoprostol solution is easier to administer than titrated intravenous oxytocin, it is worth conducting these treatment regimens for labor induction or augmentation. In addition, misoprostol offers several advantages over dinoprostone and oxytocin, including a longer shelf life, stability at room temperature, and easy administration. It is an ideal alternative to traditional dinoprostone or oxytocin for labor induction or aug-mentation. In consideration of inter- and intra-individual variations of drug response during the dosing course, it is reasonable that the titrated oral misoprostol solution may replace fixed-dosage misoprostol via the vaginal or oral route for labor induction or augmentation. In addition, the use of titrated oral misoprostol is superior to the tra-ditional use of vaginal misoprostol in completing vaginal deliveries to reduce the cesarean rate, based on previous randomized controlled trials[21]. However, further studies are needed to determine the minimal plasma misoprostol concentration necessary to induce a uterine response dur-ing labor induction at term and to validate the mathemat-ical model of titrated oral misoprostol. This information will help ensure the obstetric use of misoprostol.
REFERENCES1 Waldenström U, Hildingsson I, Rubertsson C, Rådestad I.
A negative birth experience: prevalence and risk factors in a national sample. Birth 2004; 31: 17-27 [PMID: 15015989 DOI:
10.1111/j.0730-7659.2004.0270.x]2 Nystedt A, Högberg U, Lundman B. Some Swedish women’
s experiences of prolonged labour. Midwifery 2006; 22: 56-65 [PMID: 16488810 DOI: 10.1016/j.midw.2005.05.003]
3 Bugg GJ, Stanley E, Baker PN, Taggart MJ, Johnston TA. Outcomes of labours augmented with oxytocin. Eur J Obstet Gynecol Reprod Biol 2006; 124: 37-41 [PMID: 15955617 DOI: 10.1016/j.ejogrb.2005.04.015]
4 Florica M, Stephansson O, Nordström L. Indications associ-ated with increased cesarean section rates in a Swedish hos-pital. Int J Gynaecol Obstet 2006; 92: 181-185 [PMID: 16364324 DOI: 10.1016/j.ijgo.2005.10.016]
5 ACOG Committee Opinion. American College of Obstetri-cian and Gynecologist. ACOG Committee Opinion. Num-ber 283, May 2003. New U.S. Food and Drug Administration labeling on Cytotec (misoprostol) use and pregnancy. Obstet Gynecol 2003; 101: 1049-1050 [PMID: 12738178]
6 Keirse MJ. Prostaglandins in preinduction cervical ripening. Meta-analysis of worldwide clinical experience. J Reprod Med 1993; 38: 89-100 [PMID: 8429533]
7 Sanchez-Ramos L, Kaunitz AM, Del Valle GO, Delke I, Schro-eder PA, Briones DK. Labor induction with the prostaglandin E1 methyl analogue misoprostol versus oxytocin: a random-ized trial. Obstet Gynecol 1993; 81: 332-336 [PMID: 8437780]
8 Hofmeyr GJ, Gülmezoglu AM, Alfirevic Z. Misoprostol for induction of labour: a systematic review. Br J Obstet Gynaecol 1999; 106: 798-803 [PMID: 10453829 DOI: 10.1111/j.1471-0528.1999.tb08400.x]
9 Wing DA. Labor induction with misoprostol. Am J Obstet Gynecol 1999; 181: 339-345 [PMID: 10454679]
10 Bennett KA, Butt K, Crane JM, Hutchens D, Young DC. A masked randomized comparison of oral and vaginal administration of misoprostol for labor induction. Obstet Gynecol 1998; 92: 481-486 [PMID: 9764615 DOI: 10.1016/S0029-7844(98)00226-9]
11 Kolderup L, McLean L, Grullon K, Safford K, Kilpatrick SJ. Misoprostol is more efficacious for labor induction than prostaglandin E2, but is it associated with more risk? Am J Obstet Gynecol 1999; 180: 1543-1550 [PMID: 10368502]
12 Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Da-tabase Syst Rev 2001; CD000941 [PMID: 11686970 DOI: 10.1002/14651858.CD000941]
13 Shetty A, Danielian P, Templeton A. A comparison of oral and vaginal misoprostol tablets in induction of labour at term. BJOG 2001; 108: 238-243 [PMID: 11281461 DOI: 10.1111/.1471-0528.2001.00073.x]
14 Shetty A, Danielian P, Templeton A. Sublingual misoprostol for the induction of labor at term. Am J Obstet Gynecol 2002; 186: 72-76 [PMID: 11810088 DOI: 10.1067/mob.2002.118917]
15 Shetty A, Martin R, Danielian P, Templeton A. A compari-son of two dosage regimens of oral misoprostol for labor induction at term. Acta Obstet Gynecol Scand 2002; 81: 337-342 [PMID: 11952465 DOI: 10.1034/j.1600-0412.2002.810411.x]
16 Alfirevic Z, Weeks A. Oral misoprostol for induction of labour. Cochrane Database Syst Rev 2006; CD001338 [PMID: 16625542 DOI: 10.1002/14651858.CD001338.pub2]
17 Weeks A, Alfirevic Z. Oral misoprostol administration for labor induction. Clin Obstet Gynecol 2006; 49: 658-671 [PMID: 16885670]
18 Hofmeyr GJ, Matonhodze BB, Alfirevic Z, Campbell E, de Jager M, Nikodem C. Titrated oral misoprostol solution--a new method of labour induction. S Afr Med J 2001; 91: 775-776 [PMID: 11680329]
19 Hofmeyr GJ, Alfirevic Z, Matonhodze B, Brocklehurst P, Campbell E, Nikodem VC. Titrated oral misoprostol solu-tion for induction of labour: a multi-centre, randomised trial. BJOG 2001; 108: 952-959 [PMID: 11563466 DOI: 10.1111/j.1471-0528.2001.00231.x]
20 Cheng SY, Chen TC. Pilot study of labor induction with titrat-
85 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Cheng SY. Individualized misoprostol dosing for laboring women

86 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
ed oral misoprostol. Taiwan J Obstet Gynecol 2006; 45: 225-229 [PMID: 17175468 DOI: 10.1016/S1028-4559(09)60229-1]
21 Cheng SY, Ming H, Lee JC. Titrated oral compared with vaginal misoprostol for labor induction: a randomized controlled trial. Obstet Gynecol 2008; 111: 119-125 [PMID: 18165400 DOI: 10.1097/01.AOG.0000297313.68644.71]
22 Ho M, Cheng SY, Li TC. Titrated oral misoprostol solution compared with intravenous oxytocin for labor augmentation: a randomized controlled trial. Obstet Gynecol 2010; 116: 612-618 [PMID: 20733443 DOI: 10.1097/AOG.0b013e3181ed36cc]
23 Souza AS, Scavuzzi A, Rodrigues DC, Oliveira RD, Fei-tosa FE, Amorim MM. [Titrated oral solution of misopro-stol for labour induction: a pilot study]. Rev Bras Ginecol Obstet 2010; 32: 208-213 [PMID: 21085749 DOI: 10.1590/S0100-72032010000500002]
24 Matonhodze BB, Hofmeyr GJ, Levin J. Labour induction at term--a randomised trial comparing Foley catheter plus ti-trated oral misoprostol solution, titrated oral misoprostol so-lution alone, and dinoprostone. S Afr Med J 2003; 93: 375-379 [PMID: 12830603]
25 Bricker L, Peden H, Tomlinson AJ, Al-Hussaini TK, Idama T, Candelier C, Luckas M, Furniss H, Davies A, Kumar B, Roberts J, Alfirevic Z. Titrated low-dose vaginal and/or oral misoprostol to induce labour for prelabour membrane rup-ture: a randomised trial. BJOG 2008; 115: 1503-1511 [PMID: 18752586 DOI: 10.1111/j.1471-0528.2008.01890.x]
26 Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorption kinetics of misoprostol with oral or vaginal ad-ministration. Obstet Gynecol 1997; 90: 88-92 [PMID: 9207820 DOI: 10.1016/S0029-7844(97)00111-7]
27 Foote EF, Lee DR, Karim A, Keane WF, Halstenson CE. Dis-position of misoprostol and its active metabolite in patients with normal and impaired renal function. J Clin Pharmacol 1995; 35: 384-389 [PMID: 7650228]
28 http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm154498.htm
29 Wing DA, Lovett K, Paul RH. Disruption of prior uterine incision following misoprostol for labor induction in women with previous cesarean delivery. Obstet Gynecol 1998; 91: 828-830 [PMID: 9572178]
30 Choy-Hee L, Raynor BD. Misoprostol induction of labor among women with a history of cesarean delivery. Am J Obstet Gynecol 2001; 184: 1115-1117 [PMID: 11349173 DOI: 10.1067/mob.2001.115177]
31 Blanchette HA, Nayak S, Erasmus S. Comparison of the safety and efficacy of intravaginal misoprostol (prostaglandin E1) with those of dinoprostone (prostaglandin E2) for cervi-cal ripening and induction of labor in a community hospital. Am J Obstet Gynecol 1999; 180: 1551-1559 [PMID: 10368503 DOI: 10.1016/S0002-9378(99)70051-7]
32 Bennett BB. Uterine rupture during induction of labor at term with intravaginal misoprostol. Obstet Gynecol 1997; 89: 832-833 [PMID: 9166339 DOI: 10.1016/S0029-7844(97)00036-7]
33 Khabbaz AY, Usta IM, El-Hajj MI, Abu-Musa A, Seoud M, Nassar AH. Rupture of an unscarred uterus with misopros-tol induction: case report and review of the literature. J Ma-tern Fetal Med 2001; 10: 141-145 [PMID: 11392596]
34 Thomas A, Jophy R, Maskhar A, Thomas RK. Uterine rup-ture in a primigravida with misoprostol used for induction of labour. BJOG 2003; 110: 217-218 [PMID: 12618171]
35 Chong YS, Chua S, Shen L, Arulkumaran S. Does the route of administration of misoprostol make a difference? The uterotonic effect and side effects of misoprostol given by dif-ferent routes after vaginal delivery. Eur J Obstet Gynecol Re-prod Biol 2004; 113: 191-198 [PMID: 15063959 DOI: 10.1016/j.ejogrb.2003.09.011]
36 Graber DJ, Meier KH. Acute misoprostol toxicity. Ann Emerg Med 1991; 20: 549-551 [PMID: 1902633]
37 Bond GR, Van Zee A. Overdosage of misoprostol in preg-nancy. Am J Obstet Gynecol 1994; 171: 561-562 [PMID: 8059844]
38 Austin J, Ford MD, Rouse A, Hanna E. Acute intravaginal misoprostol toxicity with fetal demise. J Emerg Med 1997; 15: 61-64 [PMID: 9017489 DOI: 10.1016/S0736-4679(96)00257-0]
39 Pastuszak AL, Schüler L, Speck-Martins CE, Coelho KE, Cordello SM, Vargas F, Brunoni D, Schwarz IV, Larranda-buru M, Safattle H, Meloni VF, Koren G. Use of misoprostol during pregnancy and Möbius’ syndrome in infants. N Engl J Med 1998; 338: 1881-1885 [PMID: 9637807 DOI: 10.1056/NEJM199806253382604]
40 Gonzalez CH, Marques-Dias MJ, Kim CA, Sugayama SM, Da Paz JA, Huson SM, Holmes LB. Congenital abnormali-ties in Brazilian children associated with misoprostol misuse in first trimester of pregnancy. Lancet 1998; 351: 1624-1627 [PMID: 9620717 DOI: 10.1016/S0140-6736(97)12363-7]
41 Vargas FR, Schuler-Faccini L, Brunoni D, Kim C, Meloni VF, Sugayama SM, Albano L, Llerena JC, Almeida JC, Duarte A, Cavalcanti DP, Goloni-Bertollo E, Conte A, Koren G, Addis A. Prenatal exposure to misoprostol and vascular disrup-tion defects: a case-control study. Am J Med Genet 2000; 95: 302-306 [PMID: 11186881]
42 Orioli IM, Castilla EE. Epidemiological assessment of misoprostol teratogenicity. BJOG 2000; 107: 519-523 [PMID: 10759272 DOI: 10.1111/j.1471-0528.2000.tb13272.x]
43 Cheng SY, Hsue CS, Hwang GH, Chen W, Li TC. Compari-son of labor induction with titrated oral misoprostol solu-tion between nulliparous and multiparous women. J Obstet Gynaecol Res 2010; 36: 72-78 [PMID: 20178530 DOI: 10.1111/j.1447-0756.2009.01118.x]
44 Betrán AP, Merialdi M, Lauer JA, Bing-Shun W, Thomas J, Van Look P, Wagner M. Rates of caesarean section: analysis of global, regional and national estimates. Paediatr Perinat Epidemiol 2007; 21: 98-113 [PMID: 17302638 DOI: 10.1111/j.1365-3016.2007.00786.x]
45 O’Driscoll K, Foley M, MacDonald D. Active management of labor as an alternative to cesarean section for dystocia. Obstet Gynecol 1984; 63: 485-490 [PMID: 6700893]
P- Reviewers: Mohammed Usta I, Rovas L, Tong C S- Editor: Zhai HH L- Editor: Roemmele A E- Editor: Zheng XM
Cheng SY. Individualized misoprostol dosing for laboring women

cheap, safe and well-tolerated alternative to HRT.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Folic acid; Hot flushes; Menopause; Nor-adrenaline; Serotonin
Core tip: Hormone replacement therapy usage by post-menopausal women with hot flushes causes concerns over possible increased risks particularly breast can-cer. The improved longevity of women in general and breast cancer survivors in particular, and the limited success shown by the non-hormonal alternatives made it imperative to find a therapy that is effective and safe. It is hypothesized that folic acid supplementation may ameliorate hot flushes by the same mechanism as es-trogen supplementation, i.e. , by reducing noradrenaline and increasing serotonin neurotransmitters. This article discusses the rationale, potential role, mechanisms of action and safety issues related to its use in these women.
Ewies AAA. Folic acid supplementation: The new dawn for postmenopausal women with hot flushes. World J Obstet Gy-necol 2013; 2(4): 87-93 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/87.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.87
CURRENT DILEMMAHot flushes, the most characteristic menopausal symp-tom, are experienced by up to 75% of menopausal wom-en, and in half of them symptoms are severe enough to seek medical advice[1]. Hot flushes are associated with estrogen deprivation and they are the most commonly re-ported side effect of the selective estrogen receptor mod-ulators[2]. Therefore, hormone replacement therapy (HRT)
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.87
World J Obstet Gynecol 2013 November 10; 2(4): 87-93ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Folic acid supplementation: The new dawn for postmenopausal women with hot flushes
Ayman AA Ewies
Ayman AA Ewies, Sandwell and West Birmingham Hospitals NHS Trust, Birmingham City Hospital, Birmingham B18 7QH, West Midlands, United KingdomAuthor contributions: Ewies AAA solely contributed to this paper.Correspondence to: Ayman A A Ewies, MBChB, MSc, FRCOG, MD, Consultant Gynaecologist, Sandwell and West Birmingham Hospitals NHS Trust, Birmingham City Hospital, Dudley Road, Birmingham B18 7QH, West Midlands, United Kingdom. [email protected]: +44-121-5074042 Fax: +44-121-5075680Received: March 29, 2013 Revised: June 12, 2013Accepted: June 18, 2013Published online: November 10, 2013
AbstractHot flushes, experienced by 75% of menopausal women, are associated with estrogen deprivation. Estrogen was shown to ameliorate hot flushes by interacting with monoamine neurotransmitters in the brain; reducing noradrenaline and increasing serotonin. Hormone re-placement therapy (HRT), the first treatment option, causes concerns over possible increased risks particularly breast cancer. Folic acid is involved in the biosynthesis of serotonin and nordrenaline, which is responsible for its effects on mood and cognition, and degrees of folate inadequacy, not severe enough to produce megaloblastic anaemia, were found to be associated with depression and cognitive malfunctioning. Also, increased age was observed to relate to reduced serum and cerebrospinal fluid folic acid levels. There is emerging evidence that folic acid supplementation ameliorates hot flushes by the same mechanism as estrogen. To explore this hypothesis, a multi-centre, double-blind, placebo-controlled random-ized is being set up to compare the effect of 5 mg folic acid vs placebo in reducing the frequency and severity of hot flushes in postmenopausal women, and on the blood level of serotonin and noradrenaline. If folic acid supple-mentation is demonstrated to be effective, this will be a turning point in the clinical practice since it represents a
THERAPEUTIC ADVANCES
87 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Ewies AAA. Folic acid supplementation and hot flushes
is the first treatment option[3]. However, the perception of the risks and benefits of HRT had changed since the publication of Women’s Health Initiative Trial in 2002[4], and an increasing number of women are seeking alterna-tives for conventional HRT because of the concerns over possible increased risks particularly breast cancer[3]. In ad-dition, there is evidence that non-hormonal mechanisms play an important role in the pathophysiology of hot flushes[3,5].
Treatment of breast and endometrial cancer frequent-ly results in the loss of ovarian function and menopausal symptoms. Symptoms of iatrogenic menopause are usu-ally more intense than those of natural menopause due to sudden onset of symptoms, younger age, and the physical and psychological impacts such as body image concerns and sexual dysfunction[6]. Furthermore, the improved longevity of breast cancer patients and the increased use, in recent years, of aromatase inhibitors over tamoxifen, leading to profound estrogen deprivation[7,8], made it imperative to find a therapy that is effective and safe. In addition, the use HRT in breast and endometrial cancer survivors is not welcomed by most women and doctors because of the potential stimulation of residual cancer and the induction of new hormone-sensitive disease[9]. The non-hormonal alternatives which are commonly proposed to these women showed a limited success[3,10-12].
HOT FLUSHES - THE MECHANISM AND ROLE OF ESTROGENThe entire episode of hot flushes usually lasts no more than 1-3 min. The frequency can range from 5 per year to 50 per day, with great variations among individuals or even within an individual, although 5-10 times per day is more common. They generally persist for 1 to 5 years, but in some women they can continue for as long as 44 years. There is no accepted metric for measuring severity of hot flushes[13].
Hot flushes exact aetiology is not yet understood. Although many theories were postulated to explain the pathophysiology, none of them could explain all aspects of hot flushes. Estrogen replacement was shown to ame-liorate hot flushes by interacting with monoamine neu-rotransmitters in the brain; noradrenaline and serotonin [5-hydroxytryptamine (5-HT)][1,2].
It was hypothesized that hot flushes are triggered within the hypothalamus by α2-adrenergic receptors on noradrenergic neurons. There is evidence to suggest increased central noradrenergic activity in women suffer-ing from flushes, leading to disturbances in the thermo-regulatory centre which is probably responsible for the occurrence of flushes[14]. It was found that yohimbine, an α2-adrenergic antagonist, increased central noradrenaline release, provoking hot flushes, while clonidine, an α2-adrenergic agonist, reduced central noradrenaline release, raised the sweating threshold and lowered the shivering threshold, leading to amelioration of flushes[14-16]. This theory was further supported by finding significantly el-
evated plasma levels of 3-methoxy 4-hydroxy phenyl gly-col (MHPG), the end metabolite of brain noradrenaline in women with hot flushes[17,18].
Furthermore, it was found that 5-HT1A, 5-HT2A and
5-HT7 receptors are implicated in hypothalamic control of temperature[2,19]. It was hypothesized that hot flushes are the net result of activation of estrogen withdrawal induced up regulated 5-HT2A receptors in the hypothala-mus by mild internal or external stimuli such as high am-bient temperatures, anxiety, coffee, or alcohol, resulting in a hyperthermic response[5]. Estrogen affects the func-tion of serotonin neural system, and the blood levels of serotonin fluctuate with the circulating levels of estrogen. In spontaneous and surgically menopausal women, it was found that blood levels of serotonin were reduced by about 50% when compared to premenopausal controls and estrogen replacement restored levels to normal[20]. Further, estrogen replacement in postmenopausal women augmented serotonergic activity, increased the excretion of 5-hydroxyindoleacetic acid (5-HIAA; the main me-tabolite of serotonin)[21] and increased the expression of tryptophan hydroxylase, the key enzyme in serotonin bio-synthesis[19]. In addition, a number of serotonergic com-pounds such as serotonin re-uptake inhibitors fluoxetine, venlafaxine, sertraline and paroxetine, and the serotonin disinhibition mianserin and mirtazapine were shown to reduce both the number and intensity of hot flushes[5].
FOLIC ACID: WHAT CLINICIANS NEED TO KNOW?Background Folic acid, a water-soluble B-Vitamin, serves as the parent for a large family of compounds having similar nutritional value to which the generic term “folates” is applied[22]. As per the definition of a vitamin, it cannot be synthesized de novo, and must be derived from diet or supplementation. Dietary folates is found in leafy green vegetables, legumes, beans, liver, citrus fruits and yeast[23]. The name “folate” derives from the Latin for leaf (folia) since leafy green vegetables do contain folate[24,25]. Multiple biochemical conversions are required for dietary folates to become tet-rahydrofolates; the metabolically active and tissue-usable forms. Folates are involved - via donation of a methyl group - in numerous biochemical pathways including monoamine neurotransmitters synthesis, which is respon-sible for its effects on mood and cognition[23-25].
PharmacokineticsFolic acid, the synthetic molecule, is highly absorbed (85%-95%) when compared to the dietary form (50%). Folate absorption takes place in the lumen of the proxi-mal small intestine. After assimilation by the intestinal ep-ithelial cells, a substantial fraction of the absorbed folate is methylated and reduced, partly through the action of “methylene tetrahydrofolate reductase enzyme”, to 5-me-thyl tetrahydrofolate, which is the main circulating form of folic acid[23]. Vitamin B12 is involved in the methyla-
88 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

tion of homocysteine to methionine, which is needed to convert 5-methyl tetrahydrofolate to tetrahydrofolate[22]. The peak folate serum level after oral administration is reached within 30 to 60 min. The average value of folic acid in serum is 7-36 nmol/L. Tetrahydrofolate and its derivatives are distributed in all body tissues. The liver, the principal storage site, contains half of the total body stores followed by erythrocytes. The normal erythrocyte level is about 320-1300 nmol/L[25,26].
Safety Folic acid is usually well-tolerated with no adverse effects associated with the consumption of excess folates from food in human[24,27]. Daily oral supplements of 5-10 mg synthetic folic acid appear to be well tolerated and rarely cause side effects in healthy individuals[28-30]. A few cases of allergic reactions have been reported including skin rash, swelling of the face, lips, tongue or throat, or bron-chospasm[26,31,32]. Caution is necessary in administering folic acid supplements alone in megaloblastic anaemia. If the cause is vitamin B12 deficiency, the megaloblastic anaemia may be corrected , but any nuerological manifes-tations (e.g., subacute combined degeneration of the cord) are likely to get worse[24]. Folic acid supplements should be used with cautions also in patients with epilepsy because seizures activity may be induced since it reduces the serum level of some anti-convulsants[28]. A recent meta-analysis found no increase in overall and site-specific cancer in-cidence in the randomized controlled trials of folic acid supplementation at doses higher than those from fortifi-cation. It included 13 trials (with 49621 participants) that compared folic acid vs placebo, had treatment duration of at least 1 year, and included at least 500 participants. It was found that, during an average treatment duration of 5.2 years, folic acid supplementation increased folate serum concentrations by 4-fold (573 nmol/L for the folic acid groups vs 135 nmol/L for the placebo groups), but had no significant effect on overall cancer incidence (1904 cancers in the folic acid groups vs 1809 cancers in the placebo groups, RR = 1.06, 95%CI: 0.99-1.13, P = 0.10). There was also no trend towards greater effect with longer treatment durations[33].
HOW FOLIC ACID COULD AFFECT BRAIN FUNCTIONFolic acid is essential for the functioning of the ner-vous system. It is necessary for the biosynthesis of the monoamine neurotransmitters serotonin, noradrenaline and dopamine. 5-methyltetrahydrofolate, participates in re-methylation of the amino acid metabolite homocys-teine, creating methionine. The downstream metabo-lite of methionine; S-adenosylmethionine, is involved in numerous one-carbon methylation reactions in the body, including those that create neurotransmitters, i.e., S-adenosylmethionine must be present as a methyl donor for both the serotonin and catecholamine pathways to function properly. After donation of its methyl group,
S-adenosylmethionine becomes homocysteine[23,34,35]. At this point, homocysteine must either be further metabo-lized to become cysteine, taurine, and glutathione or re-methylated to become methionine again. Re-methylation is done via “methionine synthetase”, which facilitates the donation of a methyl group from vitamin B12 (which gets its methyl group from 5-methyltetrahydrofolate). Therefore, some researchers believe homocysteine is sim-ply a marker of folate and/or B12 deficiency. Without the participation of 5-methyltetrahydrofolate in this pro-cess, S-adenosylmethionine and neurotransmitter levels decrease in the cerebrospinal fluid[23,34,35].
5-methyltetrahydrofolate also appears to stabilize, enhance production of, or possibly act as a substitute for tetrahydrobiopterin (BH4), which is an essential nutrient cofactor in the biosynthesis monoamine neurotransmit-ters serotonin, dopamine, noradrenaline, and adrena-line[23,34,35]. It appears to be important in regenerating BH4, which is highly susceptible to oxidation. In the absence of an adequate amount of BH4, 5-methyl tetrahydrofolate may substitutes for BH4 in the “hydroxylase enzymes” involved in monoamine neurotransmitters synthesis[36,37].
Folic acid deficiency in depression and old age Over the past four decades, degrees of folate deficiency not severe enough to produce megaloblastic anaemia, were found to be associated with psychological symp-toms, particularly depressive symptoms (e.g., apathy, fa-tigue, insomnia, irritability and concentration difficulties) and impaired cognitive functioning[38-40]. Up to 71% of individuals with severe folic acid deficiency were found to have depression[41], and a French study found a significant association between high folate intake and a lower risk of depression in middle-aged men and women[42]. Bottiglieri et al[34], in a study of 46 inpatients with severe depression, found that 52% of them were having high homocysteine. Further, depressed patients with increased serum ho-mocysteine had significantly lower (1) serum, red blood cell and cerebrospinal fluid folate; (2) cerebrospinal fluid S-adenosylmethionine; and (3) the metabolites of sero-tonin, noradrenaline and dopamine.
Several studies reported that low blood levels of folate and vitamin B12, and high levels of homocysteine were correlated with depression especially in the elderly[34,40,41]. A recent meta-analysis of 11 studies (n = 15315) found a significant relationship between the risk of depres-sion and low folate status[43,44], and it was reported that 15%-38% of adults with severe depression had border-line or low serum and red blood cell folic acid[23,45-47]. It is estimated that 20%-30% of individuals with depression have also high homocystein levels[35,43,48-50]. Investigations revealed a connection between high homocysteine levels and brain dysfunction, including cognitive function, de-mentia, Alzheimer’s disease, and depression[23] because it has a neurotoxic effect through several mechanisms, including impaired methylation, excitotoxicity, oxidative stress and hypoxia in the central nervous system[49]. Folate deficiency, by elevating homocysteine levels, may have a
89 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ewies AAA. Folic acid supplementation and hot flushes

role in depression[51], and folic acid supplementation was shown to reduce elevated homocysteine levels[52].
Increased age has been observed to relate to reduced serum and cerebrospinal fluid folic acid concentrations, and with increased, homocysteine levels at the same time[43]. The results of the studies are conflicting as re-gards the relation between depression and serum folic acid level in elderly population with some failing to iden-tify a relationship[51,53] and others showing an inverse rela-tionship[54,55]. It may be argued that folic acid deficiency in individuals with depression, particularly the elderly, might be attributed to poor nutrition, medication, chronic dis-ease, increased needs, or malabsorption; however, low folic acid levels were observed in overweight individu-als with depression, and in individuals who had gained weight inadvertently[40,47].
FOLIC ACID MAY CURE HOT FLUSHES: THE CLINICAL EVIDENCE SO FARThe scientific literatures were searched using NHS evi-dence website: www.evidence.nhs.uk on March 4, 2013. Then under Journals and Databases, “Healthcare Databas-es Advanced Search” was accessed and the following data-bases were searched; AMED, BNI, CINAHL, EMBASE, HEALTH BUSINESS ELITE; HMIC, MEDLINE, PsycINFO. The key words for search were: “folic acid and menopausal women” and “folic acid and hot flushes”. The search result was combined using “OR” and retrieved 44 articles. Only one original article[56], an abstract[57] and a hypothesis[58] were found (n = 3). The rest of the articles have been excluded; duplicates (n = 22) or non-relevant articles (n = 19).
Gaweesh et al[56], in a small prospective cohort study, examined the effect of folic acid 5 mg supplementation vs placebo for 4 wk on the occurrence of hot flushes in 46 healthy postmenopausal Egyptian women. In the treatment group, there was significant improvement of symptoms and significant lowering in plasma levels of MHPG. There was significant negative correlation be-tween clinical improvement in hot flushes and the plasma level of MHPG. The improvement was described as “good” on complete disappearance of hot flushes, and “moderate” when the frequency and intensity of the flushes were satisfactorily reduced. The level of improve-ment was subjectively decided by women based on their overall feeling as regards the number and intensity of hot flushes. In the treatment group, 9 (39.1%), 6 (26.1%) and 8 (34.8%) women had good, moderate and no im-provement, respectively. The equivalent figures for the control group were 1 (5.3%), 2 (10.5%) and 16 (84.2%), respectively. The number of women who had good im-provement was significantly higher in the treatment group (P = 0.01), but the difference between the two groups as regards moderate improvement did not reach statistical significance (P = 0.26). The number of women who had no improvement was significantly higher (P = 0.002) in the control group. On comparing the mean plasma levels
of MHPG before and after treatment in both groups, a significant lowering in mean level was found in the treat-ment group (t = 6.12, mean % change = -24.1 ± 17.9, P < 0.001) when compared with the control group (t = 1.72, mean % change = -5.59 ± 16.4, P = 0.10). In the treatment group, the test of correlation [Spearman’s rank correlation coefficient (r)] showed a significant negative correlation between clinical improvement in hot flushes and the plasma level of MHPG (r = -0.453, P = 0.03).
Although these results are encouraging, the study had many limitations. First, the study was underpowered with small number of participants which is not sufficient to generalize the results. Second, folic acid supplementation was given for a short duration disallowing evaluation of its benefit on the medium and long terms. Last, the bias in allocation and assessment cannot be excluded since it is not a randomized double blind controlled study.
The second study, which was published as an abstract and included two groups (n = 20 each), investigated the effect of 5 mg folic acid supplementation for 4 wk vs no treatment. The treatment group demonstrated an average of 57% reduction in the frequency in hot flushes by the 4th week of treatment, while no change was observed in the control group[57].
HOW MIGHT FOLIC ACID AMELIORATE HOT FLUSHES?Hot flushes possibly occur because of the increased cen-tral noradrenergic activity leading to disturbances in the thermoregulatory centre[14,17,18], and/or activation of es-trogen withdrawal induced up-regulated 5-HT2A receptors in the hypothalamus by mild internal or external stimuli resulting in a hyperthermic response[5]. Animal studies reported that folic acid, like estrogen, reduced noradrena-line secretion[59,60], and increased serotonin activity[59]. It was found that folic acid administered to mice produced an antidepressant-like effect mediated by an interaction with the noradrenergic receptors (α1 and α2) and seroto-nergic receptors (5-HT1A and 5-HT2A/2C)[59].
It was suggested that the link between folate and noradrenaline and serotonin metabolism is probably through BH4 since there is a significant positive correla-tion between its CSF levels with that of 5-HIAA and red cell folate in patients with severe depression[34,61]. As previously mentioned, 5-methyltetrahydrofolate appears to stabilize, enhance production of, or possibly act as a substitute for BH4, which an essential nutrient cofactor in the biosynthesis of serotonin and noradrenaline[23,34,35]. 5-methyltetrahydrofolate causes a significant reduction in the noradrenaline secretion to only 12.9% of control release, probably by duplicating the rate limiting behav-iour of a synthetic pteridine cofactor “DL,2-amino-4-hydroxy-6,7,dimethyltetrahydropteridine”[60]. Further, folate deficiency was associated with decreased serotonin activity[38], and supplementation with folic acid increased CSF levels of 5-HIAA in folate deficient patients with depression[62]. Interestingly, it was found that the regional
90 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ewies AAA. Folic acid supplementation and hot flushes

distribution of 5-methyltetrahydrofolate in the brain was similar to that of serotonin[63].
Słopien et al[64] suggested that there might be a role for folate and possible methionine metabolism involve-ment in the development of depression in postmeno-pausal women, and it was also reported that there is an association between hot flushes and high rate of depres-sion both in postmenopausal[65-67] and perimenopausal women[68].
THE FUTUREIt is plausible to assume that folic acid supplementation objectively ameliorates hot flushes by the same mecha-nism as estrogen replacement, i.e., by interacting with monoamine neurotransmitters in the brain; namely nor-adrenaline and serotonin. It lowers noradrenaline and increases serotonin activities. Nevertheless, there is a need for well designed studies: (1) To investigate the effect of folic acid supplementation on the frequency and severity of hot flushes; (2) To explore whether symptomatic post-menopausal women are deficient in folate, and which pa-tients are most suitable for folic acid therapy. It should be borne in mind that folate levels in the normal range might still be inadequate for the purpose of methyl donation and neurotransmitter synthesis in some individuals[23]; (3) To find out the optimum dose and the proper duration of therapy. Although 5 mg folic acid supplementation is con-sidered as the standard dose, some investigators alleged that small doses up to 2 mg administered over a long time span may be preferable because the entry of folate in the nervous system is limited by the blood brain barrier, thus rendering large quantities inefficient[41]; and (4) To study the correlation between folate levels and monoamine neu-rotransmitters serotonin and noradrenaline.
To resolve some of these issues, a multi-centre, dou-ble-blind, placebo-controlled randomized, phase III trial is being set up and sponsored by “University of Birming-ham” and “Sandwell and West Birmingham Hospitals NHS Trust”, United Kingdom to directly compare the ef-fect of 5mg folic acid vs placebo in reducing the frequency and severity of hot flushes in postmenopausal women, and on the blood level of monoamine neurotransmitters serotonin and noradrenaline. If folic acid supplementa-tion is demonstrated to be effective, this will be a turning point in the clinical practice worldwide since it represents a cheap, safe, well-tolerated alternative to the conventional HRT, particularly in breast and endometrial cancer survi-vors who have no options at the moment but to live with their disabling symptoms.
REFERENCES1 Freedman RR. Hot flashes: behavioral treatments, mecha-
nisms, and relation to sleep. Am J Med 2005; 118 Suppl 12B: 124-130 [PMID: 16414337 DOI: 10.1016/j.amjmed.2005.10.022]
2 Berendsen HH. The role of serotonin in hot flushes. Ma-turitas 2000; 36: 155-164 [PMID: 11063896 DOI: 10.1016/S0378-5122(00)00151-1]
3 Alfhaily F, Ewies AA. Acupuncture in managing menopaus-al symptoms: hope or mirage? Climacteric 2007; 10: 371-380 [PMID: 17852139 DOI: 10.1080/13697130701612315]
4 Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Jackson RD, Beresford SA, Howard BV, Johnson KC, Kotchen JM, Ockene J. Risks and benefits of estrogen plus progestin in healthy postmeno-pausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288: 321-333 [PMID: 12117397 DOI: 10.1001/jama.288.3.321]
5 Mann JJ, Stanley M, McBride PA, McEwen BS. Increased se-rotonin2 and beta-adrenergic receptor binding in the frontal cortices of suicide victims. Arch Gen Psychiatry 1986; 43: 954-959 [PMID: 3019268 DOI: 10.1001/archpsyc.1986.01800100048007]
6 Singh P, Oehler MK. Hormone replacement after gynaeco-logical cancer. Maturitas 2010; 65: 190-197 [PMID: 20018467 DOI: 10.1016/j.maturitas.2009.11.017]
7 Haspels AA, Luisi M, Kicovic PM. Endocrinological and clinical investigations in post-menopausal women following administration of vaginal cream containing oestriol. Maturi-tas 1981; 3: 321-327 [PMID: 6801440 DOI: 10.1016/0378-5122(81)90041-4]
8 Morales L, Neven P, Timmerman D, Christiaens MR, Ver-gote I, Van Limbergen E, Carbonez A, Van Huffel S, Ameye L, Paridaens R. Acute effects of tamoxifen and third-generation aromatase inhibitors on menopausal symptoms of breast cancer patients. Anticancer Drugs 2004; 15: 753-760 [PMID: 15494636 DOI: 10.1097/00001813-200409000-00003]
9 Biglia N, Mariani L, Marenco D, Robba C, Peano E, Kubatzki F, Sismondi P. Hormonal replacement therapy after gynae-cological cancer. Gynakol Geburtshilfliche Rundsch 2006; 46: 191-196 [PMID: 17068403 DOI: 10.1159/000095727]
10 Elshafie MA, Ewies AA. Transdermal natural progester-one cream for postmenopausal women: inconsistent data and complex pharmacokinetics. J Obstet Gynaecol 2007; 27: 655-659 [PMID: 17999287 DOI: 10.1080/01443610701582727]
11 Ewies AA. A comprehensive approach to the menopause: so far, one size should fit all. Obstet Gynecol Surv 2001; 56: 642-649 [PMID: 11590315 DOI: 10.1097/00006254-200110000-00023]
12 Ewies AA. Phytoestrogens in the management of the meno-pause: up-to-date. Obstet Gynecol Surv 2002; 57: 306-313 [PMID: 11997677 DOI: 10.1097/00006254-200205000-00023]
13 Feldman BM, Voda A, Gronseth E. The prevalence of hot flash and associated variables among perimenopausal wom-en. Res Nurs Health 1985; 8: 261-268 [PMID: 3852361 DOI: 10.1002/nur.4770080308]
14 Freedman RR, Woodward S, Sabharwal SC. Alpha 2-adren-ergic mechanism in menopausal hot flushes. Obstet Gynecol 1990; 76: 573-578 [PMID: 2170883]
15 Delaunay L, Herail T, Sessler DI, Lienhart A, Bonnet F. Clonidine increases the sweating threshold, but does not reduce the gain of sweating. Anesth Analg 1996; 83: 844-848 [PMID: 8831332 DOI: 10.1097/00000539-199610000-00033]
16 Delaunay L, Bonnet F, Liu N, Beydon L, Catoire P, Sessler DI. Clonidine comparably decreases the thermoregulatory thresholds for vasoconstriction and shivering in humans. Anesthesiology 1993; 79: 470-474 [PMID: 8363071 DOI: 10.1097/00000542-199309000-00009]
17 Freedman RR. Biochemical, metabolic, and vascular mecha-nisms in menopausal hot flashes. Fertil Steril 1998; 70: 332-337 [PMID: 9696230 DOI: 10.1016/S0015-0282(98)00137-X]
18 Casper RF, Yen SS. Neuroendocrinology of menopausal flushes: an hypothesis of flush mechanism. Clin Endocrinol (Oxf) 1985; 22: 293-312 [PMID: 3884189]
19 Bethea CL, Pecins-Thompson M, Schutzer WE, Gundlah C, Lu ZN. Ovarian steroids and serotonin neural function. Mol Neurobiol 1998; 18: 87-123 [PMID: 10065876 DOI: 10.1007/BF02914268]
20 Blum I, Vered Y, Lifshitz A, Harel D, Blum M, Nordenberg Y, Harsat A, Sulkes J, Gabbay U, Graff E. The effect of estro-
91 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ewies AAA. Folic acid supplementation and hot flushes

gen replacement therapy on plasma serotonin and catechol-amines of postmenopausal women. Isr J Med Sci 1996; 32: 1158-1162 [PMID: 9007144]
21 Lippert TH, Filshie M, Mück AO, Seeger H, Zwirner M. Serotonin metabolite excretion after postmenopausal estra-diol therapy. Maturitas 1996; 24: 37-41 [PMID: 8794432 DOI: 10.1016/0378-5122(95)00998-1]
22 Raible M, Kueck B, Alkan S. Red blood cell disorders. In: McClatchey K, editor. Clinical Laboratory Medicine. Phila-delphia: Lippincott Williams and Wilkins, 2002: 830-865
23 Miller AL. The methylation, neurotransmitter, and antioxi-dant connections between folate and depression. Altern Med Rev 2008; 13: 216-226 [PMID: 18950248]
24 Gover P. Biochemical aspects of anaemia. In: Marshall WJ, Bangert SK, editors. Clinical Biochemistry Metabolic and Clinical Aspects. Philadelphia: Churchill Livingstone Else-vier, 2008: 538-557
25 IPCS INCHEM. Folic Acid. 2010. Available from: URL: http://www.inchem.org/documents/pims/pharm/foli-caci.htm. Accessed on March 28, 2013
26 Informed Verlags AG. Folic Acid. 1996. Available from: URL: http://www.infomed.ch/100drugs/foltab.html. Ac-cessed on March 28, 2013
27 Drake VJ. Folic Acid: Linus Pauling Institute, Oregon State University. 2011. Available from: URL: http://lpi.oregonstate.edu/infocenter/vitamins/fa/. Accessed on March 28, 2013
28 Butterworth CE, Tamura T. Folic acid safety and toxicity: a brief review. Am J Clin Nutr 1989; 50: 353-358 [PMID: 2667316]
29 Hellström L. Lack of toxicity of folic acid given in pharma-cological doses to healthy volunteers. Lancet 1971; 1: 59-61 [PMID: 4099217 DOI: 10.1016/S0140-6736(71)90780-X]
30 Eichner ER, Pierce HI, Hillman RS. Folate balance in dietary-induced megaloblastic anemia. N Engl J Med 1971; 284: 933-938 [PMID: 5551802 DOI: 10.1056/NEJM197104292841702]
31 Actavis. Folic Acid. 2012. Available from: URL: http://xpil.medicines.org.uk/viewpil.aspx?docid=18084. Accessed on March 28, 2013
32 Wockhardt. Folic Acid. 2009. Available from: URL: http://xpil.medicines.org.uk/viewpil.aspx?docid=18738. Accessed on November 10, 2009
33 Vollset SE, Clarke R, Lewington S, Ebbing M, Halsey J, Lonn E, Armitage J, Manson JE, Hankey GJ, Spence JD, Galan P, Bønaa KH, Jamison R, Gaziano JM, Guarino P, Baron JA, Lo-gan RF, Giovannucci EL, den Heijer M, Ueland PM, Bennett D, Collins R, Peto R. Effects of folic acid supplementation on overall and site-specific cancer incidence during the ran-domised trials: meta-analyses of data on 50,000 individuals. Lancet 2013; 381: 1029-1036 [PMID: 23352552 DOI: 10.1016/S0140-6736(12)62001-7]
34 Bottiglieri T, Laundy M, Crellin R, Toone BK, Carney MW, Reynolds EH. Homocysteine, folate, methylation, and monoamine metabolism in depression. J Neurol Neurosurg Psychiatry 2000; 69: 228-232 [PMID: 10896698 DOI: 10.1136/jnnp.69.2.228]
35 Tolmunen T, Voutilainen S, Hintikka J, Rissanen T, Tans-kanen A, Viinamäki H, Kaplan GA, Salonen JT. Dietary fo-late and depressive symptoms are associated in middle-aged Finnish men. J Nutr 2003; 133: 3233-3236 [PMID: 14519816]
36 Abou-Saleh MT, Anderson DN, Collins J, Hughes K, Cattell RJ, Hamon CG, Blair JA. The role of pterins in depression and the effects of antidepressive therapy. Biol Psychiatry 1995; 38: 458-463 [PMID: 8672606 DOI: 10.1016/0006-3223(94)00323-U]
37 Hyndman ME, Verma S, Rosenfeld RJ, Anderson TJ, Parsons HG. Interaction of 5-methyltetrahydrofolate and tetrahy-drobiopterin on endothelial function. Am J Physiol Heart Circ Physiol 2002; 282: H2167-H2172 [PMID: 12003825]
38 Botez MI, Young SN, Bachevalier J, Gauthier S. Folate defi-ciency and decreased brain 5-hydroxytryptamine synthesis in man and rat. Nature 1979; 278: 182-183 [PMID: 763364
DOI: 10.1038/278182a0]39 Manzoor M, Runcie J. Folate-responsive neuropathy: report
of 10 cases. Br Med J 1976; 1: 1176-1178 [PMID: 1268613 DOI: 10.1136/bmj.1.6019.1176]
40 Lazarou C, Kapsou M. The role of folic acid in prevention and treatment of depression: an overview of existing evidence and implications for practice. Complement Ther Clin Pract 2010; 16: 161-166 [PMID: 20621278 DOI: 10.1016/j.ctcp.2010.01.003]
41 Reynolds EH. Benefits and risks of folic acid to the nervous system. J Neurol Neurosurg Psychiatry 2002; 72: 567-571 [PMID: 11971038 DOI: 10.1136/jnnp.72.5.567]
42 Astorg P, Couthouis A, de Courcy GP, Bertrais S, Arnault N, Meneton P, Galan P, Hercberg S. Association of folate intake with the occurrence of depressive episodes in middle-aged French men and women. Br J Nutr 2008; 100: 183-187 [PMID: 18062830 DOI: 10.1017/S0007114507873612]
43 Reynolds EH. Folic acid, ageing, depression, and dementia. BMJ 2002; 324: 1512-1515 [PMID: 12077044 DOI: 10.1136/bmj. 324.7352.1512]
44 Gilbody S, Lightfoot T, Sheldon T. Is low folate a risk factor for depression? A meta-analysis and exploration of heteroge-neity. J Epidemiol Community Health 2007; 61: 631-637 [PMID: 17568057 DOI: 10.1136/jech.2006.050385]
45 Alpert JE, Fava M. Nutrition and depression: the role of fo-late. Nutr Rev 1997; 55: 145-149 [PMID: 9212690 DOI: 10.1111/j.1753-4887.1997.tb06468.x]
46 Lerner V, Kanevsky M, Dwolatzky T, Rouach T, Kamin R, Miodownik C. Vitamin B12 and folate serum levels in newly admitted psychiatric patients. Clin Nutr 2006; 25: 60-67 [PMID: 16216392 DOI: 10.1016/j.clnu.2005.08.014]
47 Morris MS, Fava M, Jacques PF, Selhub J, Rosenberg IH. Depression and folate status in the US Population. Psy-chother Psychosom 2003; 72: 80-87 [PMID: 12601225 DOI: 10.1159/000068692]
48 Beydoun MA, Fanelli Kuczmarski MT, Beydoun HA, Shroff MR, Mason MA, Evans MK, Zonderman AB. The sex-specific role of plasma folate in mediating the association of dietary quality with depressive symptoms. J Nutr 2010; 140: 338-347 [PMID: 20032481 DOI: 10.3945/jn.109.113878]
49 Bottiglieri T. Homocysteine and folate metabolism in de-pression. Prog Neuropsychopharmacol Biol Psychiatry 2005; 29: 1103-1112 [DOI: 10.1016/j.pnpbp.2005.06.021]
50 D’Anci KE, Rosenberg IH. Folate and brain function in the elderly. Curr Opin Clin Nutr Metab Care 2004; 7: 659-664 [PMID: 15534434 DOI: 10.1097/00075197-200411000-00011]
51 Kamphuis MH, Geerlings MI, Grobbee DE, Kromhout D. Dietary intake of B(6-9-12) vitamins, serum homocysteine levels and their association with depressive symptoms: the Zutphen Elderly Study. Eur J Clin Nutr 2008; 62: 939-945 [PMID: 17538543 DOI: 10.1038/sj.ejcn.1602804]
52 Ubbink JB, Vermaak WJ, van der Merwe A, Becker PJ, Delport R, Potgieter HC. Vitamin requirements for the treat-ment of hyperhomocysteinemia in humans. J Nutr 1994; 124: 1927-1933 [PMID: 7931701]
53 Lindeman RD, Romero LJ, Koehler KM, Liang HC, LaRue A, Baumgartner RN, Garry PJ. Serum vitamin B12, C and folate concentrations in the New Mexico elder health survey: correlations with cognitive and affective functions. J Am Coll Nutr 2000; 19: 68-76 [PMID: 10682878]
54 Kim JM, Stewart R, Kim SW, Yang SJ, Shin IS, Yoon JS. Pre-dictive value of folate, vitamin B12 and homocysteine levels in late-life depression. Br J Psychiatry 2008; 192: 268-274 [PMID: 18378986 DOI: 10.1192/bjp.bp.107.039511]
55 Ng TP, Feng L, Niti M, Kua EH, Yap KB. Folate, vitamin B12, homocysteine, and depressive symptoms in a population sam-ple of older Chinese adults. J Am Geriatr Soc 2009; 57: 871-876 [PMID: 19484842 DOI: 10.1111/j.1532-5415.2009.02229.x]
56 Gaweesh SS, Abdel-Gawad MM, Nagaty AM, Ewies AA. Fo-lic acid supplementation may cure hot flushes in postmeno-pausal women: a prospective cohort study. Gynecol Endocrinol
92 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ewies AAA. Folic acid supplementation and hot flushes

93 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
2010; 26: 658-662 [PMID: 20230331 DOI: 10.3109/09513591003686288]
57 Grodnitskaya E, Kurtser MA. Effect of folic acid supplemen-tation on hot flushes in healthy menopausal women. Climac-teric 2011; 14: 1369-7137
58 Gaweesh S, Ewies AA. Folic acid supplementation cures hot flushes in postmenopausal women. Med Hypotheses 2010; 74: 286-288 [PMID: 19796883 DOI: 10.1016/j.mehy.2009.09.010]
59 Brocardo PS, Budni J, Kaster MP, Santos AR, Rodrigues AL. Folic acid administration produces an antidepressant-like effect in mice: evidence for the involvement of the serotonergic and noradrenergic systems. Neuropharmacology 2008; 54: 464-473 [PMID: 18078962 DOI: 10.1016/j.neuropharm.2007.10.016]
60 Lucock MD, Green M, Levene MI. Methylfolate modulates po-tassium evoked neuro-secretion: evidence for a role at the pter-idine cofactor level of tyrosine 3-hydroxylase. Neurochem Res 1995; 20: 727-736 [PMID: 7566370 DOI: 10.1007/BF01705542]
61 Bottiglieri T, Hyland K, Laundy M, Godfrey P, Carney MW, Toone BK, Reynolds EH. Folate deficiency, biopterin and monoamine metabolism in depression. Psychol Med 1992; 22: 871-876 [PMID: 1283223 DOI: 10.1017/S0033291700038447]
62 Botez MI, Young SN, Bachevalier J, Gauthier S. Effect of folic acid and vitamin B12 deficiencies on 5-hydroxyindoleace-tic acid in human cerebrospinal fluid. Ann Neurol 1982; 12: 479-484 [PMID: 6185039 DOI: 10.1002/ana.410120512]
63 Korevaar WC, Geyer MA, Knapp S, Hsu LL, Mandell AJ. Re-gional distribution of 5-methyltetrahydrofolic acid in brain.
Nat New Biol 1973; 245: 244-245 [PMID: 4518367]64 Słopien R, Jasniewicz K, Meczekalski B, Warenik-Szy-
mankiewicz A, Lianeri M, Jagodziński PP. Polymorphic vari-ants of genes encoding MTHFR, MTR, and MTHFD1 and the risk of depression in postmenopausal women in Poland. Maturitas 2008; 61: 252-255 [PMID: 18801628 DOI: 10.1016/j.maturitas.2008.08.002]
65 Cohen LS, Soares CN, Vitonis AF, Otto MW, Harlow BL. Risk for new onset of depression during the menopausal transition: the Harvard study of moods and cycles. Arch Gen Psychia-try 2006; 63: 385-390 [PMID: 16585467 DOI: 10.1001/arch-psyc.63.4.385]
66 Avis NE, Brambilla D, McKinlay SM, Vass K. A longitudinal analysis of the association between menopause and de-pression. Results from the Massachusetts Women’s Health Study. Ann Epidemiol 1994; 4: 214-220 [PMID: 8055122 DOI: 10.1016/1047-2797(94)90099-X]
67 Blümel JE, Castelo-Branco C, Cancelo MJ, Córdova AT, Binfa LE, Bonilla HG, Muñoz IG, Vergara VG, Sarrá SC. Re-lationship between psychological complaints and vasomotor symptoms during climacteric. Maturitas 2004; 49: 205-210 [PMID: 15488348 DOI: 10.1016/j.maturitas.2004.01.011]
68 Joffe H, Hall JE, Soares CN, Hennen J, Reilly CJ, Carlson K, Cohen LS. Vasomotor symptoms are associated with depres-sion in perimenopausal women seeking primary care. Meno-pause 2002; 9: 392-398 [PMID: 12439097 DOI: 10.1097/00042192-200211000-00003]
P- Reviewers: Freedman R, Ren AG, Xu XP S- Editor: Wen LL L- Editor: A E- Editor: Zheng XM
Ewies AAA. Folic acid supplementation and hot flushes

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.94
World J Obstet Gynecol 2013 November 10; 2(4): 94-100ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in epithelial ovarian cancer: State of the art
Ramez N Eskander, Luca Ansaloni, Robert E Bristow, Federico Coccolini
Ramez N Eskander, Robert E Bristow, Division of Gyneco-logic Oncology, Department of Obstetrics and Gynecology, Ir-vine Medical Center, University of California, Irvine, CA 92868, United StatesLuca Ansaloni, Federico Coccolini, Department of General and Emergency Surgery, Ospedali Riuniti, 24100 Bergamo, ItalyAuthor contributions: Eskander RN, Bristow RE, Ansaloni L and Coccolini F contributed equally to the article, with respect to literature review, writing and editing.Correspondence to: Ramez N Eskander, MD, Clinical Instruc-tor, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Irvine Medical Center, University of California, 101 the City Drive South Orange, Irvine, CA 92868, United States. [email protected]: +1-626-6443712 Fax: +1-714-4567754Received: December 13, 2012 Revised: June 26, 2013Accepted: August 4, 2013Published online: November 10, 2013
AbstractAdvanced stage epithelial ovarian cancer (EOC) is difficult to treat with low overall cure rates. A new strategy com-bining maximal cytoreductive surgery (CRS) with intra-operative hyperthermic intraperitoneal chemotherapy (HIPEC) has been proposed to treat advanced stage EOC in the primary setting. Numerous small, heterogeneous studies have been conducted exploring outcomes in pa-tients with predominantly advanced, recurrent or refrac-tory disease treated with CRS + HIPEC. Although morbid-ity rates approaching 35% have been reported, oncologic outcomes are promising. Incorporation of HIPEC for the treatment of primary EOC has continued to gain interest. Several prospective phase 2 clinical trials were recently completed evaluating the impact of CRS + HIPEC in the primary setting. This article will briefly discuss the ben-efits of optimal surgical cytoreduction and the theoretical basis of intraperitoneal chemotherapy in patients with ad-vanced stage EOC, and will then review existing literature
describing oncologic outcomes in EOC patients treated with HIPEC in the primary setting.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Epithelial ovarian cancer; Cytoreductive surgery; Hyperthermic intraperitoneal chemotherapy; Intraperitoneal chemotherapy; Survival; Toxicity
Core tip: Hyperthermic intraperitoneal chemotherapy (HIPEC), when used in combination with successful surgical cytoreduction appears to result in promising oncologic outcomes. We will eagerly await the results of the various phase 3 clinic trials, and until that time advocate the use of cytoreductive surgery + HIPEC in experienced centers under the auspices of appropriate institutional research programs.
Eskander RN, Ansaloni L, Bristow RE, Coccolini F. Cytoreduc-tive surgery and hyperthermic intraperitoneal chemotherapy in epithelial ovarian cancer: State of the art. World J Obstet Gynecol 2013; 2(4): 94-100 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/94.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.94
INTRODUCTIONEpithelial ovarian cancer (EOC) accounts for 25% of all malignancies affecting the female genital tract, and is the most lethal gynecologic malignancy[1]. In 2012 there will be an estimated 22280 new ovarian cancer cases in the United States, with 15500 deaths[1]. Advanced stage EOC is traditionally managed with surgery, followed by plati-num and taxane based combination chemotherapy[2,3].
Several factors have been identified as prognostic
94 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Eskander RN et al . HIPEC and EOC
for clinical outcome in patients with EOC, with extent of residual disease being investigated in numerous stud-ies[4]. Specifically, a differential survival impact between patients with no gross residual disease vs optimal but vis-ible residual disease (0.1-1.0 cm in maximal diameter) has been illustrated in patients with optimally resected stage 3 EOC[4]. These findings have been validated by other authors[5,6]. Currently, the Gynecologic Oncology Group (GOG) defines optimal residual disease as ≤ 1 cm. The reason cytoreductive surgery (CRS) is thought to be ef-fective when combined with chemotherapy is that it re-moves bulky disease containing poorly oxygenated, non-proliferating cells which are either resistant or potentially resistant to chemotherapy, leaving small volume tumors, with a higher proportion of cells in the proliferative phase, that are more susceptible to chemotherapy[7].
In addition to aggressive CRS, our understanding of the distribution pattern of ovarian cancer catalyzed numerous clinical studies exploring the feasibility of intraperitoneal administration of chemotherapy. Ovarian cancer typically spreads in a diffuse intra-abdominal fashion, often lim-ited to the peritoneal cavity, less frequently metastasizing via hematogenous or lymphatic routes. Despite advanced surgical techniques, microscopic tumor implants com-monly remain along the peritoneal surface. Animal mod-els suggested the ability of intraperitoneal administration of cytotoxic agents to lead to cancer cell death in lesions measuring 2-3 mm in largest diameter[8]. Therefore, suc-cessful CRS is a main pre-requisite for intraperitoneal administration of chemotherapy[9]. Furthermore, due to the presence of a peritoneal-plasma barrier, chemothera-peutic agents remain concentrated (20-1000 fold) in the peritoneal cavity for a prolonged period of time resulting in enhanced cancer cell death, with theoretically less sys-temic toxicity[7,10,11].
Three pivotal clinical trials were completed evaluating the impact of intraperitoneal (IP) chemotherapy on sur-vival in patients with advanced stage ovarian cancer[12-14]. Initially, 2 randomized phase 3 intergroup trials compar-ing intravenous (IV) to IV + IP chemotherapy showed positive results. The GOG subsequently developed and opened protocol 172, which compared IV paclitaxel (135 mg/m2) over 24 h with IV cisplatin (75 mg/m2) on day 2, vs IV paclitaxel (135 mg/m2) over 24 h, followed by IP cisplatin (100 mg/m2) on day 2 and IP paclitaxel (60 mg/m2) on day 8. A total of 6 courses were admin-istered every 3 wk[14]. All patients had optimally resected disease with residual tumor limited to less than or equal to 1 cm in size. The median survival for the IV only and IV + IP arms were 49.5 and 66.9 mo respectively. The RR of death was 0.71 in the IP group (P = 0.0076). The authors noted that tolerability for IP chemo was a con-cern as grade 3 and 4 hematologic, metabolic, and gas-trointestinal toxicities were significantly more common in the IP arm. Remarkably, only 86 patients (42%) of 205 allocated to the IP arm completed 6 cycles of chemo-therapy, and 98 (48%) received 3 cycles or fewer of the assigned treatment.
The results of GOG 172, in combination with previ-ous positive studies exploring intraperitoneal chemother-apy, resulted in a National Cancer Institute (NCI) clinical announcement recommending that women with opti-mally cytoreduced stage 3 ovarian cancer be considered for IV + IP therapy[15]. Unfortunately, adoption of the IP regimen described in protocol 172 has been limited, due to the high rate of grade 3/4 toxicities, inconvenience of in-patient administration, and poor patient tolerance.
Attempts at modification of the original regimen have been made in an effort to improve compliance and decrease toxicity. Barlin et al[16] investigated the oncologic outcomes associated with an outpatient IP regimen in 102 patients with optimally cytoreduced EOC. The modified regimen consisted of IV paclitaxel (135 mg/m2) over 3 h on day 1, IP cisplatin (75 mg/m2) on day 2, and IP pacli-taxel (60 mg/m2) on day 8, given every 21 d for 6 cycles. The median PFS and OS were 29 and 67 mo, respectively. Importantly, 80% of subjects completed 4 or more cycles of IV + IP therapy. The most frequently reported grade 3/4 toxicities included neutropenia (12%), gastrointestinal (8%) and neurologic (6%)[16]. GOG protocol 252, which completed accrual in November 2011, will help elucidate the role of intraperitoneal chemotherapy in patients with optimally resected EOC, as well as the potential role of both dose dense paclitaxel and the anti-angiogenic agent bevacizumab.
HYPERTHERMIC INTRAPERITONEAL CHEMOTHERAPY In an effort to obviate the toxicities encountered with re-petitive cycles of intraperitoneal chemotherapy, investiga-tors have explored the use of a single course of intraoper-ative hyperthermic intraperitoneal chemotherapy (HIPEC) followed by conventional intravenous chemotherapy. The concept of HIPEC is based on several important principles: (1) the direct and preferential cytotoxic effect of hyperthermia on tumor cells; (2) synergistic effects of hyperthermia when used with conventional cytotoxic agents without an associated increase in toxicity; and (3) increased drug penetration, from 3 to 5 mm, secondary to hyperthermia[17-24].
In addition, the presence of extensive adhesions in the post-operative period are hypothesized to result in both impaired drug distribution and significant toxic-ity/pain when traditional IP chemotherapy is given in the adjuvant setting. Utilization of intra-operative HIPEC, at the time of initial CRS, guarantees uniform distribution and systemic peritoneal coverage, potentially enhancing the anti-tumor efficacy of the drugs used.
Based on the theoretical principles described above, HIPEC was first examined in patients with peritoneal carcinomatosis due to gastrointestinal malignancies, pseu-domyxoma peritonei and peritoneal mesothelioma[25-28]. In the surgical setting, these trails illustrated the safety and feasibility of hyperthermic intraperitoneal drug adminis-tration.
95 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

HIPEC AND OVARIAN CANCERObservational and retrospective studiesIn 1990, Cohen and Robins proposed HIPEC for the treatment of recurrent ovarian cancer[29,30]. Steller et al[31] studied the feasibility, toxicity and pharmacokinetics of intraperitoneal hyperthermic carboplatin administration in 6 patients at the time of primary surgical cytoreduc-tion. Shortly thereafter, Hager et al[32] conducted a pro-spective clinical trial on 36 patients with recurrent ovarian cancer treated with CRS and HIPEC. The median OS from the first HIPEC chemotherapy treatment was 19 ± 4 mo. The 5-year OS of all patients from the start of the first HIPEC treatment was 16% ± 7%. The authors described the adverse effects as mild when compared to systemic chemotherapy.
This was followed by a study conducted by Piso et al[33] of 19 patients with peritoneal carcinomatosis due to pri-mary or recurrent EOC. Surgery was followed by intra-operative HIPEC using single agent cisplatin (n = 16) or mitoxantrone (n = 3). The median progression free interval was 18 mo (range 6-36 mo), with mean overall survival time of 33 mo and a 5-year survival rate of 15%. The most common complications encountered were anastomotic leak (2 of 19) and intra-abdominal abscess formation (2 of 19)[33]. Additional studies evaluating the clinical effect of HIPEC in patients with advanced stage ovarian cancer were completed in an effort to determine the most appropriate/effective chemotherapeutic agent and the ideal hyperthermic temperature (Table 1)[8,34-39].
Ryu et al[34] retrospectively reviewed 117 patients with ovarian cancer, 57 who underwent CRS (conventional treatment) with HIPEC and 60 who underwent conven-
tional treatment only. The investigators studied a HIPEC mixture consisting of carboplatin (350 mg/m2) and interferon-α (5000000 IU/m2). Intraperitoneal tempera-ture was maintained at 43-44 ℃ during surgery. The overall 5-year survival rate was significantly greater in the HIPEC group vs control (63.4% vs 52.8%, respectively, P = 0.0078). This survival advantage was more pronounced amongst the subset of patients with stage 3 disease (53.8% in the HIPEC group vs 33.3% in the control group, P = 0.0015). In multivariate analysis, HIPEC was identified as an inde-pendent prognostic factor.
HIPEC was also studied in the recurrent setting. Zanon et al[40] examined the use of combined CRS and HIPEC in 30 women with recurrent EOC. Enrolled subjects un-derwent extensive CRS followed by intraoperative HIPEC with cisplatin (100-150 mg/m2). In patient’s cytoreduced to ≤ 2.5 mm of residual disease, progression free sur-vival was 17.1 mo, with an overall survival of 37.8 mo. Major post-operative morbidity occurred in 16.7% of subjects, with gastrointestinal toxicities (anastomotic leak and perforations) being the most commonly reported. One treatment related mortality, a fatal pulmonary em-bolism, occurred 30 d following discharge. Cotte et al[41] prospectively studied combination CRS + HIPEC in 81 patients with recurrent or chemotherapy resistant perito-neal carcinomatosis from ovarian cancer. Mortality and morbidity rates were 2.5% and 13.6%, respectively. With a median follow-up of 47.1 mo, the overall and disease-free median survivals were 28.4 and 19.2 mo, respectively.
HIPEC in combination with secondary cytoreduc-tion was further investigated as consolidation therapy in patients with advanced stage EOC following surgery and systemic intravenous chemotherapy[29,42-44]. Within this
96 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Cytoreductive surgery + hyperthermic intraperitoneal chemotherapy in the treatment of advanced stage primary epithelial ovarian cancer: retrospective and observational studies: Study characteristics
Ref. n Disease stage Setting of treatment
HIPEC drug and dose Temp. (℃)
Duration of treatment
(min)
Oncologic outcome Common grade 2-3 toxicities
Mortality rate
Tentes et al[8]
43 “Locally advanced”
ovarian cancer
23 primary Doxorubicin 15 mg/m2 + Cisplatin 50 mg/m2 or
Gemcitabine 1000 mg/m2
42.5-43 60 or 90 5-yr OS: 54% Hematologic; GI; infectious
2 deaths (sepsis)20 recurrent In primary population
5-yr OS 82.5%Steller et al[31]
6 2-3 EOC 2 primary Carboplatin 800-1200 mg/m2
42 90 All alive at 15 mo follow up; 5 without evidence of disease
Hematologic No deaths4 recurrent
Piso et al[33]
19 3-4 EOC 8 primary Cisplatin 75 mg/m2 + Mitoxantrone 15 mg/m2
41.5 90 Median PFS 18 mo; mean OS 33 mo; 5 yr
survival 15%
Hematologic; GI (anastomotic leak,
fistula); bleeding; abscess
1 death (sepsis)11 recurrent
Rufián et al[35]
33 3 EOC 19 primary Paclitaxel 60 mg/m2 41-43 60 In primary population median relapse free survival was 25 mo; median OS 38 mo
Hematologic; infectious; GI (bleeding and
perforation)
No deaths14 recurrent
Lentz et al[37]
25 3 EOC 11 primary Carboplatin 400-1200 mg/m2
Inflow < 43.5
90 Not reported One PE; one superficial wound dehiscence
No deaths14 recurrent
Pavlov et al[39]
56 3-4 EOC 31 primary Doxorubicin 0.1 mg/kg + Cisplatin 15 mg/m2
40 180 Median OS 38.1 mo; 5-yr OS 67%
Hematologic; GI (anastomotic leak,
obstruction)
1 death (CVA)25 recurrent
HIPEC: Hyperthermic intraperitonealchemotherapy; Temp.: Temperature; OS: Overall survival; GI: Gastrointestinal; EOC: Epithelial ovarian cancer; PFS: Progression free survival; PE: Pulmonary embolism; CVA: Cerebral-vascular accident.
Eskander RN et al . HIPEC and EOC

cohort of patients, HIPEC (cisplatin 100 mg/m2), when given at the time of “second-look” laparotomy, resulted in an improvement in the 5-year survival rate, although the difference did not reach statistical significance (57.9% in HIPEC group vs 44.8% in the control group). This was at-tributed to the small sample size studied (29 subjects). No-tably, no HIPEC associated grade 3 or 4 toxicities were re-ported. An analogous study conducted by Yoshida et al[42] demonstrated marked median progression-free and over-all survival rates in subjects treated with HIPC who had a negative second look laparotomy (82.8 and 130.3 mo, respectively).
Investigators from The NCI of Milan studied out-comes associated with CRS and HIPEC in patients with advanced, recurrent ovarian cancer previously treated with systemic cisplatin-based, taxol-based or taxol/platinum containing regimens[45]. Within the cohort of 40 patients, 5-year OS was 15%, with mean OS and PFS of 41.4 and 23.9 mo, respectively. The morbidity, toxicity and mortal-ity rates were 5%, 15% and 0%, respectively. Dr. Helm et al[46] retrospectively evaluated the use of secondary CRS + HIPEC in patients with disease resected to ≤ 5 mm. The regimens used in the study consisted of cisplatin (100 mg/m2 in 15 patients) or mitomycin C (30-40 mg total dose in 3 patients) heated to 41-43 ℃ (105.8-109.4 degrees F) for 90 min. All patients developed grade 1 or 2 metabolic or hematologic toxicities. Grade 3 or 4 metabolic toxicity occurred in 72% and hematologic toxicity in 28%. There was one perioperative death due to pulmonary embolus. The median progression-free interval was 10 mo and me-dian overall survival was 31 mo.
Prospective phase 2 clinical trialsThe trials described above were limited by their retro-spective nature, small sample size, heterogenious patient population and variation in both dose and drug used.
These limitations prompted the creation and completion of larger prospective phase 2 clinical trials specifically exploring CRS + HIPEC in the up-front treatment of patients with advanced EOC (Table 2).
The first phase 2 clinical trial exploring the use of HIPEC in patients with primary advanced ovarian cancer was completed in 2007[47]. Forty-seven patients were en-rolled in this open, prospective, single-center nonrandom-ized study; 22 underwent primary and 25 secondary CRS plus immediate HIPEC (cisplatin 75 mg/m2) followed by systemic chemotherapy. Eighty-seven percent of the patients achieved optimal cytoreduction, whereas mac-roscopic residual disease (defined as lesions ≥ 2.5 mm) was left behind in 12.7% of subjects. Major complications (gastrointestinal fistula, intra-abdominal bleeding and thrombosis) developed in 21.3% of the patients and the in-hospital mortality rate was 4.2% (2 patients with pulmo-nary embolism). The mean overall survival was 30.4 mo, median survival was 24 mo, and mean disease-free survival was 27.4 mo. Five-year survival was 16.7%.
This was followed by a study investigating the mor-bidity and feasibility of CRS + HIPEC in patients with advanced stage primary EOC. Lim et al[48] treated 30 pa-tients with residual tumor measuring < 1 cm at the time of primary surgery, with intraoperative HIPEC (cisplatin 75 mg/m2) at a temperature of 41.5 ℃ for 90 min. All the patients subsequently received adjuvant chemother-apy with combination IV platinum and taxane. Within the cohort, 28 patients (93%) experienced complete remission, and only two patients (7%) had progressive disease. The most commonly reported toxicities included nausea/vomiting, anemia, diarrhea, pleural effusions and wound infections. No deaths or morbidities requiring re-operation or intensive care unit admission were reported. The overall survival data was not yet mature given the interim nature of the evluation.
97 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 2 Cytoreductive surgery + hyperthermic intraperitoneal chemotherapy in the treatment of advanced stage primary epithelial ovarian cancer: prospective phase 2 trials
Ref. n Disease stage
Setting of treatment
HIPEC drug used and dose
Temp. (℃)
Duration of treatment
(min)
OS (mo) PFS (mo) Common grade 2-3 toxicities
Mortality rate
Di Giorgio et al[47]
47 3C-4 EOC 22 primary Cisplatin 75 mg/m2
42-43 60 30.4 (mean) 27.4 (mean) Pleural effusions (8.5%) 4% (PE)25 recurrent Infectious (8.5%)
GI (10.6%)Bleeding (6.4%)
Lim et al[48] 30 3-4 EOC 30 primary (14 of which underwent
neoadjuvant treatment)
Cisplatin 75 mg/m2
41.5 90 NR NR Hematologic (86.7%) No deathsGI (30%)
Infectious (16.7%) Pulmonary (23.3%)
CV (13.3%)Ansaloni et al[49]
26 3-4 EOC 26 primary Cisplatin 40 mg/L
perfusate + doxorubicin
15 mg/L perfusate
42.5 90 Not reached 30 (median) Hematologic (4%) 4% (sepsis)5-yr OS 60.7% 5-yr PFS 15.2% GI (4%)
Pulmonary (14.3%)Infectious (14.3%)
Ninety-three percent with complete response to primary treatment. Seven patients with progressive disease. HIPEC: Hyperthermic intraperitonealchemotherapy; Temp.: Temperature; OS: Overall survival; PFS: Progression free survival; EOC: Epithelialovarian cancer; GI: Gastrointestinal; PE: Pulmonary embolism; NR: Not reported; CV: Cardiovascular.
Eskander RN et al . HIPEC and EOC

Ansaloni et al[49] in their open, prospective phase 2 study, included thirty-nine patients. Thirty patients (77%) had recurrent EOC and 9 (23%) had primary EOC. For HIPEC, cisplatin and paclitaxel were used for 11 patients (28%), cisplatin and doxorubicin for 26 patients (66%), paclitaxel and doxorubicin for 1 patient (3%), and doxo-rubicin alone for 1 patient (3%). All HIPEC were per-formed with open technique. The median intra-abdominal outflow temperature was 41.5 ℃. The mean peritoneal cancer index (PCI) was 11.1; according to the intraopera-tive tumor extent, the tumor volume was classified as low (PCI < 15) or high (PCI ≥ 15) in 27 patients (69%) and 12 patients (31%), respectively. Microscopically complete cytoreduction was achieved for 35 patients (90%), mac-roscopic cytoreduction was achieved for 3 patients (7%), and a gross tumor debulking was performed for 1 patient (3%). Mean hospital stay was 23.8 d. Grade Ⅰ-Ⅲ post-operative complications occurred in 7 patients (18%), and reoperations in 3 patients (8%). There was one postopera-tive death. Recurrence was seen in 23 patients (59%) with a mean recurrence time of 14.4 mo (60).
More recently, a multi-institutional phase 2 study was completed evaluating the impact of CRS + HIPEC on PFS and OS in 26 women with stage 3-4 EOC[50]. All enrolled subjects underwent CRS, followed by HIPEC using the closed-abdomen technique with cisplatin (40 mg/L perfusate) and doxorubicin (15 mg/L of per-fusate). Patients were then treated with 6 cycles of adju-vant IV carboplatin (AUC 6) and paclitaxel (175 mg/m2) administered every 3 wk. Macroscopically complete cyto-reduction was achieved in 15 patients (57%), with minimal residual disease (≤ 2.5 mm) remaining in the other 11 (43%). After a median follow-up of 25 mo, 5-year overall survival was 60.7% and 5-year progression-free survival 15.2% (median 30 mo). Excluding operative death, all the patients underwent a median of 6 cycles of systemic che-motherapy at a median of 46 d from combined treatment (range: 29-75 d)[50]. Four patients experienced ≥ grade 3 morbidity, with one post-operative death due to sepsis.
In conclusion, the incorporation of HIPEC in the treatment of primary advanced stage ovarian cancer has shown promising results in both observational studies as well as phase 2 clinical trials. The only randomized phase 3 clinical trial exploring the impact of HIPEC on survival was conducted in patients with carcinomatosis associated with colorectal cancer, showing a significant improve-ment in survival amongst patients allocated to the HIPEC arm[28]. Unfortunately, patients randomized to the non-HIPEC arm of the trial did not undergo aggressive CRS, potentially impacting survival and limiting the clinical im-plications of the study[28].
To date, no randomized phase 3 clinical trials have been completed evaluating the impact of HIPEC on survival in patients with advanced stage ovarian, fallopian tube or primary peritoneal carcinoma. Furthermore, the use of non-randomized contemporary or historical con-trol populations restricts the generalizability of results re-ported in the trials discussed above[51]. In order to address
this important clinical question, 4 randomized phase 3 clinical trials are currently in various stages of design and implementation[49].
As with any new therapeutic paradigm, the benefits of HIPEC in the treatment of patients with ovarian cancer must be weighed against the side effects. Over-all, HIPEC appears to be well tolerated in appropriately selected patient populations. Nonetheless, toxicity and mortality rates as high as 35% and 5%, respectively, have been reported[52]. Given the relative novelty of this ap-proach, improvements in patient outcome and mitigation of toxicities experienced have been described by more experienced centers[53-58]. Furthermore, quality of life studies have indicated improved emotional well being and rapid return to pre-operative levels of functioning follow-ing HIPEC treatment[59].
In summary, HIPEC, when used in combination with successful surgical cytoreduction appears to result in promising oncologic outcomes. We will eagerly await the results of the various phase 3 clinic trials, and until that time advocate the use of CRS + HIPEC in experienced centers under the auspices of appropriate institutional research programs.
REFERENCES1 Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012.
CA Cancer J Clin 2012; 62: 10-29 [PMID: 22237781 DOI: 10.3322/caac.20138]
2 Bookman MA. Trials with impact on clinical management: first line. Int J Gynecol Cancer 2009; 19 Suppl 2: S55-S62 [PMID: 19955916]
3 Cannistra SA. Cancer of the ovary. N Engl J Med 1993; 329: 1550-1559 [PMID: 8155119 DOI: 10.1056/NEJM19931118329 2108]
4 Winter WE, Maxwell GL, Tian C, Carlson JW, Ozols RF, Rose PG, Markman M, Armstrong DK, Muggia F, McGuire WP. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol 2007; 25: 3621-3627 [PMID: 17704411]
5 Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, Sonoda Y, Levine DA, Hensley M, Barakat RR. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol 2006; 103: 559-564 [PMID: 16714056 DOI: 10.1016/j.ygyno.2006.03.051]
6 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for ad-vanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167]
7 Helm CW, Bristow RE, Kusamura S, Baratti D, Deraco M. Hyperthermic intraperitoneal chemotherapy with and with-out cytoreductive surgery for epithelial ovarian cancer. J Surg Oncol 2008; 98: 283-290 [PMID: 18726895 DOI: 10.1002/jso.21083]
8 Tentes AA, Kakolyris S, Kyziridis D, Karamveri C. Cytore-ductive surgery combined with hyperthermic intraperitoneal intraoperative chemotherapy in the treatment of advanced epithelial ovarian cancer. J Oncol 2012; 2012: 358341 [PMID: 22481924]
9 Rossi CR, Foletto M, Mocellin S, Pilati P, De SM, Deraco M, Cavaliere F, Palatini P, Guasti F, Scalerta R, Lise M. Hy-perthermic intraoperative intraperitoneal chemotherapy with cisplatin and doxorubicin in patients who undergo cytoreductive surgery for peritoneal carcinomatosis and
98 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Eskander RN et al . HIPEC and EOC

sarcomatosis: phase I study. Cancer 2002; 94: 492-499 [PMID: 11900234 DOI: 10.1002/cncr.10176]
10 Markman M, Rowinsky E, Hakes T, Reichman B, Jones W, Lewis JL, Rubin S, Curtin J, Barakat R, Almadrones L. Intra-peritoneal administration of Taxol in the management of ovar-ian cancer. J Natl Cancer Inst Monogr 1993; 15: 103-106 [PMID: 7912515]
11 Markman M, Rowinsky E, Hakes T, Reichman B, Jones W, Lewis JL, Rubin S, Curtin J, Barakat R, Phillips M. Phase I trial of intraperitoneal taxol: a Gynecoloic Oncology Group study. J Clin Oncol 1992; 10: 1485-1491 [PMID: 1355523]
12 Markman M, Bundy BN, Alberts DS, Fowler JM, Clark-Pearson DL, Carson LF, Wadler S, Sickel J. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small-volume stage III ovarian carcinoma: an intergroup study of the Gyneco-logic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol 2001; 19: 1001-1007 [PMID: 11181662]
13 Alberts DS, Liu PY, Hannigan EV, O’Toole R, Williams SD, Young JA, Franklin EW, Clarke-Pearson DL, Malviya VK, DuBeshter B. Intraperitoneal cisplatin plus intravenous cy-clophosphamide versus intravenous cisplatin plus intrave-nous cyclophosphamide for stage III ovarian cancer. N Engl J Med 1996; 335: 1950-1955 [PMID: 8960474 DOI: 10.1056/NEJM199612263352603]
14 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
15 Trimble EL, Alvarez RD. Intraperitoneal chemotherapy and the NCI clinical announcement. Gynecol Oncol 2006; 103: S18-S19 [PMID: 17027073 DOI: 10.1016/j.ygyno.2006.08.020]
16 Barlin JN, Dao F, Bou Zgheib N, Ferguson SE, Sabbatini PJ, Hensley ML, Bell-McGuinn KM, Konner J, Tew WP, Agha-janian C, Chi DS. Progression-free and overall survival of a modified outpatient regimen of primary intravenous/intra-peritoneal paclitaxel and intraperitoneal cisplatin in ovar-ian, fallopian tube, and primary peritoneal cancer. Gynecol Oncol 2012; 125: 621-624 [PMID: 22446622 DOI: 10.1016/j.ygyno.2012.03.027]
17 Nicoletto MO, Padrini R, Galeotti F, Ferrazzi E, Cartei G, Riddi F, Palumbo M, De Paoli M, Corsini A. Pharmacokinet-ics of intraperitoneal hyperthermic perfusion with mitoxan-trone in ovarian cancer. Cancer Chemother Pharmacol 2000; 45: 457-462 [PMID: 10854132 DOI: 10.1007/s002800051019]
18 Ohno S, Siddik ZH, Kido Y, Zwelling LA, Bull JM. Thermal enhancement of drug uptake and DNA adducts as a possible mechanism for the effect of sequencing hyperthermia on cis-platin-induced cytotoxicity in L1210 cells. Cancer Chemother Pharmacol 1994; 34: 302-306 [PMID: 8033297 DOI: 10.1007/BF00686037]
19 Vernon C. Hyperthermia in cancer growth regulation. Biotherapy 1992; 4: 307-315 [PMID: 1622744 DOI: 10.1007/BF02172661]
20 Robins HI. Role of whole-body hyperthermia in the treat-ment of neoplastic disease: its current status and future pros-pects. Cancer Res 1984; 44: 4878s-4883s [PMID: 6467241]
21 Shiu MH, Fortner JG. Intraperitoneal hyperthermic treat-ment of implanted peritoneal cancer in rats. Cancer Res 1980; 40: 4081-4084 [PMID: 7471053]
22 Larkin JM. A clinical investigation of total-body hyperther-mia as cancer therapy. Cancer Res 1979; 39: 2252-2254 [PMID: 87262]
23 Kowal CD, Bertino JR. Possible benefits of hyperthermia to chemotherapy. Cancer Res 1979; 39: 2285-2289 [PMID: 376118]
24 Johnson RJ, Subjeck JR, Moreau DZ, Kowal H, Yakar D. Radiation and hyperthermia. Bull N Y Acad Med 1979; 55: 1193-1204 [PMID: 295251]
25 Fujimoto S, Takahashi M, Mutou T, Kobayashi K, Toyosawa T. Successful intraperitoneal hyperthermic chemoperfusion for the prevention of postoperative peritoneal recurrence in patients with advanced gastric carcinoma. Cancer 1999; 85: 529-534 [PMID: 10091726]
26 Fujimoto S, Takahashi M, Mutou T, Kobayashi K, Toyosawa T, Isawa E, Sumida M, Ohkubo H. Improved mortality rate of gastric carcinoma patients with peritoneal carcinomatosis treated with intraperitoneal hyperthermic chemoperfusion combined with surgery. Cancer 1997; 79: 884-891 [PMID: 9041149]
27 Spratt JS, Adcock RA, Muskovin M, Sherrill W, McKeown J. Clinical delivery system for intraperitoneal hyperthermic chemotherapy. Cancer Res 1980; 40: 256-260 [PMID: 6766084]
28 Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van Tinteren H, Boot H, Zoetmulder FA. Randomized trial of cy-toreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21: 3737-3743 [PMID: 14551293]
29 Gori J, Castaño R, Toziano M, Häbich D, Staringer J, De Quirós DG, Felci N. Intraperitoneal hyperthermic chemother-apy in ovarian cancer. Int J Gynecol Cancer 2005; 15: 233-239 [PMID: 15823105]
30 Cohen JD, Robins HI. Whole body hyperthermia and intra-peritoneal carboplatin in residual ovarian cancer. Adv Exp Med Biol 1990; 267: 197-202 [PMID: 2088035 DOI: 10.1007/978-1-4684-5766-7_18]
31 Steller MA, Egorin MJ, Trimble EL, Bartlett DL, Zuhowski EG, Alexander HR, Dedrick RL. A pilot phase I trial of contin-uous hyperthermic peritoneal perfusion with high-dose car-boplatin as primary treatment of patients with small-volume residual ovarian cancer. Cancer Chemother Pharmacol 1999; 43: 106-114 [PMID: 9923815 DOI: 10.1007/s002800050870]
32 Hager ED, Dziambor H, Höhmann D, Mühe N, Strama H. Intraperitoneal hyperthermic perfusion chemotherapy of pa-tients with chemotherapy-resistant peritoneal disseminated ovarian cancer. Int J Gynecol Cancer 2001; 11 Suppl 1: 57-63 [PMID: 11489005]
33 Piso P, Dahlke MH, Loss M, Schlitt HJ. Cytoreductive sur-gery and hyperthermic intraperitoneal chemotherapy in peri-toneal carcinomatosis from ovarian cancer. World J Surg On-col 2004; 2: 21 [PMID: 15222884 DOI: 10.1186/1477-7819-2-21]
34 Ryu KS, Kim JH, Ko HS, Kim JW, Ahn WS, Park YG, Kim SJ, Lee JM. Effects of intraperitoneal hyperthermic chemothera-py in ovarian cancer. Gynecol Oncol 2004; 94: 325-332 [PMID: 15297169 DOI: 10.1016/j.ygyno.2004.05.044]
35 Rufián S, Muñoz-Casares FC, Briceño J, Díaz CJ, Rubio MJ, Ortega R, Ciria R, Morillo M, Aranda E, Muntané J, Pera C. Radical surgery-peritonectomy and intraoperative intraperi-toneal chemotherapy for the treatment of peritoneal carcino-matosis in recurrent or primary ovarian cancer. J Surg Oncol 2006; 94: 316-324 [PMID: 16917864 DOI: 10.1002/jso.20597]
36 Bae JH, Lee JM, Ryu KS, Lee YS, Park YG, Hur SY, Ahn WS, Namkoong SE. Treatment of ovarian cancer with paclitaxel- or carboplatin-based intraperitoneal hyperthermic chemo-therapy during secondary surgery. Gynecol Oncol 2007; 106: 193-200 [PMID: 17466362 DOI: 10.1016/j.ygyno.2007.03.019]
37 Lentz SS, Miller BE, Kucera GL, Levine EA. Intraperitoneal hyperthermic chemotherapy using carboplatin: a phase I analysis in ovarian carcinoma. Gynecol Oncol 2007; 106: 207-210 [PMID: 17498782 DOI: 10.1016/j.ygyno.2007.03.022]
38 Kusamura S, Dominique E, Baratti D, Younan R, Deraco M. Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy. J Surg Oncol 2008; 98: 247-252 [PMID: 18726886 DOI: 10.1002/jso.21051]
39 Pavlov MJ, Kovacevic PA, Ceranic MS, Stamenkovic AB, Ivanovic AM, Kecmanovic DM. Cytoreductive surgery and modified heated intraoperative intraperitoneal chemo-therapy (HIPEC) for advanced and recurrent ovarian cancer
99 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Eskander RN et al . HIPEC and EOC

100 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
-- 12-year single center experience. Eur J Surg Oncol 2009; 35: 1186-1191 [PMID: 19356887 DOI: 10.1016/j.ejso.2009.03.004]
40 Zanon C, Clara R, Chiappino I, Bortolini M, Cornaglia S, Simone P, Bruno F, De Riu L, Airoldi M, Pedani F. Cytore-ductive surgery and intraperitoneal chemohyperthermia for recurrent peritoneal carcinomatosis from ovarian can-cer. World J Surg 2004; 28: 1040-1045 [PMID: 15573262 DOI: 10.1007/s00268-004-7461-x]
41 Cotte E, Glehen O, Mohamed F, Lamy F, Falandry C, Gol-fier F, Gilly FN. Cytoreductive surgery and intraperitoneal chemo-hyperthermia for chemo-resistant and recurrent advanced epithelial ovarian cancer: prospective study of 81 patients. World J Surg 2007; 31: 1813-1820 [PMID: 17629740 DOI: 10.1007/s00268-007-9146-8]
42 Yoshida Y, Sasaki H, Kurokawa T, Kawahara K, Shukunami K, Katayama K, Yamaguchi A, Kotsuji F. Efficacy of intraperi-toneal continuous hyperthermic chemotherapy as consolida-tion therapy in patients with advanced epithelial ovarian can-cer: a long-term follow-up. Oncol Rep 2005; 13: 121-125 [PMID: 15583812]
43 Kim JH, Lee JM, Ryu KS, Lee YS, Park YG, Hur SY, Lee KH, Lee SH, Kim SJ. Consolidation hyperthermic intraperitoneal chemotherapy using paclitaxel in patients with epithelial ovar-ian cancer. J Surg Oncol 2010; 101: 149-155 [PMID: 20035540]
44 Frenel JS, Leux C, Pouplin L, Ferron G, Berton Rigaud D, Bourbouloux E, Dravet F, Jaffre I, Classe JM. Oxaliplatin-based hyperthermic intraperitoneal chemotherapy in prima-ry or recurrent epithelial ovarian cancer: A pilot study of 31 patients. J Surg Oncol 2011; 103: 10-16 [PMID: 21031424 DOI: 10.1002/jso.21732]
45 Raspagliesi F, Kusamura S, Campos Torres JC, de Souza GA, Ditto A, Zanaboni F, Younan R, Baratti D, Mariani L, Laterza B, Deraco M. Cytoreduction combined with intra-peritoneal hyperthermic perfusion chemotherapy in ad-vanced/recurrent ovarian cancer patients: The experience of National Cancer Institute of Milan. Eur J Surg Oncol 2006; 32: 671-675 [PMID: 16621425 DOI: 10.1016/j.ejso.2006.03.011]
46 Helm CW, Randall-Whitis L, Martin RS, Metzinger DS, Gordinier ME, Parker LP, Edwards RP. Hyperthermic intra-peritoneal chemotherapy in conjunction with surgery for the treatment of recurrent ovarian carcinoma. Gynecol Oncol 2007; 105: 90-96 [PMID: 17173957 DOI: 10.1016/j.ygyno.2006.10.051]
47 Di Giorgio A, Naticchioni E, Biacchi D, Sibio S, Accarpio F, Rocco M, Tarquini S, Di Seri M, Ciardi A, Montruccoli D, Sammartino P. Cytoreductive surgery (peritonectomy proce-dures) combined with hyperthermic intraperitoneal chemo-therapy (HIPEC) in the treatment of diffuse peritoneal car-cinomatosis from ovarian cancer. Cancer 2008; 113: 315-325 [PMID: 18473354 DOI: 10.1002/cncr.23553]
48 Lim MC, Kang S, Choi J, Song YJ, Park S, Seo SS, Park SY. Hyperthermic intraperitoneal chemotherapy after extensive cytoreductive surgery in patients with primary advanced epithelial ovarian cancer: interim analysis of a phase II study. Ann Surg Oncol 2009; 16: 993-1000 [PMID: 19169758 DOI: 10.1245/s10434-008-0299-y]
49 Ansaloni L, De Iaco P, Frigerio L. Re: “cytoreductive sur-
gery and hyperthermic intraperitoneal chemotherapy as upfront therapy for advanced epithelial ovarian cancer: multi-institutional phase II trial.” - Proposal of a clinical trial of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in advanced ovarian cancer, the CHORINE study. Gynecol Oncol 2012; 125: 279-281 [PMID: 22233688 DOI: 10.1016/j.ygyno.2012.01.001]
50 Deraco M, Kusamura S, Virzì S, Puccio F, Macrì A, Famulari C, Solazzo M, Bonomi S, Iusco DR, Baratti D. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy as upfront therapy for advanced epithelial ovarian cancer: multi-institutional phase-II trial. Gynecol Oncol 2011; 122: 215-220 [PMID: 21665254 DOI: 10.1016/j.ygyno.2011.05.004]
51 Markman M. Hyperthermic intraperitoneal chemotherapy in the management of ovarian cancer: A critical need for an evidence-based evaluation. Gynecol Oncol 2009; 113: 4-5 [PMID: 19176238 DOI: 10.1016/j.ygyno.2008.12.022]
52 Verwaal VJ, van Tinteren H, Ruth SV, Zoetmulder FA. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2004; 85: 61-67 [PMID: 14755505 DOI: 10.1002/jso.20013]
53 Schierl R, Novotna J, Piso P, Böhlandt A, Nowak D. Low sur-face contamination by cis/oxaliplatin during hyperthermic intraperitoneal chemotherapy (HIPEC). Eur J Surg Oncol 2012; 38: 88-94 [PMID: 22035874 DOI: 10.1016/j.ejso.2011.10.009]
54 Li G, Gu R, Wen X, Wei D, Ming X, Chen H. The effect of early enteral nutrition on hyperthermic intraoperative in-traperitoneal chemotherapy-induced mucosal permeability following gastrectomy. JPEN J Parenter Enteral Nutr 2012; 36: 213-218 [PMID: 22038209 DOI: 10.1177/0148607111414022]
55 Kusamura S, Baratti D, Deraco M. Multidimensional analy-sis of the learning curve for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal surface malignancies. Ann Surg 2012; 255: 348-356 [PMID: 22202584 DOI: 10.1097/SLA.0b013e3182436c28]
56 Duckworth KE, McQuellon RP, Russell GB, Cashwell CS, Shen P, Stewart JH, Levine EA. Patient rated outcomes and survivorship following cytoreductive surgery plus hyper-thermic intraperitoneal chemotherapy (CS + HIPEC). J Surg Oncol 2012; 106: 376-380 [PMID: 22441970 DOI: 10.1002/jso.23089]
57 Parson EN, Lentz S, Russell G, Shen P, Levine EA, Stewart JH. Outcomes after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal surface dissemi-nation from ovarian neoplasms. Am J Surg 2011; 202: 481-486 [PMID: 21474115 DOI: 10.1016/j.amjsurg.2011.02.004]
58 Königsrainer I. Selection criteria for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in gastric cancer. World J Gastroenterol 2011; 17: 4153-4156 [PMID: 22072845 DOI: 10.3748/wjg.v17.i37.4153]
59 Hill AR, McQuellon RP, Russell GB, Shen P, Stewart JH, Levine EA. Survival and quality of life following cytoreduc-tive surgery plus hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis of colonic origin. Ann Surg Oncol 2011; 18: 3673-3679 [PMID: 21674272 DOI: 10.1245/s10434-011-1793-1]
P- Reviewer: CDutsch-Wicherek M S- Editor: Gou SX L- Editor: A E- Editor: Zheng XM
Eskander RN et al . HIPEC and EOC

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.101
World J Obstet Gynecol 2013 November 10; 2(4): 101-107ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Cytoreductive surgery after recurrent epithelial ovarian cancer and at other timepoints
Paolo Sammartino, Tommaso Cornali, Marialuisa Framarino dei Malatesta, Pompiliu Piso
Paolo Sammartino, Tommaso Cornali, Department of Surgery Pietro Valdoni, Policlinico Umberto I, 00161 Rome, ItalyMarialuisa Framarino dei Malatesta, Department of Gyneco-logical Obstetrical and Urological Sciences, Policlinico Umberto I, 00161 Rome, ItalyPompiliu Piso, Department of General Surgery, Barmherzige Brüder Hospital, 93049 Regensburg, GermanyAuthor contributions: Sammartino P, Cornali T, dei Malatesta MF and Piso P designed research, analyzed data and wrote the paper.Correspondence to: Paolo Sammartino, MD, Department of Surgery Pietro Valdoni, Rome, Policlinico Umberto I, Via del Policlinico, 00161 Rome, Italy. [email protected]: +39-33-6615632 Fax: +39-64-9972146Received: December 13, 2012 Revised: March 28, 2013Accepted: May 8, 2013Published online: November 10, 2013
AbstractIn this descriptive review we look at the role of surgery for advanced ovarian cancer at other timepoints apart from the initial cytoreduction for front-line therapy or in-terval cytoreductive surgery after neoadjuvant chemothe-rapy. The chief surgical problem to face after primary treatment is recurrent ovarian cancer. Of far more mar-ginal concern are the second-look surgical procedures or the palliative efforts intended to resolve the patient’s symptoms with no curative intent. The role of surgery in recurrent ovarian cancer remains poorly defined. Current data, albeit from non-randomized studies, nevertheless clearly support surgical cytoreduction in selected patients, a rarely curative expedient that invariably yields a marked survival advantage over chemotherapy alone. Despite these findings, some consider it too early to adopt secon-dary cytoreduction as the standard care for patients with recurrent ovarian cancer and a randomized study is nee-ded. Two ongoing randomized trials (Arbeitsgemeinschaft Gynäkologische Onkologie-Desktop Ⅲ and Gynecologic
Oncology Group 213) intend to verify the role of secon-dary cytoreduction for platinum-sensitive ovarian cancer compared with chemotherapy considered as standard care for these patients. We await the results of these two trials for a definitive answer to the matter.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Ovarian cancer; Cytoreductive surgery; Re-current ovarian cancer; Secondary cytoreduction; Sur-gery for Platinum sensitive ovarian cancer; Surgery for Platinum resistant ovarian cancer
Core tip: The chief surgical problem to face after pri-mary treatment is recurrent ovarian cancer. The role of surgery in recurrent ovarian cancer remains poorly defined. Current data, albeit from non-randomized studies, nevertheless clearly support surgical cytore-duction in selected patients, a rarely curative expedient that invariably yields a marked survival advantage over chemotherapy alone. Despite these findings, some con-sider it too early to adopt secondary cytoreduction as the standard care for patients with recurrent ovarian cancer and a randomized study is needed.
Sammartino P, Cornali T, dei Malatesta MF, Piso P. Cytoreductive surgery after recurrent epithelial ovarian cancer and at other time-points. World J Obstet Gynecol 2013; 2(4): 101-107 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/101.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.101
INTRODUCTIONRecurrent disease is a challenging problem that sooner or later (within 18 mo after primary treatment) arises in about 80% of patients initially treated for advanced ovar-
101 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Sammartino P et al . Surgery for recurrent ovarian cancer
ian cancer[1-3] and contributes substantially to the poor long-term outcome for this disease portending long-term survival in only 20%-30% of patients already at an ad-vanced stage when diagnosed[4,5].
Before considering the current options for treating patients with recurrent ovarian cancer we therefore deem it useful to analyze the possible reasons explaining why the disease recurs.
The natural history of ovarian epithelial malignancies shows that tumors originating from the epithelium lining the ovarian surface, and according to the most recent cy-togenic hypotheses also those arising from the epithelium covering the fallopian tubes and fimbria[6,7], spread early to the peritoneum and locoregional lymph nodes[8].
Peritoneal spread, frequently with ascites, follows a well-known anatomic course linked to peritoneal fluid dy-namics leading neoplastic cells to colonize distant pelvic areas early thus making ovarian carcinoma the model for peritoneal spread from an intra-abdominal malignancy (Figure 1)[9,10].
These pathophysiological events easily explain epi-demiological data showing that when the disease is first diagnosed about 75% of women already have advanced ovarian cancer [International Federation of Gynecology and Obstetrics (FIGO) Ⅲ-Ⅳ][8] with major peritoneal and lymphatic spread obviously making the whole thera-peutic strategy a complex task.
Although surgery and adjuvant chemotherapy remain the mainstay of treatment for advanced ovarian cancer the optimal therapeutic goal remains hard to reach[11]. Even though the specific single therapeutic role that each of the two principle procedures (surgery and adjuvant chemotherapy) covers in integrated treatment is difficult to investigate, we underline that the outcome benefits induced by platinum and its derivatives and paclitaxel (eventually given also by the intraperitoneal route) have presumably reached a plateau that appears arduous to im-prove until new effective anticancer drugs become avail-able[12].
Even though experience over years has recognized the prognostic importance of surgical cytoreduction (less re-sidual disease = better outcome)[13], a concept underlined in a meta-analysis conducted in recent years by Bristow et al[14], surgery remains the most highly variable and poorly standardized therapeutic factor, depending on the various surgical schools, the individual surgeon’s cancer treatment policy and aims and finally on their technical skills.
Besides, some clinical oncologists, questioning whether surgery is really curative, despite convincing clinical evi-dence, hypothesize that whenever surgery achieves opti-mal disease control biological factors come into play and exert a determinant influence on the surgical outcome[15]. Going beyond these hypotheses if we want focus on the therapeutic potential of surgery in advanced ovarian can-cer we have to analyze precisely what these surgical pro-cedures aim to achieve and most important, how they are classified.
The surgical procedure for treating ovarian cancer is defined with the term “cytoreduction”, a definition that seemingly implies residual disease after surgical debulking. Indeed, published studies invariably express their surgical results in terms of residual disease, using classifications that may overlap over time but nevertheless identify as “optimal cytoreduction” surgery leaving residual disease measuring 2 to 1 cm or less. In the latest Cochrane sys-tematic review on this topic[11] the Gynecologic Oncology Group (GOG) currently defines optimal cytoreduction as residual tumor nodules “each” measuring 1 cm or less in maximal diameter underlining, however, the ideal surgical outcome as complete cytoreduction with no visible resid-ual disease. The same review, analyzing experience gained in the most accredited world centers or most cited stud-ies, underlines that surgery achieves this ideal outcome in only a mean 28% of the patients treated and most pub-lished surgical results describe residual disease ranging from less than 1 cm to more than 2 cm. Equally impor-tant, published surgical reports fail to quantify the overall number of residual lesions in each patient. Yet for two patients at the same disease stage both classified as opti-mally cytoreduced (residual disease measuring less than 1 cm) if one patient has 10 sites of residual disease and the other, for example, has more than 100 residua, outcomes can presumably differ. Similarly, in classification systems other than those used by the GOG (completeness of cy-toreduction score, by Sugarbaker[16]) the lack of a variable quantifying the overall number of residual lesions cre-ates substantial bias in analyzing the results because the group classified as optimally cytoreduced could comprise patients with differing amounts of residual disease. This drawback, already noted previously[17] but never investi-gated further, merits study to decide how to analyze the results in a more meaningful manner. Hence we reason-ably presume that other clinical conditions (age, stage, performance status, platinum sensitivity, body surface area and therefore pharmacological dose) being equal, in two optimally cytoreduced patients in whom the number of residual lesions differs widely adjuvant chemotherapy will yield non-overlapping results.
All these observations prompt us to suggest that recurrent disease in advanced ovarian cancer should in many patients be more correctly interpreted as residual disease given that despite adjuvant chemotherapy surgery often leaves numerically rather than diametrically impor-tant residual lesions that ultimately manifest clinically as recurrence.
SECOND-LOOK SURGERYThis term defines the surgical procedure used to confirm the response status in patients who are clinically disease-free after a front-line approach (primary cytoreduction and adjuvant chemotherapy). Second-look surgery is obviously not intended merely as a diagnostic procedure given that it envisages whenever possible resecting all clinically unrecognized disease eventually found.
102 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

The rationale underlying second-look surgery origi-nally hinged on the concept that identifying residual disease foci early after front-line chemotherapy, remov-ing them and consolidating the results with second-line chemotherapy improved survival. Positive histologic findings after second-look surgery directly reflect the initial disease stage and their percentage increases fur-ther in patients whose first operation leaves macroscopic residual disease[18]. Although second-look surgical pro-cedures enjoyed wide use in the 1980s and 1990s their application gradually declined insofar as more than 50% of the patients identified at second-look surgery as com-plete responders within 12 to 24 mo thereafter went on to experience recurrent disease[19,20]. Randomized clinical trials have shown that although second-look procedures can accurately define patient responders they failed to increase survival[21]. An Italian study intended to investi-gate whether during a second-look procedure systematic aortic and pelvic lymphadenectomy had outcome advan-tages over a simple biopsy taken from clinically suspected lymph-node stations failed to show that either procedure improved outcome[22].
In synthesis, current evidence therefore suggests that second-look surgery for ovarian cancer remains a useful therapeutic option when diagnostic investigations appear contrasting and can help ascertain the patient’s clinical sta-tus and eventually treat the disease but should be reserved for individual patients and has no place as a general proce-dure. However, it may be a valid option for patients whom are detected during second-look surgery with platinum-resistant recurrent disease. If a complete macroscopic cy-toreduction can be performed, patients will benefit as oth-erwise no real treatment options are available, in particular if hyperthermic intraperitoneal chemotherapy (HIPEC) can be added to the concept.
SURGERY FOR PLATINUM-RESISTANT RECURRENT OVARIAN CANCERWithin 6 mo after undergoing treatment with the front-line approach (cytoreductive surgery plus primary ad-juvant chemotherapy) 23% of patients with advanced
ovarian cancer experience recurrent disease[23,24]. Current consensus defines these patients as platinum-resistant. Platinum-resistance is a highly complex phenomenon that can develop during the natural history of the disease after initial platinum sensitivity. Studies conducted over recent years have emphasized the role played in chemoresistance by the so-called cancerous ovarian stem cells[25]. Previous surgery and chemotherapy in platinum-resistant patients seem to provide exceedingly disappointing results with a median survival of less than 10 mo[26-29]. This concern has now stimulated research efforts thus moving basic research into pharmacologic regimens towards promising advances using biological agents alone or combined with chemotherapy agents[30-32].
From the viewpoint of the surgical approach, an ex-tremely interesting new development seems to be the cu-mulative experience from two French groups who report in a large series of patients with recurrent ovarian cancer the surgical outcome after cytoreduction (peritonectomy procedures) and HIPEC and noted similar results in pa-tients classified as platinum-sensitive and platinum-resis-tant[33]. These results seemingly underline the dual impor-tance of endoperitoneal chemotherapy and concurrent hyperthermia. Endoperitoneal infusion undoubtedly has a pharmacokinetic advantage given that the “peritoneal plasma barrier” allows dose-intensity therapy and hyper-thermia concurrently increases the chemotherapy agent’s cytotoxic action and cell penetration perhaps overcoming problems related to platinum resistance[34,35]. If further confirmed these findings open the way to interesting fu-ture therapeutic advances, in particular because the mor-tality related to the procedure including HIPEC is low after absolving the learning curve although relevant mor-bidity is still frequent but most of it seems to be related to extended surgery. However, in HIPEC performed with oxaliplatin, postoperative bleeding after 7-10 d following surgery can be a serious complication in up to one third of all patients requiering a reoperation[36].
SURGERY FOR PLATINUM-SENSITIVE RECURRENT OVARIAN CANCERThe 4th ovarian cancer consensus conference held in 2010 stated that surgery might be appropriate in selected patients with platinum-sensitive recurrent ovarian cancer and might be beneficial if it achieved complete resec-tion[24]. The therapeutic value of repeating the initial surgical treatment (cytoreduction) in patients with ad-vanced ovarian cancer who will experience tumor recur-rence remains debatable. Since Berek et al[37] in 1983 first introduced the term “secondary cytoreduction” many papers published over the ensuing years have addressed this topic[38-44] and in recent years some investigators have even introduced the concept tertiary cytoreduction[45,46]. Secondary cytoreduction after an extended treatment-free interval (from 6 to 12 mo or more) can increase sur-vival (though rarely leads to a definitive cure) because the cytoreductive effect sums up with an improved response
103 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Figure 1 Peritoneal hydrodynamics.
Sammartino P et al . Surgery for recurrent ovarian cancer
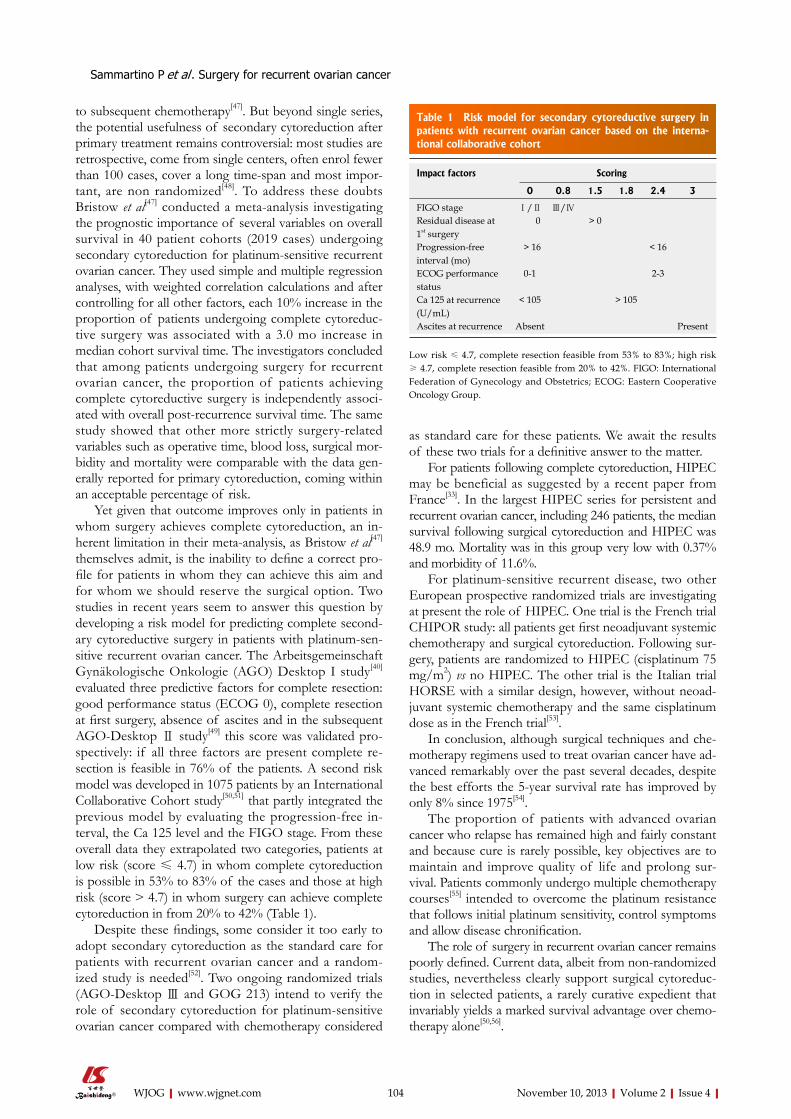
to subsequent chemotherapy[47]. But beyond single series, the potential usefulness of secondary cytoreduction after primary treatment remains controversial: most studies are retrospective, come from single centers, often enrol fewer than 100 cases, cover a long time-span and most impor-tant, are non randomized[48]. To address these doubts Bristow et al[47] conducted a meta-analysis investigating the prognostic importance of several variables on overall survival in 40 patient cohorts (2019 cases) undergoing secondary cytoreduction for platinum-sensitive recurrent ovarian cancer. They used simple and multiple regression analyses, with weighted correlation calculations and after controlling for all other factors, each 10% increase in the proportion of patients undergoing complete cytoreduc-tive surgery was associated with a 3.0 mo increase in median cohort survival time. The investigators concluded that among patients undergoing surgery for recurrent ovarian cancer, the proportion of patients achieving complete cytoreductive surgery is independently associ-ated with overall post-recurrence survival time. The same study showed that other more strictly surgery-related variables such as operative time, blood loss, surgical mor-bidity and mortality were comparable with the data gen-erally reported for primary cytoreduction, coming within an acceptable percentage of risk.
Yet given that outcome improves only in patients in whom surgery achieves complete cytoreduction, an in-herent limitation in their meta-analysis, as Bristow et al[47] themselves admit, is the inability to define a correct pro-file for patients in whom they can achieve this aim and for whom we should reserve the surgical option. Two studies in recent years seem to answer this question by developing a risk model for predicting complete second-ary cytoreductive surgery in patients with platinum-sen-sitive recurrent ovarian cancer. The Arbeitsgemeinschaft Gynäkologische Onkologie (AGO) Desktop I study[40] evaluated three predictive factors for complete resection: good performance status (ECOG 0), complete resection at first surgery, absence of ascites and in the subsequent AGO-Desktop Ⅱ study[49] this score was validated pro-spectively: if all three factors are present complete re-section is feasible in 76% of the patients. A second risk model was developed in 1075 patients by an International Collaborative Cohort study[50,51] that partly integrated the previous model by evaluating the progression-free in-terval, the Ca 125 level and the FIGO stage. From these overall data they extrapolated two categories, patients at low risk (score ≤ 4.7) in whom complete cytoreduction is possible in 53% to 83% of the cases and those at high risk (score > 4.7) in whom surgery can achieve complete cytoreduction in from 20% to 42% (Table 1).
Despite these findings, some consider it too early to adopt secondary cytoreduction as the standard care for patients with recurrent ovarian cancer and a random-ized study is needed[52]. Two ongoing randomized trials (AGO-Desktop Ⅲ and GOG 213) intend to verify the role of secondary cytoreduction for platinum-sensitive ovarian cancer compared with chemotherapy considered
as standard care for these patients. We await the results of these two trials for a definitive answer to the matter.
For patients following complete cytoreduction, HIPEC may be beneficial as suggested by a recent paper from France[33]. In the largest HIPEC series for persistent and recurrent ovarian cancer, including 246 patients, the median survival following surgical cytoreduction and HIPEC was 48.9 mo. Mortality was in this group very low with 0.37% and morbidity of 11.6%.
For platinum-sensitive recurrent disease, two other European prospective randomized trials are investigating at present the role of HIPEC. One trial is the French trial CHIPOR study: all patients get first neoadjuvant systemic chemotherapy and surgical cytoreduction. Following sur-gery, patients are randomized to HIPEC (cisplatinum 75 mg/m2) vs no HIPEC. The other trial is the Italian trial HORSE with a similar design, however, without neoad-juvant systemic chemotherapy and the same cisplatinum dose as in the French trial[53].
In conclusion, although surgical techniques and che-motherapy regimens used to treat ovarian cancer have ad-vanced remarkably over the past several decades, despite the best efforts the 5-year survival rate has improved by only 8% since 1975[54].
The proportion of patients with advanced ovarian cancer who relapse has remained high and fairly constant and because cure is rarely possible, key objectives are to maintain and improve quality of life and prolong sur-vival. Patients commonly undergo multiple chemotherapy courses[55] intended to overcome the platinum resistance that follows initial platinum sensitivity, control symptoms and allow disease chronification.
The role of surgery in recurrent ovarian cancer remains poorly defined. Current data, albeit from non-randomized studies, nevertheless clearly support surgical cytoreduc-tion in selected patients, a rarely curative expedient that invariably yields a marked survival advantage over chemo-therapy alone[50,56].
104 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Risk model for secondary cytoreductive surgery in patients with recurrent ovarian cancer based on the interna-tional collaborative cohort
Impact factors Scoring
0 0.8 1.5 1.8 2.4 3
FIGO stage Ⅰ/Ⅱ Ⅲ/ⅣResidual disease at 1st surgery
0 > 0
Progression-free interval (mo)
> 16 < 16
ECOG performance status
0-1 2-3
Ca 125 at recurrence (U/mL)
< 105 > 105
Ascites at recurrence Absent Present
Low risk ≤ 4.7, complete resection feasible from 53% to 83%; high risk ≥ 4.7, complete resection feasible from 20% to 42%. FIGO: International Federation of Gynecology and Obstetrics; ECOG: Eastern Cooperative Oncology Group.
Sammartino P et al . Surgery for recurrent ovarian cancer

Although we realize that scientific research requires level 1 evidence to conclude that one therapeutic op-tion is better than another, randomizing a patient with recurrent ovarian cancer who is technically operable (the Desktop Ⅲ protocol requires as an inclusion criterion scores known to predict complete cytoreduction) could raise ethical doubts and probably does nothing to help patient accrual.
And finally, the latest advances from studies investi-gating the pathogenesis of ovarian cancer clearly show that a “blanket approach” to ovarian cancer treatment is insufficient[7]. The key future turning point for guaran-teeing effective treatment depends on developing target therapies designed to exploit the molecular and genetic characteristics of individual tumor subtypes. These ob-servations raise further doubts on the appropriateness of randomized trials enrolling patients whose tumors differ widely in biological features.
REFERENCES1 Hennessy BT, Coleman RL, Markman M. Ovarian cancer.
Lancet 2009; 374: 1371-1382 [PMID: 19793610 DOI: 10.1016/S0140-6736(09)61338-6]
2 Ledermann JA, Raja FA. Clinical trials and decision-making strategies for optimal treatment of relapsed ovarian cancer. Eur J Cancer 2011; 47 Suppl 3: S104-S115 [PMID: 21943964 DOI: 10.1016/j.wear.2010.07.013]
3 Harter P, Heitz F, du Bois A. Surgery for relapsed ovarian cancer: when should it be offered? Curr Oncol Rep 2012; 14: 539-543 [PMID: 22918696 DOI: 10.1007/s11912-012-0260-x]
4 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
5 Ozols RF, Bundy BN, Greer BE, Fowler JM, Clarke-Pearson D, Burger RA, Mannel RS, DeGeest K, Hartenbach EM, Baer-gen R. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncol-ogy Group study. J Clin Oncol 2003; 21: 3194-3200 [PMID: 12860964 DOI: 10.1200/JCO.2003.02.153]
6 Kurman RJ, Shih IeM. Pathogenesis of ovarian cancer: les-sons from morphology and molecular biology and their clin-ical implications. Int J Gynecol Pathol 2008; 27: 151-160 [PMID: 18317228 DOI: 10.1097/PGP.0b013e318161e4f5]
7 Karst AM, Drapkin R. Ovarian cancer pathogenesis: a model in evolution. J Oncol 2010; 2010: 932371 [PMID: 19746182]
8 Fader AN, Rose PG. Role of surgery in ovarian carcinoma. J Clin Oncol 2007; 25: 2873-2883 [PMID: 17617518 DOI: 10.1200/JCO.2007.11.0932]
9 Carmignani CP, Sugarbaker TA, Bromley CM, Sugarbaker PH. Intraperitoneal cancer dissemination: mechanisms of the patterns of spread. Cancer Metastasis Rev 2003; 22: 465-472 [PMID: 12884919]
10 Feki A, Berardi P, Bellingan G, Major A, Krause KH, Petig-nat P, Zehra R, Pervaiz S, Irminger-Finger I. Dissemination of intraperitoneal ovarian cancer: Discussion of mechanisms and demonstration of lymphatic spreading in ovarian cancer model. Crit Rev Oncol Hematol 2009; 72: 1-9 [PMID: 19179094 DOI: 10.1016/j.critrevonc.2008.12.003]
11 Elattar A, Bryant A, Winter-Roach BA, Hatem M, Naik R. Optimal primary surgical treatment for advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2011; CD007565 [PMID: 21833960 DOI: 10.1002/14651858.CD007565.pub2]
12 Hoskins P, Vergote I, Cervantes A, Tu D, Stuart G, Zola P,
Poveda A, Provencher D, Katsaros D, Ojeda B, Ghatage P, Grimshaw R, Casado A, Elit L, Mendiola C, Sugimoto A, D’Hondt V, Oza A, Germa JR, Roy M, Brotto L, Chen D, Eisen-hauer EA. Advanced ovarian cancer: phase III randomized study of sequential cisplatin-topotecan and carboplatin-paclitaxel vs carboplatin-paclitaxel. J Natl Cancer Inst 2010; 102: 1547-1556 [PMID: 20937992]
13 Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr 1975; 42: 101-104 [PMID: 1234624]
14 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167 DOI: 10.1200/JCO.20.5.1248]
15 Crawford SC, Vasey PA, Paul J, Hay A, Davis JA, Kaye SB. Does aggressive surgery only benefit patients with less ad-vanced ovarian cancer? Results from an international com-parison within the SCOTROC-1 Trial. J Clin Oncol 2005; 23: 8802-8811 [PMID: 16314640 DOI: 10.1200/JCO.2005.02.1287]
16 Sugarbaker PH. Peritoneal carcinomatosis: principle of man-agement. Boston: Kluwer Academic, 1996
17 Stoeckle E, Paravis P, Floquet A, Thomas L, Tunon de Lara C, Bussières E, Macgrogan G, Picot V, Avril A. Number of residual nodules, better than size, defines optimal surgery in advanced epithelial ovarian cancer. Int J Gynecol Cancer 2004; 14: 779-787 [PMID: 15361184 DOI: 10.1111/j.1048-891X.2004.014508.x]
18 Ayhan A, Yarali H, Develioğlu O, Uren A, Ozyilmaz F. Prog-nosticators of second-look laparotomy findings in patients with epithelial ovarian cancer. J Surg Oncol 1991; 46: 222-225 [PMID: 2008088 DOI: 10.1002/jso.2930460403]
19 Podratz KC, Cliby WA. Second-look surgery in the manage-ment of epithelial ovarian carcinoma. Gynecol Oncol 1994; 55: S128-S133 [PMID: 7835796]
20 NIH consensus conference. Ovarian cancer. Screening, treat-ment, and follow-up. NIH Consensus Development Panel on Ovarian Cancer. JAMA 1995; 273: 491-497 [PMID: 7837369 DOI: 10.1001/jama.1995.03520300065039]
21 Nicoletto MO, Tumolo S, Talamini R, Salvagno L, Frances-chi S, Visonà E, Marin G, Angelini F, Brigato G, Scarabelli C, Carbone A, Cecchetto A, Prosperi A, Rosabian A, Giusto M, Cima GP, Morassut S, Nascimben O, Vinante O, Fiorentino MV. Surgical second look in ovarian cancer: a randomized study in patients with laparoscopic complete remission--a Northeastern Oncology Cooperative Group-Ovarian Can-cer Cooperative Group Study. J Clin Oncol 1997; 15: 994-999 [PMID: 9060538]
22 Dell’ Anna T, Signorelli M, Benedetti-Panici P, Maggioni A, Fossati R, Fruscio R, Milani R, Bocciolone L, Buda A, Mangioni C, Scambia G, Angioli R, Campagnutta E, Grassi R, Landoni F. Systematic lymphadenectomy in ovarian can-cer at second-look surgery: a randomised clinical trial. Br J Cancer 2012; 107: 785-792 [PMID: 22864456 DOI: 10.1038/bjc.2012.336]
23 du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekolo-gische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009; 115: 1234-1244 [PMID: 19189349]
24 Friedlander M, Trimble E, Tinker A, Alberts D, Avall-Lundqvist E, Brady M, Harter P, Pignata S, Pujade-Lauraine E, Sehouli J, Vergote I, Beale P, Bekkers R, Calvert P, Cope-land L, Glasspool R, Gonzalez-Martin A, Katsaros D, Kim JW, Miller B, Provencher D, Rubinstein L, Atri M, Zeimet A, Bacon M, Kitchener H, Stuart GC. Clinical trials in recurrent
105 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Sammartino P et al . Surgery for recurrent ovarian cancer

ovarian cancer. Int J Gynecol Cancer 2011; 21: 771-775 [PMID: 21543939]
25 Ahmed N, Abubaker K, Findlay J, Quinn M. Cancerous ovar-ian stem cells: obscure targets for therapy but relevant to che-moresistance. J Cell Biochem 2013; 114: 21-34 [PMID: 22887554 DOI: 10.1002/jcb.24317]
26 Sehouli J, Stengel D, Harter P, Kurzeder C, Belau A, Bo-genrieder T, Markmann S, Mahner S, Mueller L, Lorenz R, Nugent A, Wilke J, Kuznik A, Doering G, Wischnik A, Sommer H, Meerpohl HG, Schroeder W, Lichtenegger W, Oskay-Oezcelik G. Topotecan Weekly Versus Conventional 5-Day Schedule in Patients With Platinum-Resistant Ovarian Cancer: a randomized multicenter phase II trial of the North-Eastern German Society of Gynecological Oncology Ovarian Cancer Study Group. J Clin Oncol 2011; 29: 242-248 [PMID: 21115872 DOI: 10.1200/JCO.2009.27.8911]
27 Baumann K, Pfisterer J, Wimberger P, Burchardi N, Kurzed-er C, du Bois A, Loibl S, Sehouli J, Huober J, Schmalfeldt B, Vergote I, Lück HJ, Wagner U. Intraperitoneal treatment with the trifunctional bispecific antibody Catumaxomab in patients with platinum-resistant epithelial ovarian can-cer: a phase IIa study of the AGO Study Group. Gynecol Oncol 2011; 123: 27-32 [PMID: 21733566 DOI: 10.1016/j.ygyno.2011.06.004]
28 Morris M, Gershenson DM, Wharton JT, Copeland LJ, Ed-wards CL, Stringer CA. Secondary cytoreductive surgery for recurrent epithelial ovarian cancer. Gynecol Oncol 1989; 34: 334-338 [PMID: 2767525]
29 Segna RA, Dottino PR, Mandeli JP, Konsker K, Cohen CJ. Secondary cytoreduction for ovarian cancer following cispla-tin therapy. J Clin Oncol 1993; 11: 434-439 [PMID: 8445417]
30 Marchini S, Fruscio R, Clivio L, Beltrame L, Porcu L, Nerini IF, Cavalieri D, Chiorino G, Cattoretti G, Mangioni C, Milani R, Torri V, Romualdi C, Zambelli A, Romano M, Signorelli M, di Giandomenico S, D’Incalci M. Resistance to platinum-based chemotherapy is associated with epithelial to mesenchymal transition in epithelial ovarian cancer. Eur J Cancer 2013; 49: 520-530 [PMID: 22897840 DOI: 10.1016/j.ejca.2012.06.026]
31 Verschraegen CF, Czok S, Muller CY, Boyd L, Lee SJ, Rut-ledge T, Blank S, Pothuri B, Eberhardt S, Muggia F. Phase II study of bevacizumab with liposomal doxorubicin for patients with platinum- and taxane-resistant ovarian can-cer. Ann Oncol 2012; 23: 3104-3110 [PMID: 22851407 DOI: 10.1093/annonc/mds172]
32 Heitz F, Harter P, Barinoff J, Beutel B, Kannisto P, Grabowski JP, Heitz J, Kurzeder C, du Bois A. Bevacizumab in the treat-ment of ovarian cancer. Adv Ther 2012; 29: 723-735 [PMID: 22941523]
33 Bakrin N, Cotte E, Golfier F, Gilly FN, Freyer G, Helm W, Glehen O, Bereder JM. Cytoreductive surgery and hyper-thermic intraperitoneal chemotherapy (HIPEC) for persistent and recurrent advanced ovarian carcinoma: a multicenter, prospective study of 246 patients. Ann Surg Oncol 2012; 19: 4052-4058 [PMID: 22825772 DOI: 10.1245/s10434-012-2510-4]
34 CRILE G. The effects of heat and radiation on cancers im-planted on the feet of mice. Cancer Res 1963; 23: 372-380 [PMID: 14023863]
35 Barlogie B, Corry PM, Drewinko B. In vitro thermoche-motherapy of human colon cancer cells with cis-dichloro diammineplatinum(II) and mitomycin C. Cancer Res 1980; 40: 1165-1168 [PMID: 7188883]
36 Halkia E, Spiliotis J, Sugarbaker P. Diagnosis and manage-ment of peritoneal metastases from ovarian cancer. Gastroen-terol Res Pract 2012; 2012: 541842 [PMID: 22888339]
37 Berek JS, Hacker NF, Lagasse LD, Nieberg RK, Elashoff RM. Survival of patients following secondary cytoreductive sur-gery in ovarian cancer. Obstet Gynecol 1983; 61: 189-193 [PMID: 6823360]
38 Eisenkop SM, Friedman RL, Spirtos NM. The role of sec-
ondary cytoreductive surgery in the treatment of patients with recurrent epithelial ovarian carcinoma. Cancer 2000; 88: 144-153 [PMID: 10618617 DOI: 10.1002/(SICI)1097-0142(40000101)88:1<144::AID-CNCR20>3.0.CO;2-X]
39 Zang RY, Li ZT, Tang J, Cheng X, Cai SM, Zhang ZY, Teng NN. Secondary cytoreductive surgery for patients with relapsed epithelial ovarian carcinoma: who benefits? Can-cer 2004; 100: 1152-1161 [PMID: 15022281 DOI: 10.1002/cncr.20106]
40 Harter P, du Bois A, Hahmann M, Hasenburg A, Burges A, Loibl S, Gropp M, Huober J, Fink D, Schröder W, Muenstedt K, Schmalfeldt B, Emons G, Pfisterer J, Wollschlaeger K, Meerpohl HG, Breitbach GP, Tanner B, Sehouli J. Surgery in recurrent ovarian cancer: the Arbeitsgemeinschaft Gyn-aekologische Onkologie (AGO) DESKTOP OVAR trial. Ann Surg Oncol 2006; 13: 1702-1710 [PMID: 17009163]
41 Chi DS, McCaughty K, Diaz JP, Huh J, Schwabenbauer S, Hummer AJ, Venkatraman ES, Aghajanian C, Sonoda Y, Abu-Rustum NR, Barakat RR. Guidelines and selection cri-teria for secondary cytoreductive surgery in patients with recurrent, platinum-sensitive epithelial ovarian carcinoma. Cancer 2006; 106: 1933-1939 [PMID: 16572412 DOI: 10.1002/cncr.21845]
42 Oksefjell H, Sandstad B, Tropé C. The role of secondary cytoreduction in the management of the first relapse in epi-thelial ovarian cancer. Ann Oncol 2009; 20: 286-293 [PMID: 18725390 DOI: 10.1093/annonc/mdn591]
43 Tian WJ, Jiang R, Cheng X, Tang J, Xing Y, Zang RY. Surgery in recurrent epithelial ovarian cancer: benefits on Survival for patients with residual disease of 0.1-1 cm after second-ary cytoreduction. J Surg Oncol 2010; 101: 244-250 [PMID: 20112269]
44 Sehouli J, Richter R, Braicu EI, Bühling KJ, Bahra M, Neu-haus P, Lichtenegger W, Fotopoulou C. Role of secondary cytoreductive surgery in ovarian cancer relapse: who will benefit? A systematic analysis of 240 consecutive patients. J Surg Oncol 2010; 102: 656-662 [PMID: 20734422 DOI: 10.1002/jso.21652]
45 Shih KK, Chi DS, Barakat RR, Leitao MM. Tertiary cytore-duction in patients with recurrent epithelial ovarian, fallo-pian tube, or primary peritoneal cancer: an updated series. Gynecol Oncol 2010; 117: 330-335 [PMID: 20189234 DOI: 10.1016/j.ygyno.2010.01.046]
46 Fotopoulou C, Richter R, Braicu IE, Schmidt SC, Neuhaus P, Lichtenegger W, Sehouli J. Clinical outcome of tertiary surgi-cal cytoreduction in patients with recurrent epithelial ovar-ian cancer. Ann Surg Oncol 2011; 18: 49-57 [PMID: 20697821 DOI: 10.1245/s10434-010-1245-3]
47 Bristow RE, Puri I, Chi DS. Cytoreductive surgery for recur-rent ovarian cancer: a meta-analysis. Gynecol Oncol 2009; 112: 265-274 [PMID: 18937969 DOI: 10.1016/j.ygyno.2008.08.033]
48 Munkarah AR, Coleman RL. Critical evaluation of sec-ondary cytoreduction in recurrent ovarian cancer. Gynecol Oncol 2004; 95: 273-280 [PMID: 15491746 DOI: 10.1016/j.ygyno.2004.09.018]
49 Harter P, Sehouli J, Reuss A, Hasenburg A, Scambia G, Cib-ula D, Mahner S, Vergote I, Reinthaller A, Burges A, Hanker L, Pölcher M, Kurzeder C, Canzler U, Petry KU, Obermair A, Petru E, Schmalfeldt B, Lorusso D, du Bois A. Prospec-tive validation study of a predictive score for operability of recurrent ovarian cancer: the Multicenter Intergroup Study DESKTOP II. A project of the AGO Kommission OVAR, AGO Study Group, NOGGO, AGO-Austria, and MITO. Int J Gynecol Cancer 2011; 21: 289-295 [PMID: 21270612]
50 Zang RY, Harter P, Chi DS, Sehouli J, Jiang R, Tropé CG, Ayhan A, Cormio G, Xing Y, Wollschlaeger KM, Braicu EI, Rabbitt CA, Oksefjell H, Tian WJ, Fotopoulou C, Pfisterer J, du Bois A, Berek JS. Predictors of survival in patients with recurrent ovarian cancer undergoing secondary cytoreduc-tive surgery based on the pooled analysis of an international
106 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Sammartino P et al . Surgery for recurrent ovarian cancer

107 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
collaborative cohort. Br J Cancer 2011; 105: 890-896 [PMID: 21878937 DOI: 10.1038/bjc.2011.328]
51 Tian WJ, Chi DS, Sehouli J, Tropé CG, Jiang R, Ayhan A, Cormio G, Xing Y, Breitbach GP, Braicu EI, Rabbitt CA, Ok-sefjell H, Fotopoulou C, Meerpohl HG, du Bois A, Berek JS, Zang RY, Harter P. A risk model for secondary cytoreductive surgery in recurrent ovarian cancer: an evidence-based pro-posal for patient selection. Ann Surg Oncol 2012; 19: 597-604 [PMID: 21732142 DOI: 10.1245/s10434-011-1873-2]
52 Galaal K, Naik R, Bristow RE, Patel A, Bryant A, Dickin-son HO. Cytoreductive surgery plus chemotherapy versus chemotherapy alone for recurrent epithelial ovarian cancer. Cochrane Database Syst Rev 2010; CD007822 [PMID: 20556785]
53 Helm CW. Current status and future directions of cytore-ductive surgery and hyperthermic intraperitoneal chemo-
therapy in the treatment of ovarian cancer. Surg Oncol Clin N Am 2012; 21: 645-663 [PMID: 23021722]
54 Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin 2008; 58: 71-96 [PMID: 18287387 DOI: 10.1109/MP.2008.4475791]
55 Hanker LC, Loibl S, Burchardi N, Pfisterer J, Meier W, Pu-jade-Lauraine E, Ray-Coquard I, Sehouli J, Harter P, du Bois A. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann Oncol 2012; 23: 2605-2612 [PMID: 22910840 DOI: 10.1093/annonc/mds203]
56 Ledermann JA, Raja FA. Clinical trials and decision-making strategies for optimal treatment of relapsed ovarian cancer. Eur J Cancer 2011; 47 Suppl 3: S104-S115 [PMID: 21943964 DOI: 10.1016/S0959-8049(11)70154-X]
P- Reviewer: Diaz-Montes TP S- Editor: Gou SX L- Editor: A E- Editor: Zheng XM
Sammartino P et al . Surgery for recurrent ovarian cancer

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.108
World J Obstet Gynecol 2013 November 10; 2(4): 108-115ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Comprehensive management of epithelial ovarian cancer with peritoneal metastases
Luigi Frigerio, Luca Ansaloni, Elia Poiasina, Federico Coccolini, Paul H Sugarbaker
Luigi Frigerio, Obstetrics and Gynecology Department, Ospedali Riuniti, 24128 Bergamo, ItalyLuca Ansaloni, Elia Poiasina, Federico Coccolini, General and Emergency Surgery Department, Ospedali Riuniti, 24128 Bergamo, ItalyPaul H Sugarbaker, Washington Cancer Institute, Washington Hospital Center, Washington, DC 20010, United StatesAuthor contributions: All authors were responsible for the con-ception and design, collection and assembly of data, data analysis and interpretation; Frigerio L, Ansaloni L and Sugarbaker PH were responsible for the provision of study materials or patients and manuscript writing.Correspondence to: Dr. Paul H Sugarbaker, Washington Cancer Institute, Washington Hospital Center, 106 Irving Street, NW, Suite 3900, Washington, DC 20010, United States. [email protected]: +1-202-8773908 Fax: +1-202-8778602Received: December 15, 2012 Revised: January 5, 2012Accepted: January 11, 2013Published online: November 10, 2013
AbstractOvarian cancer has as its predominant pattern of dissem-ination metastases to the peritoneal surfaces and disease spread within the abdomen and pelvis that most com-monly causes the patients demise. To combat peritoneal metastases, cytoreductive surgery with peritoneal and visceral resections is combined with intraperitoneal and systemic chemotherapy. Chemotherapy given in the op-erating room after the complete visible removal of ovar-ian cancer is hyperthermic intraperitoneal chemotherapy. The results of the combined treatment are determined by the extent of prior surgery, the extent of disease as es-tablished by the peritoneal cancer index, and the quality of the cytoreduction as measured by the completeness of cytoreduction score. Recent clinical information on patients with recurrent ovarian cancer suggest a median overall survival of up to 60 mo. These data are greatly
improved over the one year survival observed in the past.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Peritoneal metastases; Carcinomatosis; Cy-toreductive surgery; Hyperthermic intraperitoneal che-motherapy; Intraperitoneal chemotherapy; Cisplatin; Doxorubicin; Ifosfamide; Mitomycin C; Intraperitoneal port
Frigerio L, Ansaloni L, Poiasina E, Coccolini F, Sugarbaker PH. Comprehensive management of epithelial ovarian cancer with peritoneal metastases. World J Obstet Gynecol 2013; 2(4): 108-115 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/108.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.108
INTRODUCTIONEpithelial ovarian cancer (EOC) is a global healthcare problem. It affects over 200000 women and causes 125000 deaths annually[1]. Within the United States, EOC is the ninth most common female cancer (21000 cases annually) and the fifth most common cause of cancer death (14600) in women[2]. Improved strategies for EOC are needed be-cause currently less than 50% of women with EOC will survive 5 years[3,4]. In the general population the lifetime risk of ovarian cancer is 1 in 70 but there are women with much higher risk especially those with germ line muta-tions of BRCA1 and BRCA2 tumor suppressor genes and certain mismatch repair genes[5].
SURGICAL MANAGEMENT OF OVARIAN CANCERThe surgical intervention in EOC with peritoneal metasta-
108 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Frigerio L et al . Peritoneal metastases
ses may occur with initial treatment (frontline), at interval debulking surgery following neoadjuvant chemotherapy or with recurrence. The major treatment modalities are cytoreductive surgery (CRS), perioperative chemotherapy including hyperthermic intraperitoneal chemotherapy (HIPEC), and long-term combined intravenous and in-traperitoneal chemotherapy. Second look surgery may be indicated in selected patients. It has been established that improved outcome is associated with small-volume residual disease following CRS. With current thinking a highest goal of treatment must be CRS to remove all vis-ible evidence of disease[6,7]. Or if that is not possible, sur-gery should leave the least amount of residual disease[8,9]. In the past, CRS that left residual cancerous lesions up to 2 cm in greatest dimension was considered “optimal”. However, the precise definition of optimal cytoreduction has been open to wide differences of opinion which have changed considerably over time. It is now accepted that leaving no visible disease should always be considered op-timal CRS at all time-points for EOC surgery except for palliation[10-12].
Several divergent types of surgical procedures are necessary to achieve complete cytoreduction because EOC is often widespread within the abdominal and pel-vic cavity. In the past, disease involving upper abdominal structures such as the undersurface of the diaphragm, liver surface or parenchyma, porta hepatis, pancreas, and spleen were considered obstacles to the achievement of optimal CRS. It has been shown that the resection of tumor from these sites does improve survival whether this is achieved by the gynecologic oncologists or surgical oncologists[13]. The actual sites of intra-abdominal disease not amenable to safe resection at a particular institution vary according to surgical expertise and practice. Some of the sites most likely to result in an incomplete resection include parenchymal liver metastases, extensive disease in the porta hepatis, retroperitoneal adenopathy behind and superior to the pancreas and extensive disease involving proximal small bowel and small bowel mesentery.
PATIENT SELECTION FOR A COMPREHENSIVE TREATMENT PLANSuccessful initiation of an optimal surgical outcome re-quires a knowledgeable selection of patients, a strong commitment from the surgical team, and institutional sup-port. The initial selection of patients is based on two well defined criteria: First, the ability of the patient to survive an extensive surgical procedure with acceptable morbidity and mortality and second, no evidence of intraoperative findings that would result in a futile surgical effort. Patients of advanced age, poor performance status, malnourished or with medical conditions that would decrease the likeli-hood of postoperative survival should be excluded. Also, patients with systemic metastases, multiple sites of bowel obstruction, common bile duct obstruction or ureteral ob-struction should rarely be considered for complete CRS.
Complete CRS requires dedication from a surgeon
who must have broad surgical knowledge, unusual techni-cal skills and the stamina to endure long procedures. Re-alizing that these interventions are extensive and thereby costly, institutional backing is important. An effort to ed-ucate other physicians involved in this treatment, as well as nurses and ancillary personnel, should be undertaken. The steep learning curve that characterizes this treatment strategy makes it essential to design a careful plan and to regularly critically evaluate all adverse events.
QUANTITATIVE PROGNOSTIC INDICATORSThe three assessments helpful for patient selection in order to treat patients most likely to benefit are the prior surgical score (PSS), the peritoneal cancer index (PCI) and the completeness of cytoreduction score (CC). These scores are determined from 13 abdominopelvic regions. Two transverse planes and two sagittal planes are used to divide the abdomen into 9 abdominopelvic regions (0-8). The upper transverse plane is located at the lowest aspect of the costal margin. Regions 9 and 10 define the upper and lower portions of the jejunum, and regions 11 and 12 define the upper and lower portions of the ileum[14].
Surgical trauma promotes the implantation and pro-gression of cancer nodules on peritoneal surfaces[15]. Prior surgeries may modify the natural history of ovarian cancer by inducing cancer growth at crucial anatomic sites located deep to the peritoneal layer[16]. Patients with no prior abdominopelvic surgery or biopsy only receive a PSS of 0, those with up to one abdominopelvic region dissected receive a PSS of 1, those with two to five ab-dominopelvic regions receive a PSS of 2 and those with six or more regions dissected receive a PSS of 3.
The PCI is a quantitative prognostic indicator deter-mined after abdominal exploration and complete separa-tion of intestinal adhesions (Figure 1). This index adds a lesion size parameter to the abdominopelvic regions so
109 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Peritoneal cancer index
Lesion size score
LS 0 No tumor seenLS 1 Tumor up to 0.5 cmLS 2 Tumor up to 5.0 cmLS 3 Tumor > 5.0 cm or confluence
0
6
2 31
8 4
57
10
911
12
Regions
0 Central1 Right upper2 Epigastrium3 Left upper4 Left flank5 Left lower6 Pelvis7 Right lower8 Right flank
9 Upper jejunum10 Lower jejunum11 Upper ileum12 Lower ileum
Lesion size
____________________________________
________________
PCI
Figure 1 The peritoneal cancer index uses the distribution of cancer im-plants throughout the abdomen and pelvis combined with a lesion size of these nodules in order to quantitate the disease upon abdominal explora-tion. PCI: Peritoneal cancer index.

that a numerical score estimating the extent of carcino-matosis is available. The PCI is an accurate prognostic indicator for ovarian cancer[17].
CC is a quantitative prognostic indicator determined once the surgical resection has been completed. A patient receives a CC-0 score when no visible peritoneal carci-nomatosis remains after cytoreduction, CC-1 is recorded when tumor nodules persist after cytoreduction but they measure less than 0.25 cm, CC-2 when remaining tumor measures between 0.25 to 2.5 cm. When tumor nodules are greater than 2.5 cm or there is confluence of unresectable tumor, a CC-3 score is given to the patient. Many prior studies in ovarian cancer have shown that the extent of disease remaining after cytoreduction is directly related to the survival[7-17].
PERITONECTOMY AND VISCERAL RESECTIONS USED TO ACHIEVE COMPLETE CYTOREDUCTION IN SELECTED PATIENTSThe goal of CRS is to reduce the tumor burden within the abdomen and pelvis to its absolute minimal volume. The best result is a patient who is visibly free of disease at the close of the procedure. The surgery combines a se-ries of peritonectomy procedures and visceral resections.
The peritonectomy procedures include anterior parietal peritonectomy, stripping of right and left hemidiaphragm, pelvic peritonectomy, and omental bursa peritonectomy. Visceral resections include hysterectomy and oophorec-tomy, greater and lesser omentectomy, splenectomy, right colectomy and rectosigmoid colectomy.
Construction of the surgical field to provide simultaneous exposure of the abdomen and pelvis A fixed retractor that provides a rigid frame around the whole abdomen (Thompson Surgical Instruments, Tra-verse City, Michigan) is positioned so that continuous retraction of all parts of the abdominal incision occurs (Figure 2A). The retraction system must be securely an-chored to the operating table to provide for continuous unencumbered visualization of a large operative field. An incision starting above the xiphisternal junction and continuing down to the pubis through the midline is constructed. An ellipse is created around the umbilicus to allow for the peritoneal plane to be clearly exposed throughout the extent of the abdominal incision. The fascia is divided through the linea alba from xiphoid bone to pubic bone. If there has been prior midline abdominal incision, it is widely excised. Routinely, the xiphoid is com-pletely resected at the xiphisternal junction as part of the specimen. With the fascia divided the parietal peritoneum remains intact.
110 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Undersurface left hemidiaphragm (with tumor)
Liver surface (with tumor)Umbilical fissure
Lesser omentum (with tumor)Stomach
Greater omentum (with tumor)Transverse colon
Suture ligaturesplenic A. and V.
Small bowel
Muscle-lefthemidiaphragm
Broad ligament(divided)
Mid-rectalcancer
Ovarian vessels(divided)
UreterInferior mesentericartery (ligated)
Line of peritoneal incision for complete pelvic peritonectomy
Left ext. iliac a.
Left ureter
Bladder
Vaginal cuff
Cut edge of peritoneum
Descending colon
Anvil of circular stapler
Rectum (stapled shut)
DC
BA
E
Figure 2 Peritonectomy procedures. A: A fixed retractor is used to provide exposure of the entire abdomen so that peritonectomy procedures on the anterior abdominal wall, beneath the hemidiaphragms, and within the pelvis can proceed in an efficient manner; B: Left upper quadrant peritonectomy; C: Cholecystectomy, lesser omentectomy and peritonectomy of the omental bursa; D: Rectosigmoid colon resection and complete pelvic peritonectomy; E: Reconstruction after recto-sigmoid colon resection and complete pelvic peritonectomy. The vagina is closed prior to the hyperthermic intraperitoneal chemotherapy. The low stapled colorectal anastomosis is performed after the chemotherapy lavage is complete (all from Sugarbaker [19]).
Frigerio L et al . Peritoneal metastases

Parietal peritoneal stripping from the anterior abdominal wall A single entry into the peritoneal cavity in the middle portion of the incision (peritoneal window) allows the surgeon to digitally and visibly assess the parietal peri-toneum and the small bowel surfaces. If cancer nodules are palpated on the parietal peritoneum larger than those involving the small bowel and its mesentery, a decision for a complete dissection is made. Except for the small defect in the peritoneum required for this peritoneal ex-ploration, the remainder of the peritoneum is kept intact to facilitate the peritonectomy.
Stripping the visceral peritoneum from the surface of the bladder After dissecting generously the peritoneum on both sides of the bladder, the apex of the bladder (preferably the urachus) is localized and placed on strong traction using a Babcock clamp. The peritoneum with the underlying fatty tissues are stripped away from the muscular surface of the bladder. Broad traction on the entire anterior pa-rietal peritoneal surface and frequent room temperature saline irrigation reveals the point for tissue transection that is precisely located between the bladder musculature and its adherent fatty tissue. This dissection is continued inferiorly down to the cervix.
Parietal peritoneal dissection to the paracolic sulcus and beyond The self-retaining retraction system is steadily advanced more deeply into the abdominal cavity. Firm broad trac-tion on the peritoneum at the point of dissection facili-tates accurate progress. The peritoneum strips readily from the undersurface of the hemidiaphragm. The dissec-tion connects the right and left subphrenic peritonectomy superiorly and the complete pelvic peritonectomy inferi-orly. As the dissection proceeds beyond the peritoneum overlying the paracolic sulcus (line of Toldt) the dissection becomes more rapid because of the loose connections of the peritoneum to the underlying fatty tissue at this ana-tomic site.
When the anterior parietal peritonectomy has been completed, removal of this large peritoneal layer eradi-cates cancer implants from the posterior aspect of the anterior abdominal wall. Complete exploration of the abdomen and pelvis proceeds.
Peritoneal stripping from beneath the left hemidiaphragmTo begin peritonectomy of the left upper quadrant, the peritoneum is progressively stripped off the posterior rectus sheath (Figure 2B). Broad traction must be exerted on the tumor specimen throughout the left upper quad-rant. Strong traction combined with ball-tip electrosurgi-cal dissection allows separation of the peritoneum with tumor from all normal tissue in the left upper quadrant including the diaphragm muscle, the left adrenal gland, and the superior aspect of perirenal fat. The splenic flexure of the colon is divided from the peritoneum of the left abdominal gutter and moved medially.
Greater omentectomy and splenectomy with completion of the left subphrenic peritonectomy To free the mid-abdomen of tumor, the greater omentec-tomy-splenectomy is performed. The greater omentec-tomy is elevated and then separated from the transverse colon using electrosurgery. The omental tissue on the an-terior aspect of the transverse mesocolon is also resected. The gastroepiploic vessels on the greater curvature of the stomach are ligated and divided. Also, the short gastric vessels are transected. This freely exposes the splenic ar-tery and vein at the tail of the pancreas. These vessels are ligated in continuity and proximally suture ligated taking care not to traumatize pancreas parenchyma. This allows the greater curvature of the stomach to be reflected to the right from the pylorus to the gastroesophageal junction.
Peritoneal stripping from beneath the right hemidiaphragmPeritoneum is stripped away from the right posterior rec-tus sheath to begin the peritonectomy in the right upper quadrant of the abdomen. Strong traction on the peri-toneum infiltrated by tumor is used to elevate the rolled muscular edge of the hemidiaphragm into the operative field. Again, ball-tipped electrosurgery on pure cut is used to dissect at the interface of tumor and normal tissue. Coagulation current is used to divide the blood vessels as they are encountered and before they bleed.
Cholecystectomy and peritoneal stripping of the hepatoduodenal ligamentThe gallbladder is removed in a routine fashion from its fundus toward the cystic artery and cystic duct (Figure 2C). Blunt dissection of the cystic artery and cystic duct away from the common duct and right hepatic artery distin-guishes these structures from the surrounding tumor and fatty tissue. These structures are ligated and divided.
To strip the peritoneum from the anterior aspect of the hepatoduodenal ligament, its peritoneal reflection to the liver surface is divided. Special care is taken not to injure the left hepatic artery, which is usually the most superficial of the portal structures. The peritoneum, often layered by tumor nodules, is firmly grasped using a Rus-sian forceps and peeled away from the common bile duct and hepatic artery. The underside of the hepatoduodenal ligament must be visualized and peritoneum stripped if tumor is present.
Resection of the hepatogastric ligament and lesser omentumThe left lateral segment of the liver is retracted left to right to expose the hepatogastric ligament and lesser omentum in its entirety. A circumferential release of this ligament from the fissure between the left lateral portion of the liv-er and segment 1 occurs first. The arcade of right gastric artery to left gastric artery along the lesser curvature of the stomach must be skeletonized. After electrosurgically dividing the peritoneum on the lesser curvature of the stomach, digital dissection with extreme pressure from the surgeon’s thumb and index finger separates lesser omental
111 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Frigerio L et al . Peritoneal metastases

fat and tumor from the vascular arcade. As much of the anterior vagus nerve is spared as is possible with patience and persistence. The tumor and fatty tissue surrounding the right and left gastric arteries are split away from the vascular arcade. In this manner the specimen is centralized over the major branches of the left gastric artery. With strong traction on the specimen, the lesser omentum is released from the left gastric artery and vein.
Stripping of the peritoneum from the omental bursaWith the left lateral segment of the liver retracted to the right, further exposure of the peritoneal floor of the omental bursa is achieved through elevation of the left side of the caudate lobe of the liver. The peritoneal reflection between caudate and vena cava is electrosurgically divided. Also, the peritoneal reflection towards the left hepatic vein is divided. Then, blunt stripping of the peritoneum cov-ering the crus of the right hemidiaphragm is completed. This peritoneal stripping continues over the lymph nodes along the common hepatic artery and up into the tissues of the lesser omentum. Care is taken to avoid the origin and branches of the left gastric artery. Care is also taken to eliminate tumor nodules from the shelf created by the caudate lobe beneath the posterior aspect of the hepato-duodenal ligament.
Resection of rectosigmoid colon, uterus, ovaries and cul-de-sac of Douglas To being the rectosigmoid colon resection a linear stapler is used to divide the sigmoid colon just above the limits of the pelvic peritoneal metastases; this is usually at the junction of sigmoid and descending colon. The vascular supply of the distal portion of the bowel is traced back to its origin on the aorta. The inferior mesenteric artery and vein are ligated, suture-ligated, and divided. This al-lows one to pack all the viscera, including the proximal descending colon into the upper abdomen.
Ball-tipped electrosurgery is used to dissect at the lim-its of the pelvic peritonectomy (Figure 2D). The surgeon works in a centripetal fashion. Extra-peritoneal ligation of the uterine arteries is performed just above the ureter and close to the base of the bladder. In women, the bladder is moved gently off the cervix and the vagina is entered. The vaginal cuff anterior and posterior to the cervix is tran-sected using ball-tipped electrosurgery, and the rectovagi-nal septum is entered. Ball-tipped electrosurgery is used to divide the perirectal fat beneath the peritoneal reflection. This ensures that all tumors that occupy the peritoneum within the cul-de-sac are removed intact with the speci-men. The anterior rectal musculature is skeletonized using ball-tipped electrosurgery. Preservation of the lower half of the rectum will allow for a larger stool reservoir and diminish frequent bowel movements. A stapler is used to close off the rectal stump and the rectum is sharply di-vided above the stapler.
Secure vaginal closure and colorectal anastomosis Additional sutures are placed to close the apex of the va-gina (Figure 2E). These sutures are left long so that they
may be used to elevate the vaginal cuff and clearly expose the stump of the rectum.
Systematic pelvic and aortic lymphadenectomyOnce peritonectomy and visceral resections and after para-rectal and para-vesical spaces have been observed, systematic pelvic and aortic lymphadenectomy are per-formed.
Pelvic lymphadenectomy dissection begins at the origin of the external iliac vessels and continues caudally around them along the medial border of the psoas mus-cle. The aponeurotic fascia is kept intact and the branches of the genito-femoral nerve are carefully spared to limit the risk of postoperative neurological sequelae. The dis-section proceeds through the areolar plane between the adventitia of the artery and the lymphatic tissue. The lower limit of the external iliac lymphadenectomy is rep-resented by the deep inferior epigastric vessels. Lymph nodes along the external iliac vessels are removed en bloc with those adjacent to the common iliac vessels. The pso-as fascia, superficially, and the fascia covering the internal obturator and levator ani muscles, deeply, constitute the lateral boundaries of lymphadenectomy, while the medial margin is represented by an ideal plane between the um-bilical artery, anteriorly, and the rectum, posteriorly. After obturator nerve identification, lymphadenectomy of the obturator fossa is performed with the mobilization of the superficial obturator nodes which are removed en bloc with the perilymphatic fatty tissue around the internal iliac vessels at the origin of the internal pudendal vessels. Lymphadenectomy is completed by removing deep obtu-rator and gluteal nodes.
Aortic lymphadenectomy begins at the aortic bifur-cation up to the renal vessels. After having exteriorized the transverse colon and the small bowel, the superficial intercavo-aortic, precaval, and preaortic nodal groups are removed. Lymph nodes located lateral to the vena cava (i.e., paracaval nodal group) are separated from it and removed en bloc. Removal of the lymph nodes lateral to the aorta is carried out up to the level of the left renal vein, after en-tering the plane between the Toldt’s and Gerota’s fasciae, mobilizing the descending colon from the renal capsule, the psoas muscle, and the ovarian pedicle and displacing the ureter laterally. Lastly, lymph nodes behind the vena cava (i.e., retrocaval nodal group) and the lumbar vessels (i.e., deep intercavo-aortic nodal group) are removed if enlarged, by dissecting from the pre-vertebral fascia after displacing the vena cava and the aorta laterally and medially (Figure 3).
RATIONALE FOR HIPEC AND EARLY POSTOPERATIVE INTRAPERITONEAL CHEMOTHERAPY After the completion of cytoreduction when no visible cancer remains, it is invariably true that invisible to the naked eye, an immense number of cancer cells will re-main within the peritoneal cavity. Tumor manipulation, transected lymphatic ducts leaking tumor cells throughout
112 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Frigerio L et al . Peritoneal metastases

the procedure, and small tumor nodules remaining on the abdominal and pelvic surfaces of organs not amenable to peritonectomy procedures, namely small bowel, make necessary the implementation of some method that will eradicate residual tumor cells. Another well known site for persistent disease is the suture lines that are an ideal site for cancer cell implants. Tumor cell entrapment occurs on these raw surfaces with fibrin accumulating and tissues compressed together by stitches or staples. Suture lines are at high risk for recurrence if constructed before the HIPEC.
Technique for heated intraoperative intraperitoneal chemotherapyAn abdominopelvic reservoir is constructed by tenting up the skin edges on a fixed retractor that allows hand distri-bution of the chemotherapy agent and total containment. The gloved hand guarantees that the perfusate reaches all surfaces within the peritoneal cavity, such as the space between the bowel loops, the space behind the liver, and the pelvic cavity (Figure 4).
In order to keep the temperature at a constant 42 ℃, a hyperthermia pump forces the solution through a heat exchanger. Then it proceeds into the abdominopelvic cav-ity through an inflow catheter. The hyperthermic chemo-therapy fluid is drained from the abdomen through four closed drains going back to the heat exchanger, and clos-ing the circuit. The inflow catheter and the closed suction drains are secured watertight with purse-string sutures on the skin of the abdomen to avoid leaks and spillage. The chemotherapy solution circulates for 90 min at 42 ℃.
After the 90 min of HIPEC with manual distribution,
the surgeon may assume that fibrin and tissue debris and the microscopic residual disease they contain have been eradicated. At this time, all the anastomosis and any addi-tional reconstruction can occur. Closed-suction drains and an inflow catheter are properly positioned for subsequent early postoperative intraperitoneal chemotherapy with paclitaxel. Standardized orders for bidirectional intraperi-toneal chemotherapy are given in Table 1. Cisplatin and doxorubicin are given by intraperitoneal administration and ifosfamide by intravenous continuous infusion (55-56).
Technique for early perioperative intraperitoneal chemotherapyIn the first five postoperative days the patient receives normothermic intraperitoneal paclitaxel (20-40 mg/m2 per day), with the goal of consolidating the intraperito-neal chemotherapy treatments. The extremely favorable area under the curve ratio and the remarkable drug pen-etration of up to 80 cell layers deserve mention. Stan-dardized orders for early postoperative intraperitoneal chemotherapy with paclitaxel are given in Table 2.
RESULTS OF COMPREHENSIVE TREATMENT IN ADVANCED PRIMARY AND RECURRENT OVARIAN CANCER In patients who have failed the standard treatments of pri-mary ovarian cancer the survival is short with an estimated
113 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Figure 3 Retroperitoneal space after pelvic and periaortic lymphadenec-tomy (from archives of Frigerio L).
Table 1 Intraoperative bidirectional chemotherapy orders
Add cisplatin (50 mg/m2) ________ mg to 2 L of 1.5% dextrose peritoneal dialysis solutionAdd doxorubicin (15 mg/m2) ________ mg to same 2 L of 1.5% dextrose peritoneal dialysis solutionAdd ifosfamide (1300 mg/m2) ________ mg to 1 L normal salineBegin continuous iv infusion over 90 min simultaneous with ip chemotherapyAdd mesna disulfide (260 mg/m2) ________ mg in 100 mL 0.9% sodium chloride to be given iv as a bolus 15 min prior to ifosfamide infusionAdd mesna disulfide (260 mg/m2) ________ mg in 100 mL 0.9% sodium chloride to be given iv as a bolus 4 h after ifosfamide infusionAdd mesna disulfide (260 mg/m2) ________ mg in 100 mL 0.9% sodium chloride to be given iv as a bolus 8 h after ifosfamide infusionSend all the above to operating room No. _______ at _______ o’clock on ___________ (date) for a 90-min treatment
Figure 4 Hyperthermic intraperitoneal chemotherapy proceeds by con-structing a reservoir from the abdominal space. The skin edges are elevated on a self-retaining retractor and a plastic sheet covers the open abdomen. A cruci-ate incision in this plastic sheet allows free access of the surgeon’s double-gloved hand. Uniform distribution of heat and chemotherapy is maintained throughout the 90 min of the Hyperthermic intraperitoneal chemotherapy treatment.
Frigerio L et al . Peritoneal metastases

114 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
median survival of 9 mo. The median survival of 28 pa-tients with advanced primary and recurrent EOC who had an attempt at complete cytoreduction combined with peri-operative chemotherapy at the Washington Cancer Insti-tute was 45.8 mo[16]. Further analysis by Look et al[16] of the clinical features that affected survival showed that extent of prior surgery and completeness of cytoreduction were independent factors significantly affecting survival. Those patients with extensive prior surgery, that is with three or more abdominopelvic regions subjected to surgical dissec-tion, were less likely to receive a complete cytoreduction and their survival was significantly shorter. Patients with a low PSS who had less than three abdominopelvic regions previously dissected had a median survival of 6.5 years, compared to 1.5 years for those patients with a higher PSS (P < 0.001). Patients with an adequate cytoreduction had a median survival of 55.9 mo; suboptimal cytoreduction showed an 8 mo survival (P = 0.037).
Tentes and colleagues reported on the PCI as a quan-titative prognostic indicator in 60 women with ovarian cancer[17]. Those patients with a PCI lower than 10 had a median survival of 80 mo and a 5-year survival of 65%, while those patients with a PCI greater than 10 had a me-dian survival of 38 mo and a 5-year survival rate of 29% (P = 0.0253).
Recently, Bijelic et al[18] published a systematic review analyzing 14 studies that reported on cytoreduction and HIPEC. Ten studies reported a positive impact of CRS and HIPEC on survival and in 4, survival was not ana-lyzed. Morbidity ranged from 5% to 36% and the median mortality was 3%.
Recent results of treatment This comprehensive management plan has been reported in approximately 35 manuscripts over the last two de-cades. As experience in patient selection and refinements in surgical technology have occurred, a gradual improve-ment in survival benefits and a decrease in morbidity and mortality have occurred. Clinical information from 7 recent reports are presented in Table 3.
In conclusion, this highly specialized treatment needs to be performed by qualified surgeons who are knowl-edgeable about peritonectomy procedures. Accepting the fact that there might be a selection bias, the results with this comprehensive treatment are encouraging. Multi-institutional studies are in progress to further validate the benefits of complete CRS in patients with ovarian cancer. The strong rationale, the initial favorable results by com-petent groups, and the demonstrated safety justify the cur-rent use of complete CRS.
REFERENCES1 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statis-
tics, 2002. CA Cancer J Clin 2005; 55: 74-108 [PMID: 15761078]2 American Cancer Society. Cancer Facts and Figures 2010.
Available from: URL: http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/cancer-facts-and-figures-2010. Accessed October 7, 2010
3 Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, Altekruse SF, Feuer EJ, Huang L, Mariotto A, Miller BA, Lewis DR, Eisner MP, Stinchcomb DG, Edwards BK. SEER Cancer Statistics Review, 1975-2006. Bethesda, MD: National Cancer Institute. Available from: URL: http://seer.cancer.gov/csr/1975_2006/. Based on November 2008
Table 2 Early postoperative intraperitoneal chemotherapy orders
Paclitaxel ________ mg (20-40 mg/m2 × _______ m2) (maximum dose: 80 mg) in_______mL 6% Hespan® (Braun B, Irvine, CA) via the Tenckhoff catheter or IP port dailyStart date: ________________ Stop date: __________________ (For daily doses > 500 mL total volume, pharmacy will split dose equally into two bags)Instill as rapidly as possible via the Tenckhoff catheter or ip portDwell for 23 h Drain from Jackson-Pratt drains for one hour prior to the next instillationContinue to drain the abdominal cavity by Jackson-Pratt drains after the last dose of ip chemotherapyDuring the initial 6 h after chemotherapy instillation, patient’s bed should be kept flatThe patient should be on the right side during instillationTurn ½ hour post instillation onto the left side and continue to change sides at ½ hour intervals for 6 hMonitor with a pulse oximeter during the first 6 h of each intraperitoneal chemotherapy
Table 3 Clinical information from recent reports on cytoreductive surgery and hyperthermic intraperitoneal chemotherapy with peritoneal metastases from ovarian cancer
Ref. n Median follow-up
(mo)
Median disease-free
survival (mo)
Median overall
survival (mo)
Overall 5-year
survival (mo)
Median length of hospital stay (d)
Mortality (%)
Morbidity Grade 3
(%)
Morbidity Grade 4
(%)
Bereder et al[20] 246 NR 13 49 35 17 0.4 12Pavlov et al[21] 56 60 26 38 NR 14 2 0 2Fagotti et al[22] 25 18 10 NR NR 13 0 8 8Guardiola et al[23] 47 23 14 NR NR 18 0 NR 13Di Giorgio et al[24] 47 NR 20 24 17 221 4 9 13Bae et al[25] 67 NR NR NR 66 NR 0 0 0Cotte et al[26] 81 47 19 28 NR 172 3 5 2
1Two-year survival results; 2Refers to results expressed as mean. NR: Not reported.
Frigerio L et al . Peritoneal metastases

115 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
SEER data submission, posted to the SEER web site, 2009. Accessed October 7, 2010
4 Heintz AP, Odicino F, Maisonneuve P, Quinn MA, Benedet JL, Creasman WT, Ngan HY, Pecorelli S, Beller U. Carci-noma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet 2006; 95 Suppl 1: S161-S192 [PMID: 17161157 DOI: 10.1016/S0020-7292(06)60033-7]
5 Tavassoli FA, Devilee P. World Health Organization Clas-sification of Tumours. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. Lyon: IARC Press, 2003
6 Munnell EW. The changing prognosis and treatment in cancer of the ovary. A report of 235 patients with primary ovarian carcinoma 1952-1961. Am J Obstet Gynecol 1968; 100: 790-805 [PMID: 4296050]
7 Griffiths CT, Craig JM, Kistner RW, Rothman KJ, Steiner GJ, Tomic M. Effect of castration, estrogen, and timed progestins on induced endometrial carcinoma in the rabbit. Gynecol On-col 1975; 3: 259-275 [PMID: 1213590]
8 Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influ-ence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 1992; 47: 159-166 [PMID: 1468693 DOI: 10.1016/0090-8258(92)90100-W]
9 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167 DOI: 10.1200/JCO.20.5.1248]
10 Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, Sonoda Y, Levine DA, Hensley M, Barakat RR. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol 2006; 103: 559-564 [PMID: 16714056 DOI: 10.1016/j.ygyno.2006.03.051]
11 Eisenkop SM, Spirtos NM. What are the current surgical ob-jectives, strategies, and technical capabilities of gynecologic oncologists treating advanced epithelial ovarian cancer? Gy-necol Oncol 2001; 82: 489-497 [PMID: 11520145 DOI: 10.1006/gyno.2001.6312]
12 Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreduc-tive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: a prospective study. Gynecol Oncol 1998; 69: 103-108 [PMID: 9600815 DOI: 10.1006/gyno.1998.4955]
13 Eisenhauer EL, Abu-Rustum NR, Sonoda Y, Levine DA, Poynor EA, Aghajanian C, Jarnagin WR, DeMatteo RP, D’Angelica MI, Barakat RR, Chi DS. The addition of extensive upper abdominal surgery to achieve optimal cytoreduction improves survival in patients with stages IIIC-IV epithelial ovarian cancer. Gynecol Oncol 2006; 103: 1083-1090 [PMID: 16890277 DOI: 10.1016/j.ygyno.2006.06.028]
14 Jacquet P, Sugarbaker PH. Current methodologies for clini-cal assessment of patients with peritoneal carcinomatosis. J Exp Clin Cancer Res 1996; 15: 49-58
15 Sugarbaker PH. Peritoneum as the first-line of defense in carcinomatosis. J Surg Oncol 2007; 95: 93-96 [PMID: 17262739
DOI: 10.1002/jso.20676]16 Look M, Chang D, Sugarbaker PH. Long-term results of
cytoreductive surgery for advanced and recurrent epithelial ovarian cancers and papillary serous carcinoma of the peri-toneum. Int J Gynecol Cancer 2004; 14: 35-41 [PMID: 14764027 DOI: 10.1111/j.1048-891x.2004.14008.x]
17 Tentes AA, Tripsiannis G, Markakidis SK, Karanikiotis CN, Tzegas G, Georgiadis G, Avgidou K. Peritoneal cancer index: a prognostic indicator of survival in advanced ovarian can-cer. Eur J Surg Oncol 2003; 29: 69-73 [PMID: 12559080]
18 Bijelic L, Jonson A, Sugarbaker PH. Systematic review of cy-toreductive surgery and heated intraoperative intraperitone-al chemotherapy for treatment of peritoneal carcinomatosis in primary and recurrent ovarian cancer. Ann Oncol 2007; 18: 1943-1950 [PMID: 17496308 DOI: 10.1093/annonc/mdm137]
19 Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am 2003; 12: 703-727, xiii [PMID: 14567026]
20 Bereder J, Glehen O, Habre J, Desantis M, Cotte E, Mounier N, Ray-Cocquard I, Karimdjee B, Bakrin N, Bernard J, Benchimol D, Gilly F. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the manage-ment of peritoneal carcinomatosis from ovarian cancer: A multiinstitutional study of 246 patients. J Clin Oncol 2009; 27: abstr 5542
21 Pavlov MJ, Kovacevic PA, Ceranic MS, Stamenkovic AB, Ivanovic AM, Kecmanovic DM. Cytoreductive surgery and modified heated intraoperative intraperitoneal chemo-therapy (HIPEC) for advanced and recurrent ovarian cancer -- 12-year single center experience. Eur J Surg Oncol 2009; 35: 1186-1191 [PMID: 19356887]
22 Fagotti A, Paris I, Grimolizzi F, Fanfani F, Vizzielli G, Naldi-ni A, Scambia G. Secondary cytoreduction plus oxaliplatin-based HIPEC in platinum-sensitive recurrent ovarian cancer patients: a pilot study. Gynecol Oncol 2009; 113: 335-340 [PMID: 19345401 DOI: 10.1016/j.ygyno.2009.03.004]
23 Guardiola E, Delroeux D, Heyd B, Combe M, Lorgis V, Demarchi M, Stein U, Royer B, Chauffert B, Pivot X. Intra-operative intra-peritoneal chemotherapy with cisplatin in patients with peritoneal carcinomatosis of ovarian can-cer. World J Surg Oncol 2009; 7: 14 [PMID: 19203351 DOI: 10.1186/1477-7819-7-14]
24 Di Giorgio A, Naticchioni E, Biacchi D, Sibio S, Accarpio F, Rocco M, Tarquini S, Di Seri M, Ciardi A, Montruccoli D, Sammartino P. Cytoreductive surgery (peritonectomy proce-dures) combined with hyperthermic intraperitoneal chemo-therapy (HIPEC) in the treatment of diffuse peritoneal car-cinomatosis from ovarian cancer. Cancer 2008; 113: 315-325 [PMID: 18473354 DOI: 10.1002/cncr.23553]
25 Bae JH, Lee JM, Ryu KS, Lee YS, Park YG, Hur SY, Ahn WS, Namkoong SE. Treatment of ovarian cancer with paclitaxel- or carboplatin-based intraperitoneal hyperthermic chemo-therapy during secondary surgery. Gynecol Oncol 2007; 106: 193-200 [PMID: 17466362 DOI: 10.1016/j.ygyno.2007.03.019]
26 Cotte E, Glehen O, Mohamed F, Lamy F, Falandry C, Gol-fier F, Gilly FN. Cytoreductive surgery and intraperitoneal chemo-hyperthermia for chemo-resistant and recurrent advanced epithelial ovarian cancer: prospective study of 81 patients. World J Surg 2007; 31: 1813-1820 [PMID: 17629740 DOI: 10.1007/s00268-007-9146-8]
P- Reviewer: Dursun P S- Editor: Gou SX L- Editor: A E- Editor: Zheng XM
Frigerio L et al . Peritoneal metastases
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.116
World J Obstet Gynecol 2013 November 10; 2(4): 116-123ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Cytoreductive surgery in primary advanced epithelial ovarian cancer
Luca Ansaloni, Federico Coccolini, Fausto Catena, Luigi Frigerio, Robert E Bristow
Luca Ansaloni, Federico Coccolini, Department of General and Emergency Surgery, Ospedali Riuniti, 24128 Bergamo, ItalyFausto Catena, Department of General and Emergency Surgery, Ospedale di Parma, 43121 Parma, ItalyLuigi Frigerio, Department of Obstetrics and Gynecology, Os-pedali Riuniti, 24128 Bergamo, ItalyRobert E Bristow, Division of Gynecologic Oncology, Depart-ment of Obstetrics and Gynecology, University of California, Irvine, CA 92868, United StatesAuthor contributions: Ansaloni L, Coccolini F and Bristow RE contributed to study conception, literature analysis, manuscript writing and editing; Catena F and Frigerio L contributed to litera-ture search and analysis.Correspondence to: Luca Ansaloni, MD, Department of Gen-eral and Emergency Surgery, Ospedali Riuniti, Largo Barozzi 1, 24128 Bergamo, Italy. [email protected]: +39-35-2699712 Fax: +39-35-266567Received: December 13, 2012 Revised: February 2, 2013Accepted: March 6, 2013Published online: November 10, 2013
AbstractEpithelial ovarian cancer is one of the most common ma-lignancy and one of the principal causes of death among gynaecological neoplasm. The majority of patients (about 70%) present with an advanced International Federa-tion of Gynaecology and Obstetrics stage disease. The current standard treatment for these patients consists of complete cytoreduction and combined systemic chemotherapy (CT). An increasing proportion of patients undergoing complete cytoreduction to no gross residual disease (RD) is associated with progressively longer overall survival. As a counterpart, some authors hy-pothesized the improving in survival could be due more to a less diffused initial disease than to an increase in surgical cytoreduction rate. Moreover the biology of the tumor plays an important role in survival benefit of sur-gery. It’s still undefined how the intrinsic features of the tumor make intra-abdominal implants easier to remove.
Adjuvant and hyperthermic intraperitoneal CT could play a decisive role in the coming years as the completeness of macroscopic disease removal increases with advances in surgical techniques and technology. The introduction of neo-adjuvant CT moreover will play a decisive role in the next years Anyway cytoreduction with no macro-scopic residual of disease should always be attempted. However the definition of RD is not universal. A unique and definitive definition is needed.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Ovarian cancer; Cytoreduction; Complete; Hy-perthermic intraperitoneal chemotherapy
Core tip: The present paper reviews the efficacy of com-plete cytoreductive surgery in the treatment of primary advanced epithelial ovarian cancer. Outlining the impor-tance for standard criteria in defining the completeness of cytoreduction. Moreover the biology of the tumor plays an important role in survival benefit of surgery. It’s still undefined how the intrinsic features of the tumor make intra-abdominal implants easier to remove. Adjuvant and hyperthermic intraperitoneal chemotherapy could play a decisive role in the coming years as the completeness of macroscopic disease removal increases with advances in surgical techniques and technology.
Ansaloni L, Coccolini F, Catena F, Frigerio L, Bristow RE. Cyto-reductive surgery in primary advanced epithelial ovarian cancer. World J Obstet Gynecol 2013; 2(4): 116-123 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/116.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.116
INTRODUCTIONApproximately 225500 women worldwide are diagnosed
116 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Ansaloni L et al . Complete cytoreduction in EOC
each year with ovarian cancer. About 140200 women die every year for this disease[1]. In the United States, ovarian cancer remains the leading cause of death among women diagnosed with gynaecological cancer[2]. The strongest predictor of mortality has been demonstrated to be the International Federation of Gynaecology and Obstetrics stage. Unfortunately the majority of patients have an ad-vanced-stage of disease at the time of diagnosis. This is strongly linked with the poor prognosis of the disease[3,4]. Moreover most of the patients with advanced-stage dis-ease will experience relapse. Even with a good response to primary treatment, only 20%-25% of women can be expected to be long-term survivors[5]. Survival rates are strongly influenced by the adjuvant chemotherapy (CT) regimen. However, primary cytoreductive surgery (CRS) to minimize the amount of residual disease (RD) is equally important. The fist description of a survival advantage associated with an ovarian tumor debulking procedure was published by Meigs in 1934[6]. A few de-cades after, the necessity of initial CRS in treatment of epithelial ovarian cancer (EOC) gained traction with the report by Griffiths[7]. Hoskins et al[8,9] reported two stud-ies of the Gynaecologic Oncology Group (GOG) (pro-tocols 52 and 97), that illustrated the key points of CRS for advanced-stage EOC: (1) the inverse relation between the maximal diameter of RD and overall survival (OS); (2) the maximal diameter of RD above which CRS has no appreciable effect on survival; and (3) introduced the concept of multi-factoriality of survival determinants. During the last 20 years, the improvements in surgical ca-pability have facilitated the achievement of maximal cyto-reduction in an increasingly higher percentage of patients with as consequence related decrease of the average of RD maximal diameters[9-20]. Similar advances in CT agents and regional delivery regimens have magnified the poten-tial survival advantage associated with a maximal surgical effort[7].
PRIMARY CRSTreatment of advanced EOC has advanced in last 10 years. The innovation of the last three decades in the surgical management of peritoneal cancer diffusion in-troduced the possibility to treat patients that were long considered untreatable. Peritoneal carcinomatosis had been considered as a metastatic inoperable grade of can-cer, before the Sugarbaker era. Actually, the universally accepted treatment diagram for advanced EOC consid-ers as key points the maximal CRS and the adjuvant CT also for grossly peritoneal diffused disease. Grade ⅢC and Ⅳ are no longer considered as “lost”. Many studies have demonstrated that a progressively more aggressive surgical effort is associated with improvements in disease-free and OS rates. It has been demonstrated the necessity to perform aggressive surgery in dedicated centres with high volume surgeons. High volume surgeons have, in fact, demonstrated to have an in-hospital mortality lower up to 69% than low volume surgeons[21]. The concept of
“population-based cytoreduction”, introduced in a meta-analysis in 2002, stimulated reflection about the necessity to aggressively treat each single case of advanced EOC to gain in survival for the whole considered population[22]. The more the surgeon became radical and increased his/her surgical volume the more he/she prolongs the disease-free and OS and reduces the in-hospital mortality. As a counterpart, some authors hypothesized the improving in survival could be due more to a less diffused initial dis-ease than to an increase in surgical cytoreduction rate[23-25]. Moreover the biology of the tumor plays an important role in survival benefit of surgery. It’s still undefined how the intrinsic features of the tumor make intra-abdominal implants easier to remove[26]. In general, upper abdominal tumor implants are suggestive of an aggressive tumor bi-ology[6]. Covens and Berman criticized the role of CRS in advanced EOC. They proposed that both survival and sur-gical resectability are mostly determined by tumor biology instead of the operative effort by the surgeon[24,27]. The retrospective review of data from the Scottish Random-ized Trial in Ovarian Cancer revealed in a population of 889 patients with disease stage ranging from IC to IV that the benefit of optimal debulking surgery seems to depend from the extent of disease before surgery[25]. The trial stratified patients into four pre-operative prognostic group depending on the staging. Survival was then analysed on the basis of the extent of CRS by stratification into three groups: No gross RD, RD ≤ 2 cm, RD ≥ 2 cm. Patients in the first two groups with a less extensive pre-operative disease benefited from CRS to RD ≤ 2 cm. Patients in the other two groups did not increase the survival with a CRS to RD ≤ 2 cm. Authors proposed to consider the tumor biology as determinant in survival and that CRS could not completely supply to the poor prog-nosis given by the intrinsic aggressiveness of some species of cell-clones.
The staging procedure could be performed by laparos-copy or via a vertical incision. An open staging procedure is the most trustworthy in order to assess the extent of disease and to evaluate the possibility to proceed with a complete cytoreductive procedure. All intra-abdominal surfaces and organs should be palpated, including the diaphragm, liver, spleen, gall bladder, small and large intestine, and mesentery. It’s important to carefully evalu-ate the retroperitoneum for bulky adenopathy. Sam-ples of the diffused cancer should be obtained, usually from involved omentum or adnexa. In the absence of gross extra-ovarian disease, multiple peritoneal biopsies should be obtained, along with a pelvic and para-aortic lymphadenectomy. In patients with early-stage ovarian cancer during the CRS phase, systematic lymphadenec-tomy should be part of the complete staging procedure. Maggioni et al[28] demonstrated as nearly 25% of patients with apparent early-stage ovarian cancer who undergo lymphadenectomy are upstaged to stage ⅢC due to the presence of node metastases. Some authors consider the role and benefit of systematic lymphadenectomy as un-clear in patients with advanced-stage EOC. Panici et al[29]
117 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

randomized 427 patients with stage Ⅲ/Ⅳ EOC to either systemic lymphadenectomy or resection of bulky nodes. The 5-year OS rate was of 48.5% and 47%, respectively with no statistical significance differences. However they reported a longer progression-free survival in the sys-temic lymphadenectomy group (31.2%), than in the no-lymphadenectomy group (21.6%). Parazzini et al[30] analys-ing 456 women with advanced stage Ⅲ/Ⅳ ovarian cancer, demonstrated no correlation between nodal status and survival. Moreover in advanced EOC nodal status was not a prognostic factor for patients undergone to optimal cy-toreduction.
Complete cytoreduction is reached when no visible tumor remains after the surgical procedure. Confusion ex-ists in defining the results of the surgical intervention in terms of RD. The term “optimal” cytoreduction has been variably defined during the years in the different stud-ies ranging from 0 to 2 cm in RD diameter. The GOG defined optimal the remaining of residual nodules of 1 cm or less[31]. Alternatively as optimal has been given the definition of no RD[31-35]. No residual tumor has also been described as complete cytoreduction[10,34]. A survey among members of the society of Gynaecologic Oncologists has been conducted. Results from this study demonstrated the heterogeneity of believing. About 12% of respondents defined no RD as optimal cytoreduction and 60.8% used the threshold of 1 cm to define the same concept[36]. Ac-tually however the most largely adopted is the GOG clas-sification which defines as optimal the RD of ≤ 1 cm.
Starting from this classification a number of prospec-tive and retrospective studies have been conducted to in-vestigate the feasibility of and the impact on survival of CRS in advanced EOC.
Generally CRS for EOC can be divided into simple and radical surgical procedures. Simple CRS consists of total abdominal hysterectomy, bilateral salpingo-oophorec-tomy, omentectomy, limited excision of pelvic/para-aortic lymph nodes, peritoneal excision, and sometimes segmen-tal bowel resection. These procedures can be performed in the majority of patients with low risk of complications. To achieve optimal cytoreduction, surgery for advanced EOC frequently requires the addition of radical proce-dures: radical oophorectomy, rectosigmoid colectomy, multiple bowel resections, diaphragm peritonectomy or re-section, liver resection, porta hepatis surgery, splenectomy, distal pancreatectomy, gastric resection, extensive nodal debulking, and intrathoracic surgery, These procedure could accomplish an higher rate of complications[7,37-68].
Since the first reports about the feasibility and the ef-ficacy of optimal CRS in advanced EOC many authors have published about the topic. Many of them, however, reported case series in which patients have not homoge-neously undergone CT or presented data without survival analysis focusing on the impact of RD. The more recent reports reach a major homogeneity from the chemothera-peutic point of view and have evaluated more extensively the impact and the extension of CRS and the RD.
Up to now, 15 studies have been published. The major-
ity of them report cases treated with the standard systemic treatment of combined platinum-taxanes CT and CRS. Only one analyzed cases treated also with intraperitoneal CT[69]. Published studies divide patients into different classes of cytoreduction. The most utilized is the three level divisions: RD 0, 0-1, > 1 cm. In few studies a sub-group division is adopted. Some authors preferred to divide patients either into RD 0, 0-0.5, 0.6-1, 1-2 and > 2 cm or into RD 0, 0-1, 1-2, > 2 cm. Lastly, one paper divides pa-tients into RD 0, 0-1, 1-5 and > 5 cm (Table 1).
This division demonstrated as no univocal evaluation of RD has been still adopted. Eisenkop et al[12] in 2003 reported a retrospective series of 408 patients with ⅢC stage EOC treated with either cisplatin/ciclophosfamide or paclitaxel/carboplatin CT and CRS. They reported an OS in the RD 0 group of 76.2 mo decreasing to 28.6 in the RD > 1. In the same year, Ozols et al[70] published a prospective analysis of 792 stage Ⅲ patients with a paclitaxel+cis-/carboplatin CT regimen divided into RD 0 and RD 0-1 which demonstrated an OS for the first group > 60 mo. OS reduced to 44 mo in the second group. In 2006 three papers have been published report-ing stage Ⅲ-ⅢC patients. Two retrospective studies from Chi et al[13] and Aletti et al[14] reported both series of patients treated with either cisplatin/ciclophosphamide or paclitaxel/cisplatin CT added to CRS. Chi et al[13] di-vided patients into subgroups which distributed the RD into subcentimeters families reporting an OS of 106 mo for the RD 0 group progressively decreasing to 34 mo for the RD > 2 cm. Aletti reported an OS > 84 mo for the RD 0 and of 16 mo for RD > 2 cm. The last 2006 publication is the prospective report from Armstrong et al[69]. They reported a series of 415 women treated with cisplatin/paclitaxel CT administered either intraperitone-ally or intravenously. For the two CT route (intraperitoneal and intravenous) groups they reported similar OS for RD 0 cm and RD 0-1 cm (78/75 mo and 127/135 mo respec-tively). Winter et al[15] and Wimberger et al[71] published another two retrospective reports. The first one reported about 861 patients with ⅡB-Ⅳ stage EOC which under-gone paclitaxel/cisplatin or ciclophosphamide/cisplatin CT and CRS, with OS for RD 0 group of > 84 mo. The second one analyzed a series of 1895 stage Ⅳ women with carbo-/cisplatin + paclitaxel CT with OS ranging from 71.9 to 35 mo for RD 0 cm and RD > 1 cm groups respectively. Salani et al[72] also reported their retrospec-tive series of 125 stage Ⅲ-Ⅳ patients tretated with cis-/carboplatin+palcitaxel CT with an OS ranging from 46.4 to 12 mo in RD 0 cm and RD > 1 cm respectively. The 2008 report by Winter et al[15] collected 360 women with stage Ⅳ EOC treated with carbo-/cisplatin+paclitaxel CT and CRS. They divided patients into groups ranging from RD 0 cm to RD > 5 cm. The OS ranges from 64.1 to 20.4 mo in the first and in the last group respectively. du Bois et al[17] and Bookman et al[73] published the two largest series of 3123 and 4312 patients respectively. du Bois et al[17] collected retrospectively patients with stage ⅡB-Ⅳ EOC who underwent carbo-/cisplatin+paclitaxel
118 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ansaloni L et al . Complete cytoreduction in EOC
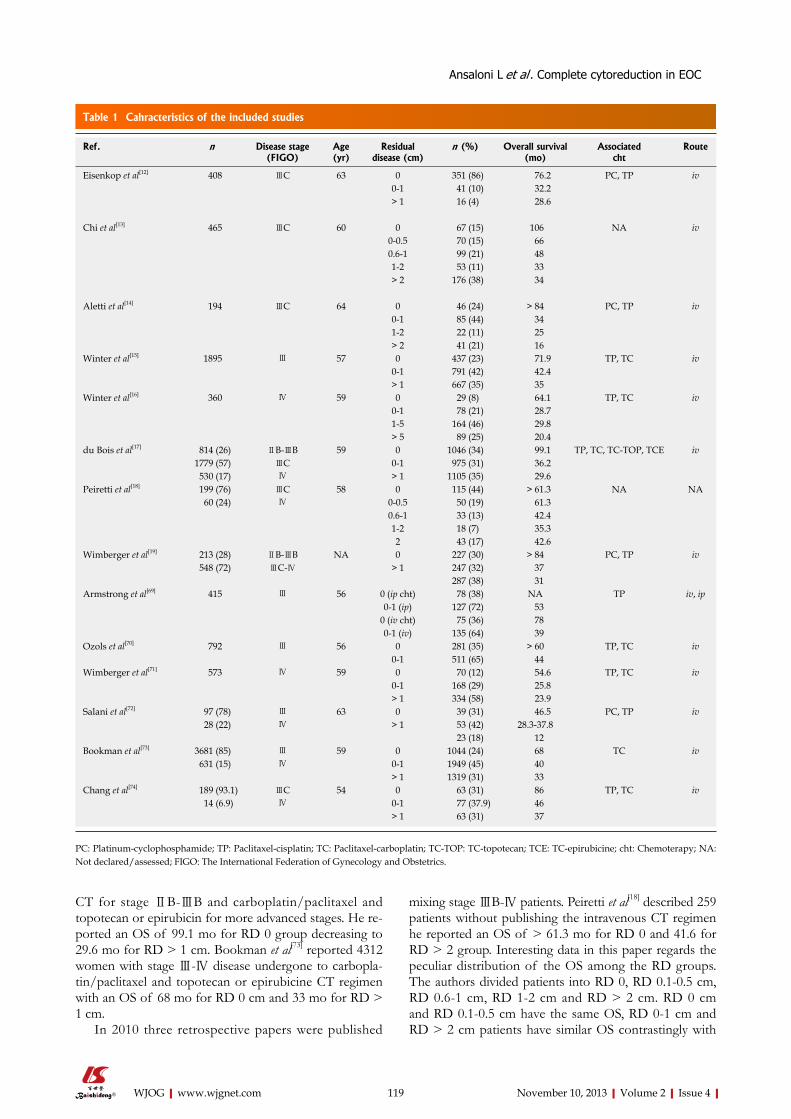
CT for stage ⅡB-ⅢB and carboplatin/paclitaxel and topotecan or epirubicin for more advanced stages. He re-ported an OS of 99.1 mo for RD 0 group decreasing to 29.6 mo for RD > 1 cm. Bookman et al[73] reported 4312 women with stage Ⅲ-Ⅳ disease undergone to carbopla-tin/paclitaxel and topotecan or epirubicine CT regimen with an OS of 68 mo for RD 0 cm and 33 mo for RD > 1 cm.
In 2010 three retrospective papers were published
mixing stage ⅢB-Ⅳ patients. Peiretti et al[18] described 259 patients without publishing the intravenous CT regimen he reported an OS of > 61.3 mo for RD 0 and 41.6 for RD > 2 group. Interesting data in this paper regards the peculiar distribution of the OS among the RD groups. The authors divided patients into RD 0, RD 0.1-0.5 cm, RD 0.6-1 cm, RD 1-2 cm and RD > 2 cm. RD 0 cm and RD 0.1-0.5 cm have the same OS, RD 0-1 cm and RD > 2 cm patients have similar OS contrastingly with
119 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Cahracteristics of the included studies
Ref. n Disease stage (FIGO)
Age (yr)
Residual disease (cm)
n (%) Overall survival (mo)
Associated cht
Route
Eisenkop et al[12] 408 ⅢC 63 0 351 (86) 76.2 PC, TP iv0-1 41 (10) 32.2> 1 16 (4) 28.6
Chi et al[13] 465 ⅢC 60 0 67 (15) 106 NA iv0-0.5 70 (15) 660.6-1 99 (21) 481-2 53 (11) 33> 2 176 (38) 34
Aletti et al[14] 194 ⅢC 64 0 46 (24) > 84 PC, TP iv0-1 85 (44) 341-2 22 (11) 25> 2 41 (21) 16
Winter et al[15] 1895 Ⅲ 57 0 437 (23) 71.9 TP, TC iv0-1 791 (42) 42.4> 1 667 (35) 35
Winter et al[16] 360 Ⅳ 59 0 29 (8) 64.1 TP, TC iv0-1 78 (21) 28.71-5 164 (46) 29.8> 5 89 (25) 20.4
du Bois et al[17] 814 (26) ⅡB-ⅢB 59 0 1046 (34) 99.1 TP, TC, TC-TOP, TCE iv1779 (57) ⅢC 0-1 975 (31) 36.2 530 (17) Ⅳ > 1 1105 (35) 29.6
Peiretti et al[18] 199 (76) ⅢC 58 0 115 (44) > 61.3 NA NA 60 (24) Ⅳ 0-0.5 50 (19) 61.3
0.6-1 33 (13) 42.41-2 18 (7) 35.32 43 (17) 42.6
Wimberger et al[19] 213 (28) ⅡB-ⅢB NA 0 227 (30) > 84 PC, TP iv 548 (72) ⅢC-Ⅳ > 1 247 (32) 37
287 (38) 31Armstrong et al[69] 415 Ⅲ 56 0 (ip cht) 78 (38) NA TP iv, ip
0-1 (ip) 127 (72) 530 (iv cht) 75 (36) 780-1 (iv) 135 (64) 39
Ozols et al[70] 792 Ⅲ 56 0 281 (35) > 60 TP, TC iv0-1 511 (65) 44
Wimberger et al[71] 573 Ⅳ 59 0 70 (12) 54.6 TP, TC iv0-1 168 (29) 25.8> 1 334 (58) 23.9
Salani et al[72] 97 (78) Ⅲ 63 0 39 (31) 46.5 PC, TP iv 28 (22) Ⅳ > 1 53 (42) 28.3-37.8
23 (18) 12Bookman et al[73] 3681 (85) Ⅲ 59 0 1044 (24) 68 TC iv
631 (15) Ⅳ 0-1 1949 (45) 40> 1 1319 (31) 33
Chang et al[74] 189 (93.1) ⅢC 54 0 63 (31) 86 TP, TC iv 14 (6.9) Ⅳ 0-1 77 (37.9) 46
> 1 63 (31) 37
PC: Platinum-cyclophosphamide; TP: Paclitaxel-cisplatin; TC: Paclitaxel-carboplatin; TC-TOP: TC-topotecan; TCE: TC-epirubicine; cht: Chemoterapy; NA: Not declared/assessed; FIGO: The International Federation of Gynecology and Obstetrics.
Ansaloni L et al . Complete cytoreduction in EOC

the OS of RD 1-2 cm group who have a 10 mo shorter OS. These data contrast with all the other studies where the OS progressively declined with the increasing of the amount of RD. Kommoss et al[20] described 287 without the intravenous CT regimen with ⅢB-Ⅳ stage disease. RD 0 cm group reached an OS of 68.8 mo and the RD > 1 cm of 18.2 mo. In 2010, Wimberger et al[19] published another retrospective trial of 573 women with stage Ⅳ disease treated with carbo-/cisplatin and paclitaxel intra-venous CT with an OS of 54.6 mo for RD 0 cm and 23.9 mo for RD > 1 cm group. The last paper about the effect of CRS in advanced EOC has been published in 2012 by Chang et al[74]. This retrospective description of 224 cases of stage ⅢC-Ⅳ patients with adjuvant platinum-paclitaxel CT with an OS of 86 mo in RD 0 cm and of 37 in RD > 1 cm group.
All the described papers demonstrated that CRS plays a pivotal role in advanced EOC treatment. The neces-sity of adjuvant CT has already been demonstrated and the necessity to reach a progressively more radical surgi-cal cytoreduction has not been contradicted in the last 30 years. Surgical effort must be absolute. The extent of cytoreduction should be extended as much as is possible. The majority of reported studies adjust data for many differently combined factors such as: ASA, performance status, ascites, histology, tumor grade, RD, operative time, diaphragm or mesentery involvement, disease site in gen-eral. Even after these adjustments, data demonstrated al-ways the same: as more the CRS is radical as more the OS is longer. The only exception to this rule derived from the study by Peiretti et al[18] in which OS rate doesn’t linearly correlate to the RD group. The correspondence between the increasing of RD and the diminishing of OS seen in all the published literature in Peiretti’s paper found a par-tial confirm.
The existing literature shows as the percentage of RD 0 procedures is absolutely different between the different centers and it doesn’t apparently depend from the number of the treated patients. The number of enrolled patients in the published studies in fact could, in our opinion, be considered as a proxy of the surgical activity of the cen-ters. In fact all the studies but three are retrospective and the evaluated periods of time are all comparable. The reported series have been all described slightly different CT regimens. Except for the Armstrong et al[69] study all the patients received intravenous CT. Observing the per-centage of RD 0 reaching it seems to not be related to the CT regimen. The same could be observed for OS. Lastly, since the first publication about the discussed topic (2003) and the last (2012), there have not been major changes in the outcome of the treatment of advanced EOC by CRS and CT. As stated before, this suggests the presence of other factors from which depend the survival outcomes. Recent studies demonstrated the possibility to apply to ovarian cancer different drugs respect to the standard platinum based CT as bevacizumab[75]. However it has to be validated on the long course. Lastly different studies have investigated the possibility to apply weekly platinum/taxanes based CT regimens[76].
One topic that has not been largely investigated by the different authors is the quality of life (QoL) in the treated patients. It is a neglected area that should be more consid-ered as a substantial part of the treatment of these wom-en. Maximizing the surgical effort to eradicate the disease necessarily conduces to more aggressive procedures with the possibility to increase the morbidity. The evaluation of the impact of such a kind of procedures on the QoL of patients will necessarily lead to exaltation of the benefits of the neo-adjuvant therapies which could potentially reduce the disease load and consequently the surgical ag-gressiveness. Moreover the evaluation of the QoL must be pivotal in treating patients with advanced EOC in situ-ations where the 5-year survival rate and so on the com-plete heal is not so relevant as the disease free survival and the quality of the gained surviving period. Introduction of neo-adjuvant CT regimen and the progressively more diffused use of hyperthermic intraperitoneal CT will play a decisive role in the next years in reaching a progressively more frequent removal of all macroscopic RD. They will also contribute to discern those factors other than CRS aggressiveness which strongly influence the survival out-comes.
CONCLUSION Authors are used to report differently the results of CRS procedures, univocal definition of CRS results is needed. In order to increase the OS complete cytoreduction (RD 0 cm) should be always attempted and the primary aim of CRS should be no macroscopic RD.
REFERENCES1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman
D. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90 [PMID: 21296855 DOI: 10.3322/caac.20107]
2 Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial dis-parities on premature cancer deaths. CA Cancer J Clin 2011; 61: 212-236 [PMID: 21685461 DOI: 10.3322/caac.20121]
3 Kim HS, Kim JW, Shouten LJ, Larsson SC, Chung HH, Kim YB, Ju W, Park NH, Song YS, Kim SC, Kang SB. Wine drink-ing and epithelial ovarian cancer risk: a meta-analysis. J Gy-necol Oncol 2010; 21: 112-118 [PMID: 20613902 DOI: 10.3802/jgo.2010.21.2.112]
4 Shih KK, Chi DS. Maximal cytoreductive effort in epithelial ovarian cancer surgery. J Gynecol Oncol 2010; 21: 75-80 [PMID: 20613895 DOI: 10.3802/jgo.2010.21.2.75]
5 Ozols RF. Treatment goals in ovarian cancer. Int J Gynecol Cancer 2005; 15 Suppl 1: 3-11 [PMID: 15839952 DOI: 10.1111/j.1525-1438.2005.15351.x]
6 Schorge JO, Garrett LA, Goodman A. Cytoreductive surgery for advanced ovarian cancer: quo vadis? Oncology (Williston Park) 2011; 25: 928-934 [PMID: 22010391]
7 Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr 1975; 42: 101-104 [PMID: 1234624]
8 Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influ-ence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 1992; 47: 159-166 [PMID: 1468693 DOI: 10.1016/0090-8258(92)90100-W]
9 Hoskins WJ, McGuire WP, Brady MF, Homesley HD,
120 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ansaloni L et al . Complete cytoreduction in EOC

Creasman WT, Berman M, Ball H, Berek JS. The effect of di-ameter of largest residual disease on survival after primary cytoreductive surgery in patients with suboptimal residual epithelial ovarian carcinoma. Am J Obstet Gynecol 1994; 170: 974-979; discussion 979-980 [PMID: 8166218]
10 Eisenkop SM, Friedman RL, Wang HJ. Complete cytoreduc-tive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: a prospective study. Gynecol Oncol 1998; 69: 103-108 [PMID: 9600815 DOI: 10.1006/gyno.1998.4955]
11 Bristow RE, Montz FJ, Lagasse LD, Leuchter RS, Karlan BY. Survival impact of surgical cytoreduction in stage IV epithe-lial ovarian cancer. Gynecol Oncol 1999; 72: 278-287 [PMID: 10053096 DOI: 10.1006/gyno.1998.5145]
12 Eisenkop SM, Spirtos NM, Friedman RL, Lin WC, Pisani AL, Perticucci S. Relative influences of tumor volume be-fore surgery and the cytoreductive outcome on survival for patients with advanced ovarian cancer: a prospective study. Gynecol Oncol 2003; 90: 390-396 [PMID: 12893206 DOI: 10.1016/S0090-8258(03)00278-6]
13 Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, Sonoda Y, Levine DA, Hensley M, Barakat RR. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol Oncol 2006; 103: 559-564 [PMID: 16714056 DOI: 10.1016/j.ygyno.2006.03.051]
14 Aletti GD, Dowdy SC, Gostout BS, Jones MB, Stanhope CR, Wilson TO, Podratz KC, Cliby WA. Aggressive surgi-cal effort and improved survival in advanced-stage ovarian cancer. Obstet Gynecol 2006; 107: 77-85 [PMID: 16394043 DOI: 10.1097/01.AOG.0000192407.04428.bb]
15 Winter WE, Maxwell GL, Tian C, Carlson JW, Ozols RF, Rose PG, Markman M, Armstrong DK, Muggia F, McGuire WP. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol 2007; 25: 3621-3627 [PMID: 17704411 DOI: 10.1200/JCO.2006.10.2517]
16 Winter WE, Maxwell GL, Tian C, Sundborg MJ, Rose GS, Rose PG, Rubin SC, Muggia F, McGuire WP. Tumor re-sidual after surgical cytoreduction in prediction of clinical outcome in stage IV epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol 2008; 26: 83-89 [PMID: 18025437 DOI: 10.1200/JCO.2007.13.1953]
17 du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekolo-gische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009; 115: 1234-1244 [PMID: 19189349 DOI: 10.1002/cncr.24149]
18 Peiretti M, Zanagnolo V, Aletti GD, Bocciolone L, Colombo N, Landoni F, Minig L, Biffi R, Radice D, Maggioni A. Role of maximal primary cytoreductive surgery in patients with advanced epithelial ovarian and tubal cancer: Surgical and oncological outcomes. Single institution experience. Gynecol Oncol 2010; 119: 259-264 [PMID: 20800269 DOI: 10.1016/j.ygyno.2010.07.032]
19 Wimberger P, Wehling M, Lehmann N, Kimmig R, Schmal-feldt B, Burges A, Harter P, Pfisterer J, du Bois A. Influence of residual tumor on outcome in ovarian cancer patients with FIGO stage IV disease: an exploratory analysis of the AGO-OVAR (Arbeitsgemeinschaft Gynaekologische Onkol-ogie Ovarian Cancer Study Group). Ann Surg Oncol 2010; 17: 1642-1648 [PMID: 20165986 DOI: 10.1245/s10434-010-0964-9]
20 Kommoss S, Rochon J, Harter P, Heitz F, Grabowski JP, Ewald-Riegler N, Haberstroh M, Neunhoeffer T, Barinoff J, Gomez R, Traut A, du Bois A. Prognostic impact of addition-al extended surgical procedures in advanced-stage primary ovarian cancer. Ann Surg Oncol 2010; 17: 279-286 [PMID:
19898901 DOI: 10.1245/s10434-009-0787-8]21 Bristow RE, Zahurak ML, Diaz-Montes TP, Giuntoli RL,
Armstrong DK. Impact of surgeon and hospital ovarian can-cer surgical case volume on in-hospital mortality and related short-term outcomes. Gynecol Oncol 2009; 115: 334-338 [PMID: 19766295 DOI: 10.1016/j.ygyno.2009.08.025]
22 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167 DOI: 10.1200/JCO.20.5.1248]
23 Covens AL. A critique of surgical cytoreduction in advanced ovarian cancer. Gynecol Oncol 2000; 78: 269-274 [PMID: 10985879 DOI: 10.1006/gyno.2000.5926]
24 Berman ML. Future directions in the surgical management of ovarian cancer. Gynecol Oncol 2003; 90: S33-S39 [PMID: 12928004 DOI: 10.1016/S0090-8258(03)00342-1]
25 Crawford SC, Vasey PA, Paul J, Hay A, Davis JA, Kaye SB. Does aggressive surgery only benefit patients with less ad-vanced ovarian cancer? Results from an international com-parison within the SCOTROC-1 Trial. J Clin Oncol 2005; 23: 8802-8811 [PMID: 16314640]
26 McCann CK, Growdon WB, Munro EG, Del Carmen MG, Boruta DM, Schorge JO, Goodman A. Prognostic significance of splenectomy as part of initial cytoreductive surgery in ovarian cancer. Ann Surg Oncol 2011; 18: 2912-2918 [PMID: 21424880 DOI: 10.1245/s10434-011-1661-z]
27 Helm CW. Current status and future directions of cytore-ductive surgery and hyperthermic intraperitoneal chemo-therapy in the treatment of ovarian cancer. Surg Oncol Clin N Am 2012; 21: 645-663 [PMID: 23021722 DOI: 10.1016/j.soc.2012.07.007]
28 Maggioni A, Benedetti Panici P, Dell’Anna T, Landoni F, Lissoni A, Pellegrino A, Rossi RS, Chiari S, Campagnutta E, Greggi S, Angioli R, Manci N, Calcagno M, Scambia G, Fos-sati R, Floriani I, Torri V, Grassi R, Mangioni C. Randomised study of systematic lymphadenectomy in patients with epi-thelial ovarian cancer macroscopically confined to the pelvis. Br J Cancer 2006; 95: 699-704 [PMID: 16940979 DOI: 10.1038/sj.bjc.6603323]
29 Panici PB, Maggioni A, Hacker N, Landoni F, Ackermann S, Campagnutta E, Tamussino K, Winter R, Pellegrino A, Greggi S, Angioli R, Manci N, Scambia G, Dell’Anna T, Fos-sati R, Floriani I, Rossi RS, Grassi R, Favalli G, Raspagliesi F, Giannarelli D, Martella L, Mangioni C. Systematic aortic and pelvic lymphadenectomy versus resection of bulky nodes only in optimally debulked advanced ovarian cancer: a randomized clinical trial. J Natl Cancer Inst 2005; 97: 560-566 [PMID: 15840878 DOI: 10.1093/jnci/dji102]
30 Parazzini F, Valsecchi G, Bolis G, Guarnerio P, Reina S, Pol-verino G, Silvestri D. Pelvic and paraortic lymph nodal status in advanced ovarian cancer and survival. Gynecol Oncol 1999; 74: 7-11 [PMID: 10385545 DOI: 10.1006/gyno.1999.5397]
31 Fader AN, Rose PG. Role of surgery in ovarian carcinoma. J Clin Oncol 2007; 25: 2873-2883 [PMID: 17617518 DOI: 10.1200/JCO.2007.11.0932]
32 Colombo N, Van Gorp T, Parma G, Amant F, Gatta G, Sessa C, Vergote I. Ovarian cancer. Crit Rev Oncol Hematol 2006; 60: 159-179 [PMID: 17018256 DOI: 10.1016/j.critrevonc.2006.03.004]
33 Vergote I, De Wever I, Tjalma W, Van Gramberen M, De-cloedt J, van Dam P. Neoadjuvant chemotherapy or primary debulking surgery in advanced ovarian carcinoma: a ret-rospective analysis of 285 patients. Gynecol Oncol 1998; 71: 431-436 [PMID: 9887245 DOI: 10.1006/gyno.1998.5213]
34 Eisenkop SM, Spirtos NM. Procedures required to accom-plish complete cytoreduction of ovarian cancer: is there a correlation with “biological aggressiveness” and survival? Gynecol Oncol 2001; 82: 435-441 [PMID: 11520137 DOI: 10.1006/gyno.2001.6313]
35 Vergote I, Trimbos BJ. Treatment of patients with early
121 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Ansaloni L et al . Complete cytoreduction in EOC

122 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
epithelial ovarian cancer. Curr Opin Oncol 2003; 15: 452-455 [PMID: 14624228 DOI: 10.1097/00001622-200311000-00008]
36 Eisenkop SM, Spirtos NM. What are the current surgical ob-jectives, strategies, and technical capabilities of gynecologic oncologists treating advanced epithelial ovarian cancer? Gy-necol Oncol 2001; 82: 489-497 [PMID: 11520145 DOI: 10.1006/gyno.2001.6312]
37 Hudson CN, Chir M. Surgical treatment of ovarian cancer. Gynecol Oncol 1973; 1: 370-378 [DOI: 10.1016/0090-8258(73)90029-2]
38 Soper JT, Couchman G, Berchuck A, Clarke-Pearson D. The role of partial sigmoid colectomy for debulking epithelial ovarian carcinoma. Gynecol Oncol 1991; 41: 239-244 [PMID: 1869102 DOI: 10.1016/0090-8258(91)90316-W]
39 Scarabelli C, Gallo A, Franceschi S, Campagnutta E, De G, Giorda G, Visentin MC, Carbone A. Primary cytoreductive surgery with rectosigmoid colon resection for patients with advanced epithelial ovarian carcinoma. Cancer 2000; 88: 389-397 [PMID: 10640973 DOI: 10.1002/(SICI)1097-0142(40000115)88:2<389::AID-CNCR21>3.0.CO;2-W]
40 Obermair A, Hagenauer S, Tamandl D, Clayton RD, Nicklin JL, Perrin LC, Ward BG, Crandon AJ. Safety and efficacy of low anterior en bloc resection as part of cytoreductive sur-gery for patients with ovarian cancer. Gynecol Oncol 2001; 83: 115-120 [PMID: 11585422 DOI: 10.1006/gyno.2001.6353]
41 Clayton RD, Obermair A, Hammond IG, Leung YC, Mc-Cartney AJ. The Western Australian experience of the use of en bloc resection of ovarian cancer with concomitant rec-tosigmoid colectomy. Gynecol Oncol 2002; 84: 53-57 [PMID: 11748976 DOI: 10.1006/gyno.2001.6469]
42 Bristow RE, del Carmen MG, Kaufman HS, Montz FJ. Radi-cal oophorectomy with primary stapled colorectal anasto-mosis for resection of locally advanced epithelial ovarian cancer. J Am Coll Surg 2003; 197: 565-574 [PMID: 14522325 DOI: 10.1016/S1072-7515(03)00478-2]
43 Mourton SM, Temple LK, Abu-Rustum NR, Gemignani ML, Sonoda Y, Bochner BH, Barakat RR, Chi DS. Morbidity of rectosigmoid resection and primary anastomosis in patients undergoing primary cytoreductive surgery for advanced ep-ithelial ovarian cancer. Gynecol Oncol 2005; 99: 608-614 [PMID: 16153697 DOI: 10.1016/j.ygyno.2005.07.112]
44 Aletti GD, Podratz KC, Jones MB, Cliby WA. Role of rec-tosigmoidectomy and stripping of pelvic peritoneum in outcomes of patients with advanced ovarian cancer. J Am Coll Surg 2006; 203: 521-526 [PMID: 17000396 DOI: 10.1016/j.jamcollsurg.2006.06.027]
45 Park JY, Seo SS, Kang S, Lee KB, Lim SY, Choi HS, Park SY. The benefits of low anterior en bloc resection as part of cytoreductive surgery for advanced primary and recur-rent epithelial ovarian cancer patients outweigh morbidity concerns. Gynecol Oncol 2006; 103: 977-984 [PMID: 16837030 DOI: 10.1016/j.ygyno.2006.06.004]
46 Houvenaeghel G, Gutowski M, Buttarelli M, Cuisenier J, Narducci F, Dalle C, Ferron G, Morice P, Meeus P, Stockle E, Bannier M, Lambaudie E, Rouanet P, Fraisse J, Leblanc E, Dauplat J, Querleu D, Martel P, Castaigne D. Modified posterior pelvic exenteration for ovarian cancer. Int J Gynecol Cancer 2009; 19: 968-973 [PMID: 19574794 DOI: 10.1111/IGC.0b013e3181a7f38b]
47 Tixier H, Fraisse J, Chauffert B, Mayer F, Causeret S, Lousta-lot C, Deville C, Bonnetain F, Sagot P, Douvier S, Cuisenier J. Evaluation of pelvic posterior exenteration in the man-agement of advanced-stage ovarian cancer. Arch Gynecol Obstet 2010; 281: 505-510 [PMID: 19847452 DOI: 10.1007/s00404-009-1175-0]
48 Gillette-Cloven N, Burger RA, Monk BJ, McMeekin DS, Vasilev S, DiSaia PJ, Kohler MF. Bowel resection at the time of primary cytoreduction for epithelial ovarian cancer. J Am Coll Surg 2001; 193: 626-632 [PMID: 11768679 DOI: 10.1016/S1072-7515(01)01090-0]
49 Hoffman MS, Griffin D, Tebes S, Cardosi RJ, Martino MA, Fiorica JV, Lockhart JL, Grendys EC. Sites of bowel resected to achieve optimal ovarian cancer cytoreduction: implica-tions regarding surgical management. Am J Obstet Gynecol 2005; 193: 582-586; discussion 586-588 [PMID: 16098902]
50 Estes JM, Leath CA, Straughn JM, Rocconi RP, Kirby TO, Huh WK, Barnes MN. Bowel resection at the time of primary debulking for epithelial ovarian carcinoma: outcomes in patients treated with platinum and taxane-based chemother-apy. J Am Coll Surg 2006; 203: 527-532 [PMID: 17000397 DOI: 10.1016/j.jamcollsurg.2006.06.019]
51 Bidzinski M, Derlatka P, Kubik P, Ziolkowska-Seta I, Dańska-Bidzinska A, Gmyrek L, Sobiczewski P, Panek G. The evaluation of intra- and postoperative complications related to debulking surgery with bowel resection in pa-tients with FIGO stage III-IV ovarian cancer. Int J Gynecol Cancer 2007; 17: 993-997 [PMID: 17367325 DOI: 10.1111/j.1525-1438.2007.00896.x]
52 Bristow RE, Peiretti M, Zanagnolo V, Salani R, Giuntoli RL, Maggioni A. Transverse colectomy in ovarian cancer surgi-cal cytoreduction: operative technique and clinical outcome. Gynecol Oncol 2008; 109: 364-369 [PMID: 18396322 DOI: 10.1016/j.ygyno.2008.02.020]
53 Silver DF, Zgheib NB. Extended left colon resections as part of complete cytoreduction for ovarian cancer: tips and considerations. Gynecol Oncol 2009; 114: 427-430 [PMID: 19555997 DOI: 10.1016/j.ygyno.2009.05.037]
54 Song YJ, Lim MC, Kang S, Seo SS, Park JW, Choi HS, Park SY. Total colectomy as part of primary cytoreductive sur-gery in advanced Müllerian cancer. Gynecol Oncol 2009; 114: 183-187 [PMID: 19427682 DOI: 10.1016/j.ygyno.2009.04.009]
55 Montz FJ, Schlaerth JB, Berek JS. Resection of diaphrag-matic peritoneum and muscle: role in cytoreductive surgery for ovarian cancer. Gynecol Oncol 1989; 35: 338-340 [PMID: 2599468 DOI: 10.1016/0090-8258(89)90074-7]
56 Silver DF. Full-thickness diaphragmatic resection with simple and secure closure to accomplish complete cytore-ductive surgery for patients with ovarian cancer. Gynecol Oncol 2004; 95: 384-387 [PMID: 15491761 DOI: 10.1016/j.ygyno.2004.07.046]
57 Cliby W, Dowdy S, Feitoza SS, Gostout BS, Podratz KC. Dia-phragm resection for ovarian cancer: technique and short-term complications. Gynecol Oncol 2004; 94: 655-660 [PMID: 15350355 DOI: 10.1016/j.ygyno.2004.04.032]
58 Chéreau E, Ballester M, Selle F, Cortez A, Pomel C, Darai E, Rouzier R. Pulmonary morbidity of diaphragmatic surgery for stage III/IV ovarian cancer. BJOG 2009; 116: 1062-1068 [PMID: 19459863 DOI: 10.1111/j.1471-0528.2009.02214.x]
59 Einenkel J, Ott R, Handzel R, Braumann UD, Horn LC. Characteristics and management of diaphragm involve-ment in patients with primary advanced-stage ovarian, fallopian tube, or peritoneal cancer. Int J Gynecol Cancer 2009; 19: 1288-1297 [PMID: 19823067 DOI: 10.1111/IGC.0b013e3181a3a833]
60 Gouy S, Chereau E, Custodio AS, Uzan C, Pautier P, Haie-Meder C, Duvillard P, Morice P. Surgical procedures and morbidities of diaphragmatic surgery in patients undergo-ing initial or interval debulking surgery for advanced-stage ovarian cancer. J Am Coll Surg 2010; 210: 509-514 [PMID: 20347745 DOI: 10.1016/j.jamcollsurg.2010.01.011]
61 Sonnendecker EW, Guidozzi F, Margolius KA. Splenectomy during primary maximal cytoreductive surgery for epithe-lial ovarian cancer. Gynecol Oncol 1989; 35: 301-306 [PMID: 2599464 DOI: 10.1016/0090-8258(89)90068-1]
62 Ayhan A, Al RA, Baykal C, Demirtas E, Ayhan A, Yüce K. The influence of splenic metastases on survival in FIGO stage IIIC epithelial ovarian cancer. Int J Gynecol Cancer 2004; 14: 51-56 [PMID: 14764029 DOI: 10.1111/j.1048-891X.2004.014940.x]
63 Yildirim Y, Sanci M. The feasibility and morbidity of distal pancreatectomy in extensive cytoreductive surgery for ad-
Ansaloni L et al . Complete cytoreduction in EOC

123 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
vanced epithelial ovarian cancer. Arch Gynecol Obstet 2005; 272: 31-34 [PMID: 15480722 DOI: 10.1007/s00404-004-0657-3]
64 Eisenkop SM, Spirtos NM, Lin WC. Splenectomy in the context of primary cytoreductive operations for advanced epithelial ovarian cancer. Gynecol Oncol 2006; 100: 344-348 [PMID: 16202446 DOI: 10.1016/j.ygyno.2005.08.036]
65 Hoffman MS, Tebes SJ, Sayer RA, Lockhart J. Extended cyto-reduction of intraabdominal metastatic ovarian cancer in the left upper quadrant utilizing en bloc resection. Am J Obstet Gynecol 2007; 197: 209.e1-209.e4; discussion 209.e4-209.e5 [PMID: 17689654]
66 Kehoe SM, Eisenhauer EL, Abu-Rustum NR, Sonoda Y, D’Angelica M, Jarnagin WR, Barakat RR, Chi DS. Incidence and management of pancreatic leaks after splenectomy with distal pancreatectomy performed during primary cytore-ductive surgery for advanced ovarian, peritoneal and fal-lopian tube cancer. Gynecol Oncol 2009; 112: 496-500 [PMID: 19091388 DOI: 10.1016/j.ygyno.2008.10.011]
67 Song YJ, Lim MC, Kang S, Seo SS, Kim SH, Han SS, Park SY. Extended cytoreduction of tumor at the porta hepatis by an interdisciplinary team approach in patients with epithelial ovarian cancer. Gynecol Oncol 2011; 121: 253-257 [PMID: 21277009 DOI: 10.1016/j.ygyno.2010.12.350]
68 Martinez A, Pomel C, Mery E, Querleu D, Gladieff L, Ferron G. Celiac lymph node resection and porta hepatis disease re-section in advanced or recurrent epithelial ovarian, fallopian tube, and primary peritoneal cancer. Gynecol Oncol 2011; 121: 258-263 [PMID: 21295334 DOI: 10.1016/j.ygyno.2010.12.328]
69 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
70 Ozols RF, Bundy BN, Greer BE, Fowler JM, Clarke-Pearson D, Burger RA, Mannel RS, DeGeest K, Hartenbach EM, Baer-gen R. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncol-ogy Group study. J Clin Oncol 2003; 21: 3194-3200 [PMID: 12860964 DOI: 10.1200/JCO.2003.02.153]
71 Wimberger P, Lehmann N, Kimmig R, Burges A, Meier W, Du Bois A. Prognostic factors for complete debulking in advanced ovarian cancer and its impact on survival. An exploratory analysis of a prospectively randomized phase III study of the Arbeitsgemeinschaft Gynaekologische Onkologie Ovarian Cancer Study Group (AGO-OVAR). Gy-necol Oncol 2007; 106: 69-74 [PMID: 17397910 DOI: 10.1016/j.ygyno.2007.02.026]
72 Salani R, Zahurak ML, Santillan A, Giuntoli RL, Bristow RE. Survival impact of multiple bowel resections in patients undergoing primary cytoreductive surgery for advanced ovarian cancer: a case-control study. Gynecol Oncol 2007; 107: 495-499 [PMID: 17854870 DOI: 10.1016/j.ygyno.2007.08.003]
73 Bookman MA, Brady MF, McGuire WP, Harper PG, Alberts DS, Friedlander M, Colombo N, Fowler JM, Argenta PA, De Geest K, Mutch DG, Burger RA, Swart AM, Trimble EL, Accario-Winslow C, Roth LM. Evaluation of new platinum-based treatment regimens in advanced-stage ovarian cancer: a Phase III Trial of the Gynecologic Cancer Intergroup. J Clin Oncol 2009; 27: 1419-1425 [PMID: 19224846 DOI: 10.1200/JCO.2008.19.1684]
74 Chang SJ, Bristow RE, Ryu HS. Impact of complete cytore-duction leaving no gross residual disease associated with radical cytoreductive surgical procedures on survival in advanced ovarian cancer. Ann Surg Oncol 2012; 19: 4059-4067 [PMID: 22766983 DOI: 10.1245/s10434-012-2446-8]
75 Stark D, Nankivell M, Pujade-Lauraine E, Kristensen G, Elit L, Stockler M, Hilpert F, Cervantes A, Brown J, Lanceley A, Velikova G, Sabate E, Pfisterer J, Carey MS, Beale P, Qian W, Swart AM, Oza A, Perren T. Standard chemotherapy with or without bevacizumab in advanced ovarian cancer: quality-of-life outcomes from the International Collaboration on Ovarian Neoplasms (ICON7) phase 3 randomised trial. Lan-cet Oncol 2013; 14: 236-243 [PMID: 23333117 DOI: 10.1016/S1470-2045(12)70567-3]
76 van der Burg ME, Boere IA, Berns PM. Dose-dense therapy is of benefit in primary treatment of ovarian cancer: contra. Ann Oncol 2011; 22 Suppl 8: viii33-viii39 [PMID: 22180397 DOI: 10.1093/annonc/mdr514]
P- Reviewers: Celik H, Zaniboni A S- Editor: Zhai HH L- Editor: A E- Editor: Zheng XM
Ansaloni L et al . Complete cytoreduction in EOC
gate the efficacy of this therapeutic approach, as well as technical details that may contribute to the standardiza-tion of the procedure and limit morbidity and mortality. In particular, new criteria are mandatory to uniformly stage the disease, to objectively evaluate the extension of cytoreduction and consequently the residual disease, to decide the best method of performing hyperthermia and to perfuse drugs. Moreover, pharmacokinetic and pharmacodynamic studies are urgently needed to as-sess the best type and dose of anticancer drugs.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Randomized trial; Ovarian cancer; Hyper-thermic intra-peritoneal chemotherapy; Hyperthermia
Core tip: Hyperthermic intra-peritoneal chemotherapy techniques are miscellaneous and not yet standard-ized. Well structured phase Ⅲ randomized trials among specialized centers are necessary to investigate the ef-ficacy of this therapeutic approach, as well as technical details that may contribute to the standardization of the procedure and limit morbidity and mortality.
Coccolini F, Ansaloni L, Corbella D, Lotti M, Glehen O. Criti-calities in randomized controlled trials on HIPEC for ovarian cancer. World J Obstet Gynecol 2013; 2(4): 124-128 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/124.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.124
INTRODUCTIONTreatment of peritoneal surface malignancies presents peculiar challenges to specialized teams who face them daily. The peritoneal spread of cancer, more than other forms of diffuse neoplastic disease, brings suffering to
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.124
World J Obstet Gynecol 2013 November 10; 2(4): 124-128ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Criticalities in randomized controlled trials on HIPEC for ovarian cancer
Federico Coccolini, Luca Ansaloni, Davide Corbella, Marco Lotti, Olivier Glehen
Federico Coccolini, Luca Ansaloni, Marco Lotti, General Sur-gery Dept., Papa Giovanni XXIII Hospital, 24128 Bergamo, ItalyDavide Corbella, Department of Anesthesiology, Papa Giovanni XXIII Hospital, 24128 Bergamo, ItalyOlivier Glehen, Department of Surgical Oncology, Centre Hos-pitalier Lyon Sud, 69495 Pierre-Bénite, FranceAuthor contributions: Coccolini F contributed to the study design, literature analysis and paper writing; Corbella D and Lotti M contributed to the literature research, literature analysis and manuscript approval; Ansaloni L and Glehen O contributed equally to the final manuscript editing and approval.Correspondence to: Federico Coccolini, MD, General Surgery Dept., Papa Giovanni XXIII Hospital, P.zza OMS 1, 24128 Ber-gamo, Italy. [email protected]: +39-35-2696464 Fax: +39-35-2674963Received: December 13, 2012 Revised: January 11, 2013Accepted: March 23, 2013Published online: November 10, 2013
AbstractSince the 1990s, many oncological surgery groups around the world started to apply hyperthermic intra-peritoneal chemotherapy (HIPEC) to the different peri-toneal spread cancers. The rationale of the application of HIPEC after surgery is to complete the cytoreductive procedure. This combined treatment has now been successfully applied to many different intra-abdominal neoplasms. However, the treatment of peritoneal sur-face malignancies and the administration of HIPEC still lack high graded evidence data, especially in ovarian cancer. Experimental data exists about every step of the treatment of peritoneal spread ovarian cancer but unfortunately they have not yet been translated into phase Ⅲ clinical randomized trials. Moreover, treatment protocols differ between different centers. A systematic review of published randomized trial protocols was per-formed. HIPEC techniques are miscellaneous and not yet standardized. Well structured phase Ⅲ randomized trials among specialized centers are needed to investi-
TOPIC HIGHLIGHT
124 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Federico Coccolini, MD, Series Editor

Coccolini F et al . Randomized trial on HIPEC
patients directly linked to the loco-regional progression. These symptoms are often strongly disabling. Innova-tive therapies are developed day by day and applied to these cohorts of patients to control and/or palliate these symptoms that are often only due to the loco-regional cancer diffusion without systemic disease. In the 1980s, Sugarbaker et al[1] from the Washington Cancer Institute started to consider peritoneal carcinomatosis from intra-abdominal neoplasms as a loco-regional disease. They promoted a loco-regional treatment combining cytore-ductive surgery (CRS) with intra-peritoneal (IP) adminis-tration of chemotherapy (CT). Adding hyperthermia to IP, CT was also investigated by Spratt et al[2] and has been successively performed and studied by many researchers and clinicians. Since the 1990s, many oncological surgery groups around the world started to apply hyperthermic intra-peritoneal chemotherapy (HIPEC) to the different peritoneal spread cancers[3]. The rationale of the applica-tion of HIPEC after CRS is to complete the cytoreduc-tion by reaching all the microscopic cancer residuals which the surgeon cannot see and consequently remove. The combined treatment of CRS and HIPEC has now been successfully applied to many different intra-abdom-inal neoplasms[4-6]. Unfortunately, the peritoneal surface malignancies and the administration of HIPEC have always been based more on common sense than on high graded evidence data. Experimental data exists about ev-ery step of the treatment of IP cancers (CT, IP CT, CRS and HIPEC) but unfortunately they have not been trans-lated into phase Ⅲ clinical randomized controlled trials (RCT) able to give high-impact results to demonstrate the real impact of HIPEC on the clinical course of IP cancers, especially of advanced epithelial ovarian cancer (EOC)[7].
RESEARCH STRATEGYA thorough literature search of MEDLINE, EMBASE, COCHRANE, ClinicalTrial.gov, WHO International Clinical Trials Registry Platform and the EU Clinical Trials Register electronic databases was performed by 2 independent reviewers (FC and DC) to identify relevant studies. Bibliography evaluation of all selected study and recent reviews was performed to identify all additional studies. The search was not limited to any time duration. Only papers written in English were considered. To en-able assimilation of all relevant published research, all search terms were expanded and all sub-categories were included. The exact syntax of search terms included ovarian neoplasms as well as randomized trial and other mesh terms.
SELECTION CRITERIAInclusion into the current systematic review was based on the following criteria for all retrieved studies: randomized trials evaluating the use of HIPEC in ovarian cancer. The purpose is to analyse discrepancies between the different
protocols by studying the same disease in terms of in-clusion/exclusion criteria, duration and kind of therapy, follow-up and primary and secondary outcomes.
IDENTIFIED STUDIESA search of the databases using the above search terms led to identification of a total of 7 papers, five published protocols and 2 proposed studies. The complete manu-scripts of all 5 published protocols were independently assessed and included in the review.
DATA EXTRACTIONInformation from the studies was extracted by 2 re-searchers (FC and DC) using the data extraction form. Disagreements about data analysis were solved by discus-sion with a third author (ML).
Seven RCTs evaluating the effectiveness of HIPEC in EOC at different time points of EOC evolution have been proposed; five are already on course (Table 1)[8-11] and two have been only proposed[12].
The first is a South Korean study (NCT01091636)[9]. It is a phase Ⅱ trial evaluating the efficacy of HIPEC in the treatment of either primary or recurrent ovarian can-cer. All patients in this trial will be scheduled to undergo CRS. After surgery, if the residual disease is less than 1 cm in the recurrent disease group, patients will always receive HIPEC. In the primary disease group, patients are randomized to receive HIPEC or not. Primary end-point is progression free survival; secondary end points are overall survival and quality of life. The sample size is 168 patients and the completion date will be December 2013. HIPEC will be performed at a mean temperature of 41.5 ℃ for 90 min with platinum at a dose of 75 mg/m2. This study enrols participants only by invitation.
The second is a study from the Netherlands (NCT00 426257)[9]. It is a phase Ⅲ trial evaluating the efficacy of HIPEC after secondary debulking surgery. The scheduled 280 patients will be randomized to receive secondary de-bulking surgery with or without HIPEC. The two criteria indicated as indication for secondary debulking are the impossibility of performing primary debulking for tumor extension or the patient’s general condition or a primary debulking procedure with a residual disease of more than 1 cm. In both cases, patients will undergo chemotherapy before the surgical procedure. Primary outcome is recur-rent free survival; secondary outcomes are toxicity, mor-bidity, quality of life, tumor response and overall survival. The finishing date will be March 2013. HIPEC will be performed with platinum at a dose of 100 mg/m2.
The last published protocol evaluating HIPEC in primary advanced EOC (NCT01628380)[8] is the CHO-RINE study. This is an Italian multicentric trial which has the peculiar characteristic of evaluating the role of HIPEC after neo-adjuvant chemotherapy. This phase Ⅲ trial is scheduled to recruit 94 patients to be random-ized into two arms. The randomization will be done after
125 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

CRS. Only patients with an optimal completeness of cytoreduction with a residual disease of a maximum of 2.5 mm will be randomized. The primary outcome will be the disease free survival and the secondary ones will be morbidity, mortality, time to chemotherapy beginning after surgery, overall survival, 1, 3, 5-year disease free survival and 1, 3, 5-year overall survival. Platinum (100 mg/m2) plus taxol (175 mg/m2) will be administered with either an open or closed technique at a temperature of 42 ℃ for 90 min for HIPEC. The scheduled finishing date will be June 2014.
Two randomized trials evaluate the efficacy in recurrent EOC. The first is the CHIPOR study (NCT01376752)[10]. This multicentric phase Ⅲ trial from France aims to study the effect of HIPEC on complete cytoreduced patients (CC-0 or CC-1 with a residual of max 0.25 cm). The ran-domization will be done after cytoreduction. If CC-0 or CC-1 criteria are reached, patients will undergo HIPEC with platinum at 75 mg/m2. Primary outcome is overall survival and the secondary outcome is relapse free survival. The scheduled number of patients is 444 and the sched-uled finishing date is April 2018.
The last registered trial is the HORSE study (NCT- 01539785)[11]. This Italian multicentric phase Ⅲ trial randomizes patients into two arms and CRS will be com-pared to CRS + HIPEC. The CRS + HIPEC arm pa-tients will be treated with platinum (75 mg/m2) at 41.5 ℃ for 60 min with a closed technique. Primary outcome is progression free interval and the secondary outcomes are overall survival, morbidity and mortality. The scheduled number of patients to be enrolled is 158 and the sched-uled finishing date is February 2015.
Lastly, two proposed trials have to be mentioned. These two proposals have been published in a letter by
Chua et al[11]. The authors proposed two trials to inves-tigate the HIPEC procedure in primary and advanced ovarian cancer, dividing patients into two arms for each study and treating them with either CRS plus HIPEC (platinum 100 mg/m2) or CRS alone. In their opinion, the CRS effort should be maximal and its aim is the absence of macroscopic residual disease.
As already stressed by other authors[12-14], the main difficulty to reach clinically relevant results in the treat-ment of EOC with HIPEC is strongly determined by the impossibility of obtaining a sufficient number of patients in a single center. In fact, in many centers, patients with peritoneal carcinomatosis are still considered as terminal and so are often not referred to the specialized surgical oncology groups to be correctly evaluated. Many clinicians are sceptical about the use of such an aggressive regimen of CRS plus HIPEC because of the potential increase in morbidity and mortality in a category of weak patients. Also, patients challenge the accrual for RCT because their referral to peritoneal surface malignancies specialized centers is mainly driven by the will to undergo CRS and HIPEC. They seldom accept to be randomized to receive HIPEC treatment or not. Lastly, the single institution is an obstacle that strongly limits the possibility of participating in a multicenter RCT. Each center in fact utilizes different procedures, surgeons operate in a different way and con-sider the completeness of cytoreduction differently at any time point[15,16], and anesthesiologists or surgeons adopt different pre- and post-operative care systems.
RCTs about HIPEC are poorly or not sponsored by pharmaceutical companies which prefer to promote tri-als where chemotherapy is administered systemically with new targeted agents[17]. Moreover, the different studies are mainly retro- or prospective phase Ⅰ and Ⅱ; insuffi-
126 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Studies included in the review
Protocol no. (Name)
Country Time point Sample size
Randomization Treatments Primary outcome
Secondary outcome
NCT01091636 South Korea Primary, recurrent OC
168 After surgery residual disease < 1 cm
CRS ± HIPEC with platinum 75 mg/m2 at 41.5 ℃ for 90 min
Progression free survival
Overall survival, quality of life
NCT00426257 The Netherlands
Secondary debulking
surgery
280 ND CRS ± HIPEC with platinum 100 mg/m2
Recurrence free survival
Toxicity, morbidity, quality of life, tumor response and overall survival
NCT01628380 (CHORINE study)
Italy Primary advanced OC after NACT
94 After surgery residual disease < 2.5 mm
CRS ± HIPEC with platinum 100 mg/m2 + taxol 175 mg/m2, at 42 ℃ for 90 min, open or closed technique
Disease free survival
Morbidity, mortality, time to chemotherapy beginning after surgery, overall survival, 1, 3, 5-yr disease free survival and 1, 3, 5-yr overall survival
NCT01376752 (CHIPOR study)
France Recurrent OC 444 After surgery residual disease < 2.5 mm
CRS ± HIPEC platinum 75 mg/m2
Overall survival Relapse free survival
NCT01539785 (HORSE study)
Italy Recurrent OC 158 ND CRS ± HIPEC platinum 75 mg/m2) at 41.5 ℃ for 60 min, closed technique
Progression free interval
Overall survival, morbidity and mortality
OC: Ovarian cancer; NACT: Neoadjuvant chemotherapy; HIPEC: Hyperthermic intraperitoneal chemotherapy; CRS: Cytoreductive surgery; ND: Not declared.
Coccolini F et al . Randomized trial on HIPEC

cient randomized phase Ⅲ trials exist. Standard treatment has to be inserted into these kinds of trials with an arm to compare, which allows discerning the real impact of HIPEC without a confounding bias. On the other hand, however, the possibility of concluding a multicentric ran-domized trial crashes against the different habits or insti-tutional lacking, which increases the difficulty of getting homogeneous proceedings in the different centers. To all these factors has to be added the lack of scientifically de-fined indications about the chemotherapy regimens. In-traperitoneal chemotherapy in fact is often administered at a “common sense dose”. Each center adopts a differ-ent dosage determined either by the patient characteris-tics or the habits or personal belief of the operators. No definitive studies exist about the drug dosages to be used intraperitoneally. No studies have in fact evaluated the optimal dose in relationship to the efficacy, tissue pen-etration and cancer penetration in big samples of popula-tion because the necessary sample size would be huge. However, we are studying the efficacy of HIPEC without knowing how its administration is done. From the sur-gical point of view, in fact, technical improvement has nearly reached its maximum. We certainly need to know if and how HIPEC allows gain in DFS or OS. However, we still do not know if and how we can gain improve-ment with chemotherapy with the commonly used drugs.
Another issue to be clarified is the duration of perfu-sion. No definitive pharmacokinetic and pharmacody-namic studies have clarified the right time, right doses or the administration interval for the different drugs. Some authors perfuse for 60 min; others for 90 min. Some ad-minister all drugs at the beginning; other fractionate the doses into 2, 3 or more administrations, in consideration of the kinetics of the molecules.
Some authors utilize the open technique; others the closed one. Experimental studies demonstrated the dif-ferent drug distribution in the different techniques. How-ever, no definitive data and consequently indication have been published.
Complications of the procedure are reported using many different reporting scales. Each scale differentiates complications in its own manner and no conclusive data could be obtained[4]. Some authors classified complica-tions and adverse events by using the Bozzetti classifica-tion[18]. Others authors have used different classification systems, such as the Clavien one or its two proposed modifications from Feldman or Elias[15]. Others have used the National Institute of Health Common Termi-nology Criteria for Adverse Events (CTCAE)[18]. These scales are not specifically designed to assess and report CRS + HIPEC complications. The 2006 peritoneal sur-face malignancies workshop (Milan, Italy) established the CTCAE as the standard system to report CRS+HIPEC complications. However, no univocal classification has been adopted yet. For this reason, no comparison be-tween the different reports could be done.
In the majority of studies dedicated to therapeutic strategy in ovarian cancer, no information is reported
regarding peritoneal disease extent as the FIGO classifica-tion is used. Stage Ⅲc includes patients with localized dis-ease and patients with extensive peritoneal carcinomatosis. When classification of the disease distribution is reported, two main grading systems are used. The Gilly classifica-tion partially considers dimension or diffusion but gives an incomplete idea of the surgical field before CRS[19]. The peritoneal cancer index (PCI) by Sugarbaker and Jac-quet precisely described dimension or distribution of the disease[20]. This allows uniform data and results. Moreover, PCI was demonstrated to have prognostic value[21,22].
The classification of the completeness of cytoreduc-tion is still controversial. Different scoring systems are used; mainly the Lyon[23] and the Sugarbaker classifica-tion[17]. The increase in DFS benefit with the increasing of the completeness of cytoreduction toward no residual disease[4,24,25] is demonstrated. The scientific community is modifying its opinion by agreeing on the meaning of complete cytoreduction as no macroscopic residual disease. However, there is no univocal opinion and con-sequently the surgical goal still has to be reached in this field.
CONCLUSIONHIPEC techniques are miscellaneous and not yet stan-dardized. Well structured phase Ⅲ randomized trials among specialized centers are necessary to investigate the efficacy of this therapeutic approach, as well as technical details that may contribute to the standardization of the procedure and limit morbidity and mortality. In particular, new criteria are mandatory to uniformly stage the disease, to objectively evaluate the extension of cytoreduction and consequently the residual disease, to decide the best method to perform hyperthermia and to perfuse drugs. Moreover pharmacokinetic and pharmacodynamic stud-ies are urgently needed to assess the best type and dose of anticancer drugs.
REFERENCES1 Sugarbaker PH, Gianola FJ, Speyer JL, Wesley R, Barofsky
I, Myers CE. Prospective randomized trial of intravenous v intraperitoneal 5-FU in patients with advanced primary colon or rectal cancer. Semin Oncol 1985; 12: 101-111 [PMID: 3901269]
2 Spratt JS, Adcock RA, Muskovin M, Sherrill W, McKeown J. Clinical delivery system for intraperitoneal hyperthermic chemotherapy. Cancer Res 1980; 40: 256-260 [PMID: 6766084]
3 Glehen O, Mohamed F, Gilly FN. Peritoneal carcinomatosis from digestive tract cancer: new management by cytoreduc-tive surgery and intraperitoneal chemohyperthermia. Lancet Oncol 2004; 5: 219-228 [PMID: 15050953]
4 Roviello F, Caruso S, Marrelli D, Pedrazzani C, Neri A, De Stefano A, Pinto E. Treatment of peritoneal carcinomatosis with cytoreductive surgery and hyperthermic intraperito-neal chemotherapy: state of the art and future developments. Surg Oncol 2011; 20: e38-e54 [PMID: 20888755 DOI: 10.1016/j.suronc.2010.09.002]
5 http://www.clinicaltrials.gov/ct2/show/record/NCT0 1376752
127 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Coccolini F et al . Randomized trial on HIPEC

6 http://www.clinicaltrials.gov/ct2/show/record/NCT0 1539785
7 Chua TC, Liauw W, Robertson G, Morris DL. Establishing evidence for change in ovarian cancer surgery--proposing clinical trials of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) in ovarian cancer peritoneal carcinomatosis. Gynecol Oncol 2009; 115: 166-168; author reply 166-168 [PMID: 19604568]
8 Bartlett DL. HIPEC: the complexities of clinical trials. Ann Surg Oncol 2008; 15: 1277-1279 [PMID: 18324445 DOI: 10.1245/s10434-007-9768-y]
9 Herzog TJ. The role of heated intraperitoneal chemother-apy (HIPEC) in ovarian cancer: hope or hoax? Ann Surg Oncol 2012; 19: 3998-4000 [PMID: 22833000 DOI: 10.1245/s10434-012-2521-1]
10 Chang SJ, Bristow RE. Evolution of surgical treatment para-digms for advanced-stage ovarian cancer: redefining ‘opti-mal’ residual disease. Gynecol Oncol 2012; 125: 483-492 [PMID: 22366151 DOI: 10.1016/j.ygyno.2012.02.024]
11 Chua TC, Liauw W, Robertson G, Chia WK, Soo KC, Alo-baid A, Al-Mohaimeed K, Morris DL. Towards randomized trials of cytoreductive surgery using peritonectomy and hyperthermic intraperitoneal chemotherapy for ovarian cancer peritoneal carcinomatosis. Gynecol Oncol 2009; 114: 137-139; author reply 139 [PMID: 19368962 DOI: 10.1016/j.ygyno.2009.03.002]
12 Younan R, Kusamura S, Baratti D, Cloutier AS, Deraco M. Morbidity, toxicity, and mortality classification systems in the local regional treatment of peritoneal surface malignan-cy. J Surg Oncol 2008; 98: 253-257 [PMID: 18726887]
13 Gilly FN, Carry PY, Sayag AC, Brachet A, Panteix G, Salle B, Bienvenu J, Burgard G, Guibert B, Banssillon V. Regional che-motherapy (with mitomycin C) and intra-operative hyper-thermia for digestive cancers with peritoneal carcinomatosis. Hepatogastroenterology 1994; 41: 124-129 [PMID: 8056398]
14 Jacquet P, Sugarbaker PH. Effects of postoperative intra-peritoneal chemotherapy on peritoneal wound healing and adhesion formation. Cancer Treat Res 1996; 82: 327-335 [PMID: 8849960]
15 Stewart JH, Shen P, Levine EA. Intraperitoneal hyperther-mic chemotherapy for peritoneal surface malignancy: cur-rent status and future directions. Ann Surg Oncol 2005; 12: 765-777 [PMID: 16132375]
16 Bakrin N, Cotte E, Golfier F, Gilly FN, Freyer G, Helm W,
Glehen O, Bereder JM. Cytoreductive surgery and hyper-thermic intraperitoneal chemotherapy (HIPEC) for persistent and recurrent advanced ovarian carcinoma: a multicentre prospective study of 246 patients. Ann Surg Oncol 2012; 19: 4052-4058 [DOI: 10.1245/s10434-012-2510-4]
17 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167]
18 Chang SJ, Bristow RE, Ryu HS. Impact of complete cytore-duction leaving no gross residual disease associated with radical cytoreductive surgical procedures on survival in advanced ovarian cancer. Ann Surg Oncol 2012; 19: 4059-4067 [PMID: 22766983]
19 Cotte E, Glehen O, Mohamed F, Lamy F, Falandry C, Gol-fier F, Gilly FN. Cytoreductive surgery and intraperitoneal chemo-hyperthermia for chemo-resistant and recurrent advanced epithelial ovarian cancer: prospective study of 81 patients. World J Surg 2007; 31: 1813-1820 [PMID: 17629740]
20 Deraco M, Virzì S, Iusco DR, Puccio F, Macrì A, Famulari C, Solazzo M, Bonomi S, Grassi A, Baratti D, Kusamura S. Sec-ondary cytoreductive surgery and hyperthermic intraperi-toneal chemotherapy for recurrent epithelial ovarian cancer: a multi-institutional study. BJOG 2012; 119: 800-809 [PMID: 22571746 DOI: 10.1111/j.1471-0528.2011.03207.x]
21 Deraco M, Kusamura S, Virzì S, Puccio F, Macrì A, Famulari C, Solazzo M, Bonomi S, Iusco DR, Baratti D. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy as upfront therapy for advanced epithelial ovarian cancer: multi-institutional phase-II trial. Gynecol Oncol 2011; 122: 215-220 [PMID: 21665254 DOI: 10.1016/j.ygyno.2011.05.004]
22 Chua TC, Robertson G, Liauw W, Farrell R, Yan TD, Morris DL. Intraoperative hyperthermic intraperitoneal chemother-apy after cytoreductive surgery in ovarian cancer peritoneal carcinomatosis: systematic review of current results. J Cancer Res Clin Oncol 2009; 135: 1637-1645 [PMID: 19701772 DOI: 10.1007/s00432-009-0667-4]
23 http://www.clinicaltrials.gov/ct2/show/record/NCT0 1628380
24 http://www.clinicaltrials.gov/ct2/show/record/NCT0 0426257
25 http://www.clinicaltrials.gov/ct2/show/record/NCT0 1091636
P- Reviewers: Inês Rosa M, Yokoyama Y S- Editor: Wen LL L- Editor: Roemmele A E- Editor: Zheng XM
128 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Coccolini F et al . Randomized trial on HIPEC
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.129
World J Obstet Gynecol 2013 November 10; 2(4): 129-136ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Anesthetic management of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy procedures
Davide Corbella, Emanuele Piraccini, Paolo Finazzi, Pietro Brambillasca, Viviana Prussiani, Massimo Ruggero Corso, Claudio Germandi, Vanni Agnoletti
Davide Corbella, Paolo Finazzi, Pietro Brambillasca, Viviana Prussiani, Department of Anesthesia, Azienda Ospedaliera Papa Giovanni XXIII, 24100 Bergamo, ItalyEmanuele Piraccini, Massimo Ruggero Corso, Vanni Agnoletti, Department of Emergency, Anesthesia Unit Morgagni-Pierantoni Hospital, 47121 Forlì, ItalyClaudio Germandi, Department of Anesthesiology, Sant’Orsola-Malpighi hospital, 40138 Bologna, ItalyAuthor contributions: Corbella D performed the bibliographic research and wrote the first version of the paper; Brambillasca P and Prussiani V revised the paper and made the preliminary bibliographic research about this topic; Finazzi P revised the pa-per and made the post-editing; Agnoletti V revised the paper and gave substantial contribution in the design and conception of the paper; Germandi C and Piraccini E revised the paper and made the preliminary bibliographic research about this topic; Corso MR revised the paper and made the post-editing; all authors read and approved the final manuscript.Correspondence to: Davide Corbella, MD, Department of Anesthesia, Azienda Ospedaliera Papa Giovanni XXIII, Piazza OMS, 1, 24100 Bergamo, Italy. [email protected]: +39-35-2675110 Fax: +39-35-2674836Received: December 13, 2012 Revised: April 17, 2013Accepted: May 18, 2013Published online: November 10, 2013
AbstractCytoreductive surgery and hyperthermic intraperitoneal chemotherapy procedure are performed with increasing frequency to treat patients with diffused peritoneal car-cinomatosis. These procedures have showed to increase life expectancy in what was previously considered a “terminal condition”. Anyway patients face major and life threatening derangements of their hemodynamic, respiratory and metabolic physiologic balance during the surgery and in the immediate postoperative period. Despite the need of an advanced organ monitoring and support all these derangements seem to be mild
and short-lived when timely addressed, at least in the majority of patients. Intensive care physicians are in-volved in providing surveillance and organ support till the patient is effectively weaned after the operation. Moreover, the anesthesiologist as perioperative physi-cian is involved in pain control, metabolic and nutritional support of this cohort of patients. This task can be chal-lenging considering that part of the patients are already on a long list of pain control medication after previous surgery or chemotherapy. A malnourished state is com-mon too and it is secondary to difficult feeding, wasting syndrome from the tumor and massive ascites. The last issue the anesthesiologists need to be aware of is the impact over the quality of life (QoL) of this procedure. The patient’s underlying pathology is unlikely to be de-finitively cured so no treatment is an acceptable choice. The possibility to withhold the treatments must be part of the consultation process like the discussion about the QoL in the immediate, as well as in the long-term, after the operation. Careful monitoring and treatment of every aspect that can impact the QoL must be taken and the efforts to be poured into an effective preserva-tion of the QoL must be doubled when compared with a patient scheduled for major abdominal surgery.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Peritoneal carcinomatosis; Anesthesia; Hy-perthermic intraperitoneal chemotherapy; Morbidity; Mortality
Core tip: The strenght of this review is to be part of an editorial project that addresses all the aspects of hyperthermic intraperitoneal chemotherapy and cytore-ductive surgery procedure. As last article of this special number it gives a comprehensive overview of the ane-stesiologic issues and an in-depth view of the perio-
129 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

perative problems and how they affect life and quality of of the patients that undergone this type of surgery. Moreover for every topic preoperative, intraoperative and postoperative considerations are provided in order to give a clear guide to the physician that approchese these patients.
Corbella D, Piraccini E, Finazzi P, Brambillasca P, Prussiani V, Corso MR, Germandi C, Agnoletti V. Anesthetic management of cytoreductive surgery and hyperthermic intraperitoneal chemo-therapy procedures. World J Obstet Gynecol 2013; 2(4): 129-136 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/129.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.129
INTRODUCTIONCytoreductive surgery (CRS) and hyperthermic intra-peritoneal chemotherapy (HIPEC) are extensive, life and quality of life (QoL) threatening procedure. All the avail-able studies covered an extremely selected population of patients usually young (less than 70 years old), without relevant comorbidity [mainly American Standards As-sociation (ASA) 1 or 2] and with a near to normal per-formance status scale (Karnofsky performance status > 80%)[1-5]. Despite this highly selected population, morbid-ity and mortality are as high as 65%[1] and 12%[6], respec-tively. Patients face major hemodynamic, respiratory and metabolic derangements during the procedure that need to be timely addressed; moreover anesthesiologists, as perioperative physicians, are committed to providing sur-veillance and organ/metabolic support in the first period after the procedure itself.
We will provide an overview of the challenges the an-esthesiologist has to face; for every issue we will provide preoperative, intraoperative and postoperative consider-ations, when appropriate.
RESPIRATORY STATUSThese patients could be pre-operatively hypoxic because of ascites, pleural effusion and atelectasis. During the HIPEC phase of the procedure there is an increase in airway pressure and a reduction in functional residual capacity. As the abdominal cavity is filled-up with the chemotherapeutic agent we observe an elevation of the diaphragm and an increase in the intra-abdominal pres-sure (IAP)[7,8]. An increased PaCO2 and a decrease in the A-a gradient and arterial pH is the hallmark of the gas exchanges deterioration. All these changes are short-lived after the HIPEC phase is terminated apart from the pH reduction, due to a persistence of the metabolic acidosis[9].
Preoperative considerationStandard evaluation with Chest X-ray and careful medi-cal history record is probably enough. However, pulmo-nary function test should be considered if a history of
Corbella D et al . Anesthetic management of CRS and HIPEC
increased bronchial reactivity is reported. Moreover due to the high incidence of hydrothorax preoperative pleu-ral effusion evacuation and Continuous Positive Airway Pressure (CPAP) periods should be considered in order to optimize pulmonary reserve before surgery.
Intraoperative considerationsAn impaired tissue oxygenation and an increase in peak airway pressures up to 30 mmHg are reported during the HIPEC phase secondary to the cranial shift of the diaphragm[4]. A lung protective strategy consisting of low tidal volume, positive end expiratory pressure and recur-rent recruitment maneuvers should be considered as the respiratory derangements are similar to those observed during long laparoscopic procedures and should be treat-ed accordingly[10]. Whenever a previous history suggestive of severe reduction of Functional Residual Capacity is reported an open abdomen technique, as the coliseum one, should be employed for its smoother impact on he-modynamic and respiratory systems[11].
Postoperative considerationsThe vast majority of patients can be extubated in the operating room at the end of surgery. Anyway, beside patients still on mechanical ventilation at the end of the procedure all the patients should be monitored post-operatively for respiratory complications. Postoperative CPAP can be extremely useful to speed up the recovery as reported by Arakelian et al[12] and should be discussed pre-operatively with the patients and planned for the first postoperative period.
HEMODYNAMIC BALANCECRS and HIPEC phase of the procedure show differ-ent hemodynamic features. During the CRS we face an extreme surface exposure, often severe bleeding, massive ascites evacuation, as in the case of ovarian tumors, and extensive tumor and peritoneal resection. Keeping normo-volemia can be difficult and fluid turnover exceeding the well-established 6-8 mL/kg per hour for major abdominal surgery[13] is often reported. About 12 mL/kg per hour is the most frequent fluid requirement observed during this procedure to keep an adequate end-organ perfusion as detected by urinary output or appropriate advanced hemo-dynamic monitoring[3,4,14,15]. HIPEC phase is characterized by two conflicting features. If hyperthermia induces a hy-perdynamic state the increased IAP, when the abdominal cavity is filled up with chemotherapeutic agent, creates a hypovolemic state due to the reduction of the venous re-turn. A plain description of the hemodynamic parameters during the HIPEC phase is: an increase in heart rate[3,15], mean central venous pressure (CVP), pulmonary artery pressure, wedge pressure[7,15], intrathoracic blood volume index[14] and cardiac index[11,15,16]; on the contrary mean arterial pressure and systemic vascular resistance showed a trend, if not a statistically significant, reduction over the baseline[9,14]. An increase in end tidal CO2
[3] and an increase
130 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

in oxygen extraction and consumption rate are the signs of the hypermetabolic state that is due to the hyperthermia[17]. All these changes are constantly reported to be short-lived after the completion of the HIPEC phase and the vast majority of patients, if not all, were weaned off from he-modynamic support at discharge from the operating room, if ever supported with an amine infusion. Moreover the hemodynamic derangements can be reduced if: an open abdomen technique is employed and the core tempera-ture is kept as close to normal as possible. Esquivel et al[11] reported only a statistically significant increase in cardiac output during the HIPEC phase when the “Coliseum Technique” was used while the increase in heart rate, mean CVP and the decrease in systemic vascular and mean arte-rial pressure were not a statistically, and clinically, significant trend. The earliest report from Shime et al[17] in 1994 on the effect of the hyperthermia on the hemodynamic bal-ance showed remarkable changes with a reduction in mean arterial pressure and systemic vascular resistance from 93.8 to 75.5 mmHg and from 2214 to 1239 dynes × s/min5
× m2, respectively, and an increase in cardiac index and wedge pressure from 3.4 to 4.6 mL/min per square meter and from 7.5 to 9.6 mmHg, respectively. Those changes were paired with a core temperature that approached 40 ℃ at the end of the perfusion whereas in more recent studies the core temperature never outreached 38 ℃[3,9]. This proportionally direct effect of temperature over the hyperdynamic state of the patient is well known. Several studies conducted during the procedures of whole-body hyperthermia showed how when the core temperature gets warmer the hyperdynamic state gets worst[18].
Preoperative considerations No study specifically targets the cohort of patients with heart failure. To this day, in the large RCTs published pa-tients with an uncontrolled cardiac disease were excluded as no patient with ASA higher than 3 was considered eli-gible[3,12]. A thorough cardiac evaluation (echocardiogram, stress test if there’s suspected reduced coronary reserve) can be a prudent approach if a history of previous heart failure or reduced physical activity is reported. In this case the patients should be referred to the cardiologist for evaluation and risk stratification. Beside this we consider it sensible to refer every patients to a cardiologist if he/she had a possible cardiotoxicity from previous chemotherapy and/or he/she developed a fast malnourishment state. Indication for HIPEC should be questioned whenever an uncontrolled cardiac disease is detected and eventually the patients should be considered for palliative care only.
Intraoperative considerations All the hemodynamic changes are constantly reported to be short lived after surgery. Despite this, major fluid shift and amine support are constantly reported too. All the available case series used at least as hemodynamic monitor: hourly urinary output, CVP and an invasive arterial line[3,9] whereas others used invasive, or advanced, monitoring such as pulmonary artery catheter[7,15,17], con-
tinuous esophageal echo-Doppler monitoring[8,11,16] or transthoracic thermodilution technique[14] (Picco; Pulsion Medical System, Munich, Germany). In our institution invasive monitoring is usually considered mandatory just for patients with a known reduced cardiac performance. Anyway some minimally invasive devices as Vigileo/flo-Trac, Pulsion Picco, trans-esophageal echocardiography can be extremely helpful in guiding transfusion and fluid turn-over therapy. Several authors[11,16,19] argued that CVP is unreliable due to the increased IAP and table tilting during the HIPEC phase. Moreover the urinary output can be reduced secondary to toxicity of chemotherapeu-tic agent or to the increased IAP itself. In this scenario the possibility to evaluate in a real time manner dynamic parameters of cardiac preload and fluid responsiveness is of utmost importance in order to reduce the risk “flood or dry” the patient and to ensure an appropriate end-organ perfusion. Beside fluid therapy amine support is an open issue during the procedure. No standardized protocol to face cardiac failure is reported and the amine used is related to the local policies of the different insti-tutions. Low doses dopamine were employed by Cafiero et al[16] and by Miao et al[9] to prevent renal dysfunction as a “renal dose” of dopamine is reported to increase renal perfusion during laparoscopic procedures[20]. Anyway dopamine seems to have little effect, if at all, because none of the studies where it was not employed showed an increased rate of renal failure.
Postoperative considerationsHemodynamic unbalances are usually short lived. Anyway Cooksley et al[8] reported that a 26% of the patients were still on vasopressor at the end of the procedure and at the arrival in intensive care unit (ICU), even if no patients developed renal failure or had a difficult weaning from hemodynamic support. Moreover fluid requirement can be difficult to anticipate as massive fluid loss through the drainages, up to 4 L a day[4], are reported. Careful fluid turn-over substitution and timely weaning from vasopres-sor support advocate for an intensive, or at least interme-diate, care to deliver adequate post-operative surveillance so to prevent renal dysfunction and decreased end-organ perfusion.
PAIN CONTROL The elective pain control modality in the vast majority of the centers is thoracic epidural[3,4,8,9,14,17,19]. Massive surface scarring is enough to justify the high level of pain report-ed and the longer use of advanced and invasive modality of pain control. For example, the cohort of patients from Schmidt et al[3] had a median of 7 d of continuous infu-sion of local anesthetic and opioids via the epidural route, which is much longer than the usual 3/4 d after major abdominal surgery.
Preoperative considerationsIt is important to notice that the patients scheduled
131 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Corbella D et al . Anesthetic management of CRS and HIPEC

for CRS and HIPEC procedure had a long, and often troubled, medical history. Some of them are already on a long list of analgesic medications and some others show features of chronic and neuropathic pain after the chemotherapy. No study specifically addresses this issue as chronic pain facilities are extremely heterogeneous around the world and the patients themselves undergo surgery with a different diagnosis of disease and had more or less invasive procedures and different chemo-therapeutic regimen. However a consult with the pallia-tive care/chronic pain physician can be useful in order to plan a follow-up of the patients when they’re discharged from the hospital. Thoracic epidural is probably the best option to control pain perioperatively. It is associ-ated with a shorter mechanical ventilation period, from 10 to 3 h[3], and a better patient satisfaction[21]. Anyway these patients seem to be efficiently and safely managed perioperatively even with high level of intravenous opi-oids. A percentage of patients ranging from 38%[3] and 21%[9] had no epidural catheter and they did not show a significant increase in perioperative complications, if we exclude a longer period on mechanical ventilation and ICU admission. Coagulation unbalances are common in these patients as they develop massive ascites or have a long-standing history of bleeding or malnourishment. However, it does not seem to affect the safety of the placement of a thoracic epidural catheter as no epidural hematoma is reported[22]. Risk benefit ratio is probably in favor of thoracic epidural considering the difficulty to control pain and wean from mechanical ventilation that these patients have.
Intraoperative considerations A continuous infusion of local anesthetic and/or opioids through the epidural route is felt unsafe by several au-thors[9,23-25] because of its high potential to worsen hypoten-sive episodes due to its synergic effect with hyperthermia in reducing the systemic vascular resistances and because of the sympathetic blockade epidural analgesia produces. Any-way Schmidt et al[3] found no detrimental effect using epidu-ral analgesia during the procedure. We can speculate wheth-er there’s any potential advantage in using epidural analgesia in the prevention of the development of chronic postop-erative pain in a similar manner to its use during thoracic surgery[26]. Beside this there’s an increasing amount of data that suggest how the use of epidural analgesia may improve patients survival rate by decreasing the incidence of tumor relapse or at least elongating the time to relapse of the tu-mor. de Oliveira et al[27] found a significantly longer time to cancer recurrence in the patients that had thoracic epidural working during the procedure of CRS, but not HIPEC, (73 mo vs 38 mo in the control group) in a cohort of patients affected by ovarian cancer. On the contrary, time for can-cer recurrence was not different between the patients that never had thoracic epidural or had it just as postoperative pain relief technique. This possible positive effect can be secondary to the increased function of nartural killer cells when the surgical stress response is reduced[28,29] and high level of intravenous opioids is avoided[30].
Postoperative considerations Postoperatively all the usual precautions and the usual surveillance should be taken. In case of the development of chronic pain the patients should be referred to a pal-liative care center or to a chronic pain clinic.
COAGULATION CONSIDERATIONSCoagulation abnormalities are always reported in this cohort of patients. They are defined as an abnormal elon-gation of prothrombin time - international normalised ratio (INR), activated partial thromboplastin time (aPTT) and/or pathological reduction of platelets count over the baseline[3,4,8,9]. This dysfunction is reported to peak around 24/48 h post-surgery[3,8], with a restoration of a normal coagulation profile in 72 h[3], even if baseline values are reached in almost 5 d[9]. Schmidt et al[3] reported that Fresh Frozen Plasma (FFP) and packed red blood cells (PRBC) were transfused in 50% of the patients intra-operatively and 28% post-operatively. Coagulation abnormality is, probably, multifactorial in its genesis. The two sides of the problems seem to be a dilutional dysfunction[31] secondary to massive fluid shift and bleeding and an impairment of coagulation factors profiles due to massive ascites[32] and malnourishment.
Preoperative considerationsStandard coagulation evaluation (INR, aPTT, platelets count, list of antithrombotic drugs) is enough and no author advocates for more expensive tests. The fear of intraoperative bleeding should not prevent us from con-sidering the high thrombotic risk that some patients may have. Some of them are women, in their fifties, with an ovarian cancer, that are going to keep for 8-10 h a gyneco-logical position on the operating table. All of these are well known prothrombotic risk factors. Special care is required by patients with massive ascites. Ascitic fluid is rich in pro-teins with a varying concentration of 0.5-4.2 g/100 mL of proteins. Of this amount 50%-70% is albumin, 30%-45% are globulins and 0.3%-4.5% is fibrinogen. The evacua-tion of up to 2-3 L of this fluid changes something more than the oncotic pressure of the patient. Vorgias et al[32] calculated the theoretical substitution requirement of pa-tients optimally debulked from ovarian cancer and found out that infusions for up to 3 d of 2 units of FFP and hu-man albumin were required.
Intraoperative considerationsCoagulation during CRS and HIPEC procedure means to deal in a short period of time with: dilution coagulopathy due to large amount of crystalloids and/or colloids infu-sion; transfusion coagulopathy due to PRBC transfusion to keep an adequate oxygen delivery, in the scenario of massive bleeding; and long-standing coagulation abnor-malities due to dysproteinemia secondary to malnourish-ment and ascites evacuation. This scenario complicates the understanding of normal coagulation tests such as INR, aPTT and platelet counts. Thromboelastography (TEG) gives the possibility of a thorough evaluation of
132 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Corbella D et al . Anesthetic management of CRS and HIPEC

the coagulation profile and it is probably more useful in this type of surgery than in others. Even if no paper spe-cifically addresses this question TEG-guided transfusion of blood products may substantially reduce bleeding and eventually blood-products requirements similarly to what happens in other major surgeries[33].
Postoperative considerationsThe coagulation profile takes at least 5 d[9] to get back to baseline values so surveillance and timely transfusion is needed. Renal status, electrolyte balance, glycemic and temperature control: renal dysfunction, electrolyte dis-order and hyperglycemia are frequently observed[3,7,9,34]. They are related to the fluids infused, end-organ perfu-sion achieved and quality and quantity of perfusate used to deliver the chemotherapeutic agent in the abdominal cavity. Temperature control is of utmost importance as it is directly related to the gravity of deregulation in the hemodynamic and coagulation balance.
RENAL STATUS, TEMPERATURE AND METABOLISMStandard evaluation: If ureteral stents are positioned pre-operatively to be used as landmark during CRS phase it should be advisable to check for their bilateral patency.
Intraoperative considerationsCalcium, potassium, sodium are routinely checked. Minor electrolyte such as magnesium should be tested too as their unbalance is reported[9]. The use of furosemide to enhance urine output to clear as much chemotherapeutic agent as possible is frequently reported[9,14,16]. Forced diure-sis by the use of high dose loop-diuretics is still considered “standard of care” during chemotherapy with compound derived from platinum. Despite this “standard practice” there is no definitive evidence of renal protection by the use of high dose of loop-diuretics, as stated by the Special Interest Group on Cancer Care of the European Society of Clinical Pharmacology[35]. They recommended a “brisk diuresis” during the platinum compound infusion and in the immediate days after by a prolonged saline infusion. In our case series of CRS and HIPEC we had three renal in-sufficiencies in 70 cases during the last year, two of them were obstructive, none of them required dialysis (unpub-lished data). This small incidence of renal impairment was probably related to the invasive monitoring of euvolemia during the procedure despite a diuretic use (20 mg of furosemide before HIPEC induction). In our opinion diuretics use has still a place in the “standard of care” of these patients as hypovolemia can be easily detected and corrected if invasive monitoring is ensued and there is no clear evidence “against” the use of loop-diretics. Drug clearance is mainly linked to renal blood flow and not to plain urine output. the prolonged use of diuretics can be misleading as we can face a good urinary output in the presence of an unnoticed end-organ perfusion decrease therefore euvolemia must be pursued with any effort. De Somer et al[34] reported hyperglycemia and hyponatremia
when a perfusate of 5% dextrose was used as a carrier for oxplatin. This paper points out the need for the anesthe-siologist to know the composition of the perfusate and to prevent possible electrolyte unbalances due to the abdomi-nal perfusion itself. Even if the peritoneal surface is re-duced the exposed area is still enough to give a statistically, and clinically, relevant impact over the electrolytes and fluid balance. Temperature control devices and strategies need to match the different requirements during the CRS and HIPEC phase of the procedure. During the cytore-duction when the abdominal cavity is open there is an in-tense warm loss and hypothermia must be prevented using all the warming devices available (i.e., forced air warming, warmed infusions, arm blankets). On the contrary patients must be cooled down during the HIPEC phase when the warm infusate is delivered into the abdominal cavity. Cold fluids, ice packs, cooling mattress[14,16,17] have been used to cool the patients during the HIPEC procedure. Sometimes those devices were used to lower the core temperature be-fore the abdominal cavity filling[7,9].
Postoperative considerationNone of these disturbances is reported to be long lasting after the completion of the procedure so just standard care is needed.
QoLCRS and HIPEC represent a radical treatment in a patient that has little possibility, if any, to be definitively cured. Data from the literature suggest that patients that under-stand their “terminal state” are likely not to wish to submit themselves to extensive, life and QoL threatening proce-dures[36]. In this scenario no treatment, obviously exclud-ing palliative and supportive care, is an acceptable choice and a careful counseling between physician and patient is mandatory. Anyway patients that are referred to a center that performs CRS and HIPEC are usually aware that the procedure will gain time for them, or at least for the ma-jority of them. Moreover McQuellon et al[37] eported that no patient in the cohort of long-term survivor regretted having undergone the procedure. Although perioperative mortality and morbidity can be high[1,6], median survival improves significantly and for colorectal cancer a survival rate of 30% at 5-year is reported[38,39]. The quality of the life gained with this procedure has been evaluated in sev-eral papers[37,40-44]. Regardless of the cohort of patients analyzed, or the scores used to describe the QoL, all the papers reported - after a drop in quality and physical func-tioning in the first few months following the procedure - a steady increase that reached baseline[4,5,42] or overshot it as in the case of patients with ovarian cancer and massive ascites[39]. McQuellon et al[37] published the only report on long-term survivors after HIPEC and CRS. They showed as 87% of the patients that survived longer than 3 years rated their health as good or excellent and none of them regretted having undergone the procedure. To interpret data from QoL studies on HIPEC patients mean to deal with at least three main problems. The first one is the non
133 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Corbella D et al . Anesthetic management of CRS and HIPEC

standardized use of score across the studies as already re-ported by Piso et al[43]. Secondarily it is extremely compli-cated to interpret data from QoL studies as, especially in a cohort of patients with a terminal disease, factors as ad-aptation to disease, response shift, dispositional optimism can deeply change some of the scoring and maybe have little effect over the life of the patients[41,45]. The typical effect is that little improvement in QoL may be not sig-nificant at a population level but, at the patient level, it can be important enough to enter or not a rehabilitation or supportive care program. Thirdly a significant proportion of the patients do not reply to the follow-up since some of them die or their conditions are so deteriorated that they cannot reply to the questionnaires. McQuellon et al[40] evaluated the QoL data of patients starting with a cohort of 64 patients at baseline but only 23 patients replied to the 1-year follow-up questionnaire. Another study[42] evaluated 96 patients at baseline but only 24 were able to complete the 1-year follow-up, similarly Schmidt et al[4], with a baseline cohort of 67 patients and a 25 patients at the time of the follow-up. Even though it is possible to consider and weigh during the analysis the effect of miss-ing data and of the non-random distribution of the results we need to focus keep in mind that probably the data just reflect the best possible outcome of this surgery and that a real “average effect” it does not exist.
POSTOPERATIVE CAREThe procedure is long and complex and even though the physiological derangements are predominately short-lived these patients deserve an intense postoperative monitor-ing. Postoperative respiratory support is not always neces-sary even if CPAP periods can be useful to get back to baseline respiratory function levels[12]. Cooksley et al[8] re-ported to have extubated all the patients in the OR before discharging them to the Critical Care Unit, whereas Miao et al[9] extubated 62% before PACU admission. Interesting-ly Schmidt et al[3] observed how the presence of a work-ing epidural analgesia was significantly associated with a reduction in the mechanical ventilation period (3.1 h vs 10.3 h, respectively) and in an higher proportion of patients extubated in the operating room (41% vs 14%, respectively). From an hemodynamic point of view these patients are rarely on amine support but suffer from high volume of fluids loss from the drains, up to 4 L a day[3], secondary to the huge wounded surface. Even if the postoperative period is less troubled than the surgery one these patients needs to be monitored for a while and all the derangements eventually corrected in a timely man-ner. No study specifically addresses the right place to be discharged after the OR or the right period of critical care monitoring. Anyway we agree with the statement by Cooksley et al[8], that a shorter hospital length of stay is probably due to admission, and prolonged observation period, in a critical care unit.
NUTRITIONAL SUPPORTNo author addressed the specific topics of the nutritional
and metabolic support in the patients undergoing CRS and HIPEC. This category of patient is known to have a poor nutritional baseline as malnutrition prevalence is reported to be as high as 67%[46] in ovarian cancer patients and 54%[47] and 83%[48] in colorectal and gastric cancer, respectively. Moreover the debulking phase of the surgery involves massive resections that are likely to cause a deep catabolic and pro-inflammatory state. All malnourished patients should have a nutritional consultation before surgery and should start a nutritional support to reach a better metabolic profile[49] before surgery. Although little is known about the effect on small bowel physiology of the hyperthermic intrabdominal chemotherapy, it is advis-able that these patients should be treated according to the guidelines about perioperative nutritional support after major surgery[50]. So nutritional states must be assessed preoperatively and enteral feeding started as soon as pos-sible after the resolution of mechanical bowel obstruction. Positioning a nasojejunal catheter can be a valuable option to start early enteral feeding as already reported in this group of patients[8]. This area of research is of increasing interest due to the fact that starvation, or better malnour-ishment, has been identified as a major determinant of surgery success and QoL recovery.
CONCLUSIONCRS and HIEPC are complex procedures. High morbid-ity and mortality rates are reported, nonetheless it has showed its power to gain life in a relevant part of the patients and its safety in high volume centers. Respiratory and hemodynamic derangements were the first ones to be extensively evaluated. Morbidity related to these two systems failure is decreasing since pathophysiology of hyperthermia is better understood and better tempera-ture, hemodynamic and respiratory control is achieved through new devices or technique. The research agenda of this procedure is an open challenge and the issue to be addressed in the next future are how to increase QoL of the patients through a better understanding of the coagu-lation derangement, and issues concerning pain patterns, nutritional support and social rehabilitation.
REFERENCES1 Verwaal VJ, van Ruth S, de Bree E, van Sloothen GW, van
Tinteren H, Boot H, Zoetmulder FA. Randomized trial of cy-toreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal can-cer. J Clin Oncol 2003; 21: 3737-3743 [PMID: 14551293 DOI: 10.1200/JCO.2003.04.187]
2 Yan TD, Links M, Xu ZY, Kam PC, Glenn D, Morris DL. Cy-toreductive surgery and perioperative intraperitoneal che-motherapy for pseudomyxoma peritonei from appendiceal mucinous neoplasms. Br J Surg 2006; 93: 1270-1276 [PMID: 16838392 DOI: 10.1002/bjs.5427]
3 Schmidt C, Creutzenberg M, Piso P, Hobbhahn J, Bucher M. Peri-operative anaesthetic management of cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Anaesthesia 2008; 63: 389-395 [PMID: 18336490 DOI: 10.1111/j.1365-2044.2007.05380.x]
134 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Corbella D et al . Anesthetic management of CRS and HIPEC

135 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
4 Schmidt U, Dahlke MH, Klempnauer J, Schlitt HJ, Piso P. Perioperative morbidity and quality of life in long-term sur-vivors following cytoreductive surgery and hyperthermic in-traperitoneal chemotherapy. Eur J Surg Oncol 2005; 31: 53-58 [PMID: 15642426]
5 Tuttle TM, Zhang Y, Greeno E, Knutsen A. Toxicity and quality of life after cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol 2006; 13: 1627-1632 [PMID: 17013686 DOI: 10.1245/s10434-006-9186-6]
6 Shen P, Hawksworth J, Lovato J, Loggie BW, Geisinger KR, Fleming RA, Levine EA. Cytoreductive surgery and intra-peritoneal hyperthermic chemotherapy with mitomycin C for peritoneal carcinomatosis from nonappendiceal colorec-tal carcinoma. Ann Surg Oncol 2004; 11: 178-186 [PMID: 14761921]
7 Kanakoudis F, Petrou A, Michaloudis D, Chortaria G, Kon-stantinidou A. Anaesthesia for intra-peritoneal perfusion of hyperthermic chemotherapy. Haemodynamic changes, oxygen consumption and delivery. Anaesthesia 1996; 51: 1033-1036 [PMID: 8943594 DOI: 10.1111/j.1365-2044.1996.tb14998.x]
8 Cooksley TJ, Haji-Michael P. Post-operative critical care management of patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy (HIPEC). World J Surg Oncol 2011; 9: 169 [PMID: 22182345 DOI: 10.1186/1477- 7819-9-169]
9 Miao N, Pingpank JF, Alexander HR, Royal R, Steinberg SM, Quezado MM, Beresnev T, Quezado ZM. Cytoreductive surgery and continuous hyperthermic peritoneal perfusion in patients with mesothelioma and peritoneal carcinomato-sis: hemodynamic, metabolic, and anesthetic considerations. Ann Surg Oncol 2009; 16: 334-344 [PMID: 19050961 DOI: 10.1245/s10434-008-0253-z]
10 Valenza F, Chevallard G, Fossali T, Salice V, Pizzocri M, Gattinoni L. Management of mechanical ventilation during laparoscopic surgery. Best Pract Res Clin Anaesthesiol 2010; 24: 227-241 [PMID: 20608559]
11 Esquivel J, Angulo F, Bland RK, Stephens AD, Sugarbaker PH. Hemodynamic and cardiac function parameters during heated intraoperative intraperitoneal chemotherapy using the open “coliseum technique”. Ann Surg Oncol 2000; 7: 296-300 [PMID: 10819370]
12 Arakelian E, Gunningberg L, Larsson J, Norlén K, Mahteme H. Factors influencing early postoperative recovery after cy-toreductive surgery and hyperthermic intraperitoneal chemo-therapy. Eur J Surg Oncol 2011; 37: 897-903 [PMID: 21783337]
13 Joshi GP. Intraoperative fluid restriction improves out-come after major elective gastrointestinal surgery. Anesth Analg 2005; 101: 601-605 [PMID: 16037184 DOI: 10.1213/01.ANE.0000159171.26521.31]
14 Raue W, Tsilimparis N, Bloch A, Menenakos C, Hartmann J. Volume therapy and cardiocircular function during hyper-thermic intraperitoneal chemotherapy. Eur Surg Res 2009; 43: 365-372 [PMID: 19844110 DOI: 10.1159/000248164]
15 Tsiftsis D, de Bree E, Romanos J, Petrou A, Sanidas E, Ask-oxylakis J, Zervos K, Michaloudis D. Peritoneal expansion by artificially produced ascites during perfusion chemo-therapy. Arch Surg 1999; 134: 545-549; discussion 550 [PMID: 10323428]
16 Cafiero T, Di Iorio C, Di Minno RM, Sivolella G, Confuorto G. Non-invasive cardiac monitoring by aortic blood flow de-termination in patients undergoing hyperthermic intraperi-toneal intraoperative chemotherapy. Minerva Anestesiol 2006; 72: 207-215 [PMID: 16570032]
17 Shime N, Lee M, Hatanaka T. Cardiovascular changes dur-ing continuous hyperthermic peritoneal perfusion. Anesth Analg 1994; 78: 938-942 [PMID: 8160994]
18 Deja M, Hildebrandt B, Ahlers O, Riess H, Wust P, Gerlach H, Kerner T. Goal-directed therapy of cardiac preload in induced whole-body hyperthermia. Chest 2005; 128: 580-586
[PMID: 16100141 DOI: 10.1378/chest.128.2.580]19 Raspe C, Piso P, Wiesenack C, Bucher M. Anesthetic man-
agement in patients undergoing hyperthermic chemothera-py. Curr Opin Anaesthesiol 2012; 25: 348-355 [PMID: 22517311 DOI: 10.1097/ACO.0b013e32835347b2]
20 Pérez J, Taurá P, Rueda J, Balust J, Anglada T, Beltran J, Lacy AM, Garcia-Valdecasas JC. Role of dopamine in renal dys-function during laparoscopic surgery. Surg Endosc 2002; 16: 1297-1301 [PMID: 12000983 DOI: 10.1007/s00464-001-9201-8]
21 Ali M, Winter DC, Hanly AM, O’Hagan C, Keaveny J, Broe P. Prospective, randomized, controlled trial of thoracic epidural or patient-controlled opiate analgesia on perioperative qual-ity of life. Br J Anaesth 2010; 104: 292-297 [PMID: 20124282 DOI: 10.1093/bja/aeq006]
22 Schmidt C, Steinke T, Moritz S, Bucher M. Thoracic epidu-ral anesthesia in patients with cytoreductive surgery and HIPEC. J Surg Oncol 2010; 102: 545-546 [PMID: 20607760 DOI: 10.1002/jso.21660]
23 de la Chapelle A, Pérus O, Soubielle J, Raucoules-Aimé M, Bernard JL, Bereder JM. High potential for epidural analge-sia neuraxial block-associated hypotension in conjunction with heated intraoperative intraperitoneal chemotherapy. Reg Anesth Pain Med 2005; 30: 313-314 [PMID: 15898044]
24 Desgranges FP, Steghens A, Rosay H, Méeus P, Stoian A, Daunizeau AL, Pouderoux-Martin S, Piriou V. [Epidural an-algesia for surgical treatment of peritoneal carcinomatosis: a risky technique?]. Ann Fr Anesth Reanim 2012; 31: 53-59 [PMID: 22154448 DOI: 10.1016/j.annfar.2011.08.020]
25 Desgranges FP, Steghens A, Mithieux F, Rosay H. Potential risks of thoracic epidural analgesia in hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2010; 101: 442 [PMID: 20213731 DOI: 10.1002/jso.21485]
26 Sentürk M, Ozcan PE, Talu GK, Kiyan E, Camci E, Ozyalçin S, Dilege S, Pembeci K. The effects of three different analge-sia techniques on long-term postthoracotomy pain. Anesth Analg 2002; 94: 11-15, table of contents [PMID: 11772793]
27 de Oliveira GS, Ahmad S, Schink JC, Singh DK, Fitzgerald PC, McCarthy RJ. Intraoperative neuraxial anesthesia but not postoperative neuraxial analgesia is associated with increased relapse-free survival in ovarian cancer patients after primary cytoreductive surgery. Reg Anesth Pain Med 2011; 36: 271-277 [PMID: 21519312 DOI: 10.1097/AAP.0b013e318217aada]
28 Pollock RE, Babcock GF, Romsdahl MM, Nishioka K. Surgi-cal stress-mediated suppression of murine natural killer cell cytotoxicity. Cancer Res 1984; 44: 3888-3891 [PMID: 6744305]
29 Pollock RE, Lotzová E, Stanford SD. Surgical stress impairs natural killer cell programming of tumor for lysis in patients with sarcomas and other solid tumors. Cancer 1992; 70: 2192-2202 [PMID: 1394051]
30 Yeager MP, Colacchio TA, Yu CT, Hildebrandt L, Howell AL, Weiss J, Guyre PM. Morphine inhibits spontaneous and cytokine-enhanced natural killer cell cytotoxicity in volun-teers. Anesthesiology 1995; 83: 500-508 [PMID: 7661350]
31 Schols SE, Lancé MD, Feijge MA, Damoiseaux J, Marcus MA, Hamulyák K, Ten Cate H, Heemskerk JW, van Pampus EC. Impaired thrombin generation and fibrin clot forma-tion in patients with dilutional coagulopathy during major surgery. Thromb Haemost 2010; 103: 318-328 [PMID: 20024495 DOI: 10.1160/TH09-06-0396]
32 Vorgias G, Iavazzo C, Mavromatis J, Leontara J, Katsoulis M, Kalinoglou N, Akrivos T. Determination of the neces-sary total protein substitution requirements in patients with advanced stage ovarian cancer and ascites, undergoing deb-ulking surgery. Correlation with plasma proteins. Ann Surg Oncol 2007; 14: 1919-1923 [PMID: 17406944 DOI: 10.1245/s10434-007-9404-x]
33 Ronald A, Dunning J. Can the use of thromboelastography predict and decrease bleeding and blood and blood product requirements in adult patients undergoing cardiac sur-gery? Interact Cardiovasc Thorac Surg 2005; 4: 456-463 [PMID:
Corbella D et al . Anesthetic management of CRS and HIPEC

136 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
17670456 DOI: 10.1510/icvts.2005.115154]34 De Somer F, Ceelen W, Delanghe J, De Smet D, Vanackere M,
Pattyn P, Mortier E. Severe hyponatremia, hyperglycemia, and hyperlactatemia are associated with intraoperative hy-perthermic intraperitoneal chemoperfusion with oxaliplatin. Perit Dial Int 2008; 28: 61-66 [PMID: 18178949]
35 Faerch K, Vaag A, Holst JJ, Glümer C, Pedersen O, Borch-Johnsen K. Impaired fasting glycaemia vs impaired glucose tolerance: similar impairment of pancreatic alpha and beta cell function but differential roles of incretin hormones and insulin action. Diabetologia 2008; 51: 853-861 [PMID: 18317726 DOI: 10.1007/s00280-008-0711-0]
36 Weeks JC, Cook EF, O’Day SJ, Peterson LM, Wenger N, Red-ing D, Harrell FE, Kussin P, Dawson NV, Connors AF, Lynn J, Phillips RS. Relationship between cancer patients’ predic-tions of prognosis and their treatment preferences. JAMA 1998; 279: 1709-1714 [PMID: 9624023]
37 McQuellon RP, Loggie BW, Lehman AB, Russell GB, Flem-ing RA, Shen P, Levine EA. Long-term survivorship and quality of life after cytoreductive surgery plus intraperito-neal hyperthermic chemotherapy for peritoneal carcinoma-tosis. Ann Surg Oncol 2003; 10: 155-162 [PMID: 12620911]
38 Rossi CR, Deraco M, De Simone M, Mocellin S, Pilati P, Foletto M, Cavaliere F, Kusamura S, Gronchi A, Lise M. Hyperthermic intraperitoneal intraoperative chemotherapy after cytoreductive surgery for the treatment of abdominal sarcomatosis: clinical outcome and prognostic factors in 60 consecutive patients. Cancer 2004; 100: 1943-1950 [PMID: 15112276 DOI: 10.1002/cncr.20192]
39 Cotte E, Passot G, Mohamed F, Vaudoyer D, Gilly FN, Glehen O. Management of peritoneal carcinomatosis from colorectal cancer: current state of practice. Cancer J 2009; 15: 243-248 [PMID: 19556911 DOI: 10.1097/PPO.0b013e3181a58d67]
40 McQuellon RP, Loggie BW, Fleming RA, Russell GB, Lehm-an AB, Rambo TD. Quality of life after intraperitoneal hyper-thermic chemotherapy (IPHC) for peritoneal carcinomatosis. Eur J Surg Oncol 2001; 27: 65-73 [PMID: 11237495]
41 McQuellon R, Gavazzi C, Piso P, Swain D, Levine E. Qual-ity of life and nutritional assessment in peritoneal surface malignancy (PSM): recommendations for care. J Surg Oncol
2008; 98: 300-305 [PMID: 18726903 DOI: 10.1002/jso.21050]42 McQuellon RP, Danhauer SC, Russell GB, Shen P, Fen-
stermaker J, Stewart JH, Levine EA. Monitoring health out-comes following cytoreductive surgery plus intraperitoneal hyperthermic chemotherapy for peritoneal carcinomatosis. Ann Surg Oncol 2007; 14: 1105-1113 [PMID: 17206478 DOI: 10.1245/s10434-006-9304-5]
43 Piso P, Glockzin G, von Breitenbuch P, Popp FC, Dahlke MH, Schlitt HJ, Nissan A. Quality of life after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal surface malignancies. J Surg Oncol 2009; 100: 317-320 [PMID: 19697438 DOI: 10.1002/jso.21327]
44 Schmidt C, Moritz S, Rath S, Grossmann E, Wiesenack C, Piso P, Graf BM, Bucher M. Perioperative management of patients with cytoreductive surgery for peritoneal carcino-matosis. J Surg Oncol 2009; 100: 297-301 [PMID: 19697426 DOI: 10.1002/jso.21322]
45 Sloan JA, Frost MH, Berzon R, Dueck A, Guyatt G, Moin-pour C, Sprangers M, Ferrans C, Cella D. The clinical signifi-cance of quality of life assessments in oncology: a summary for clinicians. Support Care Cancer 2006; 14: 988-998 [PMID: 16794811 DOI: 10.1007/s00520-006-0085-y]
46 Laky B, Janda M, Bauer J, Vavra C, Cleghorn G, Obermair A. Malnutrition among gynaecological cancer patients. Eur J Clin Nutr 2007; 61: 642-646 [PMID: 17021596 DOI: 10.1038/sj.ejcn.1602540]
47 Laviano A, Meguid MM. Nutritional issues in cancer man-agement. Nutrition 1996; 12: 358-371 [PMID: 8875522]
48 Andreyev HJ, Norman AR, Oates J, Cunningham D. Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur J Cancer 1998; 34: 503-509 [PMID: 9713300]
49 Martindale RG, Maerz LL. Management of perioperative nutrition support. Curr Opin Crit Care 2006; 12: 290-294 [PMID: 16810037 DOI: 10.1097/01.ccx.0000235204.54579.14]
50 Weimann A, Braga M, Harsanyi L, Laviano A, Ljungqvist O, Soeters P, Jauch KW, Kemen M, Hiesmayr JM, Horbach T, Kuse ER, Vestweber KH. ESPEN Guidelines on Enteral Nutri-tion: Surgery including organ transplantation. Clin Nutr 2006; 25: 224-244 [PMID: 16698152 DOI: 10.1016/j.clnu.2006.01.015]
P- Reviewers: de Bree E, Morris DL, Mura B S- Editor: Zhai HH L- Editor: A E- Editor: Zheng XM
Corbella D et al . Anesthetic management of CRS and HIPEC

© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Ovarian cancer; Hyperthermic intraperitoneal chemotherapy; Chemo-sensitivity; Time-points; Survival
Core tip: The standard treatment for advanced ovarian cancer consists in complete cytoreductive surgery and intravenous combination chemotherapy with a platinum compound and a taxane. Although response rates to initial therapy are high, many patients will recur and die of peritoneal carcinomatosis. The addition of hyper-thermic intraperitoneal chemotherapy (HIPEC) to the standard therapy aims at increasing survival by reduc-ing peritoneal recurrence. In this review we discuss the time points where HIPEC can be proposed.
De Iaco P, Perrone AM, Procaccini M, Pellegrini A, Morice P. Natural history of epithelial ovarian cancer and its rela-tion to surgical and medical treatment. World J Obstet Gyne-col 2013; 2(4): 137-142 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/137.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.137
INTRODUCTIONEpithelial ovarian cancer (EOC) represents approximately 90% of primary malignant ovarian tumors, the sixth most common cancer in women and the second most common gynecologic cancer[1]. At diagnosis, the majority of patients (70%) are in advanced stage of the disease (FIGO ⅡB-Ⅳ) with rapid and asymptomatic widespread cancer cells in the pelvic structure and peritoneal cavity[2]. Disease stage at presentation is the most important prognostic factor deter-mining outcome; 70%-80% of women at stage Ⅰ survive for five years compared to only 15% of those at stage Ⅳ[3].
Recent advances in pathology and genetics have shown that EOC is a heterogeneous disease with various
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.137
World J Obstet Gynecol 2013 November 10; 2(4): 137-142ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Natural history of epithelial ovarian cancer and its relation to surgical and medical treatment
Pierandrea De Iaco, Anna Myriam Perrone, Martina Procaccini, Alice Pellegrini, Philippe Morice
Pierandrea De Iaco, Anna Myriam Perrone, Martina Procac-cini, Alice Pellegrini, Gynecologic Oncology Unit, Sant’Orsola Malpighi Hospital, 40138 Bologna, ItalyPhilippe Morice, Gynecologic Oncology Unit, Gustave Roussy Institute, 94805 Villejuif, FranceAuthor contributions: All authors contributed equally to this manuscript.Correspondence to: Pierandrea De Iaco, MD, Gynecologic Oncology Unit, Sant’Orsola Malpighi Hospital, Via Massarenti 13, 40138 Bologna, Italy. [email protected]: +39-335-6666354 Fax: +39-51-6364392Received: December 13, 2012 Revised: March 12, 2013Accepted: April 13, 2013Published online: November 10, 2013
AbstractEpithelial ovarian cancer (EOC) represents approxi-mately 90% of primary malignant ovarian tumors, the sixth most common cancer in women and the second most common gynecologic cancer. Approximately 80%-85% of all ovarian carcinomas in Western society are serous and up to 95% of patients are in advanced stages (FIGO stage Ⅲ-Ⅳ) at diagnosis. Treatment of ovarian cancer is mainly based on three key approach-es: surgical removal of neoplasia; chemotherapy to kill cancer cells; direct chemotherapy on peritoneal surfac-es. The application of hyperthermic chemotherapy to the peritoneal cavity (HIPEC) after radical surgery may also be an attractive option. We analyzed the natural history of EOC in the literature and identified various time-points where sensitivity to chemotherapy, free-dom from disease and overall survival are different. We propose eight time-points in EOC history with homoge-neous oncological findings. The effectiveness of HIPEC in EOC treatment should be evaluated based on these eight time-points and we believe that retrospective and prospective studies of HIPEC should be evaluated ac-cording to these time-points.
TOPIC HIGHLIGHT
137 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Federico Coccolini, MD, Series Editor

De Iaco P et al . EOC surgical and medical treatment
risk factors, genetic abnormalities and oncological path-ways that partly determine biological behavior, response to chemotherapy, and prognosis[4]. A dualistic model places the major histological types into two groups: types Ⅰ and Ⅱ. Type Ⅰ cancers (mucinous, endometrioid, clear cell carcinomas and low-grade serous carcinomas) demonstrate a relatively insidious clinical course with generally better prognosis. These develop in a stepwise fashion from well-established precursor lesions, such as borderline tumors and endometriosis[5,6]. Type Ⅰ are relatively genetically stable and typically display a variety of somatic mutations in genes including K-ras, BRAF, PTEN, CTNNB1 but very rarely TP53. In contrast, Type Ⅱ cancers (high-grade serous carcinomas, high-grade transitional carcinomas, malignant mixed mesodermal tumors and undifferentiated carcinomas) are extremely aggressive neoplasms with remarkable early sensitivity to platinum-based chemotherapy but are frequently diag-nosed at advanced stages. They are chromosomally highly unstable and harbour TP53 mutations in more than 95% of cases[7,8]. Approximately 80%-85% of all ovar-ian carcinomas in Western society are serous. Up to 95% of patients with FIGO stage Ⅲ-Ⅳ disease have serous carcinomas whereas FIGO stage Ⅰ serous carcinomas are uncommon[9,10].
Like other cancers, EOC can spread through lym-phatic and blood vessels to nodes and parenchyma of distant organs (liver, lung and brain). However, a distinc-tive feature of these tumors is their ability to spread from the ovary to the abdominal cavity, forming nodules of variable size on the surface of the parietal and visceral peritoneum, including the omentum. The coalescence of nodules forms plaque or masses in the abdominal-pelvic cavity. Blockage of diaphragmatic lymphatics prevents outflow of proteinaceous fluid from the peritoneal cavity, causing the accumulation of ascites in advanced disease. Tumor dissemination from the peritoneal cavity to the pleural cavity occurs through the diaphragmatic perito-neum and leads to pleural effusion[11,12].
TREATMENT OF PRIMARY ADVANCED OVARIAN CANCER The main treatment of advanced disease consists of surgical removal of all visible nodules in the abdominal cavity followed by intravenous chemotherapy (platinum-based drugs with or without taxanes). The combined ef-fect of surgery and chemotherapy is often the complete eradication of cancer cells.
Treatment of ovarian cancer is mainly based on three key areas: surgical removal of neoplasia; chemotherapy to kill cancer cells; application of chemotherapy directly on peritoneal surfaces.
In advanced disease (FIGO stage ⅡB-ⅢC) the sur-gical removal of neoplasia with optimal cytoreduction (nodules ≤ 1 cm left) is recommended. An additional survival advantage of complete cytoreduction (no visible residual disease) has been recently reported[12]. Several studies have shown that specialized gynecological oncolo-
gist surgeons are more likely to perform optimal surgery than general surgeons[13]. The frequent presence of mul-tiple neoplastic implants on peritoneal surfaces together with pelvic and upper abdominal organs implies that surgeons must be prepared to remove organs beyond the pelvis, such as peritoneal surfaces of colic gutters, dia-phragmatic domes, and to carry out surgical procedures on the colon, bowel, liver, gallbladder, stomach, and spleen. This implies multidisciplinary surgical effort and the possibility of higher postoperative morbidity. This idea has not been accepted by the majority of gyneco-logic oncologists due to the lack of scientific data. If initial maximal cytoreduction is not carried out, interval debulking surgery (IDS) should be considered in patients responding to chemotherapy or with stable disease. IDS should ideally be carried out after three cycles of che-motherapy then followed by three further chemotherapy cycles[14].
Chemotherapeutic efficacy for ovarian carcinoma showed a dramatic shift after the introduction of plati-num compounds and since 1996 the combination of plat-inum plus paclitaxel has been the standard treatment. The current rationale of six cycles of treatment as standard is based on three randomized trials which analyzed the impact of chemotherapy duration (i.e., number of cycles) on OS. None of these studies demonstrated a difference in median survival time, but longer durations were as-sociated with increased toxicity, especially neuropathy[15]. Other chemotherapy regimens, such as gemcitabine and liposomal doxorubicin in association with carboplatin-paclitaxels were compared to carboplatin-plaxitel alone in the Phase Ⅲ Gynecologic Cancer Intergroup (GCIG) trials (GOG 0182-ICON 5). These showed no statisti-cally significant superiority or clinically useful benefit as-sociated with the three drugs compared to the controls. Currently carboplatin-paclitaxel remains the treatment of choice even though angiogenesis inhibitors in combina-tion with the standard treatment have been approved by the US Food and Drug Administration[16]. The main issue with EOC is the chemo sensitivity of cancer cells. Data shows that only 50% of patients have a complete clinical response to standard Ⅳ chemotherapy and that 30% of them have microscopic metastasis at surgical exploration. Most advanced stage patients who achieve clinical remis-sion after completion of initial treatment develop recur-rent disease and drug resistance, and their cure rate is less than 30%. These factors are major limitations in the treatment of patients with EOC. In order to overcome these limitations, different treatments such as second-ary cytoreduction, second line chemotherapy drugs, high dose chemotherapy, intra-peritoneal (IP) chemotherapy, radiotherapy, immunotherapy and hormone therapy should be considered. To date, none of these approaches, apart from IP chemotherapy, has been found to have a significant impact on survival[17].
IP chemotherapy refers to the administration of cyto-toxic agents directly to the peritoneal cavity. The rationale is that a higher concentration of cytotoxic drugs and longer duration of exposure can be achieved while re-
138 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

ducing the toxicity normally associated with intravenous therapy[18-20]. In fact, IP administered cytotoxic drugs can directly target tumor masses confined to the abdominal cavity, thus bypassing the poor vascularization of small volume disease and thereby increasing peri- and intra-tumoral drug concentration. Cisplatin can penetrate small volume tumors to a maximum depth of 1-3 mm and may therefore only benefit those patients with microscopic residual disease. By using large intra-peritoneal doses, the tumor surface can be exposed to high concentrations of cisplatin with only a small amount of drug leaking into the circulation. By this means, the amount of cisplatin reaching the tumor through capillaries is doubled when
compared to the maximum tolerated dose delivered intravenously. Several studies have documented the ad-vantages of IP compared to Ⅳ chemotherapy[20]. Post-operative adhesions after cytoreductive surgery can limit the access of the active drug to tumor areas and other complications, such as infections due to the IP catheter, may occur. Intra-operative administration of IP chemo-therapy has been designed to overcome such obstacles. Intra-peritoneal hyperthermia chemotherapy (HIPEC) is a new treatment method based on increasing the sensitiv-ity of cancer cells to the direct cytotoxic effect of chemo-therapeutic agents at high temperature and increasing the concentration of chemotherapeutic agents that penetrate
139 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Surgery
Surgery
ChemotherapyChemotherapy
Recurrence
5
4
Ovarian carcinomaStage Ⅲ
Possibility ofoptimal surgery
Surgery
Surgery
Chemotherapy
Chemotherapy
No disease
Complete or partial regression
1 3
2
Figure 1 Epithelial ovarian cancer natural history: Time-points where intra-peritoneal hyperthermia chemotherapy can be proposed.
Ref. Patients (n )
Time-point of optimal cytoreduction
Median disease free survival (mo)
Overall 3-yr survival (%)
Overall 5-yr survival (%)
Ansaloni et al[21] 39 1, 2, 3, 4, 5 421 NR NRDeraco et al[28] 56 4, 5 NR NR 23Pomel et al[30] 31 2, 3 27 672 NRBereder et al[31] 246 2, 4, 5 13 60 35Pavlov et al[32] 56 1, 4, 5 26 NR NRFagotti et al[33] 25 4, 5 10 NR NRGuardiola et al[34] 47 2 14 632 NRDi Giorgio et al[35] 47 1, 4, 5 20 NR 17Bae et al[36] 67 2, 3 NR NR 66Cotte et al[37] 81 5 19 NR NRHelm et al[38] 18 5 10 NR NRRufián et al[39] 33 1, 4 NR 46 37Raspagliesi et al[40] 40 3, 5 11 NR 15Reichman et al[41] 13 1, 4 15 55 NRGori et al[42] 29 3 571 NR NRLook et al[43] 28 1, 5 17 NR NRRyu et al[44] 57 2, 3 26 NR 54Piso et al[45] 19 1, 4, 5 18 NR 15Zanon et al[46] 30 2 17 35 12Chatzigeorgiou et al[47] 20 5 21 NR NRde Bree et al[48] 19 4, 5 26 63 42Cavaliere et al[49] 20 NR NR 502 NR
Table 1 Time-points of optimal cytoreduction and survival result of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy of 1021 patients with carcinomatosis from ovarian cancer
1Results expressed as mean; 2Two-year survival result. NR: Not reported.
De Iaco P et al . EOC surgical and medical treatment

cancer tissues[21-23].
TREATMENT OF RECURRENCEApproximately 70% of patients with advanced cancer who experience clinical remission after initial surgery and chemotherapy will develop recurrent disease[24].
In general, patients who progress during treatment with platinum are considered to have “platinum-refrac-tory” disease and patients who show recurrence < 6 mo after completion of first-line platinum chemotherapy are considered to have “platinum resistant” disease. These patients are candidates for salvage therapy with second line chemotherapy. Patients who relapse after an interval of > 6-12 mo are defined as “platinum-sensitive” and are candidates for chemotherapy and/or surgery. The concept of chemo-sensivity is based on clinical data; re-subjecting the patient to the previous chemotherapy regi-men obtains about a 20% response, but drug administra-tion is the only method by which to verify cell response. Because of the late onset of relapse, platinum-sensitive patients should in reality be regarded as including both chemo-sensitive and chemo-insensitive patients[25].
Appropriate treatment of recurrence (chemotherapy/surgery), which may be based on time and nature of re-lapse and the role of surgery, remains a field of discussion and controversy.
In general, surgical resection may be considered in platinum-sensitive patients. Resectable disease, good per-formance status and complete secondary cytoreduction are one of the best predictors of survival in these patients[26-28].
In ovarian platinum-sensitive recurrence, surgical cytoreduction offers the following potential benefits: (1) cytoreduction of tumor volume offers patients a greater
chance of response to chemotherapy; and (2) the elimina-tion of potentially chemo-resistant cells. However, surgi-cal cytoreduction is generally not undertaken without also scheduling postoperative chemotherapy since surgery alone rarely offers a cure.
ADVANCED EOC NATURAL HISTORY TIME-POINTSWe analyzed literature using the search terms “ovarian can-cer” and “HIPEC treatment”. EOC naturally presents vari-ous time-points where surgery, chemotherapy or HIPEC can be identified with homogenous chemo-sensitivity, re-sponse to therapy, and survival. Chua et al[27] proposed five time-points: (1) time of primary treatment; (2) time of IDS; (3) time of consolidation therapy after complete pathologi-cal response following initial therapy; (4) time of first recur-rence; or (5) time of salvage therapy (Figure 1). The results of the most important paper are shown in Table 1[28-49].
Given that chemo-sensitivity is an important issue for the prognosis and the homogeneity of these patients, we considered eight time-points upon which a clinical trial could be based: (1) time of primary treatment where optimal cytoreduction is achieved (group with chemo-sensitive and chemo-insensitive tumors); (2) time of IDS after neo-adjuvant chemotherapy with partial or complete response (chemo-sensitive group); (3) time of IDS after neo-adjuvant chemotherapy with stable disease (chemo-insensitive group); (4) time of consolidation therapy after complete pathological response following initial therapy (chemo-sensitive group); (5) time of first recurrence when disease relapses more than 12 mo after treatment (chemo-sensitive/chemo-insensitive group); (6) time of first recurrence when disease relapses more than 12 mo
140 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
> 12 mo disease free
Chemotherapy
< 6-12 mo disease free
Recurrence
5Surgery
Surgery
Surgery
SurgeryChemotherapy
Chemotherapy Complete or partial regression
8
6
7
4
Ovarian carcinomaStage Ⅲ
Possibility ofoptimal surgery
Surgery
Surgery
Chemotherapy
Chemotherapy
No disease
Complete or partial regression
1
3
2
Progressive or stable disease Surgery
Figure 2 Epithelial ovarian cancer natural history: Time-points where intra-peritoneal hyperthermia chemotherapy can be proposed and where chemo-sensitivity and chemo-insensitivity were evaluated.
De Iaco P et al . EOC surgical and medical treatment

after treatment and a course of chemotherapy obtains complete response (chemo-sensitive group); (7) time of first recurrence when disease relapses less than 12 mo after treatment (chemo-insensitive group); and (8) time of salvage therapy after various chemotherapy lines (chemo-insensitive group) (Figure 2). Correct analysis of past and future clinical trials should take account of these time-points in patient evaluation.
REFERENCES1 Morrison J, Haldar K, Kehoe S, Lawrie TA. Chemotherapy
versus surgery for initial treatment in advanced ovarian epi-thelial cancer. Cochrane Database Syst Rev 2012; 8: CD005343 [PMID: 22895947]
2 Fagotti A, Gallotta V, Romano F, Fanfani F, Rossitto C, Naldini A, Vigliotta M, Scambia G. Peritoneal carcinosis of ovarian ori-gin. World J Gastrointest Oncol 2010; 2: 102-108 [PMID: 21160928 DOI: 10.4251/wjgo.v2.i4.102]
3 Elattar A, Bryant A, Winter-Roach BA, Hatem M, Naik R. Op-timal primary surgical treatment for advanced epithelial ovar-ian cancer. Cochrane Database Syst Rev 2011; CD007565 [PMID: 21833960]
4 Kurman RJ, Shih IeM. The origin and pathogenesis of epi-thelial ovarian cancer: a proposed unifying theory. Am J Surg Pathol 2010; 34: 433-443 [PMID: 20154587 DOI: 10.1097/PAS.0b 013e3181cf3d79]
5 Kurman RJ, Shih IeM. Pathogenesis of ovarian cancer: les-sons from morphology and molecular biology and their clini-cal implications. Int J Gynecol Pathol 2008; 27: 151-160 [PMID: 18317228]
6 Shih IeM, Kurman RJ. Ovarian tumorigenesis: a proposed model based on morphological and molecular genetic analy-sis. Am J Pathol 2004; 164: 1511-1518 [PMID: 15111296 DOI: 10.1016/S0002-9440(10)63708-X]
7 Singer G, Stöhr R, Cope L, Dehari R, Hartmann A, Cao DF, Wang TL, Kurman RJ, Shih IeM. Patterns of p53 mutations separate ovarian serous borderline tumors and low- and high-grade carcinomas and provide support for a new model of ovarian carcinogenesis: a mutational analysis with immuno-histochemical correlation. Am J Surg Pathol 2005; 29: 218-224 [PMID: 15644779 DOI: 10.1097/01.pas.0000146025.91953.8d]
8 Bell DA. Origins and molecular pathology of ovarian cancer. Mod Pathol 2005; 18 Suppl 2: S19-S32 [PMID: 15761464 DOI: 10.1038/modpathol.3800306]
9 McCluggage WG. Morphological subtypes of ovarian car-cinoma: a review with emphasis on new developments and pathogenesis. Pathology 2011; 43: 420-432 [PMID: 21716157 DOI: 10.1097/PAT.0b013e328348a6e7]
10 Borley J, Wilhelm-Benartzi C, Brown R, Ghaem-Maghami S. Does tumour biology determine surgical success in the treat-ment of epithelial ovarian cancer? A systematic literature review. Br J Cancer 2012; 107: 1069-1074 [PMID: 22935582 DOI: 10.1038/bjc.2012.376]
11 Al Rawahi T, Lopes AD, Bristow RE, Bryant A, Elattar A, Chattopadhyay S, Galaal K. Surgical cytoreduction for recur-rent epithelial ovarian cancer. Cochrane Database Syst Rev 2013; 2: CD008765 [PMID: 23450588]
12 Hamilton CA, Miller A, Miller C, Krivak TC, Farley JH, Cher-nofsky MR, Stany MP, Rose GS, Markman M, Ozols RF, Arm-strong DK, Maxwell GL. The impact of disease distribution on survival in patients with stage III epithelial ovarian cancer cytoreduced to microscopic residual: a Gynecologic Oncol-ogy Group study. Gynecol Oncol 2011; 122: 521-526 [PMID: 21683993 DOI: 10.1016/j.ygyno.2011.04.041]
13 Chi DS, Eisenhauer EL, Lang J, Huh J, Haddad L, Abu-Rustum NR, Sonoda Y, Levine DA, Hensley M, Barakat RR. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol
Oncol 2006; 103: 559-564 [PMID: 16714056 DOI: 10.1016/j.ygyno.2006.03.051]
14 Weinberg LE, Rodriguez G, Hurteau JA. The role of neoad-juvant chemotherapy in treating advanced epithelial ovarian cancer. J Surg Oncol 2010; 101: 334-343 [PMID: 20187069 DOI: 10.1002/jso.21482]
15 Jacob JH, Gershenson DM, Morris M, Copeland LJ, Burke TW, Wharton JT. Neoadjuvant chemotherapy and interval debulking for advanced epithelial ovarian cancer. Gynecol Oncol 1991; 42: 146-150 [PMID: 1894174 DOI: 10.1016/0090-8258(91)90335-3]
16 Neijt JP, ten Bokkel Huinink WW, van der Burg ME, van Oosterom AT, Willemse PH, Heintz AP, van Lent M, Trim-bos JB, Bouma J, Vermorken JB. Randomized trial comparing two combination chemotherapy regimens (CHAP-5 v CP) in advanced ovarian carcinoma. J Clin Oncol 1987; 5: 1157-1168 [PMID: 3114434]
17 van der Burg ME, van Lent M, Buyse M, Kobierska A, Colom-bo N, Favalli G, Lacave AJ, Nardi M, Renard J, Pecorelli S. The effect of debulking surgery after induction chemotherapy on the prognosis in advanced epithelial ovarian cancer. Gyneco-logical Cancer Cooperative Group of the European Organiza-tion for Research and Treatment of Cancer. N Engl J Med 1995; 332: 629-634 [PMID: 7845426 DOI: 10.1056/NEJM1995030933 21002]
18 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cis-platin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
19 Hess LM, Benham-Hutchins M, Herzog TJ, Hsu CH, Malone DC, Skrepnek GH, Slack MK, Alberts DS. A meta-analysis of the efficacy of intraperitoneal cisplatin for the front-line treat-ment of ovarian cancer. Int J Gynecol Cancer 2007; 17: 561-570 [PMID: 17504373 DOI: 10.1111/j.1525-1438.2006.00846.x]
20 Barlin JN, Dao F, Zgheib NB, Ferguson SE, Sabbatini PJ, Hens-ley ML, Bell-McGuinn KM, Konner J, Tew WP, Aghajanian C, Chi DS. Progression-free and overall survival of a modified outpatient regimen of primary intravenous/intraperitoneal paclitaxel and intraperitoneal cisplatin in ovarian, fallopian tube, and primary peritoneal cancer. Gynecol Oncol 2012; 125: 621-624 [PMID: 22446622 DOI: 10.1016/j.ygyno.2012.03.027]
21 Ansaloni L, Agnoletti V, Amadori A, Catena F, Cavaliere D, Coccolini F, De Iaco P, Di Battista M, Framarini M, Gazzotti F, Ghermandi C, Kopf B, Saponara M, Tauceri F, Vallicelli C, Verdecchia GM, Pinna AD. Evaluation of extensive cytoreduc-tive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with advanced epithelial ovarian cancer. Int J Gynecol Cancer 2012; 22: 778-785 [PMID: 22572845 DOI: 10.1097/IGC.0b013e31824d836c]
22 Ansaloni L, De Iaco P, Frigerio L. Re: “cytoreductive surgery and hyperthermic intraperitoneal chemotherapy as upfront therapy for advanced epithelial ovarian cancer: multi-institu-tional phase II trial.” - Proposal of a clinical trial of cytoreduc-tive surgery and hyperthermic intraperitoneal chemotherapy in advanced ovarian cancer, the CHORINE study. Gynecol Oncol 2012; 125: 279-281 [PMID: 22233688 DOI: 10.1016/j.ygyno.2012.01.001]
23 Coccolini F, Lotti M, Manfredi R, Catena F, Vallicelli C, De Iaco PA, Da Pozzo L, Frigerio L, Ansaloni L. Ureteral stenting in cy-toreductive surgery plus hyperthermic intraperitoneal chemo-therapy as a routine procedure: evidence and necessity. Urol Int 2012; 89: 307-310 [PMID: 22868250 DOI: 10.1159/000339920]
24 Rustin GJ, van der Burg ME. A randomized trial in ovarian cancer of early treatment of relapse based on CA125 level alone versus delayed treatment based on conventional clinical indicators (MRC OV05/EORTC 55955 trials). J Clin Oncol 2009; 27: 18s
25 Fulham MJ, Carter J, Baldey A, Hicks RJ, Ramshaw JE, Gibson M. The impact of PET-CT in suspected recurrent ovarian can-cer: A prospective multi-centre study as part of the Australian
141 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
De Iaco P et al . EOC surgical and medical treatment

PET Data Collection Project. Gynecol Oncol 2009; 112: 462-468 [PMID: 19150121 DOI: 10.1016/j.ygyno.2008.08.027]
26 Hall M, Rustin G. Recurrent ovarian cancer: when and how to treat. Curr Oncol Rep 2011; 13: 459-471 [PMID: 22045509 DOI: 10.1007/s11912-011-0199-3]
27 Chua TC, Liauw W, Robertson G, Chia WK, Soo KC, Alobaid A, Al-Mohaimeed K, Morris DL. Towards randomized trials of cytoreductive surgery using peritonectomy and hyperthermic intraperitoneal chemotherapy for ovarian cancer peritoneal carcinomatosis. Gynecol Oncol 2009; 114: 137-19; author reply 139 [PMID: 19368962 DOI: 10.1016/j.ygyno.2009.03.002]
28 Deraco M, Virzì S, Iusco DR, Puccio F, Macrì A, Famulari C, Solazzo M, Bonomi S, Grassi A, Baratti D, Kusamura S. Secondary cytoreductive surgery and hyperthermic intraperi-toneal chemotherapy for recurrent epithelial ovarian cancer: a multi-institutional study. BJOG 2012; 119: 800-809 [PMID: 22571746 DOI: 10.1111/j.1471-0528.2011.03207.x]
29 Chua TC, Yan TD, Saxena A, Morris DL. Should the treatment of peritoneal carcinomatosis by cytoreductive surgery and hy-perthermic intraperitoneal chemotherapy still be regarded as a highly morbid procedure?: a systematic review of morbidity and mortality. Ann Surg 2009; 249: 900-907 [PMID: 19474692]
30 Pomel C, Ferron G, Lorimier G, Rey A, Lhomme C, Classe JM, Bereder JM, Quenet F, Meeus P, Marchal F, Morice P, Elias D. Hyperthermic intra-peritoneal chemotherapy using oxalipla-tin as consolidation therapy for advanced epithelial ovarian carcinoma. Results of a phase II prospective multicentre trial. CHIPOVAC study. Eur J Surg Oncol 2010; 36: 589-593 [PMID: 20466507]
31 Bereder J, Glehen O, Habre J, Desantis M, Cotte E, Mounier N, Ray-Cocquard I, Karimdjee B, Bakrin N, Bernard J, Benchimol D, Gilly F. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of perito-neal carcinomatosis from ovarian cancer: a multiinstitutional study of 246 patients. J Clin Oncol 2009; 27: 5542
32 Pavlov MJ, Kovacevic PA, Ceranic MS, Stamenkovic AB, Ivanovic AM, Kecmanovic DM. Cytoreductive surgery and modified heated intraoperative intraperitoneal chemotherapy (HIPEC) for advanced and recurrent ovarian cancer -- 12-year single center experience. Eur J Surg Oncol 2009; 35: 1186-1191 [PMID: 19356887]
33 Fagotti A, Paris I, Grimolizzi F, Fanfani F, Vizzielli G, Naldini A, Scambia G. Secondary cytoreduction plus oxaliplatin-based HIPEC in platinum-sensitive recurrent ovarian cancer patients: a pilot study. Gynecol Oncol 2009; 113: 335-340 [PMID: 19345401]
34 Guardiola E, Delroeux D, Heyd B, Combe M, Lorgis V, Demar-chi M, Stein U, Royer B, Chauffert B, Pivot X. Intra-operative intra-peritoneal chemotherapy with cisplatin in patients with peritoneal carcinomatosis of ovarian cancer. World J Surg Oncol 2009; 7: 14 [PMID: 19203351 DOI: 10.1186/1477-7819-7-14]
35 Di Giorgio A, Naticchioni E, Biacchi D, Sibio S, Accarpio F, Rocco M, Tarquini S, Di Seri M, Ciardi A, Montruccoli D, Sam-martino P. Cytoreductive surgery (peritonectomy procedures) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) in the treatment of diffuse peritoneal carcinoma-tosis from ovarian cancer. Cancer 2008; 113: 315-325 [PMID: 18473354]
36 Bae J, Lim MC, Choi JH, Song YJ, Lee KS, Kang S, Seo SS, Park SY. Prognostic factors of secondary cytoreductive surgery for patients with recurrent epithelial ovarian cancer. J Gynecol On-col 2009; 20: 101-106 [PMID: 19590721]
37 Cotte E, Glehen O, Mohamed F, Lamy F, Falandry C, Golfier F, Gilly FN. Cytoreductive surgery and intraperitoneal chemo-
hyperthermia for chemo-resistant and recurrent advanced epi-thelial ovarian cancer: prospective study of 81 patients. World J Surg 2007; 31: 1813-1820 [PMID: 17629740]
38 Helm CW, Randall-Whitis L, Martin RS, Metzinger DS, Gordi-nier ME, Parker LP, Edwards RP. Hyperthermic intraperitone-al chemotherapy in conjunction with surgery for the treatment of recurrent ovarian carcinoma. Gynecol Oncol 2007; 105: 90-96 [PMID: 17173957]
39 Rufián S, Muñoz-Casares FC, Briceño J, Díaz CJ, Rubio MJ, Ortega R, Ciria R, Morillo M, Aranda E, Muntané J, Pera C. Radical surgery-peritonectomy and intraoperative intraperito-neal chemotherapy for the treatment of peritoneal carcinoma-tosis in recurrent or primary ovarian cancer. J Surg Oncol 2006; 94: 316-324 [PMID: 16917864]
40 Raspagliesi F, Kusamura S, Campos Torres JC, de Souza GA, Ditto A, Zanaboni F, Younan R, Baratti D, Mariani L, Laterza B, Deraco M. Cytoreduction combined with intraperitoneal hyperthermic perfusion chemotherapy in advanced/recurrent ovarian cancer patients: The experience of National Cancer Institute of Milan. Eur J Surg Oncol 2006; 32: 671-675 [PMID: 16621425]
41 Reichman TW, Cracchiolo B, Sama J, Bryan M, Harrison J, Pliner L, Harrison LE. Cytoreductive surgery and intraopera-tive hyperthermic chemoperfusion for advanced ovarian car-cinoma. J Surg Oncol 2005; 90: 51-56; discussion 56-58 [PMID: 15844187]
42 Gori J, Castaño R, Toziano M, Häbich D, Staringer J, De Quirós DG, Felci N. Intraperitoneal hyperthermic chemotherapy in ovarian cancer. Int J Gynecol Cancer 2005; 15: 233-239 [PMID: 15823105]
43 Look M, Chang D, Sugarbaker PH. Long-term results of cyto-reductive surgery for advanced and recurrent epithelial ovar-ian cancers and papillary serous carcinoma of the peritoneum. Int J Gynecol Cancer 2004; 14: 35-41 [PMID: 14764027]
44 Ryu KS, Kim JH, Ko HS, Kim JW, Ahn WS, Park YG, Kim SJ, Lee JM. Effects of intraperitoneal hyperthermic chemotherapy in ovarian cancer. Gynecol Oncol 2004; 94: 325-332 [PMID: 15297169]
45 Piso P, Dahlke MH, Loss M, Schlitt HJ. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in peritoneal carcinomatosis from ovarian cancer. World J Surg Oncol 2004; 2: 21 [PMID: 15222884]
46 Zanon C, Clara R, Chiappino I, Bortolini M, Cornaglia S, Sim-one P, Bruno F, De Riu L, Airoldi M, Pedani F. Cytoreductive surgery and intraperitoneal chemohyperthermia for recurrent peritoneal carcinomatosis from ovarian cancer. World J Surg 2004; 28: 1040-1045 [PMID: 15573262]
47 Chatzigeorgiou K, Economou S, Chrysafis G, Dimasis A, Zaf-iriou G, Setzis K, Lyratzopoulos N, Minopoulos G, Manolas K, Chatzigeorgiou N. Treatment of recurrent epithelial ovarian cancer with secondary cytoreduction and continuous intra-operative intraperitoneal hyperthermic chemoperfusion (CI-IPHCP). Zentralbl Gynakol 2003; 125: 424-429 [PMID: 14628225]
48 de Bree E, Romanos J, Michalakis J, Relakis K, Georgoulias V, Melissas J, Tsiftsis DD. Intraoperative hyperthermic intraperi-toneal chemotherapy with docetaxel as second-line treatment for peritoneal carcinomatosis of gynaecological origin. Antican-cer Res 2003; 23: 3019-3027 [PMID: 12926156]
49 Cavaliere F, Di Filippo F, Botti C, Cosimelli M, Giannarelli D, Aloe L, Arcuri E, Aromatario C, Consolo S, Callopoli A, Laurenzi L, Tedesco M, Di Angelo P, Giunta S, Cavaliere R. Peritonectomy and hyperthermic antiblastic perfusion in the treatment of peritoneal carcinomatosis. Eur J Surg Oncol 2000; 26: 486-491 [PMID: 11016471]
P- Reviewers: de Andrade Urban C, Kruse AJ S- Editor: Gou SX L- Editor: Hughes D E- Editor: Zheng XM
142 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
De Iaco P et al . EOC surgical and medical treatment

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.143
World J Obstet Gynecol 2013 November 10; 2(4): 143-152ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Pharmacology of cancer chemotherapy drugs for hyperthermic intraperitoneal peroperative chemotherapy in epithelial ovarian cancer
Kurt Van der Speeten, Anthony O Stuart, Paul H Sugarbaker
Kurt Van der Speeten, Department of Surgical Oncology, Ziek-enhuis Oost-Limburg, 3600 Genk, BelgiumKurt Van der Speeten, University Hasselt, Life Sciences Fac-ulty, Oncology Research Cluster, 3000 Hasselt, BelgiumAnthony O Stuart, Paul H Sugarbaker, Washington Cancer Institute, Washington Hospital Center, Washington, DC 20010, United StatesAuthor contributions: All authors contributed the data analysis and discussion of this review.Correspondence to: Kurt Van der Speeten, MD, PhD, De-partment of Surgical Oncology, Ziekenhuis Oost-Limburg, Schi-epse Bos 6, 3600 Genk, Belgium. [email protected]: +32-89-326524 Fax: +32-89-326524Received: December 13, 2012 Revised: June 16, 2013Accepted: June 23, 2013Published online: November 10, 2013
AbstractThe peritoneal parietal and visceral surfaces of the ab-domen and pelvis are an important anatomic site for the dissemination of epithelial ovarian cancer (EOC). The transcoelomic spread of cancer cells gives rise to peritoneal carcinomatosis (PC) which, without special treatments, is a fatal manifestation of EOC. In order to control PC cytoreductive surgery to remove macroscopic disease is combined with perioperative intraperitoneal (IP) and perioperative intravenous chemotherapy to eradicate microscopic residual disease. Chemotherapy agents are selected to be administered by the IP or intra-venous route based on their pharmacologic properties. A peritoneal-plasma barrier which retards the clearance of high molecular weight chemotherapy from the peritoneal cavity results in a large exposure of small cancer nodules on abdominal and pelvic surfaces. Tissue penetration is facilitated by moderate hyperthermia (41-42 ℃) of the IP chemotherapy solution. Timing of the chemotherapy as a planned part of the surgical procedure to maximize expo-
sure of all peritoneal surfaces is crucial to success.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Intraperitoneal chemotherapy; Epithelial ovarian cancer; Ifosfamide; Cisplatin; Carboplatin; Tax-anes; Pharmacokinetics; Pharmacodynamics
Core tip: Intraperitoneal (IP) chemotherapy is an im-portant adjuvant treatment strategy in patients with advanced epithelial ovarian cancer. Although the clinical benefits have been demonstrated both in phase Ⅱ and Ⅲ trials, the pharmacologic rationale for this treatment strategy needs to be clarified. This manuscript reviews the pharmacokinetic and pharmacodynamic rationale of IP chemotherapy and analyzes the available data.
Van der Speeten K, Stuart AO, Sugarbaker PH. Pharmacology of cancer chemotherapy drugs for hyperthermic intraperitoneal peroperative chemotherapy in epithelial ovarian cancer. World J Obstet Gynecol 2013; 2(4): 143-152 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/143.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.143
INTRODUCTIONEpithelial ovarian cancer (EOC) is the second most com-mon gynecologic malignancy. Worldwide in 2008, ap-proximately 225000 women were diagnosed with EOC and 140000 died from their disease[1]. Seventy-five percent of these patients present with advanced disease outside of the pelvis at the time of diagnosis[2]. Besides the lymphatic and hematogenous routes of dissemination, transcoelomic spread of tumor cells is an acknowledged phenomenon
143 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Van der Speeten K et al . Current role of intraperitoneal chemotherapy
ultimately giving rise to peritoneal carcinomatosis (PC). In most patients, this intraperitoneal (IP) spread occurs before surgery as a direct consequence of full-thickness invasion of the involved organ by tumor and subsequently exfoliation of tumor cells in the peritoneal cavity. Alter-natively, IP spread may be the result of surgical trauma that causes release of tumor cells from transected lymph and blood vessels and manipulation of the primary tumor. The combination of optimal cytoreductive surgery (CRS) and effective platinum-based chemotherapy has resulted in significant survival benefit for these women. Nevertheless five year survival for patients with International Federa-tion of Gynecologists and Obstetrics stage ⅢC EOC only reaches 32.5%[3]. In an attempt to improve clinical results in EOC patients the IP route of chemotherapy adminis-tration has been explored both as an alternative and as an addition to systemic chemotherapy. This topic highlight manuscript aims to review the pharmacokinetic and phar-macodynamic data currently available regarding the IP de-livery of cancer chemotherapy agents in patients with PC of ovarian origin. Pubmed was questioned with the search terms; EOC, peritoneal metastases, PC, IP chemotherapy, CRS, pharmacology, pharmacokinetics, pharmacodynam-ics. No exclusion criteria were used. Relevant English lan-guage articles were reviewed both in abstract and full text.
PERITONEAL PLASMA BARRIERThe rationale of administering chemotherapeutic drugs into the peritoneal cavity is based on the relative trans-port barrier which is formed by the tissue surrounding the peritoneal space. The peritoneum is a complex three-dimensional organ covering the abdomino-pelvic organs and the abdominal wall. It contains a large potential space. The most elaborate description of the ultra structure of the peritoneum in man goes back to 1941 by Baron[4]. The peritoneum consists of a monolayer of mesothelial cells supported by a basement membrane and five layers of connective tissue which account for a total thickness of 90 μm. The connective tissue layers include interstitial cells and a matrix of collagen, hyaluron, and proteogly-cans. The cellular component consists of pericytes, paren-chymal cells and blood capillaries. The complex is often referred to as the peritoneal membrane. This description is a working model derived from research regarding the peritoneum as a dialysis membrane.
The accepted function of the peritoneum is twofold. First, it reduces friction between intraabdominal organs and the abdominal wall by producing a lubricant solution made of glycosaminoglycans and phospholipids[5]. Sec-ondly, it is of major importance together with lymphoid aggregates dispersed on the visceral and parietal perito-neum in the host defense against intraabdominal infec-tions. A third suggested function of the peritoneum in malignancy may be its role as a first line of defense against PC[6]. Any disruption in the peritoneal lining facilitates the adhesion-invasion cascade of tumor cells, resulting in the development of peritoneal tumor nodules on the abdomi-nal or pelvic surface[6,7].
Contrary to intuitive thinking the elimination of the mesothelial lining as performed during peritonectomy procedures does not significantly alter the pharmacoki-netic properties of the peritoneum in the transport of chemotherapeutic agents from the peritoneal cavity to the plasma compartment. Flessner et al[8] demonstrated in a rodent model that neither removal of the stagnant fluid layer on the mesothelium nor removal of the mesothelial lining influenced the mass transfer coefficient over the barrier. Indirect evidence supporting this hypothesis in humans can be derived from the fact that the extent of the peritonectomy in PC patients does little to alter the IP chemotherapy pharmacokinetics of Mitomycin C or 5-flu-orouracil[9,10]. Newer data suggest that major resections of visceral peritoneum increase the clearance of doxorubicin and mitomycin from peritoneal space[11,12]. Basic research rather demonstrates that not only the mesothelial lining but also the blood capillary wall and the surrounding in-terstitial matrix are the principal barrier for clearance of molecules from the abdominopelvic space[13].
Most basic research concerning the pharmacokinetic properties of the peritoneum is derived from the perito-neal dialysis literature[14]. A simplified mathematical diffu-sion model considers the plasma to be a single compart-ment separated by an effective membrane from another single compartment, the peritoneal cavity (Figure 1). This results in the following equation: Rate of mass transfer = permeability area (PA) [concentration in peritoneal cavity (CP) - concentration in the blood (CB)].
Although this offers a simple conceptional model of transport and states the importance of the effective expo-sure area, it only offers quantitative predictability once PA is empirically determined for each drug. It also does not offer insight into the actual tissue penetration at the level
144 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Elimination from body
compartment
Rate of mass transfer = PA (CP - CB)
Peritoneal and preperitoneal tissues with tumor nodules
Peritoneal cavityCP VP
Body compartmentCB VB
PA
Figure 1 Three-compartment model of peritoneal transport in which transfer of a drug from the peritoneal cavity to the blood occurs across the peritoneal membrane and preperitoneal tissues. In these tissues the peritoneal surface cancer nodules are located. The permeability-area product (PA) governs this transfer and can be calculated by measuring the rate of drug disappearance from the cavity and dividing by the overall concentration differ-ence between the peritoneal cavity and the blood (B). CB: The free drug con-centration in the blood (or plasma); VB: Volume of distribution of the drug in the body; CP: The free drug concentration in the peritoneal fluid; VP: Volume of the peritoneal cavity. Modified from Dedrick et al[16].

of the peritoneal membrane. Neither does it predict pen-etration of chemotherapy into the tumor nodules which is the single most important factor determining response to cancer treatment.
PHARMACOKINETIC RATIONALE OF PERI-OPERATIVE IP CANCER CHEMOTHERAPY Pharmacokinetics explores what the body does to the cancer chemotherapy drug and pharmacodynamics ex-plores what the drug does to the body. The IP route of delivering chemotherapy is logistically less convenient and technologically more challenging than conventional intra-venous chemotherapy. This explains why the pharmaco-kinetic rationale of IP chemotherapy needs to be clarified to justify this route of cancer chemotherapy administra-tion. IP administration of chemotherapeutic agents gives high response rates in PC patients because the peritoneal plasma barrier provides dose-intensive therapy. Based on peritoneal dialysis research, Dedrick et al[15] concluded that the peritoneal permeability of a number of hydrophilic anticancer drugs may be considerably less than the plasma clearance of that same drug. This results in a significantly higher concentration in the peritoneal cavity as compared to the plasma after IP administration. This concentra-tion difference offers the opportunity of exposing the residual tumor cells after CRS to high doses of chemo-therapeutic agents with reduced systemic concentrations and lower systemic toxicity. This advantage is expressed by the area under the curve (AUC) ratios of IP vs plasma exposure[14,15]. The marked increase in exposure of peri-toneal surfaces to chemotherapy solution as compared to plasma is illustrated in Figure 2. The chemotherapy agent, paclitaxel has a high molecular weight (853.9 kDa) and is hydrophilic compound; consequently it is slow to cross the peritoneal cavity to plasma barrier. The AUC ratio is approximately 1000[12].
An important consideration is that high IP concentra-tion or AUC IP/intravenous does not automatically con-fer a greater efficacy. Even with greatly elevated IP cancer chemotherapy concentrations, there may be limited pen-etration of the chemotherapeutic agent into the peritoneal tumor target. The ideal drug for IP chemotherapy has a high peritoneal tissue concentration as a result of direct IP administration and a high penetration into the cancer nodule[12]. This should occur along with slow diffusion through the capillary endothelium deep in the subperi-toneal space of the cancer chemotherapy solution. Low systemic concentrations and reduced systemic toxicity are maintained by rapid metabolism and excretion of drug within the body compartment.
PHARMACODYNAMICS OF IP CHEMOTHERAPYThe efficacy of IP cancer chemotherapy protocols is gov-erned by both non-pharmacokinetic variables (tumor nod-ule size, density, vascularity, interstitial fluid pressure, bind-ing, temperature) and pharmacokinetic variables. As such, the simplified two-compartment model described above may not provide an adequate theoretical model for penetra-tion of the intraoperatively administered (either intravenous or IP) chemotherapy into the peritoneal wall and into the tumor nodules. Dedrick et al[16,17] proposed a mathematical model seen in Figure 3 addressing the tissue penetration of low-molecular weight molecules. The drug diffuses from its peritoneal concentration, Cp, to its blood concentration, CB, along an exponential concentration gradient over the peritoneum and preperitoneal tissues. The extracellular “deep” concentration, Ce, can then calculated according to the formula: Ce = CB + (Cp - CB) exp[- (k/D)1/2x].
145 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
100
10
1
0.1
0.01
0.001
μg/m
L
0 2 4 6 8 10 12 14 16 18 20 22 24 t /h
Taxol pharmacokinetics - dianeal
Peritoneal fluidPlasma
Figure 2 Pharmacokinetic study of concentration versus time for intraper-itoneal paclitaxel. The chemotherapy agent at 30 mg/m2 was instilled directly into the peritoneal cavity as rapidly as possible in a 1.5% dextrose peritoneal dialysis solution. The concentration of paclitaxel was determined in peritoneal fluid and in plasma for 24 h[51].
Figure 3 Conceptual diagram of tissue adjacent to the peritoneal cavity. Solid line shows the exponential decrease in the free tissue interstitial concen-tration, Ce, as the drug diffuses down the concentration gradient and is removed by loss to the blood perfusing the tissue. Also shown are the characteristic dif-fusion length, x0, at which the concentration difference between the tissue and the blood has decreased to 37% of its maximum value, and 3x0, at which the difference has decreased to 5% of its maximum value. Cp: The free drug con-centration in the peritoneal fluid; CB: The free drug concentration in the blood (or plasma). Modified from Dedrick et al[16].
Peritoneal fluid
CB
Ce
x 0 3x 0
x
Cp
Capillary bed
Van der Speeten K et al . Current role of intraperitoneal chemotherapy
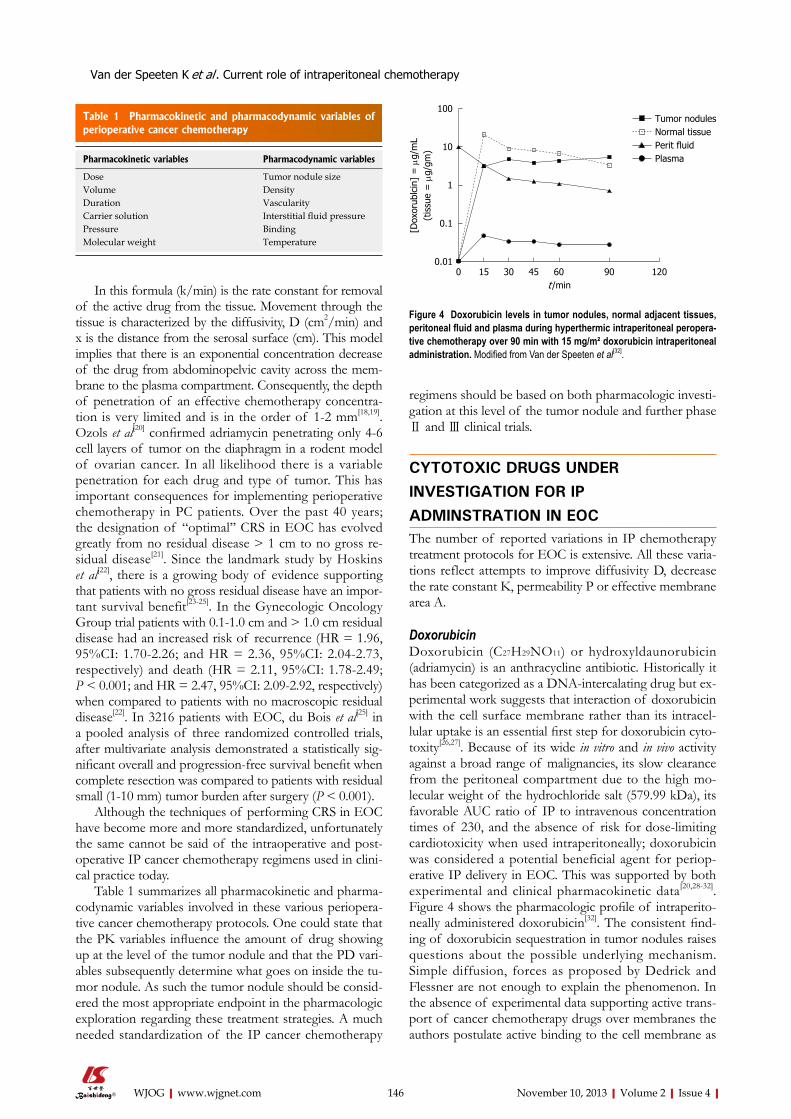
In this formula (k/min) is the rate constant for removal of the active drug from the tissue. Movement through the tissue is characterized by the diffusivity, D (cm2/min) and x is the distance from the serosal surface (cm). This model implies that there is an exponential concentration decrease of the drug from abdominopelvic cavity across the mem-brane to the plasma compartment. Consequently, the depth of penetration of an effective chemotherapy concentra-tion is very limited and is in the order of 1-2 mm[18,19]. Ozols et al[20] confirmed adriamycin penetrating only 4-6 cell layers of tumor on the diaphragm in a rodent model of ovarian cancer. In all likelihood there is a variable penetration for each drug and type of tumor. This has important consequences for implementing perioperative chemotherapy in PC patients. Over the past 40 years; the designation of “optimal’’ CRS in EOC has evolved greatly from no residual disease > 1 cm to no gross re-sidual disease[21]. Since the landmark study by Hoskins et al[22], there is a growing body of evidence supporting that patients with no gross residual disease have an impor-tant survival benefit[23-25]. In the Gynecologic Oncology Group trial patients with 0.1-1.0 cm and > 1.0 cm residual disease had an increased risk of recurrence (HR = 1.96, 95%CI: 1.70-2.26; and HR = 2.36, 95%CI: 2.04-2.73, respectively) and death (HR = 2.11, 95%CI: 1.78-2.49; P < 0.001; and HR = 2.47, 95%CI: 2.09-2.92, respectively) when compared to patients with no macroscopic residual disease[22]. In 3216 patients with EOC, du Bois et al[25] in a pooled analysis of three randomized controlled trials, after multivariate analysis demonstrated a statistically sig-nificant overall and progression-free survival benefit when complete resection was compared to patients with residual small (1-10 mm) tumor burden after surgery (P < 0.001).
Although the techniques of performing CRS in EOC have become more and more standardized, unfortunately the same cannot be said of the intraoperative and post-operative IP cancer chemotherapy regimens used in clini-cal practice today.
Table 1 summarizes all pharmacokinetic and pharma-codynamic variables involved in these various periopera-tive cancer chemotherapy protocols. One could state that the PK variables influence the amount of drug showing up at the level of the tumor nodule and that the PD vari-ables subsequently determine what goes on inside the tu-mor nodule. As such the tumor nodule should be consid-ered the most appropriate endpoint in the pharmacologic exploration regarding these treatment strategies. A much needed standardization of the IP cancer chemotherapy
regimens should be based on both pharmacologic investi-gation at this level of the tumor nodule and further phase Ⅱ and Ⅲ clinical trials.
CYTOTOXIC DRUGS UNDER INVESTIGATION FOR IP ADMINSTRATION IN EOCThe number of reported variations in IP chemotherapy treatment protocols for EOC is extensive. All these varia-tions reflect attempts to improve diffusivity D, decrease the rate constant K, permeability P or effective membrane area A.
DoxorubicinDoxorubicin (C27H29NO11) or hydroxyldaunorubicin (adriamycin) is an anthracycline antibiotic. Historically it has been categorized as a DNA-intercalating drug but ex-perimental work suggests that interaction of doxorubicin with the cell surface membrane rather than its intracel-lular uptake is an essential first step for doxorubicin cyto-toxity[26,27]. Because of its wide in vitro and in vivo activity against a broad range of malignancies, its slow clearance from the peritoneal compartment due to the high mo-lecular weight of the hydrochloride salt (579.99 kDa), its favorable AUC ratio of IP to intravenous concentration times of 230, and the absence of risk for dose-limiting cardiotoxicity when used intraperitoneally; doxorubicin was considered a potential beneficial agent for periop-erative IP delivery in EOC. This was supported by both experimental and clinical pharmacokinetic data[20,28-32]. Figure 4 shows the pharmacologic profile of intraperito-neally administered doxorubicin[32]. The consistent find-ing of doxorubicin sequestration in tumor nodules raises questions about the possible underlying mechanism. Simple diffusion, forces as proposed by Dedrick and Flessner are not enough to explain the phenomenon. In the absence of experimental data supporting active trans-port of cancer chemotherapy drugs over membranes the authors postulate active binding to the cell membrane as
146 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Pharmacokinetic and pharmacodynamic variables of perioperative cancer chemotherapy
Pharmacokinetic variables Pharmacodynamic variables
Dose Tumor nodule sizeVolume DensityDuration VascularityCarrier solution Interstitial fluid pressurePressure BindingMolecular weight Temperature
100
10
1
0.1
0.01
[Dox
orub
lcin
] =
μg/
mL
(tis
sue
= μ
g/gm
)
Tumor nodulesNormal tissuePerit fluidPlasma
0 15 30 45 60 90 120t /min
Figure 4 Doxorubicin levels in tumor nodules, normal adjacent tissues, peritoneal fluid and plasma during hyperthermic intraperitoneal peropera-tive chemotherapy over 90 min with 15 mg/m² doxorubicin intraperitoneal administration. Modified from Van der Speeten et al[32].
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

a possible mechanism. The sequestration phenomenon of doxorubicin in tumor nodules is a constant one in its presence regardless the underlying pathology or subtype. A consequence is that the cancer chemotherapy levels measured in the tumor nodules may be more important than considered in the past.
CisplatinCisplatin (cis-diamminedichloroplatinum-Ⅲ, CDDP) causes apoptotic cell death by formation of DNA ad-ducts[33]. It has been well studied in the setting of adjuvant normothermic postoperative IP chemotherapy of residual small volume ovarian cancer after CRS. Three randomized trials showed a significant survival benefit[34-36]. In the set-ting of CRS and hyperthermic intraperitoneal peropera-tive chemotherapy (HIPEC), cisplatin has been used for intracavitary therapy of ovarian cancer in several phase Ⅱ studies[37,38]. Currently three randomized phase Ⅲ stud-ies are recruiting patients to determine the role of CRS + HIPEC in primary and recurrent EOC. Schem et al[39] showed an excellent in vitro and in vivo thermal augmenta-tion of cisplatin. The penetration of cisplatin into tumor nodules was studied by several groups. Los et al[40] for the first time described intratumoral distribution of cisplatin after IP administration and suggested that the advantage over IP vs IV administration was maximal in the first 1.5 mm. van de Vaart et al[41] investigated the cisplatin induced DNA adduct formation and could measure this 3-5 mm into the tumor tissue. Esquis et al[42] in an experimental model reported an enhanced cisplatin penetration when cisplatin was administered with increased pressure.
CarboplatinCarboplatin [(1,1-cyclobutanedicarboxylato)platinum(II)] is a higher molecular weight platinum compound than cisplatin. Its main advantage is its decreased renal toxicity. As such it is currently explored in normothermic IP che-motherapy protocols in patients with advanced ovarian cancer[43,44]. Czejka et al[45] in a clinical study with normo-thermic carboplatin reported a relative bioavailability (cal-culated as AUC-values) which was at least 6 times higher in the IP fluid than in the serum for 48 h. Los et al[19] com-pared carboplatin and cisplatin after IP administration in a rat model of PC. Their data demonstrate that despite a clear pharmacokinetic advantage of IP carboplatin over cisplatin; its capacity to penetrate into peritoneal cancer nodules and tumor cells is far lower than that of cisplatin. These data limit have limited clinical its application in the past. In contrast, a more recent direct comparison reveals a comparable or better drug penetration of IP carbo-platin when compared to IP cisplatin given at equitoxic doses[46]. This has recently revived clinical interest in its IP application.
TaxanesPaclitaxel and docetaxel are taxanes considered for IP che-motherapy. The taxanes stabilize the microtubule against depolymerization; thereby disrupting normal microtubule
dynamics[47]. They exert cytotoxic activity against a broad range of tumors. Due to their high molecular weight these molecules have a remarkable high AUC ratio of re-spectively 853 and 861[48]. This translates itself into a clear pharmacokinetic advantage for IP administration[49]. The data regarding possible thermal augmentation of taxanes are conflicting[50-53]. Taxanes have been used in a neoadju-vant IP setting as well as intraoperatively and postopera-tively. Their cell-cycle specific mechanism of action makes them a particular good candidate for repetitive application such as in normothermic adjuvant postoperative IP che-motherapy[34,35]. Novel formulations of taxanes aiming at an increased bioavailability are under investigation for IP administration during HIPEC[54].
ROLE OF HYPERTHERMIAAdding hyperthermia to IP chemotherapy may increase tumor response to cancer chemotherapy through several mechanisms. First, heat alone has a direct anti-tumor ef-fect. Mild hyperthermia above 41 ℃ induces selective cytotoxicity of malignant cells by several mechanisms: impaired DNA repair, protein denaturation and, inhibi-tion of oxidative metabolism in the microenvironment of malignant cells. This leads to increased acidity, lysosomal activation and, increased apoptotic cell death[55-57]. In this setting, thermal tolerance can be induced by up regula-tion of heat shock proteins, which may limit the impor-tance of a direct anti-tumor effect of heat[58]. Second, applying mild hyperthermia augments the cytotoxic ef-fects of some chemotherapeutic agents. Synergy between heat and cancer chemotherapy drugs may arise from multiple events such as heat damage to ABC transport-ers (drug accumulation), intra-cellular drug detoxification pathways and, to repair mechanisms of drug-induced DNA adducts[59]. Such augmented effects are postulated for doxorubicin, platinum complexes, mitomycin C, melphalan, docetaxel, irinotecan and, gemcitabine[28,59-64]. Third, hyperthermia may increase the penetration depth of the cancer chemotherapy solution into tissues and tu-mor nodules. Jacquet et al[28] report tissue penetration of doxorubicin is enhanced when the cancer chemotherapy solution is administered intraperitoneally at 43 ℃. In ad-dition, hyperthermia does not affect the pharmacokinetic advantages of IP doxorubicin with low plasma and dis-tant tissue levels.
The elevated interstitial fluid pressure in tumor nod-ules, compared to normal tissue, is an acknowledged phe-nomenon[65]. Furthermore, in experimental tumors with a single nodule, interstitial fluid pressure is relatively uni-form in the nodule and drops precipitously in the periph-ery at the tumor-normal tissue interface[66]. Furthermore, Leunig et al[67] report a thermal dose-dependent decrease in interstitial fluid pressure in experimental solid tumors in an animal model after hyperthermia. All this experi-mental data however could not establish a direct effect of hyperthermia on survival. Klaver et al[68] in a rat model of PSM for first time separated the intraoperative IP chemo-
147 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

therapy from the IP hyperthermia. They demonstrated that the survival of the PC rats after CRS was highly de-pendent on the presence of the chemotherapeutic agent in the perfusate but not on the hyperthermia. No similar human data are available at this point in time.
BIDIRECTIONAL INTRAOPERATIVE CHEMOTHERAPY: RATIONALE AND PHARMACOLOGIC DATAThe Dedrick-model for peritoneal transport predicts transport by diffusion from the peritoneal compart-ment through a peritoneal and preperitoneal tissue layer to the plasma and, vice versa[15]. Figure 5 demonstrated that through combining intraoperative intravenous and intraoperative IP cancer chemotherapy, a bidirectional diffusion gradient is created through the intermediate tis-sue layer containing the cancer nodules[69]. Chemotherapy from both the IP and intravenous compartments con-verges on the tissues at the interface of peritoneal space
and peritoneal surface where the tumor nodules reside. Elias et al[70] first reported the clinical use of intraoperative intravenous 5-fluorouracil and leucovorin in conjunction with oxaliplatin-based hyperthermic IP perioperative che-motherapy in patients with PC of colorectal origin. More recently our group reported a similar effort in ovarian cancer with intravenous intraoperative ifosfamide[71]. The treatment strategy that has been employed in our studies is very similar to that published by Zylberberg et al[72] for ovarian cancer. His study showed excellent clinical results when systemic ifosfamide infusion was combined with IP cisplatin. We modified his ifosfamide regimen using an infusion over 90 min in the operating room. We demon-strated consistent high levels of ifosfamide and its active metabolite 4-OH-ifosfamide throughout and after the 90-min infusion in the peritoneal tumor nodules without increasing its systemic toxicity (Figure 6). This created a pharmacologically advantageous situation where a nor-mothermic administered IV drug became subject to the effect of the local hyperthermia in the peritoneal fluid and tumor nodule. Timing of intravenous chemotherapy (in-traoperative vs postoperative) is not pharmacokinetically neutral and as such emerges as a new pharmacokinetic variable.
TIMING OF IP CANCER CHEMOTHERAPY IN RELATION TO TIMING OF CRSIn the clinical application of IP chemotherapy in EOC patients, intervention can occur at four points in the time-line.
Induction IP and/or intravenous chemotherapy Induction IP and/or intravenous Chemotherapy is sug-gested as an option for reducing dissemination to the extra-abdominal space, testing the tumor biology and, for reducing the extent of small PC nodules and, theoreti-
148 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Transport of anticancer agent
Blood vessels
Outer layer:High drug level by direct exposure
Inner core: Drug concentration by microcirculation through systemic circulation
Intraperitoneal cavityvery high concentration of anticancer agents
Tumor tissue
Figure 5 Pharmacologic concept of bidirectional intravenous and intraperitoneal chemotherapy. Modified from Fujiwara et al[69].
100
10
1
0.1
Dru
g le
vels
(μg
/mL)
Tumor (IF)Plasma (IF)Tumor (OHIF)Plasma (OHIF)
0 30 60 90 120t /min
Figure 6 Comparison of ifosfamide and 4-hydroxyifosfamide concentra-tions in tumor nodules and in plasma during bidirectional intraoperative chemotherapy. OHIF: 4-OH-ifosfamide.
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

149 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
cally this approach, called neoadjuvant intraperitoneal and systemic chemotherapy (NIPS), may facilitate defini-tive CRS after initial exploratory laparoscopy or lapa-rotomy[73]. Radiological and clinical responses with NIPS have been reported by several groups[74-76]. However, al-though NIPS may reduce the tumor load to be addressed by CRS, it has several disadvantages. Adhesions from prior surgical interventions may interfere with adequate IP drug distribution and, as complete responses are un-usual, further cytoreduction-chemotherapy is necessary if the approach is to be curative. NIPS is reported to add to morbidity and mortality of further surgical treatment and, extensive fibrosis, as a response to chemotherapy, may occur and render judgments concerning the extent of PC difficult or impossible to assess[77].
Early postoperative intraperitoneal chemotherapyEarly postoperative intraperitoneal chemotherapy (EPIC) has some conceptual advantages. It is administered after CRS at the time of minimal residual tumor burden and, IP treatments initiated before wound healing occurs can minimize non-uniform drug distribution and eliminate residual cancer cell entrapment in postoperative fibrin deposits. The proper selection of chemotherapy agents based on pharmacologic principles suggests the use of cell-cycle specific drugs such as the taxanes. Most EPIC regimens are administered postoperatively (day 1 to day 4/5) through both an inflow catheter and outflow drains inserted at the time of CRS and, can be applied with or without HIPEC[78].
Long-term combined IP and systemic chemotherapySeveral phase Ⅲ trials demonstrated that intravenous plus IP chemotherapy improves survival in patients with optimally debulked stage Ⅲ ovarian cancer, compared to intravenous chemotherapy alone[34-36,69]. Some of these studies report a significant number of catheter-related problems and inability of the patient to complete the intended number of chemotherapy cycles This approach may alsobe used as ‘‘chemotherapeutic bridging’’ between incomplete initial surgery and definitive cytoreduction or second look surgery. This type of chemotherapy is an adjuvant and not a perioperative use of chemotherapy.
HIPECHIPEC has been explored in more than 40 studies in EOC. Unfortunately, most of these trials are small in number (< 50 patients) and have broad entry criteria[79]. Four randomized trials (NCT00426257, NCT01376752, NCT01539785 and NCT01091636) are currently explor-ing the role of HIPEC in the treatment of EOC. Failure analysis for CRS in EOC patients indicates recurrent can-cer occurs most frequently within the abdominal and pel-vic cavity. Although systemic metastases occur, treatment failures rarely occur in liver, lungs or, other systemic sites. In order to optimize the treatment of patients with PC, the greatest benefit will probably result from a combina-tion of the four treatment strategies.
CONTROVERSIES AND FUTURE DIRECTIONSDespite a growing evidence supporting the role of IP chemotherapy in the treatment of EOC, important con-troversies and questions remain to be answered. As the initial trials with IP chemotherapy in EOC were combined intravenous-IP chemotherapy regimens, some authors designate the observed effect to being the result of the dose density of the regimen, rather than the effect of the IP chemotherapy. Also, the current weekly schedules of intravenous taxanes as in JGOG 3016, MITO 7, GOG 0262 and ICON 8 have further raised the bar[80,81]. These improvements in systemic chemotherapy however do not annihilate the pharmacologic and clinical data supporting the superiority of a combined intravenous-IP approach. High grade EOC is characterized by an important overex-pression of vascular endothelial growth factor (VEGF). As a logical consequence VEGF inhibitors as bevacuz-imab are under investigation, both by the intravenous and IP route[82-84].
CONCLUSIONThe administration of perioperative IP chemotherapy in EOC patients with PC should be governed by pharma-cologic principles. Patients who have minimal residual disease as a result of optimal CRS are candidates for peri-operative chemotherapy by the IP and intravenous route. Hyperthermia of the IP chemotherapy solution might increase the cytotoxicity of the drug within the peritoneal cavity. Heating of the peritoneal and preperitoneal tis-sues will maximize the systemic chemotherapy effects on carcinomatosis, a phenomenon known as heat targeting. IP chemotherapy has become an important part of EOC treatment and should become a standard modality for prevention and treatment of a wide variety of cancers that involve the peritoneal surfaces.
REFERENCES1 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman
D. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90 [PMID: 21296855 DOI: 10.3322/caac.20107]
2 Young RC, Decker DG, Wharton JT, Piver MS, Sindelar WF, Edwards BK, Smith JP. Staging laparotomy in early ovar-ian cancer. JAMA 1983; 250: 3072-3076 [PMID: 6358558 DOI: 10.1001/jama.1983.03340220040030]
3 Heintz AP, Odicino F, Maisonneuve P, Quinn MA, Benedet JL, Creasman WT, Ngan HY, Pecorelli S, Beller U. Carci-noma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynaecol Obstet 2006; 95 Suppl 1: S161-S192 [PMID: 17161157 DOI: 10.1016/S0020-7292(06)60033-7]
4 Baron MA. Structure of the intestinal peritoneum in man. Am J Anat 1941; 69: 439-497 [DOI: 10.1002/aja.1000690305]
5 Dobbie JW. Ultrastructure and pathology of the peritoneum in peritoneal dialysis. In: Gokal R, Nolph KD, editors. The textbook of peritoneal dialysis. Dordrecht: Kluwer Academic Publishers, 1994: 17-45
6 Sugarbaker PH. Peritoneum as the first-line of defense in carcinomatosis. J Surg Oncol 2007; 95: 93-96 [PMID: 17262739
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

150 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
DOI: 10.1002/jso.20676]7 Oosterling SJ, van der Bij GJ, van Egmond M, van der Sijp
JR. Surgical trauma and peritoneal recurrence of colorectal carcinoma. Eur J Surg Oncol 2005; 31: 29-37 [PMID: 15642423 DOI: 10.1016/j.ejso.2004.10.005]
8 Flessner M, Henegar J, Bigler S, Genous L. Is the peritoneum a significant transport barrier in peritoneal dialysis? Perit Dial Int 2003; 23: 542-549 [PMID: 14703194]
9 de Lima Vazquez V, Stuart OA, Mohamed F, Sugarbaker PH. Extent of parietal peritonectomy does not change in-traperitoneal chemotherapy pharmacokinetics. Cancer Che-mother Pharmacol 2003; 52: 108-112 [PMID: 12759776 DOI: 10.1007/s00280-003-0626-8]
10 Jacquet P, Averbach A, Stephens AD, Stuart OA, Chang D, Sugarbaker PH. Heated intraoperative intraperitoneal mitomycin C and early postoperative intraperitoneal 5-fluo-rouracil: pharmacokinetic studies. Oncology 1998; 55: 130-138 [PMID: 9499187 DOI: 10.1159/000011847]
11 Sugarbaker PH, Van der Speeten K, Anthony Stuart O, Chang D. Impact of surgical and clinical factors on the phar-macology of intraperitoneal doxorubicin in 145 patients with peritoneal carcinomatosis. Eur J Surg Oncol 2011; 37: 719-726 [PMID: 21621952 DOI: 10.1016/j.ejso.2011.04.007]
12 Van der Speeten K, Stuart OA, Chang D, Mahteme H, Sug-arbaker PH. Changes induced by surgical and clinical factors in the pharmacology of intraperitoneal mitomycin C in 145 patients with peritoneal carcinomatosis. Cancer Chemother Pharmacol 2011; 68: 147-156 [PMID: 20857115 DOI: 10.1007/s00280-010-1460-4]
13 Stelin G, Rippe B. A phenomenological interpretation of the variation in dialysate volume with dwell time in CAPD. Kidney Int 1990; 38: 465-472 [PMID: 2232489 DOI: 10.1038/ki.1990.227]
14 Flessner MF. The transport barrier in intraperitoneal ther-apy. Am J Physiol Renal Physiol 2005; 288: F433-F442 [PMID: 15692055 DOI: 10.1152/ajprenal.00313.2004]
15 Dedrick RL, Myers CE, Bungay PM, DeVita VT. Pharma-cokinetic rationale for peritoneal drug administration in the treatment of ovarian cancer. Cancer Treat Rep 1978; 62: 1-11 [PMID: 626987]
16 Dedrick RL, Flessner MF. Pharmacokinetic problems in peri-toneal drug administration: tissue penetration and surface exposure. J Natl Cancer Inst 1997; 89: 480-487 [PMID: 9086004 DOI: 10.1093/jnci/89.7.480]
17 Dedrick RL, Flessner MF, Collins JM, Schultz JS. Is the peri-toneum a membrane? ASAIO J 1982; 5: 1-8
18 Los G, Mutsaers PH, Lenglet WJ, Baldew GS, McVie JG. Platinum distribution in intraperitoneal tumors after intra-peritoneal cisplatin treatment. Cancer Chemother Pharmacol 1990; 25: 389-394 [PMID: 2311166]
19 Los G, Verdegaal EM, Mutsaers PH, McVie JG. Penetration of carboplatin and cisplatin into rat peritoneal tumor nodules af-ter intraperitoneal chemotherapy. Cancer Chemother Pharmacol 1991; 28: 159-165 [PMID: 1855272 DOI: 10.1007/BF00685503]
20 Ozols RF, Locker GY, Doroshow JH, Grotzinger KR, Myers CE, Young RC. Pharmacokinetics of adriamycin and tissue penetration in murine ovarian cancer. Cancer Res 1979; 39: 3209-3214 [PMID: 455305]
21 Chang SJ, Bristow RE. Evolution of surgical treatment para-digms for advanced-stage ovarian cancer: redefining ‘opti-mal’ residual disease. Gynecol Oncol 2012; 125: 483-492 [PMID: 22366151 DOI: 10.1016/j.ygyno.2012.02.024]
22 Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influ-ence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 1992; 47: 159-166 [PMID: 1468693 DOI: 10.1016/0090-8258(92)90100-W]
23 Winter WE, Maxwell GL, Tian C, Carlson JW, Ozols RF, Rose PG, Markman M, Armstrong DK, Muggia F, McGuire
WP. Prognostic factors for stage III epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol 2007; 25: 3621-3627 [PMID: 17704411 DOI: 10.1200/JCO.2006.10.2517]
24 Winter WE, Maxwell GL, Tian C, Sundborg MJ, Rose GS, Rose PG, Rubin SC, Muggia F, McGuire WP. Tumor re-sidual after surgical cytoreduction in prediction of clinical outcome in stage IV epithelial ovarian cancer: a Gynecologic Oncology Group Study. J Clin Oncol 2008; 26: 83-89 [PMID: 18025437 DOI: 10.1200/JCO.2007.13.1953]
25 du Bois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the Arbeitsgemeinschaft Gynaekolo-gische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009; 115: 1234-1244 [PMID: 19189349 DOI: 10.1002/cncr.24149]
26 Tritton TR. Cell surface actions of adriamycin. Pharmacol Ther 1991; 49: 293-309 [PMID: 2052627 DOI: 10.1016/0163-7258(91)90060-Y]
27 Lane P, Vichi P, Bain DL, Tritton TR. Temperature depen-dence studies of adriamycin uptake and cytotoxicity. Cancer Res 1987; 47: 4038-4042 [PMID: 3607749]
28 Jacquet P, Averbach A, Stuart OA, Chang D, Sugarbaker PH. Hyperthermic intraperitoneal doxorubicin: pharmacokinet-ics, metabolism, and tissue distribution in a rat model. Can-cer Chemother Pharmacol 1998; 41: 147-154 [PMID: 9443628]
29 Johansen PB. Doxorubicin pharmacokinetics after intrave-nous and intraperitoneal administration in the nude mouse. Cancer Chemother Pharmacol 1981; 5: 267-270 [PMID: 7261254 DOI: 10.1007/BF00434396]
30 Ozols RF, Grotzinger KR, Fisher RI, Myers CE, Young RC. Kinetic characterization and response to chemotherapy in a transplantable murine ovarian cancer. Cancer Res 1979; 39: 3202-3208 [PMID: 455304]
31 Ozols RF, Young RC, Speyer JL, Sugarbaker PH, Greene R, Jenkins J, Myers CE. Phase I and pharmacological studies of adriamycin administered intraperitoneally to patients with ovarian cancer. Cancer Res 1982; 42: 4265-4269 [PMID: 7105021 DOI: 10.1097/00006254-198304000-00020]
32 Van der Speeten K, Stuart OA, Mahteme H, Sugarbaker PH. A pharmacologic analysis of intraoperative intracavitary cancer chemotherapy with doxorubicin. Cancer Chemother Pharmacol 2009; 63: 799-805 [PMID: 18654746 DOI: 10.1007/s00280-008-0800-0]
33 Cepeda V, Fuertes MA, Castilla J, Alonso C, Quevedo C, Pérez JM. Biochemical mechanisms of cisplatin cytotoxicity. Anticancer Agents Med Chem 2007; 7: 3-18 [PMID: 17266502 DOI: 10.2174/187152007779314044]
34 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
35 Markman M, Bundy BN, Alberts DS, Fowler JM, Clark-Pearson DL, Carson LF, Wadler S, Sickel J. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small-volume stage III ovarian carcinoma: an intergroup study of the Gyneco-logic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol 2001; 19: 1001-1007 [PMID: 11181662]
36 Alberts DS, Liu PY, Hannigan EV, O’Toole R, Williams SD, Young JA, Franklin EW, Clarke-Pearson DL, Malviya VK, DuBeshter B. Intraperitoneal cisplatin plus intravenous cyclophosphamide versus intravenous cisplatin plus intrave-nous cyclophosphamide for stage III ovarian cancer. N Engl J Med 1996; 335: 1950-1955 [PMID: 8960474 DOI: 10.1056/NEJM199612263352603]
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

151 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
37 Bakrin N, Cotte E, Golfier F, Gilly FN, Freyer G, Helm W, Glehen O, Bereder JM. Cytoreductive surgery and hyper-thermic intraperitoneal chemotherapy (HIPEC) for persistent and recurrent advanced ovarian carcinoma: a multicenter, prospective study of 246 patients. Ann Surg Oncol 2012; 19: 4052-4058 [PMID: 22825772 DOI: 10.1245/s10434-012-2510-4]
38 Helm CW. The role of hyperthermic intraperitoneal chemo-therapy (HIPEC) in ovarian cancer. Oncologist 2009; 14: 683-694 [PMID: 19608639 DOI: 10.1634/theoncologist.2008-0275]
39 Schem BC, Mella O, Dahl O. Thermochemotherapy with cisplatin or carboplatin in the BT4 rat glioma in vitro and in vivo. Int J Radiat Oncol Biol Phys 1992; 23: 109-114 [PMID: 1572808]
40 Los G, Mutsaers PH, van der Vijgh WJ, Baldew GS, de Graaf PW, McVie JG. Direct diffusion of cis-diamminedi chloroplatinum(II) in intraperitoneal rat tumors after intra-peritoneal chemotherapy: a comparison with systemic chemo-therapy. Cancer Res 1989; 49: 3380-3384 [PMID: 2720692]
41 van de Vaart PJ, van der Vange N, Zoetmulder FA, van Goethem AR, van Tellingen O, ten Bokkel Huinink WW, Beij-nen JH, Bartelink H, Begg AC. Intraperitoneal cisplatin with regional hyperthermia in advanced ovarian cancer: pharma-cokinetics and cisplatin-DNA adduct formation in patients and ovarian cancer cell lines. Eur J Cancer 1998; 34: 148-154 [PMID: 9624250 DOI: 10.1016/S0959-8049(97)00370-5]
42 Esquis P, Consolo D, Magnin G, Pointaire P, Moretto P, Ynsa MD, Beltramo JL, Drogoul C, Simonet M, Benoit L, Rat P, Chauffert B. High intra-abdominal pressure enhances the penetration and antitumor effect of intraperitoneal cisplatin on experimental peritoneal carcinomatosis. Ann Surg 2006; 244: 106-112 [PMID: 16794395]
43 Milczek T, Klasa-Mazurkiewicz D, Sznurkowski J, Emerich J. Regimens with intraperitoneal cisplatin plus intravenu-ous cyclophosphamide and intraperitoneal carboplatin plus intravenuous cyclophosphamide are equally effective in sec-ond line intraperitoneal chemotherapy for advanced ovarian cancer. Adv Med Sci 2012; 57: 46-50 [PMID: 22430042 DOI: 10.2478/v10039-012-0002-1]
44 Morgan MA, Sill MW, Fujiwara K, Greer B, Rubin SC, De-geest K, Yamada SD, Waggoner S, Coleman RL, Walker JL, Mannel RS. A phase I study with an expanded cohort to as-sess the feasibility of intraperitoneal carboplatin and intrave-nous paclitaxel in untreated ovarian, fallopian tube, and pri-mary peritoneal carcinoma: A Gynecologic Oncology Group study. Gynecol Oncol 2011; 121: 264-268 [PMID: 21277623 DOI: 10.1016/j.ygyno.2010.12.358]
45 Czejka M, Jäger W, Schüller J, Teherani D. [Pharmacokinet-ics of carboplatin after intraperitoneal administration]. Arch Pharm (Weinheim) 1991; 324: 183-184 [PMID: 1859253]
46 Jandial DD, Messer K, Farshchi-Heydari S, Pu M, Howell SB. Tumor platinum concentration following intraperitoneal administration of cisplatin versus carboplatin in an ovar-ian cancer model. Gynecol Oncol 2009; 115: 362-366 [PMID: 19775736 DOI: 10.1016/j.ygyno.2009.08.028]
47 Ceelen WP, Påhlman L, Mahteme H. Pharmacodynamic aspects of intraperitoneal cytotoxic therapy. Cancer Treat Res 2007; 134: 195-214 [PMID: 17633055 DOI: 10.1007/978-0-387-48993-3_12]
48 Sugarbaker PH, Mora JT, Carmignani P, Stuart OA, Yoo D. Update on chemotherapeutic agents utilized for perioperative intraperitoneal chemotherapy. Oncologist 2005; 10: 112-122 [PMID: 15709213 DOI: 10.1634/theoncologist.10-2-112]
49 Mohamed F, Sugarbaker PH. Intraperitoneal taxanes. Surg Oncol Clin N Am 2003; 12: 825-833 [PMID: 14567034 DOI: 10.1016/S1055-3207(03)00038-3]
50 Rietbroek RC, Katschinski DM, Reijers MH, Robins HI, Geerdink A, Tutsch K, d’Oleire F, Haveman J. Lack of ther-mal enhancement for taxanes in vitro. Int J Hyperthermia 1997; 13: 525-533 [PMID: 9354937]
51 Schrump DS, Zhai S, Nguyen DM, Weiser TS, Fisher BA,
Terrill RE, Flynn BM, Duray PH, Figg WD. Pharmacokinetics of paclitaxel administered by hyperthermic retrograde isolat-ed lung perfusion techniques. J Thorac Cardiovasc Surg 2002; 123: 686-694 [PMID: 11986596 DOI: 10.1067/mtc.2002.120713]
52 Cividalli A, Cruciani G, Livdi E, Pasqualetti P, Tirindelli Danesi D. Hyperthermia enhances the response of paclitaxel and radiation in a mouse adenocarcinoma. Int J Radiat Oncol Biol Phys 1999; 44: 407-412 [PMID: 10760437 DOI: 10.1016/S0360-3016(99)00008-5]
53 Mohamed F, Stuart OA, Glehen O, Urano M, Sugarbaker PH. Docetaxel and hyperthermia: factors that modify thermal enhancement. J Surg Oncol 2004; 88: 14-20 [PMID: 15384091 DOI: 10.1002/jso.20117]
54 Bouquet W, Ceelen W, Adriaens E, Almeida A, Quinten T, De Vos F, Pattyn P, Peeters M, Remon JP, Vervaet C. In vivo toxic-ity and bioavailability of Taxol and a paclitaxel/beta-cyclodex-trin formulation in a rat model during HIPEC. Ann Surg Oncol 2010; 17: 2510-2517 [PMID: 20339948 DOI: 10.1245/s10434-010-1028-x]
55 Sticca RP, Dach BW. Rationale for hyperthermia with intra-operative intraperitoneal chemotherapy agents. Surg Oncol Clin N Am 2003; 12: 689-701 [PMID: 14567025 DOI: 10.1016/S1055-3207(03)00029-2]
56 Dahl O, Dalene R, Schem BC, Mella O. Status of clinical hy-perthermia. Acta Oncol 1999; 38: 863-873 [PMID: 10606416 DOI: 10.1080/028418699432554]
57 Sugarbaker PH. Laboratory and clinical basis for hyper-thermia as a component of intracavitary chemotherapy. Int J Hyperthermia 2007; 23: 431-442 [PMID: 17701534 DOI: 10.1080/02656730701455318]
58 Lepock JR. How do cells respond to their thermal environ-ment? Int J Hyperthermia 2005; 21: 681-687 [PMID: 16338849 DOI: 10.1080/02656730500307298]
59 Kampinga HH. Cell biological effects of hyperthermia alone or combined with radiation or drugs: a short introduction to newcomers in the field. Int J Hyperthermia 2006; 22: 191-196 [PMID: 16754338 DOI: 10.1080/02656730500532028]
60 Hahn GM, Braun J, Har-Kedar I. Thermochemotherapy: syn-ergism between hyperthermia (42-43 degrees) and adriamy-cin (of bleomycin) in mammalian cell inactivation. Proc Natl Acad Sci USA 1975; 72: 937-940 [PMID: 48253 DOI: 10.1073/pnas.72.3.937]
61 Kusumoto T, Holden SA, Ara G, Teicher BA. Hyperthermia and platinum complexes: time between treatments and synergy in vitro and in vivo. Int J Hyperthermia 1995; 11: 575-586 [PMID: 7594810]
62 Barlogie B, Corry PM, Drewinko B. In vitro thermochemother-apy of human colon cancer cells with cis-dichlorodiammine platinum(II) and mitomycin C. Cancer Res 1980; 40: 1165-1168 [PMID: 7188883]
63 Urano M, Ling CC. Thermal enhancement of melphalan and ox-aliplatin cytotoxicity in vitro. Int J Hyperthermia 2002; 18: 307-315 [PMID: 12079586]
64 Mohamed F, Marchettini P, Stuart OA, Urano M, Sugarbaker PH. Thermal enhancement of new chemotherapeutic agents at moderate hyperthermia. Ann Surg Oncol 2003; 10: 463-468 [PMID: 12734097 DOI: 10.1245/ASO.2003.08.006]
65 Young JS, Lumsden CE, Stalker AL. The significance of the tissue pressure of normal testicular and of neoplastic (Brown-Pearce carcinoma) tissue in the rabbit. J Pathol Bacteriol 1950; 62: 313-333 [PMID: 14784896 DOI: 10.1002/path.1700620303]
66 Boucher Y, Baxter LT, Jain RK. Interstitial pressure gradients in tissue-isolated and subcutaneous tumors: implications for therapy. Cancer Res 1990; 50: 4478-4484 [PMID: 2369726]
67 Leunig M, Goetz AE, Dellian M, Zetterer G, Gamarra F, Jain RK, Messmer K. Interstitial fluid pressure in solid tumors following hyperthermia: possible correlation with therapeu-tic response. Cancer Res 1992; 52: 487-490 [PMID: 1728421]
68 Klaver YL, Hendriks T, Lomme RM, Rutten HJ, Bleichrodt RP, de Hingh IH. Hyperthermia and intraperitoneal che-
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

152 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
motherapy for the treatment of peritoneal carcinomatosis: an experimental study. Ann Surg 2011; 254: 125-130 [PMID: 21502859 DOI: 10.1097/SLA.0b013e3182197102]
69 Fujiwara K, Armstrong D, Morgan M, Markman M. Prin-ciples and practice of intraperitoneal chemotherapy for ovarian cancer. Int J Gynecol Cancer 2007; 17: 1-20 [PMID: 17291226 DOI: 10.1111/j.1525-1438.2007.00809.x]
70 Elias D, Bonnay M, Puizillou JM, Antoun S, Demirdjian S, El OA, Pignon JP, Drouard-Troalen L, Ouellet JF, Ducreux M. Heated intra-operative intraperitoneal oxaliplatin after complete resection of peritoneal carcinomatosis: pharmaco-kinetics and tissue distribution. Ann Oncol 2002; 13: 267-272 [PMID: 11886004 DOI: 10.1093/annonc/mdf019]
71 Van der Speeten K, Stuart OA, Mahteme H, Sugarbaker PH. Pharmacokinetic study of perioperative intravenous Ifos-famide. Int J Surg Oncol 2011; 2011: 185092 [PMID: 22312496 DOI: 10.1155/2011/185092]
72 Zylberberg B, Dormont D, Madelenat P, Daraï E. First-line intraperitoneal cisplatin-paclitaxel and intravenous ifos-famide in Stage IIIc ovarian epithelial cancer. Eur J Gynaecol Oncol 2004; 25: 327-332 [PMID: 15171311]
73 Yonemura Y, Bandou E, Sawa T, Yoshimitsu Y, Endou Y, Sasaki T, Sugarbaker PH. Neoadjuvant treatment of gastric cancer with peritoneal dissemination. Eur J Surg Oncol 2006; 32: 661-665 [PMID: 16621433 DOI: 10.1016/j.ejso.2006.03.007]
74 Sugarbaker PH. Treatment of peritoneal carcinomatosis from colon or appendiceal cancer with induction intraperito-neal chemotherapy. Cancer Treat Res 1996; 82: 317-325 [PMID: 8849959]
75 Zylberberg B, Dormont D, Janklewicz S, Darai E, Bretel JJ, Poncelet C, Guillet JL, Madelenat P. Response to neo-adju-vant intraperitoneal and intravenous immunochemotherapy followed by interval secondary cytoreduction in stage IIIc ovarian cancer. Eur J Gynaecol Oncol 2001; 22: 40-45 [PMID: 11321492]
76 Muñoz-Casares FC, Rufián S, Arjona-Sánchez Á, Rubio MJ, Díaz R, Casado Á, Naranjo Á, Díaz-Iglesias CJ, Ortega R, Muñoz-Villanueva MC, Muntané J, Aranda E. Neoadju-vant intraperitoneal chemotherapy with paclitaxel for the radical surgical treatment of peritoneal carcinomatosis in ovarian cancer: a prospective pilot study. Cancer Chemother Pharmacol 2011; 68: 267-274 [PMID: 21499894 DOI: 10.1007/s00280-011-1646-4]
77 Esquivel J, Vidal-Jove J, Steves MA, Sugarbaker PH. Morbid-ity and mortality of cytoreductive surgery and intraperitoneal chemotherapy. Surgery 1993; 113: 631-636 [PMID: 8506520]
78 Xanthoulis A, Mirelis C, Markakidis S, Bougioukas I, Beki-aridou K, Tsalkidou E, Zafeiropoulos G, Tentes AA. Com-plete cytoreduction combined with early postoperative intra-peritoneal chemotherapy for ovarian carcinosarcoma. Report of two cases. Gynecol Obstet Invest 2006; 62: 100-102 [PMID: 16645301]
79 Herzog TJ. The role of heated intraperitoneal chemother-apy (HIPEC) in ovarian cancer: hope or hoax? Ann Surg Oncol 2012; 19: 3998-4000 [PMID: 22833000 DOI: 10.1245/s10434-012-2521-1]
80 Katsumata N, Yasuda M, Takahashi F, Isonishi S, Jobo T, Aoki D, Tsuda H, Sugiyama T, Kodama S, Kimura E, Ochiai K, Noda K. Dose-dense paclitaxel once a week in combina-tion with carboplatin every 3 weeks for advanced ovarian cancer: a phase 3, open-label, randomised controlled trial. Lancet 2009; 374: 1331-1338 [PMID: 19767092 DOI: 10.1016/S0140-6736(09)61157-0]
81 Bookman MA. First-line chemotherapy in epithelial ovarian cancer. Clin Obstet Gynecol 2012; 55: 96-113 [PMID: 22343232 DOI: 10.1097/GRF.0b013e31824b45da]
82 Perren TJ, Swart AM, Pfisterer J, Ledermann JA, Pujade-Lauraine E, Kristensen G, Carey MS, Beale P, Cervantes A, Kurzeder C, du Bois A, Sehouli J, Kimmig R, Stähle A, Col-linson F, Essapen S, Gourley C, Lortholary A, Selle F, Mirza MR, Leminen A, Plante M, Stark D, Qian W, Parmar MK, Oza AM. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med 2011; 365: 2484-2496 [PMID: 22204725 DOI: 10.1056/NEJMoa1103799]
83 Burger RA, Brady MF, Bookman MA, Fleming GF, Monk BJ, Huang H, Mannel RS, Homesley HD, Fowler J, Greer BE, Boente M, Birrer MJ, Liang SX. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N Engl J Med 2011; 365: 2473-2483 [PMID: 22204724 DOI: 10.1056/NEJ-Moa1104390]
84 Rein DT, Volkmer AK, Volkmer J, Beyer IM, Janni W, Fleisch MC, Welter AK, Bauerschlag D, Schöndorf T, Bre-idenbach M. Systemic administration of bevacizumab pro-longs survival in an in vivo model of platinum pre-treated ovarian cancer. Oncol Lett 2012; 3: 530-534 [PMID: 22740945 DOI: 10.3892/ol.2012.553]
P- Reviewers: Gardner-Mutch D, Jain A S- Editor: Zhai HH L- Editor: A E- Editor: Zheng XM
Van der Speeten K et al . Current role of intraperitoneal chemotherapy

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.153
World J Obstet Gynecol 2013 November 10; 2(4): 153-166ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Neoadjuvant chemotherapy and cytoreductive surgery in epithelial ovarian cancer
Siriwan Tangjitgamol, Jitti Hanprasertpong, Marta Cubelli, Claudio Zamagni
Siriwan Tangjitgamol, Gynecologic Oncology Unit, Department of Obstetrics and Gynecology, Faculty of Medicine Vajira Hospital, University of Bangkok Metropolis, Bangkok 10300, ThailandJitti Hanprasertpong, Division of Gynecologic Oncology, De-partment of Obstetrics and Gynecology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla 90110, ThailandMarta Cubelli, Claudio Zamagni, Medical Oncology Unit, Ad-darii Institute of Oncology, Policlinico S. Orsola-Malpighi Uni-versity Hospital, 40100 Bologna, ItalyAuthor contributions: Tangjitgamol S, Hanprasertpong J, Cubelli M and Claudio Z outlined the topics of discussion, per-formed literature review, wrote portions of the initial draft, re-viewed and revised the subsequent drafts, and compiled the final manuscript; all authors reviewed, revised, compiled the manu-script, and approved the final manuscript.Correspondence to: Siriwan Tangjitgamol, MD, Gyneco-logic Oncology Unit, Department of Obstetrics and Gynecology, Faculty of Medicine Vajira Hospital, University of Bangkok Me-tropolis, 681 Samsen Road, Dusit, Bangkok 10300, Thailand. [email protected]: +66-2-2433666 Fax: +66-2-2437907Received: December 13, 2012 Revised: January 13, 2013Accepted: February 5, 2013Published online: November 10, 2013
AbstractOvarian cancer is one of the leading causes of death among gynecological cancers. This is because the ma-jority of patients present with advanced stage disease. Primary debulking surgery (PDS) followed by adjuvant chemotherapy is still a mainstay of treatment. An optimal surgery, which is currently defined by leaving no gross residual tumor, is the goal of PDS. The extent of disease as well as the operative setting, including the surgeon’s skill, influences the likelihood of successful debulking. With extensive disease and a poor chance of optimal surgery or high morbidity anticipated, neoadjuvant che-motherapy (NACT) prior to primary surgery is an op-tion. Secondary surgery after induction chemotherapy is termed interval debulking surgery (IDS). Delayed PDS
or IDS is offered to patients who show some clinical re-sponse and are without progressive disease. NACT or IDS has become more established in clinical practice and there are numerous publications regarding its advantages and disadvantages. However, data on survival are limited and inconsistent. Only one large randomized trial could demonstrate that NACT was not inferior to PDS while the few randomized trials on IDS had inconsistent results. Without a definite benefit of NACT prior to surgery over PDS, one must carefully weigh the chances of safe and successful PDS against the morbidity and risks of sub-optimal surgery. Appropriate selection of a patient to undergo PDS followed by chemotherapy or, preferably, to have NACT prior to surgery is very important. Some clinical characteristics from physical examination, serum tumor markers and/or findings from imaging studies may be predictive of resectability. However, no specific fea-tures have been consistently identified in the literature. This article will address the clinical data on prediction of surgical outcomes, the role of NACT, and the role of IDS.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Advanced stage ovarian cancer; Neoadju-vant chemotherapy; Interval debulking surgery
Core tip: Neoadjuvant chemotherapy (NACT) is an option when the primary surgery is expected to be impossible or suboptimal, or when high morbidity is anticipated. Delayed primary surgery or interval debulking surgery (IDS) is performed in patients who show some clinical response to neoadjuvant or induction chemotherapy. Preoperative clinical data to predict surgical outcomes and selection criteria for primary surgery followed by ad-juvant chemotherapy or for NACT followed by IDS will be discussed in this chapter.
Tangjitgamol S, Hanprasertpong J, Cubelli M, Zamagni C. Neo-adjuvant chemotherapy and cytoreductive surgery in epithelial
153 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
TOPIC HIGHLIGHT
Federico Coccolini, MD, Series Editor

Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer
ovarian cancer. World J Obstet Gynecol 2013; 2(4): 153-166 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/153.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.153
INTRODUCTIONBecause of the lack of effective screening procedures to detect early stage ovarian cancer, the majority of patients present with advanced disease (stage Ⅲ-Ⅳ), resulting in a poor overall survival. The current standard management of patients with advanced ovarian cancer (AOC) is “de-bulking or cytoreductive surgery” followed by platinum-based chemotherapy. The aim of primary debulking surgery (PDS) is to remove as much cancer as possible, since the amount of residual tumor is one of the most important prognostic factors for survival[1,2]. When the cytoreduction is successful, the term “optimal debulking surgery” is applied. The definition of optimal debulking surgery has changed over the past 30 years from a residual tumor sized not more than 1-2 cm to no macroscopic disease[2-4]. However, it is not always possible to debulk tumors in the pelvis and upper abdomen optimally, es-pecially when they have invaded the neighboring viscera. To achieve the goal of no residual disease and improve disease specific survival, “ultra” radical surgical techniques have been developed[5]. However, data on quality of life are not available and the documentation of adverse events is incomplete. Furthermore, many other factors must be considered, such as the patient’s status or medical contra-indications, morbidity-related treatment, and the reluc-tance or expertise of some surgeons/centers to practice such an aggressive procedure[4,6-10].
When PDS is not possible or is predicted to be un-successful, or where morbidity might be excessively high, chemotherapy prior to PDS is an option; so called “neo-adjuvant chemotherapy” (NACT)[10]. The chemotherapy is given after the diagnosis of ovarian cancer, preferably by tissue biopsy. On the other hand, when PDS is in-complete and there is a bulky residual tumor, “induction chemotherapy” is usually given for 2-3 cycles to reduce tumor size. Secondary surgery or so called “interval de-bulking surgery” (IDS) is considered before continuing more cycles of chemotherapy when there is no evidence of progressive diseases[11].
PREDICTION OF OPTIMAL SURGICAL OUTCOME The achievement of optimal surgery varies according to the extent of the disease itself and the ability of the surgical team to perform the operation. These factors must be taken into consideration in estimating whether the PDS will be possible and successful. The evaluation should be as accurate as possible, in order to avoid a fu-tile procedure or excessive morbidity and, on the other hand, to offer patients the best opportunity for optimal cytoreduction. The estimation should be based on the
combination of a number of factors: clinical characteris-tics or findings from physical examination, imaging stud-ies, serum markers, or laparoscopic findings.
Serum markersSome biological markers have been studied in relation to the stage of disease, resectability, and survival. The elevation of these markers is frequently reported in di-rect association with advanced stage diseases, suboptimal resection of ovarian cancer or decreased survival. Never-theless, different reports show variation in their diagnos-tic performance and levels of significance varied.
Inflammatory markers: Recently, the relationship be-tween cancer development and inflammation has been recognized. This relationship is explained through an inflammatory process elicited by cancer cells. Cancer cells can trigger the host inflammatory response with the release of neutrophil-releasing inflammatory cytokines, leukocytic and other phagocytic mediators. These sub-stances induce damage to cellular DNA, inhibit apoptosis and promote angiogenesis around cancer area. This will ultimately result in tumor growth, progression, and me-tastases[12-14]. Similarly, platelets can release growth factors such as platelet-derived growth factor, platelet factor 4, transforming growth factor β, vascular endothelial growth factor[15-17] and thrombospondin, which function as po-tent mitogens or as adhesive glycoproteins for various cell types including ovarian surface epithelium[18,19]. These growth factors can stimulate ovarian tumor cell prolifera-tion and adhesion to other cells, leading to tumor growth and metastases, respectively[20].
Elevation of neutrophils[21], platelets[22-24], lymphocytes as well as of the neutrophil to lymphocyte ratio (NLR)[25,26], and the platelet to lymphocyte ratio (PLR)[27,28] were found to be associated with unfavorable clinico-pathologic fea-tures in ovarian cancer. In many early studies thrombo-cytosis was found to be associated with more advanced disease, inoperable cancer, and to be an independent prognostic factor for survival of epithelial ovarian cancer patients[22-24,28]. A possible prognostic role of NLR was also studied, but with inconsistent results[25,26,28]. One study found that elevated NLR (> 2.6) and cancer antigen (CA) 125 correlated with poor survival[26] while a second study failed to demonstrate any such association and only found significant association between elevated pre-operative NLR and advanced stage or suboptimal surgery[25]. Other studies also explored the role of PLR and found that it functioned better than platelet count[28] or NLR[27,28] as a prognostic factor for poor survival and other unfavorable clinico-pathological factors, such as, advanced stage and suboptimal residual disease.
Despite the association of elevated inflammatory markers with survival and suboptimal surgery, data on the levels of significance are inconsistent among stud-ies. Different number of patients and non homogeneous patients’ characteristic (e.g., stage of disease and result of primary surgery) among the series might explain these differences. Larger studies and more homogeneous pop-
154 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

ulations are needed to validate the role of inflammatory markers as predictors for suboptimal surgery.
CA 125: Serum CA 125 is the most widely used biologi-cal marker in ovarian cancer and is abnormally high in more than 90% of patients with AOC[29]. Hence, many studies have attempted to find a reliable cut-off level of CA 125 which could predict the optimal resection of ovarian cancer.
However, the results are inconsistent among studies and it is not possible to define a single reliable cut-off value of CA 125 to predict optimal surgery (Table 1)[30-46]. Some reasons can explain these unsatisfactory results. First, all of these studies were retrospective in nature. Second, the number of patients in each study varied from less than 50 to over 400. Third, the rates of optimal cytoreduction ranged from less than 50% to 80% in the various centers. Fourth, the median value of CA 125 in the studies varied significantly. Most probably, these differences reflect the lack of homogeneity of tumor stages and in the extent of tumor burden, as well as the different criteria for operabil-ity adopted in the different centers.
Since the level of CA 125 is directly related to the stage of disease and to the amount of tumor burden, preop-erative CA 125 levels in studies with a higher number of optimal cytoreductions should, theoretically, be lower than those in studies with more unresected tumors. Nev-ertheless, some studies suggest that the aggressiveness of the surgical procedures may be a confounding factor that affects the rates of optimal cytoreduction. One mul-ticenter study by Gemer et al[35] reviewed records of 424 patients with AOC and found that clinical applicability
of CA 125 for predicting suboptimal surgery was limited. The authors found only a 57% rate of optimal surgery. Although the median CA 125 serum levels in patients with optimally cytoreduced tumor was significantly lower than that in suboptimally debulked cases (304 U/mL vs 863 U/mL), the diagnostic accuracy of CA 125 as pre-dictor of optimal debulking was only 62% with the best cut-off identified (400 U/mL). Another large study by Vorgias et al[46] also found significant association between CA 125 levels and surgical results in 426 patients: 84% of patients with CA 125 < 500 U/mL achieved opti-mal cytoreduction compared to only 15% of those with higher CA 125 levels. However, this study reported only a 42% overall rate of optimal cytoreduction. Once again, this might be the result of a less extensive surgical effort for peritoneal carcinomatosis and for metastatic lymph-nodes. The results from 2 other studies by the same groups of authors further demonstrated the importance of the surgical aggressiveness. In their first report in early 2000s, Chi et al[41] reported a 45% optimal cytoreduction in 100 AOC patients. The rate of optimal cytoreduction was significantly higher in patients with pre-operative CA 125 ≤ 500 U/mL than those with higher level: 73% vs 22%[41]. However, their subsequent study in 277 patients with similar characteristics demonstrated that the patients with a higher CA 125 level required more extensive up-per abdominal surgery to achieve optimal surgery (< 1 cm residual tumor) compared to those with a lower CA 125 level, 50% vs 27%[40]. There was no CA 125 threshold which could predict the surgical outcome. Of note, their latter study reported a higher rate of cytoreduction (80%). These studies may be affected by selection bias, a com-
155 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Studies of cancer antigen 125 for predicting the result of surgery in epithelial ovarian cancer
First author, year n Preoperative CA 125 (U/mL) Optimal surgery3
Sensitivity Specificity PPV NPV
Median Cut-off
Not clinically useful1
Gemer et al[30], 2001 40 341 500 60% 62% 83% 71% 77% Cooper et al[31], 2002 112 893 500 58% 49% 77% 74% 52% Memarzadeh et al[32], 2003 99 - 912 73% 58% 54% 78% 31% Rossi et al[33], 2004 822 1351 500 40% 40% 64% - - Alcázar et al[34], 2004 67 730 620 48% 60% - - - Gemer et al[35], 2005 424 495 400 57% 69% 57% 55% 71% Everett et al[36], 2005 56 NA 500 52% - - - - Barlow et al[37], 2006 164 364 500 47% 66% 59% 64% 36% Gilani et al[38], 2007 90 500 500 47% 68% 62% 64% 35% Arits et al[39], 2008 96 625 330 43% 80% 42% - - Chi et al[40], 2009 277 731 500 80% - - - -Probably clinically useful1
Chi et al[41], 2000 100 819 500 45% 78% 73% 78% 73% Saygili et al[42], 2002 92 494 500 52% 73% 77% 75% 75% Obeidat et al[43], 2004 40 467 500 55% 72% 73% 68% 76% Eltabbakh et al[44], 2004 72 680 500 81% 73% 74% - - Brockbank et al[45], 2004 77 397 586 68% 80% 89% 86% 80% Vorgias et al[46], 2009 426 650 500 42% 79% 90% 85% 85%
1Studies of not clinical useful and probably useful were arranged according to the comments of the authors in each study; 2Diagnostic functions of cancer antigen (CA) 125 in the study were of the whole group (22% early stages and 78% advanced stages) while the numbers of patients (n) in other studies were of stage Ⅲ or stage Ⅲ-Ⅳ disease; 3All studies defined residual disease ≤ 1 cm as optimal surgery. NPV: Negative predictive value; PPV: Positive predictive value; NA: Not available.
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

mon phenomenon in retrospective and in non-random-ized prospective trials
It is therefore difficult to make any conclusion regard-ing the possible role of CA 125 in determining resectabil-ity in advanced ovarian cancer patients. One systematic review by Kang et al[47] determined the ability of pretreat-ment CA 125 level to predict optimal cytoreduction in AOC. The authors identified 122 articles in which 15 studies including their own series met the inclusion crite-ria, and 2192 patients were analyzed in the meta-analysis. The pooled optimal cytoreduction rate and the mean of median CA 125 levels were 53.7% and 580 U/mL, re-spectively. The authors did not find any significant hetero-geneity factor (year of publication, numbers of patients, median CA 125 levels, percentage of stage Ⅳ disease, or rate of optimal cytoreduction) influencing the analysis. The diagnostic performance of CA 125 in predicting sub-optimal cytoreduction was analyzed at 3 cut-off levels of 500, 1000 and 1500 U/mL. A direct association between CA 125 levels and likelihood of suboptimal cytoreduction was found. Increasing specificity and odds ratios along with decreasing sensitivity were observed with higher CA 125 cut-off levels. At a cut-off level of 500 U/mL, the odds ratio was 3.69 (95%CI: 2.02-6.73). The authors also demonstrated that the predictive role of CA 125 was not affected by the rate of optimal cytoreduction. The odds ratios were not different among the studies which had optimal cytoreduction rate ≥ 50% vs < 50%: 4.0 vs 4.5, respectively. Against all the odds, this might suggest that the effort of a surgeon probably has little to do with the accuracy of CA 125 in predicting the result of PDS. It should be noted that, despite the strong association of CA 125 and risk of suboptimal surgery, the meta-analysis showed that CA 125 showed only a low positive likeli-hood ratio and could not accurately predict the optimal or suboptimal surgery at any cut-off level[47].
From these retrospective studies and from the system-atic review, we can conclude that although pre-operative serum CA 125 level is a reliable predictor for the extent of disease, it has limited accuracy in predicting a success-ful surgical outcome. The sensitivity and specificity in the various studies ranged from 40% to 80% and from 40% to 90%, respectively (Table 1). With a positive predictive value (PPV) of 55%-86% (approximate mean of 73%) an unsuccessful (unnecessary) surgical exploration would be performed in 27% of patients (false negative diagnosis). On the other hand, the negative predictive values (NPV) ranged from 31%-85% (approximate mean of 62%), sug-gesting that 38% of patients would be falsely interpreted to be inoperable and would miss their chance to undergo a successful operation. Hence, one should not use CA 125 as a single criterion to determine patient manage-ment: primary surgery vs NACT. Other clinical features, such as ascites or imaging studies, may add value to CA 125 in predicting an optimal cytoreduction. Neverthe-less, a high level of CA 125 should warn a surgeon that aggressive surgery will probably be required to achieve an optimal resection. This will ultimately aid in planning
the setting or level of the hospital where the operation should be performed.
Imaging studiesImaging studies are very useful to evaluate the location, nature, and extent of disease. However, some common pitfalls are encountered depending on the location and size of the lesions. Aside from having an important role in the assessment of tumor response during or after the courses chemotherapy, imaging can be used to evaluate the extent or location of disease preoperatively to estimate whether the surgery can be achieved with minimal mor-bidity and with maximal outcome. An imaging study can be an indicator alone or in combination with other clinical features, such as CA 125, in trying to improve the predic-tive role of each.
Computed tomography: Computed tomography (CT) scan is a commonly used imaging tool in AOC. Many criteria have been used to select the patients who were unlikely to have a successful surgical outcome and NACT may be a better option. These include carcinomatosis, pelvic sidewall infiltration, ascites, and extensive upper abdominal disease over diaphragm, liver, porta hepa-tis, mesentery, and bowel[48]. Using spiral CT scan, the reported sensitivity in detecting peritoneal metastases, mesenteric, and diaphragmatic surfaces ranged from 85% to 93%[49,50]. This technique yielded improved sensitivity over previous reports that used 10-mm slice CT scan-ning, which may miss subcentimetric peritoneal nodules or plague-like lesions[51].
One of the earliest studies of CT scan for predicting optimal surgery in 42 ovarian cancer patients was reported by Nelson et al[52]. The authors found that CT scan could detect the presence of ascites, mesenteric, and omental disease. However, it was poor in detecting liver involve-ment, omental attachment to the spleen, gallbladder fossa disease, and peritoneal nodules smaller than 2 cm. The overall optimal cytoreduction rate was 69%. The sensitivity was as high as 92% with specificity of 79%, while the PPV and NPV were 67% and 96%, respectively. Notably, 8 of the 42 patients had stage Ⅰ/Ⅱ disease. In patients with ad-vanced disease the specificity decreased from 79% to 71%.
A larger study by Salani et al[53] who included only stage Ⅲc/Ⅳ disease reported 92% overall rate of op-timal cytoreduction in 180 ovarian cancer patients. The authors found varying rates of optimal surgery according to the location and number of lesions identified preoper-atively: 91% optimal debulking in the presence of ascites or carcinomatosis, 94% in the presence of lesions over the diaphragm, 85% or 88% with spleen or liver involve-ment, and only 75% for lesions involving the porta hepa-tis or the lymph-nodes above the renal vessels. The rates of optimal debulking according to the number of lesions were: 95% for disease involving 1 site, 94% for 2 sites, and 82%, 93%, 80% for 3, 4, and 5 sites, respectively. The authors concluded that none of these features absolutely excluded the possibility of optimal resection.
156 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

Other studies have used several radiographic find-ings in combination to develop a score model to predict surgical outcomes. Dowdy et al[54] reported the role of CT scans in predicting suboptimal cytoreductive surgery in 87 patients with stage Ⅲ/Ⅳ ovarian cancer. The optimal cytoreduction rate was 71%. Among many radiographic criteria from CT scans, only diffuse peritoneal thickening was independently associated with suboptimal resection. Using this single criterion, the PPV and NPV were 57% and 85%, respectively. The PPV increased to 68% when ascites was added as a feature, and 79% with added asci-tes and diaphragmatic diseases. Interestingly, the authors made specific note that the predictive ability of CT crite-ria was dependent on other factors, especially the effort of the surgeon to perform extensive surgery[54]. Another study by Meyer et al[55] used a 10-score model composed of a score of 0 to 2 for a disease at each site of the fol-lowing: omentum, liver, para-aortic nodes, diaphragm, and small-bowel mesentery. The rate of optimal cytoreduction or of having residual diseases ≤ 2 cm was 57%. Score ≥ 3 had sensitivity of 58% and a specificity of 100% in pre-dicting residual disease > 2 cm. The area under the curve (AUC) was 0.94. Of note, nearly 40% of the patients in this study had early stage disease, and again, this may have led to overestimation of the role of pre-operative CT scan. Another study by Fujwara et al[56] created two models using various features of diffuse peritoneal thickening, infrarenal para-aortic or pelvic lymph node involvement, a bowel encasement tumor or bowel mesenteries or omen-tal cake ≥ 2 cm, and ascites fluid. The two models using either 4 or 6 disease sites as criterion yielded greater than 90% accuracy in predicting suboptimal surgery.
Combined CT scan and clinical data: Some studies have evaluated the combined use of CT scans with clini-cal data, including CA 125, to improve the doctor’s ability to predict the results of surgery. However, the results of these attempts to predict optimal cytoreduction were in-consistent[7,55,57-61].
As mentioned earlier, Meyer et al[55] used a 10-point scoring system from CT scan features and found an AUC of 0.94 in predicting a suboptimal surgery. The AUCs were not improved when the authors added age, ascites, or CA 125 to their index, with AUC scores of 0.91, 0.93, and 0.97, respectively[55]. A study by Byrom et al[57] evalu-ated CT scan findings in 51 ovarian cancers (49% having residual diseases). The sensitivity and specificity of the CT scan using a full model (the 4 CT features of ascites, omental cake, mesenteric disease, and diaphragmatic de-posits) or a reduced model (only omental cake and mesen-teric disease) in predicting residual disease were the same: 88% sensitivity, 98% specificity, 95% PPV, and 94% NPV. The specificity and PPV, at 98% and 95% respectively, were not improved by the addition of age and CA 125.
In addition to the chronological age of an individual, the performance status of a patient may affect the treat-ment outcome. One study by Aletti et al[7] examined the resectability of ovarian cancer by considering disease fac-
tors as well as patient status and the effort of the surgeon. Data taken into account were age, performance status, CA 125, ascites volume, carcinomatosis, diaphragmatic or mesenteric involvement, and the surgeon category (radical surgery in less than vs more than 50% of cases). Only per-formance status, carcinomatosis, and surgeon were inde-pendently associated with surgical outcome. The authors focussed on the surgical effort of the surgeon. Among the patients with high-risk factors of poorer performance status or with carcinomatosis, the rates of optimal cytore-duction varied from 42% to 67% depending on the will-ingness of the operating surgeons to perform aggressive surgery[7].
Another study by Bristow et al[58] included as many as 25 radiographic features from CT scans as well as clinical features including performance status and pre-operative serum CA 125 to predict optimal cytoreduction in 41 ovarian cancer patients. Based on the statistical probabil-ity of each factor in predicting cytoreductive outcome, performance status and 13 imaging features were selected for the final assessment model. Performance status ≥ 2, peritoneal thickening, ≥ 2 cm tumor implants on the peri-toneum, small or large bowel mesentery, ≥ 1 cm supra-renal para-aortic lymph nodes, omental extension (spleen, stomach, or lesser sac), and pelvic sidewall involvement and/or hydroureter, which were most strongly associated with surgical outcome, had a score of 2 while the other CT features had a score of 1. Scores ≥ 4 had the highest overall accuracy at 93%, with 100% sensitivity, 85% speci-ficity, 88% PPV, and 100% NPV. However, the predictive function of this model was not confirmed in other similar cross-validation studies[59,60]. Axtell et al[59] found disease over the diaphragm and large bowel mesentery as inde-pendent predictors of suboptimal cytoreduction. The authors also applied a different 14-criteria radiographic-based model to the original cohort of Bristow et al[58] as well as to the other cohorts, but found lower sensitivity, specificity, and accuracy. Another study by Gemer et al[60] compared the validity of four predictive CT scan models reported by Nelson et al[52], Dowdy et al[54], Bristow et al[58], and Qayyum et al[62]. Only the Dowdy study’s criteria for predicting the results of surgery were confirmed. The predictive performances of the other models were lower.
Finally, one recent prospective study by Ferrandina et al[61] used several features from CT scans combined with clinical data to develop a predictive index. The CT scan features were: peritoneal thickening or implants > 2 cm, bowel mesentery involvement, omental cake, pelvic sidewall involvement and/or hydroureter, suprarenal aortic lymph nodes > 1 cm or infrarenal aortic lymph nodes > 2 cm, superficial liver metastases > 2 cm and/or intraparenchimal liver metastases of any size, and ascites > 500 mL. Clini-cal data included age, CA 125, and ECOG-performance status. Radiographic and clinical features which yielded a specificity > 75%, PPV and NPV > 50%, and accuracy > 60% in predicting surgical outcomes were assigned a score of 2. The AUC was 0.78 using only radiographic features and 0.81 using both radiographic and clinical data. The
157 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

authors concluded that adding performance status led to improvement in the diagnostic performance in predicting suboptimal surgery.
Magnetic resonance imaging: Magnetic resonance im-aging (MRI) is not as commonly used as CT scans in ovarian cancer and there are fewer studies examining its role in predicting surgical outcome in patients with AOC. Qayyum et al[62] compared the possible role of CT scans (91 patients) and MRIs (46 patients) in predicting ≥ 2 cm suboptimal cytoreduction in 137 epithelial ovarian cancer patients. Using criteria from 14 different peritoneal and nodal diseases, the diagnostic performances of CT scan and MRI in predicting suboptimal diseases were similar, and optimal cytoreduction was achieved in 85% of the cases. However, these findings should be interpreted with caution because 32 patients in this study had early stage disease and only approximately one third of the patients underwent MRI. Furthermore, the results compared the findings from the two radiological techniques in all patients, rather than an individual comparison. Until we have a larger number of studies on the role of MRI in predicting surgical outcome, this technique cannot be recommended in place of CT scan as the first radiological imaging study.
Positron emission tomography and CT scans: The com-bined used of positron emission tomography and CT scans (PET/CT) has become more common in current clinical practice. This combination enables both sequen-tial functional and anatomical imaging. In the primary treatment setting, the PET/CT combination is used to evaluate the extent of disease, to predict the surgical out-
come, and to evaluate the response of a tumor to chemo-therapy[63,64].
The few studies which compared PET/CT imag-ings with other imaging tools found that PET/CT was superior to previous methods for diagnosis of malignant ovarian tumors[65,66]. The results of PET/CT were the same as operative findings in 69% to 78% of the patients. One advantage of PET/CT over other imaging methods was that it could reveal extra-abdominal ovarian tumors or co-existing malignant tumors at other sites[65,66]. We found only one prospective study by Risum et al[67], which evaluated risk using a malignancy index comprising of 10 features from PET/CT to assess 54 patients with AOC. Large bowel mesentery implants, pleural effusion or asci-tes, and peritoneal carcinomatosis identified from PET/CT were predictive factors of suboptimal cytoreduction. However, large bowel mesenteric implant was the only independent predictor. The authors concluded that find-ings from PET/CT scans should not be used to exclude patients from primary cytoreductive surgery. Nevertheless, the identification unsuspected extra-abdominal metastases by PET/CT scan (which were found in approximately one-third of all patients or half of apparent stage Ⅲ pa-tients) gave important information for making a decision on how to manage these patients[67].
Studies using a CT scan either alone or combina-tion with other clinical features to predict the results of PDS are presented in Table 2[52,54-62]. The sensitivity and specificity of imaging studies from various studies ranged from 15% to 92% and 32% to 100%, respectively. The PPV of 50%-100% (approximate mean of 82%) could suggest that 18% of the patients had a false negative diagnosis and that the expected optimal cytoreduction
158 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 2 Studies of computed tomography scan with or without clinical features to predict surgical outcome in epithelial ovarian cancer
First author, year n OS CT criteria ± clinical feature Sensitivity Specificity PPV NPV Accuracy
Using 2 cm as criteria for OS Nelson et al[52], 1993 421 69% 1 of 8 disease site 92% 79% 67% 96% 86% Meyer et al[55], 1995 281 57% 5 disease sites 58% 100% 100% 55% 79% Byrom et al[57], 2002 51 51% Full/reduced models (same values) 88% 98% 95% 94% -
CT with age and CA 125 (not useful) 88% 92% 85% 94% - Qayyum et al[62], 2005 137 15% Either CT (n = 91) or MRI (n = 46) 76% 99% 94% 96% 95% (CT),
96% (MRI)Using 1 cm as criteria for OS Dowdy et al[54], 2004 87 71% 3 disease sites (CA 125 not useful) 44% 95% 79% 81% - Fujwara et al[56], 2011 98 86% 4 or 6 disease sites (similar values) - - 50% 97% or 99% 91% or 94% Bristow et al[58], 2000 41 49% 13 disease site (predictive index ≥ 4)
(age and CA 125 not useful)100% 85% 88% 100% 93%
Axtell et al[59], 2007 (3 cohorts) 2 disease sites 65 78% Cohort A 79% 75% - - 77% 48 41% Cohort B 15% 32% - - 34% 71 87% Cohort C 72% 56% - - 64%
Gemer et al[60], 2009 123 73% Nelson’s criteria 64% 64% - - 64%Qayyum’s criteria 67% 57% - - 60%Bristow’s criteria 70% 64% - - 66%Dowdy’s criteria 79% 60% - - 65%
Ferrandina et al[61], 2009 195 44% 9 disease sites ± age, CA 125, PS AUC 0.78 for CT only and 0.81 when added with PS
119% of the patients in the study of Nelson et al[52] and 36% in the study of Meyer et al[55] had stage Ⅰ-Ⅱ diseases while all other studies included only advanced stage disease. OS: Optimal surgery; CT: Computed tomography; PPV: Positive predictive value; NPV: Negative predictive value; PS: Performance status; CA: Cancer antigen; MRI: Magnetic resonance imaging; AUC: Area under the curve.
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

159 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
could not be achieved. On the other hand, the NPVs which ranged from 55%-100% (approximate mean of 89%) or false positive diagnosis would indicate that 11% of patients could miss their chance of successful PDS.
In conclusion, although some radiological features can predict the possibility of optimal or suboptimal re-section, aggressive surgery also has impact on the surgical outcome regardless of the extent of diseases. Hence, a predictive model derived from imaging findings (which does take the effort of the surgeons into account) may not be applicable in all advanced stage ovarian cancer pa-tients in different settings.
LaparoscopyIn the absence of any absolutely reliable preoperative imaging studies or serum markers to predict surgical out-comes in AOC, other means have sought. Laparoscopy (LPS) is an emerging technology which has become more widely practiced in gynecological oncology. Laparoscopic procedures have been practiced in early stage ovarian cancer for many years[68,69]. The minimally invasive nature of LPS yields an advantage over a laparotomy in terms of the rapid recovery of the patient. A balance between comprehensive surgery and maintenance of a locally confined ovarian tumor in early stage disease must be exercised. In recent years, LPS has also been applied in AOC[70]. A direct visualization before laparotomy of tu-mor location and other pathological findings in the peri-toneal cavity will assist a surgeon to better assess the pos-sibility of surgery, particularly for optimal cytoreduction.
Few studies have evaluated a role of LPS to predict the outcome of PDS. Angioli et al[71] in 2006 performed LPS on 87 women with AOC before making the decision for laparotomy. NACT was the alternative option in the presence of viscera lesions. As much as 96% of patients, whose tumors were deemed resectable from LPS, were actually optimally debulked by PDS, yielding an 80% rate of optimal cytoreduction. It should be noted that the definition of optimal surgery in this study was “no gross residual disease”. This might have led to a higher frequency of NACT use compared to a scenario where 1 or 2 cm residual disease was used as the criterion for op-timal cytoreduction. In the same year, two other studies also reported on the role of LPS in AOC[72,73]. Deffieux
et al[72] estimated by LPS that 11 out of 15 AOC patients would have resectable peritoneal carcinomatosis. Ten of them actually had no residual disease from PDS. Another study by Fagotti et al[73] reported the results from their prospective study evaluating lesions over the omentum, diaphragm, peritoneum, mesentery, liver, bowel, and stomach in predicting the surgical outcomes in AOC. The rate of optimal cytoreduction was 67%. Using a scale of 0 to 12, a score ≥ 8 had PPV of 100%, NPV of 70%, and accuracy of 75% for optimal cytoreduction. This was confirmed by a subsequent validation study by these authors who used the same scoring model in 113 women with stage Ⅲ/Ⅳ disease[74]. The rate of optimal cytore-duction in this series was 56%. The PPV, NPV, and overall accuracy were 100%, 60%, and 93%, respectively. The au-thors concluded that a score ≥ 8 was the appropriate cut-off for predicting suboptimal cytoreduction in 100% of patients. The rate of futile exploration was only 40%. Of note, another cross-validation study by Brun et al[75], who used a score of ≥ 8 in predicting optimal surgery in stage Ⅲ/Ⅳ disease, reported an accuracy of only 60% with 89% PPV, 44% NPV, 46% sensitivity, and 89% specificity. The authors simplified the original Fagotti-scoring sys-tem and found a score ≥ 4 to be as accurate as Fagotti’s score in predicting resectability. Table 3 shows studies which have determined the role of LPS to predict surgical outcome prior to PDS or NACT and IDS[71-75].
The limitations noted in the predictive role of LPS score across a number of studies were probably due to the involvement of different surgeons with various inten-tions and skills in that particular setting. Nevertheless, a direct visualization of disease by LPS should theoretically offer the best prediction of surgical outcome compared to other preoperative markers or imaging studies. Unnec-essary laparotomies can probably be avoided with more confidence. One ongoing multicentre trial will randomize 200 patients with AOC to have a diagnostic LPS prior to a planned PDS[76]. Patients who are evaluated by LPS to have disease expected to be resectable to < 1 cm will undergo PDS followed by platinum based chemotherapy while the other patients will have NACT and IDS before continuing chemotherapy. The primary outcome will be the proportion of suboptimal surgeries in each arm of the study.
Table 3 Studies using laparoscopy to predict surgical outcome
Study n PDS (n) Optimal surgery1
Criteria of residual
diseases (cm)
Sensitivity Specificity PPV NPV Accuracy
Angioli et al[71], 2006 87 53 96% 0 - - - - -Deffieux et al[72], 2006 15 11 91% 0 - - - - -Fagotti et al[73], 20062 64 61 67% 1 30% 100% 100% 70% 74%Fagotti et al[74], 20082 113 91 50% 1 30% 100% 100% 60% 75%Brun et al[75], 20082 55 26 69% 1 46% 89% 89% 44% 60%
1Percentage of optimal surgery was obtained only in the patients who had primary debulking surgery; 2Diagnostic performance predictions in these studies used score ≥ 8 as cut-off value from the model of the study. PDS: Primary debulking surgery; NPV: Negative predictive value; PPV: Positive predictive value.
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

160 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
NACT: INDICATIONS AND SELECTION CRITERIAAs already mentioned, the standard treatment of advanced epithelial ovarian cancer (FIGO stage Ⅲ-Ⅳ) is a staging laparotomy with PDS, followed by platinum-based che-motherapy. The extent of tumour cytoreduction is consid-ered to be the most relevant prognostic factor. The defini-tion of optimal debulking has changed over time and it is currently defined by many authors as “no macroscopic re-sidual tumour”[2]. In the last decade the dogma of PDS as the preferred “one-size-fits-all” approach to the primary treatment of AOC has been challenged by NACT, that is chemotherapy delivered prior to any attempt at surgical debulking.
Two meta-analysis[77,78] and two systematic reviews[79,80]
addressed the question of the timing of surgery before or after chemotherapy in AOC patients. The Bristow and Chi meta-analysis included only phase Ⅰ/Ⅱ and retrospective studies involving 835 patients from 21 stud-ies using platinum-based NACT after a primary surgery attempt[77]. The results showed that survival of patients who had NACT followed by IDS was inferior to those who had PDS. Furthermore each incremental chemo-therapy cycle after the third course of NACT resulted in a 4.1-mo decrease in survival. This meta-analysis is, however, affected by severe methodological limitations as recognized by the authors themselves. In particular, the results are confounded by major selection biases (no information is given about criteria to establish NACT duration), by a large variety of different chemotherapeu-tic agents and administration schedules, and by the fact that prognostic factors such as performance status were not examined. It is also worth-noting that because of the limited number of studies the authors did not apply the multiple linear regression model and it is possible that one or more statistically significant variables associ-ated with survival on simple linear regression could be irrelevant if interaction among variables were taken into account. In another meta-analysis on the same 21 studies conducted by Bristow et al[77], the random effect meta-regression analysis was used instead of simple linear re-gression[78]. The year of publication (more vs less recent), the stage (Ⅲ vs Ⅳ), the use of a taxane (vs not), and the optimal cytoreduction (vs not) were associated with a bet-ter overall survival. The detrimental effect of duration of NACT was not confirmed, indicating that the allocation of poorer prognosis patients to NACT and to a greater number of chemotherapy courses is a general phenom-enon in non-randomized studies, leading to a severely confounding selection bias.
A systematic review of randomized controlled tri-als of chemotherapy vs surgery for the initial treatment in AOC patients was conducted by the Cochrane col-laborative group in 2007[81] and was recently updated[80]. The first version of the review[81] identified only one randomized trial by Liu et al[82]. Patients were random-ized to NACT by the intra-arterial route before IDS or
conventional PDS followed by adjuvant chemotherapy. This study randomized just 85 women and could not demonstrate any significant difference in overall survival between the two treatment arms. However, optimal cy-toreduction was achieved more often in the NACT/em-bolisation group, and this group had a shorter operating time, less blood loss and fewer blood transfusions. The updated review excluded this trial because the study find-ings might have been attributable to NACT, the iliac ar-tery embolization, or both.
As a consequence the only RCT included in the Co-chrane 2012 review is the Intergroup Study from Europe, Canada and South America (EORTC 55971/NCIC OV13). This is the only published randomized trial com-paring NACT (3 courses) followed by surgery and by 3 more courses of adjuvant chemotherapy with PDS fol-lowed by 6 courses of adjuvant chemotherapy (with or without IDS)[10]. The trial randomized 718 patients with stage Ⅲc-Ⅳ AOC, primary peritoneal cancer or fallo-pian tube cancer with the goal of evelauting the NACT vs the control arm in terms of overall survival (primary end-point). Secondary end-points were progression-free survival, surgical morbidity and mortality, quality of life and adverse effects. Among 670 evaluable patients, no significant differences in terms of overall survival (HR 0.98; 95%CI: 0.82-1.18) or progression-free survival (HR 1.01; 95%CI: 0.86-1.17) were found, even though the complete resection rate was higher in the NACT group (52% vs 20%, RR 2.56; 95%CI: 2.00-3.28). Grade 3 and 4 haemorrhage, venous thromboembolism and infection were more frequent in the control arm. No differences were observed in the need for blood transfusions, operat-ing times and quality of life.
The definition of selection criteria for NACT or PDS in clinical practice remains a matter of heated debate[83-85]. The supporters of PDS state that optimal debulking sur-gery can be achieved in most cases and must be pursued even when major debulking procedures and ultra-radical surgery are needed, restricting NACT to a minority of patients with diffuse extraperitoneal disease and/or too sick and elderly to tolerate a major debulking proce-dure[83]. According to this view, the lack of surgical skills among gynaecological oncologists is a critical issue that should be modified in order to improve the survival of ovarian cancer patients. The major criticism of this posi-tion is that it is based only on biased retrospective data and has never been prospectively validated in the context of a randomized controlled trial.
On the other hand, some are concerned about the feasibility of extensive surgery in a real clinical practice[84]. According to the EORTC/NCIC trial, the Leuven selec-tion criteria for NACT[85] include: tumours larger than 2 cm around the superior mesenteric artery or behind the porta hepatis, or intrahepatic (multiple) metastases or several extra-abdominal metastases (excluding resectable inguinal or supraclavicular lymph nodes), or poor general condi-tions (e.g., over 80 years of age), or extensive serosal inva-sion necessitating bowel resections greater than 1.5 m
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

161 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
or women who cannot be easily debulked to no residual tumor (e.g., more than one bowel resection, expected op-erating time greater than 4 h). The last two Leuven criteria are probably the most controversial.
Even if the level of evidence in favour of NACT as a treatment option for patients with bulky stage Ⅲc-Ⅳ AOC is limited (one single RCT), the level of evidence in favour of major debulking surgery and ultra-radical sur-gery is even lower (retrospective data only). Supporters of NACT believe that it is not recommended to submit patients to the risk and costs of major surgical proce-dures based on such a low level of evidence.
Three more prospective randomized trials are com-paring NACT vs PDS in AOC: the small Indian trial results[86] were partly presented in 2007 and in 2009 and should be published shortly (the anticipated results are similar to those of EORTC/NCIC trial). The Japanese trial JCOG0602 accrued 301 patients from November 2006 to October 2011, while the CHORUS trial recruited over 500 patients from March 2004 to July 2010 and the results are awaited[87,88]. All of these trials are investigating a short-term platinum-taxane NACT (3 courses in the In-dian and in the CHORUS trials, 4 courses in the JGOG trial).
Hence, we can state that NACT can be considered as an option in patients whose disease appears to be extensive and when the PDS is not possible, expected to be subop-timal or requiring extensive surgical demolitions. NACT should not replace PDS whenever there is a chance for a patient to have a successful standard treatment by PDS fol-lowed by adjuvant chemotherapy.
IDS: SELECTION CRITERIA AND OPTIMAL TIMINGNACT has been promoted in order to avoid non-useful surgical procedures in patients expected to have a sub-optimal surgical staging after establishing a diagnosis of AOC[89]. IDS or delayed PDS will be performed when the tumors have responded to induction or NACT in terms of complete or partial response as well as stable disease. Most studies to date have demonstrated that the advantage of NACT is the higher rate of optimal cyto-reduction at IDS compared to PDS[11,79,90,91]. The possible benefit of IDS on survival is more controversial. Several non-randomized trials which attempted to evaluate the association of IDS and patient survival had inconsistent results. Some studies showed similar survival outcomes between patients who underwent IDS and those patients who had PDS[92-95]. Other studies reported significantly longer survival of patients who had IDS[90,96] and some showed lower survival rates for patients having IDS than for those having optimal PDS[97]. To date, only three randomized trial have focused on the prognostic role of IDS[98-100], and these trials did not agree on the benefit of IDS on survival outcomes. Two trials found similar sur-vival rates between patients who had IDS and those who had conventional treatment[98,100], while the third showed
significantly longer survival in the IDS group[99]. The positive effects found in the Van der Burg study persisted after a 10-year follow-up[101]. The Cochrane Collaboration Group conducted a systematic review and meta-analysis (including the three trials just noted) involving 853 wom-en (781 evalauble)[11], and found no statistically significant difference of overall survival (HR 0.80, 95%CI: 0.61-1.06) and progression-free survival (HR 0.88, 95%CI: 0.57-1.33) between the patients who had or did not have IDS. IDS appeared to be beneficial when the PDS was not per-formed by a gynaecological oncologist or when the PDS was less extensive (HR 0.68, 95%CI: 0.53-0.87).
The timing of performing IDS is another unresolved issue. Previous studies reported the number of induc-tion or NACT cycles ranging from 2-10, with the most common being 3-4 cycles[10,11,90,91,102]. Many reasons were proposed for the earlier timing of the IDS. First, che-motherapy induced fibrosis is less extensive after 3 than after 6 cycles[103]. Second, some tumor clones may de-velop chemoresistance after 6 cycles[104]. Lastly, indirect evidence from an earlier study investigating the role of tumor debulking at the time of second-look surgery after 6 cycles of chemotherapy did not show any survival im-provement[8]. To date, only a few studies with data com-paring early with late (after 6 cycles) IDS after NACT are available. One French multicenter study investigated the results of NACT in 54 AOC patients presenting with primary unresectable tumors[105]. The authors found a higher complete response rate from late (after 6 cycles) compared to early IDS (after 3-4 cycles), 61% vs 45%. However, the survival rates were the same in both groups at 22 mo. These results were consistent with the data of Stoeckle et al[106] who compared outcomes of AOC patients who were treated with platinum-based chemo-therapy and underwent early (after 3 cycles) or late IDS (after 6 cycles). The authors also found a higher complete resection rate in the late IDS groups than that in the early IDS gropus, 58% vs 36%. These findings suggest that the chance of achieving an optimal debulking increases in a direct relationship with the number of cycles before surgery. However, one randomized trial which was unable to demonstrate different response rates or rates of opti-mal surgery (residual tumors ≤ 1 cm) between 2 cycles and 3 cycles of NACT[107]. With inconsistent results re-garding the benefit of more cycles of NACT, it should be noted that higher rates of responses and optimal debulking were not translated into an improved rate of survival[105,106]. Hence, based on the EORTC randomized trial[10], limiting NACT to 3 cycles is a reasonable practice until further data prove otherwise. Longer NACT treat-ment should be explored in the context of clinical trials.
Generally when the disease shows some response to induction chemotherapy or NACT, IDS can be per-formed unless clinical signs of progressive disease are evident. Criteria for selection of patients who are likely to have successful IDS are also important[9,108]. Patients who are still deemed inoperable or cannot have optimal IDS may be better receiving a new chemotherapy regimen. To
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

162 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
predict the results of IDS, Rodriguez et al[91] studied the role of CA 125 in 103 AOC patients who were treated with platinum-based NACT followed by IDS. Ninety-nine patients (96%) had optimal cytoreduction, defined as re-sidual disease ≤ 1 cm (47 patients or 48% had no residual disease). There was no statistical difference in CA 125 at diagnosis between those without residual disease and those with optimal surgery but with macroscopic disease. However, the CA 125 level before IDS was significantly lower in patients with no residual disease than that in patients with optimal but macroscopic disease, 92 U/mL compared to 233 U/mL (P = 0.001). Using CA 125 of ≤ 100 U/mL as a cut-off level, a significantly higher per-centage of patients without residual tumors had low pre-IDS CA 125 than the group with macroscopic residual disease, 80% vs 63%. The authors suggested that patients with pre-IDS CA 125 ≤ 100 U/mL were likely to have successful optimal cytoreduction to no residual disease. Another study by Bland et al[109] evaluated and construct-ed 3 algorithms using CA 125, CT scan, and LPS find-ings in 128 AOC women after initial chemotherapy but before surgery. The authors found that failure of CA 125 to decline dramatically was significantly associated with suboptimal surgery: 89% of the patients with optimal surgery had a decline of CA 125 > 50% compared to only 57% in the suboptimal group[109]. In the same vein, a significantly higher percentage of patients with subop-timal surgery had more small-bowel mesentery disease identified from by CT scan than found in those with op-timal surgical outcome, 38% vs 6%. Other findings which were missed in pre-operative CT scans and were found in patients with suboptimal surgery were diseases on the liver surface, small-bowel surface, large-bowel mesentery, bladder peritoneum, spleen, and diaphragm. Finally the authors proposed a predictive algorithm for identifying patients most likely to have suboptimal surgery following chemotherapy using criteria: < 50% reduction in CA 125, stable or progressive disease on CT scan, and diseases on the bladder peritoneum or liver surface identified at the time of LPS[109]. However, the number of patients in this study having either serum CA 125, CT scan, or LPS sur-gery before exploration was limited and further study is required to confirm these data.
In addition to tumor markers and imaging studies, a recent study by Fagotti et al[9] reported a role for LPS in AOC patients who had partially stable/stable disease af-ter NACT. The authors set a predictive index score based
on various features identified from staging LPS to select patients who were likely to have successful IDS (Table 4). The LPS parameters of mesentery retraction, bowel and stomach infiltration, and superficial liver metastasis were strongly associated with unresectable diseases. Using a staging LPS after serological response with NACT, the authors found the rate of inappropriate exploration was reduced from 18% to 0%. Moreover, a predictive index score > 4 could absolutely predict the probability of op-timally cytoreduction at laparotomy in all patients.
Unlike the important prognostic role of the size of residual disease after PDS[2], only limited information re-garding the size of residual disease after IDS is available. Most studies have used the same traditional definition of “optimal cytoreduction” in IDS as that in PDS. A recent randomized study and one retrospective study found that complete resection of all macroscopic disease at the time of IDS was the single most important independent prog-nostic factor in AOC[10,110].
In conclusion, standard management of advanced ovarian cancer is primary surgery followed by adjuvant chemotherapy. The aim of surgery should be a removal of all gross visible tumors because this is one of the most important prognostic factors. Prediction of surgical outcome is crucial especially when the benefit of optimal surgery and the risk of extensive surgery are equivocal. NACT followed by surgery is an alternative option with less morbidity and comparable survival outcome. IDS is another approach for patients who have suboptimal pri-mary surgery and who have no progressive disease after induction chemotherapy. This interval surgery yields sur-vival benefits particularly in patients who have had less extensive primary surgery or less than maximal efforts made by an expert surgeon.
REFERENCES1 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL,
Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167 DOI: 10.1200/JCO.20.5.1248]
2 Elattar A, Bryant A, Winter-Roach BA, Hatem M, Naik R. Optimal primary surgical treatment for advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2011; CD007565 [PMID: 21833960 DOI: 10.1002/14651858.CD007565.pub2]
3 Griffiths CT. Surgical resection of tumor bulk in the primary treatment of ovarian carcinoma. Natl Cancer Inst Monogr 1975; 42: 101-104 [PMID: 1234624]
Table 4 Laparoscopic parameters assigned a predictive index score
Predictive index parameter Point value Sensitivity Specificity PPV NPV Accuracy
Omental cake 0 72.7% 68.3% 55.8% 82.0% 69.9%Diaphragmatic carcinosis 0 77.1% 71.2% 61.4% 84.0% 73.4%Mesenteral retraction 2 64.3% 98.2% 94.7% 85.0% 87.2%Bowel infiltration 2 69.7% 86.0% 74.2% 84.1% 80.8%Stomach infiltration 2 17.6% 100% 100% 67.4% 69.6%Superficial liver metastasis 2 22.8% 100% 100% 68.9% 71.6%
NPV: Negative predictive value; PPV: Positive predictive value.
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

163 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
4 Stoeckle E, Paravis P, Floquet A, Thomas L, Tunon de Lara C, Bussières E, Macgrogan G, Picot V, Avril A. Number of residual nodules, better than size, defines optimal surgery in advanced epithelial ovarian cancer. Int J Gynecol Cancer 2004; 14: 779-787 [PMID: 15361184 DOI: 10.1111/j.1048-891X.2004.014508.x]
5 Ang C, Chan KK, Bryant A, Naik R, Dickinson HO. Ultra-radical (extensive) surgery versus standard surgery for the primary cytoreduction of advanced epithelial ovarian cancer. Cochrane Database Syst Rev 2011; CD007697 [PMID: 21491400 DOI: 10.1002/14651858.CD007697.pub2]
6 Chi DS, Liao JB, Leon LF, Venkatraman ES, Hensley ML, Bhaskaran D, Hoskins WJ. Identification of prognostic fac-tors in advanced epithelial ovarian carcinoma. Gynecol Oncol 2001; 82: 532-537 [PMID: 11520151 DOI: 10.1006/gyno.2001.6328]
7 Aletti GD, Gostout BS, Podratz KC, Cliby WA. Ovarian can-cer surgical resectability: relative impact of disease, patient status, and surgeon. Gynecol Oncol 2006; 100: 33-37 [PMID: 16153692 DOI: 10.1016/j.ygyno.2005.07.123]
8 Vergote I, van Gorp T, Amant F, Leunen K, Neven P, Ber-teloot P. Timing of debulking surgery in advanced ovarian cancer. Int J Gynecol Cancer 2008; 18 Suppl 1: 11-19 [PMID: 18336393 DOI: 10.1111/j.1525-1438.2007.01098.x]
9 Fagotti A, Fanfani F, Vizzielli G, Gallotta V, Ercoli A, Pa-glia A, Costantini B, Vigliotta M, Scambia G, Ferrandina G. Should laparoscopy be included in the work-up of advanced ovarian cancer patients attempting interval debulking sur-gery? Gynecol Oncol 2010; 116: 72-77 [PMID: 19846211 DOI: 10.1016/j.ygyno.2009.09.015]
10 Vergote I, Tropé CG, Amant F, Kristensen GB, Ehlen T, Johnson N, Verheijen RH, van der Burg ME, Lacave AJ, Pan-ici PB, Kenter GG, Casado A, Mendiola C, Coens C, Verleye L, Stuart GC, Pecorelli S, Reed NS. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med 2010; 363: 943-953 [PMID: 20818904 DOI: 10.1056/NEJ-Moa0908806]
11 Tangjitgamol S, Manusirivithaya S, Laopaiboon M, Lum-biganon P, Bryant A. Interval debulking surgery for ad-vanced epithelial ovarian cancer. Cochrane Database Syst Rev 2010; CD006014 [PMID: 20927744 DOI: 10.1002/14651858.CD006014.pub5]
12 Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet 2001; 357: 539-545 [PMID: 11229684 DOI: 10.1016/S0140-6736(00)04046-0]
13 Jackson JR, Seed MP, Kircher CH, Willoughby DA, Winkler JD. The codependence of angiogenesis and chronic inflam-mation. FASEB J 1997; 11: 457-465 [PMID: 9194526]
14 McMillan DC, Canna K, McArdle CS. Systemic inflammato-ry response predicts survival following curative resection of colorectal cancer. Br J Surg 2003; 90: 215-219 [PMID: 12555298 DOI: 10.1002/bjs.4038]
15 Assoian RK, Sporn MB. Type beta transforming growth fac-tor in human platelets: release during platelet degranulation and action on vascular smooth muscle cells. J Cell Biol 1986; 102: 1217-1223 [PMID: 3457014 DOI: 10.1083/jcb.102.4.1217]
16 Dubernard V, Arbeille BB, Lemesle MB, Legrand C. Evi-dence for an alpha-granular pool of the cytoskeletal protein alpha-actinin in human platelets that redistributes with the adhesive glycoprotein thrombospondin-1 during the exocy-totic process. Arterioscler Thromb Vasc Biol 1997; 17: 2293-2305 [PMID: 9351403 DOI: 10.1161/01.ATV.17.10.2293]
17 Kaplan KL, Broekman MJ, Chernoff A, Lesznik GR, Drill-ings M. Platelet alpha-granule proteins: studies on release and subcellular localization. Blood 1979; 53: 604-618 [PMID: 426909]
18 Qian X, Tuszynski GP. Expression of thrombospondin-1 in cancer: a role in tumor progression. Proc Soc Exp Biol Med 1996; 212: 199-207 [PMID: 8677265]
19 Dabrow MB, Francesco MR, McBrearty FX, Caradonna S.
The effects of platelet-derived growth factor and receptor on normal and neoplastic human ovarian surface epithelium. Gynecol Oncol 1998; 71: 29-37 [PMID: 9784315 DOI: 10.1006/gyno.1998.5121]
20 Stone RL, Nick AM, McNeish IA, Balkwill F, Han HD, Botts-ford-Miller J, Rupairmoole R, Armaiz-Pena GN, Pecot CV, Coward J, Deavers MT, Vasquez HG, Urbauer D, Landen CN, Hu W, Gershenson H, Matsuo K, Shahzad MM, King ER, Tekedereli I, Ozpolat B, Ahn EH, Bond VK, Wang R, Drew AF, Gushiken F, Lamkin D, Collins K, DeGeest K, Lut-gendorf SK, Chiu W, Lopez-Berestein G, Afshar-Kharghan V, Sood AK. Paraneoplastic thrombocytosis in ovarian can-cer. N Engl J Med 2012; 366: 610-618 [PMID: 22335738 DOI: 10.1056/NEJMoa1110352]
21 den Ouden M, Ubachs JM, Stoot JE, van Wersch JW. Whole blood cell counts and leucocyte differentials in patients with benign or malignant ovarian tumours. Eur J Obstet Gynecol Reprod Biol 1997; 72: 73-77 [PMID: 9076425 DOI: 10.1016/S0301-2115(96)02662-0]
22 Li AJ, Madden AC, Cass I, Leuchter RS, Lagasse LD, Karlan BY. The prognostic significance of thrombocytosis in epi-thelial ovarian carcinoma. Gynecol Oncol 2004; 92: 211-214 [PMID: 14751160 DOI: 10.1016/j.ygyno.2003.09.002]
23 Levin J, Conley CL. Thrombocytosis associated with ma-lignant disease. Arch Intern Med 1964; 114: 497-500 [PMID: 14184638 DOI: 10.1001/archinte.1964.03860100079008]
24 Tuszynski GP, Nicosia RF. The role of thrombospondin-1 in tumor progression and angiogenesis. Bioessays 1996; 18: 71-76 [PMID: 8593167 DOI: 10.1002/bies.950180113]
25 Thavaramara T, Phaloprakarn C, Tangjitgamol S, Manu-sirivithaya S. Role of neutrophil to lymphocyte ratio as a prognostic indicator for epithelial ovarian cancer. J Med As-soc Thai 2011; 94: 871-877 [PMID: 21774296]
26 Cho H, Hur HW, Kim SW, Kim SH, Kim JH, Kim YT, Lee K. Pre-treatment neutrophil to lymphocyte ratio is elevated in epithelial ovarian cancer and predicts survival after treat-ment. Cancer Immunol Immunother 2009; 58: 15-23 [PMID: 18414853 DOI: 10.1007/s00262-008-0516-3]
27 Asher V, Lee J, Innamaa A, Bali A. Preoperative platelet lymphocyte ratio as an independent prognostic marker in ovarian cancer. Clin Transl Oncol 2011; 13: 499-503 [PMID: 21775277 DOI: 10.1007/s12094-011-0687-9]
28 Raungkaewmanee S, Tangjitgamol S, Manusirivithaya S, Srijaipracharoen S, Thavaramara T. Platelet to lymphocyte ratio as a prognostic factor for epithelial ovarian cancer. J Gy-necol Oncol 2012; 23: 265-273 [PMID: 23094130 DOI: 10.3802/jgo.2012.23.4.265]
29 Jacobs I, Bast RC. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod 1989; 4: 1-12 [PMID: 2651469]
30 Gemer O, Segal S, Kopmar A. Preoperative CA-125 level as a predictor of non optimal cytoreduction of advanced epitheli-al ovarian cancer. Acta Obstet Gynecol Scand 2001; 80: 583-585 [PMID: 11380298 DOI: 10.1034/j.1600-0412.2001.080006583.x]
31 Cooper BC, Sood AK, Davis CS, Ritchie JM, Sorosky JI, An-derson B, Buller RE. Preoperative CA 125 levels: an indepen-dent prognostic factor for epithelial ovarian cancer. Obstet Gynecol 2002; 100: 59-64 [PMID: 12100804 DOI: 10.1016/S0029-7844(02)02057-4]
32 Memarzadeh S, Lee SB, Berek JS, Farias-Eisner R. CA125 levels are a weak predictor of optimal cytoreductive surgery in patients with advanced epithelial ovarian cancer. Int J Gy-necol Cancer 2003; 13: 120-124 [PMID: 12657110 DOI: 10.1046/j.1525-1438.2003.13019.x]
33 Rossi AC, Di Vagno G, Cormio G, Cazzolla A, Stefanelli S, D’Elia E, Selvaggi L. A retrospective study of preoperative CA 125 levels in 82 patients with ovarian cancer. Arch Gynecol Obstet 2004; 269: 263-265 [PMID: 14745561 DOI: 10.1007/s00404-002-0404-6]
34 Alcázar JL, Miranda D, Unanue A, Novoa E, Alemán S,
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer
164 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Madariaga L. CA-125 levels in predicting optimal cytoreduc-tive surgery in patients with advanced epithelial ovarian carcinoma. Int J Gynaecol Obstet 2004; 84: 173-174 [PMID: 14871524 DOI: 10.1016/j.ijgo.2003.10.006]
35 Gemer O, Lurian M, Gdalevich M, Kapustian V, Piura E, Schneider D, Lavie O, Levy T, Fishman A, Dgani R, Levavi H, Beller U. A multicenter study of CA 125 level as a predictor of non-optimal primary cytoreduction of advanced epithelial ovarian cancer. Eur J Surg Oncol 2005; 31: 1006-1010 [PMID: 16005601]
36 Everett EN, Heuser CC, Pastore LM, Anderson WA, Rice LW, Irvin WP, Taylor PT. Predictors of suboptimal surgical cytoreduction in women treated with initial cytoreductive surgery for advanced stage epithelial ovarian cancer. Am J Obstet Gynecol 2005; 193: 568-574; discussion 574-576 [PMID: 16098898 DOI: 10.1016/j.ajog.2005.03.058]
37 Barlow TS, Przybylski M, Schilder JM, Moore DH, Look KY. The utility of presurgical CA125 to predict optimal tu-mor cytoreduction of epithelial ovarian cancer. Int J Gynecol Cancer 2006; 16: 496-500 [PMID: 16681717 DOI: 10.1111/j.1525-1438.2006.00573.x]
38 Gilani MM, Karimi Zarchi M, Ghaemmaghami F, Behtash N, Mousavi AS, Ansaripoor S. A study to evaluate the utility of presurgical CA125 to predict optimal tumor cytoreduction of epithelial ovarian cancer. Gynecol Oncol 2007; 105: 780-783 [PMID: 17433423 DOI: 10.1016/j.ygyno.2007.02.027]
39 Arits AH, Stoot JE, Botterweck AA, Roumen FJ, Voogd AC. Preoperative serum CA125 levels do not predict suboptimal cytoreductive surgery in epithelial ovarian cancer. Int J Gyne-col Cancer 2008; 18: 621-628 [PMID: 17868339 DOI: 10.1111/j.1525-1438.2007.01064.x]
40 Chi DS, Zivanovic O, Palayekar MJ, Eisenhauer EL, Abu-Rustum NR, Sonoda Y, Levine DA, Leitao MM, Brown CL, Barakat RR. A contemporary analysis of the ability of preoperative serum CA-125 to predict primary cytoreduc-tive outcome in patients with advanced ovarian, tubal and peritoneal carcinoma. Gynecol Oncol 2009; 112: 6-10 [PMID: 19100916 DOI: 10.1016/j.ygyno.2008.10.010]
41 Chi DS, Venkatraman ES, Masson V, Hoskins WJ. The abil-ity of preoperative serum CA-125 to predict optimal primary tumor cytoreduction in stage III epithelial ovarian carci-noma. Gynecol Oncol 2000; 77: 227-231 [PMID: 10785469 DOI: 10.1006/gyno.2000.5749]
42 Saygili U, Guclu S, Uslu T, Erten O, Demir N, Onvural A. Can serum CA-125 levels predict the optimal primary cy-toreduction in patients with advanced ovarian carcinoma? Gynecol Oncol 2002; 86: 57-61 [PMID: 12079301 DOI: 10.1006/gyno.2002.6719]
43 Obeidat B, Latimer J, Crawford R. Can optimal primary cytoreduction be predicted in advanced stage epithelial ovarian cancer? Role of preoperative serum CA-125 level. Gynecol Obstet Invest 2004; 57: 153-156 [PMID: 14726621 DOI: 10.1159/000076236]
44 Eltabbakh GH, Mount SL, Beatty B, Simmons-Arnold L, Cooper K, Morgan A. Factors associated with cytoreduc-ibility among women with ovarian carcinoma. Gynecol Oncol 2004; 95: 377-383 [PMID: 15491760 DOI: 10.1016/j.ygyno.2004.07.045]
45 Brockbank EC, Ind TE, Barton DP, Shepherd JH, Gore ME, A’Hern R, Bridges JE. Preoperative predictors of subopti-mal primary surgical cytoreduction in women with clinical evidence of advanced primary epithelial ovarian cancer. Int J Gynecol Cancer 2004; 14: 42-50 [PMID: 14764028 DOI: 10.1111/j.1048-891x.2004.14065.x]
46 Vorgias G, Iavazzo C, Savvopoulos P, Myriokefalitaki E, Katsoulis M, Kalinoglou N, Akrivos T. Can the preoperative Ca-125 level predict optimal cytoreduction in patients with advanced ovarian carcinoma? A single institution cohort study. Gynecol Oncol 2009; 112: 11-15 [PMID: 19119502 DOI: 10.1016/j.ygyno.2008.09.020]
47 Kang S, Kim TJ, Nam BH, Seo SS, Kim BG, Bae DS, Park SY. Preoperative serum CA-125 levels and risk of suboptimal cy-toreduction in ovarian cancer: a meta-analysis. J Surg Oncol 2010; 101: 13-17 [PMID: 20025071 DOI: 10.1002/jso.21398]
48 Pannu HK, Horton KM, Fishman EK. Thin section dual-phase multidetector-row computed tomography detection of peritoneal metastases in gynecologic cancers. J Comput Assist Tomogr 2003; 27: 333-340 [PMID: 12794595 DOI: 10.1097/00004728-200305000-00006]
49 Pannu HK, Bristow RE, Montz FJ, Fishman EK. Multidetec-tor CT of peritoneal carcinomatosis from ovarian cancer. Ra-diographics 2003; 23: 687-701 [PMID: 12740470 DOI: 10.1148/rg.233025105]
50 Coakley FV, Choi PH, Gougoutas CA, Pothuri B, Venkatra-man E, Chi D, Bergman A, Hricak H. Peritoneal metastases: detection with spiral CT in patients with ovarian cancer. Radiology 2002; 223: 495-499 [PMID: 11997559 DOI: 10.1148/radiol.2232011081]
51 Tempany CM, Zou KH, Silverman SG, Brown DL, Kurtz AB, McNeil BJ. Staging of advanced ovarian cancer: com-parison of imaging modalities--report from the Radiological Diagnostic Oncology Group. Radiology 2000; 215: 761-767 [PMID: 10831697]
52 Nelson BE, Rosenfield AT, Schwartz PE. Preoperative ab-dominopelvic computed tomographic prediction of optimal cytoreduction in epithelial ovarian carcinoma. J Clin Oncol 1993; 11: 166-172 [PMID: 8418230]
53 Salani R, Axtell A, Gerardi M, Holschneider C, Bristow RE. Limited utility of conventional criteria for predicting unre-sectable disease in patients with advanced stage epithelial ovarian cancer. Gynecol Oncol 2008; 108: 271-275 [PMID: 18164380 DOI: 10.1016/j.ygyno.2007.11.004]
54 Dowdy SC, Mullany SA, Brandt KR, Huppert BJ, Cliby WA. The utility of computed tomography scans in predict-ing suboptimal cytoreductive surgery in women with ad-vanced ovarian carcinoma. Cancer 2004; 101: 346-352 [PMID: 15241833 DOI: 10.1002/cncr.20376]
55 Meyer JI, Kennedy AW, Friedman R, Ayoub A, Zepp RC. Ovarian carcinoma: value of CT in predicting success of debulking surgery. AJR Am J Roentgenol 1995; 165: 875-878 [PMID: 7676985]
56 Fujwara K, Yoshino K, Enomoto T, Fujita M, Ueda Y, Mi-yatake T, Kimura T, Muraji M, Fujita H, Kimura T, Hori M. Usefulness of computed tomography in predicting cytore-ductive surgical outcomes for ovarian cancer. Arch Gynecol Obstet 2011; 284: 1501-1507 [PMID: 21347681 DOI: 10.1007/s00404-011-1864-3]
57 Byrom J, Widjaja E, Redman CW, Jones PW, Tebby S. Can pre-operative computed tomography predict resect-ability of ovarian carcinoma at primary laparotomy? BJOG 2002; 109: 369-375 [PMID: 12013156 DOI: 10.1111/j.1471-0528.2002.01216.x]
58 Bristow RE, Duska LR, Lambrou NC, Fishman EK, O’Neill MJ, Trimble EL, Montz FJ. A model for predicting surgical outcome in patients with advanced ovarian carcinoma using computed tomography. Cancer 2000; 89: 1532-1540 [PMID: 11013368 DOI: 10.1002/1097-0142(20001001)89:7<1532::AID-CNCR17>3.0.CO;2-A]
59 Axtell AE, Lee MH, Bristow RE, Dowdy SC, Cliby WA, Ra-man S, Weaver JP, Gabbay M, Ngo M, Lentz S, Cass I, Li AJ, Karlan BY, Holschneider CH. Multi-institutional recipro-cal validation study of computed tomography predictors of suboptimal primary cytoreduction in patients with ad-vanced ovarian cancer. J Clin Oncol 2007; 25: 384-389 [PMID: 17264334 DOI: 10.1200/JCO.2006.07.7800]
60 Gemer O, Gdalevich M, Ravid M, Piura B, Rabinovich A, Gasper T, Khashper A, Voldarsky M, Linov L, Ben Shachar I, Anteby EY, Lavie O. A multicenter validation of computer-ized tomography models as predictors of non- optimal pri-mary cytoreduction of advanced epithelial ovarian cancer.
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

165 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Eur J Surg Oncol 2009; 35: 1109-1112 [PMID: 19329270]61 Ferrandina G, Sallustio G, Fagotti A, Vizzielli G, Paglia A,
Cucci E, Margariti A, Aquilani L, Garganese G, Scambia G. Role of CT scan-based and clinical evaluation in the pre-operative prediction of optimal cytoreduction in advanced ovarian cancer: a prospective trial. Br J Cancer 2009; 101: 1066-1073 [PMID: 19738608 DOI: 10.1038/sj.bjc.6605292]
62 Qayyum A, Coakley FV, Westphalen AC, Hricak H, Okuno WT, Powell B. Role of CT and MR imaging in predicting optimal cytoreduction of newly diagnosed primary epithe-lial ovarian cancer. Gynecol Oncol 2005; 96: 301-306 [PMID: 15661212 DOI: 10.1016/j.ygyno.2004.06.054]
63 Yoshida Y, Kurokawa T, Tsujikawa T, Okazawa H, Kotsuji F. Positron emission tomography in ovarian cancer: 18F-deoxy-glucose and 16alpha-18F-fluoro-17beta-estradiol PET. J Ovarian Res 2009; 2: 7 [PMID: 19527525 DOI: 10.1186/1757-2215-2-7]
64 Kumar Dhingra V, Kand P, Basu S. Impact of FDG-PET and -PET/CT imaging in the clinical decision-making of ovar-ian carcinoma: an evidence-based approach. Womens Health (Lond Engl) 2012; 8: 191-203 [PMID: 22375721 DOI: 10.2217/whe.11.91]
65 Nam EJ, Yun MJ, Oh YT, Kim JW, Kim JH, Kim S, Jung YW, Kim SW, Kim YT. Diagnosis and staging of primary ovarian cancer: correlation between PET/CT, Doppler US, and CT or MRI. Gynecol Oncol 2010; 116: 389-394 [PMID: 19926121 DOI: 10.1016/j.ygyno.2009.10.059]
66 Castellucci P, Perrone AM, Picchio M, Ghi T, Farsad M, Nanni C, Messa C, Meriggiola MC, Pelusi G, Al-Nahhas A, Rubello D, Fazio F, Fanti S. Diagnostic accuracy of 18F-FDG PET/CT in characterizing ovarian lesions and staging ovarian cancer: correlation with transvaginal ultrasonog-raphy, computed tomography, and histology. Nucl Med Commun 2007; 28: 589-595 [PMID: 17625380 DOI: 10.1097/MNM.0b013e3281afa256]
67 Risum S, Høgdall C, Loft A, Berthelsen AK, Høgdall E, Nedergaard L, Lundvall L, Engelholm SA. Prediction of sub-optimal primary cytoreduction in primary ovarian cancer with combined positron emission tomography/computed tomography--a prospective study. Gynecol Oncol 2008; 108: 265-270 [PMID: 18055006 DOI: 10.1016/j.ygyno.2007.11.002]
68 Childers JM, Lang J, Surwit EA, Hatch KD. Laparoscopic surgical staging of ovarian cancer. Gynecol Oncol 1995; 59: 25-33 [PMID: 7557611 DOI: 10.1006/gyno.1995.1263]
69 Ghezzi F, Malzoni M, Vizza E, Cromi A, Perone C, Corrado G, Uccella S, Cosentino F, Mancini E, Franchi M. Laparo-scopic staging of early ovarian cancer: results of a multi-in-stitutional cohort study. Ann Surg Oncol 2012; 19: 1589-1594 [PMID: 22086443 DOI: 10.1245/s10434-011-2138-9]
70 Fanning J, Yacoub E, Hojat R. Laparoscopic-assisted cyto-reduction for primary advanced ovarian cancer: success, morbidity and survival. Gynecol Oncol 2011; 123: 47-49 [PMID: 21741079 DOI: 10.1016/j.ygyno.2011.06.020]
71 Angioli R, Palaia I, Zullo MA, Muzii L, Manci N, Calcagno M, Panici PB. Diagnostic open laparoscopy in the management of advanced ovarian cancer. Gynecol Oncol 2006; 100: 455-461 [PMID: 16325244 DOI: 10.1016/j.ygyno.2005.09.060]
72 Deffieux X, Castaigne D, Pomel C. Role of laparoscopy to evaluate candidates for complete cytoreduction in advanced stages of epithelial ovarian cancer. Int J Gynecol Cancer 2006; 16 Suppl 1: 35-40 [PMID: 16515565 DOI: 10.1111/j.1525-1438.2006.00323.x]
73 Fagotti A, Ferrandina G, Fanfani F, Ercoli A, Lorusso D, Rossi M, Scambia G. A laparoscopy-based score to predict surgical outcome in patients with advanced ovarian carcino-ma: a pilot study. Ann Surg Oncol 2006; 13: 1156-1161 [PMID: 16791447 DOI: 10.1245/ASO.2006.08.021]
74 Fagotti A, Ferrandina G, Fanfani F, Garganese G, Vizzielli G, Carone V, Salerno MG, Scambia G. Prospective validation of a laparoscopic predictive model for optimal cytoreduc-
tion in advanced ovarian carcinoma. Am J Obstet Gynecol 2008; 199: 642.e1-642.e6 [PMID: 18801470 DOI: 10.1016/j.ajog.2008.06.052]
75 Brun JL, Rouzier R, Uzan S, Daraï E. External validation of a laparoscopic-based score to evaluate resectability of ad-vanced ovarian cancers: clues for a simplified score. Gynecol Oncol 2008; 110: 354-359 [PMID: 18572226 DOI: 10.1016/j.ygyno.2008.04.042]
76 Rutten MJ, Gaarenstroom KN, Van Gorp T, van Meurs HS, Arts HJ, Bossuyt PM, Ter Brugge HG, Hermans RH, Opmeer BC, Pijnenborg JM, Schreuder HW, Schutter EM, Spijkerboer AM, Wensveen CW, Zusterzeel P, Mol BW, Kenter GG, Buist MR. Laparoscopy to predict the result of primary cytoreductive surgery in advanced ovarian cancer patients (LapOvCa-trial): a multicentre randomized con-trolled study. BMC Cancer 2012; 12: 31 [PMID: 22264278 DOI: 10.1186/1471-2407-12-31]
77 Bristow RE, Chi DS. Platinum-based neoadjuvant che-motherapy and interval surgical cytoreduction for ad-vanced ovarian cancer: a meta-analysis. Gynecol Oncol 2006; 103: 1070-1076 [PMID: 16875720 DOI: 10.1016/j.ygyno.2006.06.025]
78 Kang S, Nam BH. Does neoadjuvant chemotherapy increase optimal cytoreduction rate in advanced ovarian cancer? Me-ta-analysis of 21 studies. Ann Surg Oncol 2009; 16: 2315-2320 [PMID: 19517192 DOI: 10.1245/s10434-009-0558-6]
79 Bristow RE, Eisenhauer EL, Santillan A, Chi DS. Delaying the primary surgical effort for advanced ovarian cancer: a systematic review of neoadjuvant chemotherapy and inter-val cytoreduction. Gynecol Oncol 2007; 104: 480-490 [PMID: 17166564 DOI: 10.1016/j.ygyno.2006.11.002]
80 Morrison J, Haldar K, Kehoe S, Lawrie TA. Chemotherapy versus surgery for initial treatment in advanced ovarian epi-thelial cancer. Cochrane Database Syst Rev 2012; 8: CD005343 [PMID: 22895947 DOI: 10.1002/14651858.CD005343.pub3]
81 Morrison J, Swanton A, Collins S, Kehoe S. Chemotherapy versus surgery for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev 2007; CD005343 [PMID: 17943850 DOI: 10.1002/14651858]
82 Liu EL, Mi RR. Neoadjuvant intraarterial chemotherapy and embolization in treatment of advanced ovarian epithelial carci-noma. Chin Med J (Engl) 2004; 117: 1547-1551 [PMID: 15498381]
83 Chi DS, Bristow RE, Armstrong DK, Karlan BY. Is the easier way ever the better way? J Clin Oncol 2011; 29: 4073-4075 [PMID: 21931018 DOI: 10.1200/JCO.2011.35.9935]
84 Robinson WR. Neoadjuvant chemotherapy is rarely the easy way out. J Clin Oncol 2012; 30: 1563; author reply 1563-1564 [PMID: 22412132]
85 Vergote I, Amant F, Kristensen G, Ehlen T, Reed NS, Casado A. Primary surgery or neoadjuvant chemotherapy followed by interval debulking surgery in advanced ovarian cancer. Eur J Cancer 2011; 47 Suppl 3: S88-S92 [PMID: 21944035 DOI: 10.1016/S0959-8049(11)70152-6]
86 Kumar L, Hariprasad R, Kumar S, Bhatla N, Thulkar S, Shukla NK. Neo-adjuvant chemotherapy in advanced epi-thelial ovarian cancer (EOC): A prospective, randomized study. Indian J Med Paediatr Oncol 2009; 30: 15
87 Onda T, Matsumoto K, Shibata T, Sato A, Fukuda H, Koni-shi I, Kamura T, Yoshikawa H. Phase III trial of upfront de-bulking surgery versus neoadjuvant chemotherapy for stage III/IV ovarian, tubal and peritoneal cancers: Japan Clinical Oncology Group Study JCOG0602. Jpn J Clin Oncol 2008; 38: 74-77 [PMID: 18258715 DOI: 10.1093/jjco/hym145]
88 Kehoe S, Wheeler S. CHORUS (Chemotherapy or Upfront Surgery). A randomised feasibility trial to determine the impact of timing of surgery and chemotherapy in newly di-agnosed patients with advanced epithelial ovarian, primary peritoneal or fallopian tube carcinoma. NCT00075712. Avail-able from: URL: http://clinicaltrials.gov/ct2/show/NCT00075712?term=CHORUS&rank=1. Retrieved on October 9, 2012
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer

166 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
89 Pecorelli S, Odicino F, Favalli G. Interval debulking sur-gery in advanced epithelial ovarian cancer. Best Pract Res Clin Obstet Gynaecol 2002; 16: 573-583 [PMID: 12413935 DOI: 10.1053/beog.2002.0302]
90 Vergote I, De Wever I, Tjalma W, Van Gramberen M, Decloe-dt J, van Dam P. Neoadjuvant chemotherapy or primary de-bulking surgery in advanced ovarian carcinoma: a retrospec-tive analysis of 285 patients. Gynecol Oncol 1998; 71: 431-436 [PMID: 9887245 DOI: 10.1006/gyno.1998.5213]
91 Rodriguez N, Rauh-Hain JA, Shoni M, Berkowitz RS, Muto MG, Feltmate C, Schorge JO, Del Carmen MG, Matulonis UA, Horowitz NS. Changes in serum CA-125 can predict op-timal cytoreduction to no gross residual disease in patients with advanced stage ovarian cancer treated with neoadju-vant chemotherapy. Gynecol Oncol 2012; 125: 362-366 [PMID: 22333992 DOI: 10.1016/j.ygyno.2012.02.006]
92 Schwartz PE, Rutherford TJ, Chambers JT, Kohorn EI, Thiel RP. Neoadjuvant chemotherapy for advanced ovarian can-cer: long-term survival. Gynecol Oncol 1999; 72: 93-99 [PMID: 9889037 DOI: 10.1006/gyno.1998.5236]
93 Shibata K, Kikkawa F, Mika M, Suzuki Y, Kajiyama H, Ino K, Mizutani S. Neoadjuvant chemotherapy for FIGO stage III or IV ovarian cancer: Survival benefit and prognostic factors. Int J Gynecol Cancer 2003; 13: 587-592 [PMID: 14675340 DOI: 10.1046/j.1525-1438.2003.13388.x]
94 Morice P, Dubernard G, Rey A, Atallah D, Pautier P, Pomel C, Lhommé C, Duvillard P, Castaigne D. Results of interval debulking surgery compared with primary debulking sur-gery in advanced stage ovarian cancer. J Am Coll Surg 2003; 197: 955-963 [PMID: 14644284 DOI: 10.1016/j.jamcollsurg.2003.06.004]
95 Loizzi V, Cormio G, Resta L, Rossi CA, Di Gilio AR, Cuc-covillo A, Selvaggi L. Neoadjuvant chemotherapy in ad-vanced ovarian cancer: a case-control study. Int J Gynecol Cancer 2005; 15: 217-223 [PMID: 15823102 DOI: 10.1111/j.1525-1438.2005.15206.x]
96 Kuhn W, Rutke S, Späthe K, Schmalfeldt B, Florack G, von Hundelshausen B, Pachyn D, Ulm K, Graeff H. Neoadjuvant chemotherapy followed by tumor debulking prolongs survival for patients with poor prognosis in International Federation of Gynecology and Obstetrics Stage IIIC ovarian carcinoma. Cancer 2001; 92: 2585-2591 [PMID: 11745193 DOI: 10.1002/1097-0142(20011115)92:10<2585::AID-CNCR1611>3.0.CO;2-#]
97 Fanfani F, Ferrandina G, Corrado G, Fagotti A, Zakut HV, Mancuso S, Scambia G. Impact of interval debulking surgery on clinical outcome in primary unresectable FIGO stage IIIc ovarian cancer patients. Oncology 2003; 65: 316-322 [PMID: 14707451]
98 Redman CW, Warwick J, Luesley DM, Varma R, Lawton FG, Blackledge GR. Intervention debulking surgery in ad-vanced epithelial ovarian cancer. Br J Obstet Gynaecol 1994; 101: 142-146 [PMID: 8305389 DOI: 10.1111/j.1471-0528.1994.tb13080.x]
99 van der Burg ME, van Lent M, Buyse M, Kobierska A, Co-lombo N, Favalli G, Lacave AJ, Nardi M, Renard J, Pecorelli S. The effect of debulking surgery after induction chemother-apy on the prognosis in advanced epithelial ovarian cancer. Gynecological Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer. N Engl J Med 1995; 332: 629-634 [PMID: 7845426 DOI: 10.1056/NEJM199503093321002]
100 Rose PG, Nerenstone S, Brady MF, Clarke-Pearson D, Olt G, Rubin SC, Moore DH, Small JM. Secondary surgical cy-toreduction for advanced ovarian carcinoma. N Engl J Med 2004; 351: 2489-2497 [PMID: 15590951 DOI: 10.1056/NEJ-Moa041125]
101 van der Burg ME, Coens C, van Lent M, Kobierska A, Co-lombo N, Favalli G, Lacava AJ, Theodorovic I, Pecorelli S. The survival benefit of interval debulking surgery (IDS) in advanced ovarian cancer is maintained during ten years; the EORTC GCG 55865 study: 00099. Int J Gynecol Cancer 2005; 15: 79
102 Hegazy MA, Hegazi RA, Elshafei MA, Setit AE, Elshamy MR, Eltatoongy M, Halim AA. Neoadjuvant chemotherapy versus primary surgery in advanced ovarian carcinoma. World J Surg Oncol 2005; 3: 57 [PMID: 16135251 DOI: 10.1186/1477-7819-3-57]
103 Inciura A, Simavicius A, Juozaityte E, Kurtinaitis J, Na-disauskiene R, Svedas E, Kajenas S. Comparison of adju-vant and neoadjuvant chemotherapy in the management of advanced ovarian cancer: a retrospective study of 574 patients. BMC Cancer 2006; 6: 153 [PMID: 16759398 DOI: 10.1186/1471-2407-6-153]
104 Goldie JH, Coldman AJ. The genetic origin of drug resis-tance in neoplasms: implications for systemic therapy. Can-cer Res 1984; 44: 3643-3653 [PMID: 6744284]
105 Ansquer Y, Leblanc E, Clough K, Morice P, Dauplat J, Mathevet P, Lhommé C, Scherer C, Tigaud JD, Benchaib M, Fourme E, Castaigne D, Querleu D, Dargent D. Neoadju-vant chemotherapy for unresectable ovarian carcinoma: a French multicenter study. Cancer 2001; 91: 2329-2334 [PMID: 11413522 DOI: 10.1002/1097-0142(20010615)91:12<2329::AID-CNCR1265>3.0.CO;2-U]
106 Stoeckle E, Boubli B, Floquet A, Brouste V, Sire M, Croce S, Thomas L, Guyon F. Optimal timing of interval debulking surgery in advanced ovarian cancer: yet to be defined? Eur J Obstet Gynecol Reprod Biol 2011; 159: 407-412 [PMID: 21835539 DOI: 10.1016/j.ejogrb.2011.07.014]
107 Pölcher M, Mahner S, Ortmann O, Hilfrich J, Diedrich K, Breitbach GP, Höss C, Leutner C, Braun M, Möbus V, Karbe I, Stimmler P, Rudlowski C, Schwarz J, Kuhn W. Neoadjuvant chemotherapy with carboplatin and docetaxel in advanced ovarian cancer--a prospective multicenter phase II trial (PRI-MOVAR). Oncol Rep 2009; 22: 605-613 [PMID: 19639211 DOI: 10.3892/or_00000479]
108 Stashwick C, Post MD, Arruda JS, Spillman MA, Behbakht K, Davidson SA, Kelly MG. Surgical risk score predicts suboptimal debulking or a major perioperative compli-cation in patients with advanced epithelial ovarian, fal-lopian tube, or primary peritoneal cancer. Int J Gynecol Cancer 2011; 21: 1422-1427 [PMID: 21997170 DOI: 10.1097/IGC.0b013e31822c7704]
109 Bland AE, Everett EN, Pastore LM, Andersen WA, Tay-lor PT. Predictors of suboptimal surgical cytoreduction in women with advanced epithelial ovarian cancer treated with initial chemotherapy. Int J Gynecol Cancer 2008; 18: 629-636 [PMID: 17986246 DOI: 10.1111/j.1525-1438.2007.01114.x]
110 Onda T, Yoshikawa H, Yasugi T, Matsumoto K, Taketani Y. The optimal debulking after neoadjuvant chemotherapy in ovarian cancer: proposal based on interval look during upfront surgery setting treatment. Jpn J Clin Oncol 2010; 40: 36-41 [PMID: 19820253 DOI: 10.1093/jjco/hyp127]
P- Reviewer: Yokoyama Y S- Editor: Gou SX L- Editor: Hughes D E- Editor: Zheng XM
Tangjitgamol S et al . Neoadjuvant chemotherapy and interval debulking surgery in ovarian cancer
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.167
World J Obstet Gynecol 2013 November 10; 2(4): 167-175ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Cytoreductive surgery and HIPEC after neoadjuvant chemotherapy for advanced epithelial ovarian cancer
Marco Lotti, Luisa Maria Busci, Luca Campanati, Fausto Catena, Federico Coccolini, Naoual Bakrin, Pierandrea De Iaco, Giorgio Ercolani, Giuseppe Grosso, Michele Pisano, Elia Poiasina, Diego Rossetti, Martina Rossi, Claudio Zamagni, Paolo Bertoli, Antonio Daniele Pinna, Luigi Frigerio, Luca Ansaloni
Marco Lotti, Luca Campanati, Federico Coccolini, Michele Pisano, Elia Poiasina, Diego Rossetti, Paolo Bertoli, Luca Ansaloni, Unit of General Surgery 1, Papa Giovanni XXIII Hos-pital, 24128 Bergamo, ItalyLuisa Maria Busci, Giuseppe Grosso, Diego Rossetti, Luigi Frigerio, Unit of Gynecology and Obstetrics, Papa Giovanni XXIII Hospital, 24128 Bergamo, ItalyFausto Catena, Giorgio Ercolani, Antonio Daniele Pinna, Unit of General Surgery, St.Orsola-Malpighi University Hospital, 40138 Bologna, ItalyNaoual Bakrin, Department of Gynecology, Lyon Sud Hospital, 69310 Pierre Benite, FrancePierandrea De Iaco, Martina Rossi, Unit of Gynecology and Obstetrics, St.Orsola-Malpighi University Hospital, V40138 Bo-logna, ItalyClaudio Zamagni, Medical Oncology, St.Orsola-Malpighi Uni-versity Hospital, 40138 Bologna, ItalyAuthor contributions: Lotti M and Ansaloni L designed the study protocol and wrote the article; Busci LM, Catena F, Campanati L, Coccolini F, Bakrin N, De Iaco P, Ercolani G, Grosso G, Pisano M, Poiasina E, Rossetti D, Rossi M, Zamagni C, Bertoli P, Pinna AD and Frigerio L were involved in patients’ recruitment, treatment and in providing data for analysis.Correspondence to: Dr. Luca Ansaloni, MD, Unit of General Surgery 1, Papa Giovanni XXIII Hospital, Piazza OMS, Organiz-zazione mondiale della sanità 1, 24128 Bergamo, Italy. [email protected]: +39-3-5269310 Fax: +39-3-5266898Received: February 21, 2013 Revised: April 23, 2013Accepted: July 9, 2013Published online: November 10, 2013
AbstractAIM: To reduce postoperative complications and to make possible an optimal cytoreduction, neoadjuvant chemotherapy (NACT) followed by interval debulking surgery has been applied with encouraging results.
METHODS: Between December 2009 and February
2012, patients with stage ⅢC-Ⅳ epithelial ovarian can-cer (EOC) underwent diagnostic laparoscopy, to assess the feasibility of optimal debulking surgery. The modi-fied Fagotti score was applied to assess the feasibility of resection with zero residual tumor. Patients who were not candidate for upfront debulking surgery were sub-mitted to NACT, then reassessed according to the RE-CIST 1.1 criteria and submitted to cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) if they showed clinical response or stable dis-ease. The remaining cycles of adjuvant systemic chem-otherapy (ASCT) were administered postoperatively, to complete 6 cycles of systemic chemotherapy.
RESULTS: Nine patients were included. Clinical re-sponse to NACT was complete in 3 patients and partial in 5 patients; one patient had stable disease. All pa-tients underwent CRS resulting in CC0 disease prior to HIPEC. Average operative time was 510 min. Average intensive care unit stay was 2 d. Average postoperative hospital stay was 25 d. No postoperative mortality was observed. One patient experienced pelvic abscess. One patient refused ASCT. The remaining 8 patients started ASCT. Average time to chemotherapy was 36 d. All patients are alive, with an average follow up of 11 mo. Eight patients are disease-free at follow up.
CONCLUSION: HIPEC after CRS for advanced EOC is feasible with acceptable morbidity and mortality. NACT may increase the chance for achieving complete cyto-reduction. Phase 3 studies are needed to determine the effects of HIPEC on survival.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Peritoneal carcinomatosis; Ovarian cancer; Cytoreductive surgery; Intraperitoneal chemotherapy; Hyperthermic intraperitoneal chemotherapy; Hyperthermia
BRIEF ARTICLE
167 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Lotti M et al . Preliminary report of a bi-centric observational study
Core tip: This is a report of a phase 2 prospective obser-vational study, which served as a pilot study for the CHO-RINE trial protocol (http://www.chorine.org). Our pilot study supports the feasibility of neoadjuvant chemo-therapy (NACT) followed by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for upfront treatment of advanced epithelial ovarian can-cer. This combined therapy does not reduce the possi-bility to start the postoperative systemic chemotherapy in an acceptable period of time. We believe that in the upfront setting NACT can better select chemorespon-sive patients, increasing their chance to take advantage from HIPEC, reducing the surgical stress and the peri-operative complications.
Lotti M, Busci LM, Campanati L, Catena F, Coccolini F, Bakrin N, De Iaco P, Ercolani G, Grosso G, Pisano M, Poiasina E, Rossetti D, Rossi M, Zamagni C, Bertoli P, Pinna AD, Frigerio L, Ansa-loni L. Cytoreductive surgery and HIPEC after neoadjuvant che-motherapy for advanced epithelial ovarian cancer. World J Obstet Gynecol 2013; 2(4): 167-175 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/167.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.167
INTRODUCTIONOvarian cancer is the third commonest gynecological neo-plasm[1] and accounts for 5% of all female cancer deaths. Epithelial ovarian cancer (EOC) accounts for more than 70% of all ovarian cancers. EOC typically presents with unclear gastrointestinal and constitutional symptoms, like abdominal bloating, distension, weight loss, and fatigue[2]. Due to heterogeneity of these symptoms, nearly 70% of patients with EOC are diagnosed with advanced stage disease (stage Ⅲ or Ⅳ)[3,4].
It is well known that primary cytoreductive surgery (CRS) followed by platinum-based systemic adjuvant chemotherapy (SACT), when indicated, is the mainstay of treatment for EOC: in this setting, the aim of primary surgery is to remove as much tumor as possible (possibly all the tumor), since the amount of residual tumor is one of the most important prognostic factors for survival[5-7]. Unfortunately, the achievement of optimal cytoreduc-tion (residual tumor less than 1-2 cm), mainly in advanced EOC, is not always possible, due to the amount of disease at presentation, patient’s co-morbidities, and the experi-ence of the surgeon[8-11]. Not performing optimal or com-plete CRS results in loosing the chance for longer survival.
To help achieving complete resection rate, the concept of neoadjuvant chemotherapy (NACT) followed by inter-val CRS (ICRS) has been developed for patients deemed to have unresectable disease (stage ⅢC/Ⅳ EOC). From several retrospective and prospective case-control studies, along with recent meta-analyses, it appears that NACT-ICRS compared to primary CRS offers less postoperative morbidity to patients[12]. Moreover, results of the prospec-
tive randomized controlled trial (RCT) EORTC 55971 are consistent with the majority of the previous studies, sug-gesting that NACT-ICRS results in the same survival but fewer complications than primary CRS in patients with stage ⅢC/Ⅳ EOC[13].
During its natural history, EOC tends to be chemo-sensitive and to confine itself to the surface of the peri-toneal cavity for a long period of time. These features make it an obvious target for intraperitoneal chemothera-py (IPCT), which is given by infusion of the chemothera-peutic agents directly into the peritoneal cavity. This may increase the anticancer effect with fewer systemic adverse effects in comparison to intravenous therapy. To opti-mize drug distribution, IPCT has also been applied intra-operatively, immediately after CRS. Different techniques have been used for intraoperative IPCT. An advantage of intraoperative use is that IPCT can be administered even under hyperthermic conditions, which are poorly tolerat-ed by a patient who is awake. Hyperthermia is directly cy-totoxic and enhances the efficacy and penetration depth of many drugs, while the mild locoregional hyperthermia that is used has no significant adverse effects.
The feasibility of hyperthermic intraperitoneal che-motherapy (HIPEC), as a treatment for peritoneal car-cinomatosis, was first demonstrated by Spratt et al[14]. Its development continued under Dr. Sugarbaker in the mid-1990s, who advocated a combined procedure of CRS with peritonectomy procedures (aimed at resecting peri-toneal surfaces with tumor implants) and associated vis-ceral dissections, with maximal surgical effort to remove as much tumor as macroscopically possible, followed by direct instillation of heated IPCT to address microscopic residual disease[15]. This treatment has already been shown to be beneficial for patients with peritoneal carcinomato-sis from gastric cancer[16] appendiceal cancer[17], colorectal cancer[18] and peritoneal mesothelioma[19].
The rationale to use CRS and HIPEC in EOC stands on a few considerations. First, phase 3 RCTs have estab-lished the superiority (improved progression-free and overall survival) of intraperitoneal cisplatin-based chemo-therapy compared to the systemic delivery of the agent in the treatment of small-volume residual advanced EOC[20-22]. Second, a number of prospective phase 2 studies and retro-spective institutional experiences have shown the feasibility of employing HIPEC[23-28], when complete macroscopic cytoreduction is achieved prior to the delivery of the anti-neoplastic agents. However a few concerns still exist about the application of IPCT because of the fear of possible complication linked to this way of chemotherapy admin-istration. The prospected main risk is to delay or to defini-tively obstacle the possibility to start systemic chemotherapy as soon as possible after the surgery.
For these reasons we performed a bi-centric prospec-tive observational pilot study combining NACT with carboplatin (CBCDA) and paclitaxel (PTX) to CRS and HIPEC with cisplatin (CDDP) and PTX in upfront treat-ment of advanced EOC. The aim of this study was to evaluate the feasibility of CRS and HIPEC in patients
168 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

with stage ⅢC/Ⅳ EOC, who showed partial or complete response after NACT, in terms of percentage of com-plete cytoreduction (residual disease < 2.5 mm), toxicity, postoperative complications, postoperative mortality, and time elapsed till the start of systemic chemotherapy (time to chemotherapy, TTC).
MATERIALS AND METHODSThe Study design was approved by our local Ethics Com-mittee. The selection criteria were the following: (1) In-clusion criteria. Female adult women (18 to 70 years old) patients, with EOC (FIGO stage ⅢC or Ⅳ), performance status (ECOG) 0, 1 or 2, signed informed consent, body mass index < 35 kg/m2; and (2) Exclusion criteria. Impos-sibility of an adequate follow-up, presence of other active neoplasms, active infection or other concurrent medical condition that could interfere in the ability of patients to receive the proposed treatment according to protocol, complete bowel obstruction, abnormal bone marrow indi-ces or renal and liver function, ASA Ⅳ or Ⅴ.
Patients with advanced EOC (stage ⅢC-Ⅳ) were sub-mitted to a diagnostic laparoscopy, to assess the feasibility of optimal debulking surgery with no residual disease at the end of the procedure.
Laparoscopy was performed by trained gynecologists and surgeons. In presence of ascitic fluid, a sample for cytology was obtained; otherwise, a lavage of the perito-neal cavity was performed; biopsy of eventual pelvic and peritoneal masses was obtained.
The modified Fagotti scoring system was applied[29], to assess the feasibility of resection with zero residual tumor. Patients with a score ≥ 4 were judged not can-didate for debulking surgery: a score ≥ 4 was chosen as a compromise to warrant adequate accrual, because the higher risk of inappropriate lack of exploration (27.3%) was likely to be balanced by the documented efficacy of NACT in this type of tumor.
After laparoscopic evaluation, patients who were not candidate for upfront debulking surgery were submitted to NACT with CBCDA AUC-5 and PTX 175 mg/m2, administered every 21 d.
After 3-6 cycles of chemotherapy, patients were re-as-sessed by clinical, radiologic [computed tomography (CT) scan] and laboratory (CA 125) evaluation and assigned to one of four subgroups, according to the RECIST 1.1 criteria: complete clinical response (cCR), partial clinical response (cPR), clinically stable disease (cSD), clinically disease progression (cDP)[30]. Patients with cCR, cPR or cSD after NACT, were submitted to CRS with radical in-tent.
After laparotomy, a detailed pattern of peritoneal dif-fusion of the disease was drawn according to the Perito-neal Cancer Index (PCI) scoring system[31] and then CRS was as follows: hysterectomy, bilateral salpingoophorec-tomy, pelvic and peri-aortic lymphadenectomy, radical omentectomy, random biopsy of peritoneal surfaces, as-sociated to any surgical procedure needed to obtain a ≤
2.5 mm residual tumor (peritonectomy, bowel resection, diaphragmatic stripping, gastric resection, etc.).
After CRS, patients with adequate cytoreduction (CC0, no residual disease; CC1, residual tumor ≤ 2.5 mm)[29] were submitted to HIPEC with CDDP (100 mg/m2 of body surface area) and PTX (175 mg/m2 of body surface area) at 42 ℃, with an intraperitoneal infusion time of 90 min. HIPEC was delivered using an open abdomen (coliseum) technique.
Toxicity was recorded in accordance to the National Cancer Institute Common Toxicity Criteria (NCI CTC). Surgical complications were considered as a component of the total toxicity and also registered in accordance of the NCI CTC. Treatment-related death was defined as death due to toxicity following cytoreduction and HIPEC without time interval restrictions.
As soon as the conditions of the patients allowed it (and in any case at least 4 wk after surgery) the remaining cycles of SACT were administered with the same sched-ule of NACT, to complete 6 cycles of systemic chemo-therapy.
RESULTSBetween December 2009 and February 2012, 36 patients with advanced EOC (stage ⅢC-Ⅳ) were evaluated and submitted to a diagnostic laparoscopy: 15 patients were selected who were not candidate for upfront debulk-ing surgery (13 stage ⅢC, 2 stage Ⅳ) and submitted to NACT with CBCDA AUC-5 and PTX 175 mg/m2, ad-ministered every 21 d.
After three cycles of NACT, 6 patients were excluded for evidence of cDP; in the remaining 9 patients, cCR was observed in 3 cases, cPR was observed in 5 cases, one patient had cSD: these 9 patients were enrolled in our pilot study.
Six patients underwent CRS and HIPEC after four cy-cles of NACT, 2 patients after three cycles of NACT and 1 patient after six cycles of NACT, in order to achieve op-timal clinical response (> 50%, according to the RECIST 1.1 criteria). Average age was 55.8 years (median 55 years, range 45-65 years).
At operation, average PCI was 14 (median 13, range 5-28). All patients underwent CRS resulting in CC0 dis-ease prior to HIPEC. Supramesocolic compartment peri-tonectomy was required in 5 patients. Six patients under-went colorectal resection and anastomosis, with temporary diverting ileostomy. More clinical details are available in Table 1.
All patients underwent HIPEC with CDDP 100 mg/m2 of body surface area and PTX 175 mg/m2 of body sur-face area at 42 ℃, with an intraperitoneal infusion time of 90 min.
Average operative time was 510 min (median 520 min, range 400-595 min). Average intensive care unit stay was 2 d (median 2 d, range 1-5 d). Average postoperative hos-pital stay was 25 d (median 22 d, range 9-35 d).
No postoperative mortality was observed. One patient
169 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Lotti M et al . Preliminary report of a bi-centric observational study

experienced a grade 3 postoperative complication (pelvic abscess), requiring reoperative debridement and drain-age. Grade 3 leukopenia was observed in 3 patients and was treated with administration of granulocyte colony-stimulating factor; one of these patients had also grade 3 thrombocytopenia. One more patient experienced Grade 3 thrombocytopenia, which resolved spontaneously (Table 2).
One patient refused SACT. The remaining 8 patients started SACT. Average TTC was 36 d (median 29 d, range 25-62 d). All patients are alive, with an average follow up of 12 mo (median 11 mo, range 2-28 mo). Eight patients are disease-free to date. One patient showed a raising CA 125 after 10 mo of follow up. The disease-free survival curve for the 9 patients included in the study is shown in Figure 1.
DISCUSSIONIn our presented study, 36 women with advanced EOC were evaluated by means of laparoscopy and 15 of them (41.6%) were judged not suitable for optimal CRS, adopt-ing the modified Fagotti score with a cut-off of 4. These 15 patients were treated with NACT, and then 9 of them (those with cCR, cPR or cSD) underwent CRS and HIPEC with complete cytoreduction (CC0), few postop-erative complications and no mortality. All patients but one, who refused it, were able start SACT in an average time of 36 d after CRS + HIPEC. All of them were able to complete SACT after CRS and HIPEC. Eight out of 9 patients are disease free to date and all of them are alive after a median follow up of 11 mo.
Even if the number of patients enrolled is small, our study shows that performing CRS and HIPEC after NACT was safe and led to a 100% rate of optimal cy-toreduction, in patients with advanced EOC previously judged not suitable for complete cytoreduction at diag-nostic laparoscopy. Except for the patient who refused postoperative SACT, all of the patients were able to com-plete SACT after CRS and HIPEC, with an acceptable TTC.
The strategy adopted in our study is not the recog-nized standard treatment of advanced EOC, namely maximal CRS followed by platinum-based SACT: never-theless, patients are selected for this strategy only if they are judged not suitable for complete CRS by means of laparoscopy and a recognized scoring system[29]. Those patients are offered CRS after NACT and HIPEC is added to address microscopic residual disease: our study shows that this strategy is feasible, safe and does not flaw the completion of systemic CT.
Follow up is short, but preliminary results are encour-aging and comparable to those achieved in other phase 2 studies available in the literature.
A recent article by Deraco et al[32] reported the results of a multi-center phase 2 trial using CRS and closed-abdomen HIPEC with CDDP and doxorubicin, in front-line treatment of advanced EOC. The authors accrued 26 patients over 6 years in four different Italian centers, achieving macroscopically complete cytoreduction in 15
170 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Clinical characteristics of the ovarian cancer patients
Patient Age (yr) BMI (kg/m2) Stage Histology Grade PCI No. of cycle NACT
Clinical response (%)
CC
1 47 23 ⅢC Sierous 3 15 4 100 02 50 31 Ⅳ Sierous 3 12 4 > 50 03 53 31 Ⅳ Endometrioid 3 6 4 100 04 65 19 ⅢC Sierous 2 8 4 > 50 05 55 24 ⅢC Sierous 3 21 4 100 06 55 21 ⅢC Undifferentiated 3 28 4 < 50 07 47 22 ⅢC Endometrioid 3 5 3 > 50 08 62 22.9 ⅢC Sierous 3 14 6 > 50 09 65 20 ⅢC Sierous 3 13 3 > 50 0
BMI: Body mass index; PCI: Peritoneal cancer index; NACT: Neoadjuvant chemotherapy.
Table 2 Postoperative adverse events n (%)
Patients CTCAE grade Treatment
Postoperative death 0 (0)Reoperation 1 (11)Types of complications 5 (56) Grade 3-5 morbidity 5 (56) Pelvic abscess 1 (11) 3 Reoperation Leukopenia 3 (33) 3 G-CSF Thrombocytopenia 2 (22) 3 Observation
G-CSF: Granulocyte colony-stimulating factor.
1.0
0.8
0.6
0.4
0.2
0.0
0 5 10 15 20 25t /mo
%
Figure 1 Disease free survival curve.
Lotti M et al . Preliminary report of a bi-centric observational study

patients and only minimal residual disease (≤ 2.5 mm) in the remaining 11.
Four patients experienced major complications, includ-ing one postoperative death. 25 out of 26 patients started SACT after CRS + HIPEC, with a median TTC of 46 d. Five-year overall survival was 60.7% and progression-free survival was 15.2%. Although these results are encouraging, in absence of a phase 3 trial, before suggesting that CRS + HIPEC could be a valid strategy for upfront treatment of advanced EOC a few considerations should be done.
It is well known that CRS, especially in very advanced cases, is associated to a high incidence of postoperative morbidity and mortality[33-35] and that the HIPEC proce-dure could even increase the incidence of perioperative complications[36]. For these reasons, HIPEC should be considered a burdensome procedure and before perform-ing it, every effort is needed to select which patients will achieve the maximum benefit from it.
Although the majority of patients with EOC (up to 80%) respond to first-line systemic platinum based che-motherapy, 20% of them are resistant or refractory[37]. According to these data, a certain percentage of women with chemoresistant tumor cells will not benefit from ad-ministration of high dose HIPEC after upfront CRS for advanced EOC.
Even if not detailed in the article by Deraco et al[32], the survival curve of the patients accrued in their phase 2 study shows that almost 30% of the patients recurred at 1 year. It is reasonable to suppose that these patients were not chemo-sensitive.
HIPEC should be active on chemosensitive cells and the procedure could be avoided in women with insensitive tumor cells. Even if NACT followed by CRS + HIPEC did not show better results in terms of PFS and OS[13], the evaluation of patients’ response to NACT could be a strategy to select for HIPEC only the patients who show a chemo-sensitivity to platinum and taxanes.
There are some phase 2 observational studies[32,38-51] in the literature reporting a total of 295 patients with prima-ry EOC treated with CRS and HIPEC in upfront setting, with an approach that is similar to the study of Deraco et al (Table 3).
All these phase 2 observational studies include patients where in most cases a great surgical effort has been made and the chemosensibility state was not known: in only 107 cases (36.3%) the patients had undergone NACT to test in-vivo chemosensitivity before CRS and HIPEC.
The idea of proposing NACT in patients with very advanced EOC and performing ICRS associated to HIPEC, like in our study, could have various advantages. First, NACT can select “in vivo” chemosensitive patients, thus making possible to offer the HIPEC procedure only to those patients that are highly responsive to the chemo-therapeutic molecules. Second, NACT reduces the surgi-cal load and consequently surgery obtains no residual tu-mor in the vast majority of this set of patients. Third, the less radical surgery required is associated to lesser periop-erative complications, permitting shorter recovery to start with postoperative chemotherapy. And last, this strategy could be offered to an high proportion of women with advanced EOC[13,52].
In our study, 6 out of 15 women (40%) showed cDP after NACT: this percentage of non-responders to NACT is low compared to those of previous studies including EORTC trial[13]. Anyway, we should consider that the decision to adopt the RECIST criteria in our study was made to clearly select highly responsive patients. In fact, after CRS all women were CC0.
If we consider the EORTC study, 295 out of 334 women were submitted to CRS after NACT, and residual tumor < 1 cm was achieved in 80.6% of 295 women: this means that 97 out of 334 women assigned to NACT (30%) were non-responders. Moreover, it is reasonable to think that if a residual tumor < 2.5 mm (CC1) or no residual
171 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 3 Studies on cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in upfront setting
Ref. Patients (neoadjuvant)
Type of NACT
HIPEC (technique, drug and dose, temperature, lenght of infusion time)
Period Country
Steller et al[46] 2 C, carboplatin 800-1200 mg/m2, 41-43 ℃, 90 min NR United StatesLook et al[44] 4 O, doxorubicin, NR, NR 1988-2001 SingaporePiso et al[45] 8 (1) iv TPB O, cisplatin 75 mg/m2, NR, 90 min 1995-1999 GermanyReichman et al[43] 9 (9) iv PB O, cisplatin 50 mg/m2, 40 ℃, 90 min 2001-2004 United StatesRufián et al[42] 19 O, paclitaxel 60 mg/m2, 41-43 ℃, 60 min 1997-2004 SpainRoviello et al[47] 45 (31) iv TPB C, mitomycin C 25 mg/m2 + cisplatin 100 mg/m2, 41-43 ℃, 60 min 2000-2009 ItalyPavlov et al[39] 31 C, doxorubicin 0.1 mg/kg (+ EPIC 15 mg/m2 × 5 d), NR, NR 1995-2007 SerbiaGuardiola et al[40] 31 (31) iv TPB O, cisplatin 180 mg, 37 ℃, 120min 2003-2006 FranceDi Giorgio et al[41] 22 (4) iv TPB C, cisplatin 75 mg/m2, 42-43 ℃, 60 min 2000-2007 ItalyLim et al[48] 30 (14) NR C, cisplatin 75 mg/m2, 41.5 ℃, 90 min 2007-2009 KoreaFrenel et al[49] 7 (7) iv TPB O, oxaliplatin, 360-460 mg/m2, 41-43 ℃, 30 min 2005-2008 FranceMuñoz-Casares et al[50] 10 (10) ip TB (+ in 5
pts iv PB)O, paclitaxel, 60 mg/m2, 41-43 ℃, NR 2004-2009 Spain
Parson et al[38] 51 C, carboplatin 1000 mg +mitomycin C 30 mg, 41-42 ℃, 60-120 min 1996-2009 United StatesDeraco et al[32] 26 C, cisplatin 40 mg/L of perfusate + doxorubicin 15 mg/L of
perfusate), 42.5 ℃, 90 min2004-2010 Italy
NACT: Neoadjuvant chemotherapy; O: Open method; C: Closed method; TPB: Taxanes and platinum based; PB: Platinum based; TB: Taxanes based; NR: Not reported; HIPEC: Hyperthermic intraperitoneal chemotherapy.
Lotti M et al . Preliminary report of a bi-centric observational study

tumor (CC0) was used in the EORTC trial to define opti-mal cytoreduction after CRS, a higher percentage of non-responders to NACT could have been found.
Although according to the results of our study, NACT could offer the opportunity to reduce the surgical load needed to achieve optimal cytoreduction and make pos-sible to perform CRS and HIPEC with only minor com-plications and no postoperative mortality, many scientists agree that RCTs are needed to confirm the potential ad-vantages of HIPEC associated to CRS in all time points of the natural history of advanced EOC, but especially in upfront setting[53-55]. Only RCTs will clarify the role of CRS and HIPEC in advanced EOC, as already has been done for colon and gastric cancer[56,57].
To our knowledge, regarding the use of CRS and HIPEC in advanced EOC, at least four RCTs are ongoing. The first study is a Korean RCT including primary and recurrent EOC[58]. Two different RCTs have been pro-posed by St George Hospital in Sydney (Australia), to test HIPEC in primary and recurrent EOC[59]. A third multi-centric RCT (CHIPOR trial), testing HIPEC in recurrent EOC, has been planned by French surgeons[60]. The fourth RCT, conceived by the Netherlands Cancer Institute (OVHIPEC trial), evaluates the efficacy of secondary cy-toreduction, with or without HIPEC, in patients with ad-vanced EOC, eligible for interval debulking surgery either following primary chemotherapy or following incomplete primary debulking and chemotherapy. The experimental group undergoes interval debulking with HIPEC (CDDP 100 mg/m2) at the end of CRS, while the control group is treated only with interval debulking surgery[61].
Similarly to the last described RCT, where HIPEC is used in upfront setting after primary chemotherapy, our groups have recently proposed the transformation of our above mentioned pilot study (following its philosophy) in a RCT called CHORINE Study (Cytoreduction and Hipec in the treatment of OvaRIaN cancEr). This study project is a multicentre phase 3 prospective RCT, comparing CRS and HIPEC (CDDP+PTX) vs CRS alone in stage ⅢC un-resectable EOC with partial or complete response after 3 systemic cycles of CBCDA + PTX (NACT), followed by further 3 cycles of CBCDA + PTX (SACT). The choice to add PTX to CDDP in the HIPEC perfusate takes count of the negligible toxicity observed in our pilot study and the efficacy of PTX reported in the literature, where a significant increase in survival is observed when heated intraperitoneal PTX is administered after CRS[62-67]. In the CHORINE study the primary outcome is 2-year disease-free survival.
Only patients with complete or cPR after the 3 cycles of NACT will be eligible for the study and, after signing the informed consent form, will be submitted to CRS with radical intent. The randomization (HIPEC vs no HI-PEC) will be applied during the surgical procedure after adequate CRS (residual tumor ≤ 2.5 mm): patients with suboptimal cytoreduction (residual tumor > 2.5 mm) are considered not suitable for randomization and will be ex-cluded.
The drug schedule elected in the CHORINE study is CDDP 100 mg/m2 of body surface area and PTX 175 mg/m2 of body surface area with an intraperitoneal infusion time length of 90 min.
A sample size of 47 patients for each group has been calculated to reach a confidence level of 95% with a pow-er of 80%, considering a 45% and 75% disease-free sur-vival at 2 years of follow-up in non-HIPEC and HIPEC group respectively.
On the one hand the advantages of CHORINE study are the following: (1) NACT selects for inclusion in the study only patients in whom there is a clinical response (test of in-vivo chemosensitivity) and then a response to HIPEC is expected; (2) response to NACT should make the cytoreductive effort less demanding, increasing the occurrence of complete CRS and presumably lowering the morbidity; and (3) HIPEC is the only variable be-tween groups in the study, making it possible to evaluate its effectiveness regardless of CRS, because a radical and complete cytoreduction is required either in the experi-mental arm than in the control group (as requested by many authors in the literature[53]).
On the other hand, the major limitation of the study is that the control group is not the recognized standard treatment for advanced EOC, namely maximal CRS fol-lowed by platinum-based SACT.
The CHORINE study has been approved by our review board and we are in the process to complete the administrative requirements and recruiting the other par-ticipating centers.
In conclusion, our pilot study supports the feasibil-ity of NACT followed by CRS and HIPEC for upfront treatment of advanced EOC. This combined therapy does not reduce the possibility to start the post-operative systemic chemotherapy in an acceptable period of time. We believe that in the upfront setting NACT can better select chemoresponsive patients, reducing thus the surgi-cal stress and the perioperative complications.
Based on the results of this pilot study, our proposed phase 3 trial (the CHORINE study) will clarify the relative benefits of HIPEC, that have been though to support the course of action of CRS by targeting microscopic residual tumoral intraperitoneal disease in advanced EOC.
COMMENTSBackgroundOvarian cancer is the third commonest gynecological neoplasm and accounts for 5% of all female cancer deaths. Epithelial ovarian cancer (EOC) accounts for more than 70% of all ovarian cancers. Primary cytoreductive surgery (CRS) followed by platinum-based systemic adjuvant chemotherapy (SACT), when in-dicated, is the mainstay of treatment: unfortunately, the achievement of optimal cytoreduction (residual tumor less than 1-2 cm), mainly in advanced EOC, is not always possible. To help achieving complete resection rate, the concept of neoadjuvant chemotherapy (NACT) followed by interval CRS has been devel-oped for patients deemed to have unresectable disease (stage ⅢC/Ⅳ EOC). A number of prospective phase 2 studies and retrospective institutional experi-ences have shown the feasibility of employing hyperthermic intraperitoneal chemotherapy (HIPEC) when complete macroscopic cytoreduction is achieved; however a few concerns still exist. For these reasons the authors performed a bi-centric prospective observational pilot study combining NACT with carbo-
172 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
COMMENTS
Lotti M et al . Preliminary report of a bi-centric observational study

173 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
platin (CBCDA) and paclitaxel (PTX) to CRS and HIPEC with cisplatin (CDDP) and PTX in upfront treatment of advanced EOC. The aim of this study was to evaluate the feasibility of CRS and HIPEC in patients with stage ⅢC/Ⅳ EOC, who showed partial or complete response after NACT, in terms of percentage of complete cytoreduction (residual disease < 2.5 mm), toxicity, postoperative complications, postoperative mortality, and time elapsed till the start of systemic chemotherapy (time to chemotherapy, TTC).Research frontiersBased on the results of this pilot study, the authors developed the CHORINE study protocol (www.chorine.org), a multicentre phase 3 prospective RCT, comparing CRS and HIPEC (CDDP + PTX) vs CRS alone in stage ⅢC un-resectable EOC with partial or complete response after 3 systemic cycles of CBCDA+PTX (NACT), followed by further 3 cycles of CBCDA + PTX (SACT). Only RCTs will clarify the role of CRS and HIPEC in advanced EOC, as already has been done for colon and gastric cancer.Innovations and breakthroughsThe cornerstones of developing the CHORINE study protocol are the following: (1) NACT selects for inclusion in the study only patients in whom there is a clini-cal response (test of in-vivo chemosensitivity) and then a response to HIPEC is expected; (2) response to NACT should make the cytoreductive effort less de-manding, increasing the occurrence of complete CRS and presumably lowering the morbidity; and (3) HIPEC is the only variable between groups in the study, making it possible to evaluate its effectiveness regardless of CRS, because a radical and complete cytoreduction is required either in the experimental arm than in the control group (as requested by many authors in the literature).ApplicationsThe study results suggest that NACT followed by CRS and HIPEC is a feasible strategy for upfront treatment of advanced EOC.TerminologyCRS: the aim of surgery for advanced EOC is to remove as much tumor as possible, since the amount of residual tumor is one of the most important prog-nostic factors for survival. HIPEC: during its natural history, EOC tends to be chemosensitive and to confine itself to the surface of the peritoneal cavity for a long period of time. These features make it an obvious target for intraperito-neal chemotherapy (IPCT), which is given by infusion of the chemotherapeutic agents directly into the peritoneal cavity. This may increase the anticancer ef-fect with fewer systemic adverse effects in comparison to intravenous therapy. To optimize drug distribution, IPCT has also been applied intraoperatively, immediately after CRS. An advantage of intraoperative use is that IPCT can be administered even under hyperthermic conditions, which are poorly tolerated by a patient who is awake. Hyperthermia is directly cytotoxic and enhances the efficacy and penetration depth of many drugs, while the mild locoregional hyperthermia that is used has no significant adverse effects.Peer reviewThe authors presented preliminary results from a pilot study evaluating the fea-sibility and safety of HIPEC after NACT and CRS in 9 patients with advanced ovarian cancer. They showed that this strategy was feasible and safe and had acceptable TTC. The topic of HIPEC after CRS for advanced ovarian cancer is interesting and worth being evaluated in a large-scale clinical study.
REFERENCES1 Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Can-
cer statistics, 2007. CA Cancer J Clin 2007; 57: 43-66 [PMID: 17237035 DOI: 10.3322/canjclin.57.1.43]
2 Goff BA, Mandel L, Muntz HG, Melancon CH. Ovarian carci-noma diagnosis. Cancer 2000; 89: 2068-2075 [PMID: 11066047]
3 Cannistra SA. Cancer of the ovary. N Engl J Med 2004; 351: 2519-2529 [PMID: 15590954 DOI: 10.1056/NEJMra041842]
4 Karlan BY, Markman MA, Eifel PJ. Ovarian cancer, perito-neal carcinoma and fallopian tube carcinoma. In: DeVita VT Jr, Hellman S, Rosenberg SA, editors. Cancer: principles and practice of oncology. 7th ed. Philadelphia: Lippincott Wil-liams and Wilkins, 2005: 1364-1397
5 Hoskins WJ, McGuire WP, Brady MF, Homesley HD, Creas-man WT, Berman M, Ball H, Berek JS. The effect of diameter of largest residual disease on survival after primary cytore-ductive surgery in patients with suboptimal residual epithe-
lial ovarian carcinoma. Am J Obstet Gynecol 1994; 170: 974-979; discussion 979-980 [PMID: 8166218]
6 Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influ-ence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: a Gynecologic Oncology Group study. Gynecol Oncol 1992; 47: 159-166 [PMID: 1468693 DOI: 10.1016/0090-8258(92)90100-W]
7 Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for ad-vanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol 2002; 20: 1248-1259 [PMID: 11870167]
8 Tangjitgamol S, Manusirivithaya S, Laopaiboon M, Lum-biganon P. Interval debulking surgery for advanced epithe-lial ovarian cancer: a Cochrane systematic review. Gynecol Oncol 2009; 112: 257-264 [PMID: 19017548 DOI: 10.1016/j.ygyno.2008.09.041]
9 Ansquer Y, Leblanc E, Clough K, Morice P, Dauplat J, Mathe-vet P, Lhommé C, Scherer C, Tigaud JD, Benchaib M, Fourme E, Castaigne D, Querleu D, Dargent D. Neoadjuvant chemo-therapy for unresectable ovarian carcinoma: a French multi-center study. Cancer 2001; 91: 2329-2334 [PMID: 11413522]
10 van der Burg ME. Advanced ovarian cancer. Curr Treat Op-tions Oncol 2001; 2: 109-118 [PMID: 12057129 DOI: 10.1007/s11864-001-0053-1]
11 Fioretti P, Gadducci A, Del Bravo B, Prato B. The potential of primary cytoreductive surgery in patients with FIGO stages III and IV ovarian carcinoma. Eur J Gynaecol Oncol 1990; 11: 175-179 [PMID: 2209635]
12 Bristow RE, Chi DS. Platinum-based neoadjuvant chemother-apy and interval surgical cytoreduction for advanced ovarian cancer: a meta-analysis. Gynecol Oncol 2006; 103: 1070-1076 [PMID: 16875720 DOI: 10.1016/j.ygyno.2006.06.025]
13 Vergote I, Tropé CG, Amant F, Kristensen GB, Ehlen T, Johnson N, Verheijen RH, van der Burg ME, Lacave AJ, Pan-ici PB, Kenter GG, Casado A, Mendiola C, Coens C, Verleye L, Stuart GC, Pecorelli S, Reed NS. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med 2010; 363: 943-953 [PMID: 20818904 DOI: 10.1056/NEJ-Moa0908806]
14 Spratt JS, Adcock RA, Muskovin M, Sherrill W, McKeown J. Clinical delivery system for intraperitoneal hyperthermic chemotherapy. Cancer Res 1980; 40: 256-260 [PMID: 6766084]
15 Witkamp AJ, de Bree E, Van Goethem R, Zoetmulder FA. Ra-tionale and techniques of intra-operative hyperthermic intra-peritoneal chemotherapy. Cancer Treat Rev 2001; 27: 365-374 [PMID: 11908929 DOI: 10.1053/ctrv.2001.0232]
16 Gill RS, Al-Adra DP, Nagendran J, Campbell S, Shi X, Haase E, Schiller D. Treatment of gastric cancer with peritoneal car-cinomatosis by cytoreductive surgery and HIPEC: a system-atic review of survival, mortality, and morbidity. J Surg Oncol 2011; 104: 692-698 [PMID: 21713780 DOI: 10.1002/jso.22017]
17 Yan TD, Black D, Savady R, Sugarbaker PH. A systematic review on the efficacy of cytoreductive surgery and periop-erative intraperitoneal chemotherapy for pseudomyxoma peritonei. Ann Surg Oncol 2007; 14: 484-492 [PMID: 17054002 DOI: 10.1245/s10434-006-9182-x]
18 Yan TD, Black D, Savady R, Sugarbaker PH. Systematic re-view on the efficacy of cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for peritoneal carcinomatosis from colorectal carcinoma. J Clin Oncol 2006; 24: 4011-4019 [PMID: 16921055]
19 Yan TD, Welch L, Black D, Sugarbaker PH. A systematic review on the efficacy of cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for diffuse malignancy peritoneal mesothelioma. Ann Oncol 2007; 18: 827-834 [PMID: 17130182 DOI: 10.1093/annonc/mdl428]
20 Elit L, Oliver TK, Covens A, Kwon J, Fung MF, Hirte HW, Oza AM. Intraperitoneal chemotherapy in the first-line treat-ment of women with stage III epithelial ovarian cancer: a sys-tematic review with metaanalyses. Cancer 2007; 109: 692-702
Lotti M et al . Preliminary report of a bi-centric observational study

174 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
[PMID: 17238181 DOI: 10.1002/cncr.22466]21 Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R,
Lele S, Copeland LJ, Walker JL, Burger RA. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006; 354: 34-43 [PMID: 16394300 DOI: 10.1056/NEJMoa052985]
22 Trimble EL, Alvarez RD. Intraperitoneal chemotherapy and the NCI clinical announcement. Gynecol Oncol 2006; 103: S18-S19 [PMID: 17027073 DOI: 10.1016/j.ygyno.2006.08.020]
23 Sugarbaker PH, Chang D. Results of treatment of 385 pa-tients with peritoneal surface spread of appendiceal ma-lignancy. Ann Surg Oncol 1999; 6: 727-731 [PMID: 10622499 DOI: 10.1007/s10434-999-0727-7]
24 Glehen O, Kwiatkowski F, Sugarbaker PH, Elias D, Levine EA, De Simone M, Barone R, Yonemura Y, Cavaliere F, Quenet F, Gutman M, Tentes AA, Lorimier G, Bernard JL, Bereder JM, Porcheron J, Gomez-Portilla A, Shen P, Deraco M, Rat P. Cytoreductive surgery combined with periopera-tive intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol 2004; 22: 3284-3292 [PMID: 15310771]
25 Witkamp AJ, de Bree E, Kaag MM, Boot H, Beijnen JH, van Slooten GW, van Coevorden F, Zoetmulder FA. Extensive cytoreductive surgery followed by intra-operative hyper-thermic intraperitoneal chemotherapy with mitomycin-C in patients with peritoneal carcinomatosis of colorectal origin. Eur J Cancer 2001; 37: 979-984 [PMID: 11334722 DOI: 10.1016/S0959-8049(01)00058-2]
26 Loggie BW, Fleming RA, McQuellon RP, Russell GB, Geis-inger KR. Cytoreductive surgery with intraperitoneal hyper-thermic chemotherapy for disseminated peritoneal cancer of gastrointestinal origin. Am Surg 2000; 66: 561-568 [PMID: 10888132]
27 Piso P, Bektas H, Werner U, Schlitt HJ, Kubicka S, Born-scheuer A, Manns M, Klempnauer J. Improved prognosis following peritonectomy procedures and hyperthermic intra-peritoneal chemotherapy for peritoneal carcinomatosis from appendiceal carcinoma. Eur J Surg Oncol 2001; 27: 286-290 [PMID: 11373107 DOI: 10.1053/ejso.2000.1095]
28 Sugarbaker PH. Carcinomatosis--is cure an option? J Clin Oncol 2003; 21: 762-764 [PMID: 12610170]
29 Fagotti A, Ferrandina G, Fanfani F, Garganese G, Vizzielli G, Carone V, Salerno MG, Scambia G. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in ad-vanced ovarian carcinoma. Am J Obstet Gynecol 2008; 199: 642.e1-642.e6 [PMID: 18801470 DOI: 10.1016/j.ajog.2008.06.052]
30 Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sar-gent D, Ford R, Dancey J, Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L, Kaplan R, Lacombe D, Verweij J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: 228-247 [PMID: 19097774 DOI: 10.1016/j.ejca.2008.10.026]
31 Jaquet P, Sugarbaker PH. Current methodologies for clinical assessment of patients with peritoneal carcinomatosis. J Exp Clin Cancer Res 1996; 15: 49-58
32 Deraco M, Kusamura S, Virzì S, Puccio F, Macrì A, Famulari C, Solazzo M, Bonomi S, Iusco DR, Baratti D. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy as upfront therapy for advanced epithelial ovarian cancer: multi-institutional phase-II trial. Gynecol Oncol 2011; 122: 215-220 [PMID: 21665254 DOI: 10.1016/j.ygyno.2011.05.004]
33 Gerestein CG, Nieuwenhuyzen-de Boer GM, Eijkemans MJ, Kooi GS, Burger CW. Prediction of 30-day morbidity after primary cytoreductive surgery for advanced stage ovarian cancer. Eur J Cancer 2010; 46: 102-109 [PMID: 19900801 DOI: 10.1016/j.ejca.2009.10.017]
34 Gerestein CG, Damhuis RA, Burger CW, Kooi GS. Postop-erative mortality after primary cytoreductive surgery for advanced stage epithelial ovarian cancer: a systematic re-view. Gynecol Oncol 2009; 114: 523-527 [PMID: 19344936 DOI:
10.1016/j.ygyno.2009.03.011]35 van der Burg ME, van Lent M, Buyse M, Kobierska A, Co-
lombo N, Favalli G, Lacave AJ, Nardi M, Renard J, Pecorelli S. The effect of debulking surgery after induction chemother-apy on the prognosis in advanced epithelial ovarian cancer. Gynecological Cancer Cooperative Group of the European Organization for Research and Treatment of Cancer. N Engl J Med 1995; 332: 629-634 [PMID: 7845426 DOI: 10.1056/NEJM 199503093321002]
36 Chua TC, Robertson G, Liauw W, Farrell R, Yan TD, Morris DL. Intraoperative hyperthermic intraperitoneal chemother-apy after cytoreductive surgery in ovarian cancer peritoneal carcinomatosis: systematic review of current results. J Cancer Res Clin Oncol 2009; 135: 1637-1645 [PMID: 19701772 DOI: 10.1007/s00432-009-0667-4]
37 Pignata S, Cannella L, Leopardo D, Pisano C, Bruni GS, Facchini G. Chemotherapy in epithelial ovarian cancer. Cancer Lett 2011; 303: 73-83 [PMID: 21353386 DOI: 10.1016/j.canlet.2011.01.026]
38 Parson EN, Lentz S, Russell G, Shen P, Levine EA, Stewart JH. Outcomes after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal surface dissemi-nation from ovarian neoplasms. Am J Surg 2011; 202: 481-486 [PMID: 21474115 DOI: 10.1016/j.amjsurg.2011.02.004]
39 Pavlov MJ, Kovacevic PA, Ceranic MS, Stamenkovic AB, Ivanovic AM, Kecmanovic DM. Cytoreductive surgery and modified heated intraoperative intraperitoneal chemotherapy (HIPEC) for advanced and recurrent ovarian cancer -- 12-year single center experience. Eur J Surg Oncol 2009; 35: 1186-1191 [PMID: 19356887 DOI: 10.1016/j.ejso.2009.03.004]
40 Guardiola E, Delroeux D, Heyd B, Combe M, Lorgis V, Demar-chi M, Stein U, Royer B, Chauffert B, Pivot X. Intra-operative intra-peritoneal chemotherapy with cisplatin in patients with peritoneal carcinomatosis of ovarian cancer. World J Surg Oncol 2009; 7: 14 [PMID: 19203351 DOI: 10.1186/1477-7819-7-14]
41 Di Giorgio A, Naticchioni E, Biacchi D, Sibio S, Accarpio F, Rocco M, Tarquini S, Di Seri M, Ciardi A, Montruccoli D, Sammartino P. Cytoreductive surgery (peritonectomy proce-dures) combined with hyperthermic intraperitoneal chemo-therapy (HIPEC) in the treatment of diffuse peritoneal car-cinomatosis from ovarian cancer. Cancer 2008; 113: 315-325 [PMID: 18473354 DOI: 10.1002/cncr.23553]
42 Rufián S, Muñoz-Casares FC, Briceño J, Díaz CJ, Rubio MJ, Ortega R, Ciria R, Morillo M, Aranda E, Muntané J, Pera C. Radical surgery-peritonectomy and intraoperative intraperi-toneal chemotherapy for the treatment of peritoneal carcino-matosis in recurrent or primary ovarian cancer. J Surg Oncol 2006; 94: 316-324 [PMID: 16917864 DOI: 10.1002/jso.20597]
43 Reichman TW, Cracchiolo B, Sama J, Bryan M, Harrison J, Pliner L, Harrison LE. Cytoreductive surgery and intraopera-tive hyperthermic chemoperfusion for advanced ovarian car-cinoma. J Surg Oncol 2005; 90: 51-56; discussion 56-58 [PMID: 15844187 DOI: 10.1002/jso.20243]
44 Look M, Chang D, Sugarbaker PH. Long-term results of cytoreductive surgery for advanced and recurrent epithelial ovarian cancers and papillary serous carcinoma of the peri-toneum. Int J Gynecol Cancer 2004; 14: 35-41 [PMID: 14764027 DOI: 10.1111/j.1048-891x.2004.14008.x]
45 Piso P, Dahlke MH, Loss M, Schlitt HJ. Cytoreductive sur-gery and hyperthermic intraperitoneal chemotherapy in peri-toneal carcinomatosis from ovarian cancer. World J Surg On-col 2004; 2: 21 [PMID: 15222884 DOI: 10.1186/1477-7819-2-21]
46 Steller MA, Egorin MJ, Trimble EL, Bartlett DL, Zuhowski EG, Alexander HR, Dedrick RL. A pilot phase I trial of contin-uous hyperthermic peritoneal perfusion with high-dose car-boplatin as primary treatment of patients with small-volume residual ovarian cancer. Cancer Chemother Pharmacol 1999; 43: 106-114 [PMID: 9923815 DOI: 10.1007/s002800050870]
47 Roviello F, Marrelli D, Neri A, Cerretani D, de Manzoni G, Pe-drazzani C, Cioppa T, Nastri G, Giorgi G, Pinto E. Treatment
Lotti M et al . Preliminary report of a bi-centric observational study

175 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
of peritoneal carcinomatosis by cytoreductive surgery and intraperitoneal hyperthermic chemoperfusion (IHCP): post-operative outcome and risk factors for morbidity. World J Surg 2006; 30: 2033-2040; discussion 2041-2042 [PMID: 17006608 DOI: 10.1007/s00268-006-0038-0]
48 Lim MC, Kang S, Choi J, Song YJ, Park S, Seo SS, Park SY. Hyperthermic intraperitoneal chemotherapy after extensive cytoreductive surgery in patients with primary advanced epithelial ovarian cancer: interim analysis of a phase II study. Ann Surg Oncol 2009; 16: 993-1000 [PMID: 19169758 DOI: 10.1245/s10434-008-0299-y]
49 Frenel JS, Leux C, Pouplin L, Ferron G, Berton Rigaud D, Bourbouloux E, Dravet F, Jaffre I, Classe JM. Oxaliplatin-based hyperthermic intraperitoneal chemotherapy in primary or re-current epithelial ovarian cancer: A pilot study of 31 patients. J Surg Oncol 2011; 103: 10-16 [PMID: 21031424 DOI: 10.1002/jso.21732]
50 Muñoz-Casares FC, Rufián S, Arjona-Sánchez Á, Rubio MJ, Díaz R, Casado Á, Naranjo Á, Díaz-Iglesias CJ, Ortega R, Muñoz-Villanueva MC, Muntané J, Aranda E. Neoadjuvant intraperitoneal chemotherapy with paclitaxel for the radical surgical treatment of peritoneal carcinomatosis in ovarian can-cer: a prospective pilot study. Cancer Chemother Pharmacol 2011; 68: 267-274 [PMID: 21499894 DOI: 10.1007/s00280-011-1646-4]
51 Ansaloni L, Agnoletti V, Amadori A, Catena F, Cavaliere D, Coccolini F, De Iaco P, Di Battista M, Framarini M, Gazzotti F, Ghermandi C, Kopf B, Saponara M, Tauceri F, Vallicelli C, Verdecchia GM, Pinna AD. Evaluation of extensive cyto-reductive surgery and hyperthermic intraperitoneal chemo-therapy (HIPEC) in patients with advanced epithelial ovarian cancer. Int J Gynecol Cancer 2012; 22: 778-785 [PMID: 22572845 DOI: 10.1097/IGC.0b013e31824d836c]
52 Kang S, Nam BH. Does neoadjuvant chemotherapy increase optimal cytoreduction rate in advanced ovarian cancer? Me-ta-analysis of 21 studies. Ann Surg Oncol 2009; 16: 2315-2320 [PMID: 19517192 DOI: 10.1245/s10434-009-0558-6]
53 Markman M. Hyperthermic intraperitoneal chemotherapy in the management of ovarian cancer: A critical need for an ev-idence-based evaluation. Gynecol Oncol 2009; 113: 4-5 [PMID: 19176238 DOI: 10.1016/j.ygyno.2008.12.022]
54 Chua TC, Liauw W, Robertson G, Chia WK, Soo KC, Alobaid A, Al-Mohaimeed K, Morris DL. Towards randomized trials of cytoreductive surgery using peritonectomy and hyperther-mic intraperitoneal chemotherapy for ovarian cancer perito-neal carcinomatosis. Gynecol Oncol 2009; 114: 137-139; author reply 139 [PMID: 19368962 DOI: 10.1016/j.ygyno.2009.03.002]
55 Edwards RP. Is hyperthermic intraoperative peritoneal che-motherapy and systemic chemotherapy as effective as stan-dard intraperitoneal chemotherapy: time for a prospective trial? Gynecol Oncol 2011; 122: 207-208 [PMID: 21763889 DOI: 10.1016/j.ygyno.2011.06.029]
56 Verwaal VJ, Bruin S, Boot H, van Slooten G, van Tinteren H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol 2008; 15: 2426-2432 [PMID: 18521686 DOI: 10.1245/s10434-008-9966-2]
57 Yang XJ, Huang CQ, Suo T, Mei LJ, Yang GL, Cheng FL, Zhou
YF, Xiong B, Yonemura Y, Li Y. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: final results of a phase III randomized clinical trial. Ann Surg Oncol 2011; 18: 1575-1581 [PMID: 21431408 DOI: 10.1245/s10434-011-1631-5]
58 Intraoperative Hyperthermic Intraperitoneal Chemo-therapy With Ovarian Cancer. ClinicalTrials.gov Identifier: NCT01091636. Available from: URL: http://clinicaltrials.gov/ct2/show/NCT01091636
59 Chua TC, Liauw W, Robertson G, Morris DL. Establishing evidence for change in ovarian cancer surgery--proposing clinical trials of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy (HIPEC) in ovarian cancer peritoneal carcinomatosis. Gynecol Oncol 2009; 115: 166-168; author reply 168-169 [PMID: 19604568 DOI: 10.1016/j.ygyno.2009.06.010]
60 Classe JM, Muller M, Frenel JS, Berton Rigaud D, Ferron G, Jaffré I, Gladieff L. [Intraperitoneal chemotherapy in the treatment of advanced ovarian cancer]. J Gynecol Obstet Biol Reprod (Paris) 2010; 39: 183-190 [PMID: 20116179 DOI: 10.1016/j.jgyn.2009.12.007]
61 Secondary Debulking Surgery +/- Hyperthermic Intraperi-toneal Chemotherapy in Stage III Ovarian Cancer; Clinical-Trials.gov Identifier: NCT00426257. Available from: URL: http://clinicaltrials.gov/ct2/show/NCT00426257
62 de Bree E, Rosing H, Michalakis J, Romanos J, Relakis K, Theodoropoulos PA, Beijnen JH, Georgoulias V, Tsiftsis DD. Intraperitoneal chemotherapy with taxanes for ovarian can-cer with peritoneal dissemination. Eur J Surg Oncol 2006; 32: 666-670 [PMID: 16618534 DOI: 10.1016/j.ejso.2006.03.008]
63 de Bree E, Theodoropoulos PA, Rosing H, Michalakis J, Romanos J, Beijnen JH, Tsiftsis DD. Treatment of ovarian cancer using intraperitoneal chemotherapy with taxanes: from laboratory bench to bedside. Cancer Treat Rev 2006; 32: 471-482 [PMID: 16942841 DOI: 10.1016/j.ctrv.2006.07.006]
64 Michalakis J, Georgatos SD, de Bree E, Polioudaki H, Ro-manos J, Georgoulias V, Tsiftsis DD, Theodoropoulos PA. Short-term exposure of cancer cells to micromolar doses of paclitaxel, with or without hyperthermia, induces long-term inhibition of cell proliferation and cell death in vitro. Ann Surg Oncol 2007; 14: 1220-1228 [PMID: 17206477 DOI: 10.1245/s10434-006-9305-4]
65 de Bree E, Rosing H, Filis D, Romanos J, Melisssourgaki M, Daskalakis M, Pilatou M, Sanidas E, Taflampas P, Kalbakis K, Beijnen JH, Tsiftsis DD. Cytoreductive surgery and intraopera-tive hyperthermic intraperitoneal chemotherapy with pacli-taxel: a clinical and pharmacokinetic study. Ann Surg Oncol 2008; 15: 1183-1192 [PMID: 18239973 DOI: 10.1245/s10434-007-9792-y]
66 Bae JH, Lee JM, Ryu KS, Lee YS, Park YG, Hur SY, Ahn WS, Namkoong SE. Treatment of ovarian cancer with paclitaxel- or carboplatin-based intraperitoneal hyperthermic chemo-therapy during secondary surgery. Gynecol Oncol 2007; 106: 193-200 [PMID: 17466362 DOI: 10.1016/j.ygyno.2007.03.019]
67 Kim JH, Lee JM, Ryu KS, Lee YS, Park YG, Hur SY, Lee KH, Lee SH, Kim SJ. Consolidation hyperthermic intraperitoneal chemotherapy using paclitaxel in patients with epithelial ovar-ian cancer. J Surg Oncol 2010; 101: 149-155 [PMID: 20035540]
P- Reviewer: Song SY S- Editor: Wen LL L- Editor: A E- Editor: Zheng XM
Lotti M et al . Preliminary report of a bi-centric observational study

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.176
World J Obstet Gynecol 2013 November 10; 2(4): 176-180ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Surgical repair of pelvic organ prolapse and follow-up: An institutional multi-center experience
Sarah Gustapane, Martina Leombroni, Eleonora Falò, Alessandro Santarelli, Franco Frondaroli, Marco Liberati, Emanuele Perrone, Andrea Tinelli
Sarah Gustapane, Martina Leombroni, Eleonora Falò, Ales-sandro Santarelli, Franco Frondaroli, Marco Liberati, De-partment of Obstetrics and Gynaecology, Santissima Annunziata Hospital, 66100 Chieti, ItalyEmanuele Perrone, Department of Obstetrics and Gynaecology, University of Perugia, 6100 Perugia, ItalyAndrea Tinelli, Department of Obstetrics and Gynaecology, Vito Fazzi Hospital, 73100 Lecce, ItalyAuthor contributions: Gustapane S contributed to this study as a surgeon, study planner, data analyzer and writer of the paper; Leombroni M contributed to this study as a study planner, data collector and analyzer, and writer of the paper; Falò E contributed to this study as a surgeon and writer of the paper; Santarelli A, Frondaroli F and Liberati M contributed to this study as surgeons; Perrone E and Tinelli A contributed to this study as final review-ers of the paper.Correspondence to: Sarah Gustapane, MD, Department of Obstetrics and Gynaecology, Santissima Annunziata Hospital, via dei Vestini, 66100 Chieti, Italy. [email protected]: +39-83-2661115 Fax: +39-83-2661115Received: May 9, 2013 Revised: August 22, 2013Accepted: September 14, 2013Published online: November 10, 2013
AbstractAIM: To investigate the effects of the Elevate Anterior and Posterior transvaginal mesh procedure on 30 pa-tients affected by pelvic organ prolapse (POP) at 12 mo follow-up.
METHODS: Between September 2011 and September 2012, a prospective multicenter observational study enrolled 30 consecutive patients with POP-Q ≥ stage Ⅱ. After a preoperative evaluation, patients underwent prolapse repair utilizing the Elevate Anterior and Poste-rior Prolapse Repair System (American Medical Systems, Minnetonka, MN, United States). Operative technique was standardized and performed by the same surgical team under spinal or general anesthesia. Patients were evaluated postoperatively at 1, 3, 6 and 12 mo.
RESULTS: All 30 patients completed the 12 mo follow-up. The mean age was 65.3 years (range 49-81 years) and average hospital stay was 4.5 d. The mean op-erative time was 65 min (range 40-120 min). Related adverse events reported were mesh extrusions (6.7%) and post void residual urine volume (13.3%). There were no visceral injuries, no infection of the mesh, and no symptoms of recurrent prolapse. All quality-of-life scores significantly improved from baseline.
CONCLUSION: One year’s follow-up of our 30 patients confirms the safety and the efficacy of the Elevate An-terior and Posterior transvaginal mesh procedure for POP treatment. Our final results are comforting but lon-ger term follow-up is ongoing.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Pelvic organ prolapse; Pelvic organ prolapse; Mesh; Vaginal mesh erosion
Core tip: Our initial results show that the vaginal repair of anterior/apical and posterior wall prolapse utilizing a wall mesh placed via the Elevate system is an effective, safe and minimally invasive procedure for the treatment pelvic organ prolapse and shows excellent anatomical and functional results. Recent studies of the anatomi-cal and physiological pelvic floor characteristics favored new generation prosthetic surgical techniques with ad-vanced tools and biocompatible mesh in order to allow lower recurrence rates. Our final results are interesting and comforting but longer term follow-up is ongoing.
Gustapane S, Leombroni M, Falò E, Santarelli A, Frondaroli F, Liberati M, Perrone E, Tinelli A. Surgical repair of pelvic organ prolapse and follow-up: An institutional multi-center experience. World J Obstet Gynecol 2013; 2(4): 176-180 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/176.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.176
BRIEF ARTICLE
176 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com

Gustapane S et al . Repair of pelvic organ prolapse by meshes
INTRODUCTIONPelvic organ prolapse (POP), including anterior and/or posterior vaginal prolapse, uterine prolapse and enterocele, is a common group of clinical conditions affecting mil-lions of women worldwide[1,2]. Data from the Women’s Health Initiative revealed anterior POP in 34.3%, posterior wall prolapse in 18.6%, and uterine prolapse in 14.3% of women[3].
There are approximately 250000 procedures annu-ally in the United States for POP, with a prevalence of 11.1%[1]. POP includes a range of disorders, from asymp-tomatic disturbed vaginal anatomy to complete vaginal eversion associated with considerable degrees of urinary, defecatory and sexual dysfunction. The pathophysiology of prolapse is multifactorial, including neuromuscular dysfunction and fascial defects in the integrity of the uterosacral-cardinal complex[4]; however, genetically sus-ceptible women more exposed to life events results in the development of a clinically significant prolapse.
Main risk factors are age, obstetric history[5], obesity[6], chronic lung and intestinal disease, history of hysterecto-my[7], history of previous prolapse operations, and race[8]. Estrogens have a protective role[9,10] and so menopausal women are mainly involved. The support mechanisms reduction predisposes the herniation of the pelvic organs in the vaginal canal[11], causing several symptoms related to the severity of the prolapse. The most reliable symptom is “to see or to feel a budge in the vagina”[12,13]. The evalua-tion of women with a prolapse requires a comprehensive approach, focusing on the function in all pelvic compart-ments based on a detailed patient history, physical exami-nation and investigations.
Detailed presurgical evaluation is required to select the most appropriate treatment from a variety of medical and sur-gical options[14]. Non-surgical therapy of POP is consid-ered in women with a mild to moderate prolapse, those who desire preservation of future childbearing, those in whom surgery may not be an option, or those who do not desire surgical intervention, and includes conservative behavioral management and the use of mechanical devic-es. Surgical therapy of POP includes vaginal, abdominal and laparoscopic approaches, or a combination of these approaches, with the aim to relieve or improve symptoms and restore normal vaginal anatomy.
The aim of our study is to assess the efficacy, safety and tolerability of the Elevate Anterior and Posterior transvaginal mesh procedure on 30 patients affected by POP repair at the 12 mo follow-up.
MATERIALS AND METHODSThis study is a prospective multicenter observational expe-rience of 30 consecutive women with symptomatic stage 2 or greater of prolapse that underwent anterior and/or posterior repair using the Anterior and Posterior Prolapse Repair System (American Medical Systems, Minnetonka, MN, United States).
Comprehensive preoperative urogynecological exams were completed, including an evaluation of anamnestic data, obstetric history, BMI and chronic disease, a pelvic exam with prolapse quantification utilizing the Half Way System or Baden-Walker scales[15,16], and a ultrasound evaluation. Inclusion criteria were patients with symptom-atic anterior or posterior compartment prolapse ≥ stage 2. Our patients received the Anterior and Posterior Elevate surgical procedure, with a consecutive 1 year follow-up at our center.
Operative technique was standardized and the surgery was performed by an expert surgical team under spinal or general anesthesia, according to anesthetist decision and patient’s preference. The procedure began with injection of 40-60 cc of hydrodissection solution (25 cc of 1% lidocaine with epinephrine 1:200000 diluted in 250 cc of saline) into the anterior vaginal wall. A 3 to 4 cm vertical incision is then made in the anterior vaginal wall with a full-thickness hydrodissection. Elevate Anterior and Api-cal utilizes self-fixating tips that allow safe, simple and precise mesh placement in the sacrospinous ligament and the obturator internus muscle. In the Elevate Posterior procedure, the apical mesh arms are anchored to the sa-crospinous ligaments and the distant portion of the graft was trimmed at the discretion of surgeon to fit vaginal length attached to the perineal body and rectovaginal sep-ta bilaterally. A prophylactic antibiotic (ceftriaxone 2 g + metronidazole 500 mg) was administered. Subjects were evaluated postoperatively at 1, 3, 6 and 12 mo.
Statistical analysisThe analyzed data were collected and evaluated by an ex-ternal statistician independent reviewer. Descriptive sta-tistical analysis was performed with continuous variables, summarized using mean ± SD or median, and discrete variables were reported using numbers and percentages.
RESULTSThe mean age of the 30 patients was 65.3 years (range 49- 81 years) and their mean parity was two deliveries (range 0-4). The demographic characteristics are summarized in Table 1. Of the 30 patients, 7 (23.3%) had stage Ⅱ prolapse, 20 (66.6%) stage Ⅲ and 3 (10%) had stage Ⅳ
177 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Anamnestic data and classification of the patients according to pelvic organ prolapse quantification system
Age (yr) 65.3 ± 8.2 (range 49-81)Previous hysterectomy 2 (6.7)Menopausal 28 (93.3)Pre-menopausal 2 (6.7)Parity 2.3 ± 0.9 (range 0-4)Pelvic organ prolapse’s stage Ⅱ 7 (23.3) Ⅲ 20 (66.6) Ⅳ 3 (10)
Data are expressed as absolute n (%) or mean ± SD.

on pre-operative pelvic examination. Two patients (6.7%) had a previous hysterectomy. No patients had a history of previous anterior or posterior vaginal wall repair. Four-teen patients (46.7%) had urinary problems, in particular urinary retention with a preoperative post void residual volume. Twenty-four (80%) patients underwent prolapse repair with Anterior and Apical Prolapse Repair ± Poste-rior Prolapse Repair System.
Concurrent colpohysterectomy was performed in 6 (20%) patients. There were no major intraoperative com-plications and the mean duration of operations was 65 min (range 40-120 min). There were no post-operative bleeds or hematomas and the mean postoperative body tem-perature was 37.1 ± 0.5 ℃.
The average hospital stay was 4.5 ± 1.38 d and the Fol-ey catheter was removed after 72 h. All 30 patients com-pleted the 12 mo follow-up. During follow-up, no patients had symptoms of recurrent prolapse or urinary problems. Four patients (13.3%) had a minimal asymptomatic post void residual urine volume. Two patients (6.7%) had par-tial mesh erosion; these women were treated with local application of 1 g of vaginal Promestriene (Colpotrophine, TEVA, Milan, Italy) twice a day for 1 mo.
After this therapy, patients returned to the surgery room for partial mesh excision, then the edges of the vaginal epithelium were trimmed where appropriate and re-approximated, with good results in their follow up. No mesh had to be removed secondary to allergic reaction or infections.
DISCUSSIONOver the years, numerous surgical techniques were used in the management of POP but few controlled studies were designed to assess the complexity, costs and long-term efficacy of individual procedures[17].
Surgical mesh has been used since the 1950s to repair abdominal hernias. In the 1970s, gynecologists began us-ing surgical mesh products indicated for hernia repair for abdominal repair of POP and in the 1990s, gynecologists began using surgical mesh for surgical treatment of stress urinary incontinence and transvaginal POP repair. Over the next few years, surgical mesh products for transvagi-nal POP repair became incorporated into “kits” that included tools to aid in the delivery and insertion of the mesh. Surgical mesh kits continue to evolve, adding new insertion tools, tissue fixation anchors, surgical techniques and absorbable and biological materials.
Recent studies of the anatomical and physiological pelvic floor characteristics[18]
favored new generation prosthetic surgical techniques. These involve the use of advanced tools and biocompatible mesh and allow better results and lower recurrence rates. As the implementation of synthetic materials in POP surgery has increased, so has the reporting of complications.
From 2008 to 2010, the most frequent complications re-ported to the Food and Drug Administration (FDA) from the use of surgical mesh devices for POP repair included
vaginal mesh erosion (also called exposure, extrusion or protrusion), pain (dyspareunia), infection, urinary problems, bleeding and organ perforation. There were also reports of recurrent prolapse, neuro-muscular problems, vaginal scarring and shrinkage, and emotional problems. Based on evaluation of adverse event reports and assessment of the scientific literature, the FDA has not seen conclusive evidence that using transvaginally placed mesh in POP re-pair improves clinical outcomes any more than traditional POP repair that does not use mesh, and it may expose pa-tients to a greater risk, as mesh erosion or extrusion.
For instance, when minor mesh erosion or extrusion occurs, observant management alone or the use of topi-cal estrogens cream particularly in asymptomatic women are viable options. More commonly, the excision of ex-posed mesh with re-approximation of the vaginal defect is performed. However, in severe cases such as infection, complete or total excision of the mesh is required[19].
While the literature suggests an anatomical benefit to anterior repair with mesh augmentation, this anatomical benefit may not result in superior clinical outcomes and the associated risk of adverse events should be consid-ered. Based on these findings, the FDA is considering regulatory changes that may improve our understanding of the safety and effectiveness of these devices and has specific recommendations for patients and healthcare pro-viders[20].
Our surgical treatment utilizing the Elevate Anterior and Posterior Prolapse Repair System showed excellent anatomical and functional results and an objective cure rate of 100% within 12 mo. Subjectively, no patients complained of symptomatic prolapse (100% subjective cure rate) and no patients had urinary symptoms during follow-up.
Olsen et al[1] described as many as 29% of women treated with traditional surgical techniques having to un-dergo repeat surgery. Traditional anterior and posterior compartment repair utilizing the patient’s own tissue is a compensatory procedure that utilizes weakened and/or damaged tissue and has reported failure rates in the range of 40%-60%[21]. Additionally, techniques like plication or colporrhaphy do not provide any apical support, which may also contribute to the failure rates seen with this type of repair[22].
Compared to other techniques utilizing synthetic mesh, Moore et al[22] believe the Anterior Elevate proce-dure to be less invasive and a more simplified technique for placing a wall graft.
Our mesh erosion rate (6.7%) was similar with the literature data; Stanford et al[23] reported a 5.6% of erosion rate in a 12 mo multicenter study on 142 patients at ICS 2011.
In our practice, the demand for uterine preservation during surgical management of uterovaginal prolapse is increasing. However, the current data of medical litera-ture on this clinical problem are inadequate to assist a surgeon in determining which patients are ideal for uter-ine preservation[24].
178 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Gustapane S et al . Repair of pelvic organ prolapse by meshes

At present, the decision is usually influenced by the patient’s preferences, the surgeon’s experiences[24] and the presence of uterine or cervical pathology. The current study is limited by its medium term follow-up.
In conclusion, although limited by its short follow-up period, our initial results show that the vaginal repair of anterior/apical and posterior wall prolapse utilizing a wall mesh placed via the Elevate system is an effective, safe and minimally invasive procedure for the treatment POP. It allows restoration of the vaginal length without com-promising its caliber.
We find our research needs more study for determin-ing the ideal utilized material and the optimal way to place and attach the graft vaginally. However, it can be ex-pected that improvements in technology and techniques will continue. We recommend further prospective studies with longer term follow-up to delineate more deeply the Elevate Anterior and Posterior Prolapse Repair System role in clinical practice.
COMMENTSBackgroundPelvic organ prolapse (POP), including anterior and/or posterior vaginal pro-lapse, uterine prolapse and enterocele, is a common group of clinical conditions affecting millions of women worldwide. Over the years, numerous surgical tech-niques were used in the management of POP. Research frontiersFurther prospective studies are needed to delineate more deeply the Elevate Anterior and Posterior Prolapse Repair System role in clinical practice, with longer term follow-up.Innovations and breakthroughsThe authors’ surgical treatment utilizing the Elevate Anterior and Posterior Prolapse Repair System showed excellent anatomical and functional results and an objective cure rate of 100% within 12 mo. Subjectively, no patients com-plained of symptomatic prolapse (100% subjective cure rate) and no patients had urinary symptoms during follow-up.ApplicationsThe initial results show that the vaginal repair of anterior/apical and posterior wall prolapse utilizing a wall mesh placed via the Elevate system is an effec-tive, safe and minimally invasive procedure for the treatment POP and showed excellent anatomical and functional results. Recent studies of the anatomical and physiological pelvic floor characteristics favored new generation prosthetic surgical techniques with advanced tools and biocompatible mesh in order to al-low better results and lower recurrence rates.TerminologyPOP, including anterior and/or posterior vaginal prolapse, uterine prolapse and enterocele, is a common group of clinical conditions affecting millions of women worldwide, with a prevalence of 11.1%. POP includes a range of disorders, from asymptomatic disturbed vaginal anatomy to complete vaginal eversion associ-ated with considerable degrees of urinary, defecatory and sexual dysfunction. The pathophysiology of prolapse is multifactorial and the main risk factors are age, obstetrics history, obesity, chronic lung and intestinal disease, history of hysterectomy, history of previous prolapse operations, and race. Estrogens have a protective role and so menopausal women are mainly involved.Peer reviewThe authors present a prospective multicenter observational study of 30 con-secutive female patients with symptomatic stage 2 or greater of prolapse that underwent anterior and/or posterior repair using a new minimally invasive tech-nique with a single vaginal incision. Overall, the results of the study are interest-ing and clinically relevant. The study design appears clear and straightforward, the statistics are basic, the results are interesting and clinically relevant, and the background review of the literature sufficient and supportive of the specific aims and results.
REFERENCES1 Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL.
Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol 1997; 89: 501-506 [PMID: 9083302]
2 Beer M, Kuhn A. Surgical techniques for vault prolapse: a review of the literature. Eur J Obstet Gynecol Reprod Biol 2005; 119: 144-155 [PMID: 15808370]
3 Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the Women’s Health Initiative: gravity and gravidity. Am J Obstet Gynecol 2002; 186: 1160-1166 [PMID: 12066091]
4 Richardson AC, Lyon JB, Williams NL. A new look at pelvic relaxation. Am J Obstet Gynecol 1976; 126: 568-573 [PMID: 984127 DOI: 10.1007/1-84628-238-1_8]
5 MacArthur C, Lewis M, Knox EG. Health after childbirth. Br J Obstet Gynaecol 1991; 98: 1193-1195 [PMID: 1838008]
6 Uustal Fornell E, Wingren G, Kjølhede P. Factors associated with pelvic floor dysfunction with emphasis on urinary and fecal incontinence and genital prolapse: an epidemiological study. Acta Obstet Gynecol Scand 2004; 83: 383-389 [PMID: 15005787 DOI: 10.1111/j.0001-6349.2004.00367.x]
7 Gürel H, Gürel SA. Pelvic relaxation and associated risk factors: the results of logistic regression analysis. Acta Ob-stet Gynecol Scand 1999; 78: 290-293 [PMID: 10203294 DOI: 10.1034/j.1600-0412.1999.780403.x]
8 Moalli PA, Jones Ivy S, Meyn LA, Zyczynski HM. Risk factors associated with pelvic floor disorders in women un-dergoing surgical repair. Obstet Gynecol 2003; 101: 869-874 [PMID: 12738142]
9 Blakeman PJ, Hilton P, Bulmer IN. Oestrogen status and cell cycle activity in the female lower urinary tract. Neurourol Urodyn 1996; 15: 325-326
10 Sartori MG, Feldner PC, Jarmy-Di Bella ZI, Aquino Castro R, Baracat EC, Rodrigues de Lima G, Castello Girão MJ. Sexual steroids in urogynecology. Climacteric 2011; 14: 5-14 [PMID: 20839956 DOI: 10.3109/13697137.2010.508542]
11 Tinelli A, Malvasi A, Rahimi S, Negro R, Vergara D, Martig-nago R, Pellegrino M, Cavallotti C. Age-related pelvic floor modifications and prolapse risk factors in postmenopausal women. Menopause 2010; 17: 204-212 [PMID: 19629013]
12 Ellerkmann RM, Cundiff GW, Melick CF, Nihira MA, Lef-fler K, Bent AE. Correlation of symptoms with location and severity of pelvic organ prolapse. Am J Obstet Gynecol 2001; 185: 1332-1337; discussion 1337-1338 [PMID: 11744905]
13 Barber MD, Neubauer NL, Klein-Olarte V. Can we screen for pelvic organ prolapse without a physical examination in epidemiologic studies? Am J Obstet Gynecol 2006; 195: 942-948 [PMID: 16681989]
14 Busacchi P, Gerace T, Presepi S, Suprani A, de Aloysio D. Disfunzioni del pavimento pelvico: l’importanza della dia-gnosi preoperatoria. Dati preliminari. Riv It Ost Gin 2005; 7: 340-346
15 Baden WF, Walker TA. Genesis of the vaginal profile: a cor-related classification of vaginal relaxation. Clin Obstet Gyne-col 1972; 15: 1048-1054 [PMID: 4649139]
16 Baden WF, Walker TA. Statistical evaluation of vaginal relaxation. Clin Obstet Gynecol 1972; 15: 1070-1072 [PMID: 4649141]
17 Puggioni GF, Deriu P, Corona R, Pittorra G, Succu AO. Trat-tamento dell’incontinenza urinaria da sforzo mediante sling sottouretrale: due procedure tension-free a confronto. Int Urogynecol J 2007; 21: 7-9
18 Ashton-Miller JA, DeLancey JO. Functional anatomy of the female pelvic floor. Ann N Y Acad Sci 2007; 1101: 266-296 [PMID: 17416924]
19 Kho RM. Editorial comment on the use of martius flap for repair of mesh erosion. J Minim Invasive Gynecol 2013; 20:
179 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
COMMENTS
Gustapane S et al . Repair of pelvic organ prolapse by meshes

135-136 [PMID: 23465254]20 Tijdink MM, Vierhout ME, Heesakkers JP, Withagen MI.
Surgical management of mesh-related complications after prior pelvic floor reconstructive surgery with mesh. Int Uro-gynecol J 2011; 22: 1395-1404 [PMID: 21681595 DOI: 10.1007/s00192-011-1476-2]
21 Maher C, Baessler K. Surgical management of anterior vagi-nal wall prolapse: an evidencebased literature review. Int Urogynecol J Pelvic Floor Dysfunct 2006; 17: 195-201 [PMID: 15915320]
22 Moore RD, Mitchell GK, Miklos JR. Single-incision vaginal approach to treat cystocele and vault prolapse with an an-
terior wall mesh anchored apically to the sacrospinous liga-ments. Int Urogynecol J 2012; 23: 85-91 [PMID: 21866442 DOI: 10.1007/s00192-011-1536-7]
23 Stanford EJ, Cassidenti A, Moen MD. Traditional native tis-sue versus mesh-augmented pelvic organ prolapse repairs: providing an accurate interpretation of current literature. Int Urogynecol J 2012; 23: 19-28 [PMID: 22068321 DOI: 10.1007/s00192-011-1584-z]
24 Price N, Slack A, Jackson SR. Laparoscopic hysteropexy: the initial results of a uterine suspension procedure for utero-vaginal prolapse. BJOG 2010; 117: 62-68 [PMID: 20002370 DOI: 10.1111/j.1471-0528.2009.02396.x]
P- Reviewers: Al-Mandeel HM, Sacco E, Santoro GA S- Editor: Zhai HH L- Editor: Roemmele A E- Editor: Zheng XM
180 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Gustapane S et al . Repair of pelvic organ prolapse by meshes

Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.181
World J Obstet Gynecol 2013 November 10; 2(4): 181-184ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G
Characteristics of semen parameters of Malawian men from couples seeking assisted reproduction
Fanuel Lampiao, Anna Kutengule
Fanuel Lampiao, Anna Kutengule, Division of Physiology, Department of Basic Medical Sciences, College of Medicine, Blantyre 3, MalawiAuthor contributions: Lampiao F and Kutengule A contributed to this manuscript.Correspondence to: Fanuel Lampiao, Associate Professor, Division of Physiology, Department of Basic Medical Sciences, College of Medicine, PO Box 360, Blantyre 3, Malawi. [email protected]: +265-1-878058 Fax: +265-111-872644Received: June 16, 2013 Revised: July 21, 2013Accepted: August 12, 2013Published online: November 10, 2013
AbstractAIM: To profile semen parameters of Malawian men seeking fertility testing.
METHODS: Semen analysis is a key element in the fertility evaluation of men and permits male reproduc-tive potential to be evaluated. Semen samples were collected from consenting men after 3-5 d of sexual abstinence. The samples were collected from 130 males; 78 were male partners of infertile couples while 52 were healthy semen donors. Seminal volume, motil-ity and morphology were assessed. The results were analyzed on Prism 5. All data are expressed as mean ± SD. Student’s t -test was used for statistical analysis. Differences were regarded as statistically significant if P < 0.05.
RESULTS: Semen volume, sperm concentration, pro-gressive motility and normal morphology were signifi-cantly higher in the control group when compared to the participant group. On the other hand, no statistically sig-nificant difference was found between the control group total sperm motility when compared to the participant group. Oligozoospermia was found in 25 cases, terato-zoospermia detected in 17 cases and abnormal seminal plasma in 16 cases. Asthenozoospermia and azoosper-
mia were found in 12 and 8 participants, respectively. This study has shown that most of the infertile patients seeking fertility testing had oligozoospermia. Terato-zoospermia was the second most common abnormality found in the patients seeking fertility testing.
CONCLUSION: Our study is in agreement with previ-ous studies which reported that these parameters have been shown to be good predictors for fertilization.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Infertility; Human spermatozoa; Assisted reproduction; Semen analysis
Core tip: In recent years there has been an increase in infertility and some of the causes are due to male fac-tors. Even although some causes of male infertility can be established, others are idiopathic. It has therefore become imperative to investigate infertility patterns in different countries. This paper reports the common causes of male infertility in Malawian men seeking fer-tility testing.
Lampiao F, Kutengule A. Characteristics of semen parameters of Malawian men from couples seeking assisted reproduction. World J Obstet Gynecol 2013; 2(4): 181-184 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/181.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.181
INTRODUCTIONInfertility is defined as the inability to conceive after at least 1 year of unprotected intercourse. It affects about 8%-12% of all married couples[1]. In about one third of these couples, a male factor is the primary cause and in another one quarter, both the male and female partner
BRIEF ARTICLE
181 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
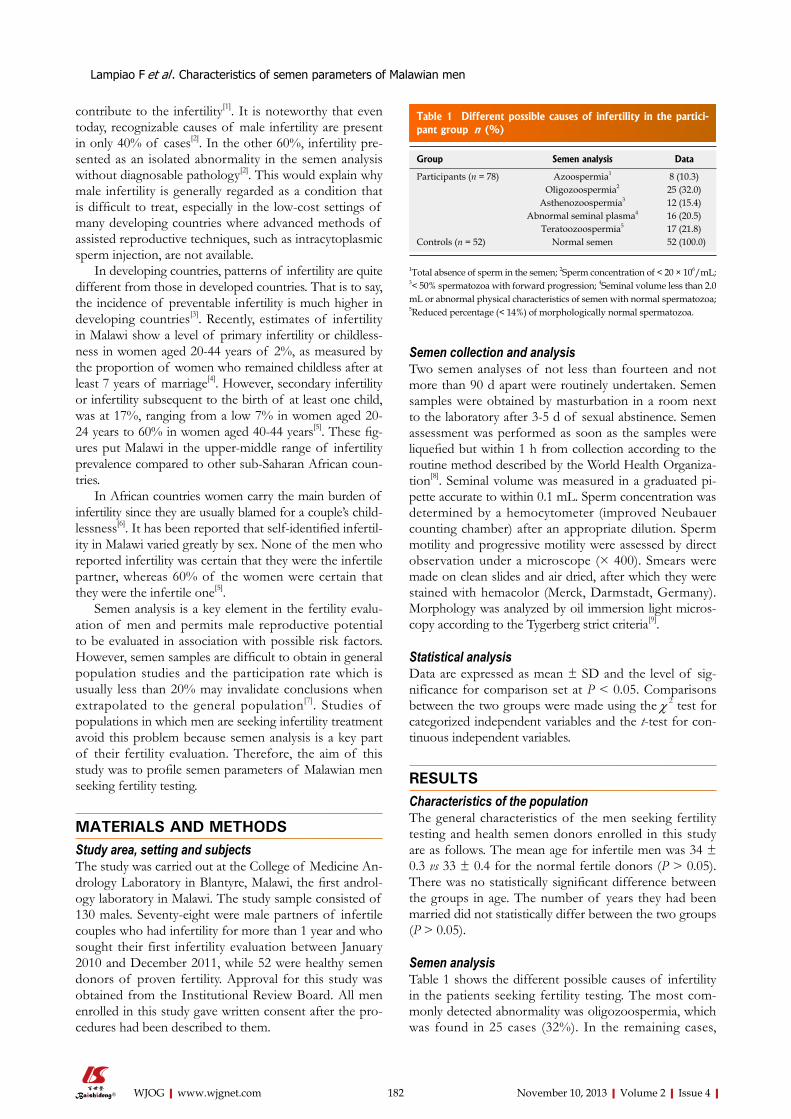
Lampiao F et al . Characteristics of semen parameters of Malawian men
contribute to the infertility[1]. It is noteworthy that even today, recognizable causes of male infertility are present in only 40% of cases[2]. In the other 60%, infertility pre-sented as an isolated abnormality in the semen analysis without diagnosable pathology[2]. This would explain why male infertility is generally regarded as a condition that is difficult to treat, especially in the low-cost settings of many developing countries where advanced methods of assisted reproductive techniques, such as intracytoplasmic sperm injection, are not available.
In developing countries, patterns of infertility are quite different from those in developed countries. That is to say, the incidence of preventable infertility is much higher in developing countries[3]. Recently, estimates of infertility in Malawi show a level of primary infertility or childless-ness in women aged 20-44 years of 2%, as measured by the proportion of women who remained childless after at least 7 years of marriage[4]. However, secondary infertility or infertility subsequent to the birth of at least one child, was at 17%, ranging from a low 7% in women aged 20- 24 years to 60% in women aged 40-44 years[5]. These fig-ures put Malawi in the upper-middle range of infertility prevalence compared to other sub-Saharan African coun-tries.
In African countries women carry the main burden of infertility since they are usually blamed for a couple’s child-lessness[6]. It has been reported that self-identified infertil-ity in Malawi varied greatly by sex. None of the men who reported infertility was certain that they were the infertile partner, whereas 60% of the women were certain that they were the infertile one[5].
Semen analysis is a key element in the fertility evalu-ation of men and permits male reproductive potential to be evaluated in association with possible risk factors. However, semen samples are difficult to obtain in general population studies and the participation rate which is usually less than 20% may invalidate conclusions when extrapolated to the general population[7]. Studies of populations in which men are seeking infertility treatment avoid this problem because semen analysis is a key part of their fertility evaluation. Therefore, the aim of this study was to profile semen parameters of Malawian men seeking fertility testing.
MATERIALS AND METHODSStudy area, setting and subjectsThe study was carried out at the College of Medicine An-drology Laboratory in Blantyre, Malawi, the first androl-ogy laboratory in Malawi. The study sample consisted of 130 males. Seventy-eight were male partners of infertile couples who had infertility for more than 1 year and who sought their first infertility evaluation between January 2010 and December 2011, while 52 were healthy semen donors of proven fertility. Approval for this study was obtained from the Institutional Review Board. All men enrolled in this study gave written consent after the pro-cedures had been described to them.
Semen collection and analysisTwo semen analyses of not less than fourteen and not more than 90 d apart were routinely undertaken. Semen samples were obtained by masturbation in a room next to the laboratory after 3-5 d of sexual abstinence. Semen assessment was performed as soon as the samples were liquefied but within 1 h from collection according to the routine method described by the World Health Organiza-tion[8]. Seminal volume was measured in a graduated pi-pette accurate to within 0.1 mL. Sperm concentration was determined by a hemocytometer (improved Neubauer counting chamber) after an appropriate dilution. Sperm motility and progressive motility were assessed by direct observation under a microscope (× 400). Smears were made on clean slides and air dried, after which they were stained with hemacolor (Merck, Darmstadt, Germany). Morphology was analyzed by oil immersion light micros-copy according to the Tygerberg strict criteria[9].
Statistical analysisData are expressed as mean ± SD and the level of sig-nificance for comparison set at P < 0.05. Comparisons between the two groups were made using the χ 2 test for categorized independent variables and the t-test for con-tinuous independent variables.
RESULTSCharacteristics of the populationThe general characteristics of the men seeking fertility testing and health semen donors enrolled in this study are as follows. The mean age for infertile men was 34 ± 0.3 vs 33 ± 0.4 for the normal fertile donors (P > 0.05). There was no statistically significant difference between the groups in age. The number of years they had been married did not statistically differ between the two groups (P > 0.05).
Semen analysisTable 1 shows the different possible causes of infertility in the patients seeking fertility testing. The most com-monly detected abnormality was oligozoospermia, which was found in 25 cases (32%). In the remaining cases,
182 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Different possible causes of infertility in the partici-pant group n (%)
Group Semen analysis Data
Participants (n = 78) Azoospermia1 8 (10.3)Oligozoospermia2 25 (32.0)
Asthenozoospermia3 12 (15.4)Abnormal seminal plasma4 16 (20.5)
Teratoozoospermia5 17 (21.8)Controls (n = 52) Normal semen 52 (100.0)
1Total absence of sperm in the semen; 2Sperm concentration of < 20 × 106/mL; 3< 50% spermatozoa with forward progression; 4Seminal volume less than 2.0 mL or abnormal physical characteristics of semen with normal spermatozoa; 5Reduced percentage (< 14%) of morphologically normal spermatozoa.

teratozoospermia was detected in 17 (21.8%) cases and abnormal seminal plasma in 16 (20.5%) cases. Astheno-zoospermia and azoospermia were found in 12 (15.4%) and 8 (10.3%) patients, respectively.
Table 2 shows the different semen parameters of the participants seeking fertility testing compared to the con-trols. Semen volume, sperm concentration, progressive motility and normal morphology were significantly higher in the control group when compared to the participant group (P < 0.05). On the other hand, no statistically sig-nificant difference was found between the control group total sperm motility when compared to the participant group (P > 0.05).
DISCUSSIONThis study has shown that most of the infertile partici-pants seeking fertility testing had oligozoospermia (sperm concentration of < 20 × 106/mL). In recent years there have been reports of declining sperm concentration in men around the world[10,11]. With assisted reproduction, participants with severe oligozoospermia can still do well in terms of fertilization and pregnancy outcome if enough sperm can be obtained with separation techniques. Kruger et al[12] reported that no impact could be found on preg-nancy outcome after assisted reproduction using the con-centration/mL in the initial sample as a yard stick.
Teratozoospermia [reduced percentage (< 14%) of morphologically normal spermatozoa] was the second common abnormality found in the participants seeking fertility testing. In this study, the Tygerberg strict criteria were used to assess sperm morphology. Using this crite-rion it has been reported that participants with fewer than 14% normal morphological forms are found to have a de-creased fertilization rate[13]. Morphological characteristics of spermatozoa have been reported to be the best predic-tor for fertilization[13,14].
The findings of our study indicate that oligozoosper-mia was the most prevalent abnormality in the semen of the infertile participants, followed by teratozoosper-mia (reduced percentage of morphologically normal spermatozoa). Our study is in agreement with previous studies which reported that these parameters have been shown to be good predictors for fertilization[13-15]. Apart from known factors that contribute to male infertility, idiopathic factors also contribute to infertility. A study in Poland trying to investigate the pattern of infertility re-ported that 16% of male infertility was due to idiopathic causes[16]. Thus, we speculate that the infertility of the
participants who took part in this study was mainly due to oligozoospermia and teratozoospermia. This study involved only 78 participants seeking fertility testing. A larger sample size would probably produce more conclu-sive results. We recommend that studies should be carried out to establish infertility patterns in different countries. These studies should involve large sample sizes in order to come up with conclusive results that can be extrapo-lated to the general population.
COMMENTSBackgroundIn recent years there has been an increase in infertility and some of the causes are due to male factors. Even although some causes of male infertility can be established, others are idiopathic. It has therefore become imperative to investi-gate infertility patterns in different countries. Research frontiersSemen analysis is a key element in the fertility evaluation of men and permits male reproductive potential to be evaluated in association with possible risk factors. However, semen samples are difficult to obtain in general population studies and the participation rate which is usually less than 20% may invalidate conclusions when extrapolated to the general population. Innovations and breakthroughsThis study has shown that most of the infertile patients seeking fertility testing had oligozoospermia. Teratozoospermia was the second most common abnor-mality found in the patients seeking fertility testing. ApplicationsStudies of populations in which men are seeking infertility treatment avoid this problem because semen analysis is a key part of their fertility evaluation. Peer reviewIt is a descriptive study that analyzes the semen of 78 male partners of infertile couples who had infertility for more than 1 year and the controls who were 52 healthy semen donors of proven fertility.
REFERENCES1 World Health Organization. Programme of Maternal and
Child Health and Family Planning Unit. Infertility: a tabula-tion of available data on prevalence of primary and second-ary infertility. Geneva: World Health Organization, 1991
2 Bhasin S, de Kretser DM, Baker HW. Clinical review 64: Pathophysiology and natural history of male infertility. J Clin Endocrinol Metab 1994; 79: 1525-1529 [PMID: 7989450 DOI: 10.1210/jc.79.6.1525]
3 Mieusset R, Bujan L. Testicular heating and its possible contributions to male infertility: a review. Int J Androl 1995; 18: 169-184 [PMID: 7591190 DOI: 10.1111/j.1365-2605.1995.tb00408.x]
4 Barden-O'Fallon J, Suchindran C, Tsui AO. Validating the self-reported fertility status of rural Malawian women. Am J Hum Biol 2006; 18: 214-218 [PMID: 16493633 DOI: 10.1002/ajhb.20485]
5 Barden-O'Fallon J. Associates of self-reported fertility status and infertility treatment-seeking in a rural district of Ma-lawi. Hum Reprod 2005; 20: 2229-2236 [PMID: 15802313 DOI: 10.1093/humrep/dei008]
6 Savage OM. Artificial donor insemination in Yaounde: some socio-cultural considerations. Soc Sci Med 1992; 35: 907-913 [PMID: 1411691 DOI: 10.1016/0277-9536(92)90105-Y]
7 Bonde JP, Ernst E, Jensen TK, Hjollund NH, Kolstad H, Henriksen TB, Scheike T, Giwercman A, Olsen J, Skak-kebaek NE. Relation between semen quality and fertility: a population-based study of 430 first-pregnancy planners. Lancet 1998; 352: 1172-1177 [PMID: 9777833 DOI: 10.1016/S0140-6736(97)10514-1]
183 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 2 Different semen parameters
Controls Participants P value
Volume (mL) 3.52 ± 0.17 1.8 ± 0.23 < 0.05Concentration (106/mL) 56.89 ± 4.34 34.21 ± 6.45 < 0.05Total motility (%) 82.56 ± 4.32 76.45 ± 8.95 > 0.05Progressive motility (%) 59.92 ± 3.54 44.34 ± 4.56 < 0.05Normal morphology (%) 19.12 ± 2.45 7.35 ± 4.45 < 0.05
COMMENTS
Lampiao F et al . Characteristics of semen parameters of Malawian men

8 World Health Organization. WHO laboratory manual for the examination of human semen and sperm-cervical mucus interaction. 4th ed. Cambridge: Cambridge University Press, 1999
9 Kruger TF, Acosta AA, Simmons KF, Swanson RJ, Matta JF, Oehninger S. Predictive value of abnormal sperm morpholo-gy in in vitro fertilization. Fertil Steril 1988; 49: 112-117 [PMID: 3335257]
10 Irvine S, Cawood E, Richardson D, MacDonald E, Aitken J. Evidence of deteriorating semen quality in the United Kingdom: birth cohort study in 577 men in Scotland over 11 years. BMJ 1996; 312: 467-471 [PMID: 8597676 DOI: 10.1136/bmj.312.7029.467]
11 Swan SH, Elkin EP, Fenster L. Have sperm densities de-clined? A reanalysis of global trend data. Environ Health Perspect 1997; 105: 1228-1232 [PMID: 9370524 DOI: 10.1289/ehp.971051228]
12 Kruger TF, Franken DR, Stander E, Swart Y, Van der Merwe JP. Effect of semen characteristics on pregnancy rate in a
gamete intrafallopian transfer program. Arch Androl 1993; 31: 127-131 [PMID: 8215692 DOI: 10.3109/01485019308988390]
13 Kruger TF, Menkveld R, Stander FS, Lombard CJ, Van der Merwe JP, van Zyl JA, Smith K. Sperm morphologic features as a prognostic factor in in vitro fertilization. Fertil Steril 1986; 46: 1118-1123 [PMID: 2946611]
14 van der Merwe JP, Kruger TF, Swart Y, Lombard CJ. The role of oocyte maturity in the treatment of infertility because of teratozoospermia and normozoospermia with gamete intrafallopian transfer. Fertil Steril 1992; 58: 581-586 [PMID: 1521655]
15 Abu Hassan Abu D, Franken DR, Hoffman B, Henkel R. Ac-curate sperm morphology assessment predicts sperm func-tion. Andrologia 2012; 44 Suppl 1: 571-577 [PMID: 22040054 DOI: 10.1111/j.1439-0272.2011.01229.x]
16 Bablok L, Dziadecki W, Szymusik I, Wolczynski S, Kurzawa R, Pawelczyk L, Jedrzejczak P, Hanke W, Kaminski P, Wiel-gos M. Patterns of infertility in Poland - multicenter study. Neuro Endocrinol Lett 2011; 32: 799-804 [PMID: 22286797]
P- Reviewers: Inês Rosa M, Khajehei M S- Editor: Gou SX L- Editor: Roemmele A E- Editor: Zheng XM
184 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Lampiao F et al . Characteristics of semen parameters of Malawian men

Pelvic arterial embolization in obstetric hemorrhage
Vidhi Chaudhary, Poonam Sachdeva, Raksha Arora, Devender Kumar, Priya Karanth
Vidhi Chaudhary, Poonam Sachdeva, Raksha Arora, Dev-ender Kumar, Priya Karanth, Department of Obstetrics and Gynecology, Maulana Azad Medical College and associated Lok Nayak Hospital and GB Pant Hospital, New Delhi 110002, IndiaAuthor contributions: Chaudhary V designed study and wrote the manuscript; Arora R, Sachdeva P, Kumar D, Chaudhary V and Karanth P were involved in medical, surgical and conserva-tive management of patients and helped in editing of article; Chaudhary V and Karanth P collected all the data including fol-low up of the patients and searched articles to support this work.Correspondence to: Dr. Vidhi Chaudhary, Senior Resident, Department of Obstetrics and Gynecology, Maulana Azad Medi-cal college and Lok Nayak Hospital, Bahadur Shah Zafar Marg, New Delhi 110002, India. [email protected]: +91-11-23239271 Received: April 29, 2013 Revised: July 3, 2013Accepted: July 17, 2013Published online: November 10, 2013
AbstractAIM: To analyze safety and efficacy of pelvic arterial embolization (PAE) in preventing and treating obstetri-cal hemorrhage.
METHODS: A consecutive study of eight cases under-going pelvic artery embolization from January 2010 to October 2012 in Department of Obstetric and Gynecol-ogy of Maulana Azad Medical College for intractable obstetric hemorrhage was done. All embolization were carried out in cath lab of cardiology Department at as-sociated GB Pant Hospital.
RESULTS: Clinical success was defined as arrest of bleeding after PAE without need for repeat PAE or ad-ditional surgery which was 75% in our series. PAE was successful in controlling obstetrical hemorrhage in all except one who had mortality. Other had hysterectomy due to secondary hemorrhage. Five resumed menstrua-tion. None of the women intended to conceive, hence are practicing contraception.
CONCLUSION: PAE is minimally invasive procedure
which should be offered early for hemostasis in intracta-ble obstetrical haemorrhage unresponsive to uterotonic. It is a fertility sparing option with minor complications.
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Key words: Pelvic artery embolization; Uterine artery embolization; Obstetric hemorrhage; Placenta accreta; Post partum hemorrhage
Core tip: Historically obstetric hysterectomy was defini-tive treatment in morbid adherent placenta, cervical ectopic pregnancy and post partum hemorrhage refrac-tory to medical and conservative surgical measures. Emergence of Pelvic arterial embolization as a mini-mally invasive procedure had led to alternative use of use of embolizing agents in controlling significant hem-orrhage in various etiologies of obstetric hemorrhage thereby conserving fertility and reducing maternal mortality and morbidity. We used P- particle and coil as embolizing material with 75% success in our series. Our study further strengthens our confidence in pelvic artery embolization for its applicability in managing ob-stetric hemorrhage.
Chaudhary V, Sachdeva P, Arora R, Kumar D, Karanth P. Pelvic arterial embolization in obstetric hemorrhage. World J Obstet Gynecol 2013; 2(4): 185-191 Available from: URL: http://www.wjgnet.com/2218-6220/full/v2/i4/185.htm DOI: http://dx.doi.org/10.5317/wjog.v2.i4.185
INTRODUCTIONPelvic arterial embolization (PAE) mainly uterine (UAE) or internal iliac artery is minimally invasive angiographic procedure which is used prophylactically and therapeuti-cally in controlling obstetric hemorrhage (OH). Major causes of obstetrical hemorrhage include post partum hemorrhage (PPH), abnormal placentation, abruptio
BRIEF ARTICLE
185 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Online Submissions: http://www.wjgnet.com/esps/[email protected]:10.5317/wjog.v2.i4.185
World J Obstet Gynecol 2013 November 10; 2(4): 185-191ISSN 2218-6220 (online)
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
World Journal ofObstetrics and GynecologyW J O G

placenta, ectopic pregnancy and incomplete abortion[1,2]. PPH has been managed by uterine massage, uterotonics and packing. In refractory cases uterine suturing, step-wise vascular ligation and finally hysterectomy has been employed[3]. Placenta accreta and cervical pregnancy have been dealt by hysterectomy in past which causes loss of reproductive potential. PAE has emerged as a safe and effective alternative to surgery in controlling obstetric hemorrhage[4]. Ever since its first use by Brown et al[5], many have reported high success rates of PAE in obstet-rical hemorrhage[6-8]. The purpose of this study was to evaluate the efficacy and safety of PAE in treatment of obstetric hemorrhage and analyze its outcomes.
MATERIALS AND METHODSA consecutive study of eight cases undergoing emboliza-tion from January 2010 to October 2012 in Department of Obstetric and Gynecology of Maulana Azad Medical College for obstetric hemorrhage was done. Study was approved by our institutional review board. Causes of hemorrhage, comorbidities, preembolization treatments, technique, outcome and complications of embolization were analyzed. All embolization were done in cath lab of cardiology Department at associated GB Pant Hospital.
Eight cases underwent embolization for obstetrical emergencies (Table 1). Initial assessment and resuscitation were carried at our obstetric unit. Hemodynamic status, comorbidities, and presence or absence of disseminated intravascular coagulopathy (DIC) were assessed. The shock was managed by administration of crystalloid or
colloid and transfusion of specific blood units. Obstetric assessment included inspection of the vagina, cervix, and perineum for lacerations, hematomas and exploration of the uterine cavity for retained products. A multispecialty team including obstetric consultant, intensive care anes-thetist and cardiologist decided the need for embolization after informed consent. The criteria for selection were active hemorrhage, deterioration of hemodynamic or clotting status despite treatment and high risk cases with anticipated hemorrhage. Angiography under C-arm was performed. Bilateral femoral approach using 5-French femoral arterial introducer was used. The internal iliac artery and uterine artery were catheterized via two punc-ture sites (one on each side). Angiography was performed to detect the site of bleeding from pelvic arteries. Highly selective angiography of uterine artery was attempted in four patients. Others had embolization of internal iliac artery (anterior branch) due to presence of severe uterine artery spasm not relieved by vasodilators. Coil emboliza-tion was done in all. Three had additional Polyvinyl Al-cohol particle instillation. All except three patients were transferred to intensive care unit (ICU) or high depen-dency obstetric units for management after procedure.
RESULTSMean age was 30.5 years. Five patients had history of previous caesarean and abortions (Table 1). In five cases emergent embolization was done as all had massive hem-orrhage following surgery or delivery despite conservative measures and developed coagulopathy (Table 2). Three
Chaudhary V et al . Embolization for obstetric hemorrhage
186 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 1 Demographic characteristics
Cases Indication Age (yr) Parity Period of gestation Previous sections
Case 1 Cervical ectopic 30 G6P3A2L2, 11 wk 12 wk 2Case 2 Placenta percreta 28 G3P2L1 36 wk 1Case 3 Placenta percreta 38 P3L3 28 wk 3Case 4 Placenta accreta 30 G3P1L1A1 27 wk 1Case 5 Placenta accreta 30 G3P1L1A1 36 wk + 5 d 1Case 6 PPH (Atonic + traumatic) 30 G2P1L1 36 wk -Case 7 PPH (Atonic + traumatic) 30 PRIMI 36 wk -Case 8 PPH (Atonic + traumatic) 28 G3P2L1 40 wk -
PPH: Post partum hemorrhage.
Table 2 Clinical characteristics
Cases Shock Comorbidity Blood loss (mL) Coagulopathy Mode of Delivery
Case 1 - - 1300 - NACase 2 - Anaemia 300 - Classical csCase 3 + Anaemia 1000 + Classical csCase 4 + Anaemia 1500 + Classical csCase 5 - Anaemia 500 - Classical csCase 6 + Anaemia, precipitate labor 1000 + NVDCase 7 + Jaundice, anaemia 1500 + NVDCase 8 + - 2500 + Forceps
NVD: Normal vaginal delivery; NA: Not applicable.

had Prophylactic embolization for cervical ectopic and after classical section for placenta accreta percreta (n = 2). Conservative measures were uterotonic, cervical and vaginal tear repair in delivered cases and classical section with leaving placenta in situ for placenta accreta.
All but one had primary hemorrhage. Secondary hem-orrhage occurred on day forty post classical preterm sec-tion done for placenta percreta. Six patients were mod-erately anaemic. Five patients were build up to adequate levels by packed cell transfusion prior to labor or section. Other presented in shock due to secondary hemorrhage and had correction after emergent embolization. All ad-herent placentas were previa as diagnosed by Doppler ultrasound and supplemented by magnetic resonance im-aging (MRI) in two cases. All underwent conservative sur-gical management with embolization. One had secondary hemorrhage post classical section which responded to primary embolization. Placenta resorbed in all.
Three cases underwent embolization for Atonic and traumatic PPH due to cervical tears unresponsive to uterotonic and repair (Table 3). Emergent CT revealed unilateral broad ligament hematoma in two. Both had massive blood loss following delivery. Traumatic PPH was initially controlled in first. Constant trickling reap-peared after twenty hours, so underwent embolization while on ventilatory support. Bleeding stopped and hematoma resolved spontaneously. Second case under-went immediate embolization due to persistent bleeding despite repair, with success. Third case had massive PPH following forceps delivery and had cardiac arrest forty minutes later because of hemorrhagic shock and was on ventilatory support. Clinically pelvic hematoma was suspected as evident by uterine deviation and abdominal fullness. Poor general condition prevented immediate imaging and surgical intervention. Patient was shifted to ICU where bleeding continued and hematocrit continued to fall in spite of blood transfusion. Emergency CECT pelvis revealed left supra-levator pelvic hematoma of size 12 cm × 10 cm. Patient underwent embolization but had cardiac arrest and expired shortly. Arrest was not re-lated to embolization. Five patients were in coagulopathy which was corrected in two prior to embolization. Three underwent emergent PAE in coagulopathy unresponsive to conservative measures and had ongoing correction
during and after embolization with success. Post embolization angiogram revealed arrest of bleed-
ing in all patients (Figure 1). Transfusion was required in all patients. No major complications during or post em-bolization was noted. Minor complications were fever (n = 2), mild groin pain (n = 2) and correctable sepsis (Table 4). Initially, PAE was successful in controlling hemor-rhage and partial resolution of cervical ectopic as evident by falling beta- HCG levels. Patient presented with sec-ondary intractable hemorrhage on day twenty one and hysterectomy was undertaken as there was technical dif-ficulty in shifting to cath lab.
Clinical success was defined as cessation of bleed-ing after PAE without need for repeat PAE or additional surgery. PAE was successful in controlling obstetrical hemorrhage in all except one who had mortality as this patient was severely hemodynamically compromised. One required hysterectomy due to secondary hemor-rhage. Clinical success in our series was 75%. In six cases mean time was three hours and twenty four hours in two. Five resumed menstruation and two are at present lost to follow up. None of the women intended to conceive, hence are practicing contraception.
DISCUSSIONObstetrical hemorrhage is a major cause of maternal mor-bidity and mortality worldwide. PPH is major contribu-tor[1]. Primary PPH is defined as excessive bleeding from genital tract of 500 mL or more in first 24 h following delivery[4]. Management is centered on administration of uterotonic, uterine packing and conservative surgical ves-sel ligations. Internal-iliac-artery ligation may not be effec-tive in controlling severe PPH in half of patients as blood flow in the distal vessel is decreased to 48% due to rich collateral network. Uterine artery ligation has 80% success in uterine atony, but is less effective in placenta accreta. Last resort is hysterectomy which causes significant mor-bidity and loss of reproductive potential. With advances in interventional radiology, PAE has emerged as an accepted option in refractory PPH[9]. Its advantage lies in its high success rates relative to ligation and hysterectomy[10].
Embolization was first used in 1972 to control arterial bleeding in pelvic fractures. First successful use of femo-
187 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Table 3 Procedural characteristics
Cases Type of embolization Type Additional treatment Time from presentation to start of embolization Embolic agent
Case 1 Uterine Prophylactic Methotrexate 4 h Coil + PVA particleCase 2 Uterine Prophylactic Methotrexate + uterotonic 3 h CoilCase 3 Uterine Emergency Methotrexate + uterotonic 1 h Coil+PVACase 4 Internal iliac artery Emergency Methotrexate + uterotonic 1 h CoilCase 5 Uterine artery Prophylactic Methotrexate + uterotonic 30 min Coil + PVACase 6 Internal iliac artery Emergency Uterotonic + cervical tear repair 2 h CoilCase 7 Internal iliac artery Emergency Uterotonic + cervical tear repair 22 h CoilCase 8 Internal iliac artery Emergency Uterotonic + cervical tear repair 26 h Coil
PVA: Polyvinyl alcohol.
Chaudhary V et al . Embolization for obstetric hemorrhage

thirty-five women with intractable PPH. Hemostatic em-bolization of uterine arteries was performed in all includ-ing two cases which underwent hysterectomy. Bleeding stopped immediately. Two patients required repeat embo-lization. Delayed hysterectomy was undertaken in case of placenta accreta[6]. Lee et al[8] published largest retrospec-tive single-center study in women who underwent PAE
ral transcatheter pelvic arterial embolization in PPH was described by Brown in 1979[5]. The reported success rate of UAE is over 90% to 100% in PPH due to atony[6,11]. Arterial embolization is performed at a more distal and specific location than vessel ligation which prevents bleeding through collaterals. Pelage et al[6] evaluated the efficacy and safety of selective arterial embolization in
188 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Post embolization
Post embolizationlack of vascularity
Pre embolization
Uterine artery
Left side
Right side
Uterine artery
Figure 1 Pre and post embolization Angiogram showing arrest of flow through uterine arteries after selective uterine artery embolization.
Table 4 Outcomes
Cases Hemorrhage controlled
Rebleeding after
embolization
hysterectomy Transfusion of blood and
its products
Post embolization fever
Sepsis Groin pain Resumption of menstrual cycles
Mortality
Case 1 + + + + - - _ - -Case 2 + - - + + (Non embolization) + (UTI) + + -Case 3 + Mild,
Hemostatics uterotonics
- + + - _ + -
Case 4 + + Mild, Hemostaticsuterotonics
- + - - _ - -
Case 5 + Mild, Hemostaticsuterotonic
- + - - _ + -
Case 6 + - - + +Non embolization cause
+ UTI, Puerperal Sepsis post exploration
+ + -
Case 7 + - - + + - _ + -Case 8 Expired after
embolizationNot applicable +
UTI: Urinary tract infection.
Chaudhary V et al . Embolization for obstetric hemorrhage

for primary PPH in terms of efficacy and factors associ-ated with failure of embolization procedure. Thirty-two patients had a clinical diagnosis of DIC. Overall bleeding control was achieved in 98.0% of the patients. Clinical success was 86.5%. Bleeding vessels, commonly bilateral uterine arteries as seen on angiography were embolized.
Embolization has a significant success in Secondary PPH. It is defined as excessive bleeding from the genital tract, with a blood loss of 500 mL or more, occurring af-ter the first 24 h following delivery until the 6th-12th week of the puerperium. It affects 1%-3% of all deliveries[7]. Secondary PPH is managed with uterotonics and curet-tage. If bleeding persists vascular ligation or hysterecto-my is required. Hence, transcatheter embolization of the uterine or pelvic arteries is an alternative in controlling secondary hemorrhage. Its first successful use was de-scribed by Pelage et al[7] in fourteen women unresponsive to uterotonic drugs or uterine curettage. We in one case of secondary hemorrhage in conservatively managed pla-centa percreta used UAE with success.
Angiographic embolization is effective in managing obstetric hemorrhage due to pelvic hematomas. It is dif-ficult to identify bleeding vessel during exploration of he-matoma due to friable genital tissues. Obstetrician must repair cervical and vaginal tears and correct coagulopathy prior to embolization to achieve therapeutic success[2,8]. But with ongoing hemorrhage and coagulopathy, emer-gent embolization can be used as it stems hemorrhage and causes hematoma resolution, facilitates uterine con-tractions releasing procoagulant factors into circulation[8]. Deux reported rapid improvement in clotting disorders and hemodynamic status after PAE[2]. Therapeutic suc-cess was 96%. Vascular spasms were dealt with injecting vasodilator thereby allowing selective catheterization[6,12].
Abnormal placentation is one of the etiological fac-tors in intractable PPH. Placenta accreta is characterized by villi abnormally adherent to the myometrium due to the absence or defects in the normal decidual basalis and fibrinous Nitabuch layer[13,14]. Recently, rate of placenta accreta has increased in conjunction with the rate of ce-sarean deliveries at a frequency of 1 per 2500[15]. Placenta accreta has become leading cause of failed vessel ligation and peripartum hysterectomy[13,15]. Presence of placenta previa and prior cesarean delivery exponentially increases the risk. Antenatal diagnosis by doppler ultrasound or MRI allows either scheduled conservative management or hysterectomy thereby decreasing morbidity[15]. Man-agement recommended is a cesarean-hysterectomy with placenta in situ in multiparous women not willing to conceive[16,17]. However hysterectomy is associated with significant morbidity like bladder and ureteric injury and renders woman sterile. Recent literature shows that leav-ing adherent placenta in utero followed by embolization avoids hysterectomy, maintains fertility with successful pregnancies in women desirous to conceive[18]. Leaving placenta in situ may result in infection and secondary PPH, which are dealt with appropriate antibiotics and repeat embolization. In a large multicenter study by Sen-
tilhes et al[13] conservative methods were successful in avoiding hysterectomy in 78.4% of women, with a severe maternal morbidity rate of only 6%. In subsequent fol-low up of women contacted, 92% resumed menstrua-tion. Eighty-eight point nine percent of women achieved successful pregnancy among who wished to conceive. Placenta accreta recurred in 28% of cases. They con-cluded conservative treatment for placenta accreta doesn’t compromise patients’ subsequent fertility or obstetric outcome[17]. Prophylactic insertion of balloon catheters before cesarean section is effective method in control-ling anticipated bleeding[19]. Embolization can be carried out without delay after uterine closure. We in two cases of adherent placenta carried prophylactic embolization immediately after classical section. It had less blood loss, surgery time and minimal complication. Methotrexate has been proposed as adjuvant treatment to hasten the post-partum involution of the uterus. No evidence currently supports its efficacy in conservative management of ac-creta. All our cases of adherent placenta received metho-trexate with no complications. We believe conservative approach has less morbidity and preserves reproductive function and should remain first line management in ad-herent placenta.
Embolization is an emerging modality in conservative management of cervical ectopic. On reviewing litera-ture PAE with methotrexate is effective in reducing the ectopic cervical mass. There is always a risk of haemor-rhage which can be dealt with repeat PAE. Hysterectomy should be last resort if all conservative methods fail[20].
Clinical success of PAE for treatment of severe PPH lies in rapid transfer and timely decision for embolization. The time from decision for embolization to achievement of hemostasis should be in the order of 2-6 h[21].
Several prognostic factors are associated with clini-cal success of embolization. Shock, DIC, Massive blood transfusion, genital tears, caesarean delivery, and placenta accreta are poor prognostic factors in embolization in different case series[6,8,22]. Lee et al[8] showed that DIC and massive transfusion of more than ten red blood cell units were significantly related to clinical failure.
Abnormal placentation accounts for over half of the failures of UAE[6]. Failure is thought to be due to myo-metrial injury caused by difficult digital separation of the placenta. Massen performed juxta renal angiogram in UAE failures and occluded ovarian arteries in PPH[23]. PAE after a failed surgical procedure is not associated with unfavorable clinical outcome[24]. In our series em-bolization was successful in patients with hemodynamic shock, coagulopathy, abnormal placentation and prevent-ed morbidity. PAE should be considered in hemodynami-cally unstable patients and in patients with coagulopathies but these patients require close monitoring in an ICU set up.
Embolization is associated with complications. Minor complications are pain, transient fever, mild transient numbness of the buttock, foot or thigh, hematoma for-mation at the site of common femoral artery puncture,
189 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Chaudhary V et al . Embolization for obstetric hemorrhage

and pelvic infection[11,25]. Lee et al[8] reported asymptom-atic dissection of the uterine artery and edema of the lower legs after PAE with no major complications. Com-plications from embolus migration to general blood cir-culation are very rare. Early intervention in form of con-firmation of embolus by angiogram, anticoagulation and embolectomy can prevent loss of limb or its function[23]. Serious complications like uterine and bladder necrosis, delayed vesicovaginal fistula after PAE are reported[23,25]. Proper informed consent from patient must be taken be-fore embolization.
The effects of PAE on menstruation and fertility are unclear. Successful pregnancies and resumption of menstruation have been reported unanimously in many case series studying long term effects of PAE[12,17,26-28]. Lee et al[8] reported resumption of regular menstruation in 97.3% of women after PAE. Sentilhes et al[12] analyzed sixty eight women who underwent embolization for PPH. 92% resumed menstruation. Those who desired pregnancy were able to conceive. Delotte in his review article included thirteen articles. Fertility follow-up of a total of one sixty eight women after PAE were analyzed. Clinical success of embolization was in 92%. Total forty five pregnancies were described of which thirty two cases resulted in live births[28]. Embolization doesn’t seem to af-fect fertility and menstruation.
In conclusion, we present two failures and six suc-cesses in various etiologies of obstetric hemorrhage in our series. Correction of shock and DIC increases suc-cess but embolization should not be delayed while at-tempting to correct above. Embolization should be done in rebleeding. Non selective embolization of anterior branch of internal iliac artery can be attempted if there is technical difficulty in accessing uterine artery in vascular spasm. It has similar efficacy and has minimal complica-tions. We believe planned embolization in case of morbid adherent placenta irrespective of parity leads to less mor-bidity and early recovery. Caesarean hysterectomy should be an alternative choice if embolization fails in morbid adherent placenta. Use of embolization as last resort is to be discouraged and should be early means of hemostasis in obstetric hemorrhage unresponsive to uterotonic.
Pelvic arterial embolization is minimally invasive pro-cedure in modern obstetrics, which is a safe alternative to surgical methods in conditions causing intractable ob-stetrical hemorrhage and is a fertility sparing option with minor complications.
COMMENTSBackground Uterine artery embolization in obstetrics was first described by Pelage et al in primary postpartum hemorrhage. Subsequently its use in obstetrics have been extended to embolization of pelvic arteries in management of primary and sec-ondary post partum hemorrhage ,traumatic hemorrhage, placenta accreta and cervical ectopics thereby conserving fertility and reducing morbidity.Research frontiersPelvic arterial embolization immediately stems hemorrhage arising from pelvic arteries and has emerged an effective hemostatic option in developing coun-
tries at tertiary level hospital. Research area is directed towards long term ef-fects of embolization for which randomized control data is needed.Innovations and breakthroughsAuthors’ paper highlights the clinical success in managing cases with obstetric hemorrhage using embolization which otherwise might have needed hysterec-tomy. Its advantage lies in its high success rates relative to ligation and hyster-ectomy in controlling hemorrhage.ApplicationsPelvic arterial embolization (PAE) can be applied as minimally invasive choice in post partum hemorrhage refractory to medical measures, prior to classical section in placenta accreta and in live cervical ectopics. Hemodynamic instabil-ity should not be considered a contraindication for PAE. TerminologyPelvic arterial Embolization- embolization of internal iliac, uterine artery and its branches using polyvinyl alcohol particles or coil. Peer reviewThis study was a case series to assess efficacy of PAE for varying etiologies of obstetric hemorrhage. It was a useful intervention option in hemorrhaging pa-tients as it stemmed hemorrhage, reduced surgical morbidity, thereby conserv-ing fertility in 75% of the patients.
REFERENCES1 Al-Zirqi I, Vangen S, Forsen L, Stray-Pedersen B. Preva-
lence and risk factors of severe obstetric haemorrhage. BJOG 2008; 115: 1265-1272 [PMID: 18715412 DOI: 10.1111/j.1471-0528.2008.01859.x]
2 Deux JF, Bazot M, Le Blanche AF, Tassart M, Khalil A, Berkane N, Uzan S, Boudghène F. Is selective emboliza-tion of uterine arteries a safe alternative to hysterectomy in patients with postpartum hemorrhage? AJR Am J Roent-genol 2001; 177: 145-149 [PMID: 11418416 DOI: 10.2214/ajr.177.1.1770145]
3 AbouZahr C, Wardlaw T. Maternal mortality in 2000: esti-mates developed by WHO, UNICEF and UNFPA. Geneva: World Health Organization, 2004
4 Gonsalves M, Belli A. The role of interventional radiology in obstetric hemorrhage. Cardiovasc Intervent Radiol 2010; 33: 887-895 [PMID: 20464555 DOI: 10.1007/s00270-010-9864-4]
5 Brown BJ, Heaston DK, Poulson AM, Gabert HA, Mineau DE, Miller FJ. Uncontrollable postpartum bleeding: a new approach to hemostasis through angiographic arterial em-bolization. Obstet Gynecol 1979; 54: 361-365 [PMID: 314075]
6 Pelage JP, Le Dref O, Mateo J, Soyer P, Jacob D, Kardache M, Dahan H, Repiquet D, Payen D, Truc JB, Merland JJ, Rymer R. Life-threatening primary postpartum hemorrhage: treat-ment with emergency selective arterial embolization. Radiol-ogy 1998; 208: 359-362 [PMID: 9680559]
7 Pelage JP, Soyer P, Repiquet D, Herbreteau D, Le Dref O, Houdart E, Jacob D, Kardache M, Schurando P, Truc JB, Ry-mer R. Secondary postpartum hemorrhage: treatment with selective arterial embolization. Radiology 1999; 212: 385-389 [PMID: 10429694]
8 Lee HY, Shin JH, Kim J, Yoon HK, Ko GY, Won HS, Gwon DI, Kim JH, Cho KS, Sung KB. Primary postpartum hem-orrhage: outcome of pelvic arterial embolization in 251 patients at a single institution. Radiology 2012; 264: 903-909 [PMID: 22829685 DOI: 10.1148/radiol.12111383]
9 Arulkumaran S, Walker JJ, Watkinson AF, Nicholson T, Kessel D, Patel J. The role of emergency and elective in-terventional radiology in postpartum hemorrhage. Royal College of Obstetricians and Gynaecologists Good Practice Guideline, 2007-01-06, cited 2013-10-06. Available from: URL: http: //www.rcog.org.uk/womenshealth/clinicaL-guidance/roleemergency-and-electiveinterventional-radiol-ogy- postpartum-haem
10 Pelage JP, Limot O. [Current indications for uterine artery embolization to treat postpartum hemorrhage]. Gynecol Ob-
190 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
COMMENTS
Chaudhary V et al . Embolization for obstetric hemorrhage

stet Fertil 2008; 36: 714-720 [PMID: 18656414 DOI: 10.1016/j.gyobfe.2008.06.004]
11 Soncini E, Pelicelli A, Larini P, Marcato C, Monaco D, Gri-gnaffini A. Uterine artery embolization in the treatment and prevention of postpartum hemorrhage. Int J Gynaecol Obstet 2007; 96: 181-185 [PMID: 17286979 DOI: 10.1016/j.ijgo.2006.12.010]
12 Sentilhes L, Gromez A, Clavier E, Resch B, Verspyck E, Marpeau L. Fertility and pregnancy following pelvic arterial embolisation for postpartum haemorrhage. BJOG 2010; 117: 84-93 [PMID: 19832826 DOI: 10.1111/j.1471-0528.2009.02381.x]
13 Sentilhes L, Ambroselli C, Kayem G, Provansal M, Fernan-dez H, Perrotin F, Winer N, Pierre F, Benachi A, Dreyfus M, Bauville E, Mahieu-Caputo D, Marpeau L, Descamps P, Gof-finet F, Bretelle F. Maternal outcome after conservative treat-ment of placenta accreta. Obstet Gynecol 2010; 115: 526-534 [PMID: 20177283 DOI: 10.1097/AOG.0b013e3181d066d4]
14 Hull AD, Resnik R. Placenta accreta and postpartum hemorrhage. Clin Obstet Gynecol 2010; 53: 228-236 [PMID: 20142659 DOI: 10.1097/GRF.0b013e3181ce6aef]
15 Tikkanen M, Paavonen J, Loukovaara M, Stefanovic V. An-tenatal diagnosis of placenta accreta leads to reduced blood loss. Acta Obstet Gynecol Scand 2011; 90: 1140-1146 [PMID: 21488840 DOI: 10.1111/j.1600-0412.2011.01147.x]
16 Placenta accreta. ACOG Committee Opinion No. 266. Ameri-can College of Obstetricians and Gynecologists. Int J Gynecol Obstet 2002; 77: 77–78 [DOI: 10.1016/S0020-7292(02)80003-0]
17 Sentilhes L, Kayem G, Ambroselli C, Provansal M, Fernan-dez H, Perrotin F, Winer N, Pierre F, Benachi A, Dreyfus M, Bauville E, Mahieu-Caputo D, Marpeau L, Descamps P, Bretelle F, Goffinet F. Fertility and pregnancy outcomes following conservative treatment for placenta accreta. Hum Reprod 2010; 25: 2803-2810 [PMID: 20833739 DOI: 10.1093/humrep/deq23]
18 Provansal M, Courbiere B, Agostini A, D’Ercole C, Boubli L, Bretelle F. Fertility and obstetric outcome after con-servative management of placenta accreta. Int J Gynaecol Obstet 2010; 109: 147-150 [PMID: 20152971 DOI: 10.1016/j.ijgo.2009.12.011]
19 Ojala K, Perälä J, Kariniemi J, Ranta P, Raudaskoski T, Tekay A. Arterial embolization and prophylactic catheter-ization for the treatment for severe obstetric hemorrhage*. Acta Obstet Gynecol Scand 2005; 84: 1075-1080 [PMID: 16232175 DOI: 10.1111/j.0001-6349.2005.00727.x]
20 Hirakawa M, Tajima T, Yoshimitsu K, Irie H, Ishigami K, Yahata H, Wake N, Honda H. Uterine artery embolization along with the administration of methotrexate for cervical ectopic pregnancy: technical and clinical outcomes. AJR Am J Roentgenol 2009; 192: 1601-1607 [PMID: 19457824 DOI: 10.2214/AJR.08.1921]
21 Boulleret C, Chahid T, Gallot D, Mofid R, Tran Hai D, Ravel A, Garcier JM, Lemery D, Boyer L. Hypogastric arte-rial selective and superselective embolization for severe postpartum hemorrhage: a retrospective review of 36 cases. Cardiovasc Intervent Radiol 2004; 27: 344-348 [PMID: 15129337 DOI: 10.1007/s00270-003-2698-6]
22 Poujade O, Zappa M, Letendre I, Ceccaldi PF, Vilgrain V, Lu-ton D. Predictive factors for failure of pelvic arterial emboli-zation for postpartum hemorrhage. Int J Gynaecol Obstet 2012; 117: 119-123 [PMID: 22361480 DOI: 10.1016/j.ijgo.2011.11.025]
23 Maassen MS, Lambers MD, Tutein Nolthenius RP, van der Valk PH, Elgersma OE. Complications and failure of uterine artery embolisation for intractable postpartum haemor-rhage. BJOG 2009; 116: 55-61 [PMID: 19016685 DOI: 10.1111/j.1471-0528.2008.01939.x]
24 Sentilhes L, Gromez A, Clavier E, Resch B, Verspyck E, Mar-peau L. Predictors of failed pelvic arterial embolization for se-vere postpartum hemorrhage. Obstet Gynecol 2009; 113: 992-999 [PMID: 19384113 DOI: 10.1097/AOG.0b013e3181a114f7]
25 Porcu G, Roger V, Jacquier A, Mazouni C, Rojat-Habib MC, Girard G, Pellegrin V, Bartoli JM, Gamerre M. Uterus and bladder necrosis after uterine artery embolisation for postpartum haemorrhage. BJOG 2005; 112: 122-123 [PMID: 15663413 DOI: 10.1111/j.1471-0528.2005.00306.x]
26 Chauleur C, Fanget C, Tourne G, Levy R, Larchez C, Sef-fert P. Serious primary post-partum hemorrhage, arterial embolization and future fertility: a retrospective study of 46 cases. Hum Reprod 2008; 23: 1553-1559 [PMID: 18460450 DOI: 10.1093/humrep/den122]
27 Gaia G, Chabrot P, Cassagnes L, Calcagno A, Gallot D, Bo-tchorishvili R, Canis M, Mage G, Boyer L. Menses recovery and fertility after artery embolization for PPH: a single-center retrospective observational study. Eur Radiol 2009; 19: 481-487 [PMID: 18766350 DOI: 10.1007/s00330-008-1140-5]
28 Delotte J, Novellas S, Koh C, Bongain A, Chevallier P. Ob-stetrical prognosis and pregnancy outcome following pelvic arterial embolisation for post-partum hemorrhage. Eur J Ob-stet Gynecol Reprod Biol 2009; 145: 129-132 [PMID: 19398259 DOI: 10.1016/j.ejogrb.2009.03.013]
P- Reviewers: TinelliA, Wang PH, Zhang XQ S- Editor: Wen LL L- Editor: A E- Editor: Lu YJ
191 November 10, 2013|Volume 2|Issue 4|WJOG|www.wjgnet.com
Chaudhary V et al . Embolization for obstetric hemorrhage

Published by Baishideng Publishing Group Co., LimitedFlat C, 23/F., Lucky Plaza,
315-321 Lockhart Road, Wan Chai, Hong Kong, ChinaFax: +852-65557188
Telephone: +852-31779906E-mail: [email protected]
http://www.wjgnet.com
© 2013 Baishideng Publishing Group Co., Limited. All rights reserved.
Related Documents